Elaine Tran and Kevin Tang are Medical Students; David Rivera and Jorge Rivera are Clinical Assistant Professors of Surgery (Ophthalmology); and Paul Greenberg is a Professor of Surgery (Ophthalmology); all at the Warren Alpert Medical School of Brown University in Providence, Rhode Island. Allison Chen is an Ophthalmology Resident at the Shiley Eye Institute, University of California San Diego Health in La Jolla. Michael Chen is a Student at Harvard University in Cambridge, Massachusetts. David Rivera and Jorge Rivera are Staff Ophthalmologists, and Paul Greenberg is Chief of Ophthalmology; all at the Providence Veterans Affairs Medical Center in Rhode Island. Correspondence: Paul Greenberg (paul_greenberg@brown.edu)
Author disclosures The authors report no actual or potential conflicts of interest for this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
Background : Refractive outcomes for cataract surgery with toric intraocular lenses (IOLs) are not well described in a teaching hospital setting. This study investigated the refractive outcomes of cataract surgery with toric IOLs at an academic-affiliated Veterans Affairs Medical Center (VAMC) and compared the accuracy of 2 biometric formulae for toric IOL power calculation.
Methods: A retrospective chart review of patients who received cataract surgery with toric IOLs from November 2013 to May 2018 was conducted. The Holladay 2 and Barrett toric IOL formulae were used to predict the postoperative refraction for each cataract surgery. The main outcome measures were best-corrected visual acuity (BCVA) and the difference in cylinder between the preoperative and postoperative manifest refractions. The accuracy of each biometric formula was also assessed using 2-tailed t tests of the mean absolute error, and subgroup analyses were conducted for short, medium, and long eyes.
Results: Of 325 charts reviewed, 283 patients met the inclusion criteria; 87% (248/283) of these surgeries were performed by resident surgeons. The median postoperative BCVA was 20/20, and 92% of patients had a postoperative BCVA of 20/25 or better. There was no statistically significant difference in mean absolute error between the 2 formulae for the entire axial length range ( P = .21), as well as the short ( P = .94), medium ( P = .49), and long axial length ( P = .08) groups.
Conclusions: To our knowledge, this is the largest study that compared the performance of the Barrett toric and Holladay 2 formulae and the first that made the comparison in a teaching hospital setting. This study suggests that the 2 formulae have similar refractive outcomes across all axial lengths.
Cataract surgery is one of the most common ambulatory procedures performed in the US.1-3 With the aging of the US population, the number of Americans with cataracts is projected to increase from 24.4 million in 2010 to 38.7 million in 2030.4
Approximately 20% of all cataract patients have preoperative astigmatism of > 1.5 diopters (D), underscoring the importance of training residents in the placement of toric intraocular lenses (IOLs).5 However, the implantation of toric IOLs is more challenging than monofocal IOLs, requiring precise surgical alignment of the IOL.6 Successful toric IOL implantation also requires accurate calculation of the IOL cylinder power and target axis of alignment. It is unclear which toric IOL calculation formula offers the most accurate refractive predictions, and practitioners have designed strategies to apply different formulae depending on the biometric dimensions of the target eye.7-9
Previous studies of resident-performed cataract surgery using toric IOLs6,10-13 and studies that compare the performance of the Barrett and Holladay toric formulae have been limited by their small sample sizes (< 107 eyes).7,14-16 Moreover, none of the studies that evaluate the comparative effectiveness of these biometric formulae were conducted at a teaching hospital.7,14-16
Given the added complexity of toric IOL placement and variable surgical experience of residents as ophthalmologists-in-training, it is important to assess outcomes in teaching hospitals.13 The primary aims of this study were to assess the visual and refractive outcomes of cataract surgery using toric IOLs in a US Department of Veterans Affairs (VA) teaching hospital and to compare the relative accuracy of the Holladay 2 or Barrett toric biometric formulae in predicting postoperative refraction outcomes.
Methods
The Providence VA Medical Center (PVAMC) Institutional Review Board approved this study. This retrospective chart review included patients with cataract and corneal astigmatism who underwent cataract surgery using Acrysof toric IOLs, model SN6AT (Alcon) at the PVAMC teaching hospital between November 2013 and May 2018.
