User login
VIDEO: Dr. Matteo Lambertini answers questions on temporary ovarian suppression
SAN ANTONIO – A meta-analysis of five trials among 873 premenopausal women with early breast cancer finds that temporarily suppressing ovarian function with a gonadotropin-releasing hormone analog during chemotherapy helps preserve fertility, reducing risk of premature ovarian insufficiency by 62% and nearly doubling the posttreatment pregnancy rate. In an interview at the San Antonio Breast Cancer Symposium, lead investigator Matteo Lambertini, MD, of the Institut Jules Bordet in Brussels, Belgium, discussed subgroup findings, the risk-benefit profile, and appropriate patient selection, as well as avenues for future research in this area.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – A meta-analysis of five trials among 873 premenopausal women with early breast cancer finds that temporarily suppressing ovarian function with a gonadotropin-releasing hormone analog during chemotherapy helps preserve fertility, reducing risk of premature ovarian insufficiency by 62% and nearly doubling the posttreatment pregnancy rate. In an interview at the San Antonio Breast Cancer Symposium, lead investigator Matteo Lambertini, MD, of the Institut Jules Bordet in Brussels, Belgium, discussed subgroup findings, the risk-benefit profile, and appropriate patient selection, as well as avenues for future research in this area.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – A meta-analysis of five trials among 873 premenopausal women with early breast cancer finds that temporarily suppressing ovarian function with a gonadotropin-releasing hormone analog during chemotherapy helps preserve fertility, reducing risk of premature ovarian insufficiency by 62% and nearly doubling the posttreatment pregnancy rate. In an interview at the San Antonio Breast Cancer Symposium, lead investigator Matteo Lambertini, MD, of the Institut Jules Bordet in Brussels, Belgium, discussed subgroup findings, the risk-benefit profile, and appropriate patient selection, as well as avenues for future research in this area.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
REPORTING FROM SABCS 2017

VIDEO: Dr. Sherene Loi discusses PANACEA trial and implications for pembrolizumab use
SAN ANTONIO – The phase 1b/2 PANACEA trial of pembrolizumab and trastuzumab in trastuzumab-resistant HER2-positive advanced breast cancer met its primary endpoint, showing an overall response rate of 15.2% in the PD-L1-positive cohort and controlling disease for almost a year without chemotherapy, Sherene Loi, MD, PhD, of the Peter MacCallum Cancer Centre in Melbourne reported on behalf of the International Breast Cancer Study Group (IBCSG). But level of antitumor immunity was key. In an interview at the San Antonio Breast Cancer Symposium, Dr. Loi discussed the findings and possible implications for use of pembrolizumab earlier in the disease course.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – The phase 1b/2 PANACEA trial of pembrolizumab and trastuzumab in trastuzumab-resistant HER2-positive advanced breast cancer met its primary endpoint, showing an overall response rate of 15.2% in the PD-L1-positive cohort and controlling disease for almost a year without chemotherapy, Sherene Loi, MD, PhD, of the Peter MacCallum Cancer Centre in Melbourne reported on behalf of the International Breast Cancer Study Group (IBCSG). But level of antitumor immunity was key. In an interview at the San Antonio Breast Cancer Symposium, Dr. Loi discussed the findings and possible implications for use of pembrolizumab earlier in the disease course.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – The phase 1b/2 PANACEA trial of pembrolizumab and trastuzumab in trastuzumab-resistant HER2-positive advanced breast cancer met its primary endpoint, showing an overall response rate of 15.2% in the PD-L1-positive cohort and controlling disease for almost a year without chemotherapy, Sherene Loi, MD, PhD, of the Peter MacCallum Cancer Centre in Melbourne reported on behalf of the International Breast Cancer Study Group (IBCSG). But level of antitumor immunity was key. In an interview at the San Antonio Breast Cancer Symposium, Dr. Loi discussed the findings and possible implications for use of pembrolizumab earlier in the disease course.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
REPORTING FROM SABCS 2017

VIDEO: Meta-analysis lead author Dr. Richard Gray on dose intensity benefit
SAN ANTONIO – Increasing the dose intensity of adjuvant chemotherapy reduced risks of breast cancer recurrence and death by about 15% in an Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) meta-analysis of individual patient data from 25 randomized trials among 34,122 women. Lead author Richard Gray, MSc, professor of medical statistics in the Nuffield Department of Population Health at University of Oxford, England, discussed the findings for various dose-intensification approaches and likely impact on clinical practice in an interview at the San Antonio Breast Cancer Symposium.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – Increasing the dose intensity of adjuvant chemotherapy reduced risks of breast cancer recurrence and death by about 15% in an Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) meta-analysis of individual patient data from 25 randomized trials among 34,122 women. Lead author Richard Gray, MSc, professor of medical statistics in the Nuffield Department of Population Health at University of Oxford, England, discussed the findings for various dose-intensification approaches and likely impact on clinical practice in an interview at the San Antonio Breast Cancer Symposium.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – Increasing the dose intensity of adjuvant chemotherapy reduced risks of breast cancer recurrence and death by about 15% in an Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) meta-analysis of individual patient data from 25 randomized trials among 34,122 women. Lead author Richard Gray, MSc, professor of medical statistics in the Nuffield Department of Population Health at University of Oxford, England, discussed the findings for various dose-intensification approaches and likely impact on clinical practice in an interview at the San Antonio Breast Cancer Symposium.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
REPORTING FROM SABCS 2017

Levofloxacin prophylaxis in AML reduces febrile neutropenia admissions
In patients with acute myeloid leukemia (AML), giving levofloxacin for febrile neutropenia prophylaxis reduced hospital admissions due to this complication by about one-quarter, according to results of a retrospective cohort study.
“Multiple studies have demonstrated the use of an oral fluoroquinolone antibiotic to prevent febrile neutropenia readmission to hospital after receiving consolidation chemotherapy,” Samantha S. F. Lee, PharmD, a clinical pharmacist at St. Michael’s Hospital in Toronto, and her colleagues wrote. “However, this is the first study to demonstrate a positive outcome specific to the AML population.”
The results support recommendations made by the Infectious Diseases Society of America and the National Comprehensive Cancer Network related to treatment of AML after receiving consolidation chemotherapy.
For the study, the investigators retrospectively reviewed the charts of consecutive patients with AML treated at London Health Sciences Centre, a tertiary academic medical center, between 2006 and 2013. They compared outcomes between 50 patients who were prescribed prophylactic levofloxacin (Levaquin) after consolidation therapy and 50 patients who were not prescribed any antibiotics.
Overall, patients given levofloxacin had a lower rate of hospital readmission due to febrile neutropenia whether given the antibiotic after the first chemotherapy consolidation cycle (42% vs. 72%, P = .002) or after all cycles (51.4% vs. 67%, P = .023).
None of the patients in the levofloxacin group developed Clostridium difficile–associated diarrhea within 30 days from discharge after receiving the first cycle of consolidation chemotherapy, compared with one patient in the group not given the antibiotic (Support Care Cancer. 2017 Nov 23. doi: 10.1007/s00520-017-3976-1).
The use of levofloxacin did not significantly impact secondary outcomes, including total days of antibiotic treatment provided to febrile neutropenic patients, days to readmission for febrile neutropenia, or the rate of positive bacterial cultures returned in febrile neutropenic patients.
It was not possible to assess differences in the rate of fluoroquinolone resistance in positive bacterial cultures because fluoroquinolone susceptibilities were infrequently reported.
“This study provides evidence of a strong association between prophylaxis with oral levofloxacin and the rate of febrile neutropenia, but further study is required to evaluate the impact of fluoroquinolone use on antibiotic resistance and [Clostridium difficile–associated diarrhea] rates in this patient setting,” the investigators wrote.
The study was limited by the small sample size, which precluded accurate ascertainment of some outcomes, including safety outcomes, they noted. Additionally, adherence to oral therapy was unknown, and some data, such as fluoroquinolone resistance, were missing for patients admitted for febrile neutropenia to outside hospitals.
Dr. Lee reported having no relevant conflicts of interest.
In patients with acute myeloid leukemia (AML), giving levofloxacin for febrile neutropenia prophylaxis reduced hospital admissions due to this complication by about one-quarter, according to results of a retrospective cohort study.
“Multiple studies have demonstrated the use of an oral fluoroquinolone antibiotic to prevent febrile neutropenia readmission to hospital after receiving consolidation chemotherapy,” Samantha S. F. Lee, PharmD, a clinical pharmacist at St. Michael’s Hospital in Toronto, and her colleagues wrote. “However, this is the first study to demonstrate a positive outcome specific to the AML population.”
The results support recommendations made by the Infectious Diseases Society of America and the National Comprehensive Cancer Network related to treatment of AML after receiving consolidation chemotherapy.
For the study, the investigators retrospectively reviewed the charts of consecutive patients with AML treated at London Health Sciences Centre, a tertiary academic medical center, between 2006 and 2013. They compared outcomes between 50 patients who were prescribed prophylactic levofloxacin (Levaquin) after consolidation therapy and 50 patients who were not prescribed any antibiotics.
Overall, patients given levofloxacin had a lower rate of hospital readmission due to febrile neutropenia whether given the antibiotic after the first chemotherapy consolidation cycle (42% vs. 72%, P = .002) or after all cycles (51.4% vs. 67%, P = .023).
None of the patients in the levofloxacin group developed Clostridium difficile–associated diarrhea within 30 days from discharge after receiving the first cycle of consolidation chemotherapy, compared with one patient in the group not given the antibiotic (Support Care Cancer. 2017 Nov 23. doi: 10.1007/s00520-017-3976-1).
The use of levofloxacin did not significantly impact secondary outcomes, including total days of antibiotic treatment provided to febrile neutropenic patients, days to readmission for febrile neutropenia, or the rate of positive bacterial cultures returned in febrile neutropenic patients.
It was not possible to assess differences in the rate of fluoroquinolone resistance in positive bacterial cultures because fluoroquinolone susceptibilities were infrequently reported.
“This study provides evidence of a strong association between prophylaxis with oral levofloxacin and the rate of febrile neutropenia, but further study is required to evaluate the impact of fluoroquinolone use on antibiotic resistance and [Clostridium difficile–associated diarrhea] rates in this patient setting,” the investigators wrote.
The study was limited by the small sample size, which precluded accurate ascertainment of some outcomes, including safety outcomes, they noted. Additionally, adherence to oral therapy was unknown, and some data, such as fluoroquinolone resistance, were missing for patients admitted for febrile neutropenia to outside hospitals.
Dr. Lee reported having no relevant conflicts of interest.
In patients with acute myeloid leukemia (AML), giving levofloxacin for febrile neutropenia prophylaxis reduced hospital admissions due to this complication by about one-quarter, according to results of a retrospective cohort study.
“Multiple studies have demonstrated the use of an oral fluoroquinolone antibiotic to prevent febrile neutropenia readmission to hospital after receiving consolidation chemotherapy,” Samantha S. F. Lee, PharmD, a clinical pharmacist at St. Michael’s Hospital in Toronto, and her colleagues wrote. “However, this is the first study to demonstrate a positive outcome specific to the AML population.”
The results support recommendations made by the Infectious Diseases Society of America and the National Comprehensive Cancer Network related to treatment of AML after receiving consolidation chemotherapy.
For the study, the investigators retrospectively reviewed the charts of consecutive patients with AML treated at London Health Sciences Centre, a tertiary academic medical center, between 2006 and 2013. They compared outcomes between 50 patients who were prescribed prophylactic levofloxacin (Levaquin) after consolidation therapy and 50 patients who were not prescribed any antibiotics.
Overall, patients given levofloxacin had a lower rate of hospital readmission due to febrile neutropenia whether given the antibiotic after the first chemotherapy consolidation cycle (42% vs. 72%, P = .002) or after all cycles (51.4% vs. 67%, P = .023).
None of the patients in the levofloxacin group developed Clostridium difficile–associated diarrhea within 30 days from discharge after receiving the first cycle of consolidation chemotherapy, compared with one patient in the group not given the antibiotic (Support Care Cancer. 2017 Nov 23. doi: 10.1007/s00520-017-3976-1).
The use of levofloxacin did not significantly impact secondary outcomes, including total days of antibiotic treatment provided to febrile neutropenic patients, days to readmission for febrile neutropenia, or the rate of positive bacterial cultures returned in febrile neutropenic patients.
