User login
According to the National Academy of Medicine (NAM), health literacy is “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions.”1 Studies suggest that millions of patients have inadequate health literacy and cannot make fully informed decisions because of this lack of knowledge.2-4 A 2007 National Patient Safety Foundation report calculated that inadequate health literacy burdens the U.S. health care system with an additional $106 to $238 billion annually.5
In 2014, the American Diabetes Association reported that diabetes affects 29.1 million Americans (9.3%) and that by 2050 1 in 3 Americans will have diabetes.6 People with diabetes have health care costs 2.3 times higher than the cost for nondiabetic patients. The cost of taking care of patients with diabetes annually is about $245 billion.6 Without interventions that address health literacy and effective self-management to reduce the risks of complications and comorbidity, health care costs related to diabetes will continue to increase.
Literature Review
According to a U.S. Department of Education assessment on adult health literacy in 2003, 88% of adults in the U.S. have inadequate health literacy.2 About 90 million Americans lack health literacy skills, according to a 2004 NAM report.3 Heinrich, who conducted a review of U.S. studies on health literacy, concluded that about 25% of Americans have low health literacy.4
The Newest Vital Sign Tool
The Newest Vital Sign (NVS) tool is a free tool developed by Pfizer (New York, NY) for assessing health literacy. Participants are asked 6 questions about nutrition based on an ice cream nutrition label (Figure). The researcher records the participant’s responses, which accommodates participants who may have difficulty reading. The tool is scored from 0 to 6. A score of below 4 indicates the possibility of limited health literacy.7 This test can be completed in about 3 minutes, is widely accepted, and provides results comparable to more extensive literacy tests.8 A study conducted by Welch and colleagues suggested the NVS tool is both cost and time efficient.9 Ryan and colleagues found that 98% of patients in their study (n = 289) did not have objections to taking the NVS assessment.10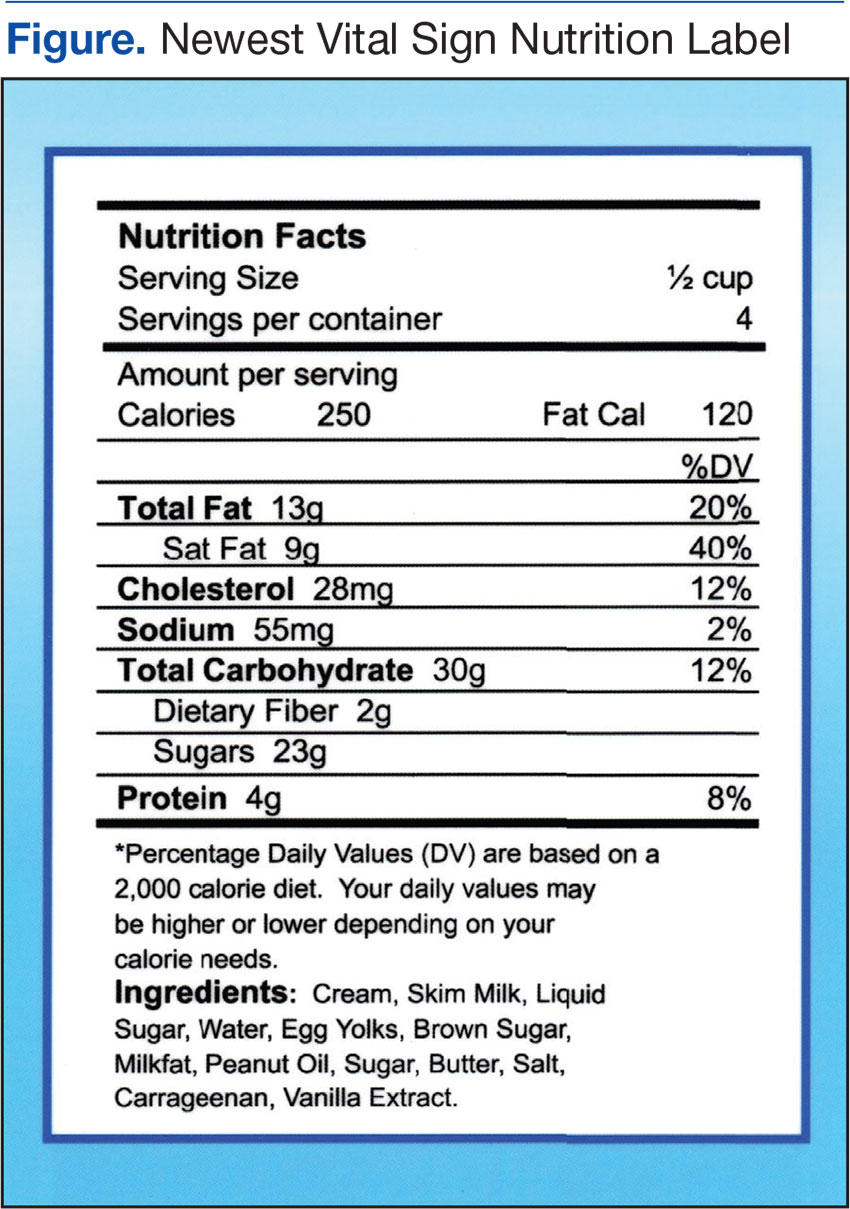
Escobedo and Weismuller’s study used the NVS health literacy tool to assess the health literacy of renal patients.3 In 2004, about 50,000 American patients with diabetes began treatment for kidney failure due to diabetes complications.6 Escobedo and Weismuller found that patients with diabetes with limited health literacy knowledge are more likely to be hospitalized, thus increasing health care costs.3 In addition, they discovered that these patients demonstrated poor adherence to prescribed treatment protocols. Welch, VanGeest, and Caskey conducted a case study on time, cost, and clinical utilization of the NVS health literacy tool and found that a patient’s lack of health literacy was linked to limited participation in personal medical decisions.7,9 Patient’s lack of knowledge was associated with delays in seeking treatment, poor self-management of the disease, and more hospital admissions.
