User login
Managing patients with binge-eating disorder (BED) often requires behavioral, medical, and psychiatric interventions.
These patients suffer from recurrent episodes of distressing, uncontrollable overeating, but they do not purge or show other compensatory weight-loss behaviors common to bulimia nervosa1 and anorexia nervosa.2-10 As a result, they are often overweight or obese and may have obesity-related illnesses, such as hypertension or type 2 diabetes. Mild to severe depression—unipolar or bipolar—is a common psychopathology.
Because no one treatment fits all patients with binge eating disorder, their management usually requires an individualized program of:
- behavioral weight control
- psychotherapy
- and sometimes medications.
In our weight management clinic, we consider medication options based on patient preference and whether BED is uncomplicated (Figure 1) or coexists with a mood disorder (Figure 2).
This article presents the evidence on which we base our comprehensive approach. General psychiatrists with knowledge of BED can treat patients with this eating disorder, although complicated cases may require referral for specialized treatment.
Figure 1 Medication options for uncomplicated BED
Clinical characteristics
Psychiatric comorbidity. BED often occurs in patients with mood, anxiety, substance-abuse, impulsecontrol, and personality disorders.4,6,10-12 Mood disorder—particularly depression—appears to be the most common comorbidity. BED can occur with bipolar disorder12—a comorbidity that in our experience is underrecognized both clinically and in the literature.
Patients with BED and bipolar disorder show increased impulsivity and mood lability. As bipolar II disorder and other “soft-spectrum” forms are more common than bipolar I disorder, BED is also more likely to occur with hypomania than mania.
Overweight. Not surprisingly, BED is associated with overweight and obesity.5,8,9,11 Not all patients with BED are overweight or obese, but most who participate in clinical trials of BED treatments are at least overweight. BED has been reported in up to:
- 30% of participants in weight-loss programs7
- 70% of participants in groups such as Overeaters Anonymous
- 50% of patients who seek bariatric surgery.5
In our experience, patients are often more distressed by their weight than by their binge eating, depression, or anxiety. Indeed, overweight and obesity are the usual reasons patients with BED present for treatment at our center.
Diagnosis. BED’s validity as a clinical diagnosis has been controversial since the disorder was first included in DSM-IV (Table 1).3 Debate continues about some definitions in the DSM criteria, including what amount of food is “definitely larger” than most people would eat and what is “loss of control over eating.”
Nevertheless, screening for BED is relatively easy. Clinicians may use the eating disorder section of the Structured Clinical Interview for DSM-IV or the Eating Disorders Examination. Alternatively, simply ask patients if they have episodes of uncontrollable overeating, during which they eat unusually large amounts of food and their eating feels out of control.
Course. BED begins in adolescence or adulthood. Disease course is variable, with periods of remission, recurrence, and chronicity.6,7,10 Interestingly, one prospective study showed that even if the binge eating resolves, persons may still develop obesity.13
Prevalence. BED affects 1.5% to 3% of the U.S. population. It is more common in women than men, equally prevalent in whites and blacks, and more prevalent than anorexia nervosa and bulimia nervosa combined.11,14 Subthreshold BED—such as obesity with infrequent or nondistressing binge eating—appears to be much more common,10 although no data are available.
Theories of binge eating
BED’s cause is unknown, but biological, familial, and psychosocial factors have been implicated.
Biological factors. The neurotransmitters serotonin (5-HT) and dopamine—as well as various peptides—have been shown to help regulate feeding behavior.10
Table 1
Diagnostic criteria for binge-eating disorder*
|
| * Research criteria, DSM-IV-TR appendix B. |
| Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th edition, text revision. Copyright 2000. American Psychiatric Association. |
Serotonin. Reduced 5-HT transporter binding has been shown in obese women with BED.15 Their 5-HT binding improved and binge eating subsided with group psychotherapy and fluoxetine, although the women continued to gain weight.
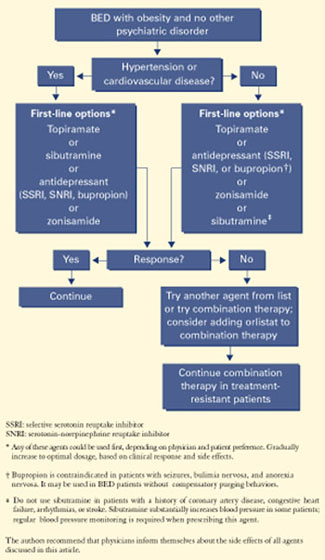
Figure 2 Medication options for BED with obesity and a mood disorder*

Dopamine. Obese patients who compulsively overeat may have lower levels of dopamine D2 receptors than do normal-weight controls.16
Genetic factors. In severely obese patients (body mass index 44±2), those with a DSM-IV diagnosis of BED exhibited mutations of the melanocortin 4 receptor gene, which affects the anorectic properties of alpha melanocyte-stimulating hormone.17
Familial factors associated with BED include parental depression and obesity.18
Psychosocial correlates include physical and sexual abuse, bullying by peers, and discrimination because of being overweight.19
Treatment recommendations
Few systematic studies have examined BED treatment. Emerging research suggests that behavioral weight-loss treatment, specialized psychotherapies, and medications may be effective in some patients with BED.4,6,8
Behavioral weight-loss treatment’s main goal is to manage the patient’s weight with a lower-calorie, healthy diet and to increase exercise.20,21
Over the short term (<1 year), behavioral weight-loss treatment produces similar weight loss in obese patients with or without BED; long-term results in both groups, however, have not been satisfactory.20,21 No studies have examined the efficacy of specialized diets (such as low-carbohydrate regimens) in patients with BED.
Specialized psychotherapy’s goal is to modify bingeeating behavior with behavioral self-management strategies, reducing interpersonal dysfunction and stress, and/or managing affective dysregulation.
Cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) have been effective in reducing binge eating, both acutely and for up to 12 months4,20-24 but less effective in achieving and maintaining weight loss. Patients who achieve remission in binge eating after undergoing CBT or IPI often experience modest but stable weight loss.20-22 For example, in a comparison study of CBT and IPT:
- After 20 weekly sessions, patients whose binge eating was in remission lost weight (mean body mass index [BMI] −0.5 ± 1.5 kg/m2), whereas those who continued to binge gained weight (mean BMI +0.4 ±2.0 kg/m2).
- At 12 months’ follow-up, patients still in remission continued to lose weight (mean BMI −1.0 ± 3.0 kg/m2), whereas those no longer in remission gained weight (mean BMI +0.7 ±2.9 kg/m2[P = 0.01]).22
Self-help and dialectical behavioral therapy (DBT) may also help reduce binge eating in BED. As with CBT and IPT, they are less effective in weight loss. In the only controlled study of DBT,24 patients achieved an average 2.5-lb weight loss after 20 weeks of DBT, compared with an average 0.6-lb weight gain in the control group. This difference was not significant, and the report did not include data on weight loss maintenance.
In summary, CBT may be more effective than behavioral weight loss treatment for reducing binge eating, but behavioral weight loss is more effective for weight loss.
Medications for BED
Medications that have been tried for BED include antidepressants, appetite suppressants, and anticonvulsants.25,26 Antidepressants are used to treat BED because:
- BED is often associated with depressive symptoms and disorders.
- BED is related to bulimia nervosa, and placebo-controlled trials have shown that the binge eating of bulimia nervosa responds to several classes of antidepressants. The selective serotonin reuptake inhibitor (SSRI) fluoxetine is the only medication indicated for treating any eating disorder (bulimia nervosa).
- Bupropion and venlafaxine—a serotonin-norepinephrine reuptake inhibitor (SNRI)—have weight-loss properties.
