User login
Tackle Medical School Debt
Overwhelmed by medical school debt? You're not alone. A 2008 American Medical Association survey showed that the average 2007 medical school graduate was left with a $139,000 debt burden and a powerful incentive to avoid primary care.
But according to Renee Zerehi, the American College of Physicians' manager of health policy, increasing numbers of students choose HM because of flexible scheduling and opportunities to reduce their debt. Zerehi and Bijo Chacko, MD, FHM, a member of SHM's Young Physicians Committee and hospitalist program medical director for Preferred Health Partners in New York City, offer these strategies for debt reduction.
•Understand your debt portfolio: Talk to a financial consultant to assess debt, your family situation, and lifestyle issues. "A strong, keen understanding of how debt impacts your budget is essential," Dr. Chacko says. Medical school loans often come with different interest rates and grace periods, so try to pay off the high-interest loans immediately, he explains.
•Consolidate your debt: Loans from different lenders with different balances, interest rates, and due dates may best be handled by a federal consolidation loan. The AMA explains it all in
"The Ins and Outs of Student Loan Consolidation."
•Student loan forgiveness: A number of hospitalist programs offer loan repayment programs. The National Health Service Corps, the Health Professions Scholarship Program, and state loan repayment programs offer loan forgiveness for physicians practicing in underserved areas. Visit the AAMC Web site for a comprehensive list.
•NIH Faculty Loan Forgiveness: For academic hospitalists doing research, the National Institutes of Health (NIH) offers up to $35,000 a year for loan repayment and tax reimbursement for each year of service.
For more information, visit SHM's Young Physician microsite.
Overwhelmed by medical school debt? You're not alone. A 2008 American Medical Association survey showed that the average 2007 medical school graduate was left with a $139,000 debt burden and a powerful incentive to avoid primary care.
But according to Renee Zerehi, the American College of Physicians' manager of health policy, increasing numbers of students choose HM because of flexible scheduling and opportunities to reduce their debt. Zerehi and Bijo Chacko, MD, FHM, a member of SHM's Young Physicians Committee and hospitalist program medical director for Preferred Health Partners in New York City, offer these strategies for debt reduction.
•Understand your debt portfolio: Talk to a financial consultant to assess debt, your family situation, and lifestyle issues. "A strong, keen understanding of how debt impacts your budget is essential," Dr. Chacko says. Medical school loans often come with different interest rates and grace periods, so try to pay off the high-interest loans immediately, he explains.
•Consolidate your debt: Loans from different lenders with different balances, interest rates, and due dates may best be handled by a federal consolidation loan. The AMA explains it all in
"The Ins and Outs of Student Loan Consolidation."
•Student loan forgiveness: A number of hospitalist programs offer loan repayment programs. The National Health Service Corps, the Health Professions Scholarship Program, and state loan repayment programs offer loan forgiveness for physicians practicing in underserved areas. Visit the AAMC Web site for a comprehensive list.
•NIH Faculty Loan Forgiveness: For academic hospitalists doing research, the National Institutes of Health (NIH) offers up to $35,000 a year for loan repayment and tax reimbursement for each year of service.
For more information, visit SHM's Young Physician microsite.
Overwhelmed by medical school debt? You're not alone. A 2008 American Medical Association survey showed that the average 2007 medical school graduate was left with a $139,000 debt burden and a powerful incentive to avoid primary care.
But according to Renee Zerehi, the American College of Physicians' manager of health policy, increasing numbers of students choose HM because of flexible scheduling and opportunities to reduce their debt. Zerehi and Bijo Chacko, MD, FHM, a member of SHM's Young Physicians Committee and hospitalist program medical director for Preferred Health Partners in New York City, offer these strategies for debt reduction.
•Understand your debt portfolio: Talk to a financial consultant to assess debt, your family situation, and lifestyle issues. "A strong, keen understanding of how debt impacts your budget is essential," Dr. Chacko says. Medical school loans often come with different interest rates and grace periods, so try to pay off the high-interest loans immediately, he explains.
•Consolidate your debt: Loans from different lenders with different balances, interest rates, and due dates may best be handled by a federal consolidation loan. The AMA explains it all in
"The Ins and Outs of Student Loan Consolidation."
•Student loan forgiveness: A number of hospitalist programs offer loan repayment programs. The National Health Service Corps, the Health Professions Scholarship Program, and state loan repayment programs offer loan forgiveness for physicians practicing in underserved areas. Visit the AAMC Web site for a comprehensive list.
•NIH Faculty Loan Forgiveness: For academic hospitalists doing research, the National Institutes of Health (NIH) offers up to $35,000 a year for loan repayment and tax reimbursement for each year of service.
For more information, visit SHM's Young Physician microsite.
Consumer-Driven Healthcare
Joseph Forrester, DO, a critical-care hospitalist and pulmonologist in Denver, discovered firsthand how scoping out and paying for healthcare now resembles shopping for other big-ticket items. Unlike purchasing and paying down a diamond ring or a 60-inch flat-screen TV, for which the final price and payment is duly noted and balances promptly adjusted, hospital billing attempted to overcharge Dr. Forrester by 500%. He already had paid $4,000 toward his 2008 out-of-pocket deductible for medical expenses and was surprised when the hospital said he would have to pay the full $5,000 deductible before he could receive care. The savvy doc went to a real-time claims adjudication tool that he uses in his own practice to show the hospital he’d already satisfied the first 80% of the $5,000 deductible.
The hospital’s billing department listened and responded.
Dr. Forrester paid the remaining $1,000 to fulfill his deductible, and his insurer covered the rest of the treatment cost. “Having access to this information allowed him to receive care immediately, without having to wait weeks for the hospital to correct its mistaken information,” says Chris Stanley, MD, a medical director with United Healthcare.
High-deductible health plans (HDHPs) like Dr. Forrester’s have been growing in popularity since the establishment of health savings accounts (HSAs). Designed to help individuals save for future medical and retiree health expenses on a tax-free basis, HSAs were signed into law by President Bush in December 2003. These products are just beginning to influence how hospitals collect fees and how patients negotiate with their physicians—including hospitalists—about which medications, tests, and procedures they’re willing to pay for.
Break from Tradition

According to the U.S. Treasury Department Web site, HSAs allow individuals to “own and control the money in your HSA. Decisions on how to spend the money are made by the consumer without relying on a third party or a health insurer. Consumers will also decide what types of investments to make with the money in the account in order to make it grow.”
HSAs only are available to individuals covered solely through an HDHP. Individuals receiving veterans benefits or already on Medicare are not eligible; however, if they establish an HSA before enrolling in Medicare, they can keep it—but not add to it.
HDHPs offer consumers—especially young, healthy individuals—low premiums and high deductibles (between $1,150 and $2,900 for individuals and $2,300 to $5,800 for family plans). In addition to paying a low premium, consumers can put money into an HSA to pay for out-of-pocket expenses, including deductibles, co-pays, and co-insurance. The maximum amount of tax-free money a consumer can stash in an HSA this year is $5,800 for individuals and $11,600 for families. (Those 55 and older can contribute an additional $1,000 annually to their HSAs to accelerate their savings rates.)
Consumers can access HSA funds through a debit card, or they can pay for a service, then file for reimbursement.
An HSA should not be confused with a flexible spending account (FSA). Both are paid for by employees with pre-tax dollars; however, FSAs:
- Carry no insurance requirements;
- Are capped at $5,000 in annual contributions;
- Do not pay interest on the account balance; and
- Must be used—or forfeited—by the end of the plan year.
In contrast, an HSA:
- Is funded by the employee or jointly by employer and employee (known as a health reimbursement account, or HRA);
- Has insurance requirements on deductibles and out-of-pocket contributions;
- Pays the provider directly and submits receipts to the account administrator;
- Accumulates interest through a financial institution; and
- Allows unused funds to be carried forward.
Easy Business Decision
Employers are jumping on the HDHP bandwagon, largely to shift more health insurance costs to employees. HDHPs allow consumers to save on upfront costs (e.g., premiums and routine medical expenses) while allowing them to partner with their physicians when deciding how and when they will spend their HSA dollars.
Allowing patients to be involved in the testing, medication, and length-of-stay decisions relative to their care is a reversal from the status quo. Physicians working with hospitalized patients aren’t used to patients questioning treatment or asking for a cost analysis of medications. Another way to think about working with patients who have nontraditional plans: If you were eating at a soup kitchen, you probably wouldn’t complain about having to eat off of paper plates. But if you were dining at a five-star restaurant, you’d freely complain to the maître d’ if your soup was cold or the salad limp.
The 2008 National Study of Employer-Sponsored Health Plans, conducted by international human resources consulting firm Mercer, reported consumer-directed health plans, coupled with either an HSA or an HRA, are offered by 45% of companies with 25,000 or more employees (up from 22% in 2005). Nine percent of companies with 10 to 499 employees offer consumer-directed health plans, up from 2% in 2005.
Mercer partner Blaine Bos notes that raising deductibles is the fallback for employers faced with medical cost increases they can’t—or won’t—absorb. “The introduction of HSAs may have changed employers’ thinking on just how high a deductible can go without causing employees to revolt,” Bos says in the survey analysis. He predicts bad economic times will accelerate consumer-directed health plan uptake in small and large firms because they deliver substantially lower costs than PPOs and HMOs. In 2008, CDHP costs averaged $6,207 per employee, compared with $7,815 for PPOs and $7,768 for HMOs.
Data from ehealthinsurance.com indicate consumers are taking full advantage of HDHPs: Fifteen percent choose the highest deductibles, 48% the mid-range, and 37% the lowest deductible.
Still on HM’s Horizon
Consumer-driven healthcare has yet to significantly affect hospitals and—by extension—HM groups, although hospital admissions were down 2% nationally in 2008 and hospital debts are climbing. Adam Singer, MD, CEO of IPC: The Hospitalist Company, says the impact of HSAs on HM isn’t noticeable yet because patients haven’t adapted to the new model. “Consumers usually aren’t price-shopping the facility, because they’re committed to their physicians and will go to the hospital where their physician has privileges,” Dr. Singer says. “Additionally, the patients hospitalists see are very sick. Many came in through the ED and had no choice about how they got there. They certainly don’t pick their hospitalists.”
By extension, the ED isn’t immune to market forces driving consumer-directed care. Karen McConnell, PhD, director of the Oregon Health and Science University’s Center for Policy and Research in Emergency Medicine, posits that rapid adoption of high-deductible plans could change ED utilization (Ann Emerg Med. 2005;46(6):536-40). Although the ED may be insulated from extensive shopping and price negotiation because visits generally are for urgent conditions, Dr. McConnell says, ED utilization patterns may change if cost-conscious HSA holders forego other necessary medical care or seek substitutes for less-urgent problems.
The reality of consumer-directed healthcare and patients footing more of their own medical bills could eventually have a significant impact on HM programs. “Hospitals are under attack,” Dr. Singer says. “The 20% to 50% of hospital medicine program revenues received as support payments from their hospitals may drop as high-deductible plans with HSAs drive down hospital revenues. So as hospital revenues fall, the subsidies—particularly some of the more absurd, seven-figure subsidies that hospitalists enjoy—are vulnerable.”
Patients Take Charge
With their own money at stake, HSA consumers are engaged in the decision to spend—or save—their healthcare dollars. Although the shift in the doctor-patient decision-making process has slowly found its way into the hospital, it is playing out in doctor’s offices—one of several pipelines for hospital admissions. As a consumer, Linda Waldmann, manager of MyCost, a real-time claims-adjudication tool offered by Alegent Health, introduced cost when making treatment decisions after she was diagnosed with carpal tunnel syndrome. She asked her orthopedic surgeon lots of questions, absorbed what he said, then made her own treatment choices.
“My orthopedist wanted me to have three tests, but I elected to postpone one test until my HSA replenished the following year,” Waldmann says. “Doctors are still hesitant about negotiating with patients, but this one understood my concern.”
Blue Cross/Blue Shield of Tennessee’s (BCBST) Maggie Fox, director of application systems, saw a large jump (to 33% in 2009 from 8% in 2008) among BCBST’s 5,000 employees opting for HSAs. The Tennessee company emphasizes prevention, education, and wellness as critical components of consumer-directed care, and the company’s HSA consumers are offered a variety of discounts for adhering to healthy lifestyles.
At BCBST, HSAs have opened dialogue between patients, physicians, and hospitals. Through a Web-based portal called “Blue Access,” providers receive information on a patient’s financial liability in as little as 10 seconds. “HSAs and HRAs have created a patient liability that never existed before,” Fox says. “Higher out-of-pocket costs change everything. Providers need to collect payment at the point of care, whether that’s the office or hospital. There’s more work at checkout, but at least patients and providers know the exact amount the care costs and how much the patient has to pay.”
Davis Liu, MD, a Wharton School of Business graduate and family physician with Northern California Permanente Medical Group, advises hospitalists to be ready for patients with HSAs to challenge treatment decisions because of the cost. He says hospitalists must prepare to communicate clearly and effectively with HSA patients, especially when it comes to necessary testing and medications. The task might be difficult because information about testing costs and procedures is limited, and prices vary dramatically by hospital and region. “While it is extremely unlikely that patients will refuse testing when hospitalized, hospitalists must be acutely aware that these patients may skip follow-up appointments, testing, and surgeries,” Dr. Liu says.
United Healthcare’s Dr. Stanley sees physician decision-making evolving as HSA patients become more aware of the economics of treatment options. “Patients are already questioning doctors who order four tests when they’re only willing to pay for three, wanting to postpone procedures, and asking about costs for additional tests and procedures,” he says. “Eventually, cost consciousness will impact group practices. They will have to decrease overhead, revamp collection processes, and strive for administrative simplicity.” Woe to the physician who believes cost isn’t their responsibility, Dr. Stanley says, as they “must realize they’re small-business owners and act accordingly.”
The Future
Consumer-driven healthcare might have little effect on hospitals right now, but change is on the horizon, according to Greg Scandlen, president and CEO of Consumers for Health Care Choice in Hagerstown, Md. He cites the 2008 National Health Interview Survey conducted by the Centers for Disease Control and Prevention, which shows 20% of Americans have an HDHP, as proof positive these new plans are increasing market penetration.
“We’re at a tipping point where every provider will have to deal with cash-paying clients,” he says. “Hospitals with Chargemaster pricing [the list price for services and procedures charged to self-pay and other uninsured clients, usually three to three and a half times the normal Medicare reimbursement] won’t get away with that much longer. They’ll have to charge reasonable, negotiated rates rather than slamming self-pay patients.”
It looks as though the days when patients entered the hospital worried about getting well and dealing with the bills later will soon be in the rearview mirror. Not far into the future, individuals with self-pay components to their health insurance might demand and receive full financial disclosure of all their expected hospital costs (see “Patients Can Shop Around,” p. 29) at the time of admission, with necessary adjustments at discharge.
