User login
Is it time to rethink the use of oral contraceptives in premenopausal women with migraine?
Part 1 Data dissection
- Migraine versus migraine with aura versus tension headache
- Baseline risk of stroke in patients with migraine
- What does the literature suggest about the risk of stroke associated with combination oral contraceptives (OCs) in women with migraine?
- What have been the objections in the past to OC use in women with migraine?
![]()
Part 2 Successful interventions for avoiding menstrual headache
- How might women with migraine benefit from OCs?
- Estrogen dose: Does it make a difference in headache avoidance?
- Is low dose or continuous OC use the best option for contraception in women with migraine?
- Should an ObGyn consult with a headache specialist before prescribing combination OCs to women with migraine?
![]()
Download transcript for Part 1
Part 1 Data dissection
- Migraine versus migraine with aura versus tension headache
- Baseline risk of stroke in patients with migraine
- What does the literature suggest about the risk of stroke associated with combination oral contraceptives (OCs) in women with migraine?
- What have been the objections in the past to OC use in women with migraine?
![]()
Part 2 Successful interventions for avoiding menstrual headache
- How might women with migraine benefit from OCs?
- Estrogen dose: Does it make a difference in headache avoidance?
- Is low dose or continuous OC use the best option for contraception in women with migraine?
- Should an ObGyn consult with a headache specialist before prescribing combination OCs to women with migraine?
![]()
Download transcript for Part 1
Part 1 Data dissection
- Migraine versus migraine with aura versus tension headache
- Baseline risk of stroke in patients with migraine
- What does the literature suggest about the risk of stroke associated with combination oral contraceptives (OCs) in women with migraine?
- What have been the objections in the past to OC use in women with migraine?
![]()
Part 2 Successful interventions for avoiding menstrual headache
- How might women with migraine benefit from OCs?
- Estrogen dose: Does it make a difference in headache avoidance?
- Is low dose or continuous OC use the best option for contraception in women with migraine?
- Should an ObGyn consult with a headache specialist before prescribing combination OCs to women with migraine?
![]()
Download transcript for Part 1
Men, women, and migraine: The role of sex, hormones, obesity, and PTSD
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
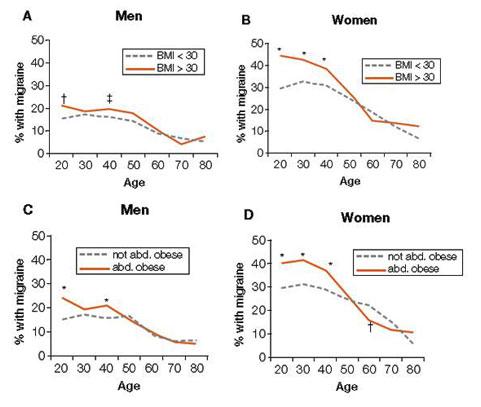
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
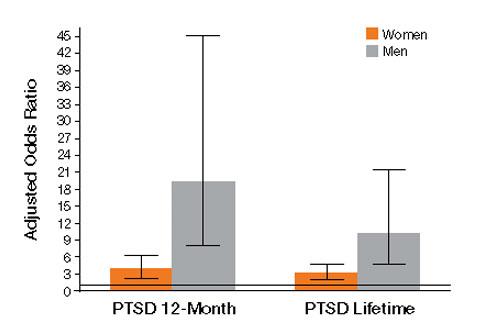
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
The gynecologist’s role in managing menstrual migraine
A.G. is a student who misses 2 or 3 days of school each month because of debilitating menstrual migraine (MM) with vomiting. Her referring physician prescribed topiramate, but the drug caused bothersome cognitive effects without relieving her headaches. She is taking a 30-μg oral contraceptive (OC) that contains ethinyl estradiol and drospirenone. Despite starting and stopping the OC several times, she has had no relief. She also takes 100 mg topiramate at bedtime, and 7 to 10 tablets of sumatriptan (100 mg) a month—usually during the menstrual week.
The ObGyn discontinues topiramate and changes dosing of the OC to active pills only for 12 consecutive weeks. During the 13th week, the patient is instructed to take 0.9 mg conjugated equine estrogens twice daily for 7 days before resuming extended-cycle oral contraception. This regimen completely eliminates menstrual migraine. The infrequent migraines the patient does experience—which she attributes to weather fronts—are successfully managed with no more than two doses of a triptan in a month.
A busy gynecology practice sees more migraineurs in a day than a neurology practice sees in a month. But most of the migraineurs who visit gynecology offices have a chief complaint other than headache, and most leave without having mentioned the migraine—returning home to continue treating themselves with the same remedies their mothers used. Many of these women fail to seek a specific diagnosis, or treatment, until they develop chronic daily headaches or become unable to work.
Current theories of migraine implicate spreading cortical depression; trigeminal nerve activation with attendant vasodilation; and neurogenic inflammation.
Menstrual migraine (MM) is, arguably, the most common disabling condition encountered in women’s health. These migraines are more severe, last longer, and are more resistant to treatment than those that occur at other times in the cycle.1,2 And, although headache specialists are adept at diagnosing migraine and prescribing a host of antiepileptic drugs and other migraine preventives, many of these specialists are uncomfortable manipulating the hormonal underpinnings of these “super migraines.”
This article outlines diagnostic criteria, treatment options, and preventive strategies, including hormonal therapy. In the process, it demonstrates how, in many cases, a gynecologist’s expertise in managing hormonal triggers may be the determinant of successful treatment.
Migraine prefers women
Migraine is the most common of all disabling headaches and afflicts 13% of the US population, but with a markedly skewed distribution: It preferentially attacks women in a 3:1 preponderance. The lifetime prevalence of migraine in women is 33%. Migraine strikes women primarily during reproductive years, when many women seek routine health care from a gynecologist rather than an internist or general practitioner.3
Menstrual migraine is defined as migraine without aura that occurs in predictable association with menses. Its onset falls within a 5-day window, spanning 2 days before the onset of menses through the third day of bleeding.5 Although the complete exclusion of migraine with aura from diagnostic criteria is controversial, headache specialists generally agree that aura is uncommonly associated with MM, probably owing to the low-estrogen environment. (Higher concentrations of estrogen are associated with an increased likelihood of aura, similar to the association between estrogen and seizure activity.)
The migraine trigger appears to be estrogen withdrawal in susceptible persons—either during the natural menstrual cycle or as a result of cycling onto inert pills in an oral contraceptive (OC) regimen. A population study found that 39% of menstruating women experience headaches with menses, and almost one third of these headaches meet established criteria for MM or menstrual-related migraine.4
The distinction between these two entities, MM and menstrual-related migraine, is largely semantic. With MM, the menstrual attack is the patient’s only migraine. The broader term implies that she may have other attacks in addition to the menstrual ones. In this article, I’ve gathered both categories under the term MM, which also includes headaches that arise at the time of estrogen withdrawal associated with OC use.
Regardless of what we call them, these headaches have proved to be particularly vexing to headache medicine specialists who hesitate to address hormonal factors.
Diagnostic criteria are clear
Formal diagnosis of migraine requires that at least two of four signature characteristics plus at least one of two associated symptoms be present.5 The four characteristics are:
- moderate or severe pain
- throbbing
- unilateral location
- intensification of headache upon activity.
Any combination of two suffices for diagnosis—much to the astonishment of many patients who mistakenly believe that migraine must be severe or one-sided.
Associated symptoms include either nausea or both photophobia and phonophobia, the latter often signified by the simple preference to be in a dark, quiet room during an attack.
Untreated, migraine usually lasts between 4 and 72 hours.
A practical, clinical approach to diagnosis is to look for the episodic disabling headache. By disabling, I mean the presence of associated nausea or the need to stop one’s activities and lie down. A stable history of attacks with predictable menstrual association offers further confirmation.
Neck tension may be present
Symptoms of neck tension do not rule out migraine. In fact, neck pain is far more common at the time of treatment than is nausea, and migraineurs frequently describe neck pain that radiates forward during an attack.6
Treatment options begin with NSAIDs
Initial treatment of MM is no different than that of other migraines. Mild and moderate attacks can often be managed with nonsteroidal anti-inflammatory drugs (NSAIDs), which concomitantly treat comorbid dysmenorrhea.
A small randomized trial found that mefenamic acid (500 mg every 8 hours, as needed) was superior to placebo for acute MM, and a small crossover trial compared two formulations of diclofenac—50-mg sachets and tablets—with placebo in the treatment of acute migraine (TABLE). Almost one quarter of the patients taking the sachet form were pain-free at 2 hours, compared with 18.5% of patients taking the tablets and 11.7% of those who received placebo.7,8
Injectable ketorolac is more potent and is proving to be as effective as or more effective than triptans or opioids for severe, persistent migraine.
When migraine is more severe, or when NSAIDs no longer suffice, treatment advances to migraine-specific medications—specifically, ergotamines and triptans.
