User login
Medical generalists tell a sad story. Their steadily declining numbers reflect a compensation system that still rewards specialists handsomely at generalists’ expense.
Even though the venerable relative value unit (RVU)-based reimbursement system was intended to equalize pay between primary care’s cognitive work and specialists’ procedure-driven high pay, it hasn’t. Since 1992, when Medicare started paying physicians using RVUs based on the resources used, the specialist-generalist gap remains. RVUs comprise three factors:
- Work (55%);
- Practice expense (42%); and
- Malpractice insurance (3%).
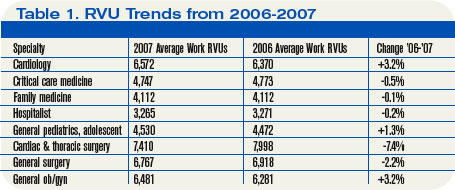
Arguably, generalist RVUs have risen and proceduralist RVUs have decreased. However, generalists argue this skewed pay scale still causes residents to shun internal medicine, hospital medicine, family practice, general pediatrics, and general surgery. Is that true?
Hospitalists and RVUs
Although RVUs don’t always figure into hospitalist compensation, they can have an effect. Vibhu Sharma, MD, of SUNY Downstate Medical Center’s section director, hospital medicine program, heads a 13-hospitalist group employed by the medical center and carries extensive teaching responsibilities.
RVUs don’t currently factor into his hospitalists’ pay but that’s becoming troublesome to Dr. Sharma. “We’d make a lot more money if RVUs were factored in, but they aren’t because we’re a teaching hospital,” he says. “Our group is only four years old, and we aren’t ready to push for it.”
Without the RVU productivity component, Dr. Sharma says he’s at a disadvantage when recruiting. Internal medicine, family practice, and other generalists “stuck with the perception that specialization is a better career option,” he says. “If payers paid us the same as non-invasive cardiologists there’d be a lot more hospitalists.”
Boosts in compensation will be slow in coming, says Dr. Sharma, because hospitalists have demonstrated only modest cost savings and LOS decreases. He adds: “Today nobody wants to be a hospitalist for the rest of their career. We perceive that the patient care we deliver isn’t well compensated, and that the RVU gap between generalists and sub-specialists can never be closed.” As for RVUs, he sees the hospital eventually adding an RVU bonus component. For now, it bumps up hospitalist salaries when the group complains.
The three-member pediatric hospitalist group at Kentucky Children’s Hospital also doesn’t use RVUs, either for compensation or as a productivity proxy. Jeff Bennett, MD, its lead hospitalist, says pediatric outcomes data aren’t robust enough to establish proper RVU benchmarks. He adds that adult RVUs are “denser” than pediatric RVUs because of lower acuity and fewer procedures with children’s illnesses. Additionally, productivity measures don’t affect pediatrics significantly because children’s hospitals “are at the bottom of the funnel,” he says. “We have to take every kid who comes our way. Pediatric hospitals tend not to be competitive. There are four hospitals in town competing for adult patients, while we’re the only tertiary care hospital for 300 miles.”
Compounding the problem is that determining pediatric hospitalist compensation is problematic. With only 2,200 pediatric hospitalists versus 20,000 who work with adults, compensation packages tend to idiosyncratic. “Compensation is important, but RVUs won’t figure into pediatrics for a while,” says Dr. Bennett. “People chose hospital medicine from residency because they’re itching for inpatient work, with its complexity and sharp edges. The shine dims quickly, though, because they are protected during residency and then have full responsibility as hospitalists.”
David Dale, MD, director of the University of Washington’s internal medicine residency program, and American College of Physicians’ president, says hospitalist careers loom large for his annual crop of 35 to 40 residents—but RVUs don’t. “For them it’s an easy transition, a guaranteed salary versus establishing a small business,” he says. “The office practice is where the RVUs really impact generalists. We have a hard job preparing residents for those reimbursement issues.”
