User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Patient Navigators for Serious Illnesses Can Now Bill Under New Medicare Codes
In a move that acknowledges the gauntlet the US health system poses for people facing serious and fatal illnesses, Medicare will pay for a new class of workers to help patients manage treatments for conditions like cancer and heart failure.
The 2024 Medicare physician fee schedule includes new billing codes, including G0023, to pay for 60 minutes a month of care coordination by certified or trained auxiliary personnel working under the direction of a clinician.
A diagnosis of cancer or another serious illness takes a toll beyond the physical effects of the disease. Patients often scramble to make adjustments in family and work schedules to manage treatment, said Samyukta Mullangi, MD, MBA, medical director of oncology at Thyme Care, a Nashville, Tennessee–based firm that provides navigation and coordination services to oncology practices and insurers.

“It just really does create a bit of a pressure cooker for patients,” Dr. Mullangi told this news organization.
Medicare has for many years paid for medical professionals to help patients cope with the complexities of disease, such as chronic care management (CCM) provided by physicians, nurses, and physician assistants.
The new principal illness navigation (PIN) payments are intended to pay for work that to date typically has been done by people without medical degrees, including those involved in peer support networks and community health programs. The US Centers for Medicare and Medicaid Services(CMS) expects these navigators will undergo training and work under the supervision of clinicians.
The new navigators may coordinate care transitions between medical settings, follow up with patients after emergency department (ED) visits, or communicate with skilled nursing facilities regarding the psychosocial needs and functional deficits of a patient, among other functions.
CMS expects the new navigators may:
- Conduct assessments to understand a patient’s life story, strengths, needs, goals, preferences, and desired outcomes, including understanding cultural and linguistic factors.
- Provide support to accomplish the clinician’s treatment plan.
- Coordinate the receipt of needed services from healthcare facilities, home- and community-based service providers, and caregivers.
Peers as Navigators
The new navigators can be former patients who have undergone similar treatments for serious diseases, CMS said. This approach sets the new program apart from other care management services Medicare already covers, program officials wrote in the 2024 physician fee schedule.
“For some conditions, patients are best able to engage with the healthcare system and access care if they have assistance from a single, dedicated individual who has ‘lived experience,’ ” according to the rule.
The agency has taken a broad initial approach in defining what kinds of illnesses a patient may have to qualify for services. Patients must have a serious condition that is expected to last at least 3 months, such as cancer, heart failure, or substance use disorder.
But those without a definitive diagnosis may also qualify to receive navigator services.
In the rule, CMS cited a case in which a CT scan identified a suspicious mass in a patient’s colon. A clinician might decide this person would benefit from navigation services due to the potential risks for an undiagnosed illness.
“Regardless of the definitive diagnosis of the mass, presence of a colonic mass for that patient may be a serious high-risk condition that could, for example, cause obstruction and lead the patient to present to the emergency department, as well as be potentially indicative of an underlying life-threatening illness such as colon cancer,” CMS wrote in the rule.
Navigators often start their work when cancer patients are screened and guide them through initial diagnosis, potential surgery, radiation, or chemotherapy, said Sharon Gentry, MSN, RN, a former nurse navigator who is now the editor in chief of the Journal of the Academy of Oncology Nurse & Patient Navigators.
The navigators are meant to be a trusted and continual presence for patients, who otherwise might be left to start anew in finding help at each phase of care.
The navigators “see the whole picture. They see the whole journey the patient takes, from pre-diagnosis all the way through diagnosis care out through survival,” Ms. Gentry said.

Gaining a special Medicare payment for these kinds of services will elevate this work, she said.
Many newer drugs can target specific mechanisms and proteins of cancer. Often, oncology treatment involves testing to find out if mutations are allowing the cancer cells to evade a patient’s immune system.
Checking these biomarkers takes time, however. Patients sometimes become frustrated because they are anxious to begin treatment. Patients may receive inaccurate information from friends or family who went through treatment previously. Navigators can provide knowledge on the current state of care for a patient’s disease, helping them better manage anxieties.
“You have to explain to them that things have changed since the guy you drink coffee with was diagnosed with cancer, and there may be a drug that could target that,” Ms. Gentry said.
Potential Challenges
Initial uptake of the new PIN codes may be slow going, however, as clinicians and health systems may already use well-established codes. These include CCM and principal care management services, which may pay higher rates, Mullangi said.
“There might be sensitivity around not wanting to cannibalize existing programs with a new program,” Dr. Mullangi said.
In addition, many patients will have a copay for the services of principal illness navigators, Dr. Mullangi said.
While many patients have additional insurance that would cover the service, not all do. People with traditional Medicare coverage can sometimes pay 20% of the cost of some medical services.
“I think that may give patients pause, particularly if they’re already feeling the financial burden of a cancer treatment journey,” Dr. Mullangi said.
Pay rates for PIN services involve calculations of regional price differences, which are posted publicly by CMS, and potential added fees for services provided by hospital-affiliated organizations.
Consider payments for code G0023, covering 60 minutes of principal navigation services provided in a single month.
A set reimbursement for patients cared for in independent medical practices exists, with variation for local costs. Medicare’s non-facility price for G0023 would be $102.41 in some parts of Silicon Valley in California, including San Jose. In Arkansas, where costs are lower, reimbursement would be $73.14 for this same service.
Patients who get services covered by code G0023 in independent medical practices would have monthly copays of about $15-$20, depending on where they live.
The tab for patients tends to be higher for these same services if delivered through a medical practice owned by a hospital, as this would trigger the addition of facility fees to the payments made to cover the services. Facility fees are difficult for the public to ascertain before getting a treatment or service.
Dr. Mullangi and Ms. Gentry reported no relevant financial disclosures outside of their employers.
A version of this article first appeared on Medscape.com.
In a move that acknowledges the gauntlet the US health system poses for people facing serious and fatal illnesses, Medicare will pay for a new class of workers to help patients manage treatments for conditions like cancer and heart failure.
The 2024 Medicare physician fee schedule includes new billing codes, including G0023, to pay for 60 minutes a month of care coordination by certified or trained auxiliary personnel working under the direction of a clinician.
A diagnosis of cancer or another serious illness takes a toll beyond the physical effects of the disease. Patients often scramble to make adjustments in family and work schedules to manage treatment, said Samyukta Mullangi, MD, MBA, medical director of oncology at Thyme Care, a Nashville, Tennessee–based firm that provides navigation and coordination services to oncology practices and insurers.
“It just really does create a bit of a pressure cooker for patients,” Dr. Mullangi told this news organization.
Medicare has for many years paid for medical professionals to help patients cope with the complexities of disease, such as chronic care management (CCM) provided by physicians, nurses, and physician assistants.
The new principal illness navigation (PIN) payments are intended to pay for work that to date typically has been done by people without medical degrees, including those involved in peer support networks and community health programs. The US Centers for Medicare and Medicaid Services(CMS) expects these navigators will undergo training and work under the supervision of clinicians.
The new navigators may coordinate care transitions between medical settings, follow up with patients after emergency department (ED) visits, or communicate with skilled nursing facilities regarding the psychosocial needs and functional deficits of a patient, among other functions.
CMS expects the new navigators may:
- Conduct assessments to understand a patient’s life story, strengths, needs, goals, preferences, and desired outcomes, including understanding cultural and linguistic factors.
- Provide support to accomplish the clinician’s treatment plan.
- Coordinate the receipt of needed services from healthcare facilities, home- and community-based service providers, and caregivers.
Peers as Navigators
The new navigators can be former patients who have undergone similar treatments for serious diseases, CMS said. This approach sets the new program apart from other care management services Medicare already covers, program officials wrote in the 2024 physician fee schedule.
“For some conditions, patients are best able to engage with the healthcare system and access care if they have assistance from a single, dedicated individual who has ‘lived experience,’ ” according to the rule.
The agency has taken a broad initial approach in defining what kinds of illnesses a patient may have to qualify for services. Patients must have a serious condition that is expected to last at least 3 months, such as cancer, heart failure, or substance use disorder.
But those without a definitive diagnosis may also qualify to receive navigator services.
In the rule, CMS cited a case in which a CT scan identified a suspicious mass in a patient’s colon. A clinician might decide this person would benefit from navigation services due to the potential risks for an undiagnosed illness.
“Regardless of the definitive diagnosis of the mass, presence of a colonic mass for that patient may be a serious high-risk condition that could, for example, cause obstruction and lead the patient to present to the emergency department, as well as be potentially indicative of an underlying life-threatening illness such as colon cancer,” CMS wrote in the rule.
Navigators often start their work when cancer patients are screened and guide them through initial diagnosis, potential surgery, radiation, or chemotherapy, said Sharon Gentry, MSN, RN, a former nurse navigator who is now the editor in chief of the Journal of the Academy of Oncology Nurse & Patient Navigators.
The navigators are meant to be a trusted and continual presence for patients, who otherwise might be left to start anew in finding help at each phase of care.
The navigators “see the whole picture. They see the whole journey the patient takes, from pre-diagnosis all the way through diagnosis care out through survival,” Ms. Gentry said.
Gaining a special Medicare payment for these kinds of services will elevate this work, she said.
Many newer drugs can target specific mechanisms and proteins of cancer. Often, oncology treatment involves testing to find out if mutations are allowing the cancer cells to evade a patient’s immune system.
Checking these biomarkers takes time, however. Patients sometimes become frustrated because they are anxious to begin treatment. Patients may receive inaccurate information from friends or family who went through treatment previously. Navigators can provide knowledge on the current state of care for a patient’s disease, helping them better manage anxieties.
“You have to explain to them that things have changed since the guy you drink coffee with was diagnosed with cancer, and there may be a drug that could target that,” Ms. Gentry said.
Potential Challenges
Initial uptake of the new PIN codes may be slow going, however, as clinicians and health systems may already use well-established codes. These include CCM and principal care management services, which may pay higher rates, Mullangi said.
“There might be sensitivity around not wanting to cannibalize existing programs with a new program,” Dr. Mullangi said.
In addition, many patients will have a copay for the services of principal illness navigators, Dr. Mullangi said.
While many patients have additional insurance that would cover the service, not all do. People with traditional Medicare coverage can sometimes pay 20% of the cost of some medical services.
“I think that may give patients pause, particularly if they’re already feeling the financial burden of a cancer treatment journey,” Dr. Mullangi said.
Pay rates for PIN services involve calculations of regional price differences, which are posted publicly by CMS, and potential added fees for services provided by hospital-affiliated organizations.
Consider payments for code G0023, covering 60 minutes of principal navigation services provided in a single month.
A set reimbursement for patients cared for in independent medical practices exists, with variation for local costs. Medicare’s non-facility price for G0023 would be $102.41 in some parts of Silicon Valley in California, including San Jose. In Arkansas, where costs are lower, reimbursement would be $73.14 for this same service.
Patients who get services covered by code G0023 in independent medical practices would have monthly copays of about $15-$20, depending on where they live.
The tab for patients tends to be higher for these same services if delivered through a medical practice owned by a hospital, as this would trigger the addition of facility fees to the payments made to cover the services. Facility fees are difficult for the public to ascertain before getting a treatment or service.
Dr. Mullangi and Ms. Gentry reported no relevant financial disclosures outside of their employers.
A version of this article first appeared on Medscape.com.
In a move that acknowledges the gauntlet the US health system poses for people facing serious and fatal illnesses, Medicare will pay for a new class of workers to help patients manage treatments for conditions like cancer and heart failure.
The 2024 Medicare physician fee schedule includes new billing codes, including G0023, to pay for 60 minutes a month of care coordination by certified or trained auxiliary personnel working under the direction of a clinician.
A diagnosis of cancer or another serious illness takes a toll beyond the physical effects of the disease. Patients often scramble to make adjustments in family and work schedules to manage treatment, said Samyukta Mullangi, MD, MBA, medical director of oncology at Thyme Care, a Nashville, Tennessee–based firm that provides navigation and coordination services to oncology practices and insurers.
“It just really does create a bit of a pressure cooker for patients,” Dr. Mullangi told this news organization.
Medicare has for many years paid for medical professionals to help patients cope with the complexities of disease, such as chronic care management (CCM) provided by physicians, nurses, and physician assistants.
The new principal illness navigation (PIN) payments are intended to pay for work that to date typically has been done by people without medical degrees, including those involved in peer support networks and community health programs. The US Centers for Medicare and Medicaid Services(CMS) expects these navigators will undergo training and work under the supervision of clinicians.
The new navigators may coordinate care transitions between medical settings, follow up with patients after emergency department (ED) visits, or communicate with skilled nursing facilities regarding the psychosocial needs and functional deficits of a patient, among other functions.
CMS expects the new navigators may:
- Conduct assessments to understand a patient’s life story, strengths, needs, goals, preferences, and desired outcomes, including understanding cultural and linguistic factors.
- Provide support to accomplish the clinician’s treatment plan.
- Coordinate the receipt of needed services from healthcare facilities, home- and community-based service providers, and caregivers.
Peers as Navigators
The new navigators can be former patients who have undergone similar treatments for serious diseases, CMS said. This approach sets the new program apart from other care management services Medicare already covers, program officials wrote in the 2024 physician fee schedule.
“For some conditions, patients are best able to engage with the healthcare system and access care if they have assistance from a single, dedicated individual who has ‘lived experience,’ ” according to the rule.
The agency has taken a broad initial approach in defining what kinds of illnesses a patient may have to qualify for services. Patients must have a serious condition that is expected to last at least 3 months, such as cancer, heart failure, or substance use disorder.
But those without a definitive diagnosis may also qualify to receive navigator services.
In the rule, CMS cited a case in which a CT scan identified a suspicious mass in a patient’s colon. A clinician might decide this person would benefit from navigation services due to the potential risks for an undiagnosed illness.
“Regardless of the definitive diagnosis of the mass, presence of a colonic mass for that patient may be a serious high-risk condition that could, for example, cause obstruction and lead the patient to present to the emergency department, as well as be potentially indicative of an underlying life-threatening illness such as colon cancer,” CMS wrote in the rule.
Navigators often start their work when cancer patients are screened and guide them through initial diagnosis, potential surgery, radiation, or chemotherapy, said Sharon Gentry, MSN, RN, a former nurse navigator who is now the editor in chief of the Journal of the Academy of Oncology Nurse & Patient Navigators.
The navigators are meant to be a trusted and continual presence for patients, who otherwise might be left to start anew in finding help at each phase of care.
The navigators “see the whole picture. They see the whole journey the patient takes, from pre-diagnosis all the way through diagnosis care out through survival,” Ms. Gentry said.
Gaining a special Medicare payment for these kinds of services will elevate this work, she said.
Many newer drugs can target specific mechanisms and proteins of cancer. Often, oncology treatment involves testing to find out if mutations are allowing the cancer cells to evade a patient’s immune system.
Checking these biomarkers takes time, however. Patients sometimes become frustrated because they are anxious to begin treatment. Patients may receive inaccurate information from friends or family who went through treatment previously. Navigators can provide knowledge on the current state of care for a patient’s disease, helping them better manage anxieties.
“You have to explain to them that things have changed since the guy you drink coffee with was diagnosed with cancer, and there may be a drug that could target that,” Ms. Gentry said.
Potential Challenges
Initial uptake of the new PIN codes may be slow going, however, as clinicians and health systems may already use well-established codes. These include CCM and principal care management services, which may pay higher rates, Mullangi said.
“There might be sensitivity around not wanting to cannibalize existing programs with a new program,” Dr. Mullangi said.
In addition, many patients will have a copay for the services of principal illness navigators, Dr. Mullangi said.
While many patients have additional insurance that would cover the service, not all do. People with traditional Medicare coverage can sometimes pay 20% of the cost of some medical services.
“I think that may give patients pause, particularly if they’re already feeling the financial burden of a cancer treatment journey,” Dr. Mullangi said.
Pay rates for PIN services involve calculations of regional price differences, which are posted publicly by CMS, and potential added fees for services provided by hospital-affiliated organizations.
Consider payments for code G0023, covering 60 minutes of principal navigation services provided in a single month.
A set reimbursement for patients cared for in independent medical practices exists, with variation for local costs. Medicare’s non-facility price for G0023 would be $102.41 in some parts of Silicon Valley in California, including San Jose. In Arkansas, where costs are lower, reimbursement would be $73.14 for this same service.
Patients who get services covered by code G0023 in independent medical practices would have monthly copays of about $15-$20, depending on where they live.
The tab for patients tends to be higher for these same services if delivered through a medical practice owned by a hospital, as this would trigger the addition of facility fees to the payments made to cover the services. Facility fees are difficult for the public to ascertain before getting a treatment or service.
Dr. Mullangi and Ms. Gentry reported no relevant financial disclosures outside of their employers.
A version of this article first appeared on Medscape.com.

Minor Progress in Gender Pay Equity, But a Big Gap Persists
Despite some recent progress in compensation equity, women in medicine continue to be paid significantly lower salaries than men.
According to the Female Compensation Report 2024 by Medscape, male doctors of any kind earned an average salary of about $400,000, whereas female doctors earned approximately $309,000 — a 29% gap.
The report analyzed survey data from 7000 practicing physicians who were recruited over a 4-month period starting in October 2023. The respondents comprised roughly 60% women representing over 29 specialties.
In the 2022 report, the pay gap between the genders was 32%. But some women in the field argued substantial headway is still needed.
“You can try and pick apart the data, but I’d say we’re not really making progress,” said Susan T. Hingle, MD, an internist in Illinois and president of the American Medical Women’s Association. “A decline by a couple of percentage points is not significantly addressing this pay gap that over a lifetime is huge, can be millions of dollars.”
The gender gap was narrower among female primary care physicians (PCPs) vs medical specialists. Female PCPs earned around $253,000 per year, whereas male PCPs earned about $295,000 per year. Hingle suggested that female PCPs may enjoy more pay equity because health systems have a harder time filling these positions.
On the other hand, the gap for specialists rose from 27% in 2022 to 31% in 2023. Differences in how aggressively women and men negotiate compensation packages may play a role, said Hingle.
“Taking negotiation out of the equation would be progress to me,” said Hingle.
Pay disparity did not appear to be the result of time spent on the job — female doctors reported an average of 49 work hours per week, whereas their male counterparts reported 50 work hours per week.
Meanwhile, the pay gap progressively worsened over time. Among doctors aged 28-34 years, men earned an average of $53,000 more than women. By ages 46-49, men earned an average of $157,000 more than women.
“I had to take my employer to court to get equal compensation, sad as it is to say,” said a hospitalist in North Carolina.
Nearly 60% of women surveyed felt they were not being paid fairly for their efforts, up from less than half reported in Medscape’s 2021 report. Hingle said that this figure may not only reflect sentiments about the compensation gap, but also less support on the job, including fewer physician assistants (PAs), nurses, and administrative staff.
