User login
Enhancing Dermatology Education: Resident Presentation Opportunities
Dermatology residency is busy with 3 years of clinical duties, academic responsibilities, and administrative work. In addition, it is a time to maximize educational experiences in dermatology from didactics to hands-on learning. It also is a time to take advantage of special opportunities that are available to residents, including attending academic meetings and giving oral and/or poster presentations. Major dermatology conferences often have designated sessions for residents that provide an excellent chance for residents to share interesting cases or present their research. This article provides a review of selected presentation opportunities available to residents at the major academic dermatology meetings.
American Academy of Dermatology
The Annual Meeting of the American Academy of Dermatology (AAD) accepts abstracts for oral presentation from both residents and fellows for its “Residents and Fellows Symposium” and “Gross and Microscopic Symposium.” The “Residents and Fellows Symposium” is an opportunity to present either clinical or laboratory research in a 9-minute oral format. Up to 20 abstracts are chosen for presentation along with 4 alternate abstracts. Furthermore, awards are given to the top 3 abstracts in both the clinical and laboratory categories. Those accepted for the “Gross and Microscopic Symposium” give a 5-minute oral presentation of a case with interesting clinical and histopathological findings. Submission guidelines for these presentations are available on the AAD Web site (https://www.aad.org/symposium/am2016).
Residents and fellows also are eligible to submit abstracts for the AAD’s electronic poster exhibits and presentations. The posters are presented electronically and are displayed and/or are available to be viewed throughout the meeting. The abstracts are blind reviewed by the Poster Exhibits Task Force on a scale from 1 (unsatisfactory) to 10 (outstanding). Presenters with abstracts that receive a passing score (2.5 or higher) by judges are allowed to discuss their poster in a live 5-minute oral presentation.
The AAD’s Summer Academy Meeting, which also takes place annually, does not have separate resident-specific poster or oral presentation sessions; however, it does offer an electronic poster exhibit and presentation session.
Pediatric Dermatology
The Annual Meeting of the Society for Pediatric Dermatology (https://pedsderm.net/meetings/annual-meeting/) accepts abstract submissions for its “Cases of the Year” session as well as poster presentations. Residents, medical students, and fellows who are chosen for a “Cases of the Year” or poster presentation are eligible for a travel award that is available on a competitive basis. The American Academy of Pediatrics’ Section on Dermatology also offers an additional travel award for a resident or fellow who presents a case or poster at the Annual Meeting of the Society for Pediatric Dermatology.
American Society for Dermatologic Surgery
The American Society for Dermatologic Surgery has an Annual Meeting (https://www.asds.net/ annualmeeting/) that includes a competitive “Resident Oral Abstracts” session. If selected, residents give a 5-minute presentation and abstracts are published in the Annual Meeting program book.
American Society of Dermatopathology
The American Society of Dermatopathology Annual Meeting has several opportunities for residents and fellows to present abstracts (https://www.asdp.org/meetings-events/annual-meeting/52nd/call-for -abtracts/). Submissions to the “General Abstracts” category are selected for either oral or poster presentation. Ambitious dermatology or pathology residents may choose to submit their case report abstracts to the “Duel in Dermatopathology” competition, which includes an oral presentation and publication of abstracts in the meeting program book. Finally, the “Dermatopathology Fellows Abstract” category is a special category for dermatopathology fellows to present an oral or poster presentation. Any resident or fellow who is accepted for oral or poster presentations is eligible for a “Physician-in-Training Award” (except winners of the “Duel in Dermatopathology” competition), which are granted to the best oral and poster presentations.
Conclusion
Beyond dermatology residency, there are many opportunities for resident education through attendance at academic meetings as well as presentation of case reports and research. The major dermatology meetings often have specific sessions to give residents a chance to share their work or interesting cases. This guide may be helpful to residents who are hoping for such venues to enhance their education and even their curriculum vitae.
Dermatology residency is busy with 3 years of clinical duties, academic responsibilities, and administrative work. In addition, it is a time to maximize educational experiences in dermatology from didactics to hands-on learning. It also is a time to take advantage of special opportunities that are available to residents, including attending academic meetings and giving oral and/or poster presentations. Major dermatology conferences often have designated sessions for residents that provide an excellent chance for residents to share interesting cases or present their research. This article provides a review of selected presentation opportunities available to residents at the major academic dermatology meetings.
American Academy of Dermatology
The Annual Meeting of the American Academy of Dermatology (AAD) accepts abstracts for oral presentation from both residents and fellows for its “Residents and Fellows Symposium” and “Gross and Microscopic Symposium.” The “Residents and Fellows Symposium” is an opportunity to present either clinical or laboratory research in a 9-minute oral format. Up to 20 abstracts are chosen for presentation along with 4 alternate abstracts. Furthermore, awards are given to the top 3 abstracts in both the clinical and laboratory categories. Those accepted for the “Gross and Microscopic Symposium” give a 5-minute oral presentation of a case with interesting clinical and histopathological findings. Submission guidelines for these presentations are available on the AAD Web site (https://www.aad.org/symposium/am2016).
Residents and fellows also are eligible to submit abstracts for the AAD’s electronic poster exhibits and presentations. The posters are presented electronically and are displayed and/or are available to be viewed throughout the meeting. The abstracts are blind reviewed by the Poster Exhibits Task Force on a scale from 1 (unsatisfactory) to 10 (outstanding). Presenters with abstracts that receive a passing score (2.5 or higher) by judges are allowed to discuss their poster in a live 5-minute oral presentation.
The AAD’s Summer Academy Meeting, which also takes place annually, does not have separate resident-specific poster or oral presentation sessions; however, it does offer an electronic poster exhibit and presentation session.
Pediatric Dermatology
The Annual Meeting of the Society for Pediatric Dermatology (https://pedsderm.net/meetings/annual-meeting/) accepts abstract submissions for its “Cases of the Year” session as well as poster presentations. Residents, medical students, and fellows who are chosen for a “Cases of the Year” or poster presentation are eligible for a travel award that is available on a competitive basis. The American Academy of Pediatrics’ Section on Dermatology also offers an additional travel award for a resident or fellow who presents a case or poster at the Annual Meeting of the Society for Pediatric Dermatology.
American Society for Dermatologic Surgery
The American Society for Dermatologic Surgery has an Annual Meeting (https://www.asds.net/ annualmeeting/) that includes a competitive “Resident Oral Abstracts” session. If selected, residents give a 5-minute presentation and abstracts are published in the Annual Meeting program book.