Brand names of drugs mentioned in this article
| Drug | Brand name |
|---|---|
| NSAIDs | |
| Diclofenac sodium | Voltaren (and others) |
| Ketorolac tromethamine | Toradol (and others) |
| Mefenamic acid | Ponstel (and others) |
| Naproxen sodium | Naprelan (and others) |
| Triptans | |
| Eletriptan hydrobromide | Relpax |
| Frovatriptan succinate | Frova |
| Naratriptan hydrochloride | Amerge |
| Sumatriptan succinate | Imitrex |
| Ergotamines | |
| Dihydroergotamine mesylate | D.H.E. 45, Migranal |
| Other | |
| Butalbital, acetaminophen, and caffeine | Fioricet |
| Leuprolide acetate | Lupron, Eligard |
Ergots and ergotamines have varied safety profiles in pregnancy
Dihydroergotamine belongs to the oldest family of migraine-specific drugs, although it is not widely used today. One reason may be that most migraineurs are women of reproductive age, and ergots are oxytocic and potential teratogens. Furthermore, they are not recommended in lactation. Ergotamines, however, are quite diverse, and some have more acceptable FDA use-in-pregnancy ratings. Injectable dihydroergotamine appears to be as effective as or less effective than triptans for migraine pain, but more effective than other drugs, such as NSAIDs or analgesics, for acute attacks.9 The nasal spray is more effective than placebo, but less effective than triptans.9
Triptans are relatively safe for women of reproductive age
Most information on use of triptans in pregnancy concerns sumatriptan. Like all triptans, it falls into Category C; however, its published profile is reassuring.10-12 Data from Sweden on 2,027 first-trimester exposures show a 3.6% risk of birth defects (major and minor), compared with an identical 3.6% risk in the general Swedish population.12 Sumatriptan is considerably less lipophilic than most of the drugs in its class and has been rated as compatible with breastfeeding.13
All triptans except eletriptan have been studied in the treatment of acute MM and found to be superior to placebo.14 These serotonin 1B/1D agonists are tailored therapy for acute migraine because, unlike analgesics, they address the underlying pathology of the attack, inhibiting the release of vasoactive peptides, promoting selective meningeal vasoconstriction, and blocking pain pathways in the brainstem. They also resolve the associated symptoms of nausea and photophobia. Triptans should not be used in the presence of untreated hypertension or vascular disease (cardiovascular, cerebrovascular, or peripheral vascular disease).
Watch for “rebound” headache. Like all acute treatment—be it a simple analgesic, NSAID, caffeine-containing compound, butalbital, ergotamine, or opioid—too-frequent use of triptans can produce medication-overuse headache, also referred to as rebound headache. In general, try to limit the use of agents for acute migraine, whether prescription or over-the-counter, to no more than 2 days a week to avoid this consequence. Also, be aware that some agents—notably, butalbital-containing compounds—may cause rebound headache, even when given as infrequently as 5 days of the month.15
Some preventive strategies are “nonspecific”
When treatment of acute MM is inadequate, management shifts toward prevention. Options include nonspecific (those that do not address the hormonal trigger) and specific (hormonal) strategies. Nonspecific strategies rely on the predictable onset of MM for proper timing of the therapeutic intervention; therefore, women who have irregular cycles are not good candidates for this approach. The presence of comorbid conditions such as dysmenorrhea, menometrorrhagia, and endometriosis may argue for early adoption of specific strategies that improve both conditions at once.
The fact that menstrual migraine (MM) is associated with estrogen withdrawal prompts a question: What happens immediately postpartum, when estrogen levels decline with loss of the placenta?
Although hormonal fluctuations generally stabilize during pregnancy, and most menstrual migraineurs experience fewer headaches during gestation, that protective effect erodes at delivery, when the incidence of migraine can be as high as 40% in the first week.41
Investigators who prospectively studied 49 migraineurs—two of whom were affected by migraine with aura and 47 by migraine without aura—found improvement in 46.8% of these women during the first trimester of pregnancy, 83% during the second trimester, and 87.2% during the third trimester, with complete remission rates of 10.6%, 53.2%, and 78.7%, respectively.42 During the first postpartum week, migraine recurred in 34% of women.42 Interestingly, women who had a history of MM were less likely to improve during the first and third trimesters of pregnancy.42
In a separate prospective investigation of 985 women who delivered over a 3-month period in one tertiary-care facility, 381 experienced postpartum headache.43 The median time to onset of the headache was 2 days, and the median duration was 4 hours. More than 75% of these headaches were primary headaches.43 Only a small percentage (4%) were incapacitating.43
When migraine may signal a more serious condition
Another question arises when a woman experiences a severe headache shortly after delivery: Could the headache be related to preeclampsia or another serious complication of pregnancy and delivery? According to Contag and colleagues, immediate assessment may be warranted.44
“Characteristics to consider are the association of the headache with elevated blood pressure (which could signal postpartum preeclampsia), the sudden onset of an atypical headache, and variations to the usual nature of the migraine, such as the onset of new neurological symptoms. Postpartum women with any of these characteristics should be evaluated in the emergency department, and neuroimaging should be strongly considered,” they write.44
Treatment reverts to prepregnancy options
Assuming preeclampsia or another serious condition is not the culprit, the treatment options for postpartum migraine revert to prepregnancy choices, as effect on the developing fetus is no longer a concern. Nonsteroidal anti-inflammatory drugs (NSAIDs) are the first line of therapy. If they are ineffective, proceed to an ergotamine or triptan.—Janelle Yates, Senior Editor
Nonhormonal (nonspecific) therapy NSAIDs may provide some relief. In one small study, naproxen sodium (550 mg twice daily) was administered for 2 weeks, beginning 1 week before the anticipated onset of menses. It modestly reduced the overall duration and severity of menstrual migraine16—a benefit that must be weighed against the risk of adverse events and the more recent FDA black box warning about its potentially serious heart and gastrointestinal risks.
Triptan regimens may prevent MM. Several triptans have been investigated for prevention of MM. A small, open-label study evaluated the use of oral sumatriptan (25 mg three times daily), beginning 2 to 3 days before the anticipated onset of MM and continuing for 5 days.17 Menstrual attacks were prevented in just over 50% of cases.
Naratriptan (1 mg twice daily), beginning 2 days before anticipated menses and continuing for 5 days, reduced the number of MM attacks by 50%, with side effects comparable to placebo.18 A higher dosage (2.5 mg twice daily) did not prove to be superior to placebo, for unexplained reasons.
In a similar trial, frovatriptan (2.5 mg daily or 2.5 mg twice daily), beginning 2 days before the anticipated onset of MM and continuing for 6 days, prevented at least 50% of MM.19 Twice-daily dosing was superior to daily administration.
Magnesium may shorten MM. In one small study, oral magnesium (360 mg daily), beginning on the 15th day of the cycle and continuing through the menses, shortened the duration of MM and improved menstrual complaints better than placebo.20
The goal of hormonal therapy is to eliminate or sufficiently minimize the premenstrual decline in estrogen that is believed to precipitate MM.21 An observational study of 229 women found that hormonal strategies prevented MM in 73% of cases (81% when taken as directed).22
It is fortunate that MM, by definition, is migraine without aura, because the use of combined OCs has been controversial in the setting of migraine with aura. International studies have reported a small but increased risk of stroke associated with their use, although a subset of women with migraine had no increased risk.23-25 In contrast, no U.S. study since 1975 has found an increased risk of stroke associated with the use of OCs.26 One large domestic study reviewed 3.6 million woman-years of use and found no increased risk of ischemic stroke with the low-dose OCs currently available, nor did a pooled analysis of U.S. studies.27,28
The discrepancy is likely explained by the strong relative contraindication, in the United States, to the use of OCs in smokers older than 35 years (the smoking prevalence in most of the European case series was more than 50%), as well as the more prevalent use of high-dose OCs in the international studies. High-dose pills were implicated in the majority of stroke cases in the World Health Organization (WHO) study, but were used by only 0.7% of cases and controls in the pooled U.S. studies.23 Nevertheless, both ACOG and WHO concluded that the risk of OC use usually outweighs the benefit in women older than 35 years whose migraines are complicated by focal neurologic deficits.
Extended-cycle OCs may offer a lengthy reprieve. Regimens that forego monthly withdrawal bleeds and provide extended administration of active pills can afford migraineurs a lengthy reprieve from MM.29 Breakthrough bleeding is the most common side effect but tends to decrease over time. It is preferable for the patient to take the pill at bedtime to avoid a drug nadir during susceptible stages of sleep, which may be associated with migraine generation. It also is prudent to avoid concomitant administration of drugs that might increase the rate of hepatic metabolism of estrogen (e.g., a high dosage of topiramate) and lead to a more rapid decline in concentration.
When using an extended-cycle regimen that allows for periodic withdrawal bleeds, give the patient supplemental estrogen during the withdrawal week if the decline in ethinyl estradiol (EE) exceeds 10 μg, a threshold that appears to elicit MM in susceptible women.21,22 For example, with an extended-cycle regimen that contains 30 μg of EE, it may be necessary to add 20 μg of estrogen during the placebo week to prevent MM, whereas an extended-cycle regimen that contains 20 μg EE, declining to 10 μg during the 13th week, would be adequate as packaged.
21/7 hormonal OCs may require supplemental estrogen to prevent MM. The late luteal-phase decline in estradiol concentration during the natural menstrual cycle is equivalent to the decline experienced with the transition to inert pills in 20- to 25-μg EE formulations. Therefore, these regimens confer the same risk of MM as the woman’s natural cycle. Products that contain incrementally higher dosages of EE (30, 35, and 50 μg) confer an increasingly greater risk of MM. Supplementation of estrogen during the placebo week may prevent MM by limiting the decline in estrogen.