SSRIs are the most extensively studied antidepressants for treating BED. SSRIs have weightloss properties, but only short term.25-26 Citalopram, fluoxetine, fluvoxamine, and sertraline have reduced binge eating and body weight more effectively than placebo during 6 to 9 weeks of treatment (Table 2).25-26 However, one controlled study23 showed that fluoxetine was not significantly more effective than placebo in reducing binge frequency or body weight after 16 weeks.
TCAs. Studies of tricyclic antidepressants (TCAs) for BED are sparse, and results have been mixed. In one trial, imipramine was similar to placebo in reducing binge frequency and body weight. In a placebo-controlled study of patients with nonpurging bulimia nervosa, desipramine reduced binge eating but had no effect on body weight.25,26
Table 2
Drug therapies shown to be effective for BED*
| Medication | Binge eating | Weight | Depression | Study size | Duration (weeks) | Dosage (mg/d) |
|---|---|---|---|---|---|---|
| Antidepressants | ||||||
| Citalopram | + | + | − | 38 | 6 | 20 to 60 |
| Fluoxetine † | + | + | + | 60 | 6 | 20 to 80 |
| Fluvoxamine | + | + | − | 85 | 9 | 50 to 300 |
| Sertraline | + | + | − | 34 | 6 | 50 to 200 |
| Appetite suppressant | ||||||
| Sibutramine | + | + | + | 60 | 12 | 15 |
| Anticonvulsant | ||||||
| Topiramate | + | + | − | 61 | 14 | 50 to 600 |
| + Improvement | ||||||
| − No improvement | ||||||
| * Randomized, controlled trials. Antidepressants were studied in patients with BED; sibutramine and topiramate were studied in patients with BED and associated obesity. | ||||||
| † One 16-week trial of fluoxetine for BED (reference 23) did not show statistically significant differences in post-treatment binge frequency or body-mass index. | ||||||
Venlafaxine. In a retrospective review of 35 consecutive obese women with BED, venlafaxine, mean 222 mg/d for 28 to 300 days (median 120 days), reduced binge eating, body weight, and depressive symptoms.27
Bupropion has been more effective than placebo for treating:
- uncomplicated obesity (short- and long-term)
- obesity associated with depressive symptoms
- bulimia nervosa (although bupropion is contraindicated in these patients because of seizure risk).26,28,29
No controlled trials have studied bupropion for BED. When using dosages effective in depressive disorders, we find bupropion helpful in reducing binge eating, body weight, and depressive symptoms in BED patients.
Appetite suppressants decrease appetite and weight, may increase satiety, and may reduce depressive symptoms.
Sibutramine—a serotonin, norepinephrine, and dopamine reuptake inhibitor indicated for managing obesity—has been reported effective in BED in a 12-week, randomized, double-blind, placebo-controlled trial. A 15-mg/d dosage reduced binge frequency, body weight, and depressive symptoms more effectively than placebo in 60 obese patients with BED.30 Most-frequent adverse effects (dry mouth and constipation) were mild and benign, and no significant complications were observed.
Sibutramine’s mechanism of action in BED is unknown. However, it suppressed food intake during binge-eating episodes in patients with BED in a randomized, controlled, cross-over laboratory study.31
Orlistat. We know of no published controlled studies of the lipase inhibitor orlistat in treating BED. In our experience, some patients do well with this agent, though we have observed infrequent purging episodes with it in patients with BED.
With orlistat, 120 mg tid, our BED patients have experienced weight loss comparable to that seen in uncomplicated obesity at similar dosages. Orlistat seems most effective for:
- patients whose binge eating is in remission
- those who responded to behavioral weightloss treatment, a psychological treatment, or another medication.
Anticonvulsants such as topiramate and zonisamide have been shown effective in treating obesity32,33 and are sometimes used to treat BED. Obese BED patients with mood disorders often do best with psychotherapy plus medication
Topiramate at dosages of 50 to 600 mg/d (median 212 mg/d) reduced binge-eating frequency, obsessive-compulsive features of binge eating, and body weight more effectively than placebo in a 14-week study of 61 obese patients with BED. These effects were maintained across 48 weeks in an open-label extension trial.34
Zonisamide, mean 513 mg/d, produced similar results during a prospective, open-label, 12-week trial in 15 patients with BED.35 A controlled trial to replicate these findings is ongoing.
BED may respond to anticonvulsant therapy for several reasons:
- Some anticonvulsants are effective in treating bipolar disorder, which may occur with BED.12
- Some anticonvulsants have shown benefit in conditions associated with pathologic impulsivity, such as substance abuse, impulse-control, and cluster B disorders.10
Growing evidence shows that bulimia nervosa and BED may be associated with pathologic impulsivity.
Combination therapies are generally more effective than monotherapies in patients with mood disorders, uncomplicated obesity, and possibly bulimia nervosa. Even so, few trials have systematically studied combination therapy in managing patients with BED.
Two studies compared psychotherapy and antidepressants alone and in combination in treating BED.21,23 Both showed that CBT alone was more effective in decreasing binge frequency than desipramine alone,21 fluoxetine alone,23 and the combination of CBT and medication. On the other hand, patients who took desipramine either alone or in combination experienced a greater degree of weight loss than those who did not take desipramine.21
In another combination therapy, exercise has been shown to be an effective adjunct to CBT in maintenance treatment of obese women with BED.36
No studies have compared behavioral weight management or a specialized psychotherapy in combination with an antiobesity drug or a weight-loss anticonvulsant in treating BED.
Treatment recommendations
In our experience, BED patients—particularly those with obesity and psychopathology—often do best with some combination of psychological treatment and medication:
- The psychological component may be behavioral weight-loss treatment, a specialized psychotherapy such as CBT or IPT, or some combination of behavioral weight-loss treatment and specialized psychotherapy.
- The medication component may consist of an antidepressant, anticonvulsant, antiobesity drug, or multiple drugs (such as an SSRI or sibutramine with topiramate for BED with major depression, or topiramate with lithium for BED with bipolar disorder).
Although combination therapies may be optimal for some patients, this approach remains unproven in controlled trials.
Patient preference. In addition to comorbidities, patient preference is an important consideration when choosing BED treatments. We determine our patients’ preferences by educating them as much as possible about their options. We explain the benefits and weaknesses of all treatments and encourage them to participate in forming their individualized treatment plans.
Patients sometimes have strong treatment preferences. Some prefer psychological treatments, whereas others prefer medications. Working with patient preferences enhances treatment adherence. For example, patients who fail a preferred treatment are often more willing to adhere to another treatment modality about which they initially were skeptical.
Related resources
- Bray GA, Bouchard C (eds). Handbook of obesity: clinical applications (2nd ed). New York, NY: Marcel Dekker, 2004.
- Cooper Z, Zairburn CG, Hawker DM. Cognitive behavioral treatment of obesity. A clinician’s guide. New York: Guilford Press, 2003.
- Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Eskalith, others
- Orlistat • Xenical
- Sertraline • Zoloft
- Sibutramine • Meridia
- Topiramate • Topamax
- Venlafaxine • Effexor
- Zonisamide • Zonegran
Disclosure
Dr. Kotwal receives grant support from Elan Corporation and is a speaker for Ortho-McNeil Pharmaceutical and Pfizer Inc.
Dr. Kaneria and Ms. Guerdjikova report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. McElroy is a consultant to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corporation, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Co., and Ortho-McNeil Pharmaceutical. She receives grant/research support from Elan Pharmaceuticals, Forest Pharmaceuticals, Merck & Co., Ortho-McNeil Pharmaceutical, and Sanofi-Synthelabo and is a speaker for Eli Lilly and Co. and Ortho-McNeil Pharmaceutical.
1. Pope HG, Hudson JI. Bulimia nervosa: Persistent disorders requires equally persistent treatment. Current Psychiatry 2004;3(1):13-22.
