User login
› Consider recommending Iyengar yoga or Viniyoga for the treatment of chronic low back pain in patients who express an interest in this modality. B
› Consider recommending yoga for the treatment of depression and anxiety symptoms in patients who are interested in exploring this approach. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Yoga is practiced by 15.8 million Americans,1 and is often recommended as therapy for a variety of medical conditions. However, the scientific literature on yoga is limited in scope and quality. This article presents good evidence for yoga as treatment for chronic back pain, depression, and anxiety, and fair evidence for treating asthma, symptoms of menopause, hypertension, and mobility issues in the elderly.
Yoga’s rising popularity as therapy
Yoga is a system of movement and breathing exercises meant to foster mind-body connection. Its roots are in ancient Indian practices codified by the writer Patanjali in the first or second century BCE.2
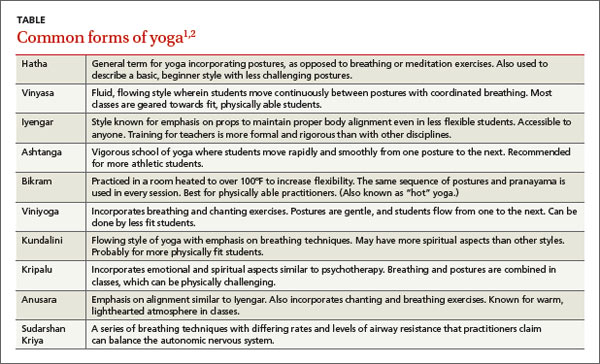
The practice of yoga was introduced to the Western world by a series of popular gurus from the 1930s to 1970s and consists primarily of asanas, or postures, and breathing exercises known as pranayama. Since then, yoga has been further subdivided into different schools and brands (TABLE1,2), some of which are extremely taxing and vigorous and should be performed only by fit and healthy individuals, while others are gentle and accessible to anyone. Yoga has steadily gained in popularity, and nearly half of those who practice it say they do so to improve their health.1
How useful is the research on yoga therapy?
Yoga has been a subject of Western scientific inquiry for more than 100 years. It has been deemed effective for treating conditions from hypertension to epilepsy,3 but many claims are poorly substantiated. Most studies report on a single case or series. The few investigational studies are mainly very small, of short duration, and lacking in appropriate blinding.
Moreover, yoga practices used in the interventions vary markedly, making comparison of results difficult. Interventions range from a single 1-hour session to weekly sessions over several months to inpatient treatment that includes many lifestyle modifications. Some studies required subjects to practice physically demanding asanas, while others focused on pranayama or practices similar to guided relaxation.
Helping patients navigate the yoga domain
The variability in practices described as “yoga” and the lack of a standardized credentialing for yoga teachers make it challenging for patients to find a source suitable for their particular needs. Although choosing a style of yoga appropriate to one’s fitness level and finding an experienced instructor are not straightforward undertakings, physicians familiar with the styles, risks, and benefits of yoga can help direct patients seeking this type of therapy.
The Yoga Alliance is the best-known credentialing organization; it offers a 200-hour and 500-hour curriculum covering anatomy, yoga philosophy, and hands-on practice, and grants credit for years of experience in teaching.4 However, the Yoga Alliance began its current credentialing project just 7 years ago, and it is far from ubiquitous in the industry. Some types of yoga, such as Iyengar and Bikram, have their own certification systems that teachers may preferentially use.
Therapy credentialing. The International Association of Yoga Therapists (IAYT) was founded in 1989 to define yoga therapy and to organize practitioners attempting to use yoga to treat health conditions. As of July 2012, it had published suggested curricula for yoga therapists requiring 800 hours of study.4 Clearly, it will take time for these standards to become disseminated through the industry. At this point, IAYT membership does not require any certification or credentials.4 Moreover, the broad and decentralized nature of yoga practice means that any type of teacher and therapist credentialing or licensure will be controversial and not universally accepted among practitioners. Because of the relative newness of teacher and therapist licensing programs, many experienced and well-respected instructors may lack formal credentials or certifications.
Patients should do extensive research before choosing a type of yoga and an instructor (see “Finding a yoga instructor”). They should choose a type of yoga suited to their fitness level and general health (TABLE1,2) to avoid serious injury, which can include fractures, neuralgia, and arterial dissection.2
Two organizations may be useful in helping your patient locate a yoga instructor or therapist in your area. The International Association of Yoga Therapists (IAYT) and the Yoga Alliance both offer online search tools: http://iayt.site-ym.com/search/custom.asp?id=1156 IA (IAYT) and https://www.yogaalliance.org/yogaregistry (Yoga Alliance). Important areas of questioning for potential therapists include length of teaching experience, training programs completed, and the amount of experience the instructor or therapist has had in working with individuals with a specific medical condition. It may be prudent in certain situations to refer patients to a physical therapist for evaluation before beginning yoga study.
The evidence for yoga’s benefits for specific conditions
The promotion of yoga as medical treatment is rife with dubious claims, but there is solid evidence for its benefits in some common conditions. The evidence summaries that follow reflect searches on Medline, via PubMed, and the Cochrane Database using the phrase “yoga review.”
Back pain
Often a stress-related musculoskeletal problem, back pain seems an appropriate indication for treatment with yoga, and there is a large body of literature on the subject.5 In a systematic review, Chou and Huffman6 found only 3 studies meeting inclusion criteria on yoga’s effectiveness for subacute or chronic low back pain. One large study found 6 weeks of Viniyoga was superior to conventional exercise programs and a self-care booklet in reducing pain and “bothersomeness” scores, as well as reducing the need for analgesic medication.7 Physician visits for back pain were not reduced in the treatment group, however.7 Also included in the systematic review were 2 smaller studies of Iyengar yoga on low back pain; results did not rise to statistical significance.6
A review by Posadzki and Ernst8 included 4 randomized controlled trials (RCTs) not included in Chou and Huffman, although only one of these had >50 subjects. Yoga practices for the treatment groups were mostly Iyengar and Viniyoga and lasted for 12 to 24 weeks, although one study used a 7-day intensive inpatient treatment program. Yoga practitioners had lower pain scores and lower Roland Morris Disability scores.8 A 2004 Clinical Inquiry in The Journal of Family Practice found limited evidence to suggest yoga may speed healing for patients with chronic back pain.9
Most recently, Cramer et al10 found 12 studies meeting inclusion criteria that reported on Viniyoga, Iyengar, and Hatha yoga interventions. Ten of these studies were included in the meta-analysis, which strongly favored yoga over control interventions for reducing pain and disability scores.10
Depression and anxiety
Yoga therapy for depression and anxiety has been commonly studied, given that aspects of mindfulness and relaxation are thought to be important parts of treatment. Moreover, patients uncomfortable with pharmacologic therapy for their disorders may be amenable to yoga treatment. In a recent Clinical Inquiry, Skowronek et al11 found evidence (strength of recommendation [SOR] B) for yoga to treat depression and anxiety symptoms based on 3 recently published review articles that commented on a total of 23 RCTs.
