User login
Do routine eye exams reduce occurrence of blindness from type 2 diabetes?
Screening eye exams for patients with type 2 diabetes can detect retinopathy early enough so treatment can prevent vision loss. Patients without diabetic retinopathy who are systematically screened by mydriatic retinal photography have a 95% probability of remaining free of sight-threatening retinopathy over the next 5 years. If background or preproliferative retinopathy is found at screening (Figure), the 95% probability interval for remaining free of sight-threatening retinopathy is reduced to 12 and 4 months, respectively (strength of recommendation [SOR]: B, based on 1 prospective cohort study).
A reliably sensitive screening exam requires mydriatic retinal photography augmented by ophthalmoscopy when photographs are inconclusive (SOR: A, based on a systematic review). For patients with diabetes not differentiated by type, photocoagu-lation significantly decreases visual deterioration and reduces the chances of blindness (SOR: A, based on randomized controlled trials [RCT]).
FIGURE
Nonproliferative and proliferative diabetic retinopathy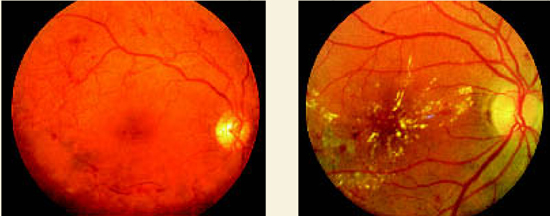
Background (nonproliferative) diabetic retinopathyis characterized by macular retinal exudates, edematous retinal thickening, dot and blot retinal hemorrhages, and retinal capillary microaneurysms.
Proliferative diabetic retinopathy. Note the network of abnormal preretinal new blood vessels just super-otemporal to the macula and the linear accumulations of blood in the preretinal vitreous below the macula.
Evidence summary
The Liverpool Diabetic Eye Study1 prospectively evaluated the risk of vision-threatening retinopathy in a cohort that included all patients with diabetes mellitus who were registered with a general practitioner and were not under the care of an ophthalmologist. A subgroup of 4770 patients with type 2 diabetes who did not have sightthreatening retinopathy at baseline underwent at least 1 additional screen. Screening included non-stereoscopic 3-field (45° or 50° field) mydriatic photography. Median follow-up was 3.5 years (range, 1–8.5 years).
The patients were divided into cohorts based on level of demonstrated retinopathy. The mean screening interval for a 95% probability of remaining free of sight-threatening retinopathy was calculated for each grade of baseline retinopathy. Screening patients with no retinopathy every 5 years provided a 95% probability of remaining free of sight-threatening retinopathy. Patients with background retinopathy must be screened annually to achieve the same result, and patients with mild preproliferative retinopathy need to be screened every 4 months ( Table ).
A systematic review2 of multiple small English-language studies evaluating screening and monitoring of diabetic retinopathy found consistent results. Screening by direct or indirect ophthalmoscopy alone detected 65% of patients with sight-threatening retinopathy. Screening by mydriatic retinal photography, augmented by ophthal-moscopy when the photographs were inconclusive, detected 88% to 100% of such cases.
An RCT of 1700 patients with diabetes and retinopathy evaluated preservation of vision with photocoagulation.3 Patients were not differentiated by type of diabetes. Each patient had initial and follow-up stereoscopic fundus photography. One eye was selected at random to receive treatment and the other remained untreated to serve as a control. Because of the magnitude of difference in vision between the eyes, the study was halted at 2 years to permit photocoagulation of the untreated eyes. Patients whose eyes had new vessels on or near the disk lost vision (defined as visual acuity less than 5/200) more often in untreated eyes (18.3% cumulative rate at 2 years) compared with treated eyes (6.4%; number needed to treat [NNT]=8.4).
