User login
What is your hospital doing to mark DVT Awareness Month this year? Consider that last year a Virginia hospital used this occasion to educate their staff on VTE, which encompasses both DVT and PE. This training was the first step in the implementation of a multidisciplinary, hospital-wide process that resulted in the vast majority of patients receiving proper preventive treatment of this common killer.
According to the Society of Critical Care Medicine, VTE is the No. 1 preventable cause of hospital-associated death for medical inpatients. Most hospitals are struggling to decrease the number of DVTs and PEs in their patient population by teaching or reminding staff to check for risk factors in each patient and, if necessary, provide VTE prophylaxis. While this seems like a simple solution, anyone who’s currently struggling to turn the numbers around this way can assure you that it is an uphill battle. The good news is that Carilion Medical Center in Roanoke, Va., may have found a key to winning that battle.
First Steps toward Improvement
Carilion Medical Center is 625-bed tertiary care facility that typically operates at peak census. With a level-one trauma center and a separate building housing the women’s and children’s hospital, Carilion offers every kind of care except burn treatment and full organ transplants.
“We recognized that VTE prophylaxis is a very important area and that we had not addressed it,” says James Franko, MD, FACP, medical director, General Medicine and Hospitalist Services.
Carilion’s first attempt to tackle the problem was not effective, but it laid the groundwork for later success.
“In April of 2004 we began working with a committee, conducting an investigation to see how frequently patients were receiving VTE prophylaxis,” recalls Dr. Franko. “We found that it was about 30%, based on patient population where more than 80% met the criteria for receiving this prophylaxis.”
The committee then broke down the data to examine who was ordering the VTE prophylaxis and found that there were three groups of physicians.
“There were those who almost always ordered the treatment, including our trauma surgeons,” says Dr. Franko. “Then there were those who did it sometimes and another group of those who never ordered it. We saw that this was obviously a good opportunity for education.”
Initial Research and Planning
In summer 2004, the group implemented a pilot program for screening every single patient on one floor of the hospital—a floor where physicians were predominantly hospitalists. The pilot involved including an information sheet on each medical chart with a list of VTE risk and exclusion criteria. The results: “We saw only a modest increase in prophylaxis,” says Dr. Franko.
So he pushed to find a better way to focus attention on VTE prophylaxis, this time using the channel that Carilion Medical Center has in place to address quality improvement issues.
“Someone can pitch an idea to our Quality Council and ask for a charter team,” explains Kris Peters, RN, human resources education consultant for Carilion Medical Center. “That team is given a time frame and asked to perform research and make recommendations. We have a charter team for pneumonia, for heart failure, for MCI, … that’s worked well for us.”
In fall 2004, Carilion’s Quality Council commissioned a new charter team and gave them the mission of increasing the percentage of patients receiving VTE prophylaxis. The team consisted of Dr. Franko and other physicians, nursing staff, a pharmacist, researchers, a staff member from the medical records department, secretaries, and—as a late addition—Peters.
“There was strong emotional buy-in from everyone on the team,” recalls Dr. Franko, “because almost everyone has a family member or friend who have had an experience with a blood clot.”
Dr. Franko and other members of the team proceeded to gather information on the rates of use and made projections for prophylaxis. They also reviewed the first attempt to increase use.
“We realized that it was necessary to make this a mandatory approach, or there would be no improvement whatsoever,” says Dr. Franko.
One possibility the team explored and then rejected was incorporating VTE prophylaxis with a patient’s admission. “When patients are admitted, we fill out a very thorough nursing assessment form,” explains Dr. Franko. “This is a good point to gather the information, but we decided it was just too cumbersome.”
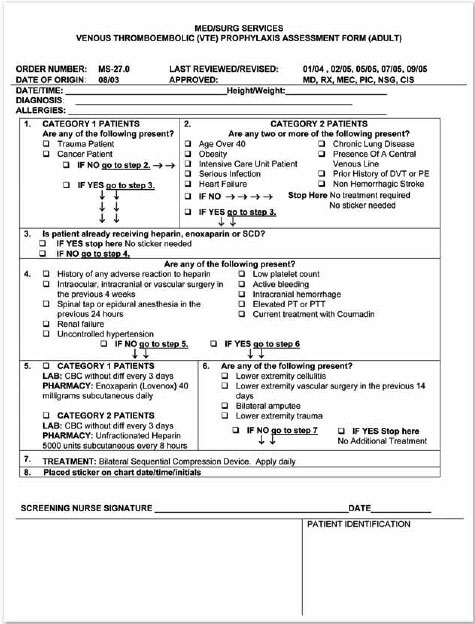
The team decided on the inclusion of a form with each patient’s medical chart that would lead the nursing staff through simple questions to determine whether the person should receive VTE prophylaxis. (See “VTE Prophylaxis Assessment Form [Adult],” at right.) The default is prophylaxis. “This was a bold step,” says Dr. Franko. With the form, “your patients are going to get VTE prophylaxis unless you tell us not to give it to them.”
