Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
Author Affiliations Rebecca Rottman-Sagebiel, Nicole Cupples, and Stephanie Pastewait are Clinical Pharmacy Specialists; Chen Pin Wang is a Biostatistician; Seth Cope and Hanna Braden are Medical Students; Daniel MacCarthy is a Data Analyst; Melody Moris is a Project Manager; Eneida-Yvette Gonzalez is a Program Support Assistant; Alicia Conde is a Research Assistant and Sara Espinoza is a Geriatrician at the University of Texas Health Science Center in San Antonio; all at the Geriatrics Research, Education and Clinical Center (GRECC) at the South Texas Veterans Health Care System (STVHCS) in San Antonio, Texas.
Transitional care program status was determined whether or not the individual received the transitional care program for each index admission. This analysis allowed us to model repeated measures of index admissions as a function of the project period and whether the patient was seen by the GMED CPS during the index admission. The patient identifier was used as a cluster variable in the GEE analysis. Inverse propensity scores of receiving GMED at the index admission were adjusted as weights in the GEE analysis to minimize confounding and, hence, to strengthen the causal interpretation of the effect of the transitional care program. If there was ≥ 1 index admission, the GMED status (yes vs no) at the initial index admission was used as the dependent variable to calculate propensity scores. The propensity scores of transitional care program status were derived from the logistic regression analysis that modeled the log-odds of receiving the transitional care program at the index admission as a linear function of age, CCI, frailty, and prior hospitalization during the 1-year period prior to the index admission.
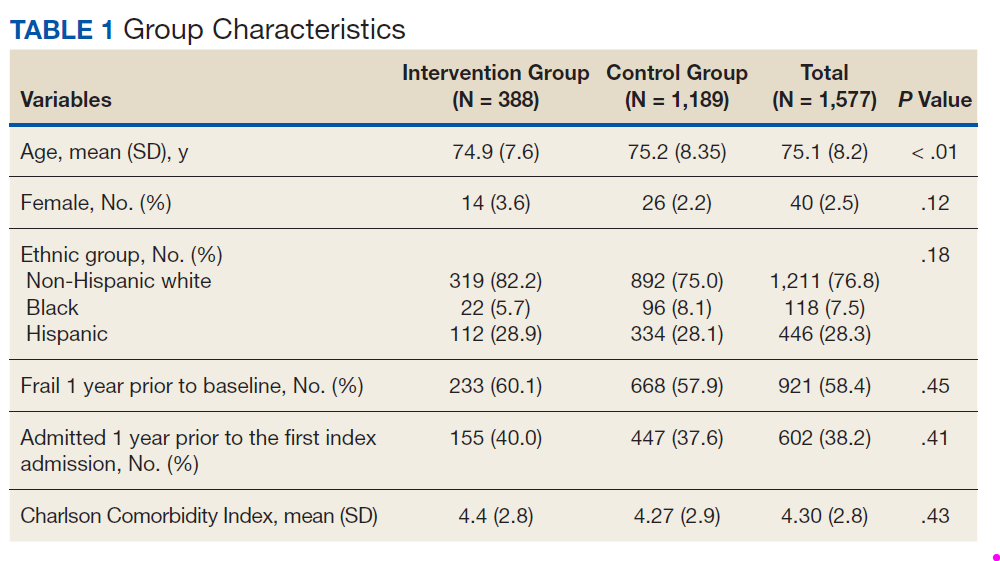
The GMED CPS saw 435 patients during the project period; 47 (10.8%) died prior to 30 days and were excluded, leaving 388 patients who received the transitional care program included in this evaluation.
Another 1,189 patients met the eligibility criteria but were not included and were included in the comparison group. Patients in the transitional care program group were similar to those receiving usual care in the comparison group with regard to sex, ethnic group, frailty status, and CCI score (Table 1).
