Studies analyzing the causes of and patterns associated with polypharmacy have increased over the past decade.1-3 Disadvantages to polypharmacy include but are not limited to higher risk of drug-drug interactions, greater potential for adverse effects (AEs), higher risk of nonadherence, and higher costs for the patient and health care systems.1 Compounding the disadvantages associated with polypharmacy, medication storage and disposal are areas of environmental concern. A recent study by Wieczorkiewicz and colleagues examined how patients use, store, and dispose of medications and found that “almost all respondents had excess and leftover medications in their homes.”4 The authors concluded that both overprescribing and poor medication adherence contribute to excess medications at home.
As health care systems become more fiscally responsible, it is beneficial to review prescribing and dispensing patterns, which contribute to polypharmacy and excess medications in patient homes. One of the specific areas that came to the attention of the authors was the number of medication returns received at Evans Army Community Hospital (EACH). As Wiesczorkiewicz and colleagues discovered, it is common that medicine cabinets are filled with expired drugs or medications no longer in use. Although some of these medications can be disposed of in the trash or toilets, some facilities take back unused drugs.5
In an attempt to keep patients and the environment safe, EACH takes back unused medications daily for destruction. These patient returns must be destroyed for both legal and ethical reasons, because there is the potential that medications that have left the system may have been adulterated. The purpose of this quality improvement (QI) project was to evaluate the cost of patient medication returns and explore any additional sources of waste in the prescribing and dispensing processes.
As a QI project assessing current prescribing and dispensing processes and improving patient-centered performance, Institutional Review Board approval was not required. The QI project and manuscript submission did receive approval from the EACH Command Team. Patient prescription returns were collected at the main and outlying hospital pharmacies between December 16, 2012, and April 5, 2013. Patients were encouraged to bring all medications to clinic visits, and if it was determined that the patient was no longer taking the medication or that the medication was discontinued, the clinician would bring the medication(s) to the patient return collection bin for destruction.
Related: New Guidance on Compounded Drugs
Patients also presented medications no longer used to the pharmacy for the patient return collection bin. A pharmacy technician recorded the medication name, strength, original amount prescribed, and the number of tablets/capsules remaining in the vial. Quantities dispensed greater than the quantities prescribed were later segregated for additional analysis. The brand name of the product was recorded only when the brand name was dispensed. The cost per unit was obtained from the pharmaceutical distributor and recorded to quantify the total cost of each prescription and the total cost of the medications returned. Medications that were classified as hazardous waste were assessed, as were all other medications, and then were segregated to the hospital’s satellite accumulation point for disposal by the Directorate of Public Works Environmental Division. Partial creams and ointments were excluded from the analysis, because the total amount returned was not easily quantifiable.
The total value of the medications collected from December 16, 2012, through April 5, 2013, was $63,183 (1,174 prescriptions). Furthermore, there was the cost of the vials; printer ink; labels; labor to pay pharmacists to process, check, and dispense the medications; and the time of technician staff to fill the prescriptions and later sort the medications to look for hazardous waste and controlled substances. These additional expenses were not quantified and therefore were not included in the aforementioned value.
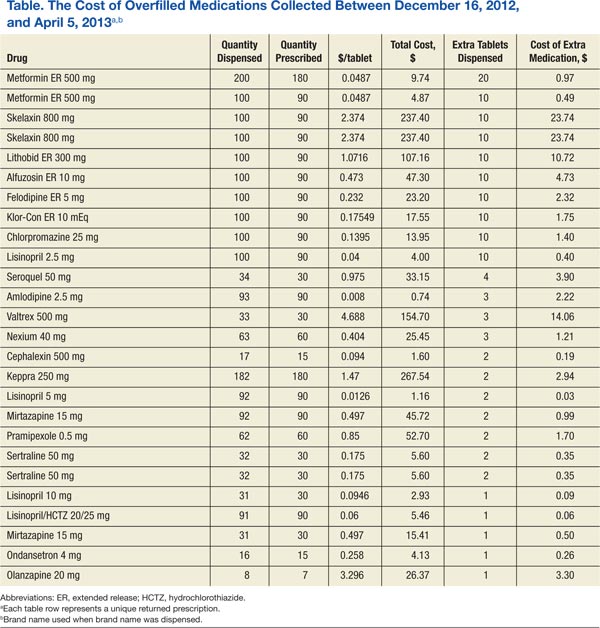
A subanalysis was conducted after it was observed that several prescriptions had greater quantities dispensed than the quantity prescribed (Table). An excess of $102.41 was dispensed and later collected during the study period. Of the 26 prescriptions that were overfilled, 10 were not due to human error but were intentionally overfilled as evidenced by sealed manufacturer bottles; the cost of the medications overfilled for these 10 prescriptions was $70.26.
The top returned drugs in descending order were lisinopril (42), bupropion (32), prazosin (28), gabapentin (27), and ondansetron (26). The top classifications of medications returned in descending order were antidepressants (198), antihypertensives (185), anticonvulsants (61), antilipemics (60), antibiotics (57), and antipsychotics (57). Also noteworthy is that a total of 91 prescriptions (7.8%) for over-the-counter (OTC) products were returned.
As suggested by Wieczorkiewicz and colleagues, prescribing and dispensing patterns may be contributing to the accumulation of unwanted and unused medications.4 Patient feedback would also give insight to this problem. Furthermore, the data highlighted improvement opportunities related to back order/shortage and high-dollar medications. Additional exploration into prescribing, dispensing, and consumer patterns as well as potential cost-saving strategies addressing the aforementioned processes is warranted.