User login
Dr. Baum describes his number one strategy to retain patients (Audiocast, March 2013)
Pillar 2: Attract new patients (May 2013)
Pillar 3: Obtain and maintain physician referrals (June 2013)
Pillar 4: Motivate your staff (August 2013)
The medical landscape has changed. No one is quite certain what the future will hold. One thing we do know: 20 million more Americans, half of them women, will enter the health-care system in the very near future, as the Affordable Care Act continues to unfold. This flood of new patients will affect nearly every ObGyn practice in the country because we lack an adequate increase in the number of physicians to care for them. In the meantime, what can you do to ensure the continued success of your practice? This series focuses on four key areas. I call them the “four pillars”:
- Keep existing patients happy
- Attract new patients
- Nurture relationships with your medical colleagues and other health-care providers, such as physician assistants and nurse practitioners
- Maintain the morale of your staff.
No pillar is more important than the others; all four are necessary to guarantee success.
It is more cost-effective to keep an existing customer than to attract
a new one
In this article, I explain why it is vital to ensure that every patient has a positive experience of your practice, from the moment they make their first telephone call for an appointment, through their wait in the reception area, to the moment they are seen by the staff or the physician, and beyond—when they tell others about their stellar experience.
It’s nice to get new patients, but it is more important to keep the ones you already have. In most professions and businesses, the cost of keeping an established customer is one-fifth the cost of acquiring a new one. Medical practices are no exception. If you are not doing a good job with the patients you already have, spending thousands of dollars on a marketing plan to bring in new patients is pointless. The patients you have right now are the backbone of your practice.
Give your practice a checkup
Look at your practice from your patients’ perspective
Today, it is critical to know the needs and expectations of your patients and referring physicians. The best way to do this is to ask your patients what they think, which also will reveal your practice’s strengths and weaknesses. This information can be obtained easily by surveying patients about various aspects of your practice. (Even practices that are full or closed need to evaluate their services periodically and listen to their patients. Changes always occur, and the cup may not “runneth over” forever.)
Tom Peters, the nationally renowned author of In Search of Excellence, has described two keys to success in business:
- Find out what the customer (patient) wants and give him or her more of it
- Find out what the customer (patient) does not want and be sure to avoid it.
Techniques to gather the patient’s perspective
There are five effective techniques for determining how patients perceive your practice and for evaluating your performance and reputation:
- Conduct personal interviews
- Conduct patient surveys
- Create a focus group
- Use a suggestion box
- Commission evaluation by a mystery shopper.
Although I have used all five techniques, my favorite and most cost-effective involves a survey card that is given to every patient on every office visit (FIGURE 1). The card is given to the patient when she checks in, and she can complete it in the reception area or exam room and return it to the receptionist before leaving the practice. The cards are reviewed by a nurse, who addresses positive and negative comments. Most negative comments are addressed with a phone call. If necessary, I respond to the patient’s complaint.
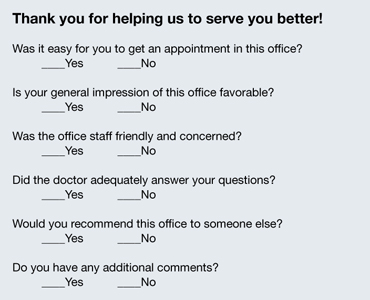
FIGURE 1: Patient survey card
There is another benefit to the survey card. The flip side of the card prompts the patient to write down the three questions she would like you to address on her current visit to the office (FIGURE 2). Conducting the appointment according to these concerns can help keep patients from initiating a last-minute discussion, often after you have closed the chart or electronic medical record, that you don’t have time to address adequately. Since my office has implemented use of this survey card, we seldom get follow-up phone calls from patients about issues they forgot to ask about. The survey card demonstrates that we are listening to the patient and want to be certain that all her questions have been answered at the time of her office visit.
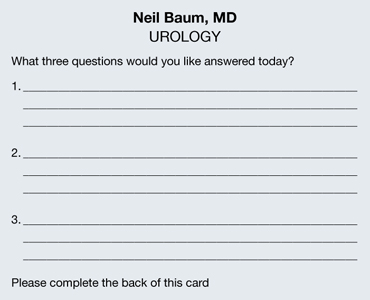
FIGURE 2: Focus of the appointment
Develop an on-time practice philosophy
You know the adage: Timeliness is next to godliness. (Actually, it’s cleanliness that’s next to godliness, but timeliness is vital, too.) The most common complaint patients have about the health-care experience is “waiting for the doctor.” Spending time in the reception area probably accounts for more patient dissatisfaction than any other aspect of medical care. In one recent survey, nearly one in four patients (24%) claimed to have waited 30 minutes or longer. With so many more women entering the marketplace, this statistic is only going to get worse.
