Methods
This study examined attitudes and knowledge about LGBT patient health among 45 primary care providers (PCPs) in 4 VA community-based outpatient clinics (CBOCs). The first clinical question examined whether PCPs desired more education and training on LGBT health. The second clinical question asked whether there were gender differences in attitudes among providers about the need for LGBT health education. Subsequently, the study’s findings are expected to be disseminated to VHA stakeholders to further examine HCP education and training needs on LGBT topics to facilitate improvement of HCP point of care behaviors, patient outcomes, and LGBT empowerment within the VHA environment.
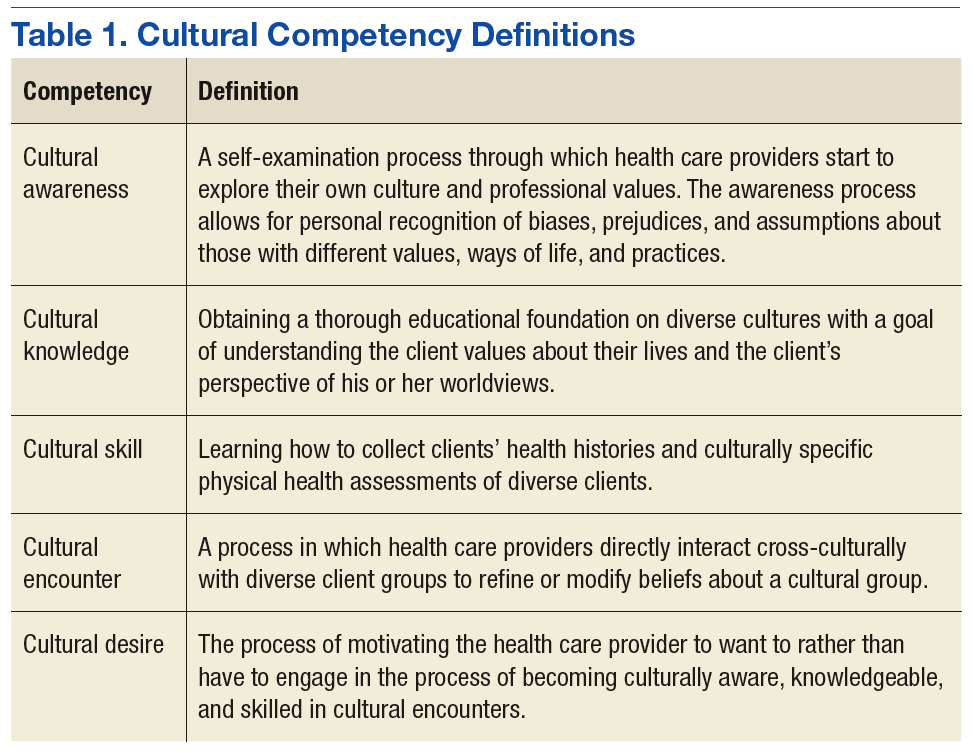
The model presented in The Process of Cultural Competence in the Delivery of Healthcare Services by Campinha-Bacote provides an applicable conceptualization to guide HCPs’ actions toward delivering culturally responsive health care services to increasingly diverse health populations.21 The model defines cultural competence as an ongoing dynamic process of striving to effectively work within the cultural context of the client (person, family, or community). The model integrates 5 constructs that are fundamental to becoming culturally competent to provide appropriate culturally responsive care to diverse clients: cultural awareness, cultural knowledge, cultural skill, cultural encounters, and cultural desires.21 The level of competence of the HCP is believed to have a direct relationship with their ability to provide culturally competent health care services. Table 1 provides the definitions of the 5 constructs and highlights the role of education and training in influencing competence in providing LGBT health services.21
This project used a descriptive, cross-sectional one-group design to target physicians, nurse practitioners (NPs), and physician assistants (PAs) at VA Southern Nevada Healthcare System (VASNHS) CBOCs. Participation in the project was voluntary. The duration of project from data collection to completion of analysis and summation of the results was 4 months. The study was approved by the institutional review board (IRB) at the University of Alabama in Huntsville, and it was exempt from the VA IRB.
The survey consisted of 74 questions, including 8 demographic questions and 66 LGBT-related questions. The survey instrument, renamed the Perception and Knowledge of Sexual and Gender Minority Health (PKSGMH) survey was adapted with permission from an original study by Jabson and colleagues and used its format without revision or restructuring.22
Attitudinal questions asked personal opinions on LGBT orientation and gender identity (eAppendix:
) For example, is being LGBT right, wrong, or disgusting? Is LGBT a natural expression of sexuality or gender identity? Did providers feel competent in giving LGBT care; would providers prefer not to provide LGBT care; could providers give LGBT care in a sensitive manner? Was medical training adequate to address the needs of LGBT patients? Knowledge questions asked about the prevalence of depression, anxiety, obesity, alcohol, drug abuse, tobacco, obesity, STDs and chronic diseases in LGBT populations. Belief questions asked about respect for LGBT clients, the need for more training, education, and skills in LGBT care, and provider awareness of antidiscrimination and visitation policies in the workplace.Measures
The survey instrument integrated components of 4 different measures on attitudes and knowledge of LGBT health with questions about familiarity with organizational policies on discrimination, visitation, and staff training in LGBT care. The PKSGMH survey measured attitudes and knowledge levels on LGBT health by calculating the mean scores for each of 4 measures.
General Attitudes Toward LGBT Nonpatients. The attitudes toward LGBT nonpatients measure includes 4 subscales with 3 identical questions on how providers felt about LGBT individuals: (a) attitudes toward lesbians (α: .78); (b) attitudes toward gay men (α: .76); (c) attitudes toward bisexuals (α: 78); and (d) attitudes toward transgender people (α: .70). Each subscale used a 5-point Likert scale (5 = strongly agree).
Physician Attitudes Toward LGBT (ATLG) Patients. The attitudes toward LGBT scale assessed physicians’ feelings toward providing care to LGBT patients. This scale of 6 questions had modest reliability with a Cronbach α of .5. The measure used a 5-point Likert scale (5 = strongly agree). For this project, this scale was renamed the Provider subscale.
Knowledge of LGBT (KLGBT) Patients. The knowledge of LGBT patients’ scale included 13 true/false questions and had a Cronbach α of .74.
Gender and Sexual Minority Affirmative Practice (GSMAP). The GSMAP affirmative practice scale evaluated HCPs’ attitudes and beliefs about the treatment of LGBT patients. The 11-question measure with 2 subscales used a 5-point Likert scale with high reliability on the clinicians’ beliefs and behaviors subscales. Both subscales had a Cronbach α of .93 and .94, respectively.
Demographics and Data Analyses
Health care providers answered demographic questions about gender, sexual orientation, and marital status. They also were asked whether they had ever received any focused training in LGBT patient care. Descriptive and demographic data analyses were performed using SPSS version 24.0 (Armonk, New York). A significance level of P < .05 was used for all analyses. Analysis of variance (ANOVA) statistical analysis was conducted to evaluate the differences in mean scores between male and female PCP groups on the 4 attitudes toward LGBT subscales and the Provider subscale.