It was not possible to assess differences in the rate of fluoroquinolone resistance in positive bacterial cultures because fluoroquinolone susceptibilities were infrequently reported.
“This study provides evidence of a strong association between prophylaxis with oral levofloxacin and the rate of febrile neutropenia, but further study is required to evaluate the impact of fluoroquinolone use on antibiotic resistance and [Clostridium difficile–associated diarrhea] rates in this patient setting,” the investigators wrote.
The study was limited by the small sample size, which precluded accurate ascertainment of some outcomes, including safety outcomes, they noted. Additionally, adherence to oral therapy was unknown, and some data, such as fluoroquinolone resistance, were missing for patients admitted for febrile neutropenia to outside hospitals.
Dr. Lee reported having no relevant conflicts of interest.
FROM SUPPORTIVE CARE IN CANCER
Key clinical point:
Major finding: Patients given levofloxacin had lower rates of hospital readmission due to febrile neutropenia whether it was given after the first consolidation cycle (42% vs. 72%, P = .002) or after all cycles (51.4% vs. 67%, P = .023).
Data source: A single-center retrospective cohort study of 100 patients with AML, half of whom were prescribed levofloxacin after consolidation chemotherapy.
Disclosures: Dr. Lee reported having no relevant conflicts of interest.
Cancer patients with TKI-induced hypothyroidism had better survival rates
VICTORIA, B.C. – When it comes to the adverse effects of tyrosine kinase inhibitors (TKIs), hypothyroidism appears to have a bright side, according to a retrospective cohort study among patients with nonthyroid cancers.
While taking one of these targeted agents, roughly a quarter of patients became overtly hypothyroid, an adverse effect that appears to be due in part to immune destruction. Risk was higher for women and earlier in therapy.
Relative to counterparts who remained euthyroid, overtly hypothyroid patients were 44% less likely to die after other factors were taken into account.
Hypothyroidism may reflect changes in immune activation, Dr. Angell proposed. “Additional studies may be helpful, both prospectively looking at the clinical importance of this finding [of survival benefit], and also potentially mechanistically, to understand the relationship between hypothyroidism and survival in these patients.”
“This is an innovative study that looked at an interesting clinical question,” observed session cochair Angela M. Leung, MD, of the University of California, Los Angeles, and an endocrinologist at both UCLA and the VA Greater Los Angeles Healthcare System.
Thyroid dysfunction is a well-known, common side effect of TKI therapy, Dr. Angell noted. “The possible mechanisms that have been suggested for this are direct toxicity on the thyroid gland, destructive thyroiditis, increased thyroid hormone clearance, and vascular endothelial growth factor (VEGF) inhibition, among others.”
Some previous research has suggested a possible survival benefit of TKI-induced hypothyroidism. But “there are limitations in our understanding of hypothyroidism in this setting, including the timing of onset, what risk factors there may be, and the effect of additional clinical variables on the survival effect seen,” Dr. Angell pointed out.
He and his coinvestigators studied 538 adult patients with nonthyroid cancers (mostly stage III or IV) who received a first TKI during 2000-2013 and were followed up through 2017. They excluded those who had preexisting thyroid disease or were on thyroid-related medications.
During TKI therapy, 26.7% of patients developed overt hypothyroidism, and another 13.2% developed subclinical hypothyroidism.
“For a given drug, patients were less likely to develop hypothyroidism when they were given it subsequent to another TKI, as opposed to it being the initial TKI,” Dr. Angell reported. But median time to onset of hypothyroidism was about 2.5 months, regardless.
Cumulative months of all TKI exposure during cancer treatment were not significantly associated with development of hypothyroidism.
In a multivariate analysis, patients were significantly more likely to develop hypothyroidism if they were female (odds ratio, 1.99) and significantly less likely if they had a longer total time on treatment (OR, 0.98) or received a non-TKI VEGF inhibitor (OR, 0.43). Age, race, and cumulative TKI exposure did not influence the outcome.
In a second multivariate analysis, patients’ risk of death was significantly lower if they developed overt hypothyroidism (hazard ratio, 0.56; P less than .0001), but not if they developed subclinical hypothyroidism (HR, 0.79; P = .1655).
Treatment of hypothyroidism did not appear to influence survival, according to Dr. Angell. However, “there wasn’t a specific decision on who was treated, how they were treated, [or] when they were treated,” he said. “So, it is difficult within this cohort to look specifically at which cutoff would be ideal” for initiating treatment.
Similarly, thyroid function testing was not standardized in this retrospectively identified cohort, so it was not possible to determine how long patients were hypothyroid and whether that had an impact, according to Dr. Angell.
Dr. Angell had no relevant conflicts of interest.
VICTORIA, B.C. – When it comes to the adverse effects of tyrosine kinase inhibitors (TKIs), hypothyroidism appears to have a bright side, according to a retrospective cohort study among patients with nonthyroid cancers.
While taking one of these targeted agents, roughly a quarter of patients became overtly hypothyroid, an adverse effect that appears to be due in part to immune destruction. Risk was higher for women and earlier in therapy.
Relative to counterparts who remained euthyroid, overtly hypothyroid patients were 44% less likely to die after other factors were taken into account.
Hypothyroidism may reflect changes in immune activation, Dr. Angell proposed. “Additional studies may be helpful, both prospectively looking at the clinical importance of this finding [of survival benefit], and also potentially mechanistically, to understand the relationship between hypothyroidism and survival in these patients.”
“This is an innovative study that looked at an interesting clinical question,” observed session cochair Angela M. Leung, MD, of the University of California, Los Angeles, and an endocrinologist at both UCLA and the VA Greater Los Angeles Healthcare System.
Thyroid dysfunction is a well-known, common side effect of TKI therapy, Dr. Angell noted. “The possible mechanisms that have been suggested for this are direct toxicity on the thyroid gland, destructive thyroiditis, increased thyroid hormone clearance, and vascular endothelial growth factor (VEGF) inhibition, among others.”
Some previous research has suggested a possible survival benefit of TKI-induced hypothyroidism. But “there are limitations in our understanding of hypothyroidism in this setting, including the timing of onset, what risk factors there may be, and the effect of additional clinical variables on the survival effect seen,” Dr. Angell pointed out.
He and his coinvestigators studied 538 adult patients with nonthyroid cancers (mostly stage III or IV) who received a first TKI during 2000-2013 and were followed up through 2017. They excluded those who had preexisting thyroid disease or were on thyroid-related medications.
During TKI therapy, 26.7% of patients developed overt hypothyroidism, and another 13.2% developed subclinical hypothyroidism.
“For a given drug, patients were less likely to develop hypothyroidism when they were given it subsequent to another TKI, as opposed to it being the initial TKI,” Dr. Angell reported. But median time to onset of hypothyroidism was about 2.5 months, regardless.
Cumulative months of all TKI exposure during cancer treatment were not significantly associated with development of hypothyroidism.
In a multivariate analysis, patients were significantly more likely to develop hypothyroidism if they were female (odds ratio, 1.99) and significantly less likely if they had a longer total time on treatment (OR, 0.98) or received a non-TKI VEGF inhibitor (OR, 0.43). Age, race, and cumulative TKI exposure did not influence the outcome.
In a second multivariate analysis, patients’ risk of death was significantly lower if they developed overt hypothyroidism (hazard ratio, 0.56; P less than .0001), but not if they developed subclinical hypothyroidism (HR, 0.79; P = .1655).
Treatment of hypothyroidism did not appear to influence survival, according to Dr. Angell. However, “there wasn’t a specific decision on who was treated, how they were treated, [or] when they were treated,” he said. “So, it is difficult within this cohort to look specifically at which cutoff would be ideal” for initiating treatment.
Similarly, thyroid function testing was not standardized in this retrospectively identified cohort, so it was not possible to determine how long patients were hypothyroid and whether that had an impact, according to Dr. Angell.
Dr. Angell had no relevant conflicts of interest.
VICTORIA, B.C. – When it comes to the adverse effects of tyrosine kinase inhibitors (TKIs), hypothyroidism appears to have a bright side, according to a retrospective cohort study among patients with nonthyroid cancers.
While taking one of these targeted agents, roughly a quarter of patients became overtly hypothyroid, an adverse effect that appears to be due in part to immune destruction. Risk was higher for women and earlier in therapy.
Relative to counterparts who remained euthyroid, overtly hypothyroid patients were 44% less likely to die after other factors were taken into account.
Hypothyroidism may reflect changes in immune activation, Dr. Angell proposed. “Additional studies may be helpful, both prospectively looking at the clinical importance of this finding [of survival benefit], and also potentially mechanistically, to understand the relationship between hypothyroidism and survival in these patients.”
“This is an innovative study that looked at an interesting clinical question,” observed session cochair Angela M. Leung, MD, of the University of California, Los Angeles, and an endocrinologist at both UCLA and the VA Greater Los Angeles Healthcare System.
Thyroid dysfunction is a well-known, common side effect of TKI therapy, Dr. Angell noted. “The possible mechanisms that have been suggested for this are direct toxicity on the thyroid gland, destructive thyroiditis, increased thyroid hormone clearance, and vascular endothelial growth factor (VEGF) inhibition, among others.”
Some previous research has suggested a possible survival benefit of TKI-induced hypothyroidism. But “there are limitations in our understanding of hypothyroidism in this setting, including the timing of onset, what risk factors there may be, and the effect of additional clinical variables on the survival effect seen,” Dr. Angell pointed out.
He and his coinvestigators studied 538 adult patients with nonthyroid cancers (mostly stage III or IV) who received a first TKI during 2000-2013 and were followed up through 2017. They excluded those who had preexisting thyroid disease or were on thyroid-related medications.
During TKI therapy, 26.7% of patients developed overt hypothyroidism, and another 13.2% developed subclinical hypothyroidism.
“For a given drug, patients were less likely to develop hypothyroidism when they were given it subsequent to another TKI, as opposed to it being the initial TKI,” Dr. Angell reported. But median time to onset of hypothyroidism was about 2.5 months, regardless.
Cumulative months of all TKI exposure during cancer treatment were not significantly associated with development of hypothyroidism.
In a multivariate analysis, patients were significantly more likely to develop hypothyroidism if they were female (odds ratio, 1.99) and significantly less likely if they had a longer total time on treatment (OR, 0.98) or received a non-TKI VEGF inhibitor (OR, 0.43). Age, race, and cumulative TKI exposure did not influence the outcome.
In a second multivariate analysis, patients’ risk of death was significantly lower if they developed overt hypothyroidism (hazard ratio, 0.56; P less than .0001), but not if they developed subclinical hypothyroidism (HR, 0.79; P = .1655).
Treatment of hypothyroidism did not appear to influence survival, according to Dr. Angell. However, “there wasn’t a specific decision on who was treated, how they were treated, [or] when they were treated,” he said. “So, it is difficult within this cohort to look specifically at which cutoff would be ideal” for initiating treatment.
Similarly, thyroid function testing was not standardized in this retrospectively identified cohort, so it was not possible to determine how long patients were hypothyroid and whether that had an impact, according to Dr. Angell.
Dr. Angell had no relevant conflicts of interest.
AT ATA 2017
Key clinical point:
Major finding: Relative to peers who remained euthyroid, patients who developed overt hypothyroidism had a reduced risk of death (HR, 0.56; P less than .0001).
Data source: A retrospective cohort study of 538 adult patients with mainly advanced nonthyroid cancers treated with a tyrosine kinase inhibitor.
Disclosures: Dr. Angell had no relevant conflicts of interest.
Pediatric thyroid nodules: Experienced radiologists best ultrasound risk stratification
VICTORIA, B.C. – Ultrasound risk criteria for adults are no match for the training, skill, and gut instinct of an experienced radiologist when evaluating pediatric thyroid nodules, results of a retrospective cohort study reported at the annual meeting of the American Thyroid Association suggest.
“In 2015, the ATA commissioned a pediatric task force that developed valuable guidelines specific to our pediatric patients. These guidelines recommend performing an FNA [fine-needle aspiration biopsy] in any nodule with a concerning clinical history or a concerning ultrasound feature,” commented first author Ana L. Creo, MD, a pediatric endocrinology fellow at the Mayo Clinic in Rochester, Minn.
She and her colleagues analyzed findings from diagnostic ultrasound in 112 patients aged under 21 years who had 145 thyroid nodules that were ultimately assessed histologically or cytologically.