Only 1 eye was included from each study subject to avoid compounding of data with the use of bilateral eyes.17 In addition, bilateral cataract surgery was only performed on some patients at the PVAMC, so including both eyes from eligible patients would disproportionately weigh those patients’ outcomes. If both eyes had cataract surgery and their postoperative visual acuities were unequal, we chose the eye with the better postoperative visual acuity since refraction accuracy decreases with worsening best-corrected visual acuity (BCVA). If both eyes had cataract surgery and the postoperative visual acuity was the same, the first operated eye was chosen.17,18
Exclusion criteria included worse than 20/40 BCVA, posterior capsular rupture, sulcus IOL, history of corneal disease, history of refractive surgery (laser-assisted in situ keratomileusis [LASIK]/photorefractive keratectomy [PRK]), axial length not measurable by the Lenstar optical biometer (Haag-Streit USA), or no postoperative refraction within 3 weeks to 4 months.19,20
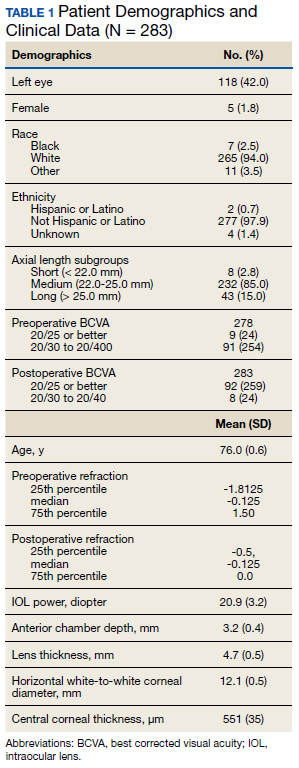
Patient age, race/ethnicity, gender, preoperative refraction, preoperative BCVA, postoperative refraction, postoperative BCVA, and IOL power were recorded from patient charts (Table 1). Preoperative and postoperative refractive values were converted to spherical equivalents. The preoperative biometry and most of the postoperative refractions were performed by experienced technicians certified by the Joint Commission on Allied Health Personnel in Ophthalmology. The main outcomes for the assessment of surgeries included the postoperative BCVA, postoperative spherical equivalent refraction, and postoperative residual refractive astigmatism.
Axial length (AL), preoperative anterior chamber depth (ACD), preoperative flat corneal front power (K1), preoperative steep corneal front power (K2), lens thickness, horizontal white-to-white (WTW) corneal diameter, and central corneal thickness (CCT) were recorded from the Lenstar biometric device. Predicted postoperative refractions for the Holladay 2 formula were calculated using Holladay IOL Consultant software (Holladay Consulting). Predicted postoperative refractions for the Barrett toric IOL formula were calculated using the online Barrett toric formula calculator.21 Since previous studies have shown that both the Holladay and Barrett formulae account for posterior corneal astigmatism, a comparison of refractive outcomes in eyes with against-the-rule astigmatism vs with-the-rule astigmatism was not performed.14An estimated standardized value for surgically-induced astigmatism was entered into both formulae; 0.3 diopter (D) was chosen based on previously published averages.22-24
A formula’s prediction error is defined as the predicted postoperative refraction minus the actual postoperative refraction. The mean absolute prediction error (MAE), defined as the mean of the absolute values of the prediction errors, and the median absolute prediction error (MedAE), defined as the median of the absolute values of the prediction errors, were used to assess the overall accuracy of each formula. Also, the percentages of eyes with postoperative refraction within ≥ 0.25 D, ≥ 0.50 D, and ≥ 1.0 D were calculated for both formulae. Two-tailed t tests were performed to compare the MAE between the formulae. Subgroup analyses were performed for short eyes (AL < 22 mm), medium length eyes (AL = 22-25 mm), and long eyes (AL > 25 mm). Statistical analysis was performed using STATA 11 (STATA Corp). The preoperative corneal astigmatism and postoperative refractive astigmatism of all the cases were compared in double-angle plots to assess how well the toric IOL neutralized the corneal astigmatism.