User login
When attendings at Denver Health Medical Center (DHMC) were asked to be available to help supervise the teams of residents and interns with the hand-off process, Eugene Chu, MD, director of the hospital medicine program, quickly knew there was a problem.
“They didn’t really know what they were teaching,” says Dr. Chu. “They had an idea of how to do a hand-off, but they had never explicitly learned what a good hand-off was because it had never been described before. Some of our attendings fell back on what they did best—teach medicine. But that was not necessarily what the house staff wanted at that time of day.”
The house staff did want to learn to give safe, effective, and efficient hand-offs. “Giving a lecture on renal failure was not really the point of the hand-off,” says Dr. Chu.
Time for Training
“Sign outs serve a lot of purposes, not just information [transfer],” says Leora Horwitz, MD, an assistant professor in the division of general internal medicine at Yale School of Medicine, New Haven, Conn. “Signout is also a time for training. It is a time for socialization in terms of how we talk about patients and what is expected. And it is a time for catching errors and for rethinking plans and diagnoses because as you are describing something to someone, they might pick up on gaps or inconsistencies or things that should be done differently.”
Dr. Horwitz, who is also associate medical director of the Center for Outcomes Research and Evaluation at Yale-New Haven Hospital, has researched training for transfer of care over the past three years.1
“The most important thing is that hospitalists should not assume that residents have any skills [pertaining to transfer of care],” says Dr. Horwitz. “In medical schools, students are taught over and over how to present a patient for the first time. There’s a rigid order in which the information is supposed to flow, and there is a rigid list of categories of information that should be conveyed. People are taught that same order and that same flow and that same list of categories at all med schools. Consequently, as residents, everybody has the same sense of how to represent an initial history and physical. There is no such thing for hand-offs.”
Resident duty-hour limitations have increased the number of hand-offs, which creates greater risks for discontinuity of care and patient safety.2, 3 “Hand-offs occur two or three times a day and a patient presentation only occurs once—when the patient shows up,” says Dr. Horwitz. On top of that, when residents appear in their clinical duties, the attendings tend to forget residents don’t have the skills to execute a comprehensive and well-communicated hand-off. “The first thing to remember is that people need to be trained,” she says.
In a study in the Archives of Internal Medicine in 2006 (for which Dr. Horwitz is first author), the investigators asked internal medicine chief residents whether their program provides direct training in how to perform sign outs. Sign-out training varied considerably, and fewer than half the 202 programs that responded (62% of all U.S. residency programs) provided formal sign-out skill training: 40% of the programs taught sign-out skills through a lecture or workshop, 45% supervised oral sign outs, and 38% reviewed written sign outs.4 Residents in 27% of the programs received no training or supervision. Further, in more than one-third of training programs they found hand-offs were left to interns. “Residency programs need to recognize the problem and address it in some way,” Dr. Horwitz says.
Be Explicit, Create a Model
“Many residency programs have a standardized form that residents use to sign out to the cross-covering physician,” says Sunil Kripalani, MD, MSc, director of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. “However, there is often not much attention given to the actual process of transferring patient information to another physician.”
For example, residents may tack the form up to a wall or leave it on a computer, he says, because this may be more convenient than meeting for a verbal, face-to-face sign out. “It is important that residents receive training about how to best sign out patients, so it is viewed as a priority area,” he says.
The initial training should cover best practices for hand-offs, says Dr. Kripalani. “It may not be intuitive, especially to new residents, that poorly executed hand-offs can be perilous,” he says.
It is also important to teach trainees how to best convey that information. “Sometimes you’ll think more is better,” says Dr. Horwitz, “but that’s not the case; people turn off or get distracted. There is a tension between providing enough information to take care of the person overnight versus providing too much information.”
Modeling best behaviors is also an important part of training, says Jay Routson, MD, a teaching hospitalist and clinical assistant professor of medicine in the Idaho State University Department of Family Medicine in Pocatello, Idaho. Dr. Routson, trained in internal medicine, thinks opportunities to train residents and students in transfer of care are also a chance to model what you expect of them.
This is particularly important in Dr. Routson’s circumstances because of the nature of his university’s family medicine residency: It is conducted at a number of locations. At morning report on the first day of a block, residents who have been on the previous rotation are to transfer patient care to the incoming residents. But they may have already left for their new pediatrics or NICU assignments, for instance, not only elsewhere in Pocatello but perhaps in Boise or Logan.
