User login
AMLEXANOX appears to be most effective overall. Amlexanox 5% paste reduces ulcer size, pain duration, and healing time (strength of recommendation [SOR]: A, multiple randomized controlled trials [RCTs]).
Topical steroids may alleviate pain and decrease ulcer burden, defined as total number of ulcers over a measured time, usually 4 to 6 weeks (SOR: B, multiple small heterogenous RCTs). Chemical cautery agents also lessen pain (SOR: A, single RCTs on differing agents), and chlorhexidine mouthwashes may reduce overall ulcer burden (SOR: B, heterogeneous RCTs). The herbal preparation Eupatorium laevigatum alleviates pain and improves healing (SOR: B, single RCT).
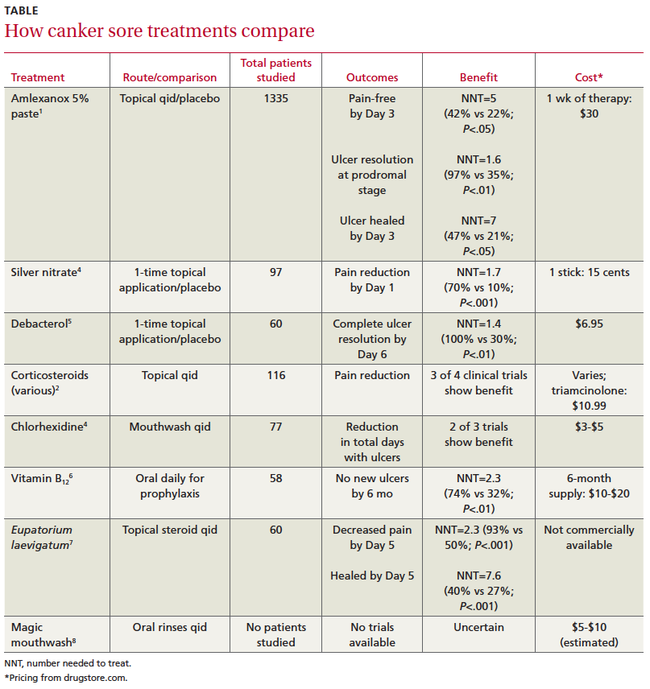
Oral vitamin B12 supplements and avoiding toothpastes containing sodium lauryl sulfate may prevent recurrent ulcers (SOR: B, small RCTs). The TABLE compares ulcer treatments.
Evidence summary
A systematic review of 4 double-blind RCTs found that the anti-inflammatory amlexanox 5% paste significantly reduced ulcer size compared with placebo (–1 vs 0 mm on Day 3 and–3 vs–1 mm on Day 5; P<.01). It also decreased healing time by Day 3 and duration of pain. When applied during the prodromal stage, amlexanox dramatically reduced the number of patients who progressed to full ulcers.1
Clobetasol also reduces pain, ulcer size
A double-blind RCT comparing amlexanox 5% with another anti-inflammatory, clobetasol propionate 0.05% paste, showed equal declines in visual analog pain scores (an average drop from 6 to 2 points out of 10 for each treatment by Day 3 compared with baseline; P<.001). Both treatments produced equivalent reductions in ulcer size from baseline by Day 5 (P<.001).2
Corticosteroids decrease pain, number of ulcers
In a systematic review of 9 small RCTs comparing corticosteroids with placebo, 3 out of 4 RCTs reported significant pain relief. One trial found that 11 of 15 patients treated with beclomethasone spray experienced less pain compared with 0 of 15 patients in the placebo group (P<.05).3
Beclomethasone also decreased the ulcer index (number of ulcers each day over time) in 2 of 4 RCTS (eg, 13 of 15 patients [drug] vs 0 of 15 patients [placebo]; P<.01).3
Chemical cautery relieves pain but may not speed healing
An RCT of 97 patients compared physician-applied silver nitrate with placebo after patients in each group received a 2% lidocaine swab. Silver nitrate treatment was associated with more pain-free patients at Day 1 but didn’t decrease time until resolution.4
Debacterol reduced pain more than placebo by Day 3 (–45 vs–15 points on a visual analog scale; P<.001) and resolved symptoms more effectively by Day 6.5
Antiseptic mouthwashes lower ulcer index
A systematic review of 5 low-quality RCTs (small size, incomplete reporting of data, varied outcomes) comparing chlorhexidine with placebo reported that in 2 of 3 studies that measured the ulcer index, chlorhexidine reduced the index more than placebo (eg, 0.83 with chlorhexidine vs 1.66 with placebo; P<.05). Three of 4 studies that evaluated ulcer duration didn’t show a significant decrease (5.02 days with chlorhexidine vs 5.78 days with placebo; P>.05).2
One small RCT found that a commercial mouthwash (Listerine antiseptic containing menthol, thymol, methyl salicylate, and eucalyptol) modestly decreased ulcer duration (–1.43 days per outbreak for Listerine compared with–0.54 days for placebo; P<.001) and severity (–0.53 points on a 10-point pain scale with mouthwash vs 0 points with placebo; P<.001).6
Herbal preparation relieves pain, improves healing
