User login
What are the most effective ways you can help patients stop smoking?
Brief counseling, nicotine replacement therapy, antidepressants, and varenicline all work well. Physician intervention should begin with routine assessment of smoking status for all patients. Brief (3 minutes or less) smoking cessation counseling improves quit rates (strength of recommendation [SOR]: A, Cochrane systematic review). Nicotine replacement therapy (NRT), antidepressants (bupropion and nortriptyline), and the nicotine receptor partial agonist varenicline are effective and should be offered to help smokers quit (SOR: A, Cochrane systematic reviews and randomized controlled trials [RCTs]).
Ask and act
Julia Fashner, MD
St. Joseph Regional Medical Center, South Bend, Ind
Physician counseling can help patients stop using tobacco. Medications, including NRT, increase abstinence rates even more. I find the American Academy of Family Physicians’ smoking cessation program, “Ask and Act,” easier to use than the United States Public Health Services “5 A’s” approach, which is described later in this Clinical Inquiry.
Several materials that support the Ask and Act program are available free online at www.aafp.org (click on “Ask and Act” under “Clinical Care & Research”). I have used the prescription sheet for smoking cessation when talking to patients about quitting; the coding reference gives some guidance about charging for cessation counseling. A prescribing guideline for medications, including side effects and contraindications, is also available.
Evidence summary
Brief counseling works
Good evidence suggests that physician-administered smoking cessation counseling lasting less than 3 minutes improves quit rates.1 A Cochrane analysis of pooled data from 17 randomized trials that compared brief advice to no advice or usual care showed a small but significant increase in the odds of smoking cessation (odds ratio [OR]=1.74; 95% confidence interval [CI], 1.48-2.05).2 The absolute difference in cessation rate was about 2.5% (number needed to treat [NNT]=40).
Another systematic review of 188 RCTs concluded that an estimated 2% (95% CI, 1%-3%; P<.001) of all smokers stopped smoking and did not relapse for as long as a year after receiving advice and encouragement to quit smoking from their physician in a single routine consultation.3
NRT is effective and safe for heart patients
NRT reduces withdrawal symptoms associated with stopping smoking by partially replacing nicotine in the blood. Abstinence rates are superior to placebo based on a Cochrane review (OR=1.77; 95% CI, 1.66-1.88; NNT=20; 95% CI, 17-23).4 The Cochrane review also concluded that all commercially available forms of NRT are effective for smoking cessation. Also, recent studies have established no association between NRT and further cardiac events.1
Antidepressants are good treatment options
Bupropion acts by increasing brain levels of dopamine and norepinephrine and is a nicotine antagonist. A large double-blind, placebo controlled trial compared the relative efficacy of sustained-release bupropion (n=244), nicotine patch (n=244), bupropion plus nicotine patch (n=245), and placebo (n=160).5 At 1 year, the bupropion groups had higher self-reported point-prevalence abstinence rates (abstinence during the previous 7 days) than the placebo and nicotine-patch-alone groups (bupropion 30%, placebo 16%, nicotine-patch-alone 16%; absolute risk reduction [ARR]=0.14, NNT=7, P<.001).
Continuous abstinence (abstinence from quit date) was also higher for the bupropion groups compared with placebo (bupropion 18%, placebo 6%; ARR=0.12; NNT=8; P<.001). Adding nicotine replacement to bupropion therapy increased 1-year smoking cessation rates by 5% over bupropion alone but was not statistically significant.
A Cochrane review assessing the efficacy of antidepressants for smoking cessation showed that, when used as monotherapy, bupropion (31 trials; OR=1.94; 95% CI, 1.72-2.19) and nortriptyline (4 trials; OR=2.34; 95% CI, 1.61-3.41) both doubled the odds of smoking cessation.6
Another option: Varenicline
Varenicline, a partial agonist at the α4β2 nicotinic acetylcholine receptor, aids smoking cessation by relieving nicotine withdrawal symptoms. A Cochrane meta-analysis concluded that varenicline resulted in significantly greater continuous abstinence at 12 months than placebo (OR=3.22; 95% CI, 2.43-4.27; NNT=8; 95% CI, 5-11).7
Recommendations
The US Preventive Service Task Force (USPSTF) strongly recommends that clinicians screen all adults for tobacco use and provide tobacco cessation interventions as needed.8 The USPSTF’s Clinical Practice Guideline for treating tobacco dependence recommends following a 5-step (5 A’s) intervention for smoking cessation in patients willing to quit.1
- Ask the patient about smoking status at every visit.
- Advise the patient to stop smoking.
- Assess the patient’s willingness to quit.
- Assist the patient by setting a date to quit smoking, providing self-help materials, and recommending the use of pharmacologic agents.
- Arrange for follow-up visits.
1. Fiore MC. US public health service clinical practice guideline: treating tobacco use and dependence. Respir Care. 2000;45:1200-1262.
2. Lancaster T, Stead L. Physician advice for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD000165.-
3. Law M, Tang JL. An analysis of the effectiveness of interventions intended to help people stop smoking. Arch Intern Med. 1995;155:1933-1941.
4. Silagy C, Lancaster T, Stead L, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000146.-
5. Jorenby DE, Leischo SJ, Nides MA, et al. A controlled trial of sustained-release bupropion, a nicotine patch, or both for smoking cessation. N Engl J Med. 1999;340:685-691.
6. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2007(1);CD000031.-
7. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2007;(1):CD006103.-
8. US Preventive Services Task Force. Counseling to Prevent Tobacco Use and Tobacco-Related Diseases: Recommendation Statement. Rockville, MD: Agency for Healthcare Research and Quality; 2003.
Brief counseling, nicotine replacement therapy, antidepressants, and varenicline all work well. Physician intervention should begin with routine assessment of smoking status for all patients. Brief (3 minutes or less) smoking cessation counseling improves quit rates (strength of recommendation [SOR]: A, Cochrane systematic review). Nicotine replacement therapy (NRT), antidepressants (bupropion and nortriptyline), and the nicotine receptor partial agonist varenicline are effective and should be offered to help smokers quit (SOR: A, Cochrane systematic reviews and randomized controlled trials [RCTs]).
Ask and act
Julia Fashner, MD
St. Joseph Regional Medical Center, South Bend, Ind
Physician counseling can help patients stop using tobacco. Medications, including NRT, increase abstinence rates even more. I find the American Academy of Family Physicians’ smoking cessation program, “Ask and Act,” easier to use than the United States Public Health Services “5 A’s” approach, which is described later in this Clinical Inquiry.
Several materials that support the Ask and Act program are available free online at www.aafp.org (click on “Ask and Act” under “Clinical Care & Research”). I have used the prescription sheet for smoking cessation when talking to patients about quitting; the coding reference gives some guidance about charging for cessation counseling. A prescribing guideline for medications, including side effects and contraindications, is also available.
Evidence summary
Brief counseling works
Good evidence suggests that physician-administered smoking cessation counseling lasting less than 3 minutes improves quit rates.1 A Cochrane analysis of pooled data from 17 randomized trials that compared brief advice to no advice or usual care showed a small but significant increase in the odds of smoking cessation (odds ratio [OR]=1.74; 95% confidence interval [CI], 1.48-2.05).2 The absolute difference in cessation rate was about 2.5% (number needed to treat [NNT]=40).
Another systematic review of 188 RCTs concluded that an estimated 2% (95% CI, 1%-3%; P<.001) of all smokers stopped smoking and did not relapse for as long as a year after receiving advice and encouragement to quit smoking from their physician in a single routine consultation.3
NRT is effective and safe for heart patients
NRT reduces withdrawal symptoms associated with stopping smoking by partially replacing nicotine in the blood. Abstinence rates are superior to placebo based on a Cochrane review (OR=1.77; 95% CI, 1.66-1.88; NNT=20; 95% CI, 17-23).4 The Cochrane review also concluded that all commercially available forms of NRT are effective for smoking cessation. Also, recent studies have established no association between NRT and further cardiac events.1
Antidepressants are good treatment options
Bupropion acts by increasing brain levels of dopamine and norepinephrine and is a nicotine antagonist. A large double-blind, placebo controlled trial compared the relative efficacy of sustained-release bupropion (n=244), nicotine patch (n=244), bupropion plus nicotine patch (n=245), and placebo (n=160).5 At 1 year, the bupropion groups had higher self-reported point-prevalence abstinence rates (abstinence during the previous 7 days) than the placebo and nicotine-patch-alone groups (bupropion 30%, placebo 16%, nicotine-patch-alone 16%; absolute risk reduction [ARR]=0.14, NNT=7, P<.001).
Continuous abstinence (abstinence from quit date) was also higher for the bupropion groups compared with placebo (bupropion 18%, placebo 6%; ARR=0.12; NNT=8; P<.001). Adding nicotine replacement to bupropion therapy increased 1-year smoking cessation rates by 5% over bupropion alone but was not statistically significant.
A Cochrane review assessing the efficacy of antidepressants for smoking cessation showed that, when used as monotherapy, bupropion (31 trials; OR=1.94; 95% CI, 1.72-2.19) and nortriptyline (4 trials; OR=2.34; 95% CI, 1.61-3.41) both doubled the odds of smoking cessation.6
Another option: Varenicline
Varenicline, a partial agonist at the α4β2 nicotinic acetylcholine receptor, aids smoking cessation by relieving nicotine withdrawal symptoms. A Cochrane meta-analysis concluded that varenicline resulted in significantly greater continuous abstinence at 12 months than placebo (OR=3.22; 95% CI, 2.43-4.27; NNT=8; 95% CI, 5-11).7
Recommendations
The US Preventive Service Task Force (USPSTF) strongly recommends that clinicians screen all adults for tobacco use and provide tobacco cessation interventions as needed.8 The USPSTF’s Clinical Practice Guideline for treating tobacco dependence recommends following a 5-step (5 A’s) intervention for smoking cessation in patients willing to quit.1
- Ask the patient about smoking status at every visit.
- Advise the patient to stop smoking.
- Assess the patient’s willingness to quit.
- Assist the patient by setting a date to quit smoking, providing self-help materials, and recommending the use of pharmacologic agents.
- Arrange for follow-up visits.
Brief counseling, nicotine replacement therapy, antidepressants, and varenicline all work well. Physician intervention should begin with routine assessment of smoking status for all patients. Brief (3 minutes or less) smoking cessation counseling improves quit rates (strength of recommendation [SOR]: A, Cochrane systematic review). Nicotine replacement therapy (NRT), antidepressants (bupropion and nortriptyline), and the nicotine receptor partial agonist varenicline are effective and should be offered to help smokers quit (SOR: A, Cochrane systematic reviews and randomized controlled trials [RCTs]).
Ask and act
Julia Fashner, MD
St. Joseph Regional Medical Center, South Bend, Ind
Physician counseling can help patients stop using tobacco. Medications, including NRT, increase abstinence rates even more. I find the American Academy of Family Physicians’ smoking cessation program, “Ask and Act,” easier to use than the United States Public Health Services “5 A’s” approach, which is described later in this Clinical Inquiry.
Several materials that support the Ask and Act program are available free online at www.aafp.org (click on “Ask and Act” under “Clinical Care & Research”). I have used the prescription sheet for smoking cessation when talking to patients about quitting; the coding reference gives some guidance about charging for cessation counseling. A prescribing guideline for medications, including side effects and contraindications, is also available.
Evidence summary
Brief counseling works
Good evidence suggests that physician-administered smoking cessation counseling lasting less than 3 minutes improves quit rates.1 A Cochrane analysis of pooled data from 17 randomized trials that compared brief advice to no advice or usual care showed a small but significant increase in the odds of smoking cessation (odds ratio [OR]=1.74; 95% confidence interval [CI], 1.48-2.05).2 The absolute difference in cessation rate was about 2.5% (number needed to treat [NNT]=40).
Another systematic review of 188 RCTs concluded that an estimated 2% (95% CI, 1%-3%; P<.001) of all smokers stopped smoking and did not relapse for as long as a year after receiving advice and encouragement to quit smoking from their physician in a single routine consultation.3
NRT is effective and safe for heart patients
NRT reduces withdrawal symptoms associated with stopping smoking by partially replacing nicotine in the blood. Abstinence rates are superior to placebo based on a Cochrane review (OR=1.77; 95% CI, 1.66-1.88; NNT=20; 95% CI, 17-23).4 The Cochrane review also concluded that all commercially available forms of NRT are effective for smoking cessation. Also, recent studies have established no association between NRT and further cardiac events.1
Antidepressants are good treatment options
Bupropion acts by increasing brain levels of dopamine and norepinephrine and is a nicotine antagonist. A large double-blind, placebo controlled trial compared the relative efficacy of sustained-release bupropion (n=244), nicotine patch (n=244), bupropion plus nicotine patch (n=245), and placebo (n=160).5 At 1 year, the bupropion groups had higher self-reported point-prevalence abstinence rates (abstinence during the previous 7 days) than the placebo and nicotine-patch-alone groups (bupropion 30%, placebo 16%, nicotine-patch-alone 16%; absolute risk reduction [ARR]=0.14, NNT=7, P<.001).
Continuous abstinence (abstinence from quit date) was also higher for the bupropion groups compared with placebo (bupropion 18%, placebo 6%; ARR=0.12; NNT=8; P<.001). Adding nicotine replacement to bupropion therapy increased 1-year smoking cessation rates by 5% over bupropion alone but was not statistically significant.
A Cochrane review assessing the efficacy of antidepressants for smoking cessation showed that, when used as monotherapy, bupropion (31 trials; OR=1.94; 95% CI, 1.72-2.19) and nortriptyline (4 trials; OR=2.34; 95% CI, 1.61-3.41) both doubled the odds of smoking cessation.6
Another option: Varenicline
Varenicline, a partial agonist at the α4β2 nicotinic acetylcholine receptor, aids smoking cessation by relieving nicotine withdrawal symptoms. A Cochrane meta-analysis concluded that varenicline resulted in significantly greater continuous abstinence at 12 months than placebo (OR=3.22; 95% CI, 2.43-4.27; NNT=8; 95% CI, 5-11).7
Recommendations
The US Preventive Service Task Force (USPSTF) strongly recommends that clinicians screen all adults for tobacco use and provide tobacco cessation interventions as needed.8 The USPSTF’s Clinical Practice Guideline for treating tobacco dependence recommends following a 5-step (5 A’s) intervention for smoking cessation in patients willing to quit.1
- Ask the patient about smoking status at every visit.
- Advise the patient to stop smoking.
- Assess the patient’s willingness to quit.
- Assist the patient by setting a date to quit smoking, providing self-help materials, and recommending the use of pharmacologic agents.
- Arrange for follow-up visits.
1. Fiore MC. US public health service clinical practice guideline: treating tobacco use and dependence. Respir Care. 2000;45:1200-1262.
