User login
Ferning in amniotic fluid: Is it a useful indicator of ruptured membranes?
YES. The presence of arborized crystals (ferning) in amniotic fluid is both sensitive (74%-100%) and specific (77%-100%) for diagnosing rupture of membranes in laboring women who report loss of fluid (strength of recommendation [SOR]: A, multiple prospective cohort studies). However, it is much less sensitive and specific for women with fluid loss who aren’t in labor (SOR: B, 1 prospective cohort study).
Gross contamination of amniotic fluid with blood or antiseptic solutions may decrease the diagnostic accuracy of ferning, whereas contamination with meconium doesn’t (SOR: C, bench research).
Evidence summary
A nonsystematic review of 11 prospective cohort studies (N=2804) reported that ferning was both sensitive and specific for the presence of amniotic fluid in laboring women who reported fluid loss. Labor was defined as contractions with subsequent delivery of a baby. Ferning had a mean sensitivity of 96% (range, 74%-100%) and a mean specificity of 96.2% (range, 77%-100%).1
Helpful in laboring women, but less so in those who are nonlaboring
A prospective cohort study evaluated the sensitivity and specificity of ferning among women reporting fluid loss who were in labor compared with women who weren’t in labor. Investigators classified laboring women (n=51) as having continued fluid loss and no fetal membranes covering the presenting part and progressing to delivery. They considered women to be nonlaboring (n=100) if they had minimal fluid loss and fetal membranes covering the presenting part or didn’t progress to delivery (investigators diagnosed 39 women with ruptured membranes on clinical grounds). Ferning was 98% sensitive and 88.2% specific in laboring women, and 51.3% sensitive and 70.5% specific in nonlaboring women.1
Ferning occurs from 14 weeks of gestation onward
A prospective case series (N=400) determined that amniotic fluid would fern at all gestational ages between 14 and 41 weeks. Investigators obtained fluid samples by amniocentesis and confirmed that they were 100% nitrazine-positive.2 They found more consistent ferning in samples dried on a slide for 10 minutes than samples dried over a flame (100% vs 86.7% of 112 samples).
Some contaminants in amniotic samples affect ferning
In vitro studies evaluated ferning in samples of amniotic fluid mixed with blood, meconium, or vaginal fluids. Blood contamination didn’t affect ferning unless the sample contained more than 10% blood.3-5 Meconium (which itself verifies ruptured membranes) didn’t change the fern pattern at any dilution,6 nor did vaginal discharge.3
Antiseptic solution may cause false-positive results, as may semen, fingerprints, and cervical mucus—although none of these show the fine arborization or discrete crystallization seen in uncontaminated amniotic fluid.6,7
Recommendations
The American College of Obstetricians and Gynecologists says that ferning is a confirmatory test for ruptured membranes, to be used along with pooling in the vaginal vault, and that premature membrane rupture is confirmed by fluid passing from the cervical canal.8
1. De Haan HH, Offermans PM, Smits F, et al. Value of the fern test to confirm or reject the diagnosis of ruptured membranes is modest in nonlaboring women presenting with nonspecific vaginal fluid loss. Am J Perinatol. 1994;11:46-50.
2. Bennett SL, Cullen JB, Sherer DM, et al. The ferning and nitrazine tests of amniotic fluid between 12 and 41 weeks gestation. Am J Perinatol. 1993;10:101-104.
3. Brookes C, Shand K, Jones WR. A reevaluation of the ferning test to detect ruptured membranes. Aust N Z J Obstet Gynaecol. 1986;26:260-264.
4. Reece EA, Chervenak FA, Moya FR, et al. Amniotic fluid arborization: effect of blood, meconium, and pH alterations. Obstet Gynecol. 1984;64:248-250.
5. Rosemond RL, Lombardi SJ, Boehm FH. Ferning of amniotic fluid contaminated with blood. Obstet Gyncol. 1990;75:338-340.
6. McGregor JA, Johnson S. “Fig leaf” ferning and positive nitrazine testing: semen as a cause of misdiagnosis of premature rupture of membranes. Am J Obstet Gynecol. 1985;151:1142-1143.
7. Lodeiro JG, Hsieh KA, Byers JH, et al. The fingerprint, a false-positive fern test. Obstet Gynecol. 1989;73:873-874.
8. American College of Obstetricians and Gynecologists. Premature rupture of membranes. ACOG Practice Bulletin No. 80. Obstet Gynecol. 2007;109:1007-1019.
YES. The presence of arborized crystals (ferning) in amniotic fluid is both sensitive (74%-100%) and specific (77%-100%) for diagnosing rupture of membranes in laboring women who report loss of fluid (strength of recommendation [SOR]: A, multiple prospective cohort studies). However, it is much less sensitive and specific for women with fluid loss who aren’t in labor (SOR: B, 1 prospective cohort study).
Gross contamination of amniotic fluid with blood or antiseptic solutions may decrease the diagnostic accuracy of ferning, whereas contamination with meconium doesn’t (SOR: C, bench research).
Evidence summary
A nonsystematic review of 11 prospective cohort studies (N=2804) reported that ferning was both sensitive and specific for the presence of amniotic fluid in laboring women who reported fluid loss. Labor was defined as contractions with subsequent delivery of a baby. Ferning had a mean sensitivity of 96% (range, 74%-100%) and a mean specificity of 96.2% (range, 77%-100%).1
Helpful in laboring women, but less so in those who are nonlaboring
A prospective cohort study evaluated the sensitivity and specificity of ferning among women reporting fluid loss who were in labor compared with women who weren’t in labor. Investigators classified laboring women (n=51) as having continued fluid loss and no fetal membranes covering the presenting part and progressing to delivery. They considered women to be nonlaboring (n=100) if they had minimal fluid loss and fetal membranes covering the presenting part or didn’t progress to delivery (investigators diagnosed 39 women with ruptured membranes on clinical grounds). Ferning was 98% sensitive and 88.2% specific in laboring women, and 51.3% sensitive and 70.5% specific in nonlaboring women.1
Ferning occurs from 14 weeks of gestation onward
A prospective case series (N=400) determined that amniotic fluid would fern at all gestational ages between 14 and 41 weeks. Investigators obtained fluid samples by amniocentesis and confirmed that they were 100% nitrazine-positive.2 They found more consistent ferning in samples dried on a slide for 10 minutes than samples dried over a flame (100% vs 86.7% of 112 samples).
Some contaminants in amniotic samples affect ferning
In vitro studies evaluated ferning in samples of amniotic fluid mixed with blood, meconium, or vaginal fluids. Blood contamination didn’t affect ferning unless the sample contained more than 10% blood.3-5 Meconium (which itself verifies ruptured membranes) didn’t change the fern pattern at any dilution,6 nor did vaginal discharge.3
Antiseptic solution may cause false-positive results, as may semen, fingerprints, and cervical mucus—although none of these show the fine arborization or discrete crystallization seen in uncontaminated amniotic fluid.6,7
Recommendations
The American College of Obstetricians and Gynecologists says that ferning is a confirmatory test for ruptured membranes, to be used along with pooling in the vaginal vault, and that premature membrane rupture is confirmed by fluid passing from the cervical canal.8
YES. The presence of arborized crystals (ferning) in amniotic fluid is both sensitive (74%-100%) and specific (77%-100%) for diagnosing rupture of membranes in laboring women who report loss of fluid (strength of recommendation [SOR]: A, multiple prospective cohort studies). However, it is much less sensitive and specific for women with fluid loss who aren’t in labor (SOR: B, 1 prospective cohort study).
Gross contamination of amniotic fluid with blood or antiseptic solutions may decrease the diagnostic accuracy of ferning, whereas contamination with meconium doesn’t (SOR: C, bench research).
Evidence summary
A nonsystematic review of 11 prospective cohort studies (N=2804) reported that ferning was both sensitive and specific for the presence of amniotic fluid in laboring women who reported fluid loss. Labor was defined as contractions with subsequent delivery of a baby. Ferning had a mean sensitivity of 96% (range, 74%-100%) and a mean specificity of 96.2% (range, 77%-100%).1
Helpful in laboring women, but less so in those who are nonlaboring
A prospective cohort study evaluated the sensitivity and specificity of ferning among women reporting fluid loss who were in labor compared with women who weren’t in labor. Investigators classified laboring women (n=51) as having continued fluid loss and no fetal membranes covering the presenting part and progressing to delivery. They considered women to be nonlaboring (n=100) if they had minimal fluid loss and fetal membranes covering the presenting part or didn’t progress to delivery (investigators diagnosed 39 women with ruptured membranes on clinical grounds). Ferning was 98% sensitive and 88.2% specific in laboring women, and 51.3% sensitive and 70.5% specific in nonlaboring women.1
Ferning occurs from 14 weeks of gestation onward
A prospective case series (N=400) determined that amniotic fluid would fern at all gestational ages between 14 and 41 weeks. Investigators obtained fluid samples by amniocentesis and confirmed that they were 100% nitrazine-positive.2 They found more consistent ferning in samples dried on a slide for 10 minutes than samples dried over a flame (100% vs 86.7% of 112 samples).
Some contaminants in amniotic samples affect ferning
In vitro studies evaluated ferning in samples of amniotic fluid mixed with blood, meconium, or vaginal fluids. Blood contamination didn’t affect ferning unless the sample contained more than 10% blood.3-5 Meconium (which itself verifies ruptured membranes) didn’t change the fern pattern at any dilution,6 nor did vaginal discharge.3
Antiseptic solution may cause false-positive results, as may semen, fingerprints, and cervical mucus—although none of these show the fine arborization or discrete crystallization seen in uncontaminated amniotic fluid.6,7
Recommendations
The American College of Obstetricians and Gynecologists says that ferning is a confirmatory test for ruptured membranes, to be used along with pooling in the vaginal vault, and that premature membrane rupture is confirmed by fluid passing from the cervical canal.8
1. De Haan HH, Offermans PM, Smits F, et al. Value of the fern test to confirm or reject the diagnosis of ruptured membranes is modest in nonlaboring women presenting with nonspecific vaginal fluid loss. Am J Perinatol. 1994;11:46-50.
2. Bennett SL, Cullen JB, Sherer DM, et al. The ferning and nitrazine tests of amniotic fluid between 12 and 41 weeks gestation. Am J Perinatol. 1993;10:101-104.
3. Brookes C, Shand K, Jones WR. A reevaluation of the ferning test to detect ruptured membranes. Aust N Z J Obstet Gynaecol. 1986;26:260-264.
4. Reece EA, Chervenak FA, Moya FR, et al. Amniotic fluid arborization: effect of blood, meconium, and pH alterations. Obstet Gynecol. 1984;64:248-250.
5. Rosemond RL, Lombardi SJ, Boehm FH. Ferning of amniotic fluid contaminated with blood. Obstet Gyncol. 1990;75:338-340.
6. McGregor JA, Johnson S. “Fig leaf” ferning and positive nitrazine testing: semen as a cause of misdiagnosis of premature rupture of membranes. Am J Obstet Gynecol. 1985;151:1142-1143.
7. Lodeiro JG, Hsieh KA, Byers JH, et al. The fingerprint, a false-positive fern test. Obstet Gynecol. 1989;73:873-874.
8. American College of Obstetricians and Gynecologists. Premature rupture of membranes. ACOG Practice Bulletin No. 80. Obstet Gynecol. 2007;109:1007-1019.
1. De Haan HH, Offermans PM, Smits F, et al. Value of the fern test to confirm or reject the diagnosis of ruptured membranes is modest in nonlaboring women presenting with nonspecific vaginal fluid loss. Am J Perinatol. 1994;11:46-50.
2. Bennett SL, Cullen JB, Sherer DM, et al. The ferning and nitrazine tests of amniotic fluid between 12 and 41 weeks gestation. Am J Perinatol. 1993;10:101-104.
3. Brookes C, Shand K, Jones WR. A reevaluation of the ferning test to detect ruptured membranes. Aust N Z J Obstet Gynaecol. 1986;26:260-264.
4. Reece EA, Chervenak FA, Moya FR, et al. Amniotic fluid arborization: effect of blood, meconium, and pH alterations. Obstet Gynecol. 1984;64:248-250.
