User login
Diabetes: Health Literacy Education Improves Veteran Outcomes
According to the National Academy of Medicine (NAM), health literacy is “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions.”1 Studies suggest that millions of patients have inadequate health literacy and cannot make fully informed decisions because of this lack of knowledge.2-4 A 2007 National Patient Safety Foundation report calculated that inadequate health literacy burdens the U.S. health care system with an additional $106 to $238 billion annually.5
In 2014, the American Diabetes Association reported that diabetes affects 29.1 million Americans (9.3%) and that by 2050 1 in 3 Americans will have diabetes.6 People with diabetes have health care costs 2.3 times higher than the cost for nondiabetic patients. The cost of taking care of patients with diabetes annually is about $245 billion.6 Without interventions that address health literacy and effective self-management to reduce the risks of complications and comorbidity, health care costs related to diabetes will continue to increase.
Literature Review
According to a U.S. Department of Education assessment on adult health literacy in 2003, 88% of adults in the U.S. have inadequate health literacy.2 About 90 million Americans lack health literacy skills, according to a 2004 NAM report.3 Heinrich, who conducted a review of U.S. studies on health literacy, concluded that about 25% of Americans have low health literacy.4
The Newest Vital Sign Tool
The Newest Vital Sign (NVS) tool is a free tool developed by Pfizer (New York, NY) for assessing health literacy. Participants are asked 6 questions about nutrition based on an ice cream nutrition label (Figure). The researcher records the participant’s responses, which accommodates participants who may have difficulty reading. The tool is scored from 0 to 6. A score of below 4 indicates the possibility of limited health literacy.7 This test can be completed in about 3 minutes, is widely accepted, and provides results comparable to more extensive literacy tests.8 A study conducted by Welch and colleagues suggested the NVS tool is both cost and time efficient.9 Ryan and colleagues found that 98% of patients in their study (n = 289) did not have objections to taking the NVS assessment.10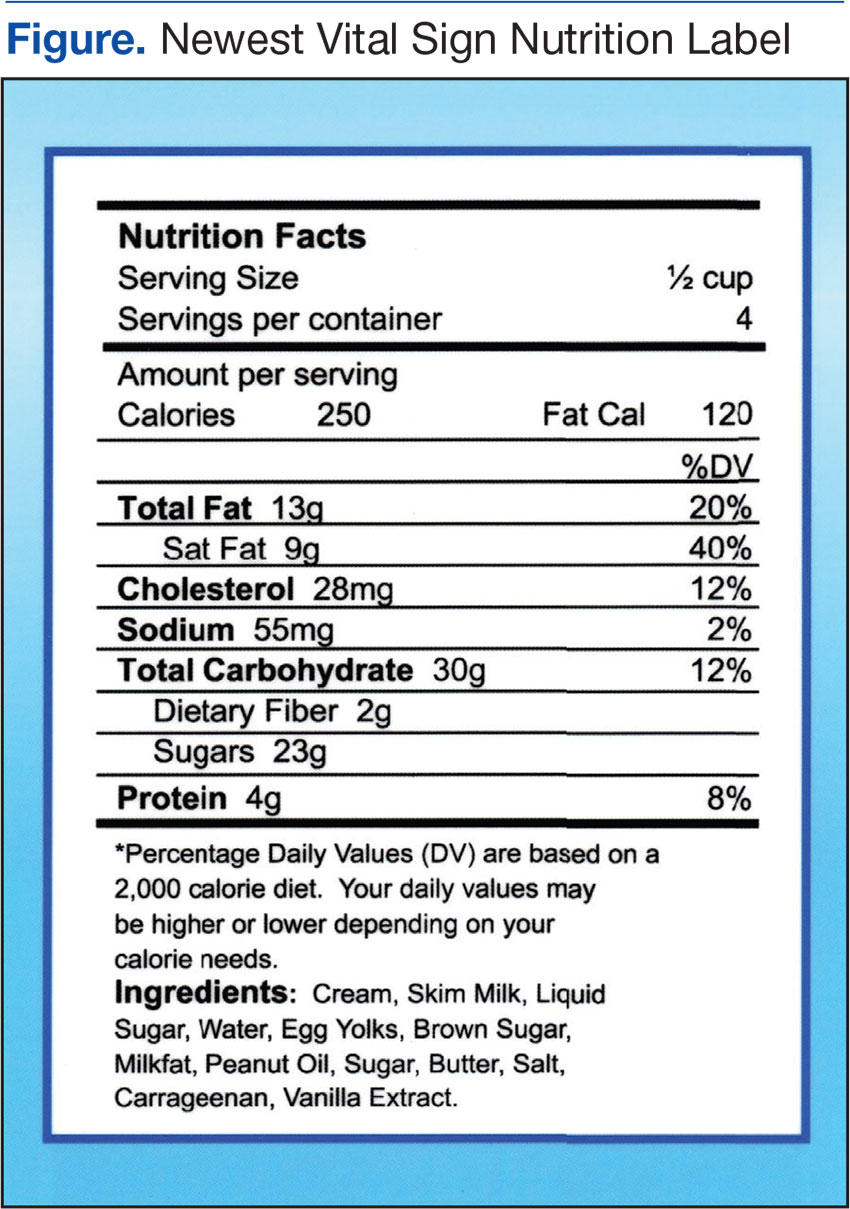
Escobedo and Weismuller’s study used the NVS health literacy tool to assess the health literacy of renal patients.3 In 2004, about 50,000 American patients with diabetes began treatment for kidney failure due to diabetes complications.6 Escobedo and Weismuller found that patients with diabetes with limited health literacy knowledge are more likely to be hospitalized, thus increasing health care costs.3 In addition, they discovered that these patients demonstrated poor adherence to prescribed treatment protocols. Welch, VanGeest, and Caskey conducted a case study on time, cost, and clinical utilization of the NVS health literacy tool and found that a patient’s lack of health literacy was linked to limited participation in personal medical decisions.7,9 Patient’s lack of knowledge was associated with delays in seeking treatment, poor self-management of the disease, and more hospital admissions.
Health Literacy and Diabetes
Studies specific to diabetes and inadequate health literacy support the premise that better health literacy leads to improved patient outcomes. Using the NVS tool, Heinrich conducted a study of the health literacy of 54 patients with diabetes in a primary care setting. The study showed that 65% had inadequate health literacy and that patients with diabetes with inadequate health literacy were more likely to have poor glycemic control compared with patients with diabetes and adequate health literacy levels.4 McCleary-Jones examined diet, foot care, and exercise of 50 African American participants with diabetes from a community health center, finding a positive relationship between health literacy and diabetes knowledge.11
Long and Gambling conducted a 2-year prospective, observational study that incorporated motivational interviewing and patient-centered care into a self-management program, examining the effectiveness of scheduled phone interventions to assist patients with diabetes in the management of their disease.12 The interventions used structured and consistent questions supported by a protocol and script that examined medication adherence and lifestyle choices. Long and Gambling concluded that “the findings demonstrate not only changes in the depth and detail of diabetes-related knowledge and confidence, but also enhanced competence in translating knowledge into every day self-care.”12 These researchers concluded that increased knowledge translated into better patient self-management of their disease. The Long and Gambling study included general self-management characteristics of monitoring HbA1c, diet, exercise, medication management, and general self-care. These researchers contend that diabetes self-management education must be a long-term endeavor to promote change.12
Mendoza and Rosenburg’s meta-analysis on self-management programs for diabetes and chronic conditions found a statistically significant 0.81% reduction in hemoglobin A1c (HbA1c). Characteristics of self-management programs that were linked to improved outcomes included nurse and provider education on medications, diet and/or exercise, and demonstrated use of motivational interviewing and biofeedback. Mendoza and Rosenburg suggested motivational interviewing focuses on the patient’s perspective and facilitates the process that the patient uses to assess their needs and to think about possible solutions.13 Mulimba and Bryo-Daniel found that motivational interviewing is a valuable tool for primary care nurses’ health promotion practice, and Thompson and colleagues found that it was effective in changing behavior.14,15
Nurse’s Role in Health Literacy
Nurses play a vital role in educating and securing adherence of patients in the management of their disease(s).13 In addition to educating patients, families, and friends of the family, nurses assist with helping them make informed decisions.16 The VHA uses the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) to teach health care staff about diabetes self-management education (DSME). Tisdel and colleagues found that DSME established through telemedicine or clinical mentoring improved patient outcomes.17 Mendoza and Rosenburgfound nurse-led DSME was linked to minimizing cardiovascular risk factors and improvements in HbA1c.13
Background
Staunton Community Based Outpatient Clinic (CBOC) in rural Virginia is a primary care clinic that serves veterans in the surrounding area. About one-fourth of the Staunton patients have diabetes. According to June 2014 data from the VHA Support Service Center, the physician at the Staunton CBOC was responsible for 946 patients (225 with diabetes) and the nurse practitioner was responsible for 707 (184 with diabetes). The VHA Support Service Center 2014 data indicated that veterans with poorly self-managed diabetes were at increased risk for poor outcomes, such as kidney failure, cardiovascular disease, and limb amputation. Veterans with diabetes use the emergency department more often and are admitted to the hospital more often than are veterans who do not have diabetes.18
Methods
The primary objective of this pilot study was to explore whether weekly structured nursing education sessions lasting 45 minutes and subsequent follow-up weekly conferences would improve their HbA1c for veterans identified as having ≥ 9 HbA1c and ≤ 3 health literacy score on the NVS 7 study assessment. Most recent HbA1c prior to beginning the study was used to identify potential participants. After completion of 12 weekly education interventions, an additional HbA1c was obtained.
The Salem VAMC and Eastern Mennonite University Institutional Review Board approved the study. Veterans’ questions were answered prior to signing consent forms. All data collected were kept confidential.
Veterans with ≥ 9 HbA1c were evaluated for possible participation. Forty-nine veterans met the criteria to participate in this pilot study. Exclusion criteria included diagnosis of any cognitive disorder, such as dementia, Alzheimer disease, or memory impairment. In addition, veterans unwilling or unable to commit to weekly follow-up sessions were excluded. The veterans eligible for participation were contacted by telephone, and 9 agreed to participate in the pilot study. Inclusion criteria included those aged ≥ 18 years and a diagnosis of diabetes with most recent HbA1c of ≥ 9 and a score of < 4 on the NVS health literacy assessment. After taking the NVS health literacy assessment, 6 of the 9 participants qualified to continue in the study.
Education interventions included assessing medication adherence, discussing diet, reviewing physical activity for the previous week (based on diet and activity logs), and reviewing home blood glucose monitoring. Weekly education sessions were either face-to-face or by telephone. This choice was given to accommodate veterans who may have had transportation issues. A total of 12 weekly appointments were scheduled for each participant, and education was directed at the specific needs and goals of each participant. Interventions for education were based on those found in previous studies.13,14,18,19
Data Collection and Analysis
All 6 participants were white male veterans who were diagnosed with diabetes for at least 3 years. Their ages ranged from 59 to 72. Three participants were service connected for diabetes and 3 were not. One participant dropped from the study after completing 4 appointments, stating he was just too busy to be available for a weekly appointment. Another participant completed 6 appointments and removed himself from the study due to time constraints. The 4 participants who completed the pilot study were followed for 12 weeks by a registered nurse (RN), and all had reductions in their HbA1c.
Participants were assessed at weekly appointments using a predetermined template for medication adherence, diet, activity, and blood glucose monitoring. Responses of the participants guided the education interventions to meet the individual veteran’s learning needs. For example, one veteran was given specific education on carbohydrate counting and another was educated on how to read food labels. Participants were also encouraged to express satisfaction, frustration, anger, or other emotions in managing their chronic illness. The premise for spending additional time with the veteran was to promote positive self-management behaviors as recommended by Radhakrishnan.19
Veterans who completed the study stated that the education interventions positively impacted their health status. One veteran was able to delay dialysis due to self-directed improvement in his lifestyle (exercising and watching his diet), which improved his HbA1c. This veteran attributed his health improvement to the individualized education sessions with the RN and knowing he had to be accountable to someone. Additionally, it was found there was a strong familial-social component to diabetes self-management. Several veterans were knowledgeable about diabetes self-management as evidenced by their responses to weekly questions. However, disease management for these veterans was strongly impacted by family and life events.
One veteran did not manage his disease for an entire week due to “being busy with a death in the family and planning for a wedding.” This veteran took his medication but did not check his blood glucose or monitor his diet. Another veteran spoke of eating ice cream and other concentrated sweets because his young grandson was with him for the week. A third veteran was able to manage his diet better when his wife packed snacks for him but when left to his own accord did not do well with his food selection. Even though these veterans understood how to effectively manage their diabetes, they may have chosen to inconsistently translate that knowledge into practice if they perceive those familial-social forces to be more important or more powerful.
Discussion
The findings from this small pilot study from a single clinic cannot be generalized. However, this pilot study adds to the literature of the positive impact of individualized, structured, tailored nursing interventions delivered with careful consideration of the participants’ personal goals and health care needs for diabetes self-management.
Participants monitored home blood glucose levels, diet, and activity and maintained adherence with prescribed diabetes medications. The HbA1c level for participants decreased by the end of the program. During the course of the pilot study a pharmacist managed the veterans’ medications. Participant 1 began a new medication regimen the first day of the study. Previously, the patient was self-regulating his medication. However, during the 12-week study, he had no medication adjustments. Participant 4 had several increases to his insulin dose (insulin aspart protamine and insulin aspart rdna origin) during the course of the study. Participants 5 and 6 had no medication adjustments during the study.
Even though participants had medication adjustments, which contributed to the HbA1c decrease, they became more aware of the medical need to control their blood sugar through the one-on-one education provided. Although there was variation in the depth and detail that participants maintained their food/activity log and home blood glucose monitoring, all participants agreed that they were more likely to be adherent with prescribed self-monitoring “knowing they were going to have to report self-monitoring information” to the RN.
Health care professionals may not realize the impact of familial-social events on blood glucose control. Veterans in this study found that having weekly sessions with the RN helped them through such events, even though they did not adhere strictly to their regimen. One suggestion is having veterans anticipate future familial-social events that may trigger nonadherence to their diabetes health plan and then discuss those events with the health care professional.
Future Research
This small exploratory pilot study has implications for future research. Increasing the study’s sample size and using a control group is recommended to compare veterans who have an educational intervention with those that do not and the impact it has on blood glucose control. The study was limited to 1 CBOC. Incorporating additional CBOCs could increase the sample size. Additionally, although this study was only 3 months in duration, a longer study could reveal significant patterns of change over time as well as the long-term benefit of a tailored educational intervention. In addition, adjusting the study inclusion criteria of > 9 HbA1c to include those with > 8 HbA1c also may increase the sample size.
Limited financial resources for the study could have negatively impacted the sample size. Incorporating recruitment or advertising strategy may increase the number of participants. Research also is needed on education interventions with a diverse group of male and female veterans that extends beyond 3 months. Exploring the value of including the veteran’s family in the education sessions is needed. Finally, this study examined only diabetes education. Researchers need to consider other diseases and the value of individualized education.
Limitations
Limitations included a small sample size and no control group. Due to the study’s small sample size, extrapolating data from it becomes difficult. However, this pilot study sets the groundwork for other researchers to expand the importance of education interventions and health literacy. Recruitment was challenging since an eligibility criterion was the NVS score, and patients were sometimes difficult to contact.7 The pilot study started with 6 white male participants but only 4 finished. During the course of the pilot study, 1 veteran had medication adjustments as part of routine care and 1 veteran had medication adjustments prior to the study, which could have altered the HbA1c results.
In hindsight, using the NVS to assess both prestudy with poststudy health literacy scores would have provided additional information about the education intervention. There is possible bias because the researcher was a VAMC employee, and the RN that implemented the interventions had previously worked with the patients.
Conclusion
Although this is a small descriptive pilot study, it adds to the body of research on the value of nurse-driven interventions to help veterans manage diabetes by enhancing their health literacy. It also raises questions and opportunities for further research into the power of familial-social influences on a veteran’s willingness to manage their diabetes. The majority of veterans who declined to participate in this study, even though they qualified, stated that they would “not follow any recommendations.” Further investigation is needed about why some veterans elect not to obtain help that could positively impact their health and possibly extend their life. Additionally, scientific quantitative and qualitative research is needed to evaluate the statistical significance between health care literacy and educational intervention on patient adherence among individuals diagnosed with diabetes.
1. Stiles E. Promoting health literacy in patients with diabetes. Nurs Stand. 2011;26(8):35-40.
2. Baum NH, Dowling RA. Health literacy: how do your patients rate? http://urologytimes.modernmedicine.com/urology-times/news/modernmedicine/modern-medicine-now/health-literacy-how-do-your-patients-rate. Published August 1, 2011. Accessed December 2, 2016.
3. Escobedo W, Weismuller P. Assessing health literacy in renal failure and kidney transplant patients. Prog Transplant. 2013;23(1):47-54.
4. Heinrich C. Health literacy: the sixth vital sign. J Am Acad Nurse Pract. 2012;24(4):218-223.
5. Roett MA, Wessel L. Help your patient “get” what you just said: health literacy guide. J Fam Pract. 2012;61(4):190-196.
6. American Diabetes Association. Statistics about diabetes. http://www.diabetes.org/diabetes-basics/statistics/?loc=feat1.Updated December 12, 2016. Accessed December 14, 2016.
7. Pfizer. The newest vital sign. http://www.pfizer.com/files/health/nvs_flipbook_english_final.pdf. Published February 2011. Accessed December 2, 2016.
8. Shah LC, West P, Bremmeyr K, Savoy-Moore RT. Health literacy instrument in family medicine: the “newest vital sign” ease of use and correlates. J Am Board Fam Med. 2010;23(2):195-203.
9. Welch VL, VanGeest JB, Caskey R. Time, costs, and clinical utilization of screening for health literacy: a case study using the Newest Vital Sign (NVS) instrument. J Am Board Fam Med. 2011;24(3):281-289.
10. Ryan JG, Leguen F, Weiss BD, et al. Will patients agree to have their literacy skills assessed in clinical practice? Health Educ Res. 2008;23(4):603-611.
11. McCleary-Jones V. Health literacy and its association with diabetes knowledge, self-efficacy and disease self-management among African Americans with diabetes mellitus. ABNF J. 2011;22(2):25-32.
12. Long AF, Gambling T. Enhancing health literacy and behavioral change within a tele-care education and support intervention for people with type 2 diabetes. Health Expect. 2012;15(3):267-282.
13. Mendoza M, Rosenberg T. Self-management of type 2 diabetes: A good idea-or not? J Fam Pract. 2013;62(5):244-248.
14. A Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs. 2014;23(1):8-14.
15. Thompson DR, Chair SY, Chan SW, Astin F, Davidson PM, Ski CF. Motivational interviewing: a useful approach to improving cardiovascular health? J Clin Nurs. 2011;20;(9-10):1236-1244.
16. Protheroe J, Rowlands G. Matching clinical information with levels of patient health literacy. Nurs Manag (Harrow). 2013;20(3):20-21.
17. Tisdel KA, Bedwell M, Tarkington PE, Mundy A, Fredrickson SK. Diabetes specialists share experience remotely with RN care managers. Fed Pract. 2013;30(suppl 7):15S-20S.