Health Literacy and Diabetes
Studies specific to diabetes and inadequate health literacy support the premise that better health literacy leads to improved patient outcomes. Using the NVS tool, Heinrich conducted a study of the health literacy of 54 patients with diabetes in a primary care setting. The study showed that 65% had inadequate health literacy and that patients with diabetes with inadequate health literacy were more likely to have poor glycemic control compared with patients with diabetes and adequate health literacy levels.4 McCleary-Jones examined diet, foot care, and exercise of 50 African American participants with diabetes from a community health center, finding a positive relationship between health literacy and diabetes knowledge.11
Long and Gambling conducted a 2-year prospective, observational study that incorporated motivational interviewing and patient-centered care into a self-management program, examining the effectiveness of scheduled phone interventions to assist patients with diabetes in the management of their disease.12 The interventions used structured and consistent questions supported by a protocol and script that examined medication adherence and lifestyle choices. Long and Gambling concluded that “the findings demonstrate not only changes in the depth and detail of diabetes-related knowledge and confidence, but also enhanced competence in translating knowledge into every day self-care.”12 These researchers concluded that increased knowledge translated into better patient self-management of their disease. The Long and Gambling study included general self-management characteristics of monitoring HbA1c, diet, exercise, medication management, and general self-care. These researchers contend that diabetes self-management education must be a long-term endeavor to promote change.12
Mendoza and Rosenburg’s meta-analysis on self-management programs for diabetes and chronic conditions found a statistically significant 0.81% reduction in hemoglobin A1c (HbA1c). Characteristics of self-management programs that were linked to improved outcomes included nurse and provider education on medications, diet and/or exercise, and demonstrated use of motivational interviewing and biofeedback. Mendoza and Rosenburg suggested motivational interviewing focuses on the patient’s perspective and facilitates the process that the patient uses to assess their needs and to think about possible solutions.13 Mulimba and Bryo-Daniel found that motivational interviewing is a valuable tool for primary care nurses’ health promotion practice, and Thompson and colleagues found that it was effective in changing behavior.14,15
Nurse’s Role in Health Literacy
Nurses play a vital role in educating and securing adherence of patients in the management of their disease(s).13 In addition to educating patients, families, and friends of the family, nurses assist with helping them make informed decisions.16 The VHA uses the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) to teach health care staff about diabetes self-management education (DSME). Tisdel and colleagues found that DSME established through telemedicine or clinical mentoring improved patient outcomes.17 Mendoza and Rosenburgfound nurse-led DSME was linked to minimizing cardiovascular risk factors and improvements in HbA1c.13
Background
Staunton Community Based Outpatient Clinic (CBOC) in rural Virginia is a primary care clinic that serves veterans in the surrounding area. About one-fourth of the Staunton patients have diabetes. According to June 2014 data from the VHA Support Service Center, the physician at the Staunton CBOC was responsible for 946 patients (225 with diabetes) and the nurse practitioner was responsible for 707 (184 with diabetes). The VHA Support Service Center 2014 data indicated that veterans with poorly self-managed diabetes were at increased risk for poor outcomes, such as kidney failure, cardiovascular disease, and limb amputation. Veterans with diabetes use the emergency department more often and are admitted to the hospital more often than are veterans who do not have diabetes.18
Methods
The primary objective of this pilot study was to explore whether weekly structured nursing education sessions lasting 45 minutes and subsequent follow-up weekly conferences would improve their HbA1c for veterans identified as having ≥ 9 HbA1c and ≤ 3 health literacy score on the NVS 7 study assessment. Most recent HbA1c prior to beginning the study was used to identify potential participants. After completion of 12 weekly education interventions, an additional HbA1c was obtained.
The Salem VAMC and Eastern Mennonite University Institutional Review Board approved the study. Veterans’ questions were answered prior to signing consent forms. All data collected were kept confidential.
Veterans with ≥ 9 HbA1c were evaluated for possible participation. Forty-nine veterans met the criteria to participate in this pilot study. Exclusion criteria included diagnosis of any cognitive disorder, such as dementia, Alzheimer disease, or memory impairment. In addition, veterans unwilling or unable to commit to weekly follow-up sessions were excluded. The veterans eligible for participation were contacted by telephone, and 9 agreed to participate in the pilot study. Inclusion criteria included those aged ≥ 18 years and a diagnosis of diabetes with most recent HbA1c of ≥ 9 and a score of < 4 on the NVS health literacy assessment. After taking the NVS health literacy assessment, 6 of the 9 participants qualified to continue in the study.
Education interventions included assessing medication adherence, discussing diet, reviewing physical activity for the previous week (based on diet and activity logs), and reviewing home blood glucose monitoring. Weekly education sessions were either face-to-face or by telephone. This choice was given to accommodate veterans who may have had transportation issues. A total of 12 weekly appointments were scheduled for each participant, and education was directed at the specific needs and goals of each participant. Interventions for education were based on those found in previous studies.13,14,18,19
Data Collection and Analysis
All 6 participants were white male veterans who were diagnosed with diabetes for at least 3 years. Their ages ranged from 59 to 72. Three participants were service connected for diabetes and 3 were not. One participant dropped from the study after completing 4 appointments, stating he was just too busy to be available for a weekly appointment. Another participant completed 6 appointments and removed himself from the study due to time constraints. The 4 participants who completed the pilot study were followed for 12 weeks by a registered nurse (RN), and all had reductions in their HbA1c.
Participants were assessed at weekly appointments using a predetermined template for medication adherence, diet, activity, and blood glucose monitoring. Responses of the participants guided the education interventions to meet the individual veteran’s learning needs. For example, one veteran was given specific education on carbohydrate counting and another was educated on how to read food labels. Participants were also encouraged to express satisfaction, frustration, anger, or other emotions in managing their chronic illness. The premise for spending additional time with the veteran was to promote positive self-management behaviors as recommended by Radhakrishnan.19
Veterans who completed the study stated that the education interventions positively impacted their health status. One veteran was able to delay dialysis due to self-directed improvement in his lifestyle (exercising and watching his diet), which improved his HbA1c. This veteran attributed his health improvement to the individualized education sessions with the RN and knowing he had to be accountable to someone. Additionally, it was found there was a strong familial-social component to diabetes self-management. Several veterans were knowledgeable about diabetes self-management as evidenced by their responses to weekly questions. However, disease management for these veterans was strongly impacted by family and life events.
One veteran did not manage his disease for an entire week due to “being busy with a death in the family and planning for a wedding.” This veteran took his medication but did not check his blood glucose or monitor his diet. Another veteran spoke of eating ice cream and other concentrated sweets because his young grandson was with him for the week. A third veteran was able to manage his diet better when his wife packed snacks for him but when left to his own accord did not do well with his food selection. Even though these veterans understood how to effectively manage their diabetes, they may have chosen to inconsistently translate that knowledge into practice if they perceive those familial-social forces to be more important or more powerful.
Discussion
The findings from this small pilot study from a single clinic cannot be generalized. However, this pilot study adds to the literature of the positive impact of individualized, structured, tailored nursing interventions delivered with careful consideration of the participants’ personal goals and health care needs for diabetes self-management.
