User login
Electronic solutions to implementing lipid guidelines
Scenario
John is a 50-year-old man with treated hypertension; his blood pressure is 144/84 mm Hg. His lipid panel shows a total cholesterol level of 236 mg/dL, a low-density lipoprotein (LDL) level of 153 mg/dL, and high-density lipoprotein level of 48 mg/dL after therapeutic lifestyle changes. Should John be started on drug therapy to lower his lipid levels?
Solutions
John’s physician might decide whether to initiate drug therapy by “eyeballing” the lipids and making a clinical “guesstimate,” or by determining the Framingham 10-year risk. The Framingham 10-year risk determination is recommended by the Adult Treatment Panel (ATP III) of the National Institutes of Health.1 Although these calculations can be made using published charts,1 the charts are unwieldy and often not available at the point of care. Here are 3 electronic solutions that provide a better way to determine the ATP III-recommended strategy for your patients.
Atp III Cholesterol Management Guidelines
The first, downloadable free from the National Institutes of Health (Table 1), is entitled ATP III Cholesterol Management Guidelines (NIH-ATP3) and is available only for Palm operating system devices. The user enters the patient’s lipid values, age, and sex (Figure 1A). Known risk factors are checked via taps on the touch-sensitive palm-top device’s screen. If additional information is needed, such as the blood pressure, a second screen asks for those values. Then, the assessment is provided with options for additional information if desired (Figure 1B). The ATP III, or Framingham, risk percentage is for “hard” coronary heart disease (CHD) end points (myocardial infarction and cardiac death) during the next 10 years. NIH-ATP3 is not beamable from one handheld unit to another.
TABLE 1
Sources of programs
| Program | Source |
|---|---|
| NIH-ATP3 | http://hin.nhlbi.nih.gov/palmapps.htm |
| Stat Cholesterol | http://www.statcoder.com |
| Cholesterol 1.1 | http://www.ScyMed.com |
FIGURE 1
Sample screens from ATP III Cholesterol Management Guidelines (NIH-ATP3)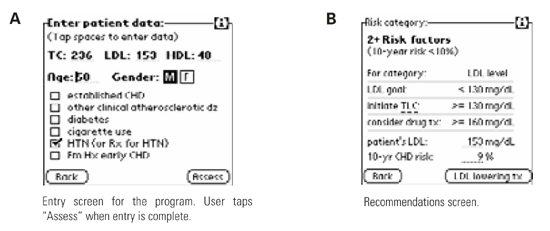
Another option for the Palm operating system is STAT Cholesterol, also downloadable. The price for it is banner advertising occupying about the bottom third of the screen (Figure 2A). STAT Cholesterol also uses ATP III treatment guidelines, but the presentation is different. Rather than numeric entry of lipid values, age, and blood pressure, these data are chosen from drop-down menus specifying ranges. Both ATP III CHD (hard end point) risk and total CHD risk are shown, along with the “average” risk and a “low” risk for age and sex (independent of other factors). As the user changes the values shown on the first screen (age, sex, blood pressure, lipids, and 3 check boxes), the 10-year ATP III risk and total CHD risk percentages change in real time, which is unique among these programs.
The therapeutic recommendations are not as clear on STAT Cholesterol as on the other programs. For example, when a patient is in the highest risk category, NIH-ATP3 clearly specifies that drug therapy is optional for LDL levels of 100 to 129 mg/dL and should be considered when LDL levels are ≥130 mg/dL. STAT Cholesterol lists drug treatment at an LDL level of ≥130 mg/dL but, in STAT Cholesterol, the user has to drill down into the details and scroll down to find that drug treatment is an option for LDL levels of 100 to 129 mg/dL (Figure 2B). However, STAT Cholesterol presents a check-box list for metabolic syndrome, with the appropriate boxes already checked from information previously entered. (Abdominal girth and, for nondiabetic individuals, assessment of fasting blood glucose, are additional user entries to complete this assessment.) This program is the only one of the 3 in this review that allows users (via Menu/options) to choose units of either mg/dL (United States) or mmol/L (the rest of the world). Stat Cholesterol is freely beamable among Palm operating system devices.
FIGURE 2
Sample screens from STAT Cholesterol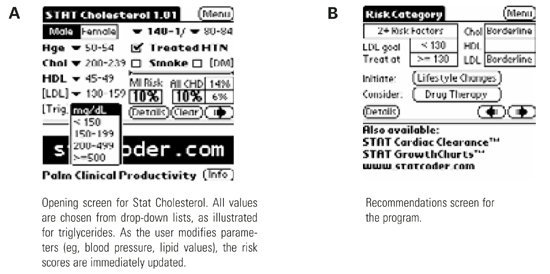
Cholesterol 1.1
The third program is Cholesterol 1.1 by ScyMed, and runs on desktop computers using the Windows operating system. It is available in a CD-only version ($49.95) or a Web-based version. The Web-based version also includes the other resources on ScyMed’s Web site (a medical calculator and history/physical examination templates; single user, $149 per year). Like the other 2 programs, users enter pertinent data, then click “Create Profile.” Appropriately, the program does not force the user to enter all data on the entry screen. A new page opens that contains a summary of the data, including a table explicitly listing Framingham points for each pertinent entry (eg, the points for the age-sex category), the 10-year Framingham CHD (ATP III) risk, and specific suggestions for ATP III-compliant therapy (Figure 3).
Obviously, a major advantage of a PC-based system is the ability to produce a printout for the patient and for the chart. Printouts can be personalized with physician and patient name if the user chooses to enter this information. For physicians who have PC or Internet access in examination rooms or who generally preview laboratory reports in an office with such access, the CD or Web-based system presents an interesting option. Both Cholesterol 1.1 incarnations (CD and Web) include the complete ATP III Executive Summary. The therapy recommendations are hyperlinked to the relevant sections of the ATP-III Summary for users who wish to review any specifics in the recommendations.
FIGURE 3
Sample screen from Cholesterol 1.1
Conclusion
In summary, all 3 options “work.” All are meant to facilitate implementation of the ATP III guidelines. For physicians who wish to use ATP III guidelines to support their therapeutic decisions, all of these options simplify calculation and are better than simply guessing about whether—and which—therapy is appropriate. Regarding the 2 applications for the Palm operating system, Stat Cholesterol has a few more screens than NIH-ATP3, but these serve as helpful reminders about metabolic syndrome and triglyceride levels. Stat Cholesterol’s unique features include choice of units (mmol/L, mg/dL) and “real time” changes in 10-year risk numbers as data are entered or modified. NIH-ATP3 is the “cleanest” and simplest in my opinion. For physicians who have the computer resources and most especially for those who want personalized, printed information for the patient or chart (and are willing to enter these additional data), Cholesterol 1.1 for desktop computers is the way to go.
