User login
Advancing Toward the Ideal Hospital Discharge for the Elderly Patient
The interval between hospital discharge and the continuity provider’s first post-hospital patient visit is being increasingly recognized as a hazardous hiatus (1). The patient is vulnerable to a variety of factors that may result in morbidity or hospital readmission, including the recurrence of symptoms that prompted the initial hospitalization, adverse drug events from new medications, new drug-drug interactions, or issues of care coordination, such as followup visits and tests. Inadequate social support can further exacerbate the medical complexity of care transition from the inpatient to the outpatient setting.
Many post-discharge adverse events are preventable or “ameliorable” by careful discharge planning and timely followup (1). However, existing guidelines and standards regarding the discharge process have been disease specific and have not focused on populations, such as the elderly, that may be at especially high risk regardless of their specific medical issues. For example, CMS currently requires that all patients have an assessment of cognition, mobility, and family support before final discharge plans are set. Experienced hospitalists know that these basic elements are only the beginning of a more complex and robust algorithm of discharge planning; including trimming and reconciling medications; planning followup tests; engineering followup appointments; and activating any required community resources, durable medical good needs, or home health care. In fact, many SHM members have already begun to implement local strategies to ease the care transition at the time of discharge.
The SHM Hospital Quality & Patient Safety (HQPS) Committee believes that hospitalists will play an important role in shaping the ideal discharge process. With support from the Hartford foundation, HQPS has formulated a strategy to develop “discharge best practices,” integrating evidence-based care with the experience and expert opinion of hospitalist leaders. To our knowledge, no national society or professional organization has undertaken such an activity to improve the quality of care at discharge and after hospitalization.
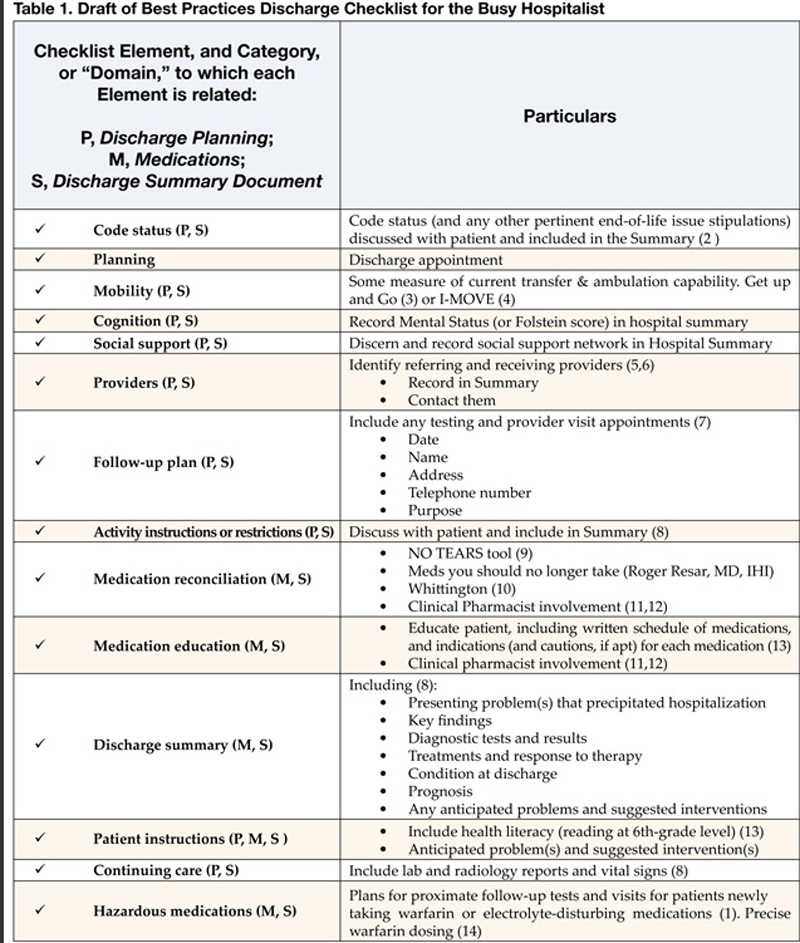
The process began with a literature review in 2004 that showed no commonly accepted compendium or consolidated list of activities that could form the basis for the ideal discharge. Drawing upon SHM member experience and the literature, HQPS committee members formulated a list of potential best practices, which are presented in Table 1. Although many discharge activities are required and many are done automatically (such as writing a discharge order or prescriptions) the committee chose to focus on important but discretionary activities that may be overlooked by a busy physician. To complement this checklist of activities, the committee is developing a discharge framework with the input of experts in the area of care transitions.