Another RCT4 of patients with diabetes showed that photocoagulation maintained vision in diabetic retinopathy if the disease was not too advanced. Ninety-nine patients, also not differentiated by type of diabetes, were each treated in 1 eye chosen at random with a xenon-arc photocoagulator. Patients underwent follow-up treatments to the treated eye by clinical indication. The untreated eyes were observed as controls. Blindness occurred significantly less often in the treated eyes (19% total after 5 to 7 years) than in the control eyes (39%; NNT=5 to prevent 1 blind eye). Patients without proliferative retinopathy at onset experienced the most dramatic slowing of deterioration; photocoagulation was more useful in maintaining than in improving vision.
TABLE
Screening frequency for sight-threatening retinopathy
| Stage of retinal disease | Screening frequency* |
|---|---|
| None | 5 years |
| Background retinopathy | 1 year |
| Mild preproliferative retinopathy | 4 months |
| *For 95% chance of remaining free of sight-threatening retinopathy. | |
Recommendations from others
The American Diabetes Association 2003 Clinical Practice Recommendations5 state that patients with type 2 diabetes should have an initial dilated and comprehensive eye examination by an ophthalmologist or optometrist shortly after diagnosis of diabetes. An ophthalmologist or optometrist who is knowledgeable and experienced in diagnosing diabetic retinopathy and is aware of its management should repeat subsequent examinations for both type 1 and type 2 diabetic patients annually. Examinations are required more frequently if retinopathy is progressing.
Screen for retinal complications early, regularly, by an experienced eye doctor
Tsveti Markova, MD
Department of Family Medicine, Wayne State University, Detroit, Mich
Family physicians play a central role in the diabetes care team. They must not only achieve good blood sugar control, but also monitor for complications and coordinate their treatment. Educating patients and reaching common ground with them is essential for success. Evidence suggests that screening for eye complications reduces blindness. Patients with early retinopathy changes are usually asymptomatic; therefore it takes a committed and educated patient to comply with screening recommendations. Also, many patients have the misconception that a visual acuity exam by an optometrist is sufficient for their diabetes eye screening. Family physicians must convey the importance of screening for retinal complications early, regularly and by an optometrist or ophthalmologist experienced in management of diabetes.
1. Younis N, Broadbent DM, Vora JP, Harding SP. Incidence of sight-threatening retinopathy in patients with type 2 diabetes in the Liverpool Diabetic Eye Study: a cohort study. Lancet 2003;361:195-200.
2. Hutchinson A, McIntosh A, Peters J, et al. Effectiveness of screening and monitoring tests for diabetic retinopa-thy—a systematic review. Diabet Med 2000;17:495-506.
3. The Diabetic Retinopathy Study Research Group. Preliminary report on effects of photocoagulation therapy. Am J Ophthalmol 1976;81:383-396.
4. British Multicentre Study Group. Photocoagulation from diabetic maculopathy: a randomized controlled clinical trial using the xenon arc. Diabetes 1983;32:1010-1016.
5. Fong DS, Aiello L, Gardner TW, et al. American Diabetes Association. Diabetic retinopathy. Diabetes Care 2004;26 Suppl 1:S84-S87.
Screening eye exams for patients with type 2 diabetes can detect retinopathy early enough so treatment can prevent vision loss. Patients without diabetic retinopathy who are systematically screened by mydriatic retinal photography have a 95% probability of remaining free of sight-threatening retinopathy over the next 5 years. If background or preproliferative retinopathy is found at screening (Figure), the 95% probability interval for remaining free of sight-threatening retinopathy is reduced to 12 and 4 months, respectively (strength of recommendation [SOR]: B, based on 1 prospective cohort study).
A reliably sensitive screening exam requires mydriatic retinal photography augmented by ophthalmoscopy when photographs are inconclusive (SOR: A, based on a systematic review). For patients with diabetes not differentiated by type, photocoagu-lation significantly decreases visual deterioration and reduces the chances of blindness (SOR: A, based on randomized controlled trials [RCT]).
FIGURE
Nonproliferative and proliferative diabetic retinopathy
Background (nonproliferative) diabetic retinopathyis characterized by macular retinal exudates, edematous retinal thickening, dot and blot retinal hemorrhages, and retinal capillary microaneurysms.