Another problem in his program’s training for transfer of care, says Dr. Routson, is that less-experienced residents are not always aware of the important things to check. What one resident thinks is important to follow up on the next resident may put at the bottom of his or her list.
“I think that you have to model the importance you place on [hand-offs],” says Dr. Routson. “You have to set aside time during the day and make it a priority. Model the behavior when you’re checking out to a new attending, make sure the residents and interns know it’s a priority, especially early in the academic year.”
Supervision and Feedback
Supervised evaluation of performance and feedback are key aspects of training for transfer of care.
“Training residents means supervising them,” says Dr. Horwitz. “Are they getting the concepts? Are they incorporating the key points into everyday communication and actions?” Having more senior and experienced doctors present during sign out or at the very least prepare people for sign out is crucial, she says, because an issue such as anticipatory guidance/contingency planning is difficult for less-experienced residents.
“As a chief resident I made a point of periodically going around and observing sign outs,” she says. “Nobody ever watches sign out because it happens at the odd hours of the day; nobody gets feedback or evaluation. Ideally an attending should, at least now and again, be involved.”
Questions to ask include:
- Do the residents meet face to face in a dedicated time and place?
- Do they fill out a standardized template and updating it appropriately, especially with regard to medications?
- Do residents measure aspects of hand-offs to ensure they are being done?
Two-Way Street
Just as the DHMC team recognized that communication for hand-offs is a two-way street, the same is true for performing a discharge communication exchange. Are primary care providers considering best practices to train themselves in this integral aspect of patient care and safety?5, 6
“I don’t think the primary care community has gotten together and come up with a consensus of what they want to know and how much interaction they want,” Dr. Horwitz says. “There should be a standard for that.”
That is a first step to encourage greater training all around. She urges collaboration between SHM and a national organization, such as the American Academy on Family Practice, and hopes SHM will open that dialogue.
In that regard, some steps have been taken.7 Dr. Kripalani is a member of the SHM Hand-off and Communication Standards Task Force, which is developing national standards (The Hospitalist, August 2007, p. 17). There is a working list of nine best practices for hand-offs at shift changes or rotation ends, and the group plans to publish a final list in the upcoming year. The list is designed primarily for practicing hospitalists but will also be suitable for residents. The task force hopes other groups, such as internal medicine program directors and chief residents, will disseminate the best practices to trainees. National best practices are also likely to affect providers in the community.
“My suspicion is that a lot of community-based programs are interested in improving hand-offs, but each program may develop a different set of procedures,” says Dr. Kripalani. “One of the main reasons for developing national standards is so that both academic and community groups can refer to a list of evidence-based best practices.”
Evolution of Training
“Training for transfer of care and transfer of care are very different things, says Dr. Chu, “but they’re interrelated.” He and his colleague Gregory Misky, MD, a hospitalist and instructor with the University of Colorado Health Sciences Center (UCHSC), have been disseminating that training program throughout the UCHSC internal medicine residency program for the past three years.
In order to develop a structured, standard method for patient hand-offs, they took on teaching and supervising interns during their internal medicine ward rotations. Although much of the literature advocates the SBAR (situation, background, assessment, and recommendation) communication technique, the UCHSC team has developed a verbal structure specifically for hand-offs that differs from the SBAR model.8
Having learned many lessons their first year of training the trainers and the trainees, the Colorado hospitalists regrouped the next year. Because there were two interns coming on duty each evening, both taking cross cover, one attending could supervise only one of the interns. And, those hospitalists were getting called away to handle their clinical responsibilities.
“We felt it was important that attendings were available to guide the process safely,” says Dr. Chu. Therefore, because the evening hand-offs were conducted at 6 p.m. and a hospitalist was in house daily at that time, they began having the evening person, who was on each night until about 11, supervise the interns.
To improve the quality and consistency of the teaching, only four of the Division of Hospital Medicine’s eight attendings focused on supervising intern hand-offs. Also, in a series of focus-group meetings with attendings and house staff, they discussed supervision and identified several structures and standards for teaching hand-offs.
In addition to determining a consistent time and place for hand-off exchanges, they developed a consistent written template and a standard for verbal communication that provides an order of thinking and presenting, just as they use for presenting patient history and physical or daily patient progress updates. “The written template and the verbal are not necessarily the same thing,” says Dr. Chu. “We distinguished them as being two separate standards, just as they are with the written and verbal of morning rounds.”