American Society of Dermatopathology
The American Society of Dermatopathology Annual Meeting has several opportunities for residents and fellows to present abstracts (https://www.asdp.org/meetings-events/annual-meeting/52nd/call-for -abtracts/). Submissions to the “General Abstracts” category are selected for either oral or poster presentation. Ambitious dermatology or pathology residents may choose to submit their case report abstracts to the “Duel in Dermatopathology” competition, which includes an oral presentation and publication of abstracts in the meeting program book. Finally, the “Dermatopathology Fellows Abstract” category is a special category for dermatopathology fellows to present an oral or poster presentation. Any resident or fellow who is accepted for oral or poster presentations is eligible for a “Physician-in-Training Award” (except winners of the “Duel in Dermatopathology” competition), which are granted to the best oral and poster presentations.
Conclusion
Beyond dermatology residency, there are many opportunities for resident education through attendance at academic meetings as well as presentation of case reports and research. The major dermatology meetings often have specific sessions to give residents a chance to share their work or interesting cases. This guide may be helpful to residents who are hoping for such venues to enhance their education and even their curriculum vitae.
Dermatology residency is busy with 3 years of clinical duties, academic responsibilities, and administrative work. In addition, it is a time to maximize educational experiences in dermatology from didactics to hands-on learning. It also is a time to take advantage of special opportunities that are available to residents, including attending academic meetings and giving oral and/or poster presentations. Major dermatology conferences often have designated sessions for residents that provide an excellent chance for residents to share interesting cases or present their research. This article provides a review of selected presentation opportunities available to residents at the major academic dermatology meetings.
American Academy of Dermatology
The Annual Meeting of the American Academy of Dermatology (AAD) accepts abstracts for oral presentation from both residents and fellows for its “Residents and Fellows Symposium” and “Gross and Microscopic Symposium.” The “Residents and Fellows Symposium” is an opportunity to present either clinical or laboratory research in a 9-minute oral format. Up to 20 abstracts are chosen for presentation along with 4 alternate abstracts. Furthermore, awards are given to the top 3 abstracts in both the clinical and laboratory categories. Those accepted for the “Gross and Microscopic Symposium” give a 5-minute oral presentation of a case with interesting clinical and histopathological findings. Submission guidelines for these presentations are available on the AAD Web site (https://www.aad.org/symposium/am2016).
Residents and fellows also are eligible to submit abstracts for the AAD’s electronic poster exhibits and presentations. The posters are presented electronically and are displayed and/or are available to be viewed throughout the meeting. The abstracts are blind reviewed by the Poster Exhibits Task Force on a scale from 1 (unsatisfactory) to 10 (outstanding). Presenters with abstracts that receive a passing score (2.5 or higher) by judges are allowed to discuss their poster in a live 5-minute oral presentation.
The AAD’s Summer Academy Meeting, which also takes place annually, does not have separate resident-specific poster or oral presentation sessions; however, it does offer an electronic poster exhibit and presentation session.
Pediatric Dermatology
The Annual Meeting of the Society for Pediatric Dermatology (https://pedsderm.net/meetings/annual-meeting/) accepts abstract submissions for its “Cases of the Year” session as well as poster presentations. Residents, medical students, and fellows who are chosen for a “Cases of the Year” or poster presentation are eligible for a travel award that is available on a competitive basis. The American Academy of Pediatrics’ Section on Dermatology also offers an additional travel award for a resident or fellow who presents a case or poster at the Annual Meeting of the Society for Pediatric Dermatology.
American Society for Dermatologic Surgery
The American Society for Dermatologic Surgery has an Annual Meeting (https://www.asds.net/ annualmeeting/) that includes a competitive “Resident Oral Abstracts” session. If selected, residents give a 5-minute presentation and abstracts are published in the Annual Meeting program book.
American Society of Dermatopathology
The American Society of Dermatopathology Annual Meeting has several opportunities for residents and fellows to present abstracts (https://www.asdp.org/meetings-events/annual-meeting/52nd/call-for -abtracts/). Submissions to the “General Abstracts” category are selected for either oral or poster presentation. Ambitious dermatology or pathology residents may choose to submit their case report abstracts to the “Duel in Dermatopathology” competition, which includes an oral presentation and publication of abstracts in the meeting program book. Finally, the “Dermatopathology Fellows Abstract” category is a special category for dermatopathology fellows to present an oral or poster presentation. Any resident or fellow who is accepted for oral or poster presentations is eligible for a “Physician-in-Training Award” (except winners of the “Duel in Dermatopathology” competition), which are granted to the best oral and poster presentations.
Conclusion
Beyond dermatology residency, there are many opportunities for resident education through attendance at academic meetings as well as presentation of case reports and research. The major dermatology meetings often have specific sessions to give residents a chance to share their work or interesting cases. This guide may be helpful to residents who are hoping for such venues to enhance their education and even their curriculum vitae.

Minimize That “Pinch and Burn”: Tips and Tricks to Reduce Injection Pain With Local Anesthetics
The use of local anesthetics, particularly local anesthetic injections, is a core part of the practice of dermatology. The use of anesthetics in both diagnosis and management make the administration and usage of these medications a foundational skill for all dermatology residents. Minimizing that familiar “pinch and burn” and giving patients a nearly pain-free experience can result in satisfaction for both patients and physicians. This column describes several useful and easily implemented techniques that residents can incorporate into their daily practice.
Buffer
Plain lidocaine is less acidic than the more commonly utilized lidocaine 1% with 1:100,000 epinephrine. When the latter is buffered with sodium bicarbonate in a 10:1 dilution, it is superior to its unbuffered counterpart.1 This method works by raising the pH of the solution, which is normally 4.2, to a physiologic and more comfortable 7.4.2 Of note, bupivacaine is more acidic than lidocaine.3
Warm
Warming anesthetics has been shown to reduce injection pain. Warming anesthetics to body temperature or up to 40°C to 54.4°C (104°F–130°F) has been studied and recommended.4-7 Warming combined with buffering may result in the least painful injection.4-6
Use Smaller-Gauge Needles
A more obvious tip, using smaller-gauge needles can reduce injection pain. Generally, 27- or 30-gauge needles are commonly recommended.8,9
Limit Repeated Use of the Same Needle
Switch to a fresh needle when you have to inject multiple times in the same lesion or when you have multiple injection sites. In addition, use different needles for drawing up and for the actual injection procedure. A dull needle means more pain.