In order to gain an accurate picture of what is happening in regard to the schedule in your practice, I suggest conducting a “time and motion” study. For a period of 3 to 5 days, place a sheet on each patient’s record or superbill and log in the following:
- time of her appointment
- time she arrived
- time she left the office
- how much time she spent with her physician.
You will be amazed to discover that patients are waiting 1 or 2 hours or longer to see the physician, and that the physician is spending only 5 minutes with the patient. Ask any patient on a survey if she feels she is getting bang for her buck, and she will answer, “No!”
By conducting a time and motion study, you will discover that there are predictable periods when backlogs occur. Often, these delays are the result of “working a patient in” to the schedule. Unscheduled patients who call to report vaginal bleeding, pelvic pain, urinary tract infection, or another problem are often told to come in without an appointment, but they inevitably displace women already scheduled and delay their visit. This problem affects almost every ObGyn.
One way to avoid this scenario is to create “sacred” time slots. These are 15-minute intervals at the end of the morning or afternoon in which unscheduled patients can be worked into the round of visits. Instead of telling the patient to “just come in,” I tell her to report at a specific time. These time slots cannot be filled with routine appointments. Nor can they be filled prior to 9 am each day. This leaves two or three slots open for patients who must be seen immediately.
Few ObGyns can change health-care policy. But all of us can be more sensitive to our patients’ time and make an effort to see them as soon as possible, thereby eliminating one of patients’ most common complaints: the long wait to see their doctor.
Make the patient’s experience memorable
All of us can provide a diagnosis and treatment strategy for most women’s medical problems. But how many of us can make the experience memorable for the woman? Often, it is a few little things that can be easily and inexpensively performed that make a big difference.
Go with cloth, not paper. There’s a sharp contrast between a paper sheet, a paper gown, and a soft robe. You don’t step out of the shower in a fine hotel and put on a paper robe. If you are offering five-star service, you need to offer five-star amenities. If you want to attract special patients, treat your patients special. It doesn’t cost that much to add a few dozen robes to your office supplies, laundering them after each use and placing them on hangers or in a plastic bag that each patient can use during her visit. I can assure you that this single idea will set you apart from most other ObGyns in your community.
Stirrups are cold! Here’s another idea: Use pads to cover the metal of the stirrups for the pelvic exam. Those stirrups are cold steel, and no woman who is already naked and concerned about her dignity wants to place her feet on those chilly structures. You can have lamb’s wool pads created by a seamstress for a few dollars—or if you prefer to go low-tech, you can use potholders to cover the stirrups.
Warm the speculum. My wife shared with me how uncomfortable it is to have a metal speculum inserted and how much she appreciated her gynecologist warming the instrument with tap water before its insertion. I have found that this saves on the use of lubricant jelly, too, because the water serves as a lubricant!
Keep the temperature in mind. Most medical offices are kept at 70° to 72° F to keep the doctor and staff comfortable. However, when a woman puts on her gown or robe, she often becomes cold and uncomfortable. On days when it is cold outside or the office is cold, use an inexpensive heater to make the room comfortable for the patient.
Talk to your patient “eyeball to eyeball.” You make big points with your patient if you speak to her when she is fully dressed and when your eyes are at the same level as hers. A woman lying on her back in a gown or robe does not hear or recall what her doctor is telling her. However, if the doctor and nurse leave the room and allow the patient to get dressed, and if the doctor sits with the patient without barriers between them, she is far more likely to listen and recall what has been discussed.
Pick up the telephone. I am often asked for my “best” idea to keep patients happy. My numero uno suggestion is to take a few minutes to call the patient at home. Which patients should you call? Women undergoing outpatient studies or procedures, those recently discharged from the hospital, and those who require a little more hand holding and attention. You can be sure that every patient who undergoes a procedure or is discharged from the hospital has questions about the findings, any precautions, medications, and follow-up. A call from a nurse or doctor does a lot to allay her apprehension—and it often keeps the patient from calling the office with her questions and concerns.
My nurse identifies key patients and contacts them at the end of the workday. She is usually able to answer all the questions but may identify two or three that require my attention. She tells the patient what time I will call so she can keep the phone line free.
Calling patients usually takes no more than 5 to 10 minutes a day and provides me with great satisfaction. Patients are usually shocked—and happy—that their physician is calling them at home. The advantages of this strategy include:
- fewer calls from your patients
- more efficient use of your time
- deep appreciation by the patient.
