User login
New coding policies to prevent surprise billing for CRC screening
The Departments of Labor, Health & Human Services, and the Treasury issued guidance in 2022 that plans and insurers “must cover and may not impose cost sharing with respect to a colonoscopy conducted after a positive non-invasive stool-based screening test” for plan or policy years1 beginning on or after May 31, 2022, and, further, “may not impose cost-sharing with respect to a polyp removal during a colonoscopy performed as a screening procedure.”2 So why are so many patients still being charged fees for these screening services? In many cases, the answer comes down to missing code modifiers.
Commercial insurers want you to use modifier 33
AGA spoke to Elevance (formerly Anthem), Cigna, Aetna, and Blue Cross Blue Shield Association about how physicians should report colorectal cancer screening procedures and tests. They said using the 33 modifier (preventive service) is essential for their systems to trigger the screening benefits for beneficiaries. Without the 33 modifier, the claim will be processed as a diagnostic service, and coinsurance may apply.
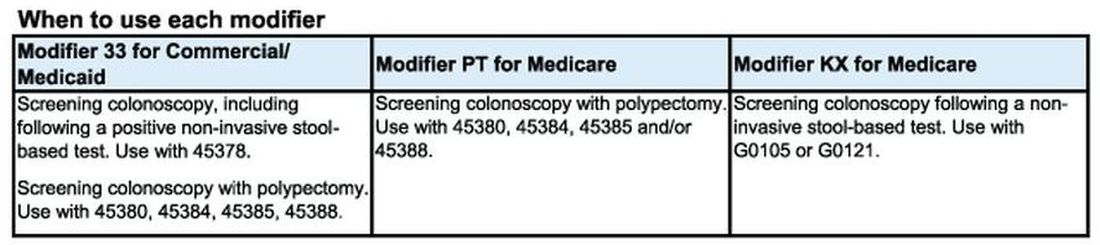
According to the CPT manual, modifier 33 should be used “when the primary purpose of the service is the delivery of an evidence-based service in accordance with a U.S. Preventive Services Task Force A or B rating in effect and other preventive services identified in preventive mandates (legislative or regulatory) ...” Use modifier 33 with colonoscopies that start out as screening procedures and with colonoscopies following a positive non-invasive stool-based test, like fecal immunochemical test (FIT) or Cologuard™ multi-target stool DNA test.
It is important to note that modifier 33 won’t ensure all screening colonoscopy claims are paid, because not all commercial plans are required to cover 100 percent of the costs of CRC screening tests and procedures. For example, employer-sponsored insurance plans and legacy plans can choose not to adopt the expanded CRC benefits. Patients who are covered under these plans may not be aware that their CRC test or procedure will not be fully covered. These patients may still receive a “surprise” bill if their screening colonoscopy requires removal of polyps or if they have a colonoscopy following a positive non-invasive CRC test.
Medicare wants you to use modifiers PT and KX, but not together
CMS uses Healthcare Common Procedural Coding System (HCPCS) codes to differentiate between screening and diagnostic colonoscopies to apply screening benefits. For Medicare beneficiaries who choose colonoscopy as their CRC screening, use HCPCS code G0105 (Colorectal cancer screening; colonoscopy on individual at high risk) or G0121 (Colorectal cancer screening; colonoscopy on individual not meeting the criteria for high risk) for screening colonoscopies as appropriate. No modifier is necessary with G0105 or G0121.
Effective for claims with dates of service on or after 1/1/2023, use the appropriate HCPCS codes G0105 or G0121 with the KX modifier for colonoscopy following a positive result for any of the following non-invasive stool-based CRC screening tests:
• Screening guaiac-based fecal occult blood test (gFOBT) (CPT 82270)
• Screening immunoassay-based fecal occult blood test (iFOBT) (HCPCS G0328)
• Cologuard™ – multi-target stool DNA (sDNA) test (CPT 81528)
According to the guidance in the CMS Manual System, if modifier KX is not added to G0105 or G0121 for colonoscopy following a positive non-invasive stool-based test, Medicare will return the screening colonoscopy claim as “unprocessable.”3 If this happens, add modifier KX and resubmit the claim.
If polyps are removed during a screening colonoscopy, use the appropriate CPT code (45380, 45384, 45385, 45388) and add modifier PT (colorectal cancer screening test; converted to diagnostic test or other procedure) to each CPT code for Medicare. However, it is important to note that if a polyp is removed during a screening colonoscopy, the Medicare beneficiary is responsible for 15% of the cost from 2023 to 2026. This falls to 10% of the cost from 2027 to 2029, and by 2030 it will be covered 100% by Medicare. Some Medicare beneficiaries are not aware that Medicare has not fully eliminated the coinsurance responsibility yet.
What to do if your patient gets an unexpected bill
If your patient gets an unexpected bill and you coded the procedure correctly with the correct modifier, direct them to the AGA GI Patient Care Center’s “Colorectal cancer screening: what to expect when paying” resource for help with next steps.4
The authors have no conflicts to declare.
References
1. U.S. Department of Labor (2022, Jan. 10) FAQs About Affordable Care Act Implementation Part 51. https://www.dol.gov/sites/dolgov/files/EBSA/about-ebsa/our-activities/resource-center/faqs/aca-part-51.pdf
2. Centers for Medicare and Medicaid Services (n.d.) Affordable Care Act Implementation FAQs - Set 12. https://www.cms.gov/CCIIO/Resources/Fact-Sheets-and-FAQs/aca_implementation_faqs12.
3. Centers for Medicare and Medicaid Services (2023, Jan. 27) CMS Manual System Pub 100-03 Medicare National Coverage Determinations Transmittal 11824. https://www.cms.gov/files/document/r11824ncd.pdf.