Dr. Dale says between two-thirds and three-quarters of his residents become hospitalists, although that’s often not their final career destination. “Some don’t treat hospitalist medicine as a long-term career because the work is hard and the hours are stressful. Many are waiting for a fellowship track to specialization.”
The General Surgeon
A 2007 article by Josef Fischer, MD, in the Journal of the American Medical Association raises questions about the dwindling general surgeon cadre.1 Dr. Fischer posits that RVUs can’t boost surgeons’ incomes because surgeons can’t increase utilization when reimbursement decreases.
For example, since patients have only one gallbladder and indications for removal are constant, there’s no way to increase surgical RVUs. He says this unattractive RVU scheme dissuades residents from general surgery careers.
Dr. Fischer’s concerns don’t faze David Joyce, CEO of Morrisville, N.C.-based Delphi Healthcare Partners, which has three surgicalist programs nationally. Each employs two general surgeons working two weeks on, two weeks off, covering indigent and unassigned patients.
On average, each sees eight patients daily, two requiring surgery. The surgicalists all are either age 50 to 55 or under 35 and reject the hassles of office-based practices at both ends of the career ladder. They earn fixed salaries; Delphi uses RVUs for reimbursement but not for productivity bonuses.
“RVUs aren’t very important in our surgicalist equation, which is a winning situation for everyone involved,” Joyce says. “Private-practice surgeons are thrilled because they don’t cover call and can build their practices. The hospitals do well and don’t mind kicking in several hundred thousand dollars to cover surgicalist compensation.
“In our Charleston, W. Va., program the hospital derived $1.6 million above our program’s cost because the private docs did more surgeries, our surgicalists do what they were trained to do and are well compensated. It’s great,” he says.
Delphi surgicalist Richard Fogle, MD, works at Thomas Memorial Hospital in South Charleston, W. Va., and doesn’t think about RVUs. “The problem with surgeons is lifestyle,” he asserts. “If you have 10 surgeons, you cover call once every 10 days. With three surgeons it’s once every three days.”
Delphi solved his hospital’s problem by recruiting him and another surgicalist. “Before we came most general surgeons had left,” Dr. Fogle says. “Now, two have come back, and four more have settled here. We’re not competing with them for business, and they can build their office practices — particularly with outpatient procedures.”
As a surgicalist, Dr. Fogle, doesn’t miss spending 50% of revenues on office overhead, or leaving 20 patients sitting in his office while answering a hospital page. “I keep waiting for the other shoe to drop, but it hasn’t,” he says of his freedom to practice surgery unfettered by office busyness. He’s happy with the compensation but has a bone to pick with the RVU system. “RVUs are too low for general surgery, and anyone who discounts the cognitive part of surgery procedures is seriously mistaken,” he says.
Different Strokes
John Marcelis, MD, an Erickson Retirement Communities regional medical director of 19 providers in four communities, gives the RVU discussion another twist. He practices at Ann’s Choice in Warminster, Pa., with four other physicians, each of whom acts as the group’s hospitalist once every five weeks.
Previously he spent 10 years at the University of Pennsylvania hospital system, where RVUs figured in significantly and volume was highly rewarded. Taking a huge pay cut to practice at Erickson, he happily left the RVU treadmill. “I didn’t like seeing patients at RVU factories,” he recalls. “At Erickson, we have half-hour office visits and see our hospitalized patients as needed. An RVU system doesn’t compute with us.”
Dr. Marcelis, who lost sleep when he was part of an RVU system, sees a bimodal curve of doctors—some thrive on RVUs, others don’t. “There are some doctors who want to see 50 MIs in a day,” he says. “They relish the high-volume intensity. ‘Bring ’em on,’ they say. RVU systems work well for them. For doctors who value longitudinal relationships with patients, RVUs don’t work well.”
He doesn’t see the cognitive vs. procedure gap leading to RVUs ever closing: “There’s a pool of dollars, and shifting 5% from procedures to cognitive work can’t change things. If payers lower RVUs for procedures, specialists will just do more procedures.” TH
Marlene Piturro is a medical writer based in New York.