“At my job, I do the work of multiple people,” said a survey respondent. “Junior resident, senior resident, social worker, nurse practitioner, PA — as well as try to be a teacher, researcher, [and] an excellent doctor and have the time to make patients feel as if they are not in a rush.”
Roughly 30% of women physicians said they would not choose to go into medicine again if given the chance compared with 26% of male physicians.
“Gender inequities in our profession have a direct impact,” said Shikha Jain, MD, an oncologist in Chicago and founder of the Women in Medicine nonprofit. “I think women in general don’t feel valued in the care they’re providing.”
Jain cited bullying, harassment, and fewer opportunities for leadership and recognition as factors beyond pay that affect female physicians’ feelings of being valued.
A version of this article first appeared on Medscape.com.
Despite some recent progress in compensation equity, women in medicine continue to be paid significantly lower salaries than men.
According to the Female Compensation Report 2024 by Medscape, male doctors of any kind earned an average salary of about $400,000, whereas female doctors earned approximately $309,000 — a 29% gap.
The report analyzed survey data from 7000 practicing physicians who were recruited over a 4-month period starting in October 2023. The respondents comprised roughly 60% women representing over 29 specialties.
In the 2022 report, the pay gap between the genders was 32%. But some women in the field argued substantial headway is still needed.
“You can try and pick apart the data, but I’d say we’re not really making progress,” said Susan T. Hingle, MD, an internist in Illinois and president of the American Medical Women’s Association. “A decline by a couple of percentage points is not significantly addressing this pay gap that over a lifetime is huge, can be millions of dollars.”
The gender gap was narrower among female primary care physicians (PCPs) vs medical specialists. Female PCPs earned around $253,000 per year, whereas male PCPs earned about $295,000 per year. Hingle suggested that female PCPs may enjoy more pay equity because health systems have a harder time filling these positions.
On the other hand, the gap for specialists rose from 27% in 2022 to 31% in 2023. Differences in how aggressively women and men negotiate compensation packages may play a role, said Hingle.
“Taking negotiation out of the equation would be progress to me,” said Hingle.
Pay disparity did not appear to be the result of time spent on the job — female doctors reported an average of 49 work hours per week, whereas their male counterparts reported 50 work hours per week.
Meanwhile, the pay gap progressively worsened over time. Among doctors aged 28-34 years, men earned an average of $53,000 more than women. By ages 46-49, men earned an average of $157,000 more than women.
“I had to take my employer to court to get equal compensation, sad as it is to say,” said a hospitalist in North Carolina.
Nearly 60% of women surveyed felt they were not being paid fairly for their efforts, up from less than half reported in Medscape’s 2021 report. Hingle said that this figure may not only reflect sentiments about the compensation gap, but also less support on the job, including fewer physician assistants (PAs), nurses, and administrative staff.
“At my job, I do the work of multiple people,” said a survey respondent. “Junior resident, senior resident, social worker, nurse practitioner, PA — as well as try to be a teacher, researcher, [and] an excellent doctor and have the time to make patients feel as if they are not in a rush.”
Roughly 30% of women physicians said they would not choose to go into medicine again if given the chance compared with 26% of male physicians.
“Gender inequities in our profession have a direct impact,” said Shikha Jain, MD, an oncologist in Chicago and founder of the Women in Medicine nonprofit. “I think women in general don’t feel valued in the care they’re providing.”
Jain cited bullying, harassment, and fewer opportunities for leadership and recognition as factors beyond pay that affect female physicians’ feelings of being valued.
A version of this article first appeared on Medscape.com.
Despite some recent progress in compensation equity, women in medicine continue to be paid significantly lower salaries than men.
According to the Female Compensation Report 2024 by Medscape, male doctors of any kind earned an average salary of about $400,000, whereas female doctors earned approximately $309,000 — a 29% gap.
The report analyzed survey data from 7000 practicing physicians who were recruited over a 4-month period starting in October 2023. The respondents comprised roughly 60% women representing over 29 specialties.
In the 2022 report, the pay gap between the genders was 32%. But some women in the field argued substantial headway is still needed.
“You can try and pick apart the data, but I’d say we’re not really making progress,” said Susan T. Hingle, MD, an internist in Illinois and president of the American Medical Women’s Association. “A decline by a couple of percentage points is not significantly addressing this pay gap that over a lifetime is huge, can be millions of dollars.”
The gender gap was narrower among female primary care physicians (PCPs) vs medical specialists. Female PCPs earned around $253,000 per year, whereas male PCPs earned about $295,000 per year. Hingle suggested that female PCPs may enjoy more pay equity because health systems have a harder time filling these positions.
On the other hand, the gap for specialists rose from 27% in 2022 to 31% in 2023. Differences in how aggressively women and men negotiate compensation packages may play a role, said Hingle.
“Taking negotiation out of the equation would be progress to me,” said Hingle.
Pay disparity did not appear to be the result of time spent on the job — female doctors reported an average of 49 work hours per week, whereas their male counterparts reported 50 work hours per week.
Meanwhile, the pay gap progressively worsened over time. Among doctors aged 28-34 years, men earned an average of $53,000 more than women. By ages 46-49, men earned an average of $157,000 more than women.
“I had to take my employer to court to get equal compensation, sad as it is to say,” said a hospitalist in North Carolina.
Nearly 60% of women surveyed felt they were not being paid fairly for their efforts, up from less than half reported in Medscape’s 2021 report. Hingle said that this figure may not only reflect sentiments about the compensation gap, but also less support on the job, including fewer physician assistants (PAs), nurses, and administrative staff.
“At my job, I do the work of multiple people,” said a survey respondent. “Junior resident, senior resident, social worker, nurse practitioner, PA — as well as try to be a teacher, researcher, [and] an excellent doctor and have the time to make patients feel as if they are not in a rush.”
Roughly 30% of women physicians said they would not choose to go into medicine again if given the chance compared with 26% of male physicians.
“Gender inequities in our profession have a direct impact,” said Shikha Jain, MD, an oncologist in Chicago and founder of the Women in Medicine nonprofit. “I think women in general don’t feel valued in the care they’re providing.”
Jain cited bullying, harassment, and fewer opportunities for leadership and recognition as factors beyond pay that affect female physicians’ feelings of being valued.
A version of this article first appeared on Medscape.com.
Michigan Oncologist Charged in Scheme to Illegally Sell Cancer Drugs
In late October, a federal grand jury charged a Detroit-area medical oncologist Naveed Aslam, MD, in an indictment for his part in a scheme to illegally sell cancer drugs.
According to the indictment, Aslam acquired and sold more than $17 million in cancer drugs and personally netted more than $2.5 million during the scheme.
The charges against Aslam, filed on October 23 in the US District Court for the Eastern District of Michigan, include 10 counts of illegally selling or trading prescription drugs and one count of conspiring to do so.
“Dr. Aslam’s alleged participation in this scheme not only allowed him to profit unlawfully from the sale of cancer drugs but it also posed a serious threat by potentially placing these medications into the wrong hands,” Cheyvoryea Gibson, special agent in charge of the FBI in Michigan, said in a press release announcing the indictment.
The investigation is being conducted jointly by the FBI, the US Food and Drug Administration (FDA), the US Department of Health and Human Services Office of Inspector General, and Homeland Security Investigations.
The indictment alleges that Aslam was recruited by an unnamed operator of a Michigan corporation that engaged in business as a retail pharmacy and in the wholesale distribution of expensive prescription drugs, largely oncology drugs.
According to the indictment, Aslam and the operator came to an agreement where Aslam would purchase these expensive drugs from an authorized distributor under the false pretense that he was going to prescribe them to patients.
Instead, Aslam allegedly “sold and transferred the prescription drugs” to or through the Michigan business, with involvement from the unnamed operator and a second unnamed individual.
The unnamed individuals “identified customers interested in buying prescription cancer drugs” and “communicated with Dr. Aslam about what cancer drugs were requested,” according to the press release. “Dr. Aslam used his access to certain cancer drugs through his medical practice, Somerset Hematology and Oncology, P.C., to order and purchase the cancer drugs from his supplier.”
The indictment lays out that Aslam allegedly profited from this scheme in several ways, which included charging the Michigan business more than he paid the distributor for the drugs, sharing the profits when the business resold the drugs at a markup, and receiving rebates and discounts from the distributor “based on the amount of qualifying drugs he purchased and resold.”
According to the indictment, the scheme ran from early 2019 to mid-2023 and included four antibody drug conjugates — trastuzumab deruxtecan (Enhertu), enfortumab vedotin (Padcev), tisotumab vedotin (Tivdak), and sacituzumab govitecan (Trodelvy) — and the monoclonal antibody mogamulizumab (Poteligeo) for cutaneous T-cell lymphoma.
By working with Aslam, the operatives “obtained prescription drugs from an authorized distributor that they would not otherwise have been permitted to purchase, and which they were able to sell at a profit,” according to the indictment.
Both the prosecuting assistant US attorney, Andrew Lievense, and Aslam’s defense lawyer, Daniel Dena, declined to comment for this news organization.
The prosecutor is seeking to recoup the more than $2.5 million Aslam allegedly pocketed, according to the indictment. The press release also noted that an “indictment is only a charge and is not evidence of guilt.”
A version of this article first appeared on Medscape.com.
In late October, a federal grand jury charged a Detroit-area medical oncologist Naveed Aslam, MD, in an indictment for his part in a scheme to illegally sell cancer drugs.
According to the indictment, Aslam acquired and sold more than $17 million in cancer drugs and personally netted more than $2.5 million during the scheme.
The charges against Aslam, filed on October 23 in the US District Court for the Eastern District of Michigan, include 10 counts of illegally selling or trading prescription drugs and one count of conspiring to do so.
“Dr. Aslam’s alleged participation in this scheme not only allowed him to profit unlawfully from the sale of cancer drugs but it also posed a serious threat by potentially placing these medications into the wrong hands,” Cheyvoryea Gibson, special agent in charge of the FBI in Michigan, said in a press release announcing the indictment.
The investigation is being conducted jointly by the FBI, the US Food and Drug Administration (FDA), the US Department of Health and Human Services Office of Inspector General, and Homeland Security Investigations.
The indictment alleges that Aslam was recruited by an unnamed operator of a Michigan corporation that engaged in business as a retail pharmacy and in the wholesale distribution of expensive prescription drugs, largely oncology drugs.
According to the indictment, Aslam and the operator came to an agreement where Aslam would purchase these expensive drugs from an authorized distributor under the false pretense that he was going to prescribe them to patients.
Instead, Aslam allegedly “sold and transferred the prescription drugs” to or through the Michigan business, with involvement from the unnamed operator and a second unnamed individual.
The unnamed individuals “identified customers interested in buying prescription cancer drugs” and “communicated with Dr. Aslam about what cancer drugs were requested,” according to the press release. “Dr. Aslam used his access to certain cancer drugs through his medical practice, Somerset Hematology and Oncology, P.C., to order and purchase the cancer drugs from his supplier.”
The indictment lays out that Aslam allegedly profited from this scheme in several ways, which included charging the Michigan business more than he paid the distributor for the drugs, sharing the profits when the business resold the drugs at a markup, and receiving rebates and discounts from the distributor “based on the amount of qualifying drugs he purchased and resold.”
According to the indictment, the scheme ran from early 2019 to mid-2023 and included four antibody drug conjugates — trastuzumab deruxtecan (Enhertu), enfortumab vedotin (Padcev), tisotumab vedotin (Tivdak), and sacituzumab govitecan (Trodelvy) — and the monoclonal antibody mogamulizumab (Poteligeo) for cutaneous T-cell lymphoma.
By working with Aslam, the operatives “obtained prescription drugs from an authorized distributor that they would not otherwise have been permitted to purchase, and which they were able to sell at a profit,” according to the indictment.
Both the prosecuting assistant US attorney, Andrew Lievense, and Aslam’s defense lawyer, Daniel Dena, declined to comment for this news organization.
The prosecutor is seeking to recoup the more than $2.5 million Aslam allegedly pocketed, according to the indictment. The press release also noted that an “indictment is only a charge and is not evidence of guilt.”
A version of this article first appeared on Medscape.com.
In late October, a federal grand jury charged a Detroit-area medical oncologist Naveed Aslam, MD, in an indictment for his part in a scheme to illegally sell cancer drugs.
According to the indictment, Aslam acquired and sold more than $17 million in cancer drugs and personally netted more than $2.5 million during the scheme.
The charges against Aslam, filed on October 23 in the US District Court for the Eastern District of Michigan, include 10 counts of illegally selling or trading prescription drugs and one count of conspiring to do so.
“Dr. Aslam’s alleged participation in this scheme not only allowed him to profit unlawfully from the sale of cancer drugs but it also posed a serious threat by potentially placing these medications into the wrong hands,” Cheyvoryea Gibson, special agent in charge of the FBI in Michigan, said in a press release announcing the indictment.
The investigation is being conducted jointly by the FBI, the US Food and Drug Administration (FDA), the US Department of Health and Human Services Office of Inspector General, and Homeland Security Investigations.
The indictment alleges that Aslam was recruited by an unnamed operator of a Michigan corporation that engaged in business as a retail pharmacy and in the wholesale distribution of expensive prescription drugs, largely oncology drugs.
According to the indictment, Aslam and the operator came to an agreement where Aslam would purchase these expensive drugs from an authorized distributor under the false pretense that he was going to prescribe them to patients.
Instead, Aslam allegedly “sold and transferred the prescription drugs” to or through the Michigan business, with involvement from the unnamed operator and a second unnamed individual.
The unnamed individuals “identified customers interested in buying prescription cancer drugs” and “communicated with Dr. Aslam about what cancer drugs were requested,” according to the press release. “Dr. Aslam used his access to certain cancer drugs through his medical practice, Somerset Hematology and Oncology, P.C., to order and purchase the cancer drugs from his supplier.”
The indictment lays out that Aslam allegedly profited from this scheme in several ways, which included charging the Michigan business more than he paid the distributor for the drugs, sharing the profits when the business resold the drugs at a markup, and receiving rebates and discounts from the distributor “based on the amount of qualifying drugs he purchased and resold.”
According to the indictment, the scheme ran from early 2019 to mid-2023 and included four antibody drug conjugates — trastuzumab deruxtecan (Enhertu), enfortumab vedotin (Padcev), tisotumab vedotin (Tivdak), and sacituzumab govitecan (Trodelvy) — and the monoclonal antibody mogamulizumab (Poteligeo) for cutaneous T-cell lymphoma.
By working with Aslam, the operatives “obtained prescription drugs from an authorized distributor that they would not otherwise have been permitted to purchase, and which they were able to sell at a profit,” according to the indictment.
Both the prosecuting assistant US attorney, Andrew Lievense, and Aslam’s defense lawyer, Daniel Dena, declined to comment for this news organization.
The prosecutor is seeking to recoup the more than $2.5 million Aslam allegedly pocketed, according to the indictment. The press release also noted that an “indictment is only a charge and is not evidence of guilt.”
A version of this article first appeared on Medscape.com.
Low-Volume Bowel Prep Easier, as Effective as Standard Prep in Hospitalized Patients
PHILADELPHIA — according to a study presented at the annual meeting of the American College of Gastroenterology (ACG).
Patients who received MoviPrep (2L of polyethylene glycol and ascorbic acid) reported higher tolerability and willingness to repeat colonoscopy preparation in the future than those taking GoLYTELY (4L of polyethylene glycol and electrolytes). In addition, the rates of electrolyte abnormalities and acute kidney injury were low and similar between the two groups.
“Bowel preparation remains a challenge in the inpatient setting, where 20%-50% of all colonoscopies can have inadequate bowel preparation,” said lead author Karen Xiao, MD, assistant professor in the section of digestive diseases at Yale School of Medicine, New Haven, Connecticut.
Previous studies have indicated that low-volume (2L), split-dose preparations are noninferior to high-volume (4L), split-dose regimens, and patients generally prefer low-volume options, she said. However, the current standard of care for inpatients continues to include high-volume polyethylene glycol electrocyte lavage, which may be less tolerable.
“Similar to prior studies, our study supports that MoviPrep may be a suitable alternative to traditional high-volume bowel preparation in hospitalized patients undergoing colonoscopy,” she said.
In a single-blind, multi-site, randomized controlled trial, Xiao and colleagues in the Yale–New Haven Health System randomly assigned inpatients undergoing colonoscopy to MoviPrep or GoLYTELY between January 2022 and July 2024. They excluded patients with prior small or large bowel resection, foreign body removal, or medical contraindications, such as obstruction, pregnancy, phenylketonuria, or glucose-6-phosphate dehydrogenase deficiency.
After bowel prep but before colonoscopy, patients took the Mayo Clinic Bowel Preparation survey. Colonoscopies were then recorded, and videos were scored by a single-blinded central reviewer. The primary outcome included the adequacy of bowel prep as defined by a Boston Bowel Preparation Scale score of 6 or higher, with each segment scoring 2 or higher.
In the final analysis, 202 patients received MoviPrep and 210 received GoLYTELY. In both groups, the average age was 62; about 60% were men; and 66% were White, about 22% Black, and 13%-15% Hispanic. About 65% of patients in both arms had an American Society of Anesthesiologists (ASA) score of 3, with another 20% in each group having an ASA score of 4, “reflective of a sicker inpatient population,” Xiao said.
Inpatient colonoscopy was indicated for gastrointestinal bleeding (55%), diarrhea (15%-20%), abnormal imaging (10%-13%), inflammatory bowel disease (4%), or other (35%-41%). Patients could have more than one indication for colonoscopy.
Overall, bowel preparation was scored as adequate in 111 patients with MoviPrep (55%) and 111 patients with GoLYTELY (52.9%), and was inadequate in 91 patients with MoviPrep (45%) and 99 patients with GoLYTELY (47.1%). With a rate difference of 2.1% and a P value of .007, MoviPrep was considered noninferior to GoLYTELY for adequate bowel preparation.
In terms of secondary outcomes, there wasn’t a significant difference in the length of hospital stay, with a median stay of 6 days. Similarly, there were no differences in the rates of adverse events, including acute kidney injury and electrolyte abnormalities, with rates ranging from 1% to 9%. MoviPrep patients were slightly more likely to need additional bowel prep but also had a slightly shorter time to colonoscopy.
Ease of Use Is a Plus
On the basis of the Mayo Clinic Bowel Preparation survey, there wasn’t a difference between the groups in how much bowel prep solution was left in the bottle. However, more than twice as many patients who took MoviPrep said the prep was “easy,” and more MoviPrep patients called it “acceptable,” whereas more GoLYTELY patients said prep was “somewhat difficult” or “very difficult.”