In a small, open-label study, women took an OC containing 20 μg EE at bedtime on days 1 to 21 of the cycle, followed by 0.9 mg of conjugated equine estrogens (CEE) on days 22 to 28. All patients reported a reduction in migraine frequency of at least 50%, with a mean reduction of 78%.30
Parenteral options can be created utilizing a transdermal 20-μg EE/norelgestromin patch or a 15-μg EE/etonogestrel vaginal ring. With the first approach, I recommend adding a 0.1-mg EE patch during the withdrawal week to prevent MM. With the latter, a 0.075-mg EE patch may be used during the week following ring removal.31
Consider a menstrually targeted estrogen supplement. Some women who have contraindications to use of an OC may still be candidates for targeted strategies using lower dosages of supplemental estrogen rather than a combination OC. Among the options is perimenstrual administration of an estradiol patch or gel.32 One study found a 0.1-mg estrogen patch (worn 7 days and applied just before the expected onset of menses) to be effective, but lower dosages (0.025 to 0.05 mg EE) were not.33 Daily application of 1.5 mg estradiol gel for 7 days, beginning before the onset of MM, was also effective in preventing MM.34-36
With targeted strategies, timing is critical; if estrogen is begun too early, the incidence of migraine may rise after cessation.36
GnRH agonists may benefit women who have isolated MM. Administration of gonadotropin-releasing hormone (GnRH) agonists has been shown to ease MM, but the baseline frequency of headaches appears to be an important variable in the success of these agents.37-39 Leuprolide acetate markedly diminished MM in women who seldom experienced headaches other than their menstrual attacks.37 It did not benefit women who experienced migraine in the setting of chronic headache (≥15 days/month), probably because chronic migraine is influenced by other variables, such as nonrestorative sleep and overuse of medication.15,38,40
No evidence that progestin-only contraceptives are effective. Although these agents have been proposed for treatment of migraine, evidence of their benefit is lacking. It is my opinion that, more often than not, they exacerbate migraine.
1. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63(2):351-353.
2. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24(9):707-716.
3. Launer LJ, Terwindt GM, Ferrari MD. The prevalence and characteristics of migraine in a population-based cohort: the GEM study. Neurology. 1999;53(3):537-542.
4. Couturier EG, Bomhof MA, Neven AK, van Duijn NP. Menstrual migraine in a representative Dutch population sample: prevalence, disability and treatment. Cephalalgia. 2003;23(4):302-308.
5. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders. 2nd ed. Cephalalgia. 2004;24(suppl 1):9-160.
6. Calhoun AH, Ford S, Millen C, Finkel AG, Truong Y, Nie Y. The prevalence of neck pain in migraine [abstract]. Headache. 2010 Jan 20.-[Epub ahead of print].
7. Al-Waili NS. Treatment of menstrual migraine with prostaglandin synthesis inhibitor mefenamic acid: double-blind study with placebo. Eur J Med Res. 2000;5(4):176-182.
8. Diener HC, Montagna P, Gács G, et al. Efficacy and tolerability of diclofenac potassium sachets in migraine: a randomized, double-blind, cross-over study in comparison with diclofenac potassium tablets and placebo. Cephalalgia. 2006;26(5):537-547.
9. Schürks M. Dihydroergotamine: role in the treatment of migraine. Expert Opin Drug Metab Toxicol. 2009;5(9):1141-1148.
10. Loder E. Safety of sumatriptan in pregnancy: a review of the data so far. CNS Drugs. 2003;17(1):1-7.
11. Shuhaiber S, Pastuszak A, Schick B, et al. Pregnancy outcome following first trimester exposure to sumatriptan. Neurology. 1998;51(2):581-583.
12. Cunnington M, Ephross S, Churchill P. The safety of sumatriptan and naratriptan in pregnancy: what have we learned? Headache. 2009;49(10):1414-1422.
13. Ressel G. AAP updates statement for transfer of drugs and other chemicals into breast milk. American Academy of Pediatrics. Am Fam Physician. 2002;65(5):979-980.
14. Ashkenazi A, Silberstein S. Menstrual migraine: a review of hormonal causes, prophylaxis and treatment. Expert Opin Pharmacother. 2007;8(11):1605-1613.
15. Bigal ME, Serrano D, Buse D, Scher A, Stewart WF, Lipton RB. Acute migraine medications and evolution from episodic to chronic migraine: a longitudinal population-based study. Headache. 2008;48(8):1157-1168.
16. Sances G, Martignoni E, Fioroni L, Blandini F, Facchinetti F, Nappi G. Naproxen sodium in menstrual migraine prophylaxis: a double-blind placebo controlled study. Headache. 1990;30(11):705-709.
17. Newman LC, Lipton RB, Lay CL, Solomon S. A pilot study of oral sumatriptan as intermittent prophylaxis of menstruation-related migraine. Neurology. 1998;51(1):307-309.
18. Newman L, Mannix LK, Landy S, et al. Naratriptan as short-term prophylaxis of menstrually associated migraine: a randomized, double-blind, placebo-controlled study. Headache. 2001;41(3):248-256.
19. Silberstein SD, Elkind AH, Schreiber C, Keywood C. A randomized trial of frovatriptan for the intermittent prevention of menstrual migraine. Neurology. 2004;63(2):261-269.
20. Facchinetti F, Sances G, Borella P, Genazzani AR, Nappi G. Magnesium prophylaxis of menstrual migraine: effects on intracellular magnesium. Headache. 1991;31(5):298-301.
21. Calhoun A. Women’s Issues in Headache. In: Loder E, ed. Headache. Philadelphia: American College of Physicians; 2004:157-177.
22. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48(8):1186-1193.
23. Ischaemic stroke and combined oral contraceptives: results of an international, multicentre, case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet. 1996;348:498-505.
24. Chan WS, Ray J, Wai EK, et al. Risk of stroke in women exposed to low-dose oral contraceptives: a critical evaluation of the evidence. Arch Intern Med. 2004;164(7):741-747.
25. Etminan M, Takkouche B, Isorna FC, Samii A. Risk of ischaemic stroke in people with migraine: systematic review and meta-analysis of observational studies. BMJ. 2005;330(7482):63.-
26. Oral contraceptives and stroke in young women. Associated risk factors. JAMA. 1975;231:718-722.
27. Petitti DB, Sidney S, Bernstein A, Wolf S, Quesenberry C, Ziel HK. Stroke in users of low-dose oral contraceptives. N Engl J Med. 1996;335(1):8-15.
28. Schwartz SM, Petitti DB, Siscovick DS, et al. Stroke and use of low-dose oral contraceptives in young women: a pooled analysis of two US studies. Stroke. 1998;29(11):2277-2284.
29. Sulak PJ, Scow RD, Preece C, Riggs MW, Kuehl TJ. Hormone withdrawal symptoms in oral contraceptive users. Obstet Gynecol. 2000;95(2):261-266.
30. Calhoun AH. A novel specific prophylaxis for menstrual-associated migraine. South Med J. 2004;97(9):819-822.
31. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep. 2009;13(5):381-385.
32. Pringsheim T, Davenport WJ, Dodick D. Acute treatment and prevention of menstrually related migraine headache: evidence-based review. Neurology. 2008;70(17):1555-1563.
33. Pradalier A VD, Beaulieu PH, et al. Correlation between oestradiol plasma level and therapeutic effect on menstrual migraine. In: FC Rose, ed. New advances in headache research. London: Smith-Gordon; 1994:129-132.
34. de Lignières B, Vincens M, Mauvais-Jarvis P, Mas JL, Touboul PJ, Bousser MG. Prevention of menstrual migraine by percutaneous oestradiol. Br Med J (Clin Res Ed). 1986;293(6561):1540.-
35. Dennerstein L, Morse C, Burrows G, Oats J, Brown J, Smith M. Menstrual migraine: a double-blind trial of percutaneous estradiol. Gynecol Endocrinol. 1988;2(2):113-120.
36. MacGregor EA, Frith A, Ellis J, Aspinall L, Hackshaw A. Prevention of menstrual attacks of migraine: a double-blind placebo-controlled crossover study. Neurology. 2006;67(12):2159-2163.
37. Murray SC, Muse KN. Effective treatment of severe menstrual migraine headaches with gonadotropin-releasing hormone agonist and “add-back” therapy. Fertil Steril. 1997;67(2):390-393.
38. Martin V, Wernke S, Mandell K, et al. Medical oophorectomy with and without estrogen add-back therapy in the prevention of migraine headache. Headache. 2003;43(4):309-321.
39. Lichten EM, Lichten JB, Whitty A, Pieper D. The confirmation of a biochemical marker for women’s hormonal migraine: the depo-estradiol challenge test. Headache. 1996;36(6):367-371.
40. Calhoun AH, Ford S. Behavioral sleep modification may revert transformed migraine to episodic migraine. Headache. 2007;47(8):1178-1183.
41. Stein GS. Headaches in the first postpartum week and their relationship to migraine. Headache. 1981;21(5):201-205.
42. Sances G, Granella F, Nappi RE, et al. Course of migraine during pregnancy and postpartum: a prospective study. Cephalalgia. 2003;23(3):197-205.
43. Goldszmidt E, Kern R, Chaput A, Macarthur A. The incidence and etiology of postpartum headaches: a prospective cohort study. Can J Anaesth. 2005;52(9):971-977.
44. Contag SA, Mertz HL, Bushnell CD. Migraine during pregnancy: Is it more than a headache? Nat Rev Neurol. 2009;5(8):449-456.
A.G. is a student who misses 2 or 3 days of school each month because of debilitating menstrual migraine (MM) with vomiting. Her referring physician prescribed topiramate, but the drug caused bothersome cognitive effects without relieving her headaches. She is taking a 30-μg oral contraceptive (OC) that contains ethinyl estradiol and drospirenone. Despite starting and stopping the OC several times, she has had no relief. She also takes 100 mg topiramate at bedtime, and 7 to 10 tablets of sumatriptan (100 mg) a month—usually during the menstrual week.
The ObGyn discontinues topiramate and changes dosing of the OC to active pills only for 12 consecutive weeks. During the 13th week, the patient is instructed to take 0.9 mg conjugated equine estrogens twice daily for 7 days before resuming extended-cycle oral contraception. This regimen completely eliminates menstrual migraine. The infrequent migraines the patient does experience—which she attributes to weather fronts—are successfully managed with no more than two doses of a triptan in a month.