4. American Gastroenterological Association (2023, Feb. 21) AGA GI Patient Center Colorectal Cancer Screening: What to expect when paying. https://patient.gastro.org/paying-for-your-colonoscopy/.
The Departments of Labor, Health & Human Services, and the Treasury issued guidance in 2022 that plans and insurers “must cover and may not impose cost sharing with respect to a colonoscopy conducted after a positive non-invasive stool-based screening test” for plan or policy years1 beginning on or after May 31, 2022, and, further, “may not impose cost-sharing with respect to a polyp removal during a colonoscopy performed as a screening procedure.”2 So why are so many patients still being charged fees for these screening services? In many cases, the answer comes down to missing code modifiers.
Commercial insurers want you to use modifier 33
AGA spoke to Elevance (formerly Anthem), Cigna, Aetna, and Blue Cross Blue Shield Association about how physicians should report colorectal cancer screening procedures and tests. They said using the 33 modifier (preventive service) is essential for their systems to trigger the screening benefits for beneficiaries. Without the 33 modifier, the claim will be processed as a diagnostic service, and coinsurance may apply.
According to the CPT manual, modifier 33 should be used “when the primary purpose of the service is the delivery of an evidence-based service in accordance with a U.S. Preventive Services Task Force A or B rating in effect and other preventive services identified in preventive mandates (legislative or regulatory) ...” Use modifier 33 with colonoscopies that start out as screening procedures and with colonoscopies following a positive non-invasive stool-based test, like fecal immunochemical test (FIT) or Cologuard™ multi-target stool DNA test.
It is important to note that modifier 33 won’t ensure all screening colonoscopy claims are paid, because not all commercial plans are required to cover 100 percent of the costs of CRC screening tests and procedures. For example, employer-sponsored insurance plans and legacy plans can choose not to adopt the expanded CRC benefits. Patients who are covered under these plans may not be aware that their CRC test or procedure will not be fully covered. These patients may still receive a “surprise” bill if their screening colonoscopy requires removal of polyps or if they have a colonoscopy following a positive non-invasive CRC test.
Medicare wants you to use modifiers PT and KX, but not together
CMS uses Healthcare Common Procedural Coding System (HCPCS) codes to differentiate between screening and diagnostic colonoscopies to apply screening benefits. For Medicare beneficiaries who choose colonoscopy as their CRC screening, use HCPCS code G0105 (Colorectal cancer screening; colonoscopy on individual at high risk) or G0121 (Colorectal cancer screening; colonoscopy on individual not meeting the criteria for high risk) for screening colonoscopies as appropriate. No modifier is necessary with G0105 or G0121.
Effective for claims with dates of service on or after 1/1/2023, use the appropriate HCPCS codes G0105 or G0121 with the KX modifier for colonoscopy following a positive result for any of the following non-invasive stool-based CRC screening tests:
• Screening guaiac-based fecal occult blood test (gFOBT) (CPT 82270)
• Screening immunoassay-based fecal occult blood test (iFOBT) (HCPCS G0328)
• Cologuard™ – multi-target stool DNA (sDNA) test (CPT 81528)
According to the guidance in the CMS Manual System, if modifier KX is not added to G0105 or G0121 for colonoscopy following a positive non-invasive stool-based test, Medicare will return the screening colonoscopy claim as “unprocessable.”3 If this happens, add modifier KX and resubmit the claim.
If polyps are removed during a screening colonoscopy, use the appropriate CPT code (45380, 45384, 45385, 45388) and add modifier PT (colorectal cancer screening test; converted to diagnostic test or other procedure) to each CPT code for Medicare. However, it is important to note that if a polyp is removed during a screening colonoscopy, the Medicare beneficiary is responsible for 15% of the cost from 2023 to 2026. This falls to 10% of the cost from 2027 to 2029, and by 2030 it will be covered 100% by Medicare. Some Medicare beneficiaries are not aware that Medicare has not fully eliminated the coinsurance responsibility yet.
What to do if your patient gets an unexpected bill
If your patient gets an unexpected bill and you coded the procedure correctly with the correct modifier, direct them to the AGA GI Patient Care Center’s “Colorectal cancer screening: what to expect when paying” resource for help with next steps.4
The authors have no conflicts to declare.
References
1. U.S. Department of Labor (2022, Jan. 10) FAQs About Affordable Care Act Implementation Part 51. https://www.dol.gov/sites/dolgov/files/EBSA/about-ebsa/our-activities/resource-center/faqs/aca-part-51.pdf
2. Centers for Medicare and Medicaid Services (n.d.) Affordable Care Act Implementation FAQs - Set 12. https://www.cms.gov/CCIIO/Resources/Fact-Sheets-and-FAQs/aca_implementation_faqs12.
3. Centers for Medicare and Medicaid Services (2023, Jan. 27) CMS Manual System Pub 100-03 Medicare National Coverage Determinations Transmittal 11824. https://www.cms.gov/files/document/r11824ncd.pdf.
4. American Gastroenterological Association (2023, Feb. 21) AGA GI Patient Center Colorectal Cancer Screening: What to expect when paying. https://patient.gastro.org/paying-for-your-colonoscopy/.
The Departments of Labor, Health & Human Services, and the Treasury issued guidance in 2022 that plans and insurers “must cover and may not impose cost sharing with respect to a colonoscopy conducted after a positive non-invasive stool-based screening test” for plan or policy years1 beginning on or after May 31, 2022, and, further, “may not impose cost-sharing with respect to a polyp removal during a colonoscopy performed as a screening procedure.”2 So why are so many patients still being charged fees for these screening services? In many cases, the answer comes down to missing code modifiers.
