User login
An ECHO-Based Program to Provide Geriatric Specialty Care Consultation and Education
Veterans aged > 85 years are the fastest growing cohort; they are living longer with multiple chronic conditions and functional impairments.1,2 The majority of older veterans (94.6% or about 1.89 million) seeking services in the VA obtain care through primary care providers (PCPs) who are usually not formally trained in geriatrics.1,3 A 2008 Institute of Medicine report noted that geriatric training was inadequate not only for physicians, but also for all health professions.4 For these reasons, new models of care are needed to improve access to geriatric specialists and to improve geriatric care provided by PCPs, especially in rural settings.
In 2010, VA adopted the Patient Aligned Care Team (PACT), based on the patient-centered medical home model, to improve primary care services.5 The PACT was designed to deliver patient-centered care and incorporate a team approach to provide comprehensive, coordinated, and personalized care—common themes found in quality geriatric care.4-6
To provide specialty care support, other programs also were initiated, including the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO). It was implemented in 2011 to increase veteran’s access to specialty care providers and educate PCPs in the treatment of specific diseases. The SCAN-ECHO program is a case-based provider education program conducted via a videoconference that usually occurs monthly and is initiated by a referring PCP for a specific disease or topic.
An interdisciplinary team developed the Geriatric SCAN-ECHO program to help improve veteran access to geriatric specialists and influence care provided to older patients seen by PACTs. The team consisted of a geriatrician, gerontological nurse practitioner (NP), registered nurse (RN), neuropsychologist, social worker (SW), pharmacist, and clinic manager. The geriatric team was located in an urban, academic geriatric specialty clinic in VISN 22 that served 2 ambulatory care centers and 8 satellite community-based outpatient clinics (CBOCs). Veterans using the CBOCs had no direct access to geriatric specialists without traveling to the clinic, which for some could be up to 200 miles away.
This article describes the lessons learned from the implementation of a Geriatric SCAN-ECHO program, preliminary staff survey and chart review results. The program began in January 2013 and ended in February 2014. The article also offers recommendations to increase understanding of geriatric principles for PCP teams.
The Geriatric SCAN-ECHO Program
After obtaining patient consent, primary care clinicians submitted a consult that included the reason for referral (Figure 1). This list of reasons (eg, behavioral management of geriatric syndromes, care management strategies for patients with dementia, caregiver support strategies, and strategies for the patient to continue living in the community safely) assisted the referring clinician in identifying potential cases that might benefit from a geriatric interdisciplinary case review. Patient approval to contact a caregiver or spouse was requested so the Geriatric SCAN-ECHO team could gather additional information.
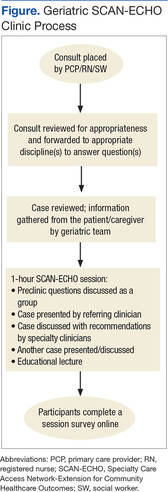
After the team received the consult, the gerontological NP or geriatrician reviewed the case and identified other relevant members of the team. The electronic medical record (EMR) was reviewed and a phone call made to the patient and/or their caregiver by the appropriate team member to obtain more information, which could include the patient’s current living situation by the social worker, a medication review by the pharmacist, and functional assessment (eg, basic and instrumental activities of daily living) by the nurse. If appropriate, the geriatrician used the Montreal Cognitive Assessment (MoCA)-BLIND to assess the patient’s cognitive abilities.7 Finally, the team met to reach a consensus on final recommendations and to identify the didactic lecture topic related to the case being reviewed and presented by members of the Geriatric SCAN-ECHO team.
At the start of each SCAN-ECHO session, the geriatrician asked participants 2 to 3 questions on the clinical topic to be covered to elicit interest and motivation to learn. The referring clinician provided a short summary of the case and reason for referral, and the Geriatric SCAN-ECHO team then provided individual findings and recommendations. Due to the complexity of the referrals, the team usually was able to process 1 to 2 cases during the 1-hour session, with 15 minutes allocated for the didactic.
The didactic lectures consisted of evidence-based tools and guidelines that focused on changing provider practice behavior (eg, Assessing Care of Vulnerable Elders criteria) and were posted on the Geriatric SCAN-ECHO SharePoint site after the session for clinicians to download.8 The topics covered included fall risk and prevention; the screening, diagnosis, and management of cognitive disorders; psychosocial considerations in older adults; use of anticholinergic drugs; and assessment and management of unsafe geriatric drivers. Participants were then sent a survey to evaluate the usefulness of the session and its impact on the clinician’s practice. At the end of each session, a summary of findings and recommendations by the geriatric team also was documented in the patient’s EMR and forwarded to the referring clinician. Several factors differentiated the Geriatric from other SCAN-ECHO specialty programs. First, nurses and SWs were invited to place consults, because they were often the first clinicians to identify problems. In a typical SCAN-ECHO program, only PCPs place a consult to the specialty clinic. Second, an interdisciplinary team responded to consults. This was done so that members of the PACT could learn about domains covered by the other disciplines and receive discipline-specific guidance (SCAN-ECHO consults are often answered by a specialist). Third, the team supplemented EMR records with telephone-based assessments. Most SCAN-ECHO programs relied mainly on EMR records.
Facilitators
Although the Geriatric SCAN-ECHO program began in January 2013, the VA Greater Los Angeles Healthcare System facility already had several SCAN-ECHO programs. An experienced SCAN-ECHO project director assisted in the implementation of the program. The specialists used existing documents to guide the program, such as a service agreement between SCAN-ECHO and the participating satellite facilities and templates for consults and documentation. Other benefits of the established SCAN-ECHO presence included availability of videoconferencing equipment; local clinical informatics staff who were familiar with the setup of interfacility consults, clinic encounters, and workload credit in the EMR; and PACT clinicians who were familiar with the SCAN-ECHO program and format. Finally, the geriatric interdisciplinary team members had worked together cohesively for years and were supported by the Geriatric Research Education and Clinical Center to implement clinical demonstration projects, such as the SCAN-ECHO program.