Perpendicular Injection Technique
Compared to a 45° injection angle, lidocaine injected at a 90° angle reduces pain,10 as this technique minimizes the number of nerve endings that come in contact with the needle.8
Inject Slowly
A slow injection technique using small volumes can substantially minimize pain, as it allows for the nerve endings in the skin to accommodate for the distortion caused by anesthetic infiltration.2
Pulse Injection
Pulse injections can be less painful than injecting an anesthetic in a continuous fashion. It has been recommended that 0.1 cc of anesthetic be injected followed by a 3-second pause, then repeating this step 2 to 3 times. More volumes may subsequently be administered.8
Thoughtful Reinsertion
When larger surface areas must be anesthetized, the needle may have to be reinserted multiple times. In these instances, injection within 1 cm of the visibly blanched area of skin ensures that lidocaine (and epinephrine, if such a solution is used) has already infiltrated that area.2
Distraction
There is merit to the idea of distracting the patient when injecting local anesthetics. Distraction methods including engaging in simple conversation with the patient, having the patient look away, playing background music, and even suggesting that the procedure is painless or has minimal pain have shown utility in minimizing injection pain.8,11
Other distraction techniques are physical, including stretching and scratching the skin, pinching, local vibration, and pressure.12,13
Combination Anesthetic Technique
Topical anesthetic application, such as lidocaine 2.5%–prilocaine 2.5% cream, can be applied 60 to 120 minutes prior to intralesional anesthetic injection to attenuate injection pain.2,8 Ice or ethyl chloride spray also can be utilized and has a faster onset of action than topical anesthetics.2,8
Conclusion
The knowledge and application of techniques to minimize pain associated with local anesthetic injection can greatly enhance a resident’s practice. Learning and incorporating these techniques early on in resident training can help instill these skills that can be useful for the remainder of a dermatologist’s career.
1. Burns CA, Ferris G, Feng C, et al. Decreasing the pain of local anesthesia: a prospective, double-blind comparison of buffered, premixed 1% lidocaine with epinephrine versus 1% lidocaine freshly mixed with epinephrine. J Am Acad Dermatol. 2006;54:128-131.
2. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
3. Knowles WR. Minimizing pain due to local anesthesia. J Dermatol Surg Oncol. 1990;16:489.
4. Colaric KB, Overton DT, Moore K. Pain reduction in lidocaine administration through buffering and warming. Am J Emerg Med. 1998;16:353-356.
5. Mader TJ, Playe SJ, Garb JL. Reducing the pain of local anesthetic infiltration: warming and buffering have a synergistic effect. Ann Emerg Med. 1994;23:550-554.
6. Yang CH, Hsu HC, Shen SC, et al. Warm and neutral tumescent anesthetic solutions are essential factors for a less painful injection. Dermatol Surg. 2006;32:1119-1122.
7. Krathen RA, Donnelly HB. Warmed local anesthetic for dermatologic surgery. Dermatol Surg. 2008;34:1239-1240.
8. Zilinsky I, Bar-Meir E, Zaslansky R, et al. Ten commandments for minimal pain during administration of local anesthetics. J Drugs Dermatol. 2005;4:212-216.
9. Mustoe TA, Buck DW II, Lalonde DH. The safe management of anesthesia, sedation, and pain in plastic surgery. Plast Reconstr Surg. 2010;126:e165-e176.
10. Martires KJ, Malbasa CL, Bordeaux JS. A randomized controlled crossover trial: lidocaine injected at a 90-degree angle causes less pain than lidocaine injected at a 45-degree angle. J Am Acad Dermatol. 2011;65:1231-1233.
11. Uman LS, Chambers CT, McGrath PJ, et al. A systematic review of randomized controlled trials examining psychological interventions for needle-related procedural pain and distress in children and adolescents: an abbreviated Cochrane review. J Pediatr Psychol. 2008;33:842-854.
12. Ong EL, Lim NL, Koay CK. Towards a pain-free venepuncture. Anaesthesia. 2000;55:260-262.
13. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
The use of local anesthetics, particularly local anesthetic injections, is a core part of the practice of dermatology. The use of anesthetics in both diagnosis and management make the administration and usage of these medications a foundational skill for all dermatology residents. Minimizing that familiar “pinch and burn” and giving patients a nearly pain-free experience can result in satisfaction for both patients and physicians. This column describes several useful and easily implemented techniques that residents can incorporate into their daily practice.
Buffer
Plain lidocaine is less acidic than the more commonly utilized lidocaine 1% with 1:100,000 epinephrine. When the latter is buffered with sodium bicarbonate in a 10:1 dilution, it is superior to its unbuffered counterpart.1 This method works by raising the pH of the solution, which is normally 4.2, to a physiologic and more comfortable 7.4.2 Of note, bupivacaine is more acidic than lidocaine.3
Warm
Warming anesthetics has been shown to reduce injection pain. Warming anesthetics to body temperature or up to 40°C to 54.4°C (104°F–130°F) has been studied and recommended.4-7 Warming combined with buffering may result in the least painful injection.4-6
Use Smaller-Gauge Needles
A more obvious tip, using smaller-gauge needles can reduce injection pain. Generally, 27- or 30-gauge needles are commonly recommended.8,9
Limit Repeated Use of the Same Needle
Switch to a fresh needle when you have to inject multiple times in the same lesion or when you have multiple injection sites. In addition, use different needles for drawing up and for the actual injection procedure. A dull needle means more pain.
Perpendicular Injection Technique
Compared to a 45° injection angle, lidocaine injected at a 90° angle reduces pain,10 as this technique minimizes the number of nerve endings that come in contact with the needle.8
Inject Slowly
A slow injection technique using small volumes can substantially minimize pain, as it allows for the nerve endings in the skin to accommodate for the distortion caused by anesthetic infiltration.2
Pulse Injection
Pulse injections can be less painful than injecting an anesthetic in a continuous fashion. It has been recommended that 0.1 cc of anesthetic be injected followed by a 3-second pause, then repeating this step 2 to 3 times. More volumes may subsequently be administered.8
Thoughtful Reinsertion
When larger surface areas must be anesthetized, the needle may have to be reinserted multiple times. In these instances, injection within 1 cm of the visibly blanched area of skin ensures that lidocaine (and epinephrine, if such a solution is used) has already infiltrated that area.2
Distraction
There is merit to the idea of distracting the patient when injecting local anesthetics. Distraction methods including engaging in simple conversation with the patient, having the patient look away, playing background music, and even suggesting that the procedure is painless or has minimal pain have shown utility in minimizing injection pain.8,11
Other distraction techniques are physical, including stretching and scratching the skin, pinching, local vibration, and pressure.12,13
Combination Anesthetic Technique
Topical anesthetic application, such as lidocaine 2.5%–prilocaine 2.5% cream, can be applied 60 to 120 minutes prior to intralesional anesthetic injection to attenuate injection pain.2,8 Ice or ethyl chloride spray also can be utilized and has a faster onset of action than topical anesthetics.2,8
Conclusion
The knowledge and application of techniques to minimize pain associated with local anesthetic injection can greatly enhance a resident’s practice. Learning and incorporating these techniques early on in resident training can help instill these skills that can be useful for the remainder of a dermatologist’s career.