5. Rosemond RL, Lombardi SJ, Boehm FH. Ferning of amniotic fluid contaminated with blood. Obstet Gyncol. 1990;75:338-340.
6. McGregor JA, Johnson S. “Fig leaf” ferning and positive nitrazine testing: semen as a cause of misdiagnosis of premature rupture of membranes. Am J Obstet Gynecol. 1985;151:1142-1143.
7. Lodeiro JG, Hsieh KA, Byers JH, et al. The fingerprint, a false-positive fern test. Obstet Gynecol. 1989;73:873-874.
8. American College of Obstetricians and Gynecologists. Premature rupture of membranes. ACOG Practice Bulletin No. 80. Obstet Gynecol. 2007;109:1007-1019.
Evidence-based answers from the Family Physicians Inquiries Network
What is the most effective way to treat recurrent canker sores?
AMLEXANOX appears to be most effective overall. Amlexanox 5% paste reduces ulcer size, pain duration, and healing time (strength of recommendation [SOR]: A, multiple randomized controlled trials [RCTs]).
Topical steroids may alleviate pain and decrease ulcer burden, defined as total number of ulcers over a measured time, usually 4 to 6 weeks (SOR: B, multiple small heterogenous RCTs). Chemical cautery agents also lessen pain (SOR: A, single RCTs on differing agents), and chlorhexidine mouthwashes may reduce overall ulcer burden (SOR: B, heterogeneous RCTs). The herbal preparation Eupatorium laevigatum alleviates pain and improves healing (SOR: B, single RCT).
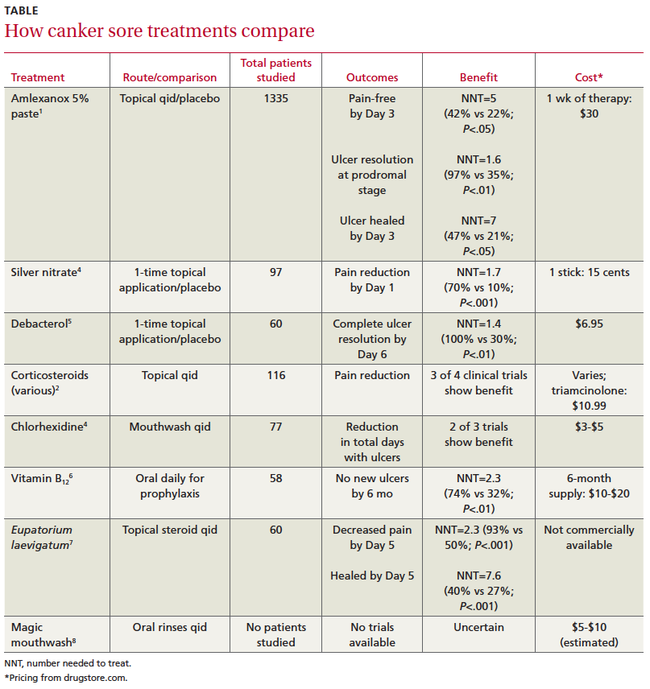
Oral vitamin B12 supplements and avoiding toothpastes containing sodium lauryl sulfate may prevent recurrent ulcers (SOR: B, small RCTs). The TABLE compares ulcer treatments.
Evidence summary
A systematic review of 4 double-blind RCTs found that the anti-inflammatory amlexanox 5% paste significantly reduced ulcer size compared with placebo (–1 vs 0 mm on Day 3 and–3 vs–1 mm on Day 5; P<.01). It also decreased healing time by Day 3 and duration of pain. When applied during the prodromal stage, amlexanox dramatically reduced the number of patients who progressed to full ulcers.1
Clobetasol also reduces pain, ulcer size
A double-blind RCT comparing amlexanox 5% with another anti-inflammatory, clobetasol propionate 0.05% paste, showed equal declines in visual analog pain scores (an average drop from 6 to 2 points out of 10 for each treatment by Day 3 compared with baseline; P<.001). Both treatments produced equivalent reductions in ulcer size from baseline by Day 5 (P<.001).2
Corticosteroids decrease pain, number of ulcers
In a systematic review of 9 small RCTs comparing corticosteroids with placebo, 3 out of 4 RCTs reported significant pain relief. One trial found that 11 of 15 patients treated with beclomethasone spray experienced less pain compared with 0 of 15 patients in the placebo group (P<.05).3
Beclomethasone also decreased the ulcer index (number of ulcers each day over time) in 2 of 4 RCTS (eg, 13 of 15 patients [drug] vs 0 of 15 patients [placebo]; P<.01).3
Chemical cautery relieves pain but may not speed healing
An RCT of 97 patients compared physician-applied silver nitrate with placebo after patients in each group received a 2% lidocaine swab. Silver nitrate treatment was associated with more pain-free patients at Day 1 but didn’t decrease time until resolution.4
Debacterol reduced pain more than placebo by Day 3 (–45 vs–15 points on a visual analog scale; P<.001) and resolved symptoms more effectively by Day 6.5
Antiseptic mouthwashes lower ulcer index
A systematic review of 5 low-quality RCTs (small size, incomplete reporting of data, varied outcomes) comparing chlorhexidine with placebo reported that in 2 of 3 studies that measured the ulcer index, chlorhexidine reduced the index more than placebo (eg, 0.83 with chlorhexidine vs 1.66 with placebo; P<.05). Three of 4 studies that evaluated ulcer duration didn’t show a significant decrease (5.02 days with chlorhexidine vs 5.78 days with placebo; P>.05).2
One small RCT found that a commercial mouthwash (Listerine antiseptic containing menthol, thymol, methyl salicylate, and eucalyptol) modestly decreased ulcer duration (–1.43 days per outbreak for Listerine compared with–0.54 days for placebo; P<.001) and severity (–0.53 points on a 10-point pain scale with mouthwash vs 0 points with placebo; P<.001).6
Herbal preparation relieves pain, improves healing
In a small double-blind trial, Eupatorium laevigatum paste improved 5-day cure rates and pain relief more than triamcinolone 0.1% paste.7
Vitamin B12, avoiding certain toothpastes, helps prevent recurrence
A small RCT comparing 1000 mcg of oral vitamin B12 daily with placebo for prophylaxis found that B12 reduced ulcer duration more than placebo (1.98±3.77 vs 4.84±5.71 days; P<.05), number of ulcers (3.88±7.98 vs 13.39±23; P<.05), and pain (0.64±1.45 vs 2.36 ±2.21 points; P<.01) by 5 months of treatment and increased the percentage of ulcer-free patients by 6 months.8
In 3 of 4 small trials, avoiding toothpaste containing sodium lauryl sulfate slightly but significantly reduced recurrent ulcers.9 Bioadherent agents such as Rincinol appear to have minimal benefit.9
“Magic mouthwashes” lack efficacy data
Clinicians often prescribe “magic mouthwashes” (various combinations of viscous lidocaine, benzocaine, milk of magnesia, kaolin pectate, chlorhexidine, or diphenhydramine), but we found no studies evaluating their effectiveness.
Recommendations
The British National Health Service Clinical Knowledge Summary suggests avoiding aggravating foods and life stressors, using a soft bristled toothbrush, quitting smoking, and using topical corticosteroids, antimicrobial mouthwashes, and topical anesthetics.10
1. Bell J. Amlexanox for the treatment of recurrent aphthous ulcers. Clin Drug Investig. 2005;25:555566.
2. Rodriguez M, Rubio JA, Sanchez R. Effectiveness of two oral pastes for the treatment of recurrent aphthous stomatitis. Oral Dis. 2007;13:490-494.
3. Porter S, Scully C. Aphthous ulcers (recurrent). BMJ Clin Evid. 2007;12(1303):1-9.
4. Alidaee MR, Taheri A, Mansoori P, et al. Silver nitrate cautery in aphthous stomatitis: a randomized controlled trial. Br J Dermatol. 2005;153:521-525.
5. Rhodus NL, Bereuter J. An evaluation of a chemical cautery agent and an anti-inflammatory ointment for the treatment of recurrent aphthous stomatitis: a pilot study. Quintessence Int. 1998;29:769-773.
6. Meiller TF, Kutcher MJ, Overholser CD, et al. Effect of an antimicrobial mouth rinse on recurrent aphthous ulcerations. Oral Surg Oral Med Oral Pathol. 1991;72:425-429.
7. Paulo Filho W, Ribeiro JE, Pinto DS. Safety and efficacy of Eupatorium laevigatum paste as therapy for buccal aphthae: randomized, double-blind comparison with triamcinolone 0.1% orabase. Adv Ther. 2000;17:272-281.
8. Volkov I, Rudoy I, Freud T, et al. Effectiveness of vitamin B12 in treating recurrent aphthous stomatitis: a randomized, double blind placebo-controlled trial. J Am Board Fam Med. 2009;22:9-16.
9. DynaMed Editorial Team. Aphthous ulcers, treatment and prevention. Last updated October 27, 2009. Available at: http://www.ebscohost.com/dynamed. Accessed November 6, 2009.
10. National Health Service Clinical Knowledge Summaries: aphthous ulcer—management: how should I manage aphthous ulcers? Available at: http://www.cks.nhs.uk/aphthous_ulcer/management/detailed_answers/managing_aphthous_ulcers#. Accessed January 28, 2010.
AMLEXANOX appears to be most effective overall. Amlexanox 5% paste reduces ulcer size, pain duration, and healing time (strength of recommendation [SOR]: A, multiple randomized controlled trials [RCTs]).
Topical steroids may alleviate pain and decrease ulcer burden, defined as total number of ulcers over a measured time, usually 4 to 6 weeks (SOR: B, multiple small heterogenous RCTs). Chemical cautery agents also lessen pain (SOR: A, single RCTs on differing agents), and chlorhexidine mouthwashes may reduce overall ulcer burden (SOR: B, heterogeneous RCTs). The herbal preparation Eupatorium laevigatum alleviates pain and improves healing (SOR: B, single RCT).
Oral vitamin B12 supplements and avoiding toothpastes containing sodium lauryl sulfate may prevent recurrent ulcers (SOR: B, small RCTs). The TABLE compares ulcer treatments.
Evidence summary
A systematic review of 4 double-blind RCTs found that the anti-inflammatory amlexanox 5% paste significantly reduced ulcer size compared with placebo (–1 vs 0 mm on Day 3 and–3 vs–1 mm on Day 5; P<.01). It also decreased healing time by Day 3 and duration of pain. When applied during the prodromal stage, amlexanox dramatically reduced the number of patients who progressed to full ulcers.1
Clobetasol also reduces pain, ulcer size
A double-blind RCT comparing amlexanox 5% with another anti-inflammatory, clobetasol propionate 0.05% paste, showed equal declines in visual analog pain scores (an average drop from 6 to 2 points out of 10 for each treatment by Day 3 compared with baseline; P<.001). Both treatments produced equivalent reductions in ulcer size from baseline by Day 5 (P<.001).2
Corticosteroids decrease pain, number of ulcers
In a systematic review of 9 small RCTs comparing corticosteroids with placebo, 3 out of 4 RCTs reported significant pain relief. One trial found that 11 of 15 patients treated with beclomethasone spray experienced less pain compared with 0 of 15 patients in the placebo group (P<.05).3
Beclomethasone also decreased the ulcer index (number of ulcers each day over time) in 2 of 4 RCTS (eg, 13 of 15 patients [drug] vs 0 of 15 patients [placebo]; P<.01).3
Chemical cautery relieves pain but may not speed healing
An RCT of 97 patients compared physician-applied silver nitrate with placebo after patients in each group received a 2% lidocaine swab. Silver nitrate treatment was associated with more pain-free patients at Day 1 but didn’t decrease time until resolution.4
Debacterol reduced pain more than placebo by Day 3 (–45 vs–15 points on a visual analog scale; P<.001) and resolved symptoms more effectively by Day 6.5
Antiseptic mouthwashes lower ulcer index
A systematic review of 5 low-quality RCTs (small size, incomplete reporting of data, varied outcomes) comparing chlorhexidine with placebo reported that in 2 of 3 studies that measured the ulcer index, chlorhexidine reduced the index more than placebo (eg, 0.83 with chlorhexidine vs 1.66 with placebo; P<.05). Three of 4 studies that evaluated ulcer duration didn’t show a significant decrease (5.02 days with chlorhexidine vs 5.78 days with placebo; P>.05).2
One small RCT found that a commercial mouthwash (Listerine antiseptic containing menthol, thymol, methyl salicylate, and eucalyptol) modestly decreased ulcer duration (–1.43 days per outbreak for Listerine compared with–0.54 days for placebo; P<.001) and severity (–0.53 points on a 10-point pain scale with mouthwash vs 0 points with placebo; P<.001).6
Herbal preparation relieves pain, improves healing
In a small double-blind trial, Eupatorium laevigatum paste improved 5-day cure rates and pain relief more than triamcinolone 0.1% paste.7
Vitamin B12, avoiding certain toothpastes, helps prevent recurrence
A small RCT comparing 1000 mcg of oral vitamin B12 daily with placebo for prophylaxis found that B12 reduced ulcer duration more than placebo (1.98±3.77 vs 4.84±5.71 days; P<.05), number of ulcers (3.88±7.98 vs 13.39±23; P<.05), and pain (0.64±1.45 vs 2.36 ±2.21 points; P<.01) by 5 months of treatment and increased the percentage of ulcer-free patients by 6 months.8
In 3 of 4 small trials, avoiding toothpaste containing sodium lauryl sulfate slightly but significantly reduced recurrent ulcers.9 Bioadherent agents such as Rincinol appear to have minimal benefit.9
“Magic mouthwashes” lack efficacy data
Clinicians often prescribe “magic mouthwashes” (various combinations of viscous lidocaine, benzocaine, milk of magnesia, kaolin pectate, chlorhexidine, or diphenhydramine), but we found no studies evaluating their effectiveness.
