User login
Advance care planning: Beyond the living will
Mr. B., an 82-year-old retired accountant with hypertension, was diagnosed with early Alzheimer disease 6 years ago. He now needs supervision with bathing and dressing and no longer consistently recognizes family members. You are seeing him in the office today after a hospitalization for aspiration pneumonia, his second in the past 6 months.
In the hospital, a brain scan showed that atrophy had progressed and white-matter disease was more extensive than 3 years earlier. A barium swallow study showed esophageal dysmotility and aspiration. He was prescribed a “dysphagia diet,”1 which he dislikes.
Since returning home, he has been disoriented, he has been wandering about the house, and he has fallen several times. He has lost 10 pounds in 6 months. Because of his confusion, his wife cannot take him out, and she is exhausted caring for him.
Reviewing his medical record, you note that 10 years ago, Mr. B. completed a living will and designated his wife as his proxy decision-maker via a medical power of attorney document.
PLANNING IS OFTEN NEGLECTED
Many clinicians and older patients feel a strong need to document, in advance, the patient’s wishes regarding medical care in the event the patient becomes seriously ill and unable to participate in treatment decisions. Professional societies such as the American Geriatrics Society promote advance care planning,2 and some indices of the quality of medical care include whether advance directives have been discussed and completed.3
Yet, despite the high profile of advance care planning,4 few patients actually fill out advance directives,5 with completion rates that vary widely,6–8 sometimes by ethnicity and sex.9,10 Furthermore, in a crisis, these directives are seldom followed.11
In this paper, we recommend an approach to advance care planning for older adults that redirects the focus from “signing away” interventions such as dialysis, mechanical ventilation, and tube feeding. Instead, the focus is on the goals of care. We also advocate naming a surrogate decision-maker, since the medical power of attorney is more flexible and more widely applicable than the living will.
START BY LISTENING
A change in function resulting from disease progression, hospitalization, trauma, or other reasons is an ideal opportunity to introduce the process of advance care planning.
The first step is to find out how well the patient and family understand the patient’s relevant medical conditions, and what their expectations, hopes, and concerns are. This listening phase can provide insight into the patient’s values and goals and how much the patient and family want to engage in these discussions.
In matters of health behavior (such as advance care planning), people change only when they are ready to change.12,13 Thus, we advise physicians to defer extensive discussions of values and goals of care until patients and families are ready to listen, hear, and talk about these topics (often, after a change for the worse in prognosis).
And it is a process. Advance care directives are most likely to be set up and followed if the patient and doctor discuss this issue during multiple visits, rather than if the physician merely hands the patient a packet of forms and information.14–16
CASE CONTINUED: A PEG TUBE REFUSED
Mrs. B. says that Mr. B. is in good health except for his memory: he does not have a serious condition such as diabetes, heart failure, or cancer. While Mr. B. was in the hospital, the hospitalist recommended placing a percutaneous endoscopic gastrostomy (PEG) tube, but Mrs. B. declined the recommendation because her husband had a living will that specified “no artificially or technologically supplied nutrition or hydration.”
At this point, Mrs. B. begins to cry. She has slept poorly because of his wandering. Also, her two daughters do not support her refusal of the PEG tube.
Comment. This brief conversation illuminates knowledge deficits in Mrs. B.’s understanding of Alzheimer disease and the circumstances in which the living will applies. Although one could argue that Mr. B.’s Alzheimer disease has advanced to the point that he is likely to die of a complication of that condition, he is not likely to die in the near future. If he is not considered by law and his physician to be terminally ill or permanently unconscious, a living will likely does not offer guidance about artificial feeding.
LIMITATIONS OF A LIVING WILL
A living will, a commonly used advance directive, states that the patient does not wish to receive life-sustaining treatment in the event that he or she suffers an incurable, irreversible disease and cannot give informed consent, and it often lists specific treatments that the patient does not want. However, we believe that approaching the patient with a list of life-sustaining measures to accept or reject, before discussing goals of care and prognosis, puts the cart before the horse. This approach threatens to distract from the need to ascertain values and offer appropriate care. Additionally, a living will is active only within a very limited scenario and does not address relatively routine but important decisions in a person’s care.
All ‘terminal illness’ isn’t the same
A living will goes into effect only if the patient either enters a permanent vegetative state following an event such as cardiac arrest or severe brain trauma, or is diagnosed with a terminal illness such as metastatic cancer, and lacks decision-making capacity.
But what is terminal illness? The definition differs from state to state, but it is generally defined as an irreversible condition leading to death in a relatively short time. The time may not be specified, as in Florida statute 765. In contrast, Ohio Revised Code 2133.01(AA) uses the phrase “relatively short,” while other states specify a time, such as within 6 months (Texas Health and Safety Code 166.002). The Medicare hospice benefit also carries a short time limit, usually less than 6 months.
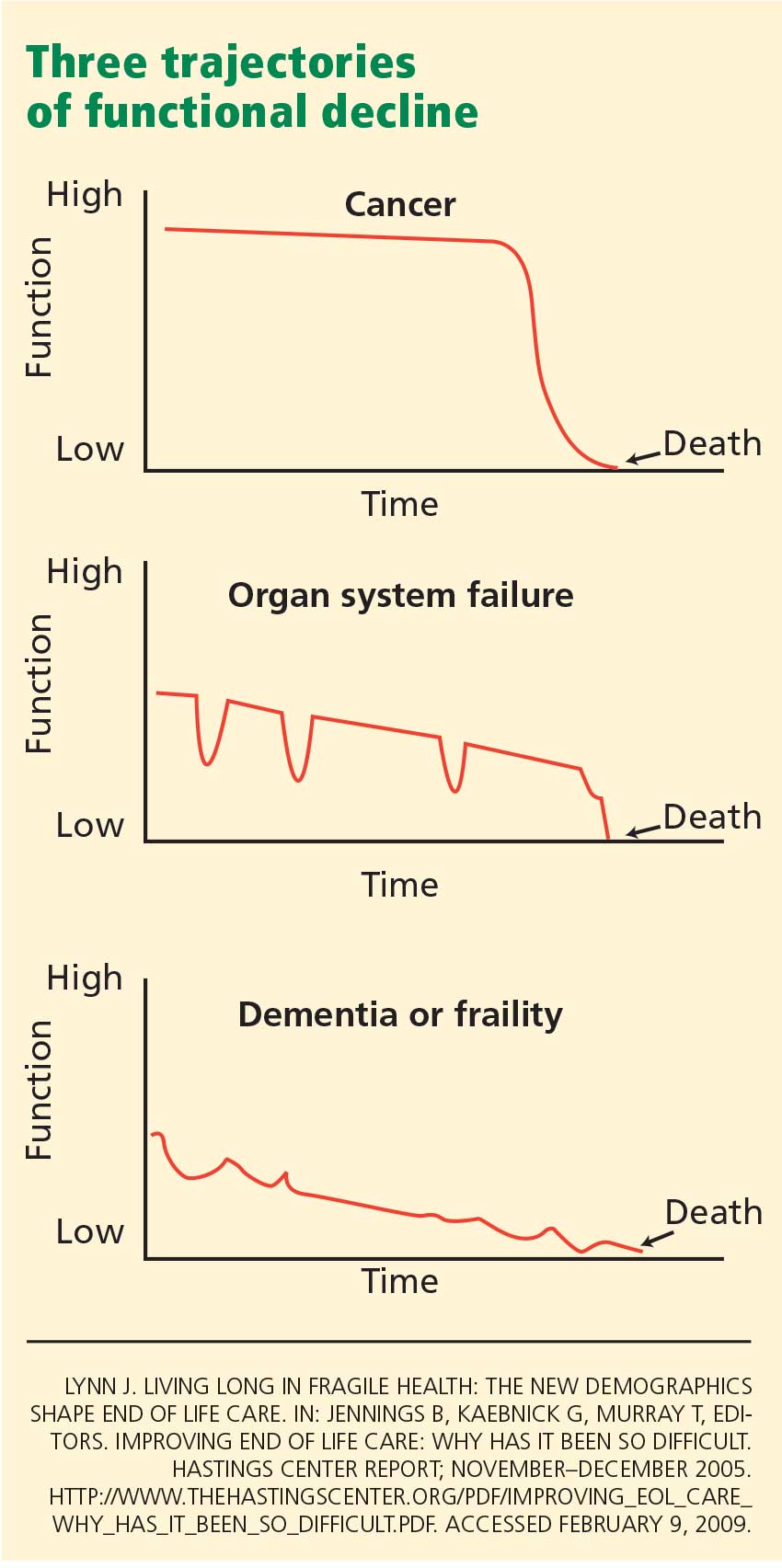
The middle panel in Figure 1 depicts a more typical decline from serial organ insults such as stroke followed by infection from aspiration or followed by falls. Older adults with dementia or with multiple progressive diseases such as heart failure, diabetes, hypertension, or cancer decline in a trajectory such as in the bottom panel of Figure 1.
A living will might not be activated in the latter two scenarios until years into the condition because the patient would not be considered terminally ill—by state law, by the health care provider, or even by the patient.
The living will does not address routine interventions
In most states, living wills address only life-sustaining treatments such as dialysis, mechanical ventilation, and medically supplied nutrition and hydration. Living wills do not address relatively common diseases in older adults that could cause severe debility, such as a major stroke or advanced dementia.