One patient I called at home wrote me a note that I think is worth mentioning: “This is the first time a member of your profession has taken the time to call me at home and check on my condition. Undoubtedly, it will foster a better relationship between you and me.”
Results of an informal poll indicate the answer is mostly “Yes”
As outlined in the article by Neil Baum, MD, the need to keep existing patients happy—and to determine how they’re feeling about your practice—seems as though it should occupy a berth rather high on your list of priorities. To gauge how widespread the practice of measuring patient satisfaction is among ObGyns, we polled our Virtual Board of Editors (VBE) on the subject. Because these physicians range from private practitioners to academic professionals and hospital employees, we find them to be one bellwether of wider practice patterns.
When we asked, 65% of our VBE members reported that they regularly measure the satisfaction of their patients. Among the reasons given for this tactic were corporate policy, but the vast majority of respondents indicated that they “need to know what patients like and don’t like” in order to “improve our services.” As one physician noted, “all practices can improve in some respects.” Regular inquiries about patient satisfaction provide a method and rationale for improvement.
Another respondent observed that the information gained from assessments of patient satisfaction is useful during insurance contracting. Another said, simply, “It’s the right thing to do.”
When asked exactly how they measure patient satisfaction, almost 60% of respondents who regularly assess this component of practice said they use surveys to do so, compared with 14% who use interviews, 17% who make a suggestion box available, and 11% who employ a “mystery shopper” (The percentages add up to more than 100% because some VBE members employ more than one approach.) None of the VBE members reported convening a focus group.
When asked to rate the importance of patient-satisfaction assessments, just over half of all respondents characterized it as “very important.” Only one physician reported that the practice of measuring patient satisfaction is “not important.”
“It is critical—especially for doctors with younger practices who are trying to build a reputation or practice—to get feedback to improve care and increase their patient load,” noted one respondent. Another reported: “We do a detailed satisfaction survey after every surgery on every patient. We actively seek feedback and use our Web site and social media to find ways to improve.”
“We are in a large city (over 500,000 population), so there is competition, and patients have choices,” wrote another VBE member. “In smaller communities, patients may have fewer options and have to accept the few available providers. My basic method of achieving patient satisfaction is outdated: I spend a lot of time per patient, see few patients per day, and try to help with whatever issues they have (not just breast and pelvic). I make less money practicing this way—I accepted a long time ago that really caring for patients means spending more time and being paid less for it.”
Another VBE member said, “I promise what I’ll do for patients, and I keep that promise! I use the telephone as a tool. Patients are very impressed and thankful when I talk to them about their problems and test results.”
—Janelle Yates, Senior Editor
The bottom line
Word of mouth was the time-honored method of attracting new patients for thousands of years. That method still works today. Ensuring that your patients have an outstanding experience during their visit is one of the smartest strategies to market and promote your practice.
We want to hear from you! Tell us what you think.
CLICK HERE to access 10 recent articles on managing your ObGyn practice.
| Dr. Baum describes his number one strategy to retain patients |
Neil H. Baum, MD
Dr. Baum practices urology in New Orleans, Louisiana. He is Associate Clinical Professor of Urology at Tulane Medical School and Louisiana State University Medical School, both in New Orleans. He is also on the medical staff at Touro Infirmary in New Orleans, and East Jefferson General Hospital in Metairie, Louisiana. And he is the author of Marketing Your Clinical Practice: Ethically, Effectively, Economically (4th edition, 2009; Jones & Bartlett).
The author reports no financial relationships relevant to this article.
| Dr. Baum describes his number one strategy to retain patients |
Neil H. Baum, MD
Dr. Baum practices urology in New Orleans, Louisiana. He is Associate Clinical Professor of Urology at Tulane Medical School and Louisiana State University Medical School, both in New Orleans. He is also on the medical staff at Touro Infirmary in New Orleans, and East Jefferson General Hospital in Metairie, Louisiana. And he is the author of Marketing Your Clinical Practice: Ethically, Effectively, Economically (4th edition, 2009; Jones & Bartlett).
The author reports no financial relationships relevant to this article.
| Dr. Baum describes his number one strategy to retain patients |
Neil H. Baum, MD
Dr. Baum practices urology in New Orleans, Louisiana. He is Associate Clinical Professor of Urology at Tulane Medical School and Louisiana State University Medical School, both in New Orleans. He is also on the medical staff at Touro Infirmary in New Orleans, and East Jefferson General Hospital in Metairie, Louisiana. And he is the author of Marketing Your Clinical Practice: Ethically, Effectively, Economically (4th edition, 2009; Jones & Bartlett).