2. Halmi KA. Anorexia nervosa: Dual therapy can bring patients back from the brink. Current Psychiatry 2004;3(3):39-56.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed). Washington, DC: American Psychiatric Association, 1994.
4. Agras WS. Treatment of binge eating disorder. In: Gabbard GO (ed). Treatments of psychiatric disorders (3rd ed). Washington, DC: American Psychiatric Press, 2001;2209-19.
5. de Zwaan M. Binge eating disorder and obesity. Int J Obes Relat Metab Disord 2001;25(suppl 1):S51-5.
6. Dingemans AE, Bruna MJ, van Furth EF. Binge eating disorder: a review. Int J Obes Relat Metab Disord 2002;26:299-307.
7. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361:407-16.
8. Walsh BT (ed). The current status of binge eating disorder. Int J Eat Disord 2003;34(suppl):S1-120.
9. Devlin MJ, Goldfein JA, Dobrow I. What is this thing called BED? Current status of binge eating disorder nosology. Int J Eat Disord 2003;34(suppl):S2-18.
10. McElroy SL, Kotwal R. Binge eating. In: Hollander E, Stein D (eds). Handbook of impulse control disorders Washington, DC: American Psychiatric Press (in press).
11. Smith DE, Marcus MD, Lewis CE, et al. Prevalence of binge eating disorder, obesity, and depression in a biracial cohort of young adults. Ann Behav Med 1998;20:227-32.
12. Kruger S, Shugar G, Cooke RG. Comorbidity of binge eating disorder and the partial binge eating syndrome with bipolar disorder. Int J Eat Disord 1996;19:45-52.
13. Fairburn CG, Cooper Z, Doll H, et al. The natural course of bulimia nervosa and binge eating disorder in young women. Arch Gen Psychiatry 2000;57:659-65.
14. Striegel-Moore RH, Franko DL. Epidemiology of binge eating disorder. Int J Eat Disord 2003;34(suppl):S19-29.
15. Tammela LI, Rissanen A, Kuikka JT, et al. Treatment improves serotonin transporter binding and reduces binge eating. Psychopharmacology (Berl) 2003;170:89-93.
16. Wang GJ, Volkow ND, Logan J, et al. Brain dopamine and obesity. Lancet 2001;357:354-7.
17. Branson R, Potoczna N, Kral JG, et al. Binge eating as a major phenotype of melanocortin 4 receptor gene mutations. N Engl J Med 2003;348:1096-103.
18. Fairburn CG, Doll HA, Welch SL, et al. Risk factors for binge eating disorder: a community-based, case-control study. Arch Gen Psychiatry 1998;55:425-32.
19. Striegel-Moore RH, Dohm FA, Pike KM, et al. Abuse, bullying, and discrimination as risk factors for binge eating disorder. Am J Psychiatry 2002;159:1902-7.
20. Wonderlich SA, de Zwaan M, Mitchell JE, et al. Psychological and dietary treatments of binge eating disorder: conceptual implications. Int J Eat Disord 2003;34(suppl):S58-78.
21. Agras WS, Telch DF, Arnow B, et al. Weight loss, cognitive-behavioral, and desipramine treatments in binge eating disorder. An additive design. Behav Ther 1994;25:225-38.
22. Wilfley DE, Welch RR, Stein RI, et al. A randomized comparison of group cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge eating disorder. Arch Gen Psychiatry 2002;59:713-21.
23. Grilo CM. A controlled study of cognitive behavioral therapy and fluoxetine for binge eating disorder (presentation) Charleston, SC: Eating Disorders Research Society annual meeting, 2002.
24. Telch CF, Agras WS, Linehan MM. Dialectical behavior therapy for binge eating disorder. J Consult Clin Psychol 2001;69:1061-5.
25. Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
26. Appolinario JC, McElroy SL. Pharmacologic approaches in the treatment of binge eating disorder. Curr Drug Targets (in press).
27. Malhotra S, King KH, Welge JA, et al. Venlafaxine treatment of binge-eating disorder associated with obesity: a series of 35 patients. J Clin Psychiatry 2002;63:802-6.
28. Anderson JW, Greenway FL, Fujioka K, et al. Bupropion SR enhances weight loss: a 48-week double-blind, placebo-controlled trial. Obes Res 2002;10:633-41.
29. McElroy SL, Kotwal R, Malhotra S, et al. Are mood disorders and obesity related? A review for the mental health professional. J Clin Psychiatry (in press).
30. Appolinario JC, Bacaltchuk J, Sichieri R, et al. A randomized, double-blind, placebo-controlled study of sibutramine in the treatment of binge-eating disorder. Arch Gen Psychiatry 2003;60:1109-16.
31. Mitchell JE, Gosnell BA, Roerig JL, et al. Effects of sibutramine on binge eating, hunger, and fullness in a laboratory human feeding paradigm. Obes Res 2003;11:599-602.
32. Bray GA, Hollander P, Klein S, et al. A 6-month randomized, placebo-controlled, dose-ranging trial of topiramate for weight loss in obesity. Obes Res 2003;11:722-33.
33. Gadde KM, Franciscy DM, Wagner HR, 2nd, Krishnan KR. Zonisamide for weight loss in obese adults: a randomized controlled trial. JAMA 2003;289:1820-5.
34. McElroy SL, Arnold LM, Shapira NA, et al. Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial. Am J Psychiatry 2003;160:255-61.
35. McElroy SL, Kotwal R, Hudson JI, et al. Zonisamide in the treatment of binge-eating disorder: an open-label, prospective trial. J Clin Psychiatry 2004;65:50-6.
36. Pendleton VR, Goodrick GK, Poston WSC, et al. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int J Eat Disord 2002;31(2):172-84.
Managing patients with binge-eating disorder (BED) often requires behavioral, medical, and psychiatric interventions.
These patients suffer from recurrent episodes of distressing, uncontrollable overeating, but they do not purge or show other compensatory weight-loss behaviors common to bulimia nervosa1 and anorexia nervosa.2-10 As a result, they are often overweight or obese and may have obesity-related illnesses, such as hypertension or type 2 diabetes. Mild to severe depression—unipolar or bipolar—is a common psychopathology.
Because no one treatment fits all patients with binge eating disorder, their management usually requires an individualized program of:
- behavioral weight control
- psychotherapy
- and sometimes medications.
In our weight management clinic, we consider medication options based on patient preference and whether BED is uncomplicated (Figure 1) or coexists with a mood disorder (Figure 2).
This article presents the evidence on which we base our comprehensive approach. General psychiatrists with knowledge of BED can treat patients with this eating disorder, although complicated cases may require referral for specialized treatment.
Figure 1 Medication options for uncomplicated BED
Clinical characteristics
Psychiatric comorbidity. BED often occurs in patients with mood, anxiety, substance-abuse, impulsecontrol, and personality disorders.4,6,10-12 Mood disorder—particularly depression—appears to be the most common comorbidity. BED can occur with bipolar disorder12—a comorbidity that in our experience is underrecognized both clinically and in the literature.
Patients with BED and bipolar disorder show increased impulsivity and mood lability. As bipolar II disorder and other “soft-spectrum” forms are more common than bipolar I disorder, BED is also more likely to occur with hypomania than mania.
Overweight. Not surprisingly, BED is associated with overweight and obesity.5,8,9,11 Not all patients with BED are overweight or obese, but most who participate in clinical trials of BED treatments are at least overweight. BED has been reported in up to:
- 30% of participants in weight-loss programs7
- 70% of participants in groups such as Overeaters Anonymous
- 50% of patients who seek bariatric surgery.5
In our experience, patients are often more distressed by their weight than by their binge eating, depression, or anxiety. Indeed, overweight and obesity are the usual reasons patients with BED present for treatment at our center.