Commercial insurers want you to use modifier 33
AGA spoke to Elevance (formerly Anthem), Cigna, Aetna, and Blue Cross Blue Shield Association about how physicians should report colorectal cancer screening procedures and tests. They said using the 33 modifier (preventive service) is essential for their systems to trigger the screening benefits for beneficiaries. Without the 33 modifier, the claim will be processed as a diagnostic service, and coinsurance may apply.
According to the CPT manual, modifier 33 should be used “when the primary purpose of the service is the delivery of an evidence-based service in accordance with a U.S. Preventive Services Task Force A or B rating in effect and other preventive services identified in preventive mandates (legislative or regulatory) ...” Use modifier 33 with colonoscopies that start out as screening procedures and with colonoscopies following a positive non-invasive stool-based test, like fecal immunochemical test (FIT) or Cologuard™ multi-target stool DNA test.
It is important to note that modifier 33 won’t ensure all screening colonoscopy claims are paid, because not all commercial plans are required to cover 100 percent of the costs of CRC screening tests and procedures. For example, employer-sponsored insurance plans and legacy plans can choose not to adopt the expanded CRC benefits. Patients who are covered under these plans may not be aware that their CRC test or procedure will not be fully covered. These patients may still receive a “surprise” bill if their screening colonoscopy requires removal of polyps or if they have a colonoscopy following a positive non-invasive CRC test.
Medicare wants you to use modifiers PT and KX, but not together
CMS uses Healthcare Common Procedural Coding System (HCPCS) codes to differentiate between screening and diagnostic colonoscopies to apply screening benefits. For Medicare beneficiaries who choose colonoscopy as their CRC screening, use HCPCS code G0105 (Colorectal cancer screening; colonoscopy on individual at high risk) or G0121 (Colorectal cancer screening; colonoscopy on individual not meeting the criteria for high risk) for screening colonoscopies as appropriate. No modifier is necessary with G0105 or G0121.
Effective for claims with dates of service on or after 1/1/2023, use the appropriate HCPCS codes G0105 or G0121 with the KX modifier for colonoscopy following a positive result for any of the following non-invasive stool-based CRC screening tests:
• Screening guaiac-based fecal occult blood test (gFOBT) (CPT 82270)
• Screening immunoassay-based fecal occult blood test (iFOBT) (HCPCS G0328)
• Cologuard™ – multi-target stool DNA (sDNA) test (CPT 81528)
According to the guidance in the CMS Manual System, if modifier KX is not added to G0105 or G0121 for colonoscopy following a positive non-invasive stool-based test, Medicare will return the screening colonoscopy claim as “unprocessable.”3 If this happens, add modifier KX and resubmit the claim.
If polyps are removed during a screening colonoscopy, use the appropriate CPT code (45380, 45384, 45385, 45388) and add modifier PT (colorectal cancer screening test; converted to diagnostic test or other procedure) to each CPT code for Medicare. However, it is important to note that if a polyp is removed during a screening colonoscopy, the Medicare beneficiary is responsible for 15% of the cost from 2023 to 2026. This falls to 10% of the cost from 2027 to 2029, and by 2030 it will be covered 100% by Medicare. Some Medicare beneficiaries are not aware that Medicare has not fully eliminated the coinsurance responsibility yet.
What to do if your patient gets an unexpected bill
If your patient gets an unexpected bill and you coded the procedure correctly with the correct modifier, direct them to the AGA GI Patient Care Center’s “Colorectal cancer screening: what to expect when paying” resource for help with next steps.4
The authors have no conflicts to declare.
References
1. U.S. Department of Labor (2022, Jan. 10) FAQs About Affordable Care Act Implementation Part 51. https://www.dol.gov/sites/dolgov/files/EBSA/about-ebsa/our-activities/resource-center/faqs/aca-part-51.pdf
2. Centers for Medicare and Medicaid Services (n.d.) Affordable Care Act Implementation FAQs - Set 12. https://www.cms.gov/CCIIO/Resources/Fact-Sheets-and-FAQs/aca_implementation_faqs12.
3. Centers for Medicare and Medicaid Services (2023, Jan. 27) CMS Manual System Pub 100-03 Medicare National Coverage Determinations Transmittal 11824. https://www.cms.gov/files/document/r11824ncd.pdf.
4. American Gastroenterological Association (2023, Feb. 21) AGA GI Patient Center Colorectal Cancer Screening: What to expect when paying. https://patient.gastro.org/paying-for-your-colonoscopy/.
AGA’s GI Opportunity Fund invests in EndoSound®
EndoSound is an Oregon-based medical device innovator developing technology that enhances access, reduces costs, and increases the safety of endoscopic ultrasound (EUS) procedures.
The EndoSound Vision System® (EVS®) is a disruptive EUS platform. Its attachable transducer and supportive components transform a conventional upper endoscope into a fully functional endoscopic ultrasound device. The cost of existing EUS systems has limited the availability of this crucial modality in the United States and around the world.
By reducing this cost, the EVS will provide physicians with a technological option that can enable care for their patients in a greater number of locations and settings. This brings the potential for enormous benefits to patients, payers, and providers by reducing costs in the healthcare system.
EndoSound is an Oregon-based medical device innovator developing technology that enhances access, reduces costs, and increases the safety of endoscopic ultrasound (EUS) procedures.
The EndoSound Vision System® (EVS®) is a disruptive EUS platform. Its attachable transducer and supportive components transform a conventional upper endoscope into a fully functional endoscopic ultrasound device. The cost of existing EUS systems has limited the availability of this crucial modality in the United States and around the world.
By reducing this cost, the EVS will provide physicians with a technological option that can enable care for their patients in a greater number of locations and settings. This brings the potential for enormous benefits to patients, payers, and providers by reducing costs in the healthcare system.