With these protocols in place, attendings now had distinctions to watch for and a clear-cut means by which to supervise. In the third year of training at UCHSC, the hospitalist attendings provided training and feedback on the first night of call for the first four months beginning in July and in small-group sessions during the first week of the ward month.
The Reviews Are In
In response to a survey, the vast majority of UCHSC internal medicine residents said the new protocols were useful or extremely useful. Responses also revealed that training increased interns’ self-perceived hand-off skills and knowledge. The common denominator of a same time and place for hand-offs was judged the most useful element of the program; lectures were considered the least useful element.
Word got around of the program’s success. Eva Aagaard, MD, associate chair for education in the department of medicine, approached the originators to incorporate the program into the medical school’s interclinical curriculum, given to students between the third and fourth years as additional skills they would need in their sub-internships. Originally offered as an elective, demand for the course exceeded the class limit. Plans are under way to make this course mandatory.
“This past year, for the first time, we specifically taught our medical students hand-offs,” says Dr. Chu. He and his colleagues presented an abstract at SHM’s annual meeting in Dallas and are preparing a manuscript for publication.
Until now, all physicians have managed to do hand-offs without formal training. “Most residents figure out their own way of doing things after a while, but what we’re trying to do is not let it be a random evolution of learning,” says Dr. Chu. “It’s like learning to drive or ski with no lesson s: If you point your skis downhill, eventually you’ll learn how to ski, but you’ll have a lot of crashes. In hand-offs, that means communication failures, and a patient may suffer morbidity. We want to train and supervise [residents] so they learn in a progressive fashion and have fewer crashes.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
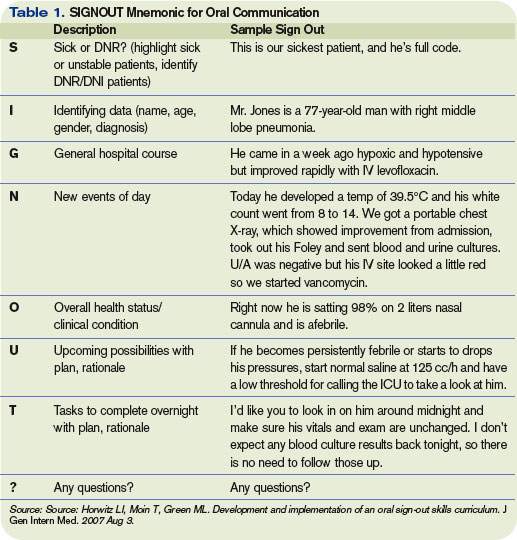
- Horwitz LI, Moin T, Green ML. Development and implementation of an oral sign-out skills curriculum. J Gen Intern Med. 2007 Aug 3.
- Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831-841.
- Vidyarthi AR, Arora V, Schnipper JL, et al. Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign-out. J Hosp Med. 2006;1(4):257-266.
- Horwitz LI, Krumholz HM, Green ML,. Transfers of patient care between house staff on internal medicine wards: a national survey. Arch Intern Med. 2006 Jun;166(11):1173-1177.
- Coleman EA, Berenson RA. Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004 Oct;141(7):533-536.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006 Nov;1(6):354-360.
- Pantilat SZ, Lindenauer PK, Katz PP, et al. Primary care physician attitudes regarding communication with hospitalists. Am J Med. 2001;111(9, Supplement 2):15-20.
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12(4):40-41.
When attendings at Denver Health Medical Center (DHMC) were asked to be available to help supervise the teams of residents and interns with the hand-off process, Eugene Chu, MD, director of the hospital medicine program, quickly knew there was a problem.
“They didn’t really know what they were teaching,” says Dr. Chu. “They had an idea of how to do a hand-off, but they had never explicitly learned what a good hand-off was because it had never been described before. Some of our attendings fell back on what they did best—teach medicine. But that was not necessarily what the house staff wanted at that time of day.”
The house staff did want to learn to give safe, effective, and efficient hand-offs. “Giving a lecture on renal failure was not really the point of the hand-off,” says Dr. Chu.