2. Lancaster T, Stead L. Physician advice for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD000165.-
3. Law M, Tang JL. An analysis of the effectiveness of interventions intended to help people stop smoking. Arch Intern Med. 1995;155:1933-1941.
4. Silagy C, Lancaster T, Stead L, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000146.-
5. Jorenby DE, Leischo SJ, Nides MA, et al. A controlled trial of sustained-release bupropion, a nicotine patch, or both for smoking cessation. N Engl J Med. 1999;340:685-691.
6. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2007(1);CD000031.-
7. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2007;(1):CD006103.-
8. US Preventive Services Task Force. Counseling to Prevent Tobacco Use and Tobacco-Related Diseases: Recommendation Statement. Rockville, MD: Agency for Healthcare Research and Quality; 2003.
1. Fiore MC. US public health service clinical practice guideline: treating tobacco use and dependence. Respir Care. 2000;45:1200-1262.
2. Lancaster T, Stead L. Physician advice for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD000165.-
3. Law M, Tang JL. An analysis of the effectiveness of interventions intended to help people stop smoking. Arch Intern Med. 1995;155:1933-1941.
4. Silagy C, Lancaster T, Stead L, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000146.-
5. Jorenby DE, Leischo SJ, Nides MA, et al. A controlled trial of sustained-release bupropion, a nicotine patch, or both for smoking cessation. N Engl J Med. 1999;340:685-691.
6. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2007(1);CD000031.-
7. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2007;(1):CD006103.-
8. US Preventive Services Task Force. Counseling to Prevent Tobacco Use and Tobacco-Related Diseases: Recommendation Statement. Rockville, MD: Agency for Healthcare Research and Quality; 2003.
Evidence-based answers from the Family Physicians Inquiries Network
What is the best treatment for pertussis?
A short-term course of erythromycin, azithromycin, or clarithromycin is as effective as a long-term (2-week) erythromycin therapy in eradicating Bordetella pertussis from the nasopharynx (strength of recommendation [SOR]: A; based on one meta-analysis of randomized controlled trials [RCTs]). Evidence is insufficient to determine the benefit of antibiotic prophylaxis for pertussis contacts. However, due to high mortality and morbidity, prophylaxis is recommended for families who have an infant less than 6 months old (SOR: C; based on expert opinion).
Fewer doses and lower cost make compliance more likely
Marcia Warren, MD
Departments of Family and Community Medicine and Pediatrics, Baylor College of Medicine, Houston, Tex
I found this Clinical Inquiry on the treatment and prophylaxis of Bordetella pertussis invaluable as it addresses ease of dosing and cost, 2 things important in my pediatric community health practice with its inherent financial and social constraints. The alternatives suggested are easy to use and are as equally effective as the first-line therapy of erythromycin estolate, the long-term treatment recommended by the CDC and the AAP. These alternatives, clarithromycin and azithromycin, require either twice a day or a once a day dosing for 7 days or 3 days respectively, can be accommodated in busy households, thus promoting better compliance.
The cost of medication also relates to compliance. The cost difference between the first-line therapy and the alternative therapy is significant, and may be as much as $89. In an underinsured population, this out-of-pocket cost for the alternatives would prove prohibitive, resulting in decreased compliance. Where cost is not a great issue and concerns of compliance important, choosing the short-term treatment may be a preferable option. For the financially strapped, the 1-week regimen of erythromycin estolate would be preferable. The importance of counseling cannot be overstated in all dosing regimens, especially in those with a more difficult dosing schedule and in cases of prophylaxis in a household with an infant less than 6 months old.
Evidence summary
A 2005 Cochrane review of 11 RCTs and 1 quasi-randomized trial, with a total of 1720 adults and children, investigated several antibiotics for treatment and prophylaxis of pertussis. The outcome measures used to assess the efficacy of antibiotic treatment or prophylaxis vary between the trials and most of them did not report the immunization status of the participants. The Cochrane review included 1 meta-analysis of 3 studies with 252 participants, comparing azithromycin for 3 days, erythromycin estolate for 7 days, and clarithromycin for 7 days (short-term treatment) with erythromycin estolate for fourteen days (long-term treatment). The study showed equal efficacy in eradication of B pertussis from the nasopharynx of 99.2% to 97.7% (absolute risk reduction [ARR]=1.44%; 95% confidence interval [CI], –1.58 to 4.46). There were fewer side effects with the short-term treatment (32.1% vs 48.9%; ARR=16%; 95% CI, 7.84 to 25.84).1
A large, multicenter RCT of 477 children of 6 months to 16 years of age demonstrated that a 5-day treatment with azithromycin eradicated B pertussis from the nasopharynx as effectively as a 10-day course of erythromycin estolate.2 Similarly, trimethoprim/sulfamethoxazole proved as effective as erythromycin in eliminating B pertussis from the nasopharynx.
Although tetracycline and chloramphenicol are effective treatments for pertussis, they are not recommended because of their side effects.1 Six randomized trials failed to show any statistically significant difference between antibiotics and placebo on frequency and severity of cough or duration of pertussis disease.1 A randomized, placebo-controlled trial studied 300 household contacts of children with culture-positive pertussis. There was no statistically significant difference in either the frequency of pertussis disease or rate of positive cultures in household contacts between the erythromycin group (2.1%) and the placebo group (5.1%) (ARR=2.95%; 95% CI, –1.21 to 7.11).1
Another Cochrane review of 8 trials examined the effectiveness of the symptomatic treatment of cough in children and adults with pertussis. There were many problems with the methodological quality of these trials, including small sample sizes and poor reporting of the methods. Diphenhydramine, pertussis immunoglobulin, corticosteroids and salbutamol were compared with placebo. There were no statistically significant differences in coughing paroxysms, mean number of whoops per 24 hours or in duration of hospital stay between these interventions and placebo.3
Extracorporeal circulatory life support has been used to maintain perfusion for patients with severe disease. The mortality of these patients is very high.4 No RCTs of the effectiveness of this intervention has been performed.
TABLE
Antibiotics for treatment and prophylaxis of pertussis in children and adults
| FIRST-LINE THERAPY | DOSAGE FOR CHILDREN | DOSAGE FOR ADULTS | COST* |
|---|---|---|---|
| Erythromycin | 40-50 mg/kg orally or intravenously in 4 divided doses for 14 days5,7 | 1–2 g orally or intravenously in 4 divided doses for 14 days5,7 | 56 tabs (500 mg), $16 (generic) |
| ALTERNATIVE THERAPY IF PATIENT DOESN’T TOLERATE ERYTHROMYCIN | |||
| Clarithromycin | 15-20 mg/per kg orally divided every 12 hours for 10-14 days7or 14-15 mg/kg orally divided every 12 hours for 7 days1,5 | 500 mg orally every 12 hours for 7 days5 | 20 tabs (500 mg), $78 28 tabs (500 mg), $109 (generic) |
| Azithromycin | 10-12 mg/kg orally as single daily dose for 5 to 7 days5,7or 10 mg/kg orally single daily dose for 3 days1 | 500 mg orally once, then 250 daily on days 2-55,7 | 5 tabs (500 mg), $75 7 tabs (500 mg), $105 (no generic) |
| Trimethoprim-sulfamethoxazole | 8 mg of TMP, 40 mg/kg SMX per kg orally divided every 12 hours for 14 days5,7 | 160 mg of TMP, 800 SMX orally (1 tab DS) every 12 hours for 14 days5,7 | 28 tabs $8 (generic) |
| All these therapies have gastrointestinal side effects and risk for hypersensitivity reactions. | |||
| *Approximate retail price for adult dose. Available at: http://www.drugstore.com. Accessed on June 28, 2005. | |||
Recommendations from others
The Centers for Disease Control and Prevention recommends erythromycin for 14 days as a first choice for the treatment and prophylaxis of pertussis. Antibiotics should be started no later than 3 weeks after the onset of cough. Trimethoprim-sulfamethoxazole can be used as an alternative treatment for patients who do not tolerate erythromycin. Prophylaxis is recommended for all household and close contacts if pertussis is highly suspected.5
The American Academy of Pediatrics recommends the use of azithromycin and clarithromycin as an alternative treatment for patients who do not tolerate erythromycin. 5
A national consensus conference on pertussis held in Canada recommended prophylaxis for household contacts of an infant aged <1 year, pregnant women during the third trimester, and for vulnerable individuals who have had face-to-face exposure, or have shared confined air for >1 hour.6
1. Altunaiji S, Kukuruzovic R, Curtis N, Massie J. Antibiotics for whooping cough (pertussis) (Cochrane Review). Cochrane Database Syst Rev 2005;(1):CD004404.
2. Langley JM, Halperin SA, Boucher FD, Smith B. Pediatric Investigators Collaborative Network on Infections in Canada (PICNIC) Azithromycin is as effective as and better tolerated than erythromycin estolate for the treatment of pertussis. Pediatrics 2004;114:e96-101.
3. Pillay V, Swingler G. Symptomatic treatment of the cough in whooping cough (Cochrane Review). Cochrane Database Syst Rev 2003;(4):CD003257.
4. Williams GD, Numa A, Sokol J, Tobias V, Duffy BJ. ECLS in pertussis: does it have a role? Intensive Care Med 1998;24:1089-1092.
5. Guris D. Treatment and Chemoprophylaxis. Guidelines for the Control of Pertussis Outbreaks. Atlanta, Ga: Centers for Disease Control and Prevention, 2000. Last updated January 2005. Available at: www.cdc.gov/nip/publications/pertussis/guide.htm. Accessed on November 14, 2005.
6. National consensus conference on pertussis Can Commun Dis Rep 2003;29(Suppl 3):S1-S33 (English), S1-S36 (French). Last updated June 5, 2003. Available at: www.phac-aspc.gc.ca/publicat/ccdr-rmtc/03vol29/29s3/index.html. Accessed on November 14, 2005.
7. Pertussis Information for Physicians: Diagnostic and Treatment Criteria Texas Department of Health Pertussis Treatment Guidelines. TDH Immunization Division; 2004;Last updated January 26, 2004. Available at: www.tdh.state.tx.us/immunize/html/pert_physician_txt.htm. Accessed on November 14, 2005.
A short-term course of erythromycin, azithromycin, or clarithromycin is as effective as a long-term (2-week) erythromycin therapy in eradicating Bordetella pertussis from the nasopharynx (strength of recommendation [SOR]: A; based on one meta-analysis of randomized controlled trials [RCTs]). Evidence is insufficient to determine the benefit of antibiotic prophylaxis for pertussis contacts. However, due to high mortality and morbidity, prophylaxis is recommended for families who have an infant less than 6 months old (SOR: C; based on expert opinion).
Fewer doses and lower cost make compliance more likely
Marcia Warren, MD
Departments of Family and Community Medicine and Pediatrics, Baylor College of Medicine, Houston, Tex
I found this Clinical Inquiry on the treatment and prophylaxis of Bordetella pertussis invaluable as it addresses ease of dosing and cost, 2 things important in my pediatric community health practice with its inherent financial and social constraints. The alternatives suggested are easy to use and are as equally effective as the first-line therapy of erythromycin estolate, the long-term treatment recommended by the CDC and the AAP. These alternatives, clarithromycin and azithromycin, require either twice a day or a once a day dosing for 7 days or 3 days respectively, can be accommodated in busy households, thus promoting better compliance.
The cost of medication also relates to compliance. The cost difference between the first-line therapy and the alternative therapy is significant, and may be as much as $89. In an underinsured population, this out-of-pocket cost for the alternatives would prove prohibitive, resulting in decreased compliance. Where cost is not a great issue and concerns of compliance important, choosing the short-term treatment may be a preferable option. For the financially strapped, the 1-week regimen of erythromycin estolate would be preferable. The importance of counseling cannot be overstated in all dosing regimens, especially in those with a more difficult dosing schedule and in cases of prophylaxis in a household with an infant less than 6 months old.
Evidence summary
A 2005 Cochrane review of 11 RCTs and 1 quasi-randomized trial, with a total of 1720 adults and children, investigated several antibiotics for treatment and prophylaxis of pertussis. The outcome measures used to assess the efficacy of antibiotic treatment or prophylaxis vary between the trials and most of them did not report the immunization status of the participants. The Cochrane review included 1 meta-analysis of 3 studies with 252 participants, comparing azithromycin for 3 days, erythromycin estolate for 7 days, and clarithromycin for 7 days (short-term treatment) with erythromycin estolate for fourteen days (long-term treatment). The study showed equal efficacy in eradication of B pertussis from the nasopharynx of 99.2% to 97.7% (absolute risk reduction [ARR]=1.44%; 95% confidence interval [CI], –1.58 to 4.46). There were fewer side effects with the short-term treatment (32.1% vs 48.9%; ARR=16%; 95% CI, 7.84 to 25.84).1
A large, multicenter RCT of 477 children of 6 months to 16 years of age demonstrated that a 5-day treatment with azithromycin eradicated B pertussis from the nasopharynx as effectively as a 10-day course of erythromycin estolate.2 Similarly, trimethoprim/sulfamethoxazole proved as effective as erythromycin in eliminating B pertussis from the nasopharynx.
Although tetracycline and chloramphenicol are effective treatments for pertussis, they are not recommended because of their side effects.1 Six randomized trials failed to show any statistically significant difference between antibiotics and placebo on frequency and severity of cough or duration of pertussis disease.1 A randomized, placebo-controlled trial studied 300 household contacts of children with culture-positive pertussis. There was no statistically significant difference in either the frequency of pertussis disease or rate of positive cultures in household contacts between the erythromycin group (2.1%) and the placebo group (5.1%) (ARR=2.95%; 95% CI, –1.21 to 7.11).1
Another Cochrane review of 8 trials examined the effectiveness of the symptomatic treatment of cough in children and adults with pertussis. There were many problems with the methodological quality of these trials, including small sample sizes and poor reporting of the methods. Diphenhydramine, pertussis immunoglobulin, corticosteroids and salbutamol were compared with placebo. There were no statistically significant differences in coughing paroxysms, mean number of whoops per 24 hours or in duration of hospital stay between these interventions and placebo.3
Extracorporeal circulatory life support has been used to maintain perfusion for patients with severe disease. The mortality of these patients is very high.4 No RCTs of the effectiveness of this intervention has been performed.