If an older patient has dementia, a living will is unlikely to provide guidance about interventions such as intubation to get through an episode of potentially reversible respiratory failure, a feeding tube to correct weight loss, or cardiac catheterization or bypass surgery to treat angina. Yet these important decisions often arise as function declines and comorbidities progress.
Patients may change their minds
Many older adults are reluctant to sign documents to “micromanage” their future care if they should become ill.19 Many people change their mind as the situation changes.11,20,21 Although few claim they would want burdensome interventions if they had dementia22 or if their prognosis were poor,23 patients may tolerate more burdensome interventions if they are already receiving treatments for chronic illnesses such as end-stage renal disease.24
Thus, a living will may help if unexpected trauma occurs in a healthy person, but not so much if chronic illness progresses over a period of years.
Advance directives may not be honored
Even if completed, written advance directives may not be followed, for a variety of reasons. Physicians may not know the patient has a living will, and fewer than one-third of people who actually complete an advance directive have discussed its content with a physician.25 The people named as surrogate decision-makers may not know the patient’s wishes. Family members may disagree with the goals and plan of care and may interfere with implementation of the advance care plan. A patient may see multiple physicians at different institutions who may not communicate with each other about the patient’s wishes. Also, physicians and patients may interpret terms such as “terminally ill” differently, making it difficult to translate the documents into an action plan.
CASE CONTINUED: RELIEVING CAREGIVER STRESS
Returning to Mr. B., your first goal is to address care issues, including caregiver stress. Skilled services in the home are appropriate for him at this time (and Medicare will pay for them) because he is still homebound. These services could include physical therapy, occupational therapy, and speech (swallowing) therapy. A home care agency may also provide an aide for a few weeks to assist with bathing and other personal needs.
You strongly recommend that the family (including both daughters) participate in the Alzheimer’s Association educational programs. You recommend that Mrs. B. locate an adult day care program now so that when Mr. B. completes his home therapy course and is no longer homebound, he may attend. Day care would provide a therapeutic environment for him and respite for her.
You request that the home care agency provide a social worker to advise her on community resources. Meta-analysis suggests that structured, multicomponent interventions with caregivers of demented patients reduce several types of caregiver burden and delay institutionalization.26
He improves with conservative measures
Three weeks later, Mr. B. is sleeping better and has stopped wandering. However, he dislikes the thickened liquids required by the dysphagia diet and has lost another 2 pounds. If his beverages are not thickened, he coughs profusely when he swallows. His daughters are still pressuring Mrs. B. for a PEG tube; one of them has angrily asserted that the doctors are going to allow her father to die.
You explain the burdens of PEG tubes: surgical risks, continued aspiration, disrupted bowel habits, the risk of the tube being accidentally or intentionally dislodged by the patient, and special binders (which may be uncomfortable) or restraints (which may cause further functional decline) that may be necessary to prevent this complication.
You request that the speech therapist work with the patient more aggressively in the use of swallowing techniques such as the chin tuck, which may be at least as effective as thickeners in preventing both aspiration pneumonia and dehydration.27 The therapist will need to include Mrs. B. in these sessions, since she will be Mr. B.’s coach at mealtime.
With more aggressive speech therapy, the patient’s weight stabilizes over the next 4 weeks. He is in day care 3 days a week, and Mrs. B. is more rested and relaxed.
Cardiopulmonary resuscitation
You continue the advance care planning discussion and suggest that if Mr. B. aspirates, is hospitalized again, and declines further care, it would be helpful to delineate instructions for resuscitation. Right now, although his Alzheimer disease is advanced, he is not clearly terminal. Thus, his living will does not strictly apply and provides limited guidance about intubation, cardiopulmonary resuscitation (CPR), or medically supplied nutrition and hydration. However, because Mrs. B. is his agent in the medical power of attorney, this document enables her to make a wide spectrum of treatment decisions on his behalf.
Mrs. B. asks about her husband’s prognosis and why CPR would not be helpful.
Comment. Further discussion with her could be guided by an estimate of Mr. B.’s prognosis. Function-based tools28,29 may also be useful. For example,28,30 an 80-year-old man with high functional status might have a life expectancy of more than 10 years. Mr. B., with multiple medical problems and declining function, would have an estimated life expectancy of approximately 3 years. Even without specifically categorizing function, impaired cognition by itself predicted a shorter life expectancy in population-based studies.31,32
Regarding CPR, patients and families may overestimate successful outcomes. A recent study33 of 10 years of outcomes of in-hospital cardiac arrest found that only 6.6% of patients survived to discharge. The average age of the survivors was 59 years, and fewer than half of them survived 3 years after cardiac arrest. In eight studies of CPR outcomes in nursing homes,34 three studies had no survivors, and all but one study had a survival rate below 5%.
PROVIDING APPROPRIATE CARE, NOT LIMITING TREATMENTS
In the case of Mr. B., as in many situations encountered with older patients, written advance directives provide little help or guidance. Instead, we recommend a model of advance care planning that takes place during multiple office visits over time, and that maintains a focus on providing appropriate care rather than on limiting life-sustaining treatments. We recommend providing estimates of prognosis and CPR outcomes when the family appeares ready to hear them. This approach should result in a care-oriented process while moving the family towards decisions regarding artificial feeding and CPR.
All patients, particularly those unwilling or unable to participate in advance care planning, are encouraged to identify one or more surrogate decision-makers and articulate how much flexibility that person should be given in important health care decisions. The medical power of attorney can be activated any time the patient lacks decision-making capacity and deactivated when decision-making capacity returns.38,39
As in the case of Mr. B., a tailored approach to advance care planning requires clinicians to estimate life expectancy (more than 5 years, less than 5 years, or less than 1 year) and to determine the patient’s and the family’s readiness to focus on a values-oriented and goal-oriented care plan. Some patients are not receptive to advance care planning, and clinical time and effort are optimized by providing the right amount of information to patients when they are ready to receive it.
For relatively healthy older adults
Figure 2 is the algorithm for older patients who are expected to live at least 5 years, ie, who are relatively healthy and functional. Patients with little or no interest in advance care planning can be asked about it annually, or sooner if their medical condition changes. Patients with limited interest can be given written information, specifically living will and medical power of attorney documents recognized in their state. Patients more open to advance care planning can be offered a values history form (Table 1), Web sites, and educational materials, with a plan to discuss them at future appointments.
Periodic reevaluation of values and goals of care is important. Patients may assert that particular interventions (eg, a PEG tube or dialysis) are “worse than death” when they are healthy, but they may change their views over time.21 Additionally, although a recent hospitalization or a decline in function may predispose patients to want to limit life-sustaining treatments, they may return to their earlier values and wishes a few months later, particularly if their medical condition stabilizes. 20 Values and decisions should be reassessed not only when medical conditions deteriorate, but also when they improve.
For chronically ill patients
Caregiver stress is important to identify and address, since caregivers often neglect themselves.40–42
For terminally ill patients
In this situation, patients and families need information about community resources that can assist them in the home. Some older adults with cognitive impairment may be exploited or neglect themselves, and referral to an adult protective services agency may be needed.
Treatment burden, particularly due to multiple prescribed medications, may be high and should be reassessed in light of the goals of treatment. Polypharmacy reduction is especially important at this stage in the illness, since the goals of care may be different than when the medications were prescribed.
Physical or psychosocial symptoms may be the cue to bring up the topic of palliative care. If the patient is expected to live less than 6 months, hospice referral is appropriate. With either palliative care or hospice, the focus of attention shifts explicitly from curing the disease to managing symptoms, and from the patient to the patient-family dyad. Interventions such as CPR and ventilatory support should be discussed and information from Table 2 provided to the patient and family.
Complete advance care planning incorporates taking a values history, estimating life expectancy, determining physical, psychosocial and spiritual needs, clarifying treatment goals, and estimating manageable treatment burden. Offering statistics on CPR and providing state-specific living will and medical power of attorney documents are important but are only one facet of effective advance care planning. In fact, shifting the emphasis of advance care planning from statistics and forms to values and goals of care may help in developing a more comprehensive care plan.
Goals of care range from curing the disease (with aggressive therapy, which may be burdensome) to simply improving function or decreasing pain. In the latter case, one may be able to discontinue some of the patient’s drugs, utilize medical and community resources more effectively, and better meet the patient’s needs.
Woven through all these discussions should be reassurance that the plan can be revisited and possibly revised, and that the physician will be there to help with those decisions.
For acutely ill patients in the hospital
Episodic, staged advance care planning is appropriate not only in the office but also in other settings such as assisted living and nursing facilities.
In the hospital, however, a different approach is needed, since patients are usually admitted because of an acute illness or sudden functional decline, or both. Decisions about technological interventions such as CPR, mechanical ventilation, or dialysis may be needed urgently. Often, patients are unable to provide guidance to physicians during acute illness because of delirium and other impediments. Developing a plan for care in the hospital may require urgent family meetings. However, if a surrogate decision-maker is in place, and if the patient has already participated in some form of advance care planning as an outpatient, the values and goals of care previously identified can contribute to decision-making during hospitalization.
As mentioned above, fragmentation of health care across providers and health care systems may limit the effectiveness of office-based advance care planning. It may be reasonable to train office staff to place advance care planning documentation in easily accessible sections of the patient’s medical record and to forward these to specialists involved in a patient’s care.