The committee held a consensus-building workshop at the SHM annual meeting entitled “Developing the Ideal Discharge Process.” This session provided a forum to discuss the checklist of best practices and discharge framework with attendees, receive their feedback, and identify hospitalists interested in validating and refining the materials over time. The committee will continue revising the materials in 2005, with the goal of developing a usable and valuable consensus statement addressing the steps involved in the ideal hospital discharge.
References
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161-7.
- Guidelines for appropriate use of “Do-Not-Resuscitate” orders. Council on Ethical and Judicial Affairs. American Medical Association. JAMA. 1991;265:1868-71.
- Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “getup and go” test. Arch Phys Med Rehabil. 1986;67:387-9.
- Manning DM, Keller AS, Frank DL. Independent Mobility Validation Exam (IMOVE): A tool for periodic reassessment of fallrisk and discharge planning. Abstract and poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- van Walraven C, Mamdani M, Fang J, Austin PC. Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004;19:624-31.
- van Walraven C, Seth R, Austin PC, Laupacis A. Effect of discharge summary availability during the post-discharge visits on hospital readmission. J Gen Intern Med. 2002;17:186-92.
- Whitford K, Huddleston JM. Specific appointments after pneumonia hospitalization reduce readmissions. Abstract and Poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- JCAHO Manual: Information Management (IM) 6.10 and Patient Care (PC) 15.30.
- Lewis T. Using the NO TEARS tool for medication review. BMJ. 2004;329:434.
- Whittington J, Cohen H. OSF healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-9.
- Kucukarslan SN, Peters M, Mlynarek M, Nafziger D. Pharmacists on rounding teams reduce preventable adverse events in hospital general medicine units. Arch Intern Med. 2003;163:2014-18.
- Dudas V, Bookwalter T, Kerr K, Pantilat SZ. The impact of followup telephone calls to patients after hospitalization. Am J Med. 2001;111(9B):26S-30S.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds. Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press; 2004.
- Manning DM. Toward safer warfarin therapy: does precise daily dosing improve international normalized ratio control? Mayo Clin Proc. 2002;77:873-5.
Resources (including Medline Search: “patient discharge” and/ or “quality indicators” and “quality of care”):
- Bull MJ, Hansen HE, Gross CR. Predictors of elder and family caregiver satisfaction with discharge planning. J Cardiovasc Nurs. 2000;14:76-87.
- Charles C, Gauld M, Chambers L, O’Brien B, Haynes RB, Labelle R. How was your hospital stay? Patients’ report about their care in Canadian hospitals. CMAJ. 1994; 150:1813-22.
- Cleary PD. A hospitalization from hell: a patient’s perspective on quality. Ann Intern Med. 2003:138:33-9.
- Demlo LK, Campbell PM. Improving hospital discharge data: lessons from the National Hospital Discharge Survey. Med Care. 1981 Oct;19(10):1030-40.
- Felden JM, scott S, Horne JG. An investigation of patient satisfaction following discharge after total hip replacement surgery. Orthop Nurs. 2003;22:429-36.
- Frain JP, Frain AE, Carr PH. Experience of medical senior house officers in preparing discharge summaries. BMJ. 1996;312:350.
- Gombeski WR, Miller PJ, Hahn JH, et al. Patient callback program. J Health Care Mark 1993;13:60-5.