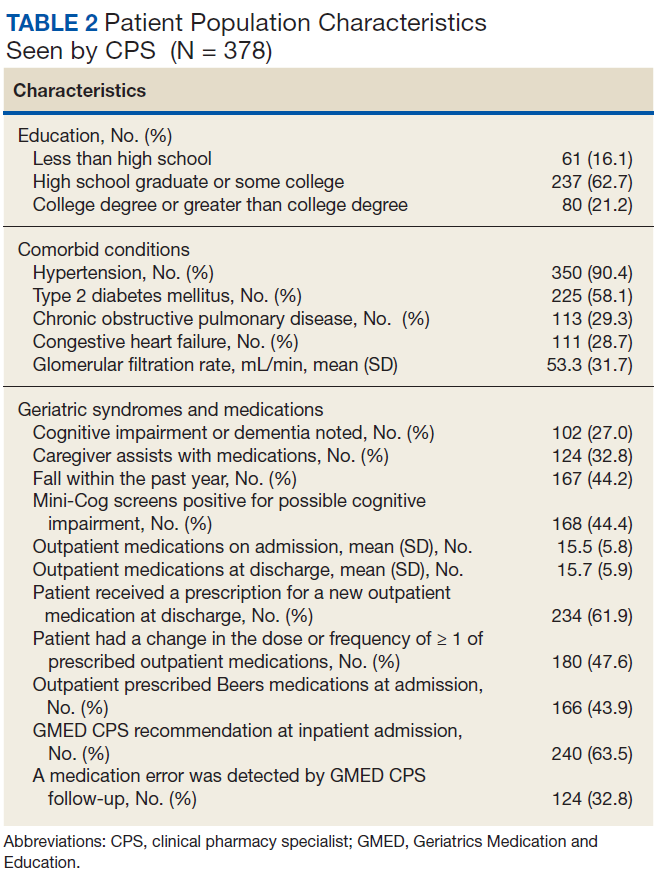
Data from the CPS-patient interviews and chart reviews were available for 378 of the 388 patients (Table 2). Patients were primarily male, non-Hispanic white, with a high school education. More than half (65%) the patients were admitted for a new diagnosis or clinical condition.
The majority of patients had diabetes mellitus, and about one-third had chronic obstructive pulmonary disease, congestive heart failure, or cognitive impairment. Although about 60% of patients were prescribed a new medication as a result of the hospital admission, the number of medications from admission to discharge did not differ significantly (15.4 ± 5.5 vs 15.7 ± 5.8; P = .08).
The 30-day readmission rate was 15.6% for the transitional care program group and 21.9% for the comparison group. Three hundred seventy-one patients received the transitional care program only once, 16 patients received the transitional care program twice (ie, they had 2 index admissions during the study period and received the intervention both times), and 1 patient received the transitional care program 3 times.
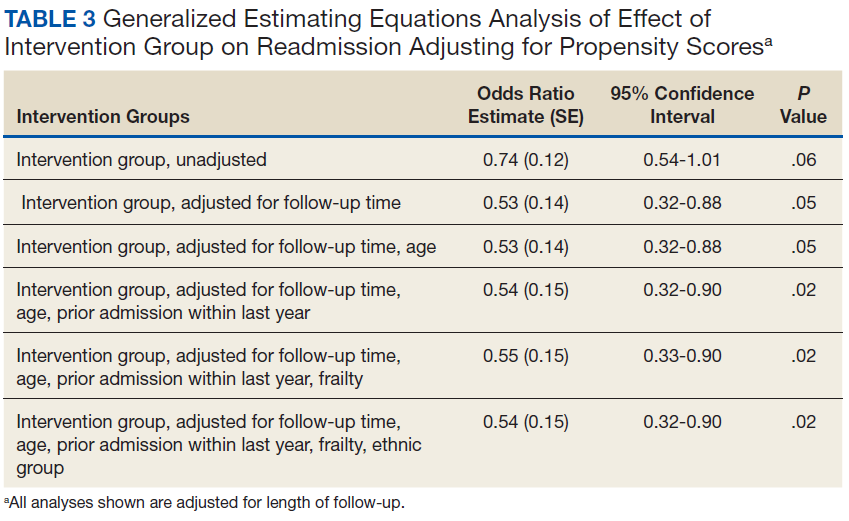
In an unadjusted GEE model, the odds ratio (OR) for readmission in the transitional care program group was 0.74 (95% CI, 0.54-1.0, P = .06) compared with the usual care group (Table 3).