The author reports no financial relationships relevant to this article.
Dr. Baum describes his number one strategy to retain patients (Audiocast, March 2013)
Pillar 2: Attract new patients (May 2013)
Pillar 3: Obtain and maintain physician referrals (June 2013)
Pillar 4: Motivate your staff (August 2013)
The medical landscape has changed. No one is quite certain what the future will hold. One thing we do know: 20 million more Americans, half of them women, will enter the health-care system in the very near future, as the Affordable Care Act continues to unfold. This flood of new patients will affect nearly every ObGyn practice in the country because we lack an adequate increase in the number of physicians to care for them. In the meantime, what can you do to ensure the continued success of your practice? This series focuses on four key areas. I call them the “four pillars”:
- Keep existing patients happy
- Attract new patients
- Nurture relationships with your medical colleagues and other health-care providers, such as physician assistants and nurse practitioners
- Maintain the morale of your staff.
No pillar is more important than the others; all four are necessary to guarantee success.
It is more cost-effective to keep an existing customer than to attract
a new one
In this article, I explain why it is vital to ensure that every patient has a positive experience of your practice, from the moment they make their first telephone call for an appointment, through their wait in the reception area, to the moment they are seen by the staff or the physician, and beyond—when they tell others about their stellar experience.
It’s nice to get new patients, but it is more important to keep the ones you already have. In most professions and businesses, the cost of keeping an established customer is one-fifth the cost of acquiring a new one. Medical practices are no exception. If you are not doing a good job with the patients you already have, spending thousands of dollars on a marketing plan to bring in new patients is pointless. The patients you have right now are the backbone of your practice.
Give your practice a checkup
Look at your practice from your patients’ perspective
Today, it is critical to know the needs and expectations of your patients and referring physicians. The best way to do this is to ask your patients what they think, which also will reveal your practice’s strengths and weaknesses. This information can be obtained easily by surveying patients about various aspects of your practice. (Even practices that are full or closed need to evaluate their services periodically and listen to their patients. Changes always occur, and the cup may not “runneth over” forever.)
Tom Peters, the nationally renowned author of In Search of Excellence, has described two keys to success in business:
- Find out what the customer (patient) wants and give him or her more of it
- Find out what the customer (patient) does not want and be sure to avoid it.
Techniques to gather the patient’s perspective
There are five effective techniques for determining how patients perceive your practice and for evaluating your performance and reputation:
- Conduct personal interviews
- Conduct patient surveys
- Create a focus group
- Use a suggestion box
- Commission evaluation by a mystery shopper.
Although I have used all five techniques, my favorite and most cost-effective involves a survey card that is given to every patient on every office visit (FIGURE 1). The card is given to the patient when she checks in, and she can complete it in the reception area or exam room and return it to the receptionist before leaving the practice. The cards are reviewed by a nurse, who addresses positive and negative comments. Most negative comments are addressed with a phone call. If necessary, I respond to the patient’s complaint.
FIGURE 1: Patient survey card
There is another benefit to the survey card. The flip side of the card prompts the patient to write down the three questions she would like you to address on her current visit to the office (FIGURE 2). Conducting the appointment according to these concerns can help keep patients from initiating a last-minute discussion, often after you have closed the chart or electronic medical record, that you don’t have time to address adequately. Since my office has implemented use of this survey card, we seldom get follow-up phone calls from patients about issues they forgot to ask about. The survey card demonstrates that we are listening to the patient and want to be certain that all her questions have been answered at the time of her office visit.
FIGURE 2: Focus of the appointment
Develop an on-time practice philosophy
You know the adage: Timeliness is next to godliness. (Actually, it’s cleanliness that’s next to godliness, but timeliness is vital, too.) The most common complaint patients have about the health-care experience is “waiting for the doctor.” Spending time in the reception area probably accounts for more patient dissatisfaction than any other aspect of medical care. In one recent survey, nearly one in four patients (24%) claimed to have waited 30 minutes or longer. With so many more women entering the marketplace, this statistic is only going to get worse.
In order to gain an accurate picture of what is happening in regard to the schedule in your practice, I suggest conducting a “time and motion” study. For a period of 3 to 5 days, place a sheet on each patient’s record or superbill and log in the following:
- time of her appointment
- time she arrived
- time she left the office
- how much time she spent with her physician.
You will be amazed to discover that patients are waiting 1 or 2 hours or longer to see the physician, and that the physician is spending only 5 minutes with the patient. Ask any patient on a survey if she feels she is getting bang for her buck, and she will answer, “No!”