Results showed that the radiologists’ overall impression and the ATA risk-stratification system for adults had the same high sensitivity, picking up 9 out of 10 malignant cases, she reported. But the radiologists’ overall impression had much higher specificity, correctly classifying 8 out of 10 benign cases, versus about 5 out of 10 for the risk stratification.
“These findings may have implications in trying to avoid unnecessary FNAs, particularly in our population,” Dr. Creo summarized. “Our million dollar question is trying to get in the heads of the radiologists to figure out what really goes into that overall impression. And if we can apply a specific score to that, I think that would be most clinically useful.”
“Based upon these results, further work is needed to determine the usefulness of the adult ATA ultrasound risk stratification in children, moving towards an ultrasound-based stratification system specific to our pediatric patients,” she concluded.
One session cochair, Catherine A. Dinauer, MD, a pediatric endocrinologist and clinician at the Yale Pediatric Thyroid Center, New Haven, Conn., commented, “It seems as though we’re pretty good at picking up which nodules are malignant, but I still feel like so many of the nodules that are benign are suspicious by ultrasound. Trying to tease out what is it about those benign ones may allow us to figure out in which ones we could avoid biopsy. That’s where we see we are not that good at it.”
Nodule attributes that might help in this regard include subtypes of microcalcifications, irregular margins, and position of the nodule in the gland relative to the skin, she proposed.
The other session cochair, Yaron Tomer, MD, chair of the department of medicine and the Anita and Jack Saltz Chair in Diabetes Research at the Montefiore Medical Center, New York, stressed knowing one’s radiologist and questioned the generalizability of the findings.
“You have to know your own radiologist well and how well you can trust them. Probably, the investigators chose some of the top radiologists in their institution and maybe even in the nation, so we have to be careful as to whether this applies to places that don’t have access to such great radiologists,” he commented. “But I think even if the guidelines are not perfect, they are the best we have right now.”
Study details
The investigators studied pediatric patients (mean age, 15.5 years) with thyroid nodules who underwent initial ultrasound at the Mayo Clinic during 1996-2015, had at least a year of follow-up, and for whom histology or cytology results were available. Those with a known genetic tumor syndrome or a history of radiation exposure were excluded.
Two blinded radiologists assessed nodule ultrasound features using the Thyroid Imaging and Reporting Data System (TIRADS) (J Am Coll Radiol. 2015;12[12 Pt A]:1272-9) and then rendered their overall impression: malignant, indeterminate, or benign.
Next, an independent reviewer assigned each nodule an ATA adult risk category (Thyroid. 2016;26:1-133): high, intermediate, low, or very low suspicion.
Finally, both measures were compared against the reference standard of the nodule’s histology or cytology results.
Ultimately, 34% of the patients had malignant nodules, Dr. Creo reported. “This is likely quite a bit elevated from the true prevalence due to our intentional study design requiring follow-up, likely excluding some patients with benign nodules,” she commented.
Patients with benign and malignant nodules did not differ significantly on any of a variety of sociodemographic and clinical factors, such as family history and mode of detection.
For comparison of sensitivity, the investigators combined the ATA risk categories of high and intermediate suspicion and combined the overall radiologists’ impression of malignant and indeterminate. “We felt this best answered the practical clinical question of how many malignant nodules would be missed if FNA was not performed, assuming FNA would typically be performed if the ATA risk stratification was high or intermediate or if the radiologist’s overall impression was malignant or indeterminate,” Dr. Creo explained.
Results here showed that the ATA risk stratification and the radiologists’ overall impression had the same high sensitivity of 90%.
For comparison of specificity, the investigators compared the ATA risk category of high suspicion with the radiologists’ overall impression of malignant.
Results showed that the overall impression had specificity of 80%, whereas the risk category had a specificity of only about 52%. Findings were similar when analyses instead used ATA high suspicion and intermediate suspicion combined.
“The key ultrasound characteristics that drove the diagnosis included having a solid component, calcifications, irregular margins, and hypoechogenicity – all similar to those seen in pediatric studies and similar to those in adult studies as well,” Dr. Creo noted.
Compared with benign nodules, malignant nodules significantly more often had a greater than 75% solid component (84% vs. 64%; P = .01), contained calcifications (60% vs. 18%; P less than .0001), had irregular margins (70% vs. 46%; P = .0073), and were hypoechogenic (74% vs. 51%; P = .0073). Notably, size and presence of halo did not differ significantly.
“Our study adds to previous work in that it had a relatively large pediatric sample size, used strict inclusion criteria with at least a year of follow-up to increase the validity of the diagnosis, and had precise definitions of the ultrasound features,” concluded Dr. Creo, who disclosed that she had no relevant conflicts of interest.
At the same time, the study had limitations, such as its use of a referral population, likely loss to follow-up of some patients with benign nodules, and possible clustering effect. “Lastly, we had the benefit of extremely experienced pediatric radiologists, and their overall diagnostic accuracy may not universally apply across all radiologists,” she said.
VICTORIA, B.C. – Ultrasound risk criteria for adults are no match for the training, skill, and gut instinct of an experienced radiologist when evaluating pediatric thyroid nodules, results of a retrospective cohort study reported at the annual meeting of the American Thyroid Association suggest.
“In 2015, the ATA commissioned a pediatric task force that developed valuable guidelines specific to our pediatric patients. These guidelines recommend performing an FNA [fine-needle aspiration biopsy] in any nodule with a concerning clinical history or a concerning ultrasound feature,” commented first author Ana L. Creo, MD, a pediatric endocrinology fellow at the Mayo Clinic in Rochester, Minn.
She and her colleagues analyzed findings from diagnostic ultrasound in 112 patients aged under 21 years who had 145 thyroid nodules that were ultimately assessed histologically or cytologically.
Results showed that the radiologists’ overall impression and the ATA risk-stratification system for adults had the same high sensitivity, picking up 9 out of 10 malignant cases, she reported. But the radiologists’ overall impression had much higher specificity, correctly classifying 8 out of 10 benign cases, versus about 5 out of 10 for the risk stratification.
“These findings may have implications in trying to avoid unnecessary FNAs, particularly in our population,” Dr. Creo summarized. “Our million dollar question is trying to get in the heads of the radiologists to figure out what really goes into that overall impression. And if we can apply a specific score to that, I think that would be most clinically useful.”
“Based upon these results, further work is needed to determine the usefulness of the adult ATA ultrasound risk stratification in children, moving towards an ultrasound-based stratification system specific to our pediatric patients,” she concluded.
One session cochair, Catherine A. Dinauer, MD, a pediatric endocrinologist and clinician at the Yale Pediatric Thyroid Center, New Haven, Conn., commented, “It seems as though we’re pretty good at picking up which nodules are malignant, but I still feel like so many of the nodules that are benign are suspicious by ultrasound. Trying to tease out what is it about those benign ones may allow us to figure out in which ones we could avoid biopsy. That’s where we see we are not that good at it.”
Nodule attributes that might help in this regard include subtypes of microcalcifications, irregular margins, and position of the nodule in the gland relative to the skin, she proposed.
The other session cochair, Yaron Tomer, MD, chair of the department of medicine and the Anita and Jack Saltz Chair in Diabetes Research at the Montefiore Medical Center, New York, stressed knowing one’s radiologist and questioned the generalizability of the findings.
“You have to know your own radiologist well and how well you can trust them. Probably, the investigators chose some of the top radiologists in their institution and maybe even in the nation, so we have to be careful as to whether this applies to places that don’t have access to such great radiologists,” he commented. “But I think even if the guidelines are not perfect, they are the best we have right now.”
Study details
The investigators studied pediatric patients (mean age, 15.5 years) with thyroid nodules who underwent initial ultrasound at the Mayo Clinic during 1996-2015, had at least a year of follow-up, and for whom histology or cytology results were available. Those with a known genetic tumor syndrome or a history of radiation exposure were excluded.
Two blinded radiologists assessed nodule ultrasound features using the Thyroid Imaging and Reporting Data System (TIRADS) (J Am Coll Radiol. 2015;12[12 Pt A]:1272-9) and then rendered their overall impression: malignant, indeterminate, or benign.
Next, an independent reviewer assigned each nodule an ATA adult risk category (Thyroid. 2016;26:1-133): high, intermediate, low, or very low suspicion.
Finally, both measures were compared against the reference standard of the nodule’s histology or cytology results.
Ultimately, 34% of the patients had malignant nodules, Dr. Creo reported. “This is likely quite a bit elevated from the true prevalence due to our intentional study design requiring follow-up, likely excluding some patients with benign nodules,” she commented.
Patients with benign and malignant nodules did not differ significantly on any of a variety of sociodemographic and clinical factors, such as family history and mode of detection.
For comparison of sensitivity, the investigators combined the ATA risk categories of high and intermediate suspicion and combined the overall radiologists’ impression of malignant and indeterminate. “We felt this best answered the practical clinical question of how many malignant nodules would be missed if FNA was not performed, assuming FNA would typically be performed if the ATA risk stratification was high or intermediate or if the radiologist’s overall impression was malignant or indeterminate,” Dr. Creo explained.
Results here showed that the ATA risk stratification and the radiologists’ overall impression had the same high sensitivity of 90%.
For comparison of specificity, the investigators compared the ATA risk category of high suspicion with the radiologists’ overall impression of malignant.
Results showed that the overall impression had specificity of 80%, whereas the risk category had a specificity of only about 52%. Findings were similar when analyses instead used ATA high suspicion and intermediate suspicion combined.
“The key ultrasound characteristics that drove the diagnosis included having a solid component, calcifications, irregular margins, and hypoechogenicity – all similar to those seen in pediatric studies and similar to those in adult studies as well,” Dr. Creo noted.
Compared with benign nodules, malignant nodules significantly more often had a greater than 75% solid component (84% vs. 64%; P = .01), contained calcifications (60% vs. 18%; P less than .0001), had irregular margins (70% vs. 46%; P = .0073), and were hypoechogenic (74% vs. 51%; P = .0073). Notably, size and presence of halo did not differ significantly.
“Our study adds to previous work in that it had a relatively large pediatric sample size, used strict inclusion criteria with at least a year of follow-up to increase the validity of the diagnosis, and had precise definitions of the ultrasound features,” concluded Dr. Creo, who disclosed that she had no relevant conflicts of interest.
At the same time, the study had limitations, such as its use of a referral population, likely loss to follow-up of some patients with benign nodules, and possible clustering effect. “Lastly, we had the benefit of extremely experienced pediatric radiologists, and their overall diagnostic accuracy may not universally apply across all radiologists,” she said.
VICTORIA, B.C. – Ultrasound risk criteria for adults are no match for the training, skill, and gut instinct of an experienced radiologist when evaluating pediatric thyroid nodules, results of a retrospective cohort study reported at the annual meeting of the American Thyroid Association suggest.
“In 2015, the ATA commissioned a pediatric task force that developed valuable guidelines specific to our pediatric patients. These guidelines recommend performing an FNA [fine-needle aspiration biopsy] in any nodule with a concerning clinical history or a concerning ultrasound feature,” commented first author Ana L. Creo, MD, a pediatric endocrinology fellow at the Mayo Clinic in Rochester, Minn.
She and her colleagues analyzed findings from diagnostic ultrasound in 112 patients aged under 21 years who had 145 thyroid nodules that were ultimately assessed histologically or cytologically.
Results showed that the radiologists’ overall impression and the ATA risk-stratification system for adults had the same high sensitivity, picking up 9 out of 10 malignant cases, she reported. But the radiologists’ overall impression had much higher specificity, correctly classifying 8 out of 10 benign cases, versus about 5 out of 10 for the risk stratification.
“These findings may have implications in trying to avoid unnecessary FNAs, particularly in our population,” Dr. Creo summarized. “Our million dollar question is trying to get in the heads of the radiologists to figure out what really goes into that overall impression. And if we can apply a specific score to that, I think that would be most clinically useful.”
“Based upon these results, further work is needed to determine the usefulness of the adult ATA ultrasound risk stratification in children, moving towards an ultrasound-based stratification system specific to our pediatric patients,” she concluded.