- Hickey ML, Kleefield SF, Pearson SD, et al. Payer-hospital collaboration to improve patient satisfaction with hospital discharge. Jt Comm J Qual Improv. 1996;22:336-44.
- Kroenke K, Stump T, Clark DO, Callahan CM, McDonald CJ. Symptoms in hospitalized patients: outcome and satisfaction with care. Am J Med 1999;107: 425-31.
- Macaulay EM, Cooper GC, Engeset J, Naylor AR. Prospective audit of discharge summary errors. Br J Surg. 1996;83:788-90.
- Moher D, Weinberg A, Hanlon R, Runnalls K. Effects of a medical team coordinator on length of hospital stay. CMAJ. 1992;146:511-5.
- Minnick A, Young WB. Comparison between reports of care obtained by post-discharge telephone interview and pre-discharge personal interview. Outcomes Manag Nurs Pract 1999;3:32-7.
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home followup of hospitalized elders: a randomized clinical trial. JAMA. 1999;281:613-20.
- Parkes J, Shepperd S. Discharge planning from hospital to home. Cochrane Database Syst Rev. 2004. Review.
- Reiley P, Pike A, Phipps M, et al. Learning from patients: a discharge planning improvement project. Jt Comm J Qual Improv. 1996;22:31122.
- van Walraven C, Weinberg AL. Quality assessment of a discharge summary system. CMAJ. 1995;152:1437-42.
- van Walraven C, Rokosh E. What is necessary for high-quality discharge summaries? Am J Med Qual. 1999;14: 160-9.
- Zwicker D, Picariello G. Discharge planning for the older adult. In: Mezey M, Fulmer T, Abraaham I, Zwicker D, eds. Geriatric Nursing Protocols for Best Practice. 2nd ed. New York: Springer Publishing 2003;292-316.
The interval between hospital discharge and the continuity provider’s first post-hospital patient visit is being increasingly recognized as a hazardous hiatus (1). The patient is vulnerable to a variety of factors that may result in morbidity or hospital readmission, including the recurrence of symptoms that prompted the initial hospitalization, adverse drug events from new medications, new drug-drug interactions, or issues of care coordination, such as followup visits and tests. Inadequate social support can further exacerbate the medical complexity of care transition from the inpatient to the outpatient setting.
Many post-discharge adverse events are preventable or “ameliorable” by careful discharge planning and timely followup (1). However, existing guidelines and standards regarding the discharge process have been disease specific and have not focused on populations, such as the elderly, that may be at especially high risk regardless of their specific medical issues. For example, CMS currently requires that all patients have an assessment of cognition, mobility, and family support before final discharge plans are set. Experienced hospitalists know that these basic elements are only the beginning of a more complex and robust algorithm of discharge planning; including trimming and reconciling medications; planning followup tests; engineering followup appointments; and activating any required community resources, durable medical good needs, or home health care. In fact, many SHM members have already begun to implement local strategies to ease the care transition at the time of discharge.
The SHM Hospital Quality & Patient Safety (HQPS) Committee believes that hospitalists will play an important role in shaping the ideal discharge process. With support from the Hartford foundation, HQPS has formulated a strategy to develop “discharge best practices,” integrating evidence-based care with the experience and expert opinion of hospitalist leaders. To our knowledge, no national society or professional organization has undertaken such an activity to improve the quality of care at discharge and after hospitalization.
The process began with a literature review in 2004 that showed no commonly accepted compendium or consolidated list of activities that could form the basis for the ideal discharge. Drawing upon SHM member experience and the literature, HQPS committee members formulated a list of potential best practices, which are presented in Table 1. Although many discharge activities are required and many are done automatically (such as writing a discharge order or prescriptions) the committee chose to focus on important but discretionary activities that may be overlooked by a busy physician. To complement this checklist of activities, the committee is developing a discharge framework with the input of experts in the area of care transitions.
The committee held a consensus-building workshop at the SHM annual meeting entitled “Developing the Ideal Discharge Process.” This session provided a forum to discuss the checklist of best practices and discharge framework with attendees, receive their feedback, and identify hospitalists interested in validating and refining the materials over time. The committee will continue revising the materials in 2005, with the goal of developing a usable and valuable consensus statement addressing the steps involved in the ideal hospital discharge.