Reference
- Fischer J. The impending disappearance of the general surgeon. JAMA. 2007;298:2191-2193.
Medical generalists tell a sad story. Their steadily declining numbers reflect a compensation system that still rewards specialists handsomely at generalists’ expense.
Even though the venerable relative value unit (RVU)-based reimbursement system was intended to equalize pay between primary care’s cognitive work and specialists’ procedure-driven high pay, it hasn’t. Since 1992, when Medicare started paying physicians using RVUs based on the resources used, the specialist-generalist gap remains. RVUs comprise three factors:
- Work (55%);
- Practice expense (42%); and
- Malpractice insurance (3%).
Arguably, generalist RVUs have risen and proceduralist RVUs have decreased. However, generalists argue this skewed pay scale still causes residents to shun internal medicine, hospital medicine, family practice, general pediatrics, and general surgery. Is that true?
Hospitalists and RVUs
Although RVUs don’t always figure into hospitalist compensation, they can have an effect. Vibhu Sharma, MD, of SUNY Downstate Medical Center’s section director, hospital medicine program, heads a 13-hospitalist group employed by the medical center and carries extensive teaching responsibilities.
RVUs don’t currently factor into his hospitalists’ pay but that’s becoming troublesome to Dr. Sharma. “We’d make a lot more money if RVUs were factored in, but they aren’t because we’re a teaching hospital,” he says. “Our group is only four years old, and we aren’t ready to push for it.”
Without the RVU productivity component, Dr. Sharma says he’s at a disadvantage when recruiting. Internal medicine, family practice, and other generalists “stuck with the perception that specialization is a better career option,” he says. “If payers paid us the same as non-invasive cardiologists there’d be a lot more hospitalists.”
Boosts in compensation will be slow in coming, says Dr. Sharma, because hospitalists have demonstrated only modest cost savings and LOS decreases. He adds: “Today nobody wants to be a hospitalist for the rest of their career. We perceive that the patient care we deliver isn’t well compensated, and that the RVU gap between generalists and sub-specialists can never be closed.” As for RVUs, he sees the hospital eventually adding an RVU bonus component. For now, it bumps up hospitalist salaries when the group complains.
The three-member pediatric hospitalist group at Kentucky Children’s Hospital also doesn’t use RVUs, either for compensation or as a productivity proxy. Jeff Bennett, MD, its lead hospitalist, says pediatric outcomes data aren’t robust enough to establish proper RVU benchmarks. He adds that adult RVUs are “denser” than pediatric RVUs because of lower acuity and fewer procedures with children’s illnesses. Additionally, productivity measures don’t affect pediatrics significantly because children’s hospitals “are at the bottom of the funnel,” he says. “We have to take every kid who comes our way. Pediatric hospitals tend not to be competitive. There are four hospitals in town competing for adult patients, while we’re the only tertiary care hospital for 300 miles.”
Compounding the problem is that determining pediatric hospitalist compensation is problematic. With only 2,200 pediatric hospitalists versus 20,000 who work with adults, compensation packages tend to idiosyncratic. “Compensation is important, but RVUs won’t figure into pediatrics for a while,” says Dr. Bennett. “People chose hospital medicine from residency because they’re itching for inpatient work, with its complexity and sharp edges. The shine dims quickly, though, because they are protected during residency and then have full responsibility as hospitalists.”
David Dale, MD, director of the University of Washington’s internal medicine residency program, and American College of Physicians’ president, says hospitalist careers loom large for his annual crop of 35 to 40 residents—but RVUs don’t. “For them it’s an easy transition, a guaranteed salary versus establishing a small business,” he says. “The office practice is where the RVUs really impact generalists. We have a hard job preparing residents for those reimbursement issues.”
Dr. Dale says between two-thirds and three-quarters of his residents become hospitalists, although that’s often not their final career destination. “Some don’t treat hospitalist medicine as a long-term career because the work is hard and the hours are stressful. Many are waiting for a fellowship track to specialization.”