A handful of additional review papers on this subject have selected slightly different groups of studies to include in their analyses, but all have found generally positive results.12-14 Inclusion criteria varied: one review omitted breathing-only modalities such as Sudarshan Kriya yoga, while another included them.12,14 One omitted Mindfulness-Based Stress Reduction (MBSR), which is a program developed in the United States based on several Eastern and Western methodologies including yoga.12 MBSR already has a large body of literature supporting its use for anxiety and depression.12
One of these reviews,12 which involved a meta-analysis of 9 studies regarding depression, also included a meta-analysis of 5 studies on yoga for anxiety. Pooled results for depression showed significant benefit for yoga over usual care, and smaller but still significant benefit for yoga over aerobic exercise or other relaxation techniques. For anxiety, pooled analysis showed yoga to be equal to usual care but superior to other relaxation modalities.12 As with earlier reviews, study groups were heterogeneous and included young and older adults, caregivers for dementia patients, and those receiving inpatient treatment for alcohol dependency; symptoms of depression ranged from mild to severe.12
In a review focusing on anxiety disorders, Kirkwood et al15 located 8 trials, 6 of which were randomized. Many of these were published in the 1970s and 80s. The yoga interventions varied and included weekly Kundalini sessions, pranayama techniques, and savasana (a pose in which practitioners lie supine while focusing on breathing and muscle relaxation). These practices were compared with anxiolytic medication, progressive muscular relaxation, placebo capsule, and no treatment. All found a statistically significant reduction in anxiety indices in the yoga treatment groups, and the authors noted that the positive effects of yoga for those suffering from obsessive-compulsive disorders are particularly well documented.15 More recently, Li and Goldsmith16 reviewed 6 interventional studies that included some trials without randomization, blinding, or a control group. Subjects of the studies included cancer patients, postmenopausal women, pregnant women, and firefighters. Six of 9 trials showed improvement in externally validated anxiety indices such as the State-Trait Anxiety Inventory or Perceived Stress Scale.
Asthma
With its focus on awareness of breath and the mechanics of breathing, yoga would seem a natural adjunct to conventional asthma therapy. One systematic review found 4 trials (3 RCTs) that showed statistically significant improvements in spirometric measurements in patients with asthma who practiced yoga techniques.17 An additional 3 RCTs showed no improvements with yoga over conventional treatments.17 Overall, the reviewers noted that study quality was poor, although they said several studies were appropriately designed. Again, the interventions described as “yoga” varied considerably, from Iyengar-type classes to meditation-focused techniques to pranayama exercises. Follow-up ranged from 6 weeks to 6 months.17
A more recent and thorough review found 14 RCTs using yoga to treat asthma symptoms.18 The investigators performed pooled analysis despite significant heterogeneity in the studies. The analysis showed some improvement in the yoga group compared with usual therapy, but no difference in comparison with sham yoga or non-yoga breathing exercises.18
Symptoms of menopause
Studies have focused on alternative or adjunctive therapies for menopause symptoms, primarily hot flashes, since hormone replacement therapy and other conventional medical therapies have been found to have a high incidence of adverse effects. However, evidence that yoga can reduce hot flashes is sparse.
A Cochrane review examined the effects of exercise on hot flashes and found 2 RCTs using yoga as a treatment modality. Neither one found statistically significant differences between the yoga groups and conventional exercise groups.19 The authors concluded there was insufficient evidence to show yoga was more effective than other forms of exercise on vasomotor symptoms of menopause. However, a large RCT included in the Cochrane review did show lower stress levels and decreased overall symptoms in the yoga arm.20
The yoga intervention in this study consisted of pranayama, sun salutation (a repetitive sequence of 12 yoga postures), and cyclic meditation.20 Lee et al21 reviewed the 2 studies used in the Cochrane paper as well as 5 other studies. Two were RCTs showing that yoga intervention was not superior to a no-treatment control. Four studies showed favorable results for yoga interventions; however, one was a nonrandomized controlled trial and 3 lacked control groups.
Cramer et al22 attempted pooled analysis of 5 studies, including those in the Cochrane paper, with similar results: Yoga interventions were not efficacious for somatic, vasomotor, or urogenital symptoms of menopause. Yoga was somewhat efficacious for psychological symptoms associated with menopause.22 More recently, an RCT (N=249) found that yoga reduces vasomotor symptoms no more frequently than non-yoga exercise.23
Hypertension
Yoga is often said to reduce blood pressure (BP), which would make sense given the emphasis put on relaxation by many schools of yoga. In the past 2 years, 3 review articles have been published, as well as 2 relevant RCTs not included in those reviews.
Hagins et al24 found 17 RCTs using yoga to treat adults with hypertension and prehypertension. These included both blinded and unblinded studies, and yoga interventions were compared with usual treatment, education, or non-yoga exercise. The authors included only studies of asanas intervention, and excluded interventions using only breathing or relaxation techniques.24 In meta-analysis, pooled data showed the yoga treatment decreased both diastolic BP (DBP) and systolic BP (SBP) by 3 to 4 mm Hg compared with usual treatment, but not when compared with other exercise therapies.24 Reviewers concluded that yoga was likely as effective for lowering BP as other types of physical activity.24
In a review without meta-analysis, Posadzki et al25 also found 17 blinded RCTs using yoga to treat hypertension or prehypertension in adults. Eleven of the 17 studies favored yoga, with 8 showing a decrease in SBP and 5 in DBP.25 All but 2 studies were found to be of poor quality, especially with regard to blinding.25 The authors noted that studies using subjects with prehypertension or hypertension with comorbidities were more likely to show significant results, speculating that yoga may be more effective for these populations.25
In an ambitious review article on yoga as treatment for a variety of risk factors for cardiovascular disease, Cramer et al26 located 28 RCTs that addressed effects of yoga on BP. Seven of the studies in the Posadzki review25 were included. Meta-analysis showed a statistically significant decrease in SBP of 5.85 mm Hg and in DBP of 4.12 mm Hg.26 Although wide in scope, this meta-analysis included many studies of healthy patients without hypertension who could conceivably have differing neuroendocrine responses to yoga practice.
In a pilot RCT, Cohen et al27 found a significant decrease in BP among subjects randomized into Iyengar yoga classes for 24 weeks compared with a control group educated about lifestyle modification. A larger study with 102 subjects is currently underway.28 These studies were unique in that no subjects were currently being treated with antihypertensive medications27,28; most other trials on this subject enrolled participants on antihypertensive medications if their regimens had been stable for some time.
In an RCT published recently by Hagins et al,29 68 subjects with pre- or stage I hypertension were randomized into Ashtanga yoga classes or non-aerobic exercise classes formulated to burn equivalent METs. After 12 weeks of treatment, the yoga subjects’ BP had significantly decreased from starting values, but was not improved compared with the exercise subjects.29 This further supports the assertion that yoga is equivalent to other forms of physical activity in decreasing BP among hypertensive subjects.
Balance and stability in the elderly
With its emphasis on strength, balance, and body awareness, yoga would seem a helpful intervention for older patients at risk of injury from falls. Unfortunately this area of research lacks significant numbers of controlled trails. In a Cochrane review of exercise interventions for improving balance in the elderly, the reviewers were unable find any studies specifically using yoga that met their criteria.30 Jeter et al31 attempted a review more recently, and found 15 studies meeting inclusion criteria, 5 of which were RCTs. Overall, however, the poor quality of the studies and variation in both the type of yoga used as intervention and measurements of balance precluded pooled analysis, although some studies did have positive results.
A small but well-designed pilot RCT was recently published showing that an Iyengar yoga intervention significantly improved timed one-leg balancing among community dwelling older adults.32 However, this study did not show a significant difference in a standardized fall risk survey after the intervention.32
Cautioning against yoga in this context are several articles chronicling increased risks of some yoga exercises, especially for those with osteoporosis or other risks for fractures.33 At this point, the well-documented risks of yoga practice in this group probably outweigh the unsubstantiated rewards.
CORRESPONDENCE
Genevieve Verrastro, MD, MAHEC Family Health Center at Biltmore, 123 Hendersonville Road, Asheville, NC 28803; genevieve.verrastro@gmail.com
1. Yoga Journal. Yoga in America study 2012 [press release]. Santa Cruz, CA: Santa Cruz Bay Publishing; 2008. Available at: http://www.yogajournal.com/press/yoga_in_america. Accessed August 19, 2014.
