User login
High-dose antipsychotics: Desperation or data-driven?
When nothing else works, desperate clinicians are resorting to progressively more-tenuous and unpredictable treatments, trying to improve the lives of patients with refractory schizophrenia. High-dose antipsychotics is a common strategy.
Does boosting antipsychotic doses beyond the recommended range—but short of the neuroleptic threshold—enhance efficacy? This article attempts to answer that question by presenting the evidence on higher-than-recommended doses of atypical antipsychotics.
Lessons from neuroleptics
Up to 30% of patients with schizophrenia do not respond to antipsychotics and are considered “treatment refractory.”1 Even among those who do respond, improving symptoms by 20%—as research defines “treatment response”—does not necessarily yield clinical or functional improvement. Clozapine is the only atypical antipsychotic with well-established efficacy in these chronically ill patients,2 but its daunting side effects greatly curtail its use.
Before atypical antipsychotics, patients who did not respond to usual dosages of the typical neuroleptics were treated with higher dosages or switched to another drug class. Although many clinicians embraced high-dose neuroleptics, subsequent research discredited “rapid neuroleptization” in any clinical circumstance and showed that exceeding an antipsychotic’s neuroleptic threshold—the dose at which extrapyramidal side effects (EPS) occur—reduces its efficacy (Figure 1).3-5 In some instances, reducing neuroleptic dosages improves treatment-resistant patients’ symptoms and reduces druginduced side effects.6
Figure 1 Typical antipsychotics’ dose-response curve
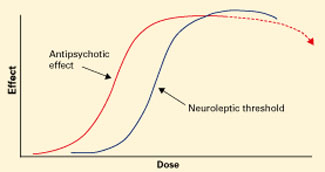
Narrow therapeutic window between antipsychotic effect and neuroleptic threshold. Dotted line indicates declining efficacy.
Figure 2 Atypical antipsychotics’ dose-response curve
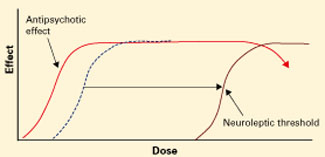
Wider therapeutic window with atypicals, compared with typical antipsychotics, as neuroleptic threshold (dotted line) moves right.Atypical antipsychotics are defined by their relative lack of EPS at recommended dosages (Figure 2). Because these agents can cause EPS if dosed too high, however, our historical habit of testing this dose limit risks losing “atypicality” and encountering other untoward events (Figure 3).
What is the safest, most effective dosage? Consider the evidence for each atypical antipsychotic.
Risperidone
Recommended dosage too high? When using atypicals at recommended doses, you are most likely to encounter the neuroleptic threshold with risperidone, with EPS risk increasing substantially at >6 mg/d.7 Post-approval studies set the most effective and safest dosage at approximately 4 mg/d, though this dosage was not studied in North American pre-approval trials. Dosages of 2 to 4 mg/d have been associated with more-favorable outcomes, suggesting that the initial recommendation to titrate to 6 mg/d within the first 3 days was ill-advised.8
In our study of patients with treatment-refractory schizophrenia,9 those treated with risperidone, 6 mg/d, improved significantly more after 4 weeks than did those receiving haloperidol, 15 mg/d, based on Brief Psychiatric Rating Scale (BPRS) scores. No additional benefit was seen after risperidone was increased to >6 mg/d at 8 weeks. Akathisia and tardive dyskinesia occurred significantly more often in the haloperidol group.
Conclusion. Some patients respond to higher-dose risperidone, but emerging EPS suggest the need to reduce the dosage rather than add an antiparkinsonian agent.
Figure 3 Unknown effects of high-dose atypical antipsychotic therapy
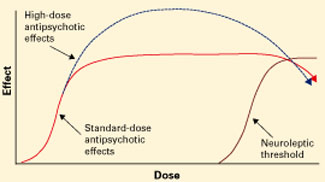
Dotted line indicates potential for greater antipsychotic effect with increasing dose.
Olanzapine
Mixed results. Case reports suggest that some patients who did not respond to previous antipsychotic trials or olanzapine, 20 mg/d, improved sig-nificantly—without substanial side effects—when olanzapine was increased up to 60 mg/d.10-14 Other case studies, however, report EPS, increased heart rate, increased transaminases, hyperprolactinemia, and prolonged QTc interval with high-dose olanzapine.14-16
In an open-label trial,17 43 patients with schizophrenia received olanzapine, up to 40 mg/d, after inadequate response to neuroleptics and risperidone or clozapine. Olanzapine was titrated to 20 mg/d by week 4 and increased 5 mg every 2 weeks if symptoms did not improve. After 14 weeks, improvement was modest and only 17% of patients met response criteria. However, >20 mg/d reduced symptoms more than did <20 mg/d, suggesting that high-dose olanzapine was more effective.
In a randomized trial,18 patients who did not respond to at least one atypical antipsychotic then received 8 weeks of fixed, standard-dose treatment with (mean dosages):
- haloperidol, 18.9 mg/d
- risperidone, 7.9 mg/d
- olanzapine, 19.6 mg/d
- clozapine, 401.6 mg/d.
Flexible dosing was then allowed for 6 weeks, and mean dosages were:
- haloperidol, 25.7 mg/d
- risperidone, 11.6 mg/d
- olanzapine, 30.4 mg/d
- clozapine, 526.6 mg/d.
Symptoms improved modestly at best for all medications, although patients taking olanzapine or clozapine improved significantly more than those treated with haloperidol as shown by mean changes in total Positive and Negative Syndrome Scale (PANSS) scores.
PANSS scores for olanzapine-treated patients showed additional improvement at week 14—when higher dosages were used—compared with week 8. This was not the case for the other medications, for which response plateaued. These findings suggest that high-dose risperidone and haloperidol are incrementally ineffective, but high-dose olanzapine could help some patients with refractory symptoms.
Results were different in a randomized, double-blind, 16-week, crossover study,19 when 13 patients with inadequate response to neuroleptics, risperidone, or conventional-dose olanzapine then received olanzapine, 50 mg/d, or clozapine, 450 mg/d. No olanzapine-treated patients and 20% of clozapine-treated patients met criteria for treatment response (20% improvement in BPRS score and final BPRS score <35 or 1-point improvement on Clinical Global Impressions-Severity of Illness scale).
Negative results don’t make headlines. Published clinical trials and case reports are subject to selective reporting of positive outcomes. Cases in which high-dose therapy proved ineffectivemay outnumber positive results but are less likely to be published.
Numbers don’t lie. Using high doses will almost always increase side effect risk and drug therapy costs, contributing to a poor risk-benefit ratio when efficacy remains unchanged. Resorting to an “if-it’s-not-working, double-it” strategy may seem reasonable, but two times zero is still zero.
Desperation warps perception. Clinicians tend to rely on observational experience. The desperation inherent in treating refractory patients, however, often creates a strong desire for improvement and therefore a potentially biased perception of outcome.
Likewise, patients may inaccurately portray themselves as improved to avoid disappointing their doctors. Controlled trials reduce these biases to better assess efficacy.
Antipsychotics work in 6 to 8 weeks. Improvements seen when pushing medications beyond recommended dosing may not be an effect of dose but of additional time on the medication. Antipsychotics usually take 6 to 8 weeks to produce maximal response, so high-dose therapy should not be started during this initial phase. This pace may not satisfy pressures for expedient stabilization and hospital discharge, but it is unrealistic to expect antipsychotics to work more quickly than they do.
Oversedation does not equal improvement. Patients who become excessively sedated from high-dose therapy or adjunctive medications may appear less psychotic but may not be so. The family or hospital staff may desire such sedation, but it can adversely affect the patient’s quality of life or medication adherence.
Polypharmacy clouds the issue. Many patients treated with high-dose antipsychotics are taking multiple agents, making it difficult to attribute improvement (or side effects) to any single one. A well-designed study of high-dose therapy would therefore:
- control for time
- examine concomitant medications’ effects
- determine whether “improvements” are related to sedation or reduced psychosis.
Medication may not need to change. When a patient decompensates, many forces pressure clinicians to change or add medications or increase dosages. Change may not be necessary, however, as nonadherence or substance abuse often trigger psychotic exacerbations. For example, Steingard et al27 added fluphenazine or placebo to antipsychotic regimens of newly hospitalized patients and found that increasing antipsychotic dosage did not improve outcome.
Subjects switching from clozapine to olanzapine tended to worsen, whereas those switching from olanzapine to clozapine tended to improve. Olanzapine-treated patients experienced more anticholinergic side effects and more weight gain than did clozapine-treated subjects.20
Conclusion. These mixed findings on high-dose olanzapine suggest questionable efficacy in patients with treatment-resistant schizophrenia and an uncertain risk of increased toxicity.
Quetiapine
Early placebo-controlled studies of quetiapine in schizophrenia concluded that statistically significant improvement begins at 150 mg/d and falls off after 600 mg/d.21 Although few high-dose quetiapine cases have been presented, clinical opinion holds that:
- most patients with chronic schizophrenia require 400 to 800 mg/d
- some treatment-refractory patients might benefit from >800 mg/d.
One patient responded to quetiapine, 1,600 mg/d, after not responding to olanzapine, 40 mg/d, and quetiapine, 800 mg/d. Constipation was the only reported side effect.22
Our group23 reported a series of 7 patients who responded (by clinician report) to quetiapine, 1,200 to 2,400 mg/d, after not responding to quetiapine, 800 mg/d, or to neuroleptics, risperidone, or olanzapine. Six responded to high-dose quetiapine and 1 to high-dose quetiapine plus risperidone, 2 mg/d; 4 received adjunctive dival-proex sodium, 1,500 to 3,000 mg/d. Psychopathology, violence, and behavioral disturbances were reduced throughout 5 to 14 months of monitoring. Side effects included sedation, orthostasis, and dysphagia.
When Nelson et al24 treated 13 subjects for 14 weeks with quetiapine, 1,000 to 1,400 mg/d, mean weight, glucose, total cholesterol, prolactin, and QTc interval duration did not change significantly. Heart rate increased significantly (though not to tachycardia), and headache, constipation, and lethargy were the most frequent side effects.
Summary. Although encouraging, these reports are preliminary, unpublished, and lack peer review. Controlled trials of high-dose quetiapine’s efficacy and safety are needed.
Ziprasidone and aripiprazole
No studies of high-dose ziprasidone or aripiprazole have been published. In premarketing trials:
- ziprasidone was studied at 200 mg/d and released with a maximum recommended dosage of 160 mg/d
- aripiprazole, 30 mg/d, was not more effective than 15 mg/d.25
Deutschman et al26 reviewed the charts of 31 patients who received ziprasidone, 240 to 320 mg/d, after an “incomplete” response to 160 mg/d. At the higher dosing:
- psychosis, affective symptoms, or anxiety improved in nearly one-half of patients
- 15% reported sedation, but most reported no side effects
- none developed QTc intervals >500 msec.
Caveats and precautions
These uncontrolled case reports and open-label studies do not “prove” efficacy or safety but reflect clinical practice. More than anything, they show that we need controlled trials to gauge high-dose antipsychotic therapy’s efficacy and safety and to curb our collective habit of relying on anecdotal experience and idiosyncratic beliefs.
Despite its side-effect profile, clozapine remains the treatment of choice for refractory schizophrenia. Given high-dose antipsychotic therapy’s uncertain efficacy and unknown risks, the evidence supports a clozapine trial before higher-than-recommended dosing is attempted.
Because educated guesswork plays a role in premarketing dosing studies, a medication’s optimal dose may be:
- overestimated (as with risperidone)
- underestimated (as perhaps with olanzapine and quetiapine).
Keep in mind some important caveats when you consider giving a patient high-dose antipsychotic therapy (Box).27 Of course, nonadherence is often the cause of apparent medication nonresponse. Increasing the dosage of a medication a patient is not taking rarely improves adherence. Interventions to enhance adherence—careful assessment, psychoeducation, and using longacting intramuscular medication—may be useful.
Related resources
- Marder SR, Essock SM, Miller AL, et al. The Mount Sinai Conference on the pharmacotherapy of schizophrenia. Schizophrenia Bull 2002;28:5-16.
- Practice guideline for the treatment of patients with schizophrenia (2nd ed). Am J Psychiatry 2004;161(suppl):1-56.
- Texas Medication Algorithm Project antipsychotic algorithm. http://www.mhmr.state.tx.us/centraloffice/medicaldirector/timascz1algo.pdf
Drug brand names
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Divalproex • Depakote
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
Dr. Pierre receives research support from Cephalon Inc., and is a consultant to and/or speaker for Pfizer Inc., Bristol-Myers Squibb Co., AstraZeneca Pharmaceuticals, and Janssen Pharmaceutica.
Dr. Donna Wirshing receives research support from, is a consultant to, and/or is a speaker for Bristol-Myers Squibb Co., Pfizer Inc., Eli Lilly & Co., Janssen Pharmaceutica, AstraZeneca Pharmaceuticals, and Abbott Laboratories.
Dr. William Wirshing receives research support from, is a consultant to, and/or is a speaker for Bristol-Myers Squibb Co., Pfizer Inc., Eli Lilly & Co., Janssen Pharmaceutica, and AstraZeneca Pharmaceuticals.
1. Conley RR, Buchanan RW. Evaluation of treatment-resistant schizophrenia. Schizophr Bull 1997;23:663-74.
2. Chakos M, Lieberman J, Hoffman E, et al. Effectiveness of second-generation antipsychotics in patients with treatment-resistant schizophrenia: A review and meta-analysis of randomized trials. Am J Psychiatry 2001;158:518-26.
3. Baldessarini RJ, Cohen BM, Teicher MH. Significance of neuroleptic dose and plasma level in the pharmacological treatment of psychoses. Arch Gen Psych 1988;45:79-91.
4. McEvoy JP, Hogarty GE, Steingard S. Optimal dose of neuroleptic in acute schizophrenia: A controlled study of the neuroleptic threshold and higher haloperidol dose. Arch Gen Psychiatry 1991;48:739-45.
5. Van Putten T, Marder SR, Mintz J, Poland R. Haloperidol plasma levels and clinical response: A therapeutic window relationship. Am J Psychiatry 1992;149:500-5.
6. Van Putten T, Marshall BD, Liberman R, et al. Systematic dosage reduction in treatment-resistant schizophrenic patients. Psychopharmacol Bull 1993;29:315-20.
7. Marder SR, Meibach RC. Risperidone in the treatment of schizophrenia. Am J Psychiatry 1994;151:825-36.
8. Love RC, Conley RR, Kelly DL, Bartko JJ. A dose-outcome analysis of risperidone. J Clin Psychiatry 1999;60:771-5.
9. Wirshing DA, Marshall BD, Jr, Green MF, et al. Risperidone in treatment-refractory schizophrenia. Am J Psychiatry 1999;156:1374-9.
10. Fanous A, Lindenmayer JP. Schizophrenia and schizoaffective disorder treated with high doses of olanzapine. J Clin Psychopharmacol 1999;19:275-6.
11. Reich J. Use of high-dose olanzapine in refractory psychosis. Am J Psychiatry 1999;156:661.-
12. Dursun SM, Gardner DM, Bird DC, Flinn J. Olanzapine for patients with treatment-resistant schizophrenia: A naturalistic case-series outcome study. Can J Psychiatry 1999;44:701-4.
13. Lerner V. High-dose olanzapine for treatment-refractory schizophrenia. Clin Neuropharmacol 2003;26:58-61.
14. Sheitman BB, Lindgren JC, Early JE, Sved M. High-dose olanzapine for treatment-refractory schizophrenia. Am J Psychiatry 1997;154:1626.
15. Bronson BD, Lindenmayer JP. Adverse effects of high-dose olanzapine in treatment-refractory schizophrenia. J Clin Psychopharmacol 2000;20:383-4.
16. Dineen S, Withrow K, Voronovitch L, et al. QTc prolongation and high-dose olanzapine. Psychosomatics 2003;44:174-5.
17. Lindenmayer JP, Volavka J, Lieberman J, et al. Olanzapine for schizophrenia refractory to typical and atypical antipsychotics: An open-label, prospective trial. J Clin Psychopharmacol. 2001;21:448-53.
18. Volavka J, Czobor P, Sheitman B, et al. Clozapine, olanzapine, risperidone, and haloperidol in the treatment of patients with chronic schizophrenia and schizoaffective disorder. Am J Psychiatry 2002;159:255-62.
19. Conley RR, Kelly DL, Richardson CM, et al. The efficacy of high-dose olanzapine versus clozapine in treatment-resistant schizophrenia: A double-blind cross-over study. J Clin Psychopharmacol 2003;23:668-71.
20. Kelly DL, Conley RR, Richardson CM, et al. Adverse effects and laboratory parameters of high-dose olanzapine vs. clozapine in treatment-resistant schizophrenia. Ann Clin Psychiatry 2003;15:181-6.
21. Arvanitis LA, Miller BG. and the Seroquel Trial 13 Study Group. Multiple fixed doses of “Seroquel” (quetiapine) in patients with acute exacerbation of schizophrenia: A comparison with haloperidol and placebo. Biol Psychiatry 1997;42:233-46.
22. Bobes J, Garcia-Portilla MP, Saiz PA, et al. High degree of tolerability for monotherapy with high doses of quetiapine: A case report. J Clin Psychiatry 2002;63:1048-9.
23. Pierre JM, Wirshing DA, Cannell J, et al. High-dose quetiapine in treatment refractory schizophrenia (poster). Colorado Springs, CO: International Congress of Schizophrenia Research, 2003; abstracted in Schizophrenia Res 2003;60(supp):299.-
24. Nelson MW, Reynolds R, Kelly DL, et al. Safety and tolerability of high-dose quetiapine in treatment-refractory schizophrenia: Preliminary results from an open-label trial (poster). Colorado Springs, CO: International Congress of Schizophrenia Research, 2003; abstracted in Schizophrenia Res 2003;60(supp):363.-
25. Potkin SG, Saha AR, Kujawa MJ, et al. Aripiprazole, an antipsychotic with a novel mechanism of action, and risperidone vs placebo in patients with schizophrenia and schizoaffective disorder. Arch Gen Psychiatry 2003;60:681-90.
26. Deutschman DA, Deutschman DH. High-dose ziprasidone: effectiveness and tolerability in clinical practice (poster). Boston, MA: American Psychiatric Association Institute on Psychiatric Services annual meeting, 2003.
27. Steingard S, Allen M, Schooler MR. A study of pharmacologic treatment on medication-compliant schizophrenics who relapse. J Clin Psychiatry 1994;55:470-2.
When nothing else works, desperate clinicians are resorting to progressively more-tenuous and unpredictable treatments, trying to improve the lives of patients with refractory schizophrenia. High-dose antipsychotics is a common strategy.
Does boosting antipsychotic doses beyond the recommended range—but short of the neuroleptic threshold—enhance efficacy? This article attempts to answer that question by presenting the evidence on higher-than-recommended doses of atypical antipsychotics.
Lessons from neuroleptics
Up to 30% of patients with schizophrenia do not respond to antipsychotics and are considered “treatment refractory.”1 Even among those who do respond, improving symptoms by 20%—as research defines “treatment response”—does not necessarily yield clinical or functional improvement. Clozapine is the only atypical antipsychotic with well-established efficacy in these chronically ill patients,2 but its daunting side effects greatly curtail its use.
Before atypical antipsychotics, patients who did not respond to usual dosages of the typical neuroleptics were treated with higher dosages or switched to another drug class. Although many clinicians embraced high-dose neuroleptics, subsequent research discredited “rapid neuroleptization” in any clinical circumstance and showed that exceeding an antipsychotic’s neuroleptic threshold—the dose at which extrapyramidal side effects (EPS) occur—reduces its efficacy (Figure 1).3-5 In some instances, reducing neuroleptic dosages improves treatment-resistant patients’ symptoms and reduces druginduced side effects.6
Figure 1 Typical antipsychotics’ dose-response curve
Narrow therapeutic window between antipsychotic effect and neuroleptic threshold. Dotted line indicates declining efficacy.
Figure 2 Atypical antipsychotics’ dose-response curve
Wider therapeutic window with atypicals, compared with typical antipsychotics, as neuroleptic threshold (dotted line) moves right.Atypical antipsychotics are defined by their relative lack of EPS at recommended dosages (Figure 2). Because these agents can cause EPS if dosed too high, however, our historical habit of testing this dose limit risks losing “atypicality” and encountering other untoward events (Figure 3).
What is the safest, most effective dosage? Consider the evidence for each atypical antipsychotic.
Risperidone
Recommended dosage too high? When using atypicals at recommended doses, you are most likely to encounter the neuroleptic threshold with risperidone, with EPS risk increasing substantially at >6 mg/d.7 Post-approval studies set the most effective and safest dosage at approximately 4 mg/d, though this dosage was not studied in North American pre-approval trials. Dosages of 2 to 4 mg/d have been associated with more-favorable outcomes, suggesting that the initial recommendation to titrate to 6 mg/d within the first 3 days was ill-advised.8
In our study of patients with treatment-refractory schizophrenia,9 those treated with risperidone, 6 mg/d, improved significantly more after 4 weeks than did those receiving haloperidol, 15 mg/d, based on Brief Psychiatric Rating Scale (BPRS) scores. No additional benefit was seen after risperidone was increased to >6 mg/d at 8 weeks. Akathisia and tardive dyskinesia occurred significantly more often in the haloperidol group.
Conclusion. Some patients respond to higher-dose risperidone, but emerging EPS suggest the need to reduce the dosage rather than add an antiparkinsonian agent.
Figure 3 Unknown effects of high-dose atypical antipsychotic therapy
Dotted line indicates potential for greater antipsychotic effect with increasing dose.
Olanzapine
Mixed results. Case reports suggest that some patients who did not respond to previous antipsychotic trials or olanzapine, 20 mg/d, improved sig-nificantly—without substanial side effects—when olanzapine was increased up to 60 mg/d.10-14 Other case studies, however, report EPS, increased heart rate, increased transaminases, hyperprolactinemia, and prolonged QTc interval with high-dose olanzapine.14-16
In an open-label trial,17 43 patients with schizophrenia received olanzapine, up to 40 mg/d, after inadequate response to neuroleptics and risperidone or clozapine. Olanzapine was titrated to 20 mg/d by week 4 and increased 5 mg every 2 weeks if symptoms did not improve. After 14 weeks, improvement was modest and only 17% of patients met response criteria. However, >20 mg/d reduced symptoms more than did <20 mg/d, suggesting that high-dose olanzapine was more effective.
In a randomized trial,18 patients who did not respond to at least one atypical antipsychotic then received 8 weeks of fixed, standard-dose treatment with (mean dosages):
- haloperidol, 18.9 mg/d
- risperidone, 7.9 mg/d
- olanzapine, 19.6 mg/d
- clozapine, 401.6 mg/d.
Flexible dosing was then allowed for 6 weeks, and mean dosages were:
- haloperidol, 25.7 mg/d
- risperidone, 11.6 mg/d
- olanzapine, 30.4 mg/d
- clozapine, 526.6 mg/d.
Symptoms improved modestly at best for all medications, although patients taking olanzapine or clozapine improved significantly more than those treated with haloperidol as shown by mean changes in total Positive and Negative Syndrome Scale (PANSS) scores.
PANSS scores for olanzapine-treated patients showed additional improvement at week 14—when higher dosages were used—compared with week 8. This was not the case for the other medications, for which response plateaued. These findings suggest that high-dose risperidone and haloperidol are incrementally ineffective, but high-dose olanzapine could help some patients with refractory symptoms.
Results were different in a randomized, double-blind, 16-week, crossover study,19 when 13 patients with inadequate response to neuroleptics, risperidone, or conventional-dose olanzapine then received olanzapine, 50 mg/d, or clozapine, 450 mg/d. No olanzapine-treated patients and 20% of clozapine-treated patients met criteria for treatment response (20% improvement in BPRS score and final BPRS score <35 or 1-point improvement on Clinical Global Impressions-Severity of Illness scale).
Negative results don’t make headlines. Published clinical trials and case reports are subject to selective reporting of positive outcomes. Cases in which high-dose therapy proved ineffectivemay outnumber positive results but are less likely to be published.
Numbers don’t lie. Using high doses will almost always increase side effect risk and drug therapy costs, contributing to a poor risk-benefit ratio when efficacy remains unchanged. Resorting to an “if-it’s-not-working, double-it” strategy may seem reasonable, but two times zero is still zero.
Desperation warps perception. Clinicians tend to rely on observational experience. The desperation inherent in treating refractory patients, however, often creates a strong desire for improvement and therefore a potentially biased perception of outcome.
Likewise, patients may inaccurately portray themselves as improved to avoid disappointing their doctors. Controlled trials reduce these biases to better assess efficacy.
Antipsychotics work in 6 to 8 weeks. Improvements seen when pushing medications beyond recommended dosing may not be an effect of dose but of additional time on the medication. Antipsychotics usually take 6 to 8 weeks to produce maximal response, so high-dose therapy should not be started during this initial phase. This pace may not satisfy pressures for expedient stabilization and hospital discharge, but it is unrealistic to expect antipsychotics to work more quickly than they do.
Oversedation does not equal improvement. Patients who become excessively sedated from high-dose therapy or adjunctive medications may appear less psychotic but may not be so. The family or hospital staff may desire such sedation, but it can adversely affect the patient’s quality of life or medication adherence.
Polypharmacy clouds the issue. Many patients treated with high-dose antipsychotics are taking multiple agents, making it difficult to attribute improvement (or side effects) to any single one. A well-designed study of high-dose therapy would therefore:
- control for time
- examine concomitant medications’ effects
- determine whether “improvements” are related to sedation or reduced psychosis.
Medication may not need to change. When a patient decompensates, many forces pressure clinicians to change or add medications or increase dosages. Change may not be necessary, however, as nonadherence or substance abuse often trigger psychotic exacerbations. For example, Steingard et al27 added fluphenazine or placebo to antipsychotic regimens of newly hospitalized patients and found that increasing antipsychotic dosage did not improve outcome.