A busy gynecology practice sees more migraineurs in a day than a neurology practice sees in a month. But most of the migraineurs who visit gynecology offices have a chief complaint other than headache, and most leave without having mentioned the migraine—returning home to continue treating themselves with the same remedies their mothers used. Many of these women fail to seek a specific diagnosis, or treatment, until they develop chronic daily headaches or become unable to work.
Current theories of migraine implicate spreading cortical depression; trigeminal nerve activation with attendant vasodilation; and neurogenic inflammation.
Menstrual migraine (MM) is, arguably, the most common disabling condition encountered in women’s health. These migraines are more severe, last longer, and are more resistant to treatment than those that occur at other times in the cycle.1,2 And, although headache specialists are adept at diagnosing migraine and prescribing a host of antiepileptic drugs and other migraine preventives, many of these specialists are uncomfortable manipulating the hormonal underpinnings of these “super migraines.”
This article outlines diagnostic criteria, treatment options, and preventive strategies, including hormonal therapy. In the process, it demonstrates how, in many cases, a gynecologist’s expertise in managing hormonal triggers may be the determinant of successful treatment.
Migraine prefers women
Migraine is the most common of all disabling headaches and afflicts 13% of the US population, but with a markedly skewed distribution: It preferentially attacks women in a 3:1 preponderance. The lifetime prevalence of migraine in women is 33%. Migraine strikes women primarily during reproductive years, when many women seek routine health care from a gynecologist rather than an internist or general practitioner.3
Menstrual migraine is defined as migraine without aura that occurs in predictable association with menses. Its onset falls within a 5-day window, spanning 2 days before the onset of menses through the third day of bleeding.5 Although the complete exclusion of migraine with aura from diagnostic criteria is controversial, headache specialists generally agree that aura is uncommonly associated with MM, probably owing to the low-estrogen environment. (Higher concentrations of estrogen are associated with an increased likelihood of aura, similar to the association between estrogen and seizure activity.)
The migraine trigger appears to be estrogen withdrawal in susceptible persons—either during the natural menstrual cycle or as a result of cycling onto inert pills in an oral contraceptive (OC) regimen. A population study found that 39% of menstruating women experience headaches with menses, and almost one third of these headaches meet established criteria for MM or menstrual-related migraine.4
The distinction between these two entities, MM and menstrual-related migraine, is largely semantic. With MM, the menstrual attack is the patient’s only migraine. The broader term implies that she may have other attacks in addition to the menstrual ones. In this article, I’ve gathered both categories under the term MM, which also includes headaches that arise at the time of estrogen withdrawal associated with OC use.
Regardless of what we call them, these headaches have proved to be particularly vexing to headache medicine specialists who hesitate to address hormonal factors.
Diagnostic criteria are clear
Formal diagnosis of migraine requires that at least two of four signature characteristics plus at least one of two associated symptoms be present.5 The four characteristics are:
- moderate or severe pain
- throbbing
- unilateral location
- intensification of headache upon activity.
Any combination of two suffices for diagnosis—much to the astonishment of many patients who mistakenly believe that migraine must be severe or one-sided.
Associated symptoms include either nausea or both photophobia and phonophobia, the latter often signified by the simple preference to be in a dark, quiet room during an attack.
Untreated, migraine usually lasts between 4 and 72 hours.
A practical, clinical approach to diagnosis is to look for the episodic disabling headache. By disabling, I mean the presence of associated nausea or the need to stop one’s activities and lie down. A stable history of attacks with predictable menstrual association offers further confirmation.
Neck tension may be present
Symptoms of neck tension do not rule out migraine. In fact, neck pain is far more common at the time of treatment than is nausea, and migraineurs frequently describe neck pain that radiates forward during an attack.6
Treatment options begin with NSAIDs
Initial treatment of MM is no different than that of other migraines. Mild and moderate attacks can often be managed with nonsteroidal anti-inflammatory drugs (NSAIDs), which concomitantly treat comorbid dysmenorrhea.
A small randomized trial found that mefenamic acid (500 mg every 8 hours, as needed) was superior to placebo for acute MM, and a small crossover trial compared two formulations of diclofenac—50-mg sachets and tablets—with placebo in the treatment of acute migraine (TABLE). Almost one quarter of the patients taking the sachet form were pain-free at 2 hours, compared with 18.5% of patients taking the tablets and 11.7% of those who received placebo.7,8
Injectable ketorolac is more potent and is proving to be as effective as or more effective than triptans or opioids for severe, persistent migraine.
When migraine is more severe, or when NSAIDs no longer suffice, treatment advances to migraine-specific medications—specifically, ergotamines and triptans.
Brand names of drugs mentioned in this article
| Drug | Brand name |
|---|---|
| NSAIDs | |
| Diclofenac sodium | Voltaren (and others) |
| Ketorolac tromethamine | Toradol (and others) |
| Mefenamic acid | Ponstel (and others) |
| Naproxen sodium | Naprelan (and others) |
| Triptans | |
| Eletriptan hydrobromide | Relpax |
| Frovatriptan succinate | Frova |
| Naratriptan hydrochloride | Amerge |
| Sumatriptan succinate | Imitrex |
| Ergotamines | |
| Dihydroergotamine mesylate | D.H.E. 45, Migranal |
| Other | |
| Butalbital, acetaminophen, and caffeine | Fioricet |
| Leuprolide acetate | Lupron, Eligard |
Ergots and ergotamines have varied safety profiles in pregnancy
Dihydroergotamine belongs to the oldest family of migraine-specific drugs, although it is not widely used today. One reason may be that most migraineurs are women of reproductive age, and ergots are oxytocic and potential teratogens. Furthermore, they are not recommended in lactation. Ergotamines, however, are quite diverse, and some have more acceptable FDA use-in-pregnancy ratings. Injectable dihydroergotamine appears to be as effective as or less effective than triptans for migraine pain, but more effective than other drugs, such as NSAIDs or analgesics, for acute attacks.9 The nasal spray is more effective than placebo, but less effective than triptans.9
Triptans are relatively safe for women of reproductive age
Most information on use of triptans in pregnancy concerns sumatriptan. Like all triptans, it falls into Category C; however, its published profile is reassuring.10-12 Data from Sweden on 2,027 first-trimester exposures show a 3.6% risk of birth defects (major and minor), compared with an identical 3.6% risk in the general Swedish population.12 Sumatriptan is considerably less lipophilic than most of the drugs in its class and has been rated as compatible with breastfeeding.13
All triptans except eletriptan have been studied in the treatment of acute MM and found to be superior to placebo.14 These serotonin 1B/1D agonists are tailored therapy for acute migraine because, unlike analgesics, they address the underlying pathology of the attack, inhibiting the release of vasoactive peptides, promoting selective meningeal vasoconstriction, and blocking pain pathways in the brainstem. They also resolve the associated symptoms of nausea and photophobia. Triptans should not be used in the presence of untreated hypertension or vascular disease (cardiovascular, cerebrovascular, or peripheral vascular disease).
Watch for “rebound” headache. Like all acute treatment—be it a simple analgesic, NSAID, caffeine-containing compound, butalbital, ergotamine, or opioid—too-frequent use of triptans can produce medication-overuse headache, also referred to as rebound headache. In general, try to limit the use of agents for acute migraine, whether prescription or over-the-counter, to no more than 2 days a week to avoid this consequence. Also, be aware that some agents—notably, butalbital-containing compounds—may cause rebound headache, even when given as infrequently as 5 days of the month.15
Some preventive strategies are “nonspecific”
When treatment of acute MM is inadequate, management shifts toward prevention. Options include nonspecific (those that do not address the hormonal trigger) and specific (hormonal) strategies. Nonspecific strategies rely on the predictable onset of MM for proper timing of the therapeutic intervention; therefore, women who have irregular cycles are not good candidates for this approach. The presence of comorbid conditions such as dysmenorrhea, menometrorrhagia, and endometriosis may argue for early adoption of specific strategies that improve both conditions at once.
The fact that menstrual migraine (MM) is associated with estrogen withdrawal prompts a question: What happens immediately postpartum, when estrogen levels decline with loss of the placenta?
Although hormonal fluctuations generally stabilize during pregnancy, and most menstrual migraineurs experience fewer headaches during gestation, that protective effect erodes at delivery, when the incidence of migraine can be as high as 40% in the first week.41
Investigators who prospectively studied 49 migraineurs—two of whom were affected by migraine with aura and 47 by migraine without aura—found improvement in 46.8% of these women during the first trimester of pregnancy, 83% during the second trimester, and 87.2% during the third trimester, with complete remission rates of 10.6%, 53.2%, and 78.7%, respectively.42 During the first postpartum week, migraine recurred in 34% of women.42 Interestingly, women who had a history of MM were less likely to improve during the first and third trimesters of pregnancy.42
In a separate prospective investigation of 985 women who delivered over a 3-month period in one tertiary-care facility, 381 experienced postpartum headache.43 The median time to onset of the headache was 2 days, and the median duration was 4 hours. More than 75% of these headaches were primary headaches.43 Only a small percentage (4%) were incapacitating.43
When migraine may signal a more serious condition
Another question arises when a woman experiences a severe headache shortly after delivery: Could the headache be related to preeclampsia or another serious complication of pregnancy and delivery? According to Contag and colleagues, immediate assessment may be warranted.44
“Characteristics to consider are the association of the headache with elevated blood pressure (which could signal postpartum preeclampsia), the sudden onset of an atypical headache, and variations to the usual nature of the migraine, such as the onset of new neurological symptoms. Postpartum women with any of these characteristics should be evaluated in the emergency department, and neuroimaging should be strongly considered,” they write.44
Treatment reverts to prepregnancy options
Assuming preeclampsia or another serious condition is not the culprit, the treatment options for postpartum migraine revert to prepregnancy choices, as effect on the developing fetus is no longer a concern. Nonsteroidal anti-inflammatory drugs (NSAIDs) are the first line of therapy. If they are ineffective, proceed to an ergotamine or triptan.—Janelle Yates, Senior Editor
Nonhormonal (nonspecific) therapy NSAIDs may provide some relief. In one small study, naproxen sodium (550 mg twice daily) was administered for 2 weeks, beginning 1 week before the anticipated onset of menses. It modestly reduced the overall duration and severity of menstrual migraine16—a benefit that must be weighed against the risk of adverse events and the more recent FDA black box warning about its potentially serious heart and gastrointestinal risks.