One session cochair, Catherine A. Dinauer, MD, a pediatric endocrinologist and clinician at the Yale Pediatric Thyroid Center, New Haven, Conn., commented, “It seems as though we’re pretty good at picking up which nodules are malignant, but I still feel like so many of the nodules that are benign are suspicious by ultrasound. Trying to tease out what is it about those benign ones may allow us to figure out in which ones we could avoid biopsy. That’s where we see we are not that good at it.”
Nodule attributes that might help in this regard include subtypes of microcalcifications, irregular margins, and position of the nodule in the gland relative to the skin, she proposed.
The other session cochair, Yaron Tomer, MD, chair of the department of medicine and the Anita and Jack Saltz Chair in Diabetes Research at the Montefiore Medical Center, New York, stressed knowing one’s radiologist and questioned the generalizability of the findings.
“You have to know your own radiologist well and how well you can trust them. Probably, the investigators chose some of the top radiologists in their institution and maybe even in the nation, so we have to be careful as to whether this applies to places that don’t have access to such great radiologists,” he commented. “But I think even if the guidelines are not perfect, they are the best we have right now.”
Study details
The investigators studied pediatric patients (mean age, 15.5 years) with thyroid nodules who underwent initial ultrasound at the Mayo Clinic during 1996-2015, had at least a year of follow-up, and for whom histology or cytology results were available. Those with a known genetic tumor syndrome or a history of radiation exposure were excluded.
Two blinded radiologists assessed nodule ultrasound features using the Thyroid Imaging and Reporting Data System (TIRADS) (J Am Coll Radiol. 2015;12[12 Pt A]:1272-9) and then rendered their overall impression: malignant, indeterminate, or benign.
Next, an independent reviewer assigned each nodule an ATA adult risk category (Thyroid. 2016;26:1-133): high, intermediate, low, or very low suspicion.
Finally, both measures were compared against the reference standard of the nodule’s histology or cytology results.
Ultimately, 34% of the patients had malignant nodules, Dr. Creo reported. “This is likely quite a bit elevated from the true prevalence due to our intentional study design requiring follow-up, likely excluding some patients with benign nodules,” she commented.
Patients with benign and malignant nodules did not differ significantly on any of a variety of sociodemographic and clinical factors, such as family history and mode of detection.
For comparison of sensitivity, the investigators combined the ATA risk categories of high and intermediate suspicion and combined the overall radiologists’ impression of malignant and indeterminate. “We felt this best answered the practical clinical question of how many malignant nodules would be missed if FNA was not performed, assuming FNA would typically be performed if the ATA risk stratification was high or intermediate or if the radiologist’s overall impression was malignant or indeterminate,” Dr. Creo explained.
Results here showed that the ATA risk stratification and the radiologists’ overall impression had the same high sensitivity of 90%.
For comparison of specificity, the investigators compared the ATA risk category of high suspicion with the radiologists’ overall impression of malignant.
Results showed that the overall impression had specificity of 80%, whereas the risk category had a specificity of only about 52%. Findings were similar when analyses instead used ATA high suspicion and intermediate suspicion combined.
“The key ultrasound characteristics that drove the diagnosis included having a solid component, calcifications, irregular margins, and hypoechogenicity – all similar to those seen in pediatric studies and similar to those in adult studies as well,” Dr. Creo noted.
Compared with benign nodules, malignant nodules significantly more often had a greater than 75% solid component (84% vs. 64%; P = .01), contained calcifications (60% vs. 18%; P less than .0001), had irregular margins (70% vs. 46%; P = .0073), and were hypoechogenic (74% vs. 51%; P = .0073). Notably, size and presence of halo did not differ significantly.
“Our study adds to previous work in that it had a relatively large pediatric sample size, used strict inclusion criteria with at least a year of follow-up to increase the validity of the diagnosis, and had precise definitions of the ultrasound features,” concluded Dr. Creo, who disclosed that she had no relevant conflicts of interest.
At the same time, the study had limitations, such as its use of a referral population, likely loss to follow-up of some patients with benign nodules, and possible clustering effect. “Lastly, we had the benefit of extremely experienced pediatric radiologists, and their overall diagnostic accuracy may not universally apply across all radiologists,” she said.
AT ATA 2017
Key clinical point:
Major finding: Radiologists’ overall impression and ATA risk stratification had the same good sensitivity (90% for each), but the former had higher specificity (80% vs. 52%).
Data source: A retrospective cohort study of 112 patients younger than 21 who had 145 thyroid nodules.
Disclosures: Dr. Creo disclosed that she had no relevant conflicts of interest.
Generic, brand-name levothyroxine have similar cardiovascular outcomes
VICTORIA, B.C. – Hypothyroid patients have similar cardiovascular outcomes in the shorter term whether they take generic or brand-name levothyroxine, results of a retrospective propensity-matched cohort study reported at the annual meeting of the American Thyroid Association suggest.
Investigators led by Robert Smallridge, MD, an endocrinologist at the Mayo Clinic, in Jacksonville, Fla., used a large administrative database to study nearly 88,000 treatment-naive hypothyroid patients (most having benign thyroid disease) who started levothyroxine.
However, monthly total medication costs with the brand-name medication were more than twice those with the generic.
“I don’t think we are ready yet to say everybody ought to be on generic,” Dr. Smallridge said in an interview, citing the limited treatment duration captured in the study because patients switched medications or changed insurers. “But I think, at least in the short term, it’s giving us some data that we can build upon.”
He and his coinvestigators plan additional analyses looking at longer-term users, other types of thyroid hormone preparations, and the very small group of patients who had thyroid cancer.
“I primarily take care of cancer patients, and we purposely push these patients to slightly lower [thyroid-stimulating hormone levels] in general, which presumably is going to increase your risk of atrial fibrillation and could affect these events,” he said. “The numbers are somewhat smaller, clearly, but I’d like to see that explored also, to see if there is a difference between brand and generics in that subset who are probably getting a little bit more thyroid medication.”
Both hypothyroidism and its overtreatment with thyroid hormone therapy can increase cardiovascular risk, Dr. Smallridge noted.
For the study, the investigators analyzed data from a large administrative claims database (OptumLabs Data Warehouse) for the years 2006-2014. Patients having any prior use of any thyroid hormone preparation, amiodarone, or lithium were excluded. And patients were censored if they left the insurance plan, stopped treatment, or switched medication category.
The investigators identified 201,056 hypothyroid patients who started some type of thyroid hormone therapy. The majority (70.8%) started generic levothyroxine, and 22.1% started brand-name levothyroxine (Synthroid, Levoxyl, Tirosint, Unithroid). The small remaining group started another thyroid extract, triiodothyronine (T3), or a compounded preparation.
Primary care physicians were the main identifiable prescribers (60.3%), followed by endocrinologists (10.8%). “Endocrinologists tended to prescribe brand significantly more than the primary care physicians,” Dr. Smallridge said.
The investigators used propensity matching on a variety of factors (age, sex, race, census region, Charlson comorbidity index, year of index prescription, and a dozen baseline comorbidities) to compare patients starting brand-name versus generic levothyroxine. Outcomes were assessed during a median follow-up of 1 year (range, 0-9.3 years).
Event rates per 1,000 patient-years with branded versus generic levothyroxine were similar for atrial fibrillation (2.19 vs. 1.82; hazard ratio, 1.22, P = .19), myocardial infarction (1.83 vs. 2.12; HR, 0.86, P = .35), and congestive heart failure (2.00 vs. 2.27; HR, 0.88, P = .41). There was a borderline-significant difference on hospitalization for stroke, with marginally lower risk with brand-name levothyroxine (2.38 vs. 3.10; HR, 0.77; P = .05).
Findings were essentially the same in age-stratified analyses, splitting patients into subgroups younger and older than age 65.
When average 30-day costs were compared for users of branded versus generic levothyroxine, total cost for the branded drug was more than twice as high ($18.47 vs. $8.18).
“Thyroid preparations have been the most prescribed drug in the United States for several recent years. In the neighborhood of 25 million different patients a year take thyroid medications,” Dr. Smallridge said. “In terms of the dollars spent, it’s considerably less than some of the other drugs out there. But because of sheer numbers of patients, in terms of impact on health care dollars, it’s still a significant amount of money. And this is a lifelong treatment – once you go on thyroid hormones, you’re on them for life.”
The study had several strengths. “This is a very large, diverse, real-world population across the entire country with a wide range of ages,” Dr. Smallridge explained. “We got pharmacy claims documenting that they were continuing to get the refills, although we didn’t do pill counts, so we don’t know whether they were taking the medication. And a really important thing was the propensity score matching.”
At the same time, limitations included possible variations in coding and billing, and some residual confounding. “Key issues are that we need more data on longer-term follow-up, and we didn’t have lab values,” he added.
Dr. Smallridge reported that he had no relevant conflicts of interest.
VICTORIA, B.C. – Hypothyroid patients have similar cardiovascular outcomes in the shorter term whether they take generic or brand-name levothyroxine, results of a retrospective propensity-matched cohort study reported at the annual meeting of the American Thyroid Association suggest.
Investigators led by Robert Smallridge, MD, an endocrinologist at the Mayo Clinic, in Jacksonville, Fla., used a large administrative database to study nearly 88,000 treatment-naive hypothyroid patients (most having benign thyroid disease) who started levothyroxine.
However, monthly total medication costs with the brand-name medication were more than twice those with the generic.
“I don’t think we are ready yet to say everybody ought to be on generic,” Dr. Smallridge said in an interview, citing the limited treatment duration captured in the study because patients switched medications or changed insurers. “But I think, at least in the short term, it’s giving us some data that we can build upon.”
He and his coinvestigators plan additional analyses looking at longer-term users, other types of thyroid hormone preparations, and the very small group of patients who had thyroid cancer.
“I primarily take care of cancer patients, and we purposely push these patients to slightly lower [thyroid-stimulating hormone levels] in general, which presumably is going to increase your risk of atrial fibrillation and could affect these events,” he said. “The numbers are somewhat smaller, clearly, but I’d like to see that explored also, to see if there is a difference between brand and generics in that subset who are probably getting a little bit more thyroid medication.”
Both hypothyroidism and its overtreatment with thyroid hormone therapy can increase cardiovascular risk, Dr. Smallridge noted.
For the study, the investigators analyzed data from a large administrative claims database (OptumLabs Data Warehouse) for the years 2006-2014. Patients having any prior use of any thyroid hormone preparation, amiodarone, or lithium were excluded. And patients were censored if they left the insurance plan, stopped treatment, or switched medication category.
The investigators identified 201,056 hypothyroid patients who started some type of thyroid hormone therapy. The majority (70.8%) started generic levothyroxine, and 22.1% started brand-name levothyroxine (Synthroid, Levoxyl, Tirosint, Unithroid). The small remaining group started another thyroid extract, triiodothyronine (T3), or a compounded preparation.
Primary care physicians were the main identifiable prescribers (60.3%), followed by endocrinologists (10.8%). “Endocrinologists tended to prescribe brand significantly more than the primary care physicians,” Dr. Smallridge said.
The investigators used propensity matching on a variety of factors (age, sex, race, census region, Charlson comorbidity index, year of index prescription, and a dozen baseline comorbidities) to compare patients starting brand-name versus generic levothyroxine. Outcomes were assessed during a median follow-up of 1 year (range, 0-9.3 years).
Event rates per 1,000 patient-years with branded versus generic levothyroxine were similar for atrial fibrillation (2.19 vs. 1.82; hazard ratio, 1.22, P = .19), myocardial infarction (1.83 vs. 2.12; HR, 0.86, P = .35), and congestive heart failure (2.00 vs. 2.27; HR, 0.88, P = .41). There was a borderline-significant difference on hospitalization for stroke, with marginally lower risk with brand-name levothyroxine (2.38 vs. 3.10; HR, 0.77; P = .05).
Findings were essentially the same in age-stratified analyses, splitting patients into subgroups younger and older than age 65.
When average 30-day costs were compared for users of branded versus generic levothyroxine, total cost for the branded drug was more than twice as high ($18.47 vs. $8.18).
“Thyroid preparations have been the most prescribed drug in the United States for several recent years. In the neighborhood of 25 million different patients a year take thyroid medications,” Dr. Smallridge said. “In terms of the dollars spent, it’s considerably less than some of the other drugs out there. But because of sheer numbers of patients, in terms of impact on health care dollars, it’s still a significant amount of money. And this is a lifelong treatment – once you go on thyroid hormones, you’re on them for life.”