Implementation Barriers
Initially the program received few consults. The Geriatric SCAN-ECHO program used a sample case to start the discussion and focused on falls. At times there were also only a small number of facilities and attendees who participated. Most of the attendees were MDs and NPs from Primary Care and Psychiatry. None of the nurses or SWs who were invited by their local leadership participated early on. Informal communication with CBOC staff found that they were feeling overwhelmed with other competing demands. There were multiple SCAN-ECHO programs and no protected time to attend the sessions. In addition, nurses might not have identified the program as a priority because the training topic was too general (geriatrics vs pressure ulcer or pain management).
The Geriatric SCAN-ECHO program adjusted the timing of sessions to convene every other month on a day that most CBOCs had staff meetings, allowing for protected time for staff participation. The CBOC staff was invited again to participate. The gerontological NP contacted the referring clinician to report the date of the case review and followed up afterward to ensure that all questions were answered and recommendations were clear.
The increase in marketing and networking led to more facilities participating; however, the number of staff participants remained low. The program team then changed tactics and focused on facilitating specific clinician behavior changes related to common geriatric syndromes instead of case reviews. The team conducted a session providing an overview of dementia recognition and diagnosis, rationale for objective measures, and a demonstration on the administration of the Mini-Cog Assessment Instrument for Dementia and Montreal Cognitive Assessment (MoCA) tools.7 This session had the highest number of total attendees (38), half of whom were nurses.
Feedback after the session resulted in an additional session the following month, which focused on the scoring and documentation of the tools as well as interpretation of the results and how this might be further evaluated by the team. Informal feedback gathered from nurses during this second session included a request for more training, tips on how to administer the tools, and how to document competency in tool administration. A new educational project that would empower PACT nurses to proactively identify and initiate cognitive impairment/dementia evaluations was then started independent of the Geriatric SCAN-ECHO program.
Results
Participants of SCAN-ECHO programs were surveyed on usefulness of information and its influence on their practice (Table 1). A total of 41 respondents (the same person may have attended more than 1 session) completed surveys on 9 Geriatric SCAN-ECHO sessions. Nineteen (46%) were medical doctors, 8 (20%) were NPs, and 14 (34%) were from other disciplines. Overall, the sessions were well received, and participants found the information useful. Because the respondents were from different disciplines and roles, it was not surprising that only 13 respondents (32%) felt that the information would influence their prescribing practices, and only 18 respondents (44%) agreed that the session changed their ordering of diagnostic tests and studies.
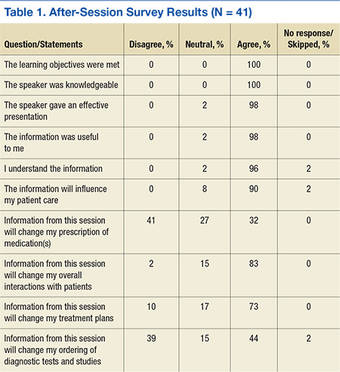
Chart Reviews
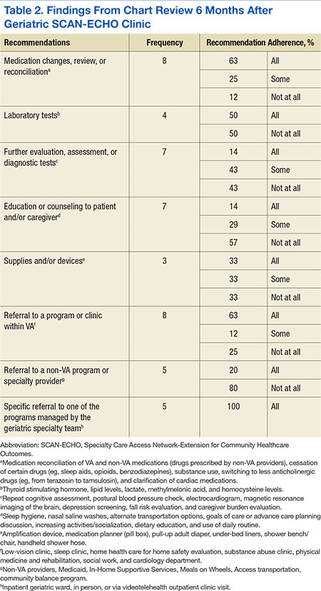
Six months after completion of the Geriatric SCAN-ECHO session, the gerontological NP reviewed patient charts and identified rates of adherence for geriatric team recommendations. Eight patient cases were reviewed in 6 of the 9 sessions. The other sessions used sample cases from the team’s experience due to lack of submitted consults. Physicians referred 4 cases, and the rest were from NPs; all were from primary care except for a primary mental health NP. Half of the referred cases were forwarded from other departments (eg, neurobehavior and dementia clinics) to avoid travel. Reasons for referral included geriatric syndrome workup and specific medical questions. All patients were men aged 66 to 94 years (mean = 83.25; SD = 8.29).
Table 2 lists the frequency and adherence to recommendations. If the recommendation was discussed but refused by the patient, it was still noted as completed. Several recommendations might have been presented; thus, adherence to recommendations was categorized as “all,” “some,” or “not at all” adherent. Because the referrals involved complex cases, most cases were referred to other clinical programs managed by the geriatric specialty team for further evaluation and management.
Discussion
Although the Geriatric SCAN-ECHO sessions were well received, the impact of the program was limited by the lack of consults and PACT team involvement. Impact was markedly improved once the focus of the sessions changed from case studies to specific clinical tool administration/practice change. Leadership support and coordination to provide protected team learning time was essential. Incentives to participate might include making geriatric quality indicators part of performance measures to improve practice and quality of care. Although the VA monitors several frail elderly measures that are a reflection of quality geriatric care, it is up to each VISN to determine its performance measures (Kenneth Shay, e-mail communication, February 12, 2013).
The most frequently followed recommendation was referral to a program managed by the geriatric specialty team. Full compliance with this recommendation may be due to the ease of placing a single consult and the interaction between the SCAN-ECHO team and the geriatric specialty services staff. The next most commonly followed recommendations were for medication changes/review and referral to a different program or clinic (not inpatient or outpatient geriatric specialty programs). Because completion of medication reconciliation reminders are tied to pay incentives for VA physicians, this may explain why it was fulfilled at a higher rates compared with other recommendations, suggesting that bonus incentives could boost participation.
