User login
RADIANCE II: Positive signal for ultrasound renal denervation
Top-line results released on July 26 from the RADIANCE II trial show the Paradise ultrasound renal denervation system significantly reduces daytime ambulatory systolic blood pressure, compared with a sham procedure at 2 months in patients with mild to moderate uncontrolled hypertension.
The trial was conducted in 224 patients who were previously treated with up to two medications and were randomized while off medication at more than 60 centers in 8 countries. No further details or results were provided.
The pivotal RADIANCE II trial, required for FDA approval, is the third and largest randomized, sham-controlled study following positive results reported by RADIANCE-HTN SOLO and RADIANCE-HTN TRIO, ReCor Medical and its subsidiary Otsuka Medical Devices noted in the announcement.
The field of renal denervation fell out of favor after the largest trial in 535 patients, SYMPLICITY HTN-3, failed to show a significant reduction in systolic blood pressure at 6 months, compared with sham control in resistant hypertension.
A version of this article first appeared on Medscape.com.
Top-line results released on July 26 from the RADIANCE II trial show the Paradise ultrasound renal denervation system significantly reduces daytime ambulatory systolic blood pressure, compared with a sham procedure at 2 months in patients with mild to moderate uncontrolled hypertension.
The trial was conducted in 224 patients who were previously treated with up to two medications and were randomized while off medication at more than 60 centers in 8 countries. No further details or results were provided.
The pivotal RADIANCE II trial, required for FDA approval, is the third and largest randomized, sham-controlled study following positive results reported by RADIANCE-HTN SOLO and RADIANCE-HTN TRIO, ReCor Medical and its subsidiary Otsuka Medical Devices noted in the announcement.
The field of renal denervation fell out of favor after the largest trial in 535 patients, SYMPLICITY HTN-3, failed to show a significant reduction in systolic blood pressure at 6 months, compared with sham control in resistant hypertension.
A version of this article first appeared on Medscape.com.
Top-line results released on July 26 from the RADIANCE II trial show the Paradise ultrasound renal denervation system significantly reduces daytime ambulatory systolic blood pressure, compared with a sham procedure at 2 months in patients with mild to moderate uncontrolled hypertension.
The trial was conducted in 224 patients who were previously treated with up to two medications and were randomized while off medication at more than 60 centers in 8 countries. No further details or results were provided.
The pivotal RADIANCE II trial, required for FDA approval, is the third and largest randomized, sham-controlled study following positive results reported by RADIANCE-HTN SOLO and RADIANCE-HTN TRIO, ReCor Medical and its subsidiary Otsuka Medical Devices noted in the announcement.
The field of renal denervation fell out of favor after the largest trial in 535 patients, SYMPLICITY HTN-3, failed to show a significant reduction in systolic blood pressure at 6 months, compared with sham control in resistant hypertension.
A version of this article first appeared on Medscape.com.
Exceeding exercise guidelines boosts survival, to a point
A new study suggests that going beyond current guidance on moderate and vigorous physical activity levels may add years to one’s life.
Americans are advised to do a minimum of 150-300 minutes a week of moderate exercise or 75-150 minutes a week of vigorous exercise, or an equivalent combination of both, according to U.S. Department of Health and Human Services Physical Activity Guidelines.
Results from more than 100,000 U.S. adults followed for 30 years showed that .
Adults who reported completing four times the minimum recommended activity levels saw no clear incremental mortality benefit but also no harm, according to the study, published in the journal Circulation.
“I think we’re worried more about the lower end and people that are not even doing the minimum, but this should be reassuring to people who like to do a lot of exercise,” senior author Edward Giovannucci, MD, ScD, with the Harvard T.H. Chan School of Public Health, Boston, told this news organization.
Some studies have suggested that long-term, high-intensity exercise (e.g., marathons, triathlons, and long-distance cycling) may be associated with increased risks of atrial fibrillation, coronary artery calcification, and sudden cardiac death.
A recent analysis from the Copenhagen City Heart Study showed a U-shaped association between long-term all-cause mortality and 0 to 2.5 hours and more than 10 hours of weekly, leisure-time sports activities.
Most studies suggesting harm, however, have used only one measurement of physical activity capturing a mix of people who chronically exercise at high levels and those who do it sporadically, which possibly can be harmful, Dr. Giovannucci said. “We were better able to look at consistent long-term activity and saw there was no harm.”
The study included 116,221 participants in the Nurses’ Health Study and the Health Professionals Follow-up Study between 1988 and 2018, who completed up to 15 (median, 11) questionnaires on their health and leisure-time physical activity that were updated every 2 years.
Most were White (96%), 63% were female, and the average age and body mass index over follow-up was 66 years and 26 kg/m2. During 30 years of follow-up, there were 47,596 deaths.
‘Any effort is worthwhile’
The analysis found that individuals who met the guideline for long-term vigorous physical activity (75-150 min/week) cut their adjusted risk of death from cardiovascular disease (CVD) by a whopping 31%, from non-CVD causes by 15%, and all-causes by 19%, compared with those with no long-term vigorous activity.
Those completing two to four times the recommended minimum (150-299 min/week) had a 27%-33% lower risk of CVD mortality, 19% lower risk of non-CVD mortality, and 21%-23% lower risk of all-cause mortality.
Higher levels did not appear to further lower mortality risk. For example, 300-374 min/week of vigorous physical activity was associated with a 32% lower risk of CVD death, 18% lower risk of non-CVD death, and 22% lower risk of dying from any cause.
The analysis also found that individuals who met the guidelines for moderate physical activity had lower CVD, non-CVD, and all-cause mortality risks whether they were active 150-244 min/week (22%, 19%, and 20%, respectively) or 225-299 min/week (21%, 25%, and 20%, respectively), compared with those with almost no long-term moderate activity.
Those fitting in two to four times the recommended minimum (300-599 min/week) had a 28%-38% lower risk of CVD mortality, 25%-27% lower risk of non-CVD mortality, and 26%-31% lower risk of all-cause mortality.
The mortality benefit appeared to plateau, with 600 min/week of moderate physical activity showing associations similar to 300-599 min/week.
“The sweet spot seems to be two to four times the recommended levels but for people who are sedentary, I think one of the key messages that I give my patients is that any effort is worthwhile; that any physical activity, even less than the recommended, has some mortality reduction,” Erin Michos, MD, MHS, associate director of preventive cardiology at Johns Hopkins University, Baltimore, said in an interview.
Indeed, individuals who reported doing just 20-74 minutes of moderate exercise per week had a 19% lower risk of dying from any cause and a 13% lower risk of dying from CVD compared with those doing less.
Current American Heart Association (AHA) recommendations are for at least 150 minutes per week of moderate-intensity aerobic exercise or 75 minutes per week of vigorous aerobic exercise, or a combination of both.
“This suggests that even more is probably better, in the range of two to four times that, so maybe we should move our targets a little bit higher, which is kind of what the Department of Health and Human Services has already done,” said Dr. Michos, who was not involved in the study.
Former AHA president Donna K. Arnett, PhD, who was not involved in the study, said in a statement that “we’ve known for a long time that moderate or intense levels of physical exercise can reduce a person’s risk of both atherosclerotic cardiovascular disease and mortality.
“We have also seen that getting more than 300 minutes of moderate-intensity aerobic physical activity or more than 150 minutes of vigorous-intensity aerobic physical exercise each week may reduce a person’s risk of atherosclerotic cardiovascular disease even further, so it makes sense that getting those extra minutes of exercise may also decrease mortality,” she added.
Mix and match
Dr. Giovannucci noted that the joint effects of the two types of exercise on mortality have not been studied and “there are some questions, for example, about whether doing a lot of moderate activity is sufficient or can you get more benefits by doing vigorous activity also.”
Joint analyses of both exercise intensities found that additional vigorous physical activity was associated with lower mortality among participants with insufficient (less than 300 min/week) levels of moderate exercise but not among those with at least 300 min/week of moderate exercise.
“The main message is that you can get essentially all of the benefit by just doing moderate exercise,” Dr. Giovannucci said. “There’s no magic benefit of doing vigorous [exercise]. But if someone wants to do vigorous, they can get the benefit in about half the time. So if you only have 2-3 hours a week to exercise and can do, say 2 or 3 hours of running, you can get pretty much the maximum benefit.”
Sensitivity analyses showed a consistent association between long-term leisure physical activity and mortality without adjustment for body mass index/calorie intake.
“Some people think the effect of exercise is to lower your body weight or keep it down, which could be one of the benefits, but even independent of that, you get benefits even if it has no effect on your weight,” he said. “So, definitely, that’s important.”
Dr. Michos pointed out that vigorous physical activity may seem daunting for many individuals but that moderate exercise can include activities such as brisk walking, ballroom dancing, active yoga, and recreational swimming.
“The nice thing is that you can really combine or substitute both and get just as similar mortality reductions with moderate physical activity, because a lot of patients may not want to do vigorous activity,” she said. “They don’t want to get on the treadmill; that’s too intimidating or stressful.”
The study was supported by the National Institutes of Health. The authors and Dr. Michos report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study suggests that going beyond current guidance on moderate and vigorous physical activity levels may add years to one’s life.
Americans are advised to do a minimum of 150-300 minutes a week of moderate exercise or 75-150 minutes a week of vigorous exercise, or an equivalent combination of both, according to U.S. Department of Health and Human Services Physical Activity Guidelines.
Results from more than 100,000 U.S. adults followed for 30 years showed that .
Adults who reported completing four times the minimum recommended activity levels saw no clear incremental mortality benefit but also no harm, according to the study, published in the journal Circulation.
“I think we’re worried more about the lower end and people that are not even doing the minimum, but this should be reassuring to people who like to do a lot of exercise,” senior author Edward Giovannucci, MD, ScD, with the Harvard T.H. Chan School of Public Health, Boston, told this news organization.
Some studies have suggested that long-term, high-intensity exercise (e.g., marathons, triathlons, and long-distance cycling) may be associated with increased risks of atrial fibrillation, coronary artery calcification, and sudden cardiac death.
A recent analysis from the Copenhagen City Heart Study showed a U-shaped association between long-term all-cause mortality and 0 to 2.5 hours and more than 10 hours of weekly, leisure-time sports activities.
Most studies suggesting harm, however, have used only one measurement of physical activity capturing a mix of people who chronically exercise at high levels and those who do it sporadically, which possibly can be harmful, Dr. Giovannucci said. “We were better able to look at consistent long-term activity and saw there was no harm.”
The study included 116,221 participants in the Nurses’ Health Study and the Health Professionals Follow-up Study between 1988 and 2018, who completed up to 15 (median, 11) questionnaires on their health and leisure-time physical activity that were updated every 2 years.
Most were White (96%), 63% were female, and the average age and body mass index over follow-up was 66 years and 26 kg/m2. During 30 years of follow-up, there were 47,596 deaths.
‘Any effort is worthwhile’
The analysis found that individuals who met the guideline for long-term vigorous physical activity (75-150 min/week) cut their adjusted risk of death from cardiovascular disease (CVD) by a whopping 31%, from non-CVD causes by 15%, and all-causes by 19%, compared with those with no long-term vigorous activity.
Those completing two to four times the recommended minimum (150-299 min/week) had a 27%-33% lower risk of CVD mortality, 19% lower risk of non-CVD mortality, and 21%-23% lower risk of all-cause mortality.
Higher levels did not appear to further lower mortality risk. For example, 300-374 min/week of vigorous physical activity was associated with a 32% lower risk of CVD death, 18% lower risk of non-CVD death, and 22% lower risk of dying from any cause.
The analysis also found that individuals who met the guidelines for moderate physical activity had lower CVD, non-CVD, and all-cause mortality risks whether they were active 150-244 min/week (22%, 19%, and 20%, respectively) or 225-299 min/week (21%, 25%, and 20%, respectively), compared with those with almost no long-term moderate activity.
Those fitting in two to four times the recommended minimum (300-599 min/week) had a 28%-38% lower risk of CVD mortality, 25%-27% lower risk of non-CVD mortality, and 26%-31% lower risk of all-cause mortality.
The mortality benefit appeared to plateau, with 600 min/week of moderate physical activity showing associations similar to 300-599 min/week.
“The sweet spot seems to be two to four times the recommended levels but for people who are sedentary, I think one of the key messages that I give my patients is that any effort is worthwhile; that any physical activity, even less than the recommended, has some mortality reduction,” Erin Michos, MD, MHS, associate director of preventive cardiology at Johns Hopkins University, Baltimore, said in an interview.
Indeed, individuals who reported doing just 20-74 minutes of moderate exercise per week had a 19% lower risk of dying from any cause and a 13% lower risk of dying from CVD compared with those doing less.
Current American Heart Association (AHA) recommendations are for at least 150 minutes per week of moderate-intensity aerobic exercise or 75 minutes per week of vigorous aerobic exercise, or a combination of both.
“This suggests that even more is probably better, in the range of two to four times that, so maybe we should move our targets a little bit higher, which is kind of what the Department of Health and Human Services has already done,” said Dr. Michos, who was not involved in the study.
Former AHA president Donna K. Arnett, PhD, who was not involved in the study, said in a statement that “we’ve known for a long time that moderate or intense levels of physical exercise can reduce a person’s risk of both atherosclerotic cardiovascular disease and mortality.
“We have also seen that getting more than 300 minutes of moderate-intensity aerobic physical activity or more than 150 minutes of vigorous-intensity aerobic physical exercise each week may reduce a person’s risk of atherosclerotic cardiovascular disease even further, so it makes sense that getting those extra minutes of exercise may also decrease mortality,” she added.
Mix and match
Dr. Giovannucci noted that the joint effects of the two types of exercise on mortality have not been studied and “there are some questions, for example, about whether doing a lot of moderate activity is sufficient or can you get more benefits by doing vigorous activity also.”
Joint analyses of both exercise intensities found that additional vigorous physical activity was associated with lower mortality among participants with insufficient (less than 300 min/week) levels of moderate exercise but not among those with at least 300 min/week of moderate exercise.
“The main message is that you can get essentially all of the benefit by just doing moderate exercise,” Dr. Giovannucci said. “There’s no magic benefit of doing vigorous [exercise]. But if someone wants to do vigorous, they can get the benefit in about half the time. So if you only have 2-3 hours a week to exercise and can do, say 2 or 3 hours of running, you can get pretty much the maximum benefit.”
Sensitivity analyses showed a consistent association between long-term leisure physical activity and mortality without adjustment for body mass index/calorie intake.
“Some people think the effect of exercise is to lower your body weight or keep it down, which could be one of the benefits, but even independent of that, you get benefits even if it has no effect on your weight,” he said. “So, definitely, that’s important.”
Dr. Michos pointed out that vigorous physical activity may seem daunting for many individuals but that moderate exercise can include activities such as brisk walking, ballroom dancing, active yoga, and recreational swimming.
“The nice thing is that you can really combine or substitute both and get just as similar mortality reductions with moderate physical activity, because a lot of patients may not want to do vigorous activity,” she said. “They don’t want to get on the treadmill; that’s too intimidating or stressful.”
The study was supported by the National Institutes of Health. The authors and Dr. Michos report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study suggests that going beyond current guidance on moderate and vigorous physical activity levels may add years to one’s life.
Americans are advised to do a minimum of 150-300 minutes a week of moderate exercise or 75-150 minutes a week of vigorous exercise, or an equivalent combination of both, according to U.S. Department of Health and Human Services Physical Activity Guidelines.
Results from more than 100,000 U.S. adults followed for 30 years showed that .
Adults who reported completing four times the minimum recommended activity levels saw no clear incremental mortality benefit but also no harm, according to the study, published in the journal Circulation.
“I think we’re worried more about the lower end and people that are not even doing the minimum, but this should be reassuring to people who like to do a lot of exercise,” senior author Edward Giovannucci, MD, ScD, with the Harvard T.H. Chan School of Public Health, Boston, told this news organization.
Some studies have suggested that long-term, high-intensity exercise (e.g., marathons, triathlons, and long-distance cycling) may be associated with increased risks of atrial fibrillation, coronary artery calcification, and sudden cardiac death.
A recent analysis from the Copenhagen City Heart Study showed a U-shaped association between long-term all-cause mortality and 0 to 2.5 hours and more than 10 hours of weekly, leisure-time sports activities.
Most studies suggesting harm, however, have used only one measurement of physical activity capturing a mix of people who chronically exercise at high levels and those who do it sporadically, which possibly can be harmful, Dr. Giovannucci said. “We were better able to look at consistent long-term activity and saw there was no harm.”
The study included 116,221 participants in the Nurses’ Health Study and the Health Professionals Follow-up Study between 1988 and 2018, who completed up to 15 (median, 11) questionnaires on their health and leisure-time physical activity that were updated every 2 years.
Most were White (96%), 63% were female, and the average age and body mass index over follow-up was 66 years and 26 kg/m2. During 30 years of follow-up, there were 47,596 deaths.
‘Any effort is worthwhile’
The analysis found that individuals who met the guideline for long-term vigorous physical activity (75-150 min/week) cut their adjusted risk of death from cardiovascular disease (CVD) by a whopping 31%, from non-CVD causes by 15%, and all-causes by 19%, compared with those with no long-term vigorous activity.
Those completing two to four times the recommended minimum (150-299 min/week) had a 27%-33% lower risk of CVD mortality, 19% lower risk of non-CVD mortality, and 21%-23% lower risk of all-cause mortality.
Higher levels did not appear to further lower mortality risk. For example, 300-374 min/week of vigorous physical activity was associated with a 32% lower risk of CVD death, 18% lower risk of non-CVD death, and 22% lower risk of dying from any cause.
The analysis also found that individuals who met the guidelines for moderate physical activity had lower CVD, non-CVD, and all-cause mortality risks whether they were active 150-244 min/week (22%, 19%, and 20%, respectively) or 225-299 min/week (21%, 25%, and 20%, respectively), compared with those with almost no long-term moderate activity.
Those fitting in two to four times the recommended minimum (300-599 min/week) had a 28%-38% lower risk of CVD mortality, 25%-27% lower risk of non-CVD mortality, and 26%-31% lower risk of all-cause mortality.
The mortality benefit appeared to plateau, with 600 min/week of moderate physical activity showing associations similar to 300-599 min/week.
“The sweet spot seems to be two to four times the recommended levels but for people who are sedentary, I think one of the key messages that I give my patients is that any effort is worthwhile; that any physical activity, even less than the recommended, has some mortality reduction,” Erin Michos, MD, MHS, associate director of preventive cardiology at Johns Hopkins University, Baltimore, said in an interview.
Indeed, individuals who reported doing just 20-74 minutes of moderate exercise per week had a 19% lower risk of dying from any cause and a 13% lower risk of dying from CVD compared with those doing less.
Current American Heart Association (AHA) recommendations are for at least 150 minutes per week of moderate-intensity aerobic exercise or 75 minutes per week of vigorous aerobic exercise, or a combination of both.
“This suggests that even more is probably better, in the range of two to four times that, so maybe we should move our targets a little bit higher, which is kind of what the Department of Health and Human Services has already done,” said Dr. Michos, who was not involved in the study.
Former AHA president Donna K. Arnett, PhD, who was not involved in the study, said in a statement that “we’ve known for a long time that moderate or intense levels of physical exercise can reduce a person’s risk of both atherosclerotic cardiovascular disease and mortality.
“We have also seen that getting more than 300 minutes of moderate-intensity aerobic physical activity or more than 150 minutes of vigorous-intensity aerobic physical exercise each week may reduce a person’s risk of atherosclerotic cardiovascular disease even further, so it makes sense that getting those extra minutes of exercise may also decrease mortality,” she added.
Mix and match
Dr. Giovannucci noted that the joint effects of the two types of exercise on mortality have not been studied and “there are some questions, for example, about whether doing a lot of moderate activity is sufficient or can you get more benefits by doing vigorous activity also.”
Joint analyses of both exercise intensities found that additional vigorous physical activity was associated with lower mortality among participants with insufficient (less than 300 min/week) levels of moderate exercise but not among those with at least 300 min/week of moderate exercise.
“The main message is that you can get essentially all of the benefit by just doing moderate exercise,” Dr. Giovannucci said. “There’s no magic benefit of doing vigorous [exercise]. But if someone wants to do vigorous, they can get the benefit in about half the time. So if you only have 2-3 hours a week to exercise and can do, say 2 or 3 hours of running, you can get pretty much the maximum benefit.”
Sensitivity analyses showed a consistent association between long-term leisure physical activity and mortality without adjustment for body mass index/calorie intake.
“Some people think the effect of exercise is to lower your body weight or keep it down, which could be one of the benefits, but even independent of that, you get benefits even if it has no effect on your weight,” he said. “So, definitely, that’s important.”
Dr. Michos pointed out that vigorous physical activity may seem daunting for many individuals but that moderate exercise can include activities such as brisk walking, ballroom dancing, active yoga, and recreational swimming.
“The nice thing is that you can really combine or substitute both and get just as similar mortality reductions with moderate physical activity, because a lot of patients may not want to do vigorous activity,” she said. “They don’t want to get on the treadmill; that’s too intimidating or stressful.”