Recommendations
The British National Health Service Clinical Knowledge Summary suggests avoiding aggravating foods and life stressors, using a soft bristled toothbrush, quitting smoking, and using topical corticosteroids, antimicrobial mouthwashes, and topical anesthetics.10
AMLEXANOX appears to be most effective overall. Amlexanox 5% paste reduces ulcer size, pain duration, and healing time (strength of recommendation [SOR]: A, multiple randomized controlled trials [RCTs]).
Topical steroids may alleviate pain and decrease ulcer burden, defined as total number of ulcers over a measured time, usually 4 to 6 weeks (SOR: B, multiple small heterogenous RCTs). Chemical cautery agents also lessen pain (SOR: A, single RCTs on differing agents), and chlorhexidine mouthwashes may reduce overall ulcer burden (SOR: B, heterogeneous RCTs). The herbal preparation Eupatorium laevigatum alleviates pain and improves healing (SOR: B, single RCT).
Oral vitamin B12 supplements and avoiding toothpastes containing sodium lauryl sulfate may prevent recurrent ulcers (SOR: B, small RCTs). The TABLE compares ulcer treatments.
Evidence summary
A systematic review of 4 double-blind RCTs found that the anti-inflammatory amlexanox 5% paste significantly reduced ulcer size compared with placebo (–1 vs 0 mm on Day 3 and–3 vs–1 mm on Day 5; P<.01). It also decreased healing time by Day 3 and duration of pain. When applied during the prodromal stage, amlexanox dramatically reduced the number of patients who progressed to full ulcers.1
Clobetasol also reduces pain, ulcer size
A double-blind RCT comparing amlexanox 5% with another anti-inflammatory, clobetasol propionate 0.05% paste, showed equal declines in visual analog pain scores (an average drop from 6 to 2 points out of 10 for each treatment by Day 3 compared with baseline; P<.001). Both treatments produced equivalent reductions in ulcer size from baseline by Day 5 (P<.001).2
Corticosteroids decrease pain, number of ulcers
In a systematic review of 9 small RCTs comparing corticosteroids with placebo, 3 out of 4 RCTs reported significant pain relief. One trial found that 11 of 15 patients treated with beclomethasone spray experienced less pain compared with 0 of 15 patients in the placebo group (P<.05).3
Beclomethasone also decreased the ulcer index (number of ulcers each day over time) in 2 of 4 RCTS (eg, 13 of 15 patients [drug] vs 0 of 15 patients [placebo]; P<.01).3
Chemical cautery relieves pain but may not speed healing
An RCT of 97 patients compared physician-applied silver nitrate with placebo after patients in each group received a 2% lidocaine swab. Silver nitrate treatment was associated with more pain-free patients at Day 1 but didn’t decrease time until resolution.4
Debacterol reduced pain more than placebo by Day 3 (–45 vs–15 points on a visual analog scale; P<.001) and resolved symptoms more effectively by Day 6.5
Antiseptic mouthwashes lower ulcer index
A systematic review of 5 low-quality RCTs (small size, incomplete reporting of data, varied outcomes) comparing chlorhexidine with placebo reported that in 2 of 3 studies that measured the ulcer index, chlorhexidine reduced the index more than placebo (eg, 0.83 with chlorhexidine vs 1.66 with placebo; P<.05). Three of 4 studies that evaluated ulcer duration didn’t show a significant decrease (5.02 days with chlorhexidine vs 5.78 days with placebo; P>.05).2
One small RCT found that a commercial mouthwash (Listerine antiseptic containing menthol, thymol, methyl salicylate, and eucalyptol) modestly decreased ulcer duration (–1.43 days per outbreak for Listerine compared with–0.54 days for placebo; P<.001) and severity (–0.53 points on a 10-point pain scale with mouthwash vs 0 points with placebo; P<.001).6
Herbal preparation relieves pain, improves healing
In a small double-blind trial, Eupatorium laevigatum paste improved 5-day cure rates and pain relief more than triamcinolone 0.1% paste.7
Vitamin B12, avoiding certain toothpastes, helps prevent recurrence
A small RCT comparing 1000 mcg of oral vitamin B12 daily with placebo for prophylaxis found that B12 reduced ulcer duration more than placebo (1.98±3.77 vs 4.84±5.71 days; P<.05), number of ulcers (3.88±7.98 vs 13.39±23; P<.05), and pain (0.64±1.45 vs 2.36 ±2.21 points; P<.01) by 5 months of treatment and increased the percentage of ulcer-free patients by 6 months.8
In 3 of 4 small trials, avoiding toothpaste containing sodium lauryl sulfate slightly but significantly reduced recurrent ulcers.9 Bioadherent agents such as Rincinol appear to have minimal benefit.9
“Magic mouthwashes” lack efficacy data
Clinicians often prescribe “magic mouthwashes” (various combinations of viscous lidocaine, benzocaine, milk of magnesia, kaolin pectate, chlorhexidine, or diphenhydramine), but we found no studies evaluating their effectiveness.
Recommendations
The British National Health Service Clinical Knowledge Summary suggests avoiding aggravating foods and life stressors, using a soft bristled toothbrush, quitting smoking, and using topical corticosteroids, antimicrobial mouthwashes, and topical anesthetics.10
1. Bell J. Amlexanox for the treatment of recurrent aphthous ulcers. Clin Drug Investig. 2005;25:555566.
2. Rodriguez M, Rubio JA, Sanchez R. Effectiveness of two oral pastes for the treatment of recurrent aphthous stomatitis. Oral Dis. 2007;13:490-494.
3. Porter S, Scully C. Aphthous ulcers (recurrent). BMJ Clin Evid. 2007;12(1303):1-9.
4. Alidaee MR, Taheri A, Mansoori P, et al. Silver nitrate cautery in aphthous stomatitis: a randomized controlled trial. Br J Dermatol. 2005;153:521-525.
5. Rhodus NL, Bereuter J. An evaluation of a chemical cautery agent and an anti-inflammatory ointment for the treatment of recurrent aphthous stomatitis: a pilot study. Quintessence Int. 1998;29:769-773.
6. Meiller TF, Kutcher MJ, Overholser CD, et al. Effect of an antimicrobial mouth rinse on recurrent aphthous ulcerations. Oral Surg Oral Med Oral Pathol. 1991;72:425-429.
7. Paulo Filho W, Ribeiro JE, Pinto DS. Safety and efficacy of Eupatorium laevigatum paste as therapy for buccal aphthae: randomized, double-blind comparison with triamcinolone 0.1% orabase. Adv Ther. 2000;17:272-281.
8. Volkov I, Rudoy I, Freud T, et al. Effectiveness of vitamin B12 in treating recurrent aphthous stomatitis: a randomized, double blind placebo-controlled trial. J Am Board Fam Med. 2009;22:9-16.
9. DynaMed Editorial Team. Aphthous ulcers, treatment and prevention. Last updated October 27, 2009. Available at: http://www.ebscohost.com/dynamed. Accessed November 6, 2009.
10. National Health Service Clinical Knowledge Summaries: aphthous ulcer—management: how should I manage aphthous ulcers? Available at: http://www.cks.nhs.uk/aphthous_ulcer/management/detailed_answers/managing_aphthous_ulcers#. Accessed January 28, 2010.
1. Bell J. Amlexanox for the treatment of recurrent aphthous ulcers. Clin Drug Investig. 2005;25:555566.
2. Rodriguez M, Rubio JA, Sanchez R. Effectiveness of two oral pastes for the treatment of recurrent aphthous stomatitis. Oral Dis. 2007;13:490-494.
3. Porter S, Scully C. Aphthous ulcers (recurrent). BMJ Clin Evid. 2007;12(1303):1-9.
4. Alidaee MR, Taheri A, Mansoori P, et al. Silver nitrate cautery in aphthous stomatitis: a randomized controlled trial. Br J Dermatol. 2005;153:521-525.
5. Rhodus NL, Bereuter J. An evaluation of a chemical cautery agent and an anti-inflammatory ointment for the treatment of recurrent aphthous stomatitis: a pilot study. Quintessence Int. 1998;29:769-773.
6. Meiller TF, Kutcher MJ, Overholser CD, et al. Effect of an antimicrobial mouth rinse on recurrent aphthous ulcerations. Oral Surg Oral Med Oral Pathol. 1991;72:425-429.
7. Paulo Filho W, Ribeiro JE, Pinto DS. Safety and efficacy of Eupatorium laevigatum paste as therapy for buccal aphthae: randomized, double-blind comparison with triamcinolone 0.1% orabase. Adv Ther. 2000;17:272-281.
8. Volkov I, Rudoy I, Freud T, et al. Effectiveness of vitamin B12 in treating recurrent aphthous stomatitis: a randomized, double blind placebo-controlled trial. J Am Board Fam Med. 2009;22:9-16.
9. DynaMed Editorial Team. Aphthous ulcers, treatment and prevention. Last updated October 27, 2009. Available at: http://www.ebscohost.com/dynamed. Accessed November 6, 2009.
10. National Health Service Clinical Knowledge Summaries: aphthous ulcer—management: how should I manage aphthous ulcers? Available at: http://www.cks.nhs.uk/aphthous_ulcer/management/detailed_answers/managing_aphthous_ulcers#. Accessed January 28, 2010.
Evidence-based answers from the Family Physicians Inquiries Network
Which treatments provide the most relief for pharyngitis pain?
NONSTEROIDAL ANTI-INFLAMMATORY DRUGS (NSAIDs), acetaminophen, antibiotics, and oral and intramuscular steroids are effective (strength of recommendation [SOR]: A, meta-analysis).
Ibuprofen relieves pain more effectively than acetaminophen (SOR: A, meta-analysis). Antibiotics reduce pain in confirmed bacterial infections (SOR: A, multiple randomized controlled trials [RCTs]). Steroids are superior to placebo (SOR: A, meta-analysis).
Traditional demulcents, agents that help form a film over mucous membranes, provide less than 30 minutes of pain relief (SOR: B, small RCT); demulcents that contain benzocaine or lidocaine are longer acting (SOR: B, small RCT).
The efficacy of herbal remedies can’t be determined because of lack of high-quality studies (SOR: A, meta-analysis). Zinc doesn’t reduce pharyngitis symptoms (SOR: A, meta-analysis).
