Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
Author Affiliations Rebecca Rottman-Sagebiel, Nicole Cupples, and Stephanie Pastewait are Clinical Pharmacy Specialists; Chen Pin Wang is a Biostatistician; Seth Cope and Hanna Braden are Medical Students; Daniel MacCarthy is a Data Analyst; Melody Moris is a Project Manager; Eneida-Yvette Gonzalez is a Program Support Assistant; Alicia Conde is a Research Assistant and Sara Espinoza is a Geriatrician at the University of Texas Health Science Center in San Antonio; all at the Geriatrics Research, Education and Clinical Center (GRECC) at the South Texas Veterans Health Care System (STVHCS) in San Antonio, Texas.
Patients were excluded if they were expected to be discharged to any facility where the patient and/or the caregiver were not primarily responsible for medication administration after discharge. Patients who met eligibility criteria but were not seen by the transitional program pharmacist (due to staff capacity) were included in this analysis as a convenience comparison group of patients who received usual care. Patients were not randomized. All communication occurred in English, but this project did not exclude patients with limited English proficiency.
A program support assistant conducted the daily query of the hospital database. The pharmacist conducted the chart review to determine eligibility and delivered the intervention. Eligible patients were selected at random for the intervention with the intention of providing the intervention to as many veterans as possible.
The GMED Intervention
The GMED program included 2 phases, which were both conducted by a CPS with oversight from a senior CPS with geriatric pharmacology expertise and an internist/geriatrician.
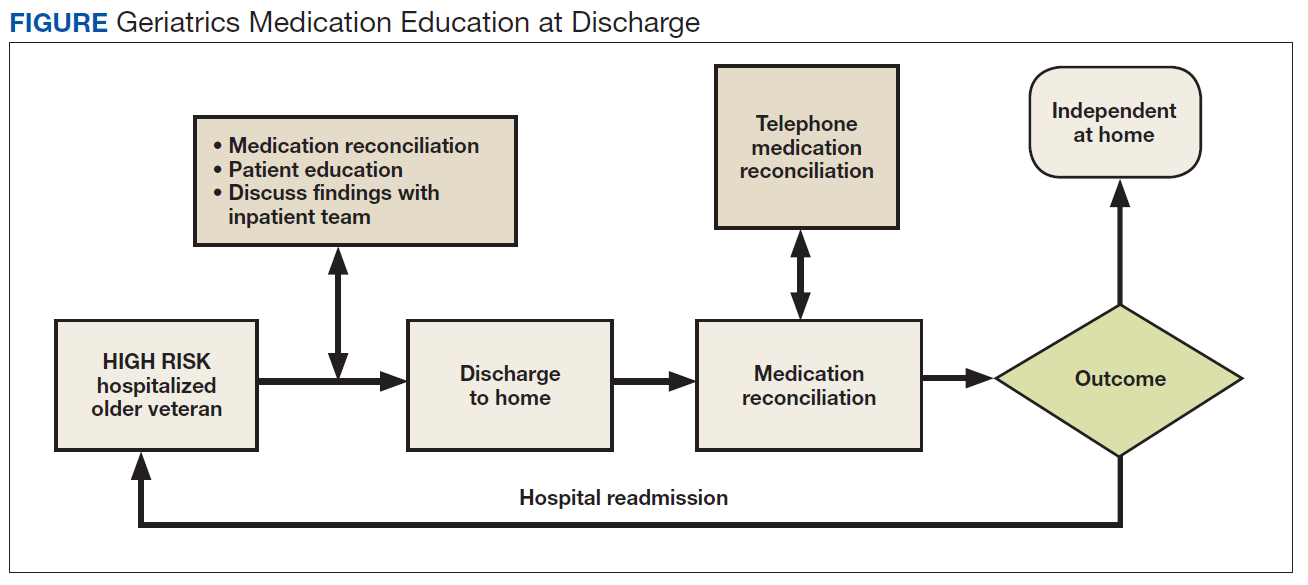
The CPS carrying out the transitional care program was involved in the planning and design of the project and met weekly with the geriatrician. The Figure provides an overview of the intervention.
The first phase of the transitional care program included an individual, face-to-face meeting between the CPS and the patient during the hospitalization. If a veteran was not present in the room at the time of an attempted visit, the pharmacist made 2 additional attempts (3 total) to include the patient in the transitional care program during the hospitalization.