TABLE
Antibiotics for treatment and prophylaxis of pertussis in children and adults
| FIRST-LINE THERAPY | DOSAGE FOR CHILDREN | DOSAGE FOR ADULTS | COST* |
|---|---|---|---|
| Erythromycin | 40-50 mg/kg orally or intravenously in 4 divided doses for 14 days5,7 | 1–2 g orally or intravenously in 4 divided doses for 14 days5,7 | 56 tabs (500 mg), $16 (generic) |
| ALTERNATIVE THERAPY IF PATIENT DOESN’T TOLERATE ERYTHROMYCIN | |||
| Clarithromycin | 15-20 mg/per kg orally divided every 12 hours for 10-14 days7or 14-15 mg/kg orally divided every 12 hours for 7 days1,5 | 500 mg orally every 12 hours for 7 days5 | 20 tabs (500 mg), $78 28 tabs (500 mg), $109 (generic) |
| Azithromycin | 10-12 mg/kg orally as single daily dose for 5 to 7 days5,7or 10 mg/kg orally single daily dose for 3 days1 | 500 mg orally once, then 250 daily on days 2-55,7 | 5 tabs (500 mg), $75 7 tabs (500 mg), $105 (no generic) |
| Trimethoprim-sulfamethoxazole | 8 mg of TMP, 40 mg/kg SMX per kg orally divided every 12 hours for 14 days5,7 | 160 mg of TMP, 800 SMX orally (1 tab DS) every 12 hours for 14 days5,7 | 28 tabs $8 (generic) |
| All these therapies have gastrointestinal side effects and risk for hypersensitivity reactions. | |||
| *Approximate retail price for adult dose. Available at: http://www.drugstore.com. Accessed on June 28, 2005. | |||
Recommendations from others
The Centers for Disease Control and Prevention recommends erythromycin for 14 days as a first choice for the treatment and prophylaxis of pertussis. Antibiotics should be started no later than 3 weeks after the onset of cough. Trimethoprim-sulfamethoxazole can be used as an alternative treatment for patients who do not tolerate erythromycin. Prophylaxis is recommended for all household and close contacts if pertussis is highly suspected.5
The American Academy of Pediatrics recommends the use of azithromycin and clarithromycin as an alternative treatment for patients who do not tolerate erythromycin. 5
A national consensus conference on pertussis held in Canada recommended prophylaxis for household contacts of an infant aged <1 year, pregnant women during the third trimester, and for vulnerable individuals who have had face-to-face exposure, or have shared confined air for >1 hour.6
A short-term course of erythromycin, azithromycin, or clarithromycin is as effective as a long-term (2-week) erythromycin therapy in eradicating Bordetella pertussis from the nasopharynx (strength of recommendation [SOR]: A; based on one meta-analysis of randomized controlled trials [RCTs]). Evidence is insufficient to determine the benefit of antibiotic prophylaxis for pertussis contacts. However, due to high mortality and morbidity, prophylaxis is recommended for families who have an infant less than 6 months old (SOR: C; based on expert opinion).
Fewer doses and lower cost make compliance more likely
Marcia Warren, MD
Departments of Family and Community Medicine and Pediatrics, Baylor College of Medicine, Houston, Tex
I found this Clinical Inquiry on the treatment and prophylaxis of Bordetella pertussis invaluable as it addresses ease of dosing and cost, 2 things important in my pediatric community health practice with its inherent financial and social constraints. The alternatives suggested are easy to use and are as equally effective as the first-line therapy of erythromycin estolate, the long-term treatment recommended by the CDC and the AAP. These alternatives, clarithromycin and azithromycin, require either twice a day or a once a day dosing for 7 days or 3 days respectively, can be accommodated in busy households, thus promoting better compliance.
The cost of medication also relates to compliance. The cost difference between the first-line therapy and the alternative therapy is significant, and may be as much as $89. In an underinsured population, this out-of-pocket cost for the alternatives would prove prohibitive, resulting in decreased compliance. Where cost is not a great issue and concerns of compliance important, choosing the short-term treatment may be a preferable option. For the financially strapped, the 1-week regimen of erythromycin estolate would be preferable. The importance of counseling cannot be overstated in all dosing regimens, especially in those with a more difficult dosing schedule and in cases of prophylaxis in a household with an infant less than 6 months old.
Evidence summary
A 2005 Cochrane review of 11 RCTs and 1 quasi-randomized trial, with a total of 1720 adults and children, investigated several antibiotics for treatment and prophylaxis of pertussis. The outcome measures used to assess the efficacy of antibiotic treatment or prophylaxis vary between the trials and most of them did not report the immunization status of the participants. The Cochrane review included 1 meta-analysis of 3 studies with 252 participants, comparing azithromycin for 3 days, erythromycin estolate for 7 days, and clarithromycin for 7 days (short-term treatment) with erythromycin estolate for fourteen days (long-term treatment). The study showed equal efficacy in eradication of B pertussis from the nasopharynx of 99.2% to 97.7% (absolute risk reduction [ARR]=1.44%; 95% confidence interval [CI], –1.58 to 4.46). There were fewer side effects with the short-term treatment (32.1% vs 48.9%; ARR=16%; 95% CI, 7.84 to 25.84).1
A large, multicenter RCT of 477 children of 6 months to 16 years of age demonstrated that a 5-day treatment with azithromycin eradicated B pertussis from the nasopharynx as effectively as a 10-day course of erythromycin estolate.2 Similarly, trimethoprim/sulfamethoxazole proved as effective as erythromycin in eliminating B pertussis from the nasopharynx.
Although tetracycline and chloramphenicol are effective treatments for pertussis, they are not recommended because of their side effects.1 Six randomized trials failed to show any statistically significant difference between antibiotics and placebo on frequency and severity of cough or duration of pertussis disease.1 A randomized, placebo-controlled trial studied 300 household contacts of children with culture-positive pertussis. There was no statistically significant difference in either the frequency of pertussis disease or rate of positive cultures in household contacts between the erythromycin group (2.1%) and the placebo group (5.1%) (ARR=2.95%; 95% CI, –1.21 to 7.11).1
Another Cochrane review of 8 trials examined the effectiveness of the symptomatic treatment of cough in children and adults with pertussis. There were many problems with the methodological quality of these trials, including small sample sizes and poor reporting of the methods. Diphenhydramine, pertussis immunoglobulin, corticosteroids and salbutamol were compared with placebo. There were no statistically significant differences in coughing paroxysms, mean number of whoops per 24 hours or in duration of hospital stay between these interventions and placebo.3
Extracorporeal circulatory life support has been used to maintain perfusion for patients with severe disease. The mortality of these patients is very high.4 No RCTs of the effectiveness of this intervention has been performed.
TABLE
Antibiotics for treatment and prophylaxis of pertussis in children and adults
| FIRST-LINE THERAPY | DOSAGE FOR CHILDREN | DOSAGE FOR ADULTS | COST* |
|---|---|---|---|
| Erythromycin | 40-50 mg/kg orally or intravenously in 4 divided doses for 14 days5,7 | 1–2 g orally or intravenously in 4 divided doses for 14 days5,7 | 56 tabs (500 mg), $16 (generic) |
| ALTERNATIVE THERAPY IF PATIENT DOESN’T TOLERATE ERYTHROMYCIN | |||
| Clarithromycin | 15-20 mg/per kg orally divided every 12 hours for 10-14 days7or 14-15 mg/kg orally divided every 12 hours for 7 days1,5 | 500 mg orally every 12 hours for 7 days5 | 20 tabs (500 mg), $78 28 tabs (500 mg), $109 (generic) |
| Azithromycin | 10-12 mg/kg orally as single daily dose for 5 to 7 days5,7or 10 mg/kg orally single daily dose for 3 days1 | 500 mg orally once, then 250 daily on days 2-55,7 | 5 tabs (500 mg), $75 7 tabs (500 mg), $105 (no generic) |
| Trimethoprim-sulfamethoxazole | 8 mg of TMP, 40 mg/kg SMX per kg orally divided every 12 hours for 14 days5,7 | 160 mg of TMP, 800 SMX orally (1 tab DS) every 12 hours for 14 days5,7 | 28 tabs $8 (generic) |
| All these therapies have gastrointestinal side effects and risk for hypersensitivity reactions. | |||
| *Approximate retail price for adult dose. Available at: http://www.drugstore.com. Accessed on June 28, 2005. | |||
Recommendations from others
The Centers for Disease Control and Prevention recommends erythromycin for 14 days as a first choice for the treatment and prophylaxis of pertussis. Antibiotics should be started no later than 3 weeks after the onset of cough. Trimethoprim-sulfamethoxazole can be used as an alternative treatment for patients who do not tolerate erythromycin. Prophylaxis is recommended for all household and close contacts if pertussis is highly suspected.5
The American Academy of Pediatrics recommends the use of azithromycin and clarithromycin as an alternative treatment for patients who do not tolerate erythromycin. 5
A national consensus conference on pertussis held in Canada recommended prophylaxis for household contacts of an infant aged <1 year, pregnant women during the third trimester, and for vulnerable individuals who have had face-to-face exposure, or have shared confined air for >1 hour.6
1. Altunaiji S, Kukuruzovic R, Curtis N, Massie J. Antibiotics for whooping cough (pertussis) (Cochrane Review). Cochrane Database Syst Rev 2005;(1):CD004404.
2. Langley JM, Halperin SA, Boucher FD, Smith B. Pediatric Investigators Collaborative Network on Infections in Canada (PICNIC) Azithromycin is as effective as and better tolerated than erythromycin estolate for the treatment of pertussis. Pediatrics 2004;114:e96-101.
3. Pillay V, Swingler G. Symptomatic treatment of the cough in whooping cough (Cochrane Review). Cochrane Database Syst Rev 2003;(4):CD003257.
4. Williams GD, Numa A, Sokol J, Tobias V, Duffy BJ. ECLS in pertussis: does it have a role? Intensive Care Med 1998;24:1089-1092.
5. Guris D. Treatment and Chemoprophylaxis. Guidelines for the Control of Pertussis Outbreaks. Atlanta, Ga: Centers for Disease Control and Prevention, 2000. Last updated January 2005. Available at: www.cdc.gov/nip/publications/pertussis/guide.htm. Accessed on November 14, 2005.
6. National consensus conference on pertussis Can Commun Dis Rep 2003;29(Suppl 3):S1-S33 (English), S1-S36 (French). Last updated June 5, 2003. Available at: www.phac-aspc.gc.ca/publicat/ccdr-rmtc/03vol29/29s3/index.html. Accessed on November 14, 2005.
7. Pertussis Information for Physicians: Diagnostic and Treatment Criteria Texas Department of Health Pertussis Treatment Guidelines. TDH Immunization Division; 2004;Last updated January 26, 2004. Available at: www.tdh.state.tx.us/immunize/html/pert_physician_txt.htm. Accessed on November 14, 2005.
1. Altunaiji S, Kukuruzovic R, Curtis N, Massie J. Antibiotics for whooping cough (pertussis) (Cochrane Review). Cochrane Database Syst Rev 2005;(1):CD004404.
2. Langley JM, Halperin SA, Boucher FD, Smith B. Pediatric Investigators Collaborative Network on Infections in Canada (PICNIC) Azithromycin is as effective as and better tolerated than erythromycin estolate for the treatment of pertussis. Pediatrics 2004;114:e96-101.
3. Pillay V, Swingler G. Symptomatic treatment of the cough in whooping cough (Cochrane Review). Cochrane Database Syst Rev 2003;(4):CD003257.
4. Williams GD, Numa A, Sokol J, Tobias V, Duffy BJ. ECLS in pertussis: does it have a role? Intensive Care Med 1998;24:1089-1092.
5. Guris D. Treatment and Chemoprophylaxis. Guidelines for the Control of Pertussis Outbreaks. Atlanta, Ga: Centers for Disease Control and Prevention, 2000. Last updated January 2005. Available at: www.cdc.gov/nip/publications/pertussis/guide.htm. Accessed on November 14, 2005.
6. National consensus conference on pertussis Can Commun Dis Rep 2003;29(Suppl 3):S1-S33 (English), S1-S36 (French). Last updated June 5, 2003. Available at: www.phac-aspc.gc.ca/publicat/ccdr-rmtc/03vol29/29s3/index.html. Accessed on November 14, 2005.
7. Pertussis Information for Physicians: Diagnostic and Treatment Criteria Texas Department of Health Pertussis Treatment Guidelines. TDH Immunization Division; 2004;Last updated January 26, 2004. Available at: www.tdh.state.tx.us/immunize/html/pert_physician_txt.htm. Accessed on November 14, 2005.
Evidence-based answers from the Family Physicians Inquiries Network
Do steroid injections help with osteoarthritis of the knee?
Intra-articular steroid injections appear to provide 2 to 6 weeks of pain relief for patients with knee osteoarthritis (strength of recommendation [SOR]: A). Higher-dose steroids with or without joint lavage can provide pain relief up to 24 weeks (SOR: A). Steroid injections may be an appropriate adjunct in the treatment of osteoarthritis, which includes nonpharmacologic treatments (education, weight loss, physical therapy) and pharmacologic therapy (nonsteroidal anti-inflammatory drugs [NSAIDs], topical and opioid analgesics).1,2
Evidence summary
Osteoarthritis, also known as degenerative joint disease, is the most prevalent form of arthritis in the United States.3 For the elderly, it is a common cause of pain and disability, affecting patients’ ability to perform activities of daily living. Common causes of osteoarthritis include past and present biomechanical stresses affecting the articular cartilage, sub-chondral bone changes, and biochemical changes in the articular cartilage and synovial membrane.3
Treatment of patients with osteoarthritis of the knee should be individualized to the severity of symptoms for each patient. A treatment plan can include patient education, physical and occupational therapy, non-opioid oral and topical agents, NSAIDs, intra-articular corticosteroid injections, viscosupplementation injections, arthroscopic lavage, and total knee replacements.
Our knowledge of the long-term safety and efficacy of intra-articular knee corticosteroid injection is based on limited data. In a randomized, double-blind, placebo-controlled crossover study, investigators randomized 59 patients aged 51 to 89 years to receive either an intra-articular injection of 1 mL of 40 mg methylprednisolone or 1 mL of 0.9% saline. After 3 weeks, patients receiving steroid injection had a minimal change in baseline visual analogue score for pain compared with those receiving saline (median change: –2.0 mm vs 0 mm on a 100-mm scale).4
A randomized, single-blinded study involving 84 patients demonstrated significant self-report-ed “overall improvement” for patients given intra-articular triamcinolone hexacetonide (78%) compared with placebo (49%) after 1 week (P<.05).5 It also confirmed reports that visual analogue score for pain and distance walked in 1 minute improves significantly for both steroid- and placebo-treated groups up to 6 weeks. Only the steroid-treated patients exhibited improved walking distance at 1 week compared with baseline (P<.001).