The least frequently completed recommendations were referrals to non-VA programs or specialty providers. This may be a reflection of poor communication with non-VA providers and/or documentation of such communications and lack of the availability of the programs near the patient’s residence. Developing remote site referral guides might improve this communication.
Another type of recommendation that was partially or not at all followed was for further evaluation, assessment, or diagnostic tests of specific problems identified by the Geriatric SCAN-ECHO team. This may be due to lack of easy access to specific diagnostic tests in outpatient clinics or lack of staff knowledge and skills on doing geriatric-specific evaluations. The chart reviewer also noted that even when the PCP did the evaluations, the quality was below standard; for example, for depression screening, the chart noted that the patient was asked about having depression; however, no specific tool was used to aid in the diagnosis. Further specificity regarding geriatric syndrome evaluations and increasing staff knowledge of common tools to aid in diagnosis and evaluation are needed.
In 2 of the 8 cases reviewed, the Geriatric SCAN-ECHO program recommended that specific family members needed to be involved in the care of the patient. Unfortunately, most often family members only were used as a means of communication or for coordination of care with the PACT teams (eg, scheduling appointments). Changes needed to provide quality care for geriatric veterans are to include family members, use a fully-realized PACT approach, and have nurses “practice to the full extent of their education and training,” as recommended by the Institute of Medicine.9
Limitations
This article reported on the experience of a geriatric team that implemented an interdisciplinary telehealth-based consultation program. Facilitators and barriers to program execution may be limited to the local site and VA. The survey following the session was developed by the VA SCAN-ECHO program and was not specific to this local program. Limitations of the chart review include a short follow-up of only 6 months after the program. Many of the behavioral changes or educational recommendations might have been discussed but were not documented. Also services done by non-VA providers might not have been documented and, therefore, would not have been included in this chart review.
Conclusions
The geriatric team decided to discontinue the Geriatric SCAN-ECHO program. The key metric for program success was number of cases reviewed. Only 1 to 2 cases were reviewed every other month. Participation in the program markedly increased when the specific learning needs of PACT teams were addressed; however, most cases were referred to GRECC due to the case complexity and were not appropriate for the SCAN-ECHO format. The chart review, patient and caregiver contact, and presentation preparation required the program staff to invest a significant amount time. It took 3 to 4 hours for the staff to prepare for each case. Furthermore, adherence to recommendations was also poor.
Case-based education and training without follow-up of the recommendations likely is not the best approach to improve care of older veterans in the primary care setting. The authors hope that focusing on specific practice changes and working directly with PACTs and specific team members will be more productive and result in improved outcomes for older veterans. Due to the complexity of geriatric cases involving physical, cognitive, and emotional vulnerabilities, these cases may be better handled by direct multidisciplinary examinations.
Acknowledgments
Funding for this project was supported by the Veterans Health Administration Office of Specialty Care Services T-21 funding initiative.
1. U.S. Department of Veterans Affairs. Geriatric ambulatory care. VHA handbook 1140.10. U.S. Department of Veterans Affairs Website. http://www.va.gov/vhapublications/publications.cfm?pub=2. Published April 26, 2010. Accessed March 9, 2016.
2. Federal Interagency Forum on Aging-Related Statistics. Older Americans 2012: Key Indicators of Well-Being. Washington, DC: U.S. Government Printing Office; 2012.
3. Shay K, Schectman G. Primary care for older veterans. Generations. 2010;34(2):35-42.
4. Institute of Medicine. Retooling for an Aging America: Building the Health Care Workforce. Washington, DC: The National Academies Press; 2008.
5. U.S. Department of Veterans Affairs. Patient centered medical home model concept paper. U.S. Department of Veterans Affairs Website. http://www.vacareers.va.gov/assets/common/print/pcmh_conceptpaper.pdf. Published May 23, 2012. Accessed March 9, 2016.
6. Berenson RA, Devers KJ, Burton RA. Will the patient-centered medical home transform the delivery of health care? Urban Institute Website. http://www.urban.org/sites/default/files/alfresco/publication-pdfs/412373-Will-the-Patient-Centered-Medical-Home-Transform-the-Delivery-of-Health-Care-.pdf. Published August 2011. Accessed March 9, 2016.
7. Nasreddine D. MoCA-BLIND. Version 7.1 Original Version. Montreal Cognitive Assessment Website. http://www.mocatest.org/pdf_files/test/MoCA-Test-BLIND.pdf. Accessed March 9, 2016.
8. RAND Health Researchers. Assessing care of vulnerable elders (ACOVE). RAND Corporation Website. http://www.rand.org/health/projects.acove.html. Accessed March 9, 2016.
9. Institute of Medicine. The future of nursing: leading change, advancing health. Institute of Medicine Website. http://www.iom.edu/Reports/2010/The-future-of-nursing-leading-change-advancing-health.aspx. Published October 5, 2010. Updated October 5, 2015. Accessed March 9, 2016.
Veterans aged > 85 years are the fastest growing cohort; they are living longer with multiple chronic conditions and functional impairments.1,2 The majority of older veterans (94.6% or about 1.89 million) seeking services in the VA obtain care through primary care providers (PCPs) who are usually not formally trained in geriatrics.1,3 A 2008 Institute of Medicine report noted that geriatric training was inadequate not only for physicians, but also for all health professions.4 For these reasons, new models of care are needed to improve access to geriatric specialists and to improve geriatric care provided by PCPs, especially in rural settings.
In 2010, VA adopted the Patient Aligned Care Team (PACT), based on the patient-centered medical home model, to improve primary care services.5 The PACT was designed to deliver patient-centered care and incorporate a team approach to provide comprehensive, coordinated, and personalized care—common themes found in quality geriatric care.4-6
To provide specialty care support, other programs also were initiated, including the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO). It was implemented in 2011 to increase veteran’s access to specialty care providers and educate PCPs in the treatment of specific diseases. The SCAN-ECHO program is a case-based provider education program conducted via a videoconference that usually occurs monthly and is initiated by a referring PCP for a specific disease or topic.
