User login
ANSWER
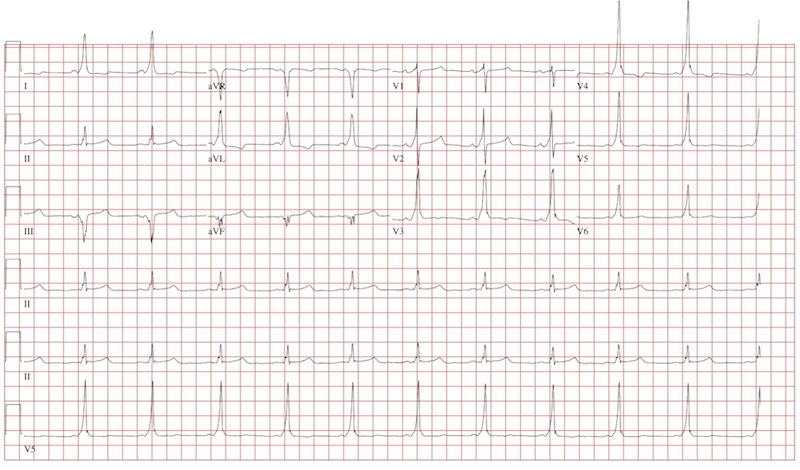
The ECG reveals a short PR interval (< 120 ms), a slurred upstroke (delta wave) of the initiation of the QRS complex indicating ventricular preexcitation, a broad QRS (> 110 ms) as a result of the delta wave, and secondary ST- and T-wave changes consistent with Wolf-Parkinson-White (WPW) syndrome. The delta wave is an indicator of an electrical impulse that bypasses normal AV nodal conduction through one or more accessory pathways that allow direct antegrade conduction between the atria and ventricles.
If the delta wave is positive in lead V1, the accessory pathway is located between the left atrium and left ventricle. If the delta wave is negative in aVF, as indicated in this ECG, the accessory pathway can be further located to the lateral wall of the left atrium. This localization aids in estimating the location of the accessory pathway prior to electrophysiology study and ablation.
ANSWER
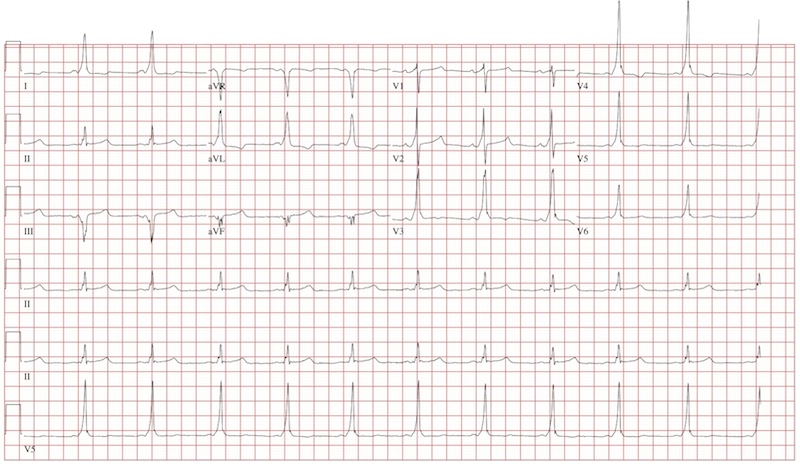
The ECG reveals a short PR interval (< 120 ms), a slurred upstroke (delta wave) of the initiation of the QRS complex indicating ventricular preexcitation, a broad QRS (> 110 ms) as a result of the delta wave, and secondary ST- and T-wave changes consistent with Wolf-Parkinson-White (WPW) syndrome. The delta wave is an indicator of an electrical impulse that bypasses normal AV nodal conduction through one or more accessory pathways that allow direct antegrade conduction between the atria and ventricles.
If the delta wave is positive in lead V1, the accessory pathway is located between the left atrium and left ventricle. If the delta wave is negative in aVF, as indicated in this ECG, the accessory pathway can be further located to the lateral wall of the left atrium. This localization aids in estimating the location of the accessory pathway prior to electrophysiology study and ablation.
ANSWER
The ECG reveals a short PR interval (< 120 ms), a slurred upstroke (delta wave) of the initiation of the QRS complex indicating ventricular preexcitation, a broad QRS (> 110 ms) as a result of the delta wave, and secondary ST- and T-wave changes consistent with Wolf-Parkinson-White (WPW) syndrome. The delta wave is an indicator of an electrical impulse that bypasses normal AV nodal conduction through one or more accessory pathways that allow direct antegrade conduction between the atria and ventricles.
If the delta wave is positive in lead V1, the accessory pathway is located between the left atrium and left ventricle. If the delta wave is negative in aVF, as indicated in this ECG, the accessory pathway can be further located to the lateral wall of the left atrium. This localization aids in estimating the location of the accessory pathway prior to electrophysiology study and ablation.
An 18-year-old man has palpitations that occur with variable frequency: sometimes several times per day, and often weeks without an occurrence. The onset is typically abrupt, lasting a few seconds to several minutes before abruptly terminating. He describes them as a “rapid fluttering” sensation in his chest with a “full feeling” in his throat. Associated symptoms include lightheadedness and chest discomfort. He denies chest pain. He had an episode of near-syncope at age 14 and another approximately four weeks ago; the latter prompted him to schedule an appointment in your clinic. He has not been ill recently and has no history to suggest hypovolemia or anemia as a contributing factor for his recent episode of near-syncope. Medical history is unremarkable, with the exception of tonsillectomy at age 7. He is not taking any medications and has no known drug allergies. Family history is positive for coronary artery disease in his father, which required revascularization at age 62, and diabetes in a grandparent. Social history reveals he is a full-time undergraduate student at a local junior college. He drinks approximately one six-pack of beer on weekends despite being under age, but denies use of illegal, illicit, or performance-enhancing drugs. The review of systems is noncontributory. The physical examination reveals a thin, healthy-appearing male in no distress. His blood pressure is 104/62 mm Hg; pulse, 66 beats/min; and respiratory rate, 14 breaths/min. The patient is afebrile. The chest is clear to auscultation bilaterally with good excursion. The cardiac exam reveals a regular rate and rhythm with no murmurs, rubs, gallops, or extra heart sounds. There is no jugular venous distention or peripheral edema. The remainder of the physical exam shows no abnormalities or deficits. Despite the “normal” physical, you are concerned about the patient’s history of frequent palpitations and two previous episodes of near-syncope. You order an ECG, the results of which show: a ventricular rate of 66 beats/min; PR interval, 116 ms; QRS duration, 142 ms; QT/QTc interval, 456/478 ms; P axis, 0°; R axis, –7°; and T axis, 105°. What is your interpretation of this ECG?