A recent randomized, double-blind, placebo-controlled trial studied the long-term safety and efficacy of treatment of knee osteoarthritis with repeated steroid injections.6 These investigators studied 66 patients aged 40 to 80 years recruited from rheumatology clinics. One half (n=33) received injections of triamcinolone acetonide 40 mg, and the other half received saline injections every 3 months for 2 years. At 1- and 2-year interval follow-ups, no statistically significant difference was seen between the 2 groups in loss of joint space and no progression of degenerative disease, as demonstrated by measurements of joint space widths by standardized fluoroscopically guided radiographs. Although the primary outcome measure of this study was to assess radiologic joint space narrowing with repeated injections, knee pain and stiffness appeared to improve after 2 years, although these results were not well quantified.
A limitation of most studies testing intraarticular therapy has been sample size. Combining studies may allow the ability to detect levels of pain relief not found in individual studies. A recent meta-analysis of 6 randomized controlled trials using intra-articular corticosteroid knee injections found short-term relief of pain for 2 weeks (relative risk [RR]=1.66; 95% confidence interval [CI], 1.37–2.01).7 The number needed to treat (NNT) range for these studies is 1.3 to 3.5. Two additional studies included in this study using higher-dose steroids (prednisone equivalent dose of 37.5 to 80 mg), with or without joint lavage, assessed improvement at 16 to 24 weeks. Although neither individual study showed statistically significant differences, the pooled data from the 2 studies favored symptom improvement at 16 to 24 weeks (RR=2.09; 95% CI, 1.2–3.7; NNT=4.4).7
Recommendations from others
Guidelines for the treatment of knee osteoarthritis were outlined by a task force for the European League Against Rheumatism (EULAR) Standing Committee for Clinical Trials. The task force recommended intra-articular steroid injection for acute exacerbation of knee pain. This task force performed an evidence-based review and concluded at least 1 randomized control trial recommended intraarticular steroid for patients with osteoarthritis. It was noted that intra-articular steroid injections were effective for only short-term pain relief and that there are no predictors of success of treatment, such as the presence or absence of such factors as joint effusion, degree of radio-logic change, age, or obesity.2
The American College of Rheumatology Subcommittee on Osteoarthritis Guidelines developed both nonpharmacological and pharmacological recommendations for the treatment of osteoarthritis of the knee.8 These recommendations include: use of intra-articular steroid injection for patients with acute exacerbations who had evidence for joint inflammation, and joint aspiration accompanying the intra-articular injection for “short-term relief.”
Intra-articular steroids provide extra relief for patients with acute exacerbations
Wail Malaty, MD
Hendersonville Family Practice Residency Program, Hendersonville, NC
This well-constructed review demonstrates that intra-articular steroid injections provide up to 3 weeks of pain relief for patients with osteoarthritis of the knee. While this may not seem like much, in practice it can be quite helpful in some situations. It provides supplemental pain relief for patients with acute exacerbations of their disease. It is also useful as a temporizing measure for patients who are candidates for total knee replacement but are not quite ready for it psychologically.
1. Rozental TD, Sculco TP. Intra-articular corticosteroids: an updated overview. Am J Orthop 2000;29:18-23.
2. Pendleton A, Arden N, Dougados M, et al. EULAR recommendations for the management of knee osteoarthritis: report of a task force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 2000;59:936-944.
3. Hochberg MC, Altman RD, Brandt KD, et al. Guidelines for the medical management of osteoarthritis. Part II. Osteoarthritis of the knee. American College of Rheumatology. Arthritis Rheum 1995;38:1541-1546.
4. Jones A, Doherty M. Intra-articular corticosteroids are effective in osteoarthritis but there are no clinical predictors of response. Ann Rheum Dis 1996;55:829-832.
5. Gaffney K, Ledingham J, Perry JD. Intra-articular triamcinolone hexacetonide in knee osteoarthritis: factors influencing the clinical response. Ann Rheum Dis 1995;54:379-381.
6. Raynauld JP, Buckland-Wright C, Ward R, et al. Safety and efficacy of long-term intraarticular steroid injections in osteoarthritis of the knee: a randomized, double-blind, placebo-controlled trial. Arthritis Rheum 2003;48:370-377.
7. Arroll B, Goodyear-Smith F. Corticosteroid injections for osteoarthritis of the knee: meta-analysis. BMJ 2004;328:869-870.
8. Altman RD, Hochberg HC, Moskowitz RW, Schnitzer TJ. Recommendations for the medical management of osteoarthritis of the hip and knee 2000 update: American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
Intra-articular steroid injections appear to provide 2 to 6 weeks of pain relief for patients with knee osteoarthritis (strength of recommendation [SOR]: A). Higher-dose steroids with or without joint lavage can provide pain relief up to 24 weeks (SOR: A). Steroid injections may be an appropriate adjunct in the treatment of osteoarthritis, which includes nonpharmacologic treatments (education, weight loss, physical therapy) and pharmacologic therapy (nonsteroidal anti-inflammatory drugs [NSAIDs], topical and opioid analgesics).1,2
Evidence summary
Osteoarthritis, also known as degenerative joint disease, is the most prevalent form of arthritis in the United States.3 For the elderly, it is a common cause of pain and disability, affecting patients’ ability to perform activities of daily living. Common causes of osteoarthritis include past and present biomechanical stresses affecting the articular cartilage, sub-chondral bone changes, and biochemical changes in the articular cartilage and synovial membrane.3
Treatment of patients with osteoarthritis of the knee should be individualized to the severity of symptoms for each patient. A treatment plan can include patient education, physical and occupational therapy, non-opioid oral and topical agents, NSAIDs, intra-articular corticosteroid injections, viscosupplementation injections, arthroscopic lavage, and total knee replacements.
Our knowledge of the long-term safety and efficacy of intra-articular knee corticosteroid injection is based on limited data. In a randomized, double-blind, placebo-controlled crossover study, investigators randomized 59 patients aged 51 to 89 years to receive either an intra-articular injection of 1 mL of 40 mg methylprednisolone or 1 mL of 0.9% saline. After 3 weeks, patients receiving steroid injection had a minimal change in baseline visual analogue score for pain compared with those receiving saline (median change: –2.0 mm vs 0 mm on a 100-mm scale).4
A randomized, single-blinded study involving 84 patients demonstrated significant self-report-ed “overall improvement” for patients given intra-articular triamcinolone hexacetonide (78%) compared with placebo (49%) after 1 week (P<.05).5 It also confirmed reports that visual analogue score for pain and distance walked in 1 minute improves significantly for both steroid- and placebo-treated groups up to 6 weeks. Only the steroid-treated patients exhibited improved walking distance at 1 week compared with baseline (P<.001).
A recent randomized, double-blind, placebo-controlled trial studied the long-term safety and efficacy of treatment of knee osteoarthritis with repeated steroid injections.6 These investigators studied 66 patients aged 40 to 80 years recruited from rheumatology clinics. One half (n=33) received injections of triamcinolone acetonide 40 mg, and the other half received saline injections every 3 months for 2 years. At 1- and 2-year interval follow-ups, no statistically significant difference was seen between the 2 groups in loss of joint space and no progression of degenerative disease, as demonstrated by measurements of joint space widths by standardized fluoroscopically guided radiographs. Although the primary outcome measure of this study was to assess radiologic joint space narrowing with repeated injections, knee pain and stiffness appeared to improve after 2 years, although these results were not well quantified.
A limitation of most studies testing intraarticular therapy has been sample size. Combining studies may allow the ability to detect levels of pain relief not found in individual studies. A recent meta-analysis of 6 randomized controlled trials using intra-articular corticosteroid knee injections found short-term relief of pain for 2 weeks (relative risk [RR]=1.66; 95% confidence interval [CI], 1.37–2.01).7 The number needed to treat (NNT) range for these studies is 1.3 to 3.5. Two additional studies included in this study using higher-dose steroids (prednisone equivalent dose of 37.5 to 80 mg), with or without joint lavage, assessed improvement at 16 to 24 weeks. Although neither individual study showed statistically significant differences, the pooled data from the 2 studies favored symptom improvement at 16 to 24 weeks (RR=2.09; 95% CI, 1.2–3.7; NNT=4.4).7
Recommendations from others
Guidelines for the treatment of knee osteoarthritis were outlined by a task force for the European League Against Rheumatism (EULAR) Standing Committee for Clinical Trials. The task force recommended intra-articular steroid injection for acute exacerbation of knee pain. This task force performed an evidence-based review and concluded at least 1 randomized control trial recommended intraarticular steroid for patients with osteoarthritis. It was noted that intra-articular steroid injections were effective for only short-term pain relief and that there are no predictors of success of treatment, such as the presence or absence of such factors as joint effusion, degree of radio-logic change, age, or obesity.2
The American College of Rheumatology Subcommittee on Osteoarthritis Guidelines developed both nonpharmacological and pharmacological recommendations for the treatment of osteoarthritis of the knee.8 These recommendations include: use of intra-articular steroid injection for patients with acute exacerbations who had evidence for joint inflammation, and joint aspiration accompanying the intra-articular injection for “short-term relief.”
Intra-articular steroids provide extra relief for patients with acute exacerbations
Wail Malaty, MD
Hendersonville Family Practice Residency Program, Hendersonville, NC
This well-constructed review demonstrates that intra-articular steroid injections provide up to 3 weeks of pain relief for patients with osteoarthritis of the knee. While this may not seem like much, in practice it can be quite helpful in some situations. It provides supplemental pain relief for patients with acute exacerbations of their disease. It is also useful as a temporizing measure for patients who are candidates for total knee replacement but are not quite ready for it psychologically.
Intra-articular steroid injections appear to provide 2 to 6 weeks of pain relief for patients with knee osteoarthritis (strength of recommendation [SOR]: A). Higher-dose steroids with or without joint lavage can provide pain relief up to 24 weeks (SOR: A). Steroid injections may be an appropriate adjunct in the treatment of osteoarthritis, which includes nonpharmacologic treatments (education, weight loss, physical therapy) and pharmacologic therapy (nonsteroidal anti-inflammatory drugs [NSAIDs], topical and opioid analgesics).1,2
Evidence summary
Osteoarthritis, also known as degenerative joint disease, is the most prevalent form of arthritis in the United States.3 For the elderly, it is a common cause of pain and disability, affecting patients’ ability to perform activities of daily living. Common causes of osteoarthritis include past and present biomechanical stresses affecting the articular cartilage, sub-chondral bone changes, and biochemical changes in the articular cartilage and synovial membrane.3
Treatment of patients with osteoarthritis of the knee should be individualized to the severity of symptoms for each patient. A treatment plan can include patient education, physical and occupational therapy, non-opioid oral and topical agents, NSAIDs, intra-articular corticosteroid injections, viscosupplementation injections, arthroscopic lavage, and total knee replacements.
Our knowledge of the long-term safety and efficacy of intra-articular knee corticosteroid injection is based on limited data. In a randomized, double-blind, placebo-controlled crossover study, investigators randomized 59 patients aged 51 to 89 years to receive either an intra-articular injection of 1 mL of 40 mg methylprednisolone or 1 mL of 0.9% saline. After 3 weeks, patients receiving steroid injection had a minimal change in baseline visual analogue score for pain compared with those receiving saline (median change: –2.0 mm vs 0 mm on a 100-mm scale).4
A randomized, single-blinded study involving 84 patients demonstrated significant self-report-ed “overall improvement” for patients given intra-articular triamcinolone hexacetonide (78%) compared with placebo (49%) after 1 week (P<.05).5 It also confirmed reports that visual analogue score for pain and distance walked in 1 minute improves significantly for both steroid- and placebo-treated groups up to 6 weeks. Only the steroid-treated patients exhibited improved walking distance at 1 week compared with baseline (P<.001).
A recent randomized, double-blind, placebo-controlled trial studied the long-term safety and efficacy of treatment of knee osteoarthritis with repeated steroid injections.6 These investigators studied 66 patients aged 40 to 80 years recruited from rheumatology clinics. One half (n=33) received injections of triamcinolone acetonide 40 mg, and the other half received saline injections every 3 months for 2 years. At 1- and 2-year interval follow-ups, no statistically significant difference was seen between the 2 groups in loss of joint space and no progression of degenerative disease, as demonstrated by measurements of joint space widths by standardized fluoroscopically guided radiographs. Although the primary outcome measure of this study was to assess radiologic joint space narrowing with repeated injections, knee pain and stiffness appeared to improve after 2 years, although these results were not well quantified.
A limitation of most studies testing intraarticular therapy has been sample size. Combining studies may allow the ability to detect levels of pain relief not found in individual studies. A recent meta-analysis of 6 randomized controlled trials using intra-articular corticosteroid knee injections found short-term relief of pain for 2 weeks (relative risk [RR]=1.66; 95% confidence interval [CI], 1.37–2.01).7 The number needed to treat (NNT) range for these studies is 1.3 to 3.5. Two additional studies included in this study using higher-dose steroids (prednisone equivalent dose of 37.5 to 80 mg), with or without joint lavage, assessed improvement at 16 to 24 weeks. Although neither individual study showed statistically significant differences, the pooled data from the 2 studies favored symptom improvement at 16 to 24 weeks (RR=2.09; 95% CI, 1.2–3.7; NNT=4.4).7
Recommendations from others
Guidelines for the treatment of knee osteoarthritis were outlined by a task force for the European League Against Rheumatism (EULAR) Standing Committee for Clinical Trials. The task force recommended intra-articular steroid injection for acute exacerbation of knee pain. This task force performed an evidence-based review and concluded at least 1 randomized control trial recommended intraarticular steroid for patients with osteoarthritis. It was noted that intra-articular steroid injections were effective for only short-term pain relief and that there are no predictors of success of treatment, such as the presence or absence of such factors as joint effusion, degree of radio-logic change, age, or obesity.2
The American College of Rheumatology Subcommittee on Osteoarthritis Guidelines developed both nonpharmacological and pharmacological recommendations for the treatment of osteoarthritis of the knee.8 These recommendations include: use of intra-articular steroid injection for patients with acute exacerbations who had evidence for joint inflammation, and joint aspiration accompanying the intra-articular injection for “short-term relief.”
Intra-articular steroids provide extra relief for patients with acute exacerbations
Wail Malaty, MD
Hendersonville Family Practice Residency Program, Hendersonville, NC
This well-constructed review demonstrates that intra-articular steroid injections provide up to 3 weeks of pain relief for patients with osteoarthritis of the knee. While this may not seem like much, in practice it can be quite helpful in some situations. It provides supplemental pain relief for patients with acute exacerbations of their disease. It is also useful as a temporizing measure for patients who are candidates for total knee replacement but are not quite ready for it psychologically.
1. Rozental TD, Sculco TP. Intra-articular corticosteroids: an updated overview. Am J Orthop 2000;29:18-23.
2. Pendleton A, Arden N, Dougados M, et al. EULAR recommendations for the management of knee osteoarthritis: report of a task force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 2000;59:936-944.
3. Hochberg MC, Altman RD, Brandt KD, et al. Guidelines for the medical management of osteoarthritis. Part II. Osteoarthritis of the knee. American College of Rheumatology. Arthritis Rheum 1995;38:1541-1546.