The use of local anesthetics, particularly local anesthetic injections, is a core part of the practice of dermatology. The use of anesthetics in both diagnosis and management make the administration and usage of these medications a foundational skill for all dermatology residents. Minimizing that familiar “pinch and burn” and giving patients a nearly pain-free experience can result in satisfaction for both patients and physicians. This column describes several useful and easily implemented techniques that residents can incorporate into their daily practice.
Buffer
Plain lidocaine is less acidic than the more commonly utilized lidocaine 1% with 1:100,000 epinephrine. When the latter is buffered with sodium bicarbonate in a 10:1 dilution, it is superior to its unbuffered counterpart.1 This method works by raising the pH of the solution, which is normally 4.2, to a physiologic and more comfortable 7.4.2 Of note, bupivacaine is more acidic than lidocaine.3
Warm
Warming anesthetics has been shown to reduce injection pain. Warming anesthetics to body temperature or up to 40°C to 54.4°C (104°F–130°F) has been studied and recommended.4-7 Warming combined with buffering may result in the least painful injection.4-6
Use Smaller-Gauge Needles
A more obvious tip, using smaller-gauge needles can reduce injection pain. Generally, 27- or 30-gauge needles are commonly recommended.8,9
Limit Repeated Use of the Same Needle
Switch to a fresh needle when you have to inject multiple times in the same lesion or when you have multiple injection sites. In addition, use different needles for drawing up and for the actual injection procedure. A dull needle means more pain.
Perpendicular Injection Technique
Compared to a 45° injection angle, lidocaine injected at a 90° angle reduces pain,10 as this technique minimizes the number of nerve endings that come in contact with the needle.8
Inject Slowly
A slow injection technique using small volumes can substantially minimize pain, as it allows for the nerve endings in the skin to accommodate for the distortion caused by anesthetic infiltration.2
Pulse Injection
Pulse injections can be less painful than injecting an anesthetic in a continuous fashion. It has been recommended that 0.1 cc of anesthetic be injected followed by a 3-second pause, then repeating this step 2 to 3 times. More volumes may subsequently be administered.8
Thoughtful Reinsertion
When larger surface areas must be anesthetized, the needle may have to be reinserted multiple times. In these instances, injection within 1 cm of the visibly blanched area of skin ensures that lidocaine (and epinephrine, if such a solution is used) has already infiltrated that area.2
Distraction
There is merit to the idea of distracting the patient when injecting local anesthetics. Distraction methods including engaging in simple conversation with the patient, having the patient look away, playing background music, and even suggesting that the procedure is painless or has minimal pain have shown utility in minimizing injection pain.8,11
Other distraction techniques are physical, including stretching and scratching the skin, pinching, local vibration, and pressure.12,13
Combination Anesthetic Technique
Topical anesthetic application, such as lidocaine 2.5%–prilocaine 2.5% cream, can be applied 60 to 120 minutes prior to intralesional anesthetic injection to attenuate injection pain.2,8 Ice or ethyl chloride spray also can be utilized and has a faster onset of action than topical anesthetics.2,8
Conclusion
The knowledge and application of techniques to minimize pain associated with local anesthetic injection can greatly enhance a resident’s practice. Learning and incorporating these techniques early on in resident training can help instill these skills that can be useful for the remainder of a dermatologist’s career.
1. Burns CA, Ferris G, Feng C, et al. Decreasing the pain of local anesthesia: a prospective, double-blind comparison of buffered, premixed 1% lidocaine with epinephrine versus 1% lidocaine freshly mixed with epinephrine. J Am Acad Dermatol. 2006;54:128-131.
2. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
3. Knowles WR. Minimizing pain due to local anesthesia. J Dermatol Surg Oncol. 1990;16:489.
4. Colaric KB, Overton DT, Moore K. Pain reduction in lidocaine administration through buffering and warming. Am J Emerg Med. 1998;16:353-356.
5. Mader TJ, Playe SJ, Garb JL. Reducing the pain of local anesthetic infiltration: warming and buffering have a synergistic effect. Ann Emerg Med. 1994;23:550-554.
6. Yang CH, Hsu HC, Shen SC, et al. Warm and neutral tumescent anesthetic solutions are essential factors for a less painful injection. Dermatol Surg. 2006;32:1119-1122.
7. Krathen RA, Donnelly HB. Warmed local anesthetic for dermatologic surgery. Dermatol Surg. 2008;34:1239-1240.
8. Zilinsky I, Bar-Meir E, Zaslansky R, et al. Ten commandments for minimal pain during administration of local anesthetics. J Drugs Dermatol. 2005;4:212-216.
9. Mustoe TA, Buck DW II, Lalonde DH. The safe management of anesthesia, sedation, and pain in plastic surgery. Plast Reconstr Surg. 2010;126:e165-e176.
10. Martires KJ, Malbasa CL, Bordeaux JS. A randomized controlled crossover trial: lidocaine injected at a 90-degree angle causes less pain than lidocaine injected at a 45-degree angle. J Am Acad Dermatol. 2011;65:1231-1233.
11. Uman LS, Chambers CT, McGrath PJ, et al. A systematic review of randomized controlled trials examining psychological interventions for needle-related procedural pain and distress in children and adolescents: an abbreviated Cochrane review. J Pediatr Psychol. 2008;33:842-854.
12. Ong EL, Lim NL, Koay CK. Towards a pain-free venepuncture. Anaesthesia. 2000;55:260-262.
13. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
1. Burns CA, Ferris G, Feng C, et al. Decreasing the pain of local anesthesia: a prospective, double-blind comparison of buffered, premixed 1% lidocaine with epinephrine versus 1% lidocaine freshly mixed with epinephrine. J Am Acad Dermatol. 2006;54:128-131.
2. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
3. Knowles WR. Minimizing pain due to local anesthesia. J Dermatol Surg Oncol. 1990;16:489.
4. Colaric KB, Overton DT, Moore K. Pain reduction in lidocaine administration through buffering and warming. Am J Emerg Med. 1998;16:353-356.
5. Mader TJ, Playe SJ, Garb JL. Reducing the pain of local anesthetic infiltration: warming and buffering have a synergistic effect. Ann Emerg Med. 1994;23:550-554.
6. Yang CH, Hsu HC, Shen SC, et al. Warm and neutral tumescent anesthetic solutions are essential factors for a less painful injection. Dermatol Surg. 2006;32:1119-1122.
7. Krathen RA, Donnelly HB. Warmed local anesthetic for dermatologic surgery. Dermatol Surg. 2008;34:1239-1240.
8. Zilinsky I, Bar-Meir E, Zaslansky R, et al. Ten commandments for minimal pain during administration of local anesthetics. J Drugs Dermatol. 2005;4:212-216.