Participants monitored home blood glucose levels, diet, and activity and maintained adherence with prescribed diabetes medications. The HbA1c level for participants decreased by the end of the program. During the course of the pilot study a pharmacist managed the veterans’ medications. Participant 1 began a new medication regimen the first day of the study. Previously, the patient was self-regulating his medication. However, during the 12-week study, he had no medication adjustments. Participant 4 had several increases to his insulin dose (insulin aspart protamine and insulin aspart rdna origin) during the course of the study. Participants 5 and 6 had no medication adjustments during the study.
Even though participants had medication adjustments, which contributed to the HbA1c decrease, they became more aware of the medical need to control their blood sugar through the one-on-one education provided. Although there was variation in the depth and detail that participants maintained their food/activity log and home blood glucose monitoring, all participants agreed that they were more likely to be adherent with prescribed self-monitoring “knowing they were going to have to report self-monitoring information” to the RN.
Health care professionals may not realize the impact of familial-social events on blood glucose control. Veterans in this study found that having weekly sessions with the RN helped them through such events, even though they did not adhere strictly to their regimen. One suggestion is having veterans anticipate future familial-social events that may trigger nonadherence to their diabetes health plan and then discuss those events with the health care professional.
Future Research
This small exploratory pilot study has implications for future research. Increasing the study’s sample size and using a control group is recommended to compare veterans who have an educational intervention with those that do not and the impact it has on blood glucose control. The study was limited to 1 CBOC. Incorporating additional CBOCs could increase the sample size. Additionally, although this study was only 3 months in duration, a longer study could reveal significant patterns of change over time as well as the long-term benefit of a tailored educational intervention. In addition, adjusting the study inclusion criteria of > 9 HbA1c to include those with > 8 HbA1c also may increase the sample size.
Limited financial resources for the study could have negatively impacted the sample size. Incorporating recruitment or advertising strategy may increase the number of participants. Research also is needed on education interventions with a diverse group of male and female veterans that extends beyond 3 months. Exploring the value of including the veteran’s family in the education sessions is needed. Finally, this study examined only diabetes education. Researchers need to consider other diseases and the value of individualized education.
Limitations
Limitations included a small sample size and no control group. Due to the study’s small sample size, extrapolating data from it becomes difficult. However, this pilot study sets the groundwork for other researchers to expand the importance of education interventions and health literacy. Recruitment was challenging since an eligibility criterion was the NVS score, and patients were sometimes difficult to contact.7 The pilot study started with 6 white male participants but only 4 finished. During the course of the pilot study, 1 veteran had medication adjustments as part of routine care and 1 veteran had medication adjustments prior to the study, which could have altered the HbA1c results.
In hindsight, using the NVS to assess both prestudy with poststudy health literacy scores would have provided additional information about the education intervention. There is possible bias because the researcher was a VAMC employee, and the RN that implemented the interventions had previously worked with the patients.
Conclusion
Although this is a small descriptive pilot study, it adds to the body of research on the value of nurse-driven interventions to help veterans manage diabetes by enhancing their health literacy. It also raises questions and opportunities for further research into the power of familial-social influences on a veteran’s willingness to manage their diabetes. The majority of veterans who declined to participate in this study, even though they qualified, stated that they would “not follow any recommendations.” Further investigation is needed about why some veterans elect not to obtain help that could positively impact their health and possibly extend their life. Additionally, scientific quantitative and qualitative research is needed to evaluate the statistical significance between health care literacy and educational intervention on patient adherence among individuals diagnosed with diabetes.
1. Stiles E. Promoting health literacy in patients with diabetes. Nurs Stand. 2011;26(8):35-40.
2. Baum NH, Dowling RA. Health literacy: how do your patients rate? http://urologytimes.modernmedicine.com/urology-times/news/modernmedicine/modern-medicine-now/health-literacy-how-do-your-patients-rate. Published August 1, 2011. Accessed December 2, 2016.
3. Escobedo W, Weismuller P. Assessing health literacy in renal failure and kidney transplant patients. Prog Transplant. 2013;23(1):47-54.
4. Heinrich C. Health literacy: the sixth vital sign. J Am Acad Nurse Pract. 2012;24(4):218-223.
5. Roett MA, Wessel L. Help your patient “get” what you just said: health literacy guide. J Fam Pract. 2012;61(4):190-196.
6. American Diabetes Association. Statistics about diabetes. http://www.diabetes.org/diabetes-basics/statistics/?loc=feat1.Updated December 12, 2016. Accessed December 14, 2016.
7. Pfizer. The newest vital sign. http://www.pfizer.com/files/health/nvs_flipbook_english_final.pdf. Published February 2011. Accessed December 2, 2016.
8. Shah LC, West P, Bremmeyr K, Savoy-Moore RT. Health literacy instrument in family medicine: the “newest vital sign” ease of use and correlates. J Am Board Fam Med. 2010;23(2):195-203.
9. Welch VL, VanGeest JB, Caskey R. Time, costs, and clinical utilization of screening for health literacy: a case study using the Newest Vital Sign (NVS) instrument. J Am Board Fam Med. 2011;24(3):281-289.
10. Ryan JG, Leguen F, Weiss BD, et al. Will patients agree to have their literacy skills assessed in clinical practice? Health Educ Res. 2008;23(4):603-611.
11. McCleary-Jones V. Health literacy and its association with diabetes knowledge, self-efficacy and disease self-management among African Americans with diabetes mellitus. ABNF J. 2011;22(2):25-32.
12. Long AF, Gambling T. Enhancing health literacy and behavioral change within a tele-care education and support intervention for people with type 2 diabetes. Health Expect. 2012;15(3):267-282.
13. Mendoza M, Rosenberg T. Self-management of type 2 diabetes: A good idea-or not? J Fam Pract. 2013;62(5):244-248.
14. A Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs. 2014;23(1):8-14.
15. Thompson DR, Chair SY, Chan SW, Astin F, Davidson PM, Ski CF. Motivational interviewing: a useful approach to improving cardiovascular health? J Clin Nurs. 2011;20;(9-10):1236-1244.
16. Protheroe J, Rowlands G. Matching clinical information with levels of patient health literacy. Nurs Manag (Harrow). 2013;20(3):20-21.
17. Tisdel KA, Bedwell M, Tarkington PE, Mundy A, Fredrickson SK. Diabetes specialists share experience remotely with RN care managers. Fed Pract. 2013;30(suppl 7):15S-20S.
18. U.S. Department of Veterans Affairs, Veterans Health Administration Support Service Center. http://vssc.med.va.gov/AlphaIndex.asp?Ltr=D.
19. Radhakrishnan K. The efficacy of tailored interventions for self-management outcomes of type 2 diabetes, hypertension, or heart disease: a systemic review. J Adv Nurs. 2012;68(3):496-510.