“Hospitals can’t have secret pricing in a transparent, consumer-driven world,” says Scandlen. “The HDHP model hasn’t fully hit hospitals yet, but they’ll get clobbered in about two years if they don’t adapt.” TH
Marlene Piturro is a freelance writer based in Hastings-on-Hudson, NY.
Joseph Forrester, DO, a critical-care hospitalist and pulmonologist in Denver, discovered firsthand how scoping out and paying for healthcare now resembles shopping for other big-ticket items. Unlike purchasing and paying down a diamond ring or a 60-inch flat-screen TV, for which the final price and payment is duly noted and balances promptly adjusted, hospital billing attempted to overcharge Dr. Forrester by 500%. He already had paid $4,000 toward his 2008 out-of-pocket deductible for medical expenses and was surprised when the hospital said he would have to pay the full $5,000 deductible before he could receive care. The savvy doc went to a real-time claims adjudication tool that he uses in his own practice to show the hospital he’d already satisfied the first 80% of the $5,000 deductible.
The hospital’s billing department listened and responded.
Dr. Forrester paid the remaining $1,000 to fulfill his deductible, and his insurer covered the rest of the treatment cost. “Having access to this information allowed him to receive care immediately, without having to wait weeks for the hospital to correct its mistaken information,” says Chris Stanley, MD, a medical director with United Healthcare.
High-deductible health plans (HDHPs) like Dr. Forrester’s have been growing in popularity since the establishment of health savings accounts (HSAs). Designed to help individuals save for future medical and retiree health expenses on a tax-free basis, HSAs were signed into law by President Bush in December 2003. These products are just beginning to influence how hospitals collect fees and how patients negotiate with their physicians—including hospitalists—about which medications, tests, and procedures they’re willing to pay for.
Break from Tradition
According to the U.S. Treasury Department Web site, HSAs allow individuals to “own and control the money in your HSA. Decisions on how to spend the money are made by the consumer without relying on a third party or a health insurer. Consumers will also decide what types of investments to make with the money in the account in order to make it grow.”
HSAs only are available to individuals covered solely through an HDHP. Individuals receiving veterans benefits or already on Medicare are not eligible; however, if they establish an HSA before enrolling in Medicare, they can keep it—but not add to it.
HDHPs offer consumers—especially young, healthy individuals—low premiums and high deductibles (between $1,150 and $2,900 for individuals and $2,300 to $5,800 for family plans). In addition to paying a low premium, consumers can put money into an HSA to pay for out-of-pocket expenses, including deductibles, co-pays, and co-insurance. The maximum amount of tax-free money a consumer can stash in an HSA this year is $5,800 for individuals and $11,600 for families. (Those 55 and older can contribute an additional $1,000 annually to their HSAs to accelerate their savings rates.)
Consumers can access HSA funds through a debit card, or they can pay for a service, then file for reimbursement.
An HSA should not be confused with a flexible spending account (FSA). Both are paid for by employees with pre-tax dollars; however, FSAs:
- Carry no insurance requirements;
- Are capped at $5,000 in annual contributions;
- Do not pay interest on the account balance; and
- Must be used—or forfeited—by the end of the plan year.
In contrast, an HSA:
- Is funded by the employee or jointly by employer and employee (known as a health reimbursement account, or HRA);
- Has insurance requirements on deductibles and out-of-pocket contributions;
- Pays the provider directly and submits receipts to the account administrator;
- Accumulates interest through a financial institution; and
- Allows unused funds to be carried forward.
Easy Business Decision
Employers are jumping on the HDHP bandwagon, largely to shift more health insurance costs to employees. HDHPs allow consumers to save on upfront costs (e.g., premiums and routine medical expenses) while allowing them to partner with their physicians when deciding how and when they will spend their HSA dollars.
Allowing patients to be involved in the testing, medication, and length-of-stay decisions relative to their care is a reversal from the status quo. Physicians working with hospitalized patients aren’t used to patients questioning treatment or asking for a cost analysis of medications. Another way to think about working with patients who have nontraditional plans: If you were eating at a soup kitchen, you probably wouldn’t complain about having to eat off of paper plates. But if you were dining at a five-star restaurant, you’d freely complain to the maître d’ if your soup was cold or the salad limp.
The 2008 National Study of Employer-Sponsored Health Plans, conducted by international human resources consulting firm Mercer, reported consumer-directed health plans, coupled with either an HSA or an HRA, are offered by 45% of companies with 25,000 or more employees (up from 22% in 2005). Nine percent of companies with 10 to 499 employees offer consumer-directed health plans, up from 2% in 2005.
Mercer partner Blaine Bos notes that raising deductibles is the fallback for employers faced with medical cost increases they can’t—or won’t—absorb. “The introduction of HSAs may have changed employers’ thinking on just how high a deductible can go without causing employees to revolt,” Bos says in the survey analysis. He predicts bad economic times will accelerate consumer-directed health plan uptake in small and large firms because they deliver substantially lower costs than PPOs and HMOs. In 2008, CDHP costs averaged $6,207 per employee, compared with $7,815 for PPOs and $7,768 for HMOs.
Data from ehealthinsurance.com indicate consumers are taking full advantage of HDHPs: Fifteen percent choose the highest deductibles, 48% the mid-range, and 37% the lowest deductible.
Still on HM’s Horizon
Consumer-driven healthcare has yet to significantly affect hospitals and—by extension—HM groups, although hospital admissions were down 2% nationally in 2008 and hospital debts are climbing. Adam Singer, MD, CEO of IPC: The Hospitalist Company, says the impact of HSAs on HM isn’t noticeable yet because patients haven’t adapted to the new model. “Consumers usually aren’t price-shopping the facility, because they’re committed to their physicians and will go to the hospital where their physician has privileges,” Dr. Singer says. “Additionally, the patients hospitalists see are very sick. Many came in through the ED and had no choice about how they got there. They certainly don’t pick their hospitalists.”
By extension, the ED isn’t immune to market forces driving consumer-directed care. Karen McConnell, PhD, director of the Oregon Health and Science University’s Center for Policy and Research in Emergency Medicine, posits that rapid adoption of high-deductible plans could change ED utilization (Ann Emerg Med. 2005;46(6):536-40). Although the ED may be insulated from extensive shopping and price negotiation because visits generally are for urgent conditions, Dr. McConnell says, ED utilization patterns may change if cost-conscious HSA holders forego other necessary medical care or seek substitutes for less-urgent problems.
The reality of consumer-directed healthcare and patients footing more of their own medical bills could eventually have a significant impact on HM programs. “Hospitals are under attack,” Dr. Singer says. “The 20% to 50% of hospital medicine program revenues received as support payments from their hospitals may drop as high-deductible plans with HSAs drive down hospital revenues. So as hospital revenues fall, the subsidies—particularly some of the more absurd, seven-figure subsidies that hospitalists enjoy—are vulnerable.”
Patients Take Charge
With their own money at stake, HSA consumers are engaged in the decision to spend—or save—their healthcare dollars. Although the shift in the doctor-patient decision-making process has slowly found its way into the hospital, it is playing out in doctor’s offices—one of several pipelines for hospital admissions. As a consumer, Linda Waldmann, manager of MyCost, a real-time claims-adjudication tool offered by Alegent Health, introduced cost when making treatment decisions after she was diagnosed with carpal tunnel syndrome. She asked her orthopedic surgeon lots of questions, absorbed what he said, then made her own treatment choices.
“My orthopedist wanted me to have three tests, but I elected to postpone one test until my HSA replenished the following year,” Waldmann says. “Doctors are still hesitant about negotiating with patients, but this one understood my concern.”
Blue Cross/Blue Shield of Tennessee’s (BCBST) Maggie Fox, director of application systems, saw a large jump (to 33% in 2009 from 8% in 2008) among BCBST’s 5,000 employees opting for HSAs. The Tennessee company emphasizes prevention, education, and wellness as critical components of consumer-directed care, and the company’s HSA consumers are offered a variety of discounts for adhering to healthy lifestyles.
At BCBST, HSAs have opened dialogue between patients, physicians, and hospitals. Through a Web-based portal called “Blue Access,” providers receive information on a patient’s financial liability in as little as 10 seconds. “HSAs and HRAs have created a patient liability that never existed before,” Fox says. “Higher out-of-pocket costs change everything. Providers need to collect payment at the point of care, whether that’s the office or hospital. There’s more work at checkout, but at least patients and providers know the exact amount the care costs and how much the patient has to pay.”
Davis Liu, MD, a Wharton School of Business graduate and family physician with Northern California Permanente Medical Group, advises hospitalists to be ready for patients with HSAs to challenge treatment decisions because of the cost. He says hospitalists must prepare to communicate clearly and effectively with HSA patients, especially when it comes to necessary testing and medications. The task might be difficult because information about testing costs and procedures is limited, and prices vary dramatically by hospital and region. “While it is extremely unlikely that patients will refuse testing when hospitalized, hospitalists must be acutely aware that these patients may skip follow-up appointments, testing, and surgeries,” Dr. Liu says.
United Healthcare’s Dr. Stanley sees physician decision-making evolving as HSA patients become more aware of the economics of treatment options. “Patients are already questioning doctors who order four tests when they’re only willing to pay for three, wanting to postpone procedures, and asking about costs for additional tests and procedures,” he says. “Eventually, cost consciousness will impact group practices. They will have to decrease overhead, revamp collection processes, and strive for administrative simplicity.” Woe to the physician who believes cost isn’t their responsibility, Dr. Stanley says, as they “must realize they’re small-business owners and act accordingly.”
The Future
Consumer-driven healthcare might have little effect on hospitals right now, but change is on the horizon, according to Greg Scandlen, president and CEO of Consumers for Health Care Choice in Hagerstown, Md. He cites the 2008 National Health Interview Survey conducted by the Centers for Disease Control and Prevention, which shows 20% of Americans have an HDHP, as proof positive these new plans are increasing market penetration.
“We’re at a tipping point where every provider will have to deal with cash-paying clients,” he says. “Hospitals with Chargemaster pricing [the list price for services and procedures charged to self-pay and other uninsured clients, usually three to three and a half times the normal Medicare reimbursement] won’t get away with that much longer. They’ll have to charge reasonable, negotiated rates rather than slamming self-pay patients.”
It looks as though the days when patients entered the hospital worried about getting well and dealing with the bills later will soon be in the rearview mirror. Not far into the future, individuals with self-pay components to their health insurance might demand and receive full financial disclosure of all their expected hospital costs (see “Patients Can Shop Around,” p. 29) at the time of admission, with necessary adjustments at discharge.
“Hospitals can’t have secret pricing in a transparent, consumer-driven world,” says Scandlen. “The HDHP model hasn’t fully hit hospitals yet, but they’ll get clobbered in about two years if they don’t adapt.” TH
Marlene Piturro is a freelance writer based in Hastings-on-Hudson, NY.
Joseph Forrester, DO, a critical-care hospitalist and pulmonologist in Denver, discovered firsthand how scoping out and paying for healthcare now resembles shopping for other big-ticket items. Unlike purchasing and paying down a diamond ring or a 60-inch flat-screen TV, for which the final price and payment is duly noted and balances promptly adjusted, hospital billing attempted to overcharge Dr. Forrester by 500%. He already had paid $4,000 toward his 2008 out-of-pocket deductible for medical expenses and was surprised when the hospital said he would have to pay the full $5,000 deductible before he could receive care. The savvy doc went to a real-time claims adjudication tool that he uses in his own practice to show the hospital he’d already satisfied the first 80% of the $5,000 deductible.
The hospital’s billing department listened and responded.
Dr. Forrester paid the remaining $1,000 to fulfill his deductible, and his insurer covered the rest of the treatment cost. “Having access to this information allowed him to receive care immediately, without having to wait weeks for the hospital to correct its mistaken information,” says Chris Stanley, MD, a medical director with United Healthcare.
High-deductible health plans (HDHPs) like Dr. Forrester’s have been growing in popularity since the establishment of health savings accounts (HSAs). Designed to help individuals save for future medical and retiree health expenses on a tax-free basis, HSAs were signed into law by President Bush in December 2003. These products are just beginning to influence how hospitals collect fees and how patients negotiate with their physicians—including hospitalists—about which medications, tests, and procedures they’re willing to pay for.
Break from Tradition
According to the U.S. Treasury Department Web site, HSAs allow individuals to “own and control the money in your HSA. Decisions on how to spend the money are made by the consumer without relying on a third party or a health insurer. Consumers will also decide what types of investments to make with the money in the account in order to make it grow.”
HSAs only are available to individuals covered solely through an HDHP. Individuals receiving veterans benefits or already on Medicare are not eligible; however, if they establish an HSA before enrolling in Medicare, they can keep it—but not add to it.
HDHPs offer consumers—especially young, healthy individuals—low premiums and high deductibles (between $1,150 and $2,900 for individuals and $2,300 to $5,800 for family plans). In addition to paying a low premium, consumers can put money into an HSA to pay for out-of-pocket expenses, including deductibles, co-pays, and co-insurance. The maximum amount of tax-free money a consumer can stash in an HSA this year is $5,800 for individuals and $11,600 for families. (Those 55 and older can contribute an additional $1,000 annually to their HSAs to accelerate their savings rates.)
Consumers can access HSA funds through a debit card, or they can pay for a service, then file for reimbursement.
An HSA should not be confused with a flexible spending account (FSA). Both are paid for by employees with pre-tax dollars; however, FSAs:
- Carry no insurance requirements;
- Are capped at $5,000 in annual contributions;
- Do not pay interest on the account balance; and
- Must be used—or forfeited—by the end of the plan year.
In contrast, an HSA:
- Is funded by the employee or jointly by employer and employee (known as a health reimbursement account, or HRA);
- Has insurance requirements on deductibles and out-of-pocket contributions;
- Pays the provider directly and submits receipts to the account administrator;
- Accumulates interest through a financial institution; and
- Allows unused funds to be carried forward.
Easy Business Decision
Employers are jumping on the HDHP bandwagon, largely to shift more health insurance costs to employees. HDHPs allow consumers to save on upfront costs (e.g., premiums and routine medical expenses) while allowing them to partner with their physicians when deciding how and when they will spend their HSA dollars.
Allowing patients to be involved in the testing, medication, and length-of-stay decisions relative to their care is a reversal from the status quo. Physicians working with hospitalized patients aren’t used to patients questioning treatment or asking for a cost analysis of medications. Another way to think about working with patients who have nontraditional plans: If you were eating at a soup kitchen, you probably wouldn’t complain about having to eat off of paper plates. But if you were dining at a five-star restaurant, you’d freely complain to the maître d’ if your soup was cold or the salad limp.
The 2008 National Study of Employer-Sponsored Health Plans, conducted by international human resources consulting firm Mercer, reported consumer-directed health plans, coupled with either an HSA or an HRA, are offered by 45% of companies with 25,000 or more employees (up from 22% in 2005). Nine percent of companies with 10 to 499 employees offer consumer-directed health plans, up from 2% in 2005.