9. Mustoe TA, Buck DW II, Lalonde DH. The safe management of anesthesia, sedation, and pain in plastic surgery. Plast Reconstr Surg. 2010;126:e165-e176.
10. Martires KJ, Malbasa CL, Bordeaux JS. A randomized controlled crossover trial: lidocaine injected at a 90-degree angle causes less pain than lidocaine injected at a 45-degree angle. J Am Acad Dermatol. 2011;65:1231-1233.
11. Uman LS, Chambers CT, McGrath PJ, et al. A systematic review of randomized controlled trials examining psychological interventions for needle-related procedural pain and distress in children and adolescents: an abbreviated Cochrane review. J Pediatr Psychol. 2008;33:842-854.
12. Ong EL, Lim NL, Koay CK. Towards a pain-free venepuncture. Anaesthesia. 2000;55:260-262.
13. Strazar R, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
Fellowships After Dermatology Residency: The Traditional and Beyond
Dermatology residents, such as myself, often wonder what we will do after graduation. There are many resources for finding job opportunities, and many of us have received solicitation e-mails from various headhunters and medical groups that are looking to hire. The American Academy of Dermatology (AAD) has a resource called the AAD Career Compass (http://www.healthecareers.com/aad), which is an exhaustive database of job listings for dermatologists. However, I could not locate a definitive resource containing information that might be useful for dermatology residents who are interested in subspecializing or pursuing fellowships.
Subspecialty training is typically pursued after successful completion of a dermatology residency training program. Fellowships are traditionally offered in dermatopathology, pediatric dermatology, micrographic surgery and dermatologic oncology (procedural dermatology), and cosmetic dermatologic surgery. Fellowships also are available in other subspecialties or for those pursuing an academic career. The goal of this article is to help dermatology residents learn more about traditional and nontraditional opportunities for graduate education and certification in various dermatologic subspecialties, with links to sources for more detailed information.
Traditional Fellowship Programs by Subspecialty
Dermatopathology
One- to 2-year dermatopathology fellowship programs are certified by both the American Board of Dermatology (ABD) and the American Board of Pathology and are available to graduates of either dermatology or pathology residency programs. These programs offer combined training in either anatomic pathology (for dermatologists) or clinical dermatology (for pathologists), along with dermatopathology; the majority of time is devoted to the latter. The Accreditation Council for Graduate Medical Education and the ABD have issued specific requirements for graduate medical education and subspecialty certification in dermatopathology.1,2 Fellowship matches are institution dependent, and the application process and match generally takes place during the second year of dermatology residency for those residents who want to start a fellowship program immediately following graduation. The American Society of Dermatopathology offers a dermatopathology fellowship program finder on its Web site.
Pediatric Dermatology
Fellowships in pediatric dermatology are typically 1- to 2-year programs that focus on dermatologic diseases in the pediatric population. Applicants are matched to these programs through the San Francisco Matching Program (SF Match) and the programs are ABD accredited.3,4 (There also are a number of non–ABD-approved training opportunities available.5) On completion of the training program, fellows may qualify for subspecialty board certification in pediatric dermatology. Applications are open starting in January, and the rank order list and match occur in August of the same year. As of 2012, there were 20 participating programs with 28 available positions, while the match included 22 applicants; of these applicants, 15 matched formally into pediatric dermatology fellowships.6
Micrographic Surgery and Dermatologic Oncology (Procedural Dermatology)
There are specific requirements issued by the Accreditation Council for Graduate Medical Education for dermatologic surgery fellowships,7 which are typically 1- to 2-year programs. Many fellowship programs also are accredited by the American College of Mohs Surgery. This subspecialty is not ABD accredited; therefore, there is no certification process upon completion of a fellowship program. The American College of Mohs Surgery sponsors the match process through SF Match. Applicant registration begins in July and the match occurs in December of the same year. As of 2013, there were 47 participating programs offering 55 positions. Of 77 applicants, 49 obtained fellowship positions formally through the match.8 The American Society for Dermatologic Surgery (ASDS) Web site provides the DermSurg Fellowship Finder, which includes information about independent fellowship programs.
Cosmetic Dermatologic Surgery
The ASDS has an accreditation program for fellowships in cosmetic dermatologic surgery,9 which are generally 1-year programs. Certification in this subspecialty is not ABD accredited. Fellowship opportunities can be found using the ASDS DermSurg Fellowship Finder.
Nontraditional Fellowship Programs
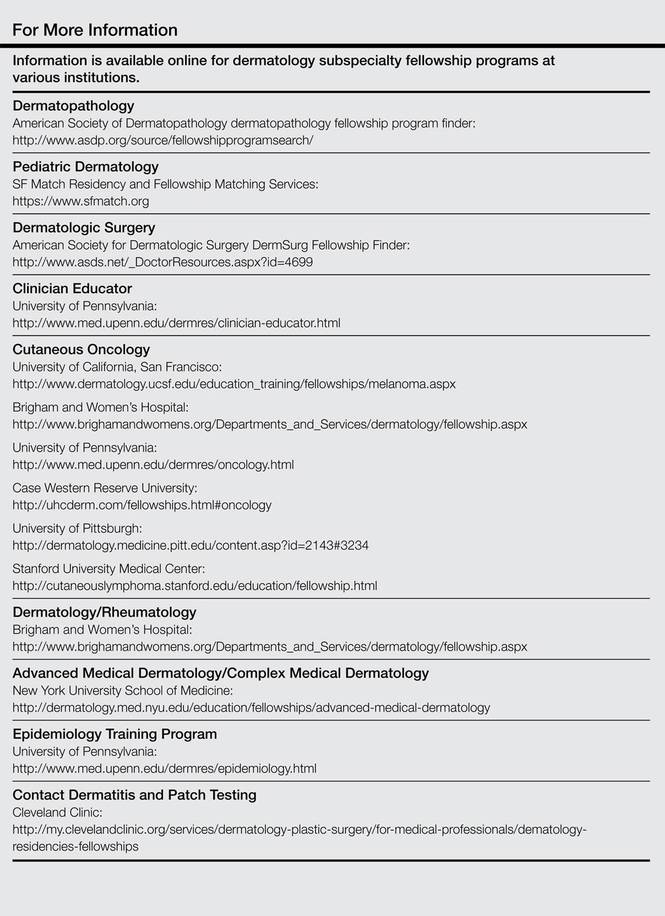
The following are fellowship programs that are in nontraditional subspecialties, are only available at certain institutions, and are not accredited. This list is not exhaustive of all available programs but are those that may be of interest to dermatology residents who are drawn to a particular dermatologic subspecialty or have an interest in academic dermatology. There is no formal match process and applications vary by institution.