Diagnosis. BED’s validity as a clinical diagnosis has been controversial since the disorder was first included in DSM-IV (Table 1).3 Debate continues about some definitions in the DSM criteria, including what amount of food is “definitely larger” than most people would eat and what is “loss of control over eating.”
Nevertheless, screening for BED is relatively easy. Clinicians may use the eating disorder section of the Structured Clinical Interview for DSM-IV or the Eating Disorders Examination. Alternatively, simply ask patients if they have episodes of uncontrollable overeating, during which they eat unusually large amounts of food and their eating feels out of control.
Course. BED begins in adolescence or adulthood. Disease course is variable, with periods of remission, recurrence, and chronicity.6,7,10 Interestingly, one prospective study showed that even if the binge eating resolves, persons may still develop obesity.13
Prevalence. BED affects 1.5% to 3% of the U.S. population. It is more common in women than men, equally prevalent in whites and blacks, and more prevalent than anorexia nervosa and bulimia nervosa combined.11,14 Subthreshold BED—such as obesity with infrequent or nondistressing binge eating—appears to be much more common,10 although no data are available.
Theories of binge eating
BED’s cause is unknown, but biological, familial, and psychosocial factors have been implicated.
Biological factors. The neurotransmitters serotonin (5-HT) and dopamine—as well as various peptides—have been shown to help regulate feeding behavior.10
Table 1
Diagnostic criteria for binge-eating disorder*
|
| * Research criteria, DSM-IV-TR appendix B. |
| Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th edition, text revision. Copyright 2000. American Psychiatric Association. |
Serotonin. Reduced 5-HT transporter binding has been shown in obese women with BED.15 Their 5-HT binding improved and binge eating subsided with group psychotherapy and fluoxetine, although the women continued to gain weight.
Figure 2 Medication options for BED with obesity and a mood disorder*
Dopamine. Obese patients who compulsively overeat may have lower levels of dopamine D2 receptors than do normal-weight controls.16
Genetic factors. In severely obese patients (body mass index 44±2), those with a DSM-IV diagnosis of BED exhibited mutations of the melanocortin 4 receptor gene, which affects the anorectic properties of alpha melanocyte-stimulating hormone.17
Familial factors associated with BED include parental depression and obesity.18
Psychosocial correlates include physical and sexual abuse, bullying by peers, and discrimination because of being overweight.19
Treatment recommendations
Few systematic studies have examined BED treatment. Emerging research suggests that behavioral weight-loss treatment, specialized psychotherapies, and medications may be effective in some patients with BED.4,6,8
Behavioral weight-loss treatment’s main goal is to manage the patient’s weight with a lower-calorie, healthy diet and to increase exercise.20,21
Over the short term (<1 year), behavioral weight-loss treatment produces similar weight loss in obese patients with or without BED; long-term results in both groups, however, have not been satisfactory.20,21 No studies have examined the efficacy of specialized diets (such as low-carbohydrate regimens) in patients with BED.
Specialized psychotherapy’s goal is to modify bingeeating behavior with behavioral self-management strategies, reducing interpersonal dysfunction and stress, and/or managing affective dysregulation.
Cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) have been effective in reducing binge eating, both acutely and for up to 12 months4,20-24 but less effective in achieving and maintaining weight loss. Patients who achieve remission in binge eating after undergoing CBT or IPI often experience modest but stable weight loss.20-22 For example, in a comparison study of CBT and IPT:
- After 20 weekly sessions, patients whose binge eating was in remission lost weight (mean body mass index [BMI] −0.5 ± 1.5 kg/m2), whereas those who continued to binge gained weight (mean BMI +0.4 ±2.0 kg/m2).
- At 12 months’ follow-up, patients still in remission continued to lose weight (mean BMI −1.0 ± 3.0 kg/m2), whereas those no longer in remission gained weight (mean BMI +0.7 ±2.9 kg/m2[P = 0.01]).22
Self-help and dialectical behavioral therapy (DBT) may also help reduce binge eating in BED. As with CBT and IPT, they are less effective in weight loss. In the only controlled study of DBT,24 patients achieved an average 2.5-lb weight loss after 20 weeks of DBT, compared with an average 0.6-lb weight gain in the control group. This difference was not significant, and the report did not include data on weight loss maintenance.
In summary, CBT may be more effective than behavioral weight loss treatment for reducing binge eating, but behavioral weight loss is more effective for weight loss.
Medications for BED
Medications that have been tried for BED include antidepressants, appetite suppressants, and anticonvulsants.25,26 Antidepressants are used to treat BED because:
- BED is often associated with depressive symptoms and disorders.
- BED is related to bulimia nervosa, and placebo-controlled trials have shown that the binge eating of bulimia nervosa responds to several classes of antidepressants. The selective serotonin reuptake inhibitor (SSRI) fluoxetine is the only medication indicated for treating any eating disorder (bulimia nervosa).
- Bupropion and venlafaxine—a serotonin-norepinephrine reuptake inhibitor (SNRI)—have weight-loss properties.
SSRIs are the most extensively studied antidepressants for treating BED. SSRIs have weightloss properties, but only short term.25-26 Citalopram, fluoxetine, fluvoxamine, and sertraline have reduced binge eating and body weight more effectively than placebo during 6 to 9 weeks of treatment (Table 2).25-26 However, one controlled study23 showed that fluoxetine was not significantly more effective than placebo in reducing binge frequency or body weight after 16 weeks.
TCAs. Studies of tricyclic antidepressants (TCAs) for BED are sparse, and results have been mixed. In one trial, imipramine was similar to placebo in reducing binge frequency and body weight. In a placebo-controlled study of patients with nonpurging bulimia nervosa, desipramine reduced binge eating but had no effect on body weight.25,26
Table 2
Drug therapies shown to be effective for BED*
| Medication | Binge eating | Weight | Depression | Study size | Duration (weeks) | Dosage (mg/d) |
|---|---|---|---|---|---|---|
| Antidepressants | ||||||
| Citalopram | + | + | − | 38 | 6 | 20 to 60 |
| Fluoxetine † | + | + | + | 60 | 6 | 20 to 80 |
| Fluvoxamine | + | + | − | 85 | 9 | 50 to 300 |
| Sertraline | + | + | − | 34 | 6 | 50 to 200 |
| Appetite suppressant | ||||||
| Sibutramine | + | + | + | 60 | 12 | 15 |
| Anticonvulsant | ||||||
| Topiramate | + | + | − | 61 | 14 | 50 to 600 |
| + Improvement | ||||||
| − No improvement | ||||||
| * Randomized, controlled trials. Antidepressants were studied in patients with BED; sibutramine and topiramate were studied in patients with BED and associated obesity. | ||||||
| † One 16-week trial of fluoxetine for BED (reference 23) did not show statistically significant differences in post-treatment binge frequency or body-mass index. | ||||||
Venlafaxine. In a retrospective review of 35 consecutive obese women with BED, venlafaxine, mean 222 mg/d for 28 to 300 days (median 120 days), reduced binge eating, body weight, and depressive symptoms.27
Bupropion has been more effective than placebo for treating:
- uncomplicated obesity (short- and long-term)
- obesity associated with depressive symptoms
- bulimia nervosa (although bupropion is contraindicated in these patients because of seizure risk).26,28,29
No controlled trials have studied bupropion for BED. When using dosages effective in depressive disorders, we find bupropion helpful in reducing binge eating, body weight, and depressive symptoms in BED patients.
Appetite suppressants decrease appetite and weight, may increase satiety, and may reduce depressive symptoms.
Sibutramine—a serotonin, norepinephrine, and dopamine reuptake inhibitor indicated for managing obesity—has been reported effective in BED in a 12-week, randomized, double-blind, placebo-controlled trial. A 15-mg/d dosage reduced binge frequency, body weight, and depressive symptoms more effectively than placebo in 60 obese patients with BED.30 Most-frequent adverse effects (dry mouth and constipation) were mild and benign, and no significant complications were observed.