Mercer partner Blaine Bos notes that raising deductibles is the fallback for employers faced with medical cost increases they can’t—or won’t—absorb. “The introduction of HSAs may have changed employers’ thinking on just how high a deductible can go without causing employees to revolt,” Bos says in the survey analysis. He predicts bad economic times will accelerate consumer-directed health plan uptake in small and large firms because they deliver substantially lower costs than PPOs and HMOs. In 2008, CDHP costs averaged $6,207 per employee, compared with $7,815 for PPOs and $7,768 for HMOs.
Data from ehealthinsurance.com indicate consumers are taking full advantage of HDHPs: Fifteen percent choose the highest deductibles, 48% the mid-range, and 37% the lowest deductible.
Still on HM’s Horizon
Consumer-driven healthcare has yet to significantly affect hospitals and—by extension—HM groups, although hospital admissions were down 2% nationally in 2008 and hospital debts are climbing. Adam Singer, MD, CEO of IPC: The Hospitalist Company, says the impact of HSAs on HM isn’t noticeable yet because patients haven’t adapted to the new model. “Consumers usually aren’t price-shopping the facility, because they’re committed to their physicians and will go to the hospital where their physician has privileges,” Dr. Singer says. “Additionally, the patients hospitalists see are very sick. Many came in through the ED and had no choice about how they got there. They certainly don’t pick their hospitalists.”
By extension, the ED isn’t immune to market forces driving consumer-directed care. Karen McConnell, PhD, director of the Oregon Health and Science University’s Center for Policy and Research in Emergency Medicine, posits that rapid adoption of high-deductible plans could change ED utilization (Ann Emerg Med. 2005;46(6):536-40). Although the ED may be insulated from extensive shopping and price negotiation because visits generally are for urgent conditions, Dr. McConnell says, ED utilization patterns may change if cost-conscious HSA holders forego other necessary medical care or seek substitutes for less-urgent problems.
The reality of consumer-directed healthcare and patients footing more of their own medical bills could eventually have a significant impact on HM programs. “Hospitals are under attack,” Dr. Singer says. “The 20% to 50% of hospital medicine program revenues received as support payments from their hospitals may drop as high-deductible plans with HSAs drive down hospital revenues. So as hospital revenues fall, the subsidies—particularly some of the more absurd, seven-figure subsidies that hospitalists enjoy—are vulnerable.”
Patients Take Charge
With their own money at stake, HSA consumers are engaged in the decision to spend—or save—their healthcare dollars. Although the shift in the doctor-patient decision-making process has slowly found its way into the hospital, it is playing out in doctor’s offices—one of several pipelines for hospital admissions. As a consumer, Linda Waldmann, manager of MyCost, a real-time claims-adjudication tool offered by Alegent Health, introduced cost when making treatment decisions after she was diagnosed with carpal tunnel syndrome. She asked her orthopedic surgeon lots of questions, absorbed what he said, then made her own treatment choices.
“My orthopedist wanted me to have three tests, but I elected to postpone one test until my HSA replenished the following year,” Waldmann says. “Doctors are still hesitant about negotiating with patients, but this one understood my concern.”
Blue Cross/Blue Shield of Tennessee’s (BCBST) Maggie Fox, director of application systems, saw a large jump (to 33% in 2009 from 8% in 2008) among BCBST’s 5,000 employees opting for HSAs. The Tennessee company emphasizes prevention, education, and wellness as critical components of consumer-directed care, and the company’s HSA consumers are offered a variety of discounts for adhering to healthy lifestyles.
At BCBST, HSAs have opened dialogue between patients, physicians, and hospitals. Through a Web-based portal called “Blue Access,” providers receive information on a patient’s financial liability in as little as 10 seconds. “HSAs and HRAs have created a patient liability that never existed before,” Fox says. “Higher out-of-pocket costs change everything. Providers need to collect payment at the point of care, whether that’s the office or hospital. There’s more work at checkout, but at least patients and providers know the exact amount the care costs and how much the patient has to pay.”
Davis Liu, MD, a Wharton School of Business graduate and family physician with Northern California Permanente Medical Group, advises hospitalists to be ready for patients with HSAs to challenge treatment decisions because of the cost. He says hospitalists must prepare to communicate clearly and effectively with HSA patients, especially when it comes to necessary testing and medications. The task might be difficult because information about testing costs and procedures is limited, and prices vary dramatically by hospital and region. “While it is extremely unlikely that patients will refuse testing when hospitalized, hospitalists must be acutely aware that these patients may skip follow-up appointments, testing, and surgeries,” Dr. Liu says.
United Healthcare’s Dr. Stanley sees physician decision-making evolving as HSA patients become more aware of the economics of treatment options. “Patients are already questioning doctors who order four tests when they’re only willing to pay for three, wanting to postpone procedures, and asking about costs for additional tests and procedures,” he says. “Eventually, cost consciousness will impact group practices. They will have to decrease overhead, revamp collection processes, and strive for administrative simplicity.” Woe to the physician who believes cost isn’t their responsibility, Dr. Stanley says, as they “must realize they’re small-business owners and act accordingly.”
The Future
Consumer-driven healthcare might have little effect on hospitals right now, but change is on the horizon, according to Greg Scandlen, president and CEO of Consumers for Health Care Choice in Hagerstown, Md. He cites the 2008 National Health Interview Survey conducted by the Centers for Disease Control and Prevention, which shows 20% of Americans have an HDHP, as proof positive these new plans are increasing market penetration.
“We’re at a tipping point where every provider will have to deal with cash-paying clients,” he says. “Hospitals with Chargemaster pricing [the list price for services and procedures charged to self-pay and other uninsured clients, usually three to three and a half times the normal Medicare reimbursement] won’t get away with that much longer. They’ll have to charge reasonable, negotiated rates rather than slamming self-pay patients.”
It looks as though the days when patients entered the hospital worried about getting well and dealing with the bills later will soon be in the rearview mirror. Not far into the future, individuals with self-pay components to their health insurance might demand and receive full financial disclosure of all their expected hospital costs (see “Patients Can Shop Around,” p. 29) at the time of admission, with necessary adjustments at discharge.
“Hospitals can’t have secret pricing in a transparent, consumer-driven world,” says Scandlen. “The HDHP model hasn’t fully hit hospitals yet, but they’ll get clobbered in about two years if they don’t adapt.” TH
Marlene Piturro is a freelance writer based in Hastings-on-Hudson, NY.
HM Group Economics 101
If ignorance is bliss, then a substantial slice of hospital medicine group (HMG) leaders are in heaven—about finance, that is. Perhaps they didn’t become physicians to solve the sub-prime mortgage mess or take their companies public, as Dr. Adam Singer, MD, CEO of IPC: The Hospitalist Company, did in January 2008.
Dr. Singer, recently named 2008 Physician Entrepreneur of the Year by Modern Physician, always has insisted HMGs can be financially self-supporting. In 2002, he wrote in Physician Executive “when revenue (fees divided by number of patient encounters) exceeds expenses, the practice becomes economically viable.” He calculated that factoring in malpractice insurance, general expenses, 10 percent of revenue for billing and collection, two patient encounters a day per full-time equivalent employee was an HMGs’ break-even point. “Even at a ridiculously minimum encounter volume of two, a hospitalist practice is viable without any outside subsidy,” he concluded. To drive home his point, Dr. Singer suggested HMGs augment their revenues by serving nursing homes and rehab facilities, teaching, securing research grants, medical directorships, and taking on contracts to manage ER unassigned patients.
Nevertheless, a recent Society of Hospital Medicine survey shows a number of HMG leaders lack the basic financial acumen to get and keep their practices fiscally healthy. Data from SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement reveals the vast majority of HMGs fall short of economic independence. Survey results show many HMG leaders’ grasp of basic finance leaves room for improvement.
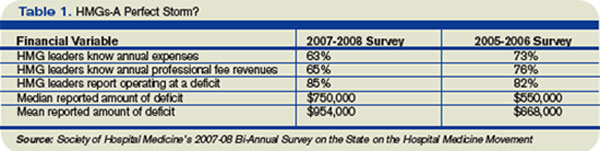
Key findings include:
- 37% of HMG leaders didn’t know their annual expenses;
- 35% didn’t know their annual professional fee revenues; and
- Among those that didn’t know their expenses and revenues, 85% were operating at a deficit.
Additionally, a negative correlation exists between HMG financial performance and compensation. HMG production remained flat, while average hospitalist compensation increased 13% to $193,000 annually. Cushiony subsidies persist; the survey showed 91% of HMGs receive some form of financial support, an average of $954,000 per group or $97,375 for each full-time physician.
Drilling down into the survey’s financial data, analysis by Joe Miller, SHM Executive Advisor to the CEO, points to an ominous monetary “perfect storm” brewing for HMG leaders. Deficits are growing as hospitalist leaders’ knowledge about their groups’ finances are declining.
The trend data also suggest subsidies obscure declining financial support in several areas. Compared to the 2005-06 SHM survey, the latest survey shows the percentage of HMGs receiving financial support dropped in all five categories in which HMGs receive subsidies. Results from the two most recent surveys showed hospital financial support dropped from 60% to 51%; other support from 17% to 12%; income guarantees fell from 72% to 61%; services in-kind declined from 71% to 60%; and case rates slid from 12% to 11%.
Fuzzy Math?
An oft-cited rationale for hospital medicine’s generous subsidies from other stakeholders is that it “creates value,” in terms of reducing hospital length of stay, costs per case and improved outcomes. Throughout the years, such savings have received increased scrutiny. Blogger and SHM member Dr. Robert Wachter, MD, professor and associated chairman of the Department of Medicine at the University of California, San Francisco, said in May “research on these metrics is disappointing. … The move toward hospitalist shift work and the resulting fragmentation of care during hospitalization may be eroding any slim advantage the model had in cost savings.” He concluded, “the bubble will burst the morning CEOs wake up and realize that there is no longer a shortage of hospitalists.”
Burke Kealey, MD, assistant medical director, Hospital Medicine Division of HealthPartners Medical Group in St. Paul, Minn., offers powerful reasons for why hospitalists struggle with Finance 101:
- Hospitalists have little incentive to meet financial performance targets;
- HMG leaders are too busy with recruiting, scheduling and retention to focus on finance;
- Difficulties obtaining useful data from hospital administrators; and
- Too few business models that centralize data from multiple hospitals, making financial analysis of an individual group difficult.
To address the needs, Dr. Kealey, who chairs SHM’s Practice Analysis Committee, has spearheaded SHM’s development of dashboards that utilize performance metrics, such as volume data, case mix, length of stay, resource utilization, productivity, and readmission rates, to help leaders guide a practice to economic health.
Steve Liu, MD, the CEO and founder of Ingenious Med, is a hospitalist in one of the nation’s largest HMGs, with 100,000-plus patient encounters annually at Emory Healthcare in Atlanta. A member of SHM’s Benchmarks Committee, Liu puts HMG leaders’ financial ignorance in the context of a growth industry. “Hospital medicine is young, it’s moving very fast, and it is filled with a youngish crowd who don’t feel they have enough time to focus on financial deficits and inefficiencies,” Dr. Liu says.
Still, a lack of financial knowledge can trip up the best of physician. Dr. Liu advises hospitalist leaders to focus on professional fee revenues, particularly on fees collected per full-time equivalent employee (FTE); eliminating high expenses from inefficiencies; and checking local and national compensation packages to address what he estimates as 30 percent of HMGs who fail to pay physicians appropriately. Other financial mistakes, he says, are HMG leaders throwing warm bodies at problems without enough back-office support; agreeing to see more patients than they can handle in a day; overspending on recruiters; and failure to understand each full-time employee’s return on investment.
Numerous hospitalists, according to Dr. Liu, believe they don’t have enough time to build partnerships with administrators that would lead to more sharing of financial data. “They may even be in a power struggle with administrators over access to financial data. … If you can’t measure it, you can’t manage it. That’s the essence of Finance 101,” Dr. Liu says, “and it’s very frustrating to hospitalists who don’t have the business skill sets and tools to succeed financially.” Since data is power, it’s imperative to ask the chief financial officer (CFO) for data; that way the HMG can work toward profitability.
Making sense of financial data is critical, says Leslie Flores, director of SHM’s Practice Management Institute. “HMG leaders have to learn to take data, such as number of encounters, relative value units, average daily census, number of days worked per year, the total subsidy for the practice, and average subsidy per hospitalist, and make sense of it. Where do the numbers come from and what do they mean are critical questions,” she says.
Big Picture
SHM’s most recent survey reflects the average hospitalist medicine group’s business model. Production is flat; compensation is up 13%; and 91% of HMGs receive subsidies nearing $1 million each. From a dollars-and-sense vantage point, the business case for hospital medicine doesn’t work. So why do hospitals go along with a broken business model, especially at a time when a hospital’s cost curve is growing faster than its revenue curve, making it even more difficult to justify HMG subsidies?
The short answer is that most hospital medicine programs are invited in by hospital administrators and serve a specific purpose related to overall revenue generation and/or cost controls. Common reasons for creating hospitalist programs are improving Emergency Department throughput, relieving community-based physicians from hospital duties, boosting subspecialist revenues with medical co-management, and cost cutting through reduced length of stay and improved resource utilization. Each has different financial metrics associated with it, and HMG leaders should understand each metric thoroughly.
If, for example, relieving the pressure on community-based doctors is the HMG’s primary goal, an HMG leader’s strategy might be to attract the best hospitalists available, offering a high compensation package and recruiting bonus. That would help cover the increased patient load, but it might pressure the hospital to shoulder a steep subsidy.
Alternatively, relying on financial and performance metrics might yield better rules about when to justify a new hire. Seasoned HMG leaders would rely on a group’s average daily census of 50 to 70 patients as the tipping point for adding a FTE hospitalist. Similarly, night admissions of 10 to 14 patients should trigger the hiring of a nocturnist, with his or her premium pay.
Brian Bossard, MD, founder of Inpatient Physicians Associates in Lincoln, Neb., relies on that type of data and other “lean” management concepts. To optimize each physicians’ patient loads and productivity, he has patients assigned by physical proximity, so his hospitalists won’t waste time running around the hospital seeing patients. Saving time and manpower contributes to an HMG’s financial health.
Once HMGs satisfy the primary service goals set by their hospitals, leaders should focus on enhancing their hospitals’ revenue generation from various sources. The typical mix of hospital revenue streams are, in size order—clinical services, research, philanthropic grants, interest income on cash assets, and royalties from intellectual property. Clinical services and research account for about 95% of the average hospital revenues, with the balance split among the other three.