The study was supported by the National Institutes of Health. The authors and Dr. Michos report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION
Pig heart transplants and the ethical challenges that lie ahead
The long-struggling field of cardiac xenotransplantation has had a very good year.
In January, the University of Maryland made history by keeping a 57-year-old man deemed too sick for a human heart transplant alive for 2 months with a genetically engineered pig heart. On July 12, New York University surgeons reported that heart function was “completely normal with excellent contractility” in two brain-dead patients with pig hearts beating in their chests for 72 hours.
The NYU team approached the project with a decedent model in mind and, after discussions with their IRB equivalent, settled on a 72-hour window because that’s the time they typically keep people ventilated when trying to place their organs, explained Robert A. Montgomery, MD, DPhil, director of the NYU Langone Transplant Institute.
“There’s no real ethical argument for that,” he said in an interview. The consideration is what the family is willing to do when trying to balance doing “something very altruistic and good versus having closure.”
Some families have religious beliefs that burial or interment has to occur very rapidly, whereas others, including one of the family donors, were willing to have the research go on much longer, Dr. Montgomery said. Indeed, the next protocol is being written to consider maintaining the bodies for 2-4 weeks.
“People do vary and you have to kind of accommodate that variation,” he said. “For some people, this isn’t going to be what they’re going to want and that’s why you have to go through the consent process.”
Informed authorization
Arthur L. Caplan, PhD, director of medical ethics at the NYU Langone Medical Center, said the Uniform Anatomical Gift Act recognizes an individual’s right to be an organ donor for transplant and research, but it “mentions nothing about maintaining you in a dead state artificially for research purposes.”
“It’s a major shift in what people are thinking about doing when they die or their relatives die,” he said.
Because organ donation is controlled at the state, not federal, level, the possibility of donating organs for xenotransplantation, like medical aid in dying, will vary between states, observed Dr. Caplan. The best way to ensure that patients whose organs are found to be unsuitable for transplantation have the option is to change state laws.
He noted that cases are already springing up where people are requesting postmortem sperm or egg donations without direct consents from the person who died. “So we have this new area opening up of handling the use of the dead body and we need to bring the law into sync with the possibilities that are out there.”
In terms of informed authorization (informed consent is reserved for the living), Dr. Caplan said there should be written evidence the person wanted to be a donor and, while not required by law, all survivors should give their permission and understand what’s going to be done in terms of the experiment, such as the use of animal parts, when the body will be returned, and the possibility of zoonotic viral infection.
“They have to fully accept that the person is dead and we’re just maintaining them artificially,” he said. “There’s no maintaining anyone who’s alive. That’s a source of a lot of confusion.”
Special committees also need to be appointed with voices from people in organ procurement, law, theology, and patient groups to monitor practice to ensure people who have given permission understood the process, that families have their questions answered independent of the research team, and that clear limits are set on how long experiments will last.
As to what those limits should be: “I think in terms of a week or 2,” Dr. Caplan said. “Obviously we could maintain bodies longer and people have. But I think, culturally in our society, going much past that starts to perhaps stress emotionally, psychologically, family and friends about getting closure.”
“I’m not as comfortable when people say things like, ‘How about 2 months?’ ” he said. “That’s a long time to sort of accept the fact that somebody has died but you can’t complete all the things that go along with the death.”
Dr. Caplan is also uncomfortable with the use of one-off emergency authorizations, as used for Maryland resident David Bennett Sr., who was rejected for standard heart transplantation and required mechanical circulatory support to stay alive.
“It’s too premature, I believe, even to try and rescue someone,” he said. “We need to learn more from the deceased models.”
A better model
Dr. Montgomery noted that primates are very imperfect models for predicting what’s going to happen in humans, and that in order to do xenotransplantation in living humans, there are only two pathways – the one-off emergency authorization or a clinical phase 1 trial.
The decedent model, he said, “will make human trials safer because it’s an intermediate step. You don’t have a living human’s life on the line when you’re trying to do iterative changes and improve the procedure.”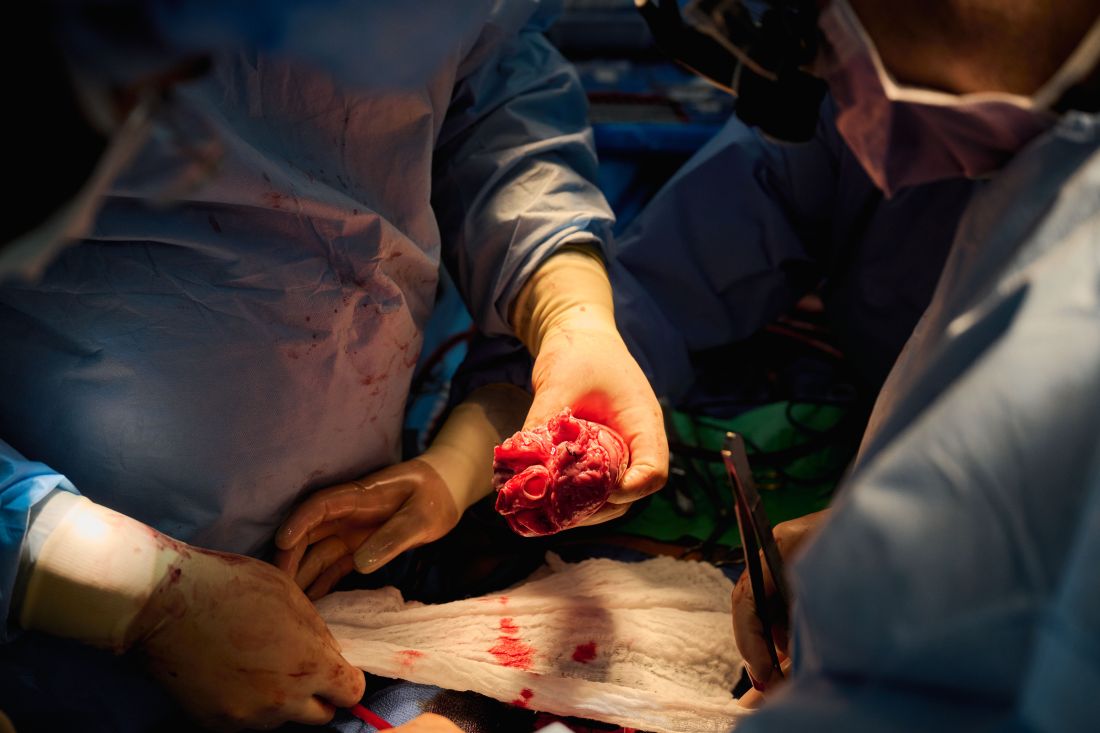
The team, for example, omitted a perfusion pump that was used in the Maryland case and would likely have made its way into phase 1 trials based on baboon data that suggested it was important to have the heart on the pump for hours before it was transplanted, he said. “We didn’t do any of that. We just did it like we would do a regular heart transplant and it started right up, immediately, and started to work.”
The researchers did not release details on the immunosuppression regimen, but noted that, unlike Maryland, they also did not use the experimental anti-CD40 antibody to tamp down the recipients’ immune system.
Although Mr. Bennett’s autopsy did not show any conventional sign of graft rejection, the transplanted pig heart was infected with porcine cytomegalovirus (PCMV) and Mr. Bennett showed traces of DNA from PCMV in his circulation.
Nailing down safety
Dr. Montgomery said he wouldn’t rule out xenotransplantation in a living human, but that the safety issues need to be nailed down. “I think that the tests used on the pig that was the donor for the Bennett case were not sensitive enough for latent virus, and that’s how it slipped through. So there was a bit of going back to the drawing board, really looking at each of the tests, and being sure we had the sensitivity to pick up a latent virus.”
He noted that United Therapeutics, which funded the research and provided the engineered pigs through its subsidiary Revivicor, has created and validated a more sensitive polymerase chain reaction test that covers some 35 different pathogens, microbes, and parasites. NYU has also developed its own platform to repeat the testing and for monitoring after the transplant. “The ones that we’re currently using would have picked up the virus.”
Stuart Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., said “the biggest thing from my perspective is those two amazing families that were willing let this happen. ... If 20 years from now, this is what we’re doing, it’s related to these families being this generous at a really tough time in their lives.”
Dr. Russell said he awaits publication of the data on what the pathology of the heart looks like, but that the experiments “help to give us a lot of reassurance that we don’t need to worry about hyperacute rejection,” which by definition is going to happen in the first 24-48 hours.
That said, longer-term data is essential to potential safety issues. Notably, among the 10 genetic modifications made to the pigs, four were porcine gene knockouts, including a growth hormone receptor knockout to prevent abnormal organ growth inside the recipient’s chest. As a result, the organs seem to be small for the age of the pig and just don’t grow that well, admitted Dr. Montgomery, who said they are currently analyzing this with echocardiography.
Dr. Russell said this may create a sizing issue, but also “if you have a heart that’s more stressed in the pig, from the point of being a donor, maybe it’s not as good a heart as if it was growing normally. But that kind of stuff, I think, is going to take more than two cases and longer-term data to sort out.”
Sharon Hunt, MD, professor emerita, Stanford (Calif.) University Medical Center, and past president of the International Society for Heart Lung Transplantation, said it’s not the technical aspects, but the biology of xenotransplantation that’s really daunting.
“It’s not the physical act of doing it, like they needed a bigger heart or a smaller heart. Those are technical problems but they’ll manage them,” she said. “The big problem is biological – and the bottom line is we don’t really know. We may have overcome hyperacute rejection, which is great, but the rest remains to be seen.”
Dr. Hunt, who worked with heart transplantation pioneer Norman Shumway, MD, and spent decades caring for patients after transplantation, said most families will consent to 24 or 48 hours or even a week of experimentation on a brain-dead loved one, but what the transplant community wants to know is whether this is workable for many months.
“So the fact that the xenotransplant works for 72 hours, yeah, that’s groovy. But, you know, the answer is kind of ‘so what,’ ” she said. “I’d like to see this go for months, like they were trying to do in the human in Maryland.”
For phase 1 trials, even longer-term survival with or without rejection or with rejection that’s treatable is needed, Dr. Hunt suggested.
“We haven’t seen that yet. The Maryland people were very valiant but they lost the cause,” she said. “There’s just so much more to do before we have a viable model to start anything like a phase 1 trial. I’d love it if that happens in my lifetime, but I’m not sure it’s going to.”
Dr. Russell and Dr. Hunt reported no relevant financial relationships. Dr. Caplan reported serving as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position) and is a contributing author and adviser for Medscape.
A version of this article first appeared on Medscape.com.
The long-struggling field of cardiac xenotransplantation has had a very good year.
In January, the University of Maryland made history by keeping a 57-year-old man deemed too sick for a human heart transplant alive for 2 months with a genetically engineered pig heart. On July 12, New York University surgeons reported that heart function was “completely normal with excellent contractility” in two brain-dead patients with pig hearts beating in their chests for 72 hours.
The NYU team approached the project with a decedent model in mind and, after discussions with their IRB equivalent, settled on a 72-hour window because that’s the time they typically keep people ventilated when trying to place their organs, explained Robert A. Montgomery, MD, DPhil, director of the NYU Langone Transplant Institute.
“There’s no real ethical argument for that,” he said in an interview. The consideration is what the family is willing to do when trying to balance doing “something very altruistic and good versus having closure.”
Some families have religious beliefs that burial or interment has to occur very rapidly, whereas others, including one of the family donors, were willing to have the research go on much longer, Dr. Montgomery said. Indeed, the next protocol is being written to consider maintaining the bodies for 2-4 weeks.
“People do vary and you have to kind of accommodate that variation,” he said. “For some people, this isn’t going to be what they’re going to want and that’s why you have to go through the consent process.”
Informed authorization
Arthur L. Caplan, PhD, director of medical ethics at the NYU Langone Medical Center, said the Uniform Anatomical Gift Act recognizes an individual’s right to be an organ donor for transplant and research, but it “mentions nothing about maintaining you in a dead state artificially for research purposes.”
“It’s a major shift in what people are thinking about doing when they die or their relatives die,” he said.
Because organ donation is controlled at the state, not federal, level, the possibility of donating organs for xenotransplantation, like medical aid in dying, will vary between states, observed Dr. Caplan. The best way to ensure that patients whose organs are found to be unsuitable for transplantation have the option is to change state laws.
He noted that cases are already springing up where people are requesting postmortem sperm or egg donations without direct consents from the person who died. “So we have this new area opening up of handling the use of the dead body and we need to bring the law into sync with the possibilities that are out there.”
In terms of informed authorization (informed consent is reserved for the living), Dr. Caplan said there should be written evidence the person wanted to be a donor and, while not required by law, all survivors should give their permission and understand what’s going to be done in terms of the experiment, such as the use of animal parts, when the body will be returned, and the possibility of zoonotic viral infection.
“They have to fully accept that the person is dead and we’re just maintaining them artificially,” he said. “There’s no maintaining anyone who’s alive. That’s a source of a lot of confusion.”
Special committees also need to be appointed with voices from people in organ procurement, law, theology, and patient groups to monitor practice to ensure people who have given permission understood the process, that families have their questions answered independent of the research team, and that clear limits are set on how long experiments will last.
As to what those limits should be: “I think in terms of a week or 2,” Dr. Caplan said. “Obviously we could maintain bodies longer and people have. But I think, culturally in our society, going much past that starts to perhaps stress emotionally, psychologically, family and friends about getting closure.”
“I’m not as comfortable when people say things like, ‘How about 2 months?’ ” he said. “That’s a long time to sort of accept the fact that somebody has died but you can’t complete all the things that go along with the death.”
Dr. Caplan is also uncomfortable with the use of one-off emergency authorizations, as used for Maryland resident David Bennett Sr., who was rejected for standard heart transplantation and required mechanical circulatory support to stay alive.
“It’s too premature, I believe, even to try and rescue someone,” he said. “We need to learn more from the deceased models.”
A better model
Dr. Montgomery noted that primates are very imperfect models for predicting what’s going to happen in humans, and that in order to do xenotransplantation in living humans, there are only two pathways – the one-off emergency authorization or a clinical phase 1 trial.
The decedent model, he said, “will make human trials safer because it’s an intermediate step. You don’t have a living human’s life on the line when you’re trying to do iterative changes and improve the procedure.”
The team, for example, omitted a perfusion pump that was used in the Maryland case and would likely have made its way into phase 1 trials based on baboon data that suggested it was important to have the heart on the pump for hours before it was transplanted, he said. “We didn’t do any of that. We just did it like we would do a regular heart transplant and it started right up, immediately, and started to work.”
The researchers did not release details on the immunosuppression regimen, but noted that, unlike Maryland, they also did not use the experimental anti-CD40 antibody to tamp down the recipients’ immune system.
Although Mr. Bennett’s autopsy did not show any conventional sign of graft rejection, the transplanted pig heart was infected with porcine cytomegalovirus (PCMV) and Mr. Bennett showed traces of DNA from PCMV in his circulation.
Nailing down safety
Dr. Montgomery said he wouldn’t rule out xenotransplantation in a living human, but that the safety issues need to be nailed down. “I think that the tests used on the pig that was the donor for the Bennett case were not sensitive enough for latent virus, and that’s how it slipped through. So there was a bit of going back to the drawing board, really looking at each of the tests, and being sure we had the sensitivity to pick up a latent virus.”
He noted that United Therapeutics, which funded the research and provided the engineered pigs through its subsidiary Revivicor, has created and validated a more sensitive polymerase chain reaction test that covers some 35 different pathogens, microbes, and parasites. NYU has also developed its own platform to repeat the testing and for monitoring after the transplant. “The ones that we’re currently using would have picked up the virus.”
Stuart Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., said “the biggest thing from my perspective is those two amazing families that were willing let this happen. ... If 20 years from now, this is what we’re doing, it’s related to these families being this generous at a really tough time in their lives.”
Dr. Russell said he awaits publication of the data on what the pathology of the heart looks like, but that the experiments “help to give us a lot of reassurance that we don’t need to worry about hyperacute rejection,” which by definition is going to happen in the first 24-48 hours.
That said, longer-term data is essential to potential safety issues. Notably, among the 10 genetic modifications made to the pigs, four were porcine gene knockouts, including a growth hormone receptor knockout to prevent abnormal organ growth inside the recipient’s chest. As a result, the organs seem to be small for the age of the pig and just don’t grow that well, admitted Dr. Montgomery, who said they are currently analyzing this with echocardiography.
Dr. Russell said this may create a sizing issue, but also “if you have a heart that’s more stressed in the pig, from the point of being a donor, maybe it’s not as good a heart as if it was growing normally. But that kind of stuff, I think, is going to take more than two cases and longer-term data to sort out.”
Sharon Hunt, MD, professor emerita, Stanford (Calif.) University Medical Center, and past president of the International Society for Heart Lung Transplantation, said it’s not the technical aspects, but the biology of xenotransplantation that’s really daunting.
“It’s not the physical act of doing it, like they needed a bigger heart or a smaller heart. Those are technical problems but they’ll manage them,” she said. “The big problem is biological – and the bottom line is we don’t really know. We may have overcome hyperacute rejection, which is great, but the rest remains to be seen.”
Dr. Hunt, who worked with heart transplantation pioneer Norman Shumway, MD, and spent decades caring for patients after transplantation, said most families will consent to 24 or 48 hours or even a week of experimentation on a brain-dead loved one, but what the transplant community wants to know is whether this is workable for many months.
“So the fact that the xenotransplant works for 72 hours, yeah, that’s groovy. But, you know, the answer is kind of ‘so what,’ ” she said. “I’d like to see this go for months, like they were trying to do in the human in Maryland.”
For phase 1 trials, even longer-term survival with or without rejection or with rejection that’s treatable is needed, Dr. Hunt suggested.
“We haven’t seen that yet. The Maryland people were very valiant but they lost the cause,” she said. “There’s just so much more to do before we have a viable model to start anything like a phase 1 trial. I’d love it if that happens in my lifetime, but I’m not sure it’s going to.”
Dr. Russell and Dr. Hunt reported no relevant financial relationships. Dr. Caplan reported serving as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position) and is a contributing author and adviser for Medscape.
A version of this article first appeared on Medscape.com.
The long-struggling field of cardiac xenotransplantation has had a very good year.
In January, the University of Maryland made history by keeping a 57-year-old man deemed too sick for a human heart transplant alive for 2 months with a genetically engineered pig heart. On July 12, New York University surgeons reported that heart function was “completely normal with excellent contractility” in two brain-dead patients with pig hearts beating in their chests for 72 hours.
The NYU team approached the project with a decedent model in mind and, after discussions with their IRB equivalent, settled on a 72-hour window because that’s the time they typically keep people ventilated when trying to place their organs, explained Robert A. Montgomery, MD, DPhil, director of the NYU Langone Transplant Institute.
“There’s no real ethical argument for that,” he said in an interview. The consideration is what the family is willing to do when trying to balance doing “something very altruistic and good versus having closure.”
Some families have religious beliefs that burial or interment has to occur very rapidly, whereas others, including one of the family donors, were willing to have the research go on much longer, Dr. Montgomery said. Indeed, the next protocol is being written to consider maintaining the bodies for 2-4 weeks.
“People do vary and you have to kind of accommodate that variation,” he said. “For some people, this isn’t going to be what they’re going to want and that’s why you have to go through the consent process.”
Informed authorization
Arthur L. Caplan, PhD, director of medical ethics at the NYU Langone Medical Center, said the Uniform Anatomical Gift Act recognizes an individual’s right to be an organ donor for transplant and research, but it “mentions nothing about maintaining you in a dead state artificially for research purposes.”
“It’s a major shift in what people are thinking about doing when they die or their relatives die,” he said.
Because organ donation is controlled at the state, not federal, level, the possibility of donating organs for xenotransplantation, like medical aid in dying, will vary between states, observed Dr. Caplan. The best way to ensure that patients whose organs are found to be unsuitable for transplantation have the option is to change state laws.
He noted that cases are already springing up where people are requesting postmortem sperm or egg donations without direct consents from the person who died. “So we have this new area opening up of handling the use of the dead body and we need to bring the law into sync with the possibilities that are out there.”
In terms of informed authorization (informed consent is reserved for the living), Dr. Caplan said there should be written evidence the person wanted to be a donor and, while not required by law, all survivors should give their permission and understand what’s going to be done in terms of the experiment, such as the use of animal parts, when the body will be returned, and the possibility of zoonotic viral infection.
“They have to fully accept that the person is dead and we’re just maintaining them artificially,” he said. “There’s no maintaining anyone who’s alive. That’s a source of a lot of confusion.”
Special committees also need to be appointed with voices from people in organ procurement, law, theology, and patient groups to monitor practice to ensure people who have given permission understood the process, that families have their questions answered independent of the research team, and that clear limits are set on how long experiments will last.
As to what those limits should be: “I think in terms of a week or 2,” Dr. Caplan said. “Obviously we could maintain bodies longer and people have. But I think, culturally in our society, going much past that starts to perhaps stress emotionally, psychologically, family and friends about getting closure.”