According to the National Academy of Medicine (NAM), health literacy is “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions.”1 Studies suggest that millions of patients have inadequate health literacy and cannot make fully informed decisions because of this lack of knowledge.2-4 A 2007 National Patient Safety Foundation report calculated that inadequate health literacy burdens the U.S. health care system with an additional $106 to $238 billion annually.5
In 2014, the American Diabetes Association reported that diabetes affects 29.1 million Americans (9.3%) and that by 2050 1 in 3 Americans will have diabetes.6 People with diabetes have health care costs 2.3 times higher than the cost for nondiabetic patients. The cost of taking care of patients with diabetes annually is about $245 billion.6 Without interventions that address health literacy and effective self-management to reduce the risks of complications and comorbidity, health care costs related to diabetes will continue to increase.
Literature Review
According to a U.S. Department of Education assessment on adult health literacy in 2003, 88% of adults in the U.S. have inadequate health literacy.2 About 90 million Americans lack health literacy skills, according to a 2004 NAM report.3 Heinrich, who conducted a review of U.S. studies on health literacy, concluded that about 25% of Americans have low health literacy.4
The Newest Vital Sign Tool
The Newest Vital Sign (NVS) tool is a free tool developed by Pfizer (New York, NY) for assessing health literacy. Participants are asked 6 questions about nutrition based on an ice cream nutrition label (Figure). The researcher records the participant’s responses, which accommodates participants who may have difficulty reading. The tool is scored from 0 to 6. A score of below 4 indicates the possibility of limited health literacy.7 This test can be completed in about 3 minutes, is widely accepted, and provides results comparable to more extensive literacy tests.8 A study conducted by Welch and colleagues suggested the NVS tool is both cost and time efficient.9 Ryan and colleagues found that 98% of patients in their study (n = 289) did not have objections to taking the NVS assessment.10
Escobedo and Weismuller’s study used the NVS health literacy tool to assess the health literacy of renal patients.3 In 2004, about 50,000 American patients with diabetes began treatment for kidney failure due to diabetes complications.6 Escobedo and Weismuller found that patients with diabetes with limited health literacy knowledge are more likely to be hospitalized, thus increasing health care costs.3 In addition, they discovered that these patients demonstrated poor adherence to prescribed treatment protocols. Welch, VanGeest, and Caskey conducted a case study on time, cost, and clinical utilization of the NVS health literacy tool and found that a patient’s lack of health literacy was linked to limited participation in personal medical decisions.7,9 Patient’s lack of knowledge was associated with delays in seeking treatment, poor self-management of the disease, and more hospital admissions.
Health Literacy and Diabetes
Studies specific to diabetes and inadequate health literacy support the premise that better health literacy leads to improved patient outcomes. Using the NVS tool, Heinrich conducted a study of the health literacy of 54 patients with diabetes in a primary care setting. The study showed that 65% had inadequate health literacy and that patients with diabetes with inadequate health literacy were more likely to have poor glycemic control compared with patients with diabetes and adequate health literacy levels.4 McCleary-Jones examined diet, foot care, and exercise of 50 African American participants with diabetes from a community health center, finding a positive relationship between health literacy and diabetes knowledge.11
Long and Gambling conducted a 2-year prospective, observational study that incorporated motivational interviewing and patient-centered care into a self-management program, examining the effectiveness of scheduled phone interventions to assist patients with diabetes in the management of their disease.12 The interventions used structured and consistent questions supported by a protocol and script that examined medication adherence and lifestyle choices. Long and Gambling concluded that “the findings demonstrate not only changes in the depth and detail of diabetes-related knowledge and confidence, but also enhanced competence in translating knowledge into every day self-care.”12 These researchers concluded that increased knowledge translated into better patient self-management of their disease. The Long and Gambling study included general self-management characteristics of monitoring HbA1c, diet, exercise, medication management, and general self-care. These researchers contend that diabetes self-management education must be a long-term endeavor to promote change.12
Mendoza and Rosenburg’s meta-analysis on self-management programs for diabetes and chronic conditions found a statistically significant 0.81% reduction in hemoglobin A1c (HbA1c). Characteristics of self-management programs that were linked to improved outcomes included nurse and provider education on medications, diet and/or exercise, and demonstrated use of motivational interviewing and biofeedback. Mendoza and Rosenburg suggested motivational interviewing focuses on the patient’s perspective and facilitates the process that the patient uses to assess their needs and to think about possible solutions.13 Mulimba and Bryo-Daniel found that motivational interviewing is a valuable tool for primary care nurses’ health promotion practice, and Thompson and colleagues found that it was effective in changing behavior.14,15
Nurse’s Role in Health Literacy
Nurses play a vital role in educating and securing adherence of patients in the management of their disease(s).13 In addition to educating patients, families, and friends of the family, nurses assist with helping them make informed decisions.16 The VHA uses the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) to teach health care staff about diabetes self-management education (DSME). Tisdel and colleagues found that DSME established through telemedicine or clinical mentoring improved patient outcomes.17 Mendoza and Rosenburgfound nurse-led DSME was linked to minimizing cardiovascular risk factors and improvements in HbA1c.13
Background
Staunton Community Based Outpatient Clinic (CBOC) in rural Virginia is a primary care clinic that serves veterans in the surrounding area. About one-fourth of the Staunton patients have diabetes. According to June 2014 data from the VHA Support Service Center, the physician at the Staunton CBOC was responsible for 946 patients (225 with diabetes) and the nurse practitioner was responsible for 707 (184 with diabetes). The VHA Support Service Center 2014 data indicated that veterans with poorly self-managed diabetes were at increased risk for poor outcomes, such as kidney failure, cardiovascular disease, and limb amputation. Veterans with diabetes use the emergency department more often and are admitted to the hospital more often than are veterans who do not have diabetes.18
Methods
The primary objective of this pilot study was to explore whether weekly structured nursing education sessions lasting 45 minutes and subsequent follow-up weekly conferences would improve their HbA1c for veterans identified as having ≥ 9 HbA1c and ≤ 3 health literacy score on the NVS 7 study assessment. Most recent HbA1c prior to beginning the study was used to identify potential participants. After completion of 12 weekly education interventions, an additional HbA1c was obtained.
The Salem VAMC and Eastern Mennonite University Institutional Review Board approved the study. Veterans’ questions were answered prior to signing consent forms. All data collected were kept confidential.