Hospitals try to boost revenue by adding product lines, enhancing the value of current products, increasing market share, and capitalizing on production efficiencies. Translating business concepts from widgets to wards, increasing both volume and acuity of patient encounters, should be commonplace and a revenue booster. Research revenues are another story, particularly with slowdowns in National Institutes of Health funding. Recruiting hospitalists who want to do research leaves hospitals covering their salaries and labs for long periods of time without revenue generation.
Focusing on proven revenue generators—enhancing the value of current products, increasing market share, and boosting production efficiencies—can help HMG leaders carve out a niche that truly creates value for the hospital.
It may take a lot for an HMG leader to build solid financial performance on a strong clinical foundation, however, it is doable. Dr. Liu sums up how HMG finances will improve: “As hospital medicine matures, expect its leaders to mature as well,” he says. “They will become more business savvy and learn to speak the language of business, even if they have to force themselves to learn.” TH
If ignorance is bliss, then a substantial slice of hospital medicine group (HMG) leaders are in heaven—about finance, that is. Perhaps they didn’t become physicians to solve the sub-prime mortgage mess or take their companies public, as Dr. Adam Singer, MD, CEO of IPC: The Hospitalist Company, did in January 2008.
Dr. Singer, recently named 2008 Physician Entrepreneur of the Year by Modern Physician, always has insisted HMGs can be financially self-supporting. In 2002, he wrote in Physician Executive “when revenue (fees divided by number of patient encounters) exceeds expenses, the practice becomes economically viable.” He calculated that factoring in malpractice insurance, general expenses, 10 percent of revenue for billing and collection, two patient encounters a day per full-time equivalent employee was an HMGs’ break-even point. “Even at a ridiculously minimum encounter volume of two, a hospitalist practice is viable without any outside subsidy,” he concluded. To drive home his point, Dr. Singer suggested HMGs augment their revenues by serving nursing homes and rehab facilities, teaching, securing research grants, medical directorships, and taking on contracts to manage ER unassigned patients.
Nevertheless, a recent Society of Hospital Medicine survey shows a number of HMG leaders lack the basic financial acumen to get and keep their practices fiscally healthy. Data from SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement reveals the vast majority of HMGs fall short of economic independence. Survey results show many HMG leaders’ grasp of basic finance leaves room for improvement.
Key findings include:
- 37% of HMG leaders didn’t know their annual expenses;
- 35% didn’t know their annual professional fee revenues; and
- Among those that didn’t know their expenses and revenues, 85% were operating at a deficit.
Additionally, a negative correlation exists between HMG financial performance and compensation. HMG production remained flat, while average hospitalist compensation increased 13% to $193,000 annually. Cushiony subsidies persist; the survey showed 91% of HMGs receive some form of financial support, an average of $954,000 per group or $97,375 for each full-time physician.
Drilling down into the survey’s financial data, analysis by Joe Miller, SHM Executive Advisor to the CEO, points to an ominous monetary “perfect storm” brewing for HMG leaders. Deficits are growing as hospitalist leaders’ knowledge about their groups’ finances are declining.
The trend data also suggest subsidies obscure declining financial support in several areas. Compared to the 2005-06 SHM survey, the latest survey shows the percentage of HMGs receiving financial support dropped in all five categories in which HMGs receive subsidies. Results from the two most recent surveys showed hospital financial support dropped from 60% to 51%; other support from 17% to 12%; income guarantees fell from 72% to 61%; services in-kind declined from 71% to 60%; and case rates slid from 12% to 11%.
Fuzzy Math?
An oft-cited rationale for hospital medicine’s generous subsidies from other stakeholders is that it “creates value,” in terms of reducing hospital length of stay, costs per case and improved outcomes. Throughout the years, such savings have received increased scrutiny. Blogger and SHM member Dr. Robert Wachter, MD, professor and associated chairman of the Department of Medicine at the University of California, San Francisco, said in May “research on these metrics is disappointing. … The move toward hospitalist shift work and the resulting fragmentation of care during hospitalization may be eroding any slim advantage the model had in cost savings.” He concluded, “the bubble will burst the morning CEOs wake up and realize that there is no longer a shortage of hospitalists.”
Burke Kealey, MD, assistant medical director, Hospital Medicine Division of HealthPartners Medical Group in St. Paul, Minn., offers powerful reasons for why hospitalists struggle with Finance 101:
- Hospitalists have little incentive to meet financial performance targets;
- HMG leaders are too busy with recruiting, scheduling and retention to focus on finance;
- Difficulties obtaining useful data from hospital administrators; and
- Too few business models that centralize data from multiple hospitals, making financial analysis of an individual group difficult.
To address the needs, Dr. Kealey, who chairs SHM’s Practice Analysis Committee, has spearheaded SHM’s development of dashboards that utilize performance metrics, such as volume data, case mix, length of stay, resource utilization, productivity, and readmission rates, to help leaders guide a practice to economic health.
Steve Liu, MD, the CEO and founder of Ingenious Med, is a hospitalist in one of the nation’s largest HMGs, with 100,000-plus patient encounters annually at Emory Healthcare in Atlanta. A member of SHM’s Benchmarks Committee, Liu puts HMG leaders’ financial ignorance in the context of a growth industry. “Hospital medicine is young, it’s moving very fast, and it is filled with a youngish crowd who don’t feel they have enough time to focus on financial deficits and inefficiencies,” Dr. Liu says.
Still, a lack of financial knowledge can trip up the best of physician. Dr. Liu advises hospitalist leaders to focus on professional fee revenues, particularly on fees collected per full-time equivalent employee (FTE); eliminating high expenses from inefficiencies; and checking local and national compensation packages to address what he estimates as 30 percent of HMGs who fail to pay physicians appropriately. Other financial mistakes, he says, are HMG leaders throwing warm bodies at problems without enough back-office support; agreeing to see more patients than they can handle in a day; overspending on recruiters; and failure to understand each full-time employee’s return on investment.
Numerous hospitalists, according to Dr. Liu, believe they don’t have enough time to build partnerships with administrators that would lead to more sharing of financial data. “They may even be in a power struggle with administrators over access to financial data. … If you can’t measure it, you can’t manage it. That’s the essence of Finance 101,” Dr. Liu says, “and it’s very frustrating to hospitalists who don’t have the business skill sets and tools to succeed financially.” Since data is power, it’s imperative to ask the chief financial officer (CFO) for data; that way the HMG can work toward profitability.
Making sense of financial data is critical, says Leslie Flores, director of SHM’s Practice Management Institute. “HMG leaders have to learn to take data, such as number of encounters, relative value units, average daily census, number of days worked per year, the total subsidy for the practice, and average subsidy per hospitalist, and make sense of it. Where do the numbers come from and what do they mean are critical questions,” she says.
Big Picture
SHM’s most recent survey reflects the average hospitalist medicine group’s business model. Production is flat; compensation is up 13%; and 91% of HMGs receive subsidies nearing $1 million each. From a dollars-and-sense vantage point, the business case for hospital medicine doesn’t work. So why do hospitals go along with a broken business model, especially at a time when a hospital’s cost curve is growing faster than its revenue curve, making it even more difficult to justify HMG subsidies?
The short answer is that most hospital medicine programs are invited in by hospital administrators and serve a specific purpose related to overall revenue generation and/or cost controls. Common reasons for creating hospitalist programs are improving Emergency Department throughput, relieving community-based physicians from hospital duties, boosting subspecialist revenues with medical co-management, and cost cutting through reduced length of stay and improved resource utilization. Each has different financial metrics associated with it, and HMG leaders should understand each metric thoroughly.
If, for example, relieving the pressure on community-based doctors is the HMG’s primary goal, an HMG leader’s strategy might be to attract the best hospitalists available, offering a high compensation package and recruiting bonus. That would help cover the increased patient load, but it might pressure the hospital to shoulder a steep subsidy.
Alternatively, relying on financial and performance metrics might yield better rules about when to justify a new hire. Seasoned HMG leaders would rely on a group’s average daily census of 50 to 70 patients as the tipping point for adding a FTE hospitalist. Similarly, night admissions of 10 to 14 patients should trigger the hiring of a nocturnist, with his or her premium pay.
Brian Bossard, MD, founder of Inpatient Physicians Associates in Lincoln, Neb., relies on that type of data and other “lean” management concepts. To optimize each physicians’ patient loads and productivity, he has patients assigned by physical proximity, so his hospitalists won’t waste time running around the hospital seeing patients. Saving time and manpower contributes to an HMG’s financial health.
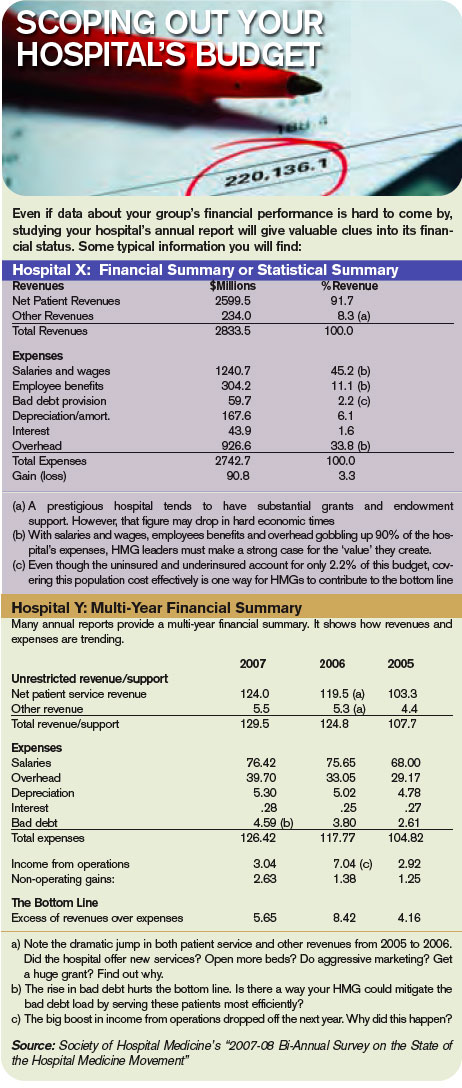
Once HMGs satisfy the primary service goals set by their hospitals, leaders should focus on enhancing their hospitals’ revenue generation from various sources. The typical mix of hospital revenue streams are, in size order—clinical services, research, philanthropic grants, interest income on cash assets, and royalties from intellectual property. Clinical services and research account for about 95% of the average hospital revenues, with the balance split among the other three.
Hospitals try to boost revenue by adding product lines, enhancing the value of current products, increasing market share, and capitalizing on production efficiencies. Translating business concepts from widgets to wards, increasing both volume and acuity of patient encounters, should be commonplace and a revenue booster. Research revenues are another story, particularly with slowdowns in National Institutes of Health funding. Recruiting hospitalists who want to do research leaves hospitals covering their salaries and labs for long periods of time without revenue generation.
Focusing on proven revenue generators—enhancing the value of current products, increasing market share, and boosting production efficiencies—can help HMG leaders carve out a niche that truly creates value for the hospital.
It may take a lot for an HMG leader to build solid financial performance on a strong clinical foundation, however, it is doable. Dr. Liu sums up how HMG finances will improve: “As hospital medicine matures, expect its leaders to mature as well,” he says. “They will become more business savvy and learn to speak the language of business, even if they have to force themselves to learn.” TH
If ignorance is bliss, then a substantial slice of hospital medicine group (HMG) leaders are in heaven—about finance, that is. Perhaps they didn’t become physicians to solve the sub-prime mortgage mess or take their companies public, as Dr. Adam Singer, MD, CEO of IPC: The Hospitalist Company, did in January 2008.
Dr. Singer, recently named 2008 Physician Entrepreneur of the Year by Modern Physician, always has insisted HMGs can be financially self-supporting. In 2002, he wrote in Physician Executive “when revenue (fees divided by number of patient encounters) exceeds expenses, the practice becomes economically viable.” He calculated that factoring in malpractice insurance, general expenses, 10 percent of revenue for billing and collection, two patient encounters a day per full-time equivalent employee was an HMGs’ break-even point. “Even at a ridiculously minimum encounter volume of two, a hospitalist practice is viable without any outside subsidy,” he concluded. To drive home his point, Dr. Singer suggested HMGs augment their revenues by serving nursing homes and rehab facilities, teaching, securing research grants, medical directorships, and taking on contracts to manage ER unassigned patients.
Nevertheless, a recent Society of Hospital Medicine survey shows a number of HMG leaders lack the basic financial acumen to get and keep their practices fiscally healthy. Data from SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement reveals the vast majority of HMGs fall short of economic independence. Survey results show many HMG leaders’ grasp of basic finance leaves room for improvement.
Key findings include:
- 37% of HMG leaders didn’t know their annual expenses;
- 35% didn’t know their annual professional fee revenues; and
- Among those that didn’t know their expenses and revenues, 85% were operating at a deficit.
Additionally, a negative correlation exists between HMG financial performance and compensation. HMG production remained flat, while average hospitalist compensation increased 13% to $193,000 annually. Cushiony subsidies persist; the survey showed 91% of HMGs receive some form of financial support, an average of $954,000 per group or $97,375 for each full-time physician.
Drilling down into the survey’s financial data, analysis by Joe Miller, SHM Executive Advisor to the CEO, points to an ominous monetary “perfect storm” brewing for HMG leaders. Deficits are growing as hospitalist leaders’ knowledge about their groups’ finances are declining.
The trend data also suggest subsidies obscure declining financial support in several areas. Compared to the 2005-06 SHM survey, the latest survey shows the percentage of HMGs receiving financial support dropped in all five categories in which HMGs receive subsidies. Results from the two most recent surveys showed hospital financial support dropped from 60% to 51%; other support from 17% to 12%; income guarantees fell from 72% to 61%; services in-kind declined from 71% to 60%; and case rates slid from 12% to 11%.
Fuzzy Math?
An oft-cited rationale for hospital medicine’s generous subsidies from other stakeholders is that it “creates value,” in terms of reducing hospital length of stay, costs per case and improved outcomes. Throughout the years, such savings have received increased scrutiny. Blogger and SHM member Dr. Robert Wachter, MD, professor and associated chairman of the Department of Medicine at the University of California, San Francisco, said in May “research on these metrics is disappointing. … The move toward hospitalist shift work and the resulting fragmentation of care during hospitalization may be eroding any slim advantage the model had in cost savings.” He concluded, “the bubble will burst the morning CEOs wake up and realize that there is no longer a shortage of hospitalists.”
Burke Kealey, MD, assistant medical director, Hospital Medicine Division of HealthPartners Medical Group in St. Paul, Minn., offers powerful reasons for why hospitalists struggle with Finance 101:
- Hospitalists have little incentive to meet financial performance targets;
- HMG leaders are too busy with recruiting, scheduling and retention to focus on finance;
- Difficulties obtaining useful data from hospital administrators; and
- Too few business models that centralize data from multiple hospitals, making financial analysis of an individual group difficult.
To address the needs, Dr. Kealey, who chairs SHM’s Practice Analysis Committee, has spearheaded SHM’s development of dashboards that utilize performance metrics, such as volume data, case mix, length of stay, resource utilization, productivity, and readmission rates, to help leaders guide a practice to economic health.