References
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161-7.
- Guidelines for appropriate use of “Do-Not-Resuscitate” orders. Council on Ethical and Judicial Affairs. American Medical Association. JAMA. 1991;265:1868-71.
- Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “getup and go” test. Arch Phys Med Rehabil. 1986;67:387-9.
- Manning DM, Keller AS, Frank DL. Independent Mobility Validation Exam (IMOVE): A tool for periodic reassessment of fallrisk and discharge planning. Abstract and poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- van Walraven C, Mamdani M, Fang J, Austin PC. Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004;19:624-31.
- van Walraven C, Seth R, Austin PC, Laupacis A. Effect of discharge summary availability during the post-discharge visits on hospital readmission. J Gen Intern Med. 2002;17:186-92.
- Whitford K, Huddleston JM. Specific appointments after pneumonia hospitalization reduce readmissions. Abstract and Poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- JCAHO Manual: Information Management (IM) 6.10 and Patient Care (PC) 15.30.
- Lewis T. Using the NO TEARS tool for medication review. BMJ. 2004;329:434.
- Whittington J, Cohen H. OSF healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-9.
- Kucukarslan SN, Peters M, Mlynarek M, Nafziger D. Pharmacists on rounding teams reduce preventable adverse events in hospital general medicine units. Arch Intern Med. 2003;163:2014-18.
- Dudas V, Bookwalter T, Kerr K, Pantilat SZ. The impact of followup telephone calls to patients after hospitalization. Am J Med. 2001;111(9B):26S-30S.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds. Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press; 2004.
- Manning DM. Toward safer warfarin therapy: does precise daily dosing improve international normalized ratio control? Mayo Clin Proc. 2002;77:873-5.
Resources (including Medline Search: “patient discharge” and/ or “quality indicators” and “quality of care”):
- Bull MJ, Hansen HE, Gross CR. Predictors of elder and family caregiver satisfaction with discharge planning. J Cardiovasc Nurs. 2000;14:76-87.
- Charles C, Gauld M, Chambers L, O’Brien B, Haynes RB, Labelle R. How was your hospital stay? Patients’ report about their care in Canadian hospitals. CMAJ. 1994; 150:1813-22.
- Cleary PD. A hospitalization from hell: a patient’s perspective on quality. Ann Intern Med. 2003:138:33-9.
- Demlo LK, Campbell PM. Improving hospital discharge data: lessons from the National Hospital Discharge Survey. Med Care. 1981 Oct;19(10):1030-40.
- Felden JM, scott S, Horne JG. An investigation of patient satisfaction following discharge after total hip replacement surgery. Orthop Nurs. 2003;22:429-36.
- Frain JP, Frain AE, Carr PH. Experience of medical senior house officers in preparing discharge summaries. BMJ. 1996;312:350.
- Gombeski WR, Miller PJ, Hahn JH, et al. Patient callback program. J Health Care Mark 1993;13:60-5.
- Hickey ML, Kleefield SF, Pearson SD, et al. Payer-hospital collaboration to improve patient satisfaction with hospital discharge. Jt Comm J Qual Improv. 1996;22:336-44.
- Kroenke K, Stump T, Clark DO, Callahan CM, McDonald CJ. Symptoms in hospitalized patients: outcome and satisfaction with care. Am J Med 1999;107: 425-31.
- Macaulay EM, Cooper GC, Engeset J, Naylor AR. Prospective audit of discharge summary errors. Br J Surg. 1996;83:788-90.
- Moher D, Weinberg A, Hanlon R, Runnalls K. Effects of a medical team coordinator on length of hospital stay. CMAJ. 1992;146:511-5.
- Minnick A, Young WB. Comparison between reports of care obtained by post-discharge telephone interview and pre-discharge personal interview. Outcomes Manag Nurs Pract 1999;3:32-7.