4. Jones A, Doherty M. Intra-articular corticosteroids are effective in osteoarthritis but there are no clinical predictors of response. Ann Rheum Dis 1996;55:829-832.
5. Gaffney K, Ledingham J, Perry JD. Intra-articular triamcinolone hexacetonide in knee osteoarthritis: factors influencing the clinical response. Ann Rheum Dis 1995;54:379-381.
6. Raynauld JP, Buckland-Wright C, Ward R, et al. Safety and efficacy of long-term intraarticular steroid injections in osteoarthritis of the knee: a randomized, double-blind, placebo-controlled trial. Arthritis Rheum 2003;48:370-377.
7. Arroll B, Goodyear-Smith F. Corticosteroid injections for osteoarthritis of the knee: meta-analysis. BMJ 2004;328:869-870.
8. Altman RD, Hochberg HC, Moskowitz RW, Schnitzer TJ. Recommendations for the medical management of osteoarthritis of the hip and knee 2000 update: American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
1. Rozental TD, Sculco TP. Intra-articular corticosteroids: an updated overview. Am J Orthop 2000;29:18-23.
2. Pendleton A, Arden N, Dougados M, et al. EULAR recommendations for the management of knee osteoarthritis: report of a task force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 2000;59:936-944.
3. Hochberg MC, Altman RD, Brandt KD, et al. Guidelines for the medical management of osteoarthritis. Part II. Osteoarthritis of the knee. American College of Rheumatology. Arthritis Rheum 1995;38:1541-1546.
4. Jones A, Doherty M. Intra-articular corticosteroids are effective in osteoarthritis but there are no clinical predictors of response. Ann Rheum Dis 1996;55:829-832.
5. Gaffney K, Ledingham J, Perry JD. Intra-articular triamcinolone hexacetonide in knee osteoarthritis: factors influencing the clinical response. Ann Rheum Dis 1995;54:379-381.
6. Raynauld JP, Buckland-Wright C, Ward R, et al. Safety and efficacy of long-term intraarticular steroid injections in osteoarthritis of the knee: a randomized, double-blind, placebo-controlled trial. Arthritis Rheum 2003;48:370-377.
7. Arroll B, Goodyear-Smith F. Corticosteroid injections for osteoarthritis of the knee: meta-analysis. BMJ 2004;328:869-870.
8. Altman RD, Hochberg HC, Moskowitz RW, Schnitzer TJ. Recommendations for the medical management of osteoarthritis of the hip and knee 2000 update: American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
Evidence-based answers from the Family Physicians Inquiries Network
Do routine eye exams reduce occurrence of blindness from type 2 diabetes?
Screening eye exams for patients with type 2 diabetes can detect retinopathy early enough so treatment can prevent vision loss. Patients without diabetic retinopathy who are systematically screened by mydriatic retinal photography have a 95% probability of remaining free of sight-threatening retinopathy over the next 5 years. If background or preproliferative retinopathy is found at screening (Figure), the 95% probability interval for remaining free of sight-threatening retinopathy is reduced to 12 and 4 months, respectively (strength of recommendation [SOR]: B, based on 1 prospective cohort study).
A reliably sensitive screening exam requires mydriatic retinal photography augmented by ophthalmoscopy when photographs are inconclusive (SOR: A, based on a systematic review). For patients with diabetes not differentiated by type, photocoagu-lation significantly decreases visual deterioration and reduces the chances of blindness (SOR: A, based on randomized controlled trials [RCT]).
FIGURE
Nonproliferative and proliferative diabetic retinopathy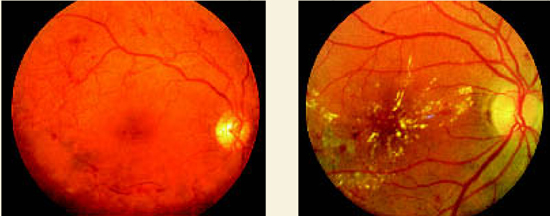
Background (nonproliferative) diabetic retinopathyis characterized by macular retinal exudates, edematous retinal thickening, dot and blot retinal hemorrhages, and retinal capillary microaneurysms.
Proliferative diabetic retinopathy. Note the network of abnormal preretinal new blood vessels just super-otemporal to the macula and the linear accumulations of blood in the preretinal vitreous below the macula.
Evidence summary
The Liverpool Diabetic Eye Study1 prospectively evaluated the risk of vision-threatening retinopathy in a cohort that included all patients with diabetes mellitus who were registered with a general practitioner and were not under the care of an ophthalmologist. A subgroup of 4770 patients with type 2 diabetes who did not have sightthreatening retinopathy at baseline underwent at least 1 additional screen. Screening included non-stereoscopic 3-field (45° or 50° field) mydriatic photography. Median follow-up was 3.5 years (range, 1–8.5 years).
The patients were divided into cohorts based on level of demonstrated retinopathy. The mean screening interval for a 95% probability of remaining free of sight-threatening retinopathy was calculated for each grade of baseline retinopathy. Screening patients with no retinopathy every 5 years provided a 95% probability of remaining free of sight-threatening retinopathy. Patients with background retinopathy must be screened annually to achieve the same result, and patients with mild preproliferative retinopathy need to be screened every 4 months ( Table ).
A systematic review2 of multiple small English-language studies evaluating screening and monitoring of diabetic retinopathy found consistent results. Screening by direct or indirect ophthalmoscopy alone detected 65% of patients with sight-threatening retinopathy. Screening by mydriatic retinal photography, augmented by ophthal-moscopy when the photographs were inconclusive, detected 88% to 100% of such cases.
An RCT of 1700 patients with diabetes and retinopathy evaluated preservation of vision with photocoagulation.3 Patients were not differentiated by type of diabetes. Each patient had initial and follow-up stereoscopic fundus photography. One eye was selected at random to receive treatment and the other remained untreated to serve as a control. Because of the magnitude of difference in vision between the eyes, the study was halted at 2 years to permit photocoagulation of the untreated eyes. Patients whose eyes had new vessels on or near the disk lost vision (defined as visual acuity less than 5/200) more often in untreated eyes (18.3% cumulative rate at 2 years) compared with treated eyes (6.4%; number needed to treat [NNT]=8.4).
Another RCT4 of patients with diabetes showed that photocoagulation maintained vision in diabetic retinopathy if the disease was not too advanced. Ninety-nine patients, also not differentiated by type of diabetes, were each treated in 1 eye chosen at random with a xenon-arc photocoagulator. Patients underwent follow-up treatments to the treated eye by clinical indication. The untreated eyes were observed as controls. Blindness occurred significantly less often in the treated eyes (19% total after 5 to 7 years) than in the control eyes (39%; NNT=5 to prevent 1 blind eye). Patients without proliferative retinopathy at onset experienced the most dramatic slowing of deterioration; photocoagulation was more useful in maintaining than in improving vision.
TABLE
Screening frequency for sight-threatening retinopathy
| Stage of retinal disease | Screening frequency* |
|---|---|
| None | 5 years |
| Background retinopathy | 1 year |
| Mild preproliferative retinopathy | 4 months |
| *For 95% chance of remaining free of sight-threatening retinopathy. | |
Recommendations from others
The American Diabetes Association 2003 Clinical Practice Recommendations5 state that patients with type 2 diabetes should have an initial dilated and comprehensive eye examination by an ophthalmologist or optometrist shortly after diagnosis of diabetes. An ophthalmologist or optometrist who is knowledgeable and experienced in diagnosing diabetic retinopathy and is aware of its management should repeat subsequent examinations for both type 1 and type 2 diabetic patients annually. Examinations are required more frequently if retinopathy is progressing.
Screen for retinal complications early, regularly, by an experienced eye doctor
Tsveti Markova, MD
Department of Family Medicine, Wayne State University, Detroit, Mich
Family physicians play a central role in the diabetes care team. They must not only achieve good blood sugar control, but also monitor for complications and coordinate their treatment. Educating patients and reaching common ground with them is essential for success. Evidence suggests that screening for eye complications reduces blindness. Patients with early retinopathy changes are usually asymptomatic; therefore it takes a committed and educated patient to comply with screening recommendations. Also, many patients have the misconception that a visual acuity exam by an optometrist is sufficient for their diabetes eye screening. Family physicians must convey the importance of screening for retinal complications early, regularly and by an optometrist or ophthalmologist experienced in management of diabetes.
1. Younis N, Broadbent DM, Vora JP, Harding SP. Incidence of sight-threatening retinopathy in patients with type 2 diabetes in the Liverpool Diabetic Eye Study: a cohort study. Lancet 2003;361:195-200.
2. Hutchinson A, McIntosh A, Peters J, et al. Effectiveness of screening and monitoring tests for diabetic retinopa-thy—a systematic review. Diabet Med 2000;17:495-506.
3. The Diabetic Retinopathy Study Research Group. Preliminary report on effects of photocoagulation therapy. Am J Ophthalmol 1976;81:383-396.
4. British Multicentre Study Group. Photocoagulation from diabetic maculopathy: a randomized controlled clinical trial using the xenon arc. Diabetes 1983;32:1010-1016.
5. Fong DS, Aiello L, Gardner TW, et al. American Diabetes Association. Diabetic retinopathy. Diabetes Care 2004;26 Suppl 1:S84-S87.
Screening eye exams for patients with type 2 diabetes can detect retinopathy early enough so treatment can prevent vision loss. Patients without diabetic retinopathy who are systematically screened by mydriatic retinal photography have a 95% probability of remaining free of sight-threatening retinopathy over the next 5 years. If background or preproliferative retinopathy is found at screening (Figure), the 95% probability interval for remaining free of sight-threatening retinopathy is reduced to 12 and 4 months, respectively (strength of recommendation [SOR]: B, based on 1 prospective cohort study).
A reliably sensitive screening exam requires mydriatic retinal photography augmented by ophthalmoscopy when photographs are inconclusive (SOR: A, based on a systematic review). For patients with diabetes not differentiated by type, photocoagu-lation significantly decreases visual deterioration and reduces the chances of blindness (SOR: A, based on randomized controlled trials [RCT]).
FIGURE
Nonproliferative and proliferative diabetic retinopathy
Background (nonproliferative) diabetic retinopathyis characterized by macular retinal exudates, edematous retinal thickening, dot and blot retinal hemorrhages, and retinal capillary microaneurysms.
Proliferative diabetic retinopathy. Note the network of abnormal preretinal new blood vessels just super-otemporal to the macula and the linear accumulations of blood in the preretinal vitreous below the macula.
Evidence summary
The Liverpool Diabetic Eye Study1 prospectively evaluated the risk of vision-threatening retinopathy in a cohort that included all patients with diabetes mellitus who were registered with a general practitioner and were not under the care of an ophthalmologist. A subgroup of 4770 patients with type 2 diabetes who did not have sightthreatening retinopathy at baseline underwent at least 1 additional screen. Screening included non-stereoscopic 3-field (45° or 50° field) mydriatic photography. Median follow-up was 3.5 years (range, 1–8.5 years).
The patients were divided into cohorts based on level of demonstrated retinopathy. The mean screening interval for a 95% probability of remaining free of sight-threatening retinopathy was calculated for each grade of baseline retinopathy. Screening patients with no retinopathy every 5 years provided a 95% probability of remaining free of sight-threatening retinopathy. Patients with background retinopathy must be screened annually to achieve the same result, and patients with mild preproliferative retinopathy need to be screened every 4 months ( Table ).
A systematic review2 of multiple small English-language studies evaluating screening and monitoring of diabetic retinopathy found consistent results. Screening by direct or indirect ophthalmoscopy alone detected 65% of patients with sight-threatening retinopathy. Screening by mydriatic retinal photography, augmented by ophthal-moscopy when the photographs were inconclusive, detected 88% to 100% of such cases.
An RCT of 1700 patients with diabetes and retinopathy evaluated preservation of vision with photocoagulation.3 Patients were not differentiated by type of diabetes. Each patient had initial and follow-up stereoscopic fundus photography. One eye was selected at random to receive treatment and the other remained untreated to serve as a control. Because of the magnitude of difference in vision between the eyes, the study was halted at 2 years to permit photocoagulation of the untreated eyes. Patients whose eyes had new vessels on or near the disk lost vision (defined as visual acuity less than 5/200) more often in untreated eyes (18.3% cumulative rate at 2 years) compared with treated eyes (6.4%; number needed to treat [NNT]=8.4).
Another RCT4 of patients with diabetes showed that photocoagulation maintained vision in diabetic retinopathy if the disease was not too advanced. Ninety-nine patients, also not differentiated by type of diabetes, were each treated in 1 eye chosen at random with a xenon-arc photocoagulator. Patients underwent follow-up treatments to the treated eye by clinical indication. The untreated eyes were observed as controls. Blindness occurred significantly less often in the treated eyes (19% total after 5 to 7 years) than in the control eyes (39%; NNT=5 to prevent 1 blind eye). Patients without proliferative retinopathy at onset experienced the most dramatic slowing of deterioration; photocoagulation was more useful in maintaining than in improving vision.
TABLE
Screening frequency for sight-threatening retinopathy
| Stage of retinal disease | Screening frequency* |
|---|---|
| None | 5 years |
| Background retinopathy | 1 year |
| Mild preproliferative retinopathy | 4 months |
| *For 95% chance of remaining free of sight-threatening retinopathy. | |
Recommendations from others
The American Diabetes Association 2003 Clinical Practice Recommendations5 state that patients with type 2 diabetes should have an initial dilated and comprehensive eye examination by an ophthalmologist or optometrist shortly after diagnosis of diabetes. An ophthalmologist or optometrist who is knowledgeable and experienced in diagnosing diabetic retinopathy and is aware of its management should repeat subsequent examinations for both type 1 and type 2 diabetic patients annually. Examinations are required more frequently if retinopathy is progressing.
Screen for retinal complications early, regularly, by an experienced eye doctor
Tsveti Markova, MD
Department of Family Medicine, Wayne State University, Detroit, Mich
Family physicians play a central role in the diabetes care team. They must not only achieve good blood sugar control, but also monitor for complications and coordinate their treatment. Educating patients and reaching common ground with them is essential for success. Evidence suggests that screening for eye complications reduces blindness. Patients with early retinopathy changes are usually asymptomatic; therefore it takes a committed and educated patient to comply with screening recommendations. Also, many patients have the misconception that a visual acuity exam by an optometrist is sufficient for their diabetes eye screening. Family physicians must convey the importance of screening for retinal complications early, regularly and by an optometrist or ophthalmologist experienced in management of diabetes.