An interdisciplinary team developed the Geriatric SCAN-ECHO program to help improve veteran access to geriatric specialists and influence care provided to older patients seen by PACTs. The team consisted of a geriatrician, gerontological nurse practitioner (NP), registered nurse (RN), neuropsychologist, social worker (SW), pharmacist, and clinic manager. The geriatric team was located in an urban, academic geriatric specialty clinic in VISN 22 that served 2 ambulatory care centers and 8 satellite community-based outpatient clinics (CBOCs). Veterans using the CBOCs had no direct access to geriatric specialists without traveling to the clinic, which for some could be up to 200 miles away.
This article describes the lessons learned from the implementation of a Geriatric SCAN-ECHO program, preliminary staff survey and chart review results. The program began in January 2013 and ended in February 2014. The article also offers recommendations to increase understanding of geriatric principles for PCP teams.
The Geriatric SCAN-ECHO Program
After obtaining patient consent, primary care clinicians submitted a consult that included the reason for referral (Figure 1). This list of reasons (eg, behavioral management of geriatric syndromes, care management strategies for patients with dementia, caregiver support strategies, and strategies for the patient to continue living in the community safely) assisted the referring clinician in identifying potential cases that might benefit from a geriatric interdisciplinary case review. Patient approval to contact a caregiver or spouse was requested so the Geriatric SCAN-ECHO team could gather additional information.
After the team received the consult, the gerontological NP or geriatrician reviewed the case and identified other relevant members of the team. The electronic medical record (EMR) was reviewed and a phone call made to the patient and/or their caregiver by the appropriate team member to obtain more information, which could include the patient’s current living situation by the social worker, a medication review by the pharmacist, and functional assessment (eg, basic and instrumental activities of daily living) by the nurse. If appropriate, the geriatrician used the Montreal Cognitive Assessment (MoCA)-BLIND to assess the patient’s cognitive abilities.7 Finally, the team met to reach a consensus on final recommendations and to identify the didactic lecture topic related to the case being reviewed and presented by members of the Geriatric SCAN-ECHO team.
At the start of each SCAN-ECHO session, the geriatrician asked participants 2 to 3 questions on the clinical topic to be covered to elicit interest and motivation to learn. The referring clinician provided a short summary of the case and reason for referral, and the Geriatric SCAN-ECHO team then provided individual findings and recommendations. Due to the complexity of the referrals, the team usually was able to process 1 to 2 cases during the 1-hour session, with 15 minutes allocated for the didactic.
The didactic lectures consisted of evidence-based tools and guidelines that focused on changing provider practice behavior (eg, Assessing Care of Vulnerable Elders criteria) and were posted on the Geriatric SCAN-ECHO SharePoint site after the session for clinicians to download.8 The topics covered included fall risk and prevention; the screening, diagnosis, and management of cognitive disorders; psychosocial considerations in older adults; use of anticholinergic drugs; and assessment and management of unsafe geriatric drivers. Participants were then sent a survey to evaluate the usefulness of the session and its impact on the clinician’s practice. At the end of each session, a summary of findings and recommendations by the geriatric team also was documented in the patient’s EMR and forwarded to the referring clinician. Several factors differentiated the Geriatric from other SCAN-ECHO specialty programs. First, nurses and SWs were invited to place consults, because they were often the first clinicians to identify problems. In a typical SCAN-ECHO program, only PCPs place a consult to the specialty clinic. Second, an interdisciplinary team responded to consults. This was done so that members of the PACT could learn about domains covered by the other disciplines and receive discipline-specific guidance (SCAN-ECHO consults are often answered by a specialist). Third, the team supplemented EMR records with telephone-based assessments. Most SCAN-ECHO programs relied mainly on EMR records.
Facilitators
Although the Geriatric SCAN-ECHO program began in January 2013, the VA Greater Los Angeles Healthcare System facility already had several SCAN-ECHO programs. An experienced SCAN-ECHO project director assisted in the implementation of the program. The specialists used existing documents to guide the program, such as a service agreement between SCAN-ECHO and the participating satellite facilities and templates for consults and documentation. Other benefits of the established SCAN-ECHO presence included availability of videoconferencing equipment; local clinical informatics staff who were familiar with the setup of interfacility consults, clinic encounters, and workload credit in the EMR; and PACT clinicians who were familiar with the SCAN-ECHO program and format. Finally, the geriatric interdisciplinary team members had worked together cohesively for years and were supported by the Geriatric Research Education and Clinical Center to implement clinical demonstration projects, such as the SCAN-ECHO program.
Implementation Barriers
Initially the program received few consults. The Geriatric SCAN-ECHO program used a sample case to start the discussion and focused on falls. At times there were also only a small number of facilities and attendees who participated. Most of the attendees were MDs and NPs from Primary Care and Psychiatry. None of the nurses or SWs who were invited by their local leadership participated early on. Informal communication with CBOC staff found that they were feeling overwhelmed with other competing demands. There were multiple SCAN-ECHO programs and no protected time to attend the sessions. In addition, nurses might not have identified the program as a priority because the training topic was too general (geriatrics vs pressure ulcer or pain management).
The Geriatric SCAN-ECHO program adjusted the timing of sessions to convene every other month on a day that most CBOCs had staff meetings, allowing for protected time for staff participation. The CBOC staff was invited again to participate. The gerontological NP contacted the referring clinician to report the date of the case review and followed up afterward to ensure that all questions were answered and recommendations were clear.