The study had several strengths. “This is a very large, diverse, real-world population across the entire country with a wide range of ages,” Dr. Smallridge explained. “We got pharmacy claims documenting that they were continuing to get the refills, although we didn’t do pill counts, so we don’t know whether they were taking the medication. And a really important thing was the propensity score matching.”
At the same time, limitations included possible variations in coding and billing, and some residual confounding. “Key issues are that we need more data on longer-term follow-up, and we didn’t have lab values,” he added.
Dr. Smallridge reported that he had no relevant conflicts of interest.
VICTORIA, B.C. – Hypothyroid patients have similar cardiovascular outcomes in the shorter term whether they take generic or brand-name levothyroxine, results of a retrospective propensity-matched cohort study reported at the annual meeting of the American Thyroid Association suggest.
Investigators led by Robert Smallridge, MD, an endocrinologist at the Mayo Clinic, in Jacksonville, Fla., used a large administrative database to study nearly 88,000 treatment-naive hypothyroid patients (most having benign thyroid disease) who started levothyroxine.
However, monthly total medication costs with the brand-name medication were more than twice those with the generic.
“I don’t think we are ready yet to say everybody ought to be on generic,” Dr. Smallridge said in an interview, citing the limited treatment duration captured in the study because patients switched medications or changed insurers. “But I think, at least in the short term, it’s giving us some data that we can build upon.”
He and his coinvestigators plan additional analyses looking at longer-term users, other types of thyroid hormone preparations, and the very small group of patients who had thyroid cancer.
“I primarily take care of cancer patients, and we purposely push these patients to slightly lower [thyroid-stimulating hormone levels] in general, which presumably is going to increase your risk of atrial fibrillation and could affect these events,” he said. “The numbers are somewhat smaller, clearly, but I’d like to see that explored also, to see if there is a difference between brand and generics in that subset who are probably getting a little bit more thyroid medication.”
Both hypothyroidism and its overtreatment with thyroid hormone therapy can increase cardiovascular risk, Dr. Smallridge noted.
For the study, the investigators analyzed data from a large administrative claims database (OptumLabs Data Warehouse) for the years 2006-2014. Patients having any prior use of any thyroid hormone preparation, amiodarone, or lithium were excluded. And patients were censored if they left the insurance plan, stopped treatment, or switched medication category.
The investigators identified 201,056 hypothyroid patients who started some type of thyroid hormone therapy. The majority (70.8%) started generic levothyroxine, and 22.1% started brand-name levothyroxine (Synthroid, Levoxyl, Tirosint, Unithroid). The small remaining group started another thyroid extract, triiodothyronine (T3), or a compounded preparation.
Primary care physicians were the main identifiable prescribers (60.3%), followed by endocrinologists (10.8%). “Endocrinologists tended to prescribe brand significantly more than the primary care physicians,” Dr. Smallridge said.
The investigators used propensity matching on a variety of factors (age, sex, race, census region, Charlson comorbidity index, year of index prescription, and a dozen baseline comorbidities) to compare patients starting brand-name versus generic levothyroxine. Outcomes were assessed during a median follow-up of 1 year (range, 0-9.3 years).
Event rates per 1,000 patient-years with branded versus generic levothyroxine were similar for atrial fibrillation (2.19 vs. 1.82; hazard ratio, 1.22, P = .19), myocardial infarction (1.83 vs. 2.12; HR, 0.86, P = .35), and congestive heart failure (2.00 vs. 2.27; HR, 0.88, P = .41). There was a borderline-significant difference on hospitalization for stroke, with marginally lower risk with brand-name levothyroxine (2.38 vs. 3.10; HR, 0.77; P = .05).
Findings were essentially the same in age-stratified analyses, splitting patients into subgroups younger and older than age 65.
When average 30-day costs were compared for users of branded versus generic levothyroxine, total cost for the branded drug was more than twice as high ($18.47 vs. $8.18).
“Thyroid preparations have been the most prescribed drug in the United States for several recent years. In the neighborhood of 25 million different patients a year take thyroid medications,” Dr. Smallridge said. “In terms of the dollars spent, it’s considerably less than some of the other drugs out there. But because of sheer numbers of patients, in terms of impact on health care dollars, it’s still a significant amount of money. And this is a lifelong treatment – once you go on thyroid hormones, you’re on them for life.”
The study had several strengths. “This is a very large, diverse, real-world population across the entire country with a wide range of ages,” Dr. Smallridge explained. “We got pharmacy claims documenting that they were continuing to get the refills, although we didn’t do pill counts, so we don’t know whether they were taking the medication. And a really important thing was the propensity score matching.”
At the same time, limitations included possible variations in coding and billing, and some residual confounding. “Key issues are that we need more data on longer-term follow-up, and we didn’t have lab values,” he added.
Dr. Smallridge reported that he had no relevant conflicts of interest.
AT ATA 2017
Key clinical point:
Major finding: Patients taking brand-name versus generic levothyroxine had similar risks of hospitalization for atrial fibrillation (HR, 1.22; P = .19), myocardial infarction (0.86; P = .35), congestive heart failure (0.88; P = .41), and stroke (0.77; P = .05).
Data source: A retrospective cohort study of 87,902 propensity-matched hypothyroid patients starting generic or brand-name levothyroxine.
Disclosures: Dr. Smallridge reported that he had no relevant conflicts of interest.
Hypothyroidism carries higher surgical risk not captured by calculator
VICTORIA, B.C. – Even with contemporary anesthesia and surgical techniques, patients who are overtly hypothyroid at the time of major surgery have a rockier course, suggests a retrospective cohort study of 58 patients in a poster presentation at the annual meeting of the American Thyroid Association.
Actual length of stay for hypothyroid patients was twice that predicted by a commonly used risk calculator, whereas actual and predicted stays aligned well for euthyroid patients. The hypothyroid group had more cases of postoperative atrial fibrillation, ileus, reintubation, and death, although numbers were too small for statistical comparison.
“This will have an impact on how we look at patients, especially from a hospital standpoint and management. That’s quite a bit longer stay and quite a bit more cost. And the longer you stay, the more complications you have, too, so it could be riskier for the patient as well,” said first author Raquel Villavicencio, MD, a fellow at Indiana University at the time of the study, and now a clinical endocrinologist at Community Hospital in Indianapolis.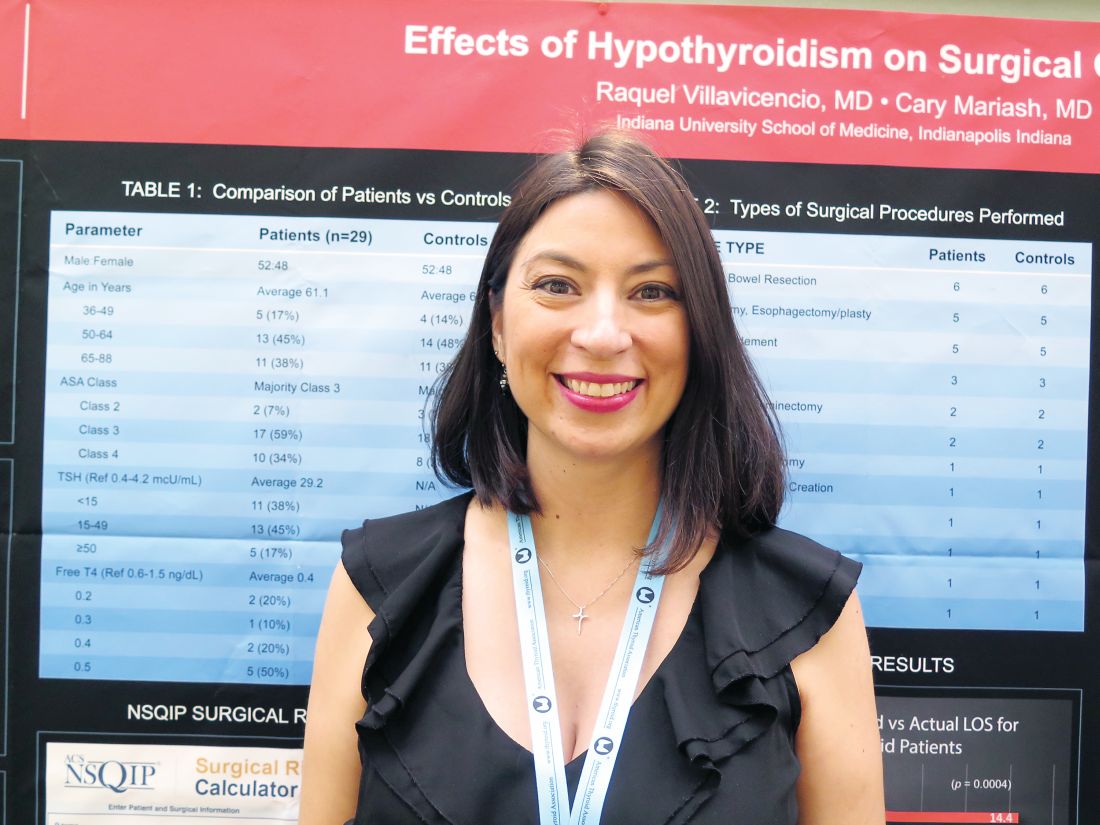
“Although we don’t consider hypothyroidism an absolute contraindication to surgery, especially if it’s necessary surgery, certainly anybody who is having elective surgery should have it postponed, in our opinion, until they are rendered euthyroid,” she said. “More studies are needed to look at this a little bit closer.”
Explaining the study’s rationale, Dr. Villavicencio noted, “This was a question that came up maybe three or four times a year, where we would get a hypothyroid patient and had to decide whether or not to clear them for surgery.”
Previous studies conducted at large institutions, the Mayo Clinic and Massachusetts General Hospital, had conflicting findings and were done about 30 years ago, she said. Anesthesia and surgical care have improved substantially since then, leading the investigators to hypothesize that hypothyroidism would not carry higher surgical risk today.
Dr. Villavicencio and her coinvestigator, Cary Mariash, MD, used their institutional database to identify 29 adult patients with a thyroid-stimulating hormone (TSH) level of greater than 10 mcU/mL alone or with a TSH level exceeding the upper limit of normal along with a free thyroxine (T4) level of less than 0.6 ng/dL who underwent surgery during 2010-2015. They matched each patient on age, sex, and surgical procedure with a control euthyroid patient.
The mean TSH level in the hypothyroid group was 29.2 mcU/mL. The majority of patients in each group – 59% of the hypothyroid group and 62% of the euthyroid group – had an American Surgical Association class of 3, denoting that this was a fairly sick population. The groups were generally similar on rates of comorbidity, except that the euthyroid patients had a slightly higher prevalence of obstructive sleep apnea.
In both groups, the majority of procedures were laparotomy and/or bowel resection; pharyngolaryngectomy and esophagectomy/esophagoplasty; and wound or bone debridement.
Main results showed that in the hypothyroid group, hospital length of stay predicted with the American College of Surgeons National Surgical Quality Improvement Program surgical risk calculator was 6.9 days, but actual length of stay was 14.4 days (P = .0004). In contrast, in the euthyroid group, predicted length of stay was a similar at 7.1 days, and actual length of stay was statistically indistinguishable at 9.2 days (P = .1).
“Hypothyroidism is not taken into account with this calculator,” Dr. Villavicencio noted, adding that she was unaware of any surgical calculators that do.
One patient in the hypothyroid group died, compared with none in the euthyroid group. In terms of postoperative cardiac complications, two patients in the hypothyroid group experienced atrial fibrillation, and there was one case of pulseless electrical–activity arrest in each group.
The groups did not differ on incidence of hypothermia, bradycardia, hyponatremia, time to extubation, and hypotension. However, mean arterial pressure tended to be lower in the hypothyroid group (51 mm Hg) than in the euthyroid group (56 mm Hg), and the former more often needed vasopressors. Furthermore, postoperative ileus and reintubation were more common in the hypothyroid group.
“I think that there are kind of a lot of little things that add up to explain [the longer stay],” said Dr. Villavicencio, who disclosed that she had no relevant conflicts of interest.
VICTORIA, B.C. – Even with contemporary anesthesia and surgical techniques, patients who are overtly hypothyroid at the time of major surgery have a rockier course, suggests a retrospective cohort study of 58 patients in a poster presentation at the annual meeting of the American Thyroid Association.
