Food Insecurity Among Veterans: Resources to Screen and Intervene
A screener was created in the VA electronic health record clinical reminder system to facilitate an interdisciplinary approach to identifying and addressing food insecurity.
Author affiliations Alicia Cohen is a Research Scientist; James Rudolph is Director; Kali Thomas is a Research Health Science Specialist; Elizabeth Archambault is a Social Worker; David Dosa is Associate Director; all at the VA Health Services Research & Development Center of Innovation in Long Term Services and Supports at the Providence VA Medical Center in Rhode Island; Thomas O’Toole is Senior Medical Advisor, Office of the Assistant Deputy Undersecretary for Health for Clinical Operations, Veterans Health Administration in Washington, DC. Megan Bowman is Assistant Chief, Nutrition and Food Services at VA Salt Lake City Health Care System in Utah. Christine Going is Executive Assistant, Office of the Assistant Deputy Undersecretary for Health for Clinical Operations, Veterans Health Administration. Michele Heisler is a Research Scientist at the Center for Clinical Management Research, Ann Arbor VA Medical Center in Michigan. Alicia Cohen is an Assistant Professor of Family Medicine and Health Services, Policy and Practice; James Rudolph is Professor of Medicine and Health Services, Policy and Practice; Kali Thomas is an Associate Professor of Health Services, Policy, and Practice; David Dosa is an Associate Professor of Medicine and Health Services, Policy and Practice; Thomas O’Toole is a Professor of Medicine; all at the Warren Alpert Medical School of Brown University and Brown University School of Public Health in Providence, Rhode Island. Michele Heisler is a Professor of Internal Medicine and Health Behavior and Health Education at the University of Michigan Medical School and School of Public Health. Megan Bowman and Christine Going are Co- Chairs, and Alicia Cohen, Kali Thomas, and Thomas O’Toole are members of the Ensuring Veteran Food Security Workgroup. Correspondence: Alicia Cohen (alicia.cohen@va.gov)
Author disclosures Alicia Cohen was supported by an Advanced Health Services Research and Development (HSR&D) postdoctoral fellowship through the VA Office of Academic Affairs. James Rudolph and David Dosa were supported by the VA HSR&D Center of Innovation in Long Term Services and Supports (CIN 13‐419). Kali Thomas was supported by a VA HSR&D Career Development Award (CDA 14-422). Michele Heisler was supported by Grant Number P30DK092926 (MCDTR) from the National Institute of Diabetes and Digestive and Kidney Diseases.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
Nearly 1 in 8 households—and 1 in 6 households with children—experienced food insecurity in 2017, defined as limited or uncertain availability of nutritionally adequate and safe foods.1 Food insecurity is often even more pronounced among households with individuals with acute or chronic medical conditions.2-6 Moreover, food insecurity is independently associated with a range of adverse health outcomes, including poorer control of diabetes mellitus, hypertension, depression and other major psychiatric disorders, HIV, and chronic lung and kidney disease, as well as poorer overall health status.7-14 Food insecurity also has been associated with increased health care costs and acute care utilization as well as increased probability of delayed or missed care.15-19