Sibutramine’s mechanism of action in BED is unknown. However, it suppressed food intake during binge-eating episodes in patients with BED in a randomized, controlled, cross-over laboratory study.31
Orlistat. We know of no published controlled studies of the lipase inhibitor orlistat in treating BED. In our experience, some patients do well with this agent, though we have observed infrequent purging episodes with it in patients with BED.
With orlistat, 120 mg tid, our BED patients have experienced weight loss comparable to that seen in uncomplicated obesity at similar dosages. Orlistat seems most effective for:
- patients whose binge eating is in remission
- those who responded to behavioral weightloss treatment, a psychological treatment, or another medication.
Anticonvulsants such as topiramate and zonisamide have been shown effective in treating obesity32,33 and are sometimes used to treat BED. Obese BED patients with mood disorders often do best with psychotherapy plus medication
Topiramate at dosages of 50 to 600 mg/d (median 212 mg/d) reduced binge-eating frequency, obsessive-compulsive features of binge eating, and body weight more effectively than placebo in a 14-week study of 61 obese patients with BED. These effects were maintained across 48 weeks in an open-label extension trial.34
Zonisamide, mean 513 mg/d, produced similar results during a prospective, open-label, 12-week trial in 15 patients with BED.35 A controlled trial to replicate these findings is ongoing.
BED may respond to anticonvulsant therapy for several reasons:
- Some anticonvulsants are effective in treating bipolar disorder, which may occur with BED.12
- Some anticonvulsants have shown benefit in conditions associated with pathologic impulsivity, such as substance abuse, impulse-control, and cluster B disorders.10
Growing evidence shows that bulimia nervosa and BED may be associated with pathologic impulsivity.
Combination therapies are generally more effective than monotherapies in patients with mood disorders, uncomplicated obesity, and possibly bulimia nervosa. Even so, few trials have systematically studied combination therapy in managing patients with BED.
Two studies compared psychotherapy and antidepressants alone and in combination in treating BED.21,23 Both showed that CBT alone was more effective in decreasing binge frequency than desipramine alone,21 fluoxetine alone,23 and the combination of CBT and medication. On the other hand, patients who took desipramine either alone or in combination experienced a greater degree of weight loss than those who did not take desipramine.21
In another combination therapy, exercise has been shown to be an effective adjunct to CBT in maintenance treatment of obese women with BED.36
No studies have compared behavioral weight management or a specialized psychotherapy in combination with an antiobesity drug or a weight-loss anticonvulsant in treating BED.
Treatment recommendations
In our experience, BED patients—particularly those with obesity and psychopathology—often do best with some combination of psychological treatment and medication:
- The psychological component may be behavioral weight-loss treatment, a specialized psychotherapy such as CBT or IPT, or some combination of behavioral weight-loss treatment and specialized psychotherapy.
- The medication component may consist of an antidepressant, anticonvulsant, antiobesity drug, or multiple drugs (such as an SSRI or sibutramine with topiramate for BED with major depression, or topiramate with lithium for BED with bipolar disorder).
Although combination therapies may be optimal for some patients, this approach remains unproven in controlled trials.
Patient preference. In addition to comorbidities, patient preference is an important consideration when choosing BED treatments. We determine our patients’ preferences by educating them as much as possible about their options. We explain the benefits and weaknesses of all treatments and encourage them to participate in forming their individualized treatment plans.
Patients sometimes have strong treatment preferences. Some prefer psychological treatments, whereas others prefer medications. Working with patient preferences enhances treatment adherence. For example, patients who fail a preferred treatment are often more willing to adhere to another treatment modality about which they initially were skeptical.
Related resources
- Bray GA, Bouchard C (eds). Handbook of obesity: clinical applications (2nd ed). New York, NY: Marcel Dekker, 2004.
- Cooper Z, Zairburn CG, Hawker DM. Cognitive behavioral treatment of obesity. A clinician’s guide. New York: Guilford Press, 2003.
- Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Eskalith, others
- Orlistat • Xenical
- Sertraline • Zoloft
- Sibutramine • Meridia
- Topiramate • Topamax
- Venlafaxine • Effexor
- Zonisamide • Zonegran
Disclosure
Dr. Kotwal receives grant support from Elan Corporation and is a speaker for Ortho-McNeil Pharmaceutical and Pfizer Inc.
Dr. Kaneria and Ms. Guerdjikova report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. McElroy is a consultant to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corporation, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Co., and Ortho-McNeil Pharmaceutical. She receives grant/research support from Elan Pharmaceuticals, Forest Pharmaceuticals, Merck & Co., Ortho-McNeil Pharmaceutical, and Sanofi-Synthelabo and is a speaker for Eli Lilly and Co. and Ortho-McNeil Pharmaceutical.
Managing patients with binge-eating disorder (BED) often requires behavioral, medical, and psychiatric interventions.
These patients suffer from recurrent episodes of distressing, uncontrollable overeating, but they do not purge or show other compensatory weight-loss behaviors common to bulimia nervosa1 and anorexia nervosa.2-10 As a result, they are often overweight or obese and may have obesity-related illnesses, such as hypertension or type 2 diabetes. Mild to severe depression—unipolar or bipolar—is a common psychopathology.
Because no one treatment fits all patients with binge eating disorder, their management usually requires an individualized program of:
- behavioral weight control
- psychotherapy
- and sometimes medications.
In our weight management clinic, we consider medication options based on patient preference and whether BED is uncomplicated (Figure 1) or coexists with a mood disorder (Figure 2).
This article presents the evidence on which we base our comprehensive approach. General psychiatrists with knowledge of BED can treat patients with this eating disorder, although complicated cases may require referral for specialized treatment.
Figure 1 Medication options for uncomplicated BED
Clinical characteristics
Psychiatric comorbidity. BED often occurs in patients with mood, anxiety, substance-abuse, impulsecontrol, and personality disorders.4,6,10-12 Mood disorder—particularly depression—appears to be the most common comorbidity. BED can occur with bipolar disorder12—a comorbidity that in our experience is underrecognized both clinically and in the literature.
Patients with BED and bipolar disorder show increased impulsivity and mood lability. As bipolar II disorder and other “soft-spectrum” forms are more common than bipolar I disorder, BED is also more likely to occur with hypomania than mania.
Overweight. Not surprisingly, BED is associated with overweight and obesity.5,8,9,11 Not all patients with BED are overweight or obese, but most who participate in clinical trials of BED treatments are at least overweight. BED has been reported in up to:
- 30% of participants in weight-loss programs7
- 70% of participants in groups such as Overeaters Anonymous
- 50% of patients who seek bariatric surgery.5
In our experience, patients are often more distressed by their weight than by their binge eating, depression, or anxiety. Indeed, overweight and obesity are the usual reasons patients with BED present for treatment at our center.
Diagnosis. BED’s validity as a clinical diagnosis has been controversial since the disorder was first included in DSM-IV (Table 1).3 Debate continues about some definitions in the DSM criteria, including what amount of food is “definitely larger” than most people would eat and what is “loss of control over eating.”
Nevertheless, screening for BED is relatively easy. Clinicians may use the eating disorder section of the Structured Clinical Interview for DSM-IV or the Eating Disorders Examination. Alternatively, simply ask patients if they have episodes of uncontrollable overeating, during which they eat unusually large amounts of food and their eating feels out of control.
Course. BED begins in adolescence or adulthood. Disease course is variable, with periods of remission, recurrence, and chronicity.6,7,10 Interestingly, one prospective study showed that even if the binge eating resolves, persons may still develop obesity.13
Prevalence. BED affects 1.5% to 3% of the U.S. population. It is more common in women than men, equally prevalent in whites and blacks, and more prevalent than anorexia nervosa and bulimia nervosa combined.11,14 Subthreshold BED—such as obesity with infrequent or nondistressing binge eating—appears to be much more common,10 although no data are available.