“I’m not as comfortable when people say things like, ‘How about 2 months?’ ” he said. “That’s a long time to sort of accept the fact that somebody has died but you can’t complete all the things that go along with the death.”
Dr. Caplan is also uncomfortable with the use of one-off emergency authorizations, as used for Maryland resident David Bennett Sr., who was rejected for standard heart transplantation and required mechanical circulatory support to stay alive.
“It’s too premature, I believe, even to try and rescue someone,” he said. “We need to learn more from the deceased models.”
A better model
Dr. Montgomery noted that primates are very imperfect models for predicting what’s going to happen in humans, and that in order to do xenotransplantation in living humans, there are only two pathways – the one-off emergency authorization or a clinical phase 1 trial.
The decedent model, he said, “will make human trials safer because it’s an intermediate step. You don’t have a living human’s life on the line when you’re trying to do iterative changes and improve the procedure.”
The team, for example, omitted a perfusion pump that was used in the Maryland case and would likely have made its way into phase 1 trials based on baboon data that suggested it was important to have the heart on the pump for hours before it was transplanted, he said. “We didn’t do any of that. We just did it like we would do a regular heart transplant and it started right up, immediately, and started to work.”
The researchers did not release details on the immunosuppression regimen, but noted that, unlike Maryland, they also did not use the experimental anti-CD40 antibody to tamp down the recipients’ immune system.
Although Mr. Bennett’s autopsy did not show any conventional sign of graft rejection, the transplanted pig heart was infected with porcine cytomegalovirus (PCMV) and Mr. Bennett showed traces of DNA from PCMV in his circulation.
Nailing down safety
Dr. Montgomery said he wouldn’t rule out xenotransplantation in a living human, but that the safety issues need to be nailed down. “I think that the tests used on the pig that was the donor for the Bennett case were not sensitive enough for latent virus, and that’s how it slipped through. So there was a bit of going back to the drawing board, really looking at each of the tests, and being sure we had the sensitivity to pick up a latent virus.”
He noted that United Therapeutics, which funded the research and provided the engineered pigs through its subsidiary Revivicor, has created and validated a more sensitive polymerase chain reaction test that covers some 35 different pathogens, microbes, and parasites. NYU has also developed its own platform to repeat the testing and for monitoring after the transplant. “The ones that we’re currently using would have picked up the virus.”
Stuart Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., said “the biggest thing from my perspective is those two amazing families that were willing let this happen. ... If 20 years from now, this is what we’re doing, it’s related to these families being this generous at a really tough time in their lives.”
Dr. Russell said he awaits publication of the data on what the pathology of the heart looks like, but that the experiments “help to give us a lot of reassurance that we don’t need to worry about hyperacute rejection,” which by definition is going to happen in the first 24-48 hours.
That said, longer-term data is essential to potential safety issues. Notably, among the 10 genetic modifications made to the pigs, four were porcine gene knockouts, including a growth hormone receptor knockout to prevent abnormal organ growth inside the recipient’s chest. As a result, the organs seem to be small for the age of the pig and just don’t grow that well, admitted Dr. Montgomery, who said they are currently analyzing this with echocardiography.
Dr. Russell said this may create a sizing issue, but also “if you have a heart that’s more stressed in the pig, from the point of being a donor, maybe it’s not as good a heart as if it was growing normally. But that kind of stuff, I think, is going to take more than two cases and longer-term data to sort out.”
Sharon Hunt, MD, professor emerita, Stanford (Calif.) University Medical Center, and past president of the International Society for Heart Lung Transplantation, said it’s not the technical aspects, but the biology of xenotransplantation that’s really daunting.
“It’s not the physical act of doing it, like they needed a bigger heart or a smaller heart. Those are technical problems but they’ll manage them,” she said. “The big problem is biological – and the bottom line is we don’t really know. We may have overcome hyperacute rejection, which is great, but the rest remains to be seen.”
Dr. Hunt, who worked with heart transplantation pioneer Norman Shumway, MD, and spent decades caring for patients after transplantation, said most families will consent to 24 or 48 hours or even a week of experimentation on a brain-dead loved one, but what the transplant community wants to know is whether this is workable for many months.
“So the fact that the xenotransplant works for 72 hours, yeah, that’s groovy. But, you know, the answer is kind of ‘so what,’ ” she said. “I’d like to see this go for months, like they were trying to do in the human in Maryland.”
For phase 1 trials, even longer-term survival with or without rejection or with rejection that’s treatable is needed, Dr. Hunt suggested.
“We haven’t seen that yet. The Maryland people were very valiant but they lost the cause,” she said. “There’s just so much more to do before we have a viable model to start anything like a phase 1 trial. I’d love it if that happens in my lifetime, but I’m not sure it’s going to.”
Dr. Russell and Dr. Hunt reported no relevant financial relationships. Dr. Caplan reported serving as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position) and is a contributing author and adviser for Medscape.
A version of this article first appeared on Medscape.com.
Overly tight sodium restriction may worsen HFpEF outcomes
Cutting out almost all salt when preparing meals was associated with a worse prognosis in patients with heart failure with preserved ejection fraction (HFpEF), according to the results of a new study.
Results from a post hoc analysis of the TOPCAT trial show that those with a cooking salt score of zero were at significantly higher risk of the primary outcome of cardiovascular (CV) death, HF hospitalization, and aborted cardiac arrest than those whose score was above zero. Survival was similar in both groups.
“Some patients restrict dietary salt intake as least as possible according to their physicians’ words or their own understanding. However, the present study found that, in patients with heart failure with preserved ejection fraction, overstrict salt restriction could lead to poor prognosis – mainly heart failure hospitalization,” explained professor Chen Liu, MD, and Weihao Liang, MD, Sun Yat-sen University First Affiliated Hospital, Guangzhou, Guangdong, China.
“Thus, when giving salt restriction advice to patients with heart failure with preserved ejection fraction, physicians should be careful instead of just saying “as least as possible,” they said in an email to this news organization.
The study was published in the journal Heart.
The authors note that HF guidelines recommend reduced salt intake, but there’s a lack of high-quality evidence to support those recommendations and no consensus on how low to go.
Previous studies have shown that reduced dietary sodium intake was associated with worse survival and higher readmission rate in patients with HF, whereas the SODIUM HF trial reported earlier this year that dietary sodium intake of less than 100 mmol (1,500 mg) per day did not improve 1-year clinical outcomes but moderately improved quality of life and New York Heart Association functional class.
“In daily clinical practice, we noticed that some physicians advised patients with heart failure to take salt as least as possible, but it could lead to hyponatremia and loss of appetite, which has been frequently reported to be associated with poor prognosis. Thus, we wanted to investigate the potential effect of overstrict salt restriction,” Dr. Liu and Dr. Liang explained.
The investigators examined data from 1,713 participants aged 50 and older with HFpEF (left ventricular ejection fraction 45% or greater) in the phase 3 TOPCAT trial, excluding those from Russia and Georgia. Patients self-reported how much salt they added to cooking staples, such as rice, pasta, potatoes, soup, meat, and vegetables, and were scored as 0 (none), 1 (⅛ teaspoon), 2 (¼ teaspoon), and 3 (½ teaspoon or more) points. Median follow-up was 2.9 years.
TOPCAT failed to show that spironolactone improved CV outcomes over placebo, but regional differences in data from Russia/Georgia and the Americas have raised concerns about its validity.
In the present analysis, almost half the participants (816) had a cooking salt score of 0, 56.4% were male, and 80.8% were White. They were more likely than participants with a salt score greater than zero to have a previous HF hospitalization, diabetes, poor renal function, and a lower ejection fraction (57% vs. 60%). Half were randomly assigned to spironolactone.
Compared with patients with a cooking salt score of 0, patients with a cooking salt score greater than 0 had significantly lower risks of the primary outcome (hazard ratio, 0.760; P = .002) and HF hospitalization (HR, 0.737; P = .003) but not all-cause (HR, 0.838) or CV (HR, 0.782) death.
The findings were consistent after full adjustment, with hazard ratios of 0.834 (P = .046), 0.791 (P = .024), 0.944, and 0.872, respectively.
Results of subgroup analyses suggested that patients aged 70 years or younger (HR, 0.644) and those of Black and other ethnicities (HR, 0.574) were at greater risk of the primary outcome from aggressive restriction of cooking salt.
“It was an interesting but unproved finding,” Dr. Liu and Dr. Liang observed. “One possible explanation is the difference in RAAS [renin-angiotensin-aldosterone system] physiology and its response to salt restriction among races, and the other is the difference in accustomed food, because the cooking salt score only accounted for sodium added during cooking but not sodium from ingredients.”
Spearman correlation analyses showed that the cooking salt score correlated significantly with systolic and diastolic blood pressure, serum sodium, and chloronium levels but not with plasma volume status, suggesting that low sodium intake did not have an intravascular volume contraction effect on patients with HFpEF.
The authors pointed out that the salt score was self-reported, hemodynamic parameters were seldom acquired in TOPCAT, and that reverse causation between low dietary sodium intake and worse HF might still exist, despite a propensity score-matching sensitivity analysis.
Reached for comment, Mary Norine Walsh, MD, the medical director of heart failure and cardiac transplantation, Ascension St. Vincent Heart Center, Indianapolis, said in an email that the authors appropriately excluded patients enrolled from Russia and Georgia because of concerns about the representativeness of patients with HFpEF in these two countries, which has been previously demonstrated.
“What limits the importance of the authors’ findings, which they acknowledge, is that the sodium intake for each patient was self-reported,” she said. “No confirmatory testing was done and recall bias could clearly have played a role.”
“Last, many patients with HFpEF have significant volume overload and dyspnea and appropriate sodium restriction is needed to help address symptoms and achieve a euvolemic state,” added Dr. Walsh, a past president of the American College of Cardiology.
Future trials are needed to determine an optimal salt restriction range for patients with heart failure, Dr. Liu and Dr. Liang suggested. “A randomized controlled trial may be hard to achieve because it is difficult to set a perfect control group. Therefore, an analysis using real-world data with a dose-response curve could be ideal.”
The study was funded by the National Natural Science Foundation of China, Guangdong Natural Science Foundation, and China Postdoctoral Science Foundation. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Cutting out almost all salt when preparing meals was associated with a worse prognosis in patients with heart failure with preserved ejection fraction (HFpEF), according to the results of a new study.
Results from a post hoc analysis of the TOPCAT trial show that those with a cooking salt score of zero were at significantly higher risk of the primary outcome of cardiovascular (CV) death, HF hospitalization, and aborted cardiac arrest than those whose score was above zero. Survival was similar in both groups.
“Some patients restrict dietary salt intake as least as possible according to their physicians’ words or their own understanding. However, the present study found that, in patients with heart failure with preserved ejection fraction, overstrict salt restriction could lead to poor prognosis – mainly heart failure hospitalization,” explained professor Chen Liu, MD, and Weihao Liang, MD, Sun Yat-sen University First Affiliated Hospital, Guangzhou, Guangdong, China.
“Thus, when giving salt restriction advice to patients with heart failure with preserved ejection fraction, physicians should be careful instead of just saying “as least as possible,” they said in an email to this news organization.
The study was published in the journal Heart.
The authors note that HF guidelines recommend reduced salt intake, but there’s a lack of high-quality evidence to support those recommendations and no consensus on how low to go.
Previous studies have shown that reduced dietary sodium intake was associated with worse survival and higher readmission rate in patients with HF, whereas the SODIUM HF trial reported earlier this year that dietary sodium intake of less than 100 mmol (1,500 mg) per day did not improve 1-year clinical outcomes but moderately improved quality of life and New York Heart Association functional class.
“In daily clinical practice, we noticed that some physicians advised patients with heart failure to take salt as least as possible, but it could lead to hyponatremia and loss of appetite, which has been frequently reported to be associated with poor prognosis. Thus, we wanted to investigate the potential effect of overstrict salt restriction,” Dr. Liu and Dr. Liang explained.
The investigators examined data from 1,713 participants aged 50 and older with HFpEF (left ventricular ejection fraction 45% or greater) in the phase 3 TOPCAT trial, excluding those from Russia and Georgia. Patients self-reported how much salt they added to cooking staples, such as rice, pasta, potatoes, soup, meat, and vegetables, and were scored as 0 (none), 1 (⅛ teaspoon), 2 (¼ teaspoon), and 3 (½ teaspoon or more) points. Median follow-up was 2.9 years.
TOPCAT failed to show that spironolactone improved CV outcomes over placebo, but regional differences in data from Russia/Georgia and the Americas have raised concerns about its validity.
In the present analysis, almost half the participants (816) had a cooking salt score of 0, 56.4% were male, and 80.8% were White. They were more likely than participants with a salt score greater than zero to have a previous HF hospitalization, diabetes, poor renal function, and a lower ejection fraction (57% vs. 60%). Half were randomly assigned to spironolactone.
Compared with patients with a cooking salt score of 0, patients with a cooking salt score greater than 0 had significantly lower risks of the primary outcome (hazard ratio, 0.760; P = .002) and HF hospitalization (HR, 0.737; P = .003) but not all-cause (HR, 0.838) or CV (HR, 0.782) death.
The findings were consistent after full adjustment, with hazard ratios of 0.834 (P = .046), 0.791 (P = .024), 0.944, and 0.872, respectively.
Results of subgroup analyses suggested that patients aged 70 years or younger (HR, 0.644) and those of Black and other ethnicities (HR, 0.574) were at greater risk of the primary outcome from aggressive restriction of cooking salt.
“It was an interesting but unproved finding,” Dr. Liu and Dr. Liang observed. “One possible explanation is the difference in RAAS [renin-angiotensin-aldosterone system] physiology and its response to salt restriction among races, and the other is the difference in accustomed food, because the cooking salt score only accounted for sodium added during cooking but not sodium from ingredients.”
Spearman correlation analyses showed that the cooking salt score correlated significantly with systolic and diastolic blood pressure, serum sodium, and chloronium levels but not with plasma volume status, suggesting that low sodium intake did not have an intravascular volume contraction effect on patients with HFpEF.
The authors pointed out that the salt score was self-reported, hemodynamic parameters were seldom acquired in TOPCAT, and that reverse causation between low dietary sodium intake and worse HF might still exist, despite a propensity score-matching sensitivity analysis.
Reached for comment, Mary Norine Walsh, MD, the medical director of heart failure and cardiac transplantation, Ascension St. Vincent Heart Center, Indianapolis, said in an email that the authors appropriately excluded patients enrolled from Russia and Georgia because of concerns about the representativeness of patients with HFpEF in these two countries, which has been previously demonstrated.
“What limits the importance of the authors’ findings, which they acknowledge, is that the sodium intake for each patient was self-reported,” she said. “No confirmatory testing was done and recall bias could clearly have played a role.”
“Last, many patients with HFpEF have significant volume overload and dyspnea and appropriate sodium restriction is needed to help address symptoms and achieve a euvolemic state,” added Dr. Walsh, a past president of the American College of Cardiology.
Future trials are needed to determine an optimal salt restriction range for patients with heart failure, Dr. Liu and Dr. Liang suggested. “A randomized controlled trial may be hard to achieve because it is difficult to set a perfect control group. Therefore, an analysis using real-world data with a dose-response curve could be ideal.”
The study was funded by the National Natural Science Foundation of China, Guangdong Natural Science Foundation, and China Postdoctoral Science Foundation. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Cutting out almost all salt when preparing meals was associated with a worse prognosis in patients with heart failure with preserved ejection fraction (HFpEF), according to the results of a new study.
Results from a post hoc analysis of the TOPCAT trial show that those with a cooking salt score of zero were at significantly higher risk of the primary outcome of cardiovascular (CV) death, HF hospitalization, and aborted cardiac arrest than those whose score was above zero. Survival was similar in both groups.
“Some patients restrict dietary salt intake as least as possible according to their physicians’ words or their own understanding. However, the present study found that, in patients with heart failure with preserved ejection fraction, overstrict salt restriction could lead to poor prognosis – mainly heart failure hospitalization,” explained professor Chen Liu, MD, and Weihao Liang, MD, Sun Yat-sen University First Affiliated Hospital, Guangzhou, Guangdong, China.
“Thus, when giving salt restriction advice to patients with heart failure with preserved ejection fraction, physicians should be careful instead of just saying “as least as possible,” they said in an email to this news organization.
The study was published in the journal Heart.
The authors note that HF guidelines recommend reduced salt intake, but there’s a lack of high-quality evidence to support those recommendations and no consensus on how low to go.
Previous studies have shown that reduced dietary sodium intake was associated with worse survival and higher readmission rate in patients with HF, whereas the SODIUM HF trial reported earlier this year that dietary sodium intake of less than 100 mmol (1,500 mg) per day did not improve 1-year clinical outcomes but moderately improved quality of life and New York Heart Association functional class.
“In daily clinical practice, we noticed that some physicians advised patients with heart failure to take salt as least as possible, but it could lead to hyponatremia and loss of appetite, which has been frequently reported to be associated with poor prognosis. Thus, we wanted to investigate the potential effect of overstrict salt restriction,” Dr. Liu and Dr. Liang explained.
The investigators examined data from 1,713 participants aged 50 and older with HFpEF (left ventricular ejection fraction 45% or greater) in the phase 3 TOPCAT trial, excluding those from Russia and Georgia. Patients self-reported how much salt they added to cooking staples, such as rice, pasta, potatoes, soup, meat, and vegetables, and were scored as 0 (none), 1 (⅛ teaspoon), 2 (¼ teaspoon), and 3 (½ teaspoon or more) points. Median follow-up was 2.9 years.
TOPCAT failed to show that spironolactone improved CV outcomes over placebo, but regional differences in data from Russia/Georgia and the Americas have raised concerns about its validity.
In the present analysis, almost half the participants (816) had a cooking salt score of 0, 56.4% were male, and 80.8% were White. They were more likely than participants with a salt score greater than zero to have a previous HF hospitalization, diabetes, poor renal function, and a lower ejection fraction (57% vs. 60%). Half were randomly assigned to spironolactone.
Compared with patients with a cooking salt score of 0, patients with a cooking salt score greater than 0 had significantly lower risks of the primary outcome (hazard ratio, 0.760; P = .002) and HF hospitalization (HR, 0.737; P = .003) but not all-cause (HR, 0.838) or CV (HR, 0.782) death.
The findings were consistent after full adjustment, with hazard ratios of 0.834 (P = .046), 0.791 (P = .024), 0.944, and 0.872, respectively.
Results of subgroup analyses suggested that patients aged 70 years or younger (HR, 0.644) and those of Black and other ethnicities (HR, 0.574) were at greater risk of the primary outcome from aggressive restriction of cooking salt.
“It was an interesting but unproved finding,” Dr. Liu and Dr. Liang observed. “One possible explanation is the difference in RAAS [renin-angiotensin-aldosterone system] physiology and its response to salt restriction among races, and the other is the difference in accustomed food, because the cooking salt score only accounted for sodium added during cooking but not sodium from ingredients.”
Spearman correlation analyses showed that the cooking salt score correlated significantly with systolic and diastolic blood pressure, serum sodium, and chloronium levels but not with plasma volume status, suggesting that low sodium intake did not have an intravascular volume contraction effect on patients with HFpEF.
The authors pointed out that the salt score was self-reported, hemodynamic parameters were seldom acquired in TOPCAT, and that reverse causation between low dietary sodium intake and worse HF might still exist, despite a propensity score-matching sensitivity analysis.
Reached for comment, Mary Norine Walsh, MD, the medical director of heart failure and cardiac transplantation, Ascension St. Vincent Heart Center, Indianapolis, said in an email that the authors appropriately excluded patients enrolled from Russia and Georgia because of concerns about the representativeness of patients with HFpEF in these two countries, which has been previously demonstrated.
“What limits the importance of the authors’ findings, which they acknowledge, is that the sodium intake for each patient was self-reported,” she said. “No confirmatory testing was done and recall bias could clearly have played a role.”
“Last, many patients with HFpEF have significant volume overload and dyspnea and appropriate sodium restriction is needed to help address symptoms and achieve a euvolemic state,” added Dr. Walsh, a past president of the American College of Cardiology.
Future trials are needed to determine an optimal salt restriction range for patients with heart failure, Dr. Liu and Dr. Liang suggested. “A randomized controlled trial may be hard to achieve because it is difficult to set a perfect control group. Therefore, an analysis using real-world data with a dose-response curve could be ideal.”
The study was funded by the National Natural Science Foundation of China, Guangdong Natural Science Foundation, and China Postdoctoral Science Foundation. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM HEART
Interventional imagers take on central role and more radiation
Interventional echocardiographers have become an increasingly critical part of the structural heart team but may be paying the price in terms of radiation exposure, a new study suggests.
Results showed that interventional echocardiographers receive threefold higher head-level radiation doses than interventional cardiologists during left atrial appendage occlusion (LAAO) closures and 11-fold higher doses during mitral valve transcatheter edge-to-edge repair (TEER).