Triptan regimens may prevent MM. Several triptans have been investigated for prevention of MM. A small, open-label study evaluated the use of oral sumatriptan (25 mg three times daily), beginning 2 to 3 days before the anticipated onset of MM and continuing for 5 days.17 Menstrual attacks were prevented in just over 50% of cases.
Naratriptan (1 mg twice daily), beginning 2 days before anticipated menses and continuing for 5 days, reduced the number of MM attacks by 50%, with side effects comparable to placebo.18 A higher dosage (2.5 mg twice daily) did not prove to be superior to placebo, for unexplained reasons.
In a similar trial, frovatriptan (2.5 mg daily or 2.5 mg twice daily), beginning 2 days before the anticipated onset of MM and continuing for 6 days, prevented at least 50% of MM.19 Twice-daily dosing was superior to daily administration.
Magnesium may shorten MM. In one small study, oral magnesium (360 mg daily), beginning on the 15th day of the cycle and continuing through the menses, shortened the duration of MM and improved menstrual complaints better than placebo.20
The goal of hormonal therapy is to eliminate or sufficiently minimize the premenstrual decline in estrogen that is believed to precipitate MM.21 An observational study of 229 women found that hormonal strategies prevented MM in 73% of cases (81% when taken as directed).22
It is fortunate that MM, by definition, is migraine without aura, because the use of combined OCs has been controversial in the setting of migraine with aura. International studies have reported a small but increased risk of stroke associated with their use, although a subset of women with migraine had no increased risk.23-25 In contrast, no U.S. study since 1975 has found an increased risk of stroke associated with the use of OCs.26 One large domestic study reviewed 3.6 million woman-years of use and found no increased risk of ischemic stroke with the low-dose OCs currently available, nor did a pooled analysis of U.S. studies.27,28
The discrepancy is likely explained by the strong relative contraindication, in the United States, to the use of OCs in smokers older than 35 years (the smoking prevalence in most of the European case series was more than 50%), as well as the more prevalent use of high-dose OCs in the international studies. High-dose pills were implicated in the majority of stroke cases in the World Health Organization (WHO) study, but were used by only 0.7% of cases and controls in the pooled U.S. studies.23 Nevertheless, both ACOG and WHO concluded that the risk of OC use usually outweighs the benefit in women older than 35 years whose migraines are complicated by focal neurologic deficits.
Extended-cycle OCs may offer a lengthy reprieve. Regimens that forego monthly withdrawal bleeds and provide extended administration of active pills can afford migraineurs a lengthy reprieve from MM.29 Breakthrough bleeding is the most common side effect but tends to decrease over time. It is preferable for the patient to take the pill at bedtime to avoid a drug nadir during susceptible stages of sleep, which may be associated with migraine generation. It also is prudent to avoid concomitant administration of drugs that might increase the rate of hepatic metabolism of estrogen (e.g., a high dosage of topiramate) and lead to a more rapid decline in concentration.
When using an extended-cycle regimen that allows for periodic withdrawal bleeds, give the patient supplemental estrogen during the withdrawal week if the decline in ethinyl estradiol (EE) exceeds 10 μg, a threshold that appears to elicit MM in susceptible women.21,22 For example, with an extended-cycle regimen that contains 30 μg of EE, it may be necessary to add 20 μg of estrogen during the placebo week to prevent MM, whereas an extended-cycle regimen that contains 20 μg EE, declining to 10 μg during the 13th week, would be adequate as packaged.
21/7 hormonal OCs may require supplemental estrogen to prevent MM. The late luteal-phase decline in estradiol concentration during the natural menstrual cycle is equivalent to the decline experienced with the transition to inert pills in 20- to 25-μg EE formulations. Therefore, these regimens confer the same risk of MM as the woman’s natural cycle. Products that contain incrementally higher dosages of EE (30, 35, and 50 μg) confer an increasingly greater risk of MM. Supplementation of estrogen during the placebo week may prevent MM by limiting the decline in estrogen.
In a small, open-label study, women took an OC containing 20 μg EE at bedtime on days 1 to 21 of the cycle, followed by 0.9 mg of conjugated equine estrogens (CEE) on days 22 to 28. All patients reported a reduction in migraine frequency of at least 50%, with a mean reduction of 78%.30
Parenteral options can be created utilizing a transdermal 20-μg EE/norelgestromin patch or a 15-μg EE/etonogestrel vaginal ring. With the first approach, I recommend adding a 0.1-mg EE patch during the withdrawal week to prevent MM. With the latter, a 0.075-mg EE patch may be used during the week following ring removal.31
Consider a menstrually targeted estrogen supplement. Some women who have contraindications to use of an OC may still be candidates for targeted strategies using lower dosages of supplemental estrogen rather than a combination OC. Among the options is perimenstrual administration of an estradiol patch or gel.32 One study found a 0.1-mg estrogen patch (worn 7 days and applied just before the expected onset of menses) to be effective, but lower dosages (0.025 to 0.05 mg EE) were not.33 Daily application of 1.5 mg estradiol gel for 7 days, beginning before the onset of MM, was also effective in preventing MM.34-36
With targeted strategies, timing is critical; if estrogen is begun too early, the incidence of migraine may rise after cessation.36
GnRH agonists may benefit women who have isolated MM. Administration of gonadotropin-releasing hormone (GnRH) agonists has been shown to ease MM, but the baseline frequency of headaches appears to be an important variable in the success of these agents.37-39 Leuprolide acetate markedly diminished MM in women who seldom experienced headaches other than their menstrual attacks.37 It did not benefit women who experienced migraine in the setting of chronic headache (≥15 days/month), probably because chronic migraine is influenced by other variables, such as nonrestorative sleep and overuse of medication.15,38,40
No evidence that progestin-only contraceptives are effective. Although these agents have been proposed for treatment of migraine, evidence of their benefit is lacking. It is my opinion that, more often than not, they exacerbate migraine.
A.G. is a student who misses 2 or 3 days of school each month because of debilitating menstrual migraine (MM) with vomiting. Her referring physician prescribed topiramate, but the drug caused bothersome cognitive effects without relieving her headaches. She is taking a 30-μg oral contraceptive (OC) that contains ethinyl estradiol and drospirenone. Despite starting and stopping the OC several times, she has had no relief. She also takes 100 mg topiramate at bedtime, and 7 to 10 tablets of sumatriptan (100 mg) a month—usually during the menstrual week.
The ObGyn discontinues topiramate and changes dosing of the OC to active pills only for 12 consecutive weeks. During the 13th week, the patient is instructed to take 0.9 mg conjugated equine estrogens twice daily for 7 days before resuming extended-cycle oral contraception. This regimen completely eliminates menstrual migraine. The infrequent migraines the patient does experience—which she attributes to weather fronts—are successfully managed with no more than two doses of a triptan in a month.
A busy gynecology practice sees more migraineurs in a day than a neurology practice sees in a month. But most of the migraineurs who visit gynecology offices have a chief complaint other than headache, and most leave without having mentioned the migraine—returning home to continue treating themselves with the same remedies their mothers used. Many of these women fail to seek a specific diagnosis, or treatment, until they develop chronic daily headaches or become unable to work.
Current theories of migraine implicate spreading cortical depression; trigeminal nerve activation with attendant vasodilation; and neurogenic inflammation.
Menstrual migraine (MM) is, arguably, the most common disabling condition encountered in women’s health. These migraines are more severe, last longer, and are more resistant to treatment than those that occur at other times in the cycle.1,2 And, although headache specialists are adept at diagnosing migraine and prescribing a host of antiepileptic drugs and other migraine preventives, many of these specialists are uncomfortable manipulating the hormonal underpinnings of these “super migraines.”
This article outlines diagnostic criteria, treatment options, and preventive strategies, including hormonal therapy. In the process, it demonstrates how, in many cases, a gynecologist’s expertise in managing hormonal triggers may be the determinant of successful treatment.
Migraine prefers women
Migraine is the most common of all disabling headaches and afflicts 13% of the US population, but with a markedly skewed distribution: It preferentially attacks women in a 3:1 preponderance. The lifetime prevalence of migraine in women is 33%. Migraine strikes women primarily during reproductive years, when many women seek routine health care from a gynecologist rather than an internist or general practitioner.3
Menstrual migraine is defined as migraine without aura that occurs in predictable association with menses. Its onset falls within a 5-day window, spanning 2 days before the onset of menses through the third day of bleeding.5 Although the complete exclusion of migraine with aura from diagnostic criteria is controversial, headache specialists generally agree that aura is uncommonly associated with MM, probably owing to the low-estrogen environment. (Higher concentrations of estrogen are associated with an increased likelihood of aura, similar to the association between estrogen and seizure activity.)
The migraine trigger appears to be estrogen withdrawal in susceptible persons—either during the natural menstrual cycle or as a result of cycling onto inert pills in an oral contraceptive (OC) regimen. A population study found that 39% of menstruating women experience headaches with menses, and almost one third of these headaches meet established criteria for MM or menstrual-related migraine.4
The distinction between these two entities, MM and menstrual-related migraine, is largely semantic. With MM, the menstrual attack is the patient’s only migraine. The broader term implies that she may have other attacks in addition to the menstrual ones. In this article, I’ve gathered both categories under the term MM, which also includes headaches that arise at the time of estrogen withdrawal associated with OC use.