Subjects switching from clozapine to olanzapine tended to worsen, whereas those switching from olanzapine to clozapine tended to improve. Olanzapine-treated patients experienced more anticholinergic side effects and more weight gain than did clozapine-treated subjects.20
Conclusion. These mixed findings on high-dose olanzapine suggest questionable efficacy in patients with treatment-resistant schizophrenia and an uncertain risk of increased toxicity.
Quetiapine
Early placebo-controlled studies of quetiapine in schizophrenia concluded that statistically significant improvement begins at 150 mg/d and falls off after 600 mg/d.21 Although few high-dose quetiapine cases have been presented, clinical opinion holds that:
- most patients with chronic schizophrenia require 400 to 800 mg/d
- some treatment-refractory patients might benefit from >800 mg/d.
One patient responded to quetiapine, 1,600 mg/d, after not responding to olanzapine, 40 mg/d, and quetiapine, 800 mg/d. Constipation was the only reported side effect.22
Our group23 reported a series of 7 patients who responded (by clinician report) to quetiapine, 1,200 to 2,400 mg/d, after not responding to quetiapine, 800 mg/d, or to neuroleptics, risperidone, or olanzapine. Six responded to high-dose quetiapine and 1 to high-dose quetiapine plus risperidone, 2 mg/d; 4 received adjunctive dival-proex sodium, 1,500 to 3,000 mg/d. Psychopathology, violence, and behavioral disturbances were reduced throughout 5 to 14 months of monitoring. Side effects included sedation, orthostasis, and dysphagia.
When Nelson et al24 treated 13 subjects for 14 weeks with quetiapine, 1,000 to 1,400 mg/d, mean weight, glucose, total cholesterol, prolactin, and QTc interval duration did not change significantly. Heart rate increased significantly (though not to tachycardia), and headache, constipation, and lethargy were the most frequent side effects.
Summary. Although encouraging, these reports are preliminary, unpublished, and lack peer review. Controlled trials of high-dose quetiapine’s efficacy and safety are needed.
Ziprasidone and aripiprazole
No studies of high-dose ziprasidone or aripiprazole have been published. In premarketing trials:
- ziprasidone was studied at 200 mg/d and released with a maximum recommended dosage of 160 mg/d
- aripiprazole, 30 mg/d, was not more effective than 15 mg/d.25
Deutschman et al26 reviewed the charts of 31 patients who received ziprasidone, 240 to 320 mg/d, after an “incomplete” response to 160 mg/d. At the higher dosing:
- psychosis, affective symptoms, or anxiety improved in nearly one-half of patients
- 15% reported sedation, but most reported no side effects
- none developed QTc intervals >500 msec.
Caveats and precautions
These uncontrolled case reports and open-label studies do not “prove” efficacy or safety but reflect clinical practice. More than anything, they show that we need controlled trials to gauge high-dose antipsychotic therapy’s efficacy and safety and to curb our collective habit of relying on anecdotal experience and idiosyncratic beliefs.
Despite its side-effect profile, clozapine remains the treatment of choice for refractory schizophrenia. Given high-dose antipsychotic therapy’s uncertain efficacy and unknown risks, the evidence supports a clozapine trial before higher-than-recommended dosing is attempted.
Because educated guesswork plays a role in premarketing dosing studies, a medication’s optimal dose may be:
- overestimated (as with risperidone)
- underestimated (as perhaps with olanzapine and quetiapine).
Keep in mind some important caveats when you consider giving a patient high-dose antipsychotic therapy (Box).27 Of course, nonadherence is often the cause of apparent medication nonresponse. Increasing the dosage of a medication a patient is not taking rarely improves adherence. Interventions to enhance adherence—careful assessment, psychoeducation, and using longacting intramuscular medication—may be useful.
Related resources
- Marder SR, Essock SM, Miller AL, et al. The Mount Sinai Conference on the pharmacotherapy of schizophrenia. Schizophrenia Bull 2002;28:5-16.
- Practice guideline for the treatment of patients with schizophrenia (2nd ed). Am J Psychiatry 2004;161(suppl):1-56.
- Texas Medication Algorithm Project antipsychotic algorithm. http://www.mhmr.state.tx.us/centraloffice/medicaldirector/timascz1algo.pdf
Drug brand names
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Divalproex • Depakote
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
Dr. Pierre receives research support from Cephalon Inc., and is a consultant to and/or speaker for Pfizer Inc., Bristol-Myers Squibb Co., AstraZeneca Pharmaceuticals, and Janssen Pharmaceutica.
Dr. Donna Wirshing receives research support from, is a consultant to, and/or is a speaker for Bristol-Myers Squibb Co., Pfizer Inc., Eli Lilly & Co., Janssen Pharmaceutica, AstraZeneca Pharmaceuticals, and Abbott Laboratories.
Dr. William Wirshing receives research support from, is a consultant to, and/or is a speaker for Bristol-Myers Squibb Co., Pfizer Inc., Eli Lilly & Co., Janssen Pharmaceutica, and AstraZeneca Pharmaceuticals.
When nothing else works, desperate clinicians are resorting to progressively more-tenuous and unpredictable treatments, trying to improve the lives of patients with refractory schizophrenia. High-dose antipsychotics is a common strategy.
Does boosting antipsychotic doses beyond the recommended range—but short of the neuroleptic threshold—enhance efficacy? This article attempts to answer that question by presenting the evidence on higher-than-recommended doses of atypical antipsychotics.
Lessons from neuroleptics
Up to 30% of patients with schizophrenia do not respond to antipsychotics and are considered “treatment refractory.”1 Even among those who do respond, improving symptoms by 20%—as research defines “treatment response”—does not necessarily yield clinical or functional improvement. Clozapine is the only atypical antipsychotic with well-established efficacy in these chronically ill patients,2 but its daunting side effects greatly curtail its use.
Before atypical antipsychotics, patients who did not respond to usual dosages of the typical neuroleptics were treated with higher dosages or switched to another drug class. Although many clinicians embraced high-dose neuroleptics, subsequent research discredited “rapid neuroleptization” in any clinical circumstance and showed that exceeding an antipsychotic’s neuroleptic threshold—the dose at which extrapyramidal side effects (EPS) occur—reduces its efficacy (Figure 1).3-5 In some instances, reducing neuroleptic dosages improves treatment-resistant patients’ symptoms and reduces druginduced side effects.6
Figure 1 Typical antipsychotics’ dose-response curve
Narrow therapeutic window between antipsychotic effect and neuroleptic threshold. Dotted line indicates declining efficacy.
Figure 2 Atypical antipsychotics’ dose-response curve
Wider therapeutic window with atypicals, compared with typical antipsychotics, as neuroleptic threshold (dotted line) moves right.Atypical antipsychotics are defined by their relative lack of EPS at recommended dosages (Figure 2). Because these agents can cause EPS if dosed too high, however, our historical habit of testing this dose limit risks losing “atypicality” and encountering other untoward events (Figure 3).
What is the safest, most effective dosage? Consider the evidence for each atypical antipsychotic.
Risperidone
Recommended dosage too high? When using atypicals at recommended doses, you are most likely to encounter the neuroleptic threshold with risperidone, with EPS risk increasing substantially at >6 mg/d.7 Post-approval studies set the most effective and safest dosage at approximately 4 mg/d, though this dosage was not studied in North American pre-approval trials. Dosages of 2 to 4 mg/d have been associated with more-favorable outcomes, suggesting that the initial recommendation to titrate to 6 mg/d within the first 3 days was ill-advised.8
In our study of patients with treatment-refractory schizophrenia,9 those treated with risperidone, 6 mg/d, improved significantly more after 4 weeks than did those receiving haloperidol, 15 mg/d, based on Brief Psychiatric Rating Scale (BPRS) scores. No additional benefit was seen after risperidone was increased to >6 mg/d at 8 weeks. Akathisia and tardive dyskinesia occurred significantly more often in the haloperidol group.
Conclusion. Some patients respond to higher-dose risperidone, but emerging EPS suggest the need to reduce the dosage rather than add an antiparkinsonian agent.
Figure 3 Unknown effects of high-dose atypical antipsychotic therapy
Dotted line indicates potential for greater antipsychotic effect with increasing dose.
Olanzapine
Mixed results. Case reports suggest that some patients who did not respond to previous antipsychotic trials or olanzapine, 20 mg/d, improved sig-nificantly—without substanial side effects—when olanzapine was increased up to 60 mg/d.10-14 Other case studies, however, report EPS, increased heart rate, increased transaminases, hyperprolactinemia, and prolonged QTc interval with high-dose olanzapine.14-16
In an open-label trial,17 43 patients with schizophrenia received olanzapine, up to 40 mg/d, after inadequate response to neuroleptics and risperidone or clozapine. Olanzapine was titrated to 20 mg/d by week 4 and increased 5 mg every 2 weeks if symptoms did not improve. After 14 weeks, improvement was modest and only 17% of patients met response criteria. However, >20 mg/d reduced symptoms more than did <20 mg/d, suggesting that high-dose olanzapine was more effective.
In a randomized trial,18 patients who did not respond to at least one atypical antipsychotic then received 8 weeks of fixed, standard-dose treatment with (mean dosages):
- haloperidol, 18.9 mg/d
- risperidone, 7.9 mg/d
- olanzapine, 19.6 mg/d
- clozapine, 401.6 mg/d.
Flexible dosing was then allowed for 6 weeks, and mean dosages were:
- haloperidol, 25.7 mg/d
- risperidone, 11.6 mg/d
- olanzapine, 30.4 mg/d
- clozapine, 526.6 mg/d.
Symptoms improved modestly at best for all medications, although patients taking olanzapine or clozapine improved significantly more than those treated with haloperidol as shown by mean changes in total Positive and Negative Syndrome Scale (PANSS) scores.
PANSS scores for olanzapine-treated patients showed additional improvement at week 14—when higher dosages were used—compared with week 8. This was not the case for the other medications, for which response plateaued. These findings suggest that high-dose risperidone and haloperidol are incrementally ineffective, but high-dose olanzapine could help some patients with refractory symptoms.
Results were different in a randomized, double-blind, 16-week, crossover study,19 when 13 patients with inadequate response to neuroleptics, risperidone, or conventional-dose olanzapine then received olanzapine, 50 mg/d, or clozapine, 450 mg/d. No olanzapine-treated patients and 20% of clozapine-treated patients met criteria for treatment response (20% improvement in BPRS score and final BPRS score <35 or 1-point improvement on Clinical Global Impressions-Severity of Illness scale).
Negative results don’t make headlines. Published clinical trials and case reports are subject to selective reporting of positive outcomes. Cases in which high-dose therapy proved ineffectivemay outnumber positive results but are less likely to be published.
Numbers don’t lie. Using high doses will almost always increase side effect risk and drug therapy costs, contributing to a poor risk-benefit ratio when efficacy remains unchanged. Resorting to an “if-it’s-not-working, double-it” strategy may seem reasonable, but two times zero is still zero.
Desperation warps perception. Clinicians tend to rely on observational experience. The desperation inherent in treating refractory patients, however, often creates a strong desire for improvement and therefore a potentially biased perception of outcome.
Likewise, patients may inaccurately portray themselves as improved to avoid disappointing their doctors. Controlled trials reduce these biases to better assess efficacy.
Antipsychotics work in 6 to 8 weeks. Improvements seen when pushing medications beyond recommended dosing may not be an effect of dose but of additional time on the medication. Antipsychotics usually take 6 to 8 weeks to produce maximal response, so high-dose therapy should not be started during this initial phase. This pace may not satisfy pressures for expedient stabilization and hospital discharge, but it is unrealistic to expect antipsychotics to work more quickly than they do.
Oversedation does not equal improvement. Patients who become excessively sedated from high-dose therapy or adjunctive medications may appear less psychotic but may not be so. The family or hospital staff may desire such sedation, but it can adversely affect the patient’s quality of life or medication adherence.
Polypharmacy clouds the issue. Many patients treated with high-dose antipsychotics are taking multiple agents, making it difficult to attribute improvement (or side effects) to any single one. A well-designed study of high-dose therapy would therefore:
- control for time
- examine concomitant medications’ effects
- determine whether “improvements” are related to sedation or reduced psychosis.
Medication may not need to change. When a patient decompensates, many forces pressure clinicians to change or add medications or increase dosages. Change may not be necessary, however, as nonadherence or substance abuse often trigger psychotic exacerbations. For example, Steingard et al27 added fluphenazine or placebo to antipsychotic regimens of newly hospitalized patients and found that increasing antipsychotic dosage did not improve outcome.
Subjects switching from clozapine to olanzapine tended to worsen, whereas those switching from olanzapine to clozapine tended to improve. Olanzapine-treated patients experienced more anticholinergic side effects and more weight gain than did clozapine-treated subjects.20
Conclusion. These mixed findings on high-dose olanzapine suggest questionable efficacy in patients with treatment-resistant schizophrenia and an uncertain risk of increased toxicity.
Quetiapine
Early placebo-controlled studies of quetiapine in schizophrenia concluded that statistically significant improvement begins at 150 mg/d and falls off after 600 mg/d.21 Although few high-dose quetiapine cases have been presented, clinical opinion holds that:
- most patients with chronic schizophrenia require 400 to 800 mg/d
- some treatment-refractory patients might benefit from >800 mg/d.
One patient responded to quetiapine, 1,600 mg/d, after not responding to olanzapine, 40 mg/d, and quetiapine, 800 mg/d. Constipation was the only reported side effect.22
Our group23 reported a series of 7 patients who responded (by clinician report) to quetiapine, 1,200 to 2,400 mg/d, after not responding to quetiapine, 800 mg/d, or to neuroleptics, risperidone, or olanzapine. Six responded to high-dose quetiapine and 1 to high-dose quetiapine plus risperidone, 2 mg/d; 4 received adjunctive dival-proex sodium, 1,500 to 3,000 mg/d. Psychopathology, violence, and behavioral disturbances were reduced throughout 5 to 14 months of monitoring. Side effects included sedation, orthostasis, and dysphagia.
When Nelson et al24 treated 13 subjects for 14 weeks with quetiapine, 1,000 to 1,400 mg/d, mean weight, glucose, total cholesterol, prolactin, and QTc interval duration did not change significantly. Heart rate increased significantly (though not to tachycardia), and headache, constipation, and lethargy were the most frequent side effects.
Summary. Although encouraging, these reports are preliminary, unpublished, and lack peer review. Controlled trials of high-dose quetiapine’s efficacy and safety are needed.
Ziprasidone and aripiprazole
No studies of high-dose ziprasidone or aripiprazole have been published. In premarketing trials:
- ziprasidone was studied at 200 mg/d and released with a maximum recommended dosage of 160 mg/d
- aripiprazole, 30 mg/d, was not more effective than 15 mg/d.25
Deutschman et al26 reviewed the charts of 31 patients who received ziprasidone, 240 to 320 mg/d, after an “incomplete” response to 160 mg/d. At the higher dosing:
- psychosis, affective symptoms, or anxiety improved in nearly one-half of patients
- 15% reported sedation, but most reported no side effects
- none developed QTc intervals >500 msec.
Caveats and precautions
These uncontrolled case reports and open-label studies do not “prove” efficacy or safety but reflect clinical practice. More than anything, they show that we need controlled trials to gauge high-dose antipsychotic therapy’s efficacy and safety and to curb our collective habit of relying on anecdotal experience and idiosyncratic beliefs.
Despite its side-effect profile, clozapine remains the treatment of choice for refractory schizophrenia. Given high-dose antipsychotic therapy’s uncertain efficacy and unknown risks, the evidence supports a clozapine trial before higher-than-recommended dosing is attempted.
Because educated guesswork plays a role in premarketing dosing studies, a medication’s optimal dose may be:
- overestimated (as with risperidone)
- underestimated (as perhaps with olanzapine and quetiapine).
Keep in mind some important caveats when you consider giving a patient high-dose antipsychotic therapy (Box).27 Of course, nonadherence is often the cause of apparent medication nonresponse. Increasing the dosage of a medication a patient is not taking rarely improves adherence. Interventions to enhance adherence—careful assessment, psychoeducation, and using longacting intramuscular medication—may be useful.
Related resources
- Marder SR, Essock SM, Miller AL, et al. The Mount Sinai Conference on the pharmacotherapy of schizophrenia. Schizophrenia Bull 2002;28:5-16.
- Practice guideline for the treatment of patients with schizophrenia (2nd ed). Am J Psychiatry 2004;161(suppl):1-56.
- Texas Medication Algorithm Project antipsychotic algorithm. http://www.mhmr.state.tx.us/centraloffice/medicaldirector/timascz1algo.pdf
Drug brand names
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Divalproex • Depakote
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
Dr. Pierre receives research support from Cephalon Inc., and is a consultant to and/or speaker for Pfizer Inc., Bristol-Myers Squibb Co., AstraZeneca Pharmaceuticals, and Janssen Pharmaceutica.
Dr. Donna Wirshing receives research support from, is a consultant to, and/or is a speaker for Bristol-Myers Squibb Co., Pfizer Inc., Eli Lilly & Co., Janssen Pharmaceutica, AstraZeneca Pharmaceuticals, and Abbott Laboratories.
Dr. William Wirshing receives research support from, is a consultant to, and/or is a speaker for Bristol-Myers Squibb Co., Pfizer Inc., Eli Lilly & Co., Janssen Pharmaceutica, and AstraZeneca Pharmaceuticals.
1. Conley RR, Buchanan RW. Evaluation of treatment-resistant schizophrenia. Schizophr Bull 1997;23:663-74.
2. Chakos M, Lieberman J, Hoffman E, et al. Effectiveness of second-generation antipsychotics in patients with treatment-resistant schizophrenia: A review and meta-analysis of randomized trials. Am J Psychiatry 2001;158:518-26.
3. Baldessarini RJ, Cohen BM, Teicher MH. Significance of neuroleptic dose and plasma level in the pharmacological treatment of psychoses. Arch Gen Psych 1988;45:79-91.
4. McEvoy JP, Hogarty GE, Steingard S. Optimal dose of neuroleptic in acute schizophrenia: A controlled study of the neuroleptic threshold and higher haloperidol dose. Arch Gen Psychiatry 1991;48:739-45.
5. Van Putten T, Marder SR, Mintz J, Poland R. Haloperidol plasma levels and clinical response: A therapeutic window relationship. Am J Psychiatry 1992;149:500-5.
6. Van Putten T, Marshall BD, Liberman R, et al. Systematic dosage reduction in treatment-resistant schizophrenic patients. Psychopharmacol Bull 1993;29:315-20.
7. Marder SR, Meibach RC. Risperidone in the treatment of schizophrenia. Am J Psychiatry 1994;151:825-36.
8. Love RC, Conley RR, Kelly DL, Bartko JJ. A dose-outcome analysis of risperidone. J Clin Psychiatry 1999;60:771-5.
9. Wirshing DA, Marshall BD, Jr, Green MF, et al. Risperidone in treatment-refractory schizophrenia. Am J Psychiatry 1999;156:1374-9.
10. Fanous A, Lindenmayer JP. Schizophrenia and schizoaffective disorder treated with high doses of olanzapine. J Clin Psychopharmacol 1999;19:275-6.
11. Reich J. Use of high-dose olanzapine in refractory psychosis. Am J Psychiatry 1999;156:661.-
12. Dursun SM, Gardner DM, Bird DC, Flinn J. Olanzapine for patients with treatment-resistant schizophrenia: A naturalistic case-series outcome study. Can J Psychiatry 1999;44:701-4.
13. Lerner V. High-dose olanzapine for treatment-refractory schizophrenia. Clin Neuropharmacol 2003;26:58-61.
14. Sheitman BB, Lindgren JC, Early JE, Sved M. High-dose olanzapine for treatment-refractory schizophrenia. Am J Psychiatry 1997;154:1626.
15. Bronson BD, Lindenmayer JP. Adverse effects of high-dose olanzapine in treatment-refractory schizophrenia. J Clin Psychopharmacol 2000;20:383-4.
16. Dineen S, Withrow K, Voronovitch L, et al. QTc prolongation and high-dose olanzapine. Psychosomatics 2003;44:174-5.
17. Lindenmayer JP, Volavka J, Lieberman J, et al. Olanzapine for schizophrenia refractory to typical and atypical antipsychotics: An open-label, prospective trial. J Clin Psychopharmacol. 2001;21:448-53.
18. Volavka J, Czobor P, Sheitman B, et al. Clozapine, olanzapine, risperidone, and haloperidol in the treatment of patients with chronic schizophrenia and schizoaffective disorder. Am J Psychiatry 2002;159:255-62.
19. Conley RR, Kelly DL, Richardson CM, et al. The efficacy of high-dose olanzapine versus clozapine in treatment-resistant schizophrenia: A double-blind cross-over study. J Clin Psychopharmacol 2003;23:668-71.
20. Kelly DL, Conley RR, Richardson CM, et al. Adverse effects and laboratory parameters of high-dose olanzapine vs. clozapine in treatment-resistant schizophrenia. Ann Clin Psychiatry 2003;15:181-6.
21. Arvanitis LA, Miller BG. and the Seroquel Trial 13 Study Group. Multiple fixed doses of “Seroquel” (quetiapine) in patients with acute exacerbation of schizophrenia: A comparison with haloperidol and placebo. Biol Psychiatry 1997;42:233-46.
22. Bobes J, Garcia-Portilla MP, Saiz PA, et al. High degree of tolerability for monotherapy with high doses of quetiapine: A case report. J Clin Psychiatry 2002;63:1048-9.
23. Pierre JM, Wirshing DA, Cannell J, et al. High-dose quetiapine in treatment refractory schizophrenia (poster). Colorado Springs, CO: International Congress of Schizophrenia Research, 2003; abstracted in Schizophrenia Res 2003;60(supp):299.-
24. Nelson MW, Reynolds R, Kelly DL, et al. Safety and tolerability of high-dose quetiapine in treatment-refractory schizophrenia: Preliminary results from an open-label trial (poster). Colorado Springs, CO: International Congress of Schizophrenia Research, 2003; abstracted in Schizophrenia Res 2003;60(supp):363.-
25. Potkin SG, Saha AR, Kujawa MJ, et al. Aripiprazole, an antipsychotic with a novel mechanism of action, and risperidone vs placebo in patients with schizophrenia and schizoaffective disorder. Arch Gen Psychiatry 2003;60:681-90.
26. Deutschman DA, Deutschman DH. High-dose ziprasidone: effectiveness and tolerability in clinical practice (poster). Boston, MA: American Psychiatric Association Institute on Psychiatric Services annual meeting, 2003.
27. Steingard S, Allen M, Schooler MR. A study of pharmacologic treatment on medication-compliant schizophrenics who relapse. J Clin Psychiatry 1994;55:470-2.
1. Conley RR, Buchanan RW. Evaluation of treatment-resistant schizophrenia. Schizophr Bull 1997;23:663-74.
2. Chakos M, Lieberman J, Hoffman E, et al. Effectiveness of second-generation antipsychotics in patients with treatment-resistant schizophrenia: A review and meta-analysis of randomized trials. Am J Psychiatry 2001;158:518-26.
3. Baldessarini RJ, Cohen BM, Teicher MH. Significance of neuroleptic dose and plasma level in the pharmacological treatment of psychoses. Arch Gen Psych 1988;45:79-91.
4. McEvoy JP, Hogarty GE, Steingard S. Optimal dose of neuroleptic in acute schizophrenia: A controlled study of the neuroleptic threshold and higher haloperidol dose. Arch Gen Psychiatry 1991;48:739-45.
5. Van Putten T, Marder SR, Mintz J, Poland R. Haloperidol plasma levels and clinical response: A therapeutic window relationship. Am J Psychiatry 1992;149:500-5.
6. Van Putten T, Marshall BD, Liberman R, et al. Systematic dosage reduction in treatment-resistant schizophrenic patients. Psychopharmacol Bull 1993;29:315-20.
7. Marder SR, Meibach RC. Risperidone in the treatment of schizophrenia. Am J Psychiatry 1994;151:825-36.
8. Love RC, Conley RR, Kelly DL, Bartko JJ. A dose-outcome analysis of risperidone. J Clin Psychiatry 1999;60:771-5.
9. Wirshing DA, Marshall BD, Jr, Green MF, et al. Risperidone in treatment-refractory schizophrenia. Am J Psychiatry 1999;156:1374-9.
10. Fanous A, Lindenmayer JP. Schizophrenia and schizoaffective disorder treated with high doses of olanzapine. J Clin Psychopharmacol 1999;19:275-6.
11. Reich J. Use of high-dose olanzapine in refractory psychosis. Am J Psychiatry 1999;156:661.-
12. Dursun SM, Gardner DM, Bird DC, Flinn J. Olanzapine for patients with treatment-resistant schizophrenia: A naturalistic case-series outcome study. Can J Psychiatry 1999;44:701-4.
13. Lerner V. High-dose olanzapine for treatment-refractory schizophrenia. Clin Neuropharmacol 2003;26:58-61.
14. Sheitman BB, Lindgren JC, Early JE, Sved M. High-dose olanzapine for treatment-refractory schizophrenia. Am J Psychiatry 1997;154:1626.
15. Bronson BD, Lindenmayer JP. Adverse effects of high-dose olanzapine in treatment-refractory schizophrenia. J Clin Psychopharmacol 2000;20:383-4.
16. Dineen S, Withrow K, Voronovitch L, et al. QTc prolongation and high-dose olanzapine. Psychosomatics 2003;44:174-5.
17. Lindenmayer JP, Volavka J, Lieberman J, et al. Olanzapine for schizophrenia refractory to typical and atypical antipsychotics: An open-label, prospective trial. J Clin Psychopharmacol. 2001;21:448-53.
18. Volavka J, Czobor P, Sheitman B, et al. Clozapine, olanzapine, risperidone, and haloperidol in the treatment of patients with chronic schizophrenia and schizoaffective disorder. Am J Psychiatry 2002;159:255-62.