In addition, significantly more MoviPrep patients (49.7% vs 33.7%) said they were “mostly willing” to drink the same prep again if they needed another colonoscopy in the future, while more GoLYTELY patients said they were “somewhat willing” (44.7% vs 34.6%) or “not willing at all” (21.6% vs 15.7%).
“Bowel prep, particularly in hospitals, is important because we do it so often. When you think about what our patients in the hospital are going through, they’re very sick and often have multiple comorbidities, so how can we give them a bowel prep that is safe for them, easiest for them, easy for our nursing staff who are experiencing shortages, and as good as the traditional bowel prep,” said the session’s moderator, Amy Oxentenko, MD, AGAF, professor of medicine and gastroenterologist at Mayo Clinic, Rochester, Minnesota.
“Here we’ve seen great data that we can provide half the volume of the prep, still get amazing results in terms of adequacy of preparation, and the patients had a better experience,” said Oxentenko, the incoming ACG president. “That’s important because they likely may need another colonoscopy in the future, and we would hate for the bowel prep in the hospital to potentially dissuade them from a future colonoscopy.”
Future studies could stratify patients on the basis of colonoscopy indication or patient history, including conditions such as chronic constipation or neurogenic bowel, where some patients may still need a high-volume prep, Oxentenko said.
“Also, in the hospital setting, we don’t always know when a patient is going to the endoscopy suite due to other patient cases that may get prolonged or pushed in,” she said. “So how do you time the second dose of the split dose in anticipation of when that patient will go to the endoscopy suite to maintain that great preparation with a smaller volume prep?”
The study was awarded the ACG Governors Award for Excellence in Clinical Research (Trainee). Xiao and Oxentenko reported no relevant disclosures.
A version of this article appeared on Medscape.com.
PHILADELPHIA — according to a study presented at the annual meeting of the American College of Gastroenterology (ACG).
Patients who received MoviPrep (2L of polyethylene glycol and ascorbic acid) reported higher tolerability and willingness to repeat colonoscopy preparation in the future than those taking GoLYTELY (4L of polyethylene glycol and electrolytes). In addition, the rates of electrolyte abnormalities and acute kidney injury were low and similar between the two groups.
“Bowel preparation remains a challenge in the inpatient setting, where 20%-50% of all colonoscopies can have inadequate bowel preparation,” said lead author Karen Xiao, MD, assistant professor in the section of digestive diseases at Yale School of Medicine, New Haven, Connecticut.
Previous studies have indicated that low-volume (2L), split-dose preparations are noninferior to high-volume (4L), split-dose regimens, and patients generally prefer low-volume options, she said. However, the current standard of care for inpatients continues to include high-volume polyethylene glycol electrocyte lavage, which may be less tolerable.
“Similar to prior studies, our study supports that MoviPrep may be a suitable alternative to traditional high-volume bowel preparation in hospitalized patients undergoing colonoscopy,” she said.
In a single-blind, multi-site, randomized controlled trial, Xiao and colleagues in the Yale–New Haven Health System randomly assigned inpatients undergoing colonoscopy to MoviPrep or GoLYTELY between January 2022 and July 2024. They excluded patients with prior small or large bowel resection, foreign body removal, or medical contraindications, such as obstruction, pregnancy, phenylketonuria, or glucose-6-phosphate dehydrogenase deficiency.
After bowel prep but before colonoscopy, patients took the Mayo Clinic Bowel Preparation survey. Colonoscopies were then recorded, and videos were scored by a single-blinded central reviewer. The primary outcome included the adequacy of bowel prep as defined by a Boston Bowel Preparation Scale score of 6 or higher, with each segment scoring 2 or higher.
In the final analysis, 202 patients received MoviPrep and 210 received GoLYTELY. In both groups, the average age was 62; about 60% were men; and 66% were White, about 22% Black, and 13%-15% Hispanic. About 65% of patients in both arms had an American Society of Anesthesiologists (ASA) score of 3, with another 20% in each group having an ASA score of 4, “reflective of a sicker inpatient population,” Xiao said.
Inpatient colonoscopy was indicated for gastrointestinal bleeding (55%), diarrhea (15%-20%), abnormal imaging (10%-13%), inflammatory bowel disease (4%), or other (35%-41%). Patients could have more than one indication for colonoscopy.
Overall, bowel preparation was scored as adequate in 111 patients with MoviPrep (55%) and 111 patients with GoLYTELY (52.9%), and was inadequate in 91 patients with MoviPrep (45%) and 99 patients with GoLYTELY (47.1%). With a rate difference of 2.1% and a P value of .007, MoviPrep was considered noninferior to GoLYTELY for adequate bowel preparation.
In terms of secondary outcomes, there wasn’t a significant difference in the length of hospital stay, with a median stay of 6 days. Similarly, there were no differences in the rates of adverse events, including acute kidney injury and electrolyte abnormalities, with rates ranging from 1% to 9%. MoviPrep patients were slightly more likely to need additional bowel prep but also had a slightly shorter time to colonoscopy.
Ease of Use Is a Plus
On the basis of the Mayo Clinic Bowel Preparation survey, there wasn’t a difference between the groups in how much bowel prep solution was left in the bottle. However, more than twice as many patients who took MoviPrep said the prep was “easy,” and more MoviPrep patients called it “acceptable,” whereas more GoLYTELY patients said prep was “somewhat difficult” or “very difficult.”
In addition, significantly more MoviPrep patients (49.7% vs 33.7%) said they were “mostly willing” to drink the same prep again if they needed another colonoscopy in the future, while more GoLYTELY patients said they were “somewhat willing” (44.7% vs 34.6%) or “not willing at all” (21.6% vs 15.7%).
“Bowel prep, particularly in hospitals, is important because we do it so often. When you think about what our patients in the hospital are going through, they’re very sick and often have multiple comorbidities, so how can we give them a bowel prep that is safe for them, easiest for them, easy for our nursing staff who are experiencing shortages, and as good as the traditional bowel prep,” said the session’s moderator, Amy Oxentenko, MD, AGAF, professor of medicine and gastroenterologist at Mayo Clinic, Rochester, Minnesota.
“Here we’ve seen great data that we can provide half the volume of the prep, still get amazing results in terms of adequacy of preparation, and the patients had a better experience,” said Oxentenko, the incoming ACG president. “That’s important because they likely may need another colonoscopy in the future, and we would hate for the bowel prep in the hospital to potentially dissuade them from a future colonoscopy.”
Future studies could stratify patients on the basis of colonoscopy indication or patient history, including conditions such as chronic constipation or neurogenic bowel, where some patients may still need a high-volume prep, Oxentenko said.
“Also, in the hospital setting, we don’t always know when a patient is going to the endoscopy suite due to other patient cases that may get prolonged or pushed in,” she said. “So how do you time the second dose of the split dose in anticipation of when that patient will go to the endoscopy suite to maintain that great preparation with a smaller volume prep?”
The study was awarded the ACG Governors Award for Excellence in Clinical Research (Trainee). Xiao and Oxentenko reported no relevant disclosures.
A version of this article appeared on Medscape.com.
PHILADELPHIA — according to a study presented at the annual meeting of the American College of Gastroenterology (ACG).
Patients who received MoviPrep (2L of polyethylene glycol and ascorbic acid) reported higher tolerability and willingness to repeat colonoscopy preparation in the future than those taking GoLYTELY (4L of polyethylene glycol and electrolytes). In addition, the rates of electrolyte abnormalities and acute kidney injury were low and similar between the two groups.
“Bowel preparation remains a challenge in the inpatient setting, where 20%-50% of all colonoscopies can have inadequate bowel preparation,” said lead author Karen Xiao, MD, assistant professor in the section of digestive diseases at Yale School of Medicine, New Haven, Connecticut.
Previous studies have indicated that low-volume (2L), split-dose preparations are noninferior to high-volume (4L), split-dose regimens, and patients generally prefer low-volume options, she said. However, the current standard of care for inpatients continues to include high-volume polyethylene glycol electrocyte lavage, which may be less tolerable.
“Similar to prior studies, our study supports that MoviPrep may be a suitable alternative to traditional high-volume bowel preparation in hospitalized patients undergoing colonoscopy,” she said.
In a single-blind, multi-site, randomized controlled trial, Xiao and colleagues in the Yale–New Haven Health System randomly assigned inpatients undergoing colonoscopy to MoviPrep or GoLYTELY between January 2022 and July 2024. They excluded patients with prior small or large bowel resection, foreign body removal, or medical contraindications, such as obstruction, pregnancy, phenylketonuria, or glucose-6-phosphate dehydrogenase deficiency.
After bowel prep but before colonoscopy, patients took the Mayo Clinic Bowel Preparation survey. Colonoscopies were then recorded, and videos were scored by a single-blinded central reviewer. The primary outcome included the adequacy of bowel prep as defined by a Boston Bowel Preparation Scale score of 6 or higher, with each segment scoring 2 or higher.
In the final analysis, 202 patients received MoviPrep and 210 received GoLYTELY. In both groups, the average age was 62; about 60% were men; and 66% were White, about 22% Black, and 13%-15% Hispanic. About 65% of patients in both arms had an American Society of Anesthesiologists (ASA) score of 3, with another 20% in each group having an ASA score of 4, “reflective of a sicker inpatient population,” Xiao said.
Inpatient colonoscopy was indicated for gastrointestinal bleeding (55%), diarrhea (15%-20%), abnormal imaging (10%-13%), inflammatory bowel disease (4%), or other (35%-41%). Patients could have more than one indication for colonoscopy.
Overall, bowel preparation was scored as adequate in 111 patients with MoviPrep (55%) and 111 patients with GoLYTELY (52.9%), and was inadequate in 91 patients with MoviPrep (45%) and 99 patients with GoLYTELY (47.1%). With a rate difference of 2.1% and a P value of .007, MoviPrep was considered noninferior to GoLYTELY for adequate bowel preparation.
In terms of secondary outcomes, there wasn’t a significant difference in the length of hospital stay, with a median stay of 6 days. Similarly, there were no differences in the rates of adverse events, including acute kidney injury and electrolyte abnormalities, with rates ranging from 1% to 9%. MoviPrep patients were slightly more likely to need additional bowel prep but also had a slightly shorter time to colonoscopy.
Ease of Use Is a Plus
On the basis of the Mayo Clinic Bowel Preparation survey, there wasn’t a difference between the groups in how much bowel prep solution was left in the bottle. However, more than twice as many patients who took MoviPrep said the prep was “easy,” and more MoviPrep patients called it “acceptable,” whereas more GoLYTELY patients said prep was “somewhat difficult” or “very difficult.”
In addition, significantly more MoviPrep patients (49.7% vs 33.7%) said they were “mostly willing” to drink the same prep again if they needed another colonoscopy in the future, while more GoLYTELY patients said they were “somewhat willing” (44.7% vs 34.6%) or “not willing at all” (21.6% vs 15.7%).
“Bowel prep, particularly in hospitals, is important because we do it so often. When you think about what our patients in the hospital are going through, they’re very sick and often have multiple comorbidities, so how can we give them a bowel prep that is safe for them, easiest for them, easy for our nursing staff who are experiencing shortages, and as good as the traditional bowel prep,” said the session’s moderator, Amy Oxentenko, MD, AGAF, professor of medicine and gastroenterologist at Mayo Clinic, Rochester, Minnesota.
“Here we’ve seen great data that we can provide half the volume of the prep, still get amazing results in terms of adequacy of preparation, and the patients had a better experience,” said Oxentenko, the incoming ACG president. “That’s important because they likely may need another colonoscopy in the future, and we would hate for the bowel prep in the hospital to potentially dissuade them from a future colonoscopy.”
Future studies could stratify patients on the basis of colonoscopy indication or patient history, including conditions such as chronic constipation or neurogenic bowel, where some patients may still need a high-volume prep, Oxentenko said.
“Also, in the hospital setting, we don’t always know when a patient is going to the endoscopy suite due to other patient cases that may get prolonged or pushed in,” she said. “So how do you time the second dose of the split dose in anticipation of when that patient will go to the endoscopy suite to maintain that great preparation with a smaller volume prep?”
The study was awarded the ACG Governors Award for Excellence in Clinical Research (Trainee). Xiao and Oxentenko reported no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM ACG 2024
GLP-1 RAs Reduce Early-Onset CRC Risk in Patients With Type 2 Diabetes
PHILADELPHIA — according to the results of a retrospective study.
“This is the first large study to investigate the impact of GLP-1 RA use on EO-CRC risk,” principal investigator Temitope Olasehinde, MD, resident physician at the University Hospitals Cleveland Medical Center, Case Western Reserve University in Cleveland, Ohio, said in an interview.
The results indicate the GLP-1 RAs have a potentially protective role to play in combating EO-CRC, the incidence of which is notably rising in younger adults, with a corresponding increase in associated mortality.
Previous studies investigating the link between GLP-1 RAs and CRC did not capture patients aged younger than 50 years; thus, it was unknown if these results could be extrapolated to a younger age group, said Olasehinde.
The researcher presented the findings at the annual meeting of the American College of Gastroenterology.
Retrospective Database Analysis
Olasehinde and colleagues analyzed data from TriNetX, a large federated deidentified health research network, to identify patients (age ≤ 49 years) with diagnosed T2D subsequently prescribed antidiabetic medications who had not received a prior diagnosis of CRC. Additionally, patients were stratified on the basis of first-time GLP-1 RA use.
They identified 2,025,034 drug-naive patients with T2D; of these, 284,685 were subsequently prescribed GLP-1 RAs, and 1,740,349 remained in the non–GLP-1 RA cohort. Following propensity score matching, there were 86,186 patients in each cohort.
Patients who received GLP-1 RAs had significantly lower odds of developing EO-CRC than those who received non–GLP-1 RAs (0.6% vs 0.9%; P < .001; odds ratio [OR], 0.61; 95% CI, 0.54-068).
Furthermore, a sub-analysis revealed that patients who were obese and taking GLP-1 RAs had significantly lower odds of developing EO-CRC than patients who were obese but not taking GLP-1 RAs (0.7% vs 1.1%; P < .001; OR, 0.58; 95% CI, 0.50-067).
A Proposed Protective Effect
Although GLP-1 RAs are indicated for the treatment of T2D and obesity, recent evidence suggests that they may play a role in reducing the risk for CRC as well. This protective effect may be produced not only by addressing T2D and obesity — both important risk factors for CRC — but also via cellular mechanisms, Olasehinde noted.
“GLP-1 receptors are widely expressed throughout the gastrointestinal tract, with various effects on tissues in the stomach, small intestine, and colon,” she explained. Specifically, activation of these receptors in the proximal and distal colon promotes the release of “important factors that protect and facilitate healing of the intestinal epithelium” and “regulate the gut microbiome.”
This is particularly relevant in EO-CRC, she added, given its greater association with T2D and obesity, both factors that “have been shown to create dysbiosis in the gut microbiome and low-grade inflammation via release of free radicals/inflammatory cytokines.”
These results provide more evidence that EO-CRC “is clinically and molecularly distinct from late-onset colorectal cancer,” which is important for both clinicians and patients to understand, said Olasehinde.
“It is imperative that we are all aware of the specific signs and symptoms this population presents with and the implications of this diagnosis in younger age groups,” she added. “Patients should continue making informed dietary and lifestyle modifications/choices to help reduce the burden of EO-CRC.”
Hypothesis-Generating Results
Aasma Shaukat, MD, MPH, who was not affiliated with the research, called the results promising but — at this stage — primarily useful for stimulating future research.
"We do need more studies such as this to generate hypotheses that can be studied prospectively," Shaukat, professor of medicine and population health, and director of GI Outcomes Research at NYU Langone Health in New York City, told Medscape Medical News.
She referred to another study, published in JAMA Oncology, that also used the TriNetX research network, which showed that GLP-1 RAs were associated with reduced CRC risk in drug-naive patients with T2D.
Shaukat also noted that the current analysis has limitations that should be considered. "The study is retrospective, and confounding is a possibility,” she said.
“How the groups that did and did not receive GLP-1 RAs differ in other risk factors that could be the drivers of the cancers is not known. Whether cancers were detected through screening or symptoms, stage, and other features that may differ are not known. Finally, since we don’t know who did or did not have colonoscopy, undiagnosed cancers are not known," she explained.
Shaukat, who was the lead author of the ACG 2021 Colorectal Cancer Screening Guidelines, added that the field would benefit from studies providing "biological plausibility information, such as animal studies to understand how GLP-1 RAs may modulate risk of colon cancer; other population-based cohort studies on the incidence of colon cancer among GLP-1 RA users and non-users; and prospective trials on chemoprevention."
The study had no specific funding. Olasehinde reported no relevant financial relationships. Shaukat reported serving as a consultant for Freenome, Medtronic, and Motus GI, as well as an advisory board member for Iterative Scopes Inc.
A version of this article appeared on Medscape.com.
PHILADELPHIA — according to the results of a retrospective study.
“This is the first large study to investigate the impact of GLP-1 RA use on EO-CRC risk,” principal investigator Temitope Olasehinde, MD, resident physician at the University Hospitals Cleveland Medical Center, Case Western Reserve University in Cleveland, Ohio, said in an interview.
The results indicate the GLP-1 RAs have a potentially protective role to play in combating EO-CRC, the incidence of which is notably rising in younger adults, with a corresponding increase in associated mortality.
Previous studies investigating the link between GLP-1 RAs and CRC did not capture patients aged younger than 50 years; thus, it was unknown if these results could be extrapolated to a younger age group, said Olasehinde.
The researcher presented the findings at the annual meeting of the American College of Gastroenterology.
Retrospective Database Analysis
Olasehinde and colleagues analyzed data from TriNetX, a large federated deidentified health research network, to identify patients (age ≤ 49 years) with diagnosed T2D subsequently prescribed antidiabetic medications who had not received a prior diagnosis of CRC. Additionally, patients were stratified on the basis of first-time GLP-1 RA use.
They identified 2,025,034 drug-naive patients with T2D; of these, 284,685 were subsequently prescribed GLP-1 RAs, and 1,740,349 remained in the non–GLP-1 RA cohort. Following propensity score matching, there were 86,186 patients in each cohort.
Patients who received GLP-1 RAs had significantly lower odds of developing EO-CRC than those who received non–GLP-1 RAs (0.6% vs 0.9%; P < .001; odds ratio [OR], 0.61; 95% CI, 0.54-068).
Furthermore, a sub-analysis revealed that patients who were obese and taking GLP-1 RAs had significantly lower odds of developing EO-CRC than patients who were obese but not taking GLP-1 RAs (0.7% vs 1.1%; P < .001; OR, 0.58; 95% CI, 0.50-067).
A Proposed Protective Effect
Although GLP-1 RAs are indicated for the treatment of T2D and obesity, recent evidence suggests that they may play a role in reducing the risk for CRC as well. This protective effect may be produced not only by addressing T2D and obesity — both important risk factors for CRC — but also via cellular mechanisms, Olasehinde noted.