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home followup of hospitalized elders: a randomized clinical trial. JAMA. 1999;281:613-20.
- Parkes J, Shepperd S. Discharge planning from hospital to home. Cochrane Database Syst Rev. 2004. Review.
- Reiley P, Pike A, Phipps M, et al. Learning from patients: a discharge planning improvement project. Jt Comm J Qual Improv. 1996;22:31122.
- van Walraven C, Weinberg AL. Quality assessment of a discharge summary system. CMAJ. 1995;152:1437-42.
- van Walraven C, Rokosh E. What is necessary for high-quality discharge summaries? Am J Med Qual. 1999;14: 160-9.
- Zwicker D, Picariello G. Discharge planning for the older adult. In: Mezey M, Fulmer T, Abraaham I, Zwicker D, eds. Geriatric Nursing Protocols for Best Practice. 2nd ed. New York: Springer Publishing 2003;292-316.
The interval between hospital discharge and the continuity provider’s first post-hospital patient visit is being increasingly recognized as a hazardous hiatus (1). The patient is vulnerable to a variety of factors that may result in morbidity or hospital readmission, including the recurrence of symptoms that prompted the initial hospitalization, adverse drug events from new medications, new drug-drug interactions, or issues of care coordination, such as followup visits and tests. Inadequate social support can further exacerbate the medical complexity of care transition from the inpatient to the outpatient setting.
Many post-discharge adverse events are preventable or “ameliorable” by careful discharge planning and timely followup (1). However, existing guidelines and standards regarding the discharge process have been disease specific and have not focused on populations, such as the elderly, that may be at especially high risk regardless of their specific medical issues. For example, CMS currently requires that all patients have an assessment of cognition, mobility, and family support before final discharge plans are set. Experienced hospitalists know that these basic elements are only the beginning of a more complex and robust algorithm of discharge planning; including trimming and reconciling medications; planning followup tests; engineering followup appointments; and activating any required community resources, durable medical good needs, or home health care. In fact, many SHM members have already begun to implement local strategies to ease the care transition at the time of discharge.
The SHM Hospital Quality & Patient Safety (HQPS) Committee believes that hospitalists will play an important role in shaping the ideal discharge process. With support from the Hartford foundation, HQPS has formulated a strategy to develop “discharge best practices,” integrating evidence-based care with the experience and expert opinion of hospitalist leaders. To our knowledge, no national society or professional organization has undertaken such an activity to improve the quality of care at discharge and after hospitalization.
The process began with a literature review in 2004 that showed no commonly accepted compendium or consolidated list of activities that could form the basis for the ideal discharge. Drawing upon SHM member experience and the literature, HQPS committee members formulated a list of potential best practices, which are presented in Table 1. Although many discharge activities are required and many are done automatically (such as writing a discharge order or prescriptions) the committee chose to focus on important but discretionary activities that may be overlooked by a busy physician. To complement this checklist of activities, the committee is developing a discharge framework with the input of experts in the area of care transitions.
The committee held a consensus-building workshop at the SHM annual meeting entitled “Developing the Ideal Discharge Process.” This session provided a forum to discuss the checklist of best practices and discharge framework with attendees, receive their feedback, and identify hospitalists interested in validating and refining the materials over time. The committee will continue revising the materials in 2005, with the goal of developing a usable and valuable consensus statement addressing the steps involved in the ideal hospital discharge.
References
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161-7.
- Guidelines for appropriate use of “Do-Not-Resuscitate” orders. Council on Ethical and Judicial Affairs. American Medical Association. JAMA. 1991;265:1868-71.
- Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “getup and go” test. Arch Phys Med Rehabil. 1986;67:387-9.
- Manning DM, Keller AS, Frank DL. Independent Mobility Validation Exam (IMOVE): A tool for periodic reassessment of fallrisk and discharge planning. Abstract and poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- van Walraven C, Mamdani M, Fang J, Austin PC. Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004;19:624-31.
- van Walraven C, Seth R, Austin PC, Laupacis A. Effect of discharge summary availability during the post-discharge visits on hospital readmission. J Gen Intern Med. 2002;17:186-92.