In a small double-blind trial, Eupatorium laevigatum paste improved 5-day cure rates and pain relief more than triamcinolone 0.1% paste.7
Vitamin B12, avoiding certain toothpastes, helps prevent recurrence
A small RCT comparing 1000 mcg of oral vitamin B12 daily with placebo for prophylaxis found that B12 reduced ulcer duration more than placebo (1.98±3.77 vs 4.84±5.71 days; P<.05), number of ulcers (3.88±7.98 vs 13.39±23; P<.05), and pain (0.64±1.45 vs 2.36 ±2.21 points; P<.01) by 5 months of treatment and increased the percentage of ulcer-free patients by 6 months.8
In 3 of 4 small trials, avoiding toothpaste containing sodium lauryl sulfate slightly but significantly reduced recurrent ulcers.9 Bioadherent agents such as Rincinol appear to have minimal benefit.9
“Magic mouthwashes” lack efficacy data
Clinicians often prescribe “magic mouthwashes” (various combinations of viscous lidocaine, benzocaine, milk of magnesia, kaolin pectate, chlorhexidine, or diphenhydramine), but we found no studies evaluating their effectiveness.
Recommendations
The British National Health Service Clinical Knowledge Summary suggests avoiding aggravating foods and life stressors, using a soft bristled toothbrush, quitting smoking, and using topical corticosteroids, antimicrobial mouthwashes, and topical anesthetics.10
1. Bell J. Amlexanox for the treatment of recurrent aphthous ulcers. Clin Drug Investig. 2005;25:555566.
2. Rodriguez M, Rubio JA, Sanchez R. Effectiveness of two oral pastes for the treatment of recurrent aphthous stomatitis. Oral Dis. 2007;13:490-494.
3. Porter S, Scully C. Aphthous ulcers (recurrent). BMJ Clin Evid. 2007;12(1303):1-9.
4. Alidaee MR, Taheri A, Mansoori P, et al. Silver nitrate cautery in aphthous stomatitis: a randomized controlled trial. Br J Dermatol. 2005;153:521-525.
5. Rhodus NL, Bereuter J. An evaluation of a chemical cautery agent and an anti-inflammatory ointment for the treatment of recurrent aphthous stomatitis: a pilot study. Quintessence Int. 1998;29:769-773.
6. Meiller TF, Kutcher MJ, Overholser CD, et al. Effect of an antimicrobial mouth rinse on recurrent aphthous ulcerations. Oral Surg Oral Med Oral Pathol. 1991;72:425-429.
7. Paulo Filho W, Ribeiro JE, Pinto DS. Safety and efficacy of Eupatorium laevigatum paste as therapy for buccal aphthae: randomized, double-blind comparison with triamcinolone 0.1% orabase. Adv Ther. 2000;17:272-281.
8. Volkov I, Rudoy I, Freud T, et al. Effectiveness of vitamin B12 in treating recurrent aphthous stomatitis: a randomized, double blind placebo-controlled trial. J Am Board Fam Med. 2009;22:9-16.
9. DynaMed Editorial Team. Aphthous ulcers, treatment and prevention. Last updated October 27, 2009. Available at: http://www.ebscohost.com/dynamed. Accessed November 6, 2009.
10. National Health Service Clinical Knowledge Summaries: aphthous ulcer—management: how should I manage aphthous ulcers? Available at: http://www.cks.nhs.uk/aphthous_ulcer/management/detailed_answers/managing_aphthous_ulcers#. Accessed January 28, 2010.
AMLEXANOX appears to be most effective overall. Amlexanox 5% paste reduces ulcer size, pain duration, and healing time (strength of recommendation [SOR]: A, multiple randomized controlled trials [RCTs]).
Topical steroids may alleviate pain and decrease ulcer burden, defined as total number of ulcers over a measured time, usually 4 to 6 weeks (SOR: B, multiple small heterogenous RCTs). Chemical cautery agents also lessen pain (SOR: A, single RCTs on differing agents), and chlorhexidine mouthwashes may reduce overall ulcer burden (SOR: B, heterogeneous RCTs). The herbal preparation Eupatorium laevigatum alleviates pain and improves healing (SOR: B, single RCT).