19. Conley RR, Kelly DL, Richardson CM, et al. The efficacy of high-dose olanzapine versus clozapine in treatment-resistant schizophrenia: A double-blind cross-over study. J Clin Psychopharmacol 2003;23:668-71.
20. Kelly DL, Conley RR, Richardson CM, et al. Adverse effects and laboratory parameters of high-dose olanzapine vs. clozapine in treatment-resistant schizophrenia. Ann Clin Psychiatry 2003;15:181-6.
21. Arvanitis LA, Miller BG. and the Seroquel Trial 13 Study Group. Multiple fixed doses of “Seroquel” (quetiapine) in patients with acute exacerbation of schizophrenia: A comparison with haloperidol and placebo. Biol Psychiatry 1997;42:233-46.
22. Bobes J, Garcia-Portilla MP, Saiz PA, et al. High degree of tolerability for monotherapy with high doses of quetiapine: A case report. J Clin Psychiatry 2002;63:1048-9.
23. Pierre JM, Wirshing DA, Cannell J, et al. High-dose quetiapine in treatment refractory schizophrenia (poster). Colorado Springs, CO: International Congress of Schizophrenia Research, 2003; abstracted in Schizophrenia Res 2003;60(supp):299.-
24. Nelson MW, Reynolds R, Kelly DL, et al. Safety and tolerability of high-dose quetiapine in treatment-refractory schizophrenia: Preliminary results from an open-label trial (poster). Colorado Springs, CO: International Congress of Schizophrenia Research, 2003; abstracted in Schizophrenia Res 2003;60(supp):363.-
25. Potkin SG, Saha AR, Kujawa MJ, et al. Aripiprazole, an antipsychotic with a novel mechanism of action, and risperidone vs placebo in patients with schizophrenia and schizoaffective disorder. Arch Gen Psychiatry 2003;60:681-90.
26. Deutschman DA, Deutschman DH. High-dose ziprasidone: effectiveness and tolerability in clinical practice (poster). Boston, MA: American Psychiatric Association Institute on Psychiatric Services annual meeting, 2003.
27. Steingard S, Allen M, Schooler MR. A study of pharmacologic treatment on medication-compliant schizophrenics who relapse. J Clin Psychiatry 1994;55:470-2.
UPDATE ON ATYPICALS: Practical tips to manage common side effects
Atypical antipsychotics are powerful medications for acute and chronic psychotic disorders, with a similarly powerful potential for adverse systemic effects. To use these agents to their greatest advantage, we must balance the benefits against the risks.
We often see patients with weight gain, diabetes, dyslipidemia, cardiac toxicity, hyperprolactinemia, and sexual dysfunction—all possible effects of atypical antipsychotics. Based on the latest evidence and our experience, we offer tips for using clozapine, olanzapine, quetiapine, risperidone, and ziprasidone, and preliminary impressions about the newly approved agent, aripiprazole.
Weight gain
Clinical trials have shown convincingly that atypical antipsychotics pose a greater risk of weight gain and central adiposity than do most older antipsychotics.1 Overweight and obesity are associated with increased risks of hypertension, type 2 diabetes, coronary heart disease, stroke, gallbladder disease, osteoarthritis, and some forms of cancer. Moreover, obesity’s socially stigmatizing effect can discourage patients with schizophrenia—particularly adolescents—from taking their medication.
Table 1
POTENTIAL FOR ADVERSE EFFECTS WITH ATYPICAL ANTIPSYCHOTICS
| Metabolic changes | Weight gain | Increased prolactin | QT interval | EPS | Sedation | Orthostasis | |
|---|---|---|---|---|---|---|---|
| Risperidone | + | + | +++ | + | ++ | + | ++ |
| Ziprasidone | + | + | − | ++ | + | + | + |
| Clozapine | +++ | +++ | − | ++ | +/− | +++ | +++ |
| Olanzapine | +++ | +++ | − | + | + | ++ | + |
| Quetiapine | ++ | ++ | − | ++ | + | ++ | ++ |
| Aripiprazole | + | + | − | + | + | +/− | +/− |
Comparative effects. Olanzapine and clozapine are associated with greater weight gain (Table 1)1-3 than risperidone and ziprasidone.4 Data regarding quetiapine are inconsistent—some studies show weight gain similar to that caused by olanzapine, and others find much less.5 Weight gain associated with quetiapine, ziprasidone, and risperidone tends to plateau within the first few months, whereas patients taking olanzapine and clozapine may continue to gain weight for 9 months or more.6
Adolescents and young adults may be particularly susceptible to antipsychotic-induced weight gain.7 No studies have directly compared weight gain in adults versus adolescents, but adolescents are exceedingly susceptible to the atypicals’ metabolic dysregulation. For example:
- A higher prevalence of extreme weight gain (>7% of baseline body mass) with olanzapine and risperidone has been reported in adolescent inpatients than among adults.7
- Extreme weight gain was seen in 78% of a group of risperidone-treated children; for 6 months, their weight gain averaged 1.2 kg/month without leveling off.8
These findings suggest that risperidone’s apparent metabolic advantage in adults disappears in children and adolescents. Risperidone’s effect on prolactin may account for a higher risk of weight gain in younger patients. These populations have exquisite end-organ sensitivity to changes in prolactin levels and may be more susceptible to the weight gain—and perhaps diabetes—believed related to hyperprolactinemia.9
Mechanisms. The mechanism(s) of weight gain may be related to the receptor systems upon which the atypicals act. These agents block noradrenergic, dopamine, serotonin, and histamine receptors, all of which are thought to affect metabolism or appetite control. Stimulation of alpha and D2 receptors by sympathomimetic amines causes weight loss, as does stimulation of certain 5HT receptors by weight-loss drugs such as fenfluramine.10 With respect to appetite, it has been suggested that peripheral antagonism of H1 receptors interferes with normal satiety signals.11 This may explain why affinity to histamine H1 receptors is among the best of correlates with potential for weight gain.12
Increases in serum levels of leptin—a peptide hormone produced in direct proportion to adiposity and thought to be anorexigenic, possibly through effects on satiety13 —parallel weight gain during treatment with atypicals. However, there is no indication that leptin imbalance causes weight gain; it may instead be the result. Altered sensitivity to leptin may be a contributing factor, perhaps at the hypothalamus.14
Diabetes
The risk of type 2 diabetes increases with weight gain,15 so it is no surprise that diabetes is more prevalent among patients taking atypicals. In a study of 38,000 schizophrenic patients, those taking atypicals were 9% more likely to have diabetes than those receiving typical antipsychotics,16 and all atypicals were associated with a significant increase in diabetes risk in patients younger than 40. The pervasiveness of diabetes17 and reports of new-onset diabetes in non-overweight patients18 suggest that—in addition to their effect on weight—atypicals may alter insulin and glucose metabolism.19
Atypical antipsychotics probably increase diabetes risk in a number of ways:
- An increase in adipose tissue can lead to insulin resistance, glucose intolerance, and ultimately diabetes.20
- Serotonin receptor antagonism may lead to hyperglycemia by decreasing pancreatic beta cell response to signals that advance insulin production.21
- Atypicals may contribute to hyperglycemia by impeding cellular uptake of glucose.22
- The increase in free fatty acids associated with atypicals can alter glucose metabolism. This may explain why clozapine and olanzapine—the atypicals with the greatest potential for severe hyperlipidemia—have the strongest association with new-onset diabetes.
Hyperlipidemia
Case reports and controlled studies have linked atypical antipsychotics with hyperlipidemia. Whether the hyperlipidemia is a consequence of weight gain or some other metabolic disturbance is unknown. Even without conclusive data, however, the link is of concern because elevated triglyceride levels represent an independent risk factor for heart disease.23
Although all atypicals increase serum triglycerides to some degree, severe hypertriglyceridemia occurs predominantly with clozapine and olanzapine.24 Both drugs have favorable efficacy profiles, and the mechanism of their antipsychotic activity may include altering the various lipid pools.
For example, studies have found that decreased triglyceride levels correlate with hostility and psychological distress.25 Increased triglycerides have been theorized to enhance membrane fluidity, which in turn may augment presynaptic reuptake of serotonin and diminish postsynaptic serotonin activity.26 In other words, elevated triglyceride levels could play a role in atypical antipsychotic-mediated inhibition of serotonin transmission. It is not yet known whether lipid-lowering drugs might alter atypicals’ efficacy.
Table 2
RECOMMENDED METABOLIC MONITORING OF PATIENTS TAKING ATYPICAL ANTIPSYCHOTICS
| Every visit | Check weight Check blood pressure |
| Every 3 months | Fasting blood glucose Fasting triglycerides Fasting cholesterol |
Metabolic monitoring
Managing mental illness concurrently with weight gain, diabetes, and hypertriglyceridemia is a challenge. In our clinic, we try to diminish the atypicals’ adverse metabolic effects by monitoring a few basic parameters and taking preventive measures (Table 2).
We routinely screen patients for diabetes symptoms by asking questions about changes in belt size (a sign of weight change), urinary frequency, and thirst (Table 3). We also document baseline weight, blood glucose (Table 4), blood chemistry, and lipid levels, with routine follow-up throughout therapy and greatest scrutiny during the first months of a new treatment.
Patients who cannot control their weight with lifestyle modifications (Table 5) may require a lipid-lowering medication—a “stain” and/or fibrate (such as gemfibrozil)—or, if those measures are ineffective, a switch to another antipsychotic. Hyperlipidemia and hyperglycemia may be reduced substantially when patients discontinue the aggravating medication.27
Although discontinuing or switching medications may reduce metabolic side effects, the hazard of psychotic decompensation is substantial. Achieving an antipsychotic effect is extremely difficult for most patients, and one should not discontinue an effective treatment without seriously considering the consequences. Antipsychotic efficacy should never be sacrificed in the pursuit of a regimen with more benign side effects. Consider switching to an atypical with a more moderate effect on weight, however, if weight gain would likely lead to noncompliance. Even the most effective treatment will not work if a patient never takes it.
Table 3
5 SCREENING QUESTIONS TO MONITOR FOR METABOLIC AND SEXUAL SIDE EFFECTS
|
Table 4
DIAGNOSTIC CRITERIA FOR DIABETES
| • Symptoms of diabetes (such as polyuria, polydipsia, or unexplained weight loss) plus nonfasting plasma glucose (PG) >200 mg/dL (11.1 mmol/L) |
| OR |
| • Fasting plasma glucose >126 mg/dL (7.0 mmol/L) |
| OR |
| • 2-hour PG >200 mg/dL during an oral glucose tolerance test |
| Source: American Diabetes Association |
Cardiac toxicity
QTc prolongation. Atypical antipsychotics—like their typical counterparts—cause QTc prolongation to varying degrees. On an ECG, the QT interval corresponds to cardiac depolarization and repolarization phases. The QT interval—which changes naturally with the time of day, stressors, and heart rate—is commonly corrected for heart rate to yield QTc.28 If QTc is prolonged beyond a certain threshold, repolarization can occur simultaneously with early depolarization. The consequence may be ventricular arrhythmias, such as torsades de pointes, which can degenerate into ventricular tachycardia, fibrillation, and even death.
All the atypicals are thought to prolong QT intervals to some degree by reducing the flow of repolarizing K+ currents, ultimately making the myocardium more excitable.29 Although there is no specific threshold above which torsades de pointes will occur, it appears there is no significant risk of developing arrhythmias below a QT interval of 500 msec.30 In fact, because the atypicals behave like type IIIa antiarrhythmics, they will overdrive the ventricle and suppress other emergent ventricular arrhythmias. Notwithstanding the FDA’s scrutiny of ziprasidone, no data indicate that this agent is disproportionately toxic.
Clinical precautions. Overall, atypicals cause only a modest increase in the QT interval. Ziprasidone and quetiapine appear to have somewhat more pronounced effects, with ziprasidone prolonging the QT interval on average about 20 msec.31 These mean increases are clinically irrelevant in most patients, but use caution when treating patients who:
- have pre-existing heart disease that is known to be associated with ventricular arrhythmias
- are taking other medications that prolong QT through the same mechanism
- have historically had idiosyncratic sensitivities to prolonged QT.32
Bradycardia, electrolyte imbalances, and endocrine disorders—which themselves increase QTc—also might make an individual more susceptible to the consequences of subtle QT prolongation.29
Managing patients at risk. In our clinic, we assess patients for risk of QT prolongation by inquiring about a family history of cardiac disease or a personal history of arrhythmia, syncope, or near syncope. In at-risk patients, we:
- monitor clinical progress more frequently, focusing on symptoms that suggest syncope or near syncope (unexplained episodic nausea, drowsiness)
- obtain routine ECGs to identify the rare population at increased risk for arrhythmia with either severely prolonged QT (>500 msec) or a serious AV conduction delay at baseline (second-degree or greater).
Laboratory tests should include electrolytes, as hypoleukemia is compellingly associated with development of arrhythmias.
Cardiac toxicity with clozapine. Reports of myocarditis and cardiomyopathy associated with clozapine have raised concern that this agent may be associated with other forms of cardiac toxicity. In January 2002, Novartis Pharmaceuticals Corp. reported 213 cases of myocarditis, 85% of which occurred while patients were taking recommended doses of clozapine within the first 2 months of therapy.33 Eosinophilia in many of the cases indicates that an IgE-mediated hypersensitivity reaction may be involved.34
Novartis also reported 178 cases of clozapineassociated cardiomyopathy, 80% of which occurred in patients younger than 50. Almost 20% of the incidents resulted in death, an alarming figure that may reflect either delay in diagnosis and treatment or simple reporting bias.
Detecting cardiac toxicity is particularly challenging because its manifestations—tachycardia, fatigue, and orthostatic hypotension—are frequently observed in clozapine-treated patients, particularly when dosages are changed.35 The poor specificity of signs for cardiac toxicity requires that we:
- identify at baseline patients with a personal or family history of heart disease
- set our threshold for suspicion of direct cardiotoxicity particularly low when titrating clozapine.36
Hyperprolactinemia
Higher elevations with risperidone. Many antipsychotics cause hyperprolactinemia because their antidopaminergic activity prevents dopamine from inhibiting prolactin secretion. Among the atypicals, however, only risperidone significantly elevates prolactin.37 Caracci et al also demonstrated a two- to four-fold greater prolactin elevation with risperidone than with typical antipsychotics38 and noted that hyperprolactinemia with risperidone could occur at standard daily doses.
We believe that risperidone’s tendency to disperse disproportionately within the plasma space accounts for its differential effect on D2 receptors in the tubuloinfundibular system (brain/plasma ratio of about 0.02 versus approximately 20 for most other antipsychotics). Thus, the lactotrophs, which are outside the blood brain barrier, are exposed to much higher levels of risperidone than are the D2 receptors within the CSF space, resulting in seemingly paradoxical co-occurence of EPS-free hyperprolactinemia.
Table 5
INTERVENTIONS TO CONTROL ANTIPSYCHOTIC-RELATEDWEIGHT GAIN
|
Clinical effects. Elevated prolactin levels do not necessarily lead to clinical symptoms. A large study comparing olanzapine and risperidone found that although more patients receiving risperidone had elevated prolactin levels, few patients in either group reported prolactin-related events such as amenorrhea, galactorrhea, gynecomastia, or sexual side effects.39 Elevated prolactin levels have not been shown to be intrinsically harmful, although they can cause hypogonadism via negative feedback and inhibition of gonadotropin-releasing hormone, leading to inadequate follicle-stimulating hormone and luteinizing hormone.
Hyperprolactinemia also reduces serum testosterone levels in men, which may lead to decreased libido, impotence, infertility, gynecomastia, and rarely galactorrhea.40 Premenopausal women may experience infertility, oligomenorrhea or amenorrhea, galactorrhea, and reduced bone mineral density.41
Treatment options. When patients develop hyperprolactinemia, switching to another antipsychotic is not the only option.42 Standard therapies for hyperprolactinemia—the prodopaminergic drugs bromocriptine and amantadine—are effective, though they may have a slight tendency to provoke or worsen psychosis.43 In our experience, most patients can be managed with judicious dosages of bromocriptine (less than 5 mg/d) or even lower dosages of cabergoline (0.25 mg weekly to twice weekly), which causes very few psychiatric side effects.
Birth control pills are a reasonable alternative for women below age 35 who are nonsmokers—a relatively small proportion of those afflicted with schizophrenia but a much higher proportion of those likely to develop endocrine toxicities.
Sexual dysfunction
Sexual dysfunction—including decreased libido, impaired arousal, and erectile orgasmic dysfunction—is common among patients receiving atypical antipsychotics.44 These effects may be caused by anticholinergic activity, alpha-1 inhibition, and hypogonadism due to hyperprolactinemia.45 Delineating one specific cause of sexual dysfunction can be difficult because:
- antipsychotics are often administered with other psychotropics that influence sexual function
- schizophrenia itself is associated with sexual dysfunction.
The asociality associated with schizophrenia’s negative symptoms may be accompanied by decreased libido, fewer sexual thoughts, and fewer sexual relationships. In surveys, patients treated with atypical antipsychotics tend to report improved sex drive and libido but more erectile dysfunction and anorgasmia.46 Untreated patients report having fewer sexual thoughts and diminished libido but better erectile function and potency.47 The atypicals’ positive effect on social behavior may facilitate a willingness to engage in sexual activity, making sexual dysfunction more apparent.48
Priapism has been reported with all atypicals except ziprasidone.49 The vascular tone of the penis is in part sympathetically mediated, and alpha-1 blockade can inhibit detumescence via its indirect tendency to increase nitric oxide levels.50 Although priapism does not appear to be common, it is a urologic emergency with potential long-term consequences, including permanent erectile dysfunction. Patients developing abnormally prolonged and painful erections must be counseled to seek immediate medical attention.
Aripiprazole: Preliminary impressions
The recently approved antipsychotic aripiprazole differs from the now-familiar dopaminergic theme by being a partial agonist at the D2 receptor. Aripiprazole has the greatest affinity for the D2 receptor of any available drug, activates the postsynaptic complex at about 30% of the full endogenous DA affect, and appears to lack the metabolic consequences of the other atypicals.
In our research laboratory, aripiprazole has shown a profound prolactin lowering effect, superior subjective tolerability, and a more salutary impact on sexual function, compared with other antipsychotics. Although not devoid of EPS, aripiprazole appears to alter a patient’s subjective distress in a way that alters the risk/benefit ratio. Although aripiprazole’s clinical niche has yet to be established, it would be reasonable to use it for overweight patients intolerant of the dysphorogenic effects of other antipsychotics.
Related resources
- Wirshing DA, Wirshing WC, Kysar L, et al. Novel antipsychotics: comparison of weight gain liabilities J Clin Psychiatry 1999;60(6)358-63.
- Wirshing DA, Spellberg B, Erhart SM, Marder SR, Wirshing WC. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44(8):778-83.
- Wirshing DA, Pierre JM, Marder SR, Saunders CS, Wirshing WC. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56(1-2):25-30.
Drug brand names
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Donna Wirshing receives grant/research support from Pfizer Inc., Eli Lilly and Co., Janssen Pharmaceutica, and AstraZeneca Pharmaceuticals; is a consultant to Bristol-Myers Squibb Co., Janssen Pharmaceutica, and Pfizer Inc., and is a speaker for Eli Lilly and Co., Pfizer Inc., and Janssen Pharmaceutica.
Itai Danovitch reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Pierre receives grant/research support from Cephalon Inc.; is a consultant to Eli Lilly and Co., Bristol-Myers Squibb Co., AstraZeneca, and Pfizer Inc.; and is a speaker for Novartis Pharmaceuticals Corp., AstraZeneca Pharmaceuticals, and Janssen Pharmaceutica.
Dr. William Wirshing receives grant/research support from Janssen Pharmaceutica, Eli Lilly and Co., Otsuka America Pharmaceutical, Abbot Laboratories, Pfizer Inc., Sanofi-Synthelabo, Organon, Bristol-Myers Squibb Co., and Knoll Pharmaceuticals, and is a consultant to Janssen Pharmaceutica, Hoechst Marion Roussel, and Eli Lilly and Co.
1. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
2. Henderson D, Cagliero E, Gray C, et al. Clozapine, diabetes mellitus, weight gain and lipid abnormalities: a five year naturalistic study. Am J Psychiatry 2000;157(6):975-81.
3. Kinon BJ, Basson BR, Gilmore JA, et al. Long-term olanzapine treatment: weight change and weight-related health factors in schizophrenia. J Clin Psychiatry 2001;62:92-100.
4. Ganguli R. Weight gain associated with antipsychotic drugs J Clin Psychiatry 1999;60:20-4.
5. McIntyre RS, McCann SM, Kennedy SH. Antipsychotic metabolic effects: weight gain, diabetes mellitus, and lipid abnormalities. Can J Psychiatry 2001;46:273-281.
6. Taylor DM, McAskill R. Atypical antipsychotics and weight gain—a systematic review. Acta Psychiatry Scand 2000;101:416-32.
7. Haapasalo-Pesu KM, Saarijarvi S. Olanzapine induces remarkable weight gain in adolescent patients. Eur Child Adolesc Psychiatry 2001;10:205-8.
8. Martin A, Landau J, Leebens P, et al. Risperidone-associated weight gain in children and adolescents: a retrospective chart review. J Child Adolesc Psychopharmacol 2000;10:259-68.
9. Wirshing DA, Spellberg BJ, Erhart SM, et al. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44:778-83.
10. Bray G. Drug treatment of obesity. Rev Endocr Metab Disord 2001;2(4):403-18.
11. Kaur G, Kulkarni SK. Studies on modulation of feeding behavior by atypical antipsychotics in female mice. Prog Neuropsychopharmacol Biol Psychiatry 2002;26:277-85.
12. Wirshing D, Wirshing W, Kysar L, et al. Novel antipsychotics: Comparison of weight gain liabilities. J Clin Psychiatry 1999;60:358-63.
13. Bray GA, York DA. Clinical review 90: Leptin and clinical medicine: a new piece in the puzzle of obesity. J Clin Endocrinol Metab 1997;82:2771-6.
14. Baptista T, Lacruz A, De Mendoza D, et al. Body weight gain after administration of antipsychotic drugs. Pharmacopsychiatry 2002;35:36.-
15. Helmrich SP, Ragland DR, Leung RW, et al. Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus. N Engl J Med 1991;325:147-52.
16. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
17. Henderson DC. Atypical antipsychotic-induced diabetes mellitus: how strong is the evidence? CNS Drugs 2002;16:77-89.
18. Ramankutty G. Olanzapine-induced destabilization of diabetes in the absence of weight gain. Acta Psychiatry Scand 2002;105:235-7.
19. Muench J, Carey M. Diabetes mellitus associated with atypical antipsychotic medications: new case report and review of the literature. J Am Board Fam Pract 2001;14:278-82.
20. Beck-Nielsen H, Groop LC. Metabolic and genetic characterization of prediabetic states. Sequence of events leading to non-insulin-dependent diabetes mellitus. J Clin Invest 1994-94:1714-21.
21. Wozniak K, Linnoila M. Hyperglycemic properties of serotonin receptor antagonists. Life Sci 1991;49:101-9.
22. Ardizzone TD, Bradley RJ, Freeman AM, 3rd, et al. Inhibition of glucose transport in PC12 cells by the atypical antipsychotic drugs risperidone and clozapine, and structural analogs of clozapine. Brain Res 2001;923:82-90.
23. Wilson PW. Established risk factors and coronary artery disease: the Framingham Study. Am J Hypertens 1994;7:7S-12S.
24. Meyer JM. Novel antipsychotics and severe hyperlipidemia. J Clin Psychopharmacol 2001;21:369-74.
25. Niaura R, Banks SM, Ward KD, et al. Hostility and the metabolic syndrome in older males: the normative aging study. Psychosom Med 2000;62:7-16.
26. Diebold K, Michel G, Schweizer J, et al. Are psychoactive-drug-induced changes in plasma lipid and lipoprotein levels of significance for clinical remission in psychiatric disorders? Pharmacopsychiatry 1998;31:60-7.
27. Bechara CI, Goldman-Levine JD. Dramatic worsening of type 2 diabetes mellitus due to olanzapine after 3 years of therapy. Pharmacotherapy 2001;21:1444-7.
28. Garson A, Jr. How to measure the QT interval—what is normal? Am J Cardiol 1993;72:14B-16B.
29. Tan HL, Hou CJ, Lauer MR, et al. Electrophysiologic mechanisms of the long QT interval syndromes and torsade de pointes. Ann Intern Med 1995;122:701-14.
30. Morganroth J, Brozovich FV, McDonald JT, et al. Variability of the QT measurement in healthy men, with implications for selection of an abnormal QT value to predict drug toxicity and proarrhythmia. Am J Cardiol 1991;67:774-6.
31. Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations: Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations Diabetes Care 2000;23:S4.-
32. Joerg C K-WS, Beasley CM. Cardiac safety parameters of olanzapine: comparison with other atypical and typical antipsychotics. J Clin Psychiatry 2001;2:35-40.
33. Association of Clozaril with cardiovascular toxicity. [Dear healthcare professional letter]. Novartis Pharmaceuticals Canada Inc, 2002.
34. Killian JG, Kerr K, Lawrence C. Myocarditis and cardiomyopathy associated with clozapine. Lancet 1999;354:1841-5.
35. Lieberman JA, Safferman AZ. Clinical profile of clozapine: adverse reactions and agranulocytosis. Psychiatr Q 1992;63:51-70.
36. Wooltorton E. Antipsychotic clozapine (Clozaril): myocarditis and cardiovascular toxicity. CMAJ 2002;166:1185-6.
37. Breier AF, Malhotra AK, Su T, et al. Clozapine and risperidone in chronic schizophrenia: effects on symptoms, parkinsonian side effects, and neuroendocrine response. Am J Psychiatry 1999;156:294-8.
38. Caracci G. Prolactin levels in premenopausal women treated with risperidone compared with those of women treated with typical neuroleptics. J Clin Psychopharmacology 1999;19:194-6.
39. Conley RR, Mahmoud R. A randomized double-blind study of risperidone and olanzapine in the treatment of schizophrenia or schizoaffective disorder. Am J Psychiatry 2001;158:765-74.