The General Surgeon
A 2007 article by Josef Fischer, MD, in the Journal of the American Medical Association raises questions about the dwindling general surgeon cadre.1 Dr. Fischer posits that RVUs can’t boost surgeons’ incomes because surgeons can’t increase utilization when reimbursement decreases.
For example, since patients have only one gallbladder and indications for removal are constant, there’s no way to increase surgical RVUs. He says this unattractive RVU scheme dissuades residents from general surgery careers.
Dr. Fischer’s concerns don’t faze David Joyce, CEO of Morrisville, N.C.-based Delphi Healthcare Partners, which has three surgicalist programs nationally. Each employs two general surgeons working two weeks on, two weeks off, covering indigent and unassigned patients.
On average, each sees eight patients daily, two requiring surgery. The surgicalists all are either age 50 to 55 or under 35 and reject the hassles of office-based practices at both ends of the career ladder. They earn fixed salaries; Delphi uses RVUs for reimbursement but not for productivity bonuses.
“RVUs aren’t very important in our surgicalist equation, which is a winning situation for everyone involved,” Joyce says. “Private-practice surgeons are thrilled because they don’t cover call and can build their practices. The hospitals do well and don’t mind kicking in several hundred thousand dollars to cover surgicalist compensation.
“In our Charleston, W. Va., program the hospital derived $1.6 million above our program’s cost because the private docs did more surgeries, our surgicalists do what they were trained to do and are well compensated. It’s great,” he says.
Delphi surgicalist Richard Fogle, MD, works at Thomas Memorial Hospital in South Charleston, W. Va., and doesn’t think about RVUs. “The problem with surgeons is lifestyle,” he asserts. “If you have 10 surgeons, you cover call once every 10 days. With three surgeons it’s once every three days.”
Delphi solved his hospital’s problem by recruiting him and another surgicalist. “Before we came most general surgeons had left,” Dr. Fogle says. “Now, two have come back, and four more have settled here. We’re not competing with them for business, and they can build their office practices — particularly with outpatient procedures.”
As a surgicalist, Dr. Fogle, doesn’t miss spending 50% of revenues on office overhead, or leaving 20 patients sitting in his office while answering a hospital page. “I keep waiting for the other shoe to drop, but it hasn’t,” he says of his freedom to practice surgery unfettered by office busyness. He’s happy with the compensation but has a bone to pick with the RVU system. “RVUs are too low for general surgery, and anyone who discounts the cognitive part of surgery procedures is seriously mistaken,” he says.
Different Strokes
John Marcelis, MD, an Erickson Retirement Communities regional medical director of 19 providers in four communities, gives the RVU discussion another twist. He practices at Ann’s Choice in Warminster, Pa., with four other physicians, each of whom acts as the group’s hospitalist once every five weeks.
Previously he spent 10 years at the University of Pennsylvania hospital system, where RVUs figured in significantly and volume was highly rewarded. Taking a huge pay cut to practice at Erickson, he happily left the RVU treadmill. “I didn’t like seeing patients at RVU factories,” he recalls. “At Erickson, we have half-hour office visits and see our hospitalized patients as needed. An RVU system doesn’t compute with us.”
Dr. Marcelis, who lost sleep when he was part of an RVU system, sees a bimodal curve of doctors—some thrive on RVUs, others don’t. “There are some doctors who want to see 50 MIs in a day,” he says. “They relish the high-volume intensity. ‘Bring ’em on,’ they say. RVU systems work well for them. For doctors who value longitudinal relationships with patients, RVUs don’t work well.”
He doesn’t see the cognitive vs. procedure gap leading to RVUs ever closing: “There’s a pool of dollars, and shifting 5% from procedures to cognitive work can’t change things. If payers lower RVUs for procedures, specialists will just do more procedures.” TH
Marlene Piturro is a medical writer based in New York.