Veterans with ≥ 9 HbA1c were evaluated for possible participation. Forty-nine veterans met the criteria to participate in this pilot study. Exclusion criteria included diagnosis of any cognitive disorder, such as dementia, Alzheimer disease, or memory impairment. In addition, veterans unwilling or unable to commit to weekly follow-up sessions were excluded. The veterans eligible for participation were contacted by telephone, and 9 agreed to participate in the pilot study. Inclusion criteria included those aged ≥ 18 years and a diagnosis of diabetes with most recent HbA1c of ≥ 9 and a score of < 4 on the NVS health literacy assessment. After taking the NVS health literacy assessment, 6 of the 9 participants qualified to continue in the study.
Education interventions included assessing medication adherence, discussing diet, reviewing physical activity for the previous week (based on diet and activity logs), and reviewing home blood glucose monitoring. Weekly education sessions were either face-to-face or by telephone. This choice was given to accommodate veterans who may have had transportation issues. A total of 12 weekly appointments were scheduled for each participant, and education was directed at the specific needs and goals of each participant. Interventions for education were based on those found in previous studies.13,14,18,19
Data Collection and Analysis
All 6 participants were white male veterans who were diagnosed with diabetes for at least 3 years. Their ages ranged from 59 to 72. Three participants were service connected for diabetes and 3 were not. One participant dropped from the study after completing 4 appointments, stating he was just too busy to be available for a weekly appointment. Another participant completed 6 appointments and removed himself from the study due to time constraints. The 4 participants who completed the pilot study were followed for 12 weeks by a registered nurse (RN), and all had reductions in their HbA1c.
Participants were assessed at weekly appointments using a predetermined template for medication adherence, diet, activity, and blood glucose monitoring. Responses of the participants guided the education interventions to meet the individual veteran’s learning needs. For example, one veteran was given specific education on carbohydrate counting and another was educated on how to read food labels. Participants were also encouraged to express satisfaction, frustration, anger, or other emotions in managing their chronic illness. The premise for spending additional time with the veteran was to promote positive self-management behaviors as recommended by Radhakrishnan.19
Veterans who completed the study stated that the education interventions positively impacted their health status. One veteran was able to delay dialysis due to self-directed improvement in his lifestyle (exercising and watching his diet), which improved his HbA1c. This veteran attributed his health improvement to the individualized education sessions with the RN and knowing he had to be accountable to someone. Additionally, it was found there was a strong familial-social component to diabetes self-management. Several veterans were knowledgeable about diabetes self-management as evidenced by their responses to weekly questions. However, disease management for these veterans was strongly impacted by family and life events.
One veteran did not manage his disease for an entire week due to “being busy with a death in the family and planning for a wedding.” This veteran took his medication but did not check his blood glucose or monitor his diet. Another veteran spoke of eating ice cream and other concentrated sweets because his young grandson was with him for the week. A third veteran was able to manage his diet better when his wife packed snacks for him but when left to his own accord did not do well with his food selection. Even though these veterans understood how to effectively manage their diabetes, they may have chosen to inconsistently translate that knowledge into practice if they perceive those familial-social forces to be more important or more powerful.
Discussion
The findings from this small pilot study from a single clinic cannot be generalized. However, this pilot study adds to the literature of the positive impact of individualized, structured, tailored nursing interventions delivered with careful consideration of the participants’ personal goals and health care needs for diabetes self-management.
Participants monitored home blood glucose levels, diet, and activity and maintained adherence with prescribed diabetes medications. The HbA1c level for participants decreased by the end of the program. During the course of the pilot study a pharmacist managed the veterans’ medications. Participant 1 began a new medication regimen the first day of the study. Previously, the patient was self-regulating his medication. However, during the 12-week study, he had no medication adjustments. Participant 4 had several increases to his insulin dose (insulin aspart protamine and insulin aspart rdna origin) during the course of the study. Participants 5 and 6 had no medication adjustments during the study.
Even though participants had medication adjustments, which contributed to the HbA1c decrease, they became more aware of the medical need to control their blood sugar through the one-on-one education provided. Although there was variation in the depth and detail that participants maintained their food/activity log and home blood glucose monitoring, all participants agreed that they were more likely to be adherent with prescribed self-monitoring “knowing they were going to have to report self-monitoring information” to the RN.
Health care professionals may not realize the impact of familial-social events on blood glucose control. Veterans in this study found that having weekly sessions with the RN helped them through such events, even though they did not adhere strictly to their regimen. One suggestion is having veterans anticipate future familial-social events that may trigger nonadherence to their diabetes health plan and then discuss those events with the health care professional.
Future Research
This small exploratory pilot study has implications for future research. Increasing the study’s sample size and using a control group is recommended to compare veterans who have an educational intervention with those that do not and the impact it has on blood glucose control. The study was limited to 1 CBOC. Incorporating additional CBOCs could increase the sample size. Additionally, although this study was only 3 months in duration, a longer study could reveal significant patterns of change over time as well as the long-term benefit of a tailored educational intervention. In addition, adjusting the study inclusion criteria of > 9 HbA1c to include those with > 8 HbA1c also may increase the sample size.
Limited financial resources for the study could have negatively impacted the sample size. Incorporating recruitment or advertising strategy may increase the number of participants. Research also is needed on education interventions with a diverse group of male and female veterans that extends beyond 3 months. Exploring the value of including the veteran’s family in the education sessions is needed. Finally, this study examined only diabetes education. Researchers need to consider other diseases and the value of individualized education.
Limitations
Limitations included a small sample size and no control group. Due to the study’s small sample size, extrapolating data from it becomes difficult. However, this pilot study sets the groundwork for other researchers to expand the importance of education interventions and health literacy. Recruitment was challenging since an eligibility criterion was the NVS score, and patients were sometimes difficult to contact.7 The pilot study started with 6 white male participants but only 4 finished. During the course of the pilot study, 1 veteran had medication adjustments as part of routine care and 1 veteran had medication adjustments prior to the study, which could have altered the HbA1c results.
In hindsight, using the NVS to assess both prestudy with poststudy health literacy scores would have provided additional information about the education intervention. There is possible bias because the researcher was a VAMC employee, and the RN that implemented the interventions had previously worked with the patients.
Conclusion
Although this is a small descriptive pilot study, it adds to the body of research on the value of nurse-driven interventions to help veterans manage diabetes by enhancing their health literacy. It also raises questions and opportunities for further research into the power of familial-social influences on a veteran’s willingness to manage their diabetes. The majority of veterans who declined to participate in this study, even though they qualified, stated that they would “not follow any recommendations.” Further investigation is needed about why some veterans elect not to obtain help that could positively impact their health and possibly extend their life. Additionally, scientific quantitative and qualitative research is needed to evaluate the statistical significance between health care literacy and educational intervention on patient adherence among individuals diagnosed with diabetes.