It is important to remember that the Framingham model was developed in individuals without known established CHD, and consisted largely of non-Hispanic white patients; thus data may not be entirely generalizable to other groups. In 1997, the American Diabetes Association2 also lowered the fasting glucose levels defining diabetes from 140 to 126 mg/dL; thus, the “mildest” forms of diabetes may not have the same prognostic significance. Finally, just because a population with a total cholesterol level of 280 mg/dL has one risk and a population with a total cholesterol level of 220 mg/dL has a lower risk, does not automatically mean that lowering the 280 cholesterol group’s cholesterol to 220 reduces their risk to that of the group whose innate cholesterol level was 220. However, it is tempting to use these data that way.
Finally, the NCEP ATP III tables offer recommendations only through age 79. Cholesterol 1.1 handles ages 80 and above improperly, but provides no error message or explanation. Stat Cholesterol allows only fixed choices from its drop-down menus; for age, these stop at age 79. NIH-ATP III appears to apply the risk values for age 79 to older individuals without modification (or notification to the user), although the product information specifies an age range up to 99 years.
1. National Cholesterol Education Program. Third Report of the Expert Panel on Detection, Evaluation, and Treatment of high blood cholesterol in adults (Adult Treatment Panel III) Executive Summary. NIH publication 01-3670, May 2001. Available from: http://www.nhlbi.nih.gov/guidelines/cholesterol/atp_iii.htm.
2. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20:1183-97.
Scenario
John is a 50-year-old man with treated hypertension; his blood pressure is 144/84 mm Hg. His lipid panel shows a total cholesterol level of 236 mg/dL, a low-density lipoprotein (LDL) level of 153 mg/dL, and high-density lipoprotein level of 48 mg/dL after therapeutic lifestyle changes. Should John be started on drug therapy to lower his lipid levels?
Solutions
John’s physician might decide whether to initiate drug therapy by “eyeballing” the lipids and making a clinical “guesstimate,” or by determining the Framingham 10-year risk. The Framingham 10-year risk determination is recommended by the Adult Treatment Panel (ATP III) of the National Institutes of Health.1 Although these calculations can be made using published charts,1 the charts are unwieldy and often not available at the point of care. Here are 3 electronic solutions that provide a better way to determine the ATP III-recommended strategy for your patients.
Atp III Cholesterol Management Guidelines
The first, downloadable free from the National Institutes of Health (Table 1), is entitled ATP III Cholesterol Management Guidelines (NIH-ATP3) and is available only for Palm operating system devices. The user enters the patient’s lipid values, age, and sex (Figure 1A). Known risk factors are checked via taps on the touch-sensitive palm-top device’s screen. If additional information is needed, such as the blood pressure, a second screen asks for those values. Then, the assessment is provided with options for additional information if desired (Figure 1B). The ATP III, or Framingham, risk percentage is for “hard” coronary heart disease (CHD) end points (myocardial infarction and cardiac death) during the next 10 years. NIH-ATP3 is not beamable from one handheld unit to another.
TABLE 1
Sources of programs
| Program | Source |
|---|---|
| NIH-ATP3 | http://hin.nhlbi.nih.gov/palmapps.htm |
| Stat Cholesterol | http://www.statcoder.com |
| Cholesterol 1.1 | http://www.ScyMed.com |
FIGURE 1
Sample screens from ATP III Cholesterol Management Guidelines (NIH-ATP3)
Another option for the Palm operating system is STAT Cholesterol, also downloadable. The price for it is banner advertising occupying about the bottom third of the screen (Figure 2A). STAT Cholesterol also uses ATP III treatment guidelines, but the presentation is different. Rather than numeric entry of lipid values, age, and blood pressure, these data are chosen from drop-down menus specifying ranges. Both ATP III CHD (hard end point) risk and total CHD risk are shown, along with the “average” risk and a “low” risk for age and sex (independent of other factors). As the user changes the values shown on the first screen (age, sex, blood pressure, lipids, and 3 check boxes), the 10-year ATP III risk and total CHD risk percentages change in real time, which is unique among these programs.
The therapeutic recommendations are not as clear on STAT Cholesterol as on the other programs. For example, when a patient is in the highest risk category, NIH-ATP3 clearly specifies that drug therapy is optional for LDL levels of 100 to 129 mg/dL and should be considered when LDL levels are ≥130 mg/dL. STAT Cholesterol lists drug treatment at an LDL level of ≥130 mg/dL but, in STAT Cholesterol, the user has to drill down into the details and scroll down to find that drug treatment is an option for LDL levels of 100 to 129 mg/dL (Figure 2B). However, STAT Cholesterol presents a check-box list for metabolic syndrome, with the appropriate boxes already checked from information previously entered. (Abdominal girth and, for nondiabetic individuals, assessment of fasting blood glucose, are additional user entries to complete this assessment.) This program is the only one of the 3 in this review that allows users (via Menu/options) to choose units of either mg/dL (United States) or mmol/L (the rest of the world). Stat Cholesterol is freely beamable among Palm operating system devices.
FIGURE 2
Sample screens from STAT Cholesterol
Cholesterol 1.1
The third program is Cholesterol 1.1 by ScyMed, and runs on desktop computers using the Windows operating system. It is available in a CD-only version ($49.95) or a Web-based version. The Web-based version also includes the other resources on ScyMed’s Web site (a medical calculator and history/physical examination templates; single user, $149 per year). Like the other 2 programs, users enter pertinent data, then click “Create Profile.” Appropriately, the program does not force the user to enter all data on the entry screen. A new page opens that contains a summary of the data, including a table explicitly listing Framingham points for each pertinent entry (eg, the points for the age-sex category), the 10-year Framingham CHD (ATP III) risk, and specific suggestions for ATP III-compliant therapy (Figure 3).
Obviously, a major advantage of a PC-based system is the ability to produce a printout for the patient and for the chart. Printouts can be personalized with physician and patient name if the user chooses to enter this information. For physicians who have PC or Internet access in examination rooms or who generally preview laboratory reports in an office with such access, the CD or Web-based system presents an interesting option. Both Cholesterol 1.1 incarnations (CD and Web) include the complete ATP III Executive Summary. The therapy recommendations are hyperlinked to the relevant sections of the ATP-III Summary for users who wish to review any specifics in the recommendations.
FIGURE 3
Sample screen from Cholesterol 1.1
Conclusion
In summary, all 3 options “work.” All are meant to facilitate implementation of the ATP III guidelines. For physicians who wish to use ATP III guidelines to support their therapeutic decisions, all of these options simplify calculation and are better than simply guessing about whether—and which—therapy is appropriate. Regarding the 2 applications for the Palm operating system, Stat Cholesterol has a few more screens than NIH-ATP3, but these serve as helpful reminders about metabolic syndrome and triglyceride levels. Stat Cholesterol’s unique features include choice of units (mmol/L, mg/dL) and “real time” changes in 10-year risk numbers as data are entered or modified. NIH-ATP3 is the “cleanest” and simplest in my opinion. For physicians who have the computer resources and most especially for those who want personalized, printed information for the patient or chart (and are willing to enter these additional data), Cholesterol 1.1 for desktop computers is the way to go.