The increase in marketing and networking led to more facilities participating; however, the number of staff participants remained low. The program team then changed tactics and focused on facilitating specific clinician behavior changes related to common geriatric syndromes instead of case reviews. The team conducted a session providing an overview of dementia recognition and diagnosis, rationale for objective measures, and a demonstration on the administration of the Mini-Cog Assessment Instrument for Dementia and Montreal Cognitive Assessment (MoCA) tools.7 This session had the highest number of total attendees (38), half of whom were nurses.
Feedback after the session resulted in an additional session the following month, which focused on the scoring and documentation of the tools as well as interpretation of the results and how this might be further evaluated by the team. Informal feedback gathered from nurses during this second session included a request for more training, tips on how to administer the tools, and how to document competency in tool administration. A new educational project that would empower PACT nurses to proactively identify and initiate cognitive impairment/dementia evaluations was then started independent of the Geriatric SCAN-ECHO program.
Results
Participants of SCAN-ECHO programs were surveyed on usefulness of information and its influence on their practice (Table 1). A total of 41 respondents (the same person may have attended more than 1 session) completed surveys on 9 Geriatric SCAN-ECHO sessions. Nineteen (46%) were medical doctors, 8 (20%) were NPs, and 14 (34%) were from other disciplines. Overall, the sessions were well received, and participants found the information useful. Because the respondents were from different disciplines and roles, it was not surprising that only 13 respondents (32%) felt that the information would influence their prescribing practices, and only 18 respondents (44%) agreed that the session changed their ordering of diagnostic tests and studies.
Chart Reviews
Six months after completion of the Geriatric SCAN-ECHO session, the gerontological NP reviewed patient charts and identified rates of adherence for geriatric team recommendations. Eight patient cases were reviewed in 6 of the 9 sessions. The other sessions used sample cases from the team’s experience due to lack of submitted consults. Physicians referred 4 cases, and the rest were from NPs; all were from primary care except for a primary mental health NP. Half of the referred cases were forwarded from other departments (eg, neurobehavior and dementia clinics) to avoid travel. Reasons for referral included geriatric syndrome workup and specific medical questions. All patients were men aged 66 to 94 years (mean = 83.25; SD = 8.29).
Table 2 lists the frequency and adherence to recommendations. If the recommendation was discussed but refused by the patient, it was still noted as completed. Several recommendations might have been presented; thus, adherence to recommendations was categorized as “all,” “some,” or “not at all” adherent. Because the referrals involved complex cases, most cases were referred to other clinical programs managed by the geriatric specialty team for further evaluation and management.
Discussion
Although the Geriatric SCAN-ECHO sessions were well received, the impact of the program was limited by the lack of consults and PACT team involvement. Impact was markedly improved once the focus of the sessions changed from case studies to specific clinical tool administration/practice change. Leadership support and coordination to provide protected team learning time was essential. Incentives to participate might include making geriatric quality indicators part of performance measures to improve practice and quality of care. Although the VA monitors several frail elderly measures that are a reflection of quality geriatric care, it is up to each VISN to determine its performance measures (Kenneth Shay, e-mail communication, February 12, 2013).
The most frequently followed recommendation was referral to a program managed by the geriatric specialty team. Full compliance with this recommendation may be due to the ease of placing a single consult and the interaction between the SCAN-ECHO team and the geriatric specialty services staff. The next most commonly followed recommendations were for medication changes/review and referral to a different program or clinic (not inpatient or outpatient geriatric specialty programs). Because completion of medication reconciliation reminders are tied to pay incentives for VA physicians, this may explain why it was fulfilled at a higher rates compared with other recommendations, suggesting that bonus incentives could boost participation.
The least frequently completed recommendations were referrals to non-VA programs or specialty providers. This may be a reflection of poor communication with non-VA providers and/or documentation of such communications and lack of the availability of the programs near the patient’s residence. Developing remote site referral guides might improve this communication.
Another type of recommendation that was partially or not at all followed was for further evaluation, assessment, or diagnostic tests of specific problems identified by the Geriatric SCAN-ECHO team. This may be due to lack of easy access to specific diagnostic tests in outpatient clinics or lack of staff knowledge and skills on doing geriatric-specific evaluations. The chart reviewer also noted that even when the PCP did the evaluations, the quality was below standard; for example, for depression screening, the chart noted that the patient was asked about having depression; however, no specific tool was used to aid in the diagnosis. Further specificity regarding geriatric syndrome evaluations and increasing staff knowledge of common tools to aid in diagnosis and evaluation are needed.
In 2 of the 8 cases reviewed, the Geriatric SCAN-ECHO program recommended that specific family members needed to be involved in the care of the patient. Unfortunately, most often family members only were used as a means of communication or for coordination of care with the PACT teams (eg, scheduling appointments). Changes needed to provide quality care for geriatric veterans are to include family members, use a fully-realized PACT approach, and have nurses “practice to the full extent of their education and training,” as recommended by the Institute of Medicine.9
Limitations
This article reported on the experience of a geriatric team that implemented an interdisciplinary telehealth-based consultation program. Facilitators and barriers to program execution may be limited to the local site and VA. The survey following the session was developed by the VA SCAN-ECHO program and was not specific to this local program. Limitations of the chart review include a short follow-up of only 6 months after the program. Many of the behavioral changes or educational recommendations might have been discussed but were not documented. Also services done by non-VA providers might not have been documented and, therefore, would not have been included in this chart review.
Conclusions
The geriatric team decided to discontinue the Geriatric SCAN-ECHO program. The key metric for program success was number of cases reviewed. Only 1 to 2 cases were reviewed every other month. Participation in the program markedly increased when the specific learning needs of PACT teams were addressed; however, most cases were referred to GRECC due to the case complexity and were not appropriate for the SCAN-ECHO format. The chart review, patient and caregiver contact, and presentation preparation required the program staff to invest a significant amount time. It took 3 to 4 hours for the staff to prepare for each case. Furthermore, adherence to recommendations was also poor.