Creating the VTE Prophylaxis Assessment Form
The multidisciplinary team needed to build the form using basic, easy-to-understand information. They began by breaking down the hospital’s patient population to determine who most needed the VTE prophylaxis. They found four groups:
- All trauma patients;
- All patients in ICU;
- Anyone with a diagnosis of cancer; and
- Anyone with a history of cancer. (See step 1 on the “VTE Prophylaxis Assessment Form,” at right.)
They also agreed that patients over age 40 with one other risk factor, such as smoking or drinking, would be considered at risk for DVT. (See step 2 on the “VTE Prophylaxis Assessment Form,” at right.)
“That is a significant percentage of our patients,” Dr. Franko points out. Because the women’s and children’s hospital is separate, a full 87% of Carilion’s patients are over 40.
The team then worked on exclusion factors that would eliminate patients in these groups from receiving prophylaxis. They agreed that patients with any of these exclusion criteria would automatically not receive prophylaxis. (See step 4 on the “VTE Prophylaxis Assessment Form,” at right.)
“We really struggled with how to administer the VTE prophylaxis,” admits Dr. Franko. “It was projected at one point that if we put all at-risk patients on low-molecular-weight heparins, we would increase our pharmacy’s budget by $3 million.”
With a great deal of reliance on the American College of Chest Physicians (ACCP) guidelines for VTE prophylaxis, the charter team decided on three treatment categories: low-molecular-weight heparins (enoxaparin, specifically), unfractionated heparins, and sequential compression devices (SCDs). (See step 5 on the “VTE Prophylaxis Assessment Form,” at right.)
“We use a lot of SCDs on our trauma patients,” says Dr. Franko, “but we still had to order more.” After talking to the hospital’s vascular surgeons and other staff, the charter team decided on patients to exclude from medications, including amputees and those who’d had recent vascular surgery. (See step 6 on the “VTE Prophylaxis Assessment Form,” at right.)
If the form indicates that prophylaxis is necessary, then the last step in completing the form is to have a physician add a bright pink sticker with his or her initials and the date and time.
“The pharmacy will prescribe with only that sticker on the chart,” says Dr. Franko. “Patients can get treatment earlier rather than later.”
Implementing the Form
The charter team still had to decide how the form would be presented to physicians and nursing staff. “We learned that there are no such things as standing orders,” says Dr. Franko. “But we can make the form a permanent part of each patient record, so that it cannot be discarded.”
The next hurdle was educating the staff, particularly nurses, on the new quality-improvement program. The team timed the implementation of the new process so that it began in March 2005, DVT Awareness Month. “We used the posters and giveaways provided by the Coalition to Prevent DVT to boost awareness in the staff,” says Peters. In April and May, the form went live.
“We used it for three months, then got information back from the nursing staff,” recalls Peters. “We went back to the committee with some suggested changes.” One of those changes was the inclusion of step 3: information on whether the patient was already receiving VTE prophylaxis.
The second wave of staff education began in late November, and the nursing staff continues to address the form in their bimonthly meetings. “Nurses fear the form, because they think it’s an order,” says Peters. “The top [of the form] will be done, but the bottom will be completely blank.”
She is working to educate nurses so that they are more comfortable with the form, and she has created an e-learning module with detailed information to supplement the form.
“This was a wonderful multidisciplinary effort,” says Dr. Franko. “I feel that the nursing service in particular has done a superb job. They get all the credit for this.”
Carolyn Webster, RN, vice president, Carilion Medical Center Nursing Operations, adds, “I’m happy that patients are being treated.”
First Findings: Dramatic Improvement
In May 2005, within two months after implementing the form, the charter team pulled 70 random patient charts to check their progress.
“We found that we had increased the percent of prophylaxis by SCD, low-molecular-weight heparins and unfractionated heparin [from 30%] to 60%,” says Dr. Franko. “And in June and July of 2005, we pulled 70 charts again. Eighty-seven percent of the patients had received prophylaxis. We were pleased with that increase.”