Screening eye exams for patients with type 2 diabetes can detect retinopathy early enough so treatment can prevent vision loss. Patients without diabetic retinopathy who are systematically screened by mydriatic retinal photography have a 95% probability of remaining free of sight-threatening retinopathy over the next 5 years. If background or preproliferative retinopathy is found at screening (Figure), the 95% probability interval for remaining free of sight-threatening retinopathy is reduced to 12 and 4 months, respectively (strength of recommendation [SOR]: B, based on 1 prospective cohort study).
A reliably sensitive screening exam requires mydriatic retinal photography augmented by ophthalmoscopy when photographs are inconclusive (SOR: A, based on a systematic review). For patients with diabetes not differentiated by type, photocoagu-lation significantly decreases visual deterioration and reduces the chances of blindness (SOR: A, based on randomized controlled trials [RCT]).
FIGURE
Nonproliferative and proliferative diabetic retinopathy
Background (nonproliferative) diabetic retinopathyis characterized by macular retinal exudates, edematous retinal thickening, dot and blot retinal hemorrhages, and retinal capillary microaneurysms.
Proliferative diabetic retinopathy. Note the network of abnormal preretinal new blood vessels just super-otemporal to the macula and the linear accumulations of blood in the preretinal vitreous below the macula.
Evidence summary
The Liverpool Diabetic Eye Study1 prospectively evaluated the risk of vision-threatening retinopathy in a cohort that included all patients with diabetes mellitus who were registered with a general practitioner and were not under the care of an ophthalmologist. A subgroup of 4770 patients with type 2 diabetes who did not have sightthreatening retinopathy at baseline underwent at least 1 additional screen. Screening included non-stereoscopic 3-field (45° or 50° field) mydriatic photography. Median follow-up was 3.5 years (range, 1–8.5 years).
The patients were divided into cohorts based on level of demonstrated retinopathy. The mean screening interval for a 95% probability of remaining free of sight-threatening retinopathy was calculated for each grade of baseline retinopathy. Screening patients with no retinopathy every 5 years provided a 95% probability of remaining free of sight-threatening retinopathy. Patients with background retinopathy must be screened annually to achieve the same result, and patients with mild preproliferative retinopathy need to be screened every 4 months ( Table ).
A systematic review2 of multiple small English-language studies evaluating screening and monitoring of diabetic retinopathy found consistent results. Screening by direct or indirect ophthalmoscopy alone detected 65% of patients with sight-threatening retinopathy. Screening by mydriatic retinal photography, augmented by ophthal-moscopy when the photographs were inconclusive, detected 88% to 100% of such cases.
An RCT of 1700 patients with diabetes and retinopathy evaluated preservation of vision with photocoagulation.3 Patients were not differentiated by type of diabetes. Each patient had initial and follow-up stereoscopic fundus photography. One eye was selected at random to receive treatment and the other remained untreated to serve as a control. Because of the magnitude of difference in vision between the eyes, the study was halted at 2 years to permit photocoagulation of the untreated eyes. Patients whose eyes had new vessels on or near the disk lost vision (defined as visual acuity less than 5/200) more often in untreated eyes (18.3% cumulative rate at 2 years) compared with treated eyes (6.4%; number needed to treat [NNT]=8.4).
Another RCT4 of patients with diabetes showed that photocoagulation maintained vision in diabetic retinopathy if the disease was not too advanced. Ninety-nine patients, also not differentiated by type of diabetes, were each treated in 1 eye chosen at random with a xenon-arc photocoagulator. Patients underwent follow-up treatments to the treated eye by clinical indication. The untreated eyes were observed as controls. Blindness occurred significantly less often in the treated eyes (19% total after 5 to 7 years) than in the control eyes (39%; NNT=5 to prevent 1 blind eye). Patients without proliferative retinopathy at onset experienced the most dramatic slowing of deterioration; photocoagulation was more useful in maintaining than in improving vision.
TABLE
Screening frequency for sight-threatening retinopathy
| Stage of retinal disease | Screening frequency* |
|---|---|
| None | 5 years |
| Background retinopathy | 1 year |
| Mild preproliferative retinopathy | 4 months |
| *For 95% chance of remaining free of sight-threatening retinopathy. | |
Recommendations from others
The American Diabetes Association 2003 Clinical Practice Recommendations5 state that patients with type 2 diabetes should have an initial dilated and comprehensive eye examination by an ophthalmologist or optometrist shortly after diagnosis of diabetes. An ophthalmologist or optometrist who is knowledgeable and experienced in diagnosing diabetic retinopathy and is aware of its management should repeat subsequent examinations for both type 1 and type 2 diabetic patients annually. Examinations are required more frequently if retinopathy is progressing.
Screen for retinal complications early, regularly, by an experienced eye doctor
Tsveti Markova, MD
Department of Family Medicine, Wayne State University, Detroit, Mich
Family physicians play a central role in the diabetes care team. They must not only achieve good blood sugar control, but also monitor for complications and coordinate their treatment. Educating patients and reaching common ground with them is essential for success. Evidence suggests that screening for eye complications reduces blindness. Patients with early retinopathy changes are usually asymptomatic; therefore it takes a committed and educated patient to comply with screening recommendations. Also, many patients have the misconception that a visual acuity exam by an optometrist is sufficient for their diabetes eye screening. Family physicians must convey the importance of screening for retinal complications early, regularly and by an optometrist or ophthalmologist experienced in management of diabetes.
1. Younis N, Broadbent DM, Vora JP, Harding SP. Incidence of sight-threatening retinopathy in patients with type 2 diabetes in the Liverpool Diabetic Eye Study: a cohort study. Lancet 2003;361:195-200.
2. Hutchinson A, McIntosh A, Peters J, et al. Effectiveness of screening and monitoring tests for diabetic retinopa-thy—a systematic review. Diabet Med 2000;17:495-506.
3. The Diabetic Retinopathy Study Research Group. Preliminary report on effects of photocoagulation therapy. Am J Ophthalmol 1976;81:383-396.
4. British Multicentre Study Group. Photocoagulation from diabetic maculopathy: a randomized controlled clinical trial using the xenon arc. Diabetes 1983;32:1010-1016.
5. Fong DS, Aiello L, Gardner TW, et al. American Diabetes Association. Diabetic retinopathy. Diabetes Care 2004;26 Suppl 1:S84-S87.
1. Younis N, Broadbent DM, Vora JP, Harding SP. Incidence of sight-threatening retinopathy in patients with type 2 diabetes in the Liverpool Diabetic Eye Study: a cohort study. Lancet 2003;361:195-200.
2. Hutchinson A, McIntosh A, Peters J, et al. Effectiveness of screening and monitoring tests for diabetic retinopa-thy—a systematic review. Diabet Med 2000;17:495-506.
3. The Diabetic Retinopathy Study Research Group. Preliminary report on effects of photocoagulation therapy. Am J Ophthalmol 1976;81:383-396.
4. British Multicentre Study Group. Photocoagulation from diabetic maculopathy: a randomized controlled clinical trial using the xenon arc. Diabetes 1983;32:1010-1016.
5. Fong DS, Aiello L, Gardner TW, et al. American Diabetes Association. Diabetic retinopathy. Diabetes Care 2004;26 Suppl 1:S84-S87.
Evidence-based answers from the Family Physicians Inquiries Network
Does yoga speed healing for patients with low back pain?
The use of yoga is consistent with recommendations for activity, as tolerated, for patients with low back pain. Literature evaluating the effectiveness of yoga for low back pain is scant, so it is unclear if yoga is equivalent to, or superior to, standard therapies (strength of recommendation: C, based on 1 randomized pilot study and limited case series).
Evidence summary
Yoga, through static physical postures (or asanas), uses stretching to improve muscular strength and flexibility, which could be beneficial for low-back-related pain management.1 Hatha yoga, which incorporates breathing and movement, has provided limited benefit in musculoskeletal-related pain.2 Hatha yoga is distinguished from other yoga practices in that it is based on the knowledge, development, and balance of psychophysical energies. A large systematic review of yoga used for various medical conditions found over 120 studies.3 Anecdotal reports were excluded. The authors reported no studies directly evaluating effect of yoga on back pain.
A randomized controlled trial studied a 6-week modified hatha yoga protocol with 22 patients.4 The yoga group spent an hour with a certified instructor twice weekly, while the control group received the same intervention delayed until the study phase was completed. This underpowered pilot study found trends in functional measurement scores for improved balance and flexibility, as well as decreased disability and depression in the yoga group, but the sample size was too small to detect significant changes.
Patients who practice hatha yoga say it is valuable for preventing and managing stress-related chronic health problems, including low back pain. In a survey of 3000 people receiving yoga for health ailments (1142 [38%] with back pain), 98% claimed that yoga benefited them.5
In a case series of 16 patients using various asanas for rehabilitation, 11 (69%) reported significant improvement, with near normal mobility and absence of pain.6 Those who reported recurring back pain also reported irregular practice of yoga. In another case series, 21 women aged ≥60 years (mean age, 75) with hyperkyphosis, participated in twice-weekly 1-hour sessions of hatha yoga for 12 weeks. Measured height increased by a mean of 0.52 cm, forward curvature diminished, patients were able to get out of chairs faster, and they had longer functional reach. Eleven patients (48%) reported increased postural awareness/improvement and improved well-being; 58% perceived improvement in their physical functioning.7
Clearly, more studies are required to determine the effects of yoga on lower back pain. Larger randomized sample sizes, group and individualized formats, and longer follow-up are needed. Control groups should involve both group and nongroup settings, to detect any benefit that may be derived from group support. No reports of harm from yoga in low-back pain therapy were reported in the few studies found.
Recommendations from others
The Philadelphia Panel formulated evidence-based guidelines for selected rehabilitation interventions in the management of low back pain for outpatient adults.8 Continuation of normal activity improves rate of return to work compared with enforced bed rest. Randomized controlled trials demonstrate no clinically important effect (15% improvement compared with control) with stretching or strengthening exercises, mechanical traction, or TENS. The panel found insufficient evidence to support the use of mechanical traction for patient global improvement and return to work. Therapeutic exercise—including stretching, strengthening, and mobility exercises—significantly reduces pain and improves function for chronic low back pain (longer than 12 weeks); but there was no clinical benefit in facilitating return to work. No specific comments on yoga appeared in their recommendations.
The US Preventive Services Task Force reports that evidence is insufficient to recommend for or against counseling patients to exercise to prevent low back pain; it makes no mention about yoga.9
Information suggests yoga—and all exercise—effective for low back pain
John Hill, MD
Rose Family Medicine Residency, Denver, Colo
Good evidence supports the concept that activity is more effective than bed rest for acute low back pain. Recent studies in the rehabilitation and physical therapy literature have emphasized core stability exercises for acute and chronic back pain. As balance, strength, and flexibility improve, the episodes and intensity of acute low back pain diminish.
It stands to reason that activities such as hatha yoga that improve muscular strength, flexibility, and balance would similarly improve function and decrease low back pain. The available information would lead me to recommend yoga for my patients with low back pain. Yoga may well be effective, and no reports in the literature show harm.
1. Luskin FM, Newell KA, Griffith M, et al. A review of mind/body therapies in the treatment of musculoskeletal disorders with implications for the elderly. Altern Ther Health Med 2000;6:46-56.
2. Hudson S. Yoga aids in back pain. Aust Nurs J 1998;5(9):27.-
3. Raub JA. Psychophysiologic effects of Hatha Yoga on musculoskeletal and cardiopulmonary function: a literature review. J Altern Complement Med 2002;8:797-812.
4. Galantino ML, Bzdewka TM, Eissler-Russo J, et al. The impact of modified Hatha yoga on chronic low back pain: a pilot study. Altern Ther Health Med. 2004;10:56-58.
5. Burton Goldberg Group. Alternative Medicine: The Definitive Guide. Puyallup, Wash: Future Medicine Publications; 1993.
6. Ananthanarayanan TV, Srinivasan TM. Asana-based exercises for the management of low-back pain. J Int Assoc Yoga Therapists 1994;4:6-15.
7. Greendale GA, McDivit A, Carpenter A, Seeger L, Huang MH. Yoga for women with hyperkyphosis: results of a pilot study. Am J Public Health, 2002;92:1611-1614.
8. Philadelphia Panel. Philadelphia Panel evidence-based clinical practice guidelines on selected rehabilitation interventions for low back pain. Phys Ther 2001;81:1641-1674.
9. US Preventive Services Task Force. Primary care interventions to prevent low back pain. Rockville, Md: US Preventive Services Tack Force; 2004. Available at: www.ahrq.gov/clinic/uspstf/uspsback.htm. Accessed on July 8, 2004.
The use of yoga is consistent with recommendations for activity, as tolerated, for patients with low back pain. Literature evaluating the effectiveness of yoga for low back pain is scant, so it is unclear if yoga is equivalent to, or superior to, standard therapies (strength of recommendation: C, based on 1 randomized pilot study and limited case series).
Evidence summary
Yoga, through static physical postures (or asanas), uses stretching to improve muscular strength and flexibility, which could be beneficial for low-back-related pain management.1 Hatha yoga, which incorporates breathing and movement, has provided limited benefit in musculoskeletal-related pain.2 Hatha yoga is distinguished from other yoga practices in that it is based on the knowledge, development, and balance of psychophysical energies. A large systematic review of yoga used for various medical conditions found over 120 studies.3 Anecdotal reports were excluded. The authors reported no studies directly evaluating effect of yoga on back pain.
A randomized controlled trial studied a 6-week modified hatha yoga protocol with 22 patients.4 The yoga group spent an hour with a certified instructor twice weekly, while the control group received the same intervention delayed until the study phase was completed. This underpowered pilot study found trends in functional measurement scores for improved balance and flexibility, as well as decreased disability and depression in the yoga group, but the sample size was too small to detect significant changes.
Patients who practice hatha yoga say it is valuable for preventing and managing stress-related chronic health problems, including low back pain. In a survey of 3000 people receiving yoga for health ailments (1142 [38%] with back pain), 98% claimed that yoga benefited them.5
In a case series of 16 patients using various asanas for rehabilitation, 11 (69%) reported significant improvement, with near normal mobility and absence of pain.6 Those who reported recurring back pain also reported irregular practice of yoga. In another case series, 21 women aged ≥60 years (mean age, 75) with hyperkyphosis, participated in twice-weekly 1-hour sessions of hatha yoga for 12 weeks. Measured height increased by a mean of 0.52 cm, forward curvature diminished, patients were able to get out of chairs faster, and they had longer functional reach. Eleven patients (48%) reported increased postural awareness/improvement and improved well-being; 58% perceived improvement in their physical functioning.7
Clearly, more studies are required to determine the effects of yoga on lower back pain. Larger randomized sample sizes, group and individualized formats, and longer follow-up are needed. Control groups should involve both group and nongroup settings, to detect any benefit that may be derived from group support. No reports of harm from yoga in low-back pain therapy were reported in the few studies found.