“GLP-1 receptors are widely expressed throughout the gastrointestinal tract, with various effects on tissues in the stomach, small intestine, and colon,” she explained. Specifically, activation of these receptors in the proximal and distal colon promotes the release of “important factors that protect and facilitate healing of the intestinal epithelium” and “regulate the gut microbiome.”
This is particularly relevant in EO-CRC, she added, given its greater association with T2D and obesity, both factors that “have been shown to create dysbiosis in the gut microbiome and low-grade inflammation via release of free radicals/inflammatory cytokines.”
These results provide more evidence that EO-CRC “is clinically and molecularly distinct from late-onset colorectal cancer,” which is important for both clinicians and patients to understand, said Olasehinde.
“It is imperative that we are all aware of the specific signs and symptoms this population presents with and the implications of this diagnosis in younger age groups,” she added. “Patients should continue making informed dietary and lifestyle modifications/choices to help reduce the burden of EO-CRC.”
Hypothesis-Generating Results
Aasma Shaukat, MD, MPH, who was not affiliated with the research, called the results promising but — at this stage — primarily useful for stimulating future research.
"We do need more studies such as this to generate hypotheses that can be studied prospectively," Shaukat, professor of medicine and population health, and director of GI Outcomes Research at NYU Langone Health in New York City, told Medscape Medical News.
She referred to another study, published in JAMA Oncology, that also used the TriNetX research network, which showed that GLP-1 RAs were associated with reduced CRC risk in drug-naive patients with T2D.
Shaukat also noted that the current analysis has limitations that should be considered. "The study is retrospective, and confounding is a possibility,” she said.
“How the groups that did and did not receive GLP-1 RAs differ in other risk factors that could be the drivers of the cancers is not known. Whether cancers were detected through screening or symptoms, stage, and other features that may differ are not known. Finally, since we don’t know who did or did not have colonoscopy, undiagnosed cancers are not known," she explained.
Shaukat, who was the lead author of the ACG 2021 Colorectal Cancer Screening Guidelines, added that the field would benefit from studies providing "biological plausibility information, such as animal studies to understand how GLP-1 RAs may modulate risk of colon cancer; other population-based cohort studies on the incidence of colon cancer among GLP-1 RA users and non-users; and prospective trials on chemoprevention."
The study had no specific funding. Olasehinde reported no relevant financial relationships. Shaukat reported serving as a consultant for Freenome, Medtronic, and Motus GI, as well as an advisory board member for Iterative Scopes Inc.
A version of this article appeared on Medscape.com.
PHILADELPHIA — according to the results of a retrospective study.
“This is the first large study to investigate the impact of GLP-1 RA use on EO-CRC risk,” principal investigator Temitope Olasehinde, MD, resident physician at the University Hospitals Cleveland Medical Center, Case Western Reserve University in Cleveland, Ohio, said in an interview.
The results indicate the GLP-1 RAs have a potentially protective role to play in combating EO-CRC, the incidence of which is notably rising in younger adults, with a corresponding increase in associated mortality.
Previous studies investigating the link between GLP-1 RAs and CRC did not capture patients aged younger than 50 years; thus, it was unknown if these results could be extrapolated to a younger age group, said Olasehinde.
The researcher presented the findings at the annual meeting of the American College of Gastroenterology.
Retrospective Database Analysis
Olasehinde and colleagues analyzed data from TriNetX, a large federated deidentified health research network, to identify patients (age ≤ 49 years) with diagnosed T2D subsequently prescribed antidiabetic medications who had not received a prior diagnosis of CRC. Additionally, patients were stratified on the basis of first-time GLP-1 RA use.
They identified 2,025,034 drug-naive patients with T2D; of these, 284,685 were subsequently prescribed GLP-1 RAs, and 1,740,349 remained in the non–GLP-1 RA cohort. Following propensity score matching, there were 86,186 patients in each cohort.
Patients who received GLP-1 RAs had significantly lower odds of developing EO-CRC than those who received non–GLP-1 RAs (0.6% vs 0.9%; P < .001; odds ratio [OR], 0.61; 95% CI, 0.54-068).
Furthermore, a sub-analysis revealed that patients who were obese and taking GLP-1 RAs had significantly lower odds of developing EO-CRC than patients who were obese but not taking GLP-1 RAs (0.7% vs 1.1%; P < .001; OR, 0.58; 95% CI, 0.50-067).
A Proposed Protective Effect
Although GLP-1 RAs are indicated for the treatment of T2D and obesity, recent evidence suggests that they may play a role in reducing the risk for CRC as well. This protective effect may be produced not only by addressing T2D and obesity — both important risk factors for CRC — but also via cellular mechanisms, Olasehinde noted.
“GLP-1 receptors are widely expressed throughout the gastrointestinal tract, with various effects on tissues in the stomach, small intestine, and colon,” she explained. Specifically, activation of these receptors in the proximal and distal colon promotes the release of “important factors that protect and facilitate healing of the intestinal epithelium” and “regulate the gut microbiome.”
This is particularly relevant in EO-CRC, she added, given its greater association with T2D and obesity, both factors that “have been shown to create dysbiosis in the gut microbiome and low-grade inflammation via release of free radicals/inflammatory cytokines.”
These results provide more evidence that EO-CRC “is clinically and molecularly distinct from late-onset colorectal cancer,” which is important for both clinicians and patients to understand, said Olasehinde.
“It is imperative that we are all aware of the specific signs and symptoms this population presents with and the implications of this diagnosis in younger age groups,” she added. “Patients should continue making informed dietary and lifestyle modifications/choices to help reduce the burden of EO-CRC.”
Hypothesis-Generating Results
Aasma Shaukat, MD, MPH, who was not affiliated with the research, called the results promising but — at this stage — primarily useful for stimulating future research.
"We do need more studies such as this to generate hypotheses that can be studied prospectively," Shaukat, professor of medicine and population health, and director of GI Outcomes Research at NYU Langone Health in New York City, told Medscape Medical News.
She referred to another study, published in JAMA Oncology, that also used the TriNetX research network, which showed that GLP-1 RAs were associated with reduced CRC risk in drug-naive patients with T2D.
Shaukat also noted that the current analysis has limitations that should be considered. "The study is retrospective, and confounding is a possibility,” she said.
“How the groups that did and did not receive GLP-1 RAs differ in other risk factors that could be the drivers of the cancers is not known. Whether cancers were detected through screening or symptoms, stage, and other features that may differ are not known. Finally, since we don’t know who did or did not have colonoscopy, undiagnosed cancers are not known," she explained.
Shaukat, who was the lead author of the ACG 2021 Colorectal Cancer Screening Guidelines, added that the field would benefit from studies providing "biological plausibility information, such as animal studies to understand how GLP-1 RAs may modulate risk of colon cancer; other population-based cohort studies on the incidence of colon cancer among GLP-1 RA users and non-users; and prospective trials on chemoprevention."
The study had no specific funding. Olasehinde reported no relevant financial relationships. Shaukat reported serving as a consultant for Freenome, Medtronic, and Motus GI, as well as an advisory board member for Iterative Scopes Inc.
A version of this article appeared on Medscape.com.
FROM ACG 2024
AI Tool Helps Detect, Differentiate Pancreatic Lesions During Endoscopic Ultrasound
PHILADELPHIA —
This was a transatlantic collaborative effort involving researchers in Portugal, Spain, the United States, and Brazil, and the AI tool “works on different platforms and different devices,” Miguel Mascarenhas, MD, PhD, with Centro Hospitalar Universitário de São João, Porto, Portugal, said in a presentation at the annual meeting of the American College of Gastroenterology.
Mascarenhas noted that pancreatic cystic lesions (PCLs) are a common incidental finding during imaging and are differentiated by whether they’re mucinous PCLs (M-PCLs) or non-mucinous PCLs (NM-PCLs). The malignancy risk is almost exclusive of PCL with a mucinous phenotype.
Pancreatic solid lesions are also prevalent, and differentiation is challenging. Pancreatic ductal adenocarcinoma (P-DAC) is the most common pancreatic solid lesion and has a poor prognosis because of late-stage disease at diagnosis. Pancreatic neuroendocrine tumors (P-NETs) are less common but have malignant potential.
EUS is the “gold standard” for pancreatic lesion evaluation, but its diagnostic accuracy is suboptimal, particularly for lesions < 10 mm, Mascarenhas noted.
With an eye toward improving diagnostic accuracy, he and colleagues developed a convolutional neural network for detecting and differentiating cystic (M-PCL and NM-PCL) and solid (P-DAC and P-NET) pancreatic lesions.
They leveraged data from 378 EUS exams with 126,000 still images — 19,528 M-PCL, 8175 NM-PCL, 64,286 P-DAC, 29,153 P-NET, and 4858 normal pancreas images.
The AI tool demonstrated 99.1% accuracy for identifying normal pancreatic tissue, and it showed 99% and 99.8% accuracy for M-PCL and NM-PCL, respectively.
For pancreatic solid lesions, P-DAC and P-NET were distinguished with 94% accuracy, with 98.7% and 83.6% sensitivity for P-DAC and P-NET, respectively.
Real-Time Validation Next
“AI is delivering promising results throughout medicine, but particularly in gastroenterology, which is one of the most fertile areas of AI research. This comes mostly from the deployment of deep-learning models, most of them convolutional neural networks, which are highly efficient for image analysis,” Mascarenhas told attendees.
This is the “first worldwide convolutional neural network” capable of detecting and differentiating both cystic and solid pancreatic lesions. The use of a large dataset from four centers in two continents helps minimize the impact of demographic bias, Mascarenhas added.
The study is based on still images, not full videos, he noted. As a next step, the team is conducting a multicenter study focused on real-time clinical validation of the model during EUS procedures.
“AI has the potential to improve the diagnostic accuracy of endoscopic ultrasound. We’re just on the tip of the iceberg. There is enormous potential to harness AI, and we welcome all the groups that might want to join our research,” Mascarenhas said.
Brennan Spiegel, MD, MSHS, AGAF, director of Health Services Research at Cedars-Sinai Medical Center, Los Angeles, who wasn’t involved in the study, is optimistic about emerging applications for AI.
“AI holds incredible promise in gastroenterology, especially for diagnosing complex pancreatic lesions where early, accurate differentiation can be lifesaving,” Spiegel said in an interview.
“This study’s high accuracy across diverse datasets is encouraging; however, as a retrospective analysis, it leaves the real-time clinical impact still to be proven. Prospective studies will be essential to confirm AI’s role in enhancing our diagnostic capabilities,” Spiegel cautioned.
“More generally, AI is rapidly transforming gastroenterology by enhancing our ability to detect, differentiate, and monitor conditions with unprecedented precision. From improving early cancer detection to guiding complex diagnostic procedures, AI stands to become an invaluable tool that complements clinical expertise. As we refine these technologies, the potential for AI to elevate both diagnostic accuracy and patient outcomes in GI is truly remarkable,” Spiegel said.
The study had no specific funding. Mascarenhas and Spiegel have declared no conflicts of interest.
A version of this article appeared on Medscape.com.
PHILADELPHIA —
This was a transatlantic collaborative effort involving researchers in Portugal, Spain, the United States, and Brazil, and the AI tool “works on different platforms and different devices,” Miguel Mascarenhas, MD, PhD, with Centro Hospitalar Universitário de São João, Porto, Portugal, said in a presentation at the annual meeting of the American College of Gastroenterology.
Mascarenhas noted that pancreatic cystic lesions (PCLs) are a common incidental finding during imaging and are differentiated by whether they’re mucinous PCLs (M-PCLs) or non-mucinous PCLs (NM-PCLs). The malignancy risk is almost exclusive of PCL with a mucinous phenotype.
Pancreatic solid lesions are also prevalent, and differentiation is challenging. Pancreatic ductal adenocarcinoma (P-DAC) is the most common pancreatic solid lesion and has a poor prognosis because of late-stage disease at diagnosis. Pancreatic neuroendocrine tumors (P-NETs) are less common but have malignant potential.
EUS is the “gold standard” for pancreatic lesion evaluation, but its diagnostic accuracy is suboptimal, particularly for lesions < 10 mm, Mascarenhas noted.
With an eye toward improving diagnostic accuracy, he and colleagues developed a convolutional neural network for detecting and differentiating cystic (M-PCL and NM-PCL) and solid (P-DAC and P-NET) pancreatic lesions.
They leveraged data from 378 EUS exams with 126,000 still images — 19,528 M-PCL, 8175 NM-PCL, 64,286 P-DAC, 29,153 P-NET, and 4858 normal pancreas images.
The AI tool demonstrated 99.1% accuracy for identifying normal pancreatic tissue, and it showed 99% and 99.8% accuracy for M-PCL and NM-PCL, respectively.
For pancreatic solid lesions, P-DAC and P-NET were distinguished with 94% accuracy, with 98.7% and 83.6% sensitivity for P-DAC and P-NET, respectively.
Real-Time Validation Next
“AI is delivering promising results throughout medicine, but particularly in gastroenterology, which is one of the most fertile areas of AI research. This comes mostly from the deployment of deep-learning models, most of them convolutional neural networks, which are highly efficient for image analysis,” Mascarenhas told attendees.
This is the “first worldwide convolutional neural network” capable of detecting and differentiating both cystic and solid pancreatic lesions. The use of a large dataset from four centers in two continents helps minimize the impact of demographic bias, Mascarenhas added.
The study is based on still images, not full videos, he noted. As a next step, the team is conducting a multicenter study focused on real-time clinical validation of the model during EUS procedures.
“AI has the potential to improve the diagnostic accuracy of endoscopic ultrasound. We’re just on the tip of the iceberg. There is enormous potential to harness AI, and we welcome all the groups that might want to join our research,” Mascarenhas said.
Brennan Spiegel, MD, MSHS, AGAF, director of Health Services Research at Cedars-Sinai Medical Center, Los Angeles, who wasn’t involved in the study, is optimistic about emerging applications for AI.
“AI holds incredible promise in gastroenterology, especially for diagnosing complex pancreatic lesions where early, accurate differentiation can be lifesaving,” Spiegel said in an interview.
“This study’s high accuracy across diverse datasets is encouraging; however, as a retrospective analysis, it leaves the real-time clinical impact still to be proven. Prospective studies will be essential to confirm AI’s role in enhancing our diagnostic capabilities,” Spiegel cautioned.
“More generally, AI is rapidly transforming gastroenterology by enhancing our ability to detect, differentiate, and monitor conditions with unprecedented precision. From improving early cancer detection to guiding complex diagnostic procedures, AI stands to become an invaluable tool that complements clinical expertise. As we refine these technologies, the potential for AI to elevate both diagnostic accuracy and patient outcomes in GI is truly remarkable,” Spiegel said.
The study had no specific funding. Mascarenhas and Spiegel have declared no conflicts of interest.
A version of this article appeared on Medscape.com.
PHILADELPHIA —
This was a transatlantic collaborative effort involving researchers in Portugal, Spain, the United States, and Brazil, and the AI tool “works on different platforms and different devices,” Miguel Mascarenhas, MD, PhD, with Centro Hospitalar Universitário de São João, Porto, Portugal, said in a presentation at the annual meeting of the American College of Gastroenterology.
Mascarenhas noted that pancreatic cystic lesions (PCLs) are a common incidental finding during imaging and are differentiated by whether they’re mucinous PCLs (M-PCLs) or non-mucinous PCLs (NM-PCLs). The malignancy risk is almost exclusive of PCL with a mucinous phenotype.
Pancreatic solid lesions are also prevalent, and differentiation is challenging. Pancreatic ductal adenocarcinoma (P-DAC) is the most common pancreatic solid lesion and has a poor prognosis because of late-stage disease at diagnosis. Pancreatic neuroendocrine tumors (P-NETs) are less common but have malignant potential.
EUS is the “gold standard” for pancreatic lesion evaluation, but its diagnostic accuracy is suboptimal, particularly for lesions < 10 mm, Mascarenhas noted.
With an eye toward improving diagnostic accuracy, he and colleagues developed a convolutional neural network for detecting and differentiating cystic (M-PCL and NM-PCL) and solid (P-DAC and P-NET) pancreatic lesions.
They leveraged data from 378 EUS exams with 126,000 still images — 19,528 M-PCL, 8175 NM-PCL, 64,286 P-DAC, 29,153 P-NET, and 4858 normal pancreas images.
The AI tool demonstrated 99.1% accuracy for identifying normal pancreatic tissue, and it showed 99% and 99.8% accuracy for M-PCL and NM-PCL, respectively.
For pancreatic solid lesions, P-DAC and P-NET were distinguished with 94% accuracy, with 98.7% and 83.6% sensitivity for P-DAC and P-NET, respectively.
Real-Time Validation Next
“AI is delivering promising results throughout medicine, but particularly in gastroenterology, which is one of the most fertile areas of AI research. This comes mostly from the deployment of deep-learning models, most of them convolutional neural networks, which are highly efficient for image analysis,” Mascarenhas told attendees.
This is the “first worldwide convolutional neural network” capable of detecting and differentiating both cystic and solid pancreatic lesions. The use of a large dataset from four centers in two continents helps minimize the impact of demographic bias, Mascarenhas added.
The study is based on still images, not full videos, he noted. As a next step, the team is conducting a multicenter study focused on real-time clinical validation of the model during EUS procedures.
“AI has the potential to improve the diagnostic accuracy of endoscopic ultrasound. We’re just on the tip of the iceberg. There is enormous potential to harness AI, and we welcome all the groups that might want to join our research,” Mascarenhas said.
Brennan Spiegel, MD, MSHS, AGAF, director of Health Services Research at Cedars-Sinai Medical Center, Los Angeles, who wasn’t involved in the study, is optimistic about emerging applications for AI.
“AI holds incredible promise in gastroenterology, especially for diagnosing complex pancreatic lesions where early, accurate differentiation can be lifesaving,” Spiegel said in an interview.
“This study’s high accuracy across diverse datasets is encouraging; however, as a retrospective analysis, it leaves the real-time clinical impact still to be proven. Prospective studies will be essential to confirm AI’s role in enhancing our diagnostic capabilities,” Spiegel cautioned.
“More generally, AI is rapidly transforming gastroenterology by enhancing our ability to detect, differentiate, and monitor conditions with unprecedented precision. From improving early cancer detection to guiding complex diagnostic procedures, AI stands to become an invaluable tool that complements clinical expertise. As we refine these technologies, the potential for AI to elevate both diagnostic accuracy and patient outcomes in GI is truly remarkable,” Spiegel said.
The study had no specific funding. Mascarenhas and Spiegel have declared no conflicts of interest.
A version of this article appeared on Medscape.com.
FROM ACG 2024
Is Being ‘Manly’ a Threat to a Man’s Health?