It is important to remember that the Framingham model was developed in individuals without known established CHD, and consisted largely of non-Hispanic white patients; thus data may not be entirely generalizable to other groups. In 1997, the American Diabetes Association2 also lowered the fasting glucose levels defining diabetes from 140 to 126 mg/dL; thus, the “mildest” forms of diabetes may not have the same prognostic significance. Finally, just because a population with a total cholesterol level of 280 mg/dL has one risk and a population with a total cholesterol level of 220 mg/dL has a lower risk, does not automatically mean that lowering the 280 cholesterol group’s cholesterol to 220 reduces their risk to that of the group whose innate cholesterol level was 220. However, it is tempting to use these data that way.
Finally, the NCEP ATP III tables offer recommendations only through age 79. Cholesterol 1.1 handles ages 80 and above improperly, but provides no error message or explanation. Stat Cholesterol allows only fixed choices from its drop-down menus; for age, these stop at age 79. NIH-ATP III appears to apply the risk values for age 79 to older individuals without modification (or notification to the user), although the product information specifies an age range up to 99 years.
Scenario
John is a 50-year-old man with treated hypertension; his blood pressure is 144/84 mm Hg. His lipid panel shows a total cholesterol level of 236 mg/dL, a low-density lipoprotein (LDL) level of 153 mg/dL, and high-density lipoprotein level of 48 mg/dL after therapeutic lifestyle changes. Should John be started on drug therapy to lower his lipid levels?
Solutions
John’s physician might decide whether to initiate drug therapy by “eyeballing” the lipids and making a clinical “guesstimate,” or by determining the Framingham 10-year risk. The Framingham 10-year risk determination is recommended by the Adult Treatment Panel (ATP III) of the National Institutes of Health.1 Although these calculations can be made using published charts,1 the charts are unwieldy and often not available at the point of care. Here are 3 electronic solutions that provide a better way to determine the ATP III-recommended strategy for your patients.
Atp III Cholesterol Management Guidelines
The first, downloadable free from the National Institutes of Health (Table 1), is entitled ATP III Cholesterol Management Guidelines (NIH-ATP3) and is available only for Palm operating system devices. The user enters the patient’s lipid values, age, and sex (Figure 1A). Known risk factors are checked via taps on the touch-sensitive palm-top device’s screen. If additional information is needed, such as the blood pressure, a second screen asks for those values. Then, the assessment is provided with options for additional information if desired (Figure 1B). The ATP III, or Framingham, risk percentage is for “hard” coronary heart disease (CHD) end points (myocardial infarction and cardiac death) during the next 10 years. NIH-ATP3 is not beamable from one handheld unit to another.
TABLE 1
Sources of programs
| Program | Source |
|---|---|
| NIH-ATP3 | http://hin.nhlbi.nih.gov/palmapps.htm |
| Stat Cholesterol | http://www.statcoder.com |
| Cholesterol 1.1 | http://www.ScyMed.com |
FIGURE 1
Sample screens from ATP III Cholesterol Management Guidelines (NIH-ATP3)
Another option for the Palm operating system is STAT Cholesterol, also downloadable. The price for it is banner advertising occupying about the bottom third of the screen (Figure 2A). STAT Cholesterol also uses ATP III treatment guidelines, but the presentation is different. Rather than numeric entry of lipid values, age, and blood pressure, these data are chosen from drop-down menus specifying ranges. Both ATP III CHD (hard end point) risk and total CHD risk are shown, along with the “average” risk and a “low” risk for age and sex (independent of other factors). As the user changes the values shown on the first screen (age, sex, blood pressure, lipids, and 3 check boxes), the 10-year ATP III risk and total CHD risk percentages change in real time, which is unique among these programs.
The therapeutic recommendations are not as clear on STAT Cholesterol as on the other programs. For example, when a patient is in the highest risk category, NIH-ATP3 clearly specifies that drug therapy is optional for LDL levels of 100 to 129 mg/dL and should be considered when LDL levels are ≥130 mg/dL. STAT Cholesterol lists drug treatment at an LDL level of ≥130 mg/dL but, in STAT Cholesterol, the user has to drill down into the details and scroll down to find that drug treatment is an option for LDL levels of 100 to 129 mg/dL (Figure 2B). However, STAT Cholesterol presents a check-box list for metabolic syndrome, with the appropriate boxes already checked from information previously entered. (Abdominal girth and, for nondiabetic individuals, assessment of fasting blood glucose, are additional user entries to complete this assessment.) This program is the only one of the 3 in this review that allows users (via Menu/options) to choose units of either mg/dL (United States) or mmol/L (the rest of the world). Stat Cholesterol is freely beamable among Palm operating system devices.
FIGURE 2
Sample screens from STAT Cholesterol
Cholesterol 1.1
The third program is Cholesterol 1.1 by ScyMed, and runs on desktop computers using the Windows operating system. It is available in a CD-only version ($49.95) or a Web-based version. The Web-based version also includes the other resources on ScyMed’s Web site (a medical calculator and history/physical examination templates; single user, $149 per year). Like the other 2 programs, users enter pertinent data, then click “Create Profile.” Appropriately, the program does not force the user to enter all data on the entry screen. A new page opens that contains a summary of the data, including a table explicitly listing Framingham points for each pertinent entry (eg, the points for the age-sex category), the 10-year Framingham CHD (ATP III) risk, and specific suggestions for ATP III-compliant therapy (Figure 3).
Obviously, a major advantage of a PC-based system is the ability to produce a printout for the patient and for the chart. Printouts can be personalized with physician and patient name if the user chooses to enter this information. For physicians who have PC or Internet access in examination rooms or who generally preview laboratory reports in an office with such access, the CD or Web-based system presents an interesting option. Both Cholesterol 1.1 incarnations (CD and Web) include the complete ATP III Executive Summary. The therapy recommendations are hyperlinked to the relevant sections of the ATP-III Summary for users who wish to review any specifics in the recommendations.
FIGURE 3
Sample screen from Cholesterol 1.1
Conclusion
In summary, all 3 options “work.” All are meant to facilitate implementation of the ATP III guidelines. For physicians who wish to use ATP III guidelines to support their therapeutic decisions, all of these options simplify calculation and are better than simply guessing about whether—and which—therapy is appropriate. Regarding the 2 applications for the Palm operating system, Stat Cholesterol has a few more screens than NIH-ATP3, but these serve as helpful reminders about metabolic syndrome and triglyceride levels. Stat Cholesterol’s unique features include choice of units (mmol/L, mg/dL) and “real time” changes in 10-year risk numbers as data are entered or modified. NIH-ATP3 is the “cleanest” and simplest in my opinion. For physicians who have the computer resources and most especially for those who want personalized, printed information for the patient or chart (and are willing to enter these additional data), Cholesterol 1.1 for desktop computers is the way to go.