Recommendations from others
The Philadelphia Panel formulated evidence-based guidelines for selected rehabilitation interventions in the management of low back pain for outpatient adults.8 Continuation of normal activity improves rate of return to work compared with enforced bed rest. Randomized controlled trials demonstrate no clinically important effect (15% improvement compared with control) with stretching or strengthening exercises, mechanical traction, or TENS. The panel found insufficient evidence to support the use of mechanical traction for patient global improvement and return to work. Therapeutic exercise—including stretching, strengthening, and mobility exercises—significantly reduces pain and improves function for chronic low back pain (longer than 12 weeks); but there was no clinical benefit in facilitating return to work. No specific comments on yoga appeared in their recommendations.
The US Preventive Services Task Force reports that evidence is insufficient to recommend for or against counseling patients to exercise to prevent low back pain; it makes no mention about yoga.9
Information suggests yoga—and all exercise—effective for low back pain
John Hill, MD
Rose Family Medicine Residency, Denver, Colo
Good evidence supports the concept that activity is more effective than bed rest for acute low back pain. Recent studies in the rehabilitation and physical therapy literature have emphasized core stability exercises for acute and chronic back pain. As balance, strength, and flexibility improve, the episodes and intensity of acute low back pain diminish.
It stands to reason that activities such as hatha yoga that improve muscular strength, flexibility, and balance would similarly improve function and decrease low back pain. The available information would lead me to recommend yoga for my patients with low back pain. Yoga may well be effective, and no reports in the literature show harm.
The use of yoga is consistent with recommendations for activity, as tolerated, for patients with low back pain. Literature evaluating the effectiveness of yoga for low back pain is scant, so it is unclear if yoga is equivalent to, or superior to, standard therapies (strength of recommendation: C, based on 1 randomized pilot study and limited case series).
Evidence summary
Yoga, through static physical postures (or asanas), uses stretching to improve muscular strength and flexibility, which could be beneficial for low-back-related pain management.1 Hatha yoga, which incorporates breathing and movement, has provided limited benefit in musculoskeletal-related pain.2 Hatha yoga is distinguished from other yoga practices in that it is based on the knowledge, development, and balance of psychophysical energies. A large systematic review of yoga used for various medical conditions found over 120 studies.3 Anecdotal reports were excluded. The authors reported no studies directly evaluating effect of yoga on back pain.
A randomized controlled trial studied a 6-week modified hatha yoga protocol with 22 patients.4 The yoga group spent an hour with a certified instructor twice weekly, while the control group received the same intervention delayed until the study phase was completed. This underpowered pilot study found trends in functional measurement scores for improved balance and flexibility, as well as decreased disability and depression in the yoga group, but the sample size was too small to detect significant changes.
Patients who practice hatha yoga say it is valuable for preventing and managing stress-related chronic health problems, including low back pain. In a survey of 3000 people receiving yoga for health ailments (1142 [38%] with back pain), 98% claimed that yoga benefited them.5
In a case series of 16 patients using various asanas for rehabilitation, 11 (69%) reported significant improvement, with near normal mobility and absence of pain.6 Those who reported recurring back pain also reported irregular practice of yoga. In another case series, 21 women aged ≥60 years (mean age, 75) with hyperkyphosis, participated in twice-weekly 1-hour sessions of hatha yoga for 12 weeks. Measured height increased by a mean of 0.52 cm, forward curvature diminished, patients were able to get out of chairs faster, and they had longer functional reach. Eleven patients (48%) reported increased postural awareness/improvement and improved well-being; 58% perceived improvement in their physical functioning.7
Clearly, more studies are required to determine the effects of yoga on lower back pain. Larger randomized sample sizes, group and individualized formats, and longer follow-up are needed. Control groups should involve both group and nongroup settings, to detect any benefit that may be derived from group support. No reports of harm from yoga in low-back pain therapy were reported in the few studies found.
Recommendations from others
The Philadelphia Panel formulated evidence-based guidelines for selected rehabilitation interventions in the management of low back pain for outpatient adults.8 Continuation of normal activity improves rate of return to work compared with enforced bed rest. Randomized controlled trials demonstrate no clinically important effect (15% improvement compared with control) with stretching or strengthening exercises, mechanical traction, or TENS. The panel found insufficient evidence to support the use of mechanical traction for patient global improvement and return to work. Therapeutic exercise—including stretching, strengthening, and mobility exercises—significantly reduces pain and improves function for chronic low back pain (longer than 12 weeks); but there was no clinical benefit in facilitating return to work. No specific comments on yoga appeared in their recommendations.
The US Preventive Services Task Force reports that evidence is insufficient to recommend for or against counseling patients to exercise to prevent low back pain; it makes no mention about yoga.9
Information suggests yoga—and all exercise—effective for low back pain
John Hill, MD
Rose Family Medicine Residency, Denver, Colo
Good evidence supports the concept that activity is more effective than bed rest for acute low back pain. Recent studies in the rehabilitation and physical therapy literature have emphasized core stability exercises for acute and chronic back pain. As balance, strength, and flexibility improve, the episodes and intensity of acute low back pain diminish.
It stands to reason that activities such as hatha yoga that improve muscular strength, flexibility, and balance would similarly improve function and decrease low back pain. The available information would lead me to recommend yoga for my patients with low back pain. Yoga may well be effective, and no reports in the literature show harm.
1. Luskin FM, Newell KA, Griffith M, et al. A review of mind/body therapies in the treatment of musculoskeletal disorders with implications for the elderly. Altern Ther Health Med 2000;6:46-56.
2. Hudson S. Yoga aids in back pain. Aust Nurs J 1998;5(9):27.-
3. Raub JA. Psychophysiologic effects of Hatha Yoga on musculoskeletal and cardiopulmonary function: a literature review. J Altern Complement Med 2002;8:797-812.
4. Galantino ML, Bzdewka TM, Eissler-Russo J, et al. The impact of modified Hatha yoga on chronic low back pain: a pilot study. Altern Ther Health Med. 2004;10:56-58.
5. Burton Goldberg Group. Alternative Medicine: The Definitive Guide. Puyallup, Wash: Future Medicine Publications; 1993.
6. Ananthanarayanan TV, Srinivasan TM. Asana-based exercises for the management of low-back pain. J Int Assoc Yoga Therapists 1994;4:6-15.
7. Greendale GA, McDivit A, Carpenter A, Seeger L, Huang MH. Yoga for women with hyperkyphosis: results of a pilot study. Am J Public Health, 2002;92:1611-1614.
8. Philadelphia Panel. Philadelphia Panel evidence-based clinical practice guidelines on selected rehabilitation interventions for low back pain. Phys Ther 2001;81:1641-1674.
9. US Preventive Services Task Force. Primary care interventions to prevent low back pain. Rockville, Md: US Preventive Services Tack Force; 2004. Available at: www.ahrq.gov/clinic/uspstf/uspsback.htm. Accessed on July 8, 2004.
1. Luskin FM, Newell KA, Griffith M, et al. A review of mind/body therapies in the treatment of musculoskeletal disorders with implications for the elderly. Altern Ther Health Med 2000;6:46-56.
2. Hudson S. Yoga aids in back pain. Aust Nurs J 1998;5(9):27.-
3. Raub JA. Psychophysiologic effects of Hatha Yoga on musculoskeletal and cardiopulmonary function: a literature review. J Altern Complement Med 2002;8:797-812.
4. Galantino ML, Bzdewka TM, Eissler-Russo J, et al. The impact of modified Hatha yoga on chronic low back pain: a pilot study. Altern Ther Health Med. 2004;10:56-58.
5. Burton Goldberg Group. Alternative Medicine: The Definitive Guide. Puyallup, Wash: Future Medicine Publications; 1993.
6. Ananthanarayanan TV, Srinivasan TM. Asana-based exercises for the management of low-back pain. J Int Assoc Yoga Therapists 1994;4:6-15.
7. Greendale GA, McDivit A, Carpenter A, Seeger L, Huang MH. Yoga for women with hyperkyphosis: results of a pilot study. Am J Public Health, 2002;92:1611-1614.
8. Philadelphia Panel. Philadelphia Panel evidence-based clinical practice guidelines on selected rehabilitation interventions for low back pain. Phys Ther 2001;81:1641-1674.
9. US Preventive Services Task Force. Primary care interventions to prevent low back pain. Rockville, Md: US Preventive Services Tack Force; 2004. Available at: www.ahrq.gov/clinic/uspstf/uspsback.htm. Accessed on July 8, 2004.
Evidence-based answers from the Family Physicians Inquiries Network
Are beta-2-agonists or anticholinergics more effective for treating COPD?
Both β2-agonists and anticholinergics appear to improve symptoms for patients with chronic obstructive pulmonary disease (COPD). Recent research indicates that adding a long-acting anti-cholinergic to a β2-agonist may improve quality of life for patients with stable COPD more than the use of β2-agonists alone.
Both drug classes increase exercise capacity and alleviate symptoms of COPD, although neither alters disease progression (strength of recommendation [SOR]: A). Combination therapy can lead to greater improvements in forced expiratory volume in 1 second (FEV1) than either drug alone (SOR: A). However, until recently there were no convincing direct head-to-head comparisons of the 2 classes, and it is unclear whether this difference is clinically significant.
Evidence summary
A review of 33 double-blind randomized placebo-controlled studies showed a significant effect of bronchodilator therapy on exercise capacity in COPD patients in about one half of studies. Anticholinergic agents had significant beneficial effects in the majority, and these effects tended to be somewhat dose-dependent. Short-acting β2-agonists improved exercise capacity in more than two thirds of the studies, but long-acting agents led to mixed outcomes. The researchers identified no superior agent between the 2 classes, citing a lack of adequate studies making a direct comparison.1
A recent Cochrane Review comparing the short-term effects of ipratropium to β2-agonists in changes in FEV1and arterial oxygen pressure (PaO2) concluded there was no evidence that the degree of bronchodilation from ipratropium was greater than that from short-acting β2-agonists.2Subjective endpoints such as dyspnea and quality of life were not assessed, and neither of the above reviews included studies focusing on long-term outcomes.
A 12-week double-blind, double-placebo-controlled parallel group study published in 2000 followed 144 patients (age 64 ± 7 years with a FEV1of 44 ±11% predicted) randomized to receive salmeterol 50 μg twice daily alone, salmeterol 50 μg twice daily plus ipratropium 40 μg 4 times daily, or placebo. Patients were assessed for changes in FEV1, daytime symptom scores, specific airway conductance, and the need for rescue medication. The study demonstrated a significant benefit from the addition of ipratropium to salmeterol in terms of reduction of airway obstruction, but not in symptom control or need for rescue medication.3 However, no patients were randomized to receive ipratropium alone, so comparison of the relative contribution of the 2 classes is limited.
A 6-month, randomized double-blind placebo-controlled study evaluating the efficacy of salmeterol 50 μg twice daily vs tiotropium (a new long-acting inhaled anticholinergic) 18 μg once daily was published in 2002. Endpoints in 623 patients were assessed using 12-hour spirometric performance, transition dyspnea index (TDI), and the St. George Respiratory Questionnaire (SGRQ). (SGRQ is a validated disease-specific instrument designed to measure impact on overall health, daily life, and perceived well-being. It measures activity limitations, symptoms, and psychosocial impact.) Tiotropium showed superiority over salmeterol in all endpoints assessed (0.14 L increase in morning FEV1vs 0.09 L, 1.02 U improvement in TDI score vs 0.24, and –5.14 U improvement of SGRQ total score from baseline vs –3.54). However, it should be noted that a difference of 1 on the TDI score was necessary to suggest a clinical benefit. While the overall difference in SGQR between tiotropium and salmeterol did not reach statistical significance, the proportion of patients in the tiotropium group that reached the clinically significant threshold of 4 units improvement in SGRQ score was significantly higher than in the salmeterol group (51% vs 40%; P<.05).4
In a similar study in 2003, 1207 patients were randomized to receive the above doses of salmeterol, tiotropium, or placebo. Over the course of 6 months, tiotropium was associated with a significant delay in onset of the first exacerbation compared with placebo, and overall it led to the fewest exacerbations per patient-year. Fewer hospital admissions were also demonstrated in the tiotropium group per patient-year, and the number of days that patients were unable to perform usual activities was lowest for the tiotropium group. Again, improvement in TDI and SGRQ scores was significantly greater with tiotropium than placebo. In almost all outcomes, the salmeterol results were intermediate between those of tiotropium and placebo, and were not statistically different from placebo.5
Recommendations from others
The GOLD (Global Strategy for the Diagnosis, Management, and Prevention of COPD) Report states that the choice between β2-agonist, anti-cholinergics, or combination therapy depends on the availability and the response of a given patient in terms of symptom relief and side effects. The 2003 GOLD Workshop Report update further recommends the use of regular treatment with long-acting bronchodilators, including tiotropium, rather than short-acting bronchodilators for moderate-to-severe COPD.6
A separate report for the Joint Expert Panel on Chronic Obstructive Pulmonary Disease of the American College of Chest Physicians and the American College of Physicians—American Society of Internal Medicine states that both are beneficial for management of acute exacerbations, but that anticholinergics should be considered first because they are associated with fewer and more benign side effects.7
Patient response and tolerance of side effects determine which drug class to use
Grant Hoekzema, MD
Mercy Family Medicine Residency, St. Louis, Mo
Although recent national guidelines for the management of COPD, such as the GOLD report, give more cohesiveness to treatment strategies for patients with COPD, there is still room for tailoring a treatment approach. I find that when choosing between beta-agonists and anticholinergics, patient response and tolerability of side effects determine what I use.
This Clinical Inquiry supports my clinical impression that neither class of drug is significantly superior to the other in regards to COPD outcome measures. In my experience, when neither drug offers a clear advantage, factors affecting compliance and tolerability tend to determine how effective it is for my patients. Therefore, a trial of either class seems reasonable at first and follow-up determines what is used in the long run.
1. Liesker JJ, Wijkstra PJ, Ten Hacken NH, Koeter GH, Postma DS, Kerstjens HA. A systematic review of the effects of bronchodilators on exercise capacity in patients with COPD. Chest 2002;121:597-608.
2. McCrory DC, Brown CD. Anti-cholinergic bronchodilators versus beta2-sympathomimetic agents for acute exacerbations of chronic obstructive pulmonary disease. In: The Cochrane Library, Issue 1,2004. Chichester, UK: John Wiley, Ltd; 2003.
3. van Noord JA, de Munck DR, Bantje TA, Hop WC, Akveld ML, Bommer AM. Long-term treatment of chronic obstructive pulmonary disease with salmeterol and the additive effect of ipratropium. Eur Respir J 2000;15:878-885.