When my normally adorable cat Biscuit bit my ankle in a playful stalking exercise gone wrong, I washed it with soap and some rubbing alcohol, slapped on a Band-Aid, and went about my day.
The next morning, when it was swollen, I told myself it was probably just a hematoma and went about my day.
The next day, when the swelling had increased and red lines started creeping up my leg, I called my doctor. Long story short, I ended up hospitalized for intravenous antibiotics.
This is all to say that, yes, I’m sort of an idiot, but also to introduce the idea that maybe I minimized my very obvious lymphangitis because I am a man.
This week, we have empirical evidence that men downplay their medical symptoms — and that manlier men downplay them even more.

I’m going to talk about a study that links manliness (or, scientifically speaking, “male gender expressivity”) to medical diagnoses that are based on hard evidence and medical diagnoses that are based on self-report. You see where this is going but I want to walk you through the methods here because they are fairly interesting.
This study used data from the US National Longitudinal Study of Adolescent to Adult Health. This study enrolled 20,000 adolescents who were in grades 7-12 in the 1994-1995 school year and has been following them ever since — about 30 years so far.
The authors wanted to link early gender roles to long-term outcomes, so they cut that 20,000 number down to the 4230 males in the group who had complete follow-up.
Now comes the first interesting question. How do you quantify the “male gender expressivity” of boys in 7th-12th grade? There was no survey item that asked them how masculine or manly they felt. What the authors did was look at the surveys that were administered and identify the questions on those surveys where boys and girls gave the most disparate answers. I have some examples here. 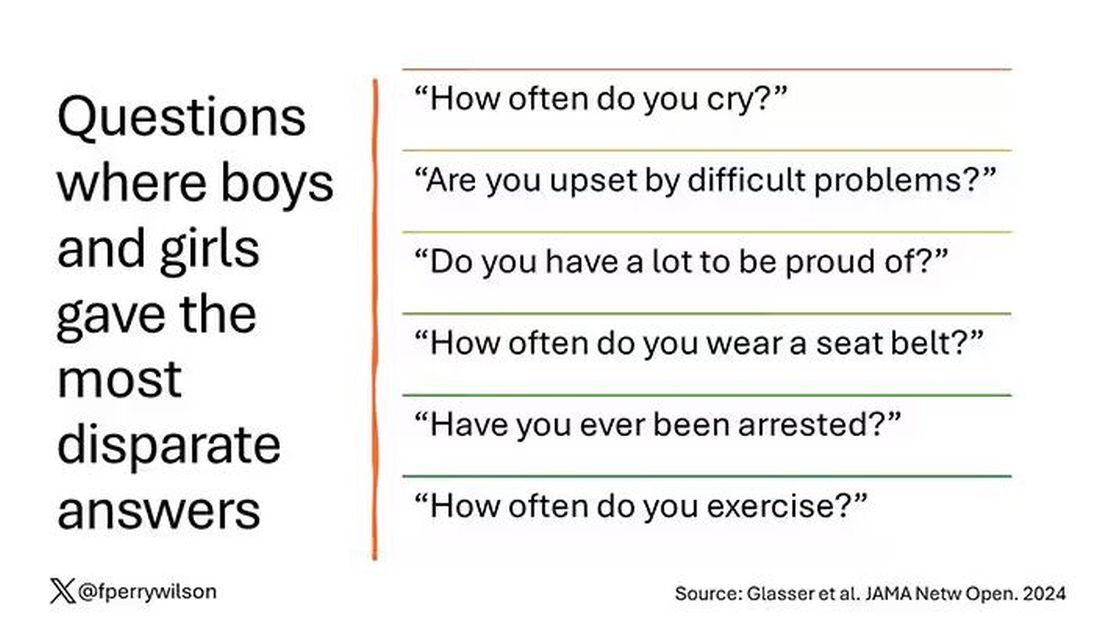
Some of these questions make sense when it comes to gender expressivity: “How often do you cry?” for example, has a lot of validity for the social construct that is gender. But some questions where boys and girls gave very different answers — like “How often do you exercise?” — don’t quite fit that mold. Regardless, this structure allowed the researchers to take individual kids’ responses to these questions and combine them into what amounts to a manliness score — how much their answers aligned with the typical male answer.
The score was established in adolescence — which is interesting because I’m sure some of this stuff may change over time — but notable because adolescence is where many gender roles develop.
Now we can fast-forward 30 years and see how these manliness scores link to various outcomes. The authors were interested in fairly common diseases: diabetes, hypertension, and hyperlipidemia.
Let’s start simply. Are males with higher gender expressivity in adolescence more or less likely to have these diseases in the future?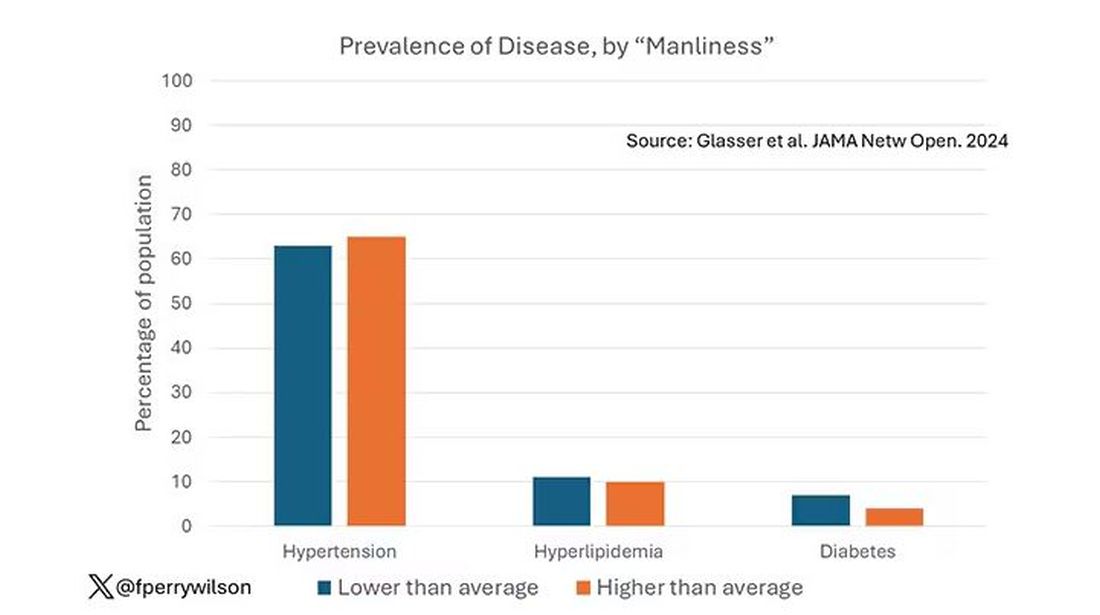
Not really. Those above the average in male gender expressivity had similar rates of hypertension and hyperlipidemia as those below the median. They were actually a bit less likely to have diabetes.
But that’s not what’s really interesting here.
I told you that there was no difference in the rate of hypertension among those with high vs low male gender expressivity. But there was a significant difference in their answer to the question “Do you have hypertension?” The same was seen for hyperlipidemia. In other words, those with higher manliness scores are less likely to admit (or perhaps know) that they have a particular disease.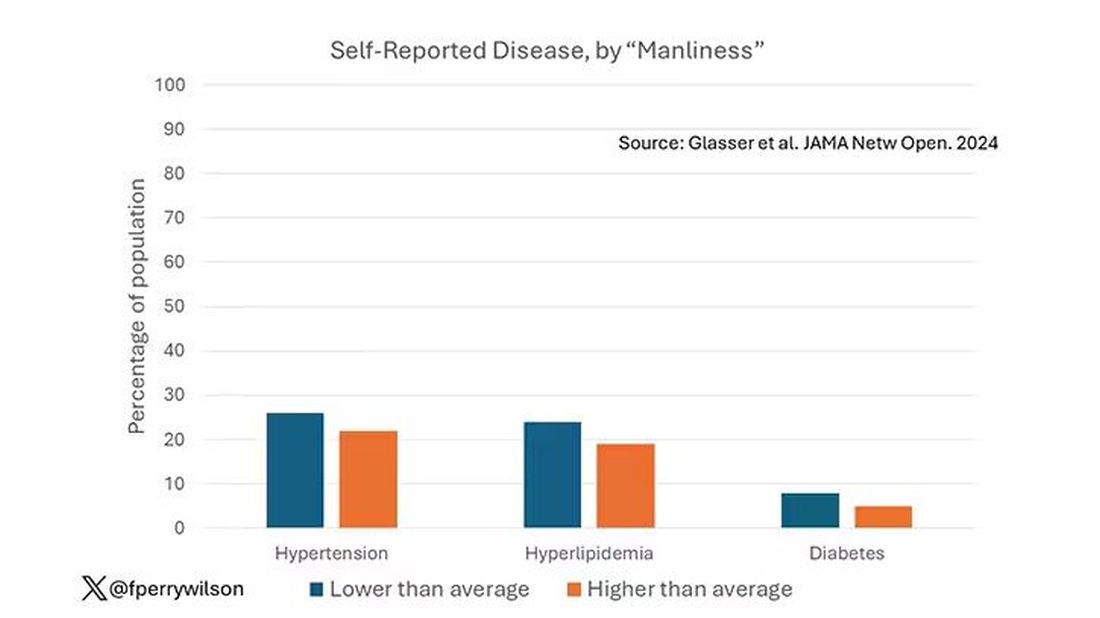
You can see the relationship across the manliness spectrum here in a series of adjusted models. The x-axis is the male gender expressivity score, and the y-axis is the percentage of people who report having the disease that we know they have based on the actual laboratory tests or vital sign measurements. As manliness increases, the self-report of a given disease decreases.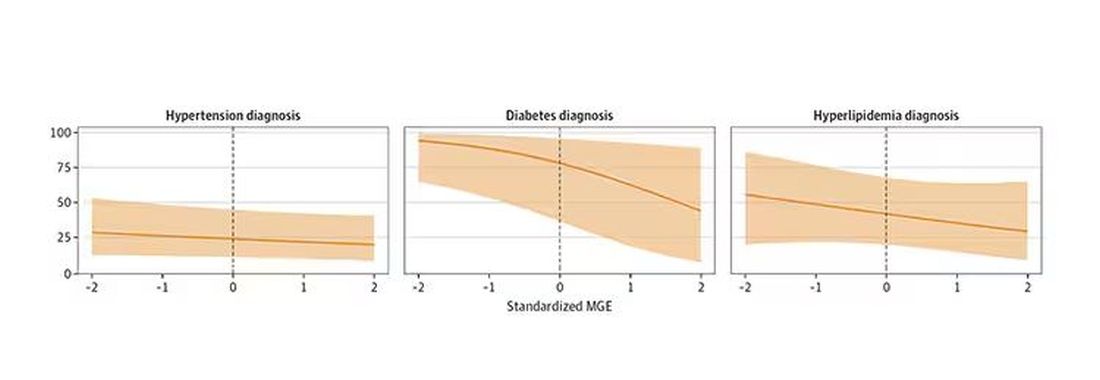
There are some important consequences of this systematic denial. Specifically, men with the diseases of interest who have higher male gender expressivity are less likely to get treatment. And, as we all know, the lack of treatment of something like hypertension puts people at risk for bad downstream outcomes.
Putting this all together, I’m not that surprised. Society trains boys from a young age to behave in certain ways: to hide emotions, to eschew vulnerability, to not complain when we are hurt. And those lessons can persist into later life. Whether the disease that strikes is hypertension or Pasteurella multocida from a slightly psychotic house cat, men are more likely to ignore it, to their detriment. 
So, gents, be brave. Get your blood tests and check your blood pressure. If there’s something wrong, admit it, and fix it. After all, fixing problems — that’s a manly thing, right?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
When my normally adorable cat Biscuit bit my ankle in a playful stalking exercise gone wrong, I washed it with soap and some rubbing alcohol, slapped on a Band-Aid, and went about my day.
The next morning, when it was swollen, I told myself it was probably just a hematoma and went about my day.
The next day, when the swelling had increased and red lines started creeping up my leg, I called my doctor. Long story short, I ended up hospitalized for intravenous antibiotics.
This is all to say that, yes, I’m sort of an idiot, but also to introduce the idea that maybe I minimized my very obvious lymphangitis because I am a man.
This week, we have empirical evidence that men downplay their medical symptoms — and that manlier men downplay them even more.
I’m going to talk about a study that links manliness (or, scientifically speaking, “male gender expressivity”) to medical diagnoses that are based on hard evidence and medical diagnoses that are based on self-report. You see where this is going but I want to walk you through the methods here because they are fairly interesting.
This study used data from the US National Longitudinal Study of Adolescent to Adult Health. This study enrolled 20,000 adolescents who were in grades 7-12 in the 1994-1995 school year and has been following them ever since — about 30 years so far.
The authors wanted to link early gender roles to long-term outcomes, so they cut that 20,000 number down to the 4230 males in the group who had complete follow-up.
Now comes the first interesting question. How do you quantify the “male gender expressivity” of boys in 7th-12th grade? There was no survey item that asked them how masculine or manly they felt. What the authors did was look at the surveys that were administered and identify the questions on those surveys where boys and girls gave the most disparate answers. I have some examples here.
Some of these questions make sense when it comes to gender expressivity: “How often do you cry?” for example, has a lot of validity for the social construct that is gender. But some questions where boys and girls gave very different answers — like “How often do you exercise?” — don’t quite fit that mold. Regardless, this structure allowed the researchers to take individual kids’ responses to these questions and combine them into what amounts to a manliness score — how much their answers aligned with the typical male answer.
The score was established in adolescence — which is interesting because I’m sure some of this stuff may change over time — but notable because adolescence is where many gender roles develop.
Now we can fast-forward 30 years and see how these manliness scores link to various outcomes. The authors were interested in fairly common diseases: diabetes, hypertension, and hyperlipidemia.
Let’s start simply. Are males with higher gender expressivity in adolescence more or less likely to have these diseases in the future?
Not really. Those above the average in male gender expressivity had similar rates of hypertension and hyperlipidemia as those below the median. They were actually a bit less likely to have diabetes.
But that’s not what’s really interesting here.
I told you that there was no difference in the rate of hypertension among those with high vs low male gender expressivity. But there was a significant difference in their answer to the question “Do you have hypertension?” The same was seen for hyperlipidemia. In other words, those with higher manliness scores are less likely to admit (or perhaps know) that they have a particular disease.
You can see the relationship across the manliness spectrum here in a series of adjusted models. The x-axis is the male gender expressivity score, and the y-axis is the percentage of people who report having the disease that we know they have based on the actual laboratory tests or vital sign measurements. As manliness increases, the self-report of a given disease decreases.
There are some important consequences of this systematic denial. Specifically, men with the diseases of interest who have higher male gender expressivity are less likely to get treatment. And, as we all know, the lack of treatment of something like hypertension puts people at risk for bad downstream outcomes.
Putting this all together, I’m not that surprised. Society trains boys from a young age to behave in certain ways: to hide emotions, to eschew vulnerability, to not complain when we are hurt. And those lessons can persist into later life. Whether the disease that strikes is hypertension or Pasteurella multocida from a slightly psychotic house cat, men are more likely to ignore it, to their detriment.
So, gents, be brave. Get your blood tests and check your blood pressure. If there’s something wrong, admit it, and fix it. After all, fixing problems — that’s a manly thing, right?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
When my normally adorable cat Biscuit bit my ankle in a playful stalking exercise gone wrong, I washed it with soap and some rubbing alcohol, slapped on a Band-Aid, and went about my day.
The next morning, when it was swollen, I told myself it was probably just a hematoma and went about my day.
The next day, when the swelling had increased and red lines started creeping up my leg, I called my doctor. Long story short, I ended up hospitalized for intravenous antibiotics.
This is all to say that, yes, I’m sort of an idiot, but also to introduce the idea that maybe I minimized my very obvious lymphangitis because I am a man.
This week, we have empirical evidence that men downplay their medical symptoms — and that manlier men downplay them even more.
I’m going to talk about a study that links manliness (or, scientifically speaking, “male gender expressivity”) to medical diagnoses that are based on hard evidence and medical diagnoses that are based on self-report. You see where this is going but I want to walk you through the methods here because they are fairly interesting.
This study used data from the US National Longitudinal Study of Adolescent to Adult Health. This study enrolled 20,000 adolescents who were in grades 7-12 in the 1994-1995 school year and has been following them ever since — about 30 years so far.
The authors wanted to link early gender roles to long-term outcomes, so they cut that 20,000 number down to the 4230 males in the group who had complete follow-up.
Now comes the first interesting question. How do you quantify the “male gender expressivity” of boys in 7th-12th grade? There was no survey item that asked them how masculine or manly they felt. What the authors did was look at the surveys that were administered and identify the questions on those surveys where boys and girls gave the most disparate answers. I have some examples here.
Some of these questions make sense when it comes to gender expressivity: “How often do you cry?” for example, has a lot of validity for the social construct that is gender. But some questions where boys and girls gave very different answers — like “How often do you exercise?” — don’t quite fit that mold. Regardless, this structure allowed the researchers to take individual kids’ responses to these questions and combine them into what amounts to a manliness score — how much their answers aligned with the typical male answer.
The score was established in adolescence — which is interesting because I’m sure some of this stuff may change over time — but notable because adolescence is where many gender roles develop.
Now we can fast-forward 30 years and see how these manliness scores link to various outcomes. The authors were interested in fairly common diseases: diabetes, hypertension, and hyperlipidemia.
Let’s start simply. Are males with higher gender expressivity in adolescence more or less likely to have these diseases in the future?
Not really. Those above the average in male gender expressivity had similar rates of hypertension and hyperlipidemia as those below the median. They were actually a bit less likely to have diabetes.
But that’s not what’s really interesting here.
I told you that there was no difference in the rate of hypertension among those with high vs low male gender expressivity. But there was a significant difference in their answer to the question “Do you have hypertension?” The same was seen for hyperlipidemia. In other words, those with higher manliness scores are less likely to admit (or perhaps know) that they have a particular disease.
You can see the relationship across the manliness spectrum here in a series of adjusted models. The x-axis is the male gender expressivity score, and the y-axis is the percentage of people who report having the disease that we know they have based on the actual laboratory tests or vital sign measurements. As manliness increases, the self-report of a given disease decreases.
There are some important consequences of this systematic denial. Specifically, men with the diseases of interest who have higher male gender expressivity are less likely to get treatment. And, as we all know, the lack of treatment of something like hypertension puts people at risk for bad downstream outcomes.
Putting this all together, I’m not that surprised. Society trains boys from a young age to behave in certain ways: to hide emotions, to eschew vulnerability, to not complain when we are hurt. And those lessons can persist into later life. Whether the disease that strikes is hypertension or Pasteurella multocida from a slightly psychotic house cat, men are more likely to ignore it, to their detriment.