2. Broad WJ. The Science of Yoga: The Risks and Rewards. New York, New York: Simon & Schuster; 2012.
3. Lamb T. Health Benefits of Yoga. International Association of Yoga Therapists Web site. Available at: http://www.iayt.org/?page=HealthBenefitsofYoga. Accessed August 21, 2014.
4. Yoga Alliance. 200-hour standards for yoga teacher trainings. Yoga Alliance Web site. Available at: http://yogaalliance.org/content/200-hour-standards. Accessed August 19, 2014.
5. Wren AA, Wright MA, Carson JW, et al. Yoga for persistent pain: New findings and directions for an ancient practice. Pain. 2011;152:477-480.
6. Chou R, Huffman LH; American Pain Society; American College of Physicians. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med. 2007;147:492-504.
7. Sherman KJ, Cherkin DC, Erro J, et al. Comparing yoga, exercise, and a self-care book for chronic low back pain: a randomized, controlled trial. Ann Intern Med. 2005;143:849-856.
8. Posadzki P, Ernst E. Yoga for low back pain: a systematic review of randomized clinical trials. Clin Rheumatol. 2011;30:1257-1262.
9. Graves N, Krepcho M, Mayo HG, et al. Does yoga speed healing for patients with low back pain? J Fam Pract. 2004;53:661-662.
10. Cramer H, Lauche R, Haller H, et al. A systematic review and meta-analysis of yoga for low back pain. Clin J Pain. 2013;29:450-460.
11. Skowronek IB, Mounsey A, Handler L. Can yoga reduce symptoms of anxiety and depression? J Fam Pract. 2013;63:398-399,407.
12. Cramer H, Lauche R, Langhorst J, et al. Yoga for depression: a systematic review and meta-analysis. Depress Anxiety. 2013;30: 1068-1083.
13. D’Silva S, Poscablo C, Habousha R, et al. Mind-body medicine therapies for a range of depression severity: a systematic review. Psychosomatics. 2012;53:407-423.
14. Balasubramaniam M, Telles S, Doraiswamy PM. Yoga on our minds: a systematic review of yoga for neuropsychiatric disorders. Front Psychiatry. 2013;3:117.
15. Kirkwood G, Rampes H, Tuffrey V, et al. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39: 884-891.
16. Li AW, Goldsmith CA. The effects of yoga on anxiety and stress. Altern Med Rev. 2012;17:21-35.
17. Posadzki P, Ernst E. Yoga for asthma? A systematic review of randomized clinical trials. J Asthma. 2011;48:632-639.
18. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol. 2014;112:503-510.e5.
19. Daley A, Stokes-Lampard H, Macarthur C. Exercise for vasomotor menopausal symptoms. Cochrane Database Syst Rev. 2011;(5):CD006108.
20. Chattha R, Nagarathna R, Padmalatha V, et al. Effect of yoga on cognitive functions in climacteric syndrome: a randomised control study. BJOG. 2008;115:991-1000.
21. Lee MS, Kim JI, Ha JY, et al. Yoga for menopausal symptoms: a systematic review. Menopause. 2009;16:602-608.
22. Cramer H, Lauche R, Langhorst J, et al. Effectiveness of yoga for menopausal symptoms: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2012;2012:863905.
23. Newton KM, Reed SD, Guthrie KA, et al. Efficacy of yoga for vasomotor symptoms: a randomized controlled trial. Menopause. 2014;21:339-346.
24. Hagins M, States R, Selfe T, et al. Effectiveness of yoga for hypertension: systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:649836.
25. Posadzki P, Cramer H, Kuzdzal A, et al. Yoga for hypertension: a systematic review of randomized clinical trials. Complement Ther Med. 2014;22:511-522.
26. Cramer H, Lauche R, Haller H, et al. Effects of yoga on cardiovascular disease risk factors: a systematic review and meta-analysis. Int J Cardiol. 2014;173:170-183.
27. Cohen DL, Bloedon LT, Rothman RL, et al. Iyengar yoga versus enhanced usual care on blood pressure in patients with prehypertension to stage I hypertension: a randomized controlled trial. Evid Based Complement Alternat Med. 2011;2011:546428.
28. Cohen DL, Bowler A, Fisher SA, et al. Lifestyle Modification in Blood Pressure Study II (LIMBS): study protocol of a randomized controlled trial assessing the efficacy of a 24 week structured yoga program versus lifestyle modification on blood pressure reduction. Contemp Clin Trials. 2013;36:32-40.
29. Hagins M, Rundle A, Consedine N, et al. A randomized controlled trial comparing the effects of yoga with an active control on ambulatory blood pressure in individuals with pre- and stage 1 hypertension. J Clin Hypertens (Greenwich). 2014;16:54-62.
30. Howe TE, Rochester L, Neil F, et al. Exercise for improving balance in older people. Cochrane Database Syst Rev. 2011;(11):CD004963.
31. Jeter PE, Nkodo AF, Moonaz SH, et al. A systematic review of yoga for balance in a healthy population. J Altern Complement Med. 2014;20:221-232.
32. Tiedemann A, O’Rourke S, Sesto R, et al. A 12-week Iyengar yoga program improved balance and mobility in older community-dwelling people: a pilot randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2013;68:1068-1075.
33. Sinaki M. Yoga spinal flexion positions and vertebral compression fracture in osteopenia or osteoporosis of spine: case series. Pain Pract. 2013;13:68-75.
› Consider recommending Iyengar yoga or Viniyoga for the treatment of chronic low back pain in patients who express an interest in this modality. B
› Consider recommending yoga for the treatment of depression and anxiety symptoms in patients who are interested in exploring this approach. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Yoga is practiced by 15.8 million Americans,1 and is often recommended as therapy for a variety of medical conditions. However, the scientific literature on yoga is limited in scope and quality. This article presents good evidence for yoga as treatment for chronic back pain, depression, and anxiety, and fair evidence for treating asthma, symptoms of menopause, hypertension, and mobility issues in the elderly.
Yoga’s rising popularity as therapy
Yoga is a system of movement and breathing exercises meant to foster mind-body connection. Its roots are in ancient Indian practices codified by the writer Patanjali in the first or second century BCE.2
The practice of yoga was introduced to the Western world by a series of popular gurus from the 1930s to 1970s and consists primarily of asanas, or postures, and breathing exercises known as pranayama. Since then, yoga has been further subdivided into different schools and brands (TABLE1,2), some of which are extremely taxing and vigorous and should be performed only by fit and healthy individuals, while others are gentle and accessible to anyone. Yoga has steadily gained in popularity, and nearly half of those who practice it say they do so to improve their health.1
How useful is the research on yoga therapy?
Yoga has been a subject of Western scientific inquiry for more than 100 years. It has been deemed effective for treating conditions from hypertension to epilepsy,3 but many claims are poorly substantiated. Most studies report on a single case or series. The few investigational studies are mainly very small, of short duration, and lacking in appropriate blinding.
Moreover, yoga practices used in the interventions vary markedly, making comparison of results difficult. Interventions range from a single 1-hour session to weekly sessions over several months to inpatient treatment that includes many lifestyle modifications. Some studies required subjects to practice physically demanding asanas, while others focused on pranayama or practices similar to guided relaxation.
Helping patients navigate the yoga domain
The variability in practices described as “yoga” and the lack of a standardized credentialing for yoga teachers make it challenging for patients to find a source suitable for their particular needs. Although choosing a style of yoga appropriate to one’s fitness level and finding an experienced instructor are not straightforward undertakings, physicians familiar with the styles, risks, and benefits of yoga can help direct patients seeking this type of therapy.