Evidence summary
A meta-analysis of 54 RCTs that investigated pain control, 5 of which focused on pharyngitis, showed that both ibuprofen and acetaminophen are more effective than placebo.1 In the 3 adult RCTs (N=346) and 2 pediatric RCTs (N=347) that studied pharyngitis specifically, 400 mg ibuprofen 3 times a day (10 mg/kg in children) provided more pain relief than 1000 mg acetaminophen 3 times a day (15 mg/kg in children).1
One of the RCTs, a double-blind, single-dose, single-center study of pharyngitis, found that 400 mg ibuprofen reduced pain by 80% at 3 hours compared with a 50% decrease for 1000 mg acetaminophen (P<.01).2 At 6 hours, ibuprofen still produced 70% relief compared with 20% for acetaminophen (P<.01). The meta-analysis demonstrated no significant difference in side effects between the 2 drugs.1
Steroids help, but concomitant antibiotics muddy the data
A meta-analysis of 8 RCTs enrolling 743 patients (369 children and 374 adults) found that oral and intramuscular steroids reduce duration and intensity of pain in moderate to severe pharyngitis and exudative pharyngitis.3 Four of the studies showed that corticosteroids completely resolve pain at 24 hours compared with placebo (number needed to treat [NNT]=3.7; 95% confidence interval [CI], 2.8-5.9), and 3 studies demonstrated pain relief at 48 hours (NNT=3.3; 95% CI, 2.4-5.6).
Although time to pain resolution varied among the studies, the research demonstrated a decrease in mean onset of pain relief by 6 hours compared with placebo (95% CI, 3.4-9.3; P<.001).3 All of the studies in the meta-analysis were limited by the fact that steroids were given in combination with antibiotics.
Demulcents have short-lived effect with a boost from anesthetics
A multicenter, prospective, randomized, double-blinded, placebo-controlled study (N=60) showed that demulcents provide short-term pain relief. On combined self-reported pain scales at 5, 10, 15, and 30 minutes, herbal tea demulcents were more effective than placebo (mean improvement in overall pain score=66.7 ± 39.2 on a 150-point scale, compared with 48.7 ± 32.8; P=.031). No difference was seen after 30 minutes.4
Demulcents with added anesthetics provide superior pain relief compared to placebo, as measured on a visual analog scale. In a single-center, randomized, double-blinded, placebo-controlled phase III study (N=240), patients who reported meaningful pain relief with lidocaine lozenges compared with placebo showed benefit from both single doses (38.3% lozenges vs 11.7% placebo; NNT=3.8) and multiple doses (73.3% lozenges vs 34.2% placebo; NNT=2.5). Additionally, pain relief lasted for >2 hours per lozenge. They also experienced more rapid onset of relief (24 minutes on average compared with 41 minutes).5
Antibiotics work better in patients with strep
A Cochrane review comparing antibiotics with placebo for sore throat showed an NNT of 5.8 (relative risk [RR]=0.68; 95% CI, 0.59-0.79) for pain resolution by Day 3 and an NNT of 21 (RR=0.49; 95% CI, 0.32-0.76) for pain resolution by Day 7. Antibiotics reduced pain more effectively in patients who tested positive for Streptococcus (RR=0.58; 95% CI, 0.48-0.71) than patients who tested negative (RR=0.78; 95% CI 0.63-0.97).6
Don’t bother with herbals or zinc
A Cochrane review of 7 RCTs of Chinese herbal remedies for sore throat pain found poor-quality methodology and thus, couldn’t recommend their use.7
A Cochrane review of zinc supplementation (13 therapeutic trials [N=966] and 2 preventive trials [N=394]) showed no significant improvement in pharyngitis symptoms compared with placebo, although zinc decreases the duration of the common cold, if taken within the first 24 hours of cold onset (standardized mean difference, -0.97; 95% CI, -1.56 to -0.38; P=.001).8 More patients in the intervention group experienced side effects (bad taste and nausea).
Recommendations
A primary care review article in the New England Journal of Medicine recommended acetaminophen as the drug of choice, while noting that ibuprofen has been shown in some studies to be more effective.9 The authors also recommended anesthetic gargles or lozenges. Antibiotics should be used in medical management only to prevent complications from Streptococcus-antigen-confirmed pharyngitis, they say.
Treatments recommended by the Institute for Clinical Systems Improvement include acetaminophen or ibuprofen, throat lozenges or hard candy, gargling with salt water (¼ tsp salt per 8 oz water), eating soft foods and frozen desserts, drinking cool or warm liquids, and antibiotics for bacterial infections.10
1. Pierce CA. Efficacy and safety of ibuprofen and acetaminophen in children and adults: a meta-analysis and qualitative review. Ann Pharmacother. 2010;44:489-506.
2. Schachtel BP, Fillingim JM, Thoden WR, et al. Sore throat pain in the evaluation of mild analgesics. Clin Pharmacol Ther. 1988;44:704-711.
3. Hayward G, Thompson M, Heneghan C, et al. Corticosteroids for pain relief in sore throat: systemic review and metaanalysis. BMJ. 2009;339:b2976.-
4. Brinckmann J, Sigwart H, van Houten L Taylor. Safety and efficacy of a traditional herbal medicine (Throat Coat) in symptomatic temporary relief of pain in patients with acute pharyngitis: a multicenter, prospective, randomized, double-blinded, placebo-controlled study. J Altern Complement Med. 2003;9:285-298.
5. Wonnemann M, Helm I, Strauss-Grabo M, et al. Lidocaine 8 mg sore throat lozenges in the treatment of acute pharyngitis. A new therapeutic option investigated in comparison to placebo treatment. Arznelmittelforschung. 2007;57:689-697.
6. Spinks A, Glasziou PP, Del Mar C. Antibiotics for sore throat. Cochrane Database Syst Rev. 2010;(2):CD000023.-
7. Shi Y, Gu R, Liu C, et al. Chinese medicinal herbs for sore throat. Cochrane Database Syst Rev. 2010;(3):CD004877.-
8. Singh M, Das RR. Zinc for the common cold. Cochrane Database Syst Rev. 2011;(2):CD001364.-
9. Bisno AL. Acute pharyngitis. N Engl J Med. 2001;344:201-211.
10. Institute for Clinical Systems Improvement. Diagnosis and treatment of respiratory illness in children and adults. Available at: www.icsi.org/guidelines_and_more/gl_os_prot/respiratory/respiratory_illness_in_children_and_adults__guideline_/respiratory_illness_in_children_and_adults__guideline__13110.html. Accessed February 10, 2011.
NONSTEROIDAL ANTI-INFLAMMATORY DRUGS (NSAIDs), acetaminophen, antibiotics, and oral and intramuscular steroids are effective (strength of recommendation [SOR]: A, meta-analysis).
Ibuprofen relieves pain more effectively than acetaminophen (SOR: A, meta-analysis). Antibiotics reduce pain in confirmed bacterial infections (SOR: A, multiple randomized controlled trials [RCTs]). Steroids are superior to placebo (SOR: A, meta-analysis).
Traditional demulcents, agents that help form a film over mucous membranes, provide less than 30 minutes of pain relief (SOR: B, small RCT); demulcents that contain benzocaine or lidocaine are longer acting (SOR: B, small RCT).
The efficacy of herbal remedies can’t be determined because of lack of high-quality studies (SOR: A, meta-analysis). Zinc doesn’t reduce pharyngitis symptoms (SOR: A, meta-analysis).
Evidence summary
A meta-analysis of 54 RCTs that investigated pain control, 5 of which focused on pharyngitis, showed that both ibuprofen and acetaminophen are more effective than placebo.1 In the 3 adult RCTs (N=346) and 2 pediatric RCTs (N=347) that studied pharyngitis specifically, 400 mg ibuprofen 3 times a day (10 mg/kg in children) provided more pain relief than 1000 mg acetaminophen 3 times a day (15 mg/kg in children).1
One of the RCTs, a double-blind, single-dose, single-center study of pharyngitis, found that 400 mg ibuprofen reduced pain by 80% at 3 hours compared with a 50% decrease for 1000 mg acetaminophen (P<.01).2 At 6 hours, ibuprofen still produced 70% relief compared with 20% for acetaminophen (P<.01). The meta-analysis demonstrated no significant difference in side effects between the 2 drugs.1
Steroids help, but concomitant antibiotics muddy the data
A meta-analysis of 8 RCTs enrolling 743 patients (369 children and 374 adults) found that oral and intramuscular steroids reduce duration and intensity of pain in moderate to severe pharyngitis and exudative pharyngitis.3 Four of the studies showed that corticosteroids completely resolve pain at 24 hours compared with placebo (number needed to treat [NNT]=3.7; 95% confidence interval [CI], 2.8-5.9), and 3 studies demonstrated pain relief at 48 hours (NNT=3.3; 95% CI, 2.4-5.6).
Although time to pain resolution varied among the studies, the research demonstrated a decrease in mean onset of pain relief by 6 hours compared with placebo (95% CI, 3.4-9.3; P<.001).3 All of the studies in the meta-analysis were limited by the fact that steroids were given in combination with antibiotics.
Demulcents have short-lived effect with a boost from anesthetics
A multicenter, prospective, randomized, double-blinded, placebo-controlled study (N=60) showed that demulcents provide short-term pain relief. On combined self-reported pain scales at 5, 10, 15, and 30 minutes, herbal tea demulcents were more effective than placebo (mean improvement in overall pain score=66.7 ± 39.2 on a 150-point scale, compared with 48.7 ± 32.8; P=.031). No difference was seen after 30 minutes.4
Demulcents with added anesthetics provide superior pain relief compared to placebo, as measured on a visual analog scale. In a single-center, randomized, double-blinded, placebo-controlled phase III study (N=240), patients who reported meaningful pain relief with lidocaine lozenges compared with placebo showed benefit from both single doses (38.3% lozenges vs 11.7% placebo; NNT=3.8) and multiple doses (73.3% lozenges vs 34.2% placebo; NNT=2.5). Additionally, pain relief lasted for >2 hours per lozenge. They also experienced more rapid onset of relief (24 minutes on average compared with 41 minutes).5
Antibiotics work better in patients with strep
A Cochrane review comparing antibiotics with placebo for sore throat showed an NNT of 5.8 (relative risk [RR]=0.68; 95% CI, 0.59-0.79) for pain resolution by Day 3 and an NNT of 21 (RR=0.49; 95% CI, 0.32-0.76) for pain resolution by Day 7. Antibiotics reduced pain more effectively in patients who tested positive for Streptococcus (RR=0.58; 95% CI, 0.48-0.71) than patients who tested negative (RR=0.78; 95% CI 0.63-0.97).6
Don’t bother with herbals or zinc
A Cochrane review of 7 RCTs of Chinese herbal remedies for sore throat pain found poor-quality methodology and thus, couldn’t recommend their use.7
A Cochrane review of zinc supplementation (13 therapeutic trials [N=966] and 2 preventive trials [N=394]) showed no significant improvement in pharyngitis symptoms compared with placebo, although zinc decreases the duration of the common cold, if taken within the first 24 hours of cold onset (standardized mean difference, -0.97; 95% CI, -1.56 to -0.38; P=.001).8 More patients in the intervention group experienced side effects (bad taste and nausea).
Recommendations
A primary care review article in the New England Journal of Medicine recommended acetaminophen as the drug of choice, while noting that ibuprofen has been shown in some studies to be more effective.9 The authors also recommended anesthetic gargles or lozenges. Antibiotics should be used in medical management only to prevent complications from Streptococcus-antigen-confirmed pharyngitis, they say.
Treatments recommended by the Institute for Clinical Systems Improvement include acetaminophen or ibuprofen, throat lozenges or hard candy, gargling with salt water (¼ tsp salt per 8 oz water), eating soft foods and frozen desserts, drinking cool or warm liquids, and antibiotics for bacterial infections.10
NONSTEROIDAL ANTI-INFLAMMATORY DRUGS (NSAIDs), acetaminophen, antibiotics, and oral and intramuscular steroids are effective (strength of recommendation [SOR]: A, meta-analysis).
Ibuprofen relieves pain more effectively than acetaminophen (SOR: A, meta-analysis). Antibiotics reduce pain in confirmed bacterial infections (SOR: A, multiple randomized controlled trials [RCTs]). Steroids are superior to placebo (SOR: A, meta-analysis).
Traditional demulcents, agents that help form a film over mucous membranes, provide less than 30 minutes of pain relief (SOR: B, small RCT); demulcents that contain benzocaine or lidocaine are longer acting (SOR: B, small RCT).