So, gents, be brave. Get your blood tests and check your blood pressure. If there’s something wrong, admit it, and fix it. After all, fixing problems — that’s a manly thing, right?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Thyroid Cancer Overdiagnosis Continues Despite Cautions
according to a recently published global study.
The proportion of thyroid cancer cases attributable to overdiagnosis globally was higher in women (78%) than in men (68%), with this rate varying substantially across countries, wrote Mengmeng Li, PhD, of the Sun Yat-sen University Cancer Center, Guangzhou, China, and coauthors in an October paper in The Lancet Diabetes & Endocrinology.
Overdiagnosis refers to the diagnosis of lesions that would not cause symptoms and that would not progress, if left alone.
Increased testing for thyroid cancer, fueled in large part by the expansion of imaging technologies and progressively more intense and disorganized scrutiny of the thyroid, led many people to be treated for often indolent lesions, exposing them to potential side effects as well as financial and emotional distress.
Li and coauthors estimate that more than 1.7 million people might have been overdiagnosed between 2013 and 2017 in 63 countries.
“Overdiagnosis clearly emerged in some high-resource countries with private-based health systems in which access to healthcare overrules regulatory controls (eg, in the USA) and in some high-quality public health systems with easy and broad access to thyroid gland diagnostic examinations (eg, in Canada),” Li and coauthors wrote. “Conversely, thyroid cancer is less commonly diagnosed in those countries in which access to diagnosis is guided by strong regulatory rules (eg, in Nordic countries).”
Their study drew from almost 40 years of research, including the latest available data from the World Health Organization’s International Agency for Research on Cancer’s (IARC’s) Global Cancer Observatory. Li and coauthors examined patterns in the time trends of thyroid cancer, mortality data, and trends in diagnosis of thyroid cancer before testing became common in many nations.
This approach is needed in estimating overdiagnosis, where it’s not possible to see what’s happening on a case-by-case level, Salvatore Vaccarella, PhD, a scientist at IARC’s Cancer Surveillance Branch, said in an interview.
Researchers can’t tell whether an individual’s detected early-stage cancers would have remained indolent for years or eventually would have put their life at risk, he said. Instead, the patterns emerge through larger studies of the reported cases of cancer like thyroid tumors and then looking at separate datasets on mortality.
“We can only see that as a big phenomenon when we look at population-based data,” Vaccarella said.
Persisting Problem
Recognition of the harms of overdiagnosis has resulted in some reduction of the incidence of thyroid cancer in the United States, Li and coauthors wrote. After adjusting for age, incidence has fallen from 19 per 100,000 women in 2013 to 16 per 100,000 women in 2017. The proportion of thyroid cancer attributed to overdiagnosis has dropped from 76% to 68% in the country.
The paper adds to the evidence suggesting that the rise in screening has not changed mortality rates for thyroid cancer. For example, Li and coauthors reported seeing “a small decrease in thyroid cancer mortality rates over time in some European countries, but this decline (less than 1 per 100,000 women) is marginal compared with the increases in incidence (reaching around 100 per 100,000 women).”
“Moreover, previous data show that the downward mortality trends had begun before the wide use of ultrasonography for early detection and that period and birth cohort effects have been declining, probably due to treatment advances and reduced prevalence of risk factors, such as the reduction in iodine deficiency,” they wrote.
In an interview, Amanda Davis, MD, of AnMed, a nonprofit health system based in Anderson, South Carolina, said the new paper from Li and Vaccarella provides further evidence for a cautious approach to thyroid nodules given concerns about overdiagnosis.
If early detection of cancer via discovery of thyroid nodules actually helped patients, mortality rates would have dropped with expansion of screening and the resulting diagnoses, said Davis, who is an associate program director at AnMed’s family medicine residency program and affiliate professor at the Medical University of South Carolina, Charleston.
In many cases, people learn they have thyroid lesions after being tested for other conditions such as ultrasound done on carotid arteries to check for stroke risk. The most common form of thyroid cancer is the papillary form. Papillary thyroid cancer tends to be slow growing, carries a low risk for distant metastasis, and in many cases poses little risk. Some small (< 1 cm) papillary thyroid cancers can be monitored with active surveillance as opposed to thyroid lobectomy.
“So just finding more nodules incidentally or through screening ultrasound and even finding more papillary cancers via these methods does not make people healthier or decrease mortality,” Davis said.
“So just finding more things and even finding more papillary cancers does not increase our ability to treat people and keep them alive longer,” Davis said.
The 5-year survival rate for thyroid cancer overall is 98.1% and varies from 99.9% for localized disease to 55.3% for distant disease, the US Preventive Services Task Force (USPSTF) said in a 2017 publication in JAMA. The task force that year gave a “D” rating on screening of asymptomatic people for thyroid cancer. That means there’s moderate certainty that screening for thyroid cancer in asymptomatic persons results in harms that outweigh the benefits. The decision to give this “D” rating meant this screening is not recommended. That’s still the panel’s view.
“You can think of it as a “D” for ‘don’t screen for thyroid cancer,’ ” in people who present no symptoms of this illness, John Wong, MD, the vice chair of the USPSTF, said in an interview.
In primary care, the challenge is assessing thyroid nodules detected when people undergo testing for another reason, such as an ultrasound of the carotid artery to check for stroke risk.
Thyroid nodules can be detected by ultrasonography in up to 68% of the general population, reported a study in American Family Physician. Nodules with suspicious features or ≥ 1 cm require fine needle aspiration. The Bethesda System for Reporting Thyroid Cytopathology can be used to classify samples, with molecular testing applied to guide treatment when fine needle aspiration yields an indeterminate result.
New Thinking on Thyroid Cancer
There’s been a shift in recent years in the approach to how physicians should proceed if certain kinds of thyroid cancer are detected, Cari M. Kitahara, PhD, of the National Cancer Institute noted in a comment accompanying the Li paper.
“Clinicians need to be judicious in the use of thyroid ultrasonography, the diagnostic follow-up of incidentally detected thyroid nodules, and determining the optimal course of treatment,” Kitahara wrote. “For low-risk and incidentally detected tumors, strong consideration should be given to less intensive treatment options (eg, lobectomy, delayed treatment, and active surveillance).”
The American Thyroid Association guidelines encourage de-escalation of treatment for low-risk papillary thyroid carcinoma up to 4 cm.
Physicians often need to make clear to patients how a diagnosis of low-risk papillary thyroid cancer differs from other oncology diagnoses, R. Michael Tuttle, MD, of Memorial Sloan Kettering Cancer Center, New York City, said in an interview.
“I’ll frequently say that everything you’ve ever learned about cancer, you need to forget,” Tuttle said.
Some patients will mistakenly think any cancer diagnosis is a likely death sentence, meaning they should rush to get aggressive treatment. Tuttle has been a leader for many years in efforts in advancing active surveillance as an option for certain people with low-risk thyroid cancer.
“I often start my consultation by saying: ‘We’re going to choose between two right answers here. One right answer is watching right. One right answer is going to surgery,’ ” Tuttle said.
Patients with low-risk thyroid cancer tend to fall into two camps, with maximalists likely to seek quick treatment and minimalists more inclined for surveillance if that’s an option for them, Tuttle said. As opinions have shifted within the medical community about approaches to low-risk thyroid cancer, there’s also been some growing awareness among the public about thyroid overdiagnosis.
“Ten or 15 years ago, people thought we were crazy” to consider active surveillance as an option for low-risk thyroid cancers,” Tuttle said. “Now we have swung, at least in some of the public opinion, to this recognition that every little speck of cancer doesn’t need to be immediately taken out of your body.”
Some patients express regret about having learned that they have low-risk thyroid cancer, Tuttle said.
“Over the last 5 years, it’s not uncommon for patients to ask me, ‘Is this one of those that needs to be treated now, or is this one of those that we wish we would have never found?’ Or people will say, ‘My doctor talked me into an ultrasound, I didn’t want it’ or ‘I had a car wreck, and I found this nodule and I wished I had never found it.’ ”
This study from Li and coauthors was funded by the National Natural Science Foundation of China, the Guangdong Basic and Applied Basic Research Foundation, the Young Talents Program of Sun Yat-sen University Cancer Center, the Italian Association for Cancer Research, and the Italian Ministry of Health. Davis and Tuttle had no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
according to a recently published global study.
The proportion of thyroid cancer cases attributable to overdiagnosis globally was higher in women (78%) than in men (68%), with this rate varying substantially across countries, wrote Mengmeng Li, PhD, of the Sun Yat-sen University Cancer Center, Guangzhou, China, and coauthors in an October paper in The Lancet Diabetes & Endocrinology.
Overdiagnosis refers to the diagnosis of lesions that would not cause symptoms and that would not progress, if left alone.
Increased testing for thyroid cancer, fueled in large part by the expansion of imaging technologies and progressively more intense and disorganized scrutiny of the thyroid, led many people to be treated for often indolent lesions, exposing them to potential side effects as well as financial and emotional distress.
Li and coauthors estimate that more than 1.7 million people might have been overdiagnosed between 2013 and 2017 in 63 countries.
“Overdiagnosis clearly emerged in some high-resource countries with private-based health systems in which access to healthcare overrules regulatory controls (eg, in the USA) and in some high-quality public health systems with easy and broad access to thyroid gland diagnostic examinations (eg, in Canada),” Li and coauthors wrote. “Conversely, thyroid cancer is less commonly diagnosed in those countries in which access to diagnosis is guided by strong regulatory rules (eg, in Nordic countries).”
Their study drew from almost 40 years of research, including the latest available data from the World Health Organization’s International Agency for Research on Cancer’s (IARC’s) Global Cancer Observatory. Li and coauthors examined patterns in the time trends of thyroid cancer, mortality data, and trends in diagnosis of thyroid cancer before testing became common in many nations.
This approach is needed in estimating overdiagnosis, where it’s not possible to see what’s happening on a case-by-case level, Salvatore Vaccarella, PhD, a scientist at IARC’s Cancer Surveillance Branch, said in an interview.
Researchers can’t tell whether an individual’s detected early-stage cancers would have remained indolent for years or eventually would have put their life at risk, he said. Instead, the patterns emerge through larger studies of the reported cases of cancer like thyroid tumors and then looking at separate datasets on mortality.
“We can only see that as a big phenomenon when we look at population-based data,” Vaccarella said.
Persisting Problem
Recognition of the harms of overdiagnosis has resulted in some reduction of the incidence of thyroid cancer in the United States, Li and coauthors wrote. After adjusting for age, incidence has fallen from 19 per 100,000 women in 2013 to 16 per 100,000 women in 2017. The proportion of thyroid cancer attributed to overdiagnosis has dropped from 76% to 68% in the country.
The paper adds to the evidence suggesting that the rise in screening has not changed mortality rates for thyroid cancer. For example, Li and coauthors reported seeing “a small decrease in thyroid cancer mortality rates over time in some European countries, but this decline (less than 1 per 100,000 women) is marginal compared with the increases in incidence (reaching around 100 per 100,000 women).”
“Moreover, previous data show that the downward mortality trends had begun before the wide use of ultrasonography for early detection and that period and birth cohort effects have been declining, probably due to treatment advances and reduced prevalence of risk factors, such as the reduction in iodine deficiency,” they wrote.
In an interview, Amanda Davis, MD, of AnMed, a nonprofit health system based in Anderson, South Carolina, said the new paper from Li and Vaccarella provides further evidence for a cautious approach to thyroid nodules given concerns about overdiagnosis.
If early detection of cancer via discovery of thyroid nodules actually helped patients, mortality rates would have dropped with expansion of screening and the resulting diagnoses, said Davis, who is an associate program director at AnMed’s family medicine residency program and affiliate professor at the Medical University of South Carolina, Charleston.
In many cases, people learn they have thyroid lesions after being tested for other conditions such as ultrasound done on carotid arteries to check for stroke risk. The most common form of thyroid cancer is the papillary form. Papillary thyroid cancer tends to be slow growing, carries a low risk for distant metastasis, and in many cases poses little risk. Some small (< 1 cm) papillary thyroid cancers can be monitored with active surveillance as opposed to thyroid lobectomy.
“So just finding more nodules incidentally or through screening ultrasound and even finding more papillary cancers via these methods does not make people healthier or decrease mortality,” Davis said.
“So just finding more things and even finding more papillary cancers does not increase our ability to treat people and keep them alive longer,” Davis said.
The 5-year survival rate for thyroid cancer overall is 98.1% and varies from 99.9% for localized disease to 55.3% for distant disease, the US Preventive Services Task Force (USPSTF) said in a 2017 publication in JAMA. The task force that year gave a “D” rating on screening of asymptomatic people for thyroid cancer. That means there’s moderate certainty that screening for thyroid cancer in asymptomatic persons results in harms that outweigh the benefits. The decision to give this “D” rating meant this screening is not recommended. That’s still the panel’s view.
“You can think of it as a “D” for ‘don’t screen for thyroid cancer,’ ” in people who present no symptoms of this illness, John Wong, MD, the vice chair of the USPSTF, said in an interview.
In primary care, the challenge is assessing thyroid nodules detected when people undergo testing for another reason, such as an ultrasound of the carotid artery to check for stroke risk.
Thyroid nodules can be detected by ultrasonography in up to 68% of the general population, reported a study in American Family Physician. Nodules with suspicious features or ≥ 1 cm require fine needle aspiration. The Bethesda System for Reporting Thyroid Cytopathology can be used to classify samples, with molecular testing applied to guide treatment when fine needle aspiration yields an indeterminate result.
New Thinking on Thyroid Cancer
There’s been a shift in recent years in the approach to how physicians should proceed if certain kinds of thyroid cancer are detected, Cari M. Kitahara, PhD, of the National Cancer Institute noted in a comment accompanying the Li paper.
“Clinicians need to be judicious in the use of thyroid ultrasonography, the diagnostic follow-up of incidentally detected thyroid nodules, and determining the optimal course of treatment,” Kitahara wrote. “For low-risk and incidentally detected tumors, strong consideration should be given to less intensive treatment options (eg, lobectomy, delayed treatment, and active surveillance).”
The American Thyroid Association guidelines encourage de-escalation of treatment for low-risk papillary thyroid carcinoma up to 4 cm.
Physicians often need to make clear to patients how a diagnosis of low-risk papillary thyroid cancer differs from other oncology diagnoses, R. Michael Tuttle, MD, of Memorial Sloan Kettering Cancer Center, New York City, said in an interview.
“I’ll frequently say that everything you’ve ever learned about cancer, you need to forget,” Tuttle said.
Some patients will mistakenly think any cancer diagnosis is a likely death sentence, meaning they should rush to get aggressive treatment. Tuttle has been a leader for many years in efforts in advancing active surveillance as an option for certain people with low-risk thyroid cancer.
“I often start my consultation by saying: ‘We’re going to choose between two right answers here. One right answer is watching right. One right answer is going to surgery,’ ” Tuttle said.
Patients with low-risk thyroid cancer tend to fall into two camps, with maximalists likely to seek quick treatment and minimalists more inclined for surveillance if that’s an option for them, Tuttle said. As opinions have shifted within the medical community about approaches to low-risk thyroid cancer, there’s also been some growing awareness among the public about thyroid overdiagnosis.
“Ten or 15 years ago, people thought we were crazy” to consider active surveillance as an option for low-risk thyroid cancers,” Tuttle said. “Now we have swung, at least in some of the public opinion, to this recognition that every little speck of cancer doesn’t need to be immediately taken out of your body.”
Some patients express regret about having learned that they have low-risk thyroid cancer, Tuttle said.
“Over the last 5 years, it’s not uncommon for patients to ask me, ‘Is this one of those that needs to be treated now, or is this one of those that we wish we would have never found?’ Or people will say, ‘My doctor talked me into an ultrasound, I didn’t want it’ or ‘I had a car wreck, and I found this nodule and I wished I had never found it.’ ”
This study from Li and coauthors was funded by the National Natural Science Foundation of China, the Guangdong Basic and Applied Basic Research Foundation, the Young Talents Program of Sun Yat-sen University Cancer Center, the Italian Association for Cancer Research, and the Italian Ministry of Health. Davis and Tuttle had no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
according to a recently published global study.
The proportion of thyroid cancer cases attributable to overdiagnosis globally was higher in women (78%) than in men (68%), with this rate varying substantially across countries, wrote Mengmeng Li, PhD, of the Sun Yat-sen University Cancer Center, Guangzhou, China, and coauthors in an October paper in The Lancet Diabetes & Endocrinology.
Overdiagnosis refers to the diagnosis of lesions that would not cause symptoms and that would not progress, if left alone.
Increased testing for thyroid cancer, fueled in large part by the expansion of imaging technologies and progressively more intense and disorganized scrutiny of the thyroid, led many people to be treated for often indolent lesions, exposing them to potential side effects as well as financial and emotional distress.
Li and coauthors estimate that more than 1.7 million people might have been overdiagnosed between 2013 and 2017 in 63 countries.
“Overdiagnosis clearly emerged in some high-resource countries with private-based health systems in which access to healthcare overrules regulatory controls (eg, in the USA) and in some high-quality public health systems with easy and broad access to thyroid gland diagnostic examinations (eg, in Canada),” Li and coauthors wrote. “Conversely, thyroid cancer is less commonly diagnosed in those countries in which access to diagnosis is guided by strong regulatory rules (eg, in Nordic countries).”
Their study drew from almost 40 years of research, including the latest available data from the World Health Organization’s International Agency for Research on Cancer’s (IARC’s) Global Cancer Observatory. Li and coauthors examined patterns in the time trends of thyroid cancer, mortality data, and trends in diagnosis of thyroid cancer before testing became common in many nations.
This approach is needed in estimating overdiagnosis, where it’s not possible to see what’s happening on a case-by-case level, Salvatore Vaccarella, PhD, a scientist at IARC’s Cancer Surveillance Branch, said in an interview.
Researchers can’t tell whether an individual’s detected early-stage cancers would have remained indolent for years or eventually would have put their life at risk, he said. Instead, the patterns emerge through larger studies of the reported cases of cancer like thyroid tumors and then looking at separate datasets on mortality.
“We can only see that as a big phenomenon when we look at population-based data,” Vaccarella said.
Persisting Problem
Recognition of the harms of overdiagnosis has resulted in some reduction of the incidence of thyroid cancer in the United States, Li and coauthors wrote. After adjusting for age, incidence has fallen from 19 per 100,000 women in 2013 to 16 per 100,000 women in 2017. The proportion of thyroid cancer attributed to overdiagnosis has dropped from 76% to 68% in the country.