Time for Training
“Sign outs serve a lot of purposes, not just information [transfer],” says Leora Horwitz, MD, an assistant professor in the division of general internal medicine at Yale School of Medicine, New Haven, Conn. “Signout is also a time for training. It is a time for socialization in terms of how we talk about patients and what is expected. And it is a time for catching errors and for rethinking plans and diagnoses because as you are describing something to someone, they might pick up on gaps or inconsistencies or things that should be done differently.”
Dr. Horwitz, who is also associate medical director of the Center for Outcomes Research and Evaluation at Yale-New Haven Hospital, has researched training for transfer of care over the past three years.1
“The most important thing is that hospitalists should not assume that residents have any skills [pertaining to transfer of care],” says Dr. Horwitz. “In medical schools, students are taught over and over how to present a patient for the first time. There’s a rigid order in which the information is supposed to flow, and there is a rigid list of categories of information that should be conveyed. People are taught that same order and that same flow and that same list of categories at all med schools. Consequently, as residents, everybody has the same sense of how to represent an initial history and physical. There is no such thing for hand-offs.”
Resident duty-hour limitations have increased the number of hand-offs, which creates greater risks for discontinuity of care and patient safety.2, 3 “Hand-offs occur two or three times a day and a patient presentation only occurs once—when the patient shows up,” says Dr. Horwitz. On top of that, when residents appear in their clinical duties, the attendings tend to forget residents don’t have the skills to execute a comprehensive and well-communicated hand-off. “The first thing to remember is that people need to be trained,” she says.
In a study in the Archives of Internal Medicine in 2006 (for which Dr. Horwitz is first author), the investigators asked internal medicine chief residents whether their program provides direct training in how to perform sign outs. Sign-out training varied considerably, and fewer than half the 202 programs that responded (62% of all U.S. residency programs) provided formal sign-out skill training: 40% of the programs taught sign-out skills through a lecture or workshop, 45% supervised oral sign outs, and 38% reviewed written sign outs.4 Residents in 27% of the programs received no training or supervision. Further, in more than one-third of training programs they found hand-offs were left to interns. “Residency programs need to recognize the problem and address it in some way,” Dr. Horwitz says.
Be Explicit, Create a Model
“Many residency programs have a standardized form that residents use to sign out to the cross-covering physician,” says Sunil Kripalani, MD, MSc, director of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. “However, there is often not much attention given to the actual process of transferring patient information to another physician.”
For example, residents may tack the form up to a wall or leave it on a computer, he says, because this may be more convenient than meeting for a verbal, face-to-face sign out. “It is important that residents receive training about how to best sign out patients, so it is viewed as a priority area,” he says.
The initial training should cover best practices for hand-offs, says Dr. Kripalani. “It may not be intuitive, especially to new residents, that poorly executed hand-offs can be perilous,” he says.
It is also important to teach trainees how to best convey that information. “Sometimes you’ll think more is better,” says Dr. Horwitz, “but that’s not the case; people turn off or get distracted. There is a tension between providing enough information to take care of the person overnight versus providing too much information.”
Modeling best behaviors is also an important part of training, says Jay Routson, MD, a teaching hospitalist and clinical assistant professor of medicine in the Idaho State University Department of Family Medicine in Pocatello, Idaho. Dr. Routson, trained in internal medicine, thinks opportunities to train residents and students in transfer of care are also a chance to model what you expect of them.
This is particularly important in Dr. Routson’s circumstances because of the nature of his university’s family medicine residency: It is conducted at a number of locations. At morning report on the first day of a block, residents who have been on the previous rotation are to transfer patient care to the incoming residents. But they may have already left for their new pediatrics or NICU assignments, for instance, not only elsewhere in Pocatello but perhaps in Boise or Logan.
Another problem in his program’s training for transfer of care, says Dr. Routson, is that less-experienced residents are not always aware of the important things to check. What one resident thinks is important to follow up on the next resident may put at the bottom of his or her list.
“I think that you have to model the importance you place on [hand-offs],” says Dr. Routson. “You have to set aside time during the day and make it a priority. Model the behavior when you’re checking out to a new attending, make sure the residents and interns know it’s a priority, especially early in the academic year.”
Supervision and Feedback
Supervised evaluation of performance and feedback are key aspects of training for transfer of care.
“Training residents means supervising them,” says Dr. Horwitz. “Are they getting the concepts? Are they incorporating the key points into everyday communication and actions?” Having more senior and experienced doctors present during sign out or at the very least prepare people for sign out is crucial, she says, because an issue such as anticipatory guidance/contingency planning is difficult for less-experienced residents.