The patient and family should be encouraged and empowered to help with this process and should have updated advance care planning documentation readily available. In some states, comprehensive medical order sets, especially for end-of-life care, are portable across care settings and address CPR, medically supplied nutrition, hospital transfer, and antibiotic treatment.43
Research suggests that health care systems are more likely to comply with patients’ end-of-life preferences when portable medical order forms are developed and disseminated.44–44 Ultimately, major changes in health care delivery, including universal electronic health records, may be needed to implement and communicate patients’ advance care planning preferences across settings.
- National Dysphagia Diet Task Force. National Dysphagia Diet: Standardization for Optimal Care. Chicago, IL: American Dietetic Association, 2002.
- Nusbaum N, Goldstein M. American Geriatrics Society. The Patient Education Forum. Advance Directives, 2008. www.americangeriatrics.org/education/forum/advance_dir.shtml. Accessed March 9, 2009.
- Wenger NS, Roth CP, Shekelle PA; COVE Investigators. Introduction to the assessing care of vulnerable elders–3 quality indicator measurement set. J Am Geriatr Soc 2007; 55(suppl 2):S247–S252.
- Emanuel LL, Danis M, Pearlman RA, Singer PA. Advance care planning as a process: structuring the discussions in practice. J Am Geriatr Soc 1995; 43:440–446.
- Teno J, Lynn J, Wenger N, et al. Advance directives for seriously ill hospitalized patients: effectiveness with the patient self-determination act and the SUPPORT intervention. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatment. J Am Geriatr Soc 1997; 45:500–507.
- Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Arch Intern Med 1998; 158:383–390.
- Gordon NP, Shade SB. Advance directives are more likely among seniors asked about end-of-life care p. Arch Intern Med 1999; 159:701–704.
- Morrison RS, Meier DE. High rates of advance care planning in New York City’s elderly population. Arch Intern Med 2004; 164:2421–2426.
- Perkins HS, Geppert CMA, Gonzales A, Cortez JD, Hazuda HP. Cross-cultural similarities and differences in attitudes about advance care planning. J Gen Intern Med 2002; 17:48–57.
- Perkins HS, Cortez JD, Hazuda HP. Advance care planning: does patient gender make a difference? Am J Med Sci 2004; 327:25–32.
- The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients. Study to Understand Prognoses and P for Outcomes and Risks of Treatments (SUPPORT). JAMA 1995; 274:1591–1598.
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol 1992; 47:1102–1114.
- Nigg CR, Burbank PM, Padula C, et al. Stages of change across ten health risk behaviors for older adults. Gerontologist 1999; 39:473–482.
- Patel RV, Sinuff T, Cook DJ. Influencing advance directive completion rates in non-terminally ill patients: a systematic review. J Crit Care 2004; 19:1–9.
- Hanson LC, Earp JA, Garrett J, Menon M, Danis M. Community physicians who provide terminal care. Arch Intern Med 1999; 159:1133–1138.
- Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: what do we need for success? J Am Geriatr Soc 2007; 55:277–283.
- Lynn J. Living long in fragile health: the new demographics shape end of life care. In:Jennings B, Kaebnick G, Murray T, editors. Improving End of Life Care: Why Has It Been So Difficult. Hastings Center Report November–December 2005: Special No:S14–S18.
- Beaumont JG, Kenealy PM. Incidence and prevalence of the vegetative and minimally conscious states. Neuropsychol Rehabil 2005; 15:184–189.
- Hawkins NA, Ditto PH, Danks JH, Smucker WD. Micromanaging death: process p, values, and goals in end-of-life medical decision making. Gerontologist 2005; 45:107–117.
- Ditto PH, Jacobson JA, Smucker WD, Danks JH, Fagerlin A. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment p. Med Decis Making 2006; 26:313–322.
- Lockhart LK, Ditto PH, Danks JH, Coppola KM, Smucker WD. The stability of older adults’ judgments of fates better and worse than death. Death Stud 2001; 25:299–317.
- Gjerdingen DK, Neff JA, Wang M, Chaloner K. Older persons’ opinions about life-sustaining procedures in the face of dementia. Arch Fam Med 1999; 8:421–425.
- Heap MJ, Munglani R, Klinck JR, Males AG. Elderly patients’ p concerning life-support treatment. Anaesthesia 1993; 48:1027–1033.
- Singer PA, Thiel EC, Naylor CD, et al. Life-sustaining treatment p of hemodialysis patients: implications for advance directives. J Am Soc Nephrol 1995; 6:1410–1417.
- Hofmann JC, Wenger NS, Davis RB, et al. Patient p for communication with physicians about end-of-life decisions. SUPPORT Investigators. Study to Understand Prognoses and Preference for Outcomes and Risks of Treatment. Ann Intern Med 1997; 127:1–12.
- Pinquart M, Sorensen S. Helping caregivers of persons with dementia: which interventions work and how large are their effects? Int Psychogeriatr 2006; 18:577–595.
- Robbins J, Gensler G, Hind J, et al. Comparison of 2 Interventions for liquid aspiration on pneumonia incidence: a randomized trial. Ann Intern Med 2008; 148:509–518.
- Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA 2001; 285:2750–2756.
- Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA 2006; 295:801–808.
- Losey R, Messinger-Rapport BJ. At what age should we discontinue colon cancer screening in the elderly? Cleve Clin J Med 2007; 74:269–272.
- Larson EB, Shadlen MF, Wang L, et al. Survival after initial diagnosis of Alzheimer disease. Ann Intern Med 2004; 140:501–509.
- Suthers K, Kim JK, Crimmins E. Life expectancy with cognitive impairment in the older population of the United States. J Gerontol B Psychol Sci Soc Sci 2003; 58:S179–S186.
- Bloom HL, Shukrullah I, Cuellar JR, Lloyd MS, Dudley SC, Zafari AM. Long-term survival after successful inhospital cardiac arrest resuscitation. Am Heart J 2007; 153:831–836.
- Finucane TE, Harper GM. Attempting resuscitation in nursing homes: policy considerations. J Am Geriatr Soc 1999; 47:1261–1264.
- Pearlman R, Startks H, Cain K, Cole W, Rosengren D, Patrick D. Your Life, Your Choices. 2nd ed. Department of Veterans Affairs, National Center for Ethics in Health Care, 2007.
- Molloy DW. Let Me Decide. Hamilton, Ontario: Newgrange Press, 1996.
- Dunn PM, Schmidt TA, Carley MM, Donius M, Weinstein MA, Dull VT. A method to communicate patient p about medically indicated life-sustaining treatment in the out-of-hospital setting. J Am Geriatr Soc 1996; 44:785–791.
- Fried TR, O’Leary J, Van Ness P, Fraenkel L. Inconsistency over time in the p of older persons with advanced illness for life-sustaining treatment. J Am Geriatr Soc 2007; 55:1007–1014.
- Fried TR, Van Ness PH, Byers AL, Towle VR, O’Leary JR, Dubin JA. Changes in p for life-sustaining treatment among older persons with advanced illness. J Gen Intern Med 2007; 22:495–501.
- Diwan S, Hougham GW, Sachs GA. Strain experienced by caregivers of dementia patients receiving palliative care: findings from the Palliative Excellence in Alzheimer Care Efforts (PEACE) Program. J Palliat Med 2004; 7:797–807.
- Covinsky KE, Yaffe K. Dementia, prognosis, and the needs of patients and caregivers. Ann Intern Med 2004; 140:573–574.
- Shega JW, Levin A, Hougham GW, et al. Palliative Excellence in Alzheimer Care Efforts (PEACE): a program description. J Palliat Med 2003; 6:315–320.
- Center for Ethics in Health Care. Physician orders for life-sustaining treatment paradigm. www.ohsu.edu/ethics/polst/. Accessed March 9, 2009.
- Lee MA, Brummel-Smith K, Meyer J, Drew N, London MR. Physician orders for life-sustaining treatment (POLST): outcomes in a PACE program. Program of All-Inclusive Care for the Elderly. J Am Geriatr Soc 2000; 48:1219–1225.
- Meyers JL, Moore C, McGrory A, Sparr J, Ahern M. Physician orders for life-sustaining treatment form: honoring end-of-life directives for nursing home residents. J Gerontol Nurs 2004; 30:37–46.
- Tolle SW, Tilden VP, Nelson CA, Dunn PM. A prospective study of the efficacy of the physician order form for life-sustaining treatment. J Am Geriatr Soc 1998; 46:1097–1102.
- Cantor MD, Pearlman RA. Advance care planning in long-term care facilities. J Am Med Dir Assoc 2004; 5(suppl 2):S72–S80.
Mr. B., an 82-year-old retired accountant with hypertension, was diagnosed with early Alzheimer disease 6 years ago. He now needs supervision with bathing and dressing and no longer consistently recognizes family members. You are seeing him in the office today after a hospitalization for aspiration pneumonia, his second in the past 6 months.
In the hospital, a brain scan showed that atrophy had progressed and white-matter disease was more extensive than 3 years earlier. A barium swallow study showed esophageal dysmotility and aspiration. He was prescribed a “dysphagia diet,”1 which he dislikes.
Since returning home, he has been disoriented, he has been wandering about the house, and he has fallen several times. He has lost 10 pounds in 6 months. Because of his confusion, his wife cannot take him out, and she is exhausted caring for him.