Regardless of what we call them, these headaches have proved to be particularly vexing to headache medicine specialists who hesitate to address hormonal factors.
Diagnostic criteria are clear
Formal diagnosis of migraine requires that at least two of four signature characteristics plus at least one of two associated symptoms be present.5 The four characteristics are:
- moderate or severe pain
- throbbing
- unilateral location
- intensification of headache upon activity.
Any combination of two suffices for diagnosis—much to the astonishment of many patients who mistakenly believe that migraine must be severe or one-sided.
Associated symptoms include either nausea or both photophobia and phonophobia, the latter often signified by the simple preference to be in a dark, quiet room during an attack.
Untreated, migraine usually lasts between 4 and 72 hours.
A practical, clinical approach to diagnosis is to look for the episodic disabling headache. By disabling, I mean the presence of associated nausea or the need to stop one’s activities and lie down. A stable history of attacks with predictable menstrual association offers further confirmation.
Neck tension may be present
Symptoms of neck tension do not rule out migraine. In fact, neck pain is far more common at the time of treatment than is nausea, and migraineurs frequently describe neck pain that radiates forward during an attack.6
Treatment options begin with NSAIDs
Initial treatment of MM is no different than that of other migraines. Mild and moderate attacks can often be managed with nonsteroidal anti-inflammatory drugs (NSAIDs), which concomitantly treat comorbid dysmenorrhea.
A small randomized trial found that mefenamic acid (500 mg every 8 hours, as needed) was superior to placebo for acute MM, and a small crossover trial compared two formulations of diclofenac—50-mg sachets and tablets—with placebo in the treatment of acute migraine (TABLE). Almost one quarter of the patients taking the sachet form were pain-free at 2 hours, compared with 18.5% of patients taking the tablets and 11.7% of those who received placebo.7,8
Injectable ketorolac is more potent and is proving to be as effective as or more effective than triptans or opioids for severe, persistent migraine.
When migraine is more severe, or when NSAIDs no longer suffice, treatment advances to migraine-specific medications—specifically, ergotamines and triptans.
Brand names of drugs mentioned in this article
| Drug | Brand name |
|---|---|
| NSAIDs | |
| Diclofenac sodium | Voltaren (and others) |
| Ketorolac tromethamine | Toradol (and others) |
| Mefenamic acid | Ponstel (and others) |
| Naproxen sodium | Naprelan (and others) |
| Triptans | |
| Eletriptan hydrobromide | Relpax |
| Frovatriptan succinate | Frova |
| Naratriptan hydrochloride | Amerge |
| Sumatriptan succinate | Imitrex |
| Ergotamines | |
| Dihydroergotamine mesylate | D.H.E. 45, Migranal |
| Other | |
| Butalbital, acetaminophen, and caffeine | Fioricet |
| Leuprolide acetate | Lupron, Eligard |
Ergots and ergotamines have varied safety profiles in pregnancy
Dihydroergotamine belongs to the oldest family of migraine-specific drugs, although it is not widely used today. One reason may be that most migraineurs are women of reproductive age, and ergots are oxytocic and potential teratogens. Furthermore, they are not recommended in lactation. Ergotamines, however, are quite diverse, and some have more acceptable FDA use-in-pregnancy ratings. Injectable dihydroergotamine appears to be as effective as or less effective than triptans for migraine pain, but more effective than other drugs, such as NSAIDs or analgesics, for acute attacks.9 The nasal spray is more effective than placebo, but less effective than triptans.9
Triptans are relatively safe for women of reproductive age
Most information on use of triptans in pregnancy concerns sumatriptan. Like all triptans, it falls into Category C; however, its published profile is reassuring.10-12 Data from Sweden on 2,027 first-trimester exposures show a 3.6% risk of birth defects (major and minor), compared with an identical 3.6% risk in the general Swedish population.12 Sumatriptan is considerably less lipophilic than most of the drugs in its class and has been rated as compatible with breastfeeding.13
All triptans except eletriptan have been studied in the treatment of acute MM and found to be superior to placebo.14 These serotonin 1B/1D agonists are tailored therapy for acute migraine because, unlike analgesics, they address the underlying pathology of the attack, inhibiting the release of vasoactive peptides, promoting selective meningeal vasoconstriction, and blocking pain pathways in the brainstem. They also resolve the associated symptoms of nausea and photophobia. Triptans should not be used in the presence of untreated hypertension or vascular disease (cardiovascular, cerebrovascular, or peripheral vascular disease).
Watch for “rebound” headache. Like all acute treatment—be it a simple analgesic, NSAID, caffeine-containing compound, butalbital, ergotamine, or opioid—too-frequent use of triptans can produce medication-overuse headache, also referred to as rebound headache. In general, try to limit the use of agents for acute migraine, whether prescription or over-the-counter, to no more than 2 days a week to avoid this consequence. Also, be aware that some agents—notably, butalbital-containing compounds—may cause rebound headache, even when given as infrequently as 5 days of the month.15
Some preventive strategies are “nonspecific”
When treatment of acute MM is inadequate, management shifts toward prevention. Options include nonspecific (those that do not address the hormonal trigger) and specific (hormonal) strategies. Nonspecific strategies rely on the predictable onset of MM for proper timing of the therapeutic intervention; therefore, women who have irregular cycles are not good candidates for this approach. The presence of comorbid conditions such as dysmenorrhea, menometrorrhagia, and endometriosis may argue for early adoption of specific strategies that improve both conditions at once.
The fact that menstrual migraine (MM) is associated with estrogen withdrawal prompts a question: What happens immediately postpartum, when estrogen levels decline with loss of the placenta?
Although hormonal fluctuations generally stabilize during pregnancy, and most menstrual migraineurs experience fewer headaches during gestation, that protective effect erodes at delivery, when the incidence of migraine can be as high as 40% in the first week.41
Investigators who prospectively studied 49 migraineurs—two of whom were affected by migraine with aura and 47 by migraine without aura—found improvement in 46.8% of these women during the first trimester of pregnancy, 83% during the second trimester, and 87.2% during the third trimester, with complete remission rates of 10.6%, 53.2%, and 78.7%, respectively.42 During the first postpartum week, migraine recurred in 34% of women.42 Interestingly, women who had a history of MM were less likely to improve during the first and third trimesters of pregnancy.42
In a separate prospective investigation of 985 women who delivered over a 3-month period in one tertiary-care facility, 381 experienced postpartum headache.43 The median time to onset of the headache was 2 days, and the median duration was 4 hours. More than 75% of these headaches were primary headaches.43 Only a small percentage (4%) were incapacitating.43
When migraine may signal a more serious condition
Another question arises when a woman experiences a severe headache shortly after delivery: Could the headache be related to preeclampsia or another serious complication of pregnancy and delivery? According to Contag and colleagues, immediate assessment may be warranted.44
“Characteristics to consider are the association of the headache with elevated blood pressure (which could signal postpartum preeclampsia), the sudden onset of an atypical headache, and variations to the usual nature of the migraine, such as the onset of new neurological symptoms. Postpartum women with any of these characteristics should be evaluated in the emergency department, and neuroimaging should be strongly considered,” they write.44
Treatment reverts to prepregnancy options
Assuming preeclampsia or another serious condition is not the culprit, the treatment options for postpartum migraine revert to prepregnancy choices, as effect on the developing fetus is no longer a concern. Nonsteroidal anti-inflammatory drugs (NSAIDs) are the first line of therapy. If they are ineffective, proceed to an ergotamine or triptan.—Janelle Yates, Senior Editor
Nonhormonal (nonspecific) therapy NSAIDs may provide some relief. In one small study, naproxen sodium (550 mg twice daily) was administered for 2 weeks, beginning 1 week before the anticipated onset of menses. It modestly reduced the overall duration and severity of menstrual migraine16—a benefit that must be weighed against the risk of adverse events and the more recent FDA black box warning about its potentially serious heart and gastrointestinal risks.
Triptan regimens may prevent MM. Several triptans have been investigated for prevention of MM. A small, open-label study evaluated the use of oral sumatriptan (25 mg three times daily), beginning 2 to 3 days before the anticipated onset of MM and continuing for 5 days.17 Menstrual attacks were prevented in just over 50% of cases.
Naratriptan (1 mg twice daily), beginning 2 days before anticipated menses and continuing for 5 days, reduced the number of MM attacks by 50%, with side effects comparable to placebo.18 A higher dosage (2.5 mg twice daily) did not prove to be superior to placebo, for unexplained reasons.
In a similar trial, frovatriptan (2.5 mg daily or 2.5 mg twice daily), beginning 2 days before the anticipated onset of MM and continuing for 6 days, prevented at least 50% of MM.19 Twice-daily dosing was superior to daily administration.