By conducting a time and motion study, you will discover that there are predictable periods when backlogs occur. Often, these delays are the result of “working a patient in” to the schedule. Unscheduled patients who call to report vaginal bleeding, pelvic pain, urinary tract infection, or another problem are often told to come in without an appointment, but they inevitably displace women already scheduled and delay their visit. This problem affects almost every ObGyn.
One way to avoid this scenario is to create “sacred” time slots. These are 15-minute intervals at the end of the morning or afternoon in which unscheduled patients can be worked into the round of visits. Instead of telling the patient to “just come in,” I tell her to report at a specific time. These time slots cannot be filled with routine appointments. Nor can they be filled prior to 9 am each day. This leaves two or three slots open for patients who must be seen immediately.
Few ObGyns can change health-care policy. But all of us can be more sensitive to our patients’ time and make an effort to see them as soon as possible, thereby eliminating one of patients’ most common complaints: the long wait to see their doctor.
Make the patient’s experience memorable
All of us can provide a diagnosis and treatment strategy for most women’s medical problems. But how many of us can make the experience memorable for the woman? Often, it is a few little things that can be easily and inexpensively performed that make a big difference.
Go with cloth, not paper. There’s a sharp contrast between a paper sheet, a paper gown, and a soft robe. You don’t step out of the shower in a fine hotel and put on a paper robe. If you are offering five-star service, you need to offer five-star amenities. If you want to attract special patients, treat your patients special. It doesn’t cost that much to add a few dozen robes to your office supplies, laundering them after each use and placing them on hangers or in a plastic bag that each patient can use during her visit. I can assure you that this single idea will set you apart from most other ObGyns in your community.
Stirrups are cold! Here’s another idea: Use pads to cover the metal of the stirrups for the pelvic exam. Those stirrups are cold steel, and no woman who is already naked and concerned about her dignity wants to place her feet on those chilly structures. You can have lamb’s wool pads created by a seamstress for a few dollars—or if you prefer to go low-tech, you can use potholders to cover the stirrups.
Warm the speculum. My wife shared with me how uncomfortable it is to have a metal speculum inserted and how much she appreciated her gynecologist warming the instrument with tap water before its insertion. I have found that this saves on the use of lubricant jelly, too, because the water serves as a lubricant!
Keep the temperature in mind. Most medical offices are kept at 70° to 72° F to keep the doctor and staff comfortable. However, when a woman puts on her gown or robe, she often becomes cold and uncomfortable. On days when it is cold outside or the office is cold, use an inexpensive heater to make the room comfortable for the patient.
Talk to your patient “eyeball to eyeball.” You make big points with your patient if you speak to her when she is fully dressed and when your eyes are at the same level as hers. A woman lying on her back in a gown or robe does not hear or recall what her doctor is telling her. However, if the doctor and nurse leave the room and allow the patient to get dressed, and if the doctor sits with the patient without barriers between them, she is far more likely to listen and recall what has been discussed.
Pick up the telephone. I am often asked for my “best” idea to keep patients happy. My numero uno suggestion is to take a few minutes to call the patient at home. Which patients should you call? Women undergoing outpatient studies or procedures, those recently discharged from the hospital, and those who require a little more hand holding and attention. You can be sure that every patient who undergoes a procedure or is discharged from the hospital has questions about the findings, any precautions, medications, and follow-up. A call from a nurse or doctor does a lot to allay her apprehension—and it often keeps the patient from calling the office with her questions and concerns.
My nurse identifies key patients and contacts them at the end of the workday. She is usually able to answer all the questions but may identify two or three that require my attention. She tells the patient what time I will call so she can keep the phone line free.
Calling patients usually takes no more than 5 to 10 minutes a day and provides me with great satisfaction. Patients are usually shocked—and happy—that their physician is calling them at home. The advantages of this strategy include:
- fewer calls from your patients
- more efficient use of your time
- deep appreciation by the patient.
One patient I called at home wrote me a note that I think is worth mentioning: “This is the first time a member of your profession has taken the time to call me at home and check on my condition. Undoubtedly, it will foster a better relationship between you and me.”
Results of an informal poll indicate the answer is mostly “Yes”
As outlined in the article by Neil Baum, MD, the need to keep existing patients happy—and to determine how they’re feeling about your practice—seems as though it should occupy a berth rather high on your list of priorities. To gauge how widespread the practice of measuring patient satisfaction is among ObGyns, we polled our Virtual Board of Editors (VBE) on the subject. Because these physicians range from private practitioners to academic professionals and hospital employees, we find them to be one bellwether of wider practice patterns.