Oral vitamin B12 supplements and avoiding toothpastes containing sodium lauryl sulfate may prevent recurrent ulcers (SOR: B, small RCTs). The TABLE compares ulcer treatments.
Evidence summary
A systematic review of 4 double-blind RCTs found that the anti-inflammatory amlexanox 5% paste significantly reduced ulcer size compared with placebo (–1 vs 0 mm on Day 3 and–3 vs–1 mm on Day 5; P<.01). It also decreased healing time by Day 3 and duration of pain. When applied during the prodromal stage, amlexanox dramatically reduced the number of patients who progressed to full ulcers.1
Clobetasol also reduces pain, ulcer size
A double-blind RCT comparing amlexanox 5% with another anti-inflammatory, clobetasol propionate 0.05% paste, showed equal declines in visual analog pain scores (an average drop from 6 to 2 points out of 10 for each treatment by Day 3 compared with baseline; P<.001). Both treatments produced equivalent reductions in ulcer size from baseline by Day 5 (P<.001).2
Corticosteroids decrease pain, number of ulcers
In a systematic review of 9 small RCTs comparing corticosteroids with placebo, 3 out of 4 RCTs reported significant pain relief. One trial found that 11 of 15 patients treated with beclomethasone spray experienced less pain compared with 0 of 15 patients in the placebo group (P<.05).3
Beclomethasone also decreased the ulcer index (number of ulcers each day over time) in 2 of 4 RCTS (eg, 13 of 15 patients [drug] vs 0 of 15 patients [placebo]; P<.01).3
Chemical cautery relieves pain but may not speed healing
An RCT of 97 patients compared physician-applied silver nitrate with placebo after patients in each group received a 2% lidocaine swab. Silver nitrate treatment was associated with more pain-free patients at Day 1 but didn’t decrease time until resolution.4
Debacterol reduced pain more than placebo by Day 3 (–45 vs–15 points on a visual analog scale; P<.001) and resolved symptoms more effectively by Day 6.5
Antiseptic mouthwashes lower ulcer index
A systematic review of 5 low-quality RCTs (small size, incomplete reporting of data, varied outcomes) comparing chlorhexidine with placebo reported that in 2 of 3 studies that measured the ulcer index, chlorhexidine reduced the index more than placebo (eg, 0.83 with chlorhexidine vs 1.66 with placebo; P<.05). Three of 4 studies that evaluated ulcer duration didn’t show a significant decrease (5.02 days with chlorhexidine vs 5.78 days with placebo; P>.05).2
One small RCT found that a commercial mouthwash (Listerine antiseptic containing menthol, thymol, methyl salicylate, and eucalyptol) modestly decreased ulcer duration (–1.43 days per outbreak for Listerine compared with–0.54 days for placebo; P<.001) and severity (–0.53 points on a 10-point pain scale with mouthwash vs 0 points with placebo; P<.001).6
Herbal preparation relieves pain, improves healing
In a small double-blind trial, Eupatorium laevigatum paste improved 5-day cure rates and pain relief more than triamcinolone 0.1% paste.7
Vitamin B12, avoiding certain toothpastes, helps prevent recurrence
A small RCT comparing 1000 mcg of oral vitamin B12 daily with placebo for prophylaxis found that B12 reduced ulcer duration more than placebo (1.98±3.77 vs 4.84±5.71 days; P<.05), number of ulcers (3.88±7.98 vs 13.39±23; P<.05), and pain (0.64±1.45 vs 2.36 ±2.21 points; P<.01) by 5 months of treatment and increased the percentage of ulcer-free patients by 6 months.8
In 3 of 4 small trials, avoiding toothpaste containing sodium lauryl sulfate slightly but significantly reduced recurrent ulcers.9 Bioadherent agents such as Rincinol appear to have minimal benefit.9
“Magic mouthwashes” lack efficacy data
Clinicians often prescribe “magic mouthwashes” (various combinations of viscous lidocaine, benzocaine, milk of magnesia, kaolin pectate, chlorhexidine, or diphenhydramine), but we found no studies evaluating their effectiveness.
Recommendations
The British National Health Service Clinical Knowledge Summary suggests avoiding aggravating foods and life stressors, using a soft bristled toothbrush, quitting smoking, and using topical corticosteroids, antimicrobial mouthwashes, and topical anesthetics.10
AMLEXANOX appears to be most effective overall. Amlexanox 5% paste reduces ulcer size, pain duration, and healing time (strength of recommendation [SOR]: A, multiple randomized controlled trials [RCTs]).