EndoSound is an Oregon-based medical device innovator developing technology that enhances access, reduces costs, and increases the safety of endoscopic ultrasound (EUS) procedures.
The EndoSound Vision System® (EVS®) is a disruptive EUS platform. Its attachable transducer and supportive components transform a conventional upper endoscope into a fully functional endoscopic ultrasound device. The cost of existing EUS systems has limited the availability of this crucial modality in the United States and around the world.
By reducing this cost, the EVS will provide physicians with a technological option that can enable care for their patients in a greater number of locations and settings. This brings the potential for enormous benefits to patients, payers, and providers by reducing costs in the healthcare system.
A special tribute: Memorial and honorary gifts
Did you know you can honor a family member, friend, or colleague through a gift to the AGA Research Foundation?
- Giving now or later. Any charitable gift can be made in honor or memory of someone.
- A gift today. An outright gift will help fund the AGA Research Awards Program. Your gift will assist in furthering basic digestive disease research, which can ultimately advance research into all digestive diseases. The financial benefits include an income tax deduction and possible elimination of capital gains tax.
- A gift through your will or living trust. You can include a bequest in your will or living trust stating that a specific asset, certain dollar amount, or more commonly a percentage of your estate will pass to the AGA Research Foundation at your death in honor of your loved one.
- Named opportunities. Individuals interested in receiving name recognition for a listed AGA Institute program can do so by contributing a new, unrestricted gift to the AGA Research Foundation. The gift can be payable over five years. Endowed opportunities are also available.
Your next step
An honorary gift is a wonderful way to acknowledge someone’s vision for the future. To learn more about ways to recognize your honoree, visit our website.
Did you know you can honor a family member, friend, or colleague through a gift to the AGA Research Foundation?
- Giving now or later. Any charitable gift can be made in honor or memory of someone.
- A gift today. An outright gift will help fund the AGA Research Awards Program. Your gift will assist in furthering basic digestive disease research, which can ultimately advance research into all digestive diseases. The financial benefits include an income tax deduction and possible elimination of capital gains tax.
- A gift through your will or living trust. You can include a bequest in your will or living trust stating that a specific asset, certain dollar amount, or more commonly a percentage of your estate will pass to the AGA Research Foundation at your death in honor of your loved one.
- Named opportunities. Individuals interested in receiving name recognition for a listed AGA Institute program can do so by contributing a new, unrestricted gift to the AGA Research Foundation. The gift can be payable over five years. Endowed opportunities are also available.
Your next step
An honorary gift is a wonderful way to acknowledge someone’s vision for the future. To learn more about ways to recognize your honoree, visit our website.
Did you know you can honor a family member, friend, or colleague through a gift to the AGA Research Foundation?
- Giving now or later. Any charitable gift can be made in honor or memory of someone.
- A gift today. An outright gift will help fund the AGA Research Awards Program. Your gift will assist in furthering basic digestive disease research, which can ultimately advance research into all digestive diseases. The financial benefits include an income tax deduction and possible elimination of capital gains tax.
- A gift through your will or living trust. You can include a bequest in your will or living trust stating that a specific asset, certain dollar amount, or more commonly a percentage of your estate will pass to the AGA Research Foundation at your death in honor of your loved one.
- Named opportunities. Individuals interested in receiving name recognition for a listed AGA Institute program can do so by contributing a new, unrestricted gift to the AGA Research Foundation. The gift can be payable over five years. Endowed opportunities are also available.
Your next step
An honorary gift is a wonderful way to acknowledge someone’s vision for the future. To learn more about ways to recognize your honoree, visit our website.
What the omnibus bill means for GI
Here’s what you need to know:
Medicare payment cuts
Unfortunately, physicians treating Medicare patients will face cuts in the new year.
It is disappointing that Congress failed to stop the full cuts. However, the Medicare payment cuts will be lower than the initially proposed 8.5% cut. Physicians will face a 2% cut because of the 4% in PAYGO relief for 2023 and 2024, plus an additional 2.5% in relief for the Centers for Medicare & Medicaid Services.
This is not an ideal outcome, but we are grateful to the more than 160 AGA members who raised their voices and sent over 600 messages to Congress. Your advocacy played a role in alleviating the final number of the cuts.
We will continue to urge Congress to stop the full cuts. Our top priority in 2023 remains addressing the Medicare reimbursement rates.
Two-year extension for telehealth
Good news! We have been ongoing supporters of telehealth expansion that resulted from the COVID-19 pandemic. The inclusion of this 2-year telehealth extension will allow doctors to continue to treat Medicare patients in a virtual setting. This is crucial since it allows patients to continue receiving treatment from their doctor in a virtual setting, and it provides patients and providers with certainty.
$2.5 billion increase for NIH
Good news! The omnibus allocates $47.5 billion for the National Institutes of Health’s budget, a $2.5 billion increase from 2023. The increased federal research funding is something we advocated for with congressional offices during Advocacy Day and will support GI researchers who are conducting innovative research and developing treatment for digestive diseases and GI cancers.
AGA-submitted report language on IBD included
Good news! Two language requests submitted by AGA on inflammatory bowel disease (IBD) were included in the omnibus: one in the 2023 Department of Labor, Health and Human Services, Education and Related Agencies funding bill and one in the 2023 Department of Agriculture, Rural Development, Food and Drug Administration and Related Agencies funding bill.
The first reaffirms the Appropriations Committee’s support for the NIH in funding basic, translational, and clinical studies on the diagnosis and treatment of IBD. The second encourages the FDA to improve diversity and patient-centricity in IBD clinical trials. The inclusion of these language requests in the omnibus highlights another successful advocacy effort by AGA.