The efficacy of herbal remedies can’t be determined because of lack of high-quality studies (SOR: A, meta-analysis). Zinc doesn’t reduce pharyngitis symptoms (SOR: A, meta-analysis).
Evidence summary
A meta-analysis of 54 RCTs that investigated pain control, 5 of which focused on pharyngitis, showed that both ibuprofen and acetaminophen are more effective than placebo.1 In the 3 adult RCTs (N=346) and 2 pediatric RCTs (N=347) that studied pharyngitis specifically, 400 mg ibuprofen 3 times a day (10 mg/kg in children) provided more pain relief than 1000 mg acetaminophen 3 times a day (15 mg/kg in children).1
One of the RCTs, a double-blind, single-dose, single-center study of pharyngitis, found that 400 mg ibuprofen reduced pain by 80% at 3 hours compared with a 50% decrease for 1000 mg acetaminophen (P<.01).2 At 6 hours, ibuprofen still produced 70% relief compared with 20% for acetaminophen (P<.01). The meta-analysis demonstrated no significant difference in side effects between the 2 drugs.1
Steroids help, but concomitant antibiotics muddy the data
A meta-analysis of 8 RCTs enrolling 743 patients (369 children and 374 adults) found that oral and intramuscular steroids reduce duration and intensity of pain in moderate to severe pharyngitis and exudative pharyngitis.3 Four of the studies showed that corticosteroids completely resolve pain at 24 hours compared with placebo (number needed to treat [NNT]=3.7; 95% confidence interval [CI], 2.8-5.9), and 3 studies demonstrated pain relief at 48 hours (NNT=3.3; 95% CI, 2.4-5.6).
Although time to pain resolution varied among the studies, the research demonstrated a decrease in mean onset of pain relief by 6 hours compared with placebo (95% CI, 3.4-9.3; P<.001).3 All of the studies in the meta-analysis were limited by the fact that steroids were given in combination with antibiotics.
Demulcents have short-lived effect with a boost from anesthetics
A multicenter, prospective, randomized, double-blinded, placebo-controlled study (N=60) showed that demulcents provide short-term pain relief. On combined self-reported pain scales at 5, 10, 15, and 30 minutes, herbal tea demulcents were more effective than placebo (mean improvement in overall pain score=66.7 ± 39.2 on a 150-point scale, compared with 48.7 ± 32.8; P=.031). No difference was seen after 30 minutes.4
Demulcents with added anesthetics provide superior pain relief compared to placebo, as measured on a visual analog scale. In a single-center, randomized, double-blinded, placebo-controlled phase III study (N=240), patients who reported meaningful pain relief with lidocaine lozenges compared with placebo showed benefit from both single doses (38.3% lozenges vs 11.7% placebo; NNT=3.8) and multiple doses (73.3% lozenges vs 34.2% placebo; NNT=2.5). Additionally, pain relief lasted for >2 hours per lozenge. They also experienced more rapid onset of relief (24 minutes on average compared with 41 minutes).5
Antibiotics work better in patients with strep
A Cochrane review comparing antibiotics with placebo for sore throat showed an NNT of 5.8 (relative risk [RR]=0.68; 95% CI, 0.59-0.79) for pain resolution by Day 3 and an NNT of 21 (RR=0.49; 95% CI, 0.32-0.76) for pain resolution by Day 7. Antibiotics reduced pain more effectively in patients who tested positive for Streptococcus (RR=0.58; 95% CI, 0.48-0.71) than patients who tested negative (RR=0.78; 95% CI 0.63-0.97).6
Don’t bother with herbals or zinc
A Cochrane review of 7 RCTs of Chinese herbal remedies for sore throat pain found poor-quality methodology and thus, couldn’t recommend their use.7
A Cochrane review of zinc supplementation (13 therapeutic trials [N=966] and 2 preventive trials [N=394]) showed no significant improvement in pharyngitis symptoms compared with placebo, although zinc decreases the duration of the common cold, if taken within the first 24 hours of cold onset (standardized mean difference, -0.97; 95% CI, -1.56 to -0.38; P=.001).8 More patients in the intervention group experienced side effects (bad taste and nausea).
Recommendations
A primary care review article in the New England Journal of Medicine recommended acetaminophen as the drug of choice, while noting that ibuprofen has been shown in some studies to be more effective.9 The authors also recommended anesthetic gargles or lozenges. Antibiotics should be used in medical management only to prevent complications from Streptococcus-antigen-confirmed pharyngitis, they say.
Treatments recommended by the Institute for Clinical Systems Improvement include acetaminophen or ibuprofen, throat lozenges or hard candy, gargling with salt water (¼ tsp salt per 8 oz water), eating soft foods and frozen desserts, drinking cool or warm liquids, and antibiotics for bacterial infections.10
1. Pierce CA. Efficacy and safety of ibuprofen and acetaminophen in children and adults: a meta-analysis and qualitative review. Ann Pharmacother. 2010;44:489-506.
2. Schachtel BP, Fillingim JM, Thoden WR, et al. Sore throat pain in the evaluation of mild analgesics. Clin Pharmacol Ther. 1988;44:704-711.
3. Hayward G, Thompson M, Heneghan C, et al. Corticosteroids for pain relief in sore throat: systemic review and metaanalysis. BMJ. 2009;339:b2976.-
4. Brinckmann J, Sigwart H, van Houten L Taylor. Safety and efficacy of a traditional herbal medicine (Throat Coat) in symptomatic temporary relief of pain in patients with acute pharyngitis: a multicenter, prospective, randomized, double-blinded, placebo-controlled study. J Altern Complement Med. 2003;9:285-298.
5. Wonnemann M, Helm I, Strauss-Grabo M, et al. Lidocaine 8 mg sore throat lozenges in the treatment of acute pharyngitis. A new therapeutic option investigated in comparison to placebo treatment. Arznelmittelforschung. 2007;57:689-697.
6. Spinks A, Glasziou PP, Del Mar C. Antibiotics for sore throat. Cochrane Database Syst Rev. 2010;(2):CD000023.-
7. Shi Y, Gu R, Liu C, et al. Chinese medicinal herbs for sore throat. Cochrane Database Syst Rev. 2010;(3):CD004877.-
8. Singh M, Das RR. Zinc for the common cold. Cochrane Database Syst Rev. 2011;(2):CD001364.-
9. Bisno AL. Acute pharyngitis. N Engl J Med. 2001;344:201-211.
10. Institute for Clinical Systems Improvement. Diagnosis and treatment of respiratory illness in children and adults. Available at: www.icsi.org/guidelines_and_more/gl_os_prot/respiratory/respiratory_illness_in_children_and_adults__guideline_/respiratory_illness_in_children_and_adults__guideline__13110.html. Accessed February 10, 2011.
1. Pierce CA. Efficacy and safety of ibuprofen and acetaminophen in children and adults: a meta-analysis and qualitative review. Ann Pharmacother. 2010;44:489-506.
2. Schachtel BP, Fillingim JM, Thoden WR, et al. Sore throat pain in the evaluation of mild analgesics. Clin Pharmacol Ther. 1988;44:704-711.
3. Hayward G, Thompson M, Heneghan C, et al. Corticosteroids for pain relief in sore throat: systemic review and metaanalysis. BMJ. 2009;339:b2976.-
4. Brinckmann J, Sigwart H, van Houten L Taylor. Safety and efficacy of a traditional herbal medicine (Throat Coat) in symptomatic temporary relief of pain in patients with acute pharyngitis: a multicenter, prospective, randomized, double-blinded, placebo-controlled study. J Altern Complement Med. 2003;9:285-298.
5. Wonnemann M, Helm I, Strauss-Grabo M, et al. Lidocaine 8 mg sore throat lozenges in the treatment of acute pharyngitis. A new therapeutic option investigated in comparison to placebo treatment. Arznelmittelforschung. 2007;57:689-697.
6. Spinks A, Glasziou PP, Del Mar C. Antibiotics for sore throat. Cochrane Database Syst Rev. 2010;(2):CD000023.-
7. Shi Y, Gu R, Liu C, et al. Chinese medicinal herbs for sore throat. Cochrane Database Syst Rev. 2010;(3):CD004877.-
8. Singh M, Das RR. Zinc for the common cold. Cochrane Database Syst Rev. 2011;(2):CD001364.-
9. Bisno AL. Acute pharyngitis. N Engl J Med. 2001;344:201-211.
10. Institute for Clinical Systems Improvement. Diagnosis and treatment of respiratory illness in children and adults. Available at: www.icsi.org/guidelines_and_more/gl_os_prot/respiratory/respiratory_illness_in_children_and_adults__guideline_/respiratory_illness_in_children_and_adults__guideline__13110.html. Accessed February 10, 2011.
Evidence-based answers from the Family Physicians Inquiries Network
Does lowering a fever >101°F in children improve clinical outcomes?
IT DEPENDS ON WHICH OUTCOMES YOU LOOK AT. Treating fever significantly increases comfort, activity, feeding, and fluid intake and decreases the patient’s temperature compared with placebo (strength of recommendation (SOR): A, multiple randomized controlled trials [RCTs]). It doesn’t shorten or prolong the overall duration of illness or reduce the recurrence of febrile seizures (SOR: A, multiple RCTs). In patients with varicella, reducing fever prolongs the time it takes for lesions to crust, but doesn’t appear to cause group A streptococcal necrotizing fasciitis (SOR: B, multiple prospective cohorts).
Ibuprofen and acetaminophen reduce fever effectively and safely; their side effect levels are similar to placebo (SOR: A, multiple RCTs). Physical methods of cooling also are effective for lowering fever (SOR: A, high-quality meta-analysis).
Evidence summary
The possible risks and benefits of lowering fever with antipyretics have prompted much discussion in the medical literature. Most evidence supporting the useful effects of fever comes from animal models. A few human studies in special populations (patients with brain trauma) suggest that antipyretics may worsen certain aspects of disease processes.1 However, many studies show that antipyretics do clinically benefit, and don’t harm, the typical child with an upper respiratory illness.2-4
Acetaminophen improves some symptoms, but doesn’t shorten fever
A double-blind, randomized, placebo-controlled trial of 210 children with upper respiratory illness showed that giving acetaminophen significantly increased short-term temperature reduction compared with placebo (0.36°F vs 0.09°F/hr; P<.001). Acetaminophen also improved subjective symptoms at 6 hours over placebo: activity (60% vs 16%; P<.001), alertness (58% vs 21%; P<.001), comfort (37% vs 7%; P<.001), mood (36% vs 12%; P<.001), appetite (20% vs 1%; P<0.001), and fluid intake (22% vs 2%; P<.001).2 Total time until complete resolution of fever (defined as no fever with or without medication) didn’t differ between treatment and placebo groups (32 hr for acetaminophen vs 36 hr for placebo; P=.23).2
A similar study failed to show a statistically significant difference between acetaminophen and placebo in fever clearance time (34.7 vs 36.1 hr), mood, comfort, or appetite. However, the study did find significant improvement in activity (38% vs 11%; P=.005) and alertness (33% vs 12%; P=.036) based on parents’ reports.3
Ibuprofen is a better antipyretic than acetaminophen
A meta-analysis (N=84,192) comparing acetaminophen with ibuprofen found both drugs to be equally efficacious analgesics; ibuprofen was a more effective antipyretic. Both drugs had the same level of adverse outcomes when compared with each other and placebo.5
Lowering fever doesn’t reduce recurrence of febrile seizures
Antipyretics don’t appear to affect the recurrence of febrile seizures. In a well-designed, randomized, double-blind, placebo-controlled trial, 230 patients 1 to 4 years of age with 1 or more risk factors for febrile seizures were randomized to fever reduction with ibuprofen or placebo. The estimated 2-year probability for recurrent febrile seizure was 32% in the ibuprofen group and 39% for the placebo group. The difference between the groups was not significant (relative risk=0.9; 95% confidence interval [CI], 0.6-1.5).6
Varicella lesions crust more slowly with acetaminophen
An RCT involving 68 children with varicella found that acetaminophen increased the time for lesions to crust compared with placebo (6.7 days for acetaminophen vs 5.6 days for placebo) and that acetaminophen didn’t alleviate itching or improve appetite. However, patients taking acetaminophen were more active by day 2.7
NSAIDs don’t cause necrotizing fasciitis
A case-control study of 48 children with varicella suggested an association between ibuprofen and increased incidence of necrotizing soft tissue infections (odds ratio [OR]=11.5; 95% CI, 1.4-96.9),8 but larger reviews haven’t borne out this finding. A review of 5 prospective studies of nonsteroidal anti-inflammatory drugs and invasive soft-tissue infections (N=912; 114 cases of necrotizing fasciitis) failed to show any connection. The largest study (474 cases) suggested a trend that was not statistically significant (OR=3.5; 95% CI, 0.8-16).9
Nonpharmacologic measures also lower fever
A Cochrane review showed that cool water sponging caused fever reduction similar to antipyretics at 1 hour; sponging combined with ibuprofen reduced the proportion of patients still febrile at 1 hour. Common side effects of sponging included goose pimples and shivering. The antipyretic effect didn’t last beyond a few hours.10
Recommendations
Concerning treatment of fever, Nelson’s Pediatrics states, “Fever with temperatures less than 39°C (102.2°F) in healthy children generally does not require treatment. As temperatures become higher, patients tend to become more uncomfortable and administration of antipyretics often makes patients feel better. Other than providing symptomatic relief, antipyretic therapy does not change the course of infectious diseases. Antipyretic therapy is beneficial in high-risk patients who have chronic cardiopulmonary diseases, metabolic disorders, or neurologic diseases and in those who are at risk for febrile seizures. Hyperpyrexia (>41°C [105.8°F]) indicates greater risk for severe infection and should always be treated with antipyretics.”11
Acknowledgement
The opinions and assertions contained herein are the private views of the authors and not to be construed as official, or as reflecting the views of the United States Air Force Medical Service or the US Air Force at large.