Steve Liu, MD, the CEO and founder of Ingenious Med, is a hospitalist in one of the nation’s largest HMGs, with 100,000-plus patient encounters annually at Emory Healthcare in Atlanta. A member of SHM’s Benchmarks Committee, Liu puts HMG leaders’ financial ignorance in the context of a growth industry. “Hospital medicine is young, it’s moving very fast, and it is filled with a youngish crowd who don’t feel they have enough time to focus on financial deficits and inefficiencies,” Dr. Liu says.
Still, a lack of financial knowledge can trip up the best of physician. Dr. Liu advises hospitalist leaders to focus on professional fee revenues, particularly on fees collected per full-time equivalent employee (FTE); eliminating high expenses from inefficiencies; and checking local and national compensation packages to address what he estimates as 30 percent of HMGs who fail to pay physicians appropriately. Other financial mistakes, he says, are HMG leaders throwing warm bodies at problems without enough back-office support; agreeing to see more patients than they can handle in a day; overspending on recruiters; and failure to understand each full-time employee’s return on investment.
Numerous hospitalists, according to Dr. Liu, believe they don’t have enough time to build partnerships with administrators that would lead to more sharing of financial data. “They may even be in a power struggle with administrators over access to financial data. … If you can’t measure it, you can’t manage it. That’s the essence of Finance 101,” Dr. Liu says, “and it’s very frustrating to hospitalists who don’t have the business skill sets and tools to succeed financially.” Since data is power, it’s imperative to ask the chief financial officer (CFO) for data; that way the HMG can work toward profitability.
Making sense of financial data is critical, says Leslie Flores, director of SHM’s Practice Management Institute. “HMG leaders have to learn to take data, such as number of encounters, relative value units, average daily census, number of days worked per year, the total subsidy for the practice, and average subsidy per hospitalist, and make sense of it. Where do the numbers come from and what do they mean are critical questions,” she says.
Big Picture
SHM’s most recent survey reflects the average hospitalist medicine group’s business model. Production is flat; compensation is up 13%; and 91% of HMGs receive subsidies nearing $1 million each. From a dollars-and-sense vantage point, the business case for hospital medicine doesn’t work. So why do hospitals go along with a broken business model, especially at a time when a hospital’s cost curve is growing faster than its revenue curve, making it even more difficult to justify HMG subsidies?
The short answer is that most hospital medicine programs are invited in by hospital administrators and serve a specific purpose related to overall revenue generation and/or cost controls. Common reasons for creating hospitalist programs are improving Emergency Department throughput, relieving community-based physicians from hospital duties, boosting subspecialist revenues with medical co-management, and cost cutting through reduced length of stay and improved resource utilization. Each has different financial metrics associated with it, and HMG leaders should understand each metric thoroughly.
If, for example, relieving the pressure on community-based doctors is the HMG’s primary goal, an HMG leader’s strategy might be to attract the best hospitalists available, offering a high compensation package and recruiting bonus. That would help cover the increased patient load, but it might pressure the hospital to shoulder a steep subsidy.
Alternatively, relying on financial and performance metrics might yield better rules about when to justify a new hire. Seasoned HMG leaders would rely on a group’s average daily census of 50 to 70 patients as the tipping point for adding a FTE hospitalist. Similarly, night admissions of 10 to 14 patients should trigger the hiring of a nocturnist, with his or her premium pay.
Brian Bossard, MD, founder of Inpatient Physicians Associates in Lincoln, Neb., relies on that type of data and other “lean” management concepts. To optimize each physicians’ patient loads and productivity, he has patients assigned by physical proximity, so his hospitalists won’t waste time running around the hospital seeing patients. Saving time and manpower contributes to an HMG’s financial health.
Once HMGs satisfy the primary service goals set by their hospitals, leaders should focus on enhancing their hospitals’ revenue generation from various sources. The typical mix of hospital revenue streams are, in size order—clinical services, research, philanthropic grants, interest income on cash assets, and royalties from intellectual property. Clinical services and research account for about 95% of the average hospital revenues, with the balance split among the other three.
Hospitals try to boost revenue by adding product lines, enhancing the value of current products, increasing market share, and capitalizing on production efficiencies. Translating business concepts from widgets to wards, increasing both volume and acuity of patient encounters, should be commonplace and a revenue booster. Research revenues are another story, particularly with slowdowns in National Institutes of Health funding. Recruiting hospitalists who want to do research leaves hospitals covering their salaries and labs for long periods of time without revenue generation.
Focusing on proven revenue generators—enhancing the value of current products, increasing market share, and boosting production efficiencies—can help HMG leaders carve out a niche that truly creates value for the hospital.
It may take a lot for an HMG leader to build solid financial performance on a strong clinical foundation, however, it is doable. Dr. Liu sums up how HMG finances will improve: “As hospital medicine matures, expect its leaders to mature as well,” he says. “They will become more business savvy and learn to speak the language of business, even if they have to force themselves to learn.” TH
HM Goes Public
You know your industry is on the map when a trailblazer takes his company public. That signals the capital markets that top executives in a leading company are confident in their business model’s ability to grow the company enough to satisfy Wall Street’s voracious hunger for profits.
It’s a tall order, and Adam Singer, MD, founder and CEO of IPC-The Hospitalist Company, based in North Hollywood, Calif., accomplished it in January.
During 2007, Dr. Singer set the wheels in motion for taking IPC public the following year. “Our company is built right, has a solid revenue stream, and the nirvana of a real healthcare company—a battle-tested, proven business model,” he says.
Dr. Singer and his management team had the usual reasons for going public: raising capital to pay for operations and to allow for growth by acquisition, reducing debt, and creating liquidity for shareholders. He also had other fish to fry with a public offering. “I wanted to be the first in our industry to make it out of the box,’’ he says. “I also wanted IPC to be a model for the many hospital medicine companies that would like to mature beyond having a bunch of doctors running around a hospital and calling themselves a hospitalist medicine company.”
For Dr. Singer, going public went beyond the desire to produce quarterly financial results that would warm investors’ hearts. It spoke to his core belief in what the business of hospital medicine should be and, from his vantage point, isn’t.
“By leading a publicly traded hospital medicine company I am debunking the myth that hospitalist groups need hospital subsidies to survive,” he says. “This is a powerful myth, one that is mired in a work force’s idea that its members should get full-time pay for less than full-time work. IPC has raised the bar for our industry. We think that hospitals should demand the overall level of sophistication, physician commitment and productivity that IPC has.”
With few publicly traded physician companies for templates for a public offering, Dr. Singer looked to a colleague, Roger Medel, MD, for direction. Dr. Medel took his company public in 1979 and has grown Sunrise, Fla.-based Pediatrix Medical Group, a provider of neonatal, maternal-fetal, and pediatric intensivist/hospitalist services, from a company with $100 million in market capitalization to $3.32 billion and a recent stock price of $67 per share. The company has a “buy” consensus rating from analysts and respectable price-to-earning and earnings-per-share values.
Economic Evolution
Medical staffing firm IPOs, such as IPC’s, are relatively rare. Most venture capital chases the next hot thing in medical information technology, biotechnology, and medical testing. The quirks of the medical staffing industry, such as hospitalist hiring—where salary increases can consume sizable chunks of a firm’s revenues—may deter potential investors.
Why are publicly traded medical staffing companies like IPC and PDX the exception rather than the rule? Because they rely so heavily on human capital—primarily physicians—for bottom-line results, they must contend with recruiting and retaining from a highly sought after talent pool that have their choice of job opportunities.
Also, many physicians fear the corporatization of medicine, an anxiety that working for a publicly traded company tends to arouse. Physician idealism—wanting to make the world a better place—may clash with a public corporation’s raison d’etre: making money. In a young field like hospital medicine, where performance metrics are evolving, balancing shareholder demands for ROI versus quality patient care requires a delicate touch.
Larry Wellikson, MD, SHM’s chief executive officer, says IPC’s entry into the public markets has been received well, indicating the maturation and strong growth of hospital medicine.
IPC’s public offering took place Jan. 30. Lead underwriters Credit Suisse Securities and Jeffries & Co. offered 5.9 million shares of IPC stock under the ticker symbol IPCM, a four-letter symbol conforming with NASDAQ’s listing requirements. The stock traded mostly at $19 per share, above the original per share estimate of between $15 to $17, raising approximately $38.3 million in net proceeds.
Since then, IPCM shares have ranged from $16.25 to $23.09 per share, trading at a thin average daily volume of 162,000. As of March 31, IPC’s market capitalization was $296 million. Six months from the IPO, average daily volume should increase, as regulations on shareholder sales are eased according to stock exchange rules.
IPC’s latest financial results were upbeat. The firm reported record operating results for the fourth quarter and full year 2007. Total patient encounters rose 29%, compared with 460,000 over the same period in 2006. Fourth-quarter net revenues were $52.6 million, a 31% increase from $40.2 million in fourth-quarter 2006. Physician practice salaries and other expenses for the period were $36.9 million vs. $29.5 million for fourth-quarter 2006. As a percentage of net revenue, physician salaries declined to 70% from 73% in the fourth quarter of 2007 vs. 2006. Dr. Singer attributed the change to higher physician productivity and increased revenue per encounter.
With the stock market retrenching since its all-time high in October, IPC’s timing on going public might seem a bit off. Yet, venture capitalists are bullish on healthcare. They sank a record $9.97 billion into the sector in 2007, topping the previous high of $9.47 billion in 2000, during the dot.com craze. Three large venture capital firms specializing in healthcare have $1.25 billion looking for good homes. The worry on Wall Street is that there won’t be enough healthcare IPOs to satisfy demand; there were only 31 in 2007 vs. 60 in 2000.
Alternatives
Going public is not the only way hospital medicine companies and other physician-intensive enterprises can raise needed capital. Venture capital plays a critical role. Brentwood, Tenn.-based Cogent Healthcare received its first round of such funding in 1997, a second infusion in 2000, and $15 million in 2002. IPC is no stranger to venture capital either: It raised $47 million in venture capital since 1998. Such capital infusions helped IPC and Cogent in their early days by providing the money needed to start hospital medicine groups, recruit top managers, expand into new markets, and improve IT and communication infrastructures.
Some entrepreneurs favor keeping their companies private. For example, John Erickson, founder and CEO of Baltimore-based Erickson Retirement Communities (ERC), is committed to growing his business without going public. There are 19 Erickson campuses in 11 states, with 21,000 residents. ERC’s business plan involves adding sites, anticipating growth to 55,000 residents in five years. Such steady expansion gobbles up capital, but Erickson is adamant about staying private. On going public he says: “I consider it whenever I need capital, but it’s hard to keep public markets happy. If your business slows down for any reason, your stock tanks and the market will punish you harshly. I will not have stock analysts pressuring me about how to run and grow my business.”
Erickson admits the competing demands of raising capital and keeping the company private aren’t easy to reconcile. “We go to midsized and large banks and [real estate investment trusts], get letters of credit, tax bonds, debt financing, mezzanine financing, etc.,” he says. He considers that others in his industry, Sunrise Senior Living (SRZ) and Brookdale Senior Living (BKD) that have gone public show the industry’s strength. “Multiple sources of capitalization in an industry provide greater options for all,” he adds.
That said, Erickson intends to resist any temptation to go public because “I must have the flexibility to implement our five-year plan correctly. If I want to invest $30 million in a medical group or hire seven doctors at $150,000 a pop, I don’t have to answer to some 30-year-old stock analyst who doesn’t like that.”
As for IPC’s public offering, Erickson says the first company to do so in an industry opens new avenues for raising capital in the public arena. “Dr. Singer’s pushing the envelope for hospital medicine, and if he can tolerate the pressure of the market—even when the strings are very tight—that’s great,” he emphasizes.
Commenting on the legal and governance issues of a public offering, Peter Olberg, corporate and finance partner at Manhattan-based law firm of Manatt, Philips and Philips says IPC’s being the first publicly traded hospitalist medicine company is a sound way to raise capital and isn’t risky in terms of disclosure. However, a specialty care provider like IPC can “become a victim of its own success. Public payers can say reimbursement is too high and cut it based on the leader’s financial performance.”
Peer Perspective
SHM President Patrick Cawley, MD, MBA, calls IPC’s public offering a major milestone because it demonstrates the maturity of the hospitalist movement. He expects IPC to use the infusion of capital to step up physician hiring, acquire more groups, and improve its proprietary IT infrastructure by refining its tools to further link outcomes and performance.
“IPC’s emphasis on quality outcomes is clearly where medicine is going,” Dr. Cawley says. And, “Putting pressure on hospitalists to be more productive has a huge potential in helping hospital medicine get more efficient by seeing more patients.”
To put the IPC public offering in perspective Dr. Cawley captures Dr. Singer’s vision. “To run a public company, you focus beyond daily stock prices and on the intermediate and short-term. What Wall Street thinks about your business matters. Our product [hospital medicine] has a great future, and I applaud Adam Singer for taking this step.”
Giving Dr. Singer the last word, he says “I’m a big believer in not worrying about things I can’t control like stock market fluctuations. We can handle good news and bad. We have a good business model and we’ll stick to the knitting.” TH
Marlene Piturro is a medical writer based in New York.
You know your industry is on the map when a trailblazer takes his company public. That signals the capital markets that top executives in a leading company are confident in their business model’s ability to grow the company enough to satisfy Wall Street’s voracious hunger for profits.
It’s a tall order, and Adam Singer, MD, founder and CEO of IPC-The Hospitalist Company, based in North Hollywood, Calif., accomplished it in January.
During 2007, Dr. Singer set the wheels in motion for taking IPC public the following year. “Our company is built right, has a solid revenue stream, and the nirvana of a real healthcare company—a battle-tested, proven business model,” he says.
Dr. Singer and his management team had the usual reasons for going public: raising capital to pay for operations and to allow for growth by acquisition, reducing debt, and creating liquidity for shareholders. He also had other fish to fry with a public offering. “I wanted to be the first in our industry to make it out of the box,’’ he says. “I also wanted IPC to be a model for the many hospital medicine companies that would like to mature beyond having a bunch of doctors running around a hospital and calling themselves a hospitalist medicine company.”
For Dr. Singer, going public went beyond the desire to produce quarterly financial results that would warm investors’ hearts. It spoke to his core belief in what the business of hospital medicine should be and, from his vantage point, isn’t.
“By leading a publicly traded hospital medicine company I am debunking the myth that hospitalist groups need hospital subsidies to survive,” he says. “This is a powerful myth, one that is mired in a work force’s idea that its members should get full-time pay for less than full-time work. IPC has raised the bar for our industry. We think that hospitals should demand the overall level of sophistication, physician commitment and productivity that IPC has.”