Proliferative diabetic retinopathy. Note the network of abnormal preretinal new blood vessels just super-otemporal to the macula and the linear accumulations of blood in the preretinal vitreous below the macula.
Evidence summary
The Liverpool Diabetic Eye Study1 prospectively evaluated the risk of vision-threatening retinopathy in a cohort that included all patients with diabetes mellitus who were registered with a general practitioner and were not under the care of an ophthalmologist. A subgroup of 4770 patients with type 2 diabetes who did not have sightthreatening retinopathy at baseline underwent at least 1 additional screen. Screening included non-stereoscopic 3-field (45° or 50° field) mydriatic photography. Median follow-up was 3.5 years (range, 1–8.5 years).
The patients were divided into cohorts based on level of demonstrated retinopathy. The mean screening interval for a 95% probability of remaining free of sight-threatening retinopathy was calculated for each grade of baseline retinopathy. Screening patients with no retinopathy every 5 years provided a 95% probability of remaining free of sight-threatening retinopathy. Patients with background retinopathy must be screened annually to achieve the same result, and patients with mild preproliferative retinopathy need to be screened every 4 months ( Table ).
A systematic review2 of multiple small English-language studies evaluating screening and monitoring of diabetic retinopathy found consistent results. Screening by direct or indirect ophthalmoscopy alone detected 65% of patients with sight-threatening retinopathy. Screening by mydriatic retinal photography, augmented by ophthal-moscopy when the photographs were inconclusive, detected 88% to 100% of such cases.
An RCT of 1700 patients with diabetes and retinopathy evaluated preservation of vision with photocoagulation.3 Patients were not differentiated by type of diabetes. Each patient had initial and follow-up stereoscopic fundus photography. One eye was selected at random to receive treatment and the other remained untreated to serve as a control. Because of the magnitude of difference in vision between the eyes, the study was halted at 2 years to permit photocoagulation of the untreated eyes. Patients whose eyes had new vessels on or near the disk lost vision (defined as visual acuity less than 5/200) more often in untreated eyes (18.3% cumulative rate at 2 years) compared with treated eyes (6.4%; number needed to treat [NNT]=8.4).
Another RCT4 of patients with diabetes showed that photocoagulation maintained vision in diabetic retinopathy if the disease was not too advanced. Ninety-nine patients, also not differentiated by type of diabetes, were each treated in 1 eye chosen at random with a xenon-arc photocoagulator. Patients underwent follow-up treatments to the treated eye by clinical indication. The untreated eyes were observed as controls. Blindness occurred significantly less often in the treated eyes (19% total after 5 to 7 years) than in the control eyes (39%; NNT=5 to prevent 1 blind eye). Patients without proliferative retinopathy at onset experienced the most dramatic slowing of deterioration; photocoagulation was more useful in maintaining than in improving vision.
TABLE
Screening frequency for sight-threatening retinopathy
| Stage of retinal disease | Screening frequency* |
|---|---|
| None | 5 years |
| Background retinopathy | 1 year |
| Mild preproliferative retinopathy | 4 months |
| *For 95% chance of remaining free of sight-threatening retinopathy. | |
Recommendations from others
The American Diabetes Association 2003 Clinical Practice Recommendations5 state that patients with type 2 diabetes should have an initial dilated and comprehensive eye examination by an ophthalmologist or optometrist shortly after diagnosis of diabetes. An ophthalmologist or optometrist who is knowledgeable and experienced in diagnosing diabetic retinopathy and is aware of its management should repeat subsequent examinations for both type 1 and type 2 diabetic patients annually. Examinations are required more frequently if retinopathy is progressing.