The paper adds to the evidence suggesting that the rise in screening has not changed mortality rates for thyroid cancer. For example, Li and coauthors reported seeing “a small decrease in thyroid cancer mortality rates over time in some European countries, but this decline (less than 1 per 100,000 women) is marginal compared with the increases in incidence (reaching around 100 per 100,000 women).”
“Moreover, previous data show that the downward mortality trends had begun before the wide use of ultrasonography for early detection and that period and birth cohort effects have been declining, probably due to treatment advances and reduced prevalence of risk factors, such as the reduction in iodine deficiency,” they wrote.
In an interview, Amanda Davis, MD, of AnMed, a nonprofit health system based in Anderson, South Carolina, said the new paper from Li and Vaccarella provides further evidence for a cautious approach to thyroid nodules given concerns about overdiagnosis.
If early detection of cancer via discovery of thyroid nodules actually helped patients, mortality rates would have dropped with expansion of screening and the resulting diagnoses, said Davis, who is an associate program director at AnMed’s family medicine residency program and affiliate professor at the Medical University of South Carolina, Charleston.
In many cases, people learn they have thyroid lesions after being tested for other conditions such as ultrasound done on carotid arteries to check for stroke risk. The most common form of thyroid cancer is the papillary form. Papillary thyroid cancer tends to be slow growing, carries a low risk for distant metastasis, and in many cases poses little risk. Some small (< 1 cm) papillary thyroid cancers can be monitored with active surveillance as opposed to thyroid lobectomy.
“So just finding more nodules incidentally or through screening ultrasound and even finding more papillary cancers via these methods does not make people healthier or decrease mortality,” Davis said.
“So just finding more things and even finding more papillary cancers does not increase our ability to treat people and keep them alive longer,” Davis said.
The 5-year survival rate for thyroid cancer overall is 98.1% and varies from 99.9% for localized disease to 55.3% for distant disease, the US Preventive Services Task Force (USPSTF) said in a 2017 publication in JAMA. The task force that year gave a “D” rating on screening of asymptomatic people for thyroid cancer. That means there’s moderate certainty that screening for thyroid cancer in asymptomatic persons results in harms that outweigh the benefits. The decision to give this “D” rating meant this screening is not recommended. That’s still the panel’s view.
“You can think of it as a “D” for ‘don’t screen for thyroid cancer,’ ” in people who present no symptoms of this illness, John Wong, MD, the vice chair of the USPSTF, said in an interview.
In primary care, the challenge is assessing thyroid nodules detected when people undergo testing for another reason, such as an ultrasound of the carotid artery to check for stroke risk.
Thyroid nodules can be detected by ultrasonography in up to 68% of the general population, reported a study in American Family Physician. Nodules with suspicious features or ≥ 1 cm require fine needle aspiration. The Bethesda System for Reporting Thyroid Cytopathology can be used to classify samples, with molecular testing applied to guide treatment when fine needle aspiration yields an indeterminate result.
New Thinking on Thyroid Cancer
There’s been a shift in recent years in the approach to how physicians should proceed if certain kinds of thyroid cancer are detected, Cari M. Kitahara, PhD, of the National Cancer Institute noted in a comment accompanying the Li paper.
“Clinicians need to be judicious in the use of thyroid ultrasonography, the diagnostic follow-up of incidentally detected thyroid nodules, and determining the optimal course of treatment,” Kitahara wrote. “For low-risk and incidentally detected tumors, strong consideration should be given to less intensive treatment options (eg, lobectomy, delayed treatment, and active surveillance).”
The American Thyroid Association guidelines encourage de-escalation of treatment for low-risk papillary thyroid carcinoma up to 4 cm.
Physicians often need to make clear to patients how a diagnosis of low-risk papillary thyroid cancer differs from other oncology diagnoses, R. Michael Tuttle, MD, of Memorial Sloan Kettering Cancer Center, New York City, said in an interview.
“I’ll frequently say that everything you’ve ever learned about cancer, you need to forget,” Tuttle said.
Some patients will mistakenly think any cancer diagnosis is a likely death sentence, meaning they should rush to get aggressive treatment. Tuttle has been a leader for many years in efforts in advancing active surveillance as an option for certain people with low-risk thyroid cancer.
“I often start my consultation by saying: ‘We’re going to choose between two right answers here. One right answer is watching right. One right answer is going to surgery,’ ” Tuttle said.
Patients with low-risk thyroid cancer tend to fall into two camps, with maximalists likely to seek quick treatment and minimalists more inclined for surveillance if that’s an option for them, Tuttle said. As opinions have shifted within the medical community about approaches to low-risk thyroid cancer, there’s also been some growing awareness among the public about thyroid overdiagnosis.
“Ten or 15 years ago, people thought we were crazy” to consider active surveillance as an option for low-risk thyroid cancers,” Tuttle said. “Now we have swung, at least in some of the public opinion, to this recognition that every little speck of cancer doesn’t need to be immediately taken out of your body.”
Some patients express regret about having learned that they have low-risk thyroid cancer, Tuttle said.
“Over the last 5 years, it’s not uncommon for patients to ask me, ‘Is this one of those that needs to be treated now, or is this one of those that we wish we would have never found?’ Or people will say, ‘My doctor talked me into an ultrasound, I didn’t want it’ or ‘I had a car wreck, and I found this nodule and I wished I had never found it.’ ”
This study from Li and coauthors was funded by the National Natural Science Foundation of China, the Guangdong Basic and Applied Basic Research Foundation, the Young Talents Program of Sun Yat-sen University Cancer Center, the Italian Association for Cancer Research, and the Italian Ministry of Health. Davis and Tuttle had no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
FROM THE LANCET DIABETES & ENDOCRINOLOGY
FIT Completion and Yield Similar in Younger and Older Adults
, a new study has found.
The study also found a similar low 3% rate of CRC detected at colonoscopy in both the younger and older adults.
“Our study suggests that adults ages 45-49 have a colorectal cancer risk that is similar to what we see in adults age 50,” senior author Jeffrey K. Lee, MD, MPH, gastroenterologist and research scientist at Kaiser Permanente Northern California Division of Research (DOR) in Oakland, California, said in a news release.
“The low number of cancers we found also provides support for initially offering younger adults a non-invasive test, like FIT, to determine which patients would benefit from a colonoscopy,” Lee noted.

Timely and Important Question
“This study addresses a timely and important clinical question, namely, is FIT an acceptable screening modality in patients aged 45-49,” Ziad F. Gellad, MD, MPH, AGAF, professor of medicine, Duke University Medical Center, Durham, North Carolina, who was not involved in the study, said in an interview.
“The finding that FIT completion and yield in younger patients is similar to those aged 50 and above is good news because it supports the use of this screening modality in the younger cohort,” said Gellad, section chief, gastroenterology, Durham VA Health Care System.

The study was published online in Annals of Internal Medicine.
In 2021, the US Preventive Services Task Force lowered the age to start CRC screening from 50 to 45 years, in response to studies showing an increased rate of CRC in adults aged 45-49 years.
The decision to start CRC screening at age 45 was made based on modeling studies, which are dependent on assumptions, co-first author Theodore R. Levin, MD, who is also a gastroenterologist and research scientist at Kaiser Permanente DOR, said in an interview.
“We thought it was important to collect real-world data on the experience of screening in this age group. We had no basis to know whether younger people would take up screening or if the yield of screening would be sufficiently high to warrant starting screening in this age group,” said Levin.
The researchers compared FIT screening completion and outcomes in 213,928 patients aged 45-49 years and 53,804 patients aged 50 years who received a FIT kit for the first time. The patients were from Kaiser Permanente Northern California, Washington, and Colorado.
Overall, FIT completion rates were slightly higher in the younger adults than in the 50-year-olds (38.9% vs 37.5%; adjusted risk ratio [aRR], 1.05), although the younger patients from Colorado were substantially less apt to complete a FIT (30.7% vs 40.2%; aRR, 0.77).
In the overall 45- to 49-year age group, 3.6% of adults had a positive FIT result, only slightly lower than the 4% positivity rate in the 50-year age group (aRR, 0.91).
About two thirds of adults in both groups who had a positive FIT result went on to have a colonoscopy within 3 months of receiving the test result.
Adenoma detection during colonoscopy was slightly lower in the younger than in the older group (58.8% vs 67.7%; aRR, 0.88). However, yields were similar for adenoma with advanced histology (13.2% vs 15.9%; aRR, 0.86), polyp with high-grade dysplasia (3.4% vs 5.1%; aRR, 0.68), sessile serrated lesion (10.3% vs 11.7%; aRR, 0.92), and CRC (2.8% vs 2.7%; aRR, 1.10).
FIT First Fits With Younger Adults’ Busy Lives
“Overall, people under 50 have lower incidence of cancer than people in their 50s, 60s, and 70s. However, if you do a test like FIT first, you can improve the yield of colonoscopy, which is a much more efficient strategy,” Levin said.
He noted that younger people are the least likely to be screened.
“They are busy with work and family responsibilities and may not realize that they are at risk for CRC. It is important to offer them a test that is easy to perform and does not require them to miss a day of work or arrange for a driver. They should be offered an option to screen with a stool-based test as an easy way to fit CRC screening into their busy lives,” Levin said.
Gellad said the study also highlights the limitations of FIT, “namely, that the low uptake and suboptimal colonoscopy follow-up of positive tests, also extend into the lower age group.”
Additionally, Gellad said he hopes other large systems will replicate this study to address the generalizability of these findings outside the Kaiser system.
The study was funded by the Kaiser Permanente Sydney R. Garfield Memorial Fund. Disclosures for study authors are available with the original article. Gellad consulted for Merck & Co. and Novo Nordisk and is a co-founder of Higgs Boson, Inc.
A version of this article appeared on Medscape.com.
, a new study has found.
The study also found a similar low 3% rate of CRC detected at colonoscopy in both the younger and older adults.
“Our study suggests that adults ages 45-49 have a colorectal cancer risk that is similar to what we see in adults age 50,” senior author Jeffrey K. Lee, MD, MPH, gastroenterologist and research scientist at Kaiser Permanente Northern California Division of Research (DOR) in Oakland, California, said in a news release.
“The low number of cancers we found also provides support for initially offering younger adults a non-invasive test, like FIT, to determine which patients would benefit from a colonoscopy,” Lee noted.
Timely and Important Question
“This study addresses a timely and important clinical question, namely, is FIT an acceptable screening modality in patients aged 45-49,” Ziad F. Gellad, MD, MPH, AGAF, professor of medicine, Duke University Medical Center, Durham, North Carolina, who was not involved in the study, said in an interview.
“The finding that FIT completion and yield in younger patients is similar to those aged 50 and above is good news because it supports the use of this screening modality in the younger cohort,” said Gellad, section chief, gastroenterology, Durham VA Health Care System.
The study was published online in Annals of Internal Medicine.
In 2021, the US Preventive Services Task Force lowered the age to start CRC screening from 50 to 45 years, in response to studies showing an increased rate of CRC in adults aged 45-49 years.
The decision to start CRC screening at age 45 was made based on modeling studies, which are dependent on assumptions, co-first author Theodore R. Levin, MD, who is also a gastroenterologist and research scientist at Kaiser Permanente DOR, said in an interview.
“We thought it was important to collect real-world data on the experience of screening in this age group. We had no basis to know whether younger people would take up screening or if the yield of screening would be sufficiently high to warrant starting screening in this age group,” said Levin.
The researchers compared FIT screening completion and outcomes in 213,928 patients aged 45-49 years and 53,804 patients aged 50 years who received a FIT kit for the first time. The patients were from Kaiser Permanente Northern California, Washington, and Colorado.
Overall, FIT completion rates were slightly higher in the younger adults than in the 50-year-olds (38.9% vs 37.5%; adjusted risk ratio [aRR], 1.05), although the younger patients from Colorado were substantially less apt to complete a FIT (30.7% vs 40.2%; aRR, 0.77).
In the overall 45- to 49-year age group, 3.6% of adults had a positive FIT result, only slightly lower than the 4% positivity rate in the 50-year age group (aRR, 0.91).
About two thirds of adults in both groups who had a positive FIT result went on to have a colonoscopy within 3 months of receiving the test result.
Adenoma detection during colonoscopy was slightly lower in the younger than in the older group (58.8% vs 67.7%; aRR, 0.88). However, yields were similar for adenoma with advanced histology (13.2% vs 15.9%; aRR, 0.86), polyp with high-grade dysplasia (3.4% vs 5.1%; aRR, 0.68), sessile serrated lesion (10.3% vs 11.7%; aRR, 0.92), and CRC (2.8% vs 2.7%; aRR, 1.10).
FIT First Fits With Younger Adults’ Busy Lives
“Overall, people under 50 have lower incidence of cancer than people in their 50s, 60s, and 70s. However, if you do a test like FIT first, you can improve the yield of colonoscopy, which is a much more efficient strategy,” Levin said.
He noted that younger people are the least likely to be screened.
“They are busy with work and family responsibilities and may not realize that they are at risk for CRC. It is important to offer them a test that is easy to perform and does not require them to miss a day of work or arrange for a driver. They should be offered an option to screen with a stool-based test as an easy way to fit CRC screening into their busy lives,” Levin said.
Gellad said the study also highlights the limitations of FIT, “namely, that the low uptake and suboptimal colonoscopy follow-up of positive tests, also extend into the lower age group.”
Additionally, Gellad said he hopes other large systems will replicate this study to address the generalizability of these findings outside the Kaiser system.
The study was funded by the Kaiser Permanente Sydney R. Garfield Memorial Fund. Disclosures for study authors are available with the original article. Gellad consulted for Merck & Co. and Novo Nordisk and is a co-founder of Higgs Boson, Inc.
A version of this article appeared on Medscape.com.
, a new study has found.
The study also found a similar low 3% rate of CRC detected at colonoscopy in both the younger and older adults.
“Our study suggests that adults ages 45-49 have a colorectal cancer risk that is similar to what we see in adults age 50,” senior author Jeffrey K. Lee, MD, MPH, gastroenterologist and research scientist at Kaiser Permanente Northern California Division of Research (DOR) in Oakland, California, said in a news release.
“The low number of cancers we found also provides support for initially offering younger adults a non-invasive test, like FIT, to determine which patients would benefit from a colonoscopy,” Lee noted.
Timely and Important Question
“This study addresses a timely and important clinical question, namely, is FIT an acceptable screening modality in patients aged 45-49,” Ziad F. Gellad, MD, MPH, AGAF, professor of medicine, Duke University Medical Center, Durham, North Carolina, who was not involved in the study, said in an interview.
“The finding that FIT completion and yield in younger patients is similar to those aged 50 and above is good news because it supports the use of this screening modality in the younger cohort,” said Gellad, section chief, gastroenterology, Durham VA Health Care System.
The study was published online in Annals of Internal Medicine.
In 2021, the US Preventive Services Task Force lowered the age to start CRC screening from 50 to 45 years, in response to studies showing an increased rate of CRC in adults aged 45-49 years.
The decision to start CRC screening at age 45 was made based on modeling studies, which are dependent on assumptions, co-first author Theodore R. Levin, MD, who is also a gastroenterologist and research scientist at Kaiser Permanente DOR, said in an interview.
“We thought it was important to collect real-world data on the experience of screening in this age group. We had no basis to know whether younger people would take up screening or if the yield of screening would be sufficiently high to warrant starting screening in this age group,” said Levin.
The researchers compared FIT screening completion and outcomes in 213,928 patients aged 45-49 years and 53,804 patients aged 50 years who received a FIT kit for the first time. The patients were from Kaiser Permanente Northern California, Washington, and Colorado.
Overall, FIT completion rates were slightly higher in the younger adults than in the 50-year-olds (38.9% vs 37.5%; adjusted risk ratio [aRR], 1.05), although the younger patients from Colorado were substantially less apt to complete a FIT (30.7% vs 40.2%; aRR, 0.77).
In the overall 45- to 49-year age group, 3.6% of adults had a positive FIT result, only slightly lower than the 4% positivity rate in the 50-year age group (aRR, 0.91).
About two thirds of adults in both groups who had a positive FIT result went on to have a colonoscopy within 3 months of receiving the test result.
Adenoma detection during colonoscopy was slightly lower in the younger than in the older group (58.8% vs 67.7%; aRR, 0.88). However, yields were similar for adenoma with advanced histology (13.2% vs 15.9%; aRR, 0.86), polyp with high-grade dysplasia (3.4% vs 5.1%; aRR, 0.68), sessile serrated lesion (10.3% vs 11.7%; aRR, 0.92), and CRC (2.8% vs 2.7%; aRR, 1.10).
FIT First Fits With Younger Adults’ Busy Lives
“Overall, people under 50 have lower incidence of cancer than people in their 50s, 60s, and 70s. However, if you do a test like FIT first, you can improve the yield of colonoscopy, which is a much more efficient strategy,” Levin said.
He noted that younger people are the least likely to be screened.
“They are busy with work and family responsibilities and may not realize that they are at risk for CRC. It is important to offer them a test that is easy to perform and does not require them to miss a day of work or arrange for a driver. They should be offered an option to screen with a stool-based test as an easy way to fit CRC screening into their busy lives,” Levin said.
Gellad said the study also highlights the limitations of FIT, “namely, that the low uptake and suboptimal colonoscopy follow-up of positive tests, also extend into the lower age group.”
Additionally, Gellad said he hopes other large systems will replicate this study to address the generalizability of these findings outside the Kaiser system.
The study was funded by the Kaiser Permanente Sydney R. Garfield Memorial Fund. Disclosures for study authors are available with the original article. Gellad consulted for Merck & Co. and Novo Nordisk and is a co-founder of Higgs Boson, Inc.
A version of this article appeared on Medscape.com.
Starting Mammograms at Age 40: Will Women Benefit?
Last April, the US Preventive Services Task Force (USPSTF) revised its breast cancer screening guidelines to recommend average-risk women start their screening mammograms at age 40, instead of age 50, and continue every other year until age 74.
The USPSTF’s recent recommendations align with those from major organizations, including the National Comprehensive Cancer Network and the American College of Radiology. The latest update comes from the American College of Obstetricians and Gynecologists (ACOG), which recommended a start age of 40 and continued screening either annually or every 2 years.
For USPSTF, the decision to recommend the earlier screening age, instead of keeping the choice an individualized one, was largely driven by the steady rise in breast cancer diagnoses among women in their 40s, alongside evidence that Black women are more likely to get breast cancer younger and die from the disease compared with White women.
But is this recommendation to screen earlier a change for the better?
Opinions vary.
USPSTF member John Wong, MD, chief of clinical decision making and a primary care physician at Tufts Medical Center in Boston, believes the new recommendation is the right move.
“It is now clear that screening every other year starting at age 40 has the potential to save about 20% more lives among all women and there is even greater potential benefit for Black women, who are much more likely to die from breast cancer,” Wong told Medscape last year.