When we asked, 65% of our VBE members reported that they regularly measure the satisfaction of their patients. Among the reasons given for this tactic were corporate policy, but the vast majority of respondents indicated that they “need to know what patients like and don’t like” in order to “improve our services.” As one physician noted, “all practices can improve in some respects.” Regular inquiries about patient satisfaction provide a method and rationale for improvement.
Another respondent observed that the information gained from assessments of patient satisfaction is useful during insurance contracting. Another said, simply, “It’s the right thing to do.”
When asked exactly how they measure patient satisfaction, almost 60% of respondents who regularly assess this component of practice said they use surveys to do so, compared with 14% who use interviews, 17% who make a suggestion box available, and 11% who employ a “mystery shopper” (The percentages add up to more than 100% because some VBE members employ more than one approach.) None of the VBE members reported convening a focus group.
When asked to rate the importance of patient-satisfaction assessments, just over half of all respondents characterized it as “very important.” Only one physician reported that the practice of measuring patient satisfaction is “not important.”
“It is critical—especially for doctors with younger practices who are trying to build a reputation or practice—to get feedback to improve care and increase their patient load,” noted one respondent. Another reported: “We do a detailed satisfaction survey after every surgery on every patient. We actively seek feedback and use our Web site and social media to find ways to improve.”
“We are in a large city (over 500,000 population), so there is competition, and patients have choices,” wrote another VBE member. “In smaller communities, patients may have fewer options and have to accept the few available providers. My basic method of achieving patient satisfaction is outdated: I spend a lot of time per patient, see few patients per day, and try to help with whatever issues they have (not just breast and pelvic). I make less money practicing this way—I accepted a long time ago that really caring for patients means spending more time and being paid less for it.”
Another VBE member said, “I promise what I’ll do for patients, and I keep that promise! I use the telephone as a tool. Patients are very impressed and thankful when I talk to them about their problems and test results.”
—Janelle Yates, Senior Editor
The bottom line
Word of mouth was the time-honored method of attracting new patients for thousands of years. That method still works today. Ensuring that your patients have an outstanding experience during their visit is one of the smartest strategies to market and promote your practice.
We want to hear from you! Tell us what you think.
CLICK HERE to access 10 recent articles on managing your ObGyn practice.
Dr. Baum describes his number one strategy to retain patients (Audiocast, March 2013)
Pillar 2: Attract new patients (May 2013)
Pillar 3: Obtain and maintain physician referrals (June 2013)
Pillar 4: Motivate your staff (August 2013)
The medical landscape has changed. No one is quite certain what the future will hold. One thing we do know: 20 million more Americans, half of them women, will enter the health-care system in the very near future, as the Affordable Care Act continues to unfold. This flood of new patients will affect nearly every ObGyn practice in the country because we lack an adequate increase in the number of physicians to care for them. In the meantime, what can you do to ensure the continued success of your practice? This series focuses on four key areas. I call them the “four pillars”:
- Keep existing patients happy
- Attract new patients
- Nurture relationships with your medical colleagues and other health-care providers, such as physician assistants and nurse practitioners
- Maintain the morale of your staff.
No pillar is more important than the others; all four are necessary to guarantee success.
It is more cost-effective to keep an existing customer than to attract
a new one
In this article, I explain why it is vital to ensure that every patient has a positive experience of your practice, from the moment they make their first telephone call for an appointment, through their wait in the reception area, to the moment they are seen by the staff or the physician, and beyond—when they tell others about their stellar experience.
It’s nice to get new patients, but it is more important to keep the ones you already have. In most professions and businesses, the cost of keeping an established customer is one-fifth the cost of acquiring a new one. Medical practices are no exception. If you are not doing a good job with the patients you already have, spending thousands of dollars on a marketing plan to bring in new patients is pointless. The patients you have right now are the backbone of your practice.
Give your practice a checkup
Look at your practice from your patients’ perspective
Today, it is critical to know the needs and expectations of your patients and referring physicians. The best way to do this is to ask your patients what they think, which also will reveal your practice’s strengths and weaknesses. This information can be obtained easily by surveying patients about various aspects of your practice. (Even practices that are full or closed need to evaluate their services periodically and listen to their patients. Changes always occur, and the cup may not “runneth over” forever.)
Tom Peters, the nationally renowned author of In Search of Excellence, has described two keys to success in business:
- Find out what the customer (patient) wants and give him or her more of it
- Find out what the customer (patient) does not want and be sure to avoid it.