Reference
- Fischer J. The impending disappearance of the general surgeon. JAMA. 2007;298:2191-2193.
Medical generalists tell a sad story. Their steadily declining numbers reflect a compensation system that still rewards specialists handsomely at generalists’ expense.
Even though the venerable relative value unit (RVU)-based reimbursement system was intended to equalize pay between primary care’s cognitive work and specialists’ procedure-driven high pay, it hasn’t. Since 1992, when Medicare started paying physicians using RVUs based on the resources used, the specialist-generalist gap remains. RVUs comprise three factors:
- Work (55%);
- Practice expense (42%); and
- Malpractice insurance (3%).
Arguably, generalist RVUs have risen and proceduralist RVUs have decreased. However, generalists argue this skewed pay scale still causes residents to shun internal medicine, hospital medicine, family practice, general pediatrics, and general surgery. Is that true?
Hospitalists and RVUs
Although RVUs don’t always figure into hospitalist compensation, they can have an effect. Vibhu Sharma, MD, of SUNY Downstate Medical Center’s section director, hospital medicine program, heads a 13-hospitalist group employed by the medical center and carries extensive teaching responsibilities.
RVUs don’t currently factor into his hospitalists’ pay but that’s becoming troublesome to Dr. Sharma. “We’d make a lot more money if RVUs were factored in, but they aren’t because we’re a teaching hospital,” he says. “Our group is only four years old, and we aren’t ready to push for it.”
Without the RVU productivity component, Dr. Sharma says he’s at a disadvantage when recruiting. Internal medicine, family practice, and other generalists “stuck with the perception that specialization is a better career option,” he says. “If payers paid us the same as non-invasive cardiologists there’d be a lot more hospitalists.”
Boosts in compensation will be slow in coming, says Dr. Sharma, because hospitalists have demonstrated only modest cost savings and LOS decreases. He adds: “Today nobody wants to be a hospitalist for the rest of their career. We perceive that the patient care we deliver isn’t well compensated, and that the RVU gap between generalists and sub-specialists can never be closed.” As for RVUs, he sees the hospital eventually adding an RVU bonus component. For now, it bumps up hospitalist salaries when the group complains.
The three-member pediatric hospitalist group at Kentucky Children’s Hospital also doesn’t use RVUs, either for compensation or as a productivity proxy. Jeff Bennett, MD, its lead hospitalist, says pediatric outcomes data aren’t robust enough to establish proper RVU benchmarks. He adds that adult RVUs are “denser” than pediatric RVUs because of lower acuity and fewer procedures with children’s illnesses. Additionally, productivity measures don’t affect pediatrics significantly because children’s hospitals “are at the bottom of the funnel,” he says. “We have to take every kid who comes our way. Pediatric hospitals tend not to be competitive. There are four hospitals in town competing for adult patients, while we’re the only tertiary care hospital for 300 miles.”
Compounding the problem is that determining pediatric hospitalist compensation is problematic. With only 2,200 pediatric hospitalists versus 20,000 who work with adults, compensation packages tend to idiosyncratic. “Compensation is important, but RVUs won’t figure into pediatrics for a while,” says Dr. Bennett. “People chose hospital medicine from residency because they’re itching for inpatient work, with its complexity and sharp edges. The shine dims quickly, though, because they are protected during residency and then have full responsibility as hospitalists.”
David Dale, MD, director of the University of Washington’s internal medicine residency program, and American College of Physicians’ president, says hospitalist careers loom large for his annual crop of 35 to 40 residents—but RVUs don’t. “For them it’s an easy transition, a guaranteed salary versus establishing a small business,” he says. “The office practice is where the RVUs really impact generalists. We have a hard job preparing residents for those reimbursement issues.”
Dr. Dale says between two-thirds and three-quarters of his residents become hospitalists, although that’s often not their final career destination. “Some don’t treat hospitalist medicine as a long-term career because the work is hard and the hours are stressful. Many are waiting for a fellowship track to specialization.”