According to the National Academy of Medicine (NAM), health literacy is “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions.”1 Studies suggest that millions of patients have inadequate health literacy and cannot make fully informed decisions because of this lack of knowledge.2-4 A 2007 National Patient Safety Foundation report calculated that inadequate health literacy burdens the U.S. health care system with an additional $106 to $238 billion annually.5
In 2014, the American Diabetes Association reported that diabetes affects 29.1 million Americans (9.3%) and that by 2050 1 in 3 Americans will have diabetes.6 People with diabetes have health care costs 2.3 times higher than the cost for nondiabetic patients. The cost of taking care of patients with diabetes annually is about $245 billion.6 Without interventions that address health literacy and effective self-management to reduce the risks of complications and comorbidity, health care costs related to diabetes will continue to increase.
Literature Review
According to a U.S. Department of Education assessment on adult health literacy in 2003, 88% of adults in the U.S. have inadequate health literacy.2 About 90 million Americans lack health literacy skills, according to a 2004 NAM report.3 Heinrich, who conducted a review of U.S. studies on health literacy, concluded that about 25% of Americans have low health literacy.4
The Newest Vital Sign Tool
The Newest Vital Sign (NVS) tool is a free tool developed by Pfizer (New York, NY) for assessing health literacy. Participants are asked 6 questions about nutrition based on an ice cream nutrition label (Figure). The researcher records the participant’s responses, which accommodates participants who may have difficulty reading. The tool is scored from 0 to 6. A score of below 4 indicates the possibility of limited health literacy.7 This test can be completed in about 3 minutes, is widely accepted, and provides results comparable to more extensive literacy tests.8 A study conducted by Welch and colleagues suggested the NVS tool is both cost and time efficient.9 Ryan and colleagues found that 98% of patients in their study (n = 289) did not have objections to taking the NVS assessment.10
Escobedo and Weismuller’s study used the NVS health literacy tool to assess the health literacy of renal patients.3 In 2004, about 50,000 American patients with diabetes began treatment for kidney failure due to diabetes complications.6 Escobedo and Weismuller found that patients with diabetes with limited health literacy knowledge are more likely to be hospitalized, thus increasing health care costs.3 In addition, they discovered that these patients demonstrated poor adherence to prescribed treatment protocols. Welch, VanGeest, and Caskey conducted a case study on time, cost, and clinical utilization of the NVS health literacy tool and found that a patient’s lack of health literacy was linked to limited participation in personal medical decisions.7,9 Patient’s lack of knowledge was associated with delays in seeking treatment, poor self-management of the disease, and more hospital admissions.
Health Literacy and Diabetes
Studies specific to diabetes and inadequate health literacy support the premise that better health literacy leads to improved patient outcomes. Using the NVS tool, Heinrich conducted a study of the health literacy of 54 patients with diabetes in a primary care setting. The study showed that 65% had inadequate health literacy and that patients with diabetes with inadequate health literacy were more likely to have poor glycemic control compared with patients with diabetes and adequate health literacy levels.4 McCleary-Jones examined diet, foot care, and exercise of 50 African American participants with diabetes from a community health center, finding a positive relationship between health literacy and diabetes knowledge.11
Long and Gambling conducted a 2-year prospective, observational study that incorporated motivational interviewing and patient-centered care into a self-management program, examining the effectiveness of scheduled phone interventions to assist patients with diabetes in the management of their disease.12 The interventions used structured and consistent questions supported by a protocol and script that examined medication adherence and lifestyle choices. Long and Gambling concluded that “the findings demonstrate not only changes in the depth and detail of diabetes-related knowledge and confidence, but also enhanced competence in translating knowledge into every day self-care.”12 These researchers concluded that increased knowledge translated into better patient self-management of their disease. The Long and Gambling study included general self-management characteristics of monitoring HbA1c, diet, exercise, medication management, and general self-care. These researchers contend that diabetes self-management education must be a long-term endeavor to promote change.12
Mendoza and Rosenburg’s meta-analysis on self-management programs for diabetes and chronic conditions found a statistically significant 0.81% reduction in hemoglobin A1c (HbA1c). Characteristics of self-management programs that were linked to improved outcomes included nurse and provider education on medications, diet and/or exercise, and demonstrated use of motivational interviewing and biofeedback. Mendoza and Rosenburg suggested motivational interviewing focuses on the patient’s perspective and facilitates the process that the patient uses to assess their needs and to think about possible solutions.13 Mulimba and Bryo-Daniel found that motivational interviewing is a valuable tool for primary care nurses’ health promotion practice, and Thompson and colleagues found that it was effective in changing behavior.14,15
Nurse’s Role in Health Literacy
Nurses play a vital role in educating and securing adherence of patients in the management of their disease(s).13 In addition to educating patients, families, and friends of the family, nurses assist with helping them make informed decisions.16 The VHA uses the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) to teach health care staff about diabetes self-management education (DSME). Tisdel and colleagues found that DSME established through telemedicine or clinical mentoring improved patient outcomes.17 Mendoza and Rosenburgfound nurse-led DSME was linked to minimizing cardiovascular risk factors and improvements in HbA1c.13
Background
Staunton Community Based Outpatient Clinic (CBOC) in rural Virginia is a primary care clinic that serves veterans in the surrounding area. About one-fourth of the Staunton patients have diabetes. According to June 2014 data from the VHA Support Service Center, the physician at the Staunton CBOC was responsible for 946 patients (225 with diabetes) and the nurse practitioner was responsible for 707 (184 with diabetes). The VHA Support Service Center 2014 data indicated that veterans with poorly self-managed diabetes were at increased risk for poor outcomes, such as kidney failure, cardiovascular disease, and limb amputation. Veterans with diabetes use the emergency department more often and are admitted to the hospital more often than are veterans who do not have diabetes.18
Methods
The primary objective of this pilot study was to explore whether weekly structured nursing education sessions lasting 45 minutes and subsequent follow-up weekly conferences would improve their HbA1c for veterans identified as having ≥ 9 HbA1c and ≤ 3 health literacy score on the NVS 7 study assessment. Most recent HbA1c prior to beginning the study was used to identify potential participants. After completion of 12 weekly education interventions, an additional HbA1c was obtained.
The Salem VAMC and Eastern Mennonite University Institutional Review Board approved the study. Veterans’ questions were answered prior to signing consent forms. All data collected were kept confidential.
