Veterans aged > 85 years are the fastest growing cohort; they are living longer with multiple chronic conditions and functional impairments.1,2 The majority of older veterans (94.6% or about 1.89 million) seeking services in the VA obtain care through primary care providers (PCPs) who are usually not formally trained in geriatrics.1,3 A 2008 Institute of Medicine report noted that geriatric training was inadequate not only for physicians, but also for all health professions.4 For these reasons, new models of care are needed to improve access to geriatric specialists and to improve geriatric care provided by PCPs, especially in rural settings.
In 2010, VA adopted the Patient Aligned Care Team (PACT), based on the patient-centered medical home model, to improve primary care services.5 The PACT was designed to deliver patient-centered care and incorporate a team approach to provide comprehensive, coordinated, and personalized care—common themes found in quality geriatric care.4-6
To provide specialty care support, other programs also were initiated, including the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO). It was implemented in 2011 to increase veteran’s access to specialty care providers and educate PCPs in the treatment of specific diseases. The SCAN-ECHO program is a case-based provider education program conducted via a videoconference that usually occurs monthly and is initiated by a referring PCP for a specific disease or topic.
An interdisciplinary team developed the Geriatric SCAN-ECHO program to help improve veteran access to geriatric specialists and influence care provided to older patients seen by PACTs. The team consisted of a geriatrician, gerontological nurse practitioner (NP), registered nurse (RN), neuropsychologist, social worker (SW), pharmacist, and clinic manager. The geriatric team was located in an urban, academic geriatric specialty clinic in VISN 22 that served 2 ambulatory care centers and 8 satellite community-based outpatient clinics (CBOCs). Veterans using the CBOCs had no direct access to geriatric specialists without traveling to the clinic, which for some could be up to 200 miles away.
This article describes the lessons learned from the implementation of a Geriatric SCAN-ECHO program, preliminary staff survey and chart review results. The program began in January 2013 and ended in February 2014. The article also offers recommendations to increase understanding of geriatric principles for PCP teams.
The Geriatric SCAN-ECHO Program
After obtaining patient consent, primary care clinicians submitted a consult that included the reason for referral (Figure 1). This list of reasons (eg, behavioral management of geriatric syndromes, care management strategies for patients with dementia, caregiver support strategies, and strategies for the patient to continue living in the community safely) assisted the referring clinician in identifying potential cases that might benefit from a geriatric interdisciplinary case review. Patient approval to contact a caregiver or spouse was requested so the Geriatric SCAN-ECHO team could gather additional information.
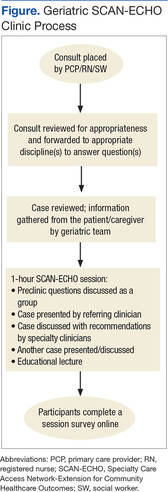
After the team received the consult, the gerontological NP or geriatrician reviewed the case and identified other relevant members of the team. The electronic medical record (EMR) was reviewed and a phone call made to the patient and/or their caregiver by the appropriate team member to obtain more information, which could include the patient’s current living situation by the social worker, a medication review by the pharmacist, and functional assessment (eg, basic and instrumental activities of daily living) by the nurse. If appropriate, the geriatrician used the Montreal Cognitive Assessment (MoCA)-BLIND to assess the patient’s cognitive abilities.7 Finally, the team met to reach a consensus on final recommendations and to identify the didactic lecture topic related to the case being reviewed and presented by members of the Geriatric SCAN-ECHO team.
At the start of each SCAN-ECHO session, the geriatrician asked participants 2 to 3 questions on the clinical topic to be covered to elicit interest and motivation to learn. The referring clinician provided a short summary of the case and reason for referral, and the Geriatric SCAN-ECHO team then provided individual findings and recommendations. Due to the complexity of the referrals, the team usually was able to process 1 to 2 cases during the 1-hour session, with 15 minutes allocated for the didactic.
The didactic lectures consisted of evidence-based tools and guidelines that focused on changing provider practice behavior (eg, Assessing Care of Vulnerable Elders criteria) and were posted on the Geriatric SCAN-ECHO SharePoint site after the session for clinicians to download.8 The topics covered included fall risk and prevention; the screening, diagnosis, and management of cognitive disorders; psychosocial considerations in older adults; use of anticholinergic drugs; and assessment and management of unsafe geriatric drivers. Participants were then sent a survey to evaluate the usefulness of the session and its impact on the clinician’s practice. At the end of each session, a summary of findings and recommendations by the geriatric team also was documented in the patient’s EMR and forwarded to the referring clinician. Several factors differentiated the Geriatric from other SCAN-ECHO specialty programs. First, nurses and SWs were invited to place consults, because they were often the first clinicians to identify problems. In a typical SCAN-ECHO program, only PCPs place a consult to the specialty clinic. Second, an interdisciplinary team responded to consults. This was done so that members of the PACT could learn about domains covered by the other disciplines and receive discipline-specific guidance (SCAN-ECHO consults are often answered by a specialist). Third, the team supplemented EMR records with telephone-based assessments. Most SCAN-ECHO programs relied mainly on EMR records.