Actual length of stay for hypothyroid patients was twice that predicted by a commonly used risk calculator, whereas actual and predicted stays aligned well for euthyroid patients. The hypothyroid group had more cases of postoperative atrial fibrillation, ileus, reintubation, and death, although numbers were too small for statistical comparison.
“This will have an impact on how we look at patients, especially from a hospital standpoint and management. That’s quite a bit longer stay and quite a bit more cost. And the longer you stay, the more complications you have, too, so it could be riskier for the patient as well,” said first author Raquel Villavicencio, MD, a fellow at Indiana University at the time of the study, and now a clinical endocrinologist at Community Hospital in Indianapolis.
“Although we don’t consider hypothyroidism an absolute contraindication to surgery, especially if it’s necessary surgery, certainly anybody who is having elective surgery should have it postponed, in our opinion, until they are rendered euthyroid,” she said. “More studies are needed to look at this a little bit closer.”
Explaining the study’s rationale, Dr. Villavicencio noted, “This was a question that came up maybe three or four times a year, where we would get a hypothyroid patient and had to decide whether or not to clear them for surgery.”
Previous studies conducted at large institutions, the Mayo Clinic and Massachusetts General Hospital, had conflicting findings and were done about 30 years ago, she said. Anesthesia and surgical care have improved substantially since then, leading the investigators to hypothesize that hypothyroidism would not carry higher surgical risk today.
Dr. Villavicencio and her coinvestigator, Cary Mariash, MD, used their institutional database to identify 29 adult patients with a thyroid-stimulating hormone (TSH) level of greater than 10 mcU/mL alone or with a TSH level exceeding the upper limit of normal along with a free thyroxine (T4) level of less than 0.6 ng/dL who underwent surgery during 2010-2015. They matched each patient on age, sex, and surgical procedure with a control euthyroid patient.
The mean TSH level in the hypothyroid group was 29.2 mcU/mL. The majority of patients in each group – 59% of the hypothyroid group and 62% of the euthyroid group – had an American Surgical Association class of 3, denoting that this was a fairly sick population. The groups were generally similar on rates of comorbidity, except that the euthyroid patients had a slightly higher prevalence of obstructive sleep apnea.
In both groups, the majority of procedures were laparotomy and/or bowel resection; pharyngolaryngectomy and esophagectomy/esophagoplasty; and wound or bone debridement.
Main results showed that in the hypothyroid group, hospital length of stay predicted with the American College of Surgeons National Surgical Quality Improvement Program surgical risk calculator was 6.9 days, but actual length of stay was 14.4 days (P = .0004). In contrast, in the euthyroid group, predicted length of stay was a similar at 7.1 days, and actual length of stay was statistically indistinguishable at 9.2 days (P = .1).
“Hypothyroidism is not taken into account with this calculator,” Dr. Villavicencio noted, adding that she was unaware of any surgical calculators that do.
One patient in the hypothyroid group died, compared with none in the euthyroid group. In terms of postoperative cardiac complications, two patients in the hypothyroid group experienced atrial fibrillation, and there was one case of pulseless electrical–activity arrest in each group.
The groups did not differ on incidence of hypothermia, bradycardia, hyponatremia, time to extubation, and hypotension. However, mean arterial pressure tended to be lower in the hypothyroid group (51 mm Hg) than in the euthyroid group (56 mm Hg), and the former more often needed vasopressors. Furthermore, postoperative ileus and reintubation were more common in the hypothyroid group.
“I think that there are kind of a lot of little things that add up to explain [the longer stay],” said Dr. Villavicencio, who disclosed that she had no relevant conflicts of interest.
VICTORIA, B.C. – Even with contemporary anesthesia and surgical techniques, patients who are overtly hypothyroid at the time of major surgery have a rockier course, suggests a retrospective cohort study of 58 patients in a poster presentation at the annual meeting of the American Thyroid Association.
Actual length of stay for hypothyroid patients was twice that predicted by a commonly used risk calculator, whereas actual and predicted stays aligned well for euthyroid patients. The hypothyroid group had more cases of postoperative atrial fibrillation, ileus, reintubation, and death, although numbers were too small for statistical comparison.
“This will have an impact on how we look at patients, especially from a hospital standpoint and management. That’s quite a bit longer stay and quite a bit more cost. And the longer you stay, the more complications you have, too, so it could be riskier for the patient as well,” said first author Raquel Villavicencio, MD, a fellow at Indiana University at the time of the study, and now a clinical endocrinologist at Community Hospital in Indianapolis.
“Although we don’t consider hypothyroidism an absolute contraindication to surgery, especially if it’s necessary surgery, certainly anybody who is having elective surgery should have it postponed, in our opinion, until they are rendered euthyroid,” she said. “More studies are needed to look at this a little bit closer.”
Explaining the study’s rationale, Dr. Villavicencio noted, “This was a question that came up maybe three or four times a year, where we would get a hypothyroid patient and had to decide whether or not to clear them for surgery.”
Previous studies conducted at large institutions, the Mayo Clinic and Massachusetts General Hospital, had conflicting findings and were done about 30 years ago, she said. Anesthesia and surgical care have improved substantially since then, leading the investigators to hypothesize that hypothyroidism would not carry higher surgical risk today.
Dr. Villavicencio and her coinvestigator, Cary Mariash, MD, used their institutional database to identify 29 adult patients with a thyroid-stimulating hormone (TSH) level of greater than 10 mcU/mL alone or with a TSH level exceeding the upper limit of normal along with a free thyroxine (T4) level of less than 0.6 ng/dL who underwent surgery during 2010-2015. They matched each patient on age, sex, and surgical procedure with a control euthyroid patient.
The mean TSH level in the hypothyroid group was 29.2 mcU/mL. The majority of patients in each group – 59% of the hypothyroid group and 62% of the euthyroid group – had an American Surgical Association class of 3, denoting that this was a fairly sick population. The groups were generally similar on rates of comorbidity, except that the euthyroid patients had a slightly higher prevalence of obstructive sleep apnea.
In both groups, the majority of procedures were laparotomy and/or bowel resection; pharyngolaryngectomy and esophagectomy/esophagoplasty; and wound or bone debridement.
Main results showed that in the hypothyroid group, hospital length of stay predicted with the American College of Surgeons National Surgical Quality Improvement Program surgical risk calculator was 6.9 days, but actual length of stay was 14.4 days (P = .0004). In contrast, in the euthyroid group, predicted length of stay was a similar at 7.1 days, and actual length of stay was statistically indistinguishable at 9.2 days (P = .1).
“Hypothyroidism is not taken into account with this calculator,” Dr. Villavicencio noted, adding that she was unaware of any surgical calculators that do.
One patient in the hypothyroid group died, compared with none in the euthyroid group. In terms of postoperative cardiac complications, two patients in the hypothyroid group experienced atrial fibrillation, and there was one case of pulseless electrical–activity arrest in each group.
The groups did not differ on incidence of hypothermia, bradycardia, hyponatremia, time to extubation, and hypotension. However, mean arterial pressure tended to be lower in the hypothyroid group (51 mm Hg) than in the euthyroid group (56 mm Hg), and the former more often needed vasopressors. Furthermore, postoperative ileus and reintubation were more common in the hypothyroid group.
“I think that there are kind of a lot of little things that add up to explain [the longer stay],” said Dr. Villavicencio, who disclosed that she had no relevant conflicts of interest.
AT ATA 2017
Key clinical point:
Major finding: Actual length of stay was significantly longer than calculator-predicted length of stay among hypothyroid patients (14.4 vs. 6.9 days, P = .0004) but not among euthyroid patients (9.2 vs. 7.1 days; P = .1).
Data source: A retrospective cohort study of 29 hypothyroid patients and 29 matched euthyroid patients undergoing major surgery.
Disclosures: Dr. Villavicencio disclosed that she had no relevant conflicts of interest.
Patients prefer higher dose of levothyroxine despite lack of objective benefit
VICTORIA, B.C. – Patient perception plays a large role in subjective benefit of levothyroxine therapy for hypothyroidism, suggests a double-blind randomized controlled trial reported at the annual meeting of the American Thyroid Association.
Mood, cognition, and quality of life (QoL) did not differ whether patients’ levothyroxine dose was adjusted to achieve thyroid-stimulating hormone (TSH) levels in the low-normal, high-normal, or mildly elevated range. But despite this lack of objective benefit, the large majority of patients preferred levothyroxine doses that they perceived to be higher – whether they actually were or not.
The study was not restricted to certain groups who might have a better response to higher levothyroxine dose, she acknowledged. Two such groups are patients with more symptoms (although volunteering for the study suggested dissatisfaction with symptom control) and patients with low tri-iodothyronine (T3) levels (although about half of patients had low baseline levels).
“We encourage further research in older subjects, men, and subjects with specific symptoms, low T3 levels, or functional polymorphisms in thyroid-relevant genes,” Dr. Samuels said. “These are really difficult, expensive studies to do, and if we are going to have any hope of getting them funded and doing them, I think that we have to be much more targeted.”
One of the session co-chairs, Catherine A. Dinauer, MD, a pediatric endocrinologist and clinician at the Yale Pediatric Thyroid Center, New Haven, Conn., commented, “I think these are really interesting data because there’s this sense among patients that their dose really affects how they feel, and this is essentially turning that on its head. It’s not really clear, then, why are these patients still maybe not feeling well.”
“It will be interesting to see more data on this and ... more about this business of checking T3 levels. Do we need to supplement with T3? I think we really don’t know that, especially in kids, but even in adults,” she added.
The other session co-chair, Yaron Tomer, MD, chair of the department of medicine and the Anita and Jack Saltz Chair in Diabetes Research at the Montefiore Medical Center, Bronx, N.Y., commented, “I think this study confirmed what a lot of us feel, that there is a lot of placebo effect when you treat in different ways to optimize the TSH or give T3.”
Other data reported in the session provide a possible explanation for the lack of benefit of adjusting pharmacologic therapy, suggesting that the volumes of various brain structures change with perturbations of thyroid function, he noted. “There might be true changes in the brain that affect how the patients feel. So these patients may truly not feel well. It’s just that we can’t fix it by adjusting the TSH level to very narrow margins or by adding T3,” he said.
Study details
“It is well known that overt hypothyroidism interferes with mood and a number of cognitive functions. However, neurocognitive effects of variations in thyroid function within the reference range and in mild or subclinical hypothyroidism are less clear,” Dr. Samuels noted, giving some background to the research.
“Observational studies of this question have tended to be negative but have often included less sensitive global screening tests of cognition. There are very few small-scale interventional studies,” she continued. “In the absence of conclusive data, many patients with mild hypothyroidism are started on levothyroxine to treat nonspecific quality of life, mood, or cognitive symptoms, and many additional treated patients request increased levothyroxine doses due to persistence of these symptoms.”
Dr. Samuels and her coinvestigators enrolled in the trial 138 hypothyroid but otherwise healthy patients who had been on a stable dose of levothyroxine (Synthroid and others) alone for at least 3 months and had normal TSH levels.
The patients were randomized to three groups in which clinicians adjusted levothyroxine dose every 6 weeks in blinded fashion to achieve different target TSH levels: low-normal TSH (0.34-2.50 mU/L), high-normal TSH (2.51-5.60 mU/L), or mildly elevated TSH (5.60-12.0 mU/L). Patients completed a battery of assessments at baseline and again at 6 months.
Main results confirmed that TSH targets were generally achieved, with significantly different mean TSH levels in the low-normal group (1.34 mU/L), high-normal group (3.74 mU/L), and mildly elevated group (9.74 mU/L) (P less than .05).
In crude analyses, results differed significantly across groups for only two of the dozens of measures of mood, cognition, and QoL assessed: bodily pain (26%, 11%, and 34% of patients reporting a high pain level in the low-normal, high-normal, and mildly elevated TSH groups, respectively; P = .03) and working memory on the N-Back test (86%, 58%, and 75% with a 1-back result; P = .002). However, there were no significant differences for any of the measures when analyses were repeated with statistical correction for multiple comparisons.
At the end of the study, patients were unable to say with any accuracy say whether they were receiving a dose of levothyroxine that was higher than, lower than, or unchanged from their baseline dose (P = .55 for actual vs. perceived).