Clinician Educator Fellowship
The clinician educator fellowship is available at the Department of Dermatology at the University of Pennsylvania (Philadelphia, Pennsylvania) and is intended to foster dermatologic clinician educators. More information can be found on the program’s Web site.
Cutaneous Oncology Fellowship
This 1- to 2-year fellowship program focuses on diagnosis and management of melanoma and nonmelanoma skin cancers as well as cutaneous lymphomas. Fellowships in cutaneous oncology are offered at the University of California, San Francisco (San Francisco, California), Brigham and Women’s Hospital (Boston, Massachusetts), the University of Pennsylvania (Philadelphia, Pennsylvania), Case Western Reserve University (Cleveland, Ohio), the University of Pittsburgh (Pittsburgh, Pennsylvania), and Stanford University Medical Center (Stanford, California).
Dermatology/Rheumatology
The dermatology/rheumatology fellowship offered by Brigham and Women’s Hospital is a 1-year program that focuses on the management of connective-tissue diseases in a multidisciplinary fashion with rheumatology.
Advanced Medical Dermatology/Complex Medical Dermatology
Several programs offer fellowships in medical dermatology under different titles but with a similar curriculum and goal: to foster dermatologists interested in careers as academic medical dermatologists or as future clinician scientists by means of specialized training and mentorship in complex medical and dermatological issues in the outpatient and inpatient settings. The 2-year program at New York University School of Medicine (New York, New York) also gives fellows the opportunity to earn a master of science in clinical investigation degree. The University of California, San Francisco, program offers protected time for career development.
Epidemiology Training Program
Fellows and residents in the University of Pennsylvania’s dermatology training program may elect to work with the Center for Clinical Epidemiology and Biostatistics and have the opportunity to earn a graduate degree (MSCE or PhD).
Contact Dermatitis and Patch Testing Fellowship
The Dermatology Department at the Cleveland Clinic (Cleveland, Ohio) offers a 1-year contact dermatitis and patch testing fellowship that includes clinical research.
Conclusion
Both traditional and nontraditional fellowship opportunities exist after dermatology residency. This guide serves as an overview of the training programs in dermatopathology, pediatric dermatology, micrographic surgery and dermatologic oncology (procedural dermatology), and cosmetic dermatologic surgery, as well as the fellowships offered at certain institutions for those interested in more specific subspecialties or academia.
1. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in dermatopathology. http://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/100_dermatopathology_2016_1-YR.pdf. Revised April 2014. Effective July 1, 2015. Accessed on February 26, 2015.
2. Subspecialty certification in dermatopathology. The American Board of Dermatology, Inc Web site. http://www.abderm.org/subspecialties/derm.html. Accessed February 26, 2015.
3. American Board of Dermatology (ABD) approved pediatric dermatology fellowship programs. The Society for Pediatric Dermatology Web site. http://pedsderm.net/training/fellowships/abd-approved-pediatric-dermatology-fellowship-programs/. Updated June 9, 2014. Accessed February 26, 2015.
4. Subspecialty certification in pediatric dermatology. The American Board of Dermatology, Inc Web site. http://www.abderm.org/subspecialties/pediatric.html. Accessed February 26, 2015.
5. Non-ABD pediatric dermatology fellowship programs. The Society for Pediatric Dermatology Web site. https://pedsderm.net/training/fellowships/non-abd-pediatric-dermatology-fellowship-programs/. Accessed February 26, 2015.
6. Pediatric dermatology match report. SF Match Web site. https://www.sfmatch.org/SpecialtyInsideAll.aspx?id=16&typ=1&name=Pediatric%20Dermatology#. Accessed March 4, 2015.
7. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in procedural dermatology. https://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/081_procedural_derm_1-YR_07012014.pdf. Effective July 2014. Accessed February 26, 2015.
8. Statistics: micrographic surgery & dermatologic oncology fellowship. SF Match Web site. https://www.sfmatch.org/SpecialtyInsideAll.aspx?id=10&typ=1&name=Micrographic%20Surgery%20and%20Dermatologic%20Oncology#. Accessed March 4, 2015.
9. ASDS cosmetic dermatologic surgery fellowship accreditation program. American Society for Dermatologic Surgery Web site. http://www.asds.net/cosmetic-accreditation/. Accessed February 26, 2015.
Dermatology residents, such as myself, often wonder what we will do after graduation. There are many resources for finding job opportunities, and many of us have received solicitation e-mails from various headhunters and medical groups that are looking to hire. The American Academy of Dermatology (AAD) has a resource called the AAD Career Compass (http://www.healthecareers.com/aad), which is an exhaustive database of job listings for dermatologists. However, I could not locate a definitive resource containing information that might be useful for dermatology residents who are interested in subspecializing or pursuing fellowships.
Subspecialty training is typically pursued after successful completion of a dermatology residency training program. Fellowships are traditionally offered in dermatopathology, pediatric dermatology, micrographic surgery and dermatologic oncology (procedural dermatology), and cosmetic dermatologic surgery. Fellowships also are available in other subspecialties or for those pursuing an academic career. The goal of this article is to help dermatology residents learn more about traditional and nontraditional opportunities for graduate education and certification in various dermatologic subspecialties, with links to sources for more detailed information.
Traditional Fellowship Programs by Subspecialty
Dermatopathology
One- to 2-year dermatopathology fellowship programs are certified by both the American Board of Dermatology (ABD) and the American Board of Pathology and are available to graduates of either dermatology or pathology residency programs. These programs offer combined training in either anatomic pathology (for dermatologists) or clinical dermatology (for pathologists), along with dermatopathology; the majority of time is devoted to the latter. The Accreditation Council for Graduate Medical Education and the ABD have issued specific requirements for graduate medical education and subspecialty certification in dermatopathology.1,2 Fellowship matches are institution dependent, and the application process and match generally takes place during the second year of dermatology residency for those residents who want to start a fellowship program immediately following graduation. The American Society of Dermatopathology offers a dermatopathology fellowship program finder on its Web site.
Pediatric Dermatology
Fellowships in pediatric dermatology are typically 1- to 2-year programs that focus on dermatologic diseases in the pediatric population. Applicants are matched to these programs through the San Francisco Matching Program (SF Match) and the programs are ABD accredited.3,4 (There also are a number of non–ABD-approved training opportunities available.5) On completion of the training program, fellows may qualify for subspecialty board certification in pediatric dermatology. Applications are open starting in January, and the rank order list and match occur in August of the same year. As of 2012, there were 20 participating programs with 28 available positions, while the match included 22 applicants; of these applicants, 15 matched formally into pediatric dermatology fellowships.6
Micrographic Surgery and Dermatologic Oncology (Procedural Dermatology)
There are specific requirements issued by the Accreditation Council for Graduate Medical Education for dermatologic surgery fellowships,7 which are typically 1- to 2-year programs. Many fellowship programs also are accredited by the American College of Mohs Surgery. This subspecialty is not ABD accredited; therefore, there is no certification process upon completion of a fellowship program. The American College of Mohs Surgery sponsors the match process through SF Match. Applicant registration begins in July and the match occurs in December of the same year. As of 2013, there were 47 participating programs offering 55 positions. Of 77 applicants, 49 obtained fellowship positions formally through the match.8 The American Society for Dermatologic Surgery (ASDS) Web site provides the DermSurg Fellowship Finder, which includes information about independent fellowship programs.