It is important to remember that the Framingham model was developed in individuals without known established CHD, and consisted largely of non-Hispanic white patients; thus data may not be entirely generalizable to other groups. In 1997, the American Diabetes Association2 also lowered the fasting glucose levels defining diabetes from 140 to 126 mg/dL; thus, the “mildest” forms of diabetes may not have the same prognostic significance. Finally, just because a population with a total cholesterol level of 280 mg/dL has one risk and a population with a total cholesterol level of 220 mg/dL has a lower risk, does not automatically mean that lowering the 280 cholesterol group’s cholesterol to 220 reduces their risk to that of the group whose innate cholesterol level was 220. However, it is tempting to use these data that way.
Finally, the NCEP ATP III tables offer recommendations only through age 79. Cholesterol 1.1 handles ages 80 and above improperly, but provides no error message or explanation. Stat Cholesterol allows only fixed choices from its drop-down menus; for age, these stop at age 79. NIH-ATP III appears to apply the risk values for age 79 to older individuals without modification (or notification to the user), although the product information specifies an age range up to 99 years.
1. National Cholesterol Education Program. Third Report of the Expert Panel on Detection, Evaluation, and Treatment of high blood cholesterol in adults (Adult Treatment Panel III) Executive Summary. NIH publication 01-3670, May 2001. Available from: http://www.nhlbi.nih.gov/guidelines/cholesterol/atp_iii.htm.
2. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20:1183-97.
1. National Cholesterol Education Program. Third Report of the Expert Panel on Detection, Evaluation, and Treatment of high blood cholesterol in adults (Adult Treatment Panel III) Executive Summary. NIH publication 01-3670, May 2001. Available from: http://www.nhlbi.nih.gov/guidelines/cholesterol/atp_iii.htm.
2. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20:1183-97.
Hand-Held Electronic Prescribing
Do any of the following situations sound familiar?
- You want to prescribe 25 mg of a drug but are uncertain whether the drug is supplied as a 25-mg or 50-mg tablet.
- An elderly patient comes in for an update on her multiple problems. At the end of a long visit, she asks to have all 17 of her prescriptions refilled.
- You need to determine whether there is a possible drug interaction between existing medications and an upcoming medicine.
- You would like to be able to generate a list of all your patients taking a recently recalled drug.
Now imagine a hand-held prescribing device the size of a prescription pad that turns on instantly, knows the date, and through a connection to your computer, knows your patient list for the day. Using this device you could quickly select the patient’s name from a drop-down list and see his or her insurance plan, age, and other demographic information. You could select medications from an alphabetic scrolling list that includes information specific to the patient’s insurance plan. You could check allergies and drug interactions against the patient’s list of previously prescribed drugs and known medication allergies, alerting you only if a clinically significant problem is detected. After selecting the medication, you could choose from a list of available dosages and specify the quantity to be dispensed Figure 1, and the prescription could be digitally signed and sent electronically to the patient’s pharmacy or to your printer. Chart documentation could be produced concurrently on a sticky-backed label that can be affixed to the patient’s medical record. The prescription would be saved for generating rapid renewals in the future. Drug information and insurance formularies would be updated regularly from central computers, and new drugs and dosage forms could appear on the hand-held devices before they show up on the pharmacists’ shelves.
Does all this sound far-fetched? It’s not. This type of technology is currently available. Systems range from simple prescription writers—a hand-held device with initial manual entry of patient data and prescription printing from an infrared-equipped printer—to full electronic medical records systems. Prospective users have to decide which features provide sufficient benefit to merit the investment of time necessary to learn them. In this article, 3 systems (PocketScript, ePhysician ePad, and AllScripts;)Table 1, Table 1a are reviewed by physicians who have successfully incorporated electronic prescribing into their practices.
A system that does nothing other than produce legible prescriptions in the same time it would take to write one by hand can benefit many physicians. One that provides an accurate record of previous prescriptions that allows the rapid renewal of multiple prescriptions is even more valuable. Another important potential benefit of an electronic prescribing system is fewer errors, including those caused by illegible handwriting, incorrect dosage selections, drug-drug or drug-disease interactions, and drug allergies.
These systems still have some limitations, however. Most do not automatically suggest a dosage adjustment for age, renal function, hepatic function, and alcohol and tobacco use (although drug monographs may be available on the hand-held device itself). Similarly, weight-based pediatric prescription information may be available in monographs on the hand-held device but is not built into the prescribing process. Some states allow electronic transmission of prescriptions, some do not, and some have made no ruling; specific rules vary. Fortunately, each of the vendors reviewed in this article made certain that their system is installed in a way that conforms to state laws.
Most primary care physicians have not made the leap to electronic medical records; package delivery services and supermarket checkouts use more technology at the point of service than the average physician does. These devices may change that by providing a relatively low-cost low-risk improvement with less impact on work processes than a full electronic medical record.
Common Features
Each of the systems we reviewed is “wired” somewhat differently Figure 2. PocketScript and AllScripts use a wireless local area network in the physician’s office to move information from the hand-held device to a desktop computer server in the physician’s office. This server is in turn connected to the vendor’s computer through a modem or other high-speed access device to get drug information updates. The office computer also sends prescriptions directly to pharmacies either as an electronic message or by fax.
A system using ePhysician includes a personal computer in the physician’s office to load patient demographic information onto the hand-held using a docking cradle. Prescriptions can be sent directly from the hand-held device to a central computer server at the vendor’s offices using a wireless modem. Alternately, they physician can dock the hand-held device in a cradle attached to the computer, which is connected by a modem to the vendor’s central computer. The vendor’s computer server then sends prescriptions to the selected pharmacy, either electronically or by fax. All systems use sophisticated encryption to protect the confidentiality of data as it is sent between computers.
The process of generating a prescription follows that of using a paper prescription pad. Prescribers may override the predetermined choices and enter personal choices for quantity, instructions, and refills. The physician then views the completed prescription information, confirms the pharmacy information, and sends it through the wireless network and the computer system to the pharmacy or prints it in the office. All products support some type of list to facilitate rapid generation of custom prescriptions. Prescriptions produced by these systems benefit from perfect legibility, fraud and error reduction, automatic drug interactions checking (except ePad), and improved formulary compliance.
Each system can connect to front office systems and move patient demographic data into the prescription writing system. A real time interface updates both applications simultaneously, so information entered in the registration system is immediately available in the prescription writing system. With a bridge program, information entered into the registration system is unavailable in the prescription-writing program until the program is run and transfers the data to the prescription writing system.
PocketScript
Reviewed by Eric Weidmann, MD
PocketScript is unique, because the user can select voice recognition, screen touch, or the keyboard to quickly compose and send prescriptions. Patients’ records may be added or edited from the hand-held PC or the physician’s server. Hand-held to server communication is fast enough to provide high-speed Internet connectivity from the examination room, which is useful for patient care, business, and personal uses. Drug-drug interactions are checked automatically when choosing a drug and before sending the prescription. Patient allergy and diagnosis fields are promised for future releases.
