User login
Primary care may be inadequate for cancer survivors

Primary care may not meet the healthcare needs of cancer survivors in the US, according to research published in JAMA Internal Medicine.
Researchers examined 12 advanced primary care practices selected from a national registry of “workforce innovators” and found that none of these practices had a comprehensive survivorship care program in place.
In addition, there were 3 main barriers to survivorship care—not treating cancer survivors as a distinct population, limitations of electronic health records, and a lack of information and guidance for clinicians.
“This is troubling because these are highly innovative practices that have a national reputation,” said study author Benjamin Crabtree, PhD, of Rutgers Robert Wood Johnson Medical School in New Brunswick, New Jersey.
Dr Crabtree and his colleagues evaluated survivorship care* at the 12 practices, which were based in Colorado, Illinois, Maine, New York, Pennsylvania, and Washington.
Over nearly 2 years, the team spent 10 to 12 days observing each of the practices and interviewing clinicians and administrators.
In this way, the researchers identified 3 main barriers to integrating survivorship care into primary medicine.
Barrier 1
The first barrier was that clinicians did not treat cancer survivors as a distinct population or clinical category.
“There is no diagnosis code for ‘cancer survivor’ that can be entered into the medical record, which is important if you want physicians to pay attention,” Dr Crabtree said.
Some of the clinicians interviewed said their care was comprehensive enough to address the needs of all patients. Other clinicians did not understand what survivorship care entails.
Barrier 2
The second barrier was that electronic health record systems didn’t support survivorship care.
Clinicians reported an inability to identify patients with a history of cancer. Even if a patient’s cancer history was included in his or her record, it might take searching through multiple screens to find the information.
In addition, medical records were sometimes lost as patients changed clinicians over the years, which left it up to patients to report their cancer histories.
Barrier 3
The third barrier was that clinicians did not receive adequate information or guidance for follow-up care of cancer survivors.
Although some of the practices received cancer-related information about their patients, it was considered “inadequate” or “not actionable.”
Clinicians expressed concerns about their knowledge gaps in cancer care and the need to monitor changing information in oncology.
“There is nothing in the residency curriculum about cancer survivorship,” Dr Crabtree said. “There is also nothing in Continuing Medical Education courses. It’s just not there.”
Dr Crabtree and his colleagues believe these barriers must be addressed so that comprehensive cancer survivorship services can move to the forefront of primary care. ![]()
* Survivorship care includes checking for cancer recurrence, monitoring long-term effects of radiation and chemotherapy, and assessing a patient’s psychological well-being.
Primary care may not meet the healthcare needs of cancer survivors in the US, according to research published in JAMA Internal Medicine.
Researchers examined 12 advanced primary care practices selected from a national registry of “workforce innovators” and found that none of these practices had a comprehensive survivorship care program in place.
In addition, there were 3 main barriers to survivorship care—not treating cancer survivors as a distinct population, limitations of electronic health records, and a lack of information and guidance for clinicians.
“This is troubling because these are highly innovative practices that have a national reputation,” said study author Benjamin Crabtree, PhD, of Rutgers Robert Wood Johnson Medical School in New Brunswick, New Jersey.
Dr Crabtree and his colleagues evaluated survivorship care* at the 12 practices, which were based in Colorado, Illinois, Maine, New York, Pennsylvania, and Washington.
Over nearly 2 years, the team spent 10 to 12 days observing each of the practices and interviewing clinicians and administrators.
In this way, the researchers identified 3 main barriers to integrating survivorship care into primary medicine.
Barrier 1
The first barrier was that clinicians did not treat cancer survivors as a distinct population or clinical category.
“There is no diagnosis code for ‘cancer survivor’ that can be entered into the medical record, which is important if you want physicians to pay attention,” Dr Crabtree said.
Some of the clinicians interviewed said their care was comprehensive enough to address the needs of all patients. Other clinicians did not understand what survivorship care entails.
Barrier 2
The second barrier was that electronic health record systems didn’t support survivorship care.
Clinicians reported an inability to identify patients with a history of cancer. Even if a patient’s cancer history was included in his or her record, it might take searching through multiple screens to find the information.
In addition, medical records were sometimes lost as patients changed clinicians over the years, which left it up to patients to report their cancer histories.
Barrier 3
The third barrier was that clinicians did not receive adequate information or guidance for follow-up care of cancer survivors.
Although some of the practices received cancer-related information about their patients, it was considered “inadequate” or “not actionable.”
Clinicians expressed concerns about their knowledge gaps in cancer care and the need to monitor changing information in oncology.
“There is nothing in the residency curriculum about cancer survivorship,” Dr Crabtree said. “There is also nothing in Continuing Medical Education courses. It’s just not there.”
Dr Crabtree and his colleagues believe these barriers must be addressed so that comprehensive cancer survivorship services can move to the forefront of primary care. ![]()
* Survivorship care includes checking for cancer recurrence, monitoring long-term effects of radiation and chemotherapy, and assessing a patient’s psychological well-being.
Primary care may not meet the healthcare needs of cancer survivors in the US, according to research published in JAMA Internal Medicine.
Researchers examined 12 advanced primary care practices selected from a national registry of “workforce innovators” and found that none of these practices had a comprehensive survivorship care program in place.
In addition, there were 3 main barriers to survivorship care—not treating cancer survivors as a distinct population, limitations of electronic health records, and a lack of information and guidance for clinicians.
“This is troubling because these are highly innovative practices that have a national reputation,” said study author Benjamin Crabtree, PhD, of Rutgers Robert Wood Johnson Medical School in New Brunswick, New Jersey.
Dr Crabtree and his colleagues evaluated survivorship care* at the 12 practices, which were based in Colorado, Illinois, Maine, New York, Pennsylvania, and Washington.
Over nearly 2 years, the team spent 10 to 12 days observing each of the practices and interviewing clinicians and administrators.
In this way, the researchers identified 3 main barriers to integrating survivorship care into primary medicine.
Barrier 1
The first barrier was that clinicians did not treat cancer survivors as a distinct population or clinical category.
“There is no diagnosis code for ‘cancer survivor’ that can be entered into the medical record, which is important if you want physicians to pay attention,” Dr Crabtree said.
Some of the clinicians interviewed said their care was comprehensive enough to address the needs of all patients. Other clinicians did not understand what survivorship care entails.
Barrier 2
The second barrier was that electronic health record systems didn’t support survivorship care.
Clinicians reported an inability to identify patients with a history of cancer. Even if a patient’s cancer history was included in his or her record, it might take searching through multiple screens to find the information.
In addition, medical records were sometimes lost as patients changed clinicians over the years, which left it up to patients to report their cancer histories.
Barrier 3
The third barrier was that clinicians did not receive adequate information or guidance for follow-up care of cancer survivors.
Although some of the practices received cancer-related information about their patients, it was considered “inadequate” or “not actionable.”
Clinicians expressed concerns about their knowledge gaps in cancer care and the need to monitor changing information in oncology.
“There is nothing in the residency curriculum about cancer survivorship,” Dr Crabtree said. “There is also nothing in Continuing Medical Education courses. It’s just not there.”
Dr Crabtree and his colleagues believe these barriers must be addressed so that comprehensive cancer survivorship services can move to the forefront of primary care. ![]()
* Survivorship care includes checking for cancer recurrence, monitoring long-term effects of radiation and chemotherapy, and assessing a patient’s psychological well-being.
Drug receives orphan designation for treatment of MDS

The European Commission has granted orphan designation to asunercept (APG101) for the treatment of myelodysplastic syndromes (MDS).
Asunercept is a fully human fusion protein that consists of the extracellular domain of the CD95 receptor and the Fc domain of an IgG1 antibody.
Asunercept binds to the CD95 ligand and blocks activation of the CD95 receptor.
Excessive stimulation of the CD95 receptor on hematopoietic precursors inhibits erythropoiesis in MDS patients.
As a result, the patients develop transfusion-dependent anemia that is refractory to erythropoiesis-stimulating agents (ESAs).
Treatment with asunercept, by inhibiting the CD95 system, stimulates the production of red blood cells and decreases transfusion dependency.
Asunercept has been evaluated in a phase 1 trial, the results of which were presented at the 2016 ASH Annual Meeting.
The trial enrolled 20 patients with low- to intermediate-risk MDS. All patients had anemia resulting in a high transfusion burden, had hemoglobin levels of less than 10 g/dL, and were refractory to ESAs.
Patients received once-weekly asunercept infusions for 12 weeks. Eight of the 20 patients (40%) experienced a reduction in transfusion frequency for 6 months.
Asunercept was considered generally well tolerated, with no grade 3 or higher treatment-related adverse events reported. The most common treatment-emergent adverse events were peripheral edema (n=6), urinary tract infection (n=4), and oral herpes (n=3).
One patient developed acute myeloid leukemia, and 1 patient died from sepsis due to pre-existing neutropenia.
“We are highly encouraged by the data from our clinical phase 1 trial with asunercept in these patients and are currently preparing to initiate a clinical phase 2 proof-of-concept trial to further evaluate the efficacy of asunercept in MDS,” said Harald Fricke, chief medical officer of Apogenix AG, the company developing asunercept.