The Yoga Alliance is the best-known credentialing organization; it offers a 200-hour and 500-hour curriculum covering anatomy, yoga philosophy, and hands-on practice, and grants credit for years of experience in teaching.4 However, the Yoga Alliance began its current credentialing project just 7 years ago, and it is far from ubiquitous in the industry. Some types of yoga, such as Iyengar and Bikram, have their own certification systems that teachers may preferentially use.
Therapy credentialing. The International Association of Yoga Therapists (IAYT) was founded in 1989 to define yoga therapy and to organize practitioners attempting to use yoga to treat health conditions. As of July 2012, it had published suggested curricula for yoga therapists requiring 800 hours of study.4 Clearly, it will take time for these standards to become disseminated through the industry. At this point, IAYT membership does not require any certification or credentials.4 Moreover, the broad and decentralized nature of yoga practice means that any type of teacher and therapist credentialing or licensure will be controversial and not universally accepted among practitioners. Because of the relative newness of teacher and therapist licensing programs, many experienced and well-respected instructors may lack formal credentials or certifications.
Patients should do extensive research before choosing a type of yoga and an instructor (see “Finding a yoga instructor”). They should choose a type of yoga suited to their fitness level and general health (TABLE1,2) to avoid serious injury, which can include fractures, neuralgia, and arterial dissection.2
Two organizations may be useful in helping your patient locate a yoga instructor or therapist in your area. The International Association of Yoga Therapists (IAYT) and the Yoga Alliance both offer online search tools: http://iayt.site-ym.com/search/custom.asp?id=1156 IA (IAYT) and https://www.yogaalliance.org/yogaregistry (Yoga Alliance). Important areas of questioning for potential therapists include length of teaching experience, training programs completed, and the amount of experience the instructor or therapist has had in working with individuals with a specific medical condition. It may be prudent in certain situations to refer patients to a physical therapist for evaluation before beginning yoga study.
The evidence for yoga’s benefits for specific conditions
The promotion of yoga as medical treatment is rife with dubious claims, but there is solid evidence for its benefits in some common conditions. The evidence summaries that follow reflect searches on Medline, via PubMed, and the Cochrane Database using the phrase “yoga review.”
Back pain
Often a stress-related musculoskeletal problem, back pain seems an appropriate indication for treatment with yoga, and there is a large body of literature on the subject.5 In a systematic review, Chou and Huffman6 found only 3 studies meeting inclusion criteria on yoga’s effectiveness for subacute or chronic low back pain. One large study found 6 weeks of Viniyoga was superior to conventional exercise programs and a self-care booklet in reducing pain and “bothersomeness” scores, as well as reducing the need for analgesic medication.7 Physician visits for back pain were not reduced in the treatment group, however.7 Also included in the systematic review were 2 smaller studies of Iyengar yoga on low back pain; results did not rise to statistical significance.6
A review by Posadzki and Ernst8 included 4 randomized controlled trials (RCTs) not included in Chou and Huffman, although only one of these had >50 subjects. Yoga practices for the treatment groups were mostly Iyengar and Viniyoga and lasted for 12 to 24 weeks, although one study used a 7-day intensive inpatient treatment program. Yoga practitioners had lower pain scores and lower Roland Morris Disability scores.8 A 2004 Clinical Inquiry in The Journal of Family Practice found limited evidence to suggest yoga may speed healing for patients with chronic back pain.9
Most recently, Cramer et al10 found 12 studies meeting inclusion criteria that reported on Viniyoga, Iyengar, and Hatha yoga interventions. Ten of these studies were included in the meta-analysis, which strongly favored yoga over control interventions for reducing pain and disability scores.10
Depression and anxiety
Yoga therapy for depression and anxiety has been commonly studied, given that aspects of mindfulness and relaxation are thought to be important parts of treatment. Moreover, patients uncomfortable with pharmacologic therapy for their disorders may be amenable to yoga treatment. In a recent Clinical Inquiry, Skowronek et al11 found evidence (strength of recommendation [SOR] B) for yoga to treat depression and anxiety symptoms based on 3 recently published review articles that commented on a total of 23 RCTs.
A handful of additional review papers on this subject have selected slightly different groups of studies to include in their analyses, but all have found generally positive results.12-14 Inclusion criteria varied: one review omitted breathing-only modalities such as Sudarshan Kriya yoga, while another included them.12,14 One omitted Mindfulness-Based Stress Reduction (MBSR), which is a program developed in the United States based on several Eastern and Western methodologies including yoga.12 MBSR already has a large body of literature supporting its use for anxiety and depression.12
One of these reviews,12 which involved a meta-analysis of 9 studies regarding depression, also included a meta-analysis of 5 studies on yoga for anxiety. Pooled results for depression showed significant benefit for yoga over usual care, and smaller but still significant benefit for yoga over aerobic exercise or other relaxation techniques. For anxiety, pooled analysis showed yoga to be equal to usual care but superior to other relaxation modalities.12 As with earlier reviews, study groups were heterogeneous and included young and older adults, caregivers for dementia patients, and those receiving inpatient treatment for alcohol dependency; symptoms of depression ranged from mild to severe.12
In a review focusing on anxiety disorders, Kirkwood et al15 located 8 trials, 6 of which were randomized. Many of these were published in the 1970s and 80s. The yoga interventions varied and included weekly Kundalini sessions, pranayama techniques, and savasana (a pose in which practitioners lie supine while focusing on breathing and muscle relaxation). These practices were compared with anxiolytic medication, progressive muscular relaxation, placebo capsule, and no treatment. All found a statistically significant reduction in anxiety indices in the yoga treatment groups, and the authors noted that the positive effects of yoga for those suffering from obsessive-compulsive disorders are particularly well documented.15 More recently, Li and Goldsmith16 reviewed 6 interventional studies that included some trials without randomization, blinding, or a control group. Subjects of the studies included cancer patients, postmenopausal women, pregnant women, and firefighters. Six of 9 trials showed improvement in externally validated anxiety indices such as the State-Trait Anxiety Inventory or Perceived Stress Scale.
Asthma
With its focus on awareness of breath and the mechanics of breathing, yoga would seem a natural adjunct to conventional asthma therapy. One systematic review found 4 trials (3 RCTs) that showed statistically significant improvements in spirometric measurements in patients with asthma who practiced yoga techniques.17 An additional 3 RCTs showed no improvements with yoga over conventional treatments.17 Overall, the reviewers noted that study quality was poor, although they said several studies were appropriately designed. Again, the interventions described as “yoga” varied considerably, from Iyengar-type classes to meditation-focused techniques to pranayama exercises. Follow-up ranged from 6 weeks to 6 months.17
A more recent and thorough review found 14 RCTs using yoga to treat asthma symptoms.18 The investigators performed pooled analysis despite significant heterogeneity in the studies. The analysis showed some improvement in the yoga group compared with usual therapy, but no difference in comparison with sham yoga or non-yoga breathing exercises.18
Symptoms of menopause
Studies have focused on alternative or adjunctive therapies for menopause symptoms, primarily hot flashes, since hormone replacement therapy and other conventional medical therapies have been found to have a high incidence of adverse effects. However, evidence that yoga can reduce hot flashes is sparse.