18. U.S. Department of Veterans Affairs, Veterans Health Administration Support Service Center. http://vssc.med.va.gov/AlphaIndex.asp?Ltr=D.
19. Radhakrishnan K. The efficacy of tailored interventions for self-management outcomes of type 2 diabetes, hypertension, or heart disease: a systemic review. J Adv Nurs. 2012;68(3):496-510.
According to the National Academy of Medicine (NAM), health literacy is “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions.”1 Studies suggest that millions of patients have inadequate health literacy and cannot make fully informed decisions because of this lack of knowledge.2-4 A 2007 National Patient Safety Foundation report calculated that inadequate health literacy burdens the U.S. health care system with an additional $106 to $238 billion annually.5
In 2014, the American Diabetes Association reported that diabetes affects 29.1 million Americans (9.3%) and that by 2050 1 in 3 Americans will have diabetes.6 People with diabetes have health care costs 2.3 times higher than the cost for nondiabetic patients. The cost of taking care of patients with diabetes annually is about $245 billion.6 Without interventions that address health literacy and effective self-management to reduce the risks of complications and comorbidity, health care costs related to diabetes will continue to increase.
Literature Review
According to a U.S. Department of Education assessment on adult health literacy in 2003, 88% of adults in the U.S. have inadequate health literacy.2 About 90 million Americans lack health literacy skills, according to a 2004 NAM report.3 Heinrich, who conducted a review of U.S. studies on health literacy, concluded that about 25% of Americans have low health literacy.4
The Newest Vital Sign Tool
The Newest Vital Sign (NVS) tool is a free tool developed by Pfizer (New York, NY) for assessing health literacy. Participants are asked 6 questions about nutrition based on an ice cream nutrition label (Figure). The researcher records the participant’s responses, which accommodates participants who may have difficulty reading. The tool is scored from 0 to 6. A score of below 4 indicates the possibility of limited health literacy.7 This test can be completed in about 3 minutes, is widely accepted, and provides results comparable to more extensive literacy tests.8 A study conducted by Welch and colleagues suggested the NVS tool is both cost and time efficient.9 Ryan and colleagues found that 98% of patients in their study (n = 289) did not have objections to taking the NVS assessment.10
Escobedo and Weismuller’s study used the NVS health literacy tool to assess the health literacy of renal patients.3 In 2004, about 50,000 American patients with diabetes began treatment for kidney failure due to diabetes complications.6 Escobedo and Weismuller found that patients with diabetes with limited health literacy knowledge are more likely to be hospitalized, thus increasing health care costs.3 In addition, they discovered that these patients demonstrated poor adherence to prescribed treatment protocols. Welch, VanGeest, and Caskey conducted a case study on time, cost, and clinical utilization of the NVS health literacy tool and found that a patient’s lack of health literacy was linked to limited participation in personal medical decisions.7,9 Patient’s lack of knowledge was associated with delays in seeking treatment, poor self-management of the disease, and more hospital admissions.
Health Literacy and Diabetes
Studies specific to diabetes and inadequate health literacy support the premise that better health literacy leads to improved patient outcomes. Using the NVS tool, Heinrich conducted a study of the health literacy of 54 patients with diabetes in a primary care setting. The study showed that 65% had inadequate health literacy and that patients with diabetes with inadequate health literacy were more likely to have poor glycemic control compared with patients with diabetes and adequate health literacy levels.4 McCleary-Jones examined diet, foot care, and exercise of 50 African American participants with diabetes from a community health center, finding a positive relationship between health literacy and diabetes knowledge.11
Long and Gambling conducted a 2-year prospective, observational study that incorporated motivational interviewing and patient-centered care into a self-management program, examining the effectiveness of scheduled phone interventions to assist patients with diabetes in the management of their disease.12 The interventions used structured and consistent questions supported by a protocol and script that examined medication adherence and lifestyle choices. Long and Gambling concluded that “the findings demonstrate not only changes in the depth and detail of diabetes-related knowledge and confidence, but also enhanced competence in translating knowledge into every day self-care.”12 These researchers concluded that increased knowledge translated into better patient self-management of their disease. The Long and Gambling study included general self-management characteristics of monitoring HbA1c, diet, exercise, medication management, and general self-care. These researchers contend that diabetes self-management education must be a long-term endeavor to promote change.12
Mendoza and Rosenburg’s meta-analysis on self-management programs for diabetes and chronic conditions found a statistically significant 0.81% reduction in hemoglobin A1c (HbA1c). Characteristics of self-management programs that were linked to improved outcomes included nurse and provider education on medications, diet and/or exercise, and demonstrated use of motivational interviewing and biofeedback. Mendoza and Rosenburg suggested motivational interviewing focuses on the patient’s perspective and facilitates the process that the patient uses to assess their needs and to think about possible solutions.13 Mulimba and Bryo-Daniel found that motivational interviewing is a valuable tool for primary care nurses’ health promotion practice, and Thompson and colleagues found that it was effective in changing behavior.14,15
Nurse’s Role in Health Literacy
Nurses play a vital role in educating and securing adherence of patients in the management of their disease(s).13 In addition to educating patients, families, and friends of the family, nurses assist with helping them make informed decisions.16 The VHA uses the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) to teach health care staff about diabetes self-management education (DSME). Tisdel and colleagues found that DSME established through telemedicine or clinical mentoring improved patient outcomes.17 Mendoza and Rosenburgfound nurse-led DSME was linked to minimizing cardiovascular risk factors and improvements in HbA1c.13
Background
Staunton Community Based Outpatient Clinic (CBOC) in rural Virginia is a primary care clinic that serves veterans in the surrounding area. About one-fourth of the Staunton patients have diabetes. According to June 2014 data from the VHA Support Service Center, the physician at the Staunton CBOC was responsible for 946 patients (225 with diabetes) and the nurse practitioner was responsible for 707 (184 with diabetes). The VHA Support Service Center 2014 data indicated that veterans with poorly self-managed diabetes were at increased risk for poor outcomes, such as kidney failure, cardiovascular disease, and limb amputation. Veterans with diabetes use the emergency department more often and are admitted to the hospital more often than are veterans who do not have diabetes.18
Methods
The primary objective of this pilot study was to explore whether weekly structured nursing education sessions lasting 45 minutes and subsequent follow-up weekly conferences would improve their HbA1c for veterans identified as having ≥ 9 HbA1c and ≤ 3 health literacy score on the NVS 7 study assessment. Most recent HbA1c prior to beginning the study was used to identify potential participants. After completion of 12 weekly education interventions, an additional HbA1c was obtained.
The Salem VAMC and Eastern Mennonite University Institutional Review Board approved the study. Veterans’ questions were answered prior to signing consent forms. All data collected were kept confidential.
Veterans with ≥ 9 HbA1c were evaluated for possible participation. Forty-nine veterans met the criteria to participate in this pilot study. Exclusion criteria included diagnosis of any cognitive disorder, such as dementia, Alzheimer disease, or memory impairment. In addition, veterans unwilling or unable to commit to weekly follow-up sessions were excluded. The veterans eligible for participation were contacted by telephone, and 9 agreed to participate in the pilot study. Inclusion criteria included those aged ≥ 18 years and a diagnosis of diabetes with most recent HbA1c of ≥ 9 and a score of < 4 on the NVS health literacy assessment. After taking the NVS health literacy assessment, 6 of the 9 participants qualified to continue in the study.
Education interventions included assessing medication adherence, discussing diet, reviewing physical activity for the previous week (based on diet and activity logs), and reviewing home blood glucose monitoring. Weekly education sessions were either face-to-face or by telephone. This choice was given to accommodate veterans who may have had transportation issues. A total of 12 weekly appointments were scheduled for each participant, and education was directed at the specific needs and goals of each participant. Interventions for education were based on those found in previous studies.13,14,18,19
Data Collection and Analysis
All 6 participants were white male veterans who were diagnosed with diabetes for at least 3 years. Their ages ranged from 59 to 72. Three participants were service connected for diabetes and 3 were not. One participant dropped from the study after completing 4 appointments, stating he was just too busy to be available for a weekly appointment. Another participant completed 6 appointments and removed himself from the study due to time constraints. The 4 participants who completed the pilot study were followed for 12 weeks by a registered nurse (RN), and all had reductions in their HbA1c.
Participants were assessed at weekly appointments using a predetermined template for medication adherence, diet, activity, and blood glucose monitoring. Responses of the participants guided the education interventions to meet the individual veteran’s learning needs. For example, one veteran was given specific education on carbohydrate counting and another was educated on how to read food labels. Participants were also encouraged to express satisfaction, frustration, anger, or other emotions in managing their chronic illness. The premise for spending additional time with the veteran was to promote positive self-management behaviors as recommended by Radhakrishnan.19
Veterans who completed the study stated that the education interventions positively impacted their health status. One veteran was able to delay dialysis due to self-directed improvement in his lifestyle (exercising and watching his diet), which improved his HbA1c. This veteran attributed his health improvement to the individualized education sessions with the RN and knowing he had to be accountable to someone. Additionally, it was found there was a strong familial-social component to diabetes self-management. Several veterans were knowledgeable about diabetes self-management as evidenced by their responses to weekly questions. However, disease management for these veterans was strongly impacted by family and life events.
One veteran did not manage his disease for an entire week due to “being busy with a death in the family and planning for a wedding.” This veteran took his medication but did not check his blood glucose or monitor his diet. Another veteran spoke of eating ice cream and other concentrated sweets because his young grandson was with him for the week. A third veteran was able to manage his diet better when his wife packed snacks for him but when left to his own accord did not do well with his food selection. Even though these veterans understood how to effectively manage their diabetes, they may have chosen to inconsistently translate that knowledge into practice if they perceive those familial-social forces to be more important or more powerful.
Discussion
The findings from this small pilot study from a single clinic cannot be generalized. However, this pilot study adds to the literature of the positive impact of individualized, structured, tailored nursing interventions delivered with careful consideration of the participants’ personal goals and health care needs for diabetes self-management.
Participants monitored home blood glucose levels, diet, and activity and maintained adherence with prescribed diabetes medications. The HbA1c level for participants decreased by the end of the program. During the course of the pilot study a pharmacist managed the veterans’ medications. Participant 1 began a new medication regimen the first day of the study. Previously, the patient was self-regulating his medication. However, during the 12-week study, he had no medication adjustments. Participant 4 had several increases to his insulin dose (insulin aspart protamine and insulin aspart rdna origin) during the course of the study. Participants 5 and 6 had no medication adjustments during the study.
Even though participants had medication adjustments, which contributed to the HbA1c decrease, they became more aware of the medical need to control their blood sugar through the one-on-one education provided. Although there was variation in the depth and detail that participants maintained their food/activity log and home blood glucose monitoring, all participants agreed that they were more likely to be adherent with prescribed self-monitoring “knowing they were going to have to report self-monitoring information” to the RN.
Health care professionals may not realize the impact of familial-social events on blood glucose control. Veterans in this study found that having weekly sessions with the RN helped them through such events, even though they did not adhere strictly to their regimen. One suggestion is having veterans anticipate future familial-social events that may trigger nonadherence to their diabetes health plan and then discuss those events with the health care professional.
Future Research
This small exploratory pilot study has implications for future research. Increasing the study’s sample size and using a control group is recommended to compare veterans who have an educational intervention with those that do not and the impact it has on blood glucose control. The study was limited to 1 CBOC. Incorporating additional CBOCs could increase the sample size. Additionally, although this study was only 3 months in duration, a longer study could reveal significant patterns of change over time as well as the long-term benefit of a tailored educational intervention. In addition, adjusting the study inclusion criteria of > 9 HbA1c to include those with > 8 HbA1c also may increase the sample size.
Limited financial resources for the study could have negatively impacted the sample size. Incorporating recruitment or advertising strategy may increase the number of participants. Research also is needed on education interventions with a diverse group of male and female veterans that extends beyond 3 months. Exploring the value of including the veteran’s family in the education sessions is needed. Finally, this study examined only diabetes education. Researchers need to consider other diseases and the value of individualized education.
Limitations
Limitations included a small sample size and no control group. Due to the study’s small sample size, extrapolating data from it becomes difficult. However, this pilot study sets the groundwork for other researchers to expand the importance of education interventions and health literacy. Recruitment was challenging since an eligibility criterion was the NVS score, and patients were sometimes difficult to contact.7 The pilot study started with 6 white male participants but only 4 finished. During the course of the pilot study, 1 veteran had medication adjustments as part of routine care and 1 veteran had medication adjustments prior to the study, which could have altered the HbA1c results.
In hindsight, using the NVS to assess both prestudy with poststudy health literacy scores would have provided additional information about the education intervention. There is possible bias because the researcher was a VAMC employee, and the RN that implemented the interventions had previously worked with the patients.
Conclusion
Although this is a small descriptive pilot study, it adds to the body of research on the value of nurse-driven interventions to help veterans manage diabetes by enhancing their health literacy. It also raises questions and opportunities for further research into the power of familial-social influences on a veteran’s willingness to manage their diabetes. The majority of veterans who declined to participate in this study, even though they qualified, stated that they would “not follow any recommendations.” Further investigation is needed about why some veterans elect not to obtain help that could positively impact their health and possibly extend their life. Additionally, scientific quantitative and qualitative research is needed to evaluate the statistical significance between health care literacy and educational intervention on patient adherence among individuals diagnosed with diabetes.
According to the National Academy of Medicine (NAM), health literacy is “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions.”1 Studies suggest that millions of patients have inadequate health literacy and cannot make fully informed decisions because of this lack of knowledge.2-4 A 2007 National Patient Safety Foundation report calculated that inadequate health literacy burdens the U.S. health care system with an additional $106 to $238 billion annually.5
In 2014, the American Diabetes Association reported that diabetes affects 29.1 million Americans (9.3%) and that by 2050 1 in 3 Americans will have diabetes.6 People with diabetes have health care costs 2.3 times higher than the cost for nondiabetic patients. The cost of taking care of patients with diabetes annually is about $245 billion.6 Without interventions that address health literacy and effective self-management to reduce the risks of complications and comorbidity, health care costs related to diabetes will continue to increase.
Literature Review
According to a U.S. Department of Education assessment on adult health literacy in 2003, 88% of adults in the U.S. have inadequate health literacy.2 About 90 million Americans lack health literacy skills, according to a 2004 NAM report.3 Heinrich, who conducted a review of U.S. studies on health literacy, concluded that about 25% of Americans have low health literacy.4
The Newest Vital Sign Tool
The Newest Vital Sign (NVS) tool is a free tool developed by Pfizer (New York, NY) for assessing health literacy. Participants are asked 6 questions about nutrition based on an ice cream nutrition label (Figure). The researcher records the participant’s responses, which accommodates participants who may have difficulty reading. The tool is scored from 0 to 6. A score of below 4 indicates the possibility of limited health literacy.7 This test can be completed in about 3 minutes, is widely accepted, and provides results comparable to more extensive literacy tests.8 A study conducted by Welch and colleagues suggested the NVS tool is both cost and time efficient.9 Ryan and colleagues found that 98% of patients in their study (n = 289) did not have objections to taking the NVS assessment.10
Escobedo and Weismuller’s study used the NVS health literacy tool to assess the health literacy of renal patients.3 In 2004, about 50,000 American patients with diabetes began treatment for kidney failure due to diabetes complications.6 Escobedo and Weismuller found that patients with diabetes with limited health literacy knowledge are more likely to be hospitalized, thus increasing health care costs.3 In addition, they discovered that these patients demonstrated poor adherence to prescribed treatment protocols. Welch, VanGeest, and Caskey conducted a case study on time, cost, and clinical utilization of the NVS health literacy tool and found that a patient’s lack of health literacy was linked to limited participation in personal medical decisions.7,9 Patient’s lack of knowledge was associated with delays in seeking treatment, poor self-management of the disease, and more hospital admissions.
Health Literacy and Diabetes
Studies specific to diabetes and inadequate health literacy support the premise that better health literacy leads to improved patient outcomes. Using the NVS tool, Heinrich conducted a study of the health literacy of 54 patients with diabetes in a primary care setting. The study showed that 65% had inadequate health literacy and that patients with diabetes with inadequate health literacy were more likely to have poor glycemic control compared with patients with diabetes and adequate health literacy levels.4 McCleary-Jones examined diet, foot care, and exercise of 50 African American participants with diabetes from a community health center, finding a positive relationship between health literacy and diabetes knowledge.11
Long and Gambling conducted a 2-year prospective, observational study that incorporated motivational interviewing and patient-centered care into a self-management program, examining the effectiveness of scheduled phone interventions to assist patients with diabetes in the management of their disease.12 The interventions used structured and consistent questions supported by a protocol and script that examined medication adherence and lifestyle choices. Long and Gambling concluded that “the findings demonstrate not only changes in the depth and detail of diabetes-related knowledge and confidence, but also enhanced competence in translating knowledge into every day self-care.”12 These researchers concluded that increased knowledge translated into better patient self-management of their disease. The Long and Gambling study included general self-management characteristics of monitoring HbA1c, diet, exercise, medication management, and general self-care. These researchers contend that diabetes self-management education must be a long-term endeavor to promote change.12
Mendoza and Rosenburg’s meta-analysis on self-management programs for diabetes and chronic conditions found a statistically significant 0.81% reduction in hemoglobin A1c (HbA1c). Characteristics of self-management programs that were linked to improved outcomes included nurse and provider education on medications, diet and/or exercise, and demonstrated use of motivational interviewing and biofeedback. Mendoza and Rosenburg suggested motivational interviewing focuses on the patient’s perspective and facilitates the process that the patient uses to assess their needs and to think about possible solutions.13 Mulimba and Bryo-Daniel found that motivational interviewing is a valuable tool for primary care nurses’ health promotion practice, and Thompson and colleagues found that it was effective in changing behavior.14,15
Nurse’s Role in Health Literacy
Nurses play a vital role in educating and securing adherence of patients in the management of their disease(s).13 In addition to educating patients, families, and friends of the family, nurses assist with helping them make informed decisions.16 The VHA uses the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) to teach health care staff about diabetes self-management education (DSME). Tisdel and colleagues found that DSME established through telemedicine or clinical mentoring improved patient outcomes.17 Mendoza and Rosenburgfound nurse-led DSME was linked to minimizing cardiovascular risk factors and improvements in HbA1c.13
Background
Staunton Community Based Outpatient Clinic (CBOC) in rural Virginia is a primary care clinic that serves veterans in the surrounding area. About one-fourth of the Staunton patients have diabetes. According to June 2014 data from the VHA Support Service Center, the physician at the Staunton CBOC was responsible for 946 patients (225 with diabetes) and the nurse practitioner was responsible for 707 (184 with diabetes). The VHA Support Service Center 2014 data indicated that veterans with poorly self-managed diabetes were at increased risk for poor outcomes, such as kidney failure, cardiovascular disease, and limb amputation. Veterans with diabetes use the emergency department more often and are admitted to the hospital more often than are veterans who do not have diabetes.18
Methods
The primary objective of this pilot study was to explore whether weekly structured nursing education sessions lasting 45 minutes and subsequent follow-up weekly conferences would improve their HbA1c for veterans identified as having ≥ 9 HbA1c and ≤ 3 health literacy score on the NVS 7 study assessment. Most recent HbA1c prior to beginning the study was used to identify potential participants. After completion of 12 weekly education interventions, an additional HbA1c was obtained.