About orphan designation
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure. ![]()
The European Commission has granted orphan designation to asunercept (APG101) for the treatment of myelodysplastic syndromes (MDS).
Asunercept is a fully human fusion protein that consists of the extracellular domain of the CD95 receptor and the Fc domain of an IgG1 antibody.
Asunercept binds to the CD95 ligand and blocks activation of the CD95 receptor.
Excessive stimulation of the CD95 receptor on hematopoietic precursors inhibits erythropoiesis in MDS patients.
As a result, the patients develop transfusion-dependent anemia that is refractory to erythropoiesis-stimulating agents (ESAs).
Treatment with asunercept, by inhibiting the CD95 system, stimulates the production of red blood cells and decreases transfusion dependency.
Asunercept has been evaluated in a phase 1 trial, the results of which were presented at the 2016 ASH Annual Meeting.
The trial enrolled 20 patients with low- to intermediate-risk MDS. All patients had anemia resulting in a high transfusion burden, had hemoglobin levels of less than 10 g/dL, and were refractory to ESAs.
Patients received once-weekly asunercept infusions for 12 weeks. Eight of the 20 patients (40%) experienced a reduction in transfusion frequency for 6 months.
Asunercept was considered generally well tolerated, with no grade 3 or higher treatment-related adverse events reported. The most common treatment-emergent adverse events were peripheral edema (n=6), urinary tract infection (n=4), and oral herpes (n=3).
One patient developed acute myeloid leukemia, and 1 patient died from sepsis due to pre-existing neutropenia.
“We are highly encouraged by the data from our clinical phase 1 trial with asunercept in these patients and are currently preparing to initiate a clinical phase 2 proof-of-concept trial to further evaluate the efficacy of asunercept in MDS,” said Harald Fricke, chief medical officer of Apogenix AG, the company developing asunercept.
About orphan designation
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure. ![]()
The European Commission has granted orphan designation to asunercept (APG101) for the treatment of myelodysplastic syndromes (MDS).
Asunercept is a fully human fusion protein that consists of the extracellular domain of the CD95 receptor and the Fc domain of an IgG1 antibody.
Asunercept binds to the CD95 ligand and blocks activation of the CD95 receptor.
Excessive stimulation of the CD95 receptor on hematopoietic precursors inhibits erythropoiesis in MDS patients.
As a result, the patients develop transfusion-dependent anemia that is refractory to erythropoiesis-stimulating agents (ESAs).
Treatment with asunercept, by inhibiting the CD95 system, stimulates the production of red blood cells and decreases transfusion dependency.
Asunercept has been evaluated in a phase 1 trial, the results of which were presented at the 2016 ASH Annual Meeting.
The trial enrolled 20 patients with low- to intermediate-risk MDS. All patients had anemia resulting in a high transfusion burden, had hemoglobin levels of less than 10 g/dL, and were refractory to ESAs.
Patients received once-weekly asunercept infusions for 12 weeks. Eight of the 20 patients (40%) experienced a reduction in transfusion frequency for 6 months.
Asunercept was considered generally well tolerated, with no grade 3 or higher treatment-related adverse events reported. The most common treatment-emergent adverse events were peripheral edema (n=6), urinary tract infection (n=4), and oral herpes (n=3).
One patient developed acute myeloid leukemia, and 1 patient died from sepsis due to pre-existing neutropenia.
“We are highly encouraged by the data from our clinical phase 1 trial with asunercept in these patients and are currently preparing to initiate a clinical phase 2 proof-of-concept trial to further evaluate the efficacy of asunercept in MDS,” said Harald Fricke, chief medical officer of Apogenix AG, the company developing asunercept.
About orphan designation
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure. ![]()
FDA grants drug orphan designation to treat cGVHD

The US Food and Drug Administration (FDA) has granted orphan drug designation to KD025 for the treatment of chronic graft-versus-host disease (cGVHD).
KD025 is a Rho-associated coiled-coil kinase (ROCK) inhibitor being developed by Kadmon Holdings, Inc.
The drug is currently under investigation in a phase 2 trial of adults with steroid-dependent or steroid-refractory cGVHD and active disease.
This dose-finding study has enrolled 48 patients divided into 3 cohorts in which patients receive KD025 at 200 mg once daily, 200 mg twice daily, or 400 mg once daily. The patients were enrolled sequentially following a safety assessment of each cohort.
In July, Kadmon Holdings, Inc. released a preliminary analysis of data from the lowest-dose cohort (n=17, 200 mg once daily).
The overall response rate in this cohort was 71% (12/17). Of responders remaining on KD025 through week 24, 89% (8/9) sustained responses. Sixty-seven percent (8/12) of responders saw an improvement in symptoms, as measured by the Lee cGVHD Symptom Scale score.
In addition to the 12 responders, 3 patients had stable disease and were still on KD025 through week 24. So an overall clinical benefit (response and stable disease) occurred in 88% (15/17) of patients.
Sixty-seven percent (8/12) of responders had a reduction in steroid doses, and 67% (4/6) of responders on tacrolimus had a reduction in tacrolimus doses.
There were no drug-related serious adverse events or drug-related elevations in liver function tests reported.
Kadmon Holdings, Inc. plans to present additional data from this study toward the end of this year.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation to KD025 for the treatment of chronic graft-versus-host disease (cGVHD).
KD025 is a Rho-associated coiled-coil kinase (ROCK) inhibitor being developed by Kadmon Holdings, Inc.
The drug is currently under investigation in a phase 2 trial of adults with steroid-dependent or steroid-refractory cGVHD and active disease.
This dose-finding study has enrolled 48 patients divided into 3 cohorts in which patients receive KD025 at 200 mg once daily, 200 mg twice daily, or 400 mg once daily. The patients were enrolled sequentially following a safety assessment of each cohort.
In July, Kadmon Holdings, Inc. released a preliminary analysis of data from the lowest-dose cohort (n=17, 200 mg once daily).
The overall response rate in this cohort was 71% (12/17). Of responders remaining on KD025 through week 24, 89% (8/9) sustained responses. Sixty-seven percent (8/12) of responders saw an improvement in symptoms, as measured by the Lee cGVHD Symptom Scale score.
In addition to the 12 responders, 3 patients had stable disease and were still on KD025 through week 24. So an overall clinical benefit (response and stable disease) occurred in 88% (15/17) of patients.
Sixty-seven percent (8/12) of responders had a reduction in steroid doses, and 67% (4/6) of responders on tacrolimus had a reduction in tacrolimus doses.
There were no drug-related serious adverse events or drug-related elevations in liver function tests reported.
Kadmon Holdings, Inc. plans to present additional data from this study toward the end of this year.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation to KD025 for the treatment of chronic graft-versus-host disease (cGVHD).
KD025 is a Rho-associated coiled-coil kinase (ROCK) inhibitor being developed by Kadmon Holdings, Inc.
The drug is currently under investigation in a phase 2 trial of adults with steroid-dependent or steroid-refractory cGVHD and active disease.
This dose-finding study has enrolled 48 patients divided into 3 cohorts in which patients receive KD025 at 200 mg once daily, 200 mg twice daily, or 400 mg once daily. The patients were enrolled sequentially following a safety assessment of each cohort.
In July, Kadmon Holdings, Inc. released a preliminary analysis of data from the lowest-dose cohort (n=17, 200 mg once daily).
The overall response rate in this cohort was 71% (12/17). Of responders remaining on KD025 through week 24, 89% (8/9) sustained responses. Sixty-seven percent (8/12) of responders saw an improvement in symptoms, as measured by the Lee cGVHD Symptom Scale score.
In addition to the 12 responders, 3 patients had stable disease and were still on KD025 through week 24. So an overall clinical benefit (response and stable disease) occurred in 88% (15/17) of patients.
Sixty-seven percent (8/12) of responders had a reduction in steroid doses, and 67% (4/6) of responders on tacrolimus had a reduction in tacrolimus doses.
There were no drug-related serious adverse events or drug-related elevations in liver function tests reported.
Kadmon Holdings, Inc. plans to present additional data from this study toward the end of this year.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
Newer blood cancer drugs may not improve OS, QOL

A study of cancer drugs approved by the European Commission from 2009 to 2013 showed that few hematology drugs were known to provide a benefit in overall survival (OS) or quality of life (QOL) over existing treatments.
Of 12 drugs approved for 17 hematology indications, 3 drugs had been shown to provide a benefit in OS (for 3 indications) at the time of approval.
None of the other hematology drugs were known to provide an OS benefit even after a median follow-up of 5.4 years.
Two hematology drugs were shown to provide a benefit in QOL (for 2 indications) after approval, but none of the drugs were known to provide a QOL benefit at the time of approval.
These findings were published in The BMJ alongside a related editorial, feature article, and patient commentary.
All cancer drugs
Researchers analyzed reports on all cancer drug approvals by the European Commission from 2009 to 2013.