1. Mackowiak PA, Plaisance KI. Benefits and risks of antipyretic therapy. Ann NY Acad Sci. 1998;856:214-223.
2. Gupta H, Shah D, Gupta P, et al. Role of paracetamol in treatment of childhood fever: a double-blind randomized placebo controlled trial. Indian Pediatr. 2007;44:903-911.
3. Kramer MS, Naimark LE, Roberts-Brauer R, et al. Risks and benefits of paracetamol antipyresis in young children with fever of presumed viral origin. Lancet. 1991;337:591-594.
4. Bernard GR, Wheeler AP, Russell JA, et al. The effects of ibuprophen on the physiology and survival of patients with sepsis. The Ibuprofen in Sepsis Study Group. N Engl J Med. 1997;336:912-918.
5. Perrott DA, Pirra T, Goodenough B, et al. Efficacy and safety of acetaminophen vs ibuprofen for treating children’s pain or fever: a meta-analysis. Arch Pediatr Adolesc Med. 2004;158:521-526.
6. Van Stuijvenberg M, Derksen-Lubsen G, Steyerberg EW, et al. Randomized, controlled trial of ibuprofen syrup administered during febrile illnesses to prevent febrile seizure recurrence. Pediatrics. 1998;102:E51.-
7. Doran TF, DeAngelis C, Baumgardner RA, et al. Acetaminophen: more harm than good for chickenpox? J Pediatr. 1989;114:1045-1048.
8. Zerr DM, Alexander ER, Duchin JS, et al. A case control study of necrotizing fasciitis during primary varicella. Pediatrics. 1999;103:783-790.
9. Aronoff DM, Bloch KC. Assessing the relationship between the use of nonsteroidal antiinflammatory drugs and necrotizing fasciitis caused by group A streptococcus. Medicine (Baltimore). 2003;82:225-235.
10. Meremikwu M, Oyo-Ita A. Physical methods for treating fever in children. Cochrane Database Syst Rev. 2003;(2):CD004264.-
11. Powell K. Fever. In: Kliegman RM, Behrman RE, Jenson HB, et al., eds. Nelson Textbook of Pediatrics. 18th ed. Philadelphia: Saunders Elsevier; 2007:1084-1086.
IT DEPENDS ON WHICH OUTCOMES YOU LOOK AT. Treating fever significantly increases comfort, activity, feeding, and fluid intake and decreases the patient’s temperature compared with placebo (strength of recommendation (SOR): A, multiple randomized controlled trials [RCTs]). It doesn’t shorten or prolong the overall duration of illness or reduce the recurrence of febrile seizures (SOR: A, multiple RCTs). In patients with varicella, reducing fever prolongs the time it takes for lesions to crust, but doesn’t appear to cause group A streptococcal necrotizing fasciitis (SOR: B, multiple prospective cohorts).
Ibuprofen and acetaminophen reduce fever effectively and safely; their side effect levels are similar to placebo (SOR: A, multiple RCTs). Physical methods of cooling also are effective for lowering fever (SOR: A, high-quality meta-analysis).
Evidence summary
The possible risks and benefits of lowering fever with antipyretics have prompted much discussion in the medical literature. Most evidence supporting the useful effects of fever comes from animal models. A few human studies in special populations (patients with brain trauma) suggest that antipyretics may worsen certain aspects of disease processes.1 However, many studies show that antipyretics do clinically benefit, and don’t harm, the typical child with an upper respiratory illness.2-4
Acetaminophen improves some symptoms, but doesn’t shorten fever
A double-blind, randomized, placebo-controlled trial of 210 children with upper respiratory illness showed that giving acetaminophen significantly increased short-term temperature reduction compared with placebo (0.36°F vs 0.09°F/hr; P<.001). Acetaminophen also improved subjective symptoms at 6 hours over placebo: activity (60% vs 16%; P<.001), alertness (58% vs 21%; P<.001), comfort (37% vs 7%; P<.001), mood (36% vs 12%; P<.001), appetite (20% vs 1%; P<0.001), and fluid intake (22% vs 2%; P<.001).2 Total time until complete resolution of fever (defined as no fever with or without medication) didn’t differ between treatment and placebo groups (32 hr for acetaminophen vs 36 hr for placebo; P=.23).2
A similar study failed to show a statistically significant difference between acetaminophen and placebo in fever clearance time (34.7 vs 36.1 hr), mood, comfort, or appetite. However, the study did find significant improvement in activity (38% vs 11%; P=.005) and alertness (33% vs 12%; P=.036) based on parents’ reports.3
Ibuprofen is a better antipyretic than acetaminophen
A meta-analysis (N=84,192) comparing acetaminophen with ibuprofen found both drugs to be equally efficacious analgesics; ibuprofen was a more effective antipyretic. Both drugs had the same level of adverse outcomes when compared with each other and placebo.5
Lowering fever doesn’t reduce recurrence of febrile seizures
Antipyretics don’t appear to affect the recurrence of febrile seizures. In a well-designed, randomized, double-blind, placebo-controlled trial, 230 patients 1 to 4 years of age with 1 or more risk factors for febrile seizures were randomized to fever reduction with ibuprofen or placebo. The estimated 2-year probability for recurrent febrile seizure was 32% in the ibuprofen group and 39% for the placebo group. The difference between the groups was not significant (relative risk=0.9; 95% confidence interval [CI], 0.6-1.5).6
Varicella lesions crust more slowly with acetaminophen
An RCT involving 68 children with varicella found that acetaminophen increased the time for lesions to crust compared with placebo (6.7 days for acetaminophen vs 5.6 days for placebo) and that acetaminophen didn’t alleviate itching or improve appetite. However, patients taking acetaminophen were more active by day 2.7
NSAIDs don’t cause necrotizing fasciitis
A case-control study of 48 children with varicella suggested an association between ibuprofen and increased incidence of necrotizing soft tissue infections (odds ratio [OR]=11.5; 95% CI, 1.4-96.9),8 but larger reviews haven’t borne out this finding. A review of 5 prospective studies of nonsteroidal anti-inflammatory drugs and invasive soft-tissue infections (N=912; 114 cases of necrotizing fasciitis) failed to show any connection. The largest study (474 cases) suggested a trend that was not statistically significant (OR=3.5; 95% CI, 0.8-16).9
Nonpharmacologic measures also lower fever
A Cochrane review showed that cool water sponging caused fever reduction similar to antipyretics at 1 hour; sponging combined with ibuprofen reduced the proportion of patients still febrile at 1 hour. Common side effects of sponging included goose pimples and shivering. The antipyretic effect didn’t last beyond a few hours.10
Recommendations
Concerning treatment of fever, Nelson’s Pediatrics states, “Fever with temperatures less than 39°C (102.2°F) in healthy children generally does not require treatment. As temperatures become higher, patients tend to become more uncomfortable and administration of antipyretics often makes patients feel better. Other than providing symptomatic relief, antipyretic therapy does not change the course of infectious diseases. Antipyretic therapy is beneficial in high-risk patients who have chronic cardiopulmonary diseases, metabolic disorders, or neurologic diseases and in those who are at risk for febrile seizures. Hyperpyrexia (>41°C [105.8°F]) indicates greater risk for severe infection and should always be treated with antipyretics.”11
Acknowledgement
The opinions and assertions contained herein are the private views of the authors and not to be construed as official, or as reflecting the views of the United States Air Force Medical Service or the US Air Force at large.
IT DEPENDS ON WHICH OUTCOMES YOU LOOK AT. Treating fever significantly increases comfort, activity, feeding, and fluid intake and decreases the patient’s temperature compared with placebo (strength of recommendation (SOR): A, multiple randomized controlled trials [RCTs]). It doesn’t shorten or prolong the overall duration of illness or reduce the recurrence of febrile seizures (SOR: A, multiple RCTs). In patients with varicella, reducing fever prolongs the time it takes for lesions to crust, but doesn’t appear to cause group A streptococcal necrotizing fasciitis (SOR: B, multiple prospective cohorts).
Ibuprofen and acetaminophen reduce fever effectively and safely; their side effect levels are similar to placebo (SOR: A, multiple RCTs). Physical methods of cooling also are effective for lowering fever (SOR: A, high-quality meta-analysis).
Evidence summary
The possible risks and benefits of lowering fever with antipyretics have prompted much discussion in the medical literature. Most evidence supporting the useful effects of fever comes from animal models. A few human studies in special populations (patients with brain trauma) suggest that antipyretics may worsen certain aspects of disease processes.1 However, many studies show that antipyretics do clinically benefit, and don’t harm, the typical child with an upper respiratory illness.2-4
Acetaminophen improves some symptoms, but doesn’t shorten fever
A double-blind, randomized, placebo-controlled trial of 210 children with upper respiratory illness showed that giving acetaminophen significantly increased short-term temperature reduction compared with placebo (0.36°F vs 0.09°F/hr; P<.001). Acetaminophen also improved subjective symptoms at 6 hours over placebo: activity (60% vs 16%; P<.001), alertness (58% vs 21%; P<.001), comfort (37% vs 7%; P<.001), mood (36% vs 12%; P<.001), appetite (20% vs 1%; P<0.001), and fluid intake (22% vs 2%; P<.001).2 Total time until complete resolution of fever (defined as no fever with or without medication) didn’t differ between treatment and placebo groups (32 hr for acetaminophen vs 36 hr for placebo; P=.23).2
A similar study failed to show a statistically significant difference between acetaminophen and placebo in fever clearance time (34.7 vs 36.1 hr), mood, comfort, or appetite. However, the study did find significant improvement in activity (38% vs 11%; P=.005) and alertness (33% vs 12%; P=.036) based on parents’ reports.3
Ibuprofen is a better antipyretic than acetaminophen
A meta-analysis (N=84,192) comparing acetaminophen with ibuprofen found both drugs to be equally efficacious analgesics; ibuprofen was a more effective antipyretic. Both drugs had the same level of adverse outcomes when compared with each other and placebo.5
Lowering fever doesn’t reduce recurrence of febrile seizures
Antipyretics don’t appear to affect the recurrence of febrile seizures. In a well-designed, randomized, double-blind, placebo-controlled trial, 230 patients 1 to 4 years of age with 1 or more risk factors for febrile seizures were randomized to fever reduction with ibuprofen or placebo. The estimated 2-year probability for recurrent febrile seizure was 32% in the ibuprofen group and 39% for the placebo group. The difference between the groups was not significant (relative risk=0.9; 95% confidence interval [CI], 0.6-1.5).6
Varicella lesions crust more slowly with acetaminophen
An RCT involving 68 children with varicella found that acetaminophen increased the time for lesions to crust compared with placebo (6.7 days for acetaminophen vs 5.6 days for placebo) and that acetaminophen didn’t alleviate itching or improve appetite. However, patients taking acetaminophen were more active by day 2.7
NSAIDs don’t cause necrotizing fasciitis
A case-control study of 48 children with varicella suggested an association between ibuprofen and increased incidence of necrotizing soft tissue infections (odds ratio [OR]=11.5; 95% CI, 1.4-96.9),8 but larger reviews haven’t borne out this finding. A review of 5 prospective studies of nonsteroidal anti-inflammatory drugs and invasive soft-tissue infections (N=912; 114 cases of necrotizing fasciitis) failed to show any connection. The largest study (474 cases) suggested a trend that was not statistically significant (OR=3.5; 95% CI, 0.8-16).9
Nonpharmacologic measures also lower fever
A Cochrane review showed that cool water sponging caused fever reduction similar to antipyretics at 1 hour; sponging combined with ibuprofen reduced the proportion of patients still febrile at 1 hour. Common side effects of sponging included goose pimples and shivering. The antipyretic effect didn’t last beyond a few hours.10
Recommendations
Concerning treatment of fever, Nelson’s Pediatrics states, “Fever with temperatures less than 39°C (102.2°F) in healthy children generally does not require treatment. As temperatures become higher, patients tend to become more uncomfortable and administration of antipyretics often makes patients feel better. Other than providing symptomatic relief, antipyretic therapy does not change the course of infectious diseases. Antipyretic therapy is beneficial in high-risk patients who have chronic cardiopulmonary diseases, metabolic disorders, or neurologic diseases and in those who are at risk for febrile seizures. Hyperpyrexia (>41°C [105.8°F]) indicates greater risk for severe infection and should always be treated with antipyretics.”11
Acknowledgement
The opinions and assertions contained herein are the private views of the authors and not to be construed as official, or as reflecting the views of the United States Air Force Medical Service or the US Air Force at large.