Cosmetic Dermatologic Surgery
The ASDS has an accreditation program for fellowships in cosmetic dermatologic surgery,9 which are generally 1-year programs. Certification in this subspecialty is not ABD accredited. Fellowship opportunities can be found using the ASDS DermSurg Fellowship Finder.
Nontraditional Fellowship Programs
The following are fellowship programs that are in nontraditional subspecialties, are only available at certain institutions, and are not accredited. This list is not exhaustive of all available programs but are those that may be of interest to dermatology residents who are drawn to a particular dermatologic subspecialty or have an interest in academic dermatology. There is no formal match process and applications vary by institution.
Clinician Educator Fellowship
The clinician educator fellowship is available at the Department of Dermatology at the University of Pennsylvania (Philadelphia, Pennsylvania) and is intended to foster dermatologic clinician educators. More information can be found on the program’s Web site.
Cutaneous Oncology Fellowship
This 1- to 2-year fellowship program focuses on diagnosis and management of melanoma and nonmelanoma skin cancers as well as cutaneous lymphomas. Fellowships in cutaneous oncology are offered at the University of California, San Francisco (San Francisco, California), Brigham and Women’s Hospital (Boston, Massachusetts), the University of Pennsylvania (Philadelphia, Pennsylvania), Case Western Reserve University (Cleveland, Ohio), the University of Pittsburgh (Pittsburgh, Pennsylvania), and Stanford University Medical Center (Stanford, California).
Dermatology/Rheumatology
The dermatology/rheumatology fellowship offered by Brigham and Women’s Hospital is a 1-year program that focuses on the management of connective-tissue diseases in a multidisciplinary fashion with rheumatology.
Advanced Medical Dermatology/Complex Medical Dermatology
Several programs offer fellowships in medical dermatology under different titles but with a similar curriculum and goal: to foster dermatologists interested in careers as academic medical dermatologists or as future clinician scientists by means of specialized training and mentorship in complex medical and dermatological issues in the outpatient and inpatient settings. The 2-year program at New York University School of Medicine (New York, New York) also gives fellows the opportunity to earn a master of science in clinical investigation degree. The University of California, San Francisco, program offers protected time for career development.
Epidemiology Training Program
Fellows and residents in the University of Pennsylvania’s dermatology training program may elect to work with the Center for Clinical Epidemiology and Biostatistics and have the opportunity to earn a graduate degree (MSCE or PhD).
Contact Dermatitis and Patch Testing Fellowship
The Dermatology Department at the Cleveland Clinic (Cleveland, Ohio) offers a 1-year contact dermatitis and patch testing fellowship that includes clinical research.
Conclusion
Both traditional and nontraditional fellowship opportunities exist after dermatology residency. This guide serves as an overview of the training programs in dermatopathology, pediatric dermatology, micrographic surgery and dermatologic oncology (procedural dermatology), and cosmetic dermatologic surgery, as well as the fellowships offered at certain institutions for those interested in more specific subspecialties or academia.
Dermatology residents, such as myself, often wonder what we will do after graduation. There are many resources for finding job opportunities, and many of us have received solicitation e-mails from various headhunters and medical groups that are looking to hire. The American Academy of Dermatology (AAD) has a resource called the AAD Career Compass (http://www.healthecareers.com/aad), which is an exhaustive database of job listings for dermatologists. However, I could not locate a definitive resource containing information that might be useful for dermatology residents who are interested in subspecializing or pursuing fellowships.
Subspecialty training is typically pursued after successful completion of a dermatology residency training program. Fellowships are traditionally offered in dermatopathology, pediatric dermatology, micrographic surgery and dermatologic oncology (procedural dermatology), and cosmetic dermatologic surgery. Fellowships also are available in other subspecialties or for those pursuing an academic career. The goal of this article is to help dermatology residents learn more about traditional and nontraditional opportunities for graduate education and certification in various dermatologic subspecialties, with links to sources for more detailed information.
Traditional Fellowship Programs by Subspecialty
Dermatopathology
One- to 2-year dermatopathology fellowship programs are certified by both the American Board of Dermatology (ABD) and the American Board of Pathology and are available to graduates of either dermatology or pathology residency programs. These programs offer combined training in either anatomic pathology (for dermatologists) or clinical dermatology (for pathologists), along with dermatopathology; the majority of time is devoted to the latter. The Accreditation Council for Graduate Medical Education and the ABD have issued specific requirements for graduate medical education and subspecialty certification in dermatopathology.1,2 Fellowship matches are institution dependent, and the application process and match generally takes place during the second year of dermatology residency for those residents who want to start a fellowship program immediately following graduation. The American Society of Dermatopathology offers a dermatopathology fellowship program finder on its Web site.
Pediatric Dermatology
Fellowships in pediatric dermatology are typically 1- to 2-year programs that focus on dermatologic diseases in the pediatric population. Applicants are matched to these programs through the San Francisco Matching Program (SF Match) and the programs are ABD accredited.3,4 (There also are a number of non–ABD-approved training opportunities available.5) On completion of the training program, fellows may qualify for subspecialty board certification in pediatric dermatology. Applications are open starting in January, and the rank order list and match occur in August of the same year. As of 2012, there were 20 participating programs with 28 available positions, while the match included 22 applicants; of these applicants, 15 matched formally into pediatric dermatology fellowships.6
Micrographic Surgery and Dermatologic Oncology (Procedural Dermatology)
There are specific requirements issued by the Accreditation Council for Graduate Medical Education for dermatologic surgery fellowships,7 which are typically 1- to 2-year programs. Many fellowship programs also are accredited by the American College of Mohs Surgery. This subspecialty is not ABD accredited; therefore, there is no certification process upon completion of a fellowship program. The American College of Mohs Surgery sponsors the match process through SF Match. Applicant registration begins in July and the match occurs in December of the same year. As of 2013, there were 47 participating programs offering 55 positions. Of 77 applicants, 49 obtained fellowship positions formally through the match.8 The American Society for Dermatologic Surgery (ASDS) Web site provides the DermSurg Fellowship Finder, which includes information about independent fellowship programs.