There were 48 drugs approved for 68 cancer indications during this period. Fifty-one of the indications were for solid tumor malignancies, and 17 were for hematologic malignancies.
For 24 indications (35%), research had demonstrated a significant improvement in OS at the time of the drugs’ approval. For 3 indications, an improvement in OS was demonstrated after approval.
There was a known improvement in QOL for 7 of the indications (10%) at the time of approval and for 5 indications after approval.
The median follow-up was 5.4 years (range, 3.3 years to 8.1 years).
Overall, there was a significant improvement in OS or QOL during the study period for 51% of the indications (35/68). For the other half (49%, n=33), it wasn’t clear if the drugs provide any benefits in OS or QOL.
All cancer trials
The 68 approvals of cancer drugs were supported by 72 clinical trials.
Sixty approvals (88%) were supported by at least 1 randomized, controlled trial. Eight approvals (12%) were based on a single-arm study. This included 6 of 10 conditional marketing authorizations and 2 of 58 regular marketing authorizations.
Eighteen of the approvals (26%) were supported by a pivotal study powered to evaluate OS as the primary endpoint. And 37 of the approvals (54%) had a supporting pivotal trial evaluating QOL, but results were not reported for 2 of these trials.
Hematology trials and drugs
Of the 12 drugs approved for 17 hematology indications, 4 were regular approvals, 5 were conditional approvals, and 8 had orphan drug designation.
The approvals were supported by data from 18 trials—13 randomized and 5 single-arm trials.
The study drug was compared to an active comparator in 9 of the trials. The drug was evaluated as an add-on treatment in 4 trials. And the drug was not compared to anything in 5 trials (the single-arm trials).
OS was the primary endpoint in 1 of the trials, and 17 trials had OS or QOL as a secondary endpoint.
There were 3 drugs that had demonstrated an OS benefit at the time of approval but no QOL benefit at any time:
- Decitabine used for first-line treatment of acute myeloid leukemia in adults 65 and older who are ineligible for chemotherapy
- Pomalidomide in combination with dexamethasone as third-line therapy for relapsed/refractory multiple myeloma (MM)
- Rituximab plus chemotherapy for first-line treatment of chronic lymphocytic leukemia (CLL).
There were 2 drugs that had demonstrated a QOL benefit, only after approval, but they were not known to provide an OS benefit at any time:
- Nilotinib as a treatment for adults with newly diagnosed, chronic phase, Ph+ chronic myeloid leukemia (CML)
- Ofatumumab for CLL that is refractory to fludarabine and alemtuzumab
For the remaining drugs, there was no evidence of an OS or QOL benefit at any time during the period studied. The drugs included:
- Bortezomib given alone or in combination with doxorubicin or dexamethasone as second-line therapy for MM patients ineligible for hematopoietic stem cell transplant (HSCT)
- Bortezomib plus dexamethasone with or without thalidomide as first-line therapy in MM patients eligible for HSCT
- Bosutinib as second- or third-line treatment of Ph+ CML (any phase)
- Brentuximab vedotin for relapsed or refractory systemic anaplastic large-cell lymphoma
- Brentuximab vedotin for relapsed or refractory, CD30+ Hodgkin lymphoma after autologous HSCT or as third-line treatment for patients ineligible for autologous HSCT
- Dasatinib for first-line treatment of chronic phase, Ph+ CML
- Pixantrone for multiply relapsed or refractory B-cell non-Hodgkin lymphoma
- Ponatinib for patients with Ph+ acute lymphoblastic leukemia who are ineligible for imatinib or have disease that is resistant or intolerant to dasatinib or characterized by T315I mutation
- Ponatinib for patients with any phase of CML who are ineligible for imatinib or have disease that is resistant or intolerant to dasatinib/nilotinib or characterized by T315I mutation
- Rituximab as maintenance after induction for patients with follicular lymphoma
- Rituximab plus chemotherapy for relapsed or refractory CLL
- Temsirolimus for relapsed or refractory mantle cell lymphoma.

A study of cancer drugs approved by the European Commission from 2009 to 2013 showed that few hematology drugs were known to provide a benefit in overall survival (OS) or quality of life (QOL) over existing treatments.
Of 12 drugs approved for 17 hematology indications, 3 drugs had been shown to provide a benefit in OS (for 3 indications) at the time of approval.
None of the other hematology drugs were known to provide an OS benefit even after a median follow-up of 5.4 years.
Two hematology drugs were shown to provide a benefit in QOL (for 2 indications) after approval, but none of the drugs were known to provide a QOL benefit at the time of approval.
These findings were published in The BMJ alongside a related editorial, feature article, and patient commentary.
All cancer drugs
Researchers analyzed reports on all cancer drug approvals by the European Commission from 2009 to 2013.
There were 48 drugs approved for 68 cancer indications during this period. Fifty-one of the indications were for solid tumor malignancies, and 17 were for hematologic malignancies.
For 24 indications (35%), research had demonstrated a significant improvement in OS at the time of the drugs’ approval. For 3 indications, an improvement in OS was demonstrated after approval.
There was a known improvement in QOL for 7 of the indications (10%) at the time of approval and for 5 indications after approval.
The median follow-up was 5.4 years (range, 3.3 years to 8.1 years).
Overall, there was a significant improvement in OS or QOL during the study period for 51% of the indications (35/68). For the other half (49%, n=33), it wasn’t clear if the drugs provide any benefits in OS or QOL.
All cancer trials
The 68 approvals of cancer drugs were supported by 72 clinical trials.
Sixty approvals (88%) were supported by at least 1 randomized, controlled trial. Eight approvals (12%) were based on a single-arm study. This included 6 of 10 conditional marketing authorizations and 2 of 58 regular marketing authorizations.
Eighteen of the approvals (26%) were supported by a pivotal study powered to evaluate OS as the primary endpoint. And 37 of the approvals (54%) had a supporting pivotal trial evaluating QOL, but results were not reported for 2 of these trials.
Hematology trials and drugs
Of the 12 drugs approved for 17 hematology indications, 4 were regular approvals, 5 were conditional approvals, and 8 had orphan drug designation.
The approvals were supported by data from 18 trials—13 randomized and 5 single-arm trials.
The study drug was compared to an active comparator in 9 of the trials. The drug was evaluated as an add-on treatment in 4 trials. And the drug was not compared to anything in 5 trials (the single-arm trials).
OS was the primary endpoint in 1 of the trials, and 17 trials had OS or QOL as a secondary endpoint.
There were 3 drugs that had demonstrated an OS benefit at the time of approval but no QOL benefit at any time:
- Decitabine used for first-line treatment of acute myeloid leukemia in adults 65 and older who are ineligible for chemotherapy
- Pomalidomide in combination with dexamethasone as third-line therapy for relapsed/refractory multiple myeloma (MM)
- Rituximab plus chemotherapy for first-line treatment of chronic lymphocytic leukemia (CLL).
There were 2 drugs that had demonstrated a QOL benefit, only after approval, but they were not known to provide an OS benefit at any time:
- Nilotinib as a treatment for adults with newly diagnosed, chronic phase, Ph+ chronic myeloid leukemia (CML)
- Ofatumumab for CLL that is refractory to fludarabine and alemtuzumab
For the remaining drugs, there was no evidence of an OS or QOL benefit at any time during the period studied. The drugs included:
- Bortezomib given alone or in combination with doxorubicin or dexamethasone as second-line therapy for MM patients ineligible for hematopoietic stem cell transplant (HSCT)
- Bortezomib plus dexamethasone with or without thalidomide as first-line therapy in MM patients eligible for HSCT
- Bosutinib as second- or third-line treatment of Ph+ CML (any phase)
- Brentuximab vedotin for relapsed or refractory systemic anaplastic large-cell lymphoma
- Brentuximab vedotin for relapsed or refractory, CD30+ Hodgkin lymphoma after autologous HSCT or as third-line treatment for patients ineligible for autologous HSCT
- Dasatinib for first-line treatment of chronic phase, Ph+ CML
- Pixantrone for multiply relapsed or refractory B-cell non-Hodgkin lymphoma
- Ponatinib for patients with Ph+ acute lymphoblastic leukemia who are ineligible for imatinib or have disease that is resistant or intolerant to dasatinib or characterized by T315I mutation
- Ponatinib for patients with any phase of CML who are ineligible for imatinib or have disease that is resistant or intolerant to dasatinib/nilotinib or characterized by T315I mutation
- Rituximab as maintenance after induction for patients with follicular lymphoma
- Rituximab plus chemotherapy for relapsed or refractory CLL
- Temsirolimus for relapsed or refractory mantle cell lymphoma.
A study of cancer drugs approved by the European Commission from 2009 to 2013 showed that few hematology drugs were known to provide a benefit in overall survival (OS) or quality of life (QOL) over existing treatments.
Of 12 drugs approved for 17 hematology indications, 3 drugs had been shown to provide a benefit in OS (for 3 indications) at the time of approval.
None of the other hematology drugs were known to provide an OS benefit even after a median follow-up of 5.4 years.
Two hematology drugs were shown to provide a benefit in QOL (for 2 indications) after approval, but none of the drugs were known to provide a QOL benefit at the time of approval.