Case-based education and training without follow-up of the recommendations likely is not the best approach to improve care of older veterans in the primary care setting. The authors hope that focusing on specific practice changes and working directly with PACTs and specific team members will be more productive and result in improved outcomes for older veterans. Due to the complexity of geriatric cases involving physical, cognitive, and emotional vulnerabilities, these cases may be better handled by direct multidisciplinary examinations.
Acknowledgments
Funding for this project was supported by the Veterans Health Administration Office of Specialty Care Services T-21 funding initiative.
Veterans aged > 85 years are the fastest growing cohort; they are living longer with multiple chronic conditions and functional impairments.1,2 The majority of older veterans (94.6% or about 1.89 million) seeking services in the VA obtain care through primary care providers (PCPs) who are usually not formally trained in geriatrics.1,3 A 2008 Institute of Medicine report noted that geriatric training was inadequate not only for physicians, but also for all health professions.4 For these reasons, new models of care are needed to improve access to geriatric specialists and to improve geriatric care provided by PCPs, especially in rural settings.
In 2010, VA adopted the Patient Aligned Care Team (PACT), based on the patient-centered medical home model, to improve primary care services.5 The PACT was designed to deliver patient-centered care and incorporate a team approach to provide comprehensive, coordinated, and personalized care—common themes found in quality geriatric care.4-6
To provide specialty care support, other programs also were initiated, including the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO). It was implemented in 2011 to increase veteran’s access to specialty care providers and educate PCPs in the treatment of specific diseases. The SCAN-ECHO program is a case-based provider education program conducted via a videoconference that usually occurs monthly and is initiated by a referring PCP for a specific disease or topic.
An interdisciplinary team developed the Geriatric SCAN-ECHO program to help improve veteran access to geriatric specialists and influence care provided to older patients seen by PACTs. The team consisted of a geriatrician, gerontological nurse practitioner (NP), registered nurse (RN), neuropsychologist, social worker (SW), pharmacist, and clinic manager. The geriatric team was located in an urban, academic geriatric specialty clinic in VISN 22 that served 2 ambulatory care centers and 8 satellite community-based outpatient clinics (CBOCs). Veterans using the CBOCs had no direct access to geriatric specialists without traveling to the clinic, which for some could be up to 200 miles away.
This article describes the lessons learned from the implementation of a Geriatric SCAN-ECHO program, preliminary staff survey and chart review results. The program began in January 2013 and ended in February 2014. The article also offers recommendations to increase understanding of geriatric principles for PCP teams.
The Geriatric SCAN-ECHO Program
After obtaining patient consent, primary care clinicians submitted a consult that included the reason for referral (Figure 1). This list of reasons (eg, behavioral management of geriatric syndromes, care management strategies for patients with dementia, caregiver support strategies, and strategies for the patient to continue living in the community safely) assisted the referring clinician in identifying potential cases that might benefit from a geriatric interdisciplinary case review. Patient approval to contact a caregiver or spouse was requested so the Geriatric SCAN-ECHO team could gather additional information.
After the team received the consult, the gerontological NP or geriatrician reviewed the case and identified other relevant members of the team. The electronic medical record (EMR) was reviewed and a phone call made to the patient and/or their caregiver by the appropriate team member to obtain more information, which could include the patient’s current living situation by the social worker, a medication review by the pharmacist, and functional assessment (eg, basic and instrumental activities of daily living) by the nurse. If appropriate, the geriatrician used the Montreal Cognitive Assessment (MoCA)-BLIND to assess the patient’s cognitive abilities.7 Finally, the team met to reach a consensus on final recommendations and to identify the didactic lecture topic related to the case being reviewed and presented by members of the Geriatric SCAN-ECHO team.
At the start of each SCAN-ECHO session, the geriatrician asked participants 2 to 3 questions on the clinical topic to be covered to elicit interest and motivation to learn. The referring clinician provided a short summary of the case and reason for referral, and the Geriatric SCAN-ECHO team then provided individual findings and recommendations. Due to the complexity of the referrals, the team usually was able to process 1 to 2 cases during the 1-hour session, with 15 minutes allocated for the didactic.
The didactic lectures consisted of evidence-based tools and guidelines that focused on changing provider practice behavior (eg, Assessing Care of Vulnerable Elders criteria) and were posted on the Geriatric SCAN-ECHO SharePoint site after the session for clinicians to download.8 The topics covered included fall risk and prevention; the screening, diagnosis, and management of cognitive disorders; psychosocial considerations in older adults; use of anticholinergic drugs; and assessment and management of unsafe geriatric drivers. Participants were then sent a survey to evaluate the usefulness of the session and its impact on the clinician’s practice. At the end of each session, a summary of findings and recommendations by the geriatric team also was documented in the patient’s EMR and forwarded to the referring clinician. Several factors differentiated the Geriatric from other SCAN-ECHO specialty programs. First, nurses and SWs were invited to place consults, because they were often the first clinicians to identify problems. In a typical SCAN-ECHO program, only PCPs place a consult to the specialty clinic. Second, an interdisciplinary team responded to consults. This was done so that members of the PACT could learn about domains covered by the other disciplines and receive discipline-specific guidance (SCAN-ECHO consults are often answered by a specialist). Third, the team supplemented EMR records with telephone-based assessments. Most SCAN-ECHO programs relied mainly on EMR records.
Facilitators
Although the Geriatric SCAN-ECHO program began in January 2013, the VA Greater Los Angeles Healthcare System facility already had several SCAN-ECHO programs. An experienced SCAN-ECHO project director assisted in the implementation of the program. The specialists used existing documents to guide the program, such as a service agreement between SCAN-ECHO and the participating satellite facilities and templates for consults and documentation. Other benefits of the established SCAN-ECHO presence included availability of videoconferencing equipment; local clinical informatics staff who were familiar with the setup of interfacility consults, clinic encounters, and workload credit in the EMR; and PACT clinicians who were familiar with the SCAN-ECHO program and format. Finally, the geriatric interdisciplinary team members had worked together cohesively for years and were supported by the Geriatric Research Education and Clinical Center to implement clinical demonstration projects, such as the SCAN-ECHO program.