Reviewing his medical record, you note that 10 years ago, Mr. B. completed a living will and designated his wife as his proxy decision-maker via a medical power of attorney document.
PLANNING IS OFTEN NEGLECTED
Many clinicians and older patients feel a strong need to document, in advance, the patient’s wishes regarding medical care in the event the patient becomes seriously ill and unable to participate in treatment decisions. Professional societies such as the American Geriatrics Society promote advance care planning,2 and some indices of the quality of medical care include whether advance directives have been discussed and completed.3
Yet, despite the high profile of advance care planning,4 few patients actually fill out advance directives,5 with completion rates that vary widely,6–8 sometimes by ethnicity and sex.9,10 Furthermore, in a crisis, these directives are seldom followed.11
In this paper, we recommend an approach to advance care planning for older adults that redirects the focus from “signing away” interventions such as dialysis, mechanical ventilation, and tube feeding. Instead, the focus is on the goals of care. We also advocate naming a surrogate decision-maker, since the medical power of attorney is more flexible and more widely applicable than the living will.
START BY LISTENING
A change in function resulting from disease progression, hospitalization, trauma, or other reasons is an ideal opportunity to introduce the process of advance care planning.
The first step is to find out how well the patient and family understand the patient’s relevant medical conditions, and what their expectations, hopes, and concerns are. This listening phase can provide insight into the patient’s values and goals and how much the patient and family want to engage in these discussions.
In matters of health behavior (such as advance care planning), people change only when they are ready to change.12,13 Thus, we advise physicians to defer extensive discussions of values and goals of care until patients and families are ready to listen, hear, and talk about these topics (often, after a change for the worse in prognosis).
And it is a process. Advance care directives are most likely to be set up and followed if the patient and doctor discuss this issue during multiple visits, rather than if the physician merely hands the patient a packet of forms and information.14–16
CASE CONTINUED: A PEG TUBE REFUSED
Mrs. B. says that Mr. B. is in good health except for his memory: he does not have a serious condition such as diabetes, heart failure, or cancer. While Mr. B. was in the hospital, the hospitalist recommended placing a percutaneous endoscopic gastrostomy (PEG) tube, but Mrs. B. declined the recommendation because her husband had a living will that specified “no artificially or technologically supplied nutrition or hydration.”
At this point, Mrs. B. begins to cry. She has slept poorly because of his wandering. Also, her two daughters do not support her refusal of the PEG tube.
Comment. This brief conversation illuminates knowledge deficits in Mrs. B.’s understanding of Alzheimer disease and the circumstances in which the living will applies. Although one could argue that Mr. B.’s Alzheimer disease has advanced to the point that he is likely to die of a complication of that condition, he is not likely to die in the near future. If he is not considered by law and his physician to be terminally ill or permanently unconscious, a living will likely does not offer guidance about artificial feeding.
LIMITATIONS OF A LIVING WILL
A living will, a commonly used advance directive, states that the patient does not wish to receive life-sustaining treatment in the event that he or she suffers an incurable, irreversible disease and cannot give informed consent, and it often lists specific treatments that the patient does not want. However, we believe that approaching the patient with a list of life-sustaining measures to accept or reject, before discussing goals of care and prognosis, puts the cart before the horse. This approach threatens to distract from the need to ascertain values and offer appropriate care. Additionally, a living will is active only within a very limited scenario and does not address relatively routine but important decisions in a person’s care.
All ‘terminal illness’ isn’t the same
A living will goes into effect only if the patient either enters a permanent vegetative state following an event such as cardiac arrest or severe brain trauma, or is diagnosed with a terminal illness such as metastatic cancer, and lacks decision-making capacity.
But what is terminal illness? The definition differs from state to state, but it is generally defined as an irreversible condition leading to death in a relatively short time. The time may not be specified, as in Florida statute 765. In contrast, Ohio Revised Code 2133.01(AA) uses the phrase “relatively short,” while other states specify a time, such as within 6 months (Texas Health and Safety Code 166.002). The Medicare hospice benefit also carries a short time limit, usually less than 6 months.
The middle panel in Figure 1 depicts a more typical decline from serial organ insults such as stroke followed by infection from aspiration or followed by falls. Older adults with dementia or with multiple progressive diseases such as heart failure, diabetes, hypertension, or cancer decline in a trajectory such as in the bottom panel of Figure 1.
A living will might not be activated in the latter two scenarios until years into the condition because the patient would not be considered terminally ill—by state law, by the health care provider, or even by the patient.
The living will does not address routine interventions
In most states, living wills address only life-sustaining treatments such as dialysis, mechanical ventilation, and medically supplied nutrition and hydration. Living wills do not address relatively common diseases in older adults that could cause severe debility, such as a major stroke or advanced dementia.
If an older patient has dementia, a living will is unlikely to provide guidance about interventions such as intubation to get through an episode of potentially reversible respiratory failure, a feeding tube to correct weight loss, or cardiac catheterization or bypass surgery to treat angina. Yet these important decisions often arise as function declines and comorbidities progress.
Patients may change their minds
Many older adults are reluctant to sign documents to “micromanage” their future care if they should become ill.19 Many people change their mind as the situation changes.11,20,21 Although few claim they would want burdensome interventions if they had dementia22 or if their prognosis were poor,23 patients may tolerate more burdensome interventions if they are already receiving treatments for chronic illnesses such as end-stage renal disease.24
Thus, a living will may help if unexpected trauma occurs in a healthy person, but not so much if chronic illness progresses over a period of years.
Advance directives may not be honored
Even if completed, written advance directives may not be followed, for a variety of reasons. Physicians may not know the patient has a living will, and fewer than one-third of people who actually complete an advance directive have discussed its content with a physician.25 The people named as surrogate decision-makers may not know the patient’s wishes. Family members may disagree with the goals and plan of care and may interfere with implementation of the advance care plan. A patient may see multiple physicians at different institutions who may not communicate with each other about the patient’s wishes. Also, physicians and patients may interpret terms such as “terminally ill” differently, making it difficult to translate the documents into an action plan.
CASE CONTINUED: RELIEVING CAREGIVER STRESS
Returning to Mr. B., your first goal is to address care issues, including caregiver stress. Skilled services in the home are appropriate for him at this time (and Medicare will pay for them) because he is still homebound. These services could include physical therapy, occupational therapy, and speech (swallowing) therapy. A home care agency may also provide an aide for a few weeks to assist with bathing and other personal needs.
You strongly recommend that the family (including both daughters) participate in the Alzheimer’s Association educational programs. You recommend that Mrs. B. locate an adult day care program now so that when Mr. B. completes his home therapy course and is no longer homebound, he may attend. Day care would provide a therapeutic environment for him and respite for her.
You request that the home care agency provide a social worker to advise her on community resources. Meta-analysis suggests that structured, multicomponent interventions with caregivers of demented patients reduce several types of caregiver burden and delay institutionalization.26
He improves with conservative measures
Three weeks later, Mr. B. is sleeping better and has stopped wandering. However, he dislikes the thickened liquids required by the dysphagia diet and has lost another 2 pounds. If his beverages are not thickened, he coughs profusely when he swallows. His daughters are still pressuring Mrs. B. for a PEG tube; one of them has angrily asserted that the doctors are going to allow her father to die.
You explain the burdens of PEG tubes: surgical risks, continued aspiration, disrupted bowel habits, the risk of the tube being accidentally or intentionally dislodged by the patient, and special binders (which may be uncomfortable) or restraints (which may cause further functional decline) that may be necessary to prevent this complication.
You request that the speech therapist work with the patient more aggressively in the use of swallowing techniques such as the chin tuck, which may be at least as effective as thickeners in preventing both aspiration pneumonia and dehydration.27 The therapist will need to include Mrs. B. in these sessions, since she will be Mr. B.’s coach at mealtime.
With more aggressive speech therapy, the patient’s weight stabilizes over the next 4 weeks. He is in day care 3 days a week, and Mrs. B. is more rested and relaxed.
Cardiopulmonary resuscitation
You continue the advance care planning discussion and suggest that if Mr. B. aspirates, is hospitalized again, and declines further care, it would be helpful to delineate instructions for resuscitation. Right now, although his Alzheimer disease is advanced, he is not clearly terminal. Thus, his living will does not strictly apply and provides limited guidance about intubation, cardiopulmonary resuscitation (CPR), or medically supplied nutrition and hydration. However, because Mrs. B. is his agent in the medical power of attorney, this document enables her to make a wide spectrum of treatment decisions on his behalf.
Mrs. B. asks about her husband’s prognosis and why CPR would not be helpful.
Comment. Further discussion with her could be guided by an estimate of Mr. B.’s prognosis. Function-based tools28,29 may also be useful. For example,28,30 an 80-year-old man with high functional status might have a life expectancy of more than 10 years. Mr. B., with multiple medical problems and declining function, would have an estimated life expectancy of approximately 3 years. Even without specifically categorizing function, impaired cognition by itself predicted a shorter life expectancy in population-based studies.31,32
Regarding CPR, patients and families may overestimate successful outcomes. A recent study33 of 10 years of outcomes of in-hospital cardiac arrest found that only 6.6% of patients survived to discharge. The average age of the survivors was 59 years, and fewer than half of them survived 3 years after cardiac arrest. In eight studies of CPR outcomes in nursing homes,34 three studies had no survivors, and all but one study had a survival rate below 5%.