Theories of binge eating
BED’s cause is unknown, but biological, familial, and psychosocial factors have been implicated.
Biological factors. The neurotransmitters serotonin (5-HT) and dopamine—as well as various peptides—have been shown to help regulate feeding behavior.10
Table 1
Diagnostic criteria for binge-eating disorder*
|
| * Research criteria, DSM-IV-TR appendix B. |
| Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th edition, text revision. Copyright 2000. American Psychiatric Association. |
Serotonin. Reduced 5-HT transporter binding has been shown in obese women with BED.15 Their 5-HT binding improved and binge eating subsided with group psychotherapy and fluoxetine, although the women continued to gain weight.
Figure 2 Medication options for BED with obesity and a mood disorder*
Dopamine. Obese patients who compulsively overeat may have lower levels of dopamine D2 receptors than do normal-weight controls.16
Genetic factors. In severely obese patients (body mass index 44±2), those with a DSM-IV diagnosis of BED exhibited mutations of the melanocortin 4 receptor gene, which affects the anorectic properties of alpha melanocyte-stimulating hormone.17
Familial factors associated with BED include parental depression and obesity.18
Psychosocial correlates include physical and sexual abuse, bullying by peers, and discrimination because of being overweight.19
Treatment recommendations
Few systematic studies have examined BED treatment. Emerging research suggests that behavioral weight-loss treatment, specialized psychotherapies, and medications may be effective in some patients with BED.4,6,8
Behavioral weight-loss treatment’s main goal is to manage the patient’s weight with a lower-calorie, healthy diet and to increase exercise.20,21
Over the short term (<1 year), behavioral weight-loss treatment produces similar weight loss in obese patients with or without BED; long-term results in both groups, however, have not been satisfactory.20,21 No studies have examined the efficacy of specialized diets (such as low-carbohydrate regimens) in patients with BED.
Specialized psychotherapy’s goal is to modify bingeeating behavior with behavioral self-management strategies, reducing interpersonal dysfunction and stress, and/or managing affective dysregulation.
Cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) have been effective in reducing binge eating, both acutely and for up to 12 months4,20-24 but less effective in achieving and maintaining weight loss. Patients who achieve remission in binge eating after undergoing CBT or IPI often experience modest but stable weight loss.20-22 For example, in a comparison study of CBT and IPT:
- After 20 weekly sessions, patients whose binge eating was in remission lost weight (mean body mass index [BMI] −0.5 ± 1.5 kg/m2), whereas those who continued to binge gained weight (mean BMI +0.4 ±2.0 kg/m2).
- At 12 months’ follow-up, patients still in remission continued to lose weight (mean BMI −1.0 ± 3.0 kg/m2), whereas those no longer in remission gained weight (mean BMI +0.7 ±2.9 kg/m2[P = 0.01]).22
Self-help and dialectical behavioral therapy (DBT) may also help reduce binge eating in BED. As with CBT and IPT, they are less effective in weight loss. In the only controlled study of DBT,24 patients achieved an average 2.5-lb weight loss after 20 weeks of DBT, compared with an average 0.6-lb weight gain in the control group. This difference was not significant, and the report did not include data on weight loss maintenance.
In summary, CBT may be more effective than behavioral weight loss treatment for reducing binge eating, but behavioral weight loss is more effective for weight loss.
Medications for BED
Medications that have been tried for BED include antidepressants, appetite suppressants, and anticonvulsants.25,26 Antidepressants are used to treat BED because:
- BED is often associated with depressive symptoms and disorders.
- BED is related to bulimia nervosa, and placebo-controlled trials have shown that the binge eating of bulimia nervosa responds to several classes of antidepressants. The selective serotonin reuptake inhibitor (SSRI) fluoxetine is the only medication indicated for treating any eating disorder (bulimia nervosa).
- Bupropion and venlafaxine—a serotonin-norepinephrine reuptake inhibitor (SNRI)—have weight-loss properties.
SSRIs are the most extensively studied antidepressants for treating BED. SSRIs have weightloss properties, but only short term.25-26 Citalopram, fluoxetine, fluvoxamine, and sertraline have reduced binge eating and body weight more effectively than placebo during 6 to 9 weeks of treatment (Table 2).25-26 However, one controlled study23 showed that fluoxetine was not significantly more effective than placebo in reducing binge frequency or body weight after 16 weeks.
TCAs. Studies of tricyclic antidepressants (TCAs) for BED are sparse, and results have been mixed. In one trial, imipramine was similar to placebo in reducing binge frequency and body weight. In a placebo-controlled study of patients with nonpurging bulimia nervosa, desipramine reduced binge eating but had no effect on body weight.25,26
Table 2
Drug therapies shown to be effective for BED*
| Medication | Binge eating | Weight | Depression | Study size | Duration (weeks) | Dosage (mg/d) |
|---|---|---|---|---|---|---|
| Antidepressants | ||||||
| Citalopram | + | + | − | 38 | 6 | 20 to 60 |
| Fluoxetine † | + | + | + | 60 | 6 | 20 to 80 |
| Fluvoxamine | + | + | − | 85 | 9 | 50 to 300 |
| Sertraline | + | + | − | 34 | 6 | 50 to 200 |
| Appetite suppressant | ||||||
| Sibutramine | + | + | + | 60 | 12 | 15 |
| Anticonvulsant | ||||||
| Topiramate | + | + | − | 61 | 14 | 50 to 600 |
| + Improvement | ||||||
| − No improvement | ||||||
| * Randomized, controlled trials. Antidepressants were studied in patients with BED; sibutramine and topiramate were studied in patients with BED and associated obesity. | ||||||
| † One 16-week trial of fluoxetine for BED (reference 23) did not show statistically significant differences in post-treatment binge frequency or body-mass index. | ||||||
Venlafaxine. In a retrospective review of 35 consecutive obese women with BED, venlafaxine, mean 222 mg/d for 28 to 300 days (median 120 days), reduced binge eating, body weight, and depressive symptoms.27
Bupropion has been more effective than placebo for treating:
- uncomplicated obesity (short- and long-term)
- obesity associated with depressive symptoms
- bulimia nervosa (although bupropion is contraindicated in these patients because of seizure risk).26,28,29
No controlled trials have studied bupropion for BED. When using dosages effective in depressive disorders, we find bupropion helpful in reducing binge eating, body weight, and depressive symptoms in BED patients.
Appetite suppressants decrease appetite and weight, may increase satiety, and may reduce depressive symptoms.
Sibutramine—a serotonin, norepinephrine, and dopamine reuptake inhibitor indicated for managing obesity—has been reported effective in BED in a 12-week, randomized, double-blind, placebo-controlled trial. A 15-mg/d dosage reduced binge frequency, body weight, and depressive symptoms more effectively than placebo in 60 obese patients with BED.30 Most-frequent adverse effects (dry mouth and constipation) were mild and benign, and no significant complications were observed.
Sibutramine’s mechanism of action in BED is unknown. However, it suppressed food intake during binge-eating episodes in patients with BED in a randomized, controlled, cross-over laboratory study.31
Orlistat. We know of no published controlled studies of the lipase inhibitor orlistat in treating BED. In our experience, some patients do well with this agent, though we have observed infrequent purging episodes with it in patients with BED.
With orlistat, 120 mg tid, our BED patients have experienced weight loss comparable to that seen in uncomplicated obesity at similar dosages. Orlistat seems most effective for:
- patients whose binge eating is in remission
- those who responded to behavioral weightloss treatment, a psychological treatment, or another medication.