PocketScript does not have to be linked to the practice’s registration system. If not linked, each patient must be entered manually the first time only. Patient data (eg, weight, insurance plan, and so on) can be changed using the Patient Maintenance function on the hand-held device. A scrollable Favorites list can be created of the physician’s most commonly used drugs; it uses PocketScript’s standard instructions for the signature. There is a scrollable, pull-down menu called Macros containing the physician’s custom-named drugs with physician-generated customized instructions and quantities (eg, special creams or a corticosteroid taper). Internet access on the wireless hand-held provides references for specialized disease and interaction information. I use my hand-held to access my E-mail as I move between patients. The keyboard allows me to use the hand-held to reply easily. We also use the E-mail system as an intra-office memo system for routine discussion and reminders.
Most of our prescriptions are faxed from the hand-held through the computer in our office to local pharmacies with the graphic of our log-in signature. Printed prescriptions can be sent to the printer in our office, which we then manually sign. PocketScript can provide digital signing when that complies with a state’s board of pharmacy regulations. Internet-enabled pharmacies can receive prescription data electronically using an E-mail–like system. There is no option for chart documentation other than printing a second script.
PocketScript is our choice because of its strong physician leadership, ethics, design, and serious commitment to the prescription process. It is usable by even the most computer phobic provider and does not attempt to replace anything but the paper prescription pad, phone, and wasted time—at least for now. Also, the vendor does not sell profiles of our prescribing habits. Security of the patient data and prescription process are excellent and are maintained even if the hand-held device is stolen. PocketScript is intuitive, simple, and efficient, with no tolerance for errors.
The design of the PocketScript server-based system eliminates the need to dock hand-held devices, avoiding time-consuming and frustrating tasks for the physician. This system is ideal for physicians who do most of their work in one or a few sites in which wireless nodes can be installed. We have changed office processes for refill and pharmacy calls, saving an estimated 1 hour per day per nurse and 30 minutes per day per file clerk. Patients and pharmacists frequently praise the clarity, accuracy, and convenience of the PocketScript system. PocketScript is a serious medical care partner and the perfect first step into e-medicine for our group practice.
ePhysician ePad
Reviewed by Daniel E. Diamond, MD
The ePhysician system uses a wireless wide area network (WAN) rather than a wireless local area network in the physician’s office. Prescriptions can be transmitted directly to the vendor’s server through an OmniSky (or equivalent) wireless cellular-WAN modem. The physicians who do not want to use the wireless interface can use the docking cradle attached to a computer in the office for synchronization. The prescription is then securely sent through the Internet to the vendor’s computer (using the cradle takes approximately 30 seconds per synchronization). The wireless method is more efficient and allows the physician to write and send the prescription without leaving the examination room. It also allows the physician to write and send prescriptions when away from the office.
ePad has several other unique features. Because patient demographics are entered into the physician’s existing practice management system and transmitted to the hand-held when it is docked, the physician does not have to enter any patient data. To write a prescription for a patient who has not previously been entered into the system, the user docks the hand-held in the cradle for synchronization. Also, all prescriptions are transmitted from the vendor’s central computer servers either electronically or by fax to any pharmacy in the United States. Users can also print from the hand-held to a local printer. To generate chart documentation, the user can configure ePad to automatically print a copy of the prescription on the local computer when it transmits to the pharmacy. ePad currently comes bundled with ePhysician Superbill for charge capture and is integrated with Drug Facts and Comparisons. It also includes a Web interface that allows my staff to efficiently process prescription renewals, and a scheduling module that makes it possible to schedule patients on the computer. This schedule is viewable on the hand-held device.
ePad by ePhysician with the OmniSky wireless service is simple, efficient, and powerful. Its interface was designed with a focus on the physician user. Although there is a subscription charge for ePad, the fee pales in comparison with the cost of lost physician productivity due to the inefficient technology of printing prescriptions locally (or writing them by hand). Using the ePad system in our office has resulted in very positive patient feedback and increased efficiency and job satisfaction among staff.
AllScripts
Reviewed by Azar A. Korbey, MD
At the installation stage, AllScripts’ on-site team realizes that the use of these systems require change. They take the time to train the staff and make them part of the process. AllScripts differs from the other systems, because after the selection of the patient name, users select their most frequently coded diseases listed by common name and International Classification of Diseases-ninth revision code. This list is prescriber-specific, not patient-specific. Users can also access the patient’s prescription and diagnosis histories, and the AllScripts system automatically checks for previous adverse drug reactions. Next, AllScripts shows the medicines that the user most frequently prescribes for a disease. AllScripts learns each user’s prescribing preferences, so users do not need to enter their favorite prescriptions. The list also shows preferred instructions for any given medication, and if AllScripts’ office dispensing system is used, it will tell users whether they have the drug in inventory. To produce a prescription, the prescriber may modify a prescription from a frequently used list or choose from any other drug in AllScripts’ database.
Users have access to all patients in the practice through the network, regardless of provider or schedule. Patients not registered with the practice can be manually added into the hand-held device or desktop computer server. Unlike the other systems, AllScripts automatically produces a mailing address-sized label for chart documentation that includes all details of the prescription. The vendor also sells a turnkey pharmacy service (FirstFill) for in-office dispensing. It is only for common medications, and is similar to providing samples. The local wireless network is fast; high-speed access to the Internet is proving very useful.
AllScripts is complete and does what it promises. It is a well-funded, publicly traded company that is adding applications and acquiring additional companies that will allow dictation and charge-capture systems to be added. I have had long-term experience with the product and its exemplary phone support, and I believe they will both be around in the future. They are even willing to come on site immediately, if required. I strongly recommend this system.
Editor’s Note: We had hoped to include the iScribe 3000 system (www.iscribe.com) in this review but could not obtain the product and complete the review in time for publication. We plan to publish a software review of iScribe in a future issue of JFP.
Do any of the following situations sound familiar?
- You want to prescribe 25 mg of a drug but are uncertain whether the drug is supplied as a 25-mg or 50-mg tablet.
- An elderly patient comes in for an update on her multiple problems. At the end of a long visit, she asks to have all 17 of her prescriptions refilled.
- You need to determine whether there is a possible drug interaction between existing medications and an upcoming medicine.
- You would like to be able to generate a list of all your patients taking a recently recalled drug.
Now imagine a hand-held prescribing device the size of a prescription pad that turns on instantly, knows the date, and through a connection to your computer, knows your patient list for the day. Using this device you could quickly select the patient’s name from a drop-down list and see his or her insurance plan, age, and other demographic information. You could select medications from an alphabetic scrolling list that includes information specific to the patient’s insurance plan. You could check allergies and drug interactions against the patient’s list of previously prescribed drugs and known medication allergies, alerting you only if a clinically significant problem is detected. After selecting the medication, you could choose from a list of available dosages and specify the quantity to be dispensed Figure 1, and the prescription could be digitally signed and sent electronically to the patient’s pharmacy or to your printer. Chart documentation could be produced concurrently on a sticky-backed label that can be affixed to the patient’s medical record. The prescription would be saved for generating rapid renewals in the future. Drug information and insurance formularies would be updated regularly from central computers, and new drugs and dosage forms could appear on the hand-held devices before they show up on the pharmacists’ shelves.