- Whitford K, Huddleston JM. Specific appointments after pneumonia hospitalization reduce readmissions. Abstract and Poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- JCAHO Manual: Information Management (IM) 6.10 and Patient Care (PC) 15.30.
- Lewis T. Using the NO TEARS tool for medication review. BMJ. 2004;329:434.
- Whittington J, Cohen H. OSF healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-9.
- Kucukarslan SN, Peters M, Mlynarek M, Nafziger D. Pharmacists on rounding teams reduce preventable adverse events in hospital general medicine units. Arch Intern Med. 2003;163:2014-18.
- Dudas V, Bookwalter T, Kerr K, Pantilat SZ. The impact of followup telephone calls to patients after hospitalization. Am J Med. 2001;111(9B):26S-30S.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds. Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press; 2004.
- Manning DM. Toward safer warfarin therapy: does precise daily dosing improve international normalized ratio control? Mayo Clin Proc. 2002;77:873-5.
Resources (including Medline Search: “patient discharge” and/ or “quality indicators” and “quality of care”):
- Bull MJ, Hansen HE, Gross CR. Predictors of elder and family caregiver satisfaction with discharge planning. J Cardiovasc Nurs. 2000;14:76-87.
- Charles C, Gauld M, Chambers L, O’Brien B, Haynes RB, Labelle R. How was your hospital stay? Patients’ report about their care in Canadian hospitals. CMAJ. 1994; 150:1813-22.
- Cleary PD. A hospitalization from hell: a patient’s perspective on quality. Ann Intern Med. 2003:138:33-9.
- Demlo LK, Campbell PM. Improving hospital discharge data: lessons from the National Hospital Discharge Survey. Med Care. 1981 Oct;19(10):1030-40.
- Felden JM, scott S, Horne JG. An investigation of patient satisfaction following discharge after total hip replacement surgery. Orthop Nurs. 2003;22:429-36.
- Frain JP, Frain AE, Carr PH. Experience of medical senior house officers in preparing discharge summaries. BMJ. 1996;312:350.
- Gombeski WR, Miller PJ, Hahn JH, et al. Patient callback program. J Health Care Mark 1993;13:60-5.
- Hickey ML, Kleefield SF, Pearson SD, et al. Payer-hospital collaboration to improve patient satisfaction with hospital discharge. Jt Comm J Qual Improv. 1996;22:336-44.
- Kroenke K, Stump T, Clark DO, Callahan CM, McDonald CJ. Symptoms in hospitalized patients: outcome and satisfaction with care. Am J Med 1999;107: 425-31.
- Macaulay EM, Cooper GC, Engeset J, Naylor AR. Prospective audit of discharge summary errors. Br J Surg. 1996;83:788-90.
- Moher D, Weinberg A, Hanlon R, Runnalls K. Effects of a medical team coordinator on length of hospital stay. CMAJ. 1992;146:511-5.
- Minnick A, Young WB. Comparison between reports of care obtained by post-discharge telephone interview and pre-discharge personal interview. Outcomes Manag Nurs Pract 1999;3:32-7.
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home followup of hospitalized elders: a randomized clinical trial. JAMA. 1999;281:613-20.
- Parkes J, Shepperd S. Discharge planning from hospital to home. Cochrane Database Syst Rev. 2004. Review.
- Reiley P, Pike A, Phipps M, et al. Learning from patients: a discharge planning improvement project. Jt Comm J Qual Improv. 1996;22:31122.
- van Walraven C, Weinberg AL. Quality assessment of a discharge summary system. CMAJ. 1995;152:1437-42.
- van Walraven C, Rokosh E. What is necessary for high-quality discharge summaries? Am J Med Qual. 1999;14: 160-9.
- Zwicker D, Picariello G. Discharge planning for the older adult. In: Mezey M, Fulmer T, Abraaham I, Zwicker D, eds. Geriatric Nursing Protocols for Best Practice. 2nd ed. New York: Springer Publishing 2003;292-316.