An Ongoing Process
When this period of education is over and any changes are made to the form and the process, the charter team will continue to meet once or twice a year to track progress and watch for problems.
“I’m not convinced that we’re going to sustain those numbers,” says Dr. Franko of the 87% success rate. “I hope we can keep the score up, but it’s going to take constant re-education.”
One positive factor was that the hospital’s staff is now well educated about VTE prophylaxis, so awareness continues to remain high.
The project will continue—and it will continue to be a work in progress. “We’re always relying on staff feedback to make [the form] more user-friendly,” says Dr. Franko. “And the prophylaxis may change over time, too.” TH
Contributing Writer Jane Jerrard is based in Chicago.
What is your hospital doing to mark DVT Awareness Month this year? Consider that last year a Virginia hospital used this occasion to educate their staff on VTE, which encompasses both DVT and PE. This training was the first step in the implementation of a multidisciplinary, hospital-wide process that resulted in the vast majority of patients receiving proper preventive treatment of this common killer.
According to the Society of Critical Care Medicine, VTE is the No. 1 preventable cause of hospital-associated death for medical inpatients. Most hospitals are struggling to decrease the number of DVTs and PEs in their patient population by teaching or reminding staff to check for risk factors in each patient and, if necessary, provide VTE prophylaxis. While this seems like a simple solution, anyone who’s currently struggling to turn the numbers around this way can assure you that it is an uphill battle. The good news is that Carilion Medical Center in Roanoke, Va., may have found a key to winning that battle.
First Steps toward Improvement
Carilion Medical Center is 625-bed tertiary care facility that typically operates at peak census. With a level-one trauma center and a separate building housing the women’s and children’s hospital, Carilion offers every kind of care except burn treatment and full organ transplants.
“We recognized that VTE prophylaxis is a very important area and that we had not addressed it,” says James Franko, MD, FACP, medical director, General Medicine and Hospitalist Services.
Carilion’s first attempt to tackle the problem was not effective, but it laid the groundwork for later success.
“In April of 2004 we began working with a committee, conducting an investigation to see how frequently patients were receiving VTE prophylaxis,” recalls Dr. Franko. “We found that it was about 30%, based on patient population where more than 80% met the criteria for receiving this prophylaxis.”
The committee then broke down the data to examine who was ordering the VTE prophylaxis and found that there were three groups of physicians.
“There were those who almost always ordered the treatment, including our trauma surgeons,” says Dr. Franko. “Then there were those who did it sometimes and another group of those who never ordered it. We saw that this was obviously a good opportunity for education.”
Initial Research and Planning
In summer 2004, the group implemented a pilot program for screening every single patient on one floor of the hospital—a floor where physicians were predominantly hospitalists. The pilot involved including an information sheet on each medical chart with a list of VTE risk and exclusion criteria. The results: “We saw only a modest increase in prophylaxis,” says Dr. Franko.
So he pushed to find a better way to focus attention on VTE prophylaxis, this time using the channel that Carilion Medical Center has in place to address quality improvement issues.
“Someone can pitch an idea to our Quality Council and ask for a charter team,” explains Kris Peters, RN, human resources education consultant for Carilion Medical Center. “That team is given a time frame and asked to perform research and make recommendations. We have a charter team for pneumonia, for heart failure, for MCI, … that’s worked well for us.”
In fall 2004, Carilion’s Quality Council commissioned a new charter team and gave them the mission of increasing the percentage of patients receiving VTE prophylaxis. The team consisted of Dr. Franko and other physicians, nursing staff, a pharmacist, researchers, a staff member from the medical records department, secretaries, and—as a late addition—Peters.
“There was strong emotional buy-in from everyone on the team,” recalls Dr. Franko, “because almost everyone has a family member or friend who have had an experience with a blood clot.”
Dr. Franko and other members of the team proceeded to gather information on the rates of use and made projections for prophylaxis. They also reviewed the first attempt to increase use.
“We realized that it was necessary to make this a mandatory approach, or there would be no improvement whatsoever,” says Dr. Franko.
One possibility the team explored and then rejected was incorporating VTE prophylaxis with a patient’s admission. “When patients are admitted, we fill out a very thorough nursing assessment form,” explains Dr. Franko. “This is a good point to gather the information, but we decided it was just too cumbersome.”
The team decided on the inclusion of a form with each patient’s medical chart that would lead the nursing staff through simple questions to determine whether the person should receive VTE prophylaxis. (See “VTE Prophylaxis Assessment Form [Adult],” at right.) The default is prophylaxis. “This was a bold step,” says Dr. Franko. With the form, “your patients are going to get VTE prophylaxis unless you tell us not to give it to them.”