Veterans with ≥ 9 HbA1c were evaluated for possible participation. Forty-nine veterans met the criteria to participate in this pilot study. Exclusion criteria included diagnosis of any cognitive disorder, such as dementia, Alzheimer disease, or memory impairment. In addition, veterans unwilling or unable to commit to weekly follow-up sessions were excluded. The veterans eligible for participation were contacted by telephone, and 9 agreed to participate in the pilot study. Inclusion criteria included those aged ≥ 18 years and a diagnosis of diabetes with most recent HbA1c of ≥ 9 and a score of < 4 on the NVS health literacy assessment. After taking the NVS health literacy assessment, 6 of the 9 participants qualified to continue in the study.
Education interventions included assessing medication adherence, discussing diet, reviewing physical activity for the previous week (based on diet and activity logs), and reviewing home blood glucose monitoring. Weekly education sessions were either face-to-face or by telephone. This choice was given to accommodate veterans who may have had transportation issues. A total of 12 weekly appointments were scheduled for each participant, and education was directed at the specific needs and goals of each participant. Interventions for education were based on those found in previous studies.13,14,18,19
Data Collection and Analysis
All 6 participants were white male veterans who were diagnosed with diabetes for at least 3 years. Their ages ranged from 59 to 72. Three participants were service connected for diabetes and 3 were not. One participant dropped from the study after completing 4 appointments, stating he was just too busy to be available for a weekly appointment. Another participant completed 6 appointments and removed himself from the study due to time constraints. The 4 participants who completed the pilot study were followed for 12 weeks by a registered nurse (RN), and all had reductions in their HbA1c.
Participants were assessed at weekly appointments using a predetermined template for medication adherence, diet, activity, and blood glucose monitoring. Responses of the participants guided the education interventions to meet the individual veteran’s learning needs. For example, one veteran was given specific education on carbohydrate counting and another was educated on how to read food labels. Participants were also encouraged to express satisfaction, frustration, anger, or other emotions in managing their chronic illness. The premise for spending additional time with the veteran was to promote positive self-management behaviors as recommended by Radhakrishnan.19
Veterans who completed the study stated that the education interventions positively impacted their health status. One veteran was able to delay dialysis due to self-directed improvement in his lifestyle (exercising and watching his diet), which improved his HbA1c. This veteran attributed his health improvement to the individualized education sessions with the RN and knowing he had to be accountable to someone. Additionally, it was found there was a strong familial-social component to diabetes self-management. Several veterans were knowledgeable about diabetes self-management as evidenced by their responses to weekly questions. However, disease management for these veterans was strongly impacted by family and life events.
One veteran did not manage his disease for an entire week due to “being busy with a death in the family and planning for a wedding.” This veteran took his medication but did not check his blood glucose or monitor his diet. Another veteran spoke of eating ice cream and other concentrated sweets because his young grandson was with him for the week. A third veteran was able to manage his diet better when his wife packed snacks for him but when left to his own accord did not do well with his food selection. Even though these veterans understood how to effectively manage their diabetes, they may have chosen to inconsistently translate that knowledge into practice if they perceive those familial-social forces to be more important or more powerful.
Discussion
The findings from this small pilot study from a single clinic cannot be generalized. However, this pilot study adds to the literature of the positive impact of individualized, structured, tailored nursing interventions delivered with careful consideration of the participants’ personal goals and health care needs for diabetes self-management.
Participants monitored home blood glucose levels, diet, and activity and maintained adherence with prescribed diabetes medications. The HbA1c level for participants decreased by the end of the program. During the course of the pilot study a pharmacist managed the veterans’ medications. Participant 1 began a new medication regimen the first day of the study. Previously, the patient was self-regulating his medication. However, during the 12-week study, he had no medication adjustments. Participant 4 had several increases to his insulin dose (insulin aspart protamine and insulin aspart rdna origin) during the course of the study. Participants 5 and 6 had no medication adjustments during the study.
Even though participants had medication adjustments, which contributed to the HbA1c decrease, they became more aware of the medical need to control their blood sugar through the one-on-one education provided. Although there was variation in the depth and detail that participants maintained their food/activity log and home blood glucose monitoring, all participants agreed that they were more likely to be adherent with prescribed self-monitoring “knowing they were going to have to report self-monitoring information” to the RN.
Health care professionals may not realize the impact of familial-social events on blood glucose control. Veterans in this study found that having weekly sessions with the RN helped them through such events, even though they did not adhere strictly to their regimen. One suggestion is having veterans anticipate future familial-social events that may trigger nonadherence to their diabetes health plan and then discuss those events with the health care professional.
Future Research
This small exploratory pilot study has implications for future research. Increasing the study’s sample size and using a control group is recommended to compare veterans who have an educational intervention with those that do not and the impact it has on blood glucose control. The study was limited to 1 CBOC. Incorporating additional CBOCs could increase the sample size. Additionally, although this study was only 3 months in duration, a longer study could reveal significant patterns of change over time as well as the long-term benefit of a tailored educational intervention. In addition, adjusting the study inclusion criteria of > 9 HbA1c to include those with > 8 HbA1c also may increase the sample size.
Limited financial resources for the study could have negatively impacted the sample size. Incorporating recruitment or advertising strategy may increase the number of participants. Research also is needed on education interventions with a diverse group of male and female veterans that extends beyond 3 months. Exploring the value of including the veteran’s family in the education sessions is needed. Finally, this study examined only diabetes education. Researchers need to consider other diseases and the value of individualized education.
Limitations
Limitations included a small sample size and no control group. Due to the study’s small sample size, extrapolating data from it becomes difficult. However, this pilot study sets the groundwork for other researchers to expand the importance of education interventions and health literacy. Recruitment was challenging since an eligibility criterion was the NVS score, and patients were sometimes difficult to contact.7 The pilot study started with 6 white male participants but only 4 finished. During the course of the pilot study, 1 veteran had medication adjustments as part of routine care and 1 veteran had medication adjustments prior to the study, which could have altered the HbA1c results.
In hindsight, using the NVS to assess both prestudy with poststudy health literacy scores would have provided additional information about the education intervention. There is possible bias because the researcher was a VAMC employee, and the RN that implemented the interventions had previously worked with the patients.
Conclusion
Although this is a small descriptive pilot study, it adds to the body of research on the value of nurse-driven interventions to help veterans manage diabetes by enhancing their health literacy. It also raises questions and opportunities for further research into the power of familial-social influences on a veteran’s willingness to manage their diabetes. The majority of veterans who declined to participate in this study, even though they qualified, stated that they would “not follow any recommendations.” Further investigation is needed about why some veterans elect not to obtain help that could positively impact their health and possibly extend their life. Additionally, scientific quantitative and qualitative research is needed to evaluate the statistical significance between health care literacy and educational intervention on patient adherence among individuals diagnosed with diabetes.