Does all this sound far-fetched? It’s not. This type of technology is currently available. Systems range from simple prescription writers—a hand-held device with initial manual entry of patient data and prescription printing from an infrared-equipped printer—to full electronic medical records systems. Prospective users have to decide which features provide sufficient benefit to merit the investment of time necessary to learn them. In this article, 3 systems (PocketScript, ePhysician ePad, and AllScripts;)Table 1, Table 1a are reviewed by physicians who have successfully incorporated electronic prescribing into their practices.
A system that does nothing other than produce legible prescriptions in the same time it would take to write one by hand can benefit many physicians. One that provides an accurate record of previous prescriptions that allows the rapid renewal of multiple prescriptions is even more valuable. Another important potential benefit of an electronic prescribing system is fewer errors, including those caused by illegible handwriting, incorrect dosage selections, drug-drug or drug-disease interactions, and drug allergies.
These systems still have some limitations, however. Most do not automatically suggest a dosage adjustment for age, renal function, hepatic function, and alcohol and tobacco use (although drug monographs may be available on the hand-held device itself). Similarly, weight-based pediatric prescription information may be available in monographs on the hand-held device but is not built into the prescribing process. Some states allow electronic transmission of prescriptions, some do not, and some have made no ruling; specific rules vary. Fortunately, each of the vendors reviewed in this article made certain that their system is installed in a way that conforms to state laws.
Most primary care physicians have not made the leap to electronic medical records; package delivery services and supermarket checkouts use more technology at the point of service than the average physician does. These devices may change that by providing a relatively low-cost low-risk improvement with less impact on work processes than a full electronic medical record.
Common Features
Each of the systems we reviewed is “wired” somewhat differently Figure 2. PocketScript and AllScripts use a wireless local area network in the physician’s office to move information from the hand-held device to a desktop computer server in the physician’s office. This server is in turn connected to the vendor’s computer through a modem or other high-speed access device to get drug information updates. The office computer also sends prescriptions directly to pharmacies either as an electronic message or by fax.
A system using ePhysician includes a personal computer in the physician’s office to load patient demographic information onto the hand-held using a docking cradle. Prescriptions can be sent directly from the hand-held device to a central computer server at the vendor’s offices using a wireless modem. Alternately, they physician can dock the hand-held device in a cradle attached to the computer, which is connected by a modem to the vendor’s central computer. The vendor’s computer server then sends prescriptions to the selected pharmacy, either electronically or by fax. All systems use sophisticated encryption to protect the confidentiality of data as it is sent between computers.
The process of generating a prescription follows that of using a paper prescription pad. Prescribers may override the predetermined choices and enter personal choices for quantity, instructions, and refills. The physician then views the completed prescription information, confirms the pharmacy information, and sends it through the wireless network and the computer system to the pharmacy or prints it in the office. All products support some type of list to facilitate rapid generation of custom prescriptions. Prescriptions produced by these systems benefit from perfect legibility, fraud and error reduction, automatic drug interactions checking (except ePad), and improved formulary compliance.
Each system can connect to front office systems and move patient demographic data into the prescription writing system. A real time interface updates both applications simultaneously, so information entered in the registration system is immediately available in the prescription writing system. With a bridge program, information entered into the registration system is unavailable in the prescription-writing program until the program is run and transfers the data to the prescription writing system.
PocketScript
Reviewed by Eric Weidmann, MD
PocketScript is unique, because the user can select voice recognition, screen touch, or the keyboard to quickly compose and send prescriptions. Patients’ records may be added or edited from the hand-held PC or the physician’s server. Hand-held to server communication is fast enough to provide high-speed Internet connectivity from the examination room, which is useful for patient care, business, and personal uses. Drug-drug interactions are checked automatically when choosing a drug and before sending the prescription. Patient allergy and diagnosis fields are promised for future releases.
PocketScript does not have to be linked to the practice’s registration system. If not linked, each patient must be entered manually the first time only. Patient data (eg, weight, insurance plan, and so on) can be changed using the Patient Maintenance function on the hand-held device. A scrollable Favorites list can be created of the physician’s most commonly used drugs; it uses PocketScript’s standard instructions for the signature. There is a scrollable, pull-down menu called Macros containing the physician’s custom-named drugs with physician-generated customized instructions and quantities (eg, special creams or a corticosteroid taper). Internet access on the wireless hand-held provides references for specialized disease and interaction information. I use my hand-held to access my E-mail as I move between patients. The keyboard allows me to use the hand-held to reply easily. We also use the E-mail system as an intra-office memo system for routine discussion and reminders.
Most of our prescriptions are faxed from the hand-held through the computer in our office to local pharmacies with the graphic of our log-in signature. Printed prescriptions can be sent to the printer in our office, which we then manually sign. PocketScript can provide digital signing when that complies with a state’s board of pharmacy regulations. Internet-enabled pharmacies can receive prescription data electronically using an E-mail–like system. There is no option for chart documentation other than printing a second script.
PocketScript is our choice because of its strong physician leadership, ethics, design, and serious commitment to the prescription process. It is usable by even the most computer phobic provider and does not attempt to replace anything but the paper prescription pad, phone, and wasted time—at least for now. Also, the vendor does not sell profiles of our prescribing habits. Security of the patient data and prescription process are excellent and are maintained even if the hand-held device is stolen. PocketScript is intuitive, simple, and efficient, with no tolerance for errors.
The design of the PocketScript server-based system eliminates the need to dock hand-held devices, avoiding time-consuming and frustrating tasks for the physician. This system is ideal for physicians who do most of their work in one or a few sites in which wireless nodes can be installed. We have changed office processes for refill and pharmacy calls, saving an estimated 1 hour per day per nurse and 30 minutes per day per file clerk. Patients and pharmacists frequently praise the clarity, accuracy, and convenience of the PocketScript system. PocketScript is a serious medical care partner and the perfect first step into e-medicine for our group practice.
ePhysician ePad
Reviewed by Daniel E. Diamond, MD
The ePhysician system uses a wireless wide area network (WAN) rather than a wireless local area network in the physician’s office. Prescriptions can be transmitted directly to the vendor’s server through an OmniSky (or equivalent) wireless cellular-WAN modem. The physicians who do not want to use the wireless interface can use the docking cradle attached to a computer in the office for synchronization. The prescription is then securely sent through the Internet to the vendor’s computer (using the cradle takes approximately 30 seconds per synchronization). The wireless method is more efficient and allows the physician to write and send the prescription without leaving the examination room. It also allows the physician to write and send prescriptions when away from the office.
ePad has several other unique features. Because patient demographics are entered into the physician’s existing practice management system and transmitted to the hand-held when it is docked, the physician does not have to enter any patient data. To write a prescription for a patient who has not previously been entered into the system, the user docks the hand-held in the cradle for synchronization. Also, all prescriptions are transmitted from the vendor’s central computer servers either electronically or by fax to any pharmacy in the United States. Users can also print from the hand-held to a local printer. To generate chart documentation, the user can configure ePad to automatically print a copy of the prescription on the local computer when it transmits to the pharmacy. ePad currently comes bundled with ePhysician Superbill for charge capture and is integrated with Drug Facts and Comparisons. It also includes a Web interface that allows my staff to efficiently process prescription renewals, and a scheduling module that makes it possible to schedule patients on the computer. This schedule is viewable on the hand-held device.
ePad by ePhysician with the OmniSky wireless service is simple, efficient, and powerful. Its interface was designed with a focus on the physician user. Although there is a subscription charge for ePad, the fee pales in comparison with the cost of lost physician productivity due to the inefficient technology of printing prescriptions locally (or writing them by hand). Using the ePad system in our office has resulted in very positive patient feedback and increased efficiency and job satisfaction among staff.