Creating the VTE Prophylaxis Assessment Form
The multidisciplinary team needed to build the form using basic, easy-to-understand information. They began by breaking down the hospital’s patient population to determine who most needed the VTE prophylaxis. They found four groups:
- All trauma patients;
- All patients in ICU;
- Anyone with a diagnosis of cancer; and
- Anyone with a history of cancer. (See step 1 on the “VTE Prophylaxis Assessment Form,” at right.)
They also agreed that patients over age 40 with one other risk factor, such as smoking or drinking, would be considered at risk for DVT. (See step 2 on the “VTE Prophylaxis Assessment Form,” at right.)
“That is a significant percentage of our patients,” Dr. Franko points out. Because the women’s and children’s hospital is separate, a full 87% of Carilion’s patients are over 40.
The team then worked on exclusion factors that would eliminate patients in these groups from receiving prophylaxis. They agreed that patients with any of these exclusion criteria would automatically not receive prophylaxis. (See step 4 on the “VTE Prophylaxis Assessment Form,” at right.)
“We really struggled with how to administer the VTE prophylaxis,” admits Dr. Franko. “It was projected at one point that if we put all at-risk patients on low-molecular-weight heparins, we would increase our pharmacy’s budget by $3 million.”
With a great deal of reliance on the American College of Chest Physicians (ACCP) guidelines for VTE prophylaxis, the charter team decided on three treatment categories: low-molecular-weight heparins (enoxaparin, specifically), unfractionated heparins, and sequential compression devices (SCDs). (See step 5 on the “VTE Prophylaxis Assessment Form,” at right.)
“We use a lot of SCDs on our trauma patients,” says Dr. Franko, “but we still had to order more.” After talking to the hospital’s vascular surgeons and other staff, the charter team decided on patients to exclude from medications, including amputees and those who’d had recent vascular surgery. (See step 6 on the “VTE Prophylaxis Assessment Form,” at right.)
If the form indicates that prophylaxis is necessary, then the last step in completing the form is to have a physician add a bright pink sticker with his or her initials and the date and time.
“The pharmacy will prescribe with only that sticker on the chart,” says Dr. Franko. “Patients can get treatment earlier rather than later.”
Implementing the Form
The charter team still had to decide how the form would be presented to physicians and nursing staff. “We learned that there are no such things as standing orders,” says Dr. Franko. “But we can make the form a permanent part of each patient record, so that it cannot be discarded.”
The next hurdle was educating the staff, particularly nurses, on the new quality-improvement program. The team timed the implementation of the new process so that it began in March 2005, DVT Awareness Month. “We used the posters and giveaways provided by the Coalition to Prevent DVT to boost awareness in the staff,” says Peters. In April and May, the form went live.
“We used it for three months, then got information back from the nursing staff,” recalls Peters. “We went back to the committee with some suggested changes.” One of those changes was the inclusion of step 3: information on whether the patient was already receiving VTE prophylaxis.
The second wave of staff education began in late November, and the nursing staff continues to address the form in their bimonthly meetings. “Nurses fear the form, because they think it’s an order,” says Peters. “The top [of the form] will be done, but the bottom will be completely blank.”
She is working to educate nurses so that they are more comfortable with the form, and she has created an e-learning module with detailed information to supplement the form.
“This was a wonderful multidisciplinary effort,” says Dr. Franko. “I feel that the nursing service in particular has done a superb job. They get all the credit for this.”
Carolyn Webster, RN, vice president, Carilion Medical Center Nursing Operations, adds, “I’m happy that patients are being treated.”
First Findings: Dramatic Improvement
In May 2005, within two months after implementing the form, the charter team pulled 70 random patient charts to check their progress.
“We found that we had increased the percent of prophylaxis by SCD, low-molecular-weight heparins and unfractionated heparin [from 30%] to 60%,” says Dr. Franko. “And in June and July of 2005, we pulled 70 charts again. Eighty-seven percent of the patients had received prophylaxis. We were pleased with that increase.”
An Ongoing Process
When this period of education is over and any changes are made to the form and the process, the charter team will continue to meet once or twice a year to track progress and watch for problems.
“I’m not convinced that we’re going to sustain those numbers,” says Dr. Franko of the 87% success rate. “I hope we can keep the score up, but it’s going to take constant re-education.”