These findings were published in The BMJ alongside a related editorial, feature article, and patient commentary.
All cancer drugs
Researchers analyzed reports on all cancer drug approvals by the European Commission from 2009 to 2013.
There were 48 drugs approved for 68 cancer indications during this period. Fifty-one of the indications were for solid tumor malignancies, and 17 were for hematologic malignancies.
For 24 indications (35%), research had demonstrated a significant improvement in OS at the time of the drugs’ approval. For 3 indications, an improvement in OS was demonstrated after approval.
There was a known improvement in QOL for 7 of the indications (10%) at the time of approval and for 5 indications after approval.
The median follow-up was 5.4 years (range, 3.3 years to 8.1 years).
Overall, there was a significant improvement in OS or QOL during the study period for 51% of the indications (35/68). For the other half (49%, n=33), it wasn’t clear if the drugs provide any benefits in OS or QOL.
All cancer trials
The 68 approvals of cancer drugs were supported by 72 clinical trials.
Sixty approvals (88%) were supported by at least 1 randomized, controlled trial. Eight approvals (12%) were based on a single-arm study. This included 6 of 10 conditional marketing authorizations and 2 of 58 regular marketing authorizations.
Eighteen of the approvals (26%) were supported by a pivotal study powered to evaluate OS as the primary endpoint. And 37 of the approvals (54%) had a supporting pivotal trial evaluating QOL, but results were not reported for 2 of these trials.
Hematology trials and drugs
Of the 12 drugs approved for 17 hematology indications, 4 were regular approvals, 5 were conditional approvals, and 8 had orphan drug designation.
The approvals were supported by data from 18 trials—13 randomized and 5 single-arm trials.
The study drug was compared to an active comparator in 9 of the trials. The drug was evaluated as an add-on treatment in 4 trials. And the drug was not compared to anything in 5 trials (the single-arm trials).
OS was the primary endpoint in 1 of the trials, and 17 trials had OS or QOL as a secondary endpoint.
There were 3 drugs that had demonstrated an OS benefit at the time of approval but no QOL benefit at any time:
- Decitabine used for first-line treatment of acute myeloid leukemia in adults 65 and older who are ineligible for chemotherapy
- Pomalidomide in combination with dexamethasone as third-line therapy for relapsed/refractory multiple myeloma (MM)
- Rituximab plus chemotherapy for first-line treatment of chronic lymphocytic leukemia (CLL).
There were 2 drugs that had demonstrated a QOL benefit, only after approval, but they were not known to provide an OS benefit at any time:
- Nilotinib as a treatment for adults with newly diagnosed, chronic phase, Ph+ chronic myeloid leukemia (CML)
- Ofatumumab for CLL that is refractory to fludarabine and alemtuzumab
For the remaining drugs, there was no evidence of an OS or QOL benefit at any time during the period studied. The drugs included:
- Bortezomib given alone or in combination with doxorubicin or dexamethasone as second-line therapy for MM patients ineligible for hematopoietic stem cell transplant (HSCT)
- Bortezomib plus dexamethasone with or without thalidomide as first-line therapy in MM patients eligible for HSCT
- Bosutinib as second- or third-line treatment of Ph+ CML (any phase)
- Brentuximab vedotin for relapsed or refractory systemic anaplastic large-cell lymphoma
- Brentuximab vedotin for relapsed or refractory, CD30+ Hodgkin lymphoma after autologous HSCT or as third-line treatment for patients ineligible for autologous HSCT
- Dasatinib for first-line treatment of chronic phase, Ph+ CML
- Pixantrone for multiply relapsed or refractory B-cell non-Hodgkin lymphoma
- Ponatinib for patients with Ph+ acute lymphoblastic leukemia who are ineligible for imatinib or have disease that is resistant or intolerant to dasatinib or characterized by T315I mutation
- Ponatinib for patients with any phase of CML who are ineligible for imatinib or have disease that is resistant or intolerant to dasatinib/nilotinib or characterized by T315I mutation
- Rituximab as maintenance after induction for patients with follicular lymphoma
- Rituximab plus chemotherapy for relapsed or refractory CLL
- Temsirolimus for relapsed or refractory mantle cell lymphoma.
FDA approves first test for detecting Zika in blood donations
The US Food and Drug Administration (FDA) has approved the first test designed to screen blood donations for Zika virus.
The cobas Zika test is a qualitative nucleic acid test that can detect Zika virus RNA in individual plasma specimens obtained from donors of whole blood and blood components and from living organ donors.
The test is not intended for the individual diagnosis of Zika virus infection.
The cobas Zika test is intended for use on the fully automated cobas 6800 and cobas 8800 systems. These systems and the test are manufactured by Roche Molecular Systems, Inc.
“Today’s action represents the first approval of a Zika virus detection test for use with screening the nation’s blood supply,” said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research.
“Screening blood donations for the Zika virus is critical to preventing infected donations from entering the US blood supply. Today’s approval is the result of a commitment by the manufacturer to work rapidly and collaboratively with the FDA and the blood collection industry to respond to a public health crisis and ensure the safety of blood in the US and its territories.”
In August 2016, the FDA issued a guidance document recommending that all states and territories screen individual units of whole blood and blood components with an investigational blood screening test available under an investigational new drug (IND) application, or use an approved test when available.
Several blood collection establishments have used the cobas Zika test under an IND. The data collected from this testing and additional studies performed by the manufacturer demonstrated that the test is effective in screening blood donors for Zika virus infection, according to the FDA.
The test’s clinical specificity was evaluated by testing individual samples from blood donations at 5 external laboratory sites, and the specificity exceeded 99%. ![]()
The US Food and Drug Administration (FDA) has approved the first test designed to screen blood donations for Zika virus.
The cobas Zika test is a qualitative nucleic acid test that can detect Zika virus RNA in individual plasma specimens obtained from donors of whole blood and blood components and from living organ donors.
The test is not intended for the individual diagnosis of Zika virus infection.
The cobas Zika test is intended for use on the fully automated cobas 6800 and cobas 8800 systems. These systems and the test are manufactured by Roche Molecular Systems, Inc.
“Today’s action represents the first approval of a Zika virus detection test for use with screening the nation’s blood supply,” said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research.
“Screening blood donations for the Zika virus is critical to preventing infected donations from entering the US blood supply. Today’s approval is the result of a commitment by the manufacturer to work rapidly and collaboratively with the FDA and the blood collection industry to respond to a public health crisis and ensure the safety of blood in the US and its territories.”
In August 2016, the FDA issued a guidance document recommending that all states and territories screen individual units of whole blood and blood components with an investigational blood screening test available under an investigational new drug (IND) application, or use an approved test when available.
Several blood collection establishments have used the cobas Zika test under an IND. The data collected from this testing and additional studies performed by the manufacturer demonstrated that the test is effective in screening blood donors for Zika virus infection, according to the FDA.
The test’s clinical specificity was evaluated by testing individual samples from blood donations at 5 external laboratory sites, and the specificity exceeded 99%. ![]()
The US Food and Drug Administration (FDA) has approved the first test designed to screen blood donations for Zika virus.
The cobas Zika test is a qualitative nucleic acid test that can detect Zika virus RNA in individual plasma specimens obtained from donors of whole blood and blood components and from living organ donors.
The test is not intended for the individual diagnosis of Zika virus infection.
The cobas Zika test is intended for use on the fully automated cobas 6800 and cobas 8800 systems. These systems and the test are manufactured by Roche Molecular Systems, Inc.
“Today’s action represents the first approval of a Zika virus detection test for use with screening the nation’s blood supply,” said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research.
“Screening blood donations for the Zika virus is critical to preventing infected donations from entering the US blood supply. Today’s approval is the result of a commitment by the manufacturer to work rapidly and collaboratively with the FDA and the blood collection industry to respond to a public health crisis and ensure the safety of blood in the US and its territories.”
In August 2016, the FDA issued a guidance document recommending that all states and territories screen individual units of whole blood and blood components with an investigational blood screening test available under an investigational new drug (IND) application, or use an approved test when available.
Several blood collection establishments have used the cobas Zika test under an IND. The data collected from this testing and additional studies performed by the manufacturer demonstrated that the test is effective in screening blood donors for Zika virus infection, according to the FDA.
The test’s clinical specificity was evaluated by testing individual samples from blood donations at 5 external laboratory sites, and the specificity exceeded 99%. ![]()
Sperm banking may be underused by young cancer patients

New research suggests sperm banking may be underutilized by adolescent and young adult males with cancer who are at risk of infertility.
However, the study also showed that patients were more likely to attempt sperm banking if they were physically mature, met with fertility specialists, or their parents recommended sperm banking.
These findings were published in the Journal of Clinical Oncology.
“Research has found that the majority of males who survive childhood cancer desire biological children,” said study author James Klosky, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“Fertility preservation is also associated with a variety of benefits for survivors, including increased optimism about the future. While sperm banking is not for everyone, it is an effective method for preserving male fertility. Yet this study shows that sperm banking remains underutilized by at-risk patients with cancer.”