Topical steroids may alleviate pain and decrease ulcer burden, defined as total number of ulcers over a measured time, usually 4 to 6 weeks (SOR: B, multiple small heterogenous RCTs). Chemical cautery agents also lessen pain (SOR: A, single RCTs on differing agents), and chlorhexidine mouthwashes may reduce overall ulcer burden (SOR: B, heterogeneous RCTs). The herbal preparation Eupatorium laevigatum alleviates pain and improves healing (SOR: B, single RCT).
Oral vitamin B12 supplements and avoiding toothpastes containing sodium lauryl sulfate may prevent recurrent ulcers (SOR: B, small RCTs). The TABLE compares ulcer treatments.
Evidence summary
A systematic review of 4 double-blind RCTs found that the anti-inflammatory amlexanox 5% paste significantly reduced ulcer size compared with placebo (–1 vs 0 mm on Day 3 and–3 vs–1 mm on Day 5; P<.01). It also decreased healing time by Day 3 and duration of pain. When applied during the prodromal stage, amlexanox dramatically reduced the number of patients who progressed to full ulcers.1
Clobetasol also reduces pain, ulcer size
A double-blind RCT comparing amlexanox 5% with another anti-inflammatory, clobetasol propionate 0.05% paste, showed equal declines in visual analog pain scores (an average drop from 6 to 2 points out of 10 for each treatment by Day 3 compared with baseline; P<.001). Both treatments produced equivalent reductions in ulcer size from baseline by Day 5 (P<.001).2
Corticosteroids decrease pain, number of ulcers
In a systematic review of 9 small RCTs comparing corticosteroids with placebo, 3 out of 4 RCTs reported significant pain relief. One trial found that 11 of 15 patients treated with beclomethasone spray experienced less pain compared with 0 of 15 patients in the placebo group (P<.05).3
Beclomethasone also decreased the ulcer index (number of ulcers each day over time) in 2 of 4 RCTS (eg, 13 of 15 patients [drug] vs 0 of 15 patients [placebo]; P<.01).3
Chemical cautery relieves pain but may not speed healing
An RCT of 97 patients compared physician-applied silver nitrate with placebo after patients in each group received a 2% lidocaine swab. Silver nitrate treatment was associated with more pain-free patients at Day 1 but didn’t decrease time until resolution.4
Debacterol reduced pain more than placebo by Day 3 (–45 vs–15 points on a visual analog scale; P<.001) and resolved symptoms more effectively by Day 6.5
Antiseptic mouthwashes lower ulcer index
A systematic review of 5 low-quality RCTs (small size, incomplete reporting of data, varied outcomes) comparing chlorhexidine with placebo reported that in 2 of 3 studies that measured the ulcer index, chlorhexidine reduced the index more than placebo (eg, 0.83 with chlorhexidine vs 1.66 with placebo; P<.05). Three of 4 studies that evaluated ulcer duration didn’t show a significant decrease (5.02 days with chlorhexidine vs 5.78 days with placebo; P>.05).2
One small RCT found that a commercial mouthwash (Listerine antiseptic containing menthol, thymol, methyl salicylate, and eucalyptol) modestly decreased ulcer duration (–1.43 days per outbreak for Listerine compared with–0.54 days for placebo; P<.001) and severity (–0.53 points on a 10-point pain scale with mouthwash vs 0 points with placebo; P<.001).6
Herbal preparation relieves pain, improves healing
In a small double-blind trial, Eupatorium laevigatum paste improved 5-day cure rates and pain relief more than triamcinolone 0.1% paste.7
Vitamin B12, avoiding certain toothpastes, helps prevent recurrence
A small RCT comparing 1000 mcg of oral vitamin B12 daily with placebo for prophylaxis found that B12 reduced ulcer duration more than placebo (1.98±3.77 vs 4.84±5.71 days; P<.05), number of ulcers (3.88±7.98 vs 13.39±23; P<.05), and pain (0.64±1.45 vs 2.36 ±2.21 points; P<.01) by 5 months of treatment and increased the percentage of ulcer-free patients by 6 months.8
In 3 of 4 small trials, avoiding toothpaste containing sodium lauryl sulfate slightly but significantly reduced recurrent ulcers.9 Bioadherent agents such as Rincinol appear to have minimal benefit.9
“Magic mouthwashes” lack efficacy data
Clinicians often prescribe “magic mouthwashes” (various combinations of viscous lidocaine, benzocaine, milk of magnesia, kaolin pectate, chlorhexidine, or diphenhydramine), but we found no studies evaluating their effectiveness.