“As a chief resident I made a point of periodically going around and observing sign outs,” she says. “Nobody ever watches sign out because it happens at the odd hours of the day; nobody gets feedback or evaluation. Ideally an attending should, at least now and again, be involved.”
Questions to ask include:
- Do the residents meet face to face in a dedicated time and place?
- Do they fill out a standardized template and updating it appropriately, especially with regard to medications?
- Do residents measure aspects of hand-offs to ensure they are being done?
Two-Way Street
Just as the DHMC team recognized that communication for hand-offs is a two-way street, the same is true for performing a discharge communication exchange. Are primary care providers considering best practices to train themselves in this integral aspect of patient care and safety?5, 6
“I don’t think the primary care community has gotten together and come up with a consensus of what they want to know and how much interaction they want,” Dr. Horwitz says. “There should be a standard for that.”
That is a first step to encourage greater training all around. She urges collaboration between SHM and a national organization, such as the American Academy on Family Practice, and hopes SHM will open that dialogue.
In that regard, some steps have been taken.7 Dr. Kripalani is a member of the SHM Hand-off and Communication Standards Task Force, which is developing national standards (The Hospitalist, August 2007, p. 17). There is a working list of nine best practices for hand-offs at shift changes or rotation ends, and the group plans to publish a final list in the upcoming year. The list is designed primarily for practicing hospitalists but will also be suitable for residents. The task force hopes other groups, such as internal medicine program directors and chief residents, will disseminate the best practices to trainees. National best practices are also likely to affect providers in the community.
“My suspicion is that a lot of community-based programs are interested in improving hand-offs, but each program may develop a different set of procedures,” says Dr. Kripalani. “One of the main reasons for developing national standards is so that both academic and community groups can refer to a list of evidence-based best practices.”
Evolution of Training
“Training for transfer of care and transfer of care are very different things, says Dr. Chu, “but they’re interrelated.” He and his colleague Gregory Misky, MD, a hospitalist and instructor with the University of Colorado Health Sciences Center (UCHSC), have been disseminating that training program throughout the UCHSC internal medicine residency program for the past three years.
In order to develop a structured, standard method for patient hand-offs, they took on teaching and supervising interns during their internal medicine ward rotations. Although much of the literature advocates the SBAR (situation, background, assessment, and recommendation) communication technique, the UCHSC team has developed a verbal structure specifically for hand-offs that differs from the SBAR model.8
Having learned many lessons their first year of training the trainers and the trainees, the Colorado hospitalists regrouped the next year. Because there were two interns coming on duty each evening, both taking cross cover, one attending could supervise only one of the interns. And, those hospitalists were getting called away to handle their clinical responsibilities.
“We felt it was important that attendings were available to guide the process safely,” says Dr. Chu. Therefore, because the evening hand-offs were conducted at 6 p.m. and a hospitalist was in house daily at that time, they began having the evening person, who was on each night until about 11, supervise the interns.
To improve the quality and consistency of the teaching, only four of the Division of Hospital Medicine’s eight attendings focused on supervising intern hand-offs. Also, in a series of focus-group meetings with attendings and house staff, they discussed supervision and identified several structures and standards for teaching hand-offs.
In addition to determining a consistent time and place for hand-off exchanges, they developed a consistent written template and a standard for verbal communication that provides an order of thinking and presenting, just as they use for presenting patient history and physical or daily patient progress updates. “The written template and the verbal are not necessarily the same thing,” says Dr. Chu. “We distinguished them as being two separate standards, just as they are with the written and verbal of morning rounds.”
With these protocols in place, attendings now had distinctions to watch for and a clear-cut means by which to supervise. In the third year of training at UCHSC, the hospitalist attendings provided training and feedback on the first night of call for the first four months beginning in July and in small-group sessions during the first week of the ward month.
The Reviews Are In
In response to a survey, the vast majority of UCHSC internal medicine residents said the new protocols were useful or extremely useful. Responses also revealed that training increased interns’ self-perceived hand-off skills and knowledge. The common denominator of a same time and place for hand-offs was judged the most useful element of the program; lectures were considered the least useful element.