PROVIDING APPROPRIATE CARE, NOT LIMITING TREATMENTS
In the case of Mr. B., as in many situations encountered with older patients, written advance directives provide little help or guidance. Instead, we recommend a model of advance care planning that takes place during multiple office visits over time, and that maintains a focus on providing appropriate care rather than on limiting life-sustaining treatments. We recommend providing estimates of prognosis and CPR outcomes when the family appeares ready to hear them. This approach should result in a care-oriented process while moving the family towards decisions regarding artificial feeding and CPR.
All patients, particularly those unwilling or unable to participate in advance care planning, are encouraged to identify one or more surrogate decision-makers and articulate how much flexibility that person should be given in important health care decisions. The medical power of attorney can be activated any time the patient lacks decision-making capacity and deactivated when decision-making capacity returns.38,39
As in the case of Mr. B., a tailored approach to advance care planning requires clinicians to estimate life expectancy (more than 5 years, less than 5 years, or less than 1 year) and to determine the patient’s and the family’s readiness to focus on a values-oriented and goal-oriented care plan. Some patients are not receptive to advance care planning, and clinical time and effort are optimized by providing the right amount of information to patients when they are ready to receive it.
For relatively healthy older adults
Figure 2 is the algorithm for older patients who are expected to live at least 5 years, ie, who are relatively healthy and functional. Patients with little or no interest in advance care planning can be asked about it annually, or sooner if their medical condition changes. Patients with limited interest can be given written information, specifically living will and medical power of attorney documents recognized in their state. Patients more open to advance care planning can be offered a values history form (Table 1), Web sites, and educational materials, with a plan to discuss them at future appointments.
Periodic reevaluation of values and goals of care is important. Patients may assert that particular interventions (eg, a PEG tube or dialysis) are “worse than death” when they are healthy, but they may change their views over time.21 Additionally, although a recent hospitalization or a decline in function may predispose patients to want to limit life-sustaining treatments, they may return to their earlier values and wishes a few months later, particularly if their medical condition stabilizes. 20 Values and decisions should be reassessed not only when medical conditions deteriorate, but also when they improve.
For chronically ill patients
Caregiver stress is important to identify and address, since caregivers often neglect themselves.40–42
For terminally ill patients
In this situation, patients and families need information about community resources that can assist them in the home. Some older adults with cognitive impairment may be exploited or neglect themselves, and referral to an adult protective services agency may be needed.
Treatment burden, particularly due to multiple prescribed medications, may be high and should be reassessed in light of the goals of treatment. Polypharmacy reduction is especially important at this stage in the illness, since the goals of care may be different than when the medications were prescribed.
Physical or psychosocial symptoms may be the cue to bring up the topic of palliative care. If the patient is expected to live less than 6 months, hospice referral is appropriate. With either palliative care or hospice, the focus of attention shifts explicitly from curing the disease to managing symptoms, and from the patient to the patient-family dyad. Interventions such as CPR and ventilatory support should be discussed and information from Table 2 provided to the patient and family.
Complete advance care planning incorporates taking a values history, estimating life expectancy, determining physical, psychosocial and spiritual needs, clarifying treatment goals, and estimating manageable treatment burden. Offering statistics on CPR and providing state-specific living will and medical power of attorney documents are important but are only one facet of effective advance care planning. In fact, shifting the emphasis of advance care planning from statistics and forms to values and goals of care may help in developing a more comprehensive care plan.
Goals of care range from curing the disease (with aggressive therapy, which may be burdensome) to simply improving function or decreasing pain. In the latter case, one may be able to discontinue some of the patient’s drugs, utilize medical and community resources more effectively, and better meet the patient’s needs.
Woven through all these discussions should be reassurance that the plan can be revisited and possibly revised, and that the physician will be there to help with those decisions.
For acutely ill patients in the hospital
Episodic, staged advance care planning is appropriate not only in the office but also in other settings such as assisted living and nursing facilities.
In the hospital, however, a different approach is needed, since patients are usually admitted because of an acute illness or sudden functional decline, or both. Decisions about technological interventions such as CPR, mechanical ventilation, or dialysis may be needed urgently. Often, patients are unable to provide guidance to physicians during acute illness because of delirium and other impediments. Developing a plan for care in the hospital may require urgent family meetings. However, if a surrogate decision-maker is in place, and if the patient has already participated in some form of advance care planning as an outpatient, the values and goals of care previously identified can contribute to decision-making during hospitalization.
As mentioned above, fragmentation of health care across providers and health care systems may limit the effectiveness of office-based advance care planning. It may be reasonable to train office staff to place advance care planning documentation in easily accessible sections of the patient’s medical record and to forward these to specialists involved in a patient’s care.
The patient and family should be encouraged and empowered to help with this process and should have updated advance care planning documentation readily available. In some states, comprehensive medical order sets, especially for end-of-life care, are portable across care settings and address CPR, medically supplied nutrition, hospital transfer, and antibiotic treatment.43
Research suggests that health care systems are more likely to comply with patients’ end-of-life preferences when portable medical order forms are developed and disseminated.44–44 Ultimately, major changes in health care delivery, including universal electronic health records, may be needed to implement and communicate patients’ advance care planning preferences across settings.
Mr. B., an 82-year-old retired accountant with hypertension, was diagnosed with early Alzheimer disease 6 years ago. He now needs supervision with bathing and dressing and no longer consistently recognizes family members. You are seeing him in the office today after a hospitalization for aspiration pneumonia, his second in the past 6 months.
In the hospital, a brain scan showed that atrophy had progressed and white-matter disease was more extensive than 3 years earlier. A barium swallow study showed esophageal dysmotility and aspiration. He was prescribed a “dysphagia diet,”1 which he dislikes.
Since returning home, he has been disoriented, he has been wandering about the house, and he has fallen several times. He has lost 10 pounds in 6 months. Because of his confusion, his wife cannot take him out, and she is exhausted caring for him.
Reviewing his medical record, you note that 10 years ago, Mr. B. completed a living will and designated his wife as his proxy decision-maker via a medical power of attorney document.
PLANNING IS OFTEN NEGLECTED
Many clinicians and older patients feel a strong need to document, in advance, the patient’s wishes regarding medical care in the event the patient becomes seriously ill and unable to participate in treatment decisions. Professional societies such as the American Geriatrics Society promote advance care planning,2 and some indices of the quality of medical care include whether advance directives have been discussed and completed.3
Yet, despite the high profile of advance care planning,4 few patients actually fill out advance directives,5 with completion rates that vary widely,6–8 sometimes by ethnicity and sex.9,10 Furthermore, in a crisis, these directives are seldom followed.11
In this paper, we recommend an approach to advance care planning for older adults that redirects the focus from “signing away” interventions such as dialysis, mechanical ventilation, and tube feeding. Instead, the focus is on the goals of care. We also advocate naming a surrogate decision-maker, since the medical power of attorney is more flexible and more widely applicable than the living will.
START BY LISTENING
A change in function resulting from disease progression, hospitalization, trauma, or other reasons is an ideal opportunity to introduce the process of advance care planning.
The first step is to find out how well the patient and family understand the patient’s relevant medical conditions, and what their expectations, hopes, and concerns are. This listening phase can provide insight into the patient’s values and goals and how much the patient and family want to engage in these discussions.
In matters of health behavior (such as advance care planning), people change only when they are ready to change.12,13 Thus, we advise physicians to defer extensive discussions of values and goals of care until patients and families are ready to listen, hear, and talk about these topics (often, after a change for the worse in prognosis).
And it is a process. Advance care directives are most likely to be set up and followed if the patient and doctor discuss this issue during multiple visits, rather than if the physician merely hands the patient a packet of forms and information.14–16
CASE CONTINUED: A PEG TUBE REFUSED
Mrs. B. says that Mr. B. is in good health except for his memory: he does not have a serious condition such as diabetes, heart failure, or cancer. While Mr. B. was in the hospital, the hospitalist recommended placing a percutaneous endoscopic gastrostomy (PEG) tube, but Mrs. B. declined the recommendation because her husband had a living will that specified “no artificially or technologically supplied nutrition or hydration.”
At this point, Mrs. B. begins to cry. She has slept poorly because of his wandering. Also, her two daughters do not support her refusal of the PEG tube.
Comment. This brief conversation illuminates knowledge deficits in Mrs. B.’s understanding of Alzheimer disease and the circumstances in which the living will applies. Although one could argue that Mr. B.’s Alzheimer disease has advanced to the point that he is likely to die of a complication of that condition, he is not likely to die in the near future. If he is not considered by law and his physician to be terminally ill or permanently unconscious, a living will likely does not offer guidance about artificial feeding.
LIMITATIONS OF A LIVING WILL
A living will, a commonly used advance directive, states that the patient does not wish to receive life-sustaining treatment in the event that he or she suffers an incurable, irreversible disease and cannot give informed consent, and it often lists specific treatments that the patient does not want. However, we believe that approaching the patient with a list of life-sustaining measures to accept or reject, before discussing goals of care and prognosis, puts the cart before the horse. This approach threatens to distract from the need to ascertain values and offer appropriate care. Additionally, a living will is active only within a very limited scenario and does not address relatively routine but important decisions in a person’s care.