“Over the last 5-10 years there’s been exponential growth in these two procedures, TEER and LAAO, and while that’s been very exciting, I think there hasn’t been as much research into how to protect these individuals,” lead author David A. McNamara, MD, MPH, Spectrum Health, Grand Rapids, Mich., told this news organization.
The study was published in JAMA Network Open.
Previous studies have focused largely on radiation exposure and mitigation efforts during coronary interventions, but the room set-up for LAAO and TEER and shielding techniques to mitigate radiation exposure are vastly different, he noted.
A 2017 study reported that radiation exposure was significantly higher for imaging specialists than structural heart specialists and varied by procedure type.
For the current study, Dr. McNamara, an echocardiographer by training, and colleagues collected data from 30 consecutive LAAO and 30 consecutive TEER procedures performed at their institution between July 2016 and January 2018.
Interventional imagers, interventional cardiologists, and sonographers all wore a lead skirt, apron, and thyroid collar, as well as a dosimeter to collect radiation data.
Interventional cardiologists stood immediately adjacent to the procedure table and used a ceiling-mounted, upper-body lead shield and a lower-body shield extending from the table to the floor. The echocardiographer stood at the patient’s head and used a mobile accessory shield raised to a height that allowed the imager to extend their arms over the shield to manipulate a transesophageal echocardiogram probe throughout the case.
The median fluoroscopy time was 9.2 minutes for LAAO and 20.9 minutes for TEER. The median air kerma was 164 mGy and 109 mGy, respectively.
Interventional echocardiographers received a median per case radiation dose of 10.6 µSv, compared with 2.1 µSv for interventional cardiologists. The result was similar for TEER (10.5 vs. 0.9 µSv) and LAAO (10.6 vs. 3.5 µSv; P < .001 for all).
The odds of interventional echocardiographers having a radiation dose greater than 20 µSV were 7.5 times greater than for interventional cardiologists (P < .001).
“It’s not the direction of the association, but really the magnitude is what surprised us,” observed Dr. McNamara.
The team was pleasantly surprised, he said, that sonographers, a “vastly understudied group,” received significantly lower median radiation doses than interventional imagers during LAAO (0.2 µSV) and TEER procedures (0.0 µSv; P < .001 for both).
The average distances from the radiation source were 26 cm (10.2 inches) for the echocardiographer, 36 cm (14.2 inches) for the interventional cardiologist, and 250 cm (8.2 feet) for the sonographer.
“These folks [sonographers] were much further away than both the physicians performing these cases, and that is what we hypothesize drove their very low rates, but that should also help inform our mitigation techniques for physicians and for all other cath lab members in the room,” Dr. McNamara said.
He noted that Spectrum Health has been at the forefront in terms of research into radiation exposure and mitigation, has good institutional radiation safety education, and used dose-lowering fluoroscopy systems (AlluraClarity, Philips) with real-time image noise reduction technology and a frame rate of 15 frames per second for the study. “So we’re hopeful that this actually represents a somewhat best-case scenario for what is being done at multiple institutions throughout the nation.”
Nevertheless, there is a huge amount of variability in radiation exposure, Dr. McNamara observed. “First and foremost, we really just have to identify our problem and highlight that this is something that needs some advocacy from our [professional] groups.”
Sunil Rao, MD, the newly minted president of the Society of Cardiovascular Angiography and Interventions (SCAI), said, “This is a really important study, because it expands the potential occupational hazards outside of what we traditionally think of as the team that does interventional procedures ... we have to recognize that the procedures we’re doing in the cath lab have changed.”

“Showing that our colleagues are getting 3-10 times radiation exposure is a really important piece of information to have out there. I think it’s really sort of a call to action,” Dr. Rao, professor of medicine at Duke University, Durham, N.C., told this news organization.
Nevertheless, he observed that practices have shifted somewhat since the study and that interventional cardiologists working with imaging physicians are more cognizant of radiation exposure issues.
“When I talk with our folks here that are doing structural heart procedures, they’re making sure that they’re not stepping on the fluoro pedal while the echocardiographer is manipulating the TE probe,” Dr. Rao said. “The echocardiographer is oftentimes using a much bigger shield than what was described in the study, and remember there’s an exponential decrease in the radiation exposure by distance, so they’re stepping back during the fluoroscopy time.”
Although the volume of TEER and LAAO procedures, as well as tricuspid interventions, will continue to climb, Dr. Rao said he expects radiation exposure to the imaging cardiologist will fall thanks to greater use of newer-generation imaging systems with dose-reduction features and better shielding strategies.
He noted that several of SCAI’s “best practices” documents call attention to radiation safety and that SCAI is creating a pathway where imaging cardiologists can become fellows of the society, which was traditionally reserved for interventionalists.
Still, imaging and cardiovascular societies have yet to endorse standardized safety procedures for interventional imagers, nor is information routinely collected on radiation exposure in national registries.
“We just don’t have the budgets or the interest nationally to do that kind of thing, so it has to be done locally,” Dr. Rao said. “And the person who I think is responsible for that is really the cath lab director and the cath lab nurse manager, who really should work hand-in-glove to make sure that radiation safety is at the top of the priority list.”
The study was funded by the Frederik Meijer Heart & Vascular Institute, Spectrum Health, and by Corindus. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, approval of the manuscript; and the decision to submit the manuscript for publication. Senior author Ryan Madder, MD, reports receiving research support, speaker honoraria, and grants, and serving on the advisory board of Corindus. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
Interventional echocardiographers have become an increasingly critical part of the structural heart team but may be paying the price in terms of radiation exposure, a new study suggests.
Results showed that interventional echocardiographers receive threefold higher head-level radiation doses than interventional cardiologists during left atrial appendage occlusion (LAAO) closures and 11-fold higher doses during mitral valve transcatheter edge-to-edge repair (TEER).
“Over the last 5-10 years there’s been exponential growth in these two procedures, TEER and LAAO, and while that’s been very exciting, I think there hasn’t been as much research into how to protect these individuals,” lead author David A. McNamara, MD, MPH, Spectrum Health, Grand Rapids, Mich., told this news organization.
The study was published in JAMA Network Open.
Previous studies have focused largely on radiation exposure and mitigation efforts during coronary interventions, but the room set-up for LAAO and TEER and shielding techniques to mitigate radiation exposure are vastly different, he noted.
A 2017 study reported that radiation exposure was significantly higher for imaging specialists than structural heart specialists and varied by procedure type.
For the current study, Dr. McNamara, an echocardiographer by training, and colleagues collected data from 30 consecutive LAAO and 30 consecutive TEER procedures performed at their institution between July 2016 and January 2018.
Interventional imagers, interventional cardiologists, and sonographers all wore a lead skirt, apron, and thyroid collar, as well as a dosimeter to collect radiation data.
Interventional cardiologists stood immediately adjacent to the procedure table and used a ceiling-mounted, upper-body lead shield and a lower-body shield extending from the table to the floor. The echocardiographer stood at the patient’s head and used a mobile accessory shield raised to a height that allowed the imager to extend their arms over the shield to manipulate a transesophageal echocardiogram probe throughout the case.
The median fluoroscopy time was 9.2 minutes for LAAO and 20.9 minutes for TEER. The median air kerma was 164 mGy and 109 mGy, respectively.
Interventional echocardiographers received a median per case radiation dose of 10.6 µSv, compared with 2.1 µSv for interventional cardiologists. The result was similar for TEER (10.5 vs. 0.9 µSv) and LAAO (10.6 vs. 3.5 µSv; P < .001 for all).
The odds of interventional echocardiographers having a radiation dose greater than 20 µSV were 7.5 times greater than for interventional cardiologists (P < .001).
“It’s not the direction of the association, but really the magnitude is what surprised us,” observed Dr. McNamara.
The team was pleasantly surprised, he said, that sonographers, a “vastly understudied group,” received significantly lower median radiation doses than interventional imagers during LAAO (0.2 µSV) and TEER procedures (0.0 µSv; P < .001 for both).
The average distances from the radiation source were 26 cm (10.2 inches) for the echocardiographer, 36 cm (14.2 inches) for the interventional cardiologist, and 250 cm (8.2 feet) for the sonographer.
“These folks [sonographers] were much further away than both the physicians performing these cases, and that is what we hypothesize drove their very low rates, but that should also help inform our mitigation techniques for physicians and for all other cath lab members in the room,” Dr. McNamara said.
He noted that Spectrum Health has been at the forefront in terms of research into radiation exposure and mitigation, has good institutional radiation safety education, and used dose-lowering fluoroscopy systems (AlluraClarity, Philips) with real-time image noise reduction technology and a frame rate of 15 frames per second for the study. “So we’re hopeful that this actually represents a somewhat best-case scenario for what is being done at multiple institutions throughout the nation.”
Nevertheless, there is a huge amount of variability in radiation exposure, Dr. McNamara observed. “First and foremost, we really just have to identify our problem and highlight that this is something that needs some advocacy from our [professional] groups.”
Sunil Rao, MD, the newly minted president of the Society of Cardiovascular Angiography and Interventions (SCAI), said, “This is a really important study, because it expands the potential occupational hazards outside of what we traditionally think of as the team that does interventional procedures ... we have to recognize that the procedures we’re doing in the cath lab have changed.”
“Showing that our colleagues are getting 3-10 times radiation exposure is a really important piece of information to have out there. I think it’s really sort of a call to action,” Dr. Rao, professor of medicine at Duke University, Durham, N.C., told this news organization.
Nevertheless, he observed that practices have shifted somewhat since the study and that interventional cardiologists working with imaging physicians are more cognizant of radiation exposure issues.
“When I talk with our folks here that are doing structural heart procedures, they’re making sure that they’re not stepping on the fluoro pedal while the echocardiographer is manipulating the TE probe,” Dr. Rao said. “The echocardiographer is oftentimes using a much bigger shield than what was described in the study, and remember there’s an exponential decrease in the radiation exposure by distance, so they’re stepping back during the fluoroscopy time.”
Although the volume of TEER and LAAO procedures, as well as tricuspid interventions, will continue to climb, Dr. Rao said he expects radiation exposure to the imaging cardiologist will fall thanks to greater use of newer-generation imaging systems with dose-reduction features and better shielding strategies.
He noted that several of SCAI’s “best practices” documents call attention to radiation safety and that SCAI is creating a pathway where imaging cardiologists can become fellows of the society, which was traditionally reserved for interventionalists.
Still, imaging and cardiovascular societies have yet to endorse standardized safety procedures for interventional imagers, nor is information routinely collected on radiation exposure in national registries.
“We just don’t have the budgets or the interest nationally to do that kind of thing, so it has to be done locally,” Dr. Rao said. “And the person who I think is responsible for that is really the cath lab director and the cath lab nurse manager, who really should work hand-in-glove to make sure that radiation safety is at the top of the priority list.”
The study was funded by the Frederik Meijer Heart & Vascular Institute, Spectrum Health, and by Corindus. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, approval of the manuscript; and the decision to submit the manuscript for publication. Senior author Ryan Madder, MD, reports receiving research support, speaker honoraria, and grants, and serving on the advisory board of Corindus. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
Interventional echocardiographers have become an increasingly critical part of the structural heart team but may be paying the price in terms of radiation exposure, a new study suggests.
Results showed that interventional echocardiographers receive threefold higher head-level radiation doses than interventional cardiologists during left atrial appendage occlusion (LAAO) closures and 11-fold higher doses during mitral valve transcatheter edge-to-edge repair (TEER).
“Over the last 5-10 years there’s been exponential growth in these two procedures, TEER and LAAO, and while that’s been very exciting, I think there hasn’t been as much research into how to protect these individuals,” lead author David A. McNamara, MD, MPH, Spectrum Health, Grand Rapids, Mich., told this news organization.
The study was published in JAMA Network Open.
Previous studies have focused largely on radiation exposure and mitigation efforts during coronary interventions, but the room set-up for LAAO and TEER and shielding techniques to mitigate radiation exposure are vastly different, he noted.
A 2017 study reported that radiation exposure was significantly higher for imaging specialists than structural heart specialists and varied by procedure type.
For the current study, Dr. McNamara, an echocardiographer by training, and colleagues collected data from 30 consecutive LAAO and 30 consecutive TEER procedures performed at their institution between July 2016 and January 2018.
Interventional imagers, interventional cardiologists, and sonographers all wore a lead skirt, apron, and thyroid collar, as well as a dosimeter to collect radiation data.
Interventional cardiologists stood immediately adjacent to the procedure table and used a ceiling-mounted, upper-body lead shield and a lower-body shield extending from the table to the floor. The echocardiographer stood at the patient’s head and used a mobile accessory shield raised to a height that allowed the imager to extend their arms over the shield to manipulate a transesophageal echocardiogram probe throughout the case.
The median fluoroscopy time was 9.2 minutes for LAAO and 20.9 minutes for TEER. The median air kerma was 164 mGy and 109 mGy, respectively.
Interventional echocardiographers received a median per case radiation dose of 10.6 µSv, compared with 2.1 µSv for interventional cardiologists. The result was similar for TEER (10.5 vs. 0.9 µSv) and LAAO (10.6 vs. 3.5 µSv; P < .001 for all).
The odds of interventional echocardiographers having a radiation dose greater than 20 µSV were 7.5 times greater than for interventional cardiologists (P < .001).
“It’s not the direction of the association, but really the magnitude is what surprised us,” observed Dr. McNamara.
The team was pleasantly surprised, he said, that sonographers, a “vastly understudied group,” received significantly lower median radiation doses than interventional imagers during LAAO (0.2 µSV) and TEER procedures (0.0 µSv; P < .001 for both).
The average distances from the radiation source were 26 cm (10.2 inches) for the echocardiographer, 36 cm (14.2 inches) for the interventional cardiologist, and 250 cm (8.2 feet) for the sonographer.
“These folks [sonographers] were much further away than both the physicians performing these cases, and that is what we hypothesize drove their very low rates, but that should also help inform our mitigation techniques for physicians and for all other cath lab members in the room,” Dr. McNamara said.
He noted that Spectrum Health has been at the forefront in terms of research into radiation exposure and mitigation, has good institutional radiation safety education, and used dose-lowering fluoroscopy systems (AlluraClarity, Philips) with real-time image noise reduction technology and a frame rate of 15 frames per second for the study. “So we’re hopeful that this actually represents a somewhat best-case scenario for what is being done at multiple institutions throughout the nation.”
Nevertheless, there is a huge amount of variability in radiation exposure, Dr. McNamara observed. “First and foremost, we really just have to identify our problem and highlight that this is something that needs some advocacy from our [professional] groups.”
Sunil Rao, MD, the newly minted president of the Society of Cardiovascular Angiography and Interventions (SCAI), said, “This is a really important study, because it expands the potential occupational hazards outside of what we traditionally think of as the team that does interventional procedures ... we have to recognize that the procedures we’re doing in the cath lab have changed.”
“Showing that our colleagues are getting 3-10 times radiation exposure is a really important piece of information to have out there. I think it’s really sort of a call to action,” Dr. Rao, professor of medicine at Duke University, Durham, N.C., told this news organization.
Nevertheless, he observed that practices have shifted somewhat since the study and that interventional cardiologists working with imaging physicians are more cognizant of radiation exposure issues.
“When I talk with our folks here that are doing structural heart procedures, they’re making sure that they’re not stepping on the fluoro pedal while the echocardiographer is manipulating the TE probe,” Dr. Rao said. “The echocardiographer is oftentimes using a much bigger shield than what was described in the study, and remember there’s an exponential decrease in the radiation exposure by distance, so they’re stepping back during the fluoroscopy time.”
Although the volume of TEER and LAAO procedures, as well as tricuspid interventions, will continue to climb, Dr. Rao said he expects radiation exposure to the imaging cardiologist will fall thanks to greater use of newer-generation imaging systems with dose-reduction features and better shielding strategies.
He noted that several of SCAI’s “best practices” documents call attention to radiation safety and that SCAI is creating a pathway where imaging cardiologists can become fellows of the society, which was traditionally reserved for interventionalists.
Still, imaging and cardiovascular societies have yet to endorse standardized safety procedures for interventional imagers, nor is information routinely collected on radiation exposure in national registries.
“We just don’t have the budgets or the interest nationally to do that kind of thing, so it has to be done locally,” Dr. Rao said. “And the person who I think is responsible for that is really the cath lab director and the cath lab nurse manager, who really should work hand-in-glove to make sure that radiation safety is at the top of the priority list.”
The study was funded by the Frederik Meijer Heart & Vascular Institute, Spectrum Health, and by Corindus. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, approval of the manuscript; and the decision to submit the manuscript for publication. Senior author Ryan Madder, MD, reports receiving research support, speaker honoraria, and grants, and serving on the advisory board of Corindus. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
The heartache of bereavement can be fatal in heart failure
that points to the need for greater integration of psychosocial risk factors in the treatment of HF.
The adjusted relative risk of dying was nearly 30% higher among bereaved patients with HF (1.29; 95% confidence interval, 1.27-1.30) and slightly higher for those grieving the loss of more than one family member (RR, 1.35).
The highest risk was in the first week after the loss (RR, 1.78) but persisted after 5 years of follow-up (RR, 1.30).
“Heart failure is a very difficult condition and has a very poor prognosis comparable to many, many cancers,” senior author Krisztina László, PhD, Karolinska Institutet, Stockholm, said in an interview. “So it’s important for us to be aware of these increased risks and to understand them better.”
The early risk for death could be related to stress-induced cardiomyopathy, or Takotsubo syndrome, as well as activation of the hypothalamic-pituitary-adrenal axis, the renin-angiotensin-aldosterone system, and sympathetic nervous system, she explained. Higher long-term risks may reflect chronic stress, leading to poorly managed disease and an unhealthy lifestyle.
“If we understand better the underlying mechanisms maybe we can give more specific advice,” Dr. László said. “At this stage, I think having an awareness of the risk and trying to follow patients or at least not let them fall out of usual care, asking questions, trying to understand what their needs are, maybe that is what we can do well.”
A recent position paper by the European Association of Preventive Cardiology pointed out that psychosocial risk factors, like depression and social isolation, can exacerbate heart failure and calls for better integration of psychosocial factors in the treatment of patients with chronic HF.
“We don’t do a very good job of it, but I think they are very important,” observed Stuart D. Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., and was not involved in the study.
“When we hear about a spouse dying, we might call and give condolences, but it’s probably a group of patients that for the next 6 months or so we need to watch more closely and see if there are things we can impact both medically as well as socially to perhaps prevent some of this increase in mortality,” he told this news organization.
Although several studies have linked bereavement with adverse health outcomes, this is just one of two studies to look specifically at its role in HF prognosis, Dr. László noted. A 2013 study of 66,000 male veterans reported that widowers had nearly a 38% higher all-cause mortality risk than did married veterans.
The present study extends those findings to 490,527 patients in the Swedish Heart Failure Registry between 2000 and 2018 and/or in the Swedish Patient Register with a primary diagnosis of HF between 1987 and 2018. During a mean follow-up of 3.7 years, 12% of participants had a family member die, and 383,674 participants died.
Results showed the HF mortality risk increased 10% after the death of a child, 20% with the death of a spouse/partner, 13% with a sibling’s death, and 5% with the death of a grandchild.
No increased risk was seen after the death of a parent, which is likely owed to a median patient age of about 75 years and “is in line with our expectations of the life cycle,” Dr. László said.
An association between bereavement and mortality risk was observed in cases of loss caused by cardiovascular disease (RR, 1.34) and other natural causes (RR, 1.27) but also in cases of unnatural deaths, such as suicide (RR, 1.13).
The overall findings were similar regardless of left ventricular ejection fraction and New York Heart Association functional class and were not affected by sex or country of birth.
Dr. Russell agreed that the death of a parent would be expected among these older patients with HF but said that “if the mechanism of this truly is kind of this increased stress hormones and Takotsubo-type mechanism, you’d think it would be worse if it was your kid that died. That shocked me a bit.”
The strong association between mortality and the loss of a spouse or partner was not surprising, given that they’re an important source of mutual social support, he added.
“If it’s a 75-year-old whose spouse dies, we need to make sure that we have the children’s phone number or other people that we can reach out to and say: ‘Can you check on them?’ ” he said. “And we need to make sure that somebody else is coming in with them because I would guess that probably at least half of what patients hear in a clinic visit goes in one ear and out the other and it’s going to make that much better. So we need to find who that new support person is for the patient.”
Asked whether there are efforts underway to incorporate psychosocial factors into current U.S. guidelines, Dr. Russell replied, “certainly within heart failure, I don’t think we’re really discussing it and, that may be the best part of this paper. It really makes us think about a different way of approaching these older patients.”
Dr. László said that future studies are needed to investigate whether less severe sources of stress may also contribute to poor HF prognosis.
“In our population, 12% of patients were affected, which is quite high, but there are patients with heart failure who experience on a daily basis other sources of stress, which are less severe but chronic and affect large numbers,” she said. “This may also have important public health implications and will be an important next step.”