4. Donohue JF, van Noord JA, Bateman ED, et al. A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol. Chest 2002;122:47-55.
5. Brusasco V, Hodder R, Miravitlles M, Korducki L, Towse L, Kesten S. Health outcomes following treatment for six months with once daily tiotropium compared with twice daily salmeterol in patients with COPD. Thorax 2003;58:399-404.
6. Fabbri LM, Hurd SS. GOLD Scientific Committee. Global Strategy for the Diagnosis, Management, and Prevention of COPD: 2003 update. Eur Respir J 2003;22:1-2.
7. Snow V, Lascher S, Mottur-Pilson C. Joint Expert Panel on Chronic Obstructive Pulmonary Disease of the American College of Chest Physicians and the American College of Physicians-American Society of Internal Medicine. Evidence base for management of acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med 2001;134:595-599.
Both β2-agonists and anticholinergics appear to improve symptoms for patients with chronic obstructive pulmonary disease (COPD). Recent research indicates that adding a long-acting anti-cholinergic to a β2-agonist may improve quality of life for patients with stable COPD more than the use of β2-agonists alone.
Both drug classes increase exercise capacity and alleviate symptoms of COPD, although neither alters disease progression (strength of recommendation [SOR]: A). Combination therapy can lead to greater improvements in forced expiratory volume in 1 second (FEV1) than either drug alone (SOR: A). However, until recently there were no convincing direct head-to-head comparisons of the 2 classes, and it is unclear whether this difference is clinically significant.
Evidence summary
A review of 33 double-blind randomized placebo-controlled studies showed a significant effect of bronchodilator therapy on exercise capacity in COPD patients in about one half of studies. Anticholinergic agents had significant beneficial effects in the majority, and these effects tended to be somewhat dose-dependent. Short-acting β2-agonists improved exercise capacity in more than two thirds of the studies, but long-acting agents led to mixed outcomes. The researchers identified no superior agent between the 2 classes, citing a lack of adequate studies making a direct comparison.1
A recent Cochrane Review comparing the short-term effects of ipratropium to β2-agonists in changes in FEV1and arterial oxygen pressure (PaO2) concluded there was no evidence that the degree of bronchodilation from ipratropium was greater than that from short-acting β2-agonists.2Subjective endpoints such as dyspnea and quality of life were not assessed, and neither of the above reviews included studies focusing on long-term outcomes.
A 12-week double-blind, double-placebo-controlled parallel group study published in 2000 followed 144 patients (age 64 ± 7 years with a FEV1of 44 ±11% predicted) randomized to receive salmeterol 50 μg twice daily alone, salmeterol 50 μg twice daily plus ipratropium 40 μg 4 times daily, or placebo. Patients were assessed for changes in FEV1, daytime symptom scores, specific airway conductance, and the need for rescue medication. The study demonstrated a significant benefit from the addition of ipratropium to salmeterol in terms of reduction of airway obstruction, but not in symptom control or need for rescue medication.3 However, no patients were randomized to receive ipratropium alone, so comparison of the relative contribution of the 2 classes is limited.
A 6-month, randomized double-blind placebo-controlled study evaluating the efficacy of salmeterol 50 μg twice daily vs tiotropium (a new long-acting inhaled anticholinergic) 18 μg once daily was published in 2002. Endpoints in 623 patients were assessed using 12-hour spirometric performance, transition dyspnea index (TDI), and the St. George Respiratory Questionnaire (SGRQ). (SGRQ is a validated disease-specific instrument designed to measure impact on overall health, daily life, and perceived well-being. It measures activity limitations, symptoms, and psychosocial impact.) Tiotropium showed superiority over salmeterol in all endpoints assessed (0.14 L increase in morning FEV1vs 0.09 L, 1.02 U improvement in TDI score vs 0.24, and –5.14 U improvement of SGRQ total score from baseline vs –3.54). However, it should be noted that a difference of 1 on the TDI score was necessary to suggest a clinical benefit. While the overall difference in SGQR between tiotropium and salmeterol did not reach statistical significance, the proportion of patients in the tiotropium group that reached the clinically significant threshold of 4 units improvement in SGRQ score was significantly higher than in the salmeterol group (51% vs 40%; P<.05).4
In a similar study in 2003, 1207 patients were randomized to receive the above doses of salmeterol, tiotropium, or placebo. Over the course of 6 months, tiotropium was associated with a significant delay in onset of the first exacerbation compared with placebo, and overall it led to the fewest exacerbations per patient-year. Fewer hospital admissions were also demonstrated in the tiotropium group per patient-year, and the number of days that patients were unable to perform usual activities was lowest for the tiotropium group. Again, improvement in TDI and SGRQ scores was significantly greater with tiotropium than placebo. In almost all outcomes, the salmeterol results were intermediate between those of tiotropium and placebo, and were not statistically different from placebo.5
Recommendations from others
The GOLD (Global Strategy for the Diagnosis, Management, and Prevention of COPD) Report states that the choice between β2-agonist, anti-cholinergics, or combination therapy depends on the availability and the response of a given patient in terms of symptom relief and side effects. The 2003 GOLD Workshop Report update further recommends the use of regular treatment with long-acting bronchodilators, including tiotropium, rather than short-acting bronchodilators for moderate-to-severe COPD.6
A separate report for the Joint Expert Panel on Chronic Obstructive Pulmonary Disease of the American College of Chest Physicians and the American College of Physicians—American Society of Internal Medicine states that both are beneficial for management of acute exacerbations, but that anticholinergics should be considered first because they are associated with fewer and more benign side effects.7
Patient response and tolerance of side effects determine which drug class to use
Grant Hoekzema, MD
Mercy Family Medicine Residency, St. Louis, Mo
Although recent national guidelines for the management of COPD, such as the GOLD report, give more cohesiveness to treatment strategies for patients with COPD, there is still room for tailoring a treatment approach. I find that when choosing between beta-agonists and anticholinergics, patient response and tolerability of side effects determine what I use.
This Clinical Inquiry supports my clinical impression that neither class of drug is significantly superior to the other in regards to COPD outcome measures. In my experience, when neither drug offers a clear advantage, factors affecting compliance and tolerability tend to determine how effective it is for my patients. Therefore, a trial of either class seems reasonable at first and follow-up determines what is used in the long run.
Both β2-agonists and anticholinergics appear to improve symptoms for patients with chronic obstructive pulmonary disease (COPD). Recent research indicates that adding a long-acting anti-cholinergic to a β2-agonist may improve quality of life for patients with stable COPD more than the use of β2-agonists alone.
Both drug classes increase exercise capacity and alleviate symptoms of COPD, although neither alters disease progression (strength of recommendation [SOR]: A). Combination therapy can lead to greater improvements in forced expiratory volume in 1 second (FEV1) than either drug alone (SOR: A). However, until recently there were no convincing direct head-to-head comparisons of the 2 classes, and it is unclear whether this difference is clinically significant.
Evidence summary
A review of 33 double-blind randomized placebo-controlled studies showed a significant effect of bronchodilator therapy on exercise capacity in COPD patients in about one half of studies. Anticholinergic agents had significant beneficial effects in the majority, and these effects tended to be somewhat dose-dependent. Short-acting β2-agonists improved exercise capacity in more than two thirds of the studies, but long-acting agents led to mixed outcomes. The researchers identified no superior agent between the 2 classes, citing a lack of adequate studies making a direct comparison.1
A recent Cochrane Review comparing the short-term effects of ipratropium to β2-agonists in changes in FEV1and arterial oxygen pressure (PaO2) concluded there was no evidence that the degree of bronchodilation from ipratropium was greater than that from short-acting β2-agonists.2Subjective endpoints such as dyspnea and quality of life were not assessed, and neither of the above reviews included studies focusing on long-term outcomes.
A 12-week double-blind, double-placebo-controlled parallel group study published in 2000 followed 144 patients (age 64 ± 7 years with a FEV1of 44 ±11% predicted) randomized to receive salmeterol 50 μg twice daily alone, salmeterol 50 μg twice daily plus ipratropium 40 μg 4 times daily, or placebo. Patients were assessed for changes in FEV1, daytime symptom scores, specific airway conductance, and the need for rescue medication. The study demonstrated a significant benefit from the addition of ipratropium to salmeterol in terms of reduction of airway obstruction, but not in symptom control or need for rescue medication.3 However, no patients were randomized to receive ipratropium alone, so comparison of the relative contribution of the 2 classes is limited.
A 6-month, randomized double-blind placebo-controlled study evaluating the efficacy of salmeterol 50 μg twice daily vs tiotropium (a new long-acting inhaled anticholinergic) 18 μg once daily was published in 2002. Endpoints in 623 patients were assessed using 12-hour spirometric performance, transition dyspnea index (TDI), and the St. George Respiratory Questionnaire (SGRQ). (SGRQ is a validated disease-specific instrument designed to measure impact on overall health, daily life, and perceived well-being. It measures activity limitations, symptoms, and psychosocial impact.) Tiotropium showed superiority over salmeterol in all endpoints assessed (0.14 L increase in morning FEV1vs 0.09 L, 1.02 U improvement in TDI score vs 0.24, and –5.14 U improvement of SGRQ total score from baseline vs –3.54). However, it should be noted that a difference of 1 on the TDI score was necessary to suggest a clinical benefit. While the overall difference in SGQR between tiotropium and salmeterol did not reach statistical significance, the proportion of patients in the tiotropium group that reached the clinically significant threshold of 4 units improvement in SGRQ score was significantly higher than in the salmeterol group (51% vs 40%; P<.05).4
In a similar study in 2003, 1207 patients were randomized to receive the above doses of salmeterol, tiotropium, or placebo. Over the course of 6 months, tiotropium was associated with a significant delay in onset of the first exacerbation compared with placebo, and overall it led to the fewest exacerbations per patient-year. Fewer hospital admissions were also demonstrated in the tiotropium group per patient-year, and the number of days that patients were unable to perform usual activities was lowest for the tiotropium group. Again, improvement in TDI and SGRQ scores was significantly greater with tiotropium than placebo. In almost all outcomes, the salmeterol results were intermediate between those of tiotropium and placebo, and were not statistically different from placebo.5
Recommendations from others
The GOLD (Global Strategy for the Diagnosis, Management, and Prevention of COPD) Report states that the choice between β2-agonist, anti-cholinergics, or combination therapy depends on the availability and the response of a given patient in terms of symptom relief and side effects. The 2003 GOLD Workshop Report update further recommends the use of regular treatment with long-acting bronchodilators, including tiotropium, rather than short-acting bronchodilators for moderate-to-severe COPD.6
A separate report for the Joint Expert Panel on Chronic Obstructive Pulmonary Disease of the American College of Chest Physicians and the American College of Physicians—American Society of Internal Medicine states that both are beneficial for management of acute exacerbations, but that anticholinergics should be considered first because they are associated with fewer and more benign side effects.7
Patient response and tolerance of side effects determine which drug class to use
Grant Hoekzema, MD
Mercy Family Medicine Residency, St. Louis, Mo
Although recent national guidelines for the management of COPD, such as the GOLD report, give more cohesiveness to treatment strategies for patients with COPD, there is still room for tailoring a treatment approach. I find that when choosing between beta-agonists and anticholinergics, patient response and tolerability of side effects determine what I use.
This Clinical Inquiry supports my clinical impression that neither class of drug is significantly superior to the other in regards to COPD outcome measures. In my experience, when neither drug offers a clear advantage, factors affecting compliance and tolerability tend to determine how effective it is for my patients. Therefore, a trial of either class seems reasonable at first and follow-up determines what is used in the long run.
1. Liesker JJ, Wijkstra PJ, Ten Hacken NH, Koeter GH, Postma DS, Kerstjens HA. A systematic review of the effects of bronchodilators on exercise capacity in patients with COPD. Chest 2002;121:597-608.
2. McCrory DC, Brown CD. Anti-cholinergic bronchodilators versus beta2-sympathomimetic agents for acute exacerbations of chronic obstructive pulmonary disease. In: The Cochrane Library, Issue 1,2004. Chichester, UK: John Wiley, Ltd; 2003.
3. van Noord JA, de Munck DR, Bantje TA, Hop WC, Akveld ML, Bommer AM. Long-term treatment of chronic obstructive pulmonary disease with salmeterol and the additive effect of ipratropium. Eur Respir J 2000;15:878-885.
4. Donohue JF, van Noord JA, Bateman ED, et al. A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol. Chest 2002;122:47-55.
5. Brusasco V, Hodder R, Miravitlles M, Korducki L, Towse L, Kesten S. Health outcomes following treatment for six months with once daily tiotropium compared with twice daily salmeterol in patients with COPD. Thorax 2003;58:399-404.
6. Fabbri LM, Hurd SS. GOLD Scientific Committee. Global Strategy for the Diagnosis, Management, and Prevention of COPD: 2003 update. Eur Respir J 2003;22:1-2.
7. Snow V, Lascher S, Mottur-Pilson C. Joint Expert Panel on Chronic Obstructive Pulmonary Disease of the American College of Chest Physicians and the American College of Physicians-American Society of Internal Medicine. Evidence base for management of acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med 2001;134:595-599.
1. Liesker JJ, Wijkstra PJ, Ten Hacken NH, Koeter GH, Postma DS, Kerstjens HA. A systematic review of the effects of bronchodilators on exercise capacity in patients with COPD. Chest 2002;121:597-608.
2. McCrory DC, Brown CD. Anti-cholinergic bronchodilators versus beta2-sympathomimetic agents for acute exacerbations of chronic obstructive pulmonary disease. In: The Cochrane Library, Issue 1,2004. Chichester, UK: John Wiley, Ltd; 2003.
3. van Noord JA, de Munck DR, Bantje TA, Hop WC, Akveld ML, Bommer AM. Long-term treatment of chronic obstructive pulmonary disease with salmeterol and the additive effect of ipratropium. Eur Respir J 2000;15:878-885.
4. Donohue JF, van Noord JA, Bateman ED, et al. A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol. Chest 2002;122:47-55.
5. Brusasco V, Hodder R, Miravitlles M, Korducki L, Towse L, Kesten S. Health outcomes following treatment for six months with once daily tiotropium compared with twice daily salmeterol in patients with COPD. Thorax 2003;58:399-404.
6. Fabbri LM, Hurd SS. GOLD Scientific Committee. Global Strategy for the Diagnosis, Management, and Prevention of COPD: 2003 update. Eur Respir J 2003;22:1-2.
7. Snow V, Lascher S, Mottur-Pilson C. Joint Expert Panel on Chronic Obstructive Pulmonary Disease of the American College of Chest Physicians and the American College of Physicians-American Society of Internal Medicine. Evidence base for management of acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med 2001;134:595-599.
Evidence-based answers from the Family Physicians Inquiries Network