The Salem VAMC and Eastern Mennonite University Institutional Review Board approved the study. Veterans’ questions were answered prior to signing consent forms. All data collected were kept confidential.
Veterans with ≥ 9 HbA1c were evaluated for possible participation. Forty-nine veterans met the criteria to participate in this pilot study. Exclusion criteria included diagnosis of any cognitive disorder, such as dementia, Alzheimer disease, or memory impairment. In addition, veterans unwilling or unable to commit to weekly follow-up sessions were excluded. The veterans eligible for participation were contacted by telephone, and 9 agreed to participate in the pilot study. Inclusion criteria included those aged ≥ 18 years and a diagnosis of diabetes with most recent HbA1c of ≥ 9 and a score of < 4 on the NVS health literacy assessment. After taking the NVS health literacy assessment, 6 of the 9 participants qualified to continue in the study.
Education interventions included assessing medication adherence, discussing diet, reviewing physical activity for the previous week (based on diet and activity logs), and reviewing home blood glucose monitoring. Weekly education sessions were either face-to-face or by telephone. This choice was given to accommodate veterans who may have had transportation issues. A total of 12 weekly appointments were scheduled for each participant, and education was directed at the specific needs and goals of each participant. Interventions for education were based on those found in previous studies.13,14,18,19
Data Collection and Analysis
All 6 participants were white male veterans who were diagnosed with diabetes for at least 3 years. Their ages ranged from 59 to 72. Three participants were service connected for diabetes and 3 were not. One participant dropped from the study after completing 4 appointments, stating he was just too busy to be available for a weekly appointment. Another participant completed 6 appointments and removed himself from the study due to time constraints. The 4 participants who completed the pilot study were followed for 12 weeks by a registered nurse (RN), and all had reductions in their HbA1c.
Participants were assessed at weekly appointments using a predetermined template for medication adherence, diet, activity, and blood glucose monitoring. Responses of the participants guided the education interventions to meet the individual veteran’s learning needs. For example, one veteran was given specific education on carbohydrate counting and another was educated on how to read food labels. Participants were also encouraged to express satisfaction, frustration, anger, or other emotions in managing their chronic illness. The premise for spending additional time with the veteran was to promote positive self-management behaviors as recommended by Radhakrishnan.19
Veterans who completed the study stated that the education interventions positively impacted their health status. One veteran was able to delay dialysis due to self-directed improvement in his lifestyle (exercising and watching his diet), which improved his HbA1c. This veteran attributed his health improvement to the individualized education sessions with the RN and knowing he had to be accountable to someone. Additionally, it was found there was a strong familial-social component to diabetes self-management. Several veterans were knowledgeable about diabetes self-management as evidenced by their responses to weekly questions. However, disease management for these veterans was strongly impacted by family and life events.
One veteran did not manage his disease for an entire week due to “being busy with a death in the family and planning for a wedding.” This veteran took his medication but did not check his blood glucose or monitor his diet. Another veteran spoke of eating ice cream and other concentrated sweets because his young grandson was with him for the week. A third veteran was able to manage his diet better when his wife packed snacks for him but when left to his own accord did not do well with his food selection. Even though these veterans understood how to effectively manage their diabetes, they may have chosen to inconsistently translate that knowledge into practice if they perceive those familial-social forces to be more important or more powerful.
Discussion
The findings from this small pilot study from a single clinic cannot be generalized. However, this pilot study adds to the literature of the positive impact of individualized, structured, tailored nursing interventions delivered with careful consideration of the participants’ personal goals and health care needs for diabetes self-management.
Participants monitored home blood glucose levels, diet, and activity and maintained adherence with prescribed diabetes medications. The HbA1c level for participants decreased by the end of the program. During the course of the pilot study a pharmacist managed the veterans’ medications. Participant 1 began a new medication regimen the first day of the study. Previously, the patient was self-regulating his medication. However, during the 12-week study, he had no medication adjustments. Participant 4 had several increases to his insulin dose (insulin aspart protamine and insulin aspart rdna origin) during the course of the study. Participants 5 and 6 had no medication adjustments during the study.
Even though participants had medication adjustments, which contributed to the HbA1c decrease, they became more aware of the medical need to control their blood sugar through the one-on-one education provided. Although there was variation in the depth and detail that participants maintained their food/activity log and home blood glucose monitoring, all participants agreed that they were more likely to be adherent with prescribed self-monitoring “knowing they were going to have to report self-monitoring information” to the RN.
Health care professionals may not realize the impact of familial-social events on blood glucose control. Veterans in this study found that having weekly sessions with the RN helped them through such events, even though they did not adhere strictly to their regimen. One suggestion is having veterans anticipate future familial-social events that may trigger nonadherence to their diabetes health plan and then discuss those events with the health care professional.
Future Research
This small exploratory pilot study has implications for future research. Increasing the study’s sample size and using a control group is recommended to compare veterans who have an educational intervention with those that do not and the impact it has on blood glucose control. The study was limited to 1 CBOC. Incorporating additional CBOCs could increase the sample size. Additionally, although this study was only 3 months in duration, a longer study could reveal significant patterns of change over time as well as the long-term benefit of a tailored educational intervention. In addition, adjusting the study inclusion criteria of > 9 HbA1c to include those with > 8 HbA1c also may increase the sample size.
Limited financial resources for the study could have negatively impacted the sample size. Incorporating recruitment or advertising strategy may increase the number of participants. Research also is needed on education interventions with a diverse group of male and female veterans that extends beyond 3 months. Exploring the value of including the veteran’s family in the education sessions is needed. Finally, this study examined only diabetes education. Researchers need to consider other diseases and the value of individualized education.
Limitations
Limitations included a small sample size and no control group. Due to the study’s small sample size, extrapolating data from it becomes difficult. However, this pilot study sets the groundwork for other researchers to expand the importance of education interventions and health literacy. Recruitment was challenging since an eligibility criterion was the NVS score, and patients were sometimes difficult to contact.7 The pilot study started with 6 white male participants but only 4 finished. During the course of the pilot study, 1 veteran had medication adjustments as part of routine care and 1 veteran had medication adjustments prior to the study, which could have altered the HbA1c results.
In hindsight, using the NVS to assess both prestudy with poststudy health literacy scores would have provided additional information about the education intervention. There is possible bias because the researcher was a VAMC employee, and the RN that implemented the interventions had previously worked with the patients.
Conclusion
Although this is a small descriptive pilot study, it adds to the body of research on the value of nurse-driven interventions to help veterans manage diabetes by enhancing their health literacy. It also raises questions and opportunities for further research into the power of familial-social influences on a veteran’s willingness to manage their diabetes. The majority of veterans who declined to participate in this study, even though they qualified, stated that they would “not follow any recommendations.” Further investigation is needed about why some veterans elect not to obtain help that could positively impact their health and possibly extend their life. Additionally, scientific quantitative and qualitative research is needed to evaluate the statistical significance between health care literacy and educational intervention on patient adherence among individuals diagnosed with diabetes.
1. Stiles E. Promoting health literacy in patients with diabetes. Nurs Stand. 2011;26(8):35-40.
2. Baum NH, Dowling RA. Health literacy: how do your patients rate? http://urologytimes.modernmedicine.com/urology-times/news/modernmedicine/modern-medicine-now/health-literacy-how-do-your-patients-rate. Published August 1, 2011. Accessed December 2, 2016.
3. Escobedo W, Weismuller P. Assessing health literacy in renal failure and kidney transplant patients. Prog Transplant. 2013;23(1):47-54.
4. Heinrich C. Health literacy: the sixth vital sign. J Am Acad Nurse Pract. 2012;24(4):218-223.
5. Roett MA, Wessel L. Help your patient “get” what you just said: health literacy guide. J Fam Pract. 2012;61(4):190-196.
6. American Diabetes Association. Statistics about diabetes. http://www.diabetes.org/diabetes-basics/statistics/?loc=feat1.Updated December 12, 2016. Accessed December 14, 2016.
7. Pfizer. The newest vital sign. http://www.pfizer.com/files/health/nvs_flipbook_english_final.pdf. Published February 2011. Accessed December 2, 2016.
8. Shah LC, West P, Bremmeyr K, Savoy-Moore RT. Health literacy instrument in family medicine: the “newest vital sign” ease of use and correlates. J Am Board Fam Med. 2010;23(2):195-203.
9. Welch VL, VanGeest JB, Caskey R. Time, costs, and clinical utilization of screening for health literacy: a case study using the Newest Vital Sign (NVS) instrument. J Am Board Fam Med. 2011;24(3):281-289.
10. Ryan JG, Leguen F, Weiss BD, et al. Will patients agree to have their literacy skills assessed in clinical practice? Health Educ Res. 2008;23(4):603-611.
11. McCleary-Jones V. Health literacy and its association with diabetes knowledge, self-efficacy and disease self-management among African Americans with diabetes mellitus. ABNF J. 2011;22(2):25-32.
12. Long AF, Gambling T. Enhancing health literacy and behavioral change within a tele-care education and support intervention for people with type 2 diabetes. Health Expect. 2012;15(3):267-282.
13. Mendoza M, Rosenberg T. Self-management of type 2 diabetes: A good idea-or not? J Fam Pract. 2013;62(5):244-248.
14. A Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs. 2014;23(1):8-14.
15. Thompson DR, Chair SY, Chan SW, Astin F, Davidson PM, Ski CF. Motivational interviewing: a useful approach to improving cardiovascular health? J Clin Nurs. 2011;20;(9-10):1236-1244.
16. Protheroe J, Rowlands G. Matching clinical information with levels of patient health literacy. Nurs Manag (Harrow). 2013;20(3):20-21.
17. Tisdel KA, Bedwell M, Tarkington PE, Mundy A, Fredrickson SK. Diabetes specialists share experience remotely with RN care managers. Fed Pract. 2013;30(suppl 7):15S-20S.
18. U.S. Department of Veterans Affairs, Veterans Health Administration Support Service Center. http://vssc.med.va.gov/AlphaIndex.asp?Ltr=D.
19. Radhakrishnan K. The efficacy of tailored interventions for self-management outcomes of type 2 diabetes, hypertension, or heart disease: a systemic review. J Adv Nurs. 2012;68(3):496-510.
1. Stiles E. Promoting health literacy in patients with diabetes. Nurs Stand. 2011;26(8):35-40.
2. Baum NH, Dowling RA. Health literacy: how do your patients rate? http://urologytimes.modernmedicine.com/urology-times/news/modernmedicine/modern-medicine-now/health-literacy-how-do-your-patients-rate. Published August 1, 2011. Accessed December 2, 2016.
3. Escobedo W, Weismuller P. Assessing health literacy in renal failure and kidney transplant patients. Prog Transplant. 2013;23(1):47-54.
4. Heinrich C. Health literacy: the sixth vital sign. J Am Acad Nurse Pract. 2012;24(4):218-223.
5. Roett MA, Wessel L. Help your patient “get” what you just said: health literacy guide. J Fam Pract. 2012;61(4):190-196.
6. American Diabetes Association. Statistics about diabetes. http://www.diabetes.org/diabetes-basics/statistics/?loc=feat1.Updated December 12, 2016. Accessed December 14, 2016.
7. Pfizer. The newest vital sign. http://www.pfizer.com/files/health/nvs_flipbook_english_final.pdf. Published February 2011. Accessed December 2, 2016.
8. Shah LC, West P, Bremmeyr K, Savoy-Moore RT. Health literacy instrument in family medicine: the “newest vital sign” ease of use and correlates. J Am Board Fam Med. 2010;23(2):195-203.
9. Welch VL, VanGeest JB, Caskey R. Time, costs, and clinical utilization of screening for health literacy: a case study using the Newest Vital Sign (NVS) instrument. J Am Board Fam Med. 2011;24(3):281-289.
10. Ryan JG, Leguen F, Weiss BD, et al. Will patients agree to have their literacy skills assessed in clinical practice? Health Educ Res. 2008;23(4):603-611.
11. McCleary-Jones V. Health literacy and its association with diabetes knowledge, self-efficacy and disease self-management among African Americans with diabetes mellitus. ABNF J. 2011;22(2):25-32.
12. Long AF, Gambling T. Enhancing health literacy and behavioral change within a tele-care education and support intervention for people with type 2 diabetes. Health Expect. 2012;15(3):267-282.
13. Mendoza M, Rosenberg T. Self-management of type 2 diabetes: A good idea-or not? J Fam Pract. 2013;62(5):244-248.
14. A Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs. 2014;23(1):8-14.
15. Thompson DR, Chair SY, Chan SW, Astin F, Davidson PM, Ski CF. Motivational interviewing: a useful approach to improving cardiovascular health? J Clin Nurs. 2011;20;(9-10):1236-1244.
16. Protheroe J, Rowlands G. Matching clinical information with levels of patient health literacy. Nurs Manag (Harrow). 2013;20(3):20-21.
17. Tisdel KA, Bedwell M, Tarkington PE, Mundy A, Fredrickson SK. Diabetes specialists share experience remotely with RN care managers. Fed Pract. 2013;30(suppl 7):15S-20S.
18. U.S. Department of Veterans Affairs, Veterans Health Administration Support Service Center. http://vssc.med.va.gov/AlphaIndex.asp?Ltr=D.
19. Radhakrishnan K. The efficacy of tailored interventions for self-management outcomes of type 2 diabetes, hypertension, or heart disease: a systemic review. J Adv Nurs. 2012;68(3):496-510.
The Unique Value of Externships to Nursing Education and Health Care Organizations
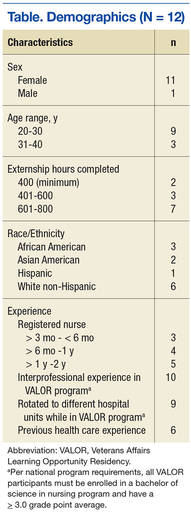
New nurse graduates often have difficulty transitioning to the role of registered nurse (RN).1 Given the complexity of the health care environment, the need is growing to prepare nursing students for nursing practice. Although nursing education provides students with a basis for practice, school alone cannot prepare them for actual practice in the hospital setting.2 Compared with nurse residency programs, which provide extended postlicensure training, the national Veterans Affairs Learning Opportunity Residency (VALOR) program provides externships independent of nursing school. Externships allow students to train in a hospital setting (generally during the summer months) before becoming a licensed RN. Nursing students who are entering their senior year of coursework in a bachelor of science nursing program and who have a minimum 3.0 grade point average can apply for this competitive national scholarship offered at VAMCs. The VALOR program is a paid learning opportunity, and students gain hands-on clinical experience under the guidance of preceptors.
Little externship research exists in the nursing literature.3,4 The authors conducted the present study to help fill the gaps in the literature and to add to the only other study findings on VALOR.3 This program, started in 1990 to aid in nursing recruitment and retention, offers students early exposure to the complexities of nursing practice.
The authors investigated RNs’ experience in the VALOR prelicensure externship during the nurses’ senior year of coursework and the impact of this experience on their nursing practice. The program offers 800 hours of hospital-based experience outside the classroom. New nurses who gained only limited clinical exposure in nursing school may feel insecure about their clinical skills.5 Casey and colleagues found that students want more clinical experience than offered by nursing school practicums.6 The VALOR participants obtain additional clinical time, which contributes to their self-confidence when transitioning to the RN role.7
Literature Review
New graduate nurses work in complex health care environments with unfamiliar technologies, shift hours, heavy patient loads, psychological and professional stressors, socialization problems, and patient safety issues.8 They often are unable to connect their educational experience with the realities of practice and find the work environment incongruent with their nursing school education.9 Although new nurses’ difficulty in transitioning to their professional role has been addressed in the literature, transitional experience has not improved.10 Studies have found that new graduate nurses want more support than is given and have suggested that unfamiliar workplace dynamics create stress for new nurses.11
Anxiety, insecurity, and fear of failure are associated with the transition from student to practicing nurse.10 Because of the additional clinical experience gained in an externship, students likely are more self-confident when they assume the RN role.12 White suggested self-confident students see themselves as nurses and feel capable of caring for patients.13 Externship experience makes the transition to professional nursing less stressful, because externship students obtain an inside view of nursing culture.14 Students increase their understanding of nurses’ multiple roles and responsibilities, because these programs focus on increasing clinical skills and competency.15 To perform successfully as RNs, new graduates need competencies and knowledge beyond those obtained in nursing school.16
In the nursing profession, an association between job satisfaction and turnover exists.17,18 Of new graduate nurses, 35% to 69% leave their position within the first year of employment.19 Replacing nurses reduces hospital productivity and efficiency and increases cost.20 New graduate nurses leave because they are dissatisfied with and overwhelmed by the complexity of the work environment.21 Prelicensure nurse externships can aid in recruiting and retaining new graduate nurses for the hospitals that host these programs.22 For host facilities, recruitment rates of 50% to 79% have been reported.23,24
In a quantitative study, Nuttall surveyed 133 RNs about job satisfaction, role socialization, professionalism, and sense of belonging.3 Of these RNs, 34 had participated in VALOR and 99 had not. There was no evidence that the RNs with VALOR experience had a higher degree of professionalism, job satisfaction, or role socialization; only sense of belonging (age-adjusted) was higher for the VALOR group. The conflicting data on prelicensure externship outcomes call for further analysis of these programs.3 Nuttall noted that her study “was the first... to evaluate the VALOR program and future research [using a qualitative approach] is needed to identify additional outcomes related to this program.”3
Methods
This study using hermeneutic phenomenology was approved by the Salem VAMC in Virginia and by the institutional review board at Nova Southeastern University.24 Study participants provided written informed consent before being interviewed.
Interviewees
Data Collection and Analysis
Data collection began in March 2013 with a pilot test of the interview questions for appropriateness. Open-ended, semistructured questions were used to elicit nurses’ descriptions of their experience. Field notes were written, and all interviews were tape-recorded and professionally transcribed verbatim. Data saturation was reached after 12 nurses were interviewed. Transcripts were analyzed and interpreted using van Manen’s line-by-line approach.26 All 12 interviewees were invited to review the findings of the data analysis. Eleven of the 12 interviewees verified and validated the study findings.
Rigor using Lincoln and Guba’s criteria of credibility, dependability, transferability, and confirmability added trustworthiness to the study findings. Bracketing helped eliminate potential bias.27 Credibility was achieved with prolonged engagement and triangulation. To further enhance credibility, the authors invited qualitative research experts to validate the emerging themes and create an audit trail. For dependability, a flow chart was created for use by researchers who might want to replicate the study. Rich, lengthy descriptions and interviewees’ quotations were provided so researchers could judge the study’s transferability to other settings. Maintaining an audit trail and having a doctor of nursing practice independently code the data aided with confirmability. This study used findings from the literature, audio recordings, member checking, and field notes to assess data accuracy.
Results
The overarching theme discovered in this study was confidence. Subthemes were transitioning to the RN role, making decisions, and interacting with interprofessional staff.
Confidence
Interviewees felt confident in transitioning to the RN role, making decisions, and interacting with interprofessional staff. They shared that they had applied to the externship to gain additional clinical experience and that the program increased their self-confidence with respect to transitioning to the new role as RN. However, it is possible that these interviewees were highly motivated and would not have had difficulty transitioning to the RN role—this is addressed in the Limitations section of this article.