Implementation Barriers
Initially the program received few consults. The Geriatric SCAN-ECHO program used a sample case to start the discussion and focused on falls. At times there were also only a small number of facilities and attendees who participated. Most of the attendees were MDs and NPs from Primary Care and Psychiatry. None of the nurses or SWs who were invited by their local leadership participated early on. Informal communication with CBOC staff found that they were feeling overwhelmed with other competing demands. There were multiple SCAN-ECHO programs and no protected time to attend the sessions. In addition, nurses might not have identified the program as a priority because the training topic was too general (geriatrics vs pressure ulcer or pain management).
The Geriatric SCAN-ECHO program adjusted the timing of sessions to convene every other month on a day that most CBOCs had staff meetings, allowing for protected time for staff participation. The CBOC staff was invited again to participate. The gerontological NP contacted the referring clinician to report the date of the case review and followed up afterward to ensure that all questions were answered and recommendations were clear.
The increase in marketing and networking led to more facilities participating; however, the number of staff participants remained low. The program team then changed tactics and focused on facilitating specific clinician behavior changes related to common geriatric syndromes instead of case reviews. The team conducted a session providing an overview of dementia recognition and diagnosis, rationale for objective measures, and a demonstration on the administration of the Mini-Cog Assessment Instrument for Dementia and Montreal Cognitive Assessment (MoCA) tools.7 This session had the highest number of total attendees (38), half of whom were nurses.
Feedback after the session resulted in an additional session the following month, which focused on the scoring and documentation of the tools as well as interpretation of the results and how this might be further evaluated by the team. Informal feedback gathered from nurses during this second session included a request for more training, tips on how to administer the tools, and how to document competency in tool administration. A new educational project that would empower PACT nurses to proactively identify and initiate cognitive impairment/dementia evaluations was then started independent of the Geriatric SCAN-ECHO program.
Results
Participants of SCAN-ECHO programs were surveyed on usefulness of information and its influence on their practice (Table 1). A total of 41 respondents (the same person may have attended more than 1 session) completed surveys on 9 Geriatric SCAN-ECHO sessions. Nineteen (46%) were medical doctors, 8 (20%) were NPs, and 14 (34%) were from other disciplines. Overall, the sessions were well received, and participants found the information useful. Because the respondents were from different disciplines and roles, it was not surprising that only 13 respondents (32%) felt that the information would influence their prescribing practices, and only 18 respondents (44%) agreed that the session changed their ordering of diagnostic tests and studies.
Chart Reviews
Six months after completion of the Geriatric SCAN-ECHO session, the gerontological NP reviewed patient charts and identified rates of adherence for geriatric team recommendations. Eight patient cases were reviewed in 6 of the 9 sessions. The other sessions used sample cases from the team’s experience due to lack of submitted consults. Physicians referred 4 cases, and the rest were from NPs; all were from primary care except for a primary mental health NP. Half of the referred cases were forwarded from other departments (eg, neurobehavior and dementia clinics) to avoid travel. Reasons for referral included geriatric syndrome workup and specific medical questions. All patients were men aged 66 to 94 years (mean = 83.25; SD = 8.29).
Table 2 lists the frequency and adherence to recommendations. If the recommendation was discussed but refused by the patient, it was still noted as completed. Several recommendations might have been presented; thus, adherence to recommendations was categorized as “all,” “some,” or “not at all” adherent. Because the referrals involved complex cases, most cases were referred to other clinical programs managed by the geriatric specialty team for further evaluation and management.
Discussion
Although the Geriatric SCAN-ECHO sessions were well received, the impact of the program was limited by the lack of consults and PACT team involvement. Impact was markedly improved once the focus of the sessions changed from case studies to specific clinical tool administration/practice change. Leadership support and coordination to provide protected team learning time was essential. Incentives to participate might include making geriatric quality indicators part of performance measures to improve practice and quality of care. Although the VA monitors several frail elderly measures that are a reflection of quality geriatric care, it is up to each VISN to determine its performance measures (Kenneth Shay, e-mail communication, February 12, 2013).
The most frequently followed recommendation was referral to a program managed by the geriatric specialty team. Full compliance with this recommendation may be due to the ease of placing a single consult and the interaction between the SCAN-ECHO team and the geriatric specialty services staff. The next most commonly followed recommendations were for medication changes/review and referral to a different program or clinic (not inpatient or outpatient geriatric specialty programs). Because completion of medication reconciliation reminders are tied to pay incentives for VA physicians, this may explain why it was fulfilled at a higher rates compared with other recommendations, suggesting that bonus incentives could boost participation.
The least frequently completed recommendations were referrals to non-VA programs or specialty providers. This may be a reflection of poor communication with non-VA providers and/or documentation of such communications and lack of the availability of the programs near the patient’s residence. Developing remote site referral guides might improve this communication.
Another type of recommendation that was partially or not at all followed was for further evaluation, assessment, or diagnostic tests of specific problems identified by the Geriatric SCAN-ECHO team. This may be due to lack of easy access to specific diagnostic tests in outpatient clinics or lack of staff knowledge and skills on doing geriatric-specific evaluations. The chart reviewer also noted that even when the PCP did the evaluations, the quality was below standard; for example, for depression screening, the chart noted that the patient was asked about having depression; however, no specific tool was used to aid in the diagnosis. Further specificity regarding geriatric syndrome evaluations and increasing staff knowledge of common tools to aid in diagnosis and evaluation are needed.