40. Segal S, Yaffe H, Laufer N, et al. Male hyperprolactinemia: effects on fertility. Fertil Steril 1979;32:556-61.
41. Schlechte J, Walkner L, Kathol M. A longitudinal analysis of premenopausal bone loss in healthy women and women with hyperprolactinemia. J Clin Endocrinol Metab 1992;75:698-703.
42. Gazzola LR, Opler LA. Return of menstruation after switching from risperidone to olanzapine. J Clin Psychopharmacol 1998;18:486-7.
43. Boyd A. Bromocriptine and psychosis: a literature review. Psychiatr Q 1995;66:87-95.
44. Aizenberg D, Modai I, Landa A, et al. Comparison of sexual dysfunction in male schizophrenic patients maintained on treatment with classical antipsychotics versus clozapine. J Clin Psychiatry 2001;62:541-4.
45. Meston CM. Sympathetic nervous system activity and female sexual arousal. Am J Cardiol 2000;86:30F-34F.
46. Wirshing DA, Pierre JM, Marder SR, et al. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56:25-30.
47. Aizenberg D, Zemishlany Z, Dorfman-Etrog P, et al. Sexual dysfunction in male schizophrenic patients. J Clin Psychiatry 1995;56:137-41.
48. Hummer M, Kemmler G, Kurz M, et al. Sexual disturbances during clozapine and haloperidol treatment for schizophrenia. Am J Psychiatry 1999;156:631-3.
49. Pais VM, Ayvazian PJ. Priapism from quetiapine overdose: first report and proposal of mechanism. Urology 2001;58:462.-
50. Compton MT, Miller AH. Priapism associated with conventional and atypical antipsychotic medications: a review. J Clin Psychiatry 2001;62:362-6.
Atypical antipsychotics are powerful medications for acute and chronic psychotic disorders, with a similarly powerful potential for adverse systemic effects. To use these agents to their greatest advantage, we must balance the benefits against the risks.
We often see patients with weight gain, diabetes, dyslipidemia, cardiac toxicity, hyperprolactinemia, and sexual dysfunction—all possible effects of atypical antipsychotics. Based on the latest evidence and our experience, we offer tips for using clozapine, olanzapine, quetiapine, risperidone, and ziprasidone, and preliminary impressions about the newly approved agent, aripiprazole.
Weight gain
Clinical trials have shown convincingly that atypical antipsychotics pose a greater risk of weight gain and central adiposity than do most older antipsychotics.1 Overweight and obesity are associated with increased risks of hypertension, type 2 diabetes, coronary heart disease, stroke, gallbladder disease, osteoarthritis, and some forms of cancer. Moreover, obesity’s socially stigmatizing effect can discourage patients with schizophrenia—particularly adolescents—from taking their medication.
Table 1
POTENTIAL FOR ADVERSE EFFECTS WITH ATYPICAL ANTIPSYCHOTICS
| Metabolic changes | Weight gain | Increased prolactin | QT interval | EPS | Sedation | Orthostasis | |
|---|---|---|---|---|---|---|---|
| Risperidone | + | + | +++ | + | ++ | + | ++ |
| Ziprasidone | + | + | − | ++ | + | + | + |
| Clozapine | +++ | +++ | − | ++ | +/− | +++ | +++ |
| Olanzapine | +++ | +++ | − | + | + | ++ | + |
| Quetiapine | ++ | ++ | − | ++ | + | ++ | ++ |
| Aripiprazole | + | + | − | + | + | +/− | +/− |
Comparative effects. Olanzapine and clozapine are associated with greater weight gain (Table 1)1-3 than risperidone and ziprasidone.4 Data regarding quetiapine are inconsistent—some studies show weight gain similar to that caused by olanzapine, and others find much less.5 Weight gain associated with quetiapine, ziprasidone, and risperidone tends to plateau within the first few months, whereas patients taking olanzapine and clozapine may continue to gain weight for 9 months or more.6
Adolescents and young adults may be particularly susceptible to antipsychotic-induced weight gain.7 No studies have directly compared weight gain in adults versus adolescents, but adolescents are exceedingly susceptible to the atypicals’ metabolic dysregulation. For example:
- A higher prevalence of extreme weight gain (>7% of baseline body mass) with olanzapine and risperidone has been reported in adolescent inpatients than among adults.7
- Extreme weight gain was seen in 78% of a group of risperidone-treated children; for 6 months, their weight gain averaged 1.2 kg/month without leveling off.8
These findings suggest that risperidone’s apparent metabolic advantage in adults disappears in children and adolescents. Risperidone’s effect on prolactin may account for a higher risk of weight gain in younger patients. These populations have exquisite end-organ sensitivity to changes in prolactin levels and may be more susceptible to the weight gain—and perhaps diabetes—believed related to hyperprolactinemia.9
Mechanisms. The mechanism(s) of weight gain may be related to the receptor systems upon which the atypicals act. These agents block noradrenergic, dopamine, serotonin, and histamine receptors, all of which are thought to affect metabolism or appetite control. Stimulation of alpha and D2 receptors by sympathomimetic amines causes weight loss, as does stimulation of certain 5HT receptors by weight-loss drugs such as fenfluramine.10 With respect to appetite, it has been suggested that peripheral antagonism of H1 receptors interferes with normal satiety signals.11 This may explain why affinity to histamine H1 receptors is among the best of correlates with potential for weight gain.12
Increases in serum levels of leptin—a peptide hormone produced in direct proportion to adiposity and thought to be anorexigenic, possibly through effects on satiety13 —parallel weight gain during treatment with atypicals. However, there is no indication that leptin imbalance causes weight gain; it may instead be the result. Altered sensitivity to leptin may be a contributing factor, perhaps at the hypothalamus.14
Diabetes
The risk of type 2 diabetes increases with weight gain,15 so it is no surprise that diabetes is more prevalent among patients taking atypicals. In a study of 38,000 schizophrenic patients, those taking atypicals were 9% more likely to have diabetes than those receiving typical antipsychotics,16 and all atypicals were associated with a significant increase in diabetes risk in patients younger than 40. The pervasiveness of diabetes17 and reports of new-onset diabetes in non-overweight patients18 suggest that—in addition to their effect on weight—atypicals may alter insulin and glucose metabolism.19
Atypical antipsychotics probably increase diabetes risk in a number of ways:
- An increase in adipose tissue can lead to insulin resistance, glucose intolerance, and ultimately diabetes.20
- Serotonin receptor antagonism may lead to hyperglycemia by decreasing pancreatic beta cell response to signals that advance insulin production.21
- Atypicals may contribute to hyperglycemia by impeding cellular uptake of glucose.22
- The increase in free fatty acids associated with atypicals can alter glucose metabolism. This may explain why clozapine and olanzapine—the atypicals with the greatest potential for severe hyperlipidemia—have the strongest association with new-onset diabetes.
Hyperlipidemia
Case reports and controlled studies have linked atypical antipsychotics with hyperlipidemia. Whether the hyperlipidemia is a consequence of weight gain or some other metabolic disturbance is unknown. Even without conclusive data, however, the link is of concern because elevated triglyceride levels represent an independent risk factor for heart disease.23
Although all atypicals increase serum triglycerides to some degree, severe hypertriglyceridemia occurs predominantly with clozapine and olanzapine.24 Both drugs have favorable efficacy profiles, and the mechanism of their antipsychotic activity may include altering the various lipid pools.
For example, studies have found that decreased triglyceride levels correlate with hostility and psychological distress.25 Increased triglycerides have been theorized to enhance membrane fluidity, which in turn may augment presynaptic reuptake of serotonin and diminish postsynaptic serotonin activity.26 In other words, elevated triglyceride levels could play a role in atypical antipsychotic-mediated inhibition of serotonin transmission. It is not yet known whether lipid-lowering drugs might alter atypicals’ efficacy.
Table 2
RECOMMENDED METABOLIC MONITORING OF PATIENTS TAKING ATYPICAL ANTIPSYCHOTICS
| Every visit | Check weight Check blood pressure |
| Every 3 months | Fasting blood glucose Fasting triglycerides Fasting cholesterol |
Metabolic monitoring
Managing mental illness concurrently with weight gain, diabetes, and hypertriglyceridemia is a challenge. In our clinic, we try to diminish the atypicals’ adverse metabolic effects by monitoring a few basic parameters and taking preventive measures (Table 2).
We routinely screen patients for diabetes symptoms by asking questions about changes in belt size (a sign of weight change), urinary frequency, and thirst (Table 3). We also document baseline weight, blood glucose (Table 4), blood chemistry, and lipid levels, with routine follow-up throughout therapy and greatest scrutiny during the first months of a new treatment.
Patients who cannot control their weight with lifestyle modifications (Table 5) may require a lipid-lowering medication—a “stain” and/or fibrate (such as gemfibrozil)—or, if those measures are ineffective, a switch to another antipsychotic. Hyperlipidemia and hyperglycemia may be reduced substantially when patients discontinue the aggravating medication.27
Although discontinuing or switching medications may reduce metabolic side effects, the hazard of psychotic decompensation is substantial. Achieving an antipsychotic effect is extremely difficult for most patients, and one should not discontinue an effective treatment without seriously considering the consequences. Antipsychotic efficacy should never be sacrificed in the pursuit of a regimen with more benign side effects. Consider switching to an atypical with a more moderate effect on weight, however, if weight gain would likely lead to noncompliance. Even the most effective treatment will not work if a patient never takes it.
Table 3
5 SCREENING QUESTIONS TO MONITOR FOR METABOLIC AND SEXUAL SIDE EFFECTS
|
Table 4
DIAGNOSTIC CRITERIA FOR DIABETES
| • Symptoms of diabetes (such as polyuria, polydipsia, or unexplained weight loss) plus nonfasting plasma glucose (PG) >200 mg/dL (11.1 mmol/L) |
| OR |
| • Fasting plasma glucose >126 mg/dL (7.0 mmol/L) |
| OR |
| • 2-hour PG >200 mg/dL during an oral glucose tolerance test |
| Source: American Diabetes Association |
Cardiac toxicity
QTc prolongation. Atypical antipsychotics—like their typical counterparts—cause QTc prolongation to varying degrees. On an ECG, the QT interval corresponds to cardiac depolarization and repolarization phases. The QT interval—which changes naturally with the time of day, stressors, and heart rate—is commonly corrected for heart rate to yield QTc.28 If QTc is prolonged beyond a certain threshold, repolarization can occur simultaneously with early depolarization. The consequence may be ventricular arrhythmias, such as torsades de pointes, which can degenerate into ventricular tachycardia, fibrillation, and even death.
All the atypicals are thought to prolong QT intervals to some degree by reducing the flow of repolarizing K+ currents, ultimately making the myocardium more excitable.29 Although there is no specific threshold above which torsades de pointes will occur, it appears there is no significant risk of developing arrhythmias below a QT interval of 500 msec.30 In fact, because the atypicals behave like type IIIa antiarrhythmics, they will overdrive the ventricle and suppress other emergent ventricular arrhythmias. Notwithstanding the FDA’s scrutiny of ziprasidone, no data indicate that this agent is disproportionately toxic.
Clinical precautions. Overall, atypicals cause only a modest increase in the QT interval. Ziprasidone and quetiapine appear to have somewhat more pronounced effects, with ziprasidone prolonging the QT interval on average about 20 msec.31 These mean increases are clinically irrelevant in most patients, but use caution when treating patients who:
- have pre-existing heart disease that is known to be associated with ventricular arrhythmias
- are taking other medications that prolong QT through the same mechanism
- have historically had idiosyncratic sensitivities to prolonged QT.32
Bradycardia, electrolyte imbalances, and endocrine disorders—which themselves increase QTc—also might make an individual more susceptible to the consequences of subtle QT prolongation.29
Managing patients at risk. In our clinic, we assess patients for risk of QT prolongation by inquiring about a family history of cardiac disease or a personal history of arrhythmia, syncope, or near syncope. In at-risk patients, we:
- monitor clinical progress more frequently, focusing on symptoms that suggest syncope or near syncope (unexplained episodic nausea, drowsiness)
- obtain routine ECGs to identify the rare population at increased risk for arrhythmia with either severely prolonged QT (>500 msec) or a serious AV conduction delay at baseline (second-degree or greater).
Laboratory tests should include electrolytes, as hypoleukemia is compellingly associated with development of arrhythmias.
Cardiac toxicity with clozapine. Reports of myocarditis and cardiomyopathy associated with clozapine have raised concern that this agent may be associated with other forms of cardiac toxicity. In January 2002, Novartis Pharmaceuticals Corp. reported 213 cases of myocarditis, 85% of which occurred while patients were taking recommended doses of clozapine within the first 2 months of therapy.33 Eosinophilia in many of the cases indicates that an IgE-mediated hypersensitivity reaction may be involved.34
Novartis also reported 178 cases of clozapineassociated cardiomyopathy, 80% of which occurred in patients younger than 50. Almost 20% of the incidents resulted in death, an alarming figure that may reflect either delay in diagnosis and treatment or simple reporting bias.
Detecting cardiac toxicity is particularly challenging because its manifestations—tachycardia, fatigue, and orthostatic hypotension—are frequently observed in clozapine-treated patients, particularly when dosages are changed.35 The poor specificity of signs for cardiac toxicity requires that we:
- identify at baseline patients with a personal or family history of heart disease
- set our threshold for suspicion of direct cardiotoxicity particularly low when titrating clozapine.36
Hyperprolactinemia
Higher elevations with risperidone. Many antipsychotics cause hyperprolactinemia because their antidopaminergic activity prevents dopamine from inhibiting prolactin secretion. Among the atypicals, however, only risperidone significantly elevates prolactin.37 Caracci et al also demonstrated a two- to four-fold greater prolactin elevation with risperidone than with typical antipsychotics38 and noted that hyperprolactinemia with risperidone could occur at standard daily doses.
We believe that risperidone’s tendency to disperse disproportionately within the plasma space accounts for its differential effect on D2 receptors in the tubuloinfundibular system (brain/plasma ratio of about 0.02 versus approximately 20 for most other antipsychotics). Thus, the lactotrophs, which are outside the blood brain barrier, are exposed to much higher levels of risperidone than are the D2 receptors within the CSF space, resulting in seemingly paradoxical co-occurence of EPS-free hyperprolactinemia.
Table 5
INTERVENTIONS TO CONTROL ANTIPSYCHOTIC-RELATEDWEIGHT GAIN
|
Clinical effects. Elevated prolactin levels do not necessarily lead to clinical symptoms. A large study comparing olanzapine and risperidone found that although more patients receiving risperidone had elevated prolactin levels, few patients in either group reported prolactin-related events such as amenorrhea, galactorrhea, gynecomastia, or sexual side effects.39 Elevated prolactin levels have not been shown to be intrinsically harmful, although they can cause hypogonadism via negative feedback and inhibition of gonadotropin-releasing hormone, leading to inadequate follicle-stimulating hormone and luteinizing hormone.
Hyperprolactinemia also reduces serum testosterone levels in men, which may lead to decreased libido, impotence, infertility, gynecomastia, and rarely galactorrhea.40 Premenopausal women may experience infertility, oligomenorrhea or amenorrhea, galactorrhea, and reduced bone mineral density.41
Treatment options. When patients develop hyperprolactinemia, switching to another antipsychotic is not the only option.42 Standard therapies for hyperprolactinemia—the prodopaminergic drugs bromocriptine and amantadine—are effective, though they may have a slight tendency to provoke or worsen psychosis.43 In our experience, most patients can be managed with judicious dosages of bromocriptine (less than 5 mg/d) or even lower dosages of cabergoline (0.25 mg weekly to twice weekly), which causes very few psychiatric side effects.
Birth control pills are a reasonable alternative for women below age 35 who are nonsmokers—a relatively small proportion of those afflicted with schizophrenia but a much higher proportion of those likely to develop endocrine toxicities.
Sexual dysfunction
Sexual dysfunction—including decreased libido, impaired arousal, and erectile orgasmic dysfunction—is common among patients receiving atypical antipsychotics.44 These effects may be caused by anticholinergic activity, alpha-1 inhibition, and hypogonadism due to hyperprolactinemia.45 Delineating one specific cause of sexual dysfunction can be difficult because:
- antipsychotics are often administered with other psychotropics that influence sexual function
- schizophrenia itself is associated with sexual dysfunction.
The asociality associated with schizophrenia’s negative symptoms may be accompanied by decreased libido, fewer sexual thoughts, and fewer sexual relationships. In surveys, patients treated with atypical antipsychotics tend to report improved sex drive and libido but more erectile dysfunction and anorgasmia.46 Untreated patients report having fewer sexual thoughts and diminished libido but better erectile function and potency.47 The atypicals’ positive effect on social behavior may facilitate a willingness to engage in sexual activity, making sexual dysfunction more apparent.48
Priapism has been reported with all atypicals except ziprasidone.49 The vascular tone of the penis is in part sympathetically mediated, and alpha-1 blockade can inhibit detumescence via its indirect tendency to increase nitric oxide levels.50 Although priapism does not appear to be common, it is a urologic emergency with potential long-term consequences, including permanent erectile dysfunction. Patients developing abnormally prolonged and painful erections must be counseled to seek immediate medical attention.
Aripiprazole: Preliminary impressions
The recently approved antipsychotic aripiprazole differs from the now-familiar dopaminergic theme by being a partial agonist at the D2 receptor. Aripiprazole has the greatest affinity for the D2 receptor of any available drug, activates the postsynaptic complex at about 30% of the full endogenous DA affect, and appears to lack the metabolic consequences of the other atypicals.
In our research laboratory, aripiprazole has shown a profound prolactin lowering effect, superior subjective tolerability, and a more salutary impact on sexual function, compared with other antipsychotics. Although not devoid of EPS, aripiprazole appears to alter a patient’s subjective distress in a way that alters the risk/benefit ratio. Although aripiprazole’s clinical niche has yet to be established, it would be reasonable to use it for overweight patients intolerant of the dysphorogenic effects of other antipsychotics.
Related resources
- Wirshing DA, Wirshing WC, Kysar L, et al. Novel antipsychotics: comparison of weight gain liabilities J Clin Psychiatry 1999;60(6)358-63.
- Wirshing DA, Spellberg B, Erhart SM, Marder SR, Wirshing WC. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44(8):778-83.
- Wirshing DA, Pierre JM, Marder SR, Saunders CS, Wirshing WC. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56(1-2):25-30.
Drug brand names
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Donna Wirshing receives grant/research support from Pfizer Inc., Eli Lilly and Co., Janssen Pharmaceutica, and AstraZeneca Pharmaceuticals; is a consultant to Bristol-Myers Squibb Co., Janssen Pharmaceutica, and Pfizer Inc., and is a speaker for Eli Lilly and Co., Pfizer Inc., and Janssen Pharmaceutica.
Itai Danovitch reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Pierre receives grant/research support from Cephalon Inc.; is a consultant to Eli Lilly and Co., Bristol-Myers Squibb Co., AstraZeneca, and Pfizer Inc.; and is a speaker for Novartis Pharmaceuticals Corp., AstraZeneca Pharmaceuticals, and Janssen Pharmaceutica.
Dr. William Wirshing receives grant/research support from Janssen Pharmaceutica, Eli Lilly and Co., Otsuka America Pharmaceutical, Abbot Laboratories, Pfizer Inc., Sanofi-Synthelabo, Organon, Bristol-Myers Squibb Co., and Knoll Pharmaceuticals, and is a consultant to Janssen Pharmaceutica, Hoechst Marion Roussel, and Eli Lilly and Co.
Atypical antipsychotics are powerful medications for acute and chronic psychotic disorders, with a similarly powerful potential for adverse systemic effects. To use these agents to their greatest advantage, we must balance the benefits against the risks.
We often see patients with weight gain, diabetes, dyslipidemia, cardiac toxicity, hyperprolactinemia, and sexual dysfunction—all possible effects of atypical antipsychotics. Based on the latest evidence and our experience, we offer tips for using clozapine, olanzapine, quetiapine, risperidone, and ziprasidone, and preliminary impressions about the newly approved agent, aripiprazole.
Weight gain
Clinical trials have shown convincingly that atypical antipsychotics pose a greater risk of weight gain and central adiposity than do most older antipsychotics.1 Overweight and obesity are associated with increased risks of hypertension, type 2 diabetes, coronary heart disease, stroke, gallbladder disease, osteoarthritis, and some forms of cancer. Moreover, obesity’s socially stigmatizing effect can discourage patients with schizophrenia—particularly adolescents—from taking their medication.
Table 1
POTENTIAL FOR ADVERSE EFFECTS WITH ATYPICAL ANTIPSYCHOTICS
| Metabolic changes | Weight gain | Increased prolactin | QT interval | EPS | Sedation | Orthostasis | |
|---|---|---|---|---|---|---|---|
| Risperidone | + | + | +++ | + | ++ | + | ++ |
| Ziprasidone | + | + | − | ++ | + | + | + |
| Clozapine | +++ | +++ | − | ++ | +/− | +++ | +++ |
| Olanzapine | +++ | +++ | − | + | + | ++ | + |
| Quetiapine | ++ | ++ | − | ++ | + | ++ | ++ |
| Aripiprazole | + | + | − | + | + | +/− | +/− |
Comparative effects. Olanzapine and clozapine are associated with greater weight gain (Table 1)1-3 than risperidone and ziprasidone.4 Data regarding quetiapine are inconsistent—some studies show weight gain similar to that caused by olanzapine, and others find much less.5 Weight gain associated with quetiapine, ziprasidone, and risperidone tends to plateau within the first few months, whereas patients taking olanzapine and clozapine may continue to gain weight for 9 months or more.6
Adolescents and young adults may be particularly susceptible to antipsychotic-induced weight gain.7 No studies have directly compared weight gain in adults versus adolescents, but adolescents are exceedingly susceptible to the atypicals’ metabolic dysregulation. For example:
- A higher prevalence of extreme weight gain (>7% of baseline body mass) with olanzapine and risperidone has been reported in adolescent inpatients than among adults.7
- Extreme weight gain was seen in 78% of a group of risperidone-treated children; for 6 months, their weight gain averaged 1.2 kg/month without leveling off.8
These findings suggest that risperidone’s apparent metabolic advantage in adults disappears in children and adolescents. Risperidone’s effect on prolactin may account for a higher risk of weight gain in younger patients. These populations have exquisite end-organ sensitivity to changes in prolactin levels and may be more susceptible to the weight gain—and perhaps diabetes—believed related to hyperprolactinemia.9
Mechanisms. The mechanism(s) of weight gain may be related to the receptor systems upon which the atypicals act. These agents block noradrenergic, dopamine, serotonin, and histamine receptors, all of which are thought to affect metabolism or appetite control. Stimulation of alpha and D2 receptors by sympathomimetic amines causes weight loss, as does stimulation of certain 5HT receptors by weight-loss drugs such as fenfluramine.10 With respect to appetite, it has been suggested that peripheral antagonism of H1 receptors interferes with normal satiety signals.11 This may explain why affinity to histamine H1 receptors is among the best of correlates with potential for weight gain.12
Increases in serum levels of leptin—a peptide hormone produced in direct proportion to adiposity and thought to be anorexigenic, possibly through effects on satiety13 —parallel weight gain during treatment with atypicals. However, there is no indication that leptin imbalance causes weight gain; it may instead be the result. Altered sensitivity to leptin may be a contributing factor, perhaps at the hypothalamus.14
Diabetes
The risk of type 2 diabetes increases with weight gain,15 so it is no surprise that diabetes is more prevalent among patients taking atypicals. In a study of 38,000 schizophrenic patients, those taking atypicals were 9% more likely to have diabetes than those receiving typical antipsychotics,16 and all atypicals were associated with a significant increase in diabetes risk in patients younger than 40. The pervasiveness of diabetes17 and reports of new-onset diabetes in non-overweight patients18 suggest that—in addition to their effect on weight—atypicals may alter insulin and glucose metabolism.19
Atypical antipsychotics probably increase diabetes risk in a number of ways:
- An increase in adipose tissue can lead to insulin resistance, glucose intolerance, and ultimately diabetes.20
- Serotonin receptor antagonism may lead to hyperglycemia by decreasing pancreatic beta cell response to signals that advance insulin production.21
- Atypicals may contribute to hyperglycemia by impeding cellular uptake of glucose.22
- The increase in free fatty acids associated with atypicals can alter glucose metabolism. This may explain why clozapine and olanzapine—the atypicals with the greatest potential for severe hyperlipidemia—have the strongest association with new-onset diabetes.
Hyperlipidemia
Case reports and controlled studies have linked atypical antipsychotics with hyperlipidemia. Whether the hyperlipidemia is a consequence of weight gain or some other metabolic disturbance is unknown. Even without conclusive data, however, the link is of concern because elevated triglyceride levels represent an independent risk factor for heart disease.23
Although all atypicals increase serum triglycerides to some degree, severe hypertriglyceridemia occurs predominantly with clozapine and olanzapine.24 Both drugs have favorable efficacy profiles, and the mechanism of their antipsychotic activity may include altering the various lipid pools.
For example, studies have found that decreased triglyceride levels correlate with hostility and psychological distress.25 Increased triglycerides have been theorized to enhance membrane fluidity, which in turn may augment presynaptic reuptake of serotonin and diminish postsynaptic serotonin activity.26 In other words, elevated triglyceride levels could play a role in atypical antipsychotic-mediated inhibition of serotonin transmission. It is not yet known whether lipid-lowering drugs might alter atypicals’ efficacy.
Table 2
RECOMMENDED METABOLIC MONITORING OF PATIENTS TAKING ATYPICAL ANTIPSYCHOTICS
| Every visit | Check weight Check blood pressure |
| Every 3 months | Fasting blood glucose Fasting triglycerides Fasting cholesterol |
Metabolic monitoring
Managing mental illness concurrently with weight gain, diabetes, and hypertriglyceridemia is a challenge. In our clinic, we try to diminish the atypicals’ adverse metabolic effects by monitoring a few basic parameters and taking preventive measures (Table 2).