Interviewees said they initially approached VALOR with fear and apprehension but completed it feeling confident about becoming an RN. One interviewee stated, “The VALOR program gave me the confidence in my own abilities, so I was not scared and had confidence that, yes, I could do this job.” Another said, “Honestly, the entire externship program, regardless of which question you ask, my answer is going to always fall back on confidence. I became prepared for the RN job, I feel, before I graduated because of the [externship] experiences.”
Transitioning to RN Role
Transitioning involved understanding the RN’s scope of practice and feeling clinically competent. Students worked 40 hours a week over the summer and gained firsthand insight into working as an RN daily. Interviewees believed completing the externship made it easy to transition to the RN role because they knew what to expect.
Working side-by-side with nurses, students gained insight into RNs’ responsibilities and scope of practice. Interviewees reported that, after the externship, they had a better understanding of their patient care and licensure legal responsibilities.
Students began to feel clinically competent during the externship. Interviewees shared that they had had several opportunities to practice basic skills, such as giving injections. One interviewee said, “I don’t think I tried to stick a single IV when I was in school or in clinical [training].” Interviewees also commented that repeatedly practicing skills increased their self-confidence.
Students also gained firsthand insight into working with veterans and their families. During the externship, they learned about communicating therapeutically, providing education for caregivers, and advocating for patients and their families. Before the externship, they felt apprehensive about communicating with patients. One interviewee said that after the program, “Eventually you had to talk to patients, and eventually figured it out that it wasn’t so scary.”
Students found that patients were not always happy with their care, and procedures did not always go as planned. They also discovered that education did not end with the patient; family members needed education as well. The externship experience heightened students’ awareness of the RN’s role as patient advocate. One interviewee explained it is the RN’s responsibility to intervene on the patient’s behalf. Interviewees were surprised that patients would not tell their health care provider that they did not understand what was said or that they wanted another course of treatment.
The externship helped decrease learning-related stress. Interviewees indicated they had learned without fear of reprisal. One described feeling free to learn: “Uninhibited learning...you can ask what you need to without fear of not graduating.” Externship students were able to focus on learning the RN role without worrying about the next test or grade. They felt free to ask questions without fear of failing their clinical rotation.
The supportive and nurturing relationships that students developed in VALOR also increased their confidence when transitioning to the RN role. One interviewee said, “There was never the sense of, no, you learn my way, or I don’t want you here.” Interviewees shared that they felt comfortable and supported.
Decision Making
Interviewees reported that after VALOR, it was easy to make decisions regarding nursing practice, delegation, care prioritization, and career choice. As students, they found the school clinical setting did not provide the decision-making opportunities VALOR did, and they quickly realized nursing practice involved more than making patient-care decisions. One interviewee said, “In a classroom, a picture is painted of an idealistic environment that may not truly mimic the hospital unit.”
Students became familiar with the practice of delegating care to the appropriate staff and the next shift. One interviewee said VALOR “provided me with a better understanding of delegation in my RN role.” VALOR participants discovered that, as new nurses, they were less anxious when delegating to others.
Before RN licensure, VALOR participants learned about prioritizing patient care. One interviewee said, “It’s like everybody has to be charted on, and all the medications have to be passed out, but it’s a matter of getting everything done while doing the more important and more dire things first.” Students learned that all aspects of nursing are important, but they had to make rational decisions.
Interacting With Professionals
Interviewees who had been in VALOR said interacting with interprofessional (different disciplines) staff contributed to their working comfortably in teams and collaborating with others. Their collaborative relationships with physicians would help them later, when as new graduate nurses they again needed to work together with doctors. Typical comments were, “When I started as an RN, I felt I was not new at it because I had communicated with doctors in the externship program.”
Discussion
The present study found that nursing students who had been in the VALOR externship felt confident in their clinical skills when they were transitioning to the RN role. Other studies similarly have found that externship students were self-confident assuming the RN role, owing to their additional clinical experience.12,28 The VALOR program allows students to work alongside nurses and receive hands-on experience while interacting with interprofessional health care teams. Findings of Nuttall’s quantitative study contradict those of the present, qualitative study. Nuttall used surveys and a control group, whereas this phenomenologic study captured the essence of study participants’ experiences through interviews.
The RNs interviewed in the present study discovered that, unlike nursing school, VALOR provided a realistic view of full-time work as an RN. This finding aligns with Starr and Conley’s finding that, before participating in an externship, most students were unaware of the extent of RNs’ roles and responsibilities, whereas after the program they understood these roles and responsibilities better.28
The interviewees in this study thought VALOR improved their skills in communicating with patients, families, and interprofessional team members. Interviewees shared that they learned patient advocacy skills and that, through firsthand experience, realized nurses provide patients with a voice. Externships can help new graduate nurses become better communicators and can teach students the importance of patient communication and advocacy.12
This study also found that students wanted more exposure to realistic nursing environments, additional nursing skills practice, and more interaction with interprofessional team members. VALOR helped bridge the theory–practice gap by providing real-world nursing experience outside the academic environment and extra time for nursing skills development. In a study by Casey and colleagues, students indicated that the time allowed for nursing skills practice during school was inadequate.6
The VALOR program helped students learn about delegating work, whereas nursing school did not provide the opportunity to practice delegation. Other studies have corroborated that students do not practice delegation during nursing school clinical time.29,30
Study respondents noted they could focus on learning without the fear of passing their clinical rotation. They felt supported by staff and were comfortable asking questions. White suggested that externship students who feel supported by nursing staff are able to focus on patients instead of on their discomfort.13 Rush and colleagues found that constraints on the student experience in traditional academic clinical rotations were replaced with “freedom and fearlessness in learning” in externships.31
Ten of the 12 study participants applied for a new graduate nurse position at the VAMC where they had their externship. A potential benefit to organizations that sponsor a nursing externship is the recruitment of new graduate nurses.14 Before applying for a full-time position, VALOR students had the opportunity to become familiar with the work environment and assess their fit with the employer. One student found staff nurse work “scary” and “stressful” and decided against it. She said the VALOR externship helped her realize exactly what nursing entailed: “Until this experience, I did not realize I would not like the hospital environment. This was a reality check for me.” Another student decided that working different shifts and working holidays would be difficult for her. These 2 students’ externship experience convinced them to seek other nursing positions.
Limitations
All participants in this study were nurses with excellent academic grades. It is possible they were highly motivated and might not have had any difficulty transitioning to the RN role. The principal investigator in this study was a VALOR program coordinator who knew 3 of the study participants—a potential source of bias. It is possible participants did not want to speak negatively about the program for several reasons: the interviewer was their coordinator, they received a salary during the externship, and several worked for the VA at the time of the survey.
Researchers have acknowledged the likelihood that not all VALOR students have positive experiences. It is possible that students with negative experiences did not discuss them or did not participate in the study. Increasing the size of the study sample may have brought in students with negative experiences. There is also the possibility of researcher misinterpretation and bias. Although bracketing was used, it was not possible to eliminate all potential sources of bias from this qualitative study.
Future Research
This is 1 of only 2 studies on the VALOR externship. Given the contradictory findings of these studies—Nuttall reported VALOR experience did not affect students’ transition to the RN role,3 whereas in the present study VALOR students thought the program positively affected their successful transition—additional quantitative and qualitative research is needed.
In addition, the low recruitment rate of VALOR students should be compared with other studies’ recruitment rates. The 38% VALOR extern recruitment rate for the period 2007 to 2012 is lower than the rate for other programs (G. Fuller, August 27, 2014, e-mail communication). The VALOR program does not track retention of participants after employment. Longitudinal studies should compare VALOR participants’ length of employment with that of nonparticipants’.
Conclusion
Externships provide clinical experience outside the classroom, expose students to the realities of nursing practice before graduation, and serve as a recruitment tool for hospitals. These programs, in conjunction with school-based practicums, increase exposure to the clinical environment. Before graduation, students have the opportunity to practice skills, interact with interprofessional staff, and experience different hospital units, all of which contribute to career decisions. The present study found that the VALOR externship helped new graduate nurses with their transition to the workplace. However, it is important to recognize the limitations of this study.
Interviewees indicated they were confident when they were transitioning to their new nurse role and caring for patients before receiving their RN licensure. New graduate nurses discovered they acclimated to the hospital environment quicker. The reality of working day-to-day in a hospital setting allowed students to select a compatible work environment and understand the daily challenges health care professionals encounter. Interviewees shared that they felt “like the RN” during the externship, which lessened the shock of actually assuming the RN role.
Van Manen asserted there is no conclusion or ending to a phenomenological study.26 Continued research on hospital-based externships will demonstrate how these programs can assist in the development of new graduate nurses, ease their transition to practice, and benefit nursing education, practice, research, and public policy.
1. Clark CM, Springer PJ. Nurse residents' first-hand accounts on transition to practice. Nurs Outlook. 2012;60(4):e2-e8.
2. Myers S, Reidy P, French B, McHale J, Chisholm M, Griffin M. Safety concerns of hospital-based new-to-practice registered nurses and their preceptors. J Contin Educ Nurs. 2010;41(4):163-171.
3. Nuttall CM. A Comparative Study Evaluating the Impact of Participation in a VALOR Nurse Externship on Job Satisfaction, Sense of Belonging, Role Socialization and Sense of Professionalism: Transition From Graduate to Registered Nurse [dissertation]. Albuquerque: University of New Mexico; 2010.
4. Steen JE, Gould EW, Raingruber B, Hill J. Effect of student nurse intern position on ease of transition from student nurse to registered nurse. J Nurs Staff Dev. 2011;27(4):181-186.
5. Ulrich B, Krozek C, Early S, Ashlock CH, Africa LM, Carman ML. Improving retention, confidence, and competence of new graduate nurses: results from a 10-year longitudinal database. Nurs Econ. 2010;28(6):363-375.
6. Casey K, Fink R, Jaynes C, Campbell L, Cook P, Wilson V. Readiness for practice: the senior practicum experience. J Nurs Educ. 2011;50(11):646-652.
7. Shipman D, Hooten J, Stanley S. The VALOR program: preparing nursing students to care for our veterans. Fed Pract. 2014;31(9):35-38.
8. Walker A, Earl C, Costa B, Cuddihy L. Graduate nurses' transition and integration into the workplace: a qualitative comparison of graduate nurses' and nurse unit managers' perspectives. Nurs Educ Today. 2013;33(3):291-296.
9. Welding NM. Creating a nursing residency: decrease turnover and increase clinical competence. Medsurg Nurs. 2011;20(1):37-40.
10. Morrow S. New graduate transitions: leaving the nest, joining the flight. J Nurs Manag. 2009;17(3):278-287.
11. Parker V, Giles M, Lantry G, McMillan M. New graduate nurses' experience in their first year of practice. Nurs Educ Today. 2014;34(1):150-156.
12. Ruth-Sahd LA, Beck J, McCall C. Transformative learning during a nursing externship program: the reflections of senior nursing students. Nurs Educ Perspect. 2010;31(2):78-83.
13. White AH. Clinical decision making among fourth-year nursing students: an interpretive study. J Nurs Educ. 2003;42(3):113-121.
14. Kropkowski LR, Most R. Set for success: nurse "externs." Nurs Manag. 2008;39(7):8-9.
15. Rhoads J, Sensenig K, Ruth-Sahd L, Thompson E. Nursing externship: a collaborative endeavor between nursing education and nursing administration. Dimens Crit Care Nurs. 2003;22(6):255-258.
16. Hillman L, Foster RR. The impact of a nursing transitions programme on retention and cost savings. J Nurs Manag. 2011;19(1):50-56.
17. Baernholdt M, Mark BA. The nurse work environment, job satisfaction and turnover rates in rural and urban nursing units. J Nurs Manag. 2009;17(8):994-1001.
18. Jones CB. Revisiting nurse turnover costs: adjusting for inflation. J Nurs Adm. 2008;38(1):11-18.
19. Pine R, Tart K. Return on investment: benefits and challenges of baccalaureate nurse residency program. Nurs Econ. 2007;25(1):13-18, 39.
20. Beecroft PC, Dorey F, Wenten M. Turnover intention in new graduate nurses: a multivariate analysis. J Adv Nurs, 2008;62(1):41-52.
21. Phillips C, Esterman A, Kenny A. The theory of organisational socialisation and its potential for improving transition experiences for new graduate nurses. Nurs Educ Today. 2015;35(1):118-124.
22. Diefenbeck CA, Plowfield LA, Herrman JW. Clinical immersion: a residency model for nursing education. Nurs Educ Perspect. 2006;27(2):72-79.
23. Cantrell MA, Browne AM. The impact of a nurse externship on the transition process from graduate to registered nurse: part III. Recruitment and retention effects. J Nurs Staff Dev. 2006;22(1):11-14.
24. Kilpatrick K, Frunchak V. The nursing extern program: innovative strategies for students in transition. Health Care Manag (Frederick). 2006;25(3):236-242.
25. Kovner CT, Brewer CS, Fairchild S, Poornima S, Kim H, Djukic CM. Newly licensed RN's characteristics, work attitudes, and intentions to work. Am J Nurs. 2007;107(9):58-70
26. van Manen M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy. Albany: State University of New York Press; 1990.
27. Lincoln YS, Guba EG. Naturalistic Inquiry. Beverly Hills, CA: Sage; 1985.
28. Starr K, Conley VM. Becoming a registered nurse: the nurse extern experience. J Contin Educ Nurs. 2006;37(2):86-92.
29. Hasson F, McKenna HP, Keeney S. Delegating and supervising unregistered professionals: the student nurse experience. Nurs Educ Today. 2013;33(3):229-235.
30. Kramer M, Maguire P, Halfer D, et al. The organizational transformative power of nurse residency programs. Nurs Adm Q. 2012;36(2):155-168.
31. Rush KL, Peel K, McCracken B. Empowered learning on the inside: an externship experience. Nurs Educ Perspect. 2004;25(6):284-291
New nurse graduates often have difficulty transitioning to the role of registered nurse (RN).1 Given the complexity of the health care environment, the need is growing to prepare nursing students for nursing practice. Although nursing education provides students with a basis for practice, school alone cannot prepare them for actual practice in the hospital setting.2 Compared with nurse residency programs, which provide extended postlicensure training, the national Veterans Affairs Learning Opportunity Residency (VALOR) program provides externships independent of nursing school. Externships allow students to train in a hospital setting (generally during the summer months) before becoming a licensed RN. Nursing students who are entering their senior year of coursework in a bachelor of science nursing program and who have a minimum 3.0 grade point average can apply for this competitive national scholarship offered at VAMCs. The VALOR program is a paid learning opportunity, and students gain hands-on clinical experience under the guidance of preceptors.
Little externship research exists in the nursing literature.3,4 The authors conducted the present study to help fill the gaps in the literature and to add to the only other study findings on VALOR.3 This program, started in 1990 to aid in nursing recruitment and retention, offers students early exposure to the complexities of nursing practice.
The authors investigated RNs’ experience in the VALOR prelicensure externship during the nurses’ senior year of coursework and the impact of this experience on their nursing practice. The program offers 800 hours of hospital-based experience outside the classroom. New nurses who gained only limited clinical exposure in nursing school may feel insecure about their clinical skills.5 Casey and colleagues found that students want more clinical experience than offered by nursing school practicums.6 The VALOR participants obtain additional clinical time, which contributes to their self-confidence when transitioning to the RN role.7
Literature Review
New graduate nurses work in complex health care environments with unfamiliar technologies, shift hours, heavy patient loads, psychological and professional stressors, socialization problems, and patient safety issues.8 They often are unable to connect their educational experience with the realities of practice and find the work environment incongruent with their nursing school education.9 Although new nurses’ difficulty in transitioning to their professional role has been addressed in the literature, transitional experience has not improved.10 Studies have found that new graduate nurses want more support than is given and have suggested that unfamiliar workplace dynamics create stress for new nurses.11
Anxiety, insecurity, and fear of failure are associated with the transition from student to practicing nurse.10 Because of the additional clinical experience gained in an externship, students likely are more self-confident when they assume the RN role.12 White suggested self-confident students see themselves as nurses and feel capable of caring for patients.13 Externship experience makes the transition to professional nursing less stressful, because externship students obtain an inside view of nursing culture.14 Students increase their understanding of nurses’ multiple roles and responsibilities, because these programs focus on increasing clinical skills and competency.15 To perform successfully as RNs, new graduates need competencies and knowledge beyond those obtained in nursing school.16
In the nursing profession, an association between job satisfaction and turnover exists.17,18 Of new graduate nurses, 35% to 69% leave their position within the first year of employment.19 Replacing nurses reduces hospital productivity and efficiency and increases cost.20 New graduate nurses leave because they are dissatisfied with and overwhelmed by the complexity of the work environment.21 Prelicensure nurse externships can aid in recruiting and retaining new graduate nurses for the hospitals that host these programs.22 For host facilities, recruitment rates of 50% to 79% have been reported.23,24
In a quantitative study, Nuttall surveyed 133 RNs about job satisfaction, role socialization, professionalism, and sense of belonging.3 Of these RNs, 34 had participated in VALOR and 99 had not. There was no evidence that the RNs with VALOR experience had a higher degree of professionalism, job satisfaction, or role socialization; only sense of belonging (age-adjusted) was higher for the VALOR group. The conflicting data on prelicensure externship outcomes call for further analysis of these programs.3 Nuttall noted that her study “was the first... to evaluate the VALOR program and future research [using a qualitative approach] is needed to identify additional outcomes related to this program.”3
Methods
This study using hermeneutic phenomenology was approved by the Salem VAMC in Virginia and by the institutional review board at Nova Southeastern University.24 Study participants provided written informed consent before being interviewed.
Interviewees
Data Collection and Analysis
Data collection began in March 2013 with a pilot test of the interview questions for appropriateness. Open-ended, semistructured questions were used to elicit nurses’ descriptions of their experience. Field notes were written, and all interviews were tape-recorded and professionally transcribed verbatim. Data saturation was reached after 12 nurses were interviewed. Transcripts were analyzed and interpreted using van Manen’s line-by-line approach.26 All 12 interviewees were invited to review the findings of the data analysis. Eleven of the 12 interviewees verified and validated the study findings.
Rigor using Lincoln and Guba’s criteria of credibility, dependability, transferability, and confirmability added trustworthiness to the study findings. Bracketing helped eliminate potential bias.27 Credibility was achieved with prolonged engagement and triangulation. To further enhance credibility, the authors invited qualitative research experts to validate the emerging themes and create an audit trail. For dependability, a flow chart was created for use by researchers who might want to replicate the study. Rich, lengthy descriptions and interviewees’ quotations were provided so researchers could judge the study’s transferability to other settings. Maintaining an audit trail and having a doctor of nursing practice independently code the data aided with confirmability. This study used findings from the literature, audio recordings, member checking, and field notes to assess data accuracy.
Results
The overarching theme discovered in this study was confidence. Subthemes were transitioning to the RN role, making decisions, and interacting with interprofessional staff.
Confidence
Interviewees felt confident in transitioning to the RN role, making decisions, and interacting with interprofessional staff. They shared that they had applied to the externship to gain additional clinical experience and that the program increased their self-confidence with respect to transitioning to the new role as RN. However, it is possible that these interviewees were highly motivated and would not have had difficulty transitioning to the RN role—this is addressed in the Limitations section of this article.
