Kathryn Tortorice is National PBM Clinical Pharmacy Program Manager at Edward Hines, Jr. VA Hospital in Hines, Illinois. Natasha Antonovich is Clinical Pharmacy Program Manager at US Department of Veterans Affairs VISN 8 Pharmacy Benefits Management in Orlando, Florida. Correspondence: Kathryn Tortorice (kathy.tortorice@va.gov)
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Introduction/Importance: Pharmacotherapy for multiple sclerosis has increased significantly since 1993 when the first disease modifying therapy was approved. The expansion of therapies has been accompanied with differences in adverse effect profiles, efficacy, and cost. The most recent therapies pose the challenge of balancing these issues while providing optimal care.
Observations: Several measures such as generic conversion and standardization of therapies can be employed to control costs of therapy. The safety and efficacy of these agents can be monitored by implementation of criteria for use and/or medication utilization evaluations.
Conclusions: A formulary management system encompasses methodologies to evaluate the relevant clinical and medical literature and includes a systematic approach for selecting medications for different diseases, conditions, and patients. Formulary systems often contain prescribing guidelines and clinical recommendations that assist health care professionals with providing high quality, value-based care for patients.
Prior to the first approved disease modifying therapy (DMT) in the 1990s, treatment approaches for multiple sclerosis (MS) were not well understood. The discovery that MS was an immune mediated inflammatory disease paved the way for the treatments we know today. In 1993, interferon β‐1b became the first DMT for MS approved by the US Food and Drug Administration (FDA). Approvals for interferon β‐1a as well as glatiramer acetate (GA) soon followed. Today, we consider these the mildest immunosuppressant DMTs; however, their success verified that suppressing the immune system had a positive effect on the MS disease process.
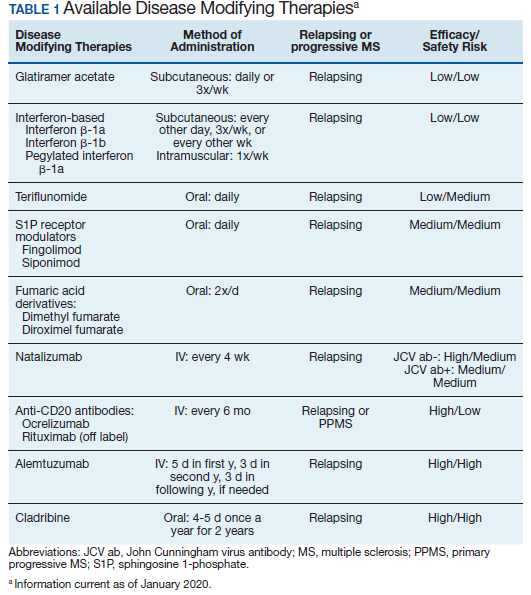
Following these approvals, the disease process in MS is now better understood. Recently approved therapies include monoclonal antibodies, which affect other immune pathways. Today, there are 14 approved DMTs (Table 1). Although the advent of these newer DMTs has revolutionized care for patients with MS, it has been accompanied by increasing costs for the agents. Direct medical costs associated with MS management, coupled with indirect costs from lost productivity, have been estimated to be $24.2 billion annually in the US.1 These increases have been seen across many levels of insurance coverage—private payer, Medicare, and the Veterans Health Administration (VHA).2,3
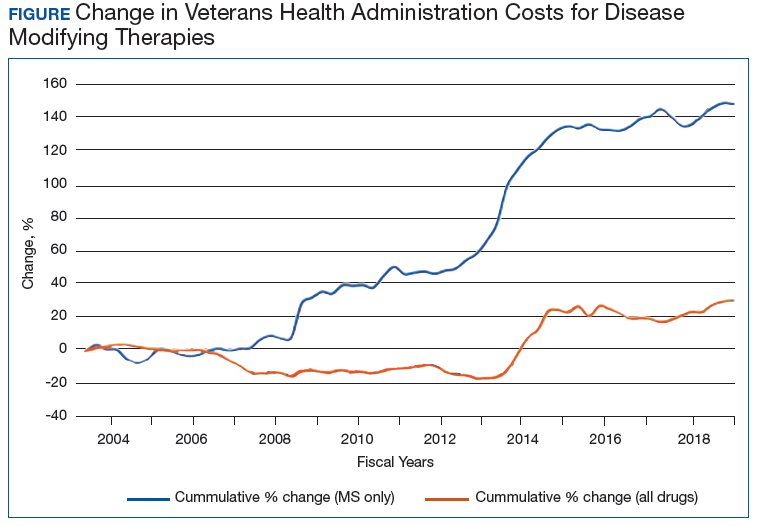
The Figure demonstrates the cost increase that have been seen across VHA between 2004 and 2019 for the DMTs identified in Table 1. Indeed, this compound annual growth rate may be an underestimate because infusion therapies (eg, natalizumab, ocrelizumab, and alemtuzumab) are difficult to track as they may be dispensed directly via a Risk Evaluation Medication Strategy (REMS) program. According to the VHA Pharmacy Benefit Management Service (PBM), in September 2019, dimethyl fumarate (DMF) had the 13th highest total outpatient drug cost for the US Department of Veterans Affairs (VA), interferon β‐1a ranked 62nd and 83rd (prefilled pen and syringe, respectively), and GA 40 mg ranked 89th.
The DMT landscape has demonstrated significant price fluctuations and given rise to a class of medications that requires extensive oversight in terms of efficacy, safety, and cost minimization. The purpose of this article is to show how delivery of this specialty group of medications can be optimized with safety, efficacy, and cost value within a large health care system.