Dr Klosky and his colleagues surveyed 146 young males with cancer who were at risk of infertility. The researchers also surveyed 144 parents or guardians and 52 oncologists and other healthcare providers.
The patients’ mean age was 16.49 (range, 13.0-21.99). Diagnoses included leukemia and lymphoma (56.2%), solid tumor malignancies (37.7%), and brain tumors (6.2%).
Slightly more than half of the patients (53.4%, n=78) attempted sperm banking prior to starting treatment. Sixty-two, or 82.1%, of those who attempted sperm banking were successful.
In all, 43.8% of the patients successfully banked sperm.
Of the 68 patients who did not attempt sperm banking, 29 reported discussing the option with their families but deciding against it. Twenty-six patients indicated they did not believe sperm banking was necessary, and 9 patients were unsure what it was.
There were several factors that influenced the likelihood of patients making sperm collection attempts as well as successfully banking sperm.
In a multivariable analysis, the following factors were associated with an increased likelihood of attempting to bank sperm:
- Meeting with a fertility specialist (odds ratio[OR]=29.96; 95% CI, 2.48 to 361.41; P=0.007)
- Parent recommending banking (OR=12.30; 95% CI, 2.01 to 75.94; P=0.007)
- Higher Tanner stage (OR=5.42; 95% CI, 1.75 to 16.78; P=0.003).
In another multivariable analysis, successful sperm banking was associated with:
- Patient history of masturbation (OR=5.99; 95% CI, 1.25 to 28.50; P=0.025)
- Higher self-efficacy for banking coordination (OR=1.23; 95% CI, 1.05 to 1.45; P=0.012)
- Medical team member recommending banking (OR=4.26; 95% CI, 1.45 to 12.43; P=0.008)
- Parent recommending banking (OR=4.62; 95% CI, 1.46 to 14.73; P=0.010).
“These results highlight factors that providers can target to empower adolescents to actively participate in their own healthcare,” Dr Klosky said. “These decisions, which are typically made at the time of diagnosis, have high potential to affect their lives as survivors.” ![]()
New research suggests sperm banking may be underutilized by adolescent and young adult males with cancer who are at risk of infertility.
However, the study also showed that patients were more likely to attempt sperm banking if they were physically mature, met with fertility specialists, or their parents recommended sperm banking.
These findings were published in the Journal of Clinical Oncology.
“Research has found that the majority of males who survive childhood cancer desire biological children,” said study author James Klosky, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“Fertility preservation is also associated with a variety of benefits for survivors, including increased optimism about the future. While sperm banking is not for everyone, it is an effective method for preserving male fertility. Yet this study shows that sperm banking remains underutilized by at-risk patients with cancer.”
Dr Klosky and his colleagues surveyed 146 young males with cancer who were at risk of infertility. The researchers also surveyed 144 parents or guardians and 52 oncologists and other healthcare providers.
The patients’ mean age was 16.49 (range, 13.0-21.99). Diagnoses included leukemia and lymphoma (56.2%), solid tumor malignancies (37.7%), and brain tumors (6.2%).
Slightly more than half of the patients (53.4%, n=78) attempted sperm banking prior to starting treatment. Sixty-two, or 82.1%, of those who attempted sperm banking were successful.
In all, 43.8% of the patients successfully banked sperm.
Of the 68 patients who did not attempt sperm banking, 29 reported discussing the option with their families but deciding against it. Twenty-six patients indicated they did not believe sperm banking was necessary, and 9 patients were unsure what it was.
There were several factors that influenced the likelihood of patients making sperm collection attempts as well as successfully banking sperm.
In a multivariable analysis, the following factors were associated with an increased likelihood of attempting to bank sperm:
- Meeting with a fertility specialist (odds ratio[OR]=29.96; 95% CI, 2.48 to 361.41; P=0.007)
- Parent recommending banking (OR=12.30; 95% CI, 2.01 to 75.94; P=0.007)
- Higher Tanner stage (OR=5.42; 95% CI, 1.75 to 16.78; P=0.003).
In another multivariable analysis, successful sperm banking was associated with:
- Patient history of masturbation (OR=5.99; 95% CI, 1.25 to 28.50; P=0.025)
- Higher self-efficacy for banking coordination (OR=1.23; 95% CI, 1.05 to 1.45; P=0.012)
- Medical team member recommending banking (OR=4.26; 95% CI, 1.45 to 12.43; P=0.008)
- Parent recommending banking (OR=4.62; 95% CI, 1.46 to 14.73; P=0.010).
“These results highlight factors that providers can target to empower adolescents to actively participate in their own healthcare,” Dr Klosky said. “These decisions, which are typically made at the time of diagnosis, have high potential to affect their lives as survivors.” ![]()
New research suggests sperm banking may be underutilized by adolescent and young adult males with cancer who are at risk of infertility.
However, the study also showed that patients were more likely to attempt sperm banking if they were physically mature, met with fertility specialists, or their parents recommended sperm banking.
These findings were published in the Journal of Clinical Oncology.
“Research has found that the majority of males who survive childhood cancer desire biological children,” said study author James Klosky, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“Fertility preservation is also associated with a variety of benefits for survivors, including increased optimism about the future. While sperm banking is not for everyone, it is an effective method for preserving male fertility. Yet this study shows that sperm banking remains underutilized by at-risk patients with cancer.”
Dr Klosky and his colleagues surveyed 146 young males with cancer who were at risk of infertility. The researchers also surveyed 144 parents or guardians and 52 oncologists and other healthcare providers.
The patients’ mean age was 16.49 (range, 13.0-21.99). Diagnoses included leukemia and lymphoma (56.2%), solid tumor malignancies (37.7%), and brain tumors (6.2%).
Slightly more than half of the patients (53.4%, n=78) attempted sperm banking prior to starting treatment. Sixty-two, or 82.1%, of those who attempted sperm banking were successful.
In all, 43.8% of the patients successfully banked sperm.
Of the 68 patients who did not attempt sperm banking, 29 reported discussing the option with their families but deciding against it. Twenty-six patients indicated they did not believe sperm banking was necessary, and 9 patients were unsure what it was.
There were several factors that influenced the likelihood of patients making sperm collection attempts as well as successfully banking sperm.
In a multivariable analysis, the following factors were associated with an increased likelihood of attempting to bank sperm:
- Meeting with a fertility specialist (odds ratio[OR]=29.96; 95% CI, 2.48 to 361.41; P=0.007)
- Parent recommending banking (OR=12.30; 95% CI, 2.01 to 75.94; P=0.007)
- Higher Tanner stage (OR=5.42; 95% CI, 1.75 to 16.78; P=0.003).
In another multivariable analysis, successful sperm banking was associated with:
- Patient history of masturbation (OR=5.99; 95% CI, 1.25 to 28.50; P=0.025)
- Higher self-efficacy for banking coordination (OR=1.23; 95% CI, 1.05 to 1.45; P=0.012)
- Medical team member recommending banking (OR=4.26; 95% CI, 1.45 to 12.43; P=0.008)
- Parent recommending banking (OR=4.62; 95% CI, 1.46 to 14.73; P=0.010).
“These results highlight factors that providers can target to empower adolescents to actively participate in their own healthcare,” Dr Klosky said. “These decisions, which are typically made at the time of diagnosis, have high potential to affect their lives as survivors.” ![]()
Some cancers linked to weight are on the rise in the US
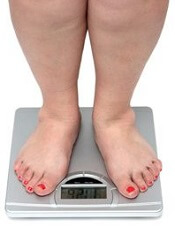
Cancers associated with being overweight or obese accounted for about 40% of all cancers diagnosed in the US in 2014, according to the latest Vital Signs report by the US Centers for Disease Control and Prevention.
The International Agency for Research on Cancer has identified 13 cancers associated with overweight and obesity—multiple myeloma (MM), meningioma, adenocarcinoma of the esophagus, and thyroid, postmenopausal breast, gallbladder, stomach, liver, pancreatic, kidney, ovarian, uterine, and colorectal cancers.
For the Vital Signs report, researchers reviewed US data from 2005 to 2014 to determine trends for cancers associated with being overweight (having a body mass index [BMI] of 25 to 29.9 kg/m2) or obese (having a BMI of 30 kg/m2 and higher).
In 2014, roughly 631,000 people were diagnosed with cancers associated with overweight and obesity, which represents 40% of all cancers diagnosed.
Fifty-five percent of all cancers diagnosed in women and 24% of those diagnosed in men were associated with overweight and obesity.
Incidence rates of the 13 cancers combined were highest in non-Hispanic blacks, followed by non-Hispanic whites, American Indians/Alaska Natives, Hispanics, and Asians/Pacific Islanders.
Incidence over time
Overall, the incidence of cancers associated with overweight and obesity decreased 2% from 2005 to 2014.
However, when colorectal cancer was excluded, the incidence of the other 12 cancers combined increased 7% from 2005 to 2014. The incidence of colorectal cancer decreased 23% during that time. Researchers said this was due, in large part, to screening.
The incidence of cancers not associated with overweight and obesity decreased 13% from 2005 to 2014.