One positive factor was that the hospital’s staff is now well educated about VTE prophylaxis, so awareness continues to remain high.
The project will continue—and it will continue to be a work in progress. “We’re always relying on staff feedback to make [the form] more user-friendly,” says Dr. Franko. “And the prophylaxis may change over time, too.” TH
Contributing Writer Jane Jerrard is based in Chicago.
What is your hospital doing to mark DVT Awareness Month this year? Consider that last year a Virginia hospital used this occasion to educate their staff on VTE, which encompasses both DVT and PE. This training was the first step in the implementation of a multidisciplinary, hospital-wide process that resulted in the vast majority of patients receiving proper preventive treatment of this common killer.
According to the Society of Critical Care Medicine, VTE is the No. 1 preventable cause of hospital-associated death for medical inpatients. Most hospitals are struggling to decrease the number of DVTs and PEs in their patient population by teaching or reminding staff to check for risk factors in each patient and, if necessary, provide VTE prophylaxis. While this seems like a simple solution, anyone who’s currently struggling to turn the numbers around this way can assure you that it is an uphill battle. The good news is that Carilion Medical Center in Roanoke, Va., may have found a key to winning that battle.
First Steps toward Improvement
Carilion Medical Center is 625-bed tertiary care facility that typically operates at peak census. With a level-one trauma center and a separate building housing the women’s and children’s hospital, Carilion offers every kind of care except burn treatment and full organ transplants.
“We recognized that VTE prophylaxis is a very important area and that we had not addressed it,” says James Franko, MD, FACP, medical director, General Medicine and Hospitalist Services.
Carilion’s first attempt to tackle the problem was not effective, but it laid the groundwork for later success.
“In April of 2004 we began working with a committee, conducting an investigation to see how frequently patients were receiving VTE prophylaxis,” recalls Dr. Franko. “We found that it was about 30%, based on patient population where more than 80% met the criteria for receiving this prophylaxis.”
The committee then broke down the data to examine who was ordering the VTE prophylaxis and found that there were three groups of physicians.
“There were those who almost always ordered the treatment, including our trauma surgeons,” says Dr. Franko. “Then there were those who did it sometimes and another group of those who never ordered it. We saw that this was obviously a good opportunity for education.”
Initial Research and Planning
In summer 2004, the group implemented a pilot program for screening every single patient on one floor of the hospital—a floor where physicians were predominantly hospitalists. The pilot involved including an information sheet on each medical chart with a list of VTE risk and exclusion criteria. The results: “We saw only a modest increase in prophylaxis,” says Dr. Franko.
So he pushed to find a better way to focus attention on VTE prophylaxis, this time using the channel that Carilion Medical Center has in place to address quality improvement issues.
“Someone can pitch an idea to our Quality Council and ask for a charter team,” explains Kris Peters, RN, human resources education consultant for Carilion Medical Center. “That team is given a time frame and asked to perform research and make recommendations. We have a charter team for pneumonia, for heart failure, for MCI, … that’s worked well for us.”
In fall 2004, Carilion’s Quality Council commissioned a new charter team and gave them the mission of increasing the percentage of patients receiving VTE prophylaxis. The team consisted of Dr. Franko and other physicians, nursing staff, a pharmacist, researchers, a staff member from the medical records department, secretaries, and—as a late addition—Peters.
“There was strong emotional buy-in from everyone on the team,” recalls Dr. Franko, “because almost everyone has a family member or friend who have had an experience with a blood clot.”
Dr. Franko and other members of the team proceeded to gather information on the rates of use and made projections for prophylaxis. They also reviewed the first attempt to increase use.
“We realized that it was necessary to make this a mandatory approach, or there would be no improvement whatsoever,” says Dr. Franko.
One possibility the team explored and then rejected was incorporating VTE prophylaxis with a patient’s admission. “When patients are admitted, we fill out a very thorough nursing assessment form,” explains Dr. Franko. “This is a good point to gather the information, but we decided it was just too cumbersome.”
The team decided on the inclusion of a form with each patient’s medical chart that would lead the nursing staff through simple questions to determine whether the person should receive VTE prophylaxis. (See “VTE Prophylaxis Assessment Form [Adult],” at right.) The default is prophylaxis. “This was a bold step,” says Dr. Franko. With the form, “your patients are going to get VTE prophylaxis unless you tell us not to give it to them.”