Interviewees said they initially approached VALOR with fear and apprehension but completed it feeling confident about becoming an RN. One interviewee stated, “The VALOR program gave me the confidence in my own abilities, so I was not scared and had confidence that, yes, I could do this job.” Another said, “Honestly, the entire externship program, regardless of which question you ask, my answer is going to always fall back on confidence. I became prepared for the RN job, I feel, before I graduated because of the [externship] experiences.”
Transitioning to RN Role
Transitioning involved understanding the RN’s scope of practice and feeling clinically competent. Students worked 40 hours a week over the summer and gained firsthand insight into working as an RN daily. Interviewees believed completing the externship made it easy to transition to the RN role because they knew what to expect.
Working side-by-side with nurses, students gained insight into RNs’ responsibilities and scope of practice. Interviewees reported that, after the externship, they had a better understanding of their patient care and licensure legal responsibilities.
Students began to feel clinically competent during the externship. Interviewees shared that they had had several opportunities to practice basic skills, such as giving injections. One interviewee said, “I don’t think I tried to stick a single IV when I was in school or in clinical [training].” Interviewees also commented that repeatedly practicing skills increased their self-confidence.
Students also gained firsthand insight into working with veterans and their families. During the externship, they learned about communicating therapeutically, providing education for caregivers, and advocating for patients and their families. Before the externship, they felt apprehensive about communicating with patients. One interviewee said that after the program, “Eventually you had to talk to patients, and eventually figured it out that it wasn’t so scary.”
Students found that patients were not always happy with their care, and procedures did not always go as planned. They also discovered that education did not end with the patient; family members needed education as well. The externship experience heightened students’ awareness of the RN’s role as patient advocate. One interviewee explained it is the RN’s responsibility to intervene on the patient’s behalf. Interviewees were surprised that patients would not tell their health care provider that they did not understand what was said or that they wanted another course of treatment.
The externship helped decrease learning-related stress. Interviewees indicated they had learned without fear of reprisal. One described feeling free to learn: “Uninhibited learning...you can ask what you need to without fear of not graduating.” Externship students were able to focus on learning the RN role without worrying about the next test or grade. They felt free to ask questions without fear of failing their clinical rotation.
The supportive and nurturing relationships that students developed in VALOR also increased their confidence when transitioning to the RN role. One interviewee said, “There was never the sense of, no, you learn my way, or I don’t want you here.” Interviewees shared that they felt comfortable and supported.
Decision Making
Interviewees reported that after VALOR, it was easy to make decisions regarding nursing practice, delegation, care prioritization, and career choice. As students, they found the school clinical setting did not provide the decision-making opportunities VALOR did, and they quickly realized nursing practice involved more than making patient-care decisions. One interviewee said, “In a classroom, a picture is painted of an idealistic environment that may not truly mimic the hospital unit.”
Students became familiar with the practice of delegating care to the appropriate staff and the next shift. One interviewee said VALOR “provided me with a better understanding of delegation in my RN role.” VALOR participants discovered that, as new nurses, they were less anxious when delegating to others.
Before RN licensure, VALOR participants learned about prioritizing patient care. One interviewee said, “It’s like everybody has to be charted on, and all the medications have to be passed out, but it’s a matter of getting everything done while doing the more important and more dire things first.” Students learned that all aspects of nursing are important, but they had to make rational decisions.
Interacting With Professionals
Interviewees who had been in VALOR said interacting with interprofessional (different disciplines) staff contributed to their working comfortably in teams and collaborating with others. Their collaborative relationships with physicians would help them later, when as new graduate nurses they again needed to work together with doctors. Typical comments were, “When I started as an RN, I felt I was not new at it because I had communicated with doctors in the externship program.”
Discussion
The present study found that nursing students who had been in the VALOR externship felt confident in their clinical skills when they were transitioning to the RN role. Other studies similarly have found that externship students were self-confident assuming the RN role, owing to their additional clinical experience.12,28 The VALOR program allows students to work alongside nurses and receive hands-on experience while interacting with interprofessional health care teams. Findings of Nuttall’s quantitative study contradict those of the present, qualitative study. Nuttall used surveys and a control group, whereas this phenomenologic study captured the essence of study participants’ experiences through interviews.
The RNs interviewed in the present study discovered that, unlike nursing school, VALOR provided a realistic view of full-time work as an RN. This finding aligns with Starr and Conley’s finding that, before participating in an externship, most students were unaware of the extent of RNs’ roles and responsibilities, whereas after the program they understood these roles and responsibilities better.28
The interviewees in this study thought VALOR improved their skills in communicating with patients, families, and interprofessional team members. Interviewees shared that they learned patient advocacy skills and that, through firsthand experience, realized nurses provide patients with a voice. Externships can help new graduate nurses become better communicators and can teach students the importance of patient communication and advocacy.12
This study also found that students wanted more exposure to realistic nursing environments, additional nursing skills practice, and more interaction with interprofessional team members. VALOR helped bridge the theory–practice gap by providing real-world nursing experience outside the academic environment and extra time for nursing skills development. In a study by Casey and colleagues, students indicated that the time allowed for nursing skills practice during school was inadequate.6
The VALOR program helped students learn about delegating work, whereas nursing school did not provide the opportunity to practice delegation. Other studies have corroborated that students do not practice delegation during nursing school clinical time.29,30
Study respondents noted they could focus on learning without the fear of passing their clinical rotation. They felt supported by staff and were comfortable asking questions. White suggested that externship students who feel supported by nursing staff are able to focus on patients instead of on their discomfort.13 Rush and colleagues found that constraints on the student experience in traditional academic clinical rotations were replaced with “freedom and fearlessness in learning” in externships.31
Ten of the 12 study participants applied for a new graduate nurse position at the VAMC where they had their externship. A potential benefit to organizations that sponsor a nursing externship is the recruitment of new graduate nurses.14 Before applying for a full-time position, VALOR students had the opportunity to become familiar with the work environment and assess their fit with the employer. One student found staff nurse work “scary” and “stressful” and decided against it. She said the VALOR externship helped her realize exactly what nursing entailed: “Until this experience, I did not realize I would not like the hospital environment. This was a reality check for me.” Another student decided that working different shifts and working holidays would be difficult for her. These 2 students’ externship experience convinced them to seek other nursing positions.
Limitations
All participants in this study were nurses with excellent academic grades. It is possible they were highly motivated and might not have had any difficulty transitioning to the RN role. The principal investigator in this study was a VALOR program coordinator who knew 3 of the study participants—a potential source of bias. It is possible participants did not want to speak negatively about the program for several reasons: the interviewer was their coordinator, they received a salary during the externship, and several worked for the VA at the time of the survey.
Researchers have acknowledged the likelihood that not all VALOR students have positive experiences. It is possible that students with negative experiences did not discuss them or did not participate in the study. Increasing the size of the study sample may have brought in students with negative experiences. There is also the possibility of researcher misinterpretation and bias. Although bracketing was used, it was not possible to eliminate all potential sources of bias from this qualitative study.
Future Research
This is 1 of only 2 studies on the VALOR externship. Given the contradictory findings of these studies—Nuttall reported VALOR experience did not affect students’ transition to the RN role,3 whereas in the present study VALOR students thought the program positively affected their successful transition—additional quantitative and qualitative research is needed.
In addition, the low recruitment rate of VALOR students should be compared with other studies’ recruitment rates. The 38% VALOR extern recruitment rate for the period 2007 to 2012 is lower than the rate for other programs (G. Fuller, August 27, 2014, e-mail communication). The VALOR program does not track retention of participants after employment. Longitudinal studies should compare VALOR participants’ length of employment with that of nonparticipants’.
Conclusion
Externships provide clinical experience outside the classroom, expose students to the realities of nursing practice before graduation, and serve as a recruitment tool for hospitals. These programs, in conjunction with school-based practicums, increase exposure to the clinical environment. Before graduation, students have the opportunity to practice skills, interact with interprofessional staff, and experience different hospital units, all of which contribute to career decisions. The present study found that the VALOR externship helped new graduate nurses with their transition to the workplace. However, it is important to recognize the limitations of this study.
Interviewees indicated they were confident when they were transitioning to their new nurse role and caring for patients before receiving their RN licensure. New graduate nurses discovered they acclimated to the hospital environment quicker. The reality of working day-to-day in a hospital setting allowed students to select a compatible work environment and understand the daily challenges health care professionals encounter. Interviewees shared that they felt “like the RN” during the externship, which lessened the shock of actually assuming the RN role.
Van Manen asserted there is no conclusion or ending to a phenomenological study.26 Continued research on hospital-based externships will demonstrate how these programs can assist in the development of new graduate nurses, ease their transition to practice, and benefit nursing education, practice, research, and public policy.
New nurse graduates often have difficulty transitioning to the role of registered nurse (RN).1 Given the complexity of the health care environment, the need is growing to prepare nursing students for nursing practice. Although nursing education provides students with a basis for practice, school alone cannot prepare them for actual practice in the hospital setting.2 Compared with nurse residency programs, which provide extended postlicensure training, the national Veterans Affairs Learning Opportunity Residency (VALOR) program provides externships independent of nursing school. Externships allow students to train in a hospital setting (generally during the summer months) before becoming a licensed RN. Nursing students who are entering their senior year of coursework in a bachelor of science nursing program and who have a minimum 3.0 grade point average can apply for this competitive national scholarship offered at VAMCs. The VALOR program is a paid learning opportunity, and students gain hands-on clinical experience under the guidance of preceptors.
Little externship research exists in the nursing literature.3,4 The authors conducted the present study to help fill the gaps in the literature and to add to the only other study findings on VALOR.3 This program, started in 1990 to aid in nursing recruitment and retention, offers students early exposure to the complexities of nursing practice.
The authors investigated RNs’ experience in the VALOR prelicensure externship during the nurses’ senior year of coursework and the impact of this experience on their nursing practice. The program offers 800 hours of hospital-based experience outside the classroom. New nurses who gained only limited clinical exposure in nursing school may feel insecure about their clinical skills.5 Casey and colleagues found that students want more clinical experience than offered by nursing school practicums.6 The VALOR participants obtain additional clinical time, which contributes to their self-confidence when transitioning to the RN role.7
Literature Review
New graduate nurses work in complex health care environments with unfamiliar technologies, shift hours, heavy patient loads, psychological and professional stressors, socialization problems, and patient safety issues.8 They often are unable to connect their educational experience with the realities of practice and find the work environment incongruent with their nursing school education.9 Although new nurses’ difficulty in transitioning to their professional role has been addressed in the literature, transitional experience has not improved.10 Studies have found that new graduate nurses want more support than is given and have suggested that unfamiliar workplace dynamics create stress for new nurses.11
Anxiety, insecurity, and fear of failure are associated with the transition from student to practicing nurse.10 Because of the additional clinical experience gained in an externship, students likely are more self-confident when they assume the RN role.12 White suggested self-confident students see themselves as nurses and feel capable of caring for patients.13 Externship experience makes the transition to professional nursing less stressful, because externship students obtain an inside view of nursing culture.14 Students increase their understanding of nurses’ multiple roles and responsibilities, because these programs focus on increasing clinical skills and competency.15 To perform successfully as RNs, new graduates need competencies and knowledge beyond those obtained in nursing school.16
In the nursing profession, an association between job satisfaction and turnover exists.17,18 Of new graduate nurses, 35% to 69% leave their position within the first year of employment.19 Replacing nurses reduces hospital productivity and efficiency and increases cost.20 New graduate nurses leave because they are dissatisfied with and overwhelmed by the complexity of the work environment.21 Prelicensure nurse externships can aid in recruiting and retaining new graduate nurses for the hospitals that host these programs.22 For host facilities, recruitment rates of 50% to 79% have been reported.23,24
In a quantitative study, Nuttall surveyed 133 RNs about job satisfaction, role socialization, professionalism, and sense of belonging.3 Of these RNs, 34 had participated in VALOR and 99 had not. There was no evidence that the RNs with VALOR experience had a higher degree of professionalism, job satisfaction, or role socialization; only sense of belonging (age-adjusted) was higher for the VALOR group. The conflicting data on prelicensure externship outcomes call for further analysis of these programs.3 Nuttall noted that her study “was the first... to evaluate the VALOR program and future research [using a qualitative approach] is needed to identify additional outcomes related to this program.”3
Methods
This study using hermeneutic phenomenology was approved by the Salem VAMC in Virginia and by the institutional review board at Nova Southeastern University.24 Study participants provided written informed consent before being interviewed.
Interviewees
Data Collection and Analysis
Data collection began in March 2013 with a pilot test of the interview questions for appropriateness. Open-ended, semistructured questions were used to elicit nurses’ descriptions of their experience. Field notes were written, and all interviews were tape-recorded and professionally transcribed verbatim. Data saturation was reached after 12 nurses were interviewed. Transcripts were analyzed and interpreted using van Manen’s line-by-line approach.26 All 12 interviewees were invited to review the findings of the data analysis. Eleven of the 12 interviewees verified and validated the study findings.
Rigor using Lincoln and Guba’s criteria of credibility, dependability, transferability, and confirmability added trustworthiness to the study findings. Bracketing helped eliminate potential bias.27 Credibility was achieved with prolonged engagement and triangulation. To further enhance credibility, the authors invited qualitative research experts to validate the emerging themes and create an audit trail. For dependability, a flow chart was created for use by researchers who might want to replicate the study. Rich, lengthy descriptions and interviewees’ quotations were provided so researchers could judge the study’s transferability to other settings. Maintaining an audit trail and having a doctor of nursing practice independently code the data aided with confirmability. This study used findings from the literature, audio recordings, member checking, and field notes to assess data accuracy.
Results
The overarching theme discovered in this study was confidence. Subthemes were transitioning to the RN role, making decisions, and interacting with interprofessional staff.
Confidence
Interviewees felt confident in transitioning to the RN role, making decisions, and interacting with interprofessional staff. They shared that they had applied to the externship to gain additional clinical experience and that the program increased their self-confidence with respect to transitioning to the new role as RN. However, it is possible that these interviewees were highly motivated and would not have had difficulty transitioning to the RN role—this is addressed in the Limitations section of this article.
Interviewees said they initially approached VALOR with fear and apprehension but completed it feeling confident about becoming an RN. One interviewee stated, “The VALOR program gave me the confidence in my own abilities, so I was not scared and had confidence that, yes, I could do this job.” Another said, “Honestly, the entire externship program, regardless of which question you ask, my answer is going to always fall back on confidence. I became prepared for the RN job, I feel, before I graduated because of the [externship] experiences.”
Transitioning to RN Role
Transitioning involved understanding the RN’s scope of practice and feeling clinically competent. Students worked 40 hours a week over the summer and gained firsthand insight into working as an RN daily. Interviewees believed completing the externship made it easy to transition to the RN role because they knew what to expect.
Working side-by-side with nurses, students gained insight into RNs’ responsibilities and scope of practice. Interviewees reported that, after the externship, they had a better understanding of their patient care and licensure legal responsibilities.
Students began to feel clinically competent during the externship. Interviewees shared that they had had several opportunities to practice basic skills, such as giving injections. One interviewee said, “I don’t think I tried to stick a single IV when I was in school or in clinical [training].” Interviewees also commented that repeatedly practicing skills increased their self-confidence.
Students also gained firsthand insight into working with veterans and their families. During the externship, they learned about communicating therapeutically, providing education for caregivers, and advocating for patients and their families. Before the externship, they felt apprehensive about communicating with patients. One interviewee said that after the program, “Eventually you had to talk to patients, and eventually figured it out that it wasn’t so scary.”
Students found that patients were not always happy with their care, and procedures did not always go as planned. They also discovered that education did not end with the patient; family members needed education as well. The externship experience heightened students’ awareness of the RN’s role as patient advocate. One interviewee explained it is the RN’s responsibility to intervene on the patient’s behalf. Interviewees were surprised that patients would not tell their health care provider that they did not understand what was said or that they wanted another course of treatment.
The externship helped decrease learning-related stress. Interviewees indicated they had learned without fear of reprisal. One described feeling free to learn: “Uninhibited learning...you can ask what you need to without fear of not graduating.” Externship students were able to focus on learning the RN role without worrying about the next test or grade. They felt free to ask questions without fear of failing their clinical rotation.
The supportive and nurturing relationships that students developed in VALOR also increased their confidence when transitioning to the RN role. One interviewee said, “There was never the sense of, no, you learn my way, or I don’t want you here.” Interviewees shared that they felt comfortable and supported.
Decision Making
Interviewees reported that after VALOR, it was easy to make decisions regarding nursing practice, delegation, care prioritization, and career choice. As students, they found the school clinical setting did not provide the decision-making opportunities VALOR did, and they quickly realized nursing practice involved more than making patient-care decisions. One interviewee said, “In a classroom, a picture is painted of an idealistic environment that may not truly mimic the hospital unit.”
Students became familiar with the practice of delegating care to the appropriate staff and the next shift. One interviewee said VALOR “provided me with a better understanding of delegation in my RN role.” VALOR participants discovered that, as new nurses, they were less anxious when delegating to others.
Before RN licensure, VALOR participants learned about prioritizing patient care. One interviewee said, “It’s like everybody has to be charted on, and all the medications have to be passed out, but it’s a matter of getting everything done while doing the more important and more dire things first.” Students learned that all aspects of nursing are important, but they had to make rational decisions.
Interacting With Professionals
Interviewees who had been in VALOR said interacting with interprofessional (different disciplines) staff contributed to their working comfortably in teams and collaborating with others. Their collaborative relationships with physicians would help them later, when as new graduate nurses they again needed to work together with doctors. Typical comments were, “When I started as an RN, I felt I was not new at it because I had communicated with doctors in the externship program.”
Discussion
The present study found that nursing students who had been in the VALOR externship felt confident in their clinical skills when they were transitioning to the RN role. Other studies similarly have found that externship students were self-confident assuming the RN role, owing to their additional clinical experience.12,28 The VALOR program allows students to work alongside nurses and receive hands-on experience while interacting with interprofessional health care teams. Findings of Nuttall’s quantitative study contradict those of the present, qualitative study. Nuttall used surveys and a control group, whereas this phenomenologic study captured the essence of study participants’ experiences through interviews.
The RNs interviewed in the present study discovered that, unlike nursing school, VALOR provided a realistic view of full-time work as an RN. This finding aligns with Starr and Conley’s finding that, before participating in an externship, most students were unaware of the extent of RNs’ roles and responsibilities, whereas after the program they understood these roles and responsibilities better.28
The interviewees in this study thought VALOR improved their skills in communicating with patients, families, and interprofessional team members. Interviewees shared that they learned patient advocacy skills and that, through firsthand experience, realized nurses provide patients with a voice. Externships can help new graduate nurses become better communicators and can teach students the importance of patient communication and advocacy.12
This study also found that students wanted more exposure to realistic nursing environments, additional nursing skills practice, and more interaction with interprofessional team members. VALOR helped bridge the theory–practice gap by providing real-world nursing experience outside the academic environment and extra time for nursing skills development. In a study by Casey and colleagues, students indicated that the time allowed for nursing skills practice during school was inadequate.6
The VALOR program helped students learn about delegating work, whereas nursing school did not provide the opportunity to practice delegation. Other studies have corroborated that students do not practice delegation during nursing school clinical time.29,30
Study respondents noted they could focus on learning without the fear of passing their clinical rotation. They felt supported by staff and were comfortable asking questions. White suggested that externship students who feel supported by nursing staff are able to focus on patients instead of on their discomfort.13 Rush and colleagues found that constraints on the student experience in traditional academic clinical rotations were replaced with “freedom and fearlessness in learning” in externships.31
Ten of the 12 study participants applied for a new graduate nurse position at the VAMC where they had their externship. A potential benefit to organizations that sponsor a nursing externship is the recruitment of new graduate nurses.14 Before applying for a full-time position, VALOR students had the opportunity to become familiar with the work environment and assess their fit with the employer. One student found staff nurse work “scary” and “stressful” and decided against it. She said the VALOR externship helped her realize exactly what nursing entailed: “Until this experience, I did not realize I would not like the hospital environment. This was a reality check for me.” Another student decided that working different shifts and working holidays would be difficult for her. These 2 students’ externship experience convinced them to seek other nursing positions.