The incidence of MM increased over the period studied, but it was not a significant increase. The incidence rate of MM was 5.6 per 100,000 persons (age-adjusted to the 2000 US standard population) in 2005 and 6.0 per 100,000 persons in 2014.
So overall, there was an 8% increase in MM incidence rate from 2005 to 2014, or a 1.1% average annual increase. There was a 2% increase in the risk of MM per 1 kg/m2 increase in BMI.
Like MM, 3 other cancers had fairly stable incidence rates over the study period—adenocarcinoma of the esophagus, gallbladder cancer, and postmenopausal breast cancer.
However, incidence rates increased significantly each year for thyroid cancer (4.0% per year), liver cancer (2.9%), gastric cardia cancer (1.2%), endometrial cancer (1.1%), pancreatic cancer (0.8%), and kidney cancer (0.7%).
And incidence rates decreased significantly each year for meningioma (-3.8%), colorectal cancer (-2.9%), and ovarian cancer (-2.0%). ![]()
Cancers associated with being overweight or obese accounted for about 40% of all cancers diagnosed in the US in 2014, according to the latest Vital Signs report by the US Centers for Disease Control and Prevention.
The International Agency for Research on Cancer has identified 13 cancers associated with overweight and obesity—multiple myeloma (MM), meningioma, adenocarcinoma of the esophagus, and thyroid, postmenopausal breast, gallbladder, stomach, liver, pancreatic, kidney, ovarian, uterine, and colorectal cancers.
For the Vital Signs report, researchers reviewed US data from 2005 to 2014 to determine trends for cancers associated with being overweight (having a body mass index [BMI] of 25 to 29.9 kg/m2) or obese (having a BMI of 30 kg/m2 and higher).
In 2014, roughly 631,000 people were diagnosed with cancers associated with overweight and obesity, which represents 40% of all cancers diagnosed.
Fifty-five percent of all cancers diagnosed in women and 24% of those diagnosed in men were associated with overweight and obesity.
Incidence rates of the 13 cancers combined were highest in non-Hispanic blacks, followed by non-Hispanic whites, American Indians/Alaska Natives, Hispanics, and Asians/Pacific Islanders.
Incidence over time
Overall, the incidence of cancers associated with overweight and obesity decreased 2% from 2005 to 2014.
However, when colorectal cancer was excluded, the incidence of the other 12 cancers combined increased 7% from 2005 to 2014. The incidence of colorectal cancer decreased 23% during that time. Researchers said this was due, in large part, to screening.
The incidence of cancers not associated with overweight and obesity decreased 13% from 2005 to 2014.
The incidence of MM increased over the period studied, but it was not a significant increase. The incidence rate of MM was 5.6 per 100,000 persons (age-adjusted to the 2000 US standard population) in 2005 and 6.0 per 100,000 persons in 2014.
So overall, there was an 8% increase in MM incidence rate from 2005 to 2014, or a 1.1% average annual increase. There was a 2% increase in the risk of MM per 1 kg/m2 increase in BMI.
Like MM, 3 other cancers had fairly stable incidence rates over the study period—adenocarcinoma of the esophagus, gallbladder cancer, and postmenopausal breast cancer.
However, incidence rates increased significantly each year for thyroid cancer (4.0% per year), liver cancer (2.9%), gastric cardia cancer (1.2%), endometrial cancer (1.1%), pancreatic cancer (0.8%), and kidney cancer (0.7%).
And incidence rates decreased significantly each year for meningioma (-3.8%), colorectal cancer (-2.9%), and ovarian cancer (-2.0%). ![]()
Cancers associated with being overweight or obese accounted for about 40% of all cancers diagnosed in the US in 2014, according to the latest Vital Signs report by the US Centers for Disease Control and Prevention.
The International Agency for Research on Cancer has identified 13 cancers associated with overweight and obesity—multiple myeloma (MM), meningioma, adenocarcinoma of the esophagus, and thyroid, postmenopausal breast, gallbladder, stomach, liver, pancreatic, kidney, ovarian, uterine, and colorectal cancers.
For the Vital Signs report, researchers reviewed US data from 2005 to 2014 to determine trends for cancers associated with being overweight (having a body mass index [BMI] of 25 to 29.9 kg/m2) or obese (having a BMI of 30 kg/m2 and higher).
In 2014, roughly 631,000 people were diagnosed with cancers associated with overweight and obesity, which represents 40% of all cancers diagnosed.
Fifty-five percent of all cancers diagnosed in women and 24% of those diagnosed in men were associated with overweight and obesity.
Incidence rates of the 13 cancers combined were highest in non-Hispanic blacks, followed by non-Hispanic whites, American Indians/Alaska Natives, Hispanics, and Asians/Pacific Islanders.
Incidence over time
Overall, the incidence of cancers associated with overweight and obesity decreased 2% from 2005 to 2014.
However, when colorectal cancer was excluded, the incidence of the other 12 cancers combined increased 7% from 2005 to 2014. The incidence of colorectal cancer decreased 23% during that time. Researchers said this was due, in large part, to screening.
The incidence of cancers not associated with overweight and obesity decreased 13% from 2005 to 2014.
The incidence of MM increased over the period studied, but it was not a significant increase. The incidence rate of MM was 5.6 per 100,000 persons (age-adjusted to the 2000 US standard population) in 2005 and 6.0 per 100,000 persons in 2014.
So overall, there was an 8% increase in MM incidence rate from 2005 to 2014, or a 1.1% average annual increase. There was a 2% increase in the risk of MM per 1 kg/m2 increase in BMI.
Like MM, 3 other cancers had fairly stable incidence rates over the study period—adenocarcinoma of the esophagus, gallbladder cancer, and postmenopausal breast cancer.
However, incidence rates increased significantly each year for thyroid cancer (4.0% per year), liver cancer (2.9%), gastric cardia cancer (1.2%), endometrial cancer (1.1%), pancreatic cancer (0.8%), and kidney cancer (0.7%).
And incidence rates decreased significantly each year for meningioma (-3.8%), colorectal cancer (-2.9%), and ovarian cancer (-2.0%).
Device could improve anemia detection
A new microfluidic device could improve testing for anemia, according to researchers.
The team said the device can detect the level of hemoglobin in a whole blood sample using optical absorbance.
The device is portable, requires only a few drops of blood for analysis, and eliminates the need for chemical preparations.
In addition, researchers believe the device could be integrated with other microfluidic approaches to blood analysis.
The researchers described their device in AIP Advances.
The team noted that blood analyzers currently on the market measure hemoglobin via hemolysis. This requires hands-on expertise to prepare and run a sample, limiting the ability to monitor anemia in many parts of the world.
“The most exciting aspect to this analyzer is that it uses whole blood and does not require the additional steps and reagents to prepare a sample,” said study author Nathan Sniadecki, PhD, of the University of Washington in Seattle.
“You just run blood into the channel, and that’s it,” added Nikita Taparia, a doctoral candidate in Sniadecki’s lab. “It can be used anywhere.”
The analyzer takes advantage of the optical properties of blood, such as absorption and scattering, to measure hemoglobin concentration. Anemic blood transmits more light than normal blood, so the severity of anemia can be measured as a ratio of transmitted to original light intensity.
To simulate anemia, the researchers diluted blood samples with a buffer solution. The blood analyzer was effective at predicting cases of moderate to severe anemia, defined as less than 10 g/dL of hemoglobin in a sample. The analyzer did not produce any false-negative results.
The optical density of samples did not increase linearly, so a higher concentration of hemoglobin defines the upper limit of detection for the device.
The researchers said the device could be integrated with other microfluidic devices to analyze whole blood samples in parallel to diagnose anemia and other underlying factors that could contribute to the condition.
The team said such an integrated diagnostic tool would “aid the global health community in their continued surveillance of anemia and its etiology in high-risk subpopulations.”
A new microfluidic device could improve testing for anemia, according to researchers.
The team said the device can detect the level of hemoglobin in a whole blood sample using optical absorbance.
The device is portable, requires only a few drops of blood for analysis, and eliminates the need for chemical preparations.
In addition, researchers believe the device could be integrated with other microfluidic approaches to blood analysis.
The researchers described their device in AIP Advances.
The team noted that blood analyzers currently on the market measure hemoglobin via hemolysis. This requires hands-on expertise to prepare and run a sample, limiting the ability to monitor anemia in many parts of the world.
“The most exciting aspect to this analyzer is that it uses whole blood and does not require the additional steps and reagents to prepare a sample,” said study author Nathan Sniadecki, PhD, of the University of Washington in Seattle.
“You just run blood into the channel, and that’s it,” added Nikita Taparia, a doctoral candidate in Sniadecki’s lab. “It can be used anywhere.”
The analyzer takes advantage of the optical properties of blood, such as absorption and scattering, to measure hemoglobin concentration. Anemic blood transmits more light than normal blood, so the severity of anemia can be measured as a ratio of transmitted to original light intensity.
To simulate anemia, the researchers diluted blood samples with a buffer solution. The blood analyzer was effective at predicting cases of moderate to severe anemia, defined as less than 10 g/dL of hemoglobin in a sample. The analyzer did not produce any false-negative results.