We routinely screen patients for diabetes symptoms by asking questions about changes in belt size (a sign of weight change), urinary frequency, and thirst (Table 3). We also document baseline weight, blood glucose (Table 4), blood chemistry, and lipid levels, with routine follow-up throughout therapy and greatest scrutiny during the first months of a new treatment.
Patients who cannot control their weight with lifestyle modifications (Table 5) may require a lipid-lowering medication—a “stain” and/or fibrate (such as gemfibrozil)—or, if those measures are ineffective, a switch to another antipsychotic. Hyperlipidemia and hyperglycemia may be reduced substantially when patients discontinue the aggravating medication.27
Although discontinuing or switching medications may reduce metabolic side effects, the hazard of psychotic decompensation is substantial. Achieving an antipsychotic effect is extremely difficult for most patients, and one should not discontinue an effective treatment without seriously considering the consequences. Antipsychotic efficacy should never be sacrificed in the pursuit of a regimen with more benign side effects. Consider switching to an atypical with a more moderate effect on weight, however, if weight gain would likely lead to noncompliance. Even the most effective treatment will not work if a patient never takes it.
Table 3
5 SCREENING QUESTIONS TO MONITOR FOR METABOLIC AND SEXUAL SIDE EFFECTS
|
Table 4
DIAGNOSTIC CRITERIA FOR DIABETES
| • Symptoms of diabetes (such as polyuria, polydipsia, or unexplained weight loss) plus nonfasting plasma glucose (PG) >200 mg/dL (11.1 mmol/L) |
| OR |
| • Fasting plasma glucose >126 mg/dL (7.0 mmol/L) |
| OR |
| • 2-hour PG >200 mg/dL during an oral glucose tolerance test |
| Source: American Diabetes Association |
Cardiac toxicity
QTc prolongation. Atypical antipsychotics—like their typical counterparts—cause QTc prolongation to varying degrees. On an ECG, the QT interval corresponds to cardiac depolarization and repolarization phases. The QT interval—which changes naturally with the time of day, stressors, and heart rate—is commonly corrected for heart rate to yield QTc.28 If QTc is prolonged beyond a certain threshold, repolarization can occur simultaneously with early depolarization. The consequence may be ventricular arrhythmias, such as torsades de pointes, which can degenerate into ventricular tachycardia, fibrillation, and even death.
All the atypicals are thought to prolong QT intervals to some degree by reducing the flow of repolarizing K+ currents, ultimately making the myocardium more excitable.29 Although there is no specific threshold above which torsades de pointes will occur, it appears there is no significant risk of developing arrhythmias below a QT interval of 500 msec.30 In fact, because the atypicals behave like type IIIa antiarrhythmics, they will overdrive the ventricle and suppress other emergent ventricular arrhythmias. Notwithstanding the FDA’s scrutiny of ziprasidone, no data indicate that this agent is disproportionately toxic.
Clinical precautions. Overall, atypicals cause only a modest increase in the QT interval. Ziprasidone and quetiapine appear to have somewhat more pronounced effects, with ziprasidone prolonging the QT interval on average about 20 msec.31 These mean increases are clinically irrelevant in most patients, but use caution when treating patients who:
- have pre-existing heart disease that is known to be associated with ventricular arrhythmias
- are taking other medications that prolong QT through the same mechanism
- have historically had idiosyncratic sensitivities to prolonged QT.32
Bradycardia, electrolyte imbalances, and endocrine disorders—which themselves increase QTc—also might make an individual more susceptible to the consequences of subtle QT prolongation.29
Managing patients at risk. In our clinic, we assess patients for risk of QT prolongation by inquiring about a family history of cardiac disease or a personal history of arrhythmia, syncope, or near syncope. In at-risk patients, we:
- monitor clinical progress more frequently, focusing on symptoms that suggest syncope or near syncope (unexplained episodic nausea, drowsiness)
- obtain routine ECGs to identify the rare population at increased risk for arrhythmia with either severely prolonged QT (>500 msec) or a serious AV conduction delay at baseline (second-degree or greater).
Laboratory tests should include electrolytes, as hypoleukemia is compellingly associated with development of arrhythmias.
Cardiac toxicity with clozapine. Reports of myocarditis and cardiomyopathy associated with clozapine have raised concern that this agent may be associated with other forms of cardiac toxicity. In January 2002, Novartis Pharmaceuticals Corp. reported 213 cases of myocarditis, 85% of which occurred while patients were taking recommended doses of clozapine within the first 2 months of therapy.33 Eosinophilia in many of the cases indicates that an IgE-mediated hypersensitivity reaction may be involved.34
Novartis also reported 178 cases of clozapineassociated cardiomyopathy, 80% of which occurred in patients younger than 50. Almost 20% of the incidents resulted in death, an alarming figure that may reflect either delay in diagnosis and treatment or simple reporting bias.
Detecting cardiac toxicity is particularly challenging because its manifestations—tachycardia, fatigue, and orthostatic hypotension—are frequently observed in clozapine-treated patients, particularly when dosages are changed.35 The poor specificity of signs for cardiac toxicity requires that we:
- identify at baseline patients with a personal or family history of heart disease
- set our threshold for suspicion of direct cardiotoxicity particularly low when titrating clozapine.36
Hyperprolactinemia
Higher elevations with risperidone. Many antipsychotics cause hyperprolactinemia because their antidopaminergic activity prevents dopamine from inhibiting prolactin secretion. Among the atypicals, however, only risperidone significantly elevates prolactin.37 Caracci et al also demonstrated a two- to four-fold greater prolactin elevation with risperidone than with typical antipsychotics38 and noted that hyperprolactinemia with risperidone could occur at standard daily doses.
We believe that risperidone’s tendency to disperse disproportionately within the plasma space accounts for its differential effect on D2 receptors in the tubuloinfundibular system (brain/plasma ratio of about 0.02 versus approximately 20 for most other antipsychotics). Thus, the lactotrophs, which are outside the blood brain barrier, are exposed to much higher levels of risperidone than are the D2 receptors within the CSF space, resulting in seemingly paradoxical co-occurence of EPS-free hyperprolactinemia.
Table 5
INTERVENTIONS TO CONTROL ANTIPSYCHOTIC-RELATEDWEIGHT GAIN
|
Clinical effects. Elevated prolactin levels do not necessarily lead to clinical symptoms. A large study comparing olanzapine and risperidone found that although more patients receiving risperidone had elevated prolactin levels, few patients in either group reported prolactin-related events such as amenorrhea, galactorrhea, gynecomastia, or sexual side effects.39 Elevated prolactin levels have not been shown to be intrinsically harmful, although they can cause hypogonadism via negative feedback and inhibition of gonadotropin-releasing hormone, leading to inadequate follicle-stimulating hormone and luteinizing hormone.
Hyperprolactinemia also reduces serum testosterone levels in men, which may lead to decreased libido, impotence, infertility, gynecomastia, and rarely galactorrhea.40 Premenopausal women may experience infertility, oligomenorrhea or amenorrhea, galactorrhea, and reduced bone mineral density.41
Treatment options. When patients develop hyperprolactinemia, switching to another antipsychotic is not the only option.42 Standard therapies for hyperprolactinemia—the prodopaminergic drugs bromocriptine and amantadine—are effective, though they may have a slight tendency to provoke or worsen psychosis.43 In our experience, most patients can be managed with judicious dosages of bromocriptine (less than 5 mg/d) or even lower dosages of cabergoline (0.25 mg weekly to twice weekly), which causes very few psychiatric side effects.
Birth control pills are a reasonable alternative for women below age 35 who are nonsmokers—a relatively small proportion of those afflicted with schizophrenia but a much higher proportion of those likely to develop endocrine toxicities.
Sexual dysfunction
Sexual dysfunction—including decreased libido, impaired arousal, and erectile orgasmic dysfunction—is common among patients receiving atypical antipsychotics.44 These effects may be caused by anticholinergic activity, alpha-1 inhibition, and hypogonadism due to hyperprolactinemia.45 Delineating one specific cause of sexual dysfunction can be difficult because:
- antipsychotics are often administered with other psychotropics that influence sexual function
- schizophrenia itself is associated with sexual dysfunction.
The asociality associated with schizophrenia’s negative symptoms may be accompanied by decreased libido, fewer sexual thoughts, and fewer sexual relationships. In surveys, patients treated with atypical antipsychotics tend to report improved sex drive and libido but more erectile dysfunction and anorgasmia.46 Untreated patients report having fewer sexual thoughts and diminished libido but better erectile function and potency.47 The atypicals’ positive effect on social behavior may facilitate a willingness to engage in sexual activity, making sexual dysfunction more apparent.48
Priapism has been reported with all atypicals except ziprasidone.49 The vascular tone of the penis is in part sympathetically mediated, and alpha-1 blockade can inhibit detumescence via its indirect tendency to increase nitric oxide levels.50 Although priapism does not appear to be common, it is a urologic emergency with potential long-term consequences, including permanent erectile dysfunction. Patients developing abnormally prolonged and painful erections must be counseled to seek immediate medical attention.
Aripiprazole: Preliminary impressions
The recently approved antipsychotic aripiprazole differs from the now-familiar dopaminergic theme by being a partial agonist at the D2 receptor. Aripiprazole has the greatest affinity for the D2 receptor of any available drug, activates the postsynaptic complex at about 30% of the full endogenous DA affect, and appears to lack the metabolic consequences of the other atypicals.
In our research laboratory, aripiprazole has shown a profound prolactin lowering effect, superior subjective tolerability, and a more salutary impact on sexual function, compared with other antipsychotics. Although not devoid of EPS, aripiprazole appears to alter a patient’s subjective distress in a way that alters the risk/benefit ratio. Although aripiprazole’s clinical niche has yet to be established, it would be reasonable to use it for overweight patients intolerant of the dysphorogenic effects of other antipsychotics.
Related resources
- Wirshing DA, Wirshing WC, Kysar L, et al. Novel antipsychotics: comparison of weight gain liabilities J Clin Psychiatry 1999;60(6)358-63.
- Wirshing DA, Spellberg B, Erhart SM, Marder SR, Wirshing WC. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44(8):778-83.
- Wirshing DA, Pierre JM, Marder SR, Saunders CS, Wirshing WC. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56(1-2):25-30.
Drug brand names
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Donna Wirshing receives grant/research support from Pfizer Inc., Eli Lilly and Co., Janssen Pharmaceutica, and AstraZeneca Pharmaceuticals; is a consultant to Bristol-Myers Squibb Co., Janssen Pharmaceutica, and Pfizer Inc., and is a speaker for Eli Lilly and Co., Pfizer Inc., and Janssen Pharmaceutica.
Itai Danovitch reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Pierre receives grant/research support from Cephalon Inc.; is a consultant to Eli Lilly and Co., Bristol-Myers Squibb Co., AstraZeneca, and Pfizer Inc.; and is a speaker for Novartis Pharmaceuticals Corp., AstraZeneca Pharmaceuticals, and Janssen Pharmaceutica.
Dr. William Wirshing receives grant/research support from Janssen Pharmaceutica, Eli Lilly and Co., Otsuka America Pharmaceutical, Abbot Laboratories, Pfizer Inc., Sanofi-Synthelabo, Organon, Bristol-Myers Squibb Co., and Knoll Pharmaceuticals, and is a consultant to Janssen Pharmaceutica, Hoechst Marion Roussel, and Eli Lilly and Co.
1. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
2. Henderson D, Cagliero E, Gray C, et al. Clozapine, diabetes mellitus, weight gain and lipid abnormalities: a five year naturalistic study. Am J Psychiatry 2000;157(6):975-81.
3. Kinon BJ, Basson BR, Gilmore JA, et al. Long-term olanzapine treatment: weight change and weight-related health factors in schizophrenia. J Clin Psychiatry 2001;62:92-100.
4. Ganguli R. Weight gain associated with antipsychotic drugs J Clin Psychiatry 1999;60:20-4.
5. McIntyre RS, McCann SM, Kennedy SH. Antipsychotic metabolic effects: weight gain, diabetes mellitus, and lipid abnormalities. Can J Psychiatry 2001;46:273-281.
6. Taylor DM, McAskill R. Atypical antipsychotics and weight gain—a systematic review. Acta Psychiatry Scand 2000;101:416-32.
7. Haapasalo-Pesu KM, Saarijarvi S. Olanzapine induces remarkable weight gain in adolescent patients. Eur Child Adolesc Psychiatry 2001;10:205-8.
8. Martin A, Landau J, Leebens P, et al. Risperidone-associated weight gain in children and adolescents: a retrospective chart review. J Child Adolesc Psychopharmacol 2000;10:259-68.
9. Wirshing DA, Spellberg BJ, Erhart SM, et al. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44:778-83.
10. Bray G. Drug treatment of obesity. Rev Endocr Metab Disord 2001;2(4):403-18.
11. Kaur G, Kulkarni SK. Studies on modulation of feeding behavior by atypical antipsychotics in female mice. Prog Neuropsychopharmacol Biol Psychiatry 2002;26:277-85.
12. Wirshing D, Wirshing W, Kysar L, et al. Novel antipsychotics: Comparison of weight gain liabilities. J Clin Psychiatry 1999;60:358-63.
13. Bray GA, York DA. Clinical review 90: Leptin and clinical medicine: a new piece in the puzzle of obesity. J Clin Endocrinol Metab 1997;82:2771-6.
14. Baptista T, Lacruz A, De Mendoza D, et al. Body weight gain after administration of antipsychotic drugs. Pharmacopsychiatry 2002;35:36.-
15. Helmrich SP, Ragland DR, Leung RW, et al. Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus. N Engl J Med 1991;325:147-52.
16. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
17. Henderson DC. Atypical antipsychotic-induced diabetes mellitus: how strong is the evidence? CNS Drugs 2002;16:77-89.
18. Ramankutty G. Olanzapine-induced destabilization of diabetes in the absence of weight gain. Acta Psychiatry Scand 2002;105:235-7.
19. Muench J, Carey M. Diabetes mellitus associated with atypical antipsychotic medications: new case report and review of the literature. J Am Board Fam Pract 2001;14:278-82.
20. Beck-Nielsen H, Groop LC. Metabolic and genetic characterization of prediabetic states. Sequence of events leading to non-insulin-dependent diabetes mellitus. J Clin Invest 1994-94:1714-21.
21. Wozniak K, Linnoila M. Hyperglycemic properties of serotonin receptor antagonists. Life Sci 1991;49:101-9.
22. Ardizzone TD, Bradley RJ, Freeman AM, 3rd, et al. Inhibition of glucose transport in PC12 cells by the atypical antipsychotic drugs risperidone and clozapine, and structural analogs of clozapine. Brain Res 2001;923:82-90.
23. Wilson PW. Established risk factors and coronary artery disease: the Framingham Study. Am J Hypertens 1994;7:7S-12S.
24. Meyer JM. Novel antipsychotics and severe hyperlipidemia. J Clin Psychopharmacol 2001;21:369-74.
25. Niaura R, Banks SM, Ward KD, et al. Hostility and the metabolic syndrome in older males: the normative aging study. Psychosom Med 2000;62:7-16.
26. Diebold K, Michel G, Schweizer J, et al. Are psychoactive-drug-induced changes in plasma lipid and lipoprotein levels of significance for clinical remission in psychiatric disorders? Pharmacopsychiatry 1998;31:60-7.
27. Bechara CI, Goldman-Levine JD. Dramatic worsening of type 2 diabetes mellitus due to olanzapine after 3 years of therapy. Pharmacotherapy 2001;21:1444-7.
28. Garson A, Jr. How to measure the QT interval—what is normal? Am J Cardiol 1993;72:14B-16B.
29. Tan HL, Hou CJ, Lauer MR, et al. Electrophysiologic mechanisms of the long QT interval syndromes and torsade de pointes. Ann Intern Med 1995;122:701-14.
30. Morganroth J, Brozovich FV, McDonald JT, et al. Variability of the QT measurement in healthy men, with implications for selection of an abnormal QT value to predict drug toxicity and proarrhythmia. Am J Cardiol 1991;67:774-6.
31. Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations: Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations Diabetes Care 2000;23:S4.-
32. Joerg C K-WS, Beasley CM. Cardiac safety parameters of olanzapine: comparison with other atypical and typical antipsychotics. J Clin Psychiatry 2001;2:35-40.
33. Association of Clozaril with cardiovascular toxicity. [Dear healthcare professional letter]. Novartis Pharmaceuticals Canada Inc, 2002.
34. Killian JG, Kerr K, Lawrence C. Myocarditis and cardiomyopathy associated with clozapine. Lancet 1999;354:1841-5.
35. Lieberman JA, Safferman AZ. Clinical profile of clozapine: adverse reactions and agranulocytosis. Psychiatr Q 1992;63:51-70.
36. Wooltorton E. Antipsychotic clozapine (Clozaril): myocarditis and cardiovascular toxicity. CMAJ 2002;166:1185-6.
37. Breier AF, Malhotra AK, Su T, et al. Clozapine and risperidone in chronic schizophrenia: effects on symptoms, parkinsonian side effects, and neuroendocrine response. Am J Psychiatry 1999;156:294-8.
38. Caracci G. Prolactin levels in premenopausal women treated with risperidone compared with those of women treated with typical neuroleptics. J Clin Psychopharmacology 1999;19:194-6.
39. Conley RR, Mahmoud R. A randomized double-blind study of risperidone and olanzapine in the treatment of schizophrenia or schizoaffective disorder. Am J Psychiatry 2001;158:765-74.
40. Segal S, Yaffe H, Laufer N, et al. Male hyperprolactinemia: effects on fertility. Fertil Steril 1979;32:556-61.
41. Schlechte J, Walkner L, Kathol M. A longitudinal analysis of premenopausal bone loss in healthy women and women with hyperprolactinemia. J Clin Endocrinol Metab 1992;75:698-703.
42. Gazzola LR, Opler LA. Return of menstruation after switching from risperidone to olanzapine. J Clin Psychopharmacol 1998;18:486-7.
43. Boyd A. Bromocriptine and psychosis: a literature review. Psychiatr Q 1995;66:87-95.
44. Aizenberg D, Modai I, Landa A, et al. Comparison of sexual dysfunction in male schizophrenic patients maintained on treatment with classical antipsychotics versus clozapine. J Clin Psychiatry 2001;62:541-4.
45. Meston CM. Sympathetic nervous system activity and female sexual arousal. Am J Cardiol 2000;86:30F-34F.
46. Wirshing DA, Pierre JM, Marder SR, et al. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56:25-30.
47. Aizenberg D, Zemishlany Z, Dorfman-Etrog P, et al. Sexual dysfunction in male schizophrenic patients. J Clin Psychiatry 1995;56:137-41.
48. Hummer M, Kemmler G, Kurz M, et al. Sexual disturbances during clozapine and haloperidol treatment for schizophrenia. Am J Psychiatry 1999;156:631-3.
49. Pais VM, Ayvazian PJ. Priapism from quetiapine overdose: first report and proposal of mechanism. Urology 2001;58:462.-
50. Compton MT, Miller AH. Priapism associated with conventional and atypical antipsychotic medications: a review. J Clin Psychiatry 2001;62:362-6.
1. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
2. Henderson D, Cagliero E, Gray C, et al. Clozapine, diabetes mellitus, weight gain and lipid abnormalities: a five year naturalistic study. Am J Psychiatry 2000;157(6):975-81.
3. Kinon BJ, Basson BR, Gilmore JA, et al. Long-term olanzapine treatment: weight change and weight-related health factors in schizophrenia. J Clin Psychiatry 2001;62:92-100.
4. Ganguli R. Weight gain associated with antipsychotic drugs J Clin Psychiatry 1999;60:20-4.
5. McIntyre RS, McCann SM, Kennedy SH. Antipsychotic metabolic effects: weight gain, diabetes mellitus, and lipid abnormalities. Can J Psychiatry 2001;46:273-281.
6. Taylor DM, McAskill R. Atypical antipsychotics and weight gain—a systematic review. Acta Psychiatry Scand 2000;101:416-32.
7. Haapasalo-Pesu KM, Saarijarvi S. Olanzapine induces remarkable weight gain in adolescent patients. Eur Child Adolesc Psychiatry 2001;10:205-8.
8. Martin A, Landau J, Leebens P, et al. Risperidone-associated weight gain in children and adolescents: a retrospective chart review. J Child Adolesc Psychopharmacol 2000;10:259-68.
9. Wirshing DA, Spellberg BJ, Erhart SM, et al. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44:778-83.
10. Bray G. Drug treatment of obesity. Rev Endocr Metab Disord 2001;2(4):403-18.
11. Kaur G, Kulkarni SK. Studies on modulation of feeding behavior by atypical antipsychotics in female mice. Prog Neuropsychopharmacol Biol Psychiatry 2002;26:277-85.
12. Wirshing D, Wirshing W, Kysar L, et al. Novel antipsychotics: Comparison of weight gain liabilities. J Clin Psychiatry 1999;60:358-63.
13. Bray GA, York DA. Clinical review 90: Leptin and clinical medicine: a new piece in the puzzle of obesity. J Clin Endocrinol Metab 1997;82:2771-6.
14. Baptista T, Lacruz A, De Mendoza D, et al. Body weight gain after administration of antipsychotic drugs. Pharmacopsychiatry 2002;35:36.-
15. Helmrich SP, Ragland DR, Leung RW, et al. Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus. N Engl J Med 1991;325:147-52.
16. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
17. Henderson DC. Atypical antipsychotic-induced diabetes mellitus: how strong is the evidence? CNS Drugs 2002;16:77-89.
18. Ramankutty G. Olanzapine-induced destabilization of diabetes in the absence of weight gain. Acta Psychiatry Scand 2002;105:235-7.
19. Muench J, Carey M. Diabetes mellitus associated with atypical antipsychotic medications: new case report and review of the literature. J Am Board Fam Pract 2001;14:278-82.
20. Beck-Nielsen H, Groop LC. Metabolic and genetic characterization of prediabetic states. Sequence of events leading to non-insulin-dependent diabetes mellitus. J Clin Invest 1994-94:1714-21.
21. Wozniak K, Linnoila M. Hyperglycemic properties of serotonin receptor antagonists. Life Sci 1991;49:101-9.
22. Ardizzone TD, Bradley RJ, Freeman AM, 3rd, et al. Inhibition of glucose transport in PC12 cells by the atypical antipsychotic drugs risperidone and clozapine, and structural analogs of clozapine. Brain Res 2001;923:82-90.
23. Wilson PW. Established risk factors and coronary artery disease: the Framingham Study. Am J Hypertens 1994;7:7S-12S.
24. Meyer JM. Novel antipsychotics and severe hyperlipidemia. J Clin Psychopharmacol 2001;21:369-74.
25. Niaura R, Banks SM, Ward KD, et al. Hostility and the metabolic syndrome in older males: the normative aging study. Psychosom Med 2000;62:7-16.
26. Diebold K, Michel G, Schweizer J, et al. Are psychoactive-drug-induced changes in plasma lipid and lipoprotein levels of significance for clinical remission in psychiatric disorders? Pharmacopsychiatry 1998;31:60-7.
27. Bechara CI, Goldman-Levine JD. Dramatic worsening of type 2 diabetes mellitus due to olanzapine after 3 years of therapy. Pharmacotherapy 2001;21:1444-7.
28. Garson A, Jr. How to measure the QT interval—what is normal? Am J Cardiol 1993;72:14B-16B.
29. Tan HL, Hou CJ, Lauer MR, et al. Electrophysiologic mechanisms of the long QT interval syndromes and torsade de pointes. Ann Intern Med 1995;122:701-14.
30. Morganroth J, Brozovich FV, McDonald JT, et al. Variability of the QT measurement in healthy men, with implications for selection of an abnormal QT value to predict drug toxicity and proarrhythmia. Am J Cardiol 1991;67:774-6.
31. Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations: Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations Diabetes Care 2000;23:S4.-
32. Joerg C K-WS, Beasley CM. Cardiac safety parameters of olanzapine: comparison with other atypical and typical antipsychotics. J Clin Psychiatry 2001;2:35-40.
33. Association of Clozaril with cardiovascular toxicity. [Dear healthcare professional letter]. Novartis Pharmaceuticals Canada Inc, 2002.
34. Killian JG, Kerr K, Lawrence C. Myocarditis and cardiomyopathy associated with clozapine. Lancet 1999;354:1841-5.
35. Lieberman JA, Safferman AZ. Clinical profile of clozapine: adverse reactions and agranulocytosis. Psychiatr Q 1992;63:51-70.
36. Wooltorton E. Antipsychotic clozapine (Clozaril): myocarditis and cardiovascular toxicity. CMAJ 2002;166:1185-6.
37. Breier AF, Malhotra AK, Su T, et al. Clozapine and risperidone in chronic schizophrenia: effects on symptoms, parkinsonian side effects, and neuroendocrine response. Am J Psychiatry 1999;156:294-8.
38. Caracci G. Prolactin levels in premenopausal women treated with risperidone compared with those of women treated with typical neuroleptics. J Clin Psychopharmacology 1999;19:194-6.
39. Conley RR, Mahmoud R. A randomized double-blind study of risperidone and olanzapine in the treatment of schizophrenia or schizoaffective disorder. Am J Psychiatry 2001;158:765-74.
40. Segal S, Yaffe H, Laufer N, et al. Male hyperprolactinemia: effects on fertility. Fertil Steril 1979;32:556-61.
41. Schlechte J, Walkner L, Kathol M. A longitudinal analysis of premenopausal bone loss in healthy women and women with hyperprolactinemia. J Clin Endocrinol Metab 1992;75:698-703.
42. Gazzola LR, Opler LA. Return of menstruation after switching from risperidone to olanzapine. J Clin Psychopharmacol 1998;18:486-7.
43. Boyd A. Bromocriptine and psychosis: a literature review. Psychiatr Q 1995;66:87-95.
44. Aizenberg D, Modai I, Landa A, et al. Comparison of sexual dysfunction in male schizophrenic patients maintained on treatment with classical antipsychotics versus clozapine. J Clin Psychiatry 2001;62:541-4.