Recommendations
The British National Health Service Clinical Knowledge Summary suggests avoiding aggravating foods and life stressors, using a soft bristled toothbrush, quitting smoking, and using topical corticosteroids, antimicrobial mouthwashes, and topical anesthetics.10
1. Bell J. Amlexanox for the treatment of recurrent aphthous ulcers. Clin Drug Investig. 2005;25:555566.
2. Rodriguez M, Rubio JA, Sanchez R. Effectiveness of two oral pastes for the treatment of recurrent aphthous stomatitis. Oral Dis. 2007;13:490-494.
3. Porter S, Scully C. Aphthous ulcers (recurrent). BMJ Clin Evid. 2007;12(1303):1-9.
4. Alidaee MR, Taheri A, Mansoori P, et al. Silver nitrate cautery in aphthous stomatitis: a randomized controlled trial. Br J Dermatol. 2005;153:521-525.
5. Rhodus NL, Bereuter J. An evaluation of a chemical cautery agent and an anti-inflammatory ointment for the treatment of recurrent aphthous stomatitis: a pilot study. Quintessence Int. 1998;29:769-773.
6. Meiller TF, Kutcher MJ, Overholser CD, et al. Effect of an antimicrobial mouth rinse on recurrent aphthous ulcerations. Oral Surg Oral Med Oral Pathol. 1991;72:425-429.
7. Paulo Filho W, Ribeiro JE, Pinto DS. Safety and efficacy of Eupatorium laevigatum paste as therapy for buccal aphthae: randomized, double-blind comparison with triamcinolone 0.1% orabase. Adv Ther. 2000;17:272-281.
8. Volkov I, Rudoy I, Freud T, et al. Effectiveness of vitamin B12 in treating recurrent aphthous stomatitis: a randomized, double blind placebo-controlled trial. J Am Board Fam Med. 2009;22:9-16.
9. DynaMed Editorial Team. Aphthous ulcers, treatment and prevention. Last updated October 27, 2009. Available at: http://www.ebscohost.com/dynamed. Accessed November 6, 2009.
10. National Health Service Clinical Knowledge Summaries: aphthous ulcer—management: how should I manage aphthous ulcers? Available at: http://www.cks.nhs.uk/aphthous_ulcer/management/detailed_answers/managing_aphthous_ulcers#. Accessed January 28, 2010.
1. Bell J. Amlexanox for the treatment of recurrent aphthous ulcers. Clin Drug Investig. 2005;25:555566.
2. Rodriguez M, Rubio JA, Sanchez R. Effectiveness of two oral pastes for the treatment of recurrent aphthous stomatitis. Oral Dis. 2007;13:490-494.
3. Porter S, Scully C. Aphthous ulcers (recurrent). BMJ Clin Evid. 2007;12(1303):1-9.
4. Alidaee MR, Taheri A, Mansoori P, et al. Silver nitrate cautery in aphthous stomatitis: a randomized controlled trial. Br J Dermatol. 2005;153:521-525.
5. Rhodus NL, Bereuter J. An evaluation of a chemical cautery agent and an anti-inflammatory ointment for the treatment of recurrent aphthous stomatitis: a pilot study. Quintessence Int. 1998;29:769-773.
6. Meiller TF, Kutcher MJ, Overholser CD, et al. Effect of an antimicrobial mouth rinse on recurrent aphthous ulcerations. Oral Surg Oral Med Oral Pathol. 1991;72:425-429.
7. Paulo Filho W, Ribeiro JE, Pinto DS. Safety and efficacy of Eupatorium laevigatum paste as therapy for buccal aphthae: randomized, double-blind comparison with triamcinolone 0.1% orabase. Adv Ther. 2000;17:272-281.
8. Volkov I, Rudoy I, Freud T, et al. Effectiveness of vitamin B12 in treating recurrent aphthous stomatitis: a randomized, double blind placebo-controlled trial. J Am Board Fam Med. 2009;22:9-16.
9. DynaMed Editorial Team. Aphthous ulcers, treatment and prevention. Last updated October 27, 2009. Available at: http://www.ebscohost.com/dynamed. Accessed November 6, 2009.
10. National Health Service Clinical Knowledge Summaries: aphthous ulcer—management: how should I manage aphthous ulcers? Available at: http://www.cks.nhs.uk/aphthous_ulcer/management/detailed_answers/managing_aphthous_ulcers#. Accessed January 28, 2010.
Evidence-based answers from the Family Physicians Inquiries Network