Limitations
All participants in this study were nurses with excellent academic grades. It is possible they were highly motivated and might not have had any difficulty transitioning to the RN role. The principal investigator in this study was a VALOR program coordinator who knew 3 of the study participants—a potential source of bias. It is possible participants did not want to speak negatively about the program for several reasons: the interviewer was their coordinator, they received a salary during the externship, and several worked for the VA at the time of the survey.
Researchers have acknowledged the likelihood that not all VALOR students have positive experiences. It is possible that students with negative experiences did not discuss them or did not participate in the study. Increasing the size of the study sample may have brought in students with negative experiences. There is also the possibility of researcher misinterpretation and bias. Although bracketing was used, it was not possible to eliminate all potential sources of bias from this qualitative study.
Future Research
This is 1 of only 2 studies on the VALOR externship. Given the contradictory findings of these studies—Nuttall reported VALOR experience did not affect students’ transition to the RN role,3 whereas in the present study VALOR students thought the program positively affected their successful transition—additional quantitative and qualitative research is needed.
In addition, the low recruitment rate of VALOR students should be compared with other studies’ recruitment rates. The 38% VALOR extern recruitment rate for the period 2007 to 2012 is lower than the rate for other programs (G. Fuller, August 27, 2014, e-mail communication). The VALOR program does not track retention of participants after employment. Longitudinal studies should compare VALOR participants’ length of employment with that of nonparticipants’.
Conclusion
Externships provide clinical experience outside the classroom, expose students to the realities of nursing practice before graduation, and serve as a recruitment tool for hospitals. These programs, in conjunction with school-based practicums, increase exposure to the clinical environment. Before graduation, students have the opportunity to practice skills, interact with interprofessional staff, and experience different hospital units, all of which contribute to career decisions. The present study found that the VALOR externship helped new graduate nurses with their transition to the workplace. However, it is important to recognize the limitations of this study.
Interviewees indicated they were confident when they were transitioning to their new nurse role and caring for patients before receiving their RN licensure. New graduate nurses discovered they acclimated to the hospital environment quicker. The reality of working day-to-day in a hospital setting allowed students to select a compatible work environment and understand the daily challenges health care professionals encounter. Interviewees shared that they felt “like the RN” during the externship, which lessened the shock of actually assuming the RN role.
Van Manen asserted there is no conclusion or ending to a phenomenological study.26 Continued research on hospital-based externships will demonstrate how these programs can assist in the development of new graduate nurses, ease their transition to practice, and benefit nursing education, practice, research, and public policy.
1. Clark CM, Springer PJ. Nurse residents' first-hand accounts on transition to practice. Nurs Outlook. 2012;60(4):e2-e8.
2. Myers S, Reidy P, French B, McHale J, Chisholm M, Griffin M. Safety concerns of hospital-based new-to-practice registered nurses and their preceptors. J Contin Educ Nurs. 2010;41(4):163-171.
3. Nuttall CM. A Comparative Study Evaluating the Impact of Participation in a VALOR Nurse Externship on Job Satisfaction, Sense of Belonging, Role Socialization and Sense of Professionalism: Transition From Graduate to Registered Nurse [dissertation]. Albuquerque: University of New Mexico; 2010.
4. Steen JE, Gould EW, Raingruber B, Hill J. Effect of student nurse intern position on ease of transition from student nurse to registered nurse. J Nurs Staff Dev. 2011;27(4):181-186.
5. Ulrich B, Krozek C, Early S, Ashlock CH, Africa LM, Carman ML. Improving retention, confidence, and competence of new graduate nurses: results from a 10-year longitudinal database. Nurs Econ. 2010;28(6):363-375.
6. Casey K, Fink R, Jaynes C, Campbell L, Cook P, Wilson V. Readiness for practice: the senior practicum experience. J Nurs Educ. 2011;50(11):646-652.
7. Shipman D, Hooten J, Stanley S. The VALOR program: preparing nursing students to care for our veterans. Fed Pract. 2014;31(9):35-38.
8. Walker A, Earl C, Costa B, Cuddihy L. Graduate nurses' transition and integration into the workplace: a qualitative comparison of graduate nurses' and nurse unit managers' perspectives. Nurs Educ Today. 2013;33(3):291-296.
9. Welding NM. Creating a nursing residency: decrease turnover and increase clinical competence. Medsurg Nurs. 2011;20(1):37-40.
10. Morrow S. New graduate transitions: leaving the nest, joining the flight. J Nurs Manag. 2009;17(3):278-287.
11. Parker V, Giles M, Lantry G, McMillan M. New graduate nurses' experience in their first year of practice. Nurs Educ Today. 2014;34(1):150-156.
12. Ruth-Sahd LA, Beck J, McCall C. Transformative learning during a nursing externship program: the reflections of senior nursing students. Nurs Educ Perspect. 2010;31(2):78-83.
13. White AH. Clinical decision making among fourth-year nursing students: an interpretive study. J Nurs Educ. 2003;42(3):113-121.
14. Kropkowski LR, Most R. Set for success: nurse "externs." Nurs Manag. 2008;39(7):8-9.
15. Rhoads J, Sensenig K, Ruth-Sahd L, Thompson E. Nursing externship: a collaborative endeavor between nursing education and nursing administration. Dimens Crit Care Nurs. 2003;22(6):255-258.
16. Hillman L, Foster RR. The impact of a nursing transitions programme on retention and cost savings. J Nurs Manag. 2011;19(1):50-56.
17. Baernholdt M, Mark BA. The nurse work environment, job satisfaction and turnover rates in rural and urban nursing units. J Nurs Manag. 2009;17(8):994-1001.
18. Jones CB. Revisiting nurse turnover costs: adjusting for inflation. J Nurs Adm. 2008;38(1):11-18.
19. Pine R, Tart K. Return on investment: benefits and challenges of baccalaureate nurse residency program. Nurs Econ. 2007;25(1):13-18, 39.
20. Beecroft PC, Dorey F, Wenten M. Turnover intention in new graduate nurses: a multivariate analysis. J Adv Nurs, 2008;62(1):41-52.
21. Phillips C, Esterman A, Kenny A. The theory of organisational socialisation and its potential for improving transition experiences for new graduate nurses. Nurs Educ Today. 2015;35(1):118-124.
22. Diefenbeck CA, Plowfield LA, Herrman JW. Clinical immersion: a residency model for nursing education. Nurs Educ Perspect. 2006;27(2):72-79.
23. Cantrell MA, Browne AM. The impact of a nurse externship on the transition process from graduate to registered nurse: part III. Recruitment and retention effects. J Nurs Staff Dev. 2006;22(1):11-14.
24. Kilpatrick K, Frunchak V. The nursing extern program: innovative strategies for students in transition. Health Care Manag (Frederick). 2006;25(3):236-242.
25. Kovner CT, Brewer CS, Fairchild S, Poornima S, Kim H, Djukic CM. Newly licensed RN's characteristics, work attitudes, and intentions to work. Am J Nurs. 2007;107(9):58-70
26. van Manen M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy. Albany: State University of New York Press; 1990.
27. Lincoln YS, Guba EG. Naturalistic Inquiry. Beverly Hills, CA: Sage; 1985.
28. Starr K, Conley VM. Becoming a registered nurse: the nurse extern experience. J Contin Educ Nurs. 2006;37(2):86-92.
29. Hasson F, McKenna HP, Keeney S. Delegating and supervising unregistered professionals: the student nurse experience. Nurs Educ Today. 2013;33(3):229-235.
30. Kramer M, Maguire P, Halfer D, et al. The organizational transformative power of nurse residency programs. Nurs Adm Q. 2012;36(2):155-168.
31. Rush KL, Peel K, McCracken B. Empowered learning on the inside: an externship experience. Nurs Educ Perspect. 2004;25(6):284-291
1. Clark CM, Springer PJ. Nurse residents' first-hand accounts on transition to practice. Nurs Outlook. 2012;60(4):e2-e8.
2. Myers S, Reidy P, French B, McHale J, Chisholm M, Griffin M. Safety concerns of hospital-based new-to-practice registered nurses and their preceptors. J Contin Educ Nurs. 2010;41(4):163-171.
3. Nuttall CM. A Comparative Study Evaluating the Impact of Participation in a VALOR Nurse Externship on Job Satisfaction, Sense of Belonging, Role Socialization and Sense of Professionalism: Transition From Graduate to Registered Nurse [dissertation]. Albuquerque: University of New Mexico; 2010.
4. Steen JE, Gould EW, Raingruber B, Hill J. Effect of student nurse intern position on ease of transition from student nurse to registered nurse. J Nurs Staff Dev. 2011;27(4):181-186.
5. Ulrich B, Krozek C, Early S, Ashlock CH, Africa LM, Carman ML. Improving retention, confidence, and competence of new graduate nurses: results from a 10-year longitudinal database. Nurs Econ. 2010;28(6):363-375.
6. Casey K, Fink R, Jaynes C, Campbell L, Cook P, Wilson V. Readiness for practice: the senior practicum experience. J Nurs Educ. 2011;50(11):646-652.
7. Shipman D, Hooten J, Stanley S. The VALOR program: preparing nursing students to care for our veterans. Fed Pract. 2014;31(9):35-38.
8. Walker A, Earl C, Costa B, Cuddihy L. Graduate nurses' transition and integration into the workplace: a qualitative comparison of graduate nurses' and nurse unit managers' perspectives. Nurs Educ Today. 2013;33(3):291-296.
9. Welding NM. Creating a nursing residency: decrease turnover and increase clinical competence. Medsurg Nurs. 2011;20(1):37-40.
10. Morrow S. New graduate transitions: leaving the nest, joining the flight. J Nurs Manag. 2009;17(3):278-287.
11. Parker V, Giles M, Lantry G, McMillan M. New graduate nurses' experience in their first year of practice. Nurs Educ Today. 2014;34(1):150-156.
12. Ruth-Sahd LA, Beck J, McCall C. Transformative learning during a nursing externship program: the reflections of senior nursing students. Nurs Educ Perspect. 2010;31(2):78-83.
13. White AH. Clinical decision making among fourth-year nursing students: an interpretive study. J Nurs Educ. 2003;42(3):113-121.
14. Kropkowski LR, Most R. Set for success: nurse "externs." Nurs Manag. 2008;39(7):8-9.
15. Rhoads J, Sensenig K, Ruth-Sahd L, Thompson E. Nursing externship: a collaborative endeavor between nursing education and nursing administration. Dimens Crit Care Nurs. 2003;22(6):255-258.
16. Hillman L, Foster RR. The impact of a nursing transitions programme on retention and cost savings. J Nurs Manag. 2011;19(1):50-56.
17. Baernholdt M, Mark BA. The nurse work environment, job satisfaction and turnover rates in rural and urban nursing units. J Nurs Manag. 2009;17(8):994-1001.
18. Jones CB. Revisiting nurse turnover costs: adjusting for inflation. J Nurs Adm. 2008;38(1):11-18.
19. Pine R, Tart K. Return on investment: benefits and challenges of baccalaureate nurse residency program. Nurs Econ. 2007;25(1):13-18, 39.
20. Beecroft PC, Dorey F, Wenten M. Turnover intention in new graduate nurses: a multivariate analysis. J Adv Nurs, 2008;62(1):41-52.
21. Phillips C, Esterman A, Kenny A. The theory of organisational socialisation and its potential for improving transition experiences for new graduate nurses. Nurs Educ Today. 2015;35(1):118-124.
22. Diefenbeck CA, Plowfield LA, Herrman JW. Clinical immersion: a residency model for nursing education. Nurs Educ Perspect. 2006;27(2):72-79.
23. Cantrell MA, Browne AM. The impact of a nurse externship on the transition process from graduate to registered nurse: part III. Recruitment and retention effects. J Nurs Staff Dev. 2006;22(1):11-14.
24. Kilpatrick K, Frunchak V. The nursing extern program: innovative strategies for students in transition. Health Care Manag (Frederick). 2006;25(3):236-242.
25. Kovner CT, Brewer CS, Fairchild S, Poornima S, Kim H, Djukic CM. Newly licensed RN's characteristics, work attitudes, and intentions to work. Am J Nurs. 2007;107(9):58-70
26. van Manen M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy. Albany: State University of New York Press; 1990.
27. Lincoln YS, Guba EG. Naturalistic Inquiry. Beverly Hills, CA: Sage; 1985.
28. Starr K, Conley VM. Becoming a registered nurse: the nurse extern experience. J Contin Educ Nurs. 2006;37(2):86-92.
29. Hasson F, McKenna HP, Keeney S. Delegating and supervising unregistered professionals: the student nurse experience. Nurs Educ Today. 2013;33(3):229-235.
30. Kramer M, Maguire P, Halfer D, et al. The organizational transformative power of nurse residency programs. Nurs Adm Q. 2012;36(2):155-168.
31. Rush KL, Peel K, McCracken B. Empowered learning on the inside: an externship experience. Nurs Educ Perspect. 2004;25(6):284-291
A Prescription for Music Lessons
Learning to play a musical instrument provides a peaceful retreat from the pressures of daily life. Therapeutic outcomes of playing music include better communication skills, improved emotional release, and decreased anxiety and agitation.1 Musical training promotes cognitive function, mental health, and a connection to others.2,3
Depression
Impacting 14.8 million people, depression is the most prevalent mental health issue for adults aged ≥ 55 years and accounts for 10% of all medical disability in the U.S. and Canada.4-6 About half the people diagnosed with depression also have an anxiety disorder, which can lead to smoking, drinking alcohol, overeating, and complicated health care issues.5 By 2020, depression is predicted to be the second most common disease in the world and cost employers about $23 billion in absenteeism.4
Hays and Minichiello found that learning to read music and play the piano might enhance mood and certain aspects of the quality of living indicators in older adults. Those aged ≥ 65 years who participated in playing music reported improved self-esteem, greater independence, and fewer feelings of isolation. In addition, playing music created a temporary escape from the stress of daily life.7 Seinfield and colleagues compared a piano training group with a control group (nonplaying) and found that those who played piano experienced a decrease in psychological distress, depression, and fatigue.8 Playing an instrument can positively impact the well-being of older adults throughout life by promoting empowerment, autonomy, and social cohesion.7-11Manalai and colleagues found that a single episode of playing the piano was beneficial for a 91-year-old female patient who previously played when she was young and who was currently experiencing psychotic and depressive symptoms. Following playing, the patient’s vocabulary and insight temporarily improved. For the first time since her admission, the patient provided many details about her past mental and physical health. Even though the patient never played again, due to her delusional disorder, the improvement in mood and cognition were sustained for several months.12 The researchers noted that the patient’s temporary improvement may have been attributed to other factors.12
Another study measured levels of anxiety, depression, and loneliness in senior citizens. Study participants who regularly participated in a keyboard class were less anxious, depressed, and lonely compared with the control group.13 Other studies support the idea that music can modulate emotional responses and enhance cognitive performance.14,15
Mind Stimulation
As people age, they will experience progressive physiologic losses in function, such as auditory, cognition, memory, and motor control.16,17 Affect or mood can also be impacted.8 Consequently, there is a focus on promoting nonpharmacologic solutions that protect against age-related health issues. For example, musical training for adults that involves sensorimotor practice produces greater changes in the auditory cortex than does the equivalent experience involving only auditory training.18 Research indicates that age-related auditory decline can be mitigated by musical training.19 Evidence also supports cognitive stimulation, which may help reduce the likelihood of cognitive impairments in advanced age.16,17
The brain works on a principle of “use it or lose it.” Therefore, exercising the brain is important, and musical training may fill that need. Learning a skill such as playing an instrument reorganizes the brain’s neural pathways.2,16 Brain plasticity is the ability of the brain to change its structure, and engaging older adults in sensory, cognitive, and motor activities creates positive outcomes.16,17 Research also indicates active participation in music lessons creates larger plasticity effects than does passively listening to music.16 Musical training provides a multisensory activity that requires integrating signals from different sensory modalities with motor responses.16 Verghese and colleagues found that individuals who played a musical instrument were less likely to experience dementia than were those whose leisure activities consisted of reading, writing, and working crossword puzzles.20 Verghese suggested that 6 months of piano lessons in older adults improved the brain’s executive functioning (regulates abilities and behaviors) and working memory (ie, keeping track of information).20 Balbag and colleagues who conducted a study of twins found that “playing an instrument in older adulthood is significantly associated with reduced likelihood of dementia and cognitive impairment.”21 Musical training is also associated with improved visual memory and the ability to divide the individual’s attention between several activities. This ability is crucial for activities such as driving and is useful for navigating crowded areas, such as a mall.22,23
Dexterity
Musical training also has been found to be beneficial for stroke survivors, because this type of training elicits a change in the reorganization of the sensorimotor cortex that results in improved movement quality.24 Piano playing can lead to meaningful improvements in manual dexterity, finger movement coordination, and functional use of upper extremities.25
Zelazny studied the effects of keyboard playing on 4 older adults with osteoarthritis who over 4 weeks had 30-minute sessions of electronic keyboard playing 4 days per week.26 The researcher found that participants reported decreased arthritic pain, increased dexterity, and increased finger strength. Playing the piano requires both eye and hand coordination, which is essential as a person ages. Improved dexterity of fine motor skills can assist individuals with the activities of daily living, such as buttoning a shirt and using a remote control.26
Stress Reduction
Life is filled with stressors, and anyone can have difficulty coping with daily stress. According to Toyoshima and colleagues, playing the piano can lower cortisol levels and decrease a person’s anxiety level.27 These researchers compared the activities of piano playing, calligraphy, and clay molding and found that playing the piano was significantly more effective at lowering stress levels when measuring salivary C-reactive protein levels and State-Trait Anxiety Inventory (STAI) scores.
