Retrospective Chart Review of Advanced Practice Pharmacist Prescribing of Controlled Substances for Pain Management at the Harry S. Truman Memorial Veterans’ Hospital
Courtney Kominek is a Clinical Pharmacy Specialist–Pain Management at the Harry S. Truman Memorial Veterans’ Hospital in Columbia, Missouri. Correspondence: Courtney Kominek (courtney.kominek@va.gov
Author disclosures The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the author and does not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Disclosures Dr. Kominek has received honoraria from Practical Pain Management, PAINWeek, and the American Society of Health-System Pharmacists.
Background: The US Department of Health and Human Services’ 5-point strategy to combat the opioid overdose public health crisis includes improved pain management. There is a shortage of adequately trained health care providers in pain management. Advanced practice pharmacists may be able to help fill that void. The objective of this project was to identify the impact of an advanced practice pharmacist with controlled substance prescriptive authority on morphine milligram equivalent dose (MME) and compliance with opioid risk mitigation.
Methods: In March 2020, a single-site retrospective chart review was conducted of patients who were prescribed controlled substances from July 1, 2018 to January 31, 2020. Patients received care through the outpatient Pharmacy Pain Clinic in-person or via telephone who were enrolled at the Harry S. Truman Memorial Veterans’ Hospital in Columbia, Missouri, or associated outlying outpatient clinics. Patients were included if they were referred to the Pharmacy Pain Clinic and prescribed a Schedule II or III opioid medication. A 2-sided t test was conducted to compare MME, and a Fisher exact test was used to compare adherence to opioid risk mitigation.
Results: Patients seen in Pharmacy Pain Clinic had a statistically significant reduction in MME from consult (93 MME) to discharge (31 MME) ( P < .01). There was also a statistically significant ( P < .01) improvement in use of opioid risk mitigation strategies, including urine drug screen, informed consent, naloxone, prescription drug monitoring program checks, and stratification tool for opioid risk mitigation dashboard reviews.
Conclusions: An advanced practice pharmacist with controlled substance prescriptive authority improved patient care with demonstrated statistically significant differences in MME and adherence with opioid risk mitigation from consult to discharge. Health care teams should look to add advanced practice pharmacists to their team as medication experts to deliver comprehensive medication management, which can include controlled substance prescribing and management.
In the midst of an opioid overdose public health crisis, the US Department of Health and Human Services developed a 5-point strategy to combat this problem. One aspect of this strategy is improved pain management.1 There is high demand for pain management services with a limited number of health care professionals appropriately trained to deliver care.2 Pharmacists are integral members of the interdisciplinary pain team and meet this demand.
Background
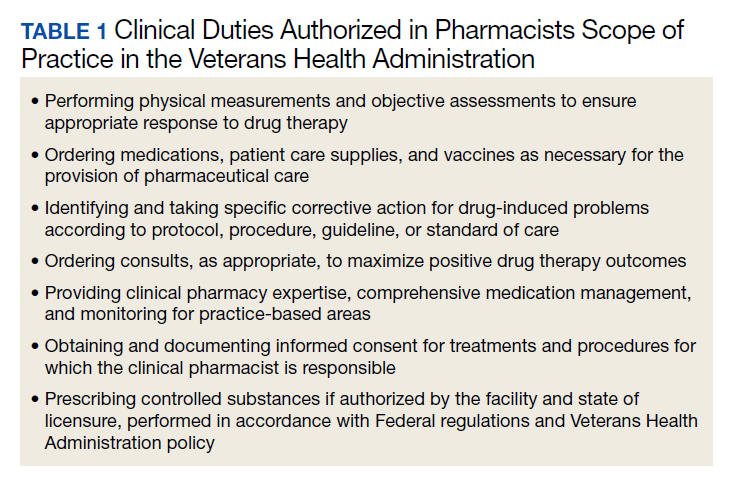
For almost 50 years, pharmacists at the US Department of Veterans Affairs (VA) have been functioning as advanced practice providers (APP).3 Clinical pharmacy specialists (CPS) provide comprehensive medication management (CMM) and have a scope of practice (SOP). The SOP serves as the collaborating agreement and outlines the clinical duties permitted in delivering patient care. In addition, the SOP may indicate specific practice areas and are standardized across VA (Table 1).4,5 Pharmacists apply for a SOP and must prove their competency in the practice area and provide documentation of their education, training, experience, knowledge, and skills.5,6 Residency and/or board certification are not required though helpful. A pharmacist’s SOP is reviewed and approved by the facility executive committee.5 Pharmacists with a SOP undergo professional practice evaluation twice a year. Prescribing controlled substances is permissible in the SOP if approved by the facility and allowed by the state of licensure. According to the US Drug Enforcement Agency (DEA) as of February 10, 2020, 8 states (California, Washington, Idaho, Massachusetts, Montana, New Mexico, North Carolina, and Ohio) allow pharmacists to prescribe controlled substances.7
The VA developed the Pharmacists Achieve Results with Medications Documentation (PhARMD) tool that allows clinical pharmacists to document specific interventions made during clinical care and is included in their progress note. Data from fiscal year 2017 demonstrates that 136,041 pain management interventions were made by pharmacists across VA. The majority of these interventions were implemented by a CPS working autonomously as an APP.8
Several articles discuss the pharmacists role in the opioid crisis, although no outcomes data were provided. Chisholm-Burns and colleagues listed multiple potential ways that pharmacists can intervene, including managing pain in primary care clinic settings by using collaborative drug therapy agreements (CDTAs), using opioid exit plans and discharge planning in collaboration with other health care providers (HCPs), or making recommendations to the prescribers before writing prescriptions.9 Compton and colleagues similarly reviewed pharmacist roles in the opioid crisis. However, their focus was on dispensing pharmacists that provided education to patients about storage and disposal of opioids, identified opioid misuse, provided opioid overdose education and naloxone, and checked prescription drug monitoring programs (PDMPs).10 Missing from these articles was the role of the clinical pharmacist working as an APP delivering direct patient care and prescribing controlled substances.
Hammer and colleagues discussed the role of an oncology CPS with controlled substance prescriptive authority in pain management at an outpatient cancer center in Washington state.11 Under a CDTA, pharmacists could prescribe medications, including controlled substances if they obtain DEA registration. The pharmacist completed a comprehensive in-person assessment. The attending physician conducted a physical examination. Then the pharmacist presented the patient and proposed regimen to the interprofessional team to determine a final plan. Ultimately, the pharmacist wrote any controlled substance prescriptions. The patient followed up every 1 to 4 weeks by telephone with a nurse, and in-person assessments occurred at least every 6 months. No outcomes data were provided.11
Dole and colleagues reviewed the role of a pharmacist who had controlled substance prescriptive authority in a pain management clinic. The pharmacist provider saw up to 18 patients a day and then managed refill requests for 3 hours a day. The main outcome was change in visual analog scale (VAS) pain scores. Findings showed that reductions in VAS pain scores were statistically significant (P < .01). The pharmacist processed about 150 refills with an unclear number of controlled substances requests a day based on a medication-refill protocol. This was felt to improve access to physicians for acute needs, improve consistency in refills, and capture patients in need of follow-up. Additionally, the clinic saved $455,238 after 1 year.12