Anticonvulsants such as topiramate and zonisamide have been shown effective in treating obesity32,33 and are sometimes used to treat BED. Obese BED patients with mood disorders often do best with psychotherapy plus medication
Topiramate at dosages of 50 to 600 mg/d (median 212 mg/d) reduced binge-eating frequency, obsessive-compulsive features of binge eating, and body weight more effectively than placebo in a 14-week study of 61 obese patients with BED. These effects were maintained across 48 weeks in an open-label extension trial.34
Zonisamide, mean 513 mg/d, produced similar results during a prospective, open-label, 12-week trial in 15 patients with BED.35 A controlled trial to replicate these findings is ongoing.
BED may respond to anticonvulsant therapy for several reasons:
- Some anticonvulsants are effective in treating bipolar disorder, which may occur with BED.12
- Some anticonvulsants have shown benefit in conditions associated with pathologic impulsivity, such as substance abuse, impulse-control, and cluster B disorders.10
Growing evidence shows that bulimia nervosa and BED may be associated with pathologic impulsivity.
Combination therapies are generally more effective than monotherapies in patients with mood disorders, uncomplicated obesity, and possibly bulimia nervosa. Even so, few trials have systematically studied combination therapy in managing patients with BED.
Two studies compared psychotherapy and antidepressants alone and in combination in treating BED.21,23 Both showed that CBT alone was more effective in decreasing binge frequency than desipramine alone,21 fluoxetine alone,23 and the combination of CBT and medication. On the other hand, patients who took desipramine either alone or in combination experienced a greater degree of weight loss than those who did not take desipramine.21
In another combination therapy, exercise has been shown to be an effective adjunct to CBT in maintenance treatment of obese women with BED.36
No studies have compared behavioral weight management or a specialized psychotherapy in combination with an antiobesity drug or a weight-loss anticonvulsant in treating BED.
Treatment recommendations
In our experience, BED patients—particularly those with obesity and psychopathology—often do best with some combination of psychological treatment and medication:
- The psychological component may be behavioral weight-loss treatment, a specialized psychotherapy such as CBT or IPT, or some combination of behavioral weight-loss treatment and specialized psychotherapy.
- The medication component may consist of an antidepressant, anticonvulsant, antiobesity drug, or multiple drugs (such as an SSRI or sibutramine with topiramate for BED with major depression, or topiramate with lithium for BED with bipolar disorder).
Although combination therapies may be optimal for some patients, this approach remains unproven in controlled trials.
Patient preference. In addition to comorbidities, patient preference is an important consideration when choosing BED treatments. We determine our patients’ preferences by educating them as much as possible about their options. We explain the benefits and weaknesses of all treatments and encourage them to participate in forming their individualized treatment plans.
Patients sometimes have strong treatment preferences. Some prefer psychological treatments, whereas others prefer medications. Working with patient preferences enhances treatment adherence. For example, patients who fail a preferred treatment are often more willing to adhere to another treatment modality about which they initially were skeptical.
Related resources
- Bray GA, Bouchard C (eds). Handbook of obesity: clinical applications (2nd ed). New York, NY: Marcel Dekker, 2004.
- Cooper Z, Zairburn CG, Hawker DM. Cognitive behavioral treatment of obesity. A clinician’s guide. New York: Guilford Press, 2003.
- Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Eskalith, others
- Orlistat • Xenical
- Sertraline • Zoloft
- Sibutramine • Meridia
- Topiramate • Topamax
- Venlafaxine • Effexor
- Zonisamide • Zonegran
Disclosure
Dr. Kotwal receives grant support from Elan Corporation and is a speaker for Ortho-McNeil Pharmaceutical and Pfizer Inc.
Dr. Kaneria and Ms. Guerdjikova report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. McElroy is a consultant to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corporation, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Co., and Ortho-McNeil Pharmaceutical. She receives grant/research support from Elan Pharmaceuticals, Forest Pharmaceuticals, Merck & Co., Ortho-McNeil Pharmaceutical, and Sanofi-Synthelabo and is a speaker for Eli Lilly and Co. and Ortho-McNeil Pharmaceutical.
1. Pope HG, Hudson JI. Bulimia nervosa: Persistent disorders requires equally persistent treatment. Current Psychiatry 2004;3(1):13-22.
2. Halmi KA. Anorexia nervosa: Dual therapy can bring patients back from the brink. Current Psychiatry 2004;3(3):39-56.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed). Washington, DC: American Psychiatric Association, 1994.
4. Agras WS. Treatment of binge eating disorder. In: Gabbard GO (ed). Treatments of psychiatric disorders (3rd ed). Washington, DC: American Psychiatric Press, 2001;2209-19.
5. de Zwaan M. Binge eating disorder and obesity. Int J Obes Relat Metab Disord 2001;25(suppl 1):S51-5.
6. Dingemans AE, Bruna MJ, van Furth EF. Binge eating disorder: a review. Int J Obes Relat Metab Disord 2002;26:299-307.
7. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361:407-16.
8. Walsh BT (ed). The current status of binge eating disorder. Int J Eat Disord 2003;34(suppl):S1-120.
9. Devlin MJ, Goldfein JA, Dobrow I. What is this thing called BED? Current status of binge eating disorder nosology. Int J Eat Disord 2003;34(suppl):S2-18.
10. McElroy SL, Kotwal R. Binge eating. In: Hollander E, Stein D (eds). Handbook of impulse control disorders Washington, DC: American Psychiatric Press (in press).
11. Smith DE, Marcus MD, Lewis CE, et al. Prevalence of binge eating disorder, obesity, and depression in a biracial cohort of young adults. Ann Behav Med 1998;20:227-32.
12. Kruger S, Shugar G, Cooke RG. Comorbidity of binge eating disorder and the partial binge eating syndrome with bipolar disorder. Int J Eat Disord 1996;19:45-52.
13. Fairburn CG, Cooper Z, Doll H, et al. The natural course of bulimia nervosa and binge eating disorder in young women. Arch Gen Psychiatry 2000;57:659-65.
14. Striegel-Moore RH, Franko DL. Epidemiology of binge eating disorder. Int J Eat Disord 2003;34(suppl):S19-29.
15. Tammela LI, Rissanen A, Kuikka JT, et al. Treatment improves serotonin transporter binding and reduces binge eating. Psychopharmacology (Berl) 2003;170:89-93.
16. Wang GJ, Volkow ND, Logan J, et al. Brain dopamine and obesity. Lancet 2001;357:354-7.
17. Branson R, Potoczna N, Kral JG, et al. Binge eating as a major phenotype of melanocortin 4 receptor gene mutations. N Engl J Med 2003;348:1096-103.
18. Fairburn CG, Doll HA, Welch SL, et al. Risk factors for binge eating disorder: a community-based, case-control study. Arch Gen Psychiatry 1998;55:425-32.
19. Striegel-Moore RH, Dohm FA, Pike KM, et al. Abuse, bullying, and discrimination as risk factors for binge eating disorder. Am J Psychiatry 2002;159:1902-7.
20. Wonderlich SA, de Zwaan M, Mitchell JE, et al. Psychological and dietary treatments of binge eating disorder: conceptual implications. Int J Eat Disord 2003;34(suppl):S58-78.
21. Agras WS, Telch DF, Arnow B, et al. Weight loss, cognitive-behavioral, and desipramine treatments in binge eating disorder. An additive design. Behav Ther 1994;25:225-38.
22. Wilfley DE, Welch RR, Stein RI, et al. A randomized comparison of group cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge eating disorder. Arch Gen Psychiatry 2002;59:713-21.
23. Grilo CM. A controlled study of cognitive behavioral therapy and fluoxetine for binge eating disorder (presentation) Charleston, SC: Eating Disorders Research Society annual meeting, 2002.
24. Telch CF, Agras WS, Linehan MM. Dialectical behavior therapy for binge eating disorder. J Consult Clin Psychol 2001;69:1061-5.
25. Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
26. Appolinario JC, McElroy SL. Pharmacologic approaches in the treatment of binge eating disorder. Curr Drug Targets (in press).
27. Malhotra S, King KH, Welge JA, et al. Venlafaxine treatment of binge-eating disorder associated with obesity: a series of 35 patients. J Clin Psychiatry 2002;63:802-6.
28. Anderson JW, Greenway FL, Fujioka K, et al. Bupropion SR enhances weight loss: a 48-week double-blind, placebo-controlled trial. Obes Res 2002;10:633-41.
29. McElroy SL, Kotwal R, Malhotra S, et al. Are mood disorders and obesity related? A review for the mental health professional. J Clin Psychiatry (in press).
30. Appolinario JC, Bacaltchuk J, Sichieri R, et al. A randomized, double-blind, placebo-controlled study of sibutramine in the treatment of binge-eating disorder. Arch Gen Psychiatry 2003;60:1109-16.
31. Mitchell JE, Gosnell BA, Roerig JL, et al. Effects of sibutramine on binge eating, hunger, and fullness in a laboratory human feeding paradigm. Obes Res 2003;11:599-602.
32. Bray GA, Hollander P, Klein S, et al. A 6-month randomized, placebo-controlled, dose-ranging trial of topiramate for weight loss in obesity. Obes Res 2003;11:722-33.
33. Gadde KM, Franciscy DM, Wagner HR, 2nd, Krishnan KR. Zonisamide for weight loss in obese adults: a randomized controlled trial. JAMA 2003;289:1820-5.
34. McElroy SL, Arnold LM, Shapira NA, et al. Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial. Am J Psychiatry 2003;160:255-61.
35. McElroy SL, Kotwal R, Hudson JI, et al. Zonisamide in the treatment of binge-eating disorder: an open-label, prospective trial. J Clin Psychiatry 2004;65:50-6.
36. Pendleton VR, Goodrick GK, Poston WSC, et al. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int J Eat Disord 2002;31(2):172-84.
1. Pope HG, Hudson JI. Bulimia nervosa: Persistent disorders requires equally persistent treatment. Current Psychiatry 2004;3(1):13-22.
2. Halmi KA. Anorexia nervosa: Dual therapy can bring patients back from the brink. Current Psychiatry 2004;3(3):39-56.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed). Washington, DC: American Psychiatric Association, 1994.
4. Agras WS. Treatment of binge eating disorder. In: Gabbard GO (ed). Treatments of psychiatric disorders (3rd ed). Washington, DC: American Psychiatric Press, 2001;2209-19.
5. de Zwaan M. Binge eating disorder and obesity. Int J Obes Relat Metab Disord 2001;25(suppl 1):S51-5.
6. Dingemans AE, Bruna MJ, van Furth EF. Binge eating disorder: a review. Int J Obes Relat Metab Disord 2002;26:299-307.
7. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361:407-16.
8. Walsh BT (ed). The current status of binge eating disorder. Int J Eat Disord 2003;34(suppl):S1-120.
9. Devlin MJ, Goldfein JA, Dobrow I. What is this thing called BED? Current status of binge eating disorder nosology. Int J Eat Disord 2003;34(suppl):S2-18.
10. McElroy SL, Kotwal R. Binge eating. In: Hollander E, Stein D (eds). Handbook of impulse control disorders Washington, DC: American Psychiatric Press (in press).
11. Smith DE, Marcus MD, Lewis CE, et al. Prevalence of binge eating disorder, obesity, and depression in a biracial cohort of young adults. Ann Behav Med 1998;20:227-32.
12. Kruger S, Shugar G, Cooke RG. Comorbidity of binge eating disorder and the partial binge eating syndrome with bipolar disorder. Int J Eat Disord 1996;19:45-52.
13. Fairburn CG, Cooper Z, Doll H, et al. The natural course of bulimia nervosa and binge eating disorder in young women. Arch Gen Psychiatry 2000;57:659-65.
14. Striegel-Moore RH, Franko DL. Epidemiology of binge eating disorder. Int J Eat Disord 2003;34(suppl):S19-29.
15. Tammela LI, Rissanen A, Kuikka JT, et al. Treatment improves serotonin transporter binding and reduces binge eating. Psychopharmacology (Berl) 2003;170:89-93.
16. Wang GJ, Volkow ND, Logan J, et al. Brain dopamine and obesity. Lancet 2001;357:354-7.
17. Branson R, Potoczna N, Kral JG, et al. Binge eating as a major phenotype of melanocortin 4 receptor gene mutations. N Engl J Med 2003;348:1096-103.
18. Fairburn CG, Doll HA, Welch SL, et al. Risk factors for binge eating disorder: a community-based, case-control study. Arch Gen Psychiatry 1998;55:425-32.
19. Striegel-Moore RH, Dohm FA, Pike KM, et al. Abuse, bullying, and discrimination as risk factors for binge eating disorder. Am J Psychiatry 2002;159:1902-7.
20. Wonderlich SA, de Zwaan M, Mitchell JE, et al. Psychological and dietary treatments of binge eating disorder: conceptual implications. Int J Eat Disord 2003;34(suppl):S58-78.
21. Agras WS, Telch DF, Arnow B, et al. Weight loss, cognitive-behavioral, and desipramine treatments in binge eating disorder. An additive design. Behav Ther 1994;25:225-38.
22. Wilfley DE, Welch RR, Stein RI, et al. A randomized comparison of group cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge eating disorder. Arch Gen Psychiatry 2002;59:713-21.
23. Grilo CM. A controlled study of cognitive behavioral therapy and fluoxetine for binge eating disorder (presentation) Charleston, SC: Eating Disorders Research Society annual meeting, 2002.
24. Telch CF, Agras WS, Linehan MM. Dialectical behavior therapy for binge eating disorder. J Consult Clin Psychol 2001;69:1061-5.
25. Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
26. Appolinario JC, McElroy SL. Pharmacologic approaches in the treatment of binge eating disorder. Curr Drug Targets (in press).
27. Malhotra S, King KH, Welge JA, et al. Venlafaxine treatment of binge-eating disorder associated with obesity: a series of 35 patients. J Clin Psychiatry 2002;63:802-6.
28. Anderson JW, Greenway FL, Fujioka K, et al. Bupropion SR enhances weight loss: a 48-week double-blind, placebo-controlled trial. Obes Res 2002;10:633-41.
29. McElroy SL, Kotwal R, Malhotra S, et al. Are mood disorders and obesity related? A review for the mental health professional. J Clin Psychiatry (in press).
30. Appolinario JC, Bacaltchuk J, Sichieri R, et al. A randomized, double-blind, placebo-controlled study of sibutramine in the treatment of binge-eating disorder. Arch Gen Psychiatry 2003;60:1109-16.
31. Mitchell JE, Gosnell BA, Roerig JL, et al. Effects of sibutramine on binge eating, hunger, and fullness in a laboratory human feeding paradigm. Obes Res 2003;11:599-602.
32. Bray GA, Hollander P, Klein S, et al. A 6-month randomized, placebo-controlled, dose-ranging trial of topiramate for weight loss in obesity. Obes Res 2003;11:722-33.
33. Gadde KM, Franciscy DM, Wagner HR, 2nd, Krishnan KR. Zonisamide for weight loss in obese adults: a randomized controlled trial. JAMA 2003;289:1820-5.
34. McElroy SL, Arnold LM, Shapira NA, et al. Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial. Am J Psychiatry 2003;160:255-61.
35. McElroy SL, Kotwal R, Hudson JI, et al. Zonisamide in the treatment of binge-eating disorder: an open-label, prospective trial. J Clin Psychiatry 2004;65:50-6.
36. Pendleton VR, Goodrick GK, Poston WSC, et al. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int J Eat Disord 2002;31(2):172-84.