Here’s what you need to know:
Medicare payment cuts
Unfortunately, physicians treating Medicare patients will face cuts in the new year.
It is disappointing that Congress failed to stop the full cuts. However, the Medicare payment cuts will be lower than the initially proposed 8.5% cut. Physicians will face a 2% cut because of the 4% in PAYGO relief for 2023 and 2024, plus an additional 2.5% in relief for the Centers for Medicare & Medicaid Services.
This is not an ideal outcome, but we are grateful to the more than 160 AGA members who raised their voices and sent over 600 messages to Congress. Your advocacy played a role in alleviating the final number of the cuts.
We will continue to urge Congress to stop the full cuts. Our top priority in 2023 remains addressing the Medicare reimbursement rates.
Two-year extension for telehealth
Good news! We have been ongoing supporters of telehealth expansion that resulted from the COVID-19 pandemic. The inclusion of this 2-year telehealth extension will allow doctors to continue to treat Medicare patients in a virtual setting. This is crucial since it allows patients to continue receiving treatment from their doctor in a virtual setting, and it provides patients and providers with certainty.
$2.5 billion increase for NIH
Good news! The omnibus allocates $47.5 billion for the National Institutes of Health’s budget, a $2.5 billion increase from 2023. The increased federal research funding is something we advocated for with congressional offices during Advocacy Day and will support GI researchers who are conducting innovative research and developing treatment for digestive diseases and GI cancers.
AGA-submitted report language on IBD included
Good news! Two language requests submitted by AGA on inflammatory bowel disease (IBD) were included in the omnibus: one in the 2023 Department of Labor, Health and Human Services, Education and Related Agencies funding bill and one in the 2023 Department of Agriculture, Rural Development, Food and Drug Administration and Related Agencies funding bill.
The first reaffirms the Appropriations Committee’s support for the NIH in funding basic, translational, and clinical studies on the diagnosis and treatment of IBD. The second encourages the FDA to improve diversity and patient-centricity in IBD clinical trials. The inclusion of these language requests in the omnibus highlights another successful advocacy effort by AGA.
Here’s what you need to know:
Medicare payment cuts
Unfortunately, physicians treating Medicare patients will face cuts in the new year.
It is disappointing that Congress failed to stop the full cuts. However, the Medicare payment cuts will be lower than the initially proposed 8.5% cut. Physicians will face a 2% cut because of the 4% in PAYGO relief for 2023 and 2024, plus an additional 2.5% in relief for the Centers for Medicare & Medicaid Services.
This is not an ideal outcome, but we are grateful to the more than 160 AGA members who raised their voices and sent over 600 messages to Congress. Your advocacy played a role in alleviating the final number of the cuts.
We will continue to urge Congress to stop the full cuts. Our top priority in 2023 remains addressing the Medicare reimbursement rates.
Two-year extension for telehealth
Good news! We have been ongoing supporters of telehealth expansion that resulted from the COVID-19 pandemic. The inclusion of this 2-year telehealth extension will allow doctors to continue to treat Medicare patients in a virtual setting. This is crucial since it allows patients to continue receiving treatment from their doctor in a virtual setting, and it provides patients and providers with certainty.
$2.5 billion increase for NIH
Good news! The omnibus allocates $47.5 billion for the National Institutes of Health’s budget, a $2.5 billion increase from 2023. The increased federal research funding is something we advocated for with congressional offices during Advocacy Day and will support GI researchers who are conducting innovative research and developing treatment for digestive diseases and GI cancers.
AGA-submitted report language on IBD included
Good news! Two language requests submitted by AGA on inflammatory bowel disease (IBD) were included in the omnibus: one in the 2023 Department of Labor, Health and Human Services, Education and Related Agencies funding bill and one in the 2023 Department of Agriculture, Rural Development, Food and Drug Administration and Related Agencies funding bill.
The first reaffirms the Appropriations Committee’s support for the NIH in funding basic, translational, and clinical studies on the diagnosis and treatment of IBD. The second encourages the FDA to improve diversity and patient-centricity in IBD clinical trials. The inclusion of these language requests in the omnibus highlights another successful advocacy effort by AGA.
Fast facts about gifts in a will and planned giving
Gifts to charitable organizations, such as the AGA Research Foundation, in your future plans ensure your support for our mission to fund young investigators continues even after your lifetime.
#1. Wills are not for older adults only.
Having a plan for the future is important – no matter your age. A will makes your wishes known and provides your loved ones with peace of mind.
#2. Planned gifts are not complicated or confusing.
They don’t have to be. There are many types of planned gifts: Most are simple and affordable, like a gift in your will or living trust. You just need to find the one that best meets your needs.
#3. Planned gifts are not for the wealthy only.
Anyone can make a planned gift. Gifts of all sizes make a difference at the AGA Research Foundation. In fact, you may even be able to make a bigger impact than you thought possible when you make a planned gift.
For 2023, consider including a gift to the AGA Research Foundation in your will. You will help support researchers and help spark future discoveries in GI.
Want to learn more about including a gift to the AGA Research Foundation in your future plans? Visit our website at https://gastro.planmylegacy.org or contact us at foundation@gastro.org.
Gifts to charitable organizations, such as the AGA Research Foundation, in your future plans ensure your support for our mission to fund young investigators continues even after your lifetime.
#1. Wills are not for older adults only.
Having a plan for the future is important – no matter your age. A will makes your wishes known and provides your loved ones with peace of mind.
#2. Planned gifts are not complicated or confusing.
They don’t have to be. There are many types of planned gifts: Most are simple and affordable, like a gift in your will or living trust. You just need to find the one that best meets your needs.
#3. Planned gifts are not for the wealthy only.