All ‘terminal illness’ isn’t the same
A living will goes into effect only if the patient either enters a permanent vegetative state following an event such as cardiac arrest or severe brain trauma, or is diagnosed with a terminal illness such as metastatic cancer, and lacks decision-making capacity.
But what is terminal illness? The definition differs from state to state, but it is generally defined as an irreversible condition leading to death in a relatively short time. The time may not be specified, as in Florida statute 765. In contrast, Ohio Revised Code 2133.01(AA) uses the phrase “relatively short,” while other states specify a time, such as within 6 months (Texas Health and Safety Code 166.002). The Medicare hospice benefit also carries a short time limit, usually less than 6 months.
The middle panel in Figure 1 depicts a more typical decline from serial organ insults such as stroke followed by infection from aspiration or followed by falls. Older adults with dementia or with multiple progressive diseases such as heart failure, diabetes, hypertension, or cancer decline in a trajectory such as in the bottom panel of Figure 1.
A living will might not be activated in the latter two scenarios until years into the condition because the patient would not be considered terminally ill—by state law, by the health care provider, or even by the patient.
The living will does not address routine interventions
In most states, living wills address only life-sustaining treatments such as dialysis, mechanical ventilation, and medically supplied nutrition and hydration. Living wills do not address relatively common diseases in older adults that could cause severe debility, such as a major stroke or advanced dementia.
If an older patient has dementia, a living will is unlikely to provide guidance about interventions such as intubation to get through an episode of potentially reversible respiratory failure, a feeding tube to correct weight loss, or cardiac catheterization or bypass surgery to treat angina. Yet these important decisions often arise as function declines and comorbidities progress.
Patients may change their minds
Many older adults are reluctant to sign documents to “micromanage” their future care if they should become ill.19 Many people change their mind as the situation changes.11,20,21 Although few claim they would want burdensome interventions if they had dementia22 or if their prognosis were poor,23 patients may tolerate more burdensome interventions if they are already receiving treatments for chronic illnesses such as end-stage renal disease.24
Thus, a living will may help if unexpected trauma occurs in a healthy person, but not so much if chronic illness progresses over a period of years.
Advance directives may not be honored
Even if completed, written advance directives may not be followed, for a variety of reasons. Physicians may not know the patient has a living will, and fewer than one-third of people who actually complete an advance directive have discussed its content with a physician.25 The people named as surrogate decision-makers may not know the patient’s wishes. Family members may disagree with the goals and plan of care and may interfere with implementation of the advance care plan. A patient may see multiple physicians at different institutions who may not communicate with each other about the patient’s wishes. Also, physicians and patients may interpret terms such as “terminally ill” differently, making it difficult to translate the documents into an action plan.
CASE CONTINUED: RELIEVING CAREGIVER STRESS
Returning to Mr. B., your first goal is to address care issues, including caregiver stress. Skilled services in the home are appropriate for him at this time (and Medicare will pay for them) because he is still homebound. These services could include physical therapy, occupational therapy, and speech (swallowing) therapy. A home care agency may also provide an aide for a few weeks to assist with bathing and other personal needs.
You strongly recommend that the family (including both daughters) participate in the Alzheimer’s Association educational programs. You recommend that Mrs. B. locate an adult day care program now so that when Mr. B. completes his home therapy course and is no longer homebound, he may attend. Day care would provide a therapeutic environment for him and respite for her.
You request that the home care agency provide a social worker to advise her on community resources. Meta-analysis suggests that structured, multicomponent interventions with caregivers of demented patients reduce several types of caregiver burden and delay institutionalization.26
He improves with conservative measures
Three weeks later, Mr. B. is sleeping better and has stopped wandering. However, he dislikes the thickened liquids required by the dysphagia diet and has lost another 2 pounds. If his beverages are not thickened, he coughs profusely when he swallows. His daughters are still pressuring Mrs. B. for a PEG tube; one of them has angrily asserted that the doctors are going to allow her father to die.
You explain the burdens of PEG tubes: surgical risks, continued aspiration, disrupted bowel habits, the risk of the tube being accidentally or intentionally dislodged by the patient, and special binders (which may be uncomfortable) or restraints (which may cause further functional decline) that may be necessary to prevent this complication.
You request that the speech therapist work with the patient more aggressively in the use of swallowing techniques such as the chin tuck, which may be at least as effective as thickeners in preventing both aspiration pneumonia and dehydration.27 The therapist will need to include Mrs. B. in these sessions, since she will be Mr. B.’s coach at mealtime.
With more aggressive speech therapy, the patient’s weight stabilizes over the next 4 weeks. He is in day care 3 days a week, and Mrs. B. is more rested and relaxed.
Cardiopulmonary resuscitation
You continue the advance care planning discussion and suggest that if Mr. B. aspirates, is hospitalized again, and declines further care, it would be helpful to delineate instructions for resuscitation. Right now, although his Alzheimer disease is advanced, he is not clearly terminal. Thus, his living will does not strictly apply and provides limited guidance about intubation, cardiopulmonary resuscitation (CPR), or medically supplied nutrition and hydration. However, because Mrs. B. is his agent in the medical power of attorney, this document enables her to make a wide spectrum of treatment decisions on his behalf.
Mrs. B. asks about her husband’s prognosis and why CPR would not be helpful.
Comment. Further discussion with her could be guided by an estimate of Mr. B.’s prognosis. Function-based tools28,29 may also be useful. For example,28,30 an 80-year-old man with high functional status might have a life expectancy of more than 10 years. Mr. B., with multiple medical problems and declining function, would have an estimated life expectancy of approximately 3 years. Even without specifically categorizing function, impaired cognition by itself predicted a shorter life expectancy in population-based studies.31,32
Regarding CPR, patients and families may overestimate successful outcomes. A recent study33 of 10 years of outcomes of in-hospital cardiac arrest found that only 6.6% of patients survived to discharge. The average age of the survivors was 59 years, and fewer than half of them survived 3 years after cardiac arrest. In eight studies of CPR outcomes in nursing homes,34 three studies had no survivors, and all but one study had a survival rate below 5%.
PROVIDING APPROPRIATE CARE, NOT LIMITING TREATMENTS
In the case of Mr. B., as in many situations encountered with older patients, written advance directives provide little help or guidance. Instead, we recommend a model of advance care planning that takes place during multiple office visits over time, and that maintains a focus on providing appropriate care rather than on limiting life-sustaining treatments. We recommend providing estimates of prognosis and CPR outcomes when the family appeares ready to hear them. This approach should result in a care-oriented process while moving the family towards decisions regarding artificial feeding and CPR.
All patients, particularly those unwilling or unable to participate in advance care planning, are encouraged to identify one or more surrogate decision-makers and articulate how much flexibility that person should be given in important health care decisions. The medical power of attorney can be activated any time the patient lacks decision-making capacity and deactivated when decision-making capacity returns.38,39
As in the case of Mr. B., a tailored approach to advance care planning requires clinicians to estimate life expectancy (more than 5 years, less than 5 years, or less than 1 year) and to determine the patient’s and the family’s readiness to focus on a values-oriented and goal-oriented care plan. Some patients are not receptive to advance care planning, and clinical time and effort are optimized by providing the right amount of information to patients when they are ready to receive it.
For relatively healthy older adults
Figure 2 is the algorithm for older patients who are expected to live at least 5 years, ie, who are relatively healthy and functional. Patients with little or no interest in advance care planning can be asked about it annually, or sooner if their medical condition changes. Patients with limited interest can be given written information, specifically living will and medical power of attorney documents recognized in their state. Patients more open to advance care planning can be offered a values history form (Table 1), Web sites, and educational materials, with a plan to discuss them at future appointments.
Periodic reevaluation of values and goals of care is important. Patients may assert that particular interventions (eg, a PEG tube or dialysis) are “worse than death” when they are healthy, but they may change their views over time.21 Additionally, although a recent hospitalization or a decline in function may predispose patients to want to limit life-sustaining treatments, they may return to their earlier values and wishes a few months later, particularly if their medical condition stabilizes. 20 Values and decisions should be reassessed not only when medical conditions deteriorate, but also when they improve.
For chronically ill patients
Caregiver stress is important to identify and address, since caregivers often neglect themselves.40–42
For terminally ill patients
In this situation, patients and families need information about community resources that can assist them in the home. Some older adults with cognitive impairment may be exploited or neglect themselves, and referral to an adult protective services agency may be needed.
Treatment burden, particularly due to multiple prescribed medications, may be high and should be reassessed in light of the goals of treatment. Polypharmacy reduction is especially important at this stage in the illness, since the goals of care may be different than when the medications were prescribed.
Physical or psychosocial symptoms may be the cue to bring up the topic of palliative care. If the patient is expected to live less than 6 months, hospice referral is appropriate. With either palliative care or hospice, the focus of attention shifts explicitly from curing the disease to managing symptoms, and from the patient to the patient-family dyad. Interventions such as CPR and ventilatory support should be discussed and information from Table 2 provided to the patient and family.
Complete advance care planning incorporates taking a values history, estimating life expectancy, determining physical, psychosocial and spiritual needs, clarifying treatment goals, and estimating manageable treatment burden. Offering statistics on CPR and providing state-specific living will and medical power of attorney documents are important but are only one facet of effective advance care planning. In fact, shifting the emphasis of advance care planning from statistics and forms to values and goals of care may help in developing a more comprehensive care plan.