1. Mackowiak PA, Plaisance KI. Benefits and risks of antipyretic therapy. Ann NY Acad Sci. 1998;856:214-223.
2. Gupta H, Shah D, Gupta P, et al. Role of paracetamol in treatment of childhood fever: a double-blind randomized placebo controlled trial. Indian Pediatr. 2007;44:903-911.
3. Kramer MS, Naimark LE, Roberts-Brauer R, et al. Risks and benefits of paracetamol antipyresis in young children with fever of presumed viral origin. Lancet. 1991;337:591-594.
4. Bernard GR, Wheeler AP, Russell JA, et al. The effects of ibuprophen on the physiology and survival of patients with sepsis. The Ibuprofen in Sepsis Study Group. N Engl J Med. 1997;336:912-918.
5. Perrott DA, Pirra T, Goodenough B, et al. Efficacy and safety of acetaminophen vs ibuprofen for treating children’s pain or fever: a meta-analysis. Arch Pediatr Adolesc Med. 2004;158:521-526.
6. Van Stuijvenberg M, Derksen-Lubsen G, Steyerberg EW, et al. Randomized, controlled trial of ibuprofen syrup administered during febrile illnesses to prevent febrile seizure recurrence. Pediatrics. 1998;102:E51.-
7. Doran TF, DeAngelis C, Baumgardner RA, et al. Acetaminophen: more harm than good for chickenpox? J Pediatr. 1989;114:1045-1048.
8. Zerr DM, Alexander ER, Duchin JS, et al. A case control study of necrotizing fasciitis during primary varicella. Pediatrics. 1999;103:783-790.
9. Aronoff DM, Bloch KC. Assessing the relationship between the use of nonsteroidal antiinflammatory drugs and necrotizing fasciitis caused by group A streptococcus. Medicine (Baltimore). 2003;82:225-235.
10. Meremikwu M, Oyo-Ita A. Physical methods for treating fever in children. Cochrane Database Syst Rev. 2003;(2):CD004264.-
11. Powell K. Fever. In: Kliegman RM, Behrman RE, Jenson HB, et al., eds. Nelson Textbook of Pediatrics. 18th ed. Philadelphia: Saunders Elsevier; 2007:1084-1086.
1. Mackowiak PA, Plaisance KI. Benefits and risks of antipyretic therapy. Ann NY Acad Sci. 1998;856:214-223.
2. Gupta H, Shah D, Gupta P, et al. Role of paracetamol in treatment of childhood fever: a double-blind randomized placebo controlled trial. Indian Pediatr. 2007;44:903-911.
3. Kramer MS, Naimark LE, Roberts-Brauer R, et al. Risks and benefits of paracetamol antipyresis in young children with fever of presumed viral origin. Lancet. 1991;337:591-594.
4. Bernard GR, Wheeler AP, Russell JA, et al. The effects of ibuprophen on the physiology and survival of patients with sepsis. The Ibuprofen in Sepsis Study Group. N Engl J Med. 1997;336:912-918.
5. Perrott DA, Pirra T, Goodenough B, et al. Efficacy and safety of acetaminophen vs ibuprofen for treating children’s pain or fever: a meta-analysis. Arch Pediatr Adolesc Med. 2004;158:521-526.
6. Van Stuijvenberg M, Derksen-Lubsen G, Steyerberg EW, et al. Randomized, controlled trial of ibuprofen syrup administered during febrile illnesses to prevent febrile seizure recurrence. Pediatrics. 1998;102:E51.-
7. Doran TF, DeAngelis C, Baumgardner RA, et al. Acetaminophen: more harm than good for chickenpox? J Pediatr. 1989;114:1045-1048.
8. Zerr DM, Alexander ER, Duchin JS, et al. A case control study of necrotizing fasciitis during primary varicella. Pediatrics. 1999;103:783-790.
9. Aronoff DM, Bloch KC. Assessing the relationship between the use of nonsteroidal antiinflammatory drugs and necrotizing fasciitis caused by group A streptococcus. Medicine (Baltimore). 2003;82:225-235.
10. Meremikwu M, Oyo-Ita A. Physical methods for treating fever in children. Cochrane Database Syst Rev. 2003;(2):CD004264.-
11. Powell K. Fever. In: Kliegman RM, Behrman RE, Jenson HB, et al., eds. Nelson Textbook of Pediatrics. 18th ed. Philadelphia: Saunders Elsevier; 2007:1084-1086.
Evidence-based answers from the Family Physicians Inquiries Network
How should you manage children born to hepatitis C-positive women?
FOR STARTERS, don’t be overly concerned with the mode of delivery; it doesn’t influence the rate of transmission of hepatitis C virus (HCV), except in women who are also infected with human immunodeficiency virus (HIV) (strength of recommendation [SOR]: B, consistent retrospective cohort studies).
Avoid internal fetal monitoring and prolonged rupture of membranes (SOR: B, single retrospective cohort study).
Advise patients that it’s OK to breastfeed. Breastfeeding doesn’t affect transmission (SOR: B, consistent prospective cohort studies).
Check HCV RNA and serum anti-HCV on 2 occasions between 2 and 6 months of age and 18 and 24 months of age (SOR: B, consistent prospective cohort studies).
Evidence summary
Perinatal transmission of HCV is rare. It occurs only when serum HCV RNA is detectable; transmission rates may be related to higher levels (>106 copies/mL).1 HCV is transmitted to 2% of infants of anti-HCV seropositive women and 4% to 7% of infants born to mothers who are HCV RNA-positive at delivery.1
Spontaneous clearance of the virus occurs in approximately 20% of infants. Most remain asymptomatic if HCV persists, but have mild elevation of liver function tests.2
Routine screening for HCV in mothers is not recommended, but pregnant women at high risk for HCV infection should be screened for anti-HCV.
Route of delivery: Only a concern for HIV-positive mothers
The mode of delivery doesn’t influence the rate of HCV transmission, except in mothers with HIV. Retrospective analysis of 503 HCV-positive mothers coinfected with HIV showed a decreased risk of transmission during cesarean delivery (odds ratio [OR]=0.36; P=.01; number needed to treat [NNT]=10).3
One study suggested an increased rate of vertical HCV transmission during vaginal delivery compared with cesarean delivery (32% vs 6%; P<.05). The study didn’t account for the percent of mothers coinfected with HIV, however.4
A meta-analysis of 11 studies showed similar rates of transmission for vaginal and cesarean delivery: adjusted rates were 4.3% and 3%, respectively.1
Internal monitoring is an issue
Avoid internal fetal monitoring to minimize HCV transmission, based on a single retrospective cohort of 244 infants born to HCV-positive mothers (relative risk [RR]= 7.7; 95% confidence interval [CI], 1.9-31.6; number needed to harm [NNH]=6).7 The same study showed an increased risk with membrane rupture longer than 6 hours (RR=9.9; 95% CI, 1.2-81; NNH=13).5
Breastfeeding doesn’t significantly affect HCV transmission. Transmission rates for breastfed and nonbreastfed infants are 3.7% and 3.9%, respectively.1
Defer postpartum lab testing
Because about 20% of infants exposed to HCV clear the virus spontaneously, and maternal antibodies can confound laboratory results, deferring postpartum diagnostic testing is appropriate. A study of 1104 children in whom vertical transmission didn’t occur after exposure to HCV showed that 95% of the children were anti-HCV antibody negative by 12 months age.6 A prospective study of 23 infants documented spontaneous clearance of HCV RNA by 6 months in all patients.7
Recommendations
The National Institutes of Health 2002 Consensus Statement recommends:8
- avoiding fetal scalp electrodes and prolonged rupture of membranes
- serum testing for HCV RNA at 2 months and 6 months of age
- anti-HCV antibody testing after 15 months of age.
The American College of Obstetricians and Gynecologists supports breastfeeding, recommends against routine HCV screening, and recommends that cesarean delivery be reserved for obstetric indications.9
The American Association for the Study of Liver Diseases recommends serum testing and liver biopsy on the same schedule as adult patients and endorses considering treatment after 3 years of age.6
The US Food and Drug Administration has approved treatment after 3 years of age for children with detectable HCV RNA levels higher than 50 IU/mL and who have had a liver biopsy with portal or bridging fibrosis and at least moderate inflammation and necrosis.
The American Gastroenterological Association recommends considering treatment with PEG-interferon and ribavirin after 3 years of age.10
Acknowledgements
The opinions and assertions contained herein are the private view of the authors and not to be construed as official, or as reflecting the view of the US Air Force Medical Service or the US Air Force at large.
1. Yeung LT, King SM, Roberts EA. Mother-to-infant transmission of hepatitis C virus. Hepatology. 2001;34:223-229.
2. European Paediatric Hepatitis C Virus Network. Three broad modalities in the natural history of vertically acquired hepatitis C virus infection. Clin Infect Dis. 2005;41:45-51.
3. European Paediatric Hepatitis C Virus Network. Effects of mode of delivery and infant feeding on the risk of mother-to-child transmission of hepatitis C virus. BJOG. 2001;108:371-377.
4. Paccagnini S, Principi N, Massironi E, et al. Perinatal transmission and manifestation of hepatitis C virus infection in a high risk population. Pediatr Infect Dis J. 1995;14:195-199.
5. Mast EE, Hwang LY, Seto DS, et al. Risk factors for perinatal transmission of hepatitis C virus (HCV) and the natural history of HCV infection acquired in infancy. J Infect Dis. 2005;192:1880-1889.
6. England K, Pembrey L, Tovo P, et al. European Paediatric Hepatitis C Virus Network. Excluding hepatitis C virus (HCV) infection by serology in young infants of HCV-infected mothers. Acta Paediatr. 2005;94:444-450.
7. Ketzinel-Gilad M, Colodner SL, Hadary R, et al. Transient transmission of hepatitis C virus from mothers to newborns. Eur J Clin Microbiol Infect Dis. 2000;19:267-274.
8. Management of Hepatitis C: 2002. National Institutes of Health Consensus Conference Statement, June 10-12, 2002. Available at: http://consensus.nih.gov/2002/2002HepatitisC2002116html.htm. Accessed August 23, 2009.
9. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 86. Viral hepatitis in pregnancy. Obstet Gynecol. 2007;110:941-956.