Screen for retinal complications early, regularly, by an experienced eye doctor
Tsveti Markova, MD
Department of Family Medicine, Wayne State University, Detroit, Mich
Family physicians play a central role in the diabetes care team. They must not only achieve good blood sugar control, but also monitor for complications and coordinate their treatment. Educating patients and reaching common ground with them is essential for success. Evidence suggests that screening for eye complications reduces blindness. Patients with early retinopathy changes are usually asymptomatic; therefore it takes a committed and educated patient to comply with screening recommendations. Also, many patients have the misconception that a visual acuity exam by an optometrist is sufficient for their diabetes eye screening. Family physicians must convey the importance of screening for retinal complications early, regularly and by an optometrist or ophthalmologist experienced in management of diabetes.
Screening eye exams for patients with type 2 diabetes can detect retinopathy early enough so treatment can prevent vision loss. Patients without diabetic retinopathy who are systematically screened by mydriatic retinal photography have a 95% probability of remaining free of sight-threatening retinopathy over the next 5 years. If background or preproliferative retinopathy is found at screening (Figure), the 95% probability interval for remaining free of sight-threatening retinopathy is reduced to 12 and 4 months, respectively (strength of recommendation [SOR]: B, based on 1 prospective cohort study).
A reliably sensitive screening exam requires mydriatic retinal photography augmented by ophthalmoscopy when photographs are inconclusive (SOR: A, based on a systematic review). For patients with diabetes not differentiated by type, photocoagu-lation significantly decreases visual deterioration and reduces the chances of blindness (SOR: A, based on randomized controlled trials [RCT]).
FIGURE
Nonproliferative and proliferative diabetic retinopathy
Background (nonproliferative) diabetic retinopathyis characterized by macular retinal exudates, edematous retinal thickening, dot and blot retinal hemorrhages, and retinal capillary microaneurysms.
Proliferative diabetic retinopathy. Note the network of abnormal preretinal new blood vessels just super-otemporal to the macula and the linear accumulations of blood in the preretinal vitreous below the macula.
Evidence summary
The Liverpool Diabetic Eye Study1 prospectively evaluated the risk of vision-threatening retinopathy in a cohort that included all patients with diabetes mellitus who were registered with a general practitioner and were not under the care of an ophthalmologist. A subgroup of 4770 patients with type 2 diabetes who did not have sightthreatening retinopathy at baseline underwent at least 1 additional screen. Screening included non-stereoscopic 3-field (45° or 50° field) mydriatic photography. Median follow-up was 3.5 years (range, 1–8.5 years).
The patients were divided into cohorts based on level of demonstrated retinopathy. The mean screening interval for a 95% probability of remaining free of sight-threatening retinopathy was calculated for each grade of baseline retinopathy. Screening patients with no retinopathy every 5 years provided a 95% probability of remaining free of sight-threatening retinopathy. Patients with background retinopathy must be screened annually to achieve the same result, and patients with mild preproliferative retinopathy need to be screened every 4 months ( Table ).
A systematic review2 of multiple small English-language studies evaluating screening and monitoring of diabetic retinopathy found consistent results. Screening by direct or indirect ophthalmoscopy alone detected 65% of patients with sight-threatening retinopathy. Screening by mydriatic retinal photography, augmented by ophthal-moscopy when the photographs were inconclusive, detected 88% to 100% of such cases.
An RCT of 1700 patients with diabetes and retinopathy evaluated preservation of vision with photocoagulation.3 Patients were not differentiated by type of diabetes. Each patient had initial and follow-up stereoscopic fundus photography. One eye was selected at random to receive treatment and the other remained untreated to serve as a control. Because of the magnitude of difference in vision between the eyes, the study was halted at 2 years to permit photocoagulation of the untreated eyes. Patients whose eyes had new vessels on or near the disk lost vision (defined as visual acuity less than 5/200) more often in untreated eyes (18.3% cumulative rate at 2 years) compared with treated eyes (6.4%; number needed to treat [NNT]=8.4).