Word got around of the program’s success. Eva Aagaard, MD, associate chair for education in the department of medicine, approached the originators to incorporate the program into the medical school’s interclinical curriculum, given to students between the third and fourth years as additional skills they would need in their sub-internships. Originally offered as an elective, demand for the course exceeded the class limit. Plans are under way to make this course mandatory.
“This past year, for the first time, we specifically taught our medical students hand-offs,” says Dr. Chu. He and his colleagues presented an abstract at SHM’s annual meeting in Dallas and are preparing a manuscript for publication.
Until now, all physicians have managed to do hand-offs without formal training. “Most residents figure out their own way of doing things after a while, but what we’re trying to do is not let it be a random evolution of learning,” says Dr. Chu. “It’s like learning to drive or ski with no lesson s: If you point your skis downhill, eventually you’ll learn how to ski, but you’ll have a lot of crashes. In hand-offs, that means communication failures, and a patient may suffer morbidity. We want to train and supervise [residents] so they learn in a progressive fashion and have fewer crashes.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Horwitz LI, Moin T, Green ML. Development and implementation of an oral sign-out skills curriculum. J Gen Intern Med. 2007 Aug 3.
- Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831-841.
- Vidyarthi AR, Arora V, Schnipper JL, et al. Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign-out. J Hosp Med. 2006;1(4):257-266.
- Horwitz LI, Krumholz HM, Green ML,. Transfers of patient care between house staff on internal medicine wards: a national survey. Arch Intern Med. 2006 Jun;166(11):1173-1177.
- Coleman EA, Berenson RA. Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004 Oct;141(7):533-536.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006 Nov;1(6):354-360.
- Pantilat SZ, Lindenauer PK, Katz PP, et al. Primary care physician attitudes regarding communication with hospitalists. Am J Med. 2001;111(9, Supplement 2):15-20.
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12(4):40-41.
When attendings at Denver Health Medical Center (DHMC) were asked to be available to help supervise the teams of residents and interns with the hand-off process, Eugene Chu, MD, director of the hospital medicine program, quickly knew there was a problem.
“They didn’t really know what they were teaching,” says Dr. Chu. “They had an idea of how to do a hand-off, but they had never explicitly learned what a good hand-off was because it had never been described before. Some of our attendings fell back on what they did best—teach medicine. But that was not necessarily what the house staff wanted at that time of day.”
The house staff did want to learn to give safe, effective, and efficient hand-offs. “Giving a lecture on renal failure was not really the point of the hand-off,” says Dr. Chu.
Time for Training
“Sign outs serve a lot of purposes, not just information [transfer],” says Leora Horwitz, MD, an assistant professor in the division of general internal medicine at Yale School of Medicine, New Haven, Conn. “Signout is also a time for training. It is a time for socialization in terms of how we talk about patients and what is expected. And it is a time for catching errors and for rethinking plans and diagnoses because as you are describing something to someone, they might pick up on gaps or inconsistencies or things that should be done differently.”
Dr. Horwitz, who is also associate medical director of the Center for Outcomes Research and Evaluation at Yale-New Haven Hospital, has researched training for transfer of care over the past three years.1
“The most important thing is that hospitalists should not assume that residents have any skills [pertaining to transfer of care],” says Dr. Horwitz. “In medical schools, students are taught over and over how to present a patient for the first time. There’s a rigid order in which the information is supposed to flow, and there is a rigid list of categories of information that should be conveyed. People are taught that same order and that same flow and that same list of categories at all med schools. Consequently, as residents, everybody has the same sense of how to represent an initial history and physical. There is no such thing for hand-offs.”
Resident duty-hour limitations have increased the number of hand-offs, which creates greater risks for discontinuity of care and patient safety.2, 3 “Hand-offs occur two or three times a day and a patient presentation only occurs once—when the patient shows up,” says Dr. Horwitz. On top of that, when residents appear in their clinical duties, the attendings tend to forget residents don’t have the skills to execute a comprehensive and well-communicated hand-off. “The first thing to remember is that people need to be trained,” she says.
In a study in the Archives of Internal Medicine in 2006 (for which Dr. Horwitz is first author), the investigators asked internal medicine chief residents whether their program provides direct training in how to perform sign outs. Sign-out training varied considerably, and fewer than half the 202 programs that responded (62% of all U.S. residency programs) provided formal sign-out skill training: 40% of the programs taught sign-out skills through a lecture or workshop, 45% supervised oral sign outs, and 38% reviewed written sign outs.4 Residents in 27% of the programs received no training or supervision. Further, in more than one-third of training programs they found hand-offs were left to interns. “Residency programs need to recognize the problem and address it in some way,” Dr. Horwitz says.