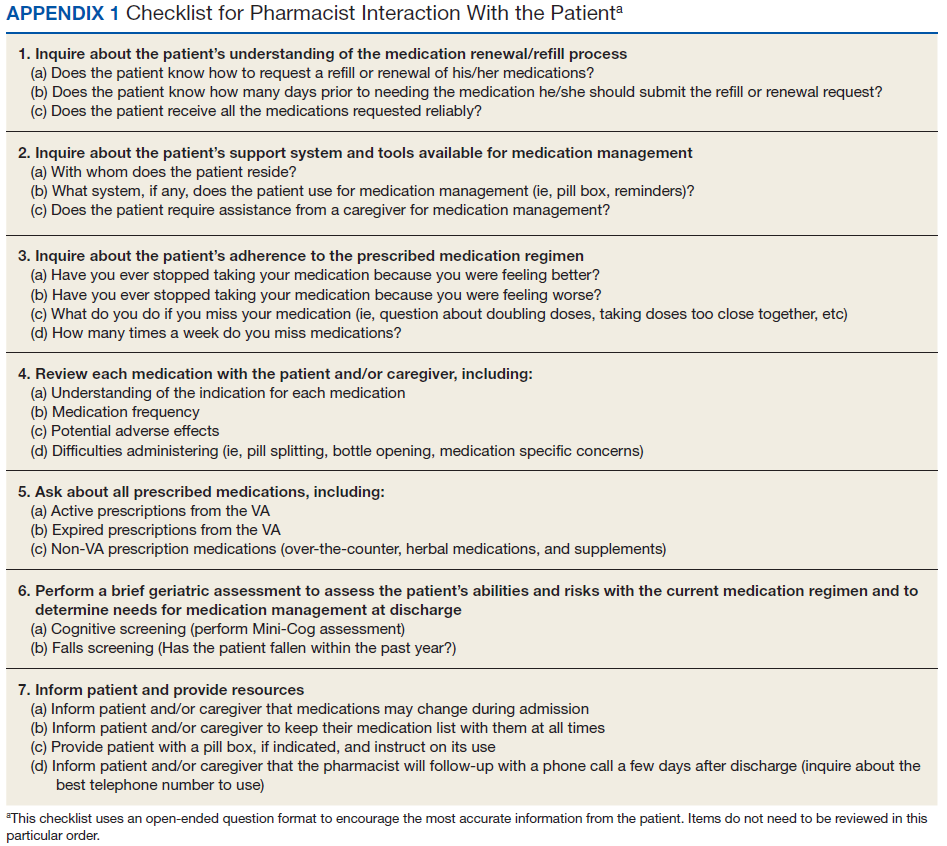
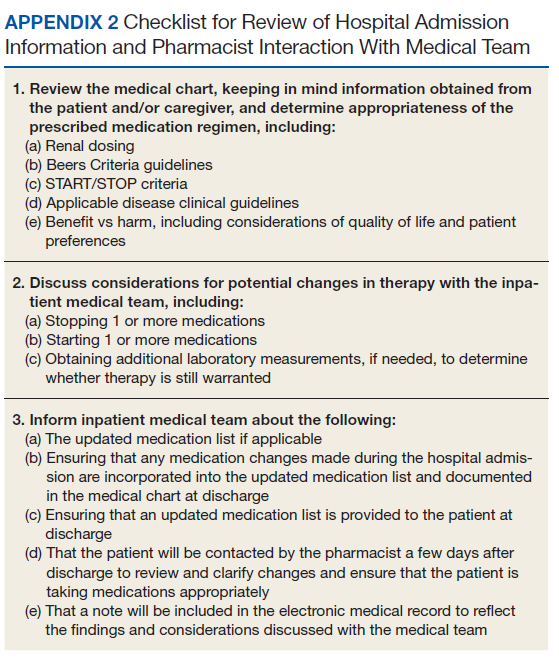
The CPS performed medication reconciliation and provided medication education regarding administration and usage of the patient’s medications, using an open-ended format.11 The caregiver, if any, was included in the discussion either at the bedside or by telephone following the face-to-face visit with the patient. The CPS communicated recommendations regarding appropriateness of therapy (including any potential barriers to medication adherence) to the medical team (including the attending, resident[s], and interns) in person or by telephone and through documentation in the CPRS.
The recommendations were based on the clinical expertise of the CPS as well as on guidelines for prescribing in older adults.10,12 The CPS used a checklist to ensure all components of the intervention were completed (Appendices 1 and 2).
The second component of the transitional care program included a telephone visit within 2 to 3 days of discharge, conducted by the same CPS who performed the face-to-face visit. The purpose of the telephone visit was to perform medication reconciliation, identify and rectify medication errors, provide further patient education, and assist in facilitating appropriate follow-up by the patient’s primary care provider (PCP), if required. At a minimum, veterans were asked a series of questions pertaining to their concerns about medication regimens, receipt of newly prescribed medications at discharge, additional education regarding medications after the CPS encounter during hospitalization, and whether the veteran required assistance with the medication regimen in the home setting. Follow-up questions were asked as needed to clarify and identify potential medication problems. All information from this telephone encounter was communicated to the PCP through CPRS documentation and by telephone as needed.