With few publicly traded physician companies for templates for a public offering, Dr. Singer looked to a colleague, Roger Medel, MD, for direction. Dr. Medel took his company public in 1979 and has grown Sunrise, Fla.-based Pediatrix Medical Group, a provider of neonatal, maternal-fetal, and pediatric intensivist/hospitalist services, from a company with $100 million in market capitalization to $3.32 billion and a recent stock price of $67 per share. The company has a “buy” consensus rating from analysts and respectable price-to-earning and earnings-per-share values.
Economic Evolution
Medical staffing firm IPOs, such as IPC’s, are relatively rare. Most venture capital chases the next hot thing in medical information technology, biotechnology, and medical testing. The quirks of the medical staffing industry, such as hospitalist hiring—where salary increases can consume sizable chunks of a firm’s revenues—may deter potential investors.
Why are publicly traded medical staffing companies like IPC and PDX the exception rather than the rule? Because they rely so heavily on human capital—primarily physicians—for bottom-line results, they must contend with recruiting and retaining from a highly sought after talent pool that have their choice of job opportunities.
Also, many physicians fear the corporatization of medicine, an anxiety that working for a publicly traded company tends to arouse. Physician idealism—wanting to make the world a better place—may clash with a public corporation’s raison d’etre: making money. In a young field like hospital medicine, where performance metrics are evolving, balancing shareholder demands for ROI versus quality patient care requires a delicate touch.
Larry Wellikson, MD, SHM’s chief executive officer, says IPC’s entry into the public markets has been received well, indicating the maturation and strong growth of hospital medicine.
IPC’s public offering took place Jan. 30. Lead underwriters Credit Suisse Securities and Jeffries & Co. offered 5.9 million shares of IPC stock under the ticker symbol IPCM, a four-letter symbol conforming with NASDAQ’s listing requirements. The stock traded mostly at $19 per share, above the original per share estimate of between $15 to $17, raising approximately $38.3 million in net proceeds.
Since then, IPCM shares have ranged from $16.25 to $23.09 per share, trading at a thin average daily volume of 162,000. As of March 31, IPC’s market capitalization was $296 million. Six months from the IPO, average daily volume should increase, as regulations on shareholder sales are eased according to stock exchange rules.
IPC’s latest financial results were upbeat. The firm reported record operating results for the fourth quarter and full year 2007. Total patient encounters rose 29%, compared with 460,000 over the same period in 2006. Fourth-quarter net revenues were $52.6 million, a 31% increase from $40.2 million in fourth-quarter 2006. Physician practice salaries and other expenses for the period were $36.9 million vs. $29.5 million for fourth-quarter 2006. As a percentage of net revenue, physician salaries declined to 70% from 73% in the fourth quarter of 2007 vs. 2006. Dr. Singer attributed the change to higher physician productivity and increased revenue per encounter.
With the stock market retrenching since its all-time high in October, IPC’s timing on going public might seem a bit off. Yet, venture capitalists are bullish on healthcare. They sank a record $9.97 billion into the sector in 2007, topping the previous high of $9.47 billion in 2000, during the dot.com craze. Three large venture capital firms specializing in healthcare have $1.25 billion looking for good homes. The worry on Wall Street is that there won’t be enough healthcare IPOs to satisfy demand; there were only 31 in 2007 vs. 60 in 2000.
Alternatives
Going public is not the only way hospital medicine companies and other physician-intensive enterprises can raise needed capital. Venture capital plays a critical role. Brentwood, Tenn.-based Cogent Healthcare received its first round of such funding in 1997, a second infusion in 2000, and $15 million in 2002. IPC is no stranger to venture capital either: It raised $47 million in venture capital since 1998. Such capital infusions helped IPC and Cogent in their early days by providing the money needed to start hospital medicine groups, recruit top managers, expand into new markets, and improve IT and communication infrastructures.
Some entrepreneurs favor keeping their companies private. For example, John Erickson, founder and CEO of Baltimore-based Erickson Retirement Communities (ERC), is committed to growing his business without going public. There are 19 Erickson campuses in 11 states, with 21,000 residents. ERC’s business plan involves adding sites, anticipating growth to 55,000 residents in five years. Such steady expansion gobbles up capital, but Erickson is adamant about staying private. On going public he says: “I consider it whenever I need capital, but it’s hard to keep public markets happy. If your business slows down for any reason, your stock tanks and the market will punish you harshly. I will not have stock analysts pressuring me about how to run and grow my business.”
Erickson admits the competing demands of raising capital and keeping the company private aren’t easy to reconcile. “We go to midsized and large banks and [real estate investment trusts], get letters of credit, tax bonds, debt financing, mezzanine financing, etc.,” he says. He considers that others in his industry, Sunrise Senior Living (SRZ) and Brookdale Senior Living (BKD) that have gone public show the industry’s strength. “Multiple sources of capitalization in an industry provide greater options for all,” he adds.
That said, Erickson intends to resist any temptation to go public because “I must have the flexibility to implement our five-year plan correctly. If I want to invest $30 million in a medical group or hire seven doctors at $150,000 a pop, I don’t have to answer to some 30-year-old stock analyst who doesn’t like that.”
As for IPC’s public offering, Erickson says the first company to do so in an industry opens new avenues for raising capital in the public arena. “Dr. Singer’s pushing the envelope for hospital medicine, and if he can tolerate the pressure of the market—even when the strings are very tight—that’s great,” he emphasizes.
Commenting on the legal and governance issues of a public offering, Peter Olberg, corporate and finance partner at Manhattan-based law firm of Manatt, Philips and Philips says IPC’s being the first publicly traded hospitalist medicine company is a sound way to raise capital and isn’t risky in terms of disclosure. However, a specialty care provider like IPC can “become a victim of its own success. Public payers can say reimbursement is too high and cut it based on the leader’s financial performance.”
Peer Perspective
SHM President Patrick Cawley, MD, MBA, calls IPC’s public offering a major milestone because it demonstrates the maturity of the hospitalist movement. He expects IPC to use the infusion of capital to step up physician hiring, acquire more groups, and improve its proprietary IT infrastructure by refining its tools to further link outcomes and performance.
“IPC’s emphasis on quality outcomes is clearly where medicine is going,” Dr. Cawley says. And, “Putting pressure on hospitalists to be more productive has a huge potential in helping hospital medicine get more efficient by seeing more patients.”
To put the IPC public offering in perspective Dr. Cawley captures Dr. Singer’s vision. “To run a public company, you focus beyond daily stock prices and on the intermediate and short-term. What Wall Street thinks about your business matters. Our product [hospital medicine] has a great future, and I applaud Adam Singer for taking this step.”
Giving Dr. Singer the last word, he says “I’m a big believer in not worrying about things I can’t control like stock market fluctuations. We can handle good news and bad. We have a good business model and we’ll stick to the knitting.” TH
Marlene Piturro is a medical writer based in New York.
You know your industry is on the map when a trailblazer takes his company public. That signals the capital markets that top executives in a leading company are confident in their business model’s ability to grow the company enough to satisfy Wall Street’s voracious hunger for profits.
It’s a tall order, and Adam Singer, MD, founder and CEO of IPC-The Hospitalist Company, based in North Hollywood, Calif., accomplished it in January.
During 2007, Dr. Singer set the wheels in motion for taking IPC public the following year. “Our company is built right, has a solid revenue stream, and the nirvana of a real healthcare company—a battle-tested, proven business model,” he says.
Dr. Singer and his management team had the usual reasons for going public: raising capital to pay for operations and to allow for growth by acquisition, reducing debt, and creating liquidity for shareholders. He also had other fish to fry with a public offering. “I wanted to be the first in our industry to make it out of the box,’’ he says. “I also wanted IPC to be a model for the many hospital medicine companies that would like to mature beyond having a bunch of doctors running around a hospital and calling themselves a hospitalist medicine company.”
For Dr. Singer, going public went beyond the desire to produce quarterly financial results that would warm investors’ hearts. It spoke to his core belief in what the business of hospital medicine should be and, from his vantage point, isn’t.
“By leading a publicly traded hospital medicine company I am debunking the myth that hospitalist groups need hospital subsidies to survive,” he says. “This is a powerful myth, one that is mired in a work force’s idea that its members should get full-time pay for less than full-time work. IPC has raised the bar for our industry. We think that hospitals should demand the overall level of sophistication, physician commitment and productivity that IPC has.”
With few publicly traded physician companies for templates for a public offering, Dr. Singer looked to a colleague, Roger Medel, MD, for direction. Dr. Medel took his company public in 1979 and has grown Sunrise, Fla.-based Pediatrix Medical Group, a provider of neonatal, maternal-fetal, and pediatric intensivist/hospitalist services, from a company with $100 million in market capitalization to $3.32 billion and a recent stock price of $67 per share. The company has a “buy” consensus rating from analysts and respectable price-to-earning and earnings-per-share values.
Economic Evolution
Medical staffing firm IPOs, such as IPC’s, are relatively rare. Most venture capital chases the next hot thing in medical information technology, biotechnology, and medical testing. The quirks of the medical staffing industry, such as hospitalist hiring—where salary increases can consume sizable chunks of a firm’s revenues—may deter potential investors.
Why are publicly traded medical staffing companies like IPC and PDX the exception rather than the rule? Because they rely so heavily on human capital—primarily physicians—for bottom-line results, they must contend with recruiting and retaining from a highly sought after talent pool that have their choice of job opportunities.
Also, many physicians fear the corporatization of medicine, an anxiety that working for a publicly traded company tends to arouse. Physician idealism—wanting to make the world a better place—may clash with a public corporation’s raison d’etre: making money. In a young field like hospital medicine, where performance metrics are evolving, balancing shareholder demands for ROI versus quality patient care requires a delicate touch.
Larry Wellikson, MD, SHM’s chief executive officer, says IPC’s entry into the public markets has been received well, indicating the maturation and strong growth of hospital medicine.
IPC’s public offering took place Jan. 30. Lead underwriters Credit Suisse Securities and Jeffries & Co. offered 5.9 million shares of IPC stock under the ticker symbol IPCM, a four-letter symbol conforming with NASDAQ’s listing requirements. The stock traded mostly at $19 per share, above the original per share estimate of between $15 to $17, raising approximately $38.3 million in net proceeds.
Since then, IPCM shares have ranged from $16.25 to $23.09 per share, trading at a thin average daily volume of 162,000. As of March 31, IPC’s market capitalization was $296 million. Six months from the IPO, average daily volume should increase, as regulations on shareholder sales are eased according to stock exchange rules.
IPC’s latest financial results were upbeat. The firm reported record operating results for the fourth quarter and full year 2007. Total patient encounters rose 29%, compared with 460,000 over the same period in 2006. Fourth-quarter net revenues were $52.6 million, a 31% increase from $40.2 million in fourth-quarter 2006. Physician practice salaries and other expenses for the period were $36.9 million vs. $29.5 million for fourth-quarter 2006. As a percentage of net revenue, physician salaries declined to 70% from 73% in the fourth quarter of 2007 vs. 2006. Dr. Singer attributed the change to higher physician productivity and increased revenue per encounter.
With the stock market retrenching since its all-time high in October, IPC’s timing on going public might seem a bit off. Yet, venture capitalists are bullish on healthcare. They sank a record $9.97 billion into the sector in 2007, topping the previous high of $9.47 billion in 2000, during the dot.com craze. Three large venture capital firms specializing in healthcare have $1.25 billion looking for good homes. The worry on Wall Street is that there won’t be enough healthcare IPOs to satisfy demand; there were only 31 in 2007 vs. 60 in 2000.
Alternatives
Going public is not the only way hospital medicine companies and other physician-intensive enterprises can raise needed capital. Venture capital plays a critical role. Brentwood, Tenn.-based Cogent Healthcare received its first round of such funding in 1997, a second infusion in 2000, and $15 million in 2002. IPC is no stranger to venture capital either: It raised $47 million in venture capital since 1998. Such capital infusions helped IPC and Cogent in their early days by providing the money needed to start hospital medicine groups, recruit top managers, expand into new markets, and improve IT and communication infrastructures.
Some entrepreneurs favor keeping their companies private. For example, John Erickson, founder and CEO of Baltimore-based Erickson Retirement Communities (ERC), is committed to growing his business without going public. There are 19 Erickson campuses in 11 states, with 21,000 residents. ERC’s business plan involves adding sites, anticipating growth to 55,000 residents in five years. Such steady expansion gobbles up capital, but Erickson is adamant about staying private. On going public he says: “I consider it whenever I need capital, but it’s hard to keep public markets happy. If your business slows down for any reason, your stock tanks and the market will punish you harshly. I will not have stock analysts pressuring me about how to run and grow my business.”
Erickson admits the competing demands of raising capital and keeping the company private aren’t easy to reconcile. “We go to midsized and large banks and [real estate investment trusts], get letters of credit, tax bonds, debt financing, mezzanine financing, etc.,” he says. He considers that others in his industry, Sunrise Senior Living (SRZ) and Brookdale Senior Living (BKD) that have gone public show the industry’s strength. “Multiple sources of capitalization in an industry provide greater options for all,” he adds.
That said, Erickson intends to resist any temptation to go public because “I must have the flexibility to implement our five-year plan correctly. If I want to invest $30 million in a medical group or hire seven doctors at $150,000 a pop, I don’t have to answer to some 30-year-old stock analyst who doesn’t like that.”
As for IPC’s public offering, Erickson says the first company to do so in an industry opens new avenues for raising capital in the public arena. “Dr. Singer’s pushing the envelope for hospital medicine, and if he can tolerate the pressure of the market—even when the strings are very tight—that’s great,” he emphasizes.
Commenting on the legal and governance issues of a public offering, Peter Olberg, corporate and finance partner at Manhattan-based law firm of Manatt, Philips and Philips says IPC’s being the first publicly traded hospitalist medicine company is a sound way to raise capital and isn’t risky in terms of disclosure. However, a specialty care provider like IPC can “become a victim of its own success. Public payers can say reimbursement is too high and cut it based on the leader’s financial performance.”
Peer Perspective
SHM President Patrick Cawley, MD, MBA, calls IPC’s public offering a major milestone because it demonstrates the maturity of the hospitalist movement. He expects IPC to use the infusion of capital to step up physician hiring, acquire more groups, and improve its proprietary IT infrastructure by refining its tools to further link outcomes and performance.
“IPC’s emphasis on quality outcomes is clearly where medicine is going,” Dr. Cawley says. And, “Putting pressure on hospitalists to be more productive has a huge potential in helping hospital medicine get more efficient by seeing more patients.”
To put the IPC public offering in perspective Dr. Cawley captures Dr. Singer’s vision. “To run a public company, you focus beyond daily stock prices and on the intermediate and short-term. What Wall Street thinks about your business matters. Our product [hospital medicine] has a great future, and I applaud Adam Singer for taking this step.”