The authors noted that they were unable to eliminate residual confounding by genetic factors or unmeasured socioeconomic-, lifestyle-, or health-related factors shared by family members. Other limitations are limited power to detect a modest effect in some of the subanalyses and that the findings may be generalizable only to countries with social and cultural contexts and health-related factors similar to those of Sweden.
The study was supported by grants from the Swedish Council for Working Life and Social Research, the Karolinska Institutet’s Research Foundation, and the China Scholarship Council. Dr. László is also supported by a grant from the Heart and Lung Foundation. All other authors and Dr. Russell reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
that points to the need for greater integration of psychosocial risk factors in the treatment of HF.
The adjusted relative risk of dying was nearly 30% higher among bereaved patients with HF (1.29; 95% confidence interval, 1.27-1.30) and slightly higher for those grieving the loss of more than one family member (RR, 1.35).
The highest risk was in the first week after the loss (RR, 1.78) but persisted after 5 years of follow-up (RR, 1.30).
“Heart failure is a very difficult condition and has a very poor prognosis comparable to many, many cancers,” senior author Krisztina László, PhD, Karolinska Institutet, Stockholm, said in an interview. “So it’s important for us to be aware of these increased risks and to understand them better.”
The early risk for death could be related to stress-induced cardiomyopathy, or Takotsubo syndrome, as well as activation of the hypothalamic-pituitary-adrenal axis, the renin-angiotensin-aldosterone system, and sympathetic nervous system, she explained. Higher long-term risks may reflect chronic stress, leading to poorly managed disease and an unhealthy lifestyle.
“If we understand better the underlying mechanisms maybe we can give more specific advice,” Dr. László said. “At this stage, I think having an awareness of the risk and trying to follow patients or at least not let them fall out of usual care, asking questions, trying to understand what their needs are, maybe that is what we can do well.”
A recent position paper by the European Association of Preventive Cardiology pointed out that psychosocial risk factors, like depression and social isolation, can exacerbate heart failure and calls for better integration of psychosocial factors in the treatment of patients with chronic HF.
“We don’t do a very good job of it, but I think they are very important,” observed Stuart D. Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., and was not involved in the study.
“When we hear about a spouse dying, we might call and give condolences, but it’s probably a group of patients that for the next 6 months or so we need to watch more closely and see if there are things we can impact both medically as well as socially to perhaps prevent some of this increase in mortality,” he told this news organization.
Although several studies have linked bereavement with adverse health outcomes, this is just one of two studies to look specifically at its role in HF prognosis, Dr. László noted. A 2013 study of 66,000 male veterans reported that widowers had nearly a 38% higher all-cause mortality risk than did married veterans.
The present study extends those findings to 490,527 patients in the Swedish Heart Failure Registry between 2000 and 2018 and/or in the Swedish Patient Register with a primary diagnosis of HF between 1987 and 2018. During a mean follow-up of 3.7 years, 12% of participants had a family member die, and 383,674 participants died.
Results showed the HF mortality risk increased 10% after the death of a child, 20% with the death of a spouse/partner, 13% with a sibling’s death, and 5% with the death of a grandchild.
No increased risk was seen after the death of a parent, which is likely owed to a median patient age of about 75 years and “is in line with our expectations of the life cycle,” Dr. László said.
An association between bereavement and mortality risk was observed in cases of loss caused by cardiovascular disease (RR, 1.34) and other natural causes (RR, 1.27) but also in cases of unnatural deaths, such as suicide (RR, 1.13).
The overall findings were similar regardless of left ventricular ejection fraction and New York Heart Association functional class and were not affected by sex or country of birth.
Dr. Russell agreed that the death of a parent would be expected among these older patients with HF but said that “if the mechanism of this truly is kind of this increased stress hormones and Takotsubo-type mechanism, you’d think it would be worse if it was your kid that died. That shocked me a bit.”
The strong association between mortality and the loss of a spouse or partner was not surprising, given that they’re an important source of mutual social support, he added.
“If it’s a 75-year-old whose spouse dies, we need to make sure that we have the children’s phone number or other people that we can reach out to and say: ‘Can you check on them?’ ” he said. “And we need to make sure that somebody else is coming in with them because I would guess that probably at least half of what patients hear in a clinic visit goes in one ear and out the other and it’s going to make that much better. So we need to find who that new support person is for the patient.”
Asked whether there are efforts underway to incorporate psychosocial factors into current U.S. guidelines, Dr. Russell replied, “certainly within heart failure, I don’t think we’re really discussing it and, that may be the best part of this paper. It really makes us think about a different way of approaching these older patients.”
Dr. László said that future studies are needed to investigate whether less severe sources of stress may also contribute to poor HF prognosis.
“In our population, 12% of patients were affected, which is quite high, but there are patients with heart failure who experience on a daily basis other sources of stress, which are less severe but chronic and affect large numbers,” she said. “This may also have important public health implications and will be an important next step.”
The authors noted that they were unable to eliminate residual confounding by genetic factors or unmeasured socioeconomic-, lifestyle-, or health-related factors shared by family members. Other limitations are limited power to detect a modest effect in some of the subanalyses and that the findings may be generalizable only to countries with social and cultural contexts and health-related factors similar to those of Sweden.
The study was supported by grants from the Swedish Council for Working Life and Social Research, the Karolinska Institutet’s Research Foundation, and the China Scholarship Council. Dr. László is also supported by a grant from the Heart and Lung Foundation. All other authors and Dr. Russell reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
that points to the need for greater integration of psychosocial risk factors in the treatment of HF.
The adjusted relative risk of dying was nearly 30% higher among bereaved patients with HF (1.29; 95% confidence interval, 1.27-1.30) and slightly higher for those grieving the loss of more than one family member (RR, 1.35).
The highest risk was in the first week after the loss (RR, 1.78) but persisted after 5 years of follow-up (RR, 1.30).
“Heart failure is a very difficult condition and has a very poor prognosis comparable to many, many cancers,” senior author Krisztina László, PhD, Karolinska Institutet, Stockholm, said in an interview. “So it’s important for us to be aware of these increased risks and to understand them better.”
The early risk for death could be related to stress-induced cardiomyopathy, or Takotsubo syndrome, as well as activation of the hypothalamic-pituitary-adrenal axis, the renin-angiotensin-aldosterone system, and sympathetic nervous system, she explained. Higher long-term risks may reflect chronic stress, leading to poorly managed disease and an unhealthy lifestyle.
“If we understand better the underlying mechanisms maybe we can give more specific advice,” Dr. László said. “At this stage, I think having an awareness of the risk and trying to follow patients or at least not let them fall out of usual care, asking questions, trying to understand what their needs are, maybe that is what we can do well.”
A recent position paper by the European Association of Preventive Cardiology pointed out that psychosocial risk factors, like depression and social isolation, can exacerbate heart failure and calls for better integration of psychosocial factors in the treatment of patients with chronic HF.
“We don’t do a very good job of it, but I think they are very important,” observed Stuart D. Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., and was not involved in the study.
“When we hear about a spouse dying, we might call and give condolences, but it’s probably a group of patients that for the next 6 months or so we need to watch more closely and see if there are things we can impact both medically as well as socially to perhaps prevent some of this increase in mortality,” he told this news organization.
Although several studies have linked bereavement with adverse health outcomes, this is just one of two studies to look specifically at its role in HF prognosis, Dr. László noted. A 2013 study of 66,000 male veterans reported that widowers had nearly a 38% higher all-cause mortality risk than did married veterans.
The present study extends those findings to 490,527 patients in the Swedish Heart Failure Registry between 2000 and 2018 and/or in the Swedish Patient Register with a primary diagnosis of HF between 1987 and 2018. During a mean follow-up of 3.7 years, 12% of participants had a family member die, and 383,674 participants died.
Results showed the HF mortality risk increased 10% after the death of a child, 20% with the death of a spouse/partner, 13% with a sibling’s death, and 5% with the death of a grandchild.
No increased risk was seen after the death of a parent, which is likely owed to a median patient age of about 75 years and “is in line with our expectations of the life cycle,” Dr. László said.
An association between bereavement and mortality risk was observed in cases of loss caused by cardiovascular disease (RR, 1.34) and other natural causes (RR, 1.27) but also in cases of unnatural deaths, such as suicide (RR, 1.13).
The overall findings were similar regardless of left ventricular ejection fraction and New York Heart Association functional class and were not affected by sex or country of birth.
Dr. Russell agreed that the death of a parent would be expected among these older patients with HF but said that “if the mechanism of this truly is kind of this increased stress hormones and Takotsubo-type mechanism, you’d think it would be worse if it was your kid that died. That shocked me a bit.”
The strong association between mortality and the loss of a spouse or partner was not surprising, given that they’re an important source of mutual social support, he added.
“If it’s a 75-year-old whose spouse dies, we need to make sure that we have the children’s phone number or other people that we can reach out to and say: ‘Can you check on them?’ ” he said. “And we need to make sure that somebody else is coming in with them because I would guess that probably at least half of what patients hear in a clinic visit goes in one ear and out the other and it’s going to make that much better. So we need to find who that new support person is for the patient.”
Asked whether there are efforts underway to incorporate psychosocial factors into current U.S. guidelines, Dr. Russell replied, “certainly within heart failure, I don’t think we’re really discussing it and, that may be the best part of this paper. It really makes us think about a different way of approaching these older patients.”
Dr. László said that future studies are needed to investigate whether less severe sources of stress may also contribute to poor HF prognosis.
“In our population, 12% of patients were affected, which is quite high, but there are patients with heart failure who experience on a daily basis other sources of stress, which are less severe but chronic and affect large numbers,” she said. “This may also have important public health implications and will be an important next step.”
The authors noted that they were unable to eliminate residual confounding by genetic factors or unmeasured socioeconomic-, lifestyle-, or health-related factors shared by family members. Other limitations are limited power to detect a modest effect in some of the subanalyses and that the findings may be generalizable only to countries with social and cultural contexts and health-related factors similar to those of Sweden.
The study was supported by grants from the Swedish Council for Working Life and Social Research, the Karolinska Institutet’s Research Foundation, and the China Scholarship Council. Dr. László is also supported by a grant from the Heart and Lung Foundation. All other authors and Dr. Russell reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JACC: HEART FAILURE
Women benefit but lag behind in intracoronary imaging in PCI
A real-world analysis reveals that women are consistently less likely to undergo intracoronary imaging as part of percutaneous coronary intervention (PCI), even though it benefits both sexes equally.
Results from nearly all PCIs performed in England and Wales between 2006 and 2019 showed the absolute rate of intracoronary imaging with either intravascular ultrasound (IVUS) or optical coherence tomography (OCT) was 5% lower in the later study years among women at 14.5%, compared with 19.6% in men (P < .001).
After adjustment, female sex was an independent predictor of lower intracoronary imaging use (odds ratio, 0.93; 95% confidence interval, 0.91-0.96), according to the study, published in JACC: Cardiovascular Interventions.
“One of the thoughts I had when we were running this analysis was, well, maybe the indications for that imaging, as recommended by guidelines, are less common in women,” Mamas Mamas, MD, told this news organization. “So what we did was to look at just cases where imaging is recommended by the EAPCI [European Association of Percutaneous Coronary Intervention].”
Again, the use of intracoronary imaging was consistently lower among women than among men for all of the following EAPCI-recommended indications:
- Acute coronary syndrome: 11.6% vs. 12.3% (P < .01).
- Stent thrombosis: 30.9% vs. 34.9% (P < .01).
- Long lesions: 13.1% vs. 16.3% (P < .01).
- Chronic total occlusions: 16.2% vs. 18.3% (P < .01).
- Left main stem PCI: 55.1% vs. 57.5% (P < .01).
- In-stent restenosis: 28.0% vs. 30.7%.
- Calcified lesions: 36.6% vs. 40.1% (P < .01).
- Renal disease: 17.4% vs. 19.5% (P < .01).
As to what might be driving the lower use, Dr. Mamas dismissed the argument that women undergo much simpler PCI, which wouldn’t benefit from imaging. Women do have smaller coronary arteries, however, and there is a belief that it’s easier to eyeball the size of vessels that are smaller rather than larger.
“I’m not convinced that’s entirely true,” he said. “I don’t have a good answer for you, I’m afraid. I don’t really know why we’re seeing it. I just think it’s one of those disparities that is important to highlight.”
Central to this belief is that the benefits of intracoronary imaging were found to be similar in men and women. Intracoronary imaging was associated with lower adjusted odds of in-hospital mortality (OR, 0.56; 95% CI, 0.48-0.64) and major adverse cardiac and cerebrovascular events (OR, 0.83; 95% CI, 0.76-0.91) in women and men (OR, 0.48; 95% CI, 0.44-0.53 and OR, 0.75; 95% CI, 0.71-0.80, respectively), compared with nonimaging groups.
“This really should be a call to arms, particularly given that we show this disparity persists, even in guideline-recommended cases where we should be using it,” said Dr. Mamas, from the Keele (England) Cardiovascular Research Group, Keele University, and Royal Stoke University Hospital, Stoke-on-Trent, England.
“Actually, I would argue that we should be using more imaging in women than men anyway because many of the presentations for acute coronary syndromes in women, like spontaneous coronary artery dissection or MINOCA [MI with nonobstructive coronary arteries], you often need intracoronary imaging to make that kind of diagnosis,” he observed.
Getting worse, not better
Previous studies have shown that women are less likely than men in acute coronary syndromes to receive the transradial approach and P2Y12 inhibitors, but none have specifically looked at intracoronary imaging, Dr. Mamas said.
To fill the gap, the researchers drew on data from 994,478 patients in the British Cardiovascular Intervention Society registry, of whom, 8.4% of 738,616 men and 7.9% of 255,862 women received intracoronary imaging.
Women in the imaging group were older, more likely to be an ethnic minority, and more likely to undergo PCI for non–ST-segment elevation MI than their male counterparts.
One of the more surprising findings was that rates of IVUS and OCT were superimposable between the sexes at the start of the study but quickly diverged starting in around 2012, when the technology took off, Dr. Mamas said. In the most recent data, use was about 3% lower in women overall and rising to 6% in those with stable angina.
“Whilst the disparities between men and women are significant, the bigger question is why are we using so little imaging in guideline-recommended cases where there is a benefit?” he said.
Possible actionable items, he suggested, include providing older physicians who didn’t have access to intracoronary imaging during their training with opportunities in their cath lab or with industry sponsors to increase their skills and confidence. Intracoronary imaging use could also be routinely captured in U.S. and European PCI registries and used as a quality metric.
“In left main, you see a massive difference between centers, and that’s the kind of data that drives discussion,” Dr. Mamas said. “If we start reporting quality metrics, such as radial use, intracoronary imaging, P2Y12 inhibitors by center, then you’ve got something to benchmark centers against.”
Nathaniel Smilowitz, MD, an interventional cardiologist at New York Langone Health, who was not associated with the study, said that it’s troubling to see that the utilization intravascular imaging is so low, despite randomized trials and large meta-analyses showing a mortality benefit associated with its use in PCI.
“Even among men, only 19.6% in the later years were getting intravascular imaging performed to guide their coronary intervention, so one out of five,” he said. “There are opportunities to improve.”
Dr. Smilowitz said he’s also perplexed as to why adoption would be lower in women but that the findings echo those in other domains where women receive less intensive cardiovascular therapy.
“There’s no biological, really plausible, mechanism as to why the need for intravascular imaging would be lower and, particularly, because they showed in stent thrombosis, for example, where intravascular imaging is tremendously important, there were still sex differences,” he said. “So even with clear indications for imaging, women just received the optimal therapy less often than men. It’s disappointing.”
Dr. Smilowitz agreed that there may be a need to incorporate intravascular imaging into metrics, which are reported back to physicians, potentially even for comparisons with peers or regional rates to incentivize physicians to improve uptake.
“As a society, we’ve been quite slow to integrate intravascular imaging to guide PCI and we can do better,” he said.
A version of this article first appeared on Medscape.com.
A real-world analysis reveals that women are consistently less likely to undergo intracoronary imaging as part of percutaneous coronary intervention (PCI), even though it benefits both sexes equally.
Results from nearly all PCIs performed in England and Wales between 2006 and 2019 showed the absolute rate of intracoronary imaging with either intravascular ultrasound (IVUS) or optical coherence tomography (OCT) was 5% lower in the later study years among women at 14.5%, compared with 19.6% in men (P < .001).
After adjustment, female sex was an independent predictor of lower intracoronary imaging use (odds ratio, 0.93; 95% confidence interval, 0.91-0.96), according to the study, published in JACC: Cardiovascular Interventions.
“One of the thoughts I had when we were running this analysis was, well, maybe the indications for that imaging, as recommended by guidelines, are less common in women,” Mamas Mamas, MD, told this news organization. “So what we did was to look at just cases where imaging is recommended by the EAPCI [European Association of Percutaneous Coronary Intervention].”
Again, the use of intracoronary imaging was consistently lower among women than among men for all of the following EAPCI-recommended indications:
- Acute coronary syndrome: 11.6% vs. 12.3% (P < .01).
- Stent thrombosis: 30.9% vs. 34.9% (P < .01).
- Long lesions: 13.1% vs. 16.3% (P < .01).
- Chronic total occlusions: 16.2% vs. 18.3% (P < .01).
- Left main stem PCI: 55.1% vs. 57.5% (P < .01).
- In-stent restenosis: 28.0% vs. 30.7%.
- Calcified lesions: 36.6% vs. 40.1% (P < .01).
- Renal disease: 17.4% vs. 19.5% (P < .01).
As to what might be driving the lower use, Dr. Mamas dismissed the argument that women undergo much simpler PCI, which wouldn’t benefit from imaging. Women do have smaller coronary arteries, however, and there is a belief that it’s easier to eyeball the size of vessels that are smaller rather than larger.
“I’m not convinced that’s entirely true,” he said. “I don’t have a good answer for you, I’m afraid. I don’t really know why we’re seeing it. I just think it’s one of those disparities that is important to highlight.”
Central to this belief is that the benefits of intracoronary imaging were found to be similar in men and women. Intracoronary imaging was associated with lower adjusted odds of in-hospital mortality (OR, 0.56; 95% CI, 0.48-0.64) and major adverse cardiac and cerebrovascular events (OR, 0.83; 95% CI, 0.76-0.91) in women and men (OR, 0.48; 95% CI, 0.44-0.53 and OR, 0.75; 95% CI, 0.71-0.80, respectively), compared with nonimaging groups.
“This really should be a call to arms, particularly given that we show this disparity persists, even in guideline-recommended cases where we should be using it,” said Dr. Mamas, from the Keele (England) Cardiovascular Research Group, Keele University, and Royal Stoke University Hospital, Stoke-on-Trent, England.
“Actually, I would argue that we should be using more imaging in women than men anyway because many of the presentations for acute coronary syndromes in women, like spontaneous coronary artery dissection or MINOCA [MI with nonobstructive coronary arteries], you often need intracoronary imaging to make that kind of diagnosis,” he observed.
Getting worse, not better
Previous studies have shown that women are less likely than men in acute coronary syndromes to receive the transradial approach and P2Y12 inhibitors, but none have specifically looked at intracoronary imaging, Dr. Mamas said.
To fill the gap, the researchers drew on data from 994,478 patients in the British Cardiovascular Intervention Society registry, of whom, 8.4% of 738,616 men and 7.9% of 255,862 women received intracoronary imaging.
Women in the imaging group were older, more likely to be an ethnic minority, and more likely to undergo PCI for non–ST-segment elevation MI than their male counterparts.
One of the more surprising findings was that rates of IVUS and OCT were superimposable between the sexes at the start of the study but quickly diverged starting in around 2012, when the technology took off, Dr. Mamas said. In the most recent data, use was about 3% lower in women overall and rising to 6% in those with stable angina.
“Whilst the disparities between men and women are significant, the bigger question is why are we using so little imaging in guideline-recommended cases where there is a benefit?” he said.
Possible actionable items, he suggested, include providing older physicians who didn’t have access to intracoronary imaging during their training with opportunities in their cath lab or with industry sponsors to increase their skills and confidence. Intracoronary imaging use could also be routinely captured in U.S. and European PCI registries and used as a quality metric.
“In left main, you see a massive difference between centers, and that’s the kind of data that drives discussion,” Dr. Mamas said. “If we start reporting quality metrics, such as radial use, intracoronary imaging, P2Y12 inhibitors by center, then you’ve got something to benchmark centers against.”
Nathaniel Smilowitz, MD, an interventional cardiologist at New York Langone Health, who was not associated with the study, said that it’s troubling to see that the utilization intravascular imaging is so low, despite randomized trials and large meta-analyses showing a mortality benefit associated with its use in PCI.
“Even among men, only 19.6% in the later years were getting intravascular imaging performed to guide their coronary intervention, so one out of five,” he said. “There are opportunities to improve.”
Dr. Smilowitz said he’s also perplexed as to why adoption would be lower in women but that the findings echo those in other domains where women receive less intensive cardiovascular therapy.
“There’s no biological, really plausible, mechanism as to why the need for intravascular imaging would be lower and, particularly, because they showed in stent thrombosis, for example, where intravascular imaging is tremendously important, there were still sex differences,” he said. “So even with clear indications for imaging, women just received the optimal therapy less often than men. It’s disappointing.”