Techniques to gather the patient’s perspective
There are five effective techniques for determining how patients perceive your practice and for evaluating your performance and reputation:
- Conduct personal interviews
- Conduct patient surveys
- Create a focus group
- Use a suggestion box
- Commission evaluation by a mystery shopper.
Although I have used all five techniques, my favorite and most cost-effective involves a survey card that is given to every patient on every office visit (FIGURE 1). The card is given to the patient when she checks in, and she can complete it in the reception area or exam room and return it to the receptionist before leaving the practice. The cards are reviewed by a nurse, who addresses positive and negative comments. Most negative comments are addressed with a phone call. If necessary, I respond to the patient’s complaint.
FIGURE 1: Patient survey card
There is another benefit to the survey card. The flip side of the card prompts the patient to write down the three questions she would like you to address on her current visit to the office (FIGURE 2). Conducting the appointment according to these concerns can help keep patients from initiating a last-minute discussion, often after you have closed the chart or electronic medical record, that you don’t have time to address adequately. Since my office has implemented use of this survey card, we seldom get follow-up phone calls from patients about issues they forgot to ask about. The survey card demonstrates that we are listening to the patient and want to be certain that all her questions have been answered at the time of her office visit.
FIGURE 2: Focus of the appointment
Develop an on-time practice philosophy
You know the adage: Timeliness is next to godliness. (Actually, it’s cleanliness that’s next to godliness, but timeliness is vital, too.) The most common complaint patients have about the health-care experience is “waiting for the doctor.” Spending time in the reception area probably accounts for more patient dissatisfaction than any other aspect of medical care. In one recent survey, nearly one in four patients (24%) claimed to have waited 30 minutes or longer. With so many more women entering the marketplace, this statistic is only going to get worse.
In order to gain an accurate picture of what is happening in regard to the schedule in your practice, I suggest conducting a “time and motion” study. For a period of 3 to 5 days, place a sheet on each patient’s record or superbill and log in the following:
- time of her appointment
- time she arrived
- time she left the office
- how much time she spent with her physician.
You will be amazed to discover that patients are waiting 1 or 2 hours or longer to see the physician, and that the physician is spending only 5 minutes with the patient. Ask any patient on a survey if she feels she is getting bang for her buck, and she will answer, “No!”
By conducting a time and motion study, you will discover that there are predictable periods when backlogs occur. Often, these delays are the result of “working a patient in” to the schedule. Unscheduled patients who call to report vaginal bleeding, pelvic pain, urinary tract infection, or another problem are often told to come in without an appointment, but they inevitably displace women already scheduled and delay their visit. This problem affects almost every ObGyn.
One way to avoid this scenario is to create “sacred” time slots. These are 15-minute intervals at the end of the morning or afternoon in which unscheduled patients can be worked into the round of visits. Instead of telling the patient to “just come in,” I tell her to report at a specific time. These time slots cannot be filled with routine appointments. Nor can they be filled prior to 9 am each day. This leaves two or three slots open for patients who must be seen immediately.
Few ObGyns can change health-care policy. But all of us can be more sensitive to our patients’ time and make an effort to see them as soon as possible, thereby eliminating one of patients’ most common complaints: the long wait to see their doctor.
Make the patient’s experience memorable
All of us can provide a diagnosis and treatment strategy for most women’s medical problems. But how many of us can make the experience memorable for the woman? Often, it is a few little things that can be easily and inexpensively performed that make a big difference.
Go with cloth, not paper. There’s a sharp contrast between a paper sheet, a paper gown, and a soft robe. You don’t step out of the shower in a fine hotel and put on a paper robe. If you are offering five-star service, you need to offer five-star amenities. If you want to attract special patients, treat your patients special. It doesn’t cost that much to add a few dozen robes to your office supplies, laundering them after each use and placing them on hangers or in a plastic bag that each patient can use during her visit. I can assure you that this single idea will set you apart from most other ObGyns in your community.
Stirrups are cold! Here’s another idea: Use pads to cover the metal of the stirrups for the pelvic exam. Those stirrups are cold steel, and no woman who is already naked and concerned about her dignity wants to place her feet on those chilly structures. You can have lamb’s wool pads created by a seamstress for a few dollars—or if you prefer to go low-tech, you can use potholders to cover the stirrups.
Warm the speculum. My wife shared with me how uncomfortable it is to have a metal speculum inserted and how much she appreciated her gynecologist warming the instrument with tap water before its insertion. I have found that this saves on the use of lubricant jelly, too, because the water serves as a lubricant!