Another study found stress reduction was significant for participants who played the keyboard compared with participants who relaxed, read magazines, or solved puzzles.28 Stress has a negative impact on the immune system, which can increase an individual’s risk of disease. According to Mohd “emotional stress is a major contributing factor to the 6 leading causes of death in the U.S.: cancer, coronary heart disease, accidental injuries, respiratory disorders, cirrhosis of the liver, and suicide.”29
PTSD and Guitars for Vets Program
Guitars for Vets is a nonprofit organization with 25 chapters that uses music to assist veterans with physical and mental health injuries.30 The program provides free guitars and weekly music lessons taught by volunteers. The weekly music lessons create a forum for veterans to socialize and share personal experiences, thus contributing to their healing process.30 A randomized, controlled pilot study was conducted with veterans diagnosed with posttraumatic stress disorder (PTSD) who may have physical and mental changes such as self-isolation from others, night sweats, flashbacks, and depression.31
The study participants had weekly private guitar lessons for 1 hour and a group learning session. The results showed positive outcomes in both PTSD and depression symptoms after 6 weeks of guitar lessons.30 One veteran with PTSD who participated in the Guitar for Vets Program stated, “I came here with some real serious anger issues; this takes my mind off everything.” This veteran noted that as he practiced, a peaceful feeling enveloped him and the memories of trauma faded.32
Personal Experience
Following the completion of my PhD, I started piano lessons as a hobby. I also found engaging in playing music helped me to psychologically cope with the overwhelming stress of having a parent with a debilitating disease.
My dad was diagnosed with Parkinson disease, making it difficult for him to view life positively. Piano lessons helped him to mentally deal with his disease. Dad genuinely looked forward to his music lessons and was able to focus on practicing the piano rather than on his disease. I believe playing the piano prevented him from becoming depressed and kept him engaged, because he was accomplishing something.
Dad’s Parkinson disease has progressed; he is now in a nursing home. My gift to Dad is playing the piano for him. I sincerely believe it helps him cope with his disease or at least temporarily forget about it. His mood changes, and he becomes more animated. In his more lucid moments, we play music together. Playing music has a magical way of creating peace within the mind. Plato is often attributed with the quote, “Music gives a soul to the universe, wings to the mind, flight to the imagination, and life to everything.”
Conclusions
A healthful lifestyle includes holistically addressing issues pertaining to mental and physical well-being. Learning how to play a musical instrument is a workout for the brain, just as physical exercise is a workout for the body; both are necessary for optimal health. Evidence exists to support the hypothesis that playing an instrument elicits brain changes that positively influence cognitive functioning and decreases stress. Despite the lifelong benefits of playing an instrument, only about 8% of adults aged > 18 years play a musical instrument.33
Playing a musical instrument provides health benefits without the adverse effects that accompany pharmacologic therapy. It also can help improve social skills and provide individuals with a sense of achievement. Group music lessons provide an opportunity for people to build bonds and positively affect lifestyle choices.
In addition, engaging individuals in learning to play music may decrease the cost of health care when considering treatments for depression, PTSD, and substance abuse. Playing an instrument may help decrease the need for antidepressants and provide a healthy recreational activity. Based on its physical and mental benefits, learning to play a musical instrument should be explored as complementary alternative medicine. Compared with filling prescription medications over an individual’s lifetime, the cost of a portable keyboard is substantially less.
Given the benefits of increased coordination, social involvement, neural responses, and ability to focus along with improving fine motor skills and reducing stress, including music lessons as part of a veteran’s health care makes sense and is well worth further investigation and research.
Acknowledgements
The author would like to thank Jack Hooten, MHA, MSN, RN, and Jennifer Hammond, MS, for their help in preparing this manuscript.
1. Music for Veterans. Program results. Music for Veterans Website. http://www.music4veterans.org/program-results-1.html. Published 2014. Accessed January 11, 2016.
2. Miendlarzewska E, Trost W. How musical training affects cognitive development: rhythm, reward and other modulating variables. Front Neurosci. 2014;7:1-18.
3. Bergland C. Musical training optimizes brain function. Psychology Today. November 2013. https://www.psychologytoday.com/blog/the-athletes-way/201311/musical-training-optimizes-brain-function. Accessed January 22, 2016.
4. Witters D, Liu D, Agrawal S. Depression costs U.S. workplaces $23 billion in absenteeism. Galllup Website. http://www.gallup.com/poll/163619/depression-costs-workplaces-billion-absenteeism.aspx. Published July 24, 2013. Accessed January 11, 2016.
5. Anxiety and Depression Association of America. Facts and statistics. Anxiety and Depression Association of America Website. http://www.adaa.org/about-adaa/press-room/facts-statistics. Updated September 2014. Accessed January 11, 2016.
6. World Health Organization. The global burden of disease: 2004 update. The World Health Organization Website. http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf. Published 2008. Accessed January 11, 2016. 7. Hays T, Minichiello V. The contribution of music to quality of life in older people: an Australian qualitative study. Aging Soc. 2005;25(2):261-278.
8. Seinfield S, Figueroa H, Ortiz-Gill J, Sanchez-Vives MV. Effects of music learning and piano practice on cognitive function, mood and quality of life in older adults. Front Psychol. 2013;4:1-13.
9. Coffman DD, Adamek MS. The contribution of wind band participation to quality of life of senior adults. Music Ther Perspect. 1999;17(1):27-31.
10. Creech A, Hallam S, McQueen H, Varvarigou M. The power of music in the lives of older adults. Res Studies Music Educ. 2013;35(1):83-98.
11. Park A-La. Can musical activities promote healthy ageing? Int J Emerg Ment Health. 2015;17(1):258-261.
12. Manalai G, Manalai P, Dutta R, Fegan G, Scrofani P. Rapid improvement of depressive symptoms and cognition in an elderly patient with a single session of piano playing: a clinical treatment report. Aging Clin Exp Res. 2012;24(3):278-280.
13. Koga M, Tims F. Music making and wellness project. Music Teachers National Association Website. www.mtna.org/media/4686/2001AOY.pdf. Published 2001. Accessed January 29, 2016.
14. Becker J. Anthropological perspectives on music and emotion. In: Juslin PN, Sloboda JA, eds. Music and Emotion: Theory and Research. New York, New York: Oxford University Press; 2001:135-160.
15. Witvliet CV, Vrana SR. Play it again Sam: repeated exposure to emotionally evocative music polarizes, liking and smiling responses, and influences other affective reports, facial EMG, and heart rate. Cogn Emot. 2003;21:3-25.
16. Dawson WJ. Benefits of music training are widespread and lifelong: a bibliographic review of their non-musical effects. Med Probl Perform Art. 2014;29(2):57-63.
17. Mahncke HW, Connor BB, Appelman J, et al. Memory enhancement in healthy older adults using a brain plasticity-based training program: a randomized, controlled study. Proc Natl Acad Sci USA. 2006;103(33):12523-12528.
18. Lappe C, Herholz SC, Trainor LJ, Pantev C. Cortical plasticity induced by short-term unimodal and multimodal musical training. J Neurosci. 2008;28(39):9632-9639.
19. Parbery-Clark A, Strait DL, Anderson S, Hittner E, Kraus N. Musical experience and the aging auditory system: implications for cognitive abilities and hearing speech in noise. PloS ONE. 2011;6(5):e18082.
20. Verghese J, Lipton RB, Katz MJ, et al. Leisure activities and the risk of dementia in the elderly. N Engl J Med. 2003;348(25):2508-2516.
21. Balbag M, Pedersen N, Garz M. Playing a musical instrument as a protective factor against dementia and cognitive impairment: a population-based twin study. Int J Alzheimers Dis. 2014;2014:1-6.
22. Oechslin MS, Van De Ville D, Lazeyras F, Hauert CA, James CE. Degree of musical expertise modulates higher order brain functioning. Cereb Cortex. 2013;23(9):2213-2224.
23. Patston LL. Balanced brains: an investigation of visuospatial ability and lateralization in musicians. Pyschmusicol. 2012;22(2):187.
24. Rodriguez-Fornells A, Rojo N, Amengual JL, Ripollés P, Altenmüller E, Münte TF. The involvement of audio-motor coupling in the music-supported therapy applied to stroke patients. Ann NY Acad Sci. 2012;1252(1):282-293.
25. Villeneuve M, Lamontagne A. Playing piano can improve upper extremity function after stroke: case studies. Stroke Res Treat. 2013;2013:1-5.
26. Zelazny CM. Therapeutic instrumental music playing in hand rehabilitation for older adults with osteoarthritis: four case studies. J Music Ther. 2001;38(2):97-113.
27. Toyoshima K, Fukui H, Kuda K. Piano playing reduces stress more than other creative activities. Intl J Music Educ. 2011;29(3):257-263.
28. Bittman B, Berk L, Shannon M, et al. Recreational music-making modulates the human stress response: a preliminary individualized gene expression study. Med Sci Monit. 2005;11(2):BR31-BR40.
29. Mohd RS. Life event, stress and illness. Malays J Med Sci. 2008;15(4):9-18.
30. U.S Department of Veterans Affairs. PPO 10-075–HSR&D study. U.S Department of Veterans Affairs Website. http://www.hsrd.research.va.gov/research/abstracts.cfm?Project_ID=2141700403. Updated March 24, 2014. Accessed January 20, 2016.
31. Hooten J, Shipman D, Osting V. Posttraumatic stress disorder in veterans: inpatient assessment and management. Fed Pract. 2008;25(1):27-37.
32. WJLA. Music therapy program helps veterans with PTSD. WJLA Website. http://wjla.com/news/nation-world/music-therapy-program-helps-veterans-with-ptsd-98564. Published December 26, 2013. Accessed January 20, 2016.
33. U.S. Census Bureau, Statistical Abstract of the United States: 2011. Arts, recreation and travel section 26. U.S. Census Bureau Website. https://www.census.gov/prod/2011pubs/11statab/arts.pdf. Published 2011. Accessed January 11, 2016.
Learning to play a musical instrument provides a peaceful retreat from the pressures of daily life. Therapeutic outcomes of playing music include better communication skills, improved emotional release, and decreased anxiety and agitation.1 Musical training promotes cognitive function, mental health, and a connection to others.2,3
Depression
Impacting 14.8 million people, depression is the most prevalent mental health issue for adults aged ≥ 55 years and accounts for 10% of all medical disability in the U.S. and Canada.4-6 About half the people diagnosed with depression also have an anxiety disorder, which can lead to smoking, drinking alcohol, overeating, and complicated health care issues.5 By 2020, depression is predicted to be the second most common disease in the world and cost employers about $23 billion in absenteeism.4
Hays and Minichiello found that learning to read music and play the piano might enhance mood and certain aspects of the quality of living indicators in older adults. Those aged ≥ 65 years who participated in playing music reported improved self-esteem, greater independence, and fewer feelings of isolation. In addition, playing music created a temporary escape from the stress of daily life.7 Seinfield and colleagues compared a piano training group with a control group (nonplaying) and found that those who played piano experienced a decrease in psychological distress, depression, and fatigue.8 Playing an instrument can positively impact the well-being of older adults throughout life by promoting empowerment, autonomy, and social cohesion.7-11Manalai and colleagues found that a single episode of playing the piano was beneficial for a 91-year-old female patient who previously played when she was young and who was currently experiencing psychotic and depressive symptoms. Following playing, the patient’s vocabulary and insight temporarily improved. For the first time since her admission, the patient provided many details about her past mental and physical health. Even though the patient never played again, due to her delusional disorder, the improvement in mood and cognition were sustained for several months.12 The researchers noted that the patient’s temporary improvement may have been attributed to other factors.12
Another study measured levels of anxiety, depression, and loneliness in senior citizens. Study participants who regularly participated in a keyboard class were less anxious, depressed, and lonely compared with the control group.13 Other studies support the idea that music can modulate emotional responses and enhance cognitive performance.14,15
Mind Stimulation
As people age, they will experience progressive physiologic losses in function, such as auditory, cognition, memory, and motor control.16,17 Affect or mood can also be impacted.8 Consequently, there is a focus on promoting nonpharmacologic solutions that protect against age-related health issues. For example, musical training for adults that involves sensorimotor practice produces greater changes in the auditory cortex than does the equivalent experience involving only auditory training.18 Research indicates that age-related auditory decline can be mitigated by musical training.19 Evidence also supports cognitive stimulation, which may help reduce the likelihood of cognitive impairments in advanced age.16,17
The brain works on a principle of “use it or lose it.” Therefore, exercising the brain is important, and musical training may fill that need. Learning a skill such as playing an instrument reorganizes the brain’s neural pathways.2,16 Brain plasticity is the ability of the brain to change its structure, and engaging older adults in sensory, cognitive, and motor activities creates positive outcomes.16,17 Research also indicates active participation in music lessons creates larger plasticity effects than does passively listening to music.16 Musical training provides a multisensory activity that requires integrating signals from different sensory modalities with motor responses.16 Verghese and colleagues found that individuals who played a musical instrument were less likely to experience dementia than were those whose leisure activities consisted of reading, writing, and working crossword puzzles.20 Verghese suggested that 6 months of piano lessons in older adults improved the brain’s executive functioning (regulates abilities and behaviors) and working memory (ie, keeping track of information).20 Balbag and colleagues who conducted a study of twins found that “playing an instrument in older adulthood is significantly associated with reduced likelihood of dementia and cognitive impairment.”21 Musical training is also associated with improved visual memory and the ability to divide the individual’s attention between several activities. This ability is crucial for activities such as driving and is useful for navigating crowded areas, such as a mall.22,23
Dexterity
Musical training also has been found to be beneficial for stroke survivors, because this type of training elicits a change in the reorganization of the sensorimotor cortex that results in improved movement quality.24 Piano playing can lead to meaningful improvements in manual dexterity, finger movement coordination, and functional use of upper extremities.25
Zelazny studied the effects of keyboard playing on 4 older adults with osteoarthritis who over 4 weeks had 30-minute sessions of electronic keyboard playing 4 days per week.26 The researcher found that participants reported decreased arthritic pain, increased dexterity, and increased finger strength. Playing the piano requires both eye and hand coordination, which is essential as a person ages. Improved dexterity of fine motor skills can assist individuals with the activities of daily living, such as buttoning a shirt and using a remote control.26
Stress Reduction
Life is filled with stressors, and anyone can have difficulty coping with daily stress. According to Toyoshima and colleagues, playing the piano can lower cortisol levels and decrease a person’s anxiety level.27 These researchers compared the activities of piano playing, calligraphy, and clay molding and found that playing the piano was significantly more effective at lowering stress levels when measuring salivary C-reactive protein levels and State-Trait Anxiety Inventory (STAI) scores.
Another study found stress reduction was significant for participants who played the keyboard compared with participants who relaxed, read magazines, or solved puzzles.28 Stress has a negative impact on the immune system, which can increase an individual’s risk of disease. According to Mohd “emotional stress is a major contributing factor to the 6 leading causes of death in the U.S.: cancer, coronary heart disease, accidental injuries, respiratory disorders, cirrhosis of the liver, and suicide.”29
PTSD and Guitars for Vets Program
Guitars for Vets is a nonprofit organization with 25 chapters that uses music to assist veterans with physical and mental health injuries.30 The program provides free guitars and weekly music lessons taught by volunteers. The weekly music lessons create a forum for veterans to socialize and share personal experiences, thus contributing to their healing process.30 A randomized, controlled pilot study was conducted with veterans diagnosed with posttraumatic stress disorder (PTSD) who may have physical and mental changes such as self-isolation from others, night sweats, flashbacks, and depression.31
The study participants had weekly private guitar lessons for 1 hour and a group learning session. The results showed positive outcomes in both PTSD and depression symptoms after 6 weeks of guitar lessons.30 One veteran with PTSD who participated in the Guitar for Vets Program stated, “I came here with some real serious anger issues; this takes my mind off everything.” This veteran noted that as he practiced, a peaceful feeling enveloped him and the memories of trauma faded.32
Personal Experience
Following the completion of my PhD, I started piano lessons as a hobby. I also found engaging in playing music helped me to psychologically cope with the overwhelming stress of having a parent with a debilitating disease.
My dad was diagnosed with Parkinson disease, making it difficult for him to view life positively. Piano lessons helped him to mentally deal with his disease. Dad genuinely looked forward to his music lessons and was able to focus on practicing the piano rather than on his disease. I believe playing the piano prevented him from becoming depressed and kept him engaged, because he was accomplishing something.
Dad’s Parkinson disease has progressed; he is now in a nursing home. My gift to Dad is playing the piano for him. I sincerely believe it helps him cope with his disease or at least temporarily forget about it. His mood changes, and he becomes more animated. In his more lucid moments, we play music together. Playing music has a magical way of creating peace within the mind. Plato is often attributed with the quote, “Music gives a soul to the universe, wings to the mind, flight to the imagination, and life to everything.”
Conclusions
A healthful lifestyle includes holistically addressing issues pertaining to mental and physical well-being. Learning how to play a musical instrument is a workout for the brain, just as physical exercise is a workout for the body; both are necessary for optimal health. Evidence exists to support the hypothesis that playing an instrument elicits brain changes that positively influence cognitive functioning and decreases stress. Despite the lifelong benefits of playing an instrument, only about 8% of adults aged > 18 years play a musical instrument.33
Playing a musical instrument provides health benefits without the adverse effects that accompany pharmacologic therapy. It also can help improve social skills and provide individuals with a sense of achievement. Group music lessons provide an opportunity for people to build bonds and positively affect lifestyle choices.
In addition, engaging individuals in learning to play music may decrease the cost of health care when considering treatments for depression, PTSD, and substance abuse. Playing an instrument may help decrease the need for antidepressants and provide a healthy recreational activity. Based on its physical and mental benefits, learning to play a musical instrument should be explored as complementary alternative medicine. Compared with filling prescription medications over an individual’s lifetime, the cost of a portable keyboard is substantially less.
Given the benefits of increased coordination, social involvement, neural responses, and ability to focus along with improving fine motor skills and reducing stress, including music lessons as part of a veteran’s health care makes sense and is well worth further investigation and research.
Acknowledgements
The author would like to thank Jack Hooten, MHA, MSN, RN, and Jennifer Hammond, MS, for their help in preparing this manuscript.