45. Meston CM. Sympathetic nervous system activity and female sexual arousal. Am J Cardiol 2000;86:30F-34F.
46. Wirshing DA, Pierre JM, Marder SR, et al. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56:25-30.
47. Aizenberg D, Zemishlany Z, Dorfman-Etrog P, et al. Sexual dysfunction in male schizophrenic patients. J Clin Psychiatry 1995;56:137-41.
48. Hummer M, Kemmler G, Kurz M, et al. Sexual disturbances during clozapine and haloperidol treatment for schizophrenia. Am J Psychiatry 1999;156:631-3.
49. Pais VM, Ayvazian PJ. Priapism from quetiapine overdose: first report and proposal of mechanism. Urology 2001;58:462.-
50. Compton MT, Miller AH. Priapism associated with conventional and atypical antipsychotic medications: a review. J Clin Psychiatry 2001;62:362-6.
UPDATE ON ATYPICALS: Practical tips to manage common side effects
Atypical antipsychotics are powerful medications for acute and chronic psychotic disorders, with a similarly powerful potential for adverse systemic effects. To use these agents to their greatest advantage, we must balance the benefits against the risks.
We often see patients with weight gain, diabetes, dyslipidemia, cardiac toxicity, hyperprolactinemia, and sexual dysfunction—all possible effects of atypical antipsychotics. Based on the latest evidence and our experience, we offer tips for using clozapine, olanzapine, quetiapine, risperidone, and ziprasidone, and preliminary impressions about the newly approved agent, aripiprazole.
Weight gain
Clinical trials have shown convincingly that atypical antipsychotics pose a greater risk of weight gain and central adiposity than do most older antipsychotics.1 Overweight and obesity are associated with increased risks of hypertension, type 2 diabetes, coronary heart disease, stroke, gallbladder disease, osteoarthritis, and some forms of cancer. Moreover, obesity’s socially stigmatizing effect can discourage patients with schizophrenia—particularly adolescents—from taking their medication.
Table 1
POTENTIAL FOR ADVERSE EFFECTS WITH ATYPICAL ANTIPSYCHOTICS
| Metabolic changes | Weight gain | Increased prolactin | QT interval | EPS | Sedation | Orthostasis | |
|---|---|---|---|---|---|---|---|
| Risperidone | + | + | +++ | + | ++ | + | ++ |
| Ziprasidone | + | + | − | ++ | + | + | + |
| Clozapine | +++ | +++ | − | ++ | +/− | +++ | +++ |
| Olanzapine | +++ | +++ | − | + | + | ++ | + |
| Quetiapine | ++ | ++ | − | ++ | + | ++ | ++ |
| Aripiprazole | + | + | − | + | + | +/− | +/− |
Comparative effects. Olanzapine and clozapine are associated with greater weight gain (Table 1)1-3 than risperidone and ziprasidone.4 Data regarding quetiapine are inconsistent—some studies show weight gain similar to that caused by olanzapine, and others find much less.5 Weight gain associated with quetiapine, ziprasidone, and risperidone tends to plateau within the first few months, whereas patients taking olanzapine and clozapine may continue to gain weight for 9 months or more.6
Adolescents and young adults may be particularly susceptible to antipsychotic-induced weight gain.7 No studies have directly compared weight gain in adults versus adolescents, but adolescents are exceedingly susceptible to the atypicals’ metabolic dysregulation. For example:
- A higher prevalence of extreme weight gain (>7% of baseline body mass) with olanzapine and risperidone has been reported in adolescent inpatients than among adults.7
- Extreme weight gain was seen in 78% of a group of risperidone-treated children; for 6 months, their weight gain averaged 1.2 kg/month without leveling off.8
These findings suggest that risperidone’s apparent metabolic advantage in adults disappears in children and adolescents. Risperidone’s effect on prolactin may account for a higher risk of weight gain in younger patients. These populations have exquisite end-organ sensitivity to changes in prolactin levels and may be more susceptible to the weight gain—and perhaps diabetes—believed related to hyperprolactinemia.9
Mechanisms. The mechanism(s) of weight gain may be related to the receptor systems upon which the atypicals act. These agents block noradrenergic, dopamine, serotonin, and histamine receptors, all of which are thought to affect metabolism or appetite control. Stimulation of alpha and D2 receptors by sympathomimetic amines causes weight loss, as does stimulation of certain 5HT receptors by weight-loss drugs such as fenfluramine.10 With respect to appetite, it has been suggested that peripheral antagonism of H1 receptors interferes with normal satiety signals.11 This may explain why affinity to histamine H1 receptors is among the best of correlates with potential for weight gain.12
Increases in serum levels of leptin—a peptide hormone produced in direct proportion to adiposity and thought to be anorexigenic, possibly through effects on satiety13 —parallel weight gain during treatment with atypicals. However, there is no indication that leptin imbalance causes weight gain; it may instead be the result. Altered sensitivity to leptin may be a contributing factor, perhaps at the hypothalamus.14
Diabetes
The risk of type 2 diabetes increases with weight gain,15 so it is no surprise that diabetes is more prevalent among patients taking atypicals. In a study of 38,000 schizophrenic patients, those taking atypicals were 9% more likely to have diabetes than those receiving typical antipsychotics,16 and all atypicals were associated with a significant increase in diabetes risk in patients younger than 40. The pervasiveness of diabetes17 and reports of new-onset diabetes in non-overweight patients18 suggest that—in addition to their effect on weight—atypicals may alter insulin and glucose metabolism.19
Atypical antipsychotics probably increase diabetes risk in a number of ways:
- An increase in adipose tissue can lead to insulin resistance, glucose intolerance, and ultimately diabetes.20
- Serotonin receptor antagonism may lead to hyperglycemia by decreasing pancreatic beta cell response to signals that advance insulin production.21
- Atypicals may contribute to hyperglycemia by impeding cellular uptake of glucose.22
- The increase in free fatty acids associated with atypicals can alter glucose metabolism. This may explain why clozapine and olanzapine—the atypicals with the greatest potential for severe hyperlipidemia—have the strongest association with new-onset diabetes.
Hyperlipidemia
Case reports and controlled studies have linked atypical antipsychotics with hyperlipidemia. Whether the hyperlipidemia is a consequence of weight gain or some other metabolic disturbance is unknown. Even without conclusive data, however, the link is of concern because elevated triglyceride levels represent an independent risk factor for heart disease.23
Although all atypicals increase serum triglycerides to some degree, severe hypertriglyceridemia occurs predominantly with clozapine and olanzapine.24 Both drugs have favorable efficacy profiles, and the mechanism of their antipsychotic activity may include altering the various lipid pools.
For example, studies have found that decreased triglyceride levels correlate with hostility and psychological distress.25 Increased triglycerides have been theorized to enhance membrane fluidity, which in turn may augment presynaptic reuptake of serotonin and diminish postsynaptic serotonin activity.26 In other words, elevated triglyceride levels could play a role in atypical antipsychotic-mediated inhibition of serotonin transmission. It is not yet known whether lipid-lowering drugs might alter atypicals’ efficacy.
Table 2
RECOMMENDED METABOLIC MONITORING OF PATIENTS TAKING ATYPICAL ANTIPSYCHOTICS
| Every visit | Check weight Check blood pressure |
| Every 3 months | Fasting blood glucose Fasting triglycerides Fasting cholesterol |
Metabolic monitoring
Managing mental illness concurrently with weight gain, diabetes, and hypertriglyceridemia is a challenge. In our clinic, we try to diminish the atypicals’ adverse metabolic effects by monitoring a few basic parameters and taking preventive measures (Table 2).
We routinely screen patients for diabetes symptoms by asking questions about changes in belt size (a sign of weight change), urinary frequency, and thirst (Table 3). We also document baseline weight, blood glucose (Table 4), blood chemistry, and lipid levels, with routine follow-up throughout therapy and greatest scrutiny during the first months of a new treatment.
Patients who cannot control their weight with lifestyle modifications (Table 5) may require a lipid-lowering medication—a “stain” and/or fibrate (such as gemfibrozil)—or, if those measures are ineffective, a switch to another antipsychotic. Hyperlipidemia and hyperglycemia may be reduced substantially when patients discontinue the aggravating medication.27
Although discontinuing or switching medications may reduce metabolic side effects, the hazard of psychotic decompensation is substantial. Achieving an antipsychotic effect is extremely difficult for most patients, and one should not discontinue an effective treatment without seriously considering the consequences. Antipsychotic efficacy should never be sacrificed in the pursuit of a regimen with more benign side effects. Consider switching to an atypical with a more moderate effect on weight, however, if weight gain would likely lead to noncompliance. Even the most effective treatment will not work if a patient never takes it.
Table 3
5 SCREENING QUESTIONS TO MONITOR FOR METABOLIC AND SEXUAL SIDE EFFECTS
|
Table 4
DIAGNOSTIC CRITERIA FOR DIABETES
| • Symptoms of diabetes (such as polyuria, polydipsia, or unexplained weight loss) plus nonfasting plasma glucose (PG) >200 mg/dL (11.1 mmol/L) |
| OR |
| • Fasting plasma glucose >126 mg/dL (7.0 mmol/L) |
| OR |
| • 2-hour PG >200 mg/dL during an oral glucose tolerance test |
| Source: American Diabetes Association |
Cardiac toxicity
QTc prolongation. Atypical antipsychotics—like their typical counterparts—cause QTc prolongation to varying degrees. On an ECG, the QT interval corresponds to cardiac depolarization and repolarization phases. The QT interval—which changes naturally with the time of day, stressors, and heart rate—is commonly corrected for heart rate to yield QTc.28 If QTc is prolonged beyond a certain threshold, repolarization can occur simultaneously with early depolarization. The consequence may be ventricular arrhythmias, such as torsades de pointes, which can degenerate into ventricular tachycardia, fibrillation, and even death.
All the atypicals are thought to prolong QT intervals to some degree by reducing the flow of repolarizing K+ currents, ultimately making the myocardium more excitable.29 Although there is no specific threshold above which torsades de pointes will occur, it appears there is no significant risk of developing arrhythmias below a QT interval of 500 msec.30 In fact, because the atypicals behave like type IIIa antiarrhythmics, they will overdrive the ventricle and suppress other emergent ventricular arrhythmias. Notwithstanding the FDA’s scrutiny of ziprasidone, no data indicate that this agent is disproportionately toxic.
Clinical precautions. Overall, atypicals cause only a modest increase in the QT interval. Ziprasidone and quetiapine appear to have somewhat more pronounced effects, with ziprasidone prolonging the QT interval on average about 20 msec.31 These mean increases are clinically irrelevant in most patients, but use caution when treating patients who:
- have pre-existing heart disease that is known to be associated with ventricular arrhythmias
- are taking other medications that prolong QT through the same mechanism
- have historically had idiosyncratic sensitivities to prolonged QT.32
Bradycardia, electrolyte imbalances, and endocrine disorders—which themselves increase QTc—also might make an individual more susceptible to the consequences of subtle QT prolongation.29
Managing patients at risk. In our clinic, we assess patients for risk of QT prolongation by inquiring about a family history of cardiac disease or a personal history of arrhythmia, syncope, or near syncope. In at-risk patients, we:
- monitor clinical progress more frequently, focusing on symptoms that suggest syncope or near syncope (unexplained episodic nausea, drowsiness)
- obtain routine ECGs to identify the rare population at increased risk for arrhythmia with either severely prolonged QT (>500 msec) or a serious AV conduction delay at baseline (second-degree or greater).
Laboratory tests should include electrolytes, as hypoleukemia is compellingly associated with development of arrhythmias.
Cardiac toxicity with clozapine. Reports of myocarditis and cardiomyopathy associated with clozapine have raised concern that this agent may be associated with other forms of cardiac toxicity. In January 2002, Novartis Pharmaceuticals Corp. reported 213 cases of myocarditis, 85% of which occurred while patients were taking recommended doses of clozapine within the first 2 months of therapy.33 Eosinophilia in many of the cases indicates that an IgE-mediated hypersensitivity reaction may be involved.34
Novartis also reported 178 cases of clozapineassociated cardiomyopathy, 80% of which occurred in patients younger than 50. Almost 20% of the incidents resulted in death, an alarming figure that may reflect either delay in diagnosis and treatment or simple reporting bias.
Detecting cardiac toxicity is particularly challenging because its manifestations—tachycardia, fatigue, and orthostatic hypotension—are frequently observed in clozapine-treated patients, particularly when dosages are changed.35 The poor specificity of signs for cardiac toxicity requires that we:
- identify at baseline patients with a personal or family history of heart disease
- set our threshold for suspicion of direct cardiotoxicity particularly low when titrating clozapine.36
Hyperprolactinemia
Higher elevations with risperidone. Many antipsychotics cause hyperprolactinemia because their antidopaminergic activity prevents dopamine from inhibiting prolactin secretion. Among the atypicals, however, only risperidone significantly elevates prolactin.37 Caracci et al also demonstrated a two- to four-fold greater prolactin elevation with risperidone than with typical antipsychotics38 and noted that hyperprolactinemia with risperidone could occur at standard daily doses.
We believe that risperidone’s tendency to disperse disproportionately within the plasma space accounts for its differential effect on D2 receptors in the tubuloinfundibular system (brain/plasma ratio of about 0.02 versus approximately 20 for most other antipsychotics). Thus, the lactotrophs, which are outside the blood brain barrier, are exposed to much higher levels of risperidone than are the D2 receptors within the CSF space, resulting in seemingly paradoxical co-occurence of EPS-free hyperprolactinemia.
Table 5
INTERVENTIONS TO CONTROL ANTIPSYCHOTIC-RELATEDWEIGHT GAIN
|
Clinical effects. Elevated prolactin levels do not necessarily lead to clinical symptoms. A large study comparing olanzapine and risperidone found that although more patients receiving risperidone had elevated prolactin levels, few patients in either group reported prolactin-related events such as amenorrhea, galactorrhea, gynecomastia, or sexual side effects.39 Elevated prolactin levels have not been shown to be intrinsically harmful, although they can cause hypogonadism via negative feedback and inhibition of gonadotropin-releasing hormone, leading to inadequate follicle-stimulating hormone and luteinizing hormone.
Hyperprolactinemia also reduces serum testosterone levels in men, which may lead to decreased libido, impotence, infertility, gynecomastia, and rarely galactorrhea.40 Premenopausal women may experience infertility, oligomenorrhea or amenorrhea, galactorrhea, and reduced bone mineral density.41
Treatment options. When patients develop hyperprolactinemia, switching to another antipsychotic is not the only option.42 Standard therapies for hyperprolactinemia—the prodopaminergic drugs bromocriptine and amantadine—are effective, though they may have a slight tendency to provoke or worsen psychosis.43 In our experience, most patients can be managed with judicious dosages of bromocriptine (less than 5 mg/d) or even lower dosages of cabergoline (0.25 mg weekly to twice weekly), which causes very few psychiatric side effects.
Birth control pills are a reasonable alternative for women below age 35 who are nonsmokers—a relatively small proportion of those afflicted with schizophrenia but a much higher proportion of those likely to develop endocrine toxicities.
Sexual dysfunction
Sexual dysfunction—including decreased libido, impaired arousal, and erectile orgasmic dysfunction—is common among patients receiving atypical antipsychotics.44 These effects may be caused by anticholinergic activity, alpha-1 inhibition, and hypogonadism due to hyperprolactinemia.45 Delineating one specific cause of sexual dysfunction can be difficult because:
- antipsychotics are often administered with other psychotropics that influence sexual function
- schizophrenia itself is associated with sexual dysfunction.
The asociality associated with schizophrenia’s negative symptoms may be accompanied by decreased libido, fewer sexual thoughts, and fewer sexual relationships. In surveys, patients treated with atypical antipsychotics tend to report improved sex drive and libido but more erectile dysfunction and anorgasmia.46 Untreated patients report having fewer sexual thoughts and diminished libido but better erectile function and potency.47 The atypicals’ positive effect on social behavior may facilitate a willingness to engage in sexual activity, making sexual dysfunction more apparent.48
Priapism has been reported with all atypicals except ziprasidone.49 The vascular tone of the penis is in part sympathetically mediated, and alpha-1 blockade can inhibit detumescence via its indirect tendency to increase nitric oxide levels.50 Although priapism does not appear to be common, it is a urologic emergency with potential long-term consequences, including permanent erectile dysfunction. Patients developing abnormally prolonged and painful erections must be counseled to seek immediate medical attention.
Aripiprazole: Preliminary impressions
The recently approved antipsychotic aripiprazole differs from the now-familiar dopaminergic theme by being a partial agonist at the D2 receptor. Aripiprazole has the greatest affinity for the D2 receptor of any available drug, activates the postsynaptic complex at about 30% of the full endogenous DA affect, and appears to lack the metabolic consequences of the other atypicals.
In our research laboratory, aripiprazole has shown a profound prolactin lowering effect, superior subjective tolerability, and a more salutary impact on sexual function, compared with other antipsychotics. Although not devoid of EPS, aripiprazole appears to alter a patient’s subjective distress in a way that alters the risk/benefit ratio. Although aripiprazole’s clinical niche has yet to be established, it would be reasonable to use it for overweight patients intolerant of the dysphorogenic effects of other antipsychotics.
Related resources
- Wirshing DA, Wirshing WC, Kysar L, et al. Novel antipsychotics: comparison of weight gain liabilities J Clin Psychiatry 1999;60(6)358-63.
- Wirshing DA, Spellberg B, Erhart SM, Marder SR, Wirshing WC. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44(8):778-83.
- Wirshing DA, Pierre JM, Marder SR, Saunders CS, Wirshing WC. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56(1-2):25-30.
Drug brand names
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Donna Wirshing receives grant/research support from Pfizer Inc., Eli Lilly and Co., Janssen Pharmaceutica, and AstraZeneca Pharmaceuticals; is a consultant to Bristol-Myers Squibb Co., Janssen Pharmaceutica, and Pfizer Inc., and is a speaker for Eli Lilly and Co., Pfizer Inc., and Janssen Pharmaceutica.
Itai Danovitch reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Pierre receives grant/research support from Cephalon Inc.; is a consultant to Eli Lilly and Co., Bristol-Myers Squibb Co., AstraZeneca, and Pfizer Inc.; and is a speaker for Novartis Pharmaceuticals Corp., AstraZeneca Pharmaceuticals, and Janssen Pharmaceutica.
Dr. William Wirshing receives grant/research support from Janssen Pharmaceutica, Eli Lilly and Co., Otsuka America Pharmaceutical, Abbot Laboratories, Pfizer Inc., Sanofi-Synthelabo, Organon, Bristol-Myers Squibb Co., and Knoll Pharmaceuticals, and is a consultant to Janssen Pharmaceutica, Hoechst Marion Roussel, and Eli Lilly and Co.
1. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
2. Henderson D, Cagliero E, Gray C, et al. Clozapine, diabetes mellitus, weight gain and lipid abnormalities: a five year naturalistic study. Am J Psychiatry 2000;157(6):975-81.
3. Kinon BJ, Basson BR, Gilmore JA, et al. Long-term olanzapine treatment: weight change and weight-related health factors in schizophrenia. J Clin Psychiatry 2001;62:92-100.
4. Ganguli R. Weight gain associated with antipsychotic drugs J Clin Psychiatry 1999;60:20-4.
5. McIntyre RS, McCann SM, Kennedy SH. Antipsychotic metabolic effects: weight gain, diabetes mellitus, and lipid abnormalities. Can J Psychiatry 2001;46:273-281.
6. Taylor DM, McAskill R. Atypical antipsychotics and weight gain—a systematic review. Acta Psychiatry Scand 2000;101:416-32.
7. Haapasalo-Pesu KM, Saarijarvi S. Olanzapine induces remarkable weight gain in adolescent patients. Eur Child Adolesc Psychiatry 2001;10:205-8.
8. Martin A, Landau J, Leebens P, et al. Risperidone-associated weight gain in children and adolescents: a retrospective chart review. J Child Adolesc Psychopharmacol 2000;10:259-68.
9. Wirshing DA, Spellberg BJ, Erhart SM, et al. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44:778-83.
10. Bray G. Drug treatment of obesity. Rev Endocr Metab Disord 2001;2(4):403-18.
11. Kaur G, Kulkarni SK. Studies on modulation of feeding behavior by atypical antipsychotics in female mice. Prog Neuropsychopharmacol Biol Psychiatry 2002;26:277-85.
12. Wirshing D, Wirshing W, Kysar L, et al. Novel antipsychotics: Comparison of weight gain liabilities. J Clin Psychiatry 1999;60:358-63.
13. Bray GA, York DA. Clinical review 90: Leptin and clinical medicine: a new piece in the puzzle of obesity. J Clin Endocrinol Metab 1997;82:2771-6.
14. Baptista T, Lacruz A, De Mendoza D, et al. Body weight gain after administration of antipsychotic drugs. Pharmacopsychiatry 2002;35:36.-
15. Helmrich SP, Ragland DR, Leung RW, et al. Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus. N Engl J Med 1991;325:147-52.
16. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
17. Henderson DC. Atypical antipsychotic-induced diabetes mellitus: how strong is the evidence? CNS Drugs 2002;16:77-89.
18. Ramankutty G. Olanzapine-induced destabilization of diabetes in the absence of weight gain. Acta Psychiatry Scand 2002;105:235-7.
19. Muench J, Carey M. Diabetes mellitus associated with atypical antipsychotic medications: new case report and review of the literature. J Am Board Fam Pract 2001;14:278-82.
20. Beck-Nielsen H, Groop LC. Metabolic and genetic characterization of prediabetic states. Sequence of events leading to non-insulin-dependent diabetes mellitus. J Clin Invest 1994-94:1714-21.
21. Wozniak K, Linnoila M. Hyperglycemic properties of serotonin receptor antagonists. Life Sci 1991;49:101-9.
22. Ardizzone TD, Bradley RJ, Freeman AM, 3rd, et al. Inhibition of glucose transport in PC12 cells by the atypical antipsychotic drugs risperidone and clozapine, and structural analogs of clozapine. Brain Res 2001;923:82-90.
23. Wilson PW. Established risk factors and coronary artery disease: the Framingham Study. Am J Hypertens 1994;7:7S-12S.
24. Meyer JM. Novel antipsychotics and severe hyperlipidemia. J Clin Psychopharmacol 2001;21:369-74.
25. Niaura R, Banks SM, Ward KD, et al. Hostility and the metabolic syndrome in older males: the normative aging study. Psychosom Med 2000;62:7-16.
26. Diebold K, Michel G, Schweizer J, et al. Are psychoactive-drug-induced changes in plasma lipid and lipoprotein levels of significance for clinical remission in psychiatric disorders? Pharmacopsychiatry 1998;31:60-7.
27. Bechara CI, Goldman-Levine JD. Dramatic worsening of type 2 diabetes mellitus due to olanzapine after 3 years of therapy. Pharmacotherapy 2001;21:1444-7.
28. Garson A, Jr. How to measure the QT interval—what is normal? Am J Cardiol 1993;72:14B-16B.
29. Tan HL, Hou CJ, Lauer MR, et al. Electrophysiologic mechanisms of the long QT interval syndromes and torsade de pointes. Ann Intern Med 1995;122:701-14.
30. Morganroth J, Brozovich FV, McDonald JT, et al. Variability of the QT measurement in healthy men, with implications for selection of an abnormal QT value to predict drug toxicity and proarrhythmia. Am J Cardiol 1991;67:774-6.
31. Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations: Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations Diabetes Care 2000;23:S4.-
32. Joerg C K-WS, Beasley CM. Cardiac safety parameters of olanzapine: comparison with other atypical and typical antipsychotics. J Clin Psychiatry 2001;2:35-40.
33. Association of Clozaril with cardiovascular toxicity. [Dear healthcare professional letter]. Novartis Pharmaceuticals Canada Inc, 2002.
34. Killian JG, Kerr K, Lawrence C. Myocarditis and cardiomyopathy associated with clozapine. Lancet 1999;354:1841-5.
35. Lieberman JA, Safferman AZ. Clinical profile of clozapine: adverse reactions and agranulocytosis. Psychiatr Q 1992;63:51-70.
36. Wooltorton E. Antipsychotic clozapine (Clozaril): myocarditis and cardiovascular toxicity. CMAJ 2002;166:1185-6.
37. Breier AF, Malhotra AK, Su T, et al. Clozapine and risperidone in chronic schizophrenia: effects on symptoms, parkinsonian side effects, and neuroendocrine response. Am J Psychiatry 1999;156:294-8.
38. Caracci G. Prolactin levels in premenopausal women treated with risperidone compared with those of women treated with typical neuroleptics. J Clin Psychopharmacology 1999;19:194-6.
39. Conley RR, Mahmoud R. A randomized double-blind study of risperidone and olanzapine in the treatment of schizophrenia or schizoaffective disorder. Am J Psychiatry 2001;158:765-74.
40. Segal S, Yaffe H, Laufer N, et al. Male hyperprolactinemia: effects on fertility. Fertil Steril 1979;32:556-61.
41. Schlechte J, Walkner L, Kathol M. A longitudinal analysis of premenopausal bone loss in healthy women and women with hyperprolactinemia. J Clin Endocrinol Metab 1992;75:698-703.
42. Gazzola LR, Opler LA. Return of menstruation after switching from risperidone to olanzapine. J Clin Psychopharmacol 1998;18:486-7.
43. Boyd A. Bromocriptine and psychosis: a literature review. Psychiatr Q 1995;66:87-95.
44. Aizenberg D, Modai I, Landa A, et al. Comparison of sexual dysfunction in male schizophrenic patients maintained on treatment with classical antipsychotics versus clozapine. J Clin Psychiatry 2001;62:541-4.
45. Meston CM. Sympathetic nervous system activity and female sexual arousal. Am J Cardiol 2000;86:30F-34F.
46. Wirshing DA, Pierre JM, Marder SR, et al. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56:25-30.
47. Aizenberg D, Zemishlany Z, Dorfman-Etrog P, et al. Sexual dysfunction in male schizophrenic patients. J Clin Psychiatry 1995;56:137-41.