Keep the temperature in mind. Most medical offices are kept at 70° to 72° F to keep the doctor and staff comfortable. However, when a woman puts on her gown or robe, she often becomes cold and uncomfortable. On days when it is cold outside or the office is cold, use an inexpensive heater to make the room comfortable for the patient.
Talk to your patient “eyeball to eyeball.” You make big points with your patient if you speak to her when she is fully dressed and when your eyes are at the same level as hers. A woman lying on her back in a gown or robe does not hear or recall what her doctor is telling her. However, if the doctor and nurse leave the room and allow the patient to get dressed, and if the doctor sits with the patient without barriers between them, she is far more likely to listen and recall what has been discussed.
Pick up the telephone. I am often asked for my “best” idea to keep patients happy. My numero uno suggestion is to take a few minutes to call the patient at home. Which patients should you call? Women undergoing outpatient studies or procedures, those recently discharged from the hospital, and those who require a little more hand holding and attention. You can be sure that every patient who undergoes a procedure or is discharged from the hospital has questions about the findings, any precautions, medications, and follow-up. A call from a nurse or doctor does a lot to allay her apprehension—and it often keeps the patient from calling the office with her questions and concerns.
My nurse identifies key patients and contacts them at the end of the workday. She is usually able to answer all the questions but may identify two or three that require my attention. She tells the patient what time I will call so she can keep the phone line free.
Calling patients usually takes no more than 5 to 10 minutes a day and provides me with great satisfaction. Patients are usually shocked—and happy—that their physician is calling them at home. The advantages of this strategy include:
- fewer calls from your patients
- more efficient use of your time
- deep appreciation by the patient.
One patient I called at home wrote me a note that I think is worth mentioning: “This is the first time a member of your profession has taken the time to call me at home and check on my condition. Undoubtedly, it will foster a better relationship between you and me.”
Results of an informal poll indicate the answer is mostly “Yes”
As outlined in the article by Neil Baum, MD, the need to keep existing patients happy—and to determine how they’re feeling about your practice—seems as though it should occupy a berth rather high on your list of priorities. To gauge how widespread the practice of measuring patient satisfaction is among ObGyns, we polled our Virtual Board of Editors (VBE) on the subject. Because these physicians range from private practitioners to academic professionals and hospital employees, we find them to be one bellwether of wider practice patterns.
When we asked, 65% of our VBE members reported that they regularly measure the satisfaction of their patients. Among the reasons given for this tactic were corporate policy, but the vast majority of respondents indicated that they “need to know what patients like and don’t like” in order to “improve our services.” As one physician noted, “all practices can improve in some respects.” Regular inquiries about patient satisfaction provide a method and rationale for improvement.
Another respondent observed that the information gained from assessments of patient satisfaction is useful during insurance contracting. Another said, simply, “It’s the right thing to do.”
When asked exactly how they measure patient satisfaction, almost 60% of respondents who regularly assess this component of practice said they use surveys to do so, compared with 14% who use interviews, 17% who make a suggestion box available, and 11% who employ a “mystery shopper” (The percentages add up to more than 100% because some VBE members employ more than one approach.) None of the VBE members reported convening a focus group.
When asked to rate the importance of patient-satisfaction assessments, just over half of all respondents characterized it as “very important.” Only one physician reported that the practice of measuring patient satisfaction is “not important.”
“It is critical—especially for doctors with younger practices who are trying to build a reputation or practice—to get feedback to improve care and increase their patient load,” noted one respondent. Another reported: “We do a detailed satisfaction survey after every surgery on every patient. We actively seek feedback and use our Web site and social media to find ways to improve.”
“We are in a large city (over 500,000 population), so there is competition, and patients have choices,” wrote another VBE member. “In smaller communities, patients may have fewer options and have to accept the few available providers. My basic method of achieving patient satisfaction is outdated: I spend a lot of time per patient, see few patients per day, and try to help with whatever issues they have (not just breast and pelvic). I make less money practicing this way—I accepted a long time ago that really caring for patients means spending more time and being paid less for it.”
Another VBE member said, “I promise what I’ll do for patients, and I keep that promise! I use the telephone as a tool. Patients are very impressed and thankful when I talk to them about their problems and test results.”
—Janelle Yates, Senior Editor
The bottom line
Word of mouth was the time-honored method of attracting new patients for thousands of years. That method still works today. Ensuring that your patients have an outstanding experience during their visit is one of the smartest strategies to market and promote your practice.
We want to hear from you! Tell us what you think.
CLICK HERE to access 10 recent articles on managing your ObGyn practice.