However, patients preferred what they perceived to be a higher dose (P less than .001 for preferred vs. perceived). In the group perceiving their end-of-study dose was higher, the majority of patients (68%) preferred that dose, and in the group perceiving their end-of-study dose was lower, most (96%) preferred their baseline dose.
The sample size may not have been adequate to detect very small effects of changes in levothyroxine dose, acknowledged Dr. Samuels, who disclosed that she had no relevant conflicts of interest. Additionally, patients were predominantly female and younger, and heterogeneous with respect to thyroid diagnosis and length of levothyroxine therapy.
VICTORIA, B.C. – Patient perception plays a large role in subjective benefit of levothyroxine therapy for hypothyroidism, suggests a double-blind randomized controlled trial reported at the annual meeting of the American Thyroid Association.
Mood, cognition, and quality of life (QoL) did not differ whether patients’ levothyroxine dose was adjusted to achieve thyroid-stimulating hormone (TSH) levels in the low-normal, high-normal, or mildly elevated range. But despite this lack of objective benefit, the large majority of patients preferred levothyroxine doses that they perceived to be higher – whether they actually were or not.
The study was not restricted to certain groups who might have a better response to higher levothyroxine dose, she acknowledged. Two such groups are patients with more symptoms (although volunteering for the study suggested dissatisfaction with symptom control) and patients with low tri-iodothyronine (T3) levels (although about half of patients had low baseline levels).
“We encourage further research in older subjects, men, and subjects with specific symptoms, low T3 levels, or functional polymorphisms in thyroid-relevant genes,” Dr. Samuels said. “These are really difficult, expensive studies to do, and if we are going to have any hope of getting them funded and doing them, I think that we have to be much more targeted.”
One of the session co-chairs, Catherine A. Dinauer, MD, a pediatric endocrinologist and clinician at the Yale Pediatric Thyroid Center, New Haven, Conn., commented, “I think these are really interesting data because there’s this sense among patients that their dose really affects how they feel, and this is essentially turning that on its head. It’s not really clear, then, why are these patients still maybe not feeling well.”
“It will be interesting to see more data on this and ... more about this business of checking T3 levels. Do we need to supplement with T3? I think we really don’t know that, especially in kids, but even in adults,” she added.
The other session co-chair, Yaron Tomer, MD, chair of the department of medicine and the Anita and Jack Saltz Chair in Diabetes Research at the Montefiore Medical Center, Bronx, N.Y., commented, “I think this study confirmed what a lot of us feel, that there is a lot of placebo effect when you treat in different ways to optimize the TSH or give T3.”
Other data reported in the session provide a possible explanation for the lack of benefit of adjusting pharmacologic therapy, suggesting that the volumes of various brain structures change with perturbations of thyroid function, he noted. “There might be true changes in the brain that affect how the patients feel. So these patients may truly not feel well. It’s just that we can’t fix it by adjusting the TSH level to very narrow margins or by adding T3,” he said.
Study details
“It is well known that overt hypothyroidism interferes with mood and a number of cognitive functions. However, neurocognitive effects of variations in thyroid function within the reference range and in mild or subclinical hypothyroidism are less clear,” Dr. Samuels noted, giving some background to the research.
“Observational studies of this question have tended to be negative but have often included less sensitive global screening tests of cognition. There are very few small-scale interventional studies,” she continued. “In the absence of conclusive data, many patients with mild hypothyroidism are started on levothyroxine to treat nonspecific quality of life, mood, or cognitive symptoms, and many additional treated patients request increased levothyroxine doses due to persistence of these symptoms.”
Dr. Samuels and her coinvestigators enrolled in the trial 138 hypothyroid but otherwise healthy patients who had been on a stable dose of levothyroxine (Synthroid and others) alone for at least 3 months and had normal TSH levels.
The patients were randomized to three groups in which clinicians adjusted levothyroxine dose every 6 weeks in blinded fashion to achieve different target TSH levels: low-normal TSH (0.34-2.50 mU/L), high-normal TSH (2.51-5.60 mU/L), or mildly elevated TSH (5.60-12.0 mU/L). Patients completed a battery of assessments at baseline and again at 6 months.
Main results confirmed that TSH targets were generally achieved, with significantly different mean TSH levels in the low-normal group (1.34 mU/L), high-normal group (3.74 mU/L), and mildly elevated group (9.74 mU/L) (P less than .05).
In crude analyses, results differed significantly across groups for only two of the dozens of measures of mood, cognition, and QoL assessed: bodily pain (26%, 11%, and 34% of patients reporting a high pain level in the low-normal, high-normal, and mildly elevated TSH groups, respectively; P = .03) and working memory on the N-Back test (86%, 58%, and 75% with a 1-back result; P = .002). However, there were no significant differences for any of the measures when analyses were repeated with statistical correction for multiple comparisons.
At the end of the study, patients were unable to say with any accuracy say whether they were receiving a dose of levothyroxine that was higher than, lower than, or unchanged from their baseline dose (P = .55 for actual vs. perceived).
However, patients preferred what they perceived to be a higher dose (P less than .001 for preferred vs. perceived). In the group perceiving their end-of-study dose was higher, the majority of patients (68%) preferred that dose, and in the group perceiving their end-of-study dose was lower, most (96%) preferred their baseline dose.
The sample size may not have been adequate to detect very small effects of changes in levothyroxine dose, acknowledged Dr. Samuels, who disclosed that she had no relevant conflicts of interest. Additionally, patients were predominantly female and younger, and heterogeneous with respect to thyroid diagnosis and length of levothyroxine therapy.
VICTORIA, B.C. – Patient perception plays a large role in subjective benefit of levothyroxine therapy for hypothyroidism, suggests a double-blind randomized controlled trial reported at the annual meeting of the American Thyroid Association.
Mood, cognition, and quality of life (QoL) did not differ whether patients’ levothyroxine dose was adjusted to achieve thyroid-stimulating hormone (TSH) levels in the low-normal, high-normal, or mildly elevated range. But despite this lack of objective benefit, the large majority of patients preferred levothyroxine doses that they perceived to be higher – whether they actually were or not.
The study was not restricted to certain groups who might have a better response to higher levothyroxine dose, she acknowledged. Two such groups are patients with more symptoms (although volunteering for the study suggested dissatisfaction with symptom control) and patients with low tri-iodothyronine (T3) levels (although about half of patients had low baseline levels).
“We encourage further research in older subjects, men, and subjects with specific symptoms, low T3 levels, or functional polymorphisms in thyroid-relevant genes,” Dr. Samuels said. “These are really difficult, expensive studies to do, and if we are going to have any hope of getting them funded and doing them, I think that we have to be much more targeted.”
One of the session co-chairs, Catherine A. Dinauer, MD, a pediatric endocrinologist and clinician at the Yale Pediatric Thyroid Center, New Haven, Conn., commented, “I think these are really interesting data because there’s this sense among patients that their dose really affects how they feel, and this is essentially turning that on its head. It’s not really clear, then, why are these patients still maybe not feeling well.”
“It will be interesting to see more data on this and ... more about this business of checking T3 levels. Do we need to supplement with T3? I think we really don’t know that, especially in kids, but even in adults,” she added.
The other session co-chair, Yaron Tomer, MD, chair of the department of medicine and the Anita and Jack Saltz Chair in Diabetes Research at the Montefiore Medical Center, Bronx, N.Y., commented, “I think this study confirmed what a lot of us feel, that there is a lot of placebo effect when you treat in different ways to optimize the TSH or give T3.”
Other data reported in the session provide a possible explanation for the lack of benefit of adjusting pharmacologic therapy, suggesting that the volumes of various brain structures change with perturbations of thyroid function, he noted. “There might be true changes in the brain that affect how the patients feel. So these patients may truly not feel well. It’s just that we can’t fix it by adjusting the TSH level to very narrow margins or by adding T3,” he said.
Study details
“It is well known that overt hypothyroidism interferes with mood and a number of cognitive functions. However, neurocognitive effects of variations in thyroid function within the reference range and in mild or subclinical hypothyroidism are less clear,” Dr. Samuels noted, giving some background to the research.
“Observational studies of this question have tended to be negative but have often included less sensitive global screening tests of cognition. There are very few small-scale interventional studies,” she continued. “In the absence of conclusive data, many patients with mild hypothyroidism are started on levothyroxine to treat nonspecific quality of life, mood, or cognitive symptoms, and many additional treated patients request increased levothyroxine doses due to persistence of these symptoms.”
Dr. Samuels and her coinvestigators enrolled in the trial 138 hypothyroid but otherwise healthy patients who had been on a stable dose of levothyroxine (Synthroid and others) alone for at least 3 months and had normal TSH levels.
The patients were randomized to three groups in which clinicians adjusted levothyroxine dose every 6 weeks in blinded fashion to achieve different target TSH levels: low-normal TSH (0.34-2.50 mU/L), high-normal TSH (2.51-5.60 mU/L), or mildly elevated TSH (5.60-12.0 mU/L). Patients completed a battery of assessments at baseline and again at 6 months.
Main results confirmed that TSH targets were generally achieved, with significantly different mean TSH levels in the low-normal group (1.34 mU/L), high-normal group (3.74 mU/L), and mildly elevated group (9.74 mU/L) (P less than .05).
In crude analyses, results differed significantly across groups for only two of the dozens of measures of mood, cognition, and QoL assessed: bodily pain (26%, 11%, and 34% of patients reporting a high pain level in the low-normal, high-normal, and mildly elevated TSH groups, respectively; P = .03) and working memory on the N-Back test (86%, 58%, and 75% with a 1-back result; P = .002). However, there were no significant differences for any of the measures when analyses were repeated with statistical correction for multiple comparisons.
At the end of the study, patients were unable to say with any accuracy say whether they were receiving a dose of levothyroxine that was higher than, lower than, or unchanged from their baseline dose (P = .55 for actual vs. perceived).
However, patients preferred what they perceived to be a higher dose (P less than .001 for preferred vs. perceived). In the group perceiving their end-of-study dose was higher, the majority of patients (68%) preferred that dose, and in the group perceiving their end-of-study dose was lower, most (96%) preferred their baseline dose.
The sample size may not have been adequate to detect very small effects of changes in levothyroxine dose, acknowledged Dr. Samuels, who disclosed that she had no relevant conflicts of interest. Additionally, patients were predominantly female and younger, and heterogeneous with respect to thyroid diagnosis and length of levothyroxine therapy.
AT ATA 2017
Key clinical point:
Major finding: Mood, cognition, and QoL were similar across levothyroxine doses targeting various TSH levels, but patients preferred what they believed was a higher dose, even when it was not (P less than .001 for preferred vs. perceived).
Data source: A randomized trial of levothyroxine adjustment among 138 hypothyroid patients on a stable dose of the drug who had normal TSH levels.
Disclosures: Dr. Samuels disclosed that she had no relevant conflicts of interest.
Long-term methimazole therapy improves Graves disease remission rate
VICTORIA, B.C. – In the debate over the optimal duration of methimazole therapy for Graves disease, findings of a new randomized, controlled trial reported at the annual meeting of the American Thyroid Association tip the balance in favor of long-term therapy.
The relapse rate among patients who stayed on the drug long term, for a median of 96 months, was about one-third that among patients who stopped after 18 months, reported lead investigator Fereidoun Azizi, MD, of the Endocrine Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran. Patients staying on the drug long term did not experience any adverse effects during that time, although only those able to tolerate the drug initially were randomized.
There may be two explanations for this benefit of long-term therapy, according to Dr. Azizi. Long-term therapy may alter immune-related molecular signaling and cell subsets in both the thymus and periphery, ultimately shifting disease course. On the other hand, establishing and maintaining euthyroidism for a prolonged period of time may quell the autoimmune response.
“We are looking at this in depth and also at some of the [molecular factors] in order to elucidate the mechanism behind our striking findings,” he said.
One of the session cochairs, Yaron Tomer, MD, chair of the department of medicine and the Anita and Jack Saltz Chair in Diabetes Research at the Montefiore Medical Center, New York, commented, “There is a move today away from radioactive iodine – many patients do not want radioactive iodine, and we do more surgery now because of that. So this opens up a new option that we didn’t have before.”
The other session cochair, Catherine A. Dinauer, MD, a pediatric endocrinologist and clinician at the Yale Pediatric Thyroid Center, New Haven, Conn., noted that duration of therapy frequently comes up in her practice.