However, in a recent Viewpoint in JAMA Internal Medicine, experts from the University of California San Francisco expressed their reservations about shifting the recommended screening age a decade earlier.
The trio — Karla Kerlikowske, MD, Laura Esserman, MD, and Jeffrey Tice, MD — called the new recommendations “surprising” given the lack of new randomized control trial data to support the change as well as data that show breast cancer deaths have been decreasing among women, including younger women.
More specifically, breast cancer deaths for women under 50 have decreased from 5.9 to 3.9 per 100,000 individuals between 2000 and 2020 — a decline that can likely be attributed to better treatments rather than increased screening effectiveness, the Viewpoint authors said.
However, moving the screening age earlier would not markedly improve survival for most women, the authors argued. According to USPSTF modeling, starting mammograms at age 40 instead of 50 could avert only 1.3 additional breast cancer deaths per 1000 women screened biennially and 1.8 additional breast cancer deaths among Black women.
Starting screening at 40, however, does come with an array of potential harms. These include 65 more benign biopsies per 1000 women screened, 1 in 2 women with a false-positive mammography result (503 per 1000), and 1 in 500 women with an over-diagnosed breast cancer, meaning the cancer would not have become clinically evident in their lifetime.
The use of digital breast tomosynthesis can slightly reduce the number of false-positives and benign biopsies compared to older mammography techniques, but these small improvements did not sway the overall pro-con assessment for the Viewpoint authors.
“False-positive results require additional imaging and are associated with anxiety for patients,” the authors noted. “Women who have benign biopsies may experience the potential adverse effects of biopsies, such as bleeding, infection, and scarring unnecessarily; and over-diagnosis may lead to unnecessary treatment.”
Kenneth Lin, MD, MPH, family physician and associate director of the Lancaster General Hospital Family Medicine Residency in Pennsylvania, agreed that starting mammograms at age 40 is not a change for the better.
Lin and colleagues conducted an analysis based on data from the USPSTF’s 2016 breast cancer screening report that similarly found 1 additional breast cancer death prevented per 1000 women screened starting at 40 vs 50, at a cost of 576 more false-positive results, 67 more benign breast biopsies, and 2 women diagnosed and treated unnecessarily.
Overall, “there is no compelling evidence to change our clinical approach to breast cancer screening for women in their 40s: individual decision-making based on patient preferences and values,” Lin wrote in a recent Medscape commentary.
But several experts not involved in the USPSTF recommendations agree with the change.
The updated recommendation to begin mammograms at age 40 for women at average risk “aligns with accumulating data suggesting that earlier and more frequent screening can save more lives, and is widely seen as a positive step,” said Lisa Abramson, MD, a radiologist specializing in breast imaging with Mount Sinai Health System and Icahn School of Medicine at Mount Sinai, New York City.
Melissa Fana, MD, a breast surgical oncologist at NYU Langone Health, agreed that the revised recommendation is justified and “will undoubtedly save lives.”
“The recent change in the screening recommendation was meant to be inclusive, and provide women, particularly women aged 40 to 49 the opportunity to screen with mammography,” Fana said.
One major argument in favor of earlier screening is that it will help address racial inequities in breast cancer diagnoses, treatment, and deaths. Despite a 5% lower incidence of breast cancer, Black women are more likely to be diagnosed with distant-stage cancer or more aggressive breast cancer subtypes, such as triple-negative, compared with White women, and are more likely to die from breast cancer.
“We hope that the earlier initiation of mammography screening across the board will have a great net benefit in outcomes for Black women especially, who have been shown to have the poorest outcomes when it comes to breast cancer, in part because of long-standing inequities in social determinants of health,” said Cherie C. Hill, MD, FACOG, an ob.gyn. at Emory Healthcare in Atlanta, who coauthored the recent ACOG recommendations.
The Viewpoint authors Kerlikowske, Esserman and Tice agreed that Black women may benefit more from earlier screening. However, earlier screening does not address the underlying disparities in treatment and follow-up care for Black women, and it is unclear whether screening alone will help improve breast cancer mortality rates for Black women, the authors noted.
There is one place where experts seem to align: the importance of educating patients about their personal risk.
The Viewpoint authors favor a risk-based approach to help women decide whether to start screening before age 50.
“Engaging women in informed decision-making based on their invasive and advanced breast cancer risk would be a patient-centered approach toward tailored screening, informing when to consider starting screening and how often to screen,” the experts wrote.
For a woman to truly make an educated decision on whether she would like to screen or wait after age 40, she would at least need to know what her specific lifetime risk of developing breast cancer is, not the average risk is for American women in general, Fana told this news organization.
“Risk assessment calculators are widely available and include factors such as family history and reproductive history, and this information can evolve over time and affect lifetime risk,” Fana noted. But “some women just do not get this information.”
Abramson explained that ob.gyns. and primary care physicians will likely play a larger role in the early assessment of breast cancer risk, including discussions about genetic testing and personal risk factors starting as early as age 25.
“For clinicians, the emphasis may be on educating patients about their individual risk, ensuring timely mammograms, and referring higher-risk individuals for further testing or consultations with specialists,” Abramson added.
Esserman reported being a Blue Cross Medical Advisory Panel member, an uncompensated board member of Quantum Leap Healthcare Collaborative, which funds the I-SPY trial through the University of California, San Francisco, and having an investigator-initiated trial for high-risk ductal carcinoma in situ (DCIS) funded through UCSF by Moderna for a DCIS phase 1 study. Tice and Kerlikowske reported receiving grants from the National Cancer Institute outside the submitted work. Abramson and Fana have no relevant disclosures.
A version of this article appeared on Medscape.com.
Last April, the US Preventive Services Task Force (USPSTF) revised its breast cancer screening guidelines to recommend average-risk women start their screening mammograms at age 40, instead of age 50, and continue every other year until age 74.
The USPSTF’s recent recommendations align with those from major organizations, including the National Comprehensive Cancer Network and the American College of Radiology. The latest update comes from the American College of Obstetricians and Gynecologists (ACOG), which recommended a start age of 40 and continued screening either annually or every 2 years.
For USPSTF, the decision to recommend the earlier screening age, instead of keeping the choice an individualized one, was largely driven by the steady rise in breast cancer diagnoses among women in their 40s, alongside evidence that Black women are more likely to get breast cancer younger and die from the disease compared with White women.
But is this recommendation to screen earlier a change for the better?
Opinions vary.
USPSTF member John Wong, MD, chief of clinical decision making and a primary care physician at Tufts Medical Center in Boston, believes the new recommendation is the right move.
“It is now clear that screening every other year starting at age 40 has the potential to save about 20% more lives among all women and there is even greater potential benefit for Black women, who are much more likely to die from breast cancer,” Wong told Medscape last year.
However, in a recent Viewpoint in JAMA Internal Medicine, experts from the University of California San Francisco expressed their reservations about shifting the recommended screening age a decade earlier.
The trio — Karla Kerlikowske, MD, Laura Esserman, MD, and Jeffrey Tice, MD — called the new recommendations “surprising” given the lack of new randomized control trial data to support the change as well as data that show breast cancer deaths have been decreasing among women, including younger women.
More specifically, breast cancer deaths for women under 50 have decreased from 5.9 to 3.9 per 100,000 individuals between 2000 and 2020 — a decline that can likely be attributed to better treatments rather than increased screening effectiveness, the Viewpoint authors said.
However, moving the screening age earlier would not markedly improve survival for most women, the authors argued. According to USPSTF modeling, starting mammograms at age 40 instead of 50 could avert only 1.3 additional breast cancer deaths per 1000 women screened biennially and 1.8 additional breast cancer deaths among Black women.
Starting screening at 40, however, does come with an array of potential harms. These include 65 more benign biopsies per 1000 women screened, 1 in 2 women with a false-positive mammography result (503 per 1000), and 1 in 500 women with an over-diagnosed breast cancer, meaning the cancer would not have become clinically evident in their lifetime.
The use of digital breast tomosynthesis can slightly reduce the number of false-positives and benign biopsies compared to older mammography techniques, but these small improvements did not sway the overall pro-con assessment for the Viewpoint authors.
“False-positive results require additional imaging and are associated with anxiety for patients,” the authors noted. “Women who have benign biopsies may experience the potential adverse effects of biopsies, such as bleeding, infection, and scarring unnecessarily; and over-diagnosis may lead to unnecessary treatment.”
Kenneth Lin, MD, MPH, family physician and associate director of the Lancaster General Hospital Family Medicine Residency in Pennsylvania, agreed that starting mammograms at age 40 is not a change for the better.
Lin and colleagues conducted an analysis based on data from the USPSTF’s 2016 breast cancer screening report that similarly found 1 additional breast cancer death prevented per 1000 women screened starting at 40 vs 50, at a cost of 576 more false-positive results, 67 more benign breast biopsies, and 2 women diagnosed and treated unnecessarily.
Overall, “there is no compelling evidence to change our clinical approach to breast cancer screening for women in their 40s: individual decision-making based on patient preferences and values,” Lin wrote in a recent Medscape commentary.
But several experts not involved in the USPSTF recommendations agree with the change.
The updated recommendation to begin mammograms at age 40 for women at average risk “aligns with accumulating data suggesting that earlier and more frequent screening can save more lives, and is widely seen as a positive step,” said Lisa Abramson, MD, a radiologist specializing in breast imaging with Mount Sinai Health System and Icahn School of Medicine at Mount Sinai, New York City.
Melissa Fana, MD, a breast surgical oncologist at NYU Langone Health, agreed that the revised recommendation is justified and “will undoubtedly save lives.”
“The recent change in the screening recommendation was meant to be inclusive, and provide women, particularly women aged 40 to 49 the opportunity to screen with mammography,” Fana said.
One major argument in favor of earlier screening is that it will help address racial inequities in breast cancer diagnoses, treatment, and deaths. Despite a 5% lower incidence of breast cancer, Black women are more likely to be diagnosed with distant-stage cancer or more aggressive breast cancer subtypes, such as triple-negative, compared with White women, and are more likely to die from breast cancer.
“We hope that the earlier initiation of mammography screening across the board will have a great net benefit in outcomes for Black women especially, who have been shown to have the poorest outcomes when it comes to breast cancer, in part because of long-standing inequities in social determinants of health,” said Cherie C. Hill, MD, FACOG, an ob.gyn. at Emory Healthcare in Atlanta, who coauthored the recent ACOG recommendations.
The Viewpoint authors Kerlikowske, Esserman and Tice agreed that Black women may benefit more from earlier screening. However, earlier screening does not address the underlying disparities in treatment and follow-up care for Black women, and it is unclear whether screening alone will help improve breast cancer mortality rates for Black women, the authors noted.
There is one place where experts seem to align: the importance of educating patients about their personal risk.
The Viewpoint authors favor a risk-based approach to help women decide whether to start screening before age 50.
“Engaging women in informed decision-making based on their invasive and advanced breast cancer risk would be a patient-centered approach toward tailored screening, informing when to consider starting screening and how often to screen,” the experts wrote.
For a woman to truly make an educated decision on whether she would like to screen or wait after age 40, she would at least need to know what her specific lifetime risk of developing breast cancer is, not the average risk is for American women in general, Fana told this news organization.
“Risk assessment calculators are widely available and include factors such as family history and reproductive history, and this information can evolve over time and affect lifetime risk,” Fana noted. But “some women just do not get this information.”
Abramson explained that ob.gyns. and primary care physicians will likely play a larger role in the early assessment of breast cancer risk, including discussions about genetic testing and personal risk factors starting as early as age 25.
“For clinicians, the emphasis may be on educating patients about their individual risk, ensuring timely mammograms, and referring higher-risk individuals for further testing or consultations with specialists,” Abramson added.
Esserman reported being a Blue Cross Medical Advisory Panel member, an uncompensated board member of Quantum Leap Healthcare Collaborative, which funds the I-SPY trial through the University of California, San Francisco, and having an investigator-initiated trial for high-risk ductal carcinoma in situ (DCIS) funded through UCSF by Moderna for a DCIS phase 1 study. Tice and Kerlikowske reported receiving grants from the National Cancer Institute outside the submitted work. Abramson and Fana have no relevant disclosures.
A version of this article appeared on Medscape.com.
Last April, the US Preventive Services Task Force (USPSTF) revised its breast cancer screening guidelines to recommend average-risk women start their screening mammograms at age 40, instead of age 50, and continue every other year until age 74.
The USPSTF’s recent recommendations align with those from major organizations, including the National Comprehensive Cancer Network and the American College of Radiology. The latest update comes from the American College of Obstetricians and Gynecologists (ACOG), which recommended a start age of 40 and continued screening either annually or every 2 years.
For USPSTF, the decision to recommend the earlier screening age, instead of keeping the choice an individualized one, was largely driven by the steady rise in breast cancer diagnoses among women in their 40s, alongside evidence that Black women are more likely to get breast cancer younger and die from the disease compared with White women.
But is this recommendation to screen earlier a change for the better?
Opinions vary.
USPSTF member John Wong, MD, chief of clinical decision making and a primary care physician at Tufts Medical Center in Boston, believes the new recommendation is the right move.
“It is now clear that screening every other year starting at age 40 has the potential to save about 20% more lives among all women and there is even greater potential benefit for Black women, who are much more likely to die from breast cancer,” Wong told Medscape last year.
However, in a recent Viewpoint in JAMA Internal Medicine, experts from the University of California San Francisco expressed their reservations about shifting the recommended screening age a decade earlier.
The trio — Karla Kerlikowske, MD, Laura Esserman, MD, and Jeffrey Tice, MD — called the new recommendations “surprising” given the lack of new randomized control trial data to support the change as well as data that show breast cancer deaths have been decreasing among women, including younger women.
More specifically, breast cancer deaths for women under 50 have decreased from 5.9 to 3.9 per 100,000 individuals between 2000 and 2020 — a decline that can likely be attributed to better treatments rather than increased screening effectiveness, the Viewpoint authors said.
However, moving the screening age earlier would not markedly improve survival for most women, the authors argued. According to USPSTF modeling, starting mammograms at age 40 instead of 50 could avert only 1.3 additional breast cancer deaths per 1000 women screened biennially and 1.8 additional breast cancer deaths among Black women.
Starting screening at 40, however, does come with an array of potential harms. These include 65 more benign biopsies per 1000 women screened, 1 in 2 women with a false-positive mammography result (503 per 1000), and 1 in 500 women with an over-diagnosed breast cancer, meaning the cancer would not have become clinically evident in their lifetime.
The use of digital breast tomosynthesis can slightly reduce the number of false-positives and benign biopsies compared to older mammography techniques, but these small improvements did not sway the overall pro-con assessment for the Viewpoint authors.
“False-positive results require additional imaging and are associated with anxiety for patients,” the authors noted. “Women who have benign biopsies may experience the potential adverse effects of biopsies, such as bleeding, infection, and scarring unnecessarily; and over-diagnosis may lead to unnecessary treatment.”
Kenneth Lin, MD, MPH, family physician and associate director of the Lancaster General Hospital Family Medicine Residency in Pennsylvania, agreed that starting mammograms at age 40 is not a change for the better.
Lin and colleagues conducted an analysis based on data from the USPSTF’s 2016 breast cancer screening report that similarly found 1 additional breast cancer death prevented per 1000 women screened starting at 40 vs 50, at a cost of 576 more false-positive results, 67 more benign breast biopsies, and 2 women diagnosed and treated unnecessarily.
Overall, “there is no compelling evidence to change our clinical approach to breast cancer screening for women in their 40s: individual decision-making based on patient preferences and values,” Lin wrote in a recent Medscape commentary.
But several experts not involved in the USPSTF recommendations agree with the change.
The updated recommendation to begin mammograms at age 40 for women at average risk “aligns with accumulating data suggesting that earlier and more frequent screening can save more lives, and is widely seen as a positive step,” said Lisa Abramson, MD, a radiologist specializing in breast imaging with Mount Sinai Health System and Icahn School of Medicine at Mount Sinai, New York City.
Melissa Fana, MD, a breast surgical oncologist at NYU Langone Health, agreed that the revised recommendation is justified and “will undoubtedly save lives.”
“The recent change in the screening recommendation was meant to be inclusive, and provide women, particularly women aged 40 to 49 the opportunity to screen with mammography,” Fana said.
One major argument in favor of earlier screening is that it will help address racial inequities in breast cancer diagnoses, treatment, and deaths. Despite a 5% lower incidence of breast cancer, Black women are more likely to be diagnosed with distant-stage cancer or more aggressive breast cancer subtypes, such as triple-negative, compared with White women, and are more likely to die from breast cancer.
“We hope that the earlier initiation of mammography screening across the board will have a great net benefit in outcomes for Black women especially, who have been shown to have the poorest outcomes when it comes to breast cancer, in part because of long-standing inequities in social determinants of health,” said Cherie C. Hill, MD, FACOG, an ob.gyn. at Emory Healthcare in Atlanta, who coauthored the recent ACOG recommendations.
The Viewpoint authors Kerlikowske, Esserman and Tice agreed that Black women may benefit more from earlier screening. However, earlier screening does not address the underlying disparities in treatment and follow-up care for Black women, and it is unclear whether screening alone will help improve breast cancer mortality rates for Black women, the authors noted.
There is one place where experts seem to align: the importance of educating patients about their personal risk.
The Viewpoint authors favor a risk-based approach to help women decide whether to start screening before age 50.
“Engaging women in informed decision-making based on their invasive and advanced breast cancer risk would be a patient-centered approach toward tailored screening, informing when to consider starting screening and how often to screen,” the experts wrote.
For a woman to truly make an educated decision on whether she would like to screen or wait after age 40, she would at least need to know what her specific lifetime risk of developing breast cancer is, not the average risk is for American women in general, Fana told this news organization.
“Risk assessment calculators are widely available and include factors such as family history and reproductive history, and this information can evolve over time and affect lifetime risk,” Fana noted. But “some women just do not get this information.”
Abramson explained that ob.gyns. and primary care physicians will likely play a larger role in the early assessment of breast cancer risk, including discussions about genetic testing and personal risk factors starting as early as age 25.
“For clinicians, the emphasis may be on educating patients about their individual risk, ensuring timely mammograms, and referring higher-risk individuals for further testing or consultations with specialists,” Abramson added.
Esserman reported being a Blue Cross Medical Advisory Panel member, an uncompensated board member of Quantum Leap Healthcare Collaborative, which funds the I-SPY trial through the University of California, San Francisco, and having an investigator-initiated trial for high-risk ductal carcinoma in situ (DCIS) funded through UCSF by Moderna for a DCIS phase 1 study. Tice and Kerlikowske reported receiving grants from the National Cancer Institute outside the submitted work. Abramson and Fana have no relevant disclosures.
A version of this article appeared on Medscape.com.