Dr. Smilowitz agreed that there may be a need to incorporate intravascular imaging into metrics, which are reported back to physicians, potentially even for comparisons with peers or regional rates to incentivize physicians to improve uptake.
“As a society, we’ve been quite slow to integrate intravascular imaging to guide PCI and we can do better,” he said.
A version of this article first appeared on Medscape.com.
A real-world analysis reveals that women are consistently less likely to undergo intracoronary imaging as part of percutaneous coronary intervention (PCI), even though it benefits both sexes equally.
Results from nearly all PCIs performed in England and Wales between 2006 and 2019 showed the absolute rate of intracoronary imaging with either intravascular ultrasound (IVUS) or optical coherence tomography (OCT) was 5% lower in the later study years among women at 14.5%, compared with 19.6% in men (P < .001).
After adjustment, female sex was an independent predictor of lower intracoronary imaging use (odds ratio, 0.93; 95% confidence interval, 0.91-0.96), according to the study, published in JACC: Cardiovascular Interventions.
“One of the thoughts I had when we were running this analysis was, well, maybe the indications for that imaging, as recommended by guidelines, are less common in women,” Mamas Mamas, MD, told this news organization. “So what we did was to look at just cases where imaging is recommended by the EAPCI [European Association of Percutaneous Coronary Intervention].”
Again, the use of intracoronary imaging was consistently lower among women than among men for all of the following EAPCI-recommended indications:
- Acute coronary syndrome: 11.6% vs. 12.3% (P < .01).
- Stent thrombosis: 30.9% vs. 34.9% (P < .01).
- Long lesions: 13.1% vs. 16.3% (P < .01).
- Chronic total occlusions: 16.2% vs. 18.3% (P < .01).
- Left main stem PCI: 55.1% vs. 57.5% (P < .01).
- In-stent restenosis: 28.0% vs. 30.7%.
- Calcified lesions: 36.6% vs. 40.1% (P < .01).
- Renal disease: 17.4% vs. 19.5% (P < .01).
As to what might be driving the lower use, Dr. Mamas dismissed the argument that women undergo much simpler PCI, which wouldn’t benefit from imaging. Women do have smaller coronary arteries, however, and there is a belief that it’s easier to eyeball the size of vessels that are smaller rather than larger.
“I’m not convinced that’s entirely true,” he said. “I don’t have a good answer for you, I’m afraid. I don’t really know why we’re seeing it. I just think it’s one of those disparities that is important to highlight.”
Central to this belief is that the benefits of intracoronary imaging were found to be similar in men and women. Intracoronary imaging was associated with lower adjusted odds of in-hospital mortality (OR, 0.56; 95% CI, 0.48-0.64) and major adverse cardiac and cerebrovascular events (OR, 0.83; 95% CI, 0.76-0.91) in women and men (OR, 0.48; 95% CI, 0.44-0.53 and OR, 0.75; 95% CI, 0.71-0.80, respectively), compared with nonimaging groups.
“This really should be a call to arms, particularly given that we show this disparity persists, even in guideline-recommended cases where we should be using it,” said Dr. Mamas, from the Keele (England) Cardiovascular Research Group, Keele University, and Royal Stoke University Hospital, Stoke-on-Trent, England.
“Actually, I would argue that we should be using more imaging in women than men anyway because many of the presentations for acute coronary syndromes in women, like spontaneous coronary artery dissection or MINOCA [MI with nonobstructive coronary arteries], you often need intracoronary imaging to make that kind of diagnosis,” he observed.
Getting worse, not better
Previous studies have shown that women are less likely than men in acute coronary syndromes to receive the transradial approach and P2Y12 inhibitors, but none have specifically looked at intracoronary imaging, Dr. Mamas said.
To fill the gap, the researchers drew on data from 994,478 patients in the British Cardiovascular Intervention Society registry, of whom, 8.4% of 738,616 men and 7.9% of 255,862 women received intracoronary imaging.
Women in the imaging group were older, more likely to be an ethnic minority, and more likely to undergo PCI for non–ST-segment elevation MI than their male counterparts.
One of the more surprising findings was that rates of IVUS and OCT were superimposable between the sexes at the start of the study but quickly diverged starting in around 2012, when the technology took off, Dr. Mamas said. In the most recent data, use was about 3% lower in women overall and rising to 6% in those with stable angina.
“Whilst the disparities between men and women are significant, the bigger question is why are we using so little imaging in guideline-recommended cases where there is a benefit?” he said.
Possible actionable items, he suggested, include providing older physicians who didn’t have access to intracoronary imaging during their training with opportunities in their cath lab or with industry sponsors to increase their skills and confidence. Intracoronary imaging use could also be routinely captured in U.S. and European PCI registries and used as a quality metric.
“In left main, you see a massive difference between centers, and that’s the kind of data that drives discussion,” Dr. Mamas said. “If we start reporting quality metrics, such as radial use, intracoronary imaging, P2Y12 inhibitors by center, then you’ve got something to benchmark centers against.”
Nathaniel Smilowitz, MD, an interventional cardiologist at New York Langone Health, who was not associated with the study, said that it’s troubling to see that the utilization intravascular imaging is so low, despite randomized trials and large meta-analyses showing a mortality benefit associated with its use in PCI.
“Even among men, only 19.6% in the later years were getting intravascular imaging performed to guide their coronary intervention, so one out of five,” he said. “There are opportunities to improve.”
Dr. Smilowitz said he’s also perplexed as to why adoption would be lower in women but that the findings echo those in other domains where women receive less intensive cardiovascular therapy.
“There’s no biological, really plausible, mechanism as to why the need for intravascular imaging would be lower and, particularly, because they showed in stent thrombosis, for example, where intravascular imaging is tremendously important, there were still sex differences,” he said. “So even with clear indications for imaging, women just received the optimal therapy less often than men. It’s disappointing.”
Dr. Smilowitz agreed that there may be a need to incorporate intravascular imaging into metrics, which are reported back to physicians, potentially even for comparisons with peers or regional rates to incentivize physicians to improve uptake.
“As a society, we’ve been quite slow to integrate intravascular imaging to guide PCI and we can do better,” he said.
A version of this article first appeared on Medscape.com.
FROM JACC: CARDIOVASCULAR INTERVENTIONS
Meta-analysis points to safety of acetylcholine coronary testing
Provocation testing with intracoronary acetylcholine is safe, particularly among Western patients, suggests a large systematic review that underscores the importance of functional coronary angiography to diagnose epicardial or microvascular spasm.
The results, derived from more than 12,000 patients in 16 studies, showed a 0.5% risk of major complications, defined as death, ventricular tachycardia/ventricular fibrillation, myocardial infarction, and shock requiring resuscitation.
Ventricular tachycardia/fibrillation were the most common events and mainly reported from two Japanese studies. There were no deaths.
Exploratory subgroup analyses revealed significantly fewer major complications in Western populations (0.0%; P for heterogeneity = .938), compared with Asian populations (2.3%; P for heterogeneity < .001).
The pooled positive vasospasm rate was also lower in Western versus Asian studies (37.9% vs. 50.7%; P for between-group heterogeneity = .010), as reported by the Microvascular Network in the Journal of the American College of Cardiology.
“If you look at the data between Asian studies versus others, mainly European or U.S. studies, primarily in Caucasian populations, it’s like zero percent history of major complications. So, it sounds extremely safe to do this testing in Caucasian populations,” Yuhei Kobayashi, MD, NewYork-Presbyterian Brooklyn Methodist Hospital, Weill Cornell Medicine, said.
Safety will need to be assessed in African Americans and other racial/ethnic groups, but “it makes us think we should end up testing more in the United States,” he told this news organization.
Intracoronary acetylcholine testing is daily practice in Japan but is limited in the United States and Europe to a few specialized centers due to safety concerns. Three deaths were reported in 1980 with intravenous ergonovine testing, whereas the safety of acetylcholine protocols has been studied largely in single-center retrospective studies, typically in Asian populations.
Growing recognition of myocardial infarction with nonobstructive coronary arteries (MINOCA) and ischemia with no obstructive coronary arteries (INOCA), however, is changing the landscape. In recent U.S. and European guidelines, intracoronary acetylcholine testing is indicated as a class 2a recommendation in MINOCA/INOCA.
“More and more institutions in Europe and the United States are starting to do acetylcholine testing, because now we know that chest pain isn’t necessarily coming from the blocked arteries,” Dr. Kobayashi said. “There are functional abnormalities, including coronary spasm, and if we diagnose it, we have appropriate medical regimens for this kind of disease.”
First safety meta-analysis
The present review and meta-analysis included 12,585 participants in 16 studies through November 2021. Of these, 63% were conducted in Western countries, and most were prospective studies published over the past decade in patients with MINOCA or INOCA.
Ten studies used the contemporary diagnostic criteria for epicardial spasm of at least 90% reduction in coronary diameter. Acetylcholine was administered into the left coronary artery at up to 100 mcg and 200 mcg in seven and six studies, respectively, and was used in the other three studies to assess endothelial function with a slower infusion of up to 36.4 mcg.
Major complications were significantly higher in studies following the contemporary diagnostic cutoff than in those using a lower cutoff of at least 75% diameter reduction (1.0% vs. 0.0%; P for between-group heterogeneity < .001).
The incidence of major complications was 0.2% with the slower infusion of up to 36.4 mcg, 0.8% with a maximum dose of 100 mcg, and 0.3% with a maximum dose of 200 mcg. The positive vasospasm rate was similar with the latter two protocols, at 46.3% and 41.4%, respectively.
Minor complications occurred in 3.3% of patients but were not detailed. They can include paroxysmal atrial fibrillation, ventricular ectopic beats, transient hypotension, and bradycardia requiring intervention.
As with major complications, minor complications were lower in studies using noncontemporary versus contemporary diagnostic cutoffs for epicardial spasm (1.8% vs. 4.7%) and in Western versus Asian populations (2.6% vs. 9.4%). Minor complications were similar between protocols with maximum doses of 100 mcg and 200 mcg (3.6% vs. 3.8%).
Dr. Kobayashi suggested that several factors may explain the racial differences, including previously reported smooth muscle hyperresponsiveness to provocation stimuli in Japanese patients and the inclusion of a wide range of patients in Japanese studies, such as those with obstructive coronary disease.
Japanese studies also used sequential acetylcholine injection into both the right and left coronaries, a faster injection speed of 20 seconds, and upfront placement of a temporary pacing catheter in case of acetylcholine-induced bradycardia, particularly with right coronary injection.
Although the protocol is largely settled in Japan, he said, provocation protocols need to be standardized because “depending on the country and depending on the institution, people are doing totally different things.”
A big step forward
Commenting on the study, C. Noel Bairey Merz, MD, from Cedars Sinai, Los Angeles, said it has “widespread relevance” because half of all coronary angiograms done invasively in the United States for suspected ischemia find no obstructive coronary disease. Left untreated, however, MINOCA has a 2.5% annual event rate, and a quarter of that is death.
“This is a big step forward with likely equal opportunity to improve women and men’s ischemic heart disease,” she said.

On the other hand, all studies were conducted at centers of excellence, so safety will need to be carefully watched as testing rolls out to more community care, Dr. Merz said. “And it always needs to be underscored that this is done by an interventional cardiologist because they’re familiar with wires that can dissect arteries, and they’re familiar with minor complications that could turn into major, if someone didn’t act appropriately.”
Dr. Merz also called for unifying protocols and the need to raise awareness within the general cardiology community to ask interventionalists for acetylcholine spasm testing. Randomized controlled data from within the WISE study and the CorMica study showed that diagnostic certainty leads to greater therapeutic certainty. “You do a much better job about who and how to treat,” she said.
There are also three ongoing randomized controlled trials – WARRIOR, MINOCA-BAT, and iCorMica – in the INOCA and MINOCA populations testing different treatment strategies for hard clinical outcomes like death and myocardial infarction.
“So in addition to this publication being guideline-forming for diagnosis, we anticipate in the next several years to have clinical trial evidence about therapeutics, again, for formulation of class 1 guidelines,” Dr. Merz said.
John Beltrame, BMBS, PhD, University of Adelaide, Australia, said the meta-analysis shows that intracoronary acetylcholine spasm testing is safe and should prompt greater adoption of invasive functional angiography.
Interventionalists are quite happy to do fractional flow reserve using intravenous adenosine to assess coronary microvascular dysfunction, he said, and “what we think is that functional angiography should test both – both the spasm as well as the microvasculature – and that will give us a clear direction because the treatments are slightly different when you’re treating the large arteries as compared to the microscopic arteries. It’s an important thing.”
Dr. Beltrame and colleagues further detail the benefits of comprehensive invasive functional angiography over structural angiography in a related editorial.
He also noted that the Coronary Vasomotion Disorders International Study Group published international diagnostic criteria for microvascular angina and that several protocols for acetylcholine spasm testing are in the works, including one from Australia. Australian investigators are also organizing an accreditation program for those performing the test.
“The protocol itself is relatively straightforward, but it’s not merely picking up a manual and following the instructions,” Dr. Beltrame said. “Just the same as when you train someone in angioplasty, you don’t just go out and do it. You need to develop some experience in it and so should be proctored.”
Dr. Kobayashi reported consulting agreements with Abbott Vascular. Coauthor disclosures are listed in the paper. Dr. Beltrame and colleagues have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Provocation testing with intracoronary acetylcholine is safe, particularly among Western patients, suggests a large systematic review that underscores the importance of functional coronary angiography to diagnose epicardial or microvascular spasm.
The results, derived from more than 12,000 patients in 16 studies, showed a 0.5% risk of major complications, defined as death, ventricular tachycardia/ventricular fibrillation, myocardial infarction, and shock requiring resuscitation.
Ventricular tachycardia/fibrillation were the most common events and mainly reported from two Japanese studies. There were no deaths.
Exploratory subgroup analyses revealed significantly fewer major complications in Western populations (0.0%; P for heterogeneity = .938), compared with Asian populations (2.3%; P for heterogeneity < .001).
The pooled positive vasospasm rate was also lower in Western versus Asian studies (37.9% vs. 50.7%; P for between-group heterogeneity = .010), as reported by the Microvascular Network in the Journal of the American College of Cardiology.
“If you look at the data between Asian studies versus others, mainly European or U.S. studies, primarily in Caucasian populations, it’s like zero percent history of major complications. So, it sounds extremely safe to do this testing in Caucasian populations,” Yuhei Kobayashi, MD, NewYork-Presbyterian Brooklyn Methodist Hospital, Weill Cornell Medicine, said.
Safety will need to be assessed in African Americans and other racial/ethnic groups, but “it makes us think we should end up testing more in the United States,” he told this news organization.
Intracoronary acetylcholine testing is daily practice in Japan but is limited in the United States and Europe to a few specialized centers due to safety concerns. Three deaths were reported in 1980 with intravenous ergonovine testing, whereas the safety of acetylcholine protocols has been studied largely in single-center retrospective studies, typically in Asian populations.
Growing recognition of myocardial infarction with nonobstructive coronary arteries (MINOCA) and ischemia with no obstructive coronary arteries (INOCA), however, is changing the landscape. In recent U.S. and European guidelines, intracoronary acetylcholine testing is indicated as a class 2a recommendation in MINOCA/INOCA.
“More and more institutions in Europe and the United States are starting to do acetylcholine testing, because now we know that chest pain isn’t necessarily coming from the blocked arteries,” Dr. Kobayashi said. “There are functional abnormalities, including coronary spasm, and if we diagnose it, we have appropriate medical regimens for this kind of disease.”
First safety meta-analysis
The present review and meta-analysis included 12,585 participants in 16 studies through November 2021. Of these, 63% were conducted in Western countries, and most were prospective studies published over the past decade in patients with MINOCA or INOCA.
Ten studies used the contemporary diagnostic criteria for epicardial spasm of at least 90% reduction in coronary diameter. Acetylcholine was administered into the left coronary artery at up to 100 mcg and 200 mcg in seven and six studies, respectively, and was used in the other three studies to assess endothelial function with a slower infusion of up to 36.4 mcg.
Major complications were significantly higher in studies following the contemporary diagnostic cutoff than in those using a lower cutoff of at least 75% diameter reduction (1.0% vs. 0.0%; P for between-group heterogeneity < .001).
The incidence of major complications was 0.2% with the slower infusion of up to 36.4 mcg, 0.8% with a maximum dose of 100 mcg, and 0.3% with a maximum dose of 200 mcg. The positive vasospasm rate was similar with the latter two protocols, at 46.3% and 41.4%, respectively.
Minor complications occurred in 3.3% of patients but were not detailed. They can include paroxysmal atrial fibrillation, ventricular ectopic beats, transient hypotension, and bradycardia requiring intervention.
As with major complications, minor complications were lower in studies using noncontemporary versus contemporary diagnostic cutoffs for epicardial spasm (1.8% vs. 4.7%) and in Western versus Asian populations (2.6% vs. 9.4%). Minor complications were similar between protocols with maximum doses of 100 mcg and 200 mcg (3.6% vs. 3.8%).
Dr. Kobayashi suggested that several factors may explain the racial differences, including previously reported smooth muscle hyperresponsiveness to provocation stimuli in Japanese patients and the inclusion of a wide range of patients in Japanese studies, such as those with obstructive coronary disease.
Japanese studies also used sequential acetylcholine injection into both the right and left coronaries, a faster injection speed of 20 seconds, and upfront placement of a temporary pacing catheter in case of acetylcholine-induced bradycardia, particularly with right coronary injection.
Although the protocol is largely settled in Japan, he said, provocation protocols need to be standardized because “depending on the country and depending on the institution, people are doing totally different things.”
A big step forward
Commenting on the study, C. Noel Bairey Merz, MD, from Cedars Sinai, Los Angeles, said it has “widespread relevance” because half of all coronary angiograms done invasively in the United States for suspected ischemia find no obstructive coronary disease. Left untreated, however, MINOCA has a 2.5% annual event rate, and a quarter of that is death.
“This is a big step forward with likely equal opportunity to improve women and men’s ischemic heart disease,” she said.
On the other hand, all studies were conducted at centers of excellence, so safety will need to be carefully watched as testing rolls out to more community care, Dr. Merz said. “And it always needs to be underscored that this is done by an interventional cardiologist because they’re familiar with wires that can dissect arteries, and they’re familiar with minor complications that could turn into major, if someone didn’t act appropriately.”
Dr. Merz also called for unifying protocols and the need to raise awareness within the general cardiology community to ask interventionalists for acetylcholine spasm testing. Randomized controlled data from within the WISE study and the CorMica study showed that diagnostic certainty leads to greater therapeutic certainty. “You do a much better job about who and how to treat,” she said.
There are also three ongoing randomized controlled trials – WARRIOR, MINOCA-BAT, and iCorMica – in the INOCA and MINOCA populations testing different treatment strategies for hard clinical outcomes like death and myocardial infarction.
“So in addition to this publication being guideline-forming for diagnosis, we anticipate in the next several years to have clinical trial evidence about therapeutics, again, for formulation of class 1 guidelines,” Dr. Merz said.
John Beltrame, BMBS, PhD, University of Adelaide, Australia, said the meta-analysis shows that intracoronary acetylcholine spasm testing is safe and should prompt greater adoption of invasive functional angiography.
Interventionalists are quite happy to do fractional flow reserve using intravenous adenosine to assess coronary microvascular dysfunction, he said, and “what we think is that functional angiography should test both – both the spasm as well as the microvasculature – and that will give us a clear direction because the treatments are slightly different when you’re treating the large arteries as compared to the microscopic arteries. It’s an important thing.”
Dr. Beltrame and colleagues further detail the benefits of comprehensive invasive functional angiography over structural angiography in a related editorial.
He also noted that the Coronary Vasomotion Disorders International Study Group published international diagnostic criteria for microvascular angina and that several protocols for acetylcholine spasm testing are in the works, including one from Australia. Australian investigators are also organizing an accreditation program for those performing the test.
“The protocol itself is relatively straightforward, but it’s not merely picking up a manual and following the instructions,” Dr. Beltrame said. “Just the same as when you train someone in angioplasty, you don’t just go out and do it. You need to develop some experience in it and so should be proctored.”
Dr. Kobayashi reported consulting agreements with Abbott Vascular. Coauthor disclosures are listed in the paper. Dr. Beltrame and colleagues have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Provocation testing with intracoronary acetylcholine is safe, particularly among Western patients, suggests a large systematic review that underscores the importance of functional coronary angiography to diagnose epicardial or microvascular spasm.
The results, derived from more than 12,000 patients in 16 studies, showed a 0.5% risk of major complications, defined as death, ventricular tachycardia/ventricular fibrillation, myocardial infarction, and shock requiring resuscitation.
Ventricular tachycardia/fibrillation were the most common events and mainly reported from two Japanese studies. There were no deaths.
Exploratory subgroup analyses revealed significantly fewer major complications in Western populations (0.0%; P for heterogeneity = .938), compared with Asian populations (2.3%; P for heterogeneity < .001).