48. Hummer M, Kemmler G, Kurz M, et al. Sexual disturbances during clozapine and haloperidol treatment for schizophrenia. Am J Psychiatry 1999;156:631-3.
49. Pais VM, Ayvazian PJ. Priapism from quetiapine overdose: first report and proposal of mechanism. Urology 2001;58:462.-
50. Compton MT, Miller AH. Priapism associated with conventional and atypical antipsychotic medications: a review. J Clin Psychiatry 2001;62:362-6.
Atypical antipsychotics are powerful medications for acute and chronic psychotic disorders, with a similarly powerful potential for adverse systemic effects. To use these agents to their greatest advantage, we must balance the benefits against the risks.
We often see patients with weight gain, diabetes, dyslipidemia, cardiac toxicity, hyperprolactinemia, and sexual dysfunction—all possible effects of atypical antipsychotics. Based on the latest evidence and our experience, we offer tips for using clozapine, olanzapine, quetiapine, risperidone, and ziprasidone, and preliminary impressions about the newly approved agent, aripiprazole.
Weight gain
Clinical trials have shown convincingly that atypical antipsychotics pose a greater risk of weight gain and central adiposity than do most older antipsychotics.1 Overweight and obesity are associated with increased risks of hypertension, type 2 diabetes, coronary heart disease, stroke, gallbladder disease, osteoarthritis, and some forms of cancer. Moreover, obesity’s socially stigmatizing effect can discourage patients with schizophrenia—particularly adolescents—from taking their medication.
Table 1
POTENTIAL FOR ADVERSE EFFECTS WITH ATYPICAL ANTIPSYCHOTICS
| Metabolic changes | Weight gain | Increased prolactin | QT interval | EPS | Sedation | Orthostasis | |
|---|---|---|---|---|---|---|---|
| Risperidone | + | + | +++ | + | ++ | + | ++ |
| Ziprasidone | + | + | − | ++ | + | + | + |
| Clozapine | +++ | +++ | − | ++ | +/− | +++ | +++ |
| Olanzapine | +++ | +++ | − | + | + | ++ | + |
| Quetiapine | ++ | ++ | − | ++ | + | ++ | ++ |
| Aripiprazole | + | + | − | + | + | +/− | +/− |
Comparative effects. Olanzapine and clozapine are associated with greater weight gain (Table 1)1-3 than risperidone and ziprasidone.4 Data regarding quetiapine are inconsistent—some studies show weight gain similar to that caused by olanzapine, and others find much less.5 Weight gain associated with quetiapine, ziprasidone, and risperidone tends to plateau within the first few months, whereas patients taking olanzapine and clozapine may continue to gain weight for 9 months or more.6
Adolescents and young adults may be particularly susceptible to antipsychotic-induced weight gain.7 No studies have directly compared weight gain in adults versus adolescents, but adolescents are exceedingly susceptible to the atypicals’ metabolic dysregulation. For example:
- A higher prevalence of extreme weight gain (>7% of baseline body mass) with olanzapine and risperidone has been reported in adolescent inpatients than among adults.7
- Extreme weight gain was seen in 78% of a group of risperidone-treated children; for 6 months, their weight gain averaged 1.2 kg/month without leveling off.8
These findings suggest that risperidone’s apparent metabolic advantage in adults disappears in children and adolescents. Risperidone’s effect on prolactin may account for a higher risk of weight gain in younger patients. These populations have exquisite end-organ sensitivity to changes in prolactin levels and may be more susceptible to the weight gain—and perhaps diabetes—believed related to hyperprolactinemia.9
Mechanisms. The mechanism(s) of weight gain may be related to the receptor systems upon which the atypicals act. These agents block noradrenergic, dopamine, serotonin, and histamine receptors, all of which are thought to affect metabolism or appetite control. Stimulation of alpha and D2 receptors by sympathomimetic amines causes weight loss, as does stimulation of certain 5HT receptors by weight-loss drugs such as fenfluramine.10 With respect to appetite, it has been suggested that peripheral antagonism of H1 receptors interferes with normal satiety signals.11 This may explain why affinity to histamine H1 receptors is among the best of correlates with potential for weight gain.12
Increases in serum levels of leptin—a peptide hormone produced in direct proportion to adiposity and thought to be anorexigenic, possibly through effects on satiety13 —parallel weight gain during treatment with atypicals. However, there is no indication that leptin imbalance causes weight gain; it may instead be the result. Altered sensitivity to leptin may be a contributing factor, perhaps at the hypothalamus.14
Diabetes
The risk of type 2 diabetes increases with weight gain,15 so it is no surprise that diabetes is more prevalent among patients taking atypicals. In a study of 38,000 schizophrenic patients, those taking atypicals were 9% more likely to have diabetes than those receiving typical antipsychotics,16 and all atypicals were associated with a significant increase in diabetes risk in patients younger than 40. The pervasiveness of diabetes17 and reports of new-onset diabetes in non-overweight patients18 suggest that—in addition to their effect on weight—atypicals may alter insulin and glucose metabolism.19
Atypical antipsychotics probably increase diabetes risk in a number of ways:
- An increase in adipose tissue can lead to insulin resistance, glucose intolerance, and ultimately diabetes.20
- Serotonin receptor antagonism may lead to hyperglycemia by decreasing pancreatic beta cell response to signals that advance insulin production.21
- Atypicals may contribute to hyperglycemia by impeding cellular uptake of glucose.22
- The increase in free fatty acids associated with atypicals can alter glucose metabolism. This may explain why clozapine and olanzapine—the atypicals with the greatest potential for severe hyperlipidemia—have the strongest association with new-onset diabetes.
Hyperlipidemia
Case reports and controlled studies have linked atypical antipsychotics with hyperlipidemia. Whether the hyperlipidemia is a consequence of weight gain or some other metabolic disturbance is unknown. Even without conclusive data, however, the link is of concern because elevated triglyceride levels represent an independent risk factor for heart disease.23
Although all atypicals increase serum triglycerides to some degree, severe hypertriglyceridemia occurs predominantly with clozapine and olanzapine.24 Both drugs have favorable efficacy profiles, and the mechanism of their antipsychotic activity may include altering the various lipid pools.
For example, studies have found that decreased triglyceride levels correlate with hostility and psychological distress.25 Increased triglycerides have been theorized to enhance membrane fluidity, which in turn may augment presynaptic reuptake of serotonin and diminish postsynaptic serotonin activity.26 In other words, elevated triglyceride levels could play a role in atypical antipsychotic-mediated inhibition of serotonin transmission. It is not yet known whether lipid-lowering drugs might alter atypicals’ efficacy.
Table 2
RECOMMENDED METABOLIC MONITORING OF PATIENTS TAKING ATYPICAL ANTIPSYCHOTICS
| Every visit | Check weight Check blood pressure |
| Every 3 months | Fasting blood glucose Fasting triglycerides Fasting cholesterol |
Metabolic monitoring
Managing mental illness concurrently with weight gain, diabetes, and hypertriglyceridemia is a challenge. In our clinic, we try to diminish the atypicals’ adverse metabolic effects by monitoring a few basic parameters and taking preventive measures (Table 2).
We routinely screen patients for diabetes symptoms by asking questions about changes in belt size (a sign of weight change), urinary frequency, and thirst (Table 3). We also document baseline weight, blood glucose (Table 4), blood chemistry, and lipid levels, with routine follow-up throughout therapy and greatest scrutiny during the first months of a new treatment.
Patients who cannot control their weight with lifestyle modifications (Table 5) may require a lipid-lowering medication—a “stain” and/or fibrate (such as gemfibrozil)—or, if those measures are ineffective, a switch to another antipsychotic. Hyperlipidemia and hyperglycemia may be reduced substantially when patients discontinue the aggravating medication.27
Although discontinuing or switching medications may reduce metabolic side effects, the hazard of psychotic decompensation is substantial. Achieving an antipsychotic effect is extremely difficult for most patients, and one should not discontinue an effective treatment without seriously considering the consequences. Antipsychotic efficacy should never be sacrificed in the pursuit of a regimen with more benign side effects. Consider switching to an atypical with a more moderate effect on weight, however, if weight gain would likely lead to noncompliance. Even the most effective treatment will not work if a patient never takes it.
Table 3
5 SCREENING QUESTIONS TO MONITOR FOR METABOLIC AND SEXUAL SIDE EFFECTS
|
Table 4
DIAGNOSTIC CRITERIA FOR DIABETES
| • Symptoms of diabetes (such as polyuria, polydipsia, or unexplained weight loss) plus nonfasting plasma glucose (PG) >200 mg/dL (11.1 mmol/L) |
| OR |
| • Fasting plasma glucose >126 mg/dL (7.0 mmol/L) |
| OR |
| • 2-hour PG >200 mg/dL during an oral glucose tolerance test |
| Source: American Diabetes Association |
Cardiac toxicity
QTc prolongation. Atypical antipsychotics—like their typical counterparts—cause QTc prolongation to varying degrees. On an ECG, the QT interval corresponds to cardiac depolarization and repolarization phases. The QT interval—which changes naturally with the time of day, stressors, and heart rate—is commonly corrected for heart rate to yield QTc.28 If QTc is prolonged beyond a certain threshold, repolarization can occur simultaneously with early depolarization. The consequence may be ventricular arrhythmias, such as torsades de pointes, which can degenerate into ventricular tachycardia, fibrillation, and even death.
All the atypicals are thought to prolong QT intervals to some degree by reducing the flow of repolarizing K+ currents, ultimately making the myocardium more excitable.29 Although there is no specific threshold above which torsades de pointes will occur, it appears there is no significant risk of developing arrhythmias below a QT interval of 500 msec.30 In fact, because the atypicals behave like type IIIa antiarrhythmics, they will overdrive the ventricle and suppress other emergent ventricular arrhythmias. Notwithstanding the FDA’s scrutiny of ziprasidone, no data indicate that this agent is disproportionately toxic.
Clinical precautions. Overall, atypicals cause only a modest increase in the QT interval. Ziprasidone and quetiapine appear to have somewhat more pronounced effects, with ziprasidone prolonging the QT interval on average about 20 msec.31 These mean increases are clinically irrelevant in most patients, but use caution when treating patients who:
- have pre-existing heart disease that is known to be associated with ventricular arrhythmias
- are taking other medications that prolong QT through the same mechanism
- have historically had idiosyncratic sensitivities to prolonged QT.32
Bradycardia, electrolyte imbalances, and endocrine disorders—which themselves increase QTc—also might make an individual more susceptible to the consequences of subtle QT prolongation.29
Managing patients at risk. In our clinic, we assess patients for risk of QT prolongation by inquiring about a family history of cardiac disease or a personal history of arrhythmia, syncope, or near syncope. In at-risk patients, we:
- monitor clinical progress more frequently, focusing on symptoms that suggest syncope or near syncope (unexplained episodic nausea, drowsiness)
- obtain routine ECGs to identify the rare population at increased risk for arrhythmia with either severely prolonged QT (>500 msec) or a serious AV conduction delay at baseline (second-degree or greater).
Laboratory tests should include electrolytes, as hypoleukemia is compellingly associated with development of arrhythmias.
Cardiac toxicity with clozapine. Reports of myocarditis and cardiomyopathy associated with clozapine have raised concern that this agent may be associated with other forms of cardiac toxicity. In January 2002, Novartis Pharmaceuticals Corp. reported 213 cases of myocarditis, 85% of which occurred while patients were taking recommended doses of clozapine within the first 2 months of therapy.33 Eosinophilia in many of the cases indicates that an IgE-mediated hypersensitivity reaction may be involved.34
Novartis also reported 178 cases of clozapineassociated cardiomyopathy, 80% of which occurred in patients younger than 50. Almost 20% of the incidents resulted in death, an alarming figure that may reflect either delay in diagnosis and treatment or simple reporting bias.
Detecting cardiac toxicity is particularly challenging because its manifestations—tachycardia, fatigue, and orthostatic hypotension—are frequently observed in clozapine-treated patients, particularly when dosages are changed.35 The poor specificity of signs for cardiac toxicity requires that we:
- identify at baseline patients with a personal or family history of heart disease
- set our threshold for suspicion of direct cardiotoxicity particularly low when titrating clozapine.36
Hyperprolactinemia
Higher elevations with risperidone. Many antipsychotics cause hyperprolactinemia because their antidopaminergic activity prevents dopamine from inhibiting prolactin secretion. Among the atypicals, however, only risperidone significantly elevates prolactin.37 Caracci et al also demonstrated a two- to four-fold greater prolactin elevation with risperidone than with typical antipsychotics38 and noted that hyperprolactinemia with risperidone could occur at standard daily doses.
We believe that risperidone’s tendency to disperse disproportionately within the plasma space accounts for its differential effect on D2 receptors in the tubuloinfundibular system (brain/plasma ratio of about 0.02 versus approximately 20 for most other antipsychotics). Thus, the lactotrophs, which are outside the blood brain barrier, are exposed to much higher levels of risperidone than are the D2 receptors within the CSF space, resulting in seemingly paradoxical co-occurence of EPS-free hyperprolactinemia.
Table 5
INTERVENTIONS TO CONTROL ANTIPSYCHOTIC-RELATEDWEIGHT GAIN
|
Clinical effects. Elevated prolactin levels do not necessarily lead to clinical symptoms. A large study comparing olanzapine and risperidone found that although more patients receiving risperidone had elevated prolactin levels, few patients in either group reported prolactin-related events such as amenorrhea, galactorrhea, gynecomastia, or sexual side effects.39 Elevated prolactin levels have not been shown to be intrinsically harmful, although they can cause hypogonadism via negative feedback and inhibition of gonadotropin-releasing hormone, leading to inadequate follicle-stimulating hormone and luteinizing hormone.
Hyperprolactinemia also reduces serum testosterone levels in men, which may lead to decreased libido, impotence, infertility, gynecomastia, and rarely galactorrhea.40 Premenopausal women may experience infertility, oligomenorrhea or amenorrhea, galactorrhea, and reduced bone mineral density.41
Treatment options. When patients develop hyperprolactinemia, switching to another antipsychotic is not the only option.42 Standard therapies for hyperprolactinemia—the prodopaminergic drugs bromocriptine and amantadine—are effective, though they may have a slight tendency to provoke or worsen psychosis.43 In our experience, most patients can be managed with judicious dosages of bromocriptine (less than 5 mg/d) or even lower dosages of cabergoline (0.25 mg weekly to twice weekly), which causes very few psychiatric side effects.
Birth control pills are a reasonable alternative for women below age 35 who are nonsmokers—a relatively small proportion of those afflicted with schizophrenia but a much higher proportion of those likely to develop endocrine toxicities.
Sexual dysfunction
Sexual dysfunction—including decreased libido, impaired arousal, and erectile orgasmic dysfunction—is common among patients receiving atypical antipsychotics.44 These effects may be caused by anticholinergic activity, alpha-1 inhibition, and hypogonadism due to hyperprolactinemia.45 Delineating one specific cause of sexual dysfunction can be difficult because:
- antipsychotics are often administered with other psychotropics that influence sexual function
- schizophrenia itself is associated with sexual dysfunction.
The asociality associated with schizophrenia’s negative symptoms may be accompanied by decreased libido, fewer sexual thoughts, and fewer sexual relationships. In surveys, patients treated with atypical antipsychotics tend to report improved sex drive and libido but more erectile dysfunction and anorgasmia.46 Untreated patients report having fewer sexual thoughts and diminished libido but better erectile function and potency.47 The atypicals’ positive effect on social behavior may facilitate a willingness to engage in sexual activity, making sexual dysfunction more apparent.48
Priapism has been reported with all atypicals except ziprasidone.49 The vascular tone of the penis is in part sympathetically mediated, and alpha-1 blockade can inhibit detumescence via its indirect tendency to increase nitric oxide levels.50 Although priapism does not appear to be common, it is a urologic emergency with potential long-term consequences, including permanent erectile dysfunction. Patients developing abnormally prolonged and painful erections must be counseled to seek immediate medical attention.
Aripiprazole: Preliminary impressions
The recently approved antipsychotic aripiprazole differs from the now-familiar dopaminergic theme by being a partial agonist at the D2 receptor. Aripiprazole has the greatest affinity for the D2 receptor of any available drug, activates the postsynaptic complex at about 30% of the full endogenous DA affect, and appears to lack the metabolic consequences of the other atypicals.
In our research laboratory, aripiprazole has shown a profound prolactin lowering effect, superior subjective tolerability, and a more salutary impact on sexual function, compared with other antipsychotics. Although not devoid of EPS, aripiprazole appears to alter a patient’s subjective distress in a way that alters the risk/benefit ratio. Although aripiprazole’s clinical niche has yet to be established, it would be reasonable to use it for overweight patients intolerant of the dysphorogenic effects of other antipsychotics.
Related resources
- Wirshing DA, Wirshing WC, Kysar L, et al. Novel antipsychotics: comparison of weight gain liabilities J Clin Psychiatry 1999;60(6)358-63.
- Wirshing DA, Spellberg B, Erhart SM, Marder SR, Wirshing WC. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44(8):778-83.
- Wirshing DA, Pierre JM, Marder SR, Saunders CS, Wirshing WC. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56(1-2):25-30.
Drug brand names
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Donna Wirshing receives grant/research support from Pfizer Inc., Eli Lilly and Co., Janssen Pharmaceutica, and AstraZeneca Pharmaceuticals; is a consultant to Bristol-Myers Squibb Co., Janssen Pharmaceutica, and Pfizer Inc., and is a speaker for Eli Lilly and Co., Pfizer Inc., and Janssen Pharmaceutica.
Itai Danovitch reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Pierre receives grant/research support from Cephalon Inc.; is a consultant to Eli Lilly and Co., Bristol-Myers Squibb Co., AstraZeneca, and Pfizer Inc.; and is a speaker for Novartis Pharmaceuticals Corp., AstraZeneca Pharmaceuticals, and Janssen Pharmaceutica.
Dr. William Wirshing receives grant/research support from Janssen Pharmaceutica, Eli Lilly and Co., Otsuka America Pharmaceutical, Abbot Laboratories, Pfizer Inc., Sanofi-Synthelabo, Organon, Bristol-Myers Squibb Co., and Knoll Pharmaceuticals, and is a consultant to Janssen Pharmaceutica, Hoechst Marion Roussel, and Eli Lilly and Co.
Atypical antipsychotics are powerful medications for acute and chronic psychotic disorders, with a similarly powerful potential for adverse systemic effects. To use these agents to their greatest advantage, we must balance the benefits against the risks.
We often see patients with weight gain, diabetes, dyslipidemia, cardiac toxicity, hyperprolactinemia, and sexual dysfunction—all possible effects of atypical antipsychotics. Based on the latest evidence and our experience, we offer tips for using clozapine, olanzapine, quetiapine, risperidone, and ziprasidone, and preliminary impressions about the newly approved agent, aripiprazole.
Weight gain
Clinical trials have shown convincingly that atypical antipsychotics pose a greater risk of weight gain and central adiposity than do most older antipsychotics.1 Overweight and obesity are associated with increased risks of hypertension, type 2 diabetes, coronary heart disease, stroke, gallbladder disease, osteoarthritis, and some forms of cancer. Moreover, obesity’s socially stigmatizing effect can discourage patients with schizophrenia—particularly adolescents—from taking their medication.
Table 1
POTENTIAL FOR ADVERSE EFFECTS WITH ATYPICAL ANTIPSYCHOTICS
| Metabolic changes | Weight gain | Increased prolactin | QT interval | EPS | Sedation | Orthostasis | |
|---|---|---|---|---|---|---|---|
| Risperidone | + | + | +++ | + | ++ | + | ++ |
| Ziprasidone | + | + | − | ++ | + | + | + |
| Clozapine | +++ | +++ | − | ++ | +/− | +++ | +++ |
| Olanzapine | +++ | +++ | − | + | + | ++ | + |
| Quetiapine | ++ | ++ | − | ++ | + | ++ | ++ |
| Aripiprazole | + | + | − | + | + | +/− | +/− |
Comparative effects. Olanzapine and clozapine are associated with greater weight gain (Table 1)1-3 than risperidone and ziprasidone.4 Data regarding quetiapine are inconsistent—some studies show weight gain similar to that caused by olanzapine, and others find much less.5 Weight gain associated with quetiapine, ziprasidone, and risperidone tends to plateau within the first few months, whereas patients taking olanzapine and clozapine may continue to gain weight for 9 months or more.6
Adolescents and young adults may be particularly susceptible to antipsychotic-induced weight gain.7 No studies have directly compared weight gain in adults versus adolescents, but adolescents are exceedingly susceptible to the atypicals’ metabolic dysregulation. For example:
- A higher prevalence of extreme weight gain (>7% of baseline body mass) with olanzapine and risperidone has been reported in adolescent inpatients than among adults.7
- Extreme weight gain was seen in 78% of a group of risperidone-treated children; for 6 months, their weight gain averaged 1.2 kg/month without leveling off.8
These findings suggest that risperidone’s apparent metabolic advantage in adults disappears in children and adolescents. Risperidone’s effect on prolactin may account for a higher risk of weight gain in younger patients. These populations have exquisite end-organ sensitivity to changes in prolactin levels and may be more susceptible to the weight gain—and perhaps diabetes—believed related to hyperprolactinemia.9
Mechanisms. The mechanism(s) of weight gain may be related to the receptor systems upon which the atypicals act. These agents block noradrenergic, dopamine, serotonin, and histamine receptors, all of which are thought to affect metabolism or appetite control. Stimulation of alpha and D2 receptors by sympathomimetic amines causes weight loss, as does stimulation of certain 5HT receptors by weight-loss drugs such as fenfluramine.10 With respect to appetite, it has been suggested that peripheral antagonism of H1 receptors interferes with normal satiety signals.11 This may explain why affinity to histamine H1 receptors is among the best of correlates with potential for weight gain.12
Increases in serum levels of leptin—a peptide hormone produced in direct proportion to adiposity and thought to be anorexigenic, possibly through effects on satiety13 —parallel weight gain during treatment with atypicals. However, there is no indication that leptin imbalance causes weight gain; it may instead be the result. Altered sensitivity to leptin may be a contributing factor, perhaps at the hypothalamus.14
Diabetes
The risk of type 2 diabetes increases with weight gain,15 so it is no surprise that diabetes is more prevalent among patients taking atypicals. In a study of 38,000 schizophrenic patients, those taking atypicals were 9% more likely to have diabetes than those receiving typical antipsychotics,16 and all atypicals were associated with a significant increase in diabetes risk in patients younger than 40. The pervasiveness of diabetes17 and reports of new-onset diabetes in non-overweight patients18 suggest that—in addition to their effect on weight—atypicals may alter insulin and glucose metabolism.19
Atypical antipsychotics probably increase diabetes risk in a number of ways:
- An increase in adipose tissue can lead to insulin resistance, glucose intolerance, and ultimately diabetes.20
- Serotonin receptor antagonism may lead to hyperglycemia by decreasing pancreatic beta cell response to signals that advance insulin production.21
- Atypicals may contribute to hyperglycemia by impeding cellular uptake of glucose.22
- The increase in free fatty acids associated with atypicals can alter glucose metabolism. This may explain why clozapine and olanzapine—the atypicals with the greatest potential for severe hyperlipidemia—have the strongest association with new-onset diabetes.
Hyperlipidemia
Case reports and controlled studies have linked atypical antipsychotics with hyperlipidemia. Whether the hyperlipidemia is a consequence of weight gain or some other metabolic disturbance is unknown. Even without conclusive data, however, the link is of concern because elevated triglyceride levels represent an independent risk factor for heart disease.23
Although all atypicals increase serum triglycerides to some degree, severe hypertriglyceridemia occurs predominantly with clozapine and olanzapine.24 Both drugs have favorable efficacy profiles, and the mechanism of their antipsychotic activity may include altering the various lipid pools.
For example, studies have found that decreased triglyceride levels correlate with hostility and psychological distress.25 Increased triglycerides have been theorized to enhance membrane fluidity, which in turn may augment presynaptic reuptake of serotonin and diminish postsynaptic serotonin activity.26 In other words, elevated triglyceride levels could play a role in atypical antipsychotic-mediated inhibition of serotonin transmission. It is not yet known whether lipid-lowering drugs might alter atypicals’ efficacy.
Table 2
RECOMMENDED METABOLIC MONITORING OF PATIENTS TAKING ATYPICAL ANTIPSYCHOTICS
| Every visit | Check weight Check blood pressure |
| Every 3 months | Fasting blood glucose Fasting triglycerides Fasting cholesterol |
Metabolic monitoring
Managing mental illness concurrently with weight gain, diabetes, and hypertriglyceridemia is a challenge. In our clinic, we try to diminish the atypicals’ adverse metabolic effects by monitoring a few basic parameters and taking preventive measures (Table 2).
We routinely screen patients for diabetes symptoms by asking questions about changes in belt size (a sign of weight change), urinary frequency, and thirst (Table 3). We also document baseline weight, blood glucose (Table 4), blood chemistry, and lipid levels, with routine follow-up throughout therapy and greatest scrutiny during the first months of a new treatment.
Patients who cannot control their weight with lifestyle modifications (Table 5) may require a lipid-lowering medication—a “stain” and/or fibrate (such as gemfibrozil)—or, if those measures are ineffective, a switch to another antipsychotic. Hyperlipidemia and hyperglycemia may be reduced substantially when patients discontinue the aggravating medication.27
Although discontinuing or switching medications may reduce metabolic side effects, the hazard of psychotic decompensation is substantial. Achieving an antipsychotic effect is extremely difficult for most patients, and one should not discontinue an effective treatment without seriously considering the consequences. Antipsychotic efficacy should never be sacrificed in the pursuit of a regimen with more benign side effects. Consider switching to an atypical with a more moderate effect on weight, however, if weight gain would likely lead to noncompliance. Even the most effective treatment will not work if a patient never takes it.