A Cochrane review examined the effects of exercise on hot flashes and found 2 RCTs using yoga as a treatment modality. Neither one found statistically significant differences between the yoga groups and conventional exercise groups.19 The authors concluded there was insufficient evidence to show yoga was more effective than other forms of exercise on vasomotor symptoms of menopause. However, a large RCT included in the Cochrane review did show lower stress levels and decreased overall symptoms in the yoga arm.20
The yoga intervention in this study consisted of pranayama, sun salutation (a repetitive sequence of 12 yoga postures), and cyclic meditation.20 Lee et al21 reviewed the 2 studies used in the Cochrane paper as well as 5 other studies. Two were RCTs showing that yoga intervention was not superior to a no-treatment control. Four studies showed favorable results for yoga interventions; however, one was a nonrandomized controlled trial and 3 lacked control groups.
Cramer et al22 attempted pooled analysis of 5 studies, including those in the Cochrane paper, with similar results: Yoga interventions were not efficacious for somatic, vasomotor, or urogenital symptoms of menopause. Yoga was somewhat efficacious for psychological symptoms associated with menopause.22 More recently, an RCT (N=249) found that yoga reduces vasomotor symptoms no more frequently than non-yoga exercise.23
Hypertension
Yoga is often said to reduce blood pressure (BP), which would make sense given the emphasis put on relaxation by many schools of yoga. In the past 2 years, 3 review articles have been published, as well as 2 relevant RCTs not included in those reviews.
Hagins et al24 found 17 RCTs using yoga to treat adults with hypertension and prehypertension. These included both blinded and unblinded studies, and yoga interventions were compared with usual treatment, education, or non-yoga exercise. The authors included only studies of asanas intervention, and excluded interventions using only breathing or relaxation techniques.24 In meta-analysis, pooled data showed the yoga treatment decreased both diastolic BP (DBP) and systolic BP (SBP) by 3 to 4 mm Hg compared with usual treatment, but not when compared with other exercise therapies.24 Reviewers concluded that yoga was likely as effective for lowering BP as other types of physical activity.24
In a review without meta-analysis, Posadzki et al25 also found 17 blinded RCTs using yoga to treat hypertension or prehypertension in adults. Eleven of the 17 studies favored yoga, with 8 showing a decrease in SBP and 5 in DBP.25 All but 2 studies were found to be of poor quality, especially with regard to blinding.25 The authors noted that studies using subjects with prehypertension or hypertension with comorbidities were more likely to show significant results, speculating that yoga may be more effective for these populations.25
In an ambitious review article on yoga as treatment for a variety of risk factors for cardiovascular disease, Cramer et al26 located 28 RCTs that addressed effects of yoga on BP. Seven of the studies in the Posadzki review25 were included. Meta-analysis showed a statistically significant decrease in SBP of 5.85 mm Hg and in DBP of 4.12 mm Hg.26 Although wide in scope, this meta-analysis included many studies of healthy patients without hypertension who could conceivably have differing neuroendocrine responses to yoga practice.
In a pilot RCT, Cohen et al27 found a significant decrease in BP among subjects randomized into Iyengar yoga classes for 24 weeks compared with a control group educated about lifestyle modification. A larger study with 102 subjects is currently underway.28 These studies were unique in that no subjects were currently being treated with antihypertensive medications27,28; most other trials on this subject enrolled participants on antihypertensive medications if their regimens had been stable for some time.
In an RCT published recently by Hagins et al,29 68 subjects with pre- or stage I hypertension were randomized into Ashtanga yoga classes or non-aerobic exercise classes formulated to burn equivalent METs. After 12 weeks of treatment, the yoga subjects’ BP had significantly decreased from starting values, but was not improved compared with the exercise subjects.29 This further supports the assertion that yoga is equivalent to other forms of physical activity in decreasing BP among hypertensive subjects.
Balance and stability in the elderly
With its emphasis on strength, balance, and body awareness, yoga would seem a helpful intervention for older patients at risk of injury from falls. Unfortunately this area of research lacks significant numbers of controlled trails. In a Cochrane review of exercise interventions for improving balance in the elderly, the reviewers were unable find any studies specifically using yoga that met their criteria.30 Jeter et al31 attempted a review more recently, and found 15 studies meeting inclusion criteria, 5 of which were RCTs. Overall, however, the poor quality of the studies and variation in both the type of yoga used as intervention and measurements of balance precluded pooled analysis, although some studies did have positive results.
A small but well-designed pilot RCT was recently published showing that an Iyengar yoga intervention significantly improved timed one-leg balancing among community dwelling older adults.32 However, this study did not show a significant difference in a standardized fall risk survey after the intervention.32
Cautioning against yoga in this context are several articles chronicling increased risks of some yoga exercises, especially for those with osteoporosis or other risks for fractures.33 At this point, the well-documented risks of yoga practice in this group probably outweigh the unsubstantiated rewards.
CORRESPONDENCE
Genevieve Verrastro, MD, MAHEC Family Health Center at Biltmore, 123 Hendersonville Road, Asheville, NC 28803; genevieve.verrastro@gmail.com
› Consider recommending Iyengar yoga or Viniyoga for the treatment of chronic low back pain in patients who express an interest in this modality. B
› Consider recommending yoga for the treatment of depression and anxiety symptoms in patients who are interested in exploring this approach. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Yoga is practiced by 15.8 million Americans,1 and is often recommended as therapy for a variety of medical conditions. However, the scientific literature on yoga is limited in scope and quality. This article presents good evidence for yoga as treatment for chronic back pain, depression, and anxiety, and fair evidence for treating asthma, symptoms of menopause, hypertension, and mobility issues in the elderly.
Yoga’s rising popularity as therapy
Yoga is a system of movement and breathing exercises meant to foster mind-body connection. Its roots are in ancient Indian practices codified by the writer Patanjali in the first or second century BCE.2
The practice of yoga was introduced to the Western world by a series of popular gurus from the 1930s to 1970s and consists primarily of asanas, or postures, and breathing exercises known as pranayama. Since then, yoga has been further subdivided into different schools and brands (TABLE1,2), some of which are extremely taxing and vigorous and should be performed only by fit and healthy individuals, while others are gentle and accessible to anyone. Yoga has steadily gained in popularity, and nearly half of those who practice it say they do so to improve their health.1
How useful is the research on yoga therapy?
Yoga has been a subject of Western scientific inquiry for more than 100 years. It has been deemed effective for treating conditions from hypertension to epilepsy,3 but many claims are poorly substantiated. Most studies report on a single case or series. The few investigational studies are mainly very small, of short duration, and lacking in appropriate blinding.
Moreover, yoga practices used in the interventions vary markedly, making comparison of results difficult. Interventions range from a single 1-hour session to weekly sessions over several months to inpatient treatment that includes many lifestyle modifications. Some studies required subjects to practice physically demanding asanas, while others focused on pranayama or practices similar to guided relaxation.
Helping patients navigate the yoga domain
The variability in practices described as “yoga” and the lack of a standardized credentialing for yoga teachers make it challenging for patients to find a source suitable for their particular needs. Although choosing a style of yoga appropriate to one’s fitness level and finding an experienced instructor are not straightforward undertakings, physicians familiar with the styles, risks, and benefits of yoga can help direct patients seeking this type of therapy.
The Yoga Alliance is the best-known credentialing organization; it offers a 200-hour and 500-hour curriculum covering anatomy, yoga philosophy, and hands-on practice, and grants credit for years of experience in teaching.4 However, the Yoga Alliance began its current credentialing project just 7 years ago, and it is far from ubiquitous in the industry. Some types of yoga, such as Iyengar and Bikram, have their own certification systems that teachers may preferentially use.