The optical density of samples did not increase linearly, so a higher concentration of hemoglobin defines the upper limit of detection for the device.
The researchers said the device could be integrated with other microfluidic devices to analyze whole blood samples in parallel to diagnose anemia and other underlying factors that could contribute to the condition.
The team said such an integrated diagnostic tool would “aid the global health community in their continued surveillance of anemia and its etiology in high-risk subpopulations.”
A new microfluidic device could improve testing for anemia, according to researchers.
The team said the device can detect the level of hemoglobin in a whole blood sample using optical absorbance.
The device is portable, requires only a few drops of blood for analysis, and eliminates the need for chemical preparations.
In addition, researchers believe the device could be integrated with other microfluidic approaches to blood analysis.
The researchers described their device in AIP Advances.
The team noted that blood analyzers currently on the market measure hemoglobin via hemolysis. This requires hands-on expertise to prepare and run a sample, limiting the ability to monitor anemia in many parts of the world.
“The most exciting aspect to this analyzer is that it uses whole blood and does not require the additional steps and reagents to prepare a sample,” said study author Nathan Sniadecki, PhD, of the University of Washington in Seattle.
“You just run blood into the channel, and that’s it,” added Nikita Taparia, a doctoral candidate in Sniadecki’s lab. “It can be used anywhere.”
The analyzer takes advantage of the optical properties of blood, such as absorption and scattering, to measure hemoglobin concentration. Anemic blood transmits more light than normal blood, so the severity of anemia can be measured as a ratio of transmitted to original light intensity.
To simulate anemia, the researchers diluted blood samples with a buffer solution. The blood analyzer was effective at predicting cases of moderate to severe anemia, defined as less than 10 g/dL of hemoglobin in a sample. The analyzer did not produce any false-negative results.
The optical density of samples did not increase linearly, so a higher concentration of hemoglobin defines the upper limit of detection for the device.
The researchers said the device could be integrated with other microfluidic devices to analyze whole blood samples in parallel to diagnose anemia and other underlying factors that could contribute to the condition.
The team said such an integrated diagnostic tool would “aid the global health community in their continued surveillance of anemia and its etiology in high-risk subpopulations.”
Researchers win Nobel Prize for developing cryo-EM
Three researchers have received the Nobel Prize in Chemistry 2017 for the development of cryo-electron microscopy (EM), which has simplified and improved the imaging of biomolecules.
Cryo-EM is a method used to image frozen biological molecules without the use of structure-altering dyes or fixatives or the need to coax the molecules into crystalline form.
This provides a simpler way to generate images of molecules in their normal states and greater understanding of biological function. It also aids the development of pharmaceuticals.
For developing cryo-EM, this year’s Nobel Prize in Chemistry* was awarded to:
- Jacques Dubochet, PhD, of University of Lausanne in Switzerland
- Joachim Frank, PhD, of Columbia University in New York, New York
- Richard Henderson, PhD, of MRC Laboratory of Molecular Biology in Cambridge, UK.
About the work
Electron microscopes were long believed to be suitable only for imaging dead matter because the electron beam destroys biological material.
However, in 1990, Dr Henderson succeeded in using an electron microscope to generate a 3-dimensional image of a protein at atomic resolution. This breakthrough proved the technology’s potential.
Dr Frank made the technology generally applicable. Between 1975 and 1986, he developed an image processing method in which the electron microscope’s fuzzy, 2-dimensional images are analyzed and merged to reveal a sharp, 3-dimensional structure.
Dr Dubochet added water to the mix. Liquid water evaporates in the electron microscope’s vacuum, which makes the biomolecules collapse.
In the early 1980s, Dr Dubochet succeeded in vitrifying water. He cooled water so rapidly that it solidified in its liquid form around a biological sample, allowing the biomolecules to retain their natural shape even in a vacuum.
Following these discoveries, the electron microscope’s every nut and bolt have been optimized. The desired atomic resolution was reached in 2013, and researchers can now routinely produce 3-dimensional structures of biomolecules.
In the past few years, the scientific literature has been filled with images of everything from proteins that cause antibiotic resistance to the surface of the Zika virus.
*The prize amount is 9 million Swedish krona to be shared equally among the Laureates.
Three researchers have received the Nobel Prize in Chemistry 2017 for the development of cryo-electron microscopy (EM), which has simplified and improved the imaging of biomolecules.
Cryo-EM is a method used to image frozen biological molecules without the use of structure-altering dyes or fixatives or the need to coax the molecules into crystalline form.
This provides a simpler way to generate images of molecules in their normal states and greater understanding of biological function. It also aids the development of pharmaceuticals.
For developing cryo-EM, this year’s Nobel Prize in Chemistry* was awarded to:
- Jacques Dubochet, PhD, of University of Lausanne in Switzerland
- Joachim Frank, PhD, of Columbia University in New York, New York
- Richard Henderson, PhD, of MRC Laboratory of Molecular Biology in Cambridge, UK.
About the work
Electron microscopes were long believed to be suitable only for imaging dead matter because the electron beam destroys biological material.
However, in 1990, Dr Henderson succeeded in using an electron microscope to generate a 3-dimensional image of a protein at atomic resolution. This breakthrough proved the technology’s potential.
Dr Frank made the technology generally applicable. Between 1975 and 1986, he developed an image processing method in which the electron microscope’s fuzzy, 2-dimensional images are analyzed and merged to reveal a sharp, 3-dimensional structure.
Dr Dubochet added water to the mix. Liquid water evaporates in the electron microscope’s vacuum, which makes the biomolecules collapse.
In the early 1980s, Dr Dubochet succeeded in vitrifying water. He cooled water so rapidly that it solidified in its liquid form around a biological sample, allowing the biomolecules to retain their natural shape even in a vacuum.
Following these discoveries, the electron microscope’s every nut and bolt have been optimized. The desired atomic resolution was reached in 2013, and researchers can now routinely produce 3-dimensional structures of biomolecules.
In the past few years, the scientific literature has been filled with images of everything from proteins that cause antibiotic resistance to the surface of the Zika virus.
*The prize amount is 9 million Swedish krona to be shared equally among the Laureates.
Three researchers have received the Nobel Prize in Chemistry 2017 for the development of cryo-electron microscopy (EM), which has simplified and improved the imaging of biomolecules.
Cryo-EM is a method used to image frozen biological molecules without the use of structure-altering dyes or fixatives or the need to coax the molecules into crystalline form.
This provides a simpler way to generate images of molecules in their normal states and greater understanding of biological function. It also aids the development of pharmaceuticals.
For developing cryo-EM, this year’s Nobel Prize in Chemistry* was awarded to:
- Jacques Dubochet, PhD, of University of Lausanne in Switzerland
- Joachim Frank, PhD, of Columbia University in New York, New York
- Richard Henderson, PhD, of MRC Laboratory of Molecular Biology in Cambridge, UK.
About the work
Electron microscopes were long believed to be suitable only for imaging dead matter because the electron beam destroys biological material.
However, in 1990, Dr Henderson succeeded in using an electron microscope to generate a 3-dimensional image of a protein at atomic resolution. This breakthrough proved the technology’s potential.
Dr Frank made the technology generally applicable. Between 1975 and 1986, he developed an image processing method in which the electron microscope’s fuzzy, 2-dimensional images are analyzed and merged to reveal a sharp, 3-dimensional structure.
Dr Dubochet added water to the mix. Liquid water evaporates in the electron microscope’s vacuum, which makes the biomolecules collapse.
In the early 1980s, Dr Dubochet succeeded in vitrifying water. He cooled water so rapidly that it solidified in its liquid form around a biological sample, allowing the biomolecules to retain their natural shape even in a vacuum.
Following these discoveries, the electron microscope’s every nut and bolt have been optimized. The desired atomic resolution was reached in 2013, and researchers can now routinely produce 3-dimensional structures of biomolecules.
In the past few years, the scientific literature has been filled with images of everything from proteins that cause antibiotic resistance to the surface of the Zika virus.
*The prize amount is 9 million Swedish krona to be shared equally among the Laureates.
Drugs may increase risk of bleeding with NOACs

Concurrent use of non-vitamin K oral anticoagulants (NOACs) and drugs that share metabolic pathways with NOACs may affect the risk of major bleeding in patients with nonvalvular atrial fibrillation (NVAF), according to a study published in JAMA.
Researchers studied more than 91,000 Taiwanese patients with NVAF who were taking dabigatran, rivaroxaban, or apixaban.
Concurrent use of these NOACs with amiodarone, fluconazole, rifampin, or phenytoin was associated with a significant increase in major bleeding, when compared to use of NOACs alone.
On the other hand, major bleeding was significantly decreased for patients concurrently receiving NOACs and atorvastatin, digoxin, or erythromycin/clarithromycin.
Chang-Fu Kuo, MD, PhD, of Chang Gung Memorial Hospital in Taoyuan, Taiwan, and colleagues conducted this study.