The General Surgeon
A 2007 article by Josef Fischer, MD, in the Journal of the American Medical Association raises questions about the dwindling general surgeon cadre.1 Dr. Fischer posits that RVUs can’t boost surgeons’ incomes because surgeons can’t increase utilization when reimbursement decreases.
For example, since patients have only one gallbladder and indications for removal are constant, there’s no way to increase surgical RVUs. He says this unattractive RVU scheme dissuades residents from general surgery careers.
Dr. Fischer’s concerns don’t faze David Joyce, CEO of Morrisville, N.C.-based Delphi Healthcare Partners, which has three surgicalist programs nationally. Each employs two general surgeons working two weeks on, two weeks off, covering indigent and unassigned patients.
On average, each sees eight patients daily, two requiring surgery. The surgicalists all are either age 50 to 55 or under 35 and reject the hassles of office-based practices at both ends of the career ladder. They earn fixed salaries; Delphi uses RVUs for reimbursement but not for productivity bonuses.
“RVUs aren’t very important in our surgicalist equation, which is a winning situation for everyone involved,” Joyce says. “Private-practice surgeons are thrilled because they don’t cover call and can build their practices. The hospitals do well and don’t mind kicking in several hundred thousand dollars to cover surgicalist compensation.
“In our Charleston, W. Va., program the hospital derived $1.6 million above our program’s cost because the private docs did more surgeries, our surgicalists do what they were trained to do and are well compensated. It’s great,” he says.
Delphi surgicalist Richard Fogle, MD, works at Thomas Memorial Hospital in South Charleston, W. Va., and doesn’t think about RVUs. “The problem with surgeons is lifestyle,” he asserts. “If you have 10 surgeons, you cover call once every 10 days. With three surgeons it’s once every three days.”
Delphi solved his hospital’s problem by recruiting him and another surgicalist. “Before we came most general surgeons had left,” Dr. Fogle says. “Now, two have come back, and four more have settled here. We’re not competing with them for business, and they can build their office practices — particularly with outpatient procedures.”
As a surgicalist, Dr. Fogle, doesn’t miss spending 50% of revenues on office overhead, or leaving 20 patients sitting in his office while answering a hospital page. “I keep waiting for the other shoe to drop, but it hasn’t,” he says of his freedom to practice surgery unfettered by office busyness. He’s happy with the compensation but has a bone to pick with the RVU system. “RVUs are too low for general surgery, and anyone who discounts the cognitive part of surgery procedures is seriously mistaken,” he says.
Different Strokes
John Marcelis, MD, an Erickson Retirement Communities regional medical director of 19 providers in four communities, gives the RVU discussion another twist. He practices at Ann’s Choice in Warminster, Pa., with four other physicians, each of whom acts as the group’s hospitalist once every five weeks.
Previously he spent 10 years at the University of Pennsylvania hospital system, where RVUs figured in significantly and volume was highly rewarded. Taking a huge pay cut to practice at Erickson, he happily left the RVU treadmill. “I didn’t like seeing patients at RVU factories,” he recalls. “At Erickson, we have half-hour office visits and see our hospitalized patients as needed. An RVU system doesn’t compute with us.”
Dr. Marcelis, who lost sleep when he was part of an RVU system, sees a bimodal curve of doctors—some thrive on RVUs, others don’t. “There are some doctors who want to see 50 MIs in a day,” he says. “They relish the high-volume intensity. ‘Bring ’em on,’ they say. RVU systems work well for them. For doctors who value longitudinal relationships with patients, RVUs don’t work well.”
He doesn’t see the cognitive vs. procedure gap leading to RVUs ever closing: “There’s a pool of dollars, and shifting 5% from procedures to cognitive work can’t change things. If payers lower RVUs for procedures, specialists will just do more procedures.” TH
Marlene Piturro is a medical writer based in New York.
Reference
- Fischer J. The impending disappearance of the general surgeon. JAMA. 2007;298:2191-2193.