Creating the VTE Prophylaxis Assessment Form
The multidisciplinary team needed to build the form using basic, easy-to-understand information. They began by breaking down the hospital’s patient population to determine who most needed the VTE prophylaxis. They found four groups:
- All trauma patients;
- All patients in ICU;
- Anyone with a diagnosis of cancer; and
- Anyone with a history of cancer. (See step 1 on the “VTE Prophylaxis Assessment Form,” at right.)
They also agreed that patients over age 40 with one other risk factor, such as smoking or drinking, would be considered at risk for DVT. (See step 2 on the “VTE Prophylaxis Assessment Form,” at right.)
“That is a significant percentage of our patients,” Dr. Franko points out. Because the women’s and children’s hospital is separate, a full 87% of Carilion’s patients are over 40.
The team then worked on exclusion factors that would eliminate patients in these groups from receiving prophylaxis. They agreed that patients with any of these exclusion criteria would automatically not receive prophylaxis. (See step 4 on the “VTE Prophylaxis Assessment Form,” at right.)
“We really struggled with how to administer the VTE prophylaxis,” admits Dr. Franko. “It was projected at one point that if we put all at-risk patients on low-molecular-weight heparins, we would increase our pharmacy’s budget by $3 million.”
With a great deal of reliance on the American College of Chest Physicians (ACCP) guidelines for VTE prophylaxis, the charter team decided on three treatment categories: low-molecular-weight heparins (enoxaparin, specifically), unfractionated heparins, and sequential compression devices (SCDs). (See step 5 on the “VTE Prophylaxis Assessment Form,” at right.)
“We use a lot of SCDs on our trauma patients,” says Dr. Franko, “but we still had to order more.” After talking to the hospital’s vascular surgeons and other staff, the charter team decided on patients to exclude from medications, including amputees and those who’d had recent vascular surgery. (See step 6 on the “VTE Prophylaxis Assessment Form,” at right.)
If the form indicates that prophylaxis is necessary, then the last step in completing the form is to have a physician add a bright pink sticker with his or her initials and the date and time.
“The pharmacy will prescribe with only that sticker on the chart,” says Dr. Franko. “Patients can get treatment earlier rather than later.”
Implementing the Form
The charter team still had to decide how the form would be presented to physicians and nursing staff. “We learned that there are no such things as standing orders,” says Dr. Franko. “But we can make the form a permanent part of each patient record, so that it cannot be discarded.”
The next hurdle was educating the staff, particularly nurses, on the new quality-improvement program. The team timed the implementation of the new process so that it began in March 2005, DVT Awareness Month. “We used the posters and giveaways provided by the Coalition to Prevent DVT to boost awareness in the staff,” says Peters. In April and May, the form went live.
“We used it for three months, then got information back from the nursing staff,” recalls Peters. “We went back to the committee with some suggested changes.” One of those changes was the inclusion of step 3: information on whether the patient was already receiving VTE prophylaxis.
The second wave of staff education began in late November, and the nursing staff continues to address the form in their bimonthly meetings. “Nurses fear the form, because they think it’s an order,” says Peters. “The top [of the form] will be done, but the bottom will be completely blank.”
She is working to educate nurses so that they are more comfortable with the form, and she has created an e-learning module with detailed information to supplement the form.
“This was a wonderful multidisciplinary effort,” says Dr. Franko. “I feel that the nursing service in particular has done a superb job. They get all the credit for this.”
Carolyn Webster, RN, vice president, Carilion Medical Center Nursing Operations, adds, “I’m happy that patients are being treated.”
First Findings: Dramatic Improvement
In May 2005, within two months after implementing the form, the charter team pulled 70 random patient charts to check their progress.
“We found that we had increased the percent of prophylaxis by SCD, low-molecular-weight heparins and unfractionated heparin [from 30%] to 60%,” says Dr. Franko. “And in June and July of 2005, we pulled 70 charts again. Eighty-seven percent of the patients had received prophylaxis. We were pleased with that increase.”
An Ongoing Process
When this period of education is over and any changes are made to the form and the process, the charter team will continue to meet once or twice a year to track progress and watch for problems.
“I’m not convinced that we’re going to sustain those numbers,” says Dr. Franko of the 87% success rate. “I hope we can keep the score up, but it’s going to take constant re-education.”
One positive factor was that the hospital’s staff is now well educated about VTE prophylaxis, so awareness continues to remain high.
The project will continue—and it will continue to be a work in progress. “We’re always relying on staff feedback to make [the form] more user-friendly,” says Dr. Franko. “And the prophylaxis may change over time, too.” TH
Contributing Writer Jane Jerrard is based in Chicago.