Another RCT4 of patients with diabetes showed that photocoagulation maintained vision in diabetic retinopathy if the disease was not too advanced. Ninety-nine patients, also not differentiated by type of diabetes, were each treated in 1 eye chosen at random with a xenon-arc photocoagulator. Patients underwent follow-up treatments to the treated eye by clinical indication. The untreated eyes were observed as controls. Blindness occurred significantly less often in the treated eyes (19% total after 5 to 7 years) than in the control eyes (39%; NNT=5 to prevent 1 blind eye). Patients without proliferative retinopathy at onset experienced the most dramatic slowing of deterioration; photocoagulation was more useful in maintaining than in improving vision.
TABLE
Screening frequency for sight-threatening retinopathy
| Stage of retinal disease | Screening frequency* |
|---|---|
| None | 5 years |
| Background retinopathy | 1 year |
| Mild preproliferative retinopathy | 4 months |
| *For 95% chance of remaining free of sight-threatening retinopathy. | |
Recommendations from others
The American Diabetes Association 2003 Clinical Practice Recommendations5 state that patients with type 2 diabetes should have an initial dilated and comprehensive eye examination by an ophthalmologist or optometrist shortly after diagnosis of diabetes. An ophthalmologist or optometrist who is knowledgeable and experienced in diagnosing diabetic retinopathy and is aware of its management should repeat subsequent examinations for both type 1 and type 2 diabetic patients annually. Examinations are required more frequently if retinopathy is progressing.
Screen for retinal complications early, regularly, by an experienced eye doctor
Tsveti Markova, MD
Department of Family Medicine, Wayne State University, Detroit, Mich
Family physicians play a central role in the diabetes care team. They must not only achieve good blood sugar control, but also monitor for complications and coordinate their treatment. Educating patients and reaching common ground with them is essential for success. Evidence suggests that screening for eye complications reduces blindness. Patients with early retinopathy changes are usually asymptomatic; therefore it takes a committed and educated patient to comply with screening recommendations. Also, many patients have the misconception that a visual acuity exam by an optometrist is sufficient for their diabetes eye screening. Family physicians must convey the importance of screening for retinal complications early, regularly and by an optometrist or ophthalmologist experienced in management of diabetes.
1. Younis N, Broadbent DM, Vora JP, Harding SP. Incidence of sight-threatening retinopathy in patients with type 2 diabetes in the Liverpool Diabetic Eye Study: a cohort study. Lancet 2003;361:195-200.
2. Hutchinson A, McIntosh A, Peters J, et al. Effectiveness of screening and monitoring tests for diabetic retinopa-thy—a systematic review. Diabet Med 2000;17:495-506.
3. The Diabetic Retinopathy Study Research Group. Preliminary report on effects of photocoagulation therapy. Am J Ophthalmol 1976;81:383-396.
4. British Multicentre Study Group. Photocoagulation from diabetic maculopathy: a randomized controlled clinical trial using the xenon arc. Diabetes 1983;32:1010-1016.
5. Fong DS, Aiello L, Gardner TW, et al. American Diabetes Association. Diabetic retinopathy. Diabetes Care 2004;26 Suppl 1:S84-S87.
1. Younis N, Broadbent DM, Vora JP, Harding SP. Incidence of sight-threatening retinopathy in patients with type 2 diabetes in the Liverpool Diabetic Eye Study: a cohort study. Lancet 2003;361:195-200.
2. Hutchinson A, McIntosh A, Peters J, et al. Effectiveness of screening and monitoring tests for diabetic retinopa-thy—a systematic review. Diabet Med 2000;17:495-506.
3. The Diabetic Retinopathy Study Research Group. Preliminary report on effects of photocoagulation therapy. Am J Ophthalmol 1976;81:383-396.
4. British Multicentre Study Group. Photocoagulation from diabetic maculopathy: a randomized controlled clinical trial using the xenon arc. Diabetes 1983;32:1010-1016.
5. Fong DS, Aiello L, Gardner TW, et al. American Diabetes Association. Diabetic retinopathy. Diabetes Care 2004;26 Suppl 1:S84-S87.
Evidence-based answers from the Family Physicians Inquiries Network