AllScripts
Reviewed by Azar A. Korbey, MD
At the installation stage, AllScripts’ on-site team realizes that the use of these systems require change. They take the time to train the staff and make them part of the process. AllScripts differs from the other systems, because after the selection of the patient name, users select their most frequently coded diseases listed by common name and International Classification of Diseases-ninth revision code. This list is prescriber-specific, not patient-specific. Users can also access the patient’s prescription and diagnosis histories, and the AllScripts system automatically checks for previous adverse drug reactions. Next, AllScripts shows the medicines that the user most frequently prescribes for a disease. AllScripts learns each user’s prescribing preferences, so users do not need to enter their favorite prescriptions. The list also shows preferred instructions for any given medication, and if AllScripts’ office dispensing system is used, it will tell users whether they have the drug in inventory. To produce a prescription, the prescriber may modify a prescription from a frequently used list or choose from any other drug in AllScripts’ database.
Users have access to all patients in the practice through the network, regardless of provider or schedule. Patients not registered with the practice can be manually added into the hand-held device or desktop computer server. Unlike the other systems, AllScripts automatically produces a mailing address-sized label for chart documentation that includes all details of the prescription. The vendor also sells a turnkey pharmacy service (FirstFill) for in-office dispensing. It is only for common medications, and is similar to providing samples. The local wireless network is fast; high-speed access to the Internet is proving very useful.
AllScripts is complete and does what it promises. It is a well-funded, publicly traded company that is adding applications and acquiring additional companies that will allow dictation and charge-capture systems to be added. I have had long-term experience with the product and its exemplary phone support, and I believe they will both be around in the future. They are even willing to come on site immediately, if required. I strongly recommend this system.
Editor’s Note: We had hoped to include the iScribe 3000 system (www.iscribe.com) in this review but could not obtain the product and complete the review in time for publication. We plan to publish a software review of iScribe in a future issue of JFP.
Do any of the following situations sound familiar?
- You want to prescribe 25 mg of a drug but are uncertain whether the drug is supplied as a 25-mg or 50-mg tablet.
- An elderly patient comes in for an update on her multiple problems. At the end of a long visit, she asks to have all 17 of her prescriptions refilled.
- You need to determine whether there is a possible drug interaction between existing medications and an upcoming medicine.
- You would like to be able to generate a list of all your patients taking a recently recalled drug.
Now imagine a hand-held prescribing device the size of a prescription pad that turns on instantly, knows the date, and through a connection to your computer, knows your patient list for the day. Using this device you could quickly select the patient’s name from a drop-down list and see his or her insurance plan, age, and other demographic information. You could select medications from an alphabetic scrolling list that includes information specific to the patient’s insurance plan. You could check allergies and drug interactions against the patient’s list of previously prescribed drugs and known medication allergies, alerting you only if a clinically significant problem is detected. After selecting the medication, you could choose from a list of available dosages and specify the quantity to be dispensed Figure 1, and the prescription could be digitally signed and sent electronically to the patient’s pharmacy or to your printer. Chart documentation could be produced concurrently on a sticky-backed label that can be affixed to the patient’s medical record. The prescription would be saved for generating rapid renewals in the future. Drug information and insurance formularies would be updated regularly from central computers, and new drugs and dosage forms could appear on the hand-held devices before they show up on the pharmacists’ shelves.
Does all this sound far-fetched? It’s not. This type of technology is currently available. Systems range from simple prescription writers—a hand-held device with initial manual entry of patient data and prescription printing from an infrared-equipped printer—to full electronic medical records systems. Prospective users have to decide which features provide sufficient benefit to merit the investment of time necessary to learn them. In this article, 3 systems (PocketScript, ePhysician ePad, and AllScripts;)Table 1, Table 1a are reviewed by physicians who have successfully incorporated electronic prescribing into their practices.
A system that does nothing other than produce legible prescriptions in the same time it would take to write one by hand can benefit many physicians. One that provides an accurate record of previous prescriptions that allows the rapid renewal of multiple prescriptions is even more valuable. Another important potential benefit of an electronic prescribing system is fewer errors, including those caused by illegible handwriting, incorrect dosage selections, drug-drug or drug-disease interactions, and drug allergies.
These systems still have some limitations, however. Most do not automatically suggest a dosage adjustment for age, renal function, hepatic function, and alcohol and tobacco use (although drug monographs may be available on the hand-held device itself). Similarly, weight-based pediatric prescription information may be available in monographs on the hand-held device but is not built into the prescribing process. Some states allow electronic transmission of prescriptions, some do not, and some have made no ruling; specific rules vary. Fortunately, each of the vendors reviewed in this article made certain that their system is installed in a way that conforms to state laws.
Most primary care physicians have not made the leap to electronic medical records; package delivery services and supermarket checkouts use more technology at the point of service than the average physician does. These devices may change that by providing a relatively low-cost low-risk improvement with less impact on work processes than a full electronic medical record.
Common Features
Each of the systems we reviewed is “wired” somewhat differently Figure 2. PocketScript and AllScripts use a wireless local area network in the physician’s office to move information from the hand-held device to a desktop computer server in the physician’s office. This server is in turn connected to the vendor’s computer through a modem or other high-speed access device to get drug information updates. The office computer also sends prescriptions directly to pharmacies either as an electronic message or by fax.
A system using ePhysician includes a personal computer in the physician’s office to load patient demographic information onto the hand-held using a docking cradle. Prescriptions can be sent directly from the hand-held device to a central computer server at the vendor’s offices using a wireless modem. Alternately, they physician can dock the hand-held device in a cradle attached to the computer, which is connected by a modem to the vendor’s central computer. The vendor’s computer server then sends prescriptions to the selected pharmacy, either electronically or by fax. All systems use sophisticated encryption to protect the confidentiality of data as it is sent between computers.