Giving Dr. Singer the last word, he says “I’m a big believer in not worrying about things I can’t control like stock market fluctuations. We can handle good news and bad. We have a good business model and we’ll stick to the knitting.” TH
Marlene Piturro is a medical writer based in New York.
Generalist
Medical generalists tell a sad story. Their steadily declining numbers reflect a compensation system that still rewards specialists handsomely at generalists’ expense.
Even though the venerable relative value unit (RVU)-based reimbursement system was intended to equalize pay between primary care’s cognitive work and specialists’ procedure-driven high pay, it hasn’t. Since 1992, when Medicare started paying physicians using RVUs based on the resources used, the specialist-generalist gap remains. RVUs comprise three factors:
- Work (55%);
- Practice expense (42%); and
- Malpractice insurance (3%).
Arguably, generalist RVUs have risen and proceduralist RVUs have decreased. However, generalists argue this skewed pay scale still causes residents to shun internal medicine, hospital medicine, family practice, general pediatrics, and general surgery. Is that true?
Hospitalists and RVUs
Although RVUs don’t always figure into hospitalist compensation, they can have an effect. Vibhu Sharma, MD, of SUNY Downstate Medical Center’s section director, hospital medicine program, heads a 13-hospitalist group employed by the medical center and carries extensive teaching responsibilities.
RVUs don’t currently factor into his hospitalists’ pay but that’s becoming troublesome to Dr. Sharma. “We’d make a lot more money if RVUs were factored in, but they aren’t because we’re a teaching hospital,” he says. “Our group is only four years old, and we aren’t ready to push for it.”
Without the RVU productivity component, Dr. Sharma says he’s at a disadvantage when recruiting. Internal medicine, family practice, and other generalists “stuck with the perception that specialization is a better career option,” he says. “If payers paid us the same as non-invasive cardiologists there’d be a lot more hospitalists.”
Boosts in compensation will be slow in coming, says Dr. Sharma, because hospitalists have demonstrated only modest cost savings and LOS decreases. He adds: “Today nobody wants to be a hospitalist for the rest of their career. We perceive that the patient care we deliver isn’t well compensated, and that the RVU gap between generalists and sub-specialists can never be closed.” As for RVUs, he sees the hospital eventually adding an RVU bonus component. For now, it bumps up hospitalist salaries when the group complains.
The three-member pediatric hospitalist group at Kentucky Children’s Hospital also doesn’t use RVUs, either for compensation or as a productivity proxy. Jeff Bennett, MD, its lead hospitalist, says pediatric outcomes data aren’t robust enough to establish proper RVU benchmarks. He adds that adult RVUs are “denser” than pediatric RVUs because of lower acuity and fewer procedures with children’s illnesses. Additionally, productivity measures don’t affect pediatrics significantly because children’s hospitals “are at the bottom of the funnel,” he says. “We have to take every kid who comes our way. Pediatric hospitals tend not to be competitive. There are four hospitals in town competing for adult patients, while we’re the only tertiary care hospital for 300 miles.”
Compounding the problem is that determining pediatric hospitalist compensation is problematic. With only 2,200 pediatric hospitalists versus 20,000 who work with adults, compensation packages tend to idiosyncratic. “Compensation is important, but RVUs won’t figure into pediatrics for a while,” says Dr. Bennett. “People chose hospital medicine from residency because they’re itching for inpatient work, with its complexity and sharp edges. The shine dims quickly, though, because they are protected during residency and then have full responsibility as hospitalists.”
David Dale, MD, director of the University of Washington’s internal medicine residency program, and American College of Physicians’ president, says hospitalist careers loom large for his annual crop of 35 to 40 residents—but RVUs don’t. “For them it’s an easy transition, a guaranteed salary versus establishing a small business,” he says. “The office practice is where the RVUs really impact generalists. We have a hard job preparing residents for those reimbursement issues.”
Dr. Dale says between two-thirds and three-quarters of his residents become hospitalists, although that’s often not their final career destination. “Some don’t treat hospitalist medicine as a long-term career because the work is hard and the hours are stressful. Many are waiting for a fellowship track to specialization.”
The General Surgeon
A 2007 article by Josef Fischer, MD, in the Journal of the American Medical Association raises questions about the dwindling general surgeon cadre.1 Dr. Fischer posits that RVUs can’t boost surgeons’ incomes because surgeons can’t increase utilization when reimbursement decreases.
For example, since patients have only one gallbladder and indications for removal are constant, there’s no way to increase surgical RVUs. He says this unattractive RVU scheme dissuades residents from general surgery careers.
Dr. Fischer’s concerns don’t faze David Joyce, CEO of Morrisville, N.C.-based Delphi Healthcare Partners, which has three surgicalist programs nationally. Each employs two general surgeons working two weeks on, two weeks off, covering indigent and unassigned patients.
On average, each sees eight patients daily, two requiring surgery. The surgicalists all are either age 50 to 55 or under 35 and reject the hassles of office-based practices at both ends of the career ladder. They earn fixed salaries; Delphi uses RVUs for reimbursement but not for productivity bonuses.
“RVUs aren’t very important in our surgicalist equation, which is a winning situation for everyone involved,” Joyce says. “Private-practice surgeons are thrilled because they don’t cover call and can build their practices. The hospitals do well and don’t mind kicking in several hundred thousand dollars to cover surgicalist compensation.
“In our Charleston, W. Va., program the hospital derived $1.6 million above our program’s cost because the private docs did more surgeries, our surgicalists do what they were trained to do and are well compensated. It’s great,” he says.
Delphi surgicalist Richard Fogle, MD, works at Thomas Memorial Hospital in South Charleston, W. Va., and doesn’t think about RVUs. “The problem with surgeons is lifestyle,” he asserts. “If you have 10 surgeons, you cover call once every 10 days. With three surgeons it’s once every three days.”
Delphi solved his hospital’s problem by recruiting him and another surgicalist. “Before we came most general surgeons had left,” Dr. Fogle says. “Now, two have come back, and four more have settled here. We’re not competing with them for business, and they can build their office practices — particularly with outpatient procedures.”
As a surgicalist, Dr. Fogle, doesn’t miss spending 50% of revenues on office overhead, or leaving 20 patients sitting in his office while answering a hospital page. “I keep waiting for the other shoe to drop, but it hasn’t,” he says of his freedom to practice surgery unfettered by office busyness. He’s happy with the compensation but has a bone to pick with the RVU system. “RVUs are too low for general surgery, and anyone who discounts the cognitive part of surgery procedures is seriously mistaken,” he says.
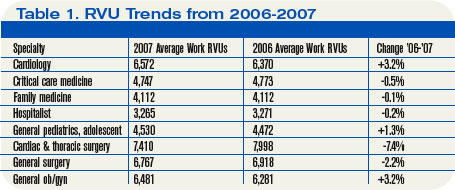
Different Strokes
John Marcelis, MD, an Erickson Retirement Communities regional medical director of 19 providers in four communities, gives the RVU discussion another twist. He practices at Ann’s Choice in Warminster, Pa., with four other physicians, each of whom acts as the group’s hospitalist once every five weeks.
Previously he spent 10 years at the University of Pennsylvania hospital system, where RVUs figured in significantly and volume was highly rewarded. Taking a huge pay cut to practice at Erickson, he happily left the RVU treadmill. “I didn’t like seeing patients at RVU factories,” he recalls. “At Erickson, we have half-hour office visits and see our hospitalized patients as needed. An RVU system doesn’t compute with us.”
Dr. Marcelis, who lost sleep when he was part of an RVU system, sees a bimodal curve of doctors—some thrive on RVUs, others don’t. “There are some doctors who want to see 50 MIs in a day,” he says. “They relish the high-volume intensity. ‘Bring ’em on,’ they say. RVU systems work well for them. For doctors who value longitudinal relationships with patients, RVUs don’t work well.”
He doesn’t see the cognitive vs. procedure gap leading to RVUs ever closing: “There’s a pool of dollars, and shifting 5% from procedures to cognitive work can’t change things. If payers lower RVUs for procedures, specialists will just do more procedures.” TH
Marlene Piturro is a medical writer based in New York.
Reference
- Fischer J. The impending disappearance of the general surgeon. JAMA. 2007;298:2191-2193.
Medical generalists tell a sad story. Their steadily declining numbers reflect a compensation system that still rewards specialists handsomely at generalists’ expense.
Even though the venerable relative value unit (RVU)-based reimbursement system was intended to equalize pay between primary care’s cognitive work and specialists’ procedure-driven high pay, it hasn’t. Since 1992, when Medicare started paying physicians using RVUs based on the resources used, the specialist-generalist gap remains. RVUs comprise three factors:
- Work (55%);
- Practice expense (42%); and
- Malpractice insurance (3%).
Arguably, generalist RVUs have risen and proceduralist RVUs have decreased. However, generalists argue this skewed pay scale still causes residents to shun internal medicine, hospital medicine, family practice, general pediatrics, and general surgery. Is that true?
Hospitalists and RVUs
Although RVUs don’t always figure into hospitalist compensation, they can have an effect. Vibhu Sharma, MD, of SUNY Downstate Medical Center’s section director, hospital medicine program, heads a 13-hospitalist group employed by the medical center and carries extensive teaching responsibilities.
RVUs don’t currently factor into his hospitalists’ pay but that’s becoming troublesome to Dr. Sharma. “We’d make a lot more money if RVUs were factored in, but they aren’t because we’re a teaching hospital,” he says. “Our group is only four years old, and we aren’t ready to push for it.”
Without the RVU productivity component, Dr. Sharma says he’s at a disadvantage when recruiting. Internal medicine, family practice, and other generalists “stuck with the perception that specialization is a better career option,” he says. “If payers paid us the same as non-invasive cardiologists there’d be a lot more hospitalists.”
Boosts in compensation will be slow in coming, says Dr. Sharma, because hospitalists have demonstrated only modest cost savings and LOS decreases. He adds: “Today nobody wants to be a hospitalist for the rest of their career. We perceive that the patient care we deliver isn’t well compensated, and that the RVU gap between generalists and sub-specialists can never be closed.” As for RVUs, he sees the hospital eventually adding an RVU bonus component. For now, it bumps up hospitalist salaries when the group complains.
The three-member pediatric hospitalist group at Kentucky Children’s Hospital also doesn’t use RVUs, either for compensation or as a productivity proxy. Jeff Bennett, MD, its lead hospitalist, says pediatric outcomes data aren’t robust enough to establish proper RVU benchmarks. He adds that adult RVUs are “denser” than pediatric RVUs because of lower acuity and fewer procedures with children’s illnesses. Additionally, productivity measures don’t affect pediatrics significantly because children’s hospitals “are at the bottom of the funnel,” he says. “We have to take every kid who comes our way. Pediatric hospitals tend not to be competitive. There are four hospitals in town competing for adult patients, while we’re the only tertiary care hospital for 300 miles.”
Compounding the problem is that determining pediatric hospitalist compensation is problematic. With only 2,200 pediatric hospitalists versus 20,000 who work with adults, compensation packages tend to idiosyncratic. “Compensation is important, but RVUs won’t figure into pediatrics for a while,” says Dr. Bennett. “People chose hospital medicine from residency because they’re itching for inpatient work, with its complexity and sharp edges. The shine dims quickly, though, because they are protected during residency and then have full responsibility as hospitalists.”
David Dale, MD, director of the University of Washington’s internal medicine residency program, and American College of Physicians’ president, says hospitalist careers loom large for his annual crop of 35 to 40 residents—but RVUs don’t. “For them it’s an easy transition, a guaranteed salary versus establishing a small business,” he says. “The office practice is where the RVUs really impact generalists. We have a hard job preparing residents for those reimbursement issues.”
Dr. Dale says between two-thirds and three-quarters of his residents become hospitalists, although that’s often not their final career destination. “Some don’t treat hospitalist medicine as a long-term career because the work is hard and the hours are stressful. Many are waiting for a fellowship track to specialization.”
The General Surgeon
A 2007 article by Josef Fischer, MD, in the Journal of the American Medical Association raises questions about the dwindling general surgeon cadre.1 Dr. Fischer posits that RVUs can’t boost surgeons’ incomes because surgeons can’t increase utilization when reimbursement decreases.
For example, since patients have only one gallbladder and indications for removal are constant, there’s no way to increase surgical RVUs. He says this unattractive RVU scheme dissuades residents from general surgery careers.
Dr. Fischer’s concerns don’t faze David Joyce, CEO of Morrisville, N.C.-based Delphi Healthcare Partners, which has three surgicalist programs nationally. Each employs two general surgeons working two weeks on, two weeks off, covering indigent and unassigned patients.
On average, each sees eight patients daily, two requiring surgery. The surgicalists all are either age 50 to 55 or under 35 and reject the hassles of office-based practices at both ends of the career ladder. They earn fixed salaries; Delphi uses RVUs for reimbursement but not for productivity bonuses.
“RVUs aren’t very important in our surgicalist equation, which is a winning situation for everyone involved,” Joyce says. “Private-practice surgeons are thrilled because they don’t cover call and can build their practices. The hospitals do well and don’t mind kicking in several hundred thousand dollars to cover surgicalist compensation.
“In our Charleston, W. Va., program the hospital derived $1.6 million above our program’s cost because the private docs did more surgeries, our surgicalists do what they were trained to do and are well compensated. It’s great,” he says.
Delphi surgicalist Richard Fogle, MD, works at Thomas Memorial Hospital in South Charleston, W. Va., and doesn’t think about RVUs. “The problem with surgeons is lifestyle,” he asserts. “If you have 10 surgeons, you cover call once every 10 days. With three surgeons it’s once every three days.”
Delphi solved his hospital’s problem by recruiting him and another surgicalist. “Before we came most general surgeons had left,” Dr. Fogle says. “Now, two have come back, and four more have settled here. We’re not competing with them for business, and they can build their office practices — particularly with outpatient procedures.”
As a surgicalist, Dr. Fogle, doesn’t miss spending 50% of revenues on office overhead, or leaving 20 patients sitting in his office while answering a hospital page. “I keep waiting for the other shoe to drop, but it hasn’t,” he says of his freedom to practice surgery unfettered by office busyness. He’s happy with the compensation but has a bone to pick with the RVU system. “RVUs are too low for general surgery, and anyone who discounts the cognitive part of surgery procedures is seriously mistaken,” he says.
Different Strokes
John Marcelis, MD, an Erickson Retirement Communities regional medical director of 19 providers in four communities, gives the RVU discussion another twist. He practices at Ann’s Choice in Warminster, Pa., with four other physicians, each of whom acts as the group’s hospitalist once every five weeks.
Previously he spent 10 years at the University of Pennsylvania hospital system, where RVUs figured in significantly and volume was highly rewarded. Taking a huge pay cut to practice at Erickson, he happily left the RVU treadmill. “I didn’t like seeing patients at RVU factories,” he recalls. “At Erickson, we have half-hour office visits and see our hospitalized patients as needed. An RVU system doesn’t compute with us.”