Table 3
5 SCREENING QUESTIONS TO MONITOR FOR METABOLIC AND SEXUAL SIDE EFFECTS
|
Table 4
DIAGNOSTIC CRITERIA FOR DIABETES
| • Symptoms of diabetes (such as polyuria, polydipsia, or unexplained weight loss) plus nonfasting plasma glucose (PG) >200 mg/dL (11.1 mmol/L) |
| OR |
| • Fasting plasma glucose >126 mg/dL (7.0 mmol/L) |
| OR |
| • 2-hour PG >200 mg/dL during an oral glucose tolerance test |
| Source: American Diabetes Association |
Cardiac toxicity
QTc prolongation. Atypical antipsychotics—like their typical counterparts—cause QTc prolongation to varying degrees. On an ECG, the QT interval corresponds to cardiac depolarization and repolarization phases. The QT interval—which changes naturally with the time of day, stressors, and heart rate—is commonly corrected for heart rate to yield QTc.28 If QTc is prolonged beyond a certain threshold, repolarization can occur simultaneously with early depolarization. The consequence may be ventricular arrhythmias, such as torsades de pointes, which can degenerate into ventricular tachycardia, fibrillation, and even death.
All the atypicals are thought to prolong QT intervals to some degree by reducing the flow of repolarizing K+ currents, ultimately making the myocardium more excitable.29 Although there is no specific threshold above which torsades de pointes will occur, it appears there is no significant risk of developing arrhythmias below a QT interval of 500 msec.30 In fact, because the atypicals behave like type IIIa antiarrhythmics, they will overdrive the ventricle and suppress other emergent ventricular arrhythmias. Notwithstanding the FDA’s scrutiny of ziprasidone, no data indicate that this agent is disproportionately toxic.
Clinical precautions. Overall, atypicals cause only a modest increase in the QT interval. Ziprasidone and quetiapine appear to have somewhat more pronounced effects, with ziprasidone prolonging the QT interval on average about 20 msec.31 These mean increases are clinically irrelevant in most patients, but use caution when treating patients who:
- have pre-existing heart disease that is known to be associated with ventricular arrhythmias
- are taking other medications that prolong QT through the same mechanism
- have historically had idiosyncratic sensitivities to prolonged QT.32
Bradycardia, electrolyte imbalances, and endocrine disorders—which themselves increase QTc—also might make an individual more susceptible to the consequences of subtle QT prolongation.29
Managing patients at risk. In our clinic, we assess patients for risk of QT prolongation by inquiring about a family history of cardiac disease or a personal history of arrhythmia, syncope, or near syncope. In at-risk patients, we:
- monitor clinical progress more frequently, focusing on symptoms that suggest syncope or near syncope (unexplained episodic nausea, drowsiness)
- obtain routine ECGs to identify the rare population at increased risk for arrhythmia with either severely prolonged QT (>500 msec) or a serious AV conduction delay at baseline (second-degree or greater).
Laboratory tests should include electrolytes, as hypoleukemia is compellingly associated with development of arrhythmias.
Cardiac toxicity with clozapine. Reports of myocarditis and cardiomyopathy associated with clozapine have raised concern that this agent may be associated with other forms of cardiac toxicity. In January 2002, Novartis Pharmaceuticals Corp. reported 213 cases of myocarditis, 85% of which occurred while patients were taking recommended doses of clozapine within the first 2 months of therapy.33 Eosinophilia in many of the cases indicates that an IgE-mediated hypersensitivity reaction may be involved.34
Novartis also reported 178 cases of clozapineassociated cardiomyopathy, 80% of which occurred in patients younger than 50. Almost 20% of the incidents resulted in death, an alarming figure that may reflect either delay in diagnosis and treatment or simple reporting bias.
Detecting cardiac toxicity is particularly challenging because its manifestations—tachycardia, fatigue, and orthostatic hypotension—are frequently observed in clozapine-treated patients, particularly when dosages are changed.35 The poor specificity of signs for cardiac toxicity requires that we:
- identify at baseline patients with a personal or family history of heart disease
- set our threshold for suspicion of direct cardiotoxicity particularly low when titrating clozapine.36
Hyperprolactinemia
Higher elevations with risperidone. Many antipsychotics cause hyperprolactinemia because their antidopaminergic activity prevents dopamine from inhibiting prolactin secretion. Among the atypicals, however, only risperidone significantly elevates prolactin.37 Caracci et al also demonstrated a two- to four-fold greater prolactin elevation with risperidone than with typical antipsychotics38 and noted that hyperprolactinemia with risperidone could occur at standard daily doses.
We believe that risperidone’s tendency to disperse disproportionately within the plasma space accounts for its differential effect on D2 receptors in the tubuloinfundibular system (brain/plasma ratio of about 0.02 versus approximately 20 for most other antipsychotics). Thus, the lactotrophs, which are outside the blood brain barrier, are exposed to much higher levels of risperidone than are the D2 receptors within the CSF space, resulting in seemingly paradoxical co-occurence of EPS-free hyperprolactinemia.
Table 5
INTERVENTIONS TO CONTROL ANTIPSYCHOTIC-RELATEDWEIGHT GAIN
|
Clinical effects. Elevated prolactin levels do not necessarily lead to clinical symptoms. A large study comparing olanzapine and risperidone found that although more patients receiving risperidone had elevated prolactin levels, few patients in either group reported prolactin-related events such as amenorrhea, galactorrhea, gynecomastia, or sexual side effects.39 Elevated prolactin levels have not been shown to be intrinsically harmful, although they can cause hypogonadism via negative feedback and inhibition of gonadotropin-releasing hormone, leading to inadequate follicle-stimulating hormone and luteinizing hormone.
Hyperprolactinemia also reduces serum testosterone levels in men, which may lead to decreased libido, impotence, infertility, gynecomastia, and rarely galactorrhea.40 Premenopausal women may experience infertility, oligomenorrhea or amenorrhea, galactorrhea, and reduced bone mineral density.41
Treatment options. When patients develop hyperprolactinemia, switching to another antipsychotic is not the only option.42 Standard therapies for hyperprolactinemia—the prodopaminergic drugs bromocriptine and amantadine—are effective, though they may have a slight tendency to provoke or worsen psychosis.43 In our experience, most patients can be managed with judicious dosages of bromocriptine (less than 5 mg/d) or even lower dosages of cabergoline (0.25 mg weekly to twice weekly), which causes very few psychiatric side effects.
Birth control pills are a reasonable alternative for women below age 35 who are nonsmokers—a relatively small proportion of those afflicted with schizophrenia but a much higher proportion of those likely to develop endocrine toxicities.
Sexual dysfunction
Sexual dysfunction—including decreased libido, impaired arousal, and erectile orgasmic dysfunction—is common among patients receiving atypical antipsychotics.44 These effects may be caused by anticholinergic activity, alpha-1 inhibition, and hypogonadism due to hyperprolactinemia.45 Delineating one specific cause of sexual dysfunction can be difficult because:
- antipsychotics are often administered with other psychotropics that influence sexual function
- schizophrenia itself is associated with sexual dysfunction.
The asociality associated with schizophrenia’s negative symptoms may be accompanied by decreased libido, fewer sexual thoughts, and fewer sexual relationships. In surveys, patients treated with atypical antipsychotics tend to report improved sex drive and libido but more erectile dysfunction and anorgasmia.46 Untreated patients report having fewer sexual thoughts and diminished libido but better erectile function and potency.47 The atypicals’ positive effect on social behavior may facilitate a willingness to engage in sexual activity, making sexual dysfunction more apparent.48
Priapism has been reported with all atypicals except ziprasidone.49 The vascular tone of the penis is in part sympathetically mediated, and alpha-1 blockade can inhibit detumescence via its indirect tendency to increase nitric oxide levels.50 Although priapism does not appear to be common, it is a urologic emergency with potential long-term consequences, including permanent erectile dysfunction. Patients developing abnormally prolonged and painful erections must be counseled to seek immediate medical attention.
Aripiprazole: Preliminary impressions
The recently approved antipsychotic aripiprazole differs from the now-familiar dopaminergic theme by being a partial agonist at the D2 receptor. Aripiprazole has the greatest affinity for the D2 receptor of any available drug, activates the postsynaptic complex at about 30% of the full endogenous DA affect, and appears to lack the metabolic consequences of the other atypicals.
In our research laboratory, aripiprazole has shown a profound prolactin lowering effect, superior subjective tolerability, and a more salutary impact on sexual function, compared with other antipsychotics. Although not devoid of EPS, aripiprazole appears to alter a patient’s subjective distress in a way that alters the risk/benefit ratio. Although aripiprazole’s clinical niche has yet to be established, it would be reasonable to use it for overweight patients intolerant of the dysphorogenic effects of other antipsychotics.
Related resources
- Wirshing DA, Wirshing WC, Kysar L, et al. Novel antipsychotics: comparison of weight gain liabilities J Clin Psychiatry 1999;60(6)358-63.
- Wirshing DA, Spellberg B, Erhart SM, Marder SR, Wirshing WC. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44(8):778-83.
- Wirshing DA, Pierre JM, Marder SR, Saunders CS, Wirshing WC. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56(1-2):25-30.
Drug brand names
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Donna Wirshing receives grant/research support from Pfizer Inc., Eli Lilly and Co., Janssen Pharmaceutica, and AstraZeneca Pharmaceuticals; is a consultant to Bristol-Myers Squibb Co., Janssen Pharmaceutica, and Pfizer Inc., and is a speaker for Eli Lilly and Co., Pfizer Inc., and Janssen Pharmaceutica.
Itai Danovitch reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Pierre receives grant/research support from Cephalon Inc.; is a consultant to Eli Lilly and Co., Bristol-Myers Squibb Co., AstraZeneca, and Pfizer Inc.; and is a speaker for Novartis Pharmaceuticals Corp., AstraZeneca Pharmaceuticals, and Janssen Pharmaceutica.
Dr. William Wirshing receives grant/research support from Janssen Pharmaceutica, Eli Lilly and Co., Otsuka America Pharmaceutical, Abbot Laboratories, Pfizer Inc., Sanofi-Synthelabo, Organon, Bristol-Myers Squibb Co., and Knoll Pharmaceuticals, and is a consultant to Janssen Pharmaceutica, Hoechst Marion Roussel, and Eli Lilly and Co.
1. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
2. Henderson D, Cagliero E, Gray C, et al. Clozapine, diabetes mellitus, weight gain and lipid abnormalities: a five year naturalistic study. Am J Psychiatry 2000;157(6):975-81.
3. Kinon BJ, Basson BR, Gilmore JA, et al. Long-term olanzapine treatment: weight change and weight-related health factors in schizophrenia. J Clin Psychiatry 2001;62:92-100.
4. Ganguli R. Weight gain associated with antipsychotic drugs J Clin Psychiatry 1999;60:20-4.
5. McIntyre RS, McCann SM, Kennedy SH. Antipsychotic metabolic effects: weight gain, diabetes mellitus, and lipid abnormalities. Can J Psychiatry 2001;46:273-281.
6. Taylor DM, McAskill R. Atypical antipsychotics and weight gain—a systematic review. Acta Psychiatry Scand 2000;101:416-32.
7. Haapasalo-Pesu KM, Saarijarvi S. Olanzapine induces remarkable weight gain in adolescent patients. Eur Child Adolesc Psychiatry 2001;10:205-8.
8. Martin A, Landau J, Leebens P, et al. Risperidone-associated weight gain in children and adolescents: a retrospective chart review. J Child Adolesc Psychopharmacol 2000;10:259-68.
9. Wirshing DA, Spellberg BJ, Erhart SM, et al. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44:778-83.
10. Bray G. Drug treatment of obesity. Rev Endocr Metab Disord 2001;2(4):403-18.
11. Kaur G, Kulkarni SK. Studies on modulation of feeding behavior by atypical antipsychotics in female mice. Prog Neuropsychopharmacol Biol Psychiatry 2002;26:277-85.
12. Wirshing D, Wirshing W, Kysar L, et al. Novel antipsychotics: Comparison of weight gain liabilities. J Clin Psychiatry 1999;60:358-63.
13. Bray GA, York DA. Clinical review 90: Leptin and clinical medicine: a new piece in the puzzle of obesity. J Clin Endocrinol Metab 1997;82:2771-6.
14. Baptista T, Lacruz A, De Mendoza D, et al. Body weight gain after administration of antipsychotic drugs. Pharmacopsychiatry 2002;35:36.-
15. Helmrich SP, Ragland DR, Leung RW, et al. Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus. N Engl J Med 1991;325:147-52.
16. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
17. Henderson DC. Atypical antipsychotic-induced diabetes mellitus: how strong is the evidence? CNS Drugs 2002;16:77-89.
18. Ramankutty G. Olanzapine-induced destabilization of diabetes in the absence of weight gain. Acta Psychiatry Scand 2002;105:235-7.
19. Muench J, Carey M. Diabetes mellitus associated with atypical antipsychotic medications: new case report and review of the literature. J Am Board Fam Pract 2001;14:278-82.
20. Beck-Nielsen H, Groop LC. Metabolic and genetic characterization of prediabetic states. Sequence of events leading to non-insulin-dependent diabetes mellitus. J Clin Invest 1994-94:1714-21.
21. Wozniak K, Linnoila M. Hyperglycemic properties of serotonin receptor antagonists. Life Sci 1991;49:101-9.
22. Ardizzone TD, Bradley RJ, Freeman AM, 3rd, et al. Inhibition of glucose transport in PC12 cells by the atypical antipsychotic drugs risperidone and clozapine, and structural analogs of clozapine. Brain Res 2001;923:82-90.
23. Wilson PW. Established risk factors and coronary artery disease: the Framingham Study. Am J Hypertens 1994;7:7S-12S.
24. Meyer JM. Novel antipsychotics and severe hyperlipidemia. J Clin Psychopharmacol 2001;21:369-74.
25. Niaura R, Banks SM, Ward KD, et al. Hostility and the metabolic syndrome in older males: the normative aging study. Psychosom Med 2000;62:7-16.
26. Diebold K, Michel G, Schweizer J, et al. Are psychoactive-drug-induced changes in plasma lipid and lipoprotein levels of significance for clinical remission in psychiatric disorders? Pharmacopsychiatry 1998;31:60-7.
27. Bechara CI, Goldman-Levine JD. Dramatic worsening of type 2 diabetes mellitus due to olanzapine after 3 years of therapy. Pharmacotherapy 2001;21:1444-7.
28. Garson A, Jr. How to measure the QT interval—what is normal? Am J Cardiol 1993;72:14B-16B.
29. Tan HL, Hou CJ, Lauer MR, et al. Electrophysiologic mechanisms of the long QT interval syndromes and torsade de pointes. Ann Intern Med 1995;122:701-14.
30. Morganroth J, Brozovich FV, McDonald JT, et al. Variability of the QT measurement in healthy men, with implications for selection of an abnormal QT value to predict drug toxicity and proarrhythmia. Am J Cardiol 1991;67:774-6.
31. Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations: Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations Diabetes Care 2000;23:S4.-
32. Joerg C K-WS, Beasley CM. Cardiac safety parameters of olanzapine: comparison with other atypical and typical antipsychotics. J Clin Psychiatry 2001;2:35-40.
33. Association of Clozaril with cardiovascular toxicity. [Dear healthcare professional letter]. Novartis Pharmaceuticals Canada Inc, 2002.
34. Killian JG, Kerr K, Lawrence C. Myocarditis and cardiomyopathy associated with clozapine. Lancet 1999;354:1841-5.
35. Lieberman JA, Safferman AZ. Clinical profile of clozapine: adverse reactions and agranulocytosis. Psychiatr Q 1992;63:51-70.
36. Wooltorton E. Antipsychotic clozapine (Clozaril): myocarditis and cardiovascular toxicity. CMAJ 2002;166:1185-6.
37. Breier AF, Malhotra AK, Su T, et al. Clozapine and risperidone in chronic schizophrenia: effects on symptoms, parkinsonian side effects, and neuroendocrine response. Am J Psychiatry 1999;156:294-8.
38. Caracci G. Prolactin levels in premenopausal women treated with risperidone compared with those of women treated with typical neuroleptics. J Clin Psychopharmacology 1999;19:194-6.
39. Conley RR, Mahmoud R. A randomized double-blind study of risperidone and olanzapine in the treatment of schizophrenia or schizoaffective disorder. Am J Psychiatry 2001;158:765-74.
40. Segal S, Yaffe H, Laufer N, et al. Male hyperprolactinemia: effects on fertility. Fertil Steril 1979;32:556-61.
41. Schlechte J, Walkner L, Kathol M. A longitudinal analysis of premenopausal bone loss in healthy women and women with hyperprolactinemia. J Clin Endocrinol Metab 1992;75:698-703.
42. Gazzola LR, Opler LA. Return of menstruation after switching from risperidone to olanzapine. J Clin Psychopharmacol 1998;18:486-7.
43. Boyd A. Bromocriptine and psychosis: a literature review. Psychiatr Q 1995;66:87-95.
44. Aizenberg D, Modai I, Landa A, et al. Comparison of sexual dysfunction in male schizophrenic patients maintained on treatment with classical antipsychotics versus clozapine. J Clin Psychiatry 2001;62:541-4.
45. Meston CM. Sympathetic nervous system activity and female sexual arousal. Am J Cardiol 2000;86:30F-34F.
46. Wirshing DA, Pierre JM, Marder SR, et al. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56:25-30.
47. Aizenberg D, Zemishlany Z, Dorfman-Etrog P, et al. Sexual dysfunction in male schizophrenic patients. J Clin Psychiatry 1995;56:137-41.
48. Hummer M, Kemmler G, Kurz M, et al. Sexual disturbances during clozapine and haloperidol treatment for schizophrenia. Am J Psychiatry 1999;156:631-3.
49. Pais VM, Ayvazian PJ. Priapism from quetiapine overdose: first report and proposal of mechanism. Urology 2001;58:462.-
50. Compton MT, Miller AH. Priapism associated with conventional and atypical antipsychotic medications: a review. J Clin Psychiatry 2001;62:362-6.
1. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
2. Henderson D, Cagliero E, Gray C, et al. Clozapine, diabetes mellitus, weight gain and lipid abnormalities: a five year naturalistic study. Am J Psychiatry 2000;157(6):975-81.
3. Kinon BJ, Basson BR, Gilmore JA, et al. Long-term olanzapine treatment: weight change and weight-related health factors in schizophrenia. J Clin Psychiatry 2001;62:92-100.
4. Ganguli R. Weight gain associated with antipsychotic drugs J Clin Psychiatry 1999;60:20-4.
5. McIntyre RS, McCann SM, Kennedy SH. Antipsychotic metabolic effects: weight gain, diabetes mellitus, and lipid abnormalities. Can J Psychiatry 2001;46:273-281.
6. Taylor DM, McAskill R. Atypical antipsychotics and weight gain—a systematic review. Acta Psychiatry Scand 2000;101:416-32.
7. Haapasalo-Pesu KM, Saarijarvi S. Olanzapine induces remarkable weight gain in adolescent patients. Eur Child Adolesc Psychiatry 2001;10:205-8.
8. Martin A, Landau J, Leebens P, et al. Risperidone-associated weight gain in children and adolescents: a retrospective chart review. J Child Adolesc Psychopharmacol 2000;10:259-68.
9. Wirshing DA, Spellberg BJ, Erhart SM, et al. Novel antipsychotics and new-onset diabetes. Biol Psychiatry 1998;44:778-83.
10. Bray G. Drug treatment of obesity. Rev Endocr Metab Disord 2001;2(4):403-18.
11. Kaur G, Kulkarni SK. Studies on modulation of feeding behavior by atypical antipsychotics in female mice. Prog Neuropsychopharmacol Biol Psychiatry 2002;26:277-85.
12. Wirshing D, Wirshing W, Kysar L, et al. Novel antipsychotics: Comparison of weight gain liabilities. J Clin Psychiatry 1999;60:358-63.
13. Bray GA, York DA. Clinical review 90: Leptin and clinical medicine: a new piece in the puzzle of obesity. J Clin Endocrinol Metab 1997;82:2771-6.
14. Baptista T, Lacruz A, De Mendoza D, et al. Body weight gain after administration of antipsychotic drugs. Pharmacopsychiatry 2002;35:36.-
15. Helmrich SP, Ragland DR, Leung RW, et al. Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus. N Engl J Med 1991;325:147-52.
16. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
17. Henderson DC. Atypical antipsychotic-induced diabetes mellitus: how strong is the evidence? CNS Drugs 2002;16:77-89.
18. Ramankutty G. Olanzapine-induced destabilization of diabetes in the absence of weight gain. Acta Psychiatry Scand 2002;105:235-7.
19. Muench J, Carey M. Diabetes mellitus associated with atypical antipsychotic medications: new case report and review of the literature. J Am Board Fam Pract 2001;14:278-82.
20. Beck-Nielsen H, Groop LC. Metabolic and genetic characterization of prediabetic states. Sequence of events leading to non-insulin-dependent diabetes mellitus. J Clin Invest 1994-94:1714-21.
21. Wozniak K, Linnoila M. Hyperglycemic properties of serotonin receptor antagonists. Life Sci 1991;49:101-9.
22. Ardizzone TD, Bradley RJ, Freeman AM, 3rd, et al. Inhibition of glucose transport in PC12 cells by the atypical antipsychotic drugs risperidone and clozapine, and structural analogs of clozapine. Brain Res 2001;923:82-90.
23. Wilson PW. Established risk factors and coronary artery disease: the Framingham Study. Am J Hypertens 1994;7:7S-12S.
24. Meyer JM. Novel antipsychotics and severe hyperlipidemia. J Clin Psychopharmacol 2001;21:369-74.
25. Niaura R, Banks SM, Ward KD, et al. Hostility and the metabolic syndrome in older males: the normative aging study. Psychosom Med 2000;62:7-16.
26. Diebold K, Michel G, Schweizer J, et al. Are psychoactive-drug-induced changes in plasma lipid and lipoprotein levels of significance for clinical remission in psychiatric disorders? Pharmacopsychiatry 1998;31:60-7.
27. Bechara CI, Goldman-Levine JD. Dramatic worsening of type 2 diabetes mellitus due to olanzapine after 3 years of therapy. Pharmacotherapy 2001;21:1444-7.
28. Garson A, Jr. How to measure the QT interval—what is normal? Am J Cardiol 1993;72:14B-16B.
29. Tan HL, Hou CJ, Lauer MR, et al. Electrophysiologic mechanisms of the long QT interval syndromes and torsade de pointes. Ann Intern Med 1995;122:701-14.
30. Morganroth J, Brozovich FV, McDonald JT, et al. Variability of the QT measurement in healthy men, with implications for selection of an abnormal QT value to predict drug toxicity and proarrhythmia. Am J Cardiol 1991;67:774-6.
31. Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations: Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus Practice Recommendations Diabetes Care 2000;23:S4.-
32. Joerg C K-WS, Beasley CM. Cardiac safety parameters of olanzapine: comparison with other atypical and typical antipsychotics. J Clin Psychiatry 2001;2:35-40.
33. Association of Clozaril with cardiovascular toxicity. [Dear healthcare professional letter]. Novartis Pharmaceuticals Canada Inc, 2002.
34. Killian JG, Kerr K, Lawrence C. Myocarditis and cardiomyopathy associated with clozapine. Lancet 1999;354:1841-5.
35. Lieberman JA, Safferman AZ. Clinical profile of clozapine: adverse reactions and agranulocytosis. Psychiatr Q 1992;63:51-70.
36. Wooltorton E. Antipsychotic clozapine (Clozaril): myocarditis and cardiovascular toxicity. CMAJ 2002;166:1185-6.
37. Breier AF, Malhotra AK, Su T, et al. Clozapine and risperidone in chronic schizophrenia: effects on symptoms, parkinsonian side effects, and neuroendocrine response. Am J Psychiatry 1999;156:294-8.
38. Caracci G. Prolactin levels in premenopausal women treated with risperidone compared with those of women treated with typical neuroleptics. J Clin Psychopharmacology 1999;19:194-6.
39. Conley RR, Mahmoud R. A randomized double-blind study of risperidone and olanzapine in the treatment of schizophrenia or schizoaffective disorder. Am J Psychiatry 2001;158:765-74.
40. Segal S, Yaffe H, Laufer N, et al. Male hyperprolactinemia: effects on fertility. Fertil Steril 1979;32:556-61.
41. Schlechte J, Walkner L, Kathol M. A longitudinal analysis of premenopausal bone loss in healthy women and women with hyperprolactinemia. J Clin Endocrinol Metab 1992;75:698-703.
42. Gazzola LR, Opler LA. Return of menstruation after switching from risperidone to olanzapine. J Clin Psychopharmacol 1998;18:486-7.
43. Boyd A. Bromocriptine and psychosis: a literature review. Psychiatr Q 1995;66:87-95.
44. Aizenberg D, Modai I, Landa A, et al. Comparison of sexual dysfunction in male schizophrenic patients maintained on treatment with classical antipsychotics versus clozapine. J Clin Psychiatry 2001;62:541-4.
45. Meston CM. Sympathetic nervous system activity and female sexual arousal. Am J Cardiol 2000;86:30F-34F.
46. Wirshing DA, Pierre JM, Marder SR, et al. Sexual side effects of novel antipsychotic medications. Schizophr Res 2002;56:25-30.
47. Aizenberg D, Zemishlany Z, Dorfman-Etrog P, et al. Sexual dysfunction in male schizophrenic patients. J Clin Psychiatry 1995;56:137-41.
48. Hummer M, Kemmler G, Kurz M, et al. Sexual disturbances during clozapine and haloperidol treatment for schizophrenia. Am J Psychiatry 1999;156:631-3.
49. Pais VM, Ayvazian PJ. Priapism from quetiapine overdose: first report and proposal of mechanism. Urology 2001;58:462.-
50. Compton MT, Miller AH. Priapism associated with conventional and atypical antipsychotic medications: a review. J Clin Psychiatry 2001;62:362-6.