10. Dienstag JL, McHutchison JG. American Gastroenterological Association medical position statement on the management of hepatitis C. Gastroenterology. 2006;130:225-230.Available at: www.gastrojournal.org/article/PIIS0016508505022717/fulltext. Accessed on August 23, 2009.
FOR STARTERS, don’t be overly concerned with the mode of delivery; it doesn’t influence the rate of transmission of hepatitis C virus (HCV), except in women who are also infected with human immunodeficiency virus (HIV) (strength of recommendation [SOR]: B, consistent retrospective cohort studies).
Avoid internal fetal monitoring and prolonged rupture of membranes (SOR: B, single retrospective cohort study).
Advise patients that it’s OK to breastfeed. Breastfeeding doesn’t affect transmission (SOR: B, consistent prospective cohort studies).
Check HCV RNA and serum anti-HCV on 2 occasions between 2 and 6 months of age and 18 and 24 months of age (SOR: B, consistent prospective cohort studies).
Evidence summary
Perinatal transmission of HCV is rare. It occurs only when serum HCV RNA is detectable; transmission rates may be related to higher levels (>106 copies/mL).1 HCV is transmitted to 2% of infants of anti-HCV seropositive women and 4% to 7% of infants born to mothers who are HCV RNA-positive at delivery.1
Spontaneous clearance of the virus occurs in approximately 20% of infants. Most remain asymptomatic if HCV persists, but have mild elevation of liver function tests.2
Routine screening for HCV in mothers is not recommended, but pregnant women at high risk for HCV infection should be screened for anti-HCV.
Route of delivery: Only a concern for HIV-positive mothers
The mode of delivery doesn’t influence the rate of HCV transmission, except in mothers with HIV. Retrospective analysis of 503 HCV-positive mothers coinfected with HIV showed a decreased risk of transmission during cesarean delivery (odds ratio [OR]=0.36; P=.01; number needed to treat [NNT]=10).3
One study suggested an increased rate of vertical HCV transmission during vaginal delivery compared with cesarean delivery (32% vs 6%; P<.05). The study didn’t account for the percent of mothers coinfected with HIV, however.4
A meta-analysis of 11 studies showed similar rates of transmission for vaginal and cesarean delivery: adjusted rates were 4.3% and 3%, respectively.1
Internal monitoring is an issue
Avoid internal fetal monitoring to minimize HCV transmission, based on a single retrospective cohort of 244 infants born to HCV-positive mothers (relative risk [RR]= 7.7; 95% confidence interval [CI], 1.9-31.6; number needed to harm [NNH]=6).7 The same study showed an increased risk with membrane rupture longer than 6 hours (RR=9.9; 95% CI, 1.2-81; NNH=13).5
Breastfeeding doesn’t significantly affect HCV transmission. Transmission rates for breastfed and nonbreastfed infants are 3.7% and 3.9%, respectively.1
Defer postpartum lab testing
Because about 20% of infants exposed to HCV clear the virus spontaneously, and maternal antibodies can confound laboratory results, deferring postpartum diagnostic testing is appropriate. A study of 1104 children in whom vertical transmission didn’t occur after exposure to HCV showed that 95% of the children were anti-HCV antibody negative by 12 months age.6 A prospective study of 23 infants documented spontaneous clearance of HCV RNA by 6 months in all patients.7
Recommendations
The National Institutes of Health 2002 Consensus Statement recommends:8
- avoiding fetal scalp electrodes and prolonged rupture of membranes
- serum testing for HCV RNA at 2 months and 6 months of age
- anti-HCV antibody testing after 15 months of age.
The American College of Obstetricians and Gynecologists supports breastfeeding, recommends against routine HCV screening, and recommends that cesarean delivery be reserved for obstetric indications.9
The American Association for the Study of Liver Diseases recommends serum testing and liver biopsy on the same schedule as adult patients and endorses considering treatment after 3 years of age.6
The US Food and Drug Administration has approved treatment after 3 years of age for children with detectable HCV RNA levels higher than 50 IU/mL and who have had a liver biopsy with portal or bridging fibrosis and at least moderate inflammation and necrosis.
The American Gastroenterological Association recommends considering treatment with PEG-interferon and ribavirin after 3 years of age.10
Acknowledgements
The opinions and assertions contained herein are the private view of the authors and not to be construed as official, or as reflecting the view of the US Air Force Medical Service or the US Air Force at large.
FOR STARTERS, don’t be overly concerned with the mode of delivery; it doesn’t influence the rate of transmission of hepatitis C virus (HCV), except in women who are also infected with human immunodeficiency virus (HIV) (strength of recommendation [SOR]: B, consistent retrospective cohort studies).
Avoid internal fetal monitoring and prolonged rupture of membranes (SOR: B, single retrospective cohort study).
Advise patients that it’s OK to breastfeed. Breastfeeding doesn’t affect transmission (SOR: B, consistent prospective cohort studies).
Check HCV RNA and serum anti-HCV on 2 occasions between 2 and 6 months of age and 18 and 24 months of age (SOR: B, consistent prospective cohort studies).
Evidence summary
Perinatal transmission of HCV is rare. It occurs only when serum HCV RNA is detectable; transmission rates may be related to higher levels (>106 copies/mL).1 HCV is transmitted to 2% of infants of anti-HCV seropositive women and 4% to 7% of infants born to mothers who are HCV RNA-positive at delivery.1
Spontaneous clearance of the virus occurs in approximately 20% of infants. Most remain asymptomatic if HCV persists, but have mild elevation of liver function tests.2
Routine screening for HCV in mothers is not recommended, but pregnant women at high risk for HCV infection should be screened for anti-HCV.
Route of delivery: Only a concern for HIV-positive mothers
The mode of delivery doesn’t influence the rate of HCV transmission, except in mothers with HIV. Retrospective analysis of 503 HCV-positive mothers coinfected with HIV showed a decreased risk of transmission during cesarean delivery (odds ratio [OR]=0.36; P=.01; number needed to treat [NNT]=10).3
One study suggested an increased rate of vertical HCV transmission during vaginal delivery compared with cesarean delivery (32% vs 6%; P<.05). The study didn’t account for the percent of mothers coinfected with HIV, however.4
A meta-analysis of 11 studies showed similar rates of transmission for vaginal and cesarean delivery: adjusted rates were 4.3% and 3%, respectively.1
Internal monitoring is an issue
Avoid internal fetal monitoring to minimize HCV transmission, based on a single retrospective cohort of 244 infants born to HCV-positive mothers (relative risk [RR]= 7.7; 95% confidence interval [CI], 1.9-31.6; number needed to harm [NNH]=6).7 The same study showed an increased risk with membrane rupture longer than 6 hours (RR=9.9; 95% CI, 1.2-81; NNH=13).5
Breastfeeding doesn’t significantly affect HCV transmission. Transmission rates for breastfed and nonbreastfed infants are 3.7% and 3.9%, respectively.1
Defer postpartum lab testing
Because about 20% of infants exposed to HCV clear the virus spontaneously, and maternal antibodies can confound laboratory results, deferring postpartum diagnostic testing is appropriate. A study of 1104 children in whom vertical transmission didn’t occur after exposure to HCV showed that 95% of the children were anti-HCV antibody negative by 12 months age.6 A prospective study of 23 infants documented spontaneous clearance of HCV RNA by 6 months in all patients.7
Recommendations
The National Institutes of Health 2002 Consensus Statement recommends:8
- avoiding fetal scalp electrodes and prolonged rupture of membranes
- serum testing for HCV RNA at 2 months and 6 months of age
- anti-HCV antibody testing after 15 months of age.
The American College of Obstetricians and Gynecologists supports breastfeeding, recommends against routine HCV screening, and recommends that cesarean delivery be reserved for obstetric indications.9
The American Association for the Study of Liver Diseases recommends serum testing and liver biopsy on the same schedule as adult patients and endorses considering treatment after 3 years of age.6
The US Food and Drug Administration has approved treatment after 3 years of age for children with detectable HCV RNA levels higher than 50 IU/mL and who have had a liver biopsy with portal or bridging fibrosis and at least moderate inflammation and necrosis.
The American Gastroenterological Association recommends considering treatment with PEG-interferon and ribavirin after 3 years of age.10
Acknowledgements
The opinions and assertions contained herein are the private view of the authors and not to be construed as official, or as reflecting the view of the US Air Force Medical Service or the US Air Force at large.
1. Yeung LT, King SM, Roberts EA. Mother-to-infant transmission of hepatitis C virus. Hepatology. 2001;34:223-229.
2. European Paediatric Hepatitis C Virus Network. Three broad modalities in the natural history of vertically acquired hepatitis C virus infection. Clin Infect Dis. 2005;41:45-51.
3. European Paediatric Hepatitis C Virus Network. Effects of mode of delivery and infant feeding on the risk of mother-to-child transmission of hepatitis C virus. BJOG. 2001;108:371-377.
4. Paccagnini S, Principi N, Massironi E, et al. Perinatal transmission and manifestation of hepatitis C virus infection in a high risk population. Pediatr Infect Dis J. 1995;14:195-199.
5. Mast EE, Hwang LY, Seto DS, et al. Risk factors for perinatal transmission of hepatitis C virus (HCV) and the natural history of HCV infection acquired in infancy. J Infect Dis. 2005;192:1880-1889.
6. England K, Pembrey L, Tovo P, et al. European Paediatric Hepatitis C Virus Network. Excluding hepatitis C virus (HCV) infection by serology in young infants of HCV-infected mothers. Acta Paediatr. 2005;94:444-450.
7. Ketzinel-Gilad M, Colodner SL, Hadary R, et al. Transient transmission of hepatitis C virus from mothers to newborns. Eur J Clin Microbiol Infect Dis. 2000;19:267-274.
8. Management of Hepatitis C: 2002. National Institutes of Health Consensus Conference Statement, June 10-12, 2002. Available at: http://consensus.nih.gov/2002/2002HepatitisC2002116html.htm. Accessed August 23, 2009.
9. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 86. Viral hepatitis in pregnancy. Obstet Gynecol. 2007;110:941-956.
10. Dienstag JL, McHutchison JG. American Gastroenterological Association medical position statement on the management of hepatitis C. Gastroenterology. 2006;130:225-230.Available at: www.gastrojournal.org/article/PIIS0016508505022717/fulltext. Accessed on August 23, 2009.
1. Yeung LT, King SM, Roberts EA. Mother-to-infant transmission of hepatitis C virus. Hepatology. 2001;34:223-229.
2. European Paediatric Hepatitis C Virus Network. Three broad modalities in the natural history of vertically acquired hepatitis C virus infection. Clin Infect Dis. 2005;41:45-51.
3. European Paediatric Hepatitis C Virus Network. Effects of mode of delivery and infant feeding on the risk of mother-to-child transmission of hepatitis C virus. BJOG. 2001;108:371-377.
4. Paccagnini S, Principi N, Massironi E, et al. Perinatal transmission and manifestation of hepatitis C virus infection in a high risk population. Pediatr Infect Dis J. 1995;14:195-199.
5. Mast EE, Hwang LY, Seto DS, et al. Risk factors for perinatal transmission of hepatitis C virus (HCV) and the natural history of HCV infection acquired in infancy. J Infect Dis. 2005;192:1880-1889.
6. England K, Pembrey L, Tovo P, et al. European Paediatric Hepatitis C Virus Network. Excluding hepatitis C virus (HCV) infection by serology in young infants of HCV-infected mothers. Acta Paediatr. 2005;94:444-450.
7. Ketzinel-Gilad M, Colodner SL, Hadary R, et al. Transient transmission of hepatitis C virus from mothers to newborns. Eur J Clin Microbiol Infect Dis. 2000;19:267-274.
8. Management of Hepatitis C: 2002. National Institutes of Health Consensus Conference Statement, June 10-12, 2002. Available at: http://consensus.nih.gov/2002/2002HepatitisC2002116html.htm. Accessed August 23, 2009.
9. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 86. Viral hepatitis in pregnancy. Obstet Gynecol. 2007;110:941-956.
10. Dienstag JL, McHutchison JG. American Gastroenterological Association medical position statement on the management of hepatitis C. Gastroenterology. 2006;130:225-230.Available at: www.gastrojournal.org/article/PIIS0016508505022717/fulltext. Accessed on August 23, 2009.
Evidence-based answers from the Family Physicians Inquiries Network