The team used data from the Taiwan National Health Insurance database to study 91,330 patients with NVAF who received at least 1 NOAC prescription of dabigatran (n=45,347), rivaroxaban (n=54,006), or apixaban (n=12,886). The patients’ mean age was 74.7, and 55.8% were male.
The researchers estimated the bleeding risk associated with or without the concurrent use of commonly prescribed medications that share metabolic pathways with NOACs—atorvastatin, digoxin, verapamil, diltiazem, amiodarone, cyclosporine, rifampin, phenytoin, dronedarone, erythromycin/clarithromycin, fluconazole, and other azoles (ketoconazole, itraconazole, voriconazole, or posaconazole).
There were 4770 major bleeding events in the patient population.
The data showed that concurrent use of amiodarone, fluconazole, rifampin, and phenytoin with NOACs significantly increased the incidence rates of major bleeding. The adjusted incidence rates per 1000 person-years were:
- 38.09 for NOAC use alone vs 52.04 for amiodarone (difference=13.94, adjusted rate ratio [aRR]=1.37, P<0.01)
- 102.77 for NOAC alone vs 241.92 for fluconazole (difference=138.46, aRR=2.35, P<0.01)
- 65.66 for NOAC alone vs 103.14 for rifampin (difference=36.90, aRR=1.57, P<0.01)
- 56.07 for NOAC alone vs 108.52 for phenytoin (difference=52.31, aRR=1.94, P<0.01).
The incidence rate for major bleeding was significantly lower with concurrent use of atorvastatin, digoxin, and erythromycin or clarithromycin. The adjusted incidence rates per 1000 person-years were:
- 48.96 for NOAC alone vs 34.57 for atorvastatin (difference=-14.38, aRR=0.71, P<0.01)
- 50.14 for NOAC alone vs 45.69 for digoxin (difference=-4.46, aRR=0.91, P<0.01)
- 99.28 for NOAC alone vs 59.38 for erythromycin/clarithromycin (difference=-39.78, aRR=0.60, P<0.01).
The incidence rates of major bleeding were not significantly different for NOAC use alone and concurrent use of NOACs with verapamil, diltiazem, cyclosporine, dronedarone, and ketoconazole, itraconazole, voriconazole, or posaconazole.
The researchers noted that this study has some limitations, including that bleeding risk and anticoagulant treatment are different in Asian and Western populations. Therefore, the external generalizability of these results, particularly to a Western population, may be limited.
Still, the team said physicians prescribing NOACs should consider the potential risks associated with concomitant use of other drugs.
Concurrent use of non-vitamin K oral anticoagulants (NOACs) and drugs that share metabolic pathways with NOACs may affect the risk of major bleeding in patients with nonvalvular atrial fibrillation (NVAF), according to a study published in JAMA.
Researchers studied more than 91,000 Taiwanese patients with NVAF who were taking dabigatran, rivaroxaban, or apixaban.
Concurrent use of these NOACs with amiodarone, fluconazole, rifampin, or phenytoin was associated with a significant increase in major bleeding, when compared to use of NOACs alone.
On the other hand, major bleeding was significantly decreased for patients concurrently receiving NOACs and atorvastatin, digoxin, or erythromycin/clarithromycin.
Chang-Fu Kuo, MD, PhD, of Chang Gung Memorial Hospital in Taoyuan, Taiwan, and colleagues conducted this study.
The team used data from the Taiwan National Health Insurance database to study 91,330 patients with NVAF who received at least 1 NOAC prescription of dabigatran (n=45,347), rivaroxaban (n=54,006), or apixaban (n=12,886). The patients’ mean age was 74.7, and 55.8% were male.
The researchers estimated the bleeding risk associated with or without the concurrent use of commonly prescribed medications that share metabolic pathways with NOACs—atorvastatin, digoxin, verapamil, diltiazem, amiodarone, cyclosporine, rifampin, phenytoin, dronedarone, erythromycin/clarithromycin, fluconazole, and other azoles (ketoconazole, itraconazole, voriconazole, or posaconazole).
There were 4770 major bleeding events in the patient population.
The data showed that concurrent use of amiodarone, fluconazole, rifampin, and phenytoin with NOACs significantly increased the incidence rates of major bleeding. The adjusted incidence rates per 1000 person-years were:
- 38.09 for NOAC use alone vs 52.04 for amiodarone (difference=13.94, adjusted rate ratio [aRR]=1.37, P<0.01)
- 102.77 for NOAC alone vs 241.92 for fluconazole (difference=138.46, aRR=2.35, P<0.01)
- 65.66 for NOAC alone vs 103.14 for rifampin (difference=36.90, aRR=1.57, P<0.01)
- 56.07 for NOAC alone vs 108.52 for phenytoin (difference=52.31, aRR=1.94, P<0.01).
The incidence rate for major bleeding was significantly lower with concurrent use of atorvastatin, digoxin, and erythromycin or clarithromycin. The adjusted incidence rates per 1000 person-years were:
- 48.96 for NOAC alone vs 34.57 for atorvastatin (difference=-14.38, aRR=0.71, P<0.01)
- 50.14 for NOAC alone vs 45.69 for digoxin (difference=-4.46, aRR=0.91, P<0.01)
- 99.28 for NOAC alone vs 59.38 for erythromycin/clarithromycin (difference=-39.78, aRR=0.60, P<0.01).
The incidence rates of major bleeding were not significantly different for NOAC use alone and concurrent use of NOACs with verapamil, diltiazem, cyclosporine, dronedarone, and ketoconazole, itraconazole, voriconazole, or posaconazole.
The researchers noted that this study has some limitations, including that bleeding risk and anticoagulant treatment are different in Asian and Western populations. Therefore, the external generalizability of these results, particularly to a Western population, may be limited.
Still, the team said physicians prescribing NOACs should consider the potential risks associated with concomitant use of other drugs.
Concurrent use of non-vitamin K oral anticoagulants (NOACs) and drugs that share metabolic pathways with NOACs may affect the risk of major bleeding in patients with nonvalvular atrial fibrillation (NVAF), according to a study published in JAMA.
Researchers studied more than 91,000 Taiwanese patients with NVAF who were taking dabigatran, rivaroxaban, or apixaban.
Concurrent use of these NOACs with amiodarone, fluconazole, rifampin, or phenytoin was associated with a significant increase in major bleeding, when compared to use of NOACs alone.
On the other hand, major bleeding was significantly decreased for patients concurrently receiving NOACs and atorvastatin, digoxin, or erythromycin/clarithromycin.
Chang-Fu Kuo, MD, PhD, of Chang Gung Memorial Hospital in Taoyuan, Taiwan, and colleagues conducted this study.
The team used data from the Taiwan National Health Insurance database to study 91,330 patients with NVAF who received at least 1 NOAC prescription of dabigatran (n=45,347), rivaroxaban (n=54,006), or apixaban (n=12,886). The patients’ mean age was 74.7, and 55.8% were male.
The researchers estimated the bleeding risk associated with or without the concurrent use of commonly prescribed medications that share metabolic pathways with NOACs—atorvastatin, digoxin, verapamil, diltiazem, amiodarone, cyclosporine, rifampin, phenytoin, dronedarone, erythromycin/clarithromycin, fluconazole, and other azoles (ketoconazole, itraconazole, voriconazole, or posaconazole).
There were 4770 major bleeding events in the patient population.
The data showed that concurrent use of amiodarone, fluconazole, rifampin, and phenytoin with NOACs significantly increased the incidence rates of major bleeding. The adjusted incidence rates per 1000 person-years were:
- 38.09 for NOAC use alone vs 52.04 for amiodarone (difference=13.94, adjusted rate ratio [aRR]=1.37, P<0.01)
- 102.77 for NOAC alone vs 241.92 for fluconazole (difference=138.46, aRR=2.35, P<0.01)
- 65.66 for NOAC alone vs 103.14 for rifampin (difference=36.90, aRR=1.57, P<0.01)
- 56.07 for NOAC alone vs 108.52 for phenytoin (difference=52.31, aRR=1.94, P<0.01).
The incidence rate for major bleeding was significantly lower with concurrent use of atorvastatin, digoxin, and erythromycin or clarithromycin. The adjusted incidence rates per 1000 person-years were:
- 48.96 for NOAC alone vs 34.57 for atorvastatin (difference=-14.38, aRR=0.71, P<0.01)
- 50.14 for NOAC alone vs 45.69 for digoxin (difference=-4.46, aRR=0.91, P<0.01)
- 99.28 for NOAC alone vs 59.38 for erythromycin/clarithromycin (difference=-39.78, aRR=0.60, P<0.01).
The incidence rates of major bleeding were not significantly different for NOAC use alone and concurrent use of NOACs with verapamil, diltiazem, cyclosporine, dronedarone, and ketoconazole, itraconazole, voriconazole, or posaconazole.
The researchers noted that this study has some limitations, including that bleeding risk and anticoagulant treatment are different in Asian and Western populations. Therefore, the external generalizability of these results, particularly to a Western population, may be limited.
Still, the team said physicians prescribing NOACs should consider the potential risks associated with concomitant use of other drugs.