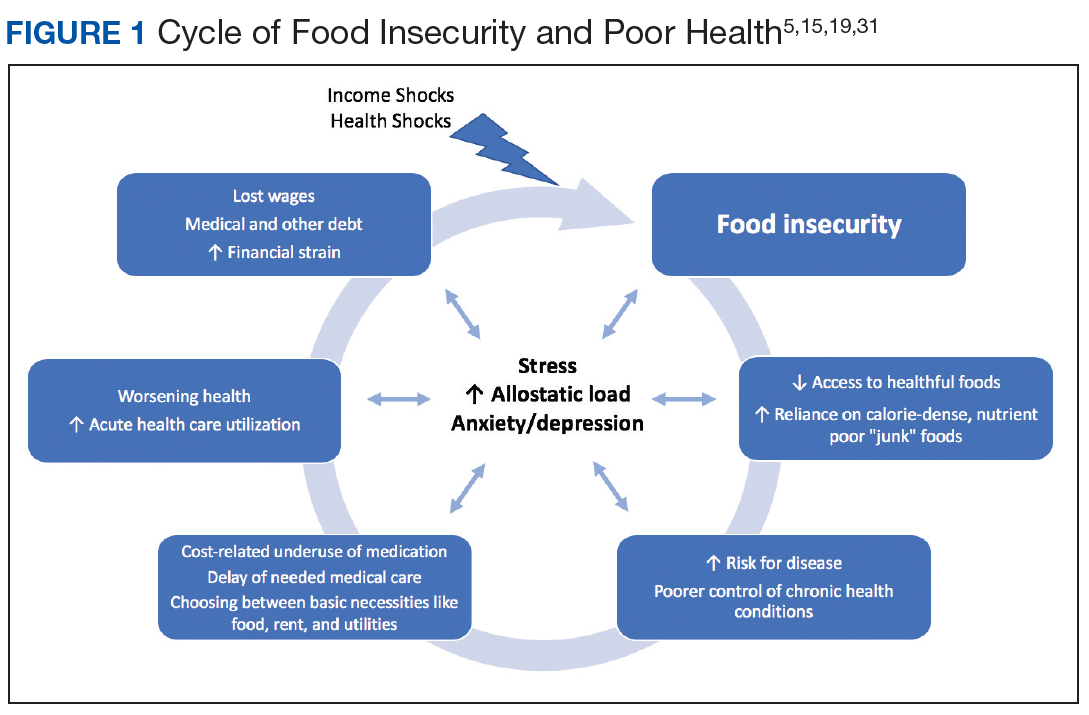
The relationship between food insecurity and poor health outcomes is a complex and often cyclic phenomenon (Figure 1). Poor nutritional status is fueled by limited access to healthful foods as well as increased reliance on calorie-dense and nutrient-poor “junk” foods, which are less expensive and often more readily available in low-income neighborhoods.5,20-24 These compensatory dietary patterns place individuals at higher risk for developing cardiometabolic conditions and for poor control of these conditions.5,8,9,12,25,26 Additionally, the physiological and psychological stressors of food insecurity may precipitate depression and anxiety or worsen existing mental health conditions, resulting in feelings of overwhelm and decreased self-management capacity.5,8,27-31 Food insecurity has further been associated with poor sleep, declines in cognitive function, and increased falls, particularly among the frail and elderly.32-34
Individuals experiencing food insecurity often report having to make trade-offs between food and other necessities, such as paying rent or utilities. Additional strategies to stretch limited resources include cost-related underuse of medication and delays in needed medical care.4,17,31,35 In a nationally representative survey among adults with at least 1 chronic medical condition, 1 in 3 reported having to choose between food and medicine; 11% were unable to afford either.3 Furthermore, the inability to reliably adhere to medication regimens that need to be taken with food can result in potentially life-threatening hypoglycemia (as can lack of food regardless of medication use).5,26,36 In addition to the more obvious risks of glucose-lowering medications, such as insulin and long-acting sulfonylureas in patients experiencing food insecurity, many drugs commonly used among nondiabetic adults such as ACE-inhibitors, β blockers, quinolones, and salicylates can also precipitate hypoglycemia, and food insecurity has been associated with experiences of hypoglycemia even among individuals without diabetes mellitus.32,37 In one study the risk for hospital admissions for hypoglycemia among low-income populations increased by 27% at the end of the month when food budgets were more likely to be exhausted.38 Worsening health status and increased emergency department visits and hospitalizations may then result in lost wages and mounting medical bills, contributing to further financial strain and worsening food insecurity.
Prevalence and Importance of Food Insecurity Among US Veterans
Nearly 1.5 million veterans in the US are living below the federal poverty level (FPL).39 An additional 2.4 million veterans are living paycheck to paycheck at < 200% of the FPL.40 Veterans living in poverty are at even higher risk than nonveterans for food insecurity, homelessness, and other material hardship.41