Therapy credentialing. The International Association of Yoga Therapists (IAYT) was founded in 1989 to define yoga therapy and to organize practitioners attempting to use yoga to treat health conditions. As of July 2012, it had published suggested curricula for yoga therapists requiring 800 hours of study.4 Clearly, it will take time for these standards to become disseminated through the industry. At this point, IAYT membership does not require any certification or credentials.4 Moreover, the broad and decentralized nature of yoga practice means that any type of teacher and therapist credentialing or licensure will be controversial and not universally accepted among practitioners. Because of the relative newness of teacher and therapist licensing programs, many experienced and well-respected instructors may lack formal credentials or certifications.
Patients should do extensive research before choosing a type of yoga and an instructor (see “Finding a yoga instructor”). They should choose a type of yoga suited to their fitness level and general health (TABLE1,2) to avoid serious injury, which can include fractures, neuralgia, and arterial dissection.2
Two organizations may be useful in helping your patient locate a yoga instructor or therapist in your area. The International Association of Yoga Therapists (IAYT) and the Yoga Alliance both offer online search tools: http://iayt.site-ym.com/search/custom.asp?id=1156 IA (IAYT) and https://www.yogaalliance.org/yogaregistry (Yoga Alliance). Important areas of questioning for potential therapists include length of teaching experience, training programs completed, and the amount of experience the instructor or therapist has had in working with individuals with a specific medical condition. It may be prudent in certain situations to refer patients to a physical therapist for evaluation before beginning yoga study.
The evidence for yoga’s benefits for specific conditions
The promotion of yoga as medical treatment is rife with dubious claims, but there is solid evidence for its benefits in some common conditions. The evidence summaries that follow reflect searches on Medline, via PubMed, and the Cochrane Database using the phrase “yoga review.”
Back pain
Often a stress-related musculoskeletal problem, back pain seems an appropriate indication for treatment with yoga, and there is a large body of literature on the subject.5 In a systematic review, Chou and Huffman6 found only 3 studies meeting inclusion criteria on yoga’s effectiveness for subacute or chronic low back pain. One large study found 6 weeks of Viniyoga was superior to conventional exercise programs and a self-care booklet in reducing pain and “bothersomeness” scores, as well as reducing the need for analgesic medication.7 Physician visits for back pain were not reduced in the treatment group, however.7 Also included in the systematic review were 2 smaller studies of Iyengar yoga on low back pain; results did not rise to statistical significance.6
A review by Posadzki and Ernst8 included 4 randomized controlled trials (RCTs) not included in Chou and Huffman, although only one of these had >50 subjects. Yoga practices for the treatment groups were mostly Iyengar and Viniyoga and lasted for 12 to 24 weeks, although one study used a 7-day intensive inpatient treatment program. Yoga practitioners had lower pain scores and lower Roland Morris Disability scores.8 A 2004 Clinical Inquiry in The Journal of Family Practice found limited evidence to suggest yoga may speed healing for patients with chronic back pain.9
Most recently, Cramer et al10 found 12 studies meeting inclusion criteria that reported on Viniyoga, Iyengar, and Hatha yoga interventions. Ten of these studies were included in the meta-analysis, which strongly favored yoga over control interventions for reducing pain and disability scores.10
Depression and anxiety
Yoga therapy for depression and anxiety has been commonly studied, given that aspects of mindfulness and relaxation are thought to be important parts of treatment. Moreover, patients uncomfortable with pharmacologic therapy for their disorders may be amenable to yoga treatment. In a recent Clinical Inquiry, Skowronek et al11 found evidence (strength of recommendation [SOR] B) for yoga to treat depression and anxiety symptoms based on 3 recently published review articles that commented on a total of 23 RCTs.
A handful of additional review papers on this subject have selected slightly different groups of studies to include in their analyses, but all have found generally positive results.12-14 Inclusion criteria varied: one review omitted breathing-only modalities such as Sudarshan Kriya yoga, while another included them.12,14 One omitted Mindfulness-Based Stress Reduction (MBSR), which is a program developed in the United States based on several Eastern and Western methodologies including yoga.12 MBSR already has a large body of literature supporting its use for anxiety and depression.12
One of these reviews,12 which involved a meta-analysis of 9 studies regarding depression, also included a meta-analysis of 5 studies on yoga for anxiety. Pooled results for depression showed significant benefit for yoga over usual care, and smaller but still significant benefit for yoga over aerobic exercise or other relaxation techniques. For anxiety, pooled analysis showed yoga to be equal to usual care but superior to other relaxation modalities.12 As with earlier reviews, study groups were heterogeneous and included young and older adults, caregivers for dementia patients, and those receiving inpatient treatment for alcohol dependency; symptoms of depression ranged from mild to severe.12
In a review focusing on anxiety disorders, Kirkwood et al15 located 8 trials, 6 of which were randomized. Many of these were published in the 1970s and 80s. The yoga interventions varied and included weekly Kundalini sessions, pranayama techniques, and savasana (a pose in which practitioners lie supine while focusing on breathing and muscle relaxation). These practices were compared with anxiolytic medication, progressive muscular relaxation, placebo capsule, and no treatment. All found a statistically significant reduction in anxiety indices in the yoga treatment groups, and the authors noted that the positive effects of yoga for those suffering from obsessive-compulsive disorders are particularly well documented.15 More recently, Li and Goldsmith16 reviewed 6 interventional studies that included some trials without randomization, blinding, or a control group. Subjects of the studies included cancer patients, postmenopausal women, pregnant women, and firefighters. Six of 9 trials showed improvement in externally validated anxiety indices such as the State-Trait Anxiety Inventory or Perceived Stress Scale.
Asthma
With its focus on awareness of breath and the mechanics of breathing, yoga would seem a natural adjunct to conventional asthma therapy. One systematic review found 4 trials (3 RCTs) that showed statistically significant improvements in spirometric measurements in patients with asthma who practiced yoga techniques.17 An additional 3 RCTs showed no improvements with yoga over conventional treatments.17 Overall, the reviewers noted that study quality was poor, although they said several studies were appropriately designed. Again, the interventions described as “yoga” varied considerably, from Iyengar-type classes to meditation-focused techniques to pranayama exercises. Follow-up ranged from 6 weeks to 6 months.17
A more recent and thorough review found 14 RCTs using yoga to treat asthma symptoms.18 The investigators performed pooled analysis despite significant heterogeneity in the studies. The analysis showed some improvement in the yoga group compared with usual therapy, but no difference in comparison with sham yoga or non-yoga breathing exercises.18
Symptoms of menopause
Studies have focused on alternative or adjunctive therapies for menopause symptoms, primarily hot flashes, since hormone replacement therapy and other conventional medical therapies have been found to have a high incidence of adverse effects. However, evidence that yoga can reduce hot flashes is sparse.
A Cochrane review examined the effects of exercise on hot flashes and found 2 RCTs using yoga as a treatment modality. Neither one found statistically significant differences between the yoga groups and conventional exercise groups.19 The authors concluded there was insufficient evidence to show yoga was more effective than other forms of exercise on vasomotor symptoms of menopause. However, a large RCT included in the Cochrane review did show lower stress levels and decreased overall symptoms in the yoga arm.20
The yoga intervention in this study consisted of pranayama, sun salutation (a repetitive sequence of 12 yoga postures), and cyclic meditation.20 Lee et al21 reviewed the 2 studies used in the Cochrane paper as well as 5 other studies. Two were RCTs showing that yoga intervention was not superior to a no-treatment control. Four studies showed favorable results for yoga interventions; however, one was a nonrandomized controlled trial and 3 lacked control groups.