Be Explicit, Create a Model
“Many residency programs have a standardized form that residents use to sign out to the cross-covering physician,” says Sunil Kripalani, MD, MSc, director of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. “However, there is often not much attention given to the actual process of transferring patient information to another physician.”
For example, residents may tack the form up to a wall or leave it on a computer, he says, because this may be more convenient than meeting for a verbal, face-to-face sign out. “It is important that residents receive training about how to best sign out patients, so it is viewed as a priority area,” he says.
The initial training should cover best practices for hand-offs, says Dr. Kripalani. “It may not be intuitive, especially to new residents, that poorly executed hand-offs can be perilous,” he says.
It is also important to teach trainees how to best convey that information. “Sometimes you’ll think more is better,” says Dr. Horwitz, “but that’s not the case; people turn off or get distracted. There is a tension between providing enough information to take care of the person overnight versus providing too much information.”
Modeling best behaviors is also an important part of training, says Jay Routson, MD, a teaching hospitalist and clinical assistant professor of medicine in the Idaho State University Department of Family Medicine in Pocatello, Idaho. Dr. Routson, trained in internal medicine, thinks opportunities to train residents and students in transfer of care are also a chance to model what you expect of them.
This is particularly important in Dr. Routson’s circumstances because of the nature of his university’s family medicine residency: It is conducted at a number of locations. At morning report on the first day of a block, residents who have been on the previous rotation are to transfer patient care to the incoming residents. But they may have already left for their new pediatrics or NICU assignments, for instance, not only elsewhere in Pocatello but perhaps in Boise or Logan.
Another problem in his program’s training for transfer of care, says Dr. Routson, is that less-experienced residents are not always aware of the important things to check. What one resident thinks is important to follow up on the next resident may put at the bottom of his or her list.
“I think that you have to model the importance you place on [hand-offs],” says Dr. Routson. “You have to set aside time during the day and make it a priority. Model the behavior when you’re checking out to a new attending, make sure the residents and interns know it’s a priority, especially early in the academic year.”
Supervision and Feedback
Supervised evaluation of performance and feedback are key aspects of training for transfer of care.
“Training residents means supervising them,” says Dr. Horwitz. “Are they getting the concepts? Are they incorporating the key points into everyday communication and actions?” Having more senior and experienced doctors present during sign out or at the very least prepare people for sign out is crucial, she says, because an issue such as anticipatory guidance/contingency planning is difficult for less-experienced residents.
“As a chief resident I made a point of periodically going around and observing sign outs,” she says. “Nobody ever watches sign out because it happens at the odd hours of the day; nobody gets feedback or evaluation. Ideally an attending should, at least now and again, be involved.”
Questions to ask include:
- Do the residents meet face to face in a dedicated time and place?
- Do they fill out a standardized template and updating it appropriately, especially with regard to medications?
- Do residents measure aspects of hand-offs to ensure they are being done?
Two-Way Street
Just as the DHMC team recognized that communication for hand-offs is a two-way street, the same is true for performing a discharge communication exchange. Are primary care providers considering best practices to train themselves in this integral aspect of patient care and safety?5, 6
“I don’t think the primary care community has gotten together and come up with a consensus of what they want to know and how much interaction they want,” Dr. Horwitz says. “There should be a standard for that.”
That is a first step to encourage greater training all around. She urges collaboration between SHM and a national organization, such as the American Academy on Family Practice, and hopes SHM will open that dialogue.
In that regard, some steps have been taken.7 Dr. Kripalani is a member of the SHM Hand-off and Communication Standards Task Force, which is developing national standards (The Hospitalist, August 2007, p. 17). There is a working list of nine best practices for hand-offs at shift changes or rotation ends, and the group plans to publish a final list in the upcoming year. The list is designed primarily for practicing hospitalists but will also be suitable for residents. The task force hopes other groups, such as internal medicine program directors and chief residents, will disseminate the best practices to trainees. National best practices are also likely to affect providers in the community.