The process of generating a prescription follows that of using a paper prescription pad. Prescribers may override the predetermined choices and enter personal choices for quantity, instructions, and refills. The physician then views the completed prescription information, confirms the pharmacy information, and sends it through the wireless network and the computer system to the pharmacy or prints it in the office. All products support some type of list to facilitate rapid generation of custom prescriptions. Prescriptions produced by these systems benefit from perfect legibility, fraud and error reduction, automatic drug interactions checking (except ePad), and improved formulary compliance.
Each system can connect to front office systems and move patient demographic data into the prescription writing system. A real time interface updates both applications simultaneously, so information entered in the registration system is immediately available in the prescription writing system. With a bridge program, information entered into the registration system is unavailable in the prescription-writing program until the program is run and transfers the data to the prescription writing system.
PocketScript
Reviewed by Eric Weidmann, MD
PocketScript is unique, because the user can select voice recognition, screen touch, or the keyboard to quickly compose and send prescriptions. Patients’ records may be added or edited from the hand-held PC or the physician’s server. Hand-held to server communication is fast enough to provide high-speed Internet connectivity from the examination room, which is useful for patient care, business, and personal uses. Drug-drug interactions are checked automatically when choosing a drug and before sending the prescription. Patient allergy and diagnosis fields are promised for future releases.
PocketScript does not have to be linked to the practice’s registration system. If not linked, each patient must be entered manually the first time only. Patient data (eg, weight, insurance plan, and so on) can be changed using the Patient Maintenance function on the hand-held device. A scrollable Favorites list can be created of the physician’s most commonly used drugs; it uses PocketScript’s standard instructions for the signature. There is a scrollable, pull-down menu called Macros containing the physician’s custom-named drugs with physician-generated customized instructions and quantities (eg, special creams or a corticosteroid taper). Internet access on the wireless hand-held provides references for specialized disease and interaction information. I use my hand-held to access my E-mail as I move between patients. The keyboard allows me to use the hand-held to reply easily. We also use the E-mail system as an intra-office memo system for routine discussion and reminders.
Most of our prescriptions are faxed from the hand-held through the computer in our office to local pharmacies with the graphic of our log-in signature. Printed prescriptions can be sent to the printer in our office, which we then manually sign. PocketScript can provide digital signing when that complies with a state’s board of pharmacy regulations. Internet-enabled pharmacies can receive prescription data electronically using an E-mail–like system. There is no option for chart documentation other than printing a second script.
PocketScript is our choice because of its strong physician leadership, ethics, design, and serious commitment to the prescription process. It is usable by even the most computer phobic provider and does not attempt to replace anything but the paper prescription pad, phone, and wasted time—at least for now. Also, the vendor does not sell profiles of our prescribing habits. Security of the patient data and prescription process are excellent and are maintained even if the hand-held device is stolen. PocketScript is intuitive, simple, and efficient, with no tolerance for errors.
The design of the PocketScript server-based system eliminates the need to dock hand-held devices, avoiding time-consuming and frustrating tasks for the physician. This system is ideal for physicians who do most of their work in one or a few sites in which wireless nodes can be installed. We have changed office processes for refill and pharmacy calls, saving an estimated 1 hour per day per nurse and 30 minutes per day per file clerk. Patients and pharmacists frequently praise the clarity, accuracy, and convenience of the PocketScript system. PocketScript is a serious medical care partner and the perfect first step into e-medicine for our group practice.
ePhysician ePad
Reviewed by Daniel E. Diamond, MD
The ePhysician system uses a wireless wide area network (WAN) rather than a wireless local area network in the physician’s office. Prescriptions can be transmitted directly to the vendor’s server through an OmniSky (or equivalent) wireless cellular-WAN modem. The physicians who do not want to use the wireless interface can use the docking cradle attached to a computer in the office for synchronization. The prescription is then securely sent through the Internet to the vendor’s computer (using the cradle takes approximately 30 seconds per synchronization). The wireless method is more efficient and allows the physician to write and send the prescription without leaving the examination room. It also allows the physician to write and send prescriptions when away from the office.
ePad has several other unique features. Because patient demographics are entered into the physician’s existing practice management system and transmitted to the hand-held when it is docked, the physician does not have to enter any patient data. To write a prescription for a patient who has not previously been entered into the system, the user docks the hand-held in the cradle for synchronization. Also, all prescriptions are transmitted from the vendor’s central computer servers either electronically or by fax to any pharmacy in the United States. Users can also print from the hand-held to a local printer. To generate chart documentation, the user can configure ePad to automatically print a copy of the prescription on the local computer when it transmits to the pharmacy. ePad currently comes bundled with ePhysician Superbill for charge capture and is integrated with Drug Facts and Comparisons. It also includes a Web interface that allows my staff to efficiently process prescription renewals, and a scheduling module that makes it possible to schedule patients on the computer. This schedule is viewable on the hand-held device.
ePad by ePhysician with the OmniSky wireless service is simple, efficient, and powerful. Its interface was designed with a focus on the physician user. Although there is a subscription charge for ePad, the fee pales in comparison with the cost of lost physician productivity due to the inefficient technology of printing prescriptions locally (or writing them by hand). Using the ePad system in our office has resulted in very positive patient feedback and increased efficiency and job satisfaction among staff.
AllScripts
Reviewed by Azar A. Korbey, MD
At the installation stage, AllScripts’ on-site team realizes that the use of these systems require change. They take the time to train the staff and make them part of the process. AllScripts differs from the other systems, because after the selection of the patient name, users select their most frequently coded diseases listed by common name and International Classification of Diseases-ninth revision code. This list is prescriber-specific, not patient-specific. Users can also access the patient’s prescription and diagnosis histories, and the AllScripts system automatically checks for previous adverse drug reactions. Next, AllScripts shows the medicines that the user most frequently prescribes for a disease. AllScripts learns each user’s prescribing preferences, so users do not need to enter their favorite prescriptions. The list also shows preferred instructions for any given medication, and if AllScripts’ office dispensing system is used, it will tell users whether they have the drug in inventory. To produce a prescription, the prescriber may modify a prescription from a frequently used list or choose from any other drug in AllScripts’ database.
Users have access to all patients in the practice through the network, regardless of provider or schedule. Patients not registered with the practice can be manually added into the hand-held device or desktop computer server. Unlike the other systems, AllScripts automatically produces a mailing address-sized label for chart documentation that includes all details of the prescription. The vendor also sells a turnkey pharmacy service (FirstFill) for in-office dispensing. It is only for common medications, and is similar to providing samples. The local wireless network is fast; high-speed access to the Internet is proving very useful.
AllScripts is complete and does what it promises. It is a well-funded, publicly traded company that is adding applications and acquiring additional companies that will allow dictation and charge-capture systems to be added. I have had long-term experience with the product and its exemplary phone support, and I believe they will both be around in the future. They are even willing to come on site immediately, if required. I strongly recommend this system.
Editor’s Note: We had hoped to include the iScribe 3000 system (www.iscribe.com) in this review but could not obtain the product and complete the review in time for publication. We plan to publish a software review of iScribe in a future issue of JFP.