After covariate adjustment, the OR for readmission was 0.54 (95% CI, 0.32-0.90, P = .02).
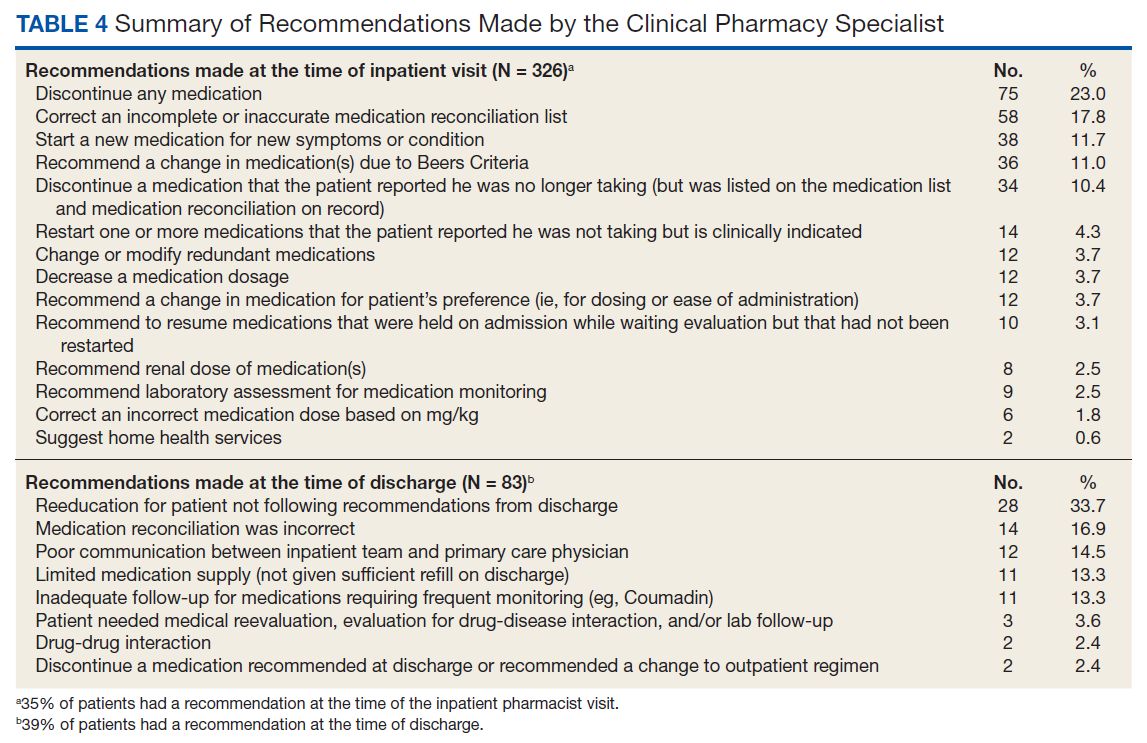
Thirty-five percent of patients had ≥ 1 CPS-recommended change in their treatment at the time of the inpatient admission (Table 4).
The most common recommendation was discontinuation of at least 1 medication (23.0%), followed by correcting the medication reconciliation list that was on record for the admission (17.8%). Thirty-nine percent of patients had ≥ 1 CPS-recommended change in their treatment at the time of the follow-up phone call. The most common recommendation was to clarify medication instructions for the patient and/or caregiver and provide medication education (33.7%). Other common recommendations were to correct a medication reconciliation (16.9%) and communicate pertinent information about the admission to the PCP (14.5%).