Study details
Relapse of hyperthyroidism after discontinuation of antithyroid drugs remains problematic, Dr. Azizi pointed out when introducing the study.
“Many of the major papers have noted that longer antithyroid drug treatment does not really influence remission rate of Graves, and therefore most of us treat for between 12 and 24 months with antithyroid drugs, and then we stop the medication,” he said. However, recent studies and in particular a meta-analysis (Thyroid. 2017;27:1223-31) suggest there may be an advantage of long-term therapy.
Dr. Azizi and coinvestigators recruited to their trial 302 consecutive patients from a single clinic who had untreated Graves disease and were started on methimazole (Tapazole) therapy.
The 258 patients completing 18 months of therapy were randomized to stop the drug or continue on a maintenance dose long term, for 60-120 months, on a single-blind basis. (The other 44 patients withdrew mainly because of side effects, relapse, and loss to follow-up.)
Patients in the long-term therapy group stayed on the drug for a median of 96 months. The decision about specifically when to stop in this group was guided by thyroid function test results and patients’ clinical status and preferences, according to Dr. Azizi.
The rate of relapse at 48 months after stopping methimazole was 51% among patients in the short-term therapy group but just 16% among patients in the long-term therapy group (P less than or equal to .001). “Definitely, this looks like a cure of the disease if we consider this very low incidence of relapse,” he commented.
Within the group treated long term, patients who did and did not experience relapse were statistically indistinguishable with respect to temporal trends in levels of triiodothyronine (T3), free thyroxine (T4), thyroid-stimulating hormone (TSH), and thyroid-stimulating hormone receptor antibody (TRAb).
Additionally, the daily dose of methimazole therapy required to maintain TSH levels in the normal range fell similarly over time, to about half the initial dose, regardless of whether patients had a relapse or not.
“At the end of treatment, the majority of patients were taking less than 5 mg/day of methimazole,” Dr. Azizi reported. “Some patients needed only two or three pills of 5-mg methimazole per week, and this is very interesting to know, that after you continue, you have definitely more response to methimazole.”
Multivariate analyses showed that in the short-term therapy group, risk factors for relapse were age, sex, and end-of-therapy levels of T3, TSH, and TRAb. In the long-term therapy group, risk factors were end-of-therapy levels of free T4 and TSH.
“We are currently performing more in-depth analysis of genetic markers, including both SNPs [single nucleotide polymorphisms] and HLA [human leukocyte antigen] subtyping on these samples to assess any potential association between relapse rates and genetic background,” Dr. Azizi noted. “However, the problem is the low number of patients who have had a relapse long term.”
During the first 18 months of methimazole therapy, 16 patients had adverse effects in the first 2 months (14 had cutaneous reactions and 2 had elevation of liver enzymes). However, there were no serious complications, such as agranulocytosis.
“It’s very reassuring that after 18 months, in those who had long-term treatment, we did not see any minor or major complications throughout, up to the 120 months of treatment we have had in some of our patients,” Dr. Azizi commented.
Dr. Azizi disclosed that he had no relevant conflicts of interest.
VICTORIA, B.C. – In the debate over the optimal duration of methimazole therapy for Graves disease, findings of a new randomized, controlled trial reported at the annual meeting of the American Thyroid Association tip the balance in favor of long-term therapy.
The relapse rate among patients who stayed on the drug long term, for a median of 96 months, was about one-third that among patients who stopped after 18 months, reported lead investigator Fereidoun Azizi, MD, of the Endocrine Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran. Patients staying on the drug long term did not experience any adverse effects during that time, although only those able to tolerate the drug initially were randomized.
There may be two explanations for this benefit of long-term therapy, according to Dr. Azizi. Long-term therapy may alter immune-related molecular signaling and cell subsets in both the thymus and periphery, ultimately shifting disease course. On the other hand, establishing and maintaining euthyroidism for a prolonged period of time may quell the autoimmune response.
“We are looking at this in depth and also at some of the [molecular factors] in order to elucidate the mechanism behind our striking findings,” he said.
One of the session cochairs, Yaron Tomer, MD, chair of the department of medicine and the Anita and Jack Saltz Chair in Diabetes Research at the Montefiore Medical Center, New York, commented, “There is a move today away from radioactive iodine – many patients do not want radioactive iodine, and we do more surgery now because of that. So this opens up a new option that we didn’t have before.”
The other session cochair, Catherine A. Dinauer, MD, a pediatric endocrinologist and clinician at the Yale Pediatric Thyroid Center, New Haven, Conn., noted that duration of therapy frequently comes up in her practice.
Study details
Relapse of hyperthyroidism after discontinuation of antithyroid drugs remains problematic, Dr. Azizi pointed out when introducing the study.
“Many of the major papers have noted that longer antithyroid drug treatment does not really influence remission rate of Graves, and therefore most of us treat for between 12 and 24 months with antithyroid drugs, and then we stop the medication,” he said. However, recent studies and in particular a meta-analysis (Thyroid. 2017;27:1223-31) suggest there may be an advantage of long-term therapy.
Dr. Azizi and coinvestigators recruited to their trial 302 consecutive patients from a single clinic who had untreated Graves disease and were started on methimazole (Tapazole) therapy.
The 258 patients completing 18 months of therapy were randomized to stop the drug or continue on a maintenance dose long term, for 60-120 months, on a single-blind basis. (The other 44 patients withdrew mainly because of side effects, relapse, and loss to follow-up.)
Patients in the long-term therapy group stayed on the drug for a median of 96 months. The decision about specifically when to stop in this group was guided by thyroid function test results and patients’ clinical status and preferences, according to Dr. Azizi.
The rate of relapse at 48 months after stopping methimazole was 51% among patients in the short-term therapy group but just 16% among patients in the long-term therapy group (P less than or equal to .001). “Definitely, this looks like a cure of the disease if we consider this very low incidence of relapse,” he commented.
Within the group treated long term, patients who did and did not experience relapse were statistically indistinguishable with respect to temporal trends in levels of triiodothyronine (T3), free thyroxine (T4), thyroid-stimulating hormone (TSH), and thyroid-stimulating hormone receptor antibody (TRAb).
Additionally, the daily dose of methimazole therapy required to maintain TSH levels in the normal range fell similarly over time, to about half the initial dose, regardless of whether patients had a relapse or not.
“At the end of treatment, the majority of patients were taking less than 5 mg/day of methimazole,” Dr. Azizi reported. “Some patients needed only two or three pills of 5-mg methimazole per week, and this is very interesting to know, that after you continue, you have definitely more response to methimazole.”
Multivariate analyses showed that in the short-term therapy group, risk factors for relapse were age, sex, and end-of-therapy levels of T3, TSH, and TRAb. In the long-term therapy group, risk factors were end-of-therapy levels of free T4 and TSH.
“We are currently performing more in-depth analysis of genetic markers, including both SNPs [single nucleotide polymorphisms] and HLA [human leukocyte antigen] subtyping on these samples to assess any potential association between relapse rates and genetic background,” Dr. Azizi noted. “However, the problem is the low number of patients who have had a relapse long term.”
During the first 18 months of methimazole therapy, 16 patients had adverse effects in the first 2 months (14 had cutaneous reactions and 2 had elevation of liver enzymes). However, there were no serious complications, such as agranulocytosis.
“It’s very reassuring that after 18 months, in those who had long-term treatment, we did not see any minor or major complications throughout, up to the 120 months of treatment we have had in some of our patients,” Dr. Azizi commented.
Dr. Azizi disclosed that he had no relevant conflicts of interest.
VICTORIA, B.C. – In the debate over the optimal duration of methimazole therapy for Graves disease, findings of a new randomized, controlled trial reported at the annual meeting of the American Thyroid Association tip the balance in favor of long-term therapy.
The relapse rate among patients who stayed on the drug long term, for a median of 96 months, was about one-third that among patients who stopped after 18 months, reported lead investigator Fereidoun Azizi, MD, of the Endocrine Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran. Patients staying on the drug long term did not experience any adverse effects during that time, although only those able to tolerate the drug initially were randomized.
There may be two explanations for this benefit of long-term therapy, according to Dr. Azizi. Long-term therapy may alter immune-related molecular signaling and cell subsets in both the thymus and periphery, ultimately shifting disease course. On the other hand, establishing and maintaining euthyroidism for a prolonged period of time may quell the autoimmune response.
“We are looking at this in depth and also at some of the [molecular factors] in order to elucidate the mechanism behind our striking findings,” he said.
One of the session cochairs, Yaron Tomer, MD, chair of the department of medicine and the Anita and Jack Saltz Chair in Diabetes Research at the Montefiore Medical Center, New York, commented, “There is a move today away from radioactive iodine – many patients do not want radioactive iodine, and we do more surgery now because of that. So this opens up a new option that we didn’t have before.”
The other session cochair, Catherine A. Dinauer, MD, a pediatric endocrinologist and clinician at the Yale Pediatric Thyroid Center, New Haven, Conn., noted that duration of therapy frequently comes up in her practice.
Study details
Relapse of hyperthyroidism after discontinuation of antithyroid drugs remains problematic, Dr. Azizi pointed out when introducing the study.
“Many of the major papers have noted that longer antithyroid drug treatment does not really influence remission rate of Graves, and therefore most of us treat for between 12 and 24 months with antithyroid drugs, and then we stop the medication,” he said. However, recent studies and in particular a meta-analysis (Thyroid. 2017;27:1223-31) suggest there may be an advantage of long-term therapy.
Dr. Azizi and coinvestigators recruited to their trial 302 consecutive patients from a single clinic who had untreated Graves disease and were started on methimazole (Tapazole) therapy.
The 258 patients completing 18 months of therapy were randomized to stop the drug or continue on a maintenance dose long term, for 60-120 months, on a single-blind basis. (The other 44 patients withdrew mainly because of side effects, relapse, and loss to follow-up.)
Patients in the long-term therapy group stayed on the drug for a median of 96 months. The decision about specifically when to stop in this group was guided by thyroid function test results and patients’ clinical status and preferences, according to Dr. Azizi.
The rate of relapse at 48 months after stopping methimazole was 51% among patients in the short-term therapy group but just 16% among patients in the long-term therapy group (P less than or equal to .001). “Definitely, this looks like a cure of the disease if we consider this very low incidence of relapse,” he commented.
Within the group treated long term, patients who did and did not experience relapse were statistically indistinguishable with respect to temporal trends in levels of triiodothyronine (T3), free thyroxine (T4), thyroid-stimulating hormone (TSH), and thyroid-stimulating hormone receptor antibody (TRAb).
Additionally, the daily dose of methimazole therapy required to maintain TSH levels in the normal range fell similarly over time, to about half the initial dose, regardless of whether patients had a relapse or not.
“At the end of treatment, the majority of patients were taking less than 5 mg/day of methimazole,” Dr. Azizi reported. “Some patients needed only two or three pills of 5-mg methimazole per week, and this is very interesting to know, that after you continue, you have definitely more response to methimazole.”
Multivariate analyses showed that in the short-term therapy group, risk factors for relapse were age, sex, and end-of-therapy levels of T3, TSH, and TRAb. In the long-term therapy group, risk factors were end-of-therapy levels of free T4 and TSH.
“We are currently performing more in-depth analysis of genetic markers, including both SNPs [single nucleotide polymorphisms] and HLA [human leukocyte antigen] subtyping on these samples to assess any potential association between relapse rates and genetic background,” Dr. Azizi noted. “However, the problem is the low number of patients who have had a relapse long term.”
During the first 18 months of methimazole therapy, 16 patients had adverse effects in the first 2 months (14 had cutaneous reactions and 2 had elevation of liver enzymes). However, there were no serious complications, such as agranulocytosis.
“It’s very reassuring that after 18 months, in those who had long-term treatment, we did not see any minor or major complications throughout, up to the 120 months of treatment we have had in some of our patients,” Dr. Azizi commented.
Dr. Azizi disclosed that he had no relevant conflicts of interest.
AT ATA 2017
Key clinical point:
Major finding: Relative to peers who stopped methimazole after 18 months, patients who continued on the drug for a median of 96 months had a lower rate of relapse after discontinuation (51% vs. 16%; P less than or equal to .001).
Data source: A randomized controlled trial among 258 patients with Graves disease who were relapse free after 18 months on methimazole.
Disclosures: Dr. Azizi disclosed that he had no relevant conflicts of interest.