Cramer et al22 attempted pooled analysis of 5 studies, including those in the Cochrane paper, with similar results: Yoga interventions were not efficacious for somatic, vasomotor, or urogenital symptoms of menopause. Yoga was somewhat efficacious for psychological symptoms associated with menopause.22 More recently, an RCT (N=249) found that yoga reduces vasomotor symptoms no more frequently than non-yoga exercise.23
Hypertension
Yoga is often said to reduce blood pressure (BP), which would make sense given the emphasis put on relaxation by many schools of yoga. In the past 2 years, 3 review articles have been published, as well as 2 relevant RCTs not included in those reviews.
Hagins et al24 found 17 RCTs using yoga to treat adults with hypertension and prehypertension. These included both blinded and unblinded studies, and yoga interventions were compared with usual treatment, education, or non-yoga exercise. The authors included only studies of asanas intervention, and excluded interventions using only breathing or relaxation techniques.24 In meta-analysis, pooled data showed the yoga treatment decreased both diastolic BP (DBP) and systolic BP (SBP) by 3 to 4 mm Hg compared with usual treatment, but not when compared with other exercise therapies.24 Reviewers concluded that yoga was likely as effective for lowering BP as other types of physical activity.24
In a review without meta-analysis, Posadzki et al25 also found 17 blinded RCTs using yoga to treat hypertension or prehypertension in adults. Eleven of the 17 studies favored yoga, with 8 showing a decrease in SBP and 5 in DBP.25 All but 2 studies were found to be of poor quality, especially with regard to blinding.25 The authors noted that studies using subjects with prehypertension or hypertension with comorbidities were more likely to show significant results, speculating that yoga may be more effective for these populations.25
In an ambitious review article on yoga as treatment for a variety of risk factors for cardiovascular disease, Cramer et al26 located 28 RCTs that addressed effects of yoga on BP. Seven of the studies in the Posadzki review25 were included. Meta-analysis showed a statistically significant decrease in SBP of 5.85 mm Hg and in DBP of 4.12 mm Hg.26 Although wide in scope, this meta-analysis included many studies of healthy patients without hypertension who could conceivably have differing neuroendocrine responses to yoga practice.
In a pilot RCT, Cohen et al27 found a significant decrease in BP among subjects randomized into Iyengar yoga classes for 24 weeks compared with a control group educated about lifestyle modification. A larger study with 102 subjects is currently underway.28 These studies were unique in that no subjects were currently being treated with antihypertensive medications27,28; most other trials on this subject enrolled participants on antihypertensive medications if their regimens had been stable for some time.
In an RCT published recently by Hagins et al,29 68 subjects with pre- or stage I hypertension were randomized into Ashtanga yoga classes or non-aerobic exercise classes formulated to burn equivalent METs. After 12 weeks of treatment, the yoga subjects’ BP had significantly decreased from starting values, but was not improved compared with the exercise subjects.29 This further supports the assertion that yoga is equivalent to other forms of physical activity in decreasing BP among hypertensive subjects.
Balance and stability in the elderly
With its emphasis on strength, balance, and body awareness, yoga would seem a helpful intervention for older patients at risk of injury from falls. Unfortunately this area of research lacks significant numbers of controlled trails. In a Cochrane review of exercise interventions for improving balance in the elderly, the reviewers were unable find any studies specifically using yoga that met their criteria.30 Jeter et al31 attempted a review more recently, and found 15 studies meeting inclusion criteria, 5 of which were RCTs. Overall, however, the poor quality of the studies and variation in both the type of yoga used as intervention and measurements of balance precluded pooled analysis, although some studies did have positive results.
A small but well-designed pilot RCT was recently published showing that an Iyengar yoga intervention significantly improved timed one-leg balancing among community dwelling older adults.32 However, this study did not show a significant difference in a standardized fall risk survey after the intervention.32
Cautioning against yoga in this context are several articles chronicling increased risks of some yoga exercises, especially for those with osteoporosis or other risks for fractures.33 At this point, the well-documented risks of yoga practice in this group probably outweigh the unsubstantiated rewards.
CORRESPONDENCE
Genevieve Verrastro, MD, MAHEC Family Health Center at Biltmore, 123 Hendersonville Road, Asheville, NC 28803; genevieve.verrastro@gmail.com
1. Yoga Journal. Yoga in America study 2012 [press release]. Santa Cruz, CA: Santa Cruz Bay Publishing; 2008. Available at: http://www.yogajournal.com/press/yoga_in_america. Accessed August 19, 2014.
2. Broad WJ. The Science of Yoga: The Risks and Rewards. New York, New York: Simon & Schuster; 2012.
3. Lamb T. Health Benefits of Yoga. International Association of Yoga Therapists Web site. Available at: http://www.iayt.org/?page=HealthBenefitsofYoga. Accessed August 21, 2014.
4. Yoga Alliance. 200-hour standards for yoga teacher trainings. Yoga Alliance Web site. Available at: http://yogaalliance.org/content/200-hour-standards. Accessed August 19, 2014.
5. Wren AA, Wright MA, Carson JW, et al. Yoga for persistent pain: New findings and directions for an ancient practice. Pain. 2011;152:477-480.
6. Chou R, Huffman LH; American Pain Society; American College of Physicians. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med. 2007;147:492-504.
7. Sherman KJ, Cherkin DC, Erro J, et al. Comparing yoga, exercise, and a self-care book for chronic low back pain: a randomized, controlled trial. Ann Intern Med. 2005;143:849-856.
8. Posadzki P, Ernst E. Yoga for low back pain: a systematic review of randomized clinical trials. Clin Rheumatol. 2011;30:1257-1262.
9. Graves N, Krepcho M, Mayo HG, et al. Does yoga speed healing for patients with low back pain? J Fam Pract. 2004;53:661-662.
10. Cramer H, Lauche R, Haller H, et al. A systematic review and meta-analysis of yoga for low back pain. Clin J Pain. 2013;29:450-460.
11. Skowronek IB, Mounsey A, Handler L. Can yoga reduce symptoms of anxiety and depression? J Fam Pract. 2013;63:398-399,407.
12. Cramer H, Lauche R, Langhorst J, et al. Yoga for depression: a systematic review and meta-analysis. Depress Anxiety. 2013;30: 1068-1083.
13. D’Silva S, Poscablo C, Habousha R, et al. Mind-body medicine therapies for a range of depression severity: a systematic review. Psychosomatics. 2012;53:407-423.
14. Balasubramaniam M, Telles S, Doraiswamy PM. Yoga on our minds: a systematic review of yoga for neuropsychiatric disorders. Front Psychiatry. 2013;3:117.
15. Kirkwood G, Rampes H, Tuffrey V, et al. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39: 884-891.
16. Li AW, Goldsmith CA. The effects of yoga on anxiety and stress. Altern Med Rev. 2012;17:21-35.
17. Posadzki P, Ernst E. Yoga for asthma? A systematic review of randomized clinical trials. J Asthma. 2011;48:632-639.
18. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol. 2014;112:503-510.e5.
19. Daley A, Stokes-Lampard H, Macarthur C. Exercise for vasomotor menopausal symptoms. Cochrane Database Syst Rev. 2011;(5):CD006108.
20. Chattha R, Nagarathna R, Padmalatha V, et al. Effect of yoga on cognitive functions in climacteric syndrome: a randomised control study. BJOG. 2008;115:991-1000.
21. Lee MS, Kim JI, Ha JY, et al. Yoga for menopausal symptoms: a systematic review. Menopause. 2009;16:602-608.
22. Cramer H, Lauche R, Langhorst J, et al. Effectiveness of yoga for menopausal symptoms: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2012;2012:863905.
23. Newton KM, Reed SD, Guthrie KA, et al. Efficacy of yoga for vasomotor symptoms: a randomized controlled trial. Menopause. 2014;21:339-346.