Magnesium may shorten MM. In one small study, oral magnesium (360 mg daily), beginning on the 15th day of the cycle and continuing through the menses, shortened the duration of MM and improved menstrual complaints better than placebo.20
The goal of hormonal therapy is to eliminate or sufficiently minimize the premenstrual decline in estrogen that is believed to precipitate MM.21 An observational study of 229 women found that hormonal strategies prevented MM in 73% of cases (81% when taken as directed).22
It is fortunate that MM, by definition, is migraine without aura, because the use of combined OCs has been controversial in the setting of migraine with aura. International studies have reported a small but increased risk of stroke associated with their use, although a subset of women with migraine had no increased risk.23-25 In contrast, no U.S. study since 1975 has found an increased risk of stroke associated with the use of OCs.26 One large domestic study reviewed 3.6 million woman-years of use and found no increased risk of ischemic stroke with the low-dose OCs currently available, nor did a pooled analysis of U.S. studies.27,28
The discrepancy is likely explained by the strong relative contraindication, in the United States, to the use of OCs in smokers older than 35 years (the smoking prevalence in most of the European case series was more than 50%), as well as the more prevalent use of high-dose OCs in the international studies. High-dose pills were implicated in the majority of stroke cases in the World Health Organization (WHO) study, but were used by only 0.7% of cases and controls in the pooled U.S. studies.23 Nevertheless, both ACOG and WHO concluded that the risk of OC use usually outweighs the benefit in women older than 35 years whose migraines are complicated by focal neurologic deficits.
Extended-cycle OCs may offer a lengthy reprieve. Regimens that forego monthly withdrawal bleeds and provide extended administration of active pills can afford migraineurs a lengthy reprieve from MM.29 Breakthrough bleeding is the most common side effect but tends to decrease over time. It is preferable for the patient to take the pill at bedtime to avoid a drug nadir during susceptible stages of sleep, which may be associated with migraine generation. It also is prudent to avoid concomitant administration of drugs that might increase the rate of hepatic metabolism of estrogen (e.g., a high dosage of topiramate) and lead to a more rapid decline in concentration.
When using an extended-cycle regimen that allows for periodic withdrawal bleeds, give the patient supplemental estrogen during the withdrawal week if the decline in ethinyl estradiol (EE) exceeds 10 μg, a threshold that appears to elicit MM in susceptible women.21,22 For example, with an extended-cycle regimen that contains 30 μg of EE, it may be necessary to add 20 μg of estrogen during the placebo week to prevent MM, whereas an extended-cycle regimen that contains 20 μg EE, declining to 10 μg during the 13th week, would be adequate as packaged.
21/7 hormonal OCs may require supplemental estrogen to prevent MM. The late luteal-phase decline in estradiol concentration during the natural menstrual cycle is equivalent to the decline experienced with the transition to inert pills in 20- to 25-μg EE formulations. Therefore, these regimens confer the same risk of MM as the woman’s natural cycle. Products that contain incrementally higher dosages of EE (30, 35, and 50 μg) confer an increasingly greater risk of MM. Supplementation of estrogen during the placebo week may prevent MM by limiting the decline in estrogen.
In a small, open-label study, women took an OC containing 20 μg EE at bedtime on days 1 to 21 of the cycle, followed by 0.9 mg of conjugated equine estrogens (CEE) on days 22 to 28. All patients reported a reduction in migraine frequency of at least 50%, with a mean reduction of 78%.30
Parenteral options can be created utilizing a transdermal 20-μg EE/norelgestromin patch or a 15-μg EE/etonogestrel vaginal ring. With the first approach, I recommend adding a 0.1-mg EE patch during the withdrawal week to prevent MM. With the latter, a 0.075-mg EE patch may be used during the week following ring removal.31
Consider a menstrually targeted estrogen supplement. Some women who have contraindications to use of an OC may still be candidates for targeted strategies using lower dosages of supplemental estrogen rather than a combination OC. Among the options is perimenstrual administration of an estradiol patch or gel.32 One study found a 0.1-mg estrogen patch (worn 7 days and applied just before the expected onset of menses) to be effective, but lower dosages (0.025 to 0.05 mg EE) were not.33 Daily application of 1.5 mg estradiol gel for 7 days, beginning before the onset of MM, was also effective in preventing MM.34-36
With targeted strategies, timing is critical; if estrogen is begun too early, the incidence of migraine may rise after cessation.36
GnRH agonists may benefit women who have isolated MM. Administration of gonadotropin-releasing hormone (GnRH) agonists has been shown to ease MM, but the baseline frequency of headaches appears to be an important variable in the success of these agents.37-39 Leuprolide acetate markedly diminished MM in women who seldom experienced headaches other than their menstrual attacks.37 It did not benefit women who experienced migraine in the setting of chronic headache (≥15 days/month), probably because chronic migraine is influenced by other variables, such as nonrestorative sleep and overuse of medication.15,38,40
No evidence that progestin-only contraceptives are effective. Although these agents have been proposed for treatment of migraine, evidence of their benefit is lacking. It is my opinion that, more often than not, they exacerbate migraine.
1. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63(2):351-353.
2. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24(9):707-716.
3. Launer LJ, Terwindt GM, Ferrari MD. The prevalence and characteristics of migraine in a population-based cohort: the GEM study. Neurology. 1999;53(3):537-542.
4. Couturier EG, Bomhof MA, Neven AK, van Duijn NP. Menstrual migraine in a representative Dutch population sample: prevalence, disability and treatment. Cephalalgia. 2003;23(4):302-308.
5. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders. 2nd ed. Cephalalgia. 2004;24(suppl 1):9-160.
6. Calhoun AH, Ford S, Millen C, Finkel AG, Truong Y, Nie Y. The prevalence of neck pain in migraine [abstract]. Headache. 2010 Jan 20.-[Epub ahead of print].
7. Al-Waili NS. Treatment of menstrual migraine with prostaglandin synthesis inhibitor mefenamic acid: double-blind study with placebo. Eur J Med Res. 2000;5(4):176-182.
8. Diener HC, Montagna P, Gács G, et al. Efficacy and tolerability of diclofenac potassium sachets in migraine: a randomized, double-blind, cross-over study in comparison with diclofenac potassium tablets and placebo. Cephalalgia. 2006;26(5):537-547.
9. Schürks M. Dihydroergotamine: role in the treatment of migraine. Expert Opin Drug Metab Toxicol. 2009;5(9):1141-1148.
10. Loder E. Safety of sumatriptan in pregnancy: a review of the data so far. CNS Drugs. 2003;17(1):1-7.
11. Shuhaiber S, Pastuszak A, Schick B, et al. Pregnancy outcome following first trimester exposure to sumatriptan. Neurology. 1998;51(2):581-583.
12. Cunnington M, Ephross S, Churchill P. The safety of sumatriptan and naratriptan in pregnancy: what have we learned? Headache. 2009;49(10):1414-1422.
13. Ressel G. AAP updates statement for transfer of drugs and other chemicals into breast milk. American Academy of Pediatrics. Am Fam Physician. 2002;65(5):979-980.
14. Ashkenazi A, Silberstein S. Menstrual migraine: a review of hormonal causes, prophylaxis and treatment. Expert Opin Pharmacother. 2007;8(11):1605-1613.
15. Bigal ME, Serrano D, Buse D, Scher A, Stewart WF, Lipton RB. Acute migraine medications and evolution from episodic to chronic migraine: a longitudinal population-based study. Headache. 2008;48(8):1157-1168.
16. Sances G, Martignoni E, Fioroni L, Blandini F, Facchinetti F, Nappi G. Naproxen sodium in menstrual migraine prophylaxis: a double-blind placebo controlled study. Headache. 1990;30(11):705-709.
17. Newman LC, Lipton RB, Lay CL, Solomon S. A pilot study of oral sumatriptan as intermittent prophylaxis of menstruation-related migraine. Neurology. 1998;51(1):307-309.
18. Newman L, Mannix LK, Landy S, et al. Naratriptan as short-term prophylaxis of menstrually associated migraine: a randomized, double-blind, placebo-controlled study. Headache. 2001;41(3):248-256.
19. Silberstein SD, Elkind AH, Schreiber C, Keywood C. A randomized trial of frovatriptan for the intermittent prevention of menstrual migraine. Neurology. 2004;63(2):261-269.
20. Facchinetti F, Sances G, Borella P, Genazzani AR, Nappi G. Magnesium prophylaxis of menstrual migraine: effects on intracellular magnesium. Headache. 1991;31(5):298-301.
21. Calhoun A. Women’s Issues in Headache. In: Loder E, ed. Headache. Philadelphia: American College of Physicians; 2004:157-177.
22. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48(8):1186-1193.
23. Ischaemic stroke and combined oral contraceptives: results of an international, multicentre, case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet. 1996;348:498-505.
24. Chan WS, Ray J, Wai EK, et al. Risk of stroke in women exposed to low-dose oral contraceptives: a critical evaluation of the evidence. Arch Intern Med. 2004;164(7):741-747.
25. Etminan M, Takkouche B, Isorna FC, Samii A. Risk of ischaemic stroke in people with migraine: systematic review and meta-analysis of observational studies. BMJ. 2005;330(7482):63.-
26. Oral contraceptives and stroke in young women. Associated risk factors. JAMA. 1975;231:718-722.
27. Petitti DB, Sidney S, Bernstein A, Wolf S, Quesenberry C, Ziel HK. Stroke in users of low-dose oral contraceptives. N Engl J Med. 1996;335(1):8-15.
28. Schwartz SM, Petitti DB, Siscovick DS, et al. Stroke and use of low-dose oral contraceptives in young women: a pooled analysis of two US studies. Stroke. 1998;29(11):2277-2284.
29. Sulak PJ, Scow RD, Preece C, Riggs MW, Kuehl TJ. Hormone withdrawal symptoms in oral contraceptive users. Obstet Gynecol. 2000;95(2):261-266.
30. Calhoun AH. A novel specific prophylaxis for menstrual-associated migraine. South Med J. 2004;97(9):819-822.
31. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep. 2009;13(5):381-385.
32. Pringsheim T, Davenport WJ, Dodick D. Acute treatment and prevention of menstrually related migraine headache: evidence-based review. Neurology. 2008;70(17):1555-1563.
33. Pradalier A VD, Beaulieu PH, et al. Correlation between oestradiol plasma level and therapeutic effect on menstrual migraine. In: FC Rose, ed. New advances in headache research. London: Smith-Gordon; 1994:129-132.