The pooled positive vasospasm rate was also lower in Western versus Asian studies (37.9% vs. 50.7%; P for between-group heterogeneity = .010), as reported by the Microvascular Network in the Journal of the American College of Cardiology.
“If you look at the data between Asian studies versus others, mainly European or U.S. studies, primarily in Caucasian populations, it’s like zero percent history of major complications. So, it sounds extremely safe to do this testing in Caucasian populations,” Yuhei Kobayashi, MD, NewYork-Presbyterian Brooklyn Methodist Hospital, Weill Cornell Medicine, said.
Safety will need to be assessed in African Americans and other racial/ethnic groups, but “it makes us think we should end up testing more in the United States,” he told this news organization.
Intracoronary acetylcholine testing is daily practice in Japan but is limited in the United States and Europe to a few specialized centers due to safety concerns. Three deaths were reported in 1980 with intravenous ergonovine testing, whereas the safety of acetylcholine protocols has been studied largely in single-center retrospective studies, typically in Asian populations.
Growing recognition of myocardial infarction with nonobstructive coronary arteries (MINOCA) and ischemia with no obstructive coronary arteries (INOCA), however, is changing the landscape. In recent U.S. and European guidelines, intracoronary acetylcholine testing is indicated as a class 2a recommendation in MINOCA/INOCA.
“More and more institutions in Europe and the United States are starting to do acetylcholine testing, because now we know that chest pain isn’t necessarily coming from the blocked arteries,” Dr. Kobayashi said. “There are functional abnormalities, including coronary spasm, and if we diagnose it, we have appropriate medical regimens for this kind of disease.”
First safety meta-analysis
The present review and meta-analysis included 12,585 participants in 16 studies through November 2021. Of these, 63% were conducted in Western countries, and most were prospective studies published over the past decade in patients with MINOCA or INOCA.
Ten studies used the contemporary diagnostic criteria for epicardial spasm of at least 90% reduction in coronary diameter. Acetylcholine was administered into the left coronary artery at up to 100 mcg and 200 mcg in seven and six studies, respectively, and was used in the other three studies to assess endothelial function with a slower infusion of up to 36.4 mcg.
Major complications were significantly higher in studies following the contemporary diagnostic cutoff than in those using a lower cutoff of at least 75% diameter reduction (1.0% vs. 0.0%; P for between-group heterogeneity < .001).
The incidence of major complications was 0.2% with the slower infusion of up to 36.4 mcg, 0.8% with a maximum dose of 100 mcg, and 0.3% with a maximum dose of 200 mcg. The positive vasospasm rate was similar with the latter two protocols, at 46.3% and 41.4%, respectively.
Minor complications occurred in 3.3% of patients but were not detailed. They can include paroxysmal atrial fibrillation, ventricular ectopic beats, transient hypotension, and bradycardia requiring intervention.
As with major complications, minor complications were lower in studies using noncontemporary versus contemporary diagnostic cutoffs for epicardial spasm (1.8% vs. 4.7%) and in Western versus Asian populations (2.6% vs. 9.4%). Minor complications were similar between protocols with maximum doses of 100 mcg and 200 mcg (3.6% vs. 3.8%).
Dr. Kobayashi suggested that several factors may explain the racial differences, including previously reported smooth muscle hyperresponsiveness to provocation stimuli in Japanese patients and the inclusion of a wide range of patients in Japanese studies, such as those with obstructive coronary disease.
Japanese studies also used sequential acetylcholine injection into both the right and left coronaries, a faster injection speed of 20 seconds, and upfront placement of a temporary pacing catheter in case of acetylcholine-induced bradycardia, particularly with right coronary injection.
Although the protocol is largely settled in Japan, he said, provocation protocols need to be standardized because “depending on the country and depending on the institution, people are doing totally different things.”
A big step forward
Commenting on the study, C. Noel Bairey Merz, MD, from Cedars Sinai, Los Angeles, said it has “widespread relevance” because half of all coronary angiograms done invasively in the United States for suspected ischemia find no obstructive coronary disease. Left untreated, however, MINOCA has a 2.5% annual event rate, and a quarter of that is death.
“This is a big step forward with likely equal opportunity to improve women and men’s ischemic heart disease,” she said.
On the other hand, all studies were conducted at centers of excellence, so safety will need to be carefully watched as testing rolls out to more community care, Dr. Merz said. “And it always needs to be underscored that this is done by an interventional cardiologist because they’re familiar with wires that can dissect arteries, and they’re familiar with minor complications that could turn into major, if someone didn’t act appropriately.”
Dr. Merz also called for unifying protocols and the need to raise awareness within the general cardiology community to ask interventionalists for acetylcholine spasm testing. Randomized controlled data from within the WISE study and the CorMica study showed that diagnostic certainty leads to greater therapeutic certainty. “You do a much better job about who and how to treat,” she said.
There are also three ongoing randomized controlled trials – WARRIOR, MINOCA-BAT, and iCorMica – in the INOCA and MINOCA populations testing different treatment strategies for hard clinical outcomes like death and myocardial infarction.
“So in addition to this publication being guideline-forming for diagnosis, we anticipate in the next several years to have clinical trial evidence about therapeutics, again, for formulation of class 1 guidelines,” Dr. Merz said.
John Beltrame, BMBS, PhD, University of Adelaide, Australia, said the meta-analysis shows that intracoronary acetylcholine spasm testing is safe and should prompt greater adoption of invasive functional angiography.
Interventionalists are quite happy to do fractional flow reserve using intravenous adenosine to assess coronary microvascular dysfunction, he said, and “what we think is that functional angiography should test both – both the spasm as well as the microvasculature – and that will give us a clear direction because the treatments are slightly different when you’re treating the large arteries as compared to the microscopic arteries. It’s an important thing.”
Dr. Beltrame and colleagues further detail the benefits of comprehensive invasive functional angiography over structural angiography in a related editorial.
He also noted that the Coronary Vasomotion Disorders International Study Group published international diagnostic criteria for microvascular angina and that several protocols for acetylcholine spasm testing are in the works, including one from Australia. Australian investigators are also organizing an accreditation program for those performing the test.
“The protocol itself is relatively straightforward, but it’s not merely picking up a manual and following the instructions,” Dr. Beltrame said. “Just the same as when you train someone in angioplasty, you don’t just go out and do it. You need to develop some experience in it and so should be proctored.”
Dr. Kobayashi reported consulting agreements with Abbott Vascular. Coauthor disclosures are listed in the paper. Dr. Beltrame and colleagues have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Data concerns mount despite ISCHEMIA substudy correction
A long-standing request to clarify data irregularities in a 2021 ISCHEMIA substudy resulted in the publication of one correction, with a second correction in the works.
Further, the lone cardiac surgeon on the ISCHEMIA trial steering committee, T. Bruce Ferguson, MD, has resigned from the committee, citing a series of factors, including an inability to reconcile data in the substudy and two additional ISCHEMIA papers currently under review.
As previously reported, cardiac surgeons Faisal Bakaeen, MD, and Joseph Sabik III, MD, notified the journal Circulation in March that the Dr. Reynolds et al. substudy had inconsistencies between data in the main paper and supplemental tables detailing patients’ coronary artery disease (CAD) and ischemia severity.
The substudy found that CAD severity, classified using the modified Duke Prognostic Index score, predicted 4-year mortality and myocardial infarction in the landmark trial.
Circulation published a correction for the substudy on May 20, explaining that a “formatting error” resulted in data being incorrectly presented in two supplemental tables. It does not mention the surgeons’ letter to the editor, which can be found by clicking the “Q” icon below the paper.
Dr. Bakaeen, from the Cleveland Clinic, and Dr. Sabik, from University Hospitals Cleveland Medical Center, told this news organization that they submitted a second letter to editor on May 23 stating that “significant discrepancies” persist.
For example, 7.2% of participants (179/2,475) had moderate stenosis in one coronary vessel in the corrected Reynolds paper (Supplemental Tables I and II) versus 23.3% (697/2,986) in the primary ISCHEMIA manuscript published in the New England Journal of Medicine (Table S5).
The number of patients with left main ≥ 50% stenosis is, surprisingly, identical in both manuscripts, at 40, they said, despite the denominator dropping from 3,845 participants in the primary study to 2,475 participants with an evaluable modified Duke Prognostic Index score in the substudy.
The number of participants with previous coronary artery bypass surgery (CABG) is also hard to reconcile between manuscripts and, importantly, the substudy doesn’t distinguish between lesions bypassed with patent grafts and unbypassed grafts or those with occluded grafts.
“The fact that the authors are working on a second correction is appreciated, but with such numerous inconsistencies, at some point you reach the conclusion that an independent review of the data is the right thing to do for such a high-profile study that received over $100 million of National Institutes of Health support,” Dr. Bakaeen said. “No one should be satisfied or happy if there is any shadow of doubt here regarding the accuracy of the data.”
Speaking to this news organization prior to the first correction, lead substudy author Harmony Reynolds, MD, NYU Langone Health, detailed in depth how the formatting glitch inadvertently upgraded the number of diseased vessels and lesion severity in two supplemental tables.

She noted, as does the correction, that the data were correctly reported in the main manuscript tables and figures and in the remainder of the supplement.
Dr. Reynolds also said they’re in the process of preparing the data for “public sharing soon,” including the Duke Prognostic score at all levels. Dr. Reynolds had not responded by the time of this publication to a request for further details or a timeline.
The surgeons’ first letter to the editor was rejected because it was submitted outside the journal’s 6-week window for letters and was posted as a public comment April 18 via the research platform, Remarq.
Dr. Bakaeen said they were told their second letter was rejected because of Circulation’s “long standing policy” not to publish letters to the editor regarding manuscript corrections but that a correction is being issued.
Circulation editor-in-chief Joseph A. Hill, MD, PhD, UT Southwestern Medical Center, Dallas, said via email that the journal will update its online policies to more clearly state its requirements for publication and that it has been fully transparent with Dr. Bakaeen and Dr. Sabik regarding where it is in the current process.
He confirmed the surgeons were told June 1 that “after additional review, the authors have determined that whereas there are no errors, an additional minor correction is warranted to clarify the description of the study population and sample size. This correction will be published soon.”
Dr. Hill thanked Dr. Bakaeen and Dr. Sabik for bringing the matter to their attention and said, “It is also important to note that both updates to the Dr. Reynolds et al. paper are published as corrections. However, the results and conclusions of the paper remain unchanged.”
The bigger issue
Importantly, the recent AHA/ACC/SCAI coronary revascularization guidelines used ISCHEMIA data to support downgrading the CABG recommendation from class 1 to class 2B in 3-vessel CAD with normal left ventricular function and from class 1 to 2a in 3-vessel CAD with mild to moderate left ventricular dysfunction.
The trial reported no significant benefit with an initial invasive strategy over medical therapy in stable patients with moderate or severe CAD. European guidelines, however, give CABG a class I recommendation for severe three- or two-vessel disease with proximal left anterior descending (LAD) involvement.
Dr. Sabik and Dr. Bakaeen say patients with severe three- or two-vessel disease with proximal LAD involvement were underrepresented in the randomized trials cited by the guidelines but are the typical CABG patients in modern-day practice.
“That is why it is important to determine the severity of CAD accurately and definitively in ISCHEMIA,” Dr. Bakaeen said. “But the more we look at the data, the more errors we encounter.”
Two U.S. surgical groups that were part of the writing process withdrew support for the revascularization guidelines, as did several international surgical societies, citing the data used to support the changes as well as the makeup of the writing committee.
Dr. Ferguson, now with the medical device manufacturer Perfusio, said he resigned from the ISCHEMIA steering committee on May 8 after being unable to accurately reconcile the ISCHEMIA surgical subset data with the Reynolds substudy and two other ISCHEMIA papers on the CABG subset. At least one of those papers, he noted, was being hurriedly pushed through the review process to counter concerns raised by surgeons regarding interpretation of ISCHEMIA.
“This is the first time in my lengthy career in medicine where a level of political agendaism was actually driving the truck,” he said. “It was appalling to me, and I would have said that if I was an interventional cardiologist looking at the results.”
ISCHEMIA results have also been touted as representing state-of-the-art care around the world, but that didn’t appear to be the case for the surgical subset where, for example, China and India performed most CABGs off pump, and globally there was considerable variation in how surgeons approached surgical revascularization strategies, Dr. Ferguson said. “Whether this variability might impact the guideline discussion and these papers coming out remains to be determined.”
He noted that the study protocol allowed for the ISCHEMIA investigators to evaluate whether the variability in the surgical subset influenced the results by comparing the data to that in the Society of Thoracic Surgeons registry, but this option was never acted upon despite being brought to their attention.
“Something political between 2020 and 2022 has crept into the ISCHEMIA trial mindset gestalt, and I don’t like it,” Dr. Ferguson said. “And this can have enormous consequences.”
Asked whether their letters to Circulation are being used to undermine confidence in the ISCHEMIA findings, Dr. Sabik replied, “It is not about undermining ISCHEMIA, but understanding how applicable ISCHEMIA is to patients having CABG today. Understanding the severity of the CAD in patients enrolled in ISCHEMIA is, therefore, necessary.”
“The authors and Circulation have admitted to errors,” he said. “We want to be sure we understand how severe the errors are.”
“This is just about accuracy in a manuscript that may affect patient treatment and therefore patient lives. We want to make sure it is correct,” Dr. Sabik added.
A version of this article first appeared on Medscape.com.
A long-standing request to clarify data irregularities in a 2021 ISCHEMIA substudy resulted in the publication of one correction, with a second correction in the works.
Further, the lone cardiac surgeon on the ISCHEMIA trial steering committee, T. Bruce Ferguson, MD, has resigned from the committee, citing a series of factors, including an inability to reconcile data in the substudy and two additional ISCHEMIA papers currently under review.
As previously reported, cardiac surgeons Faisal Bakaeen, MD, and Joseph Sabik III, MD, notified the journal Circulation in March that the Dr. Reynolds et al. substudy had inconsistencies between data in the main paper and supplemental tables detailing patients’ coronary artery disease (CAD) and ischemia severity.
The substudy found that CAD severity, classified using the modified Duke Prognostic Index score, predicted 4-year mortality and myocardial infarction in the landmark trial.
Circulation published a correction for the substudy on May 20, explaining that a “formatting error” resulted in data being incorrectly presented in two supplemental tables. It does not mention the surgeons’ letter to the editor, which can be found by clicking the “Q” icon below the paper.
Dr. Bakaeen, from the Cleveland Clinic, and Dr. Sabik, from University Hospitals Cleveland Medical Center, told this news organization that they submitted a second letter to editor on May 23 stating that “significant discrepancies” persist.
For example, 7.2% of participants (179/2,475) had moderate stenosis in one coronary vessel in the corrected Reynolds paper (Supplemental Tables I and II) versus 23.3% (697/2,986) in the primary ISCHEMIA manuscript published in the New England Journal of Medicine (Table S5).
The number of patients with left main ≥ 50% stenosis is, surprisingly, identical in both manuscripts, at 40, they said, despite the denominator dropping from 3,845 participants in the primary study to 2,475 participants with an evaluable modified Duke Prognostic Index score in the substudy.
The number of participants with previous coronary artery bypass surgery (CABG) is also hard to reconcile between manuscripts and, importantly, the substudy doesn’t distinguish between lesions bypassed with patent grafts and unbypassed grafts or those with occluded grafts.
“The fact that the authors are working on a second correction is appreciated, but with such numerous inconsistencies, at some point you reach the conclusion that an independent review of the data is the right thing to do for such a high-profile study that received over $100 million of National Institutes of Health support,” Dr. Bakaeen said. “No one should be satisfied or happy if there is any shadow of doubt here regarding the accuracy of the data.”
Speaking to this news organization prior to the first correction, lead substudy author Harmony Reynolds, MD, NYU Langone Health, detailed in depth how the formatting glitch inadvertently upgraded the number of diseased vessels and lesion severity in two supplemental tables.
She noted, as does the correction, that the data were correctly reported in the main manuscript tables and figures and in the remainder of the supplement.
Dr. Reynolds also said they’re in the process of preparing the data for “public sharing soon,” including the Duke Prognostic score at all levels. Dr. Reynolds had not responded by the time of this publication to a request for further details or a timeline.
The surgeons’ first letter to the editor was rejected because it was submitted outside the journal’s 6-week window for letters and was posted as a public comment April 18 via the research platform, Remarq.
Dr. Bakaeen said they were told their second letter was rejected because of Circulation’s “long standing policy” not to publish letters to the editor regarding manuscript corrections but that a correction is being issued.
Circulation editor-in-chief Joseph A. Hill, MD, PhD, UT Southwestern Medical Center, Dallas, said via email that the journal will update its online policies to more clearly state its requirements for publication and that it has been fully transparent with Dr. Bakaeen and Dr. Sabik regarding where it is in the current process.
He confirmed the surgeons were told June 1 that “after additional review, the authors have determined that whereas there are no errors, an additional minor correction is warranted to clarify the description of the study population and sample size. This correction will be published soon.”
Dr. Hill thanked Dr. Bakaeen and Dr. Sabik for bringing the matter to their attention and said, “It is also important to note that both updates to the Dr. Reynolds et al. paper are published as corrections. However, the results and conclusions of the paper remain unchanged.”
The bigger issue
Importantly, the recent AHA/ACC/SCAI coronary revascularization guidelines used ISCHEMIA data to support downgrading the CABG recommendation from class 1 to class 2B in 3-vessel CAD with normal left ventricular function and from class 1 to 2a in 3-vessel CAD with mild to moderate left ventricular dysfunction.
The trial reported no significant benefit with an initial invasive strategy over medical therapy in stable patients with moderate or severe CAD. European guidelines, however, give CABG a class I recommendation for severe three- or two-vessel disease with proximal left anterior descending (LAD) involvement.
Dr. Sabik and Dr. Bakaeen say patients with severe three- or two-vessel disease with proximal LAD involvement were underrepresented in the randomized trials cited by the guidelines but are the typical CABG patients in modern-day practice.
“That is why it is important to determine the severity of CAD accurately and definitively in ISCHEMIA,” Dr. Bakaeen said. “But the more we look at the data, the more errors we encounter.”
Two U.S. surgical groups that were part of the writing process withdrew support for the revascularization guidelines, as did several international surgical societies, citing the data used to support the changes as well as the makeup of the writing committee.
Dr. Ferguson, now with the medical device manufacturer Perfusio, said he resigned from the ISCHEMIA steering committee on May 8 after being unable to accurately reconcile the ISCHEMIA surgical subset data with the Reynolds substudy and two other ISCHEMIA papers on the CABG subset. At least one of those papers, he noted, was being hurriedly pushed through the review process to counter concerns raised by surgeons regarding interpretation of ISCHEMIA.
“This is the first time in my lengthy career in medicine where a level of political agendaism was actually driving the truck,” he said. “It was appalling to me, and I would have said that if I was an interventional cardiologist looking at the results.”
ISCHEMIA results have also been touted as representing state-of-the-art care around the world, but that didn’t appear to be the case for the surgical subset where, for example, China and India performed most CABGs off pump, and globally there was considerable variation in how surgeons approached surgical revascularization strategies, Dr. Ferguson said. “Whether this variability might impact the guideline discussion and these papers coming out remains to be determined.”
He noted that the study protocol allowed for the ISCHEMIA investigators to evaluate whether the variability in the surgical subset influenced the results by comparing the data to that in the Society of Thoracic Surgeons registry, but this option was never acted upon despite being brought to their attention.
“Something political between 2020 and 2022 has crept into the ISCHEMIA trial mindset gestalt, and I don’t like it,” Dr. Ferguson said. “And this can have enormous consequences.”
Asked whether their letters to Circulation are being used to undermine confidence in the ISCHEMIA findings, Dr. Sabik replied, “It is not about undermining ISCHEMIA, but understanding how applicable ISCHEMIA is to patients having CABG today. Understanding the severity of the CAD in patients enrolled in ISCHEMIA is, therefore, necessary.”
“The authors and Circulation have admitted to errors,” he said. “We want to be sure we understand how severe the errors are.”
“This is just about accuracy in a manuscript that may affect patient treatment and therefore patient lives. We want to make sure it is correct,” Dr. Sabik added.
A version of this article first appeared on Medscape.com.
A long-standing request to clarify data irregularities in a 2021 ISCHEMIA substudy resulted in the publication of one correction, with a second correction in the works.
Further, the lone cardiac surgeon on the ISCHEMIA trial steering committee, T. Bruce Ferguson, MD, has resigned from the committee, citing a series of factors, including an inability to reconcile data in the substudy and two additional ISCHEMIA papers currently under review.
As previously reported, cardiac surgeons Faisal Bakaeen, MD, and Joseph Sabik III, MD, notified the journal Circulation in March that the Dr. Reynolds et al. substudy had inconsistencies between data in the main paper and supplemental tables detailing patients’ coronary artery disease (CAD) and ischemia severity.
The substudy found that CAD severity, classified using the modified Duke Prognostic Index score, predicted 4-year mortality and myocardial infarction in the landmark trial.