Anyone can make a planned gift. Gifts of all sizes make a difference at the AGA Research Foundation. In fact, you may even be able to make a bigger impact than you thought possible when you make a planned gift.
For 2023, consider including a gift to the AGA Research Foundation in your will. You will help support researchers and help spark future discoveries in GI.
Want to learn more about including a gift to the AGA Research Foundation in your future plans? Visit our website at https://gastro.planmylegacy.org or contact us at foundation@gastro.org.
Gifts to charitable organizations, such as the AGA Research Foundation, in your future plans ensure your support for our mission to fund young investigators continues even after your lifetime.
#1. Wills are not for older adults only.
Having a plan for the future is important – no matter your age. A will makes your wishes known and provides your loved ones with peace of mind.
#2. Planned gifts are not complicated or confusing.
They don’t have to be. There are many types of planned gifts: Most are simple and affordable, like a gift in your will or living trust. You just need to find the one that best meets your needs.
#3. Planned gifts are not for the wealthy only.
Anyone can make a planned gift. Gifts of all sizes make a difference at the AGA Research Foundation. In fact, you may even be able to make a bigger impact than you thought possible when you make a planned gift.
For 2023, consider including a gift to the AGA Research Foundation in your will. You will help support researchers and help spark future discoveries in GI.
Want to learn more about including a gift to the AGA Research Foundation in your future plans? Visit our website at https://gastro.planmylegacy.org or contact us at foundation@gastro.org.
Research Awards Program
Each year, the AGA Research Foundation provides research funding to transform the lives of talented investigators.
What will the practice of gastroenterology look like in 20 years? It is our hope that physicians have an abundance of new tools and treatments to care for their patients suffering from digestive disorders.
How will we get there? New treatments and devices are the result of years of research.
To help make this dream a reality, AGA – through the AGA Research Foundation – has made a commitment to support investigators in GI and hepatology with its Research Awards Program. In the past year, the AGA Research Foundation provided $2.5 million in research funding to 61 highly qualified investigators. These diverse researchers range from young investigators to more seasoned leaders in GI, all embarking on novel research projects that will advance our understanding of digestive conditions and pave the way for future discoveries in the field.
The AGA Research Foundation sincerely thanks all of its donors – without their contributions, this work wouldn’t be possible.
You can help spark the scientific breakthroughs of today so clinicians will have the tools to improve care tomorrow. Donate your tax-deductible gift today at www.gastro.org/donateonline.
Each year, the AGA Research Foundation provides research funding to transform the lives of talented investigators.
What will the practice of gastroenterology look like in 20 years? It is our hope that physicians have an abundance of new tools and treatments to care for their patients suffering from digestive disorders.
How will we get there? New treatments and devices are the result of years of research.
To help make this dream a reality, AGA – through the AGA Research Foundation – has made a commitment to support investigators in GI and hepatology with its Research Awards Program. In the past year, the AGA Research Foundation provided $2.5 million in research funding to 61 highly qualified investigators. These diverse researchers range from young investigators to more seasoned leaders in GI, all embarking on novel research projects that will advance our understanding of digestive conditions and pave the way for future discoveries in the field.
The AGA Research Foundation sincerely thanks all of its donors – without their contributions, this work wouldn’t be possible.
You can help spark the scientific breakthroughs of today so clinicians will have the tools to improve care tomorrow. Donate your tax-deductible gift today at www.gastro.org/donateonline.
Each year, the AGA Research Foundation provides research funding to transform the lives of talented investigators.
What will the practice of gastroenterology look like in 20 years? It is our hope that physicians have an abundance of new tools and treatments to care for their patients suffering from digestive disorders.
How will we get there? New treatments and devices are the result of years of research.
To help make this dream a reality, AGA – through the AGA Research Foundation – has made a commitment to support investigators in GI and hepatology with its Research Awards Program. In the past year, the AGA Research Foundation provided $2.5 million in research funding to 61 highly qualified investigators. These diverse researchers range from young investigators to more seasoned leaders in GI, all embarking on novel research projects that will advance our understanding of digestive conditions and pave the way for future discoveries in the field.
The AGA Research Foundation sincerely thanks all of its donors – without their contributions, this work wouldn’t be possible.
You can help spark the scientific breakthroughs of today so clinicians will have the tools to improve care tomorrow. Donate your tax-deductible gift today at www.gastro.org/donateonline.
What the election results mean for GI
In the Senate, Democrats clinched the majority with 50 seats. Only one race, Georgia, is still undecided where a December runoff is planned. This race will not flip the majority since Vice President Kamala Harris casts tie-breaking votes as the President of the Senate.
Republicans recaptured control of the House after reaching 218 seats – enough to take control but the sweeping flip “red wave” did not occur as predicted. Republicans currently hold 220 seats to 213 Democratic seats, while two seats remain undecided. Margins in both chambers are slim, reflecting the division in the country.
What does this mean?
The majorities in both chambers are razor thin and compromises will need to be made to pass funding bills and other priorities.
AGA will continue to prioritize our bipartisan efforts with congressional champions on both sides of the aisle, including Rep. Ami Bera (D-Calif.), Rep. Larry Bucshon (R-Ind.), Sen. Sherrod Brown (D-Ohio), and Sen. Bill Cassidy (R-La.). For the remainder of this Congress, we will fight to:
- Encourage the Senate to take a vote on the House-passed prior authorization reform bill.
- Support robust federal research funding for gastroenterology.
- Reduce dangerous cuts in the Medicare Physician Fee Schedule, effective Jan. 1, 2023.
In the Senate, Democrats clinched the majority with 50 seats. Only one race, Georgia, is still undecided where a December runoff is planned. This race will not flip the majority since Vice President Kamala Harris casts tie-breaking votes as the President of the Senate.