Goals of care range from curing the disease (with aggressive therapy, which may be burdensome) to simply improving function or decreasing pain. In the latter case, one may be able to discontinue some of the patient’s drugs, utilize medical and community resources more effectively, and better meet the patient’s needs.
Woven through all these discussions should be reassurance that the plan can be revisited and possibly revised, and that the physician will be there to help with those decisions.
For acutely ill patients in the hospital
Episodic, staged advance care planning is appropriate not only in the office but also in other settings such as assisted living and nursing facilities.
In the hospital, however, a different approach is needed, since patients are usually admitted because of an acute illness or sudden functional decline, or both. Decisions about technological interventions such as CPR, mechanical ventilation, or dialysis may be needed urgently. Often, patients are unable to provide guidance to physicians during acute illness because of delirium and other impediments. Developing a plan for care in the hospital may require urgent family meetings. However, if a surrogate decision-maker is in place, and if the patient has already participated in some form of advance care planning as an outpatient, the values and goals of care previously identified can contribute to decision-making during hospitalization.
As mentioned above, fragmentation of health care across providers and health care systems may limit the effectiveness of office-based advance care planning. It may be reasonable to train office staff to place advance care planning documentation in easily accessible sections of the patient’s medical record and to forward these to specialists involved in a patient’s care.
The patient and family should be encouraged and empowered to help with this process and should have updated advance care planning documentation readily available. In some states, comprehensive medical order sets, especially for end-of-life care, are portable across care settings and address CPR, medically supplied nutrition, hospital transfer, and antibiotic treatment.43
Research suggests that health care systems are more likely to comply with patients’ end-of-life preferences when portable medical order forms are developed and disseminated.44–44 Ultimately, major changes in health care delivery, including universal electronic health records, may be needed to implement and communicate patients’ advance care planning preferences across settings.
- National Dysphagia Diet Task Force. National Dysphagia Diet: Standardization for Optimal Care. Chicago, IL: American Dietetic Association, 2002.
- Nusbaum N, Goldstein M. American Geriatrics Society. The Patient Education Forum. Advance Directives, 2008. www.americangeriatrics.org/education/forum/advance_dir.shtml. Accessed March 9, 2009.
- Wenger NS, Roth CP, Shekelle PA; COVE Investigators. Introduction to the assessing care of vulnerable elders–3 quality indicator measurement set. J Am Geriatr Soc 2007; 55(suppl 2):S247–S252.
- Emanuel LL, Danis M, Pearlman RA, Singer PA. Advance care planning as a process: structuring the discussions in practice. J Am Geriatr Soc 1995; 43:440–446.
- Teno J, Lynn J, Wenger N, et al. Advance directives for seriously ill hospitalized patients: effectiveness with the patient self-determination act and the SUPPORT intervention. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatment. J Am Geriatr Soc 1997; 45:500–507.
- Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Arch Intern Med 1998; 158:383–390.
- Gordon NP, Shade SB. Advance directives are more likely among seniors asked about end-of-life care p. Arch Intern Med 1999; 159:701–704.
- Morrison RS, Meier DE. High rates of advance care planning in New York City’s elderly population. Arch Intern Med 2004; 164:2421–2426.
- Perkins HS, Geppert CMA, Gonzales A, Cortez JD, Hazuda HP. Cross-cultural similarities and differences in attitudes about advance care planning. J Gen Intern Med 2002; 17:48–57.
- Perkins HS, Cortez JD, Hazuda HP. Advance care planning: does patient gender make a difference? Am J Med Sci 2004; 327:25–32.
- The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients. Study to Understand Prognoses and P for Outcomes and Risks of Treatments (SUPPORT). JAMA 1995; 274:1591–1598.
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol 1992; 47:1102–1114.
- Nigg CR, Burbank PM, Padula C, et al. Stages of change across ten health risk behaviors for older adults. Gerontologist 1999; 39:473–482.
- Patel RV, Sinuff T, Cook DJ. Influencing advance directive completion rates in non-terminally ill patients: a systematic review. J Crit Care 2004; 19:1–9.
- Hanson LC, Earp JA, Garrett J, Menon M, Danis M. Community physicians who provide terminal care. Arch Intern Med 1999; 159:1133–1138.
- Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: what do we need for success? J Am Geriatr Soc 2007; 55:277–283.
- Lynn J. Living long in fragile health: the new demographics shape end of life care. In:Jennings B, Kaebnick G, Murray T, editors. Improving End of Life Care: Why Has It Been So Difficult. Hastings Center Report November–December 2005: Special No:S14–S18.
- Beaumont JG, Kenealy PM. Incidence and prevalence of the vegetative and minimally conscious states. Neuropsychol Rehabil 2005; 15:184–189.
- Hawkins NA, Ditto PH, Danks JH, Smucker WD. Micromanaging death: process p, values, and goals in end-of-life medical decision making. Gerontologist 2005; 45:107–117.
- Ditto PH, Jacobson JA, Smucker WD, Danks JH, Fagerlin A. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment p. Med Decis Making 2006; 26:313–322.
- Lockhart LK, Ditto PH, Danks JH, Coppola KM, Smucker WD. The stability of older adults’ judgments of fates better and worse than death. Death Stud 2001; 25:299–317.
- Gjerdingen DK, Neff JA, Wang M, Chaloner K. Older persons’ opinions about life-sustaining procedures in the face of dementia. Arch Fam Med 1999; 8:421–425.
- Heap MJ, Munglani R, Klinck JR, Males AG. Elderly patients’ p concerning life-support treatment. Anaesthesia 1993; 48:1027–1033.
- Singer PA, Thiel EC, Naylor CD, et al. Life-sustaining treatment p of hemodialysis patients: implications for advance directives. J Am Soc Nephrol 1995; 6:1410–1417.
- Hofmann JC, Wenger NS, Davis RB, et al. Patient p for communication with physicians about end-of-life decisions. SUPPORT Investigators. Study to Understand Prognoses and Preference for Outcomes and Risks of Treatment. Ann Intern Med 1997; 127:1–12.
- Pinquart M, Sorensen S. Helping caregivers of persons with dementia: which interventions work and how large are their effects? Int Psychogeriatr 2006; 18:577–595.
- Robbins J, Gensler G, Hind J, et al. Comparison of 2 Interventions for liquid aspiration on pneumonia incidence: a randomized trial. Ann Intern Med 2008; 148:509–518.
- Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA 2001; 285:2750–2756.
- Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA 2006; 295:801–808.
- Losey R, Messinger-Rapport BJ. At what age should we discontinue colon cancer screening in the elderly? Cleve Clin J Med 2007; 74:269–272.
- Larson EB, Shadlen MF, Wang L, et al. Survival after initial diagnosis of Alzheimer disease. Ann Intern Med 2004; 140:501–509.
- Suthers K, Kim JK, Crimmins E. Life expectancy with cognitive impairment in the older population of the United States. J Gerontol B Psychol Sci Soc Sci 2003; 58:S179–S186.
- Bloom HL, Shukrullah I, Cuellar JR, Lloyd MS, Dudley SC, Zafari AM. Long-term survival after successful inhospital cardiac arrest resuscitation. Am Heart J 2007; 153:831–836.
- Finucane TE, Harper GM. Attempting resuscitation in nursing homes: policy considerations. J Am Geriatr Soc 1999; 47:1261–1264.
- Pearlman R, Startks H, Cain K, Cole W, Rosengren D, Patrick D. Your Life, Your Choices. 2nd ed. Department of Veterans Affairs, National Center for Ethics in Health Care, 2007.
- Molloy DW. Let Me Decide. Hamilton, Ontario: Newgrange Press, 1996.
- Dunn PM, Schmidt TA, Carley MM, Donius M, Weinstein MA, Dull VT. A method to communicate patient p about medically indicated life-sustaining treatment in the out-of-hospital setting. J Am Geriatr Soc 1996; 44:785–791.
- Fried TR, O’Leary J, Van Ness P, Fraenkel L. Inconsistency over time in the p of older persons with advanced illness for life-sustaining treatment. J Am Geriatr Soc 2007; 55:1007–1014.
- Fried TR, Van Ness PH, Byers AL, Towle VR, O’Leary JR, Dubin JA. Changes in p for life-sustaining treatment among older persons with advanced illness. J Gen Intern Med 2007; 22:495–501.
- Diwan S, Hougham GW, Sachs GA. Strain experienced by caregivers of dementia patients receiving palliative care: findings from the Palliative Excellence in Alzheimer Care Efforts (PEACE) Program. J Palliat Med 2004; 7:797–807.
- Covinsky KE, Yaffe K. Dementia, prognosis, and the needs of patients and caregivers. Ann Intern Med 2004; 140:573–574.
- Shega JW, Levin A, Hougham GW, et al. Palliative Excellence in Alzheimer Care Efforts (PEACE): a program description. J Palliat Med 2003; 6:315–320.
- Center for Ethics in Health Care. Physician orders for life-sustaining treatment paradigm. www.ohsu.edu/ethics/polst/. Accessed March 9, 2009.
- Lee MA, Brummel-Smith K, Meyer J, Drew N, London MR. Physician orders for life-sustaining treatment (POLST): outcomes in a PACE program. Program of All-Inclusive Care for the Elderly. J Am Geriatr Soc 2000; 48:1219–1225.