In 2 of the 8 cases reviewed, the Geriatric SCAN-ECHO program recommended that specific family members needed to be involved in the care of the patient. Unfortunately, most often family members only were used as a means of communication or for coordination of care with the PACT teams (eg, scheduling appointments). Changes needed to provide quality care for geriatric veterans are to include family members, use a fully-realized PACT approach, and have nurses “practice to the full extent of their education and training,” as recommended by the Institute of Medicine.9
Limitations
This article reported on the experience of a geriatric team that implemented an interdisciplinary telehealth-based consultation program. Facilitators and barriers to program execution may be limited to the local site and VA. The survey following the session was developed by the VA SCAN-ECHO program and was not specific to this local program. Limitations of the chart review include a short follow-up of only 6 months after the program. Many of the behavioral changes or educational recommendations might have been discussed but were not documented. Also services done by non-VA providers might not have been documented and, therefore, would not have been included in this chart review.
Conclusions
The geriatric team decided to discontinue the Geriatric SCAN-ECHO program. The key metric for program success was number of cases reviewed. Only 1 to 2 cases were reviewed every other month. Participation in the program markedly increased when the specific learning needs of PACT teams were addressed; however, most cases were referred to GRECC due to the case complexity and were not appropriate for the SCAN-ECHO format. The chart review, patient and caregiver contact, and presentation preparation required the program staff to invest a significant amount time. It took 3 to 4 hours for the staff to prepare for each case. Furthermore, adherence to recommendations was also poor.
Case-based education and training without follow-up of the recommendations likely is not the best approach to improve care of older veterans in the primary care setting. The authors hope that focusing on specific practice changes and working directly with PACTs and specific team members will be more productive and result in improved outcomes for older veterans. Due to the complexity of geriatric cases involving physical, cognitive, and emotional vulnerabilities, these cases may be better handled by direct multidisciplinary examinations.
Acknowledgments
Funding for this project was supported by the Veterans Health Administration Office of Specialty Care Services T-21 funding initiative.
1. U.S. Department of Veterans Affairs. Geriatric ambulatory care. VHA handbook 1140.10. U.S. Department of Veterans Affairs Website. http://www.va.gov/vhapublications/publications.cfm?pub=2. Published April 26, 2010. Accessed March 9, 2016.
2. Federal Interagency Forum on Aging-Related Statistics. Older Americans 2012: Key Indicators of Well-Being. Washington, DC: U.S. Government Printing Office; 2012.
3. Shay K, Schectman G. Primary care for older veterans. Generations. 2010;34(2):35-42.
4. Institute of Medicine. Retooling for an Aging America: Building the Health Care Workforce. Washington, DC: The National Academies Press; 2008.
5. U.S. Department of Veterans Affairs. Patient centered medical home model concept paper. U.S. Department of Veterans Affairs Website. http://www.vacareers.va.gov/assets/common/print/pcmh_conceptpaper.pdf. Published May 23, 2012. Accessed March 9, 2016.
6. Berenson RA, Devers KJ, Burton RA. Will the patient-centered medical home transform the delivery of health care? Urban Institute Website. http://www.urban.org/sites/default/files/alfresco/publication-pdfs/412373-Will-the-Patient-Centered-Medical-Home-Transform-the-Delivery-of-Health-Care-.pdf. Published August 2011. Accessed March 9, 2016.
7. Nasreddine D. MoCA-BLIND. Version 7.1 Original Version. Montreal Cognitive Assessment Website. http://www.mocatest.org/pdf_files/test/MoCA-Test-BLIND.pdf. Accessed March 9, 2016.
8. RAND Health Researchers. Assessing care of vulnerable elders (ACOVE). RAND Corporation Website. http://www.rand.org/health/projects.acove.html. Accessed March 9, 2016.
9. Institute of Medicine. The future of nursing: leading change, advancing health. Institute of Medicine Website. http://www.iom.edu/Reports/2010/The-future-of-nursing-leading-change-advancing-health.aspx. Published October 5, 2010. Updated October 5, 2015. Accessed March 9, 2016.
1. U.S. Department of Veterans Affairs. Geriatric ambulatory care. VHA handbook 1140.10. U.S. Department of Veterans Affairs Website. http://www.va.gov/vhapublications/publications.cfm?pub=2. Published April 26, 2010. Accessed March 9, 2016.
2. Federal Interagency Forum on Aging-Related Statistics. Older Americans 2012: Key Indicators of Well-Being. Washington, DC: U.S. Government Printing Office; 2012.
3. Shay K, Schectman G. Primary care for older veterans. Generations. 2010;34(2):35-42.
4. Institute of Medicine. Retooling for an Aging America: Building the Health Care Workforce. Washington, DC: The National Academies Press; 2008.
5. U.S. Department of Veterans Affairs. Patient centered medical home model concept paper. U.S. Department of Veterans Affairs Website. http://www.vacareers.va.gov/assets/common/print/pcmh_conceptpaper.pdf. Published May 23, 2012. Accessed March 9, 2016.
6. Berenson RA, Devers KJ, Burton RA. Will the patient-centered medical home transform the delivery of health care? Urban Institute Website. http://www.urban.org/sites/default/files/alfresco/publication-pdfs/412373-Will-the-Patient-Centered-Medical-Home-Transform-the-Delivery-of-Health-Care-.pdf. Published August 2011. Accessed March 9, 2016.
7. Nasreddine D. MoCA-BLIND. Version 7.1 Original Version. Montreal Cognitive Assessment Website. http://www.mocatest.org/pdf_files/test/MoCA-Test-BLIND.pdf. Accessed March 9, 2016.
8. RAND Health Researchers. Assessing care of vulnerable elders (ACOVE). RAND Corporation Website. http://www.rand.org/health/projects.acove.html. Accessed March 9, 2016.
9. Institute of Medicine. The future of nursing: leading change, advancing health. Institute of Medicine Website. http://www.iom.edu/Reports/2010/The-future-of-nursing-leading-change-advancing-health.aspx. Published October 5, 2010. Updated October 5, 2015. Accessed March 9, 2016.