Circulation published a correction for the substudy on May 20, explaining that a “formatting error” resulted in data being incorrectly presented in two supplemental tables. It does not mention the surgeons’ letter to the editor, which can be found by clicking the “Q” icon below the paper.
Dr. Bakaeen, from the Cleveland Clinic, and Dr. Sabik, from University Hospitals Cleveland Medical Center, told this news organization that they submitted a second letter to editor on May 23 stating that “significant discrepancies” persist.
For example, 7.2% of participants (179/2,475) had moderate stenosis in one coronary vessel in the corrected Reynolds paper (Supplemental Tables I and II) versus 23.3% (697/2,986) in the primary ISCHEMIA manuscript published in the New England Journal of Medicine (Table S5).
The number of patients with left main ≥ 50% stenosis is, surprisingly, identical in both manuscripts, at 40, they said, despite the denominator dropping from 3,845 participants in the primary study to 2,475 participants with an evaluable modified Duke Prognostic Index score in the substudy.
The number of participants with previous coronary artery bypass surgery (CABG) is also hard to reconcile between manuscripts and, importantly, the substudy doesn’t distinguish between lesions bypassed with patent grafts and unbypassed grafts or those with occluded grafts.
“The fact that the authors are working on a second correction is appreciated, but with such numerous inconsistencies, at some point you reach the conclusion that an independent review of the data is the right thing to do for such a high-profile study that received over $100 million of National Institutes of Health support,” Dr. Bakaeen said. “No one should be satisfied or happy if there is any shadow of doubt here regarding the accuracy of the data.”
Speaking to this news organization prior to the first correction, lead substudy author Harmony Reynolds, MD, NYU Langone Health, detailed in depth how the formatting glitch inadvertently upgraded the number of diseased vessels and lesion severity in two supplemental tables.
She noted, as does the correction, that the data were correctly reported in the main manuscript tables and figures and in the remainder of the supplement.
Dr. Reynolds also said they’re in the process of preparing the data for “public sharing soon,” including the Duke Prognostic score at all levels. Dr. Reynolds had not responded by the time of this publication to a request for further details or a timeline.
The surgeons’ first letter to the editor was rejected because it was submitted outside the journal’s 6-week window for letters and was posted as a public comment April 18 via the research platform, Remarq.
Dr. Bakaeen said they were told their second letter was rejected because of Circulation’s “long standing policy” not to publish letters to the editor regarding manuscript corrections but that a correction is being issued.
Circulation editor-in-chief Joseph A. Hill, MD, PhD, UT Southwestern Medical Center, Dallas, said via email that the journal will update its online policies to more clearly state its requirements for publication and that it has been fully transparent with Dr. Bakaeen and Dr. Sabik regarding where it is in the current process.
He confirmed the surgeons were told June 1 that “after additional review, the authors have determined that whereas there are no errors, an additional minor correction is warranted to clarify the description of the study population and sample size. This correction will be published soon.”
Dr. Hill thanked Dr. Bakaeen and Dr. Sabik for bringing the matter to their attention and said, “It is also important to note that both updates to the Dr. Reynolds et al. paper are published as corrections. However, the results and conclusions of the paper remain unchanged.”
The bigger issue
Importantly, the recent AHA/ACC/SCAI coronary revascularization guidelines used ISCHEMIA data to support downgrading the CABG recommendation from class 1 to class 2B in 3-vessel CAD with normal left ventricular function and from class 1 to 2a in 3-vessel CAD with mild to moderate left ventricular dysfunction.
The trial reported no significant benefit with an initial invasive strategy over medical therapy in stable patients with moderate or severe CAD. European guidelines, however, give CABG a class I recommendation for severe three- or two-vessel disease with proximal left anterior descending (LAD) involvement.
Dr. Sabik and Dr. Bakaeen say patients with severe three- or two-vessel disease with proximal LAD involvement were underrepresented in the randomized trials cited by the guidelines but are the typical CABG patients in modern-day practice.
“That is why it is important to determine the severity of CAD accurately and definitively in ISCHEMIA,” Dr. Bakaeen said. “But the more we look at the data, the more errors we encounter.”
Two U.S. surgical groups that were part of the writing process withdrew support for the revascularization guidelines, as did several international surgical societies, citing the data used to support the changes as well as the makeup of the writing committee.
Dr. Ferguson, now with the medical device manufacturer Perfusio, said he resigned from the ISCHEMIA steering committee on May 8 after being unable to accurately reconcile the ISCHEMIA surgical subset data with the Reynolds substudy and two other ISCHEMIA papers on the CABG subset. At least one of those papers, he noted, was being hurriedly pushed through the review process to counter concerns raised by surgeons regarding interpretation of ISCHEMIA.
“This is the first time in my lengthy career in medicine where a level of political agendaism was actually driving the truck,” he said. “It was appalling to me, and I would have said that if I was an interventional cardiologist looking at the results.”
ISCHEMIA results have also been touted as representing state-of-the-art care around the world, but that didn’t appear to be the case for the surgical subset where, for example, China and India performed most CABGs off pump, and globally there was considerable variation in how surgeons approached surgical revascularization strategies, Dr. Ferguson said. “Whether this variability might impact the guideline discussion and these papers coming out remains to be determined.”
He noted that the study protocol allowed for the ISCHEMIA investigators to evaluate whether the variability in the surgical subset influenced the results by comparing the data to that in the Society of Thoracic Surgeons registry, but this option was never acted upon despite being brought to their attention.
“Something political between 2020 and 2022 has crept into the ISCHEMIA trial mindset gestalt, and I don’t like it,” Dr. Ferguson said. “And this can have enormous consequences.”
Asked whether their letters to Circulation are being used to undermine confidence in the ISCHEMIA findings, Dr. Sabik replied, “It is not about undermining ISCHEMIA, but understanding how applicable ISCHEMIA is to patients having CABG today. Understanding the severity of the CAD in patients enrolled in ISCHEMIA is, therefore, necessary.”
“The authors and Circulation have admitted to errors,” he said. “We want to be sure we understand how severe the errors are.”
“This is just about accuracy in a manuscript that may affect patient treatment and therefore patient lives. We want to make sure it is correct,” Dr. Sabik added.
A version of this article first appeared on Medscape.com.
Distal radial snuffbox technique comes up short in DISCO RADIAL
Distal radial access is not superior to conventional radial access with regard to radial artery occlusion (RAO) but is a valid alternative for use in percutaneous procedures, according to results of the DISCO RADIAL trial.
The primary endpoint of forearm RAO at discharge was not met, occurring in 0.31% of patients whose radial artery was accessed distally (DRA) at the anatomical snuffbox and in 0.91% of patients with conventional transradial access (TRA) in the intention-to-treat analysis (P = .29).
The DRA group was also twice as likely to crossover to another access point (7.5% vs. 3.7%; P = .002) and to experience radial artery spasm (5.4% vs. 2.7%; P < .015).
“The message first is that if you do a good job with transradial access you can end up with a lower [occlusion] rate,” said coprincipal investigator Adel Aminian, MD, Hôpital Civil Marie Curie, Charleroi, Belgium. “On the other hand, it’s a trade-off between a more demanding puncture for distal radial access but also a simpler hemostatic process, which I think is one of the main advantages of distal radial access.”
The results were presented during the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, and published simultaneously in JACC: Cardiovascular Interventions.
DISCO-RADIAL (Distal Versus Conventional RADIAL Access for Coronary Angiography and Intervention) is the largest trial thus far to compare TRA with the distal radial snuffbox technique, which has shown promise for reducing RAO rates in the recent single-center randomized DAPRAO and ANGIE trials.
The trial was conducted at 15 sites across Europe and Japan in 1,309 patients with an indication for percutaneous coronary procedures using the 6Fr Glidesheath Slender (Terumo). The intention-to-treat population included 657 TRA patients and 650 DRA patients.
The two groups were well matched, with most having a chronic coronary syndrome. Operators had to have performed a minimum of 100 procedures by DRA and follow systematic best practices previously reported by the investigators to prevent RAO, Dr. Aminian said.
The use of DRA did not significantly affect the duration of the coronary procedure (27 minutes vs. 24 minutes with TRA; P = .12) or average radiation dose (1298 mGy vs. 1222 mGy; P = .70).
DRA, however, reduced the need for selective compression devices (88% vs. 99.2%) and shortened the median time to hemostasis from 180 minutes to 153 minutes (P for both < .001).
“These results establish compliance to best practice recommendations for RAO avoidance as a mandatory new reference in transradial practice,” Dr. Aminian concluded. “At the same time, distal radial artery arises as a valid alternative associated with higher crossover rates but with a simpler and shorter hemostasis process.”
A show of hands revealed that about 25% of the audience used distal radial access prior to the presentation but that enthusiasm fell off following the results.
Discussant Hany Eteiba, MD, Glasgow Royal Infirmary, said: “I salute your enthusiasm for presenting a negative trial and you tried to persuade the audience to use the distal radial artery results, but nonetheless.”
Dr. Eteiba said he could see a “potential advantage in the shorter hemostasis time,” and asked whether it might be influencing the rapid turnover for day-case angioplasty.
Dr. Aminian responded that “if you do an angioplasty you have to keep the patient for a certain amount of time, but I think for your nurse work and for the health care resources, having a very short hemostasis time is very interesting. We started with a hemostasis time of 2 hours and now we’ve decreased it to 1 hour and it will decrease even more.”
Session moderator Chaim Lotan, MD, Hadassah-Hebrew University Medical Center, Jerusalem, called DISCO-RADIAL an important study and said, “the question now is what’s the indication in your eyes for using distal radial?”
Dr. Aminian said that one message from the trial is that people who are using transradial access “have to do a better job,” and reminded the audience that RAO rates at many centers are too high, at 10% or upward.
At the same time, Dr. Aminian cautioned that operators wanting to use distal radial access “need to master the technique” or they will “end up with a relatively high failure rate.”
Discussant Eliano Navarese, MD, Nicolaus Copernicus University, Toruń, Poland, said, “I still think that it is a very valid approach, we use it for almost 20 years ... but it is very true, it is very demanding. And the learning curve of 100 cases in the trial maybe needed more cases.”
In an accompanying editorial, Grigorios Tsigkas, MD, PhD, University of Patras, Rio Patras, Greece, and colleagues wrote that the incidence of forearm RAO was “surprisingly low” but could be even lower if the authors administered adequate anticoagulation.
Still, they wrote that distal transradial access “for coronary procedures in combination with the systematic implementation of best practices for RAO prevention may be the final solution against RAO.”
The editorialists suggested that exposure to radiation could be the “main limitation of this novel vascular approach” and that forthcoming trials, such as DOSE, could shed light on this issue.
Increased procedure times in the DISCO RADIAL and ANGIE trials are secondary in stable patients, Dr. Tsigkas said, but could be a limitation in patients presenting with ST-segment elevation myocardial infarction (STEMI). Ongoing research, such as the RESERVE trial from China and a Korean trial, will provide insights into the safety and feasibility of distal transradial access in STEMI.
The study was supported by Terumo Europe. Dr. Aminian reported receiving honoraria or consultation fees from Abbott, Boston Scientific, and Terumo Interventional Systems. Dr. Tsigkas reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Distal radial access is not superior to conventional radial access with regard to radial artery occlusion (RAO) but is a valid alternative for use in percutaneous procedures, according to results of the DISCO RADIAL trial.
The primary endpoint of forearm RAO at discharge was not met, occurring in 0.31% of patients whose radial artery was accessed distally (DRA) at the anatomical snuffbox and in 0.91% of patients with conventional transradial access (TRA) in the intention-to-treat analysis (P = .29).
The DRA group was also twice as likely to crossover to another access point (7.5% vs. 3.7%; P = .002) and to experience radial artery spasm (5.4% vs. 2.7%; P < .015).
“The message first is that if you do a good job with transradial access you can end up with a lower [occlusion] rate,” said coprincipal investigator Adel Aminian, MD, Hôpital Civil Marie Curie, Charleroi, Belgium. “On the other hand, it’s a trade-off between a more demanding puncture for distal radial access but also a simpler hemostatic process, which I think is one of the main advantages of distal radial access.”
The results were presented during the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, and published simultaneously in JACC: Cardiovascular Interventions.
DISCO-RADIAL (Distal Versus Conventional RADIAL Access for Coronary Angiography and Intervention) is the largest trial thus far to compare TRA with the distal radial snuffbox technique, which has shown promise for reducing RAO rates in the recent single-center randomized DAPRAO and ANGIE trials.
The trial was conducted at 15 sites across Europe and Japan in 1,309 patients with an indication for percutaneous coronary procedures using the 6Fr Glidesheath Slender (Terumo). The intention-to-treat population included 657 TRA patients and 650 DRA patients.
The two groups were well matched, with most having a chronic coronary syndrome. Operators had to have performed a minimum of 100 procedures by DRA and follow systematic best practices previously reported by the investigators to prevent RAO, Dr. Aminian said.
The use of DRA did not significantly affect the duration of the coronary procedure (27 minutes vs. 24 minutes with TRA; P = .12) or average radiation dose (1298 mGy vs. 1222 mGy; P = .70).
DRA, however, reduced the need for selective compression devices (88% vs. 99.2%) and shortened the median time to hemostasis from 180 minutes to 153 minutes (P for both < .001).
“These results establish compliance to best practice recommendations for RAO avoidance as a mandatory new reference in transradial practice,” Dr. Aminian concluded. “At the same time, distal radial artery arises as a valid alternative associated with higher crossover rates but with a simpler and shorter hemostasis process.”
A show of hands revealed that about 25% of the audience used distal radial access prior to the presentation but that enthusiasm fell off following the results.
Discussant Hany Eteiba, MD, Glasgow Royal Infirmary, said: “I salute your enthusiasm for presenting a negative trial and you tried to persuade the audience to use the distal radial artery results, but nonetheless.”
Dr. Eteiba said he could see a “potential advantage in the shorter hemostasis time,” and asked whether it might be influencing the rapid turnover for day-case angioplasty.
Dr. Aminian responded that “if you do an angioplasty you have to keep the patient for a certain amount of time, but I think for your nurse work and for the health care resources, having a very short hemostasis time is very interesting. We started with a hemostasis time of 2 hours and now we’ve decreased it to 1 hour and it will decrease even more.”
Session moderator Chaim Lotan, MD, Hadassah-Hebrew University Medical Center, Jerusalem, called DISCO-RADIAL an important study and said, “the question now is what’s the indication in your eyes for using distal radial?”
Dr. Aminian said that one message from the trial is that people who are using transradial access “have to do a better job,” and reminded the audience that RAO rates at many centers are too high, at 10% or upward.
At the same time, Dr. Aminian cautioned that operators wanting to use distal radial access “need to master the technique” or they will “end up with a relatively high failure rate.”
Discussant Eliano Navarese, MD, Nicolaus Copernicus University, Toruń, Poland, said, “I still think that it is a very valid approach, we use it for almost 20 years ... but it is very true, it is very demanding. And the learning curve of 100 cases in the trial maybe needed more cases.”
In an accompanying editorial, Grigorios Tsigkas, MD, PhD, University of Patras, Rio Patras, Greece, and colleagues wrote that the incidence of forearm RAO was “surprisingly low” but could be even lower if the authors administered adequate anticoagulation.
Still, they wrote that distal transradial access “for coronary procedures in combination with the systematic implementation of best practices for RAO prevention may be the final solution against RAO.”
The editorialists suggested that exposure to radiation could be the “main limitation of this novel vascular approach” and that forthcoming trials, such as DOSE, could shed light on this issue.
Increased procedure times in the DISCO RADIAL and ANGIE trials are secondary in stable patients, Dr. Tsigkas said, but could be a limitation in patients presenting with ST-segment elevation myocardial infarction (STEMI). Ongoing research, such as the RESERVE trial from China and a Korean trial, will provide insights into the safety and feasibility of distal transradial access in STEMI.
The study was supported by Terumo Europe. Dr. Aminian reported receiving honoraria or consultation fees from Abbott, Boston Scientific, and Terumo Interventional Systems. Dr. Tsigkas reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Distal radial access is not superior to conventional radial access with regard to radial artery occlusion (RAO) but is a valid alternative for use in percutaneous procedures, according to results of the DISCO RADIAL trial.
The primary endpoint of forearm RAO at discharge was not met, occurring in 0.31% of patients whose radial artery was accessed distally (DRA) at the anatomical snuffbox and in 0.91% of patients with conventional transradial access (TRA) in the intention-to-treat analysis (P = .29).
The DRA group was also twice as likely to crossover to another access point (7.5% vs. 3.7%; P = .002) and to experience radial artery spasm (5.4% vs. 2.7%; P < .015).
“The message first is that if you do a good job with transradial access you can end up with a lower [occlusion] rate,” said coprincipal investigator Adel Aminian, MD, Hôpital Civil Marie Curie, Charleroi, Belgium. “On the other hand, it’s a trade-off between a more demanding puncture for distal radial access but also a simpler hemostatic process, which I think is one of the main advantages of distal radial access.”
The results were presented during the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, and published simultaneously in JACC: Cardiovascular Interventions.
DISCO-RADIAL (Distal Versus Conventional RADIAL Access for Coronary Angiography and Intervention) is the largest trial thus far to compare TRA with the distal radial snuffbox technique, which has shown promise for reducing RAO rates in the recent single-center randomized DAPRAO and ANGIE trials.
The trial was conducted at 15 sites across Europe and Japan in 1,309 patients with an indication for percutaneous coronary procedures using the 6Fr Glidesheath Slender (Terumo). The intention-to-treat population included 657 TRA patients and 650 DRA patients.
The two groups were well matched, with most having a chronic coronary syndrome. Operators had to have performed a minimum of 100 procedures by DRA and follow systematic best practices previously reported by the investigators to prevent RAO, Dr. Aminian said.
The use of DRA did not significantly affect the duration of the coronary procedure (27 minutes vs. 24 minutes with TRA; P = .12) or average radiation dose (1298 mGy vs. 1222 mGy; P = .70).
DRA, however, reduced the need for selective compression devices (88% vs. 99.2%) and shortened the median time to hemostasis from 180 minutes to 153 minutes (P for both < .001).
“These results establish compliance to best practice recommendations for RAO avoidance as a mandatory new reference in transradial practice,” Dr. Aminian concluded. “At the same time, distal radial artery arises as a valid alternative associated with higher crossover rates but with a simpler and shorter hemostasis process.”
A show of hands revealed that about 25% of the audience used distal radial access prior to the presentation but that enthusiasm fell off following the results.
Discussant Hany Eteiba, MD, Glasgow Royal Infirmary, said: “I salute your enthusiasm for presenting a negative trial and you tried to persuade the audience to use the distal radial artery results, but nonetheless.”
Dr. Eteiba said he could see a “potential advantage in the shorter hemostasis time,” and asked whether it might be influencing the rapid turnover for day-case angioplasty.
Dr. Aminian responded that “if you do an angioplasty you have to keep the patient for a certain amount of time, but I think for your nurse work and for the health care resources, having a very short hemostasis time is very interesting. We started with a hemostasis time of 2 hours and now we’ve decreased it to 1 hour and it will decrease even more.”
Session moderator Chaim Lotan, MD, Hadassah-Hebrew University Medical Center, Jerusalem, called DISCO-RADIAL an important study and said, “the question now is what’s the indication in your eyes for using distal radial?”
Dr. Aminian said that one message from the trial is that people who are using transradial access “have to do a better job,” and reminded the audience that RAO rates at many centers are too high, at 10% or upward.
At the same time, Dr. Aminian cautioned that operators wanting to use distal radial access “need to master the technique” or they will “end up with a relatively high failure rate.”
Discussant Eliano Navarese, MD, Nicolaus Copernicus University, Toruń, Poland, said, “I still think that it is a very valid approach, we use it for almost 20 years ... but it is very true, it is very demanding. And the learning curve of 100 cases in the trial maybe needed more cases.”
In an accompanying editorial, Grigorios Tsigkas, MD, PhD, University of Patras, Rio Patras, Greece, and colleagues wrote that the incidence of forearm RAO was “surprisingly low” but could be even lower if the authors administered adequate anticoagulation.
Still, they wrote that distal transradial access “for coronary procedures in combination with the systematic implementation of best practices for RAO prevention may be the final solution against RAO.”
The editorialists suggested that exposure to radiation could be the “main limitation of this novel vascular approach” and that forthcoming trials, such as DOSE, could shed light on this issue.
Increased procedure times in the DISCO RADIAL and ANGIE trials are secondary in stable patients, Dr. Tsigkas said, but could be a limitation in patients presenting with ST-segment elevation myocardial infarction (STEMI). Ongoing research, such as the RESERVE trial from China and a Korean trial, will provide insights into the safety and feasibility of distal transradial access in STEMI.
The study was supported by Terumo Europe. Dr. Aminian reported receiving honoraria or consultation fees from Abbott, Boston Scientific, and Terumo Interventional Systems. Dr. Tsigkas reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EUROPCR 2022