- Meyers JL, Moore C, McGrory A, Sparr J, Ahern M. Physician orders for life-sustaining treatment form: honoring end-of-life directives for nursing home residents. J Gerontol Nurs 2004; 30:37–46.
- Tolle SW, Tilden VP, Nelson CA, Dunn PM. A prospective study of the efficacy of the physician order form for life-sustaining treatment. J Am Geriatr Soc 1998; 46:1097–1102.
- Cantor MD, Pearlman RA. Advance care planning in long-term care facilities. J Am Med Dir Assoc 2004; 5(suppl 2):S72–S80.
- National Dysphagia Diet Task Force. National Dysphagia Diet: Standardization for Optimal Care. Chicago, IL: American Dietetic Association, 2002.
- Nusbaum N, Goldstein M. American Geriatrics Society. The Patient Education Forum. Advance Directives, 2008. www.americangeriatrics.org/education/forum/advance_dir.shtml. Accessed March 9, 2009.
- Wenger NS, Roth CP, Shekelle PA; COVE Investigators. Introduction to the assessing care of vulnerable elders–3 quality indicator measurement set. J Am Geriatr Soc 2007; 55(suppl 2):S247–S252.
- Emanuel LL, Danis M, Pearlman RA, Singer PA. Advance care planning as a process: structuring the discussions in practice. J Am Geriatr Soc 1995; 43:440–446.
- Teno J, Lynn J, Wenger N, et al. Advance directives for seriously ill hospitalized patients: effectiveness with the patient self-determination act and the SUPPORT intervention. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatment. J Am Geriatr Soc 1997; 45:500–507.
- Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Arch Intern Med 1998; 158:383–390.
- Gordon NP, Shade SB. Advance directives are more likely among seniors asked about end-of-life care p. Arch Intern Med 1999; 159:701–704.
- Morrison RS, Meier DE. High rates of advance care planning in New York City’s elderly population. Arch Intern Med 2004; 164:2421–2426.
- Perkins HS, Geppert CMA, Gonzales A, Cortez JD, Hazuda HP. Cross-cultural similarities and differences in attitudes about advance care planning. J Gen Intern Med 2002; 17:48–57.
- Perkins HS, Cortez JD, Hazuda HP. Advance care planning: does patient gender make a difference? Am J Med Sci 2004; 327:25–32.
- The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients. Study to Understand Prognoses and P for Outcomes and Risks of Treatments (SUPPORT). JAMA 1995; 274:1591–1598.
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol 1992; 47:1102–1114.
- Nigg CR, Burbank PM, Padula C, et al. Stages of change across ten health risk behaviors for older adults. Gerontologist 1999; 39:473–482.
- Patel RV, Sinuff T, Cook DJ. Influencing advance directive completion rates in non-terminally ill patients: a systematic review. J Crit Care 2004; 19:1–9.
- Hanson LC, Earp JA, Garrett J, Menon M, Danis M. Community physicians who provide terminal care. Arch Intern Med 1999; 159:1133–1138.
- Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: what do we need for success? J Am Geriatr Soc 2007; 55:277–283.
- Lynn J. Living long in fragile health: the new demographics shape end of life care. In:Jennings B, Kaebnick G, Murray T, editors. Improving End of Life Care: Why Has It Been So Difficult. Hastings Center Report November–December 2005: Special No:S14–S18.
- Beaumont JG, Kenealy PM. Incidence and prevalence of the vegetative and minimally conscious states. Neuropsychol Rehabil 2005; 15:184–189.
- Hawkins NA, Ditto PH, Danks JH, Smucker WD. Micromanaging death: process p, values, and goals in end-of-life medical decision making. Gerontologist 2005; 45:107–117.
- Ditto PH, Jacobson JA, Smucker WD, Danks JH, Fagerlin A. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment p. Med Decis Making 2006; 26:313–322.
- Lockhart LK, Ditto PH, Danks JH, Coppola KM, Smucker WD. The stability of older adults’ judgments of fates better and worse than death. Death Stud 2001; 25:299–317.
- Gjerdingen DK, Neff JA, Wang M, Chaloner K. Older persons’ opinions about life-sustaining procedures in the face of dementia. Arch Fam Med 1999; 8:421–425.
- Heap MJ, Munglani R, Klinck JR, Males AG. Elderly patients’ p concerning life-support treatment. Anaesthesia 1993; 48:1027–1033.
- Singer PA, Thiel EC, Naylor CD, et al. Life-sustaining treatment p of hemodialysis patients: implications for advance directives. J Am Soc Nephrol 1995; 6:1410–1417.
- Hofmann JC, Wenger NS, Davis RB, et al. Patient p for communication with physicians about end-of-life decisions. SUPPORT Investigators. Study to Understand Prognoses and Preference for Outcomes and Risks of Treatment. Ann Intern Med 1997; 127:1–12.
- Pinquart M, Sorensen S. Helping caregivers of persons with dementia: which interventions work and how large are their effects? Int Psychogeriatr 2006; 18:577–595.
- Robbins J, Gensler G, Hind J, et al. Comparison of 2 Interventions for liquid aspiration on pneumonia incidence: a randomized trial. Ann Intern Med 2008; 148:509–518.
- Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA 2001; 285:2750–2756.
- Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA 2006; 295:801–808.
- Losey R, Messinger-Rapport BJ. At what age should we discontinue colon cancer screening in the elderly? Cleve Clin J Med 2007; 74:269–272.
- Larson EB, Shadlen MF, Wang L, et al. Survival after initial diagnosis of Alzheimer disease. Ann Intern Med 2004; 140:501–509.
- Suthers K, Kim JK, Crimmins E. Life expectancy with cognitive impairment in the older population of the United States. J Gerontol B Psychol Sci Soc Sci 2003; 58:S179–S186.
- Bloom HL, Shukrullah I, Cuellar JR, Lloyd MS, Dudley SC, Zafari AM. Long-term survival after successful inhospital cardiac arrest resuscitation. Am Heart J 2007; 153:831–836.
- Finucane TE, Harper GM. Attempting resuscitation in nursing homes: policy considerations. J Am Geriatr Soc 1999; 47:1261–1264.
- Pearlman R, Startks H, Cain K, Cole W, Rosengren D, Patrick D. Your Life, Your Choices. 2nd ed. Department of Veterans Affairs, National Center for Ethics in Health Care, 2007.
- Molloy DW. Let Me Decide. Hamilton, Ontario: Newgrange Press, 1996.
- Dunn PM, Schmidt TA, Carley MM, Donius M, Weinstein MA, Dull VT. A method to communicate patient p about medically indicated life-sustaining treatment in the out-of-hospital setting. J Am Geriatr Soc 1996; 44:785–791.
- Fried TR, O’Leary J, Van Ness P, Fraenkel L. Inconsistency over time in the p of older persons with advanced illness for life-sustaining treatment. J Am Geriatr Soc 2007; 55:1007–1014.
- Fried TR, Van Ness PH, Byers AL, Towle VR, O’Leary JR, Dubin JA. Changes in p for life-sustaining treatment among older persons with advanced illness. J Gen Intern Med 2007; 22:495–501.
- Diwan S, Hougham GW, Sachs GA. Strain experienced by caregivers of dementia patients receiving palliative care: findings from the Palliative Excellence in Alzheimer Care Efforts (PEACE) Program. J Palliat Med 2004; 7:797–807.
- Covinsky KE, Yaffe K. Dementia, prognosis, and the needs of patients and caregivers. Ann Intern Med 2004; 140:573–574.
- Shega JW, Levin A, Hougham GW, et al. Palliative Excellence in Alzheimer Care Efforts (PEACE): a program description. J Palliat Med 2003; 6:315–320.
- Center for Ethics in Health Care. Physician orders for life-sustaining treatment paradigm. www.ohsu.edu/ethics/polst/. Accessed March 9, 2009.
- Lee MA, Brummel-Smith K, Meyer J, Drew N, London MR. Physician orders for life-sustaining treatment (POLST): outcomes in a PACE program. Program of All-Inclusive Care for the Elderly. J Am Geriatr Soc 2000; 48:1219–1225.
- Meyers JL, Moore C, McGrory A, Sparr J, Ahern M. Physician orders for life-sustaining treatment form: honoring end-of-life directives for nursing home residents. J Gerontol Nurs 2004; 30:37–46.
- Tolle SW, Tilden VP, Nelson CA, Dunn PM. A prospective study of the efficacy of the physician order form for life-sustaining treatment. J Am Geriatr Soc 1998; 46:1097–1102.
- Cantor MD, Pearlman RA. Advance care planning in long-term care facilities. J Am Med Dir Assoc 2004; 5(suppl 2):S72–S80.
KEY POINTS
- In the ambulatory setting, start by assessing the patient’s prognosis and his or her receptiveness to advance care planning.
- For a patient in declining health who is willing to participate in the care planning process, it may be useful to take a full values history and to review the goals of care.
- For a patient with advanced disease who is unable or unwilling to participate in advance care planning, a limited approach may be appropriate, ie, identifying a surrogate decision-maker and ascertaining how much flexibility the surrogate should have with health care decisions.
- Whatever the patient’s life expectancy and level of receptivity, brief, episodic discussions are more useful than a one-time description of available written advance directives.