Cosmetic Dermatologic Surgery
The ASDS has an accreditation program for fellowships in cosmetic dermatologic surgery,9 which are generally 1-year programs. Certification in this subspecialty is not ABD accredited. Fellowship opportunities can be found using the ASDS DermSurg Fellowship Finder.
Nontraditional Fellowship Programs
The following are fellowship programs that are in nontraditional subspecialties, are only available at certain institutions, and are not accredited. This list is not exhaustive of all available programs but are those that may be of interest to dermatology residents who are drawn to a particular dermatologic subspecialty or have an interest in academic dermatology. There is no formal match process and applications vary by institution.
Clinician Educator Fellowship
The clinician educator fellowship is available at the Department of Dermatology at the University of Pennsylvania (Philadelphia, Pennsylvania) and is intended to foster dermatologic clinician educators. More information can be found on the program’s Web site.
Cutaneous Oncology Fellowship
This 1- to 2-year fellowship program focuses on diagnosis and management of melanoma and nonmelanoma skin cancers as well as cutaneous lymphomas. Fellowships in cutaneous oncology are offered at the University of California, San Francisco (San Francisco, California), Brigham and Women’s Hospital (Boston, Massachusetts), the University of Pennsylvania (Philadelphia, Pennsylvania), Case Western Reserve University (Cleveland, Ohio), the University of Pittsburgh (Pittsburgh, Pennsylvania), and Stanford University Medical Center (Stanford, California).
Dermatology/Rheumatology
The dermatology/rheumatology fellowship offered by Brigham and Women’s Hospital is a 1-year program that focuses on the management of connective-tissue diseases in a multidisciplinary fashion with rheumatology.
Advanced Medical Dermatology/Complex Medical Dermatology
Several programs offer fellowships in medical dermatology under different titles but with a similar curriculum and goal: to foster dermatologists interested in careers as academic medical dermatologists or as future clinician scientists by means of specialized training and mentorship in complex medical and dermatological issues in the outpatient and inpatient settings. The 2-year program at New York University School of Medicine (New York, New York) also gives fellows the opportunity to earn a master of science in clinical investigation degree. The University of California, San Francisco, program offers protected time for career development.
Epidemiology Training Program
Fellows and residents in the University of Pennsylvania’s dermatology training program may elect to work with the Center for Clinical Epidemiology and Biostatistics and have the opportunity to earn a graduate degree (MSCE or PhD).
Contact Dermatitis and Patch Testing Fellowship
The Dermatology Department at the Cleveland Clinic (Cleveland, Ohio) offers a 1-year contact dermatitis and patch testing fellowship that includes clinical research.
Conclusion
Both traditional and nontraditional fellowship opportunities exist after dermatology residency. This guide serves as an overview of the training programs in dermatopathology, pediatric dermatology, micrographic surgery and dermatologic oncology (procedural dermatology), and cosmetic dermatologic surgery, as well as the fellowships offered at certain institutions for those interested in more specific subspecialties or academia.
1. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in dermatopathology. http://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/100_dermatopathology_2016_1-YR.pdf. Revised April 2014. Effective July 1, 2015. Accessed on February 26, 2015.
2. Subspecialty certification in dermatopathology. The American Board of Dermatology, Inc Web site. http://www.abderm.org/subspecialties/derm.html. Accessed February 26, 2015.
3. American Board of Dermatology (ABD) approved pediatric dermatology fellowship programs. The Society for Pediatric Dermatology Web site. http://pedsderm.net/training/fellowships/abd-approved-pediatric-dermatology-fellowship-programs/. Updated June 9, 2014. Accessed February 26, 2015.
4. Subspecialty certification in pediatric dermatology. The American Board of Dermatology, Inc Web site. http://www.abderm.org/subspecialties/pediatric.html. Accessed February 26, 2015.
5. Non-ABD pediatric dermatology fellowship programs. The Society for Pediatric Dermatology Web site. https://pedsderm.net/training/fellowships/non-abd-pediatric-dermatology-fellowship-programs/. Accessed February 26, 2015.
6. Pediatric dermatology match report. SF Match Web site. https://www.sfmatch.org/SpecialtyInsideAll.aspx?id=16&typ=1&name=Pediatric%20Dermatology#. Accessed March 4, 2015.
7. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in procedural dermatology. https://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/081_procedural_derm_1-YR_07012014.pdf. Effective July 2014. Accessed February 26, 2015.
8. Statistics: micrographic surgery & dermatologic oncology fellowship. SF Match Web site. https://www.sfmatch.org/SpecialtyInsideAll.aspx?id=10&typ=1&name=Micrographic%20Surgery%20and%20Dermatologic%20Oncology#. Accessed March 4, 2015.
9. ASDS cosmetic dermatologic surgery fellowship accreditation program. American Society for Dermatologic Surgery Web site. http://www.asds.net/cosmetic-accreditation/. Accessed February 26, 2015.
1. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in dermatopathology. http://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/100_dermatopathology_2016_1-YR.pdf. Revised April 2014. Effective July 1, 2015. Accessed on February 26, 2015.
2. Subspecialty certification in dermatopathology. The American Board of Dermatology, Inc Web site. http://www.abderm.org/subspecialties/derm.html. Accessed February 26, 2015.
3. American Board of Dermatology (ABD) approved pediatric dermatology fellowship programs. The Society for Pediatric Dermatology Web site. http://pedsderm.net/training/fellowships/abd-approved-pediatric-dermatology-fellowship-programs/. Updated June 9, 2014. Accessed February 26, 2015.
4. Subspecialty certification in pediatric dermatology. The American Board of Dermatology, Inc Web site. http://www.abderm.org/subspecialties/pediatric.html. Accessed February 26, 2015.
5. Non-ABD pediatric dermatology fellowship programs. The Society for Pediatric Dermatology Web site. https://pedsderm.net/training/fellowships/non-abd-pediatric-dermatology-fellowship-programs/. Accessed February 26, 2015.
6. Pediatric dermatology match report. SF Match Web site. https://www.sfmatch.org/SpecialtyInsideAll.aspx?id=16&typ=1&name=Pediatric%20Dermatology#. Accessed March 4, 2015.
7. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in procedural dermatology. https://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/081_procedural_derm_1-YR_07012014.pdf. Effective July 2014. Accessed February 26, 2015.
8. Statistics: micrographic surgery & dermatologic oncology fellowship. SF Match Web site. https://www.sfmatch.org/SpecialtyInsideAll.aspx?id=10&typ=1&name=Micrographic%20Surgery%20and%20Dermatologic%20Oncology#. Accessed March 4, 2015.
9. ASDS cosmetic dermatologic surgery fellowship accreditation program. American Society for Dermatologic Surgery Web site. http://www.asds.net/cosmetic-accreditation/. Accessed February 26, 2015.