Learning to play a musical instrument provides a peaceful retreat from the pressures of daily life. Therapeutic outcomes of playing music include better communication skills, improved emotional release, and decreased anxiety and agitation.1 Musical training promotes cognitive function, mental health, and a connection to others.2,3
Depression
Impacting 14.8 million people, depression is the most prevalent mental health issue for adults aged ≥ 55 years and accounts for 10% of all medical disability in the U.S. and Canada.4-6 About half the people diagnosed with depression also have an anxiety disorder, which can lead to smoking, drinking alcohol, overeating, and complicated health care issues.5 By 2020, depression is predicted to be the second most common disease in the world and cost employers about $23 billion in absenteeism.4
Hays and Minichiello found that learning to read music and play the piano might enhance mood and certain aspects of the quality of living indicators in older adults. Those aged ≥ 65 years who participated in playing music reported improved self-esteem, greater independence, and fewer feelings of isolation. In addition, playing music created a temporary escape from the stress of daily life.7 Seinfield and colleagues compared a piano training group with a control group (nonplaying) and found that those who played piano experienced a decrease in psychological distress, depression, and fatigue.8 Playing an instrument can positively impact the well-being of older adults throughout life by promoting empowerment, autonomy, and social cohesion.7-11Manalai and colleagues found that a single episode of playing the piano was beneficial for a 91-year-old female patient who previously played when she was young and who was currently experiencing psychotic and depressive symptoms. Following playing, the patient’s vocabulary and insight temporarily improved. For the first time since her admission, the patient provided many details about her past mental and physical health. Even though the patient never played again, due to her delusional disorder, the improvement in mood and cognition were sustained for several months.12 The researchers noted that the patient’s temporary improvement may have been attributed to other factors.12
Another study measured levels of anxiety, depression, and loneliness in senior citizens. Study participants who regularly participated in a keyboard class were less anxious, depressed, and lonely compared with the control group.13 Other studies support the idea that music can modulate emotional responses and enhance cognitive performance.14,15
Mind Stimulation
As people age, they will experience progressive physiologic losses in function, such as auditory, cognition, memory, and motor control.16,17 Affect or mood can also be impacted.8 Consequently, there is a focus on promoting nonpharmacologic solutions that protect against age-related health issues. For example, musical training for adults that involves sensorimotor practice produces greater changes in the auditory cortex than does the equivalent experience involving only auditory training.18 Research indicates that age-related auditory decline can be mitigated by musical training.19 Evidence also supports cognitive stimulation, which may help reduce the likelihood of cognitive impairments in advanced age.16,17
The brain works on a principle of “use it or lose it.” Therefore, exercising the brain is important, and musical training may fill that need. Learning a skill such as playing an instrument reorganizes the brain’s neural pathways.2,16 Brain plasticity is the ability of the brain to change its structure, and engaging older adults in sensory, cognitive, and motor activities creates positive outcomes.16,17 Research also indicates active participation in music lessons creates larger plasticity effects than does passively listening to music.16 Musical training provides a multisensory activity that requires integrating signals from different sensory modalities with motor responses.16 Verghese and colleagues found that individuals who played a musical instrument were less likely to experience dementia than were those whose leisure activities consisted of reading, writing, and working crossword puzzles.20 Verghese suggested that 6 months of piano lessons in older adults improved the brain’s executive functioning (regulates abilities and behaviors) and working memory (ie, keeping track of information).20 Balbag and colleagues who conducted a study of twins found that “playing an instrument in older adulthood is significantly associated with reduced likelihood of dementia and cognitive impairment.”21 Musical training is also associated with improved visual memory and the ability to divide the individual’s attention between several activities. This ability is crucial for activities such as driving and is useful for navigating crowded areas, such as a mall.22,23
Dexterity
Musical training also has been found to be beneficial for stroke survivors, because this type of training elicits a change in the reorganization of the sensorimotor cortex that results in improved movement quality.24 Piano playing can lead to meaningful improvements in manual dexterity, finger movement coordination, and functional use of upper extremities.25
Zelazny studied the effects of keyboard playing on 4 older adults with osteoarthritis who over 4 weeks had 30-minute sessions of electronic keyboard playing 4 days per week.26 The researcher found that participants reported decreased arthritic pain, increased dexterity, and increased finger strength. Playing the piano requires both eye and hand coordination, which is essential as a person ages. Improved dexterity of fine motor skills can assist individuals with the activities of daily living, such as buttoning a shirt and using a remote control.26
Stress Reduction
Life is filled with stressors, and anyone can have difficulty coping with daily stress. According to Toyoshima and colleagues, playing the piano can lower cortisol levels and decrease a person’s anxiety level.27 These researchers compared the activities of piano playing, calligraphy, and clay molding and found that playing the piano was significantly more effective at lowering stress levels when measuring salivary C-reactive protein levels and State-Trait Anxiety Inventory (STAI) scores.
Another study found stress reduction was significant for participants who played the keyboard compared with participants who relaxed, read magazines, or solved puzzles.28 Stress has a negative impact on the immune system, which can increase an individual’s risk of disease. According to Mohd “emotional stress is a major contributing factor to the 6 leading causes of death in the U.S.: cancer, coronary heart disease, accidental injuries, respiratory disorders, cirrhosis of the liver, and suicide.”29
PTSD and Guitars for Vets Program
Guitars for Vets is a nonprofit organization with 25 chapters that uses music to assist veterans with physical and mental health injuries.30 The program provides free guitars and weekly music lessons taught by volunteers. The weekly music lessons create a forum for veterans to socialize and share personal experiences, thus contributing to their healing process.30 A randomized, controlled pilot study was conducted with veterans diagnosed with posttraumatic stress disorder (PTSD) who may have physical and mental changes such as self-isolation from others, night sweats, flashbacks, and depression.31
The study participants had weekly private guitar lessons for 1 hour and a group learning session. The results showed positive outcomes in both PTSD and depression symptoms after 6 weeks of guitar lessons.30 One veteran with PTSD who participated in the Guitar for Vets Program stated, “I came here with some real serious anger issues; this takes my mind off everything.” This veteran noted that as he practiced, a peaceful feeling enveloped him and the memories of trauma faded.32
Personal Experience
Following the completion of my PhD, I started piano lessons as a hobby. I also found engaging in playing music helped me to psychologically cope with the overwhelming stress of having a parent with a debilitating disease.
My dad was diagnosed with Parkinson disease, making it difficult for him to view life positively. Piano lessons helped him to mentally deal with his disease. Dad genuinely looked forward to his music lessons and was able to focus on practicing the piano rather than on his disease. I believe playing the piano prevented him from becoming depressed and kept him engaged, because he was accomplishing something.
Dad’s Parkinson disease has progressed; he is now in a nursing home. My gift to Dad is playing the piano for him. I sincerely believe it helps him cope with his disease or at least temporarily forget about it. His mood changes, and he becomes more animated. In his more lucid moments, we play music together. Playing music has a magical way of creating peace within the mind. Plato is often attributed with the quote, “Music gives a soul to the universe, wings to the mind, flight to the imagination, and life to everything.”
Conclusions
A healthful lifestyle includes holistically addressing issues pertaining to mental and physical well-being. Learning how to play a musical instrument is a workout for the brain, just as physical exercise is a workout for the body; both are necessary for optimal health. Evidence exists to support the hypothesis that playing an instrument elicits brain changes that positively influence cognitive functioning and decreases stress. Despite the lifelong benefits of playing an instrument, only about 8% of adults aged > 18 years play a musical instrument.33
Playing a musical instrument provides health benefits without the adverse effects that accompany pharmacologic therapy. It also can help improve social skills and provide individuals with a sense of achievement. Group music lessons provide an opportunity for people to build bonds and positively affect lifestyle choices.
In addition, engaging individuals in learning to play music may decrease the cost of health care when considering treatments for depression, PTSD, and substance abuse. Playing an instrument may help decrease the need for antidepressants and provide a healthy recreational activity. Based on its physical and mental benefits, learning to play a musical instrument should be explored as complementary alternative medicine. Compared with filling prescription medications over an individual’s lifetime, the cost of a portable keyboard is substantially less.
Given the benefits of increased coordination, social involvement, neural responses, and ability to focus along with improving fine motor skills and reducing stress, including music lessons as part of a veteran’s health care makes sense and is well worth further investigation and research.
Acknowledgements
The author would like to thank Jack Hooten, MHA, MSN, RN, and Jennifer Hammond, MS, for their help in preparing this manuscript.
1. Music for Veterans. Program results. Music for Veterans Website. http://www.music4veterans.org/program-results-1.html. Published 2014. Accessed January 11, 2016.
2. Miendlarzewska E, Trost W. How musical training affects cognitive development: rhythm, reward and other modulating variables. Front Neurosci. 2014;7:1-18.
3. Bergland C. Musical training optimizes brain function. Psychology Today. November 2013. https://www.psychologytoday.com/blog/the-athletes-way/201311/musical-training-optimizes-brain-function. Accessed January 22, 2016.
4. Witters D, Liu D, Agrawal S. Depression costs U.S. workplaces $23 billion in absenteeism. Galllup Website. http://www.gallup.com/poll/163619/depression-costs-workplaces-billion-absenteeism.aspx. Published July 24, 2013. Accessed January 11, 2016.
5. Anxiety and Depression Association of America. Facts and statistics. Anxiety and Depression Association of America Website. http://www.adaa.org/about-adaa/press-room/facts-statistics. Updated September 2014. Accessed January 11, 2016.
6. World Health Organization. The global burden of disease: 2004 update. The World Health Organization Website. http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf. Published 2008. Accessed January 11, 2016. 7. Hays T, Minichiello V. The contribution of music to quality of life in older people: an Australian qualitative study. Aging Soc. 2005;25(2):261-278.
8. Seinfield S, Figueroa H, Ortiz-Gill J, Sanchez-Vives MV. Effects of music learning and piano practice on cognitive function, mood and quality of life in older adults. Front Psychol. 2013;4:1-13.
9. Coffman DD, Adamek MS. The contribution of wind band participation to quality of life of senior adults. Music Ther Perspect. 1999;17(1):27-31.
10. Creech A, Hallam S, McQueen H, Varvarigou M. The power of music in the lives of older adults. Res Studies Music Educ. 2013;35(1):83-98.
11. Park A-La. Can musical activities promote healthy ageing? Int J Emerg Ment Health. 2015;17(1):258-261.
12. Manalai G, Manalai P, Dutta R, Fegan G, Scrofani P. Rapid improvement of depressive symptoms and cognition in an elderly patient with a single session of piano playing: a clinical treatment report. Aging Clin Exp Res. 2012;24(3):278-280.
13. Koga M, Tims F. Music making and wellness project. Music Teachers National Association Website. www.mtna.org/media/4686/2001AOY.pdf. Published 2001. Accessed January 29, 2016.
14. Becker J. Anthropological perspectives on music and emotion. In: Juslin PN, Sloboda JA, eds. Music and Emotion: Theory and Research. New York, New York: Oxford University Press; 2001:135-160.
15. Witvliet CV, Vrana SR. Play it again Sam: repeated exposure to emotionally evocative music polarizes, liking and smiling responses, and influences other affective reports, facial EMG, and heart rate. Cogn Emot. 2003;21:3-25.
16. Dawson WJ. Benefits of music training are widespread and lifelong: a bibliographic review of their non-musical effects. Med Probl Perform Art. 2014;29(2):57-63.
17. Mahncke HW, Connor BB, Appelman J, et al. Memory enhancement in healthy older adults using a brain plasticity-based training program: a randomized, controlled study. Proc Natl Acad Sci USA. 2006;103(33):12523-12528.
18. Lappe C, Herholz SC, Trainor LJ, Pantev C. Cortical plasticity induced by short-term unimodal and multimodal musical training. J Neurosci. 2008;28(39):9632-9639.
19. Parbery-Clark A, Strait DL, Anderson S, Hittner E, Kraus N. Musical experience and the aging auditory system: implications for cognitive abilities and hearing speech in noise. PloS ONE. 2011;6(5):e18082.
20. Verghese J, Lipton RB, Katz MJ, et al. Leisure activities and the risk of dementia in the elderly. N Engl J Med. 2003;348(25):2508-2516.
21. Balbag M, Pedersen N, Garz M. Playing a musical instrument as a protective factor against dementia and cognitive impairment: a population-based twin study. Int J Alzheimers Dis. 2014;2014:1-6.
22. Oechslin MS, Van De Ville D, Lazeyras F, Hauert CA, James CE. Degree of musical expertise modulates higher order brain functioning. Cereb Cortex. 2013;23(9):2213-2224.
23. Patston LL. Balanced brains: an investigation of visuospatial ability and lateralization in musicians. Pyschmusicol. 2012;22(2):187.
24. Rodriguez-Fornells A, Rojo N, Amengual JL, Ripollés P, Altenmüller E, Münte TF. The involvement of audio-motor coupling in the music-supported therapy applied to stroke patients. Ann NY Acad Sci. 2012;1252(1):282-293.
25. Villeneuve M, Lamontagne A. Playing piano can improve upper extremity function after stroke: case studies. Stroke Res Treat. 2013;2013:1-5.
26. Zelazny CM. Therapeutic instrumental music playing in hand rehabilitation for older adults with osteoarthritis: four case studies. J Music Ther. 2001;38(2):97-113.
27. Toyoshima K, Fukui H, Kuda K. Piano playing reduces stress more than other creative activities. Intl J Music Educ. 2011;29(3):257-263.
28. Bittman B, Berk L, Shannon M, et al. Recreational music-making modulates the human stress response: a preliminary individualized gene expression study. Med Sci Monit. 2005;11(2):BR31-BR40.
29. Mohd RS. Life event, stress and illness. Malays J Med Sci. 2008;15(4):9-18.
30. U.S Department of Veterans Affairs. PPO 10-075–HSR&D study. U.S Department of Veterans Affairs Website. http://www.hsrd.research.va.gov/research/abstracts.cfm?Project_ID=2141700403. Updated March 24, 2014. Accessed January 20, 2016.
31. Hooten J, Shipman D, Osting V. Posttraumatic stress disorder in veterans: inpatient assessment and management. Fed Pract. 2008;25(1):27-37.
32. WJLA. Music therapy program helps veterans with PTSD. WJLA Website. http://wjla.com/news/nation-world/music-therapy-program-helps-veterans-with-ptsd-98564. Published December 26, 2013. Accessed January 20, 2016.
33. U.S. Census Bureau, Statistical Abstract of the United States: 2011. Arts, recreation and travel section 26. U.S. Census Bureau Website. https://www.census.gov/prod/2011pubs/11statab/arts.pdf. Published 2011. Accessed January 11, 2016.
1. Music for Veterans. Program results. Music for Veterans Website. http://www.music4veterans.org/program-results-1.html. Published 2014. Accessed January 11, 2016.
2. Miendlarzewska E, Trost W. How musical training affects cognitive development: rhythm, reward and other modulating variables. Front Neurosci. 2014;7:1-18.
3. Bergland C. Musical training optimizes brain function. Psychology Today. November 2013. https://www.psychologytoday.com/blog/the-athletes-way/201311/musical-training-optimizes-brain-function. Accessed January 22, 2016.
4. Witters D, Liu D, Agrawal S. Depression costs U.S. workplaces $23 billion in absenteeism. Galllup Website. http://www.gallup.com/poll/163619/depression-costs-workplaces-billion-absenteeism.aspx. Published July 24, 2013. Accessed January 11, 2016.
5. Anxiety and Depression Association of America. Facts and statistics. Anxiety and Depression Association of America Website. http://www.adaa.org/about-adaa/press-room/facts-statistics. Updated September 2014. Accessed January 11, 2016.
6. World Health Organization. The global burden of disease: 2004 update. The World Health Organization Website. http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf. Published 2008. Accessed January 11, 2016. 7. Hays T, Minichiello V. The contribution of music to quality of life in older people: an Australian qualitative study. Aging Soc. 2005;25(2):261-278.
8. Seinfield S, Figueroa H, Ortiz-Gill J, Sanchez-Vives MV. Effects of music learning and piano practice on cognitive function, mood and quality of life in older adults. Front Psychol. 2013;4:1-13.
9. Coffman DD, Adamek MS. The contribution of wind band participation to quality of life of senior adults. Music Ther Perspect. 1999;17(1):27-31.
10. Creech A, Hallam S, McQueen H, Varvarigou M. The power of music in the lives of older adults. Res Studies Music Educ. 2013;35(1):83-98.
11. Park A-La. Can musical activities promote healthy ageing? Int J Emerg Ment Health. 2015;17(1):258-261.
12. Manalai G, Manalai P, Dutta R, Fegan G, Scrofani P. Rapid improvement of depressive symptoms and cognition in an elderly patient with a single session of piano playing: a clinical treatment report. Aging Clin Exp Res. 2012;24(3):278-280.
13. Koga M, Tims F. Music making and wellness project. Music Teachers National Association Website. www.mtna.org/media/4686/2001AOY.pdf. Published 2001. Accessed January 29, 2016.
14. Becker J. Anthropological perspectives on music and emotion. In: Juslin PN, Sloboda JA, eds. Music and Emotion: Theory and Research. New York, New York: Oxford University Press; 2001:135-160.
15. Witvliet CV, Vrana SR. Play it again Sam: repeated exposure to emotionally evocative music polarizes, liking and smiling responses, and influences other affective reports, facial EMG, and heart rate. Cogn Emot. 2003;21:3-25.
16. Dawson WJ. Benefits of music training are widespread and lifelong: a bibliographic review of their non-musical effects. Med Probl Perform Art. 2014;29(2):57-63.
17. Mahncke HW, Connor BB, Appelman J, et al. Memory enhancement in healthy older adults using a brain plasticity-based training program: a randomized, controlled study. Proc Natl Acad Sci USA. 2006;103(33):12523-12528.
18. Lappe C, Herholz SC, Trainor LJ, Pantev C. Cortical plasticity induced by short-term unimodal and multimodal musical training. J Neurosci. 2008;28(39):9632-9639.
19. Parbery-Clark A, Strait DL, Anderson S, Hittner E, Kraus N. Musical experience and the aging auditory system: implications for cognitive abilities and hearing speech in noise. PloS ONE. 2011;6(5):e18082.
20. Verghese J, Lipton RB, Katz MJ, et al. Leisure activities and the risk of dementia in the elderly. N Engl J Med. 2003;348(25):2508-2516.
21. Balbag M, Pedersen N, Garz M. Playing a musical instrument as a protective factor against dementia and cognitive impairment: a population-based twin study. Int J Alzheimers Dis. 2014;2014:1-6.
22. Oechslin MS, Van De Ville D, Lazeyras F, Hauert CA, James CE. Degree of musical expertise modulates higher order brain functioning. Cereb Cortex. 2013;23(9):2213-2224.
23. Patston LL. Balanced brains: an investigation of visuospatial ability and lateralization in musicians. Pyschmusicol. 2012;22(2):187.
24. Rodriguez-Fornells A, Rojo N, Amengual JL, Ripollés P, Altenmüller E, Münte TF. The involvement of audio-motor coupling in the music-supported therapy applied to stroke patients. Ann NY Acad Sci. 2012;1252(1):282-293.
25. Villeneuve M, Lamontagne A. Playing piano can improve upper extremity function after stroke: case studies. Stroke Res Treat. 2013;2013:1-5.
26. Zelazny CM. Therapeutic instrumental music playing in hand rehabilitation for older adults with osteoarthritis: four case studies. J Music Ther. 2001;38(2):97-113.
27. Toyoshima K, Fukui H, Kuda K. Piano playing reduces stress more than other creative activities. Intl J Music Educ. 2011;29(3):257-263.
28. Bittman B, Berk L, Shannon M, et al. Recreational music-making modulates the human stress response: a preliminary individualized gene expression study. Med Sci Monit. 2005;11(2):BR31-BR40.
29. Mohd RS. Life event, stress and illness. Malays J Med Sci. 2008;15(4):9-18.
30. U.S Department of Veterans Affairs. PPO 10-075–HSR&D study. U.S Department of Veterans Affairs Website. http://www.hsrd.research.va.gov/research/abstracts.cfm?Project_ID=2141700403. Updated March 24, 2014. Accessed January 20, 2016.
31. Hooten J, Shipman D, Osting V. Posttraumatic stress disorder in veterans: inpatient assessment and management. Fed Pract. 2008;25(1):27-37.
32. WJLA. Music therapy program helps veterans with PTSD. WJLA Website. http://wjla.com/news/nation-world/music-therapy-program-helps-veterans-with-ptsd-98564. Published December 26, 2013. Accessed January 20, 2016.
33. U.S. Census Bureau, Statistical Abstract of the United States: 2011. Arts, recreation and travel section 26. U.S. Census Bureau Website. https://www.census.gov/prod/2011pubs/11statab/arts.pdf. Published 2011. Accessed January 11, 2016.