Republicans recaptured control of the House after reaching 218 seats – enough to take control but the sweeping flip “red wave” did not occur as predicted. Republicans currently hold 220 seats to 213 Democratic seats, while two seats remain undecided. Margins in both chambers are slim, reflecting the division in the country.
What does this mean?
The majorities in both chambers are razor thin and compromises will need to be made to pass funding bills and other priorities.
AGA will continue to prioritize our bipartisan efforts with congressional champions on both sides of the aisle, including Rep. Ami Bera (D-Calif.), Rep. Larry Bucshon (R-Ind.), Sen. Sherrod Brown (D-Ohio), and Sen. Bill Cassidy (R-La.). For the remainder of this Congress, we will fight to:
- Encourage the Senate to take a vote on the House-passed prior authorization reform bill.
- Support robust federal research funding for gastroenterology.
- Reduce dangerous cuts in the Medicare Physician Fee Schedule, effective Jan. 1, 2023.
In the Senate, Democrats clinched the majority with 50 seats. Only one race, Georgia, is still undecided where a December runoff is planned. This race will not flip the majority since Vice President Kamala Harris casts tie-breaking votes as the President of the Senate.
Republicans recaptured control of the House after reaching 218 seats – enough to take control but the sweeping flip “red wave” did not occur as predicted. Republicans currently hold 220 seats to 213 Democratic seats, while two seats remain undecided. Margins in both chambers are slim, reflecting the division in the country.
What does this mean?
The majorities in both chambers are razor thin and compromises will need to be made to pass funding bills and other priorities.
AGA will continue to prioritize our bipartisan efforts with congressional champions on both sides of the aisle, including Rep. Ami Bera (D-Calif.), Rep. Larry Bucshon (R-Ind.), Sen. Sherrod Brown (D-Ohio), and Sen. Bill Cassidy (R-La.). For the remainder of this Congress, we will fight to:
- Encourage the Senate to take a vote on the House-passed prior authorization reform bill.
- Support robust federal research funding for gastroenterology.
- Reduce dangerous cuts in the Medicare Physician Fee Schedule, effective Jan. 1, 2023.
AGA makes its first investment through new GI innovation fund
Virgo provides gastroenterologists, clinical trial sponsors, and trial site investigators with artificial intelligence–fueled, always-on endoscopic procedure recording and patient recruitment tools for clinical trials in gastroenterology, starting with inflammatory bowel disease clinical trials.
Virgo provides gastroenterologists, clinical trial sponsors, and trial site investigators with artificial intelligence–fueled, always-on endoscopic procedure recording and patient recruitment tools for clinical trials in gastroenterology, starting with inflammatory bowel disease clinical trials.
Virgo provides gastroenterologists, clinical trial sponsors, and trial site investigators with artificial intelligence–fueled, always-on endoscopic procedure recording and patient recruitment tools for clinical trials in gastroenterology, starting with inflammatory bowel disease clinical trials.
Joint society task force releases strategic plan on climate change
Key takeaway: As a procedure-intense subspecialty, gastroenterology, and in particular endoscopy, is a major contributor to health care’s carbon footprint and other environmental impacts. Endoscopy is the third largest generator of medical waste in a hospital (2 kg total waste per procedure) with most ending in landfills. With this strategic plan, the participating societies are committed to promoting and supporting a sustainable, high-quality GI practice.
The U.S. GI multisociety strategic plan, which has also been endorsed by 23 GI societies globally, is a collaborative effort that invites members to undertake initiatives to establish an environmentally sustainable, high-quality practice and promote planetary health. Each society will prioritize and adapt their initiatives in accordance with their individual societal goals. Some initiatives may be undertaken by a single society, whereas other objectives and initiatives may be approached jointly. It is a 5-year plan that covers seven major domains:
- Clinical setting.
- Education.
- Research.
- Society efforts.
- Intersociety efforts.
- Industry.
- Advocacy.
The plan was developed by the U.S. Multi-GI Society Task Force on Climate Change, which is composed of leading experts from AASLD, ACG, AGA, and ASGE.
For more information, view the full publication: GI Multisociety Strategic Plan on Environmental Sustainability, published in Gastroenterology, Gastrointestinal Endoscopy, HEPATOLOGY, and The American Journal of Gastroenterology.
Key takeaway: As a procedure-intense subspecialty, gastroenterology, and in particular endoscopy, is a major contributor to health care’s carbon footprint and other environmental impacts. Endoscopy is the third largest generator of medical waste in a hospital (2 kg total waste per procedure) with most ending in landfills. With this strategic plan, the participating societies are committed to promoting and supporting a sustainable, high-quality GI practice.
The U.S. GI multisociety strategic plan, which has also been endorsed by 23 GI societies globally, is a collaborative effort that invites members to undertake initiatives to establish an environmentally sustainable, high-quality practice and promote planetary health. Each society will prioritize and adapt their initiatives in accordance with their individual societal goals. Some initiatives may be undertaken by a single society, whereas other objectives and initiatives may be approached jointly. It is a 5-year plan that covers seven major domains:
- Clinical setting.
- Education.
- Research.
- Society efforts.
- Intersociety efforts.
- Industry.
- Advocacy.
The plan was developed by the U.S. Multi-GI Society Task Force on Climate Change, which is composed of leading experts from AASLD, ACG, AGA, and ASGE.
For more information, view the full publication: GI Multisociety Strategic Plan on Environmental Sustainability, published in Gastroenterology, Gastrointestinal Endoscopy, HEPATOLOGY, and The American Journal of Gastroenterology.