1. Stiles E. Promoting health literacy in patients with diabetes. Nurs Stand. 2011;26(8):35-40.
2. Baum NH, Dowling RA. Health literacy: how do your patients rate? http://urologytimes.modernmedicine.com/urology-times/news/modernmedicine/modern-medicine-now/health-literacy-how-do-your-patients-rate. Published August 1, 2011. Accessed December 2, 2016.
3. Escobedo W, Weismuller P. Assessing health literacy in renal failure and kidney transplant patients. Prog Transplant. 2013;23(1):47-54.
4. Heinrich C. Health literacy: the sixth vital sign. J Am Acad Nurse Pract. 2012;24(4):218-223.
5. Roett MA, Wessel L. Help your patient “get” what you just said: health literacy guide. J Fam Pract. 2012;61(4):190-196.
6. American Diabetes Association. Statistics about diabetes. http://www.diabetes.org/diabetes-basics/statistics/?loc=feat1.Updated December 12, 2016. Accessed December 14, 2016.
7. Pfizer. The newest vital sign. http://www.pfizer.com/files/health/nvs_flipbook_english_final.pdf. Published February 2011. Accessed December 2, 2016.
8. Shah LC, West P, Bremmeyr K, Savoy-Moore RT. Health literacy instrument in family medicine: the “newest vital sign” ease of use and correlates. J Am Board Fam Med. 2010;23(2):195-203.
9. Welch VL, VanGeest JB, Caskey R. Time, costs, and clinical utilization of screening for health literacy: a case study using the Newest Vital Sign (NVS) instrument. J Am Board Fam Med. 2011;24(3):281-289.
10. Ryan JG, Leguen F, Weiss BD, et al. Will patients agree to have their literacy skills assessed in clinical practice? Health Educ Res. 2008;23(4):603-611.
11. McCleary-Jones V. Health literacy and its association with diabetes knowledge, self-efficacy and disease self-management among African Americans with diabetes mellitus. ABNF J. 2011;22(2):25-32.
12. Long AF, Gambling T. Enhancing health literacy and behavioral change within a tele-care education and support intervention for people with type 2 diabetes. Health Expect. 2012;15(3):267-282.
13. Mendoza M, Rosenberg T. Self-management of type 2 diabetes: A good idea-or not? J Fam Pract. 2013;62(5):244-248.
14. A Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs. 2014;23(1):8-14.
15. Thompson DR, Chair SY, Chan SW, Astin F, Davidson PM, Ski CF. Motivational interviewing: a useful approach to improving cardiovascular health? J Clin Nurs. 2011;20;(9-10):1236-1244.
16. Protheroe J, Rowlands G. Matching clinical information with levels of patient health literacy. Nurs Manag (Harrow). 2013;20(3):20-21.
17. Tisdel KA, Bedwell M, Tarkington PE, Mundy A, Fredrickson SK. Diabetes specialists share experience remotely with RN care managers. Fed Pract. 2013;30(suppl 7):15S-20S.
18. U.S. Department of Veterans Affairs, Veterans Health Administration Support Service Center. http://vssc.med.va.gov/AlphaIndex.asp?Ltr=D.
19. Radhakrishnan K. The efficacy of tailored interventions for self-management outcomes of type 2 diabetes, hypertension, or heart disease: a systemic review. J Adv Nurs. 2012;68(3):496-510.
1. Stiles E. Promoting health literacy in patients with diabetes. Nurs Stand. 2011;26(8):35-40.
2. Baum NH, Dowling RA. Health literacy: how do your patients rate? http://urologytimes.modernmedicine.com/urology-times/news/modernmedicine/modern-medicine-now/health-literacy-how-do-your-patients-rate. Published August 1, 2011. Accessed December 2, 2016.
3. Escobedo W, Weismuller P. Assessing health literacy in renal failure and kidney transplant patients. Prog Transplant. 2013;23(1):47-54.
4. Heinrich C. Health literacy: the sixth vital sign. J Am Acad Nurse Pract. 2012;24(4):218-223.
5. Roett MA, Wessel L. Help your patient “get” what you just said: health literacy guide. J Fam Pract. 2012;61(4):190-196.
6. American Diabetes Association. Statistics about diabetes. http://www.diabetes.org/diabetes-basics/statistics/?loc=feat1.Updated December 12, 2016. Accessed December 14, 2016.
7. Pfizer. The newest vital sign. http://www.pfizer.com/files/health/nvs_flipbook_english_final.pdf. Published February 2011. Accessed December 2, 2016.
8. Shah LC, West P, Bremmeyr K, Savoy-Moore RT. Health literacy instrument in family medicine: the “newest vital sign” ease of use and correlates. J Am Board Fam Med. 2010;23(2):195-203.
9. Welch VL, VanGeest JB, Caskey R. Time, costs, and clinical utilization of screening for health literacy: a case study using the Newest Vital Sign (NVS) instrument. J Am Board Fam Med. 2011;24(3):281-289.
10. Ryan JG, Leguen F, Weiss BD, et al. Will patients agree to have their literacy skills assessed in clinical practice? Health Educ Res. 2008;23(4):603-611.
11. McCleary-Jones V. Health literacy and its association with diabetes knowledge, self-efficacy and disease self-management among African Americans with diabetes mellitus. ABNF J. 2011;22(2):25-32.
12. Long AF, Gambling T. Enhancing health literacy and behavioral change within a tele-care education and support intervention for people with type 2 diabetes. Health Expect. 2012;15(3):267-282.
13. Mendoza M, Rosenberg T. Self-management of type 2 diabetes: A good idea-or not? J Fam Pract. 2013;62(5):244-248.
14. A Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs. 2014;23(1):8-14.
15. Thompson DR, Chair SY, Chan SW, Astin F, Davidson PM, Ski CF. Motivational interviewing: a useful approach to improving cardiovascular health? J Clin Nurs. 2011;20;(9-10):1236-1244.
16. Protheroe J, Rowlands G. Matching clinical information with levels of patient health literacy. Nurs Manag (Harrow). 2013;20(3):20-21.
17. Tisdel KA, Bedwell M, Tarkington PE, Mundy A, Fredrickson SK. Diabetes specialists share experience remotely with RN care managers. Fed Pract. 2013;30(suppl 7):15S-20S.
18. U.S. Department of Veterans Affairs, Veterans Health Administration Support Service Center. http://vssc.med.va.gov/AlphaIndex.asp?Ltr=D.
19. Radhakrishnan K. The efficacy of tailored interventions for self-management outcomes of type 2 diabetes, hypertension, or heart disease: a systemic review. J Adv Nurs. 2012;68(3):496-510.