34. de Lignières B, Vincens M, Mauvais-Jarvis P, Mas JL, Touboul PJ, Bousser MG. Prevention of menstrual migraine by percutaneous oestradiol. Br Med J (Clin Res Ed). 1986;293(6561):1540.-
35. Dennerstein L, Morse C, Burrows G, Oats J, Brown J, Smith M. Menstrual migraine: a double-blind trial of percutaneous estradiol. Gynecol Endocrinol. 1988;2(2):113-120.
36. MacGregor EA, Frith A, Ellis J, Aspinall L, Hackshaw A. Prevention of menstrual attacks of migraine: a double-blind placebo-controlled crossover study. Neurology. 2006;67(12):2159-2163.
37. Murray SC, Muse KN. Effective treatment of severe menstrual migraine headaches with gonadotropin-releasing hormone agonist and “add-back” therapy. Fertil Steril. 1997;67(2):390-393.
38. Martin V, Wernke S, Mandell K, et al. Medical oophorectomy with and without estrogen add-back therapy in the prevention of migraine headache. Headache. 2003;43(4):309-321.
39. Lichten EM, Lichten JB, Whitty A, Pieper D. The confirmation of a biochemical marker for women’s hormonal migraine: the depo-estradiol challenge test. Headache. 1996;36(6):367-371.
40. Calhoun AH, Ford S. Behavioral sleep modification may revert transformed migraine to episodic migraine. Headache. 2007;47(8):1178-1183.
41. Stein GS. Headaches in the first postpartum week and their relationship to migraine. Headache. 1981;21(5):201-205.
42. Sances G, Granella F, Nappi RE, et al. Course of migraine during pregnancy and postpartum: a prospective study. Cephalalgia. 2003;23(3):197-205.
43. Goldszmidt E, Kern R, Chaput A, Macarthur A. The incidence and etiology of postpartum headaches: a prospective cohort study. Can J Anaesth. 2005;52(9):971-977.
44. Contag SA, Mertz HL, Bushnell CD. Migraine during pregnancy: Is it more than a headache? Nat Rev Neurol. 2009;5(8):449-456.
1. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63(2):351-353.
2. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24(9):707-716.
3. Launer LJ, Terwindt GM, Ferrari MD. The prevalence and characteristics of migraine in a population-based cohort: the GEM study. Neurology. 1999;53(3):537-542.
4. Couturier EG, Bomhof MA, Neven AK, van Duijn NP. Menstrual migraine in a representative Dutch population sample: prevalence, disability and treatment. Cephalalgia. 2003;23(4):302-308.
5. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders. 2nd ed. Cephalalgia. 2004;24(suppl 1):9-160.
6. Calhoun AH, Ford S, Millen C, Finkel AG, Truong Y, Nie Y. The prevalence of neck pain in migraine [abstract]. Headache. 2010 Jan 20.-[Epub ahead of print].
7. Al-Waili NS. Treatment of menstrual migraine with prostaglandin synthesis inhibitor mefenamic acid: double-blind study with placebo. Eur J Med Res. 2000;5(4):176-182.
8. Diener HC, Montagna P, Gács G, et al. Efficacy and tolerability of diclofenac potassium sachets in migraine: a randomized, double-blind, cross-over study in comparison with diclofenac potassium tablets and placebo. Cephalalgia. 2006;26(5):537-547.
9. Schürks M. Dihydroergotamine: role in the treatment of migraine. Expert Opin Drug Metab Toxicol. 2009;5(9):1141-1148.
10. Loder E. Safety of sumatriptan in pregnancy: a review of the data so far. CNS Drugs. 2003;17(1):1-7.
11. Shuhaiber S, Pastuszak A, Schick B, et al. Pregnancy outcome following first trimester exposure to sumatriptan. Neurology. 1998;51(2):581-583.
12. Cunnington M, Ephross S, Churchill P. The safety of sumatriptan and naratriptan in pregnancy: what have we learned? Headache. 2009;49(10):1414-1422.
13. Ressel G. AAP updates statement for transfer of drugs and other chemicals into breast milk. American Academy of Pediatrics. Am Fam Physician. 2002;65(5):979-980.
14. Ashkenazi A, Silberstein S. Menstrual migraine: a review of hormonal causes, prophylaxis and treatment. Expert Opin Pharmacother. 2007;8(11):1605-1613.
15. Bigal ME, Serrano D, Buse D, Scher A, Stewart WF, Lipton RB. Acute migraine medications and evolution from episodic to chronic migraine: a longitudinal population-based study. Headache. 2008;48(8):1157-1168.
16. Sances G, Martignoni E, Fioroni L, Blandini F, Facchinetti F, Nappi G. Naproxen sodium in menstrual migraine prophylaxis: a double-blind placebo controlled study. Headache. 1990;30(11):705-709.
17. Newman LC, Lipton RB, Lay CL, Solomon S. A pilot study of oral sumatriptan as intermittent prophylaxis of menstruation-related migraine. Neurology. 1998;51(1):307-309.
18. Newman L, Mannix LK, Landy S, et al. Naratriptan as short-term prophylaxis of menstrually associated migraine: a randomized, double-blind, placebo-controlled study. Headache. 2001;41(3):248-256.
19. Silberstein SD, Elkind AH, Schreiber C, Keywood C. A randomized trial of frovatriptan for the intermittent prevention of menstrual migraine. Neurology. 2004;63(2):261-269.
20. Facchinetti F, Sances G, Borella P, Genazzani AR, Nappi G. Magnesium prophylaxis of menstrual migraine: effects on intracellular magnesium. Headache. 1991;31(5):298-301.
21. Calhoun A. Women’s Issues in Headache. In: Loder E, ed. Headache. Philadelphia: American College of Physicians; 2004:157-177.
22. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48(8):1186-1193.
23. Ischaemic stroke and combined oral contraceptives: results of an international, multicentre, case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet. 1996;348:498-505.
24. Chan WS, Ray J, Wai EK, et al. Risk of stroke in women exposed to low-dose oral contraceptives: a critical evaluation of the evidence. Arch Intern Med. 2004;164(7):741-747.
25. Etminan M, Takkouche B, Isorna FC, Samii A. Risk of ischaemic stroke in people with migraine: systematic review and meta-analysis of observational studies. BMJ. 2005;330(7482):63.-
26. Oral contraceptives and stroke in young women. Associated risk factors. JAMA. 1975;231:718-722.
27. Petitti DB, Sidney S, Bernstein A, Wolf S, Quesenberry C, Ziel HK. Stroke in users of low-dose oral contraceptives. N Engl J Med. 1996;335(1):8-15.
28. Schwartz SM, Petitti DB, Siscovick DS, et al. Stroke and use of low-dose oral contraceptives in young women: a pooled analysis of two US studies. Stroke. 1998;29(11):2277-2284.
29. Sulak PJ, Scow RD, Preece C, Riggs MW, Kuehl TJ. Hormone withdrawal symptoms in oral contraceptive users. Obstet Gynecol. 2000;95(2):261-266.
30. Calhoun AH. A novel specific prophylaxis for menstrual-associated migraine. South Med J. 2004;97(9):819-822.
31. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep. 2009;13(5):381-385.
32. Pringsheim T, Davenport WJ, Dodick D. Acute treatment and prevention of menstrually related migraine headache: evidence-based review. Neurology. 2008;70(17):1555-1563.
33. Pradalier A VD, Beaulieu PH, et al. Correlation between oestradiol plasma level and therapeutic effect on menstrual migraine. In: FC Rose, ed. New advances in headache research. London: Smith-Gordon; 1994:129-132.
34. de Lignières B, Vincens M, Mauvais-Jarvis P, Mas JL, Touboul PJ, Bousser MG. Prevention of menstrual migraine by percutaneous oestradiol. Br Med J (Clin Res Ed). 1986;293(6561):1540.-
35. Dennerstein L, Morse C, Burrows G, Oats J, Brown J, Smith M. Menstrual migraine: a double-blind trial of percutaneous estradiol. Gynecol Endocrinol. 1988;2(2):113-120.
36. MacGregor EA, Frith A, Ellis J, Aspinall L, Hackshaw A. Prevention of menstrual attacks of migraine: a double-blind placebo-controlled crossover study. Neurology. 2006;67(12):2159-2163.
37. Murray SC, Muse KN. Effective treatment of severe menstrual migraine headaches with gonadotropin-releasing hormone agonist and “add-back” therapy. Fertil Steril. 1997;67(2):390-393.
38. Martin V, Wernke S, Mandell K, et al. Medical oophorectomy with and without estrogen add-back therapy in the prevention of migraine headache. Headache. 2003;43(4):309-321.
39. Lichten EM, Lichten JB, Whitty A, Pieper D. The confirmation of a biochemical marker for women’s hormonal migraine: the depo-estradiol challenge test. Headache. 1996;36(6):367-371.
40. Calhoun AH, Ford S. Behavioral sleep modification may revert transformed migraine to episodic migraine. Headache. 2007;47(8):1178-1183.
41. Stein GS. Headaches in the first postpartum week and their relationship to migraine. Headache. 1981;21(5):201-205.
42. Sances G, Granella F, Nappi RE, et al. Course of migraine during pregnancy and postpartum: a prospective study. Cephalalgia. 2003;23(3):197-205.
43. Goldszmidt E, Kern R, Chaput A, Macarthur A. The incidence and etiology of postpartum headaches: a prospective cohort study. Can J Anaesth. 2005;52(9):971-977.
44. Contag SA, Mertz HL, Bushnell CD. Migraine during pregnancy: Is it more than a headache? Nat Rev Neurol. 2009;5(8):449-456.