Key takeaway: As a procedure-intense subspecialty, gastroenterology, and in particular endoscopy, is a major contributor to health care’s carbon footprint and other environmental impacts. Endoscopy is the third largest generator of medical waste in a hospital (2 kg total waste per procedure) with most ending in landfills. With this strategic plan, the participating societies are committed to promoting and supporting a sustainable, high-quality GI practice.
The U.S. GI multisociety strategic plan, which has also been endorsed by 23 GI societies globally, is a collaborative effort that invites members to undertake initiatives to establish an environmentally sustainable, high-quality practice and promote planetary health. Each society will prioritize and adapt their initiatives in accordance with their individual societal goals. Some initiatives may be undertaken by a single society, whereas other objectives and initiatives may be approached jointly. It is a 5-year plan that covers seven major domains:
- Clinical setting.
- Education.
- Research.
- Society efforts.
- Intersociety efforts.
- Industry.
- Advocacy.
The plan was developed by the U.S. Multi-GI Society Task Force on Climate Change, which is composed of leading experts from AASLD, ACG, AGA, and ASGE.
For more information, view the full publication: GI Multisociety Strategic Plan on Environmental Sustainability, published in Gastroenterology, Gastrointestinal Endoscopy, HEPATOLOGY, and The American Journal of Gastroenterology.
What to know about 2023 Medicare payments
The Centers for Medicare and Medicaid Services released its final rules for 2023 Medicare payments.
Good news! The full CRC continuum will be covered in Medicare.
In a win for patients and thanks to our collective advocacy efforts from AGA and partner societies, CMS expanded the regulatory definition of “colorectal cancer screening tests” and will waive cost sharing for a necessary follow-up colonoscopy after a positive stool-based screening test.
Bad news: Looming cuts on the horizon, GI societies to take action.
The rule finalizes more than 4% in mandated Medicare physician reimbursement cuts through decreases in the conversion factor and expiration of temporary fixes passed by Congress. The CY 2023 conversion factor is $33.06, an unacceptable cut for our members. The GI societies continue to work with a coalition of national and state medical societies to urge Congress to prevent these cuts before Jan. 1, 2023.
Good news: ASC + hospital payments on the rise.
ASC payments and facility fee payments increase 3.8% for institutions that meet quality reporting requirements. The CY 2023 ASC conversion factor is $51.854 and the hospital outpatient conversion factor is $85.585.
CMS removed motility codes 91117 and 91122 from APC 5731, where their payments would have been cut 21%, and finalized their placement in APC 5722, where they get a 3% payment increase beginning Jan. 1, 2023. Thank you to the motility community for helping us secure this win.
CMS raises the hospital payment for ESD code C9779 to $3,260.69, a $765.65 increase from 2022. We continue to work with CMS on our request for separate codes for lower ESD and upper ESD and payments that better reflect their unique resource costs.
The Centers for Medicare and Medicaid Services released its final rules for 2023 Medicare payments.
Good news! The full CRC continuum will be covered in Medicare.
In a win for patients and thanks to our collective advocacy efforts from AGA and partner societies, CMS expanded the regulatory definition of “colorectal cancer screening tests” and will waive cost sharing for a necessary follow-up colonoscopy after a positive stool-based screening test.
Bad news: Looming cuts on the horizon, GI societies to take action.
The rule finalizes more than 4% in mandated Medicare physician reimbursement cuts through decreases in the conversion factor and expiration of temporary fixes passed by Congress. The CY 2023 conversion factor is $33.06, an unacceptable cut for our members. The GI societies continue to work with a coalition of national and state medical societies to urge Congress to prevent these cuts before Jan. 1, 2023.
Good news: ASC + hospital payments on the rise.
ASC payments and facility fee payments increase 3.8% for institutions that meet quality reporting requirements. The CY 2023 ASC conversion factor is $51.854 and the hospital outpatient conversion factor is $85.585.
CMS removed motility codes 91117 and 91122 from APC 5731, where their payments would have been cut 21%, and finalized their placement in APC 5722, where they get a 3% payment increase beginning Jan. 1, 2023. Thank you to the motility community for helping us secure this win.
CMS raises the hospital payment for ESD code C9779 to $3,260.69, a $765.65 increase from 2022. We continue to work with CMS on our request for separate codes for lower ESD and upper ESD and payments that better reflect their unique resource costs.
The Centers for Medicare and Medicaid Services released its final rules for 2023 Medicare payments.
Good news! The full CRC continuum will be covered in Medicare.
In a win for patients and thanks to our collective advocacy efforts from AGA and partner societies, CMS expanded the regulatory definition of “colorectal cancer screening tests” and will waive cost sharing for a necessary follow-up colonoscopy after a positive stool-based screening test.
Bad news: Looming cuts on the horizon, GI societies to take action.
The rule finalizes more than 4% in mandated Medicare physician reimbursement cuts through decreases in the conversion factor and expiration of temporary fixes passed by Congress. The CY 2023 conversion factor is $33.06, an unacceptable cut for our members. The GI societies continue to work with a coalition of national and state medical societies to urge Congress to prevent these cuts before Jan. 1, 2023.
Good news: ASC + hospital payments on the rise.
ASC payments and facility fee payments increase 3.8% for institutions that meet quality reporting requirements. The CY 2023 ASC conversion factor is $51.854 and the hospital outpatient conversion factor is $85.585.
CMS removed motility codes 91117 and 91122 from APC 5731, where their payments would have been cut 21%, and finalized their placement in APC 5722, where they get a 3% payment increase beginning Jan. 1, 2023. Thank you to the motility community for helping us secure this win.
CMS raises the hospital payment for ESD code C9779 to $3,260.69, a $765.65 increase from 2022. We continue to work with CMS on our request for separate codes for lower ESD and upper ESD and payments that better reflect their unique resource costs.