“My suspicion is that a lot of community-based programs are interested in improving hand-offs, but each program may develop a different set of procedures,” says Dr. Kripalani. “One of the main reasons for developing national standards is so that both academic and community groups can refer to a list of evidence-based best practices.”
Evolution of Training
“Training for transfer of care and transfer of care are very different things, says Dr. Chu, “but they’re interrelated.” He and his colleague Gregory Misky, MD, a hospitalist and instructor with the University of Colorado Health Sciences Center (UCHSC), have been disseminating that training program throughout the UCHSC internal medicine residency program for the past three years.
In order to develop a structured, standard method for patient hand-offs, they took on teaching and supervising interns during their internal medicine ward rotations. Although much of the literature advocates the SBAR (situation, background, assessment, and recommendation) communication technique, the UCHSC team has developed a verbal structure specifically for hand-offs that differs from the SBAR model.8
Having learned many lessons their first year of training the trainers and the trainees, the Colorado hospitalists regrouped the next year. Because there were two interns coming on duty each evening, both taking cross cover, one attending could supervise only one of the interns. And, those hospitalists were getting called away to handle their clinical responsibilities.
“We felt it was important that attendings were available to guide the process safely,” says Dr. Chu. Therefore, because the evening hand-offs were conducted at 6 p.m. and a hospitalist was in house daily at that time, they began having the evening person, who was on each night until about 11, supervise the interns.
To improve the quality and consistency of the teaching, only four of the Division of Hospital Medicine’s eight attendings focused on supervising intern hand-offs. Also, in a series of focus-group meetings with attendings and house staff, they discussed supervision and identified several structures and standards for teaching hand-offs.
In addition to determining a consistent time and place for hand-off exchanges, they developed a consistent written template and a standard for verbal communication that provides an order of thinking and presenting, just as they use for presenting patient history and physical or daily patient progress updates. “The written template and the verbal are not necessarily the same thing,” says Dr. Chu. “We distinguished them as being two separate standards, just as they are with the written and verbal of morning rounds.”
With these protocols in place, attendings now had distinctions to watch for and a clear-cut means by which to supervise. In the third year of training at UCHSC, the hospitalist attendings provided training and feedback on the first night of call for the first four months beginning in July and in small-group sessions during the first week of the ward month.
The Reviews Are In
In response to a survey, the vast majority of UCHSC internal medicine residents said the new protocols were useful or extremely useful. Responses also revealed that training increased interns’ self-perceived hand-off skills and knowledge. The common denominator of a same time and place for hand-offs was judged the most useful element of the program; lectures were considered the least useful element.
Word got around of the program’s success. Eva Aagaard, MD, associate chair for education in the department of medicine, approached the originators to incorporate the program into the medical school’s interclinical curriculum, given to students between the third and fourth years as additional skills they would need in their sub-internships. Originally offered as an elective, demand for the course exceeded the class limit. Plans are under way to make this course mandatory.
“This past year, for the first time, we specifically taught our medical students hand-offs,” says Dr. Chu. He and his colleagues presented an abstract at SHM’s annual meeting in Dallas and are preparing a manuscript for publication.
Until now, all physicians have managed to do hand-offs without formal training. “Most residents figure out their own way of doing things after a while, but what we’re trying to do is not let it be a random evolution of learning,” says Dr. Chu. “It’s like learning to drive or ski with no lesson s: If you point your skis downhill, eventually you’ll learn how to ski, but you’ll have a lot of crashes. In hand-offs, that means communication failures, and a patient may suffer morbidity. We want to train and supervise [residents] so they learn in a progressive fashion and have fewer crashes.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Horwitz LI, Moin T, Green ML. Development and implementation of an oral sign-out skills curriculum. J Gen Intern Med. 2007 Aug 3.
- Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831-841.
- Vidyarthi AR, Arora V, Schnipper JL, et al. Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign-out. J Hosp Med. 2006;1(4):257-266.
- Horwitz LI, Krumholz HM, Green ML,. Transfers of patient care between house staff on internal medicine wards: a national survey. Arch Intern Med. 2006 Jun;166(11):1173-1177.
- Coleman EA, Berenson RA. Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004 Oct;141(7):533-536.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006 Nov;1(6):354-360.
- Pantilat SZ, Lindenauer PK, Katz PP, et al. Primary care physician attitudes regarding communication with hospitalists. Am J Med. 2001;111(9, Supplement 2):15-20.
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12(4):40-41.