24. Hagins M, States R, Selfe T, et al. Effectiveness of yoga for hypertension: systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:649836.
25. Posadzki P, Cramer H, Kuzdzal A, et al. Yoga for hypertension: a systematic review of randomized clinical trials. Complement Ther Med. 2014;22:511-522.
26. Cramer H, Lauche R, Haller H, et al. Effects of yoga on cardiovascular disease risk factors: a systematic review and meta-analysis. Int J Cardiol. 2014;173:170-183.
27. Cohen DL, Bloedon LT, Rothman RL, et al. Iyengar yoga versus enhanced usual care on blood pressure in patients with prehypertension to stage I hypertension: a randomized controlled trial. Evid Based Complement Alternat Med. 2011;2011:546428.
28. Cohen DL, Bowler A, Fisher SA, et al. Lifestyle Modification in Blood Pressure Study II (LIMBS): study protocol of a randomized controlled trial assessing the efficacy of a 24 week structured yoga program versus lifestyle modification on blood pressure reduction. Contemp Clin Trials. 2013;36:32-40.
29. Hagins M, Rundle A, Consedine N, et al. A randomized controlled trial comparing the effects of yoga with an active control on ambulatory blood pressure in individuals with pre- and stage 1 hypertension. J Clin Hypertens (Greenwich). 2014;16:54-62.
30. Howe TE, Rochester L, Neil F, et al. Exercise for improving balance in older people. Cochrane Database Syst Rev. 2011;(11):CD004963.
31. Jeter PE, Nkodo AF, Moonaz SH, et al. A systematic review of yoga for balance in a healthy population. J Altern Complement Med. 2014;20:221-232.
32. Tiedemann A, O’Rourke S, Sesto R, et al. A 12-week Iyengar yoga program improved balance and mobility in older community-dwelling people: a pilot randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2013;68:1068-1075.
33. Sinaki M. Yoga spinal flexion positions and vertebral compression fracture in osteopenia or osteoporosis of spine: case series. Pain Pract. 2013;13:68-75.
1. Yoga Journal. Yoga in America study 2012 [press release]. Santa Cruz, CA: Santa Cruz Bay Publishing; 2008. Available at: http://www.yogajournal.com/press/yoga_in_america. Accessed August 19, 2014.
2. Broad WJ. The Science of Yoga: The Risks and Rewards. New York, New York: Simon & Schuster; 2012.
3. Lamb T. Health Benefits of Yoga. International Association of Yoga Therapists Web site. Available at: http://www.iayt.org/?page=HealthBenefitsofYoga. Accessed August 21, 2014.
4. Yoga Alliance. 200-hour standards for yoga teacher trainings. Yoga Alliance Web site. Available at: http://yogaalliance.org/content/200-hour-standards. Accessed August 19, 2014.
5. Wren AA, Wright MA, Carson JW, et al. Yoga for persistent pain: New findings and directions for an ancient practice. Pain. 2011;152:477-480.
6. Chou R, Huffman LH; American Pain Society; American College of Physicians. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med. 2007;147:492-504.
7. Sherman KJ, Cherkin DC, Erro J, et al. Comparing yoga, exercise, and a self-care book for chronic low back pain: a randomized, controlled trial. Ann Intern Med. 2005;143:849-856.
8. Posadzki P, Ernst E. Yoga for low back pain: a systematic review of randomized clinical trials. Clin Rheumatol. 2011;30:1257-1262.
9. Graves N, Krepcho M, Mayo HG, et al. Does yoga speed healing for patients with low back pain? J Fam Pract. 2004;53:661-662.
10. Cramer H, Lauche R, Haller H, et al. A systematic review and meta-analysis of yoga for low back pain. Clin J Pain. 2013;29:450-460.
11. Skowronek IB, Mounsey A, Handler L. Can yoga reduce symptoms of anxiety and depression? J Fam Pract. 2013;63:398-399,407.
12. Cramer H, Lauche R, Langhorst J, et al. Yoga for depression: a systematic review and meta-analysis. Depress Anxiety. 2013;30: 1068-1083.
13. D’Silva S, Poscablo C, Habousha R, et al. Mind-body medicine therapies for a range of depression severity: a systematic review. Psychosomatics. 2012;53:407-423.
14. Balasubramaniam M, Telles S, Doraiswamy PM. Yoga on our minds: a systematic review of yoga for neuropsychiatric disorders. Front Psychiatry. 2013;3:117.
15. Kirkwood G, Rampes H, Tuffrey V, et al. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39: 884-891.
16. Li AW, Goldsmith CA. The effects of yoga on anxiety and stress. Altern Med Rev. 2012;17:21-35.
17. Posadzki P, Ernst E. Yoga for asthma? A systematic review of randomized clinical trials. J Asthma. 2011;48:632-639.
18. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol. 2014;112:503-510.e5.
19. Daley A, Stokes-Lampard H, Macarthur C. Exercise for vasomotor menopausal symptoms. Cochrane Database Syst Rev. 2011;(5):CD006108.
20. Chattha R, Nagarathna R, Padmalatha V, et al. Effect of yoga on cognitive functions in climacteric syndrome: a randomised control study. BJOG. 2008;115:991-1000.
21. Lee MS, Kim JI, Ha JY, et al. Yoga for menopausal symptoms: a systematic review. Menopause. 2009;16:602-608.
22. Cramer H, Lauche R, Langhorst J, et al. Effectiveness of yoga for menopausal symptoms: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2012;2012:863905.
23. Newton KM, Reed SD, Guthrie KA, et al. Efficacy of yoga for vasomotor symptoms: a randomized controlled trial. Menopause. 2014;21:339-346.
24. Hagins M, States R, Selfe T, et al. Effectiveness of yoga for hypertension: systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:649836.
25. Posadzki P, Cramer H, Kuzdzal A, et al. Yoga for hypertension: a systematic review of randomized clinical trials. Complement Ther Med. 2014;22:511-522.
26. Cramer H, Lauche R, Haller H, et al. Effects of yoga on cardiovascular disease risk factors: a systematic review and meta-analysis. Int J Cardiol. 2014;173:170-183.
27. Cohen DL, Bloedon LT, Rothman RL, et al. Iyengar yoga versus enhanced usual care on blood pressure in patients with prehypertension to stage I hypertension: a randomized controlled trial. Evid Based Complement Alternat Med. 2011;2011:546428.
28. Cohen DL, Bowler A, Fisher SA, et al. Lifestyle Modification in Blood Pressure Study II (LIMBS): study protocol of a randomized controlled trial assessing the efficacy of a 24 week structured yoga program versus lifestyle modification on blood pressure reduction. Contemp Clin Trials. 2013;36:32-40.
29. Hagins M, Rundle A, Consedine N, et al. A randomized controlled trial comparing the effects of yoga with an active control on ambulatory blood pressure in individuals with pre- and stage 1 hypertension. J Clin Hypertens (Greenwich). 2014;16:54-62.
30. Howe TE, Rochester L, Neil F, et al. Exercise for improving balance in older people. Cochrane Database Syst Rev. 2011;(11):CD004963.
31. Jeter PE, Nkodo AF, Moonaz SH, et al. A systematic review of yoga for balance in a healthy population. J Altern Complement Med. 2014;20:221-232.
32. Tiedemann A, O’Rourke S, Sesto R, et al. A 12-week Iyengar yoga program improved balance and mobility in older community-dwelling people: a pilot randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2013;68:1068-1075.
33. Sinaki M. Yoga spinal flexion positions and vertebral compression fracture in osteopenia or osteoporosis of spine: case series. Pain Pract. 2013;13:68-75.