Dr. Marcelis, who lost sleep when he was part of an RVU system, sees a bimodal curve of doctors—some thrive on RVUs, others don’t. “There are some doctors who want to see 50 MIs in a day,” he says. “They relish the high-volume intensity. ‘Bring ’em on,’ they say. RVU systems work well for them. For doctors who value longitudinal relationships with patients, RVUs don’t work well.”
He doesn’t see the cognitive vs. procedure gap leading to RVUs ever closing: “There’s a pool of dollars, and shifting 5% from procedures to cognitive work can’t change things. If payers lower RVUs for procedures, specialists will just do more procedures.” TH
Marlene Piturro is a medical writer based in New York.
Reference
- Fischer J. The impending disappearance of the general surgeon. JAMA. 2007;298:2191-2193.
Medical generalists tell a sad story. Their steadily declining numbers reflect a compensation system that still rewards specialists handsomely at generalists’ expense.
Even though the venerable relative value unit (RVU)-based reimbursement system was intended to equalize pay between primary care’s cognitive work and specialists’ procedure-driven high pay, it hasn’t. Since 1992, when Medicare started paying physicians using RVUs based on the resources used, the specialist-generalist gap remains. RVUs comprise three factors:
- Work (55%);
- Practice expense (42%); and
- Malpractice insurance (3%).
Arguably, generalist RVUs have risen and proceduralist RVUs have decreased. However, generalists argue this skewed pay scale still causes residents to shun internal medicine, hospital medicine, family practice, general pediatrics, and general surgery. Is that true?
Hospitalists and RVUs
Although RVUs don’t always figure into hospitalist compensation, they can have an effect. Vibhu Sharma, MD, of SUNY Downstate Medical Center’s section director, hospital medicine program, heads a 13-hospitalist group employed by the medical center and carries extensive teaching responsibilities.
RVUs don’t currently factor into his hospitalists’ pay but that’s becoming troublesome to Dr. Sharma. “We’d make a lot more money if RVUs were factored in, but they aren’t because we’re a teaching hospital,” he says. “Our group is only four years old, and we aren’t ready to push for it.”
Without the RVU productivity component, Dr. Sharma says he’s at a disadvantage when recruiting. Internal medicine, family practice, and other generalists “stuck with the perception that specialization is a better career option,” he says. “If payers paid us the same as non-invasive cardiologists there’d be a lot more hospitalists.”
Boosts in compensation will be slow in coming, says Dr. Sharma, because hospitalists have demonstrated only modest cost savings and LOS decreases. He adds: “Today nobody wants to be a hospitalist for the rest of their career. We perceive that the patient care we deliver isn’t well compensated, and that the RVU gap between generalists and sub-specialists can never be closed.” As for RVUs, he sees the hospital eventually adding an RVU bonus component. For now, it bumps up hospitalist salaries when the group complains.
The three-member pediatric hospitalist group at Kentucky Children’s Hospital also doesn’t use RVUs, either for compensation or as a productivity proxy. Jeff Bennett, MD, its lead hospitalist, says pediatric outcomes data aren’t robust enough to establish proper RVU benchmarks. He adds that adult RVUs are “denser” than pediatric RVUs because of lower acuity and fewer procedures with children’s illnesses. Additionally, productivity measures don’t affect pediatrics significantly because children’s hospitals “are at the bottom of the funnel,” he says. “We have to take every kid who comes our way. Pediatric hospitals tend not to be competitive. There are four hospitals in town competing for adult patients, while we’re the only tertiary care hospital for 300 miles.”
Compounding the problem is that determining pediatric hospitalist compensation is problematic. With only 2,200 pediatric hospitalists versus 20,000 who work with adults, compensation packages tend to idiosyncratic. “Compensation is important, but RVUs won’t figure into pediatrics for a while,” says Dr. Bennett. “People chose hospital medicine from residency because they’re itching for inpatient work, with its complexity and sharp edges. The shine dims quickly, though, because they are protected during residency and then have full responsibility as hospitalists.”
David Dale, MD, director of the University of Washington’s internal medicine residency program, and American College of Physicians’ president, says hospitalist careers loom large for his annual crop of 35 to 40 residents—but RVUs don’t. “For them it’s an easy transition, a guaranteed salary versus establishing a small business,” he says. “The office practice is where the RVUs really impact generalists. We have a hard job preparing residents for those reimbursement issues.”
Dr. Dale says between two-thirds and three-quarters of his residents become hospitalists, although that’s often not their final career destination. “Some don’t treat hospitalist medicine as a long-term career because the work is hard and the hours are stressful. Many are waiting for a fellowship track to specialization.”
The General Surgeon
A 2007 article by Josef Fischer, MD, in the Journal of the American Medical Association raises questions about the dwindling general surgeon cadre.1 Dr. Fischer posits that RVUs can’t boost surgeons’ incomes because surgeons can’t increase utilization when reimbursement decreases.
For example, since patients have only one gallbladder and indications for removal are constant, there’s no way to increase surgical RVUs. He says this unattractive RVU scheme dissuades residents from general surgery careers.
Dr. Fischer’s concerns don’t faze David Joyce, CEO of Morrisville, N.C.-based Delphi Healthcare Partners, which has three surgicalist programs nationally. Each employs two general surgeons working two weeks on, two weeks off, covering indigent and unassigned patients.
On average, each sees eight patients daily, two requiring surgery. The surgicalists all are either age 50 to 55 or under 35 and reject the hassles of office-based practices at both ends of the career ladder. They earn fixed salaries; Delphi uses RVUs for reimbursement but not for productivity bonuses.
“RVUs aren’t very important in our surgicalist equation, which is a winning situation for everyone involved,” Joyce says. “Private-practice surgeons are thrilled because they don’t cover call and can build their practices. The hospitals do well and don’t mind kicking in several hundred thousand dollars to cover surgicalist compensation.
“In our Charleston, W. Va., program the hospital derived $1.6 million above our program’s cost because the private docs did more surgeries, our surgicalists do what they were trained to do and are well compensated. It’s great,” he says.
Delphi surgicalist Richard Fogle, MD, works at Thomas Memorial Hospital in South Charleston, W. Va., and doesn’t think about RVUs. “The problem with surgeons is lifestyle,” he asserts. “If you have 10 surgeons, you cover call once every 10 days. With three surgeons it’s once every three days.”
Delphi solved his hospital’s problem by recruiting him and another surgicalist. “Before we came most general surgeons had left,” Dr. Fogle says. “Now, two have come back, and four more have settled here. We’re not competing with them for business, and they can build their office practices — particularly with outpatient procedures.”
As a surgicalist, Dr. Fogle, doesn’t miss spending 50% of revenues on office overhead, or leaving 20 patients sitting in his office while answering a hospital page. “I keep waiting for the other shoe to drop, but it hasn’t,” he says of his freedom to practice surgery unfettered by office busyness. He’s happy with the compensation but has a bone to pick with the RVU system. “RVUs are too low for general surgery, and anyone who discounts the cognitive part of surgery procedures is seriously mistaken,” he says.
Different Strokes
John Marcelis, MD, an Erickson Retirement Communities regional medical director of 19 providers in four communities, gives the RVU discussion another twist. He practices at Ann’s Choice in Warminster, Pa., with four other physicians, each of whom acts as the group’s hospitalist once every five weeks.
Previously he spent 10 years at the University of Pennsylvania hospital system, where RVUs figured in significantly and volume was highly rewarded. Taking a huge pay cut to practice at Erickson, he happily left the RVU treadmill. “I didn’t like seeing patients at RVU factories,” he recalls. “At Erickson, we have half-hour office visits and see our hospitalized patients as needed. An RVU system doesn’t compute with us.”
Dr. Marcelis, who lost sleep when he was part of an RVU system, sees a bimodal curve of doctors—some thrive on RVUs, others don’t. “There are some doctors who want to see 50 MIs in a day,” he says. “They relish the high-volume intensity. ‘Bring ’em on,’ they say. RVU systems work well for them. For doctors who value longitudinal relationships with patients, RVUs don’t work well.”
He doesn’t see the cognitive vs. procedure gap leading to RVUs ever closing: “There’s a pool of dollars, and shifting 5% from procedures to cognitive work can’t change things. If payers lower RVUs for procedures, specialists will just do more procedures.” TH
Marlene Piturro is a medical writer based in New York.
Reference
- Fischer J. The impending disappearance of the general surgeon. JAMA. 2007;298:2191-2193.
One for the Ages
A t 77, Robert Eddy, MD, is a busy fellow. As a hospitalist at the 278-bed Brantford General Hospital in Brantford, Ontario, Canada, he works an average of 70 hours a week.
What keeps him going?
“After a long day at work I really look forward to my gin and tonic,” he says. “I have a picture of it in my mind when I’m driving home.”
On a more serious note, Dr. Eddy attributes his career longevity to good health, good genes, never smoking, and not overdoing the booze.
“I’m very lucky,” he says. “As a doctor you can keep going as long as you don’t have major health problems. My dad died in his 90s, so longevity runs in my family.”
Dr. Eddy rises early to do paperwork at his home office, then drives 20 minutes to the hospital and performs his hospitalist duties five mornings a week, Monday through Friday. On an average day he sees 12 inpatients, completes his charts, then grabs a quick lunch before heading out to see patients in a shared office practice in Burford, about nine miles away.
Scheduling around his hospitalist work and the office practice, he also makes house calls and nursing home visits to his sickest and frailest patients. He covers for his community-based colleagues and hospitalists, and twice a month organizes CME meetings for family physicians. From March to July he adds a temporary assignment at St. Joseph’s Villa in Dundas, tending to 70 patients at that retirement community.
Janice Legere, MD, medical director of the hospitalist program of Brantford General Hospital, calls him “a country guy with a very dry sense of humor. The other hospitalists look up to him because he is the real deal as a doctor.”
Not bad for a gentleman born in the same year and month as the beginning of the Great Depression—October 1929. In his sixth decade of medicine, Dr. Eddy may be the oldest practicing hospitalist.
—Sandra Eddy, wife of Robert Eddy, MD, hospitalist at Brantford General Hospital in Ontario, Canada
No Sign of Slowing
Although he has practiced medicine for more than 52 years, retirement is not on his agenda.
“I closed my solo practice in 1999 because I didn’t want to work so hard, but I’m busier than ever now,” he says.
While Dr. Eddy and his second wife, Sandra, seriously discuss the possibility of his retirement every year, they have reupped for the hospitalist work, office practice, and house/nursing home visits at least through 2008. As they describe it, the overburdened Canadian healthcare system needs every qualified pair of physician hands it can get.
Ontario’s healthcare system can ill afford to lose someone of Dr. Eddy’s commitment, knowledge, and experience.
“I love medicine and am very lucky to have the energy and the stamina to keep going,” Dr. Eddy says. “I enjoy seeing hospitalized patients because I have as much time as I need to do a general assessment of their medical condition. I get my mind around the whole patient.”
His wife affirms Dr. Eddy’s commitment.
“We have been together for 28 years, and we have a good marriage,” she says. ‘‘But he is on call 24/7, and medicine always comes first. Then there’s us.”
But Dr. Eddy’s not just a nose-to-the-grindstone type of guy—he and Sandra do relax together. Along with his nightly after-work gin and tonic and an annual week’s trip to Las Vegas, they enjoy outings to the local casino, golf, dinners with friends, and frequent visits from three grandchildren.
“I enjoy the variety in my career as a physician and the quality of my life,” he concludes.

The New Hospitalist
Becoming a hospitalist seemed a logical step for Dr. Eddy when he opted to leave full-time office practice in 1999. Brantford General Hospital, where he had admitting privileges, covered a catchment area of 80,000 people.
When the only two other hospitals in the area were closed, Brantford General was overwhelmed. Adding to the systemic distress, 80% of community doctors had given up their hospital privileges. Hospitalists were urgently needed to pick up the slack. Dr. Eddy went for it.
In Canada, hospital throughput isn’t a priority. The system lacks enough sub-acute and rehab beds to discharge patients from hospitals in a timely fashion, leaving patients hospitalized longer compared with similar care in the United States. The average length of stay for heart failure is 6.1 days in the U.S. versus 8.5 days in Canada; for aortic aneurysm repair it’s seven days (U.S.) versus nine days (Canada), according to the Journal of Cardiology.
Those bottlenecks lead to hospitalized patients ready for a less acute level of care occupying beds needed for acute patients. For example, patients wait months for knee replacement surgery, then spend three to four weeks on the rehab ward in the hospital. A step-down facility would probably be ideal but doesn’t exist. “There are people lying in the ER overnight, people who need to be in palliative care units who are in acute care beds,” Dr. Eddy notes. “It is very tough.”
As a family physician, Dr. Eddy favored a hospitalist career because he would have the time to do a general assessment—a whole-patient, complete check-up. He doesn’t admit patients or work in the ED (“Not my forte; I’m not looking for more stress,” he says), but works on the general medical units.
According to Dr. Legere, the septuagenarian physician works approximately 75% of full-time hospitalist hours. He puts in at least 40 weeks a year and covers at least 10 weekends for the hospitalist service.
Hospitalist Larry Kramer, MD, who has worked side by side with Dr. Eddy since 2002, calls him a compassionate, sensitive physician attuned to the small kindnesses patients and family appreciate, such as remembering everyone’s name.
“He’s an excellent team member, always open to referrals and consultations,” says Dr. Kramer, who’s also impressed with Dr. Eddy’s interest in mastering a Palm Pilot when he discovered how much easier and faster it was to access clinical and pharmaceutical information. “He didn’t grow up with computers, but he sure learned how to use his Palm,” adds Dr. Kramer.

The Office Practice
When he started his hospitalist career, Dr. Eddy fully intended to relinquish the office practice to another family physician. It didn’t happen that way—there were about 200 patients he couldn’t give up.
“They are elderly, and I make house calls if it’s too much of a burden for them to come to the office,” he says. “I also see them in nursing homes or retirement homes.” He also covers the office practice for the month of August so his practice partner can have the month off.
His wife, who fields home office phone calls, attends to the issues of 200 special patients and also tries to guide those looking for a primary care doctor to someone else willing to take them.
“My wife works very hard at managing my private practice,” says Dr. Eddy. “She’s a people person but is not soft-minded at all. She helps a lot of patients find primary care physicians who will take them on as well as fielding calls from my private patients.”
The Ontario Health Insurance Plan (OHIP) pays him on a fee-for-service basis. In 2000, when bureaucrats tried to avoid reimbursing him for making house calls by stipulating that at least 50% had to be for palliative care, he made a list of all 200 patients. He made his case for palliative care—“they’ll all die within four years.” The medical establishment accepted it, and he continues making house calls—for which he says the health authorities are relaxing the regulations.
As if the hospitalist and office practice weren’t enough, Dr. Eddy runs a small group practice CME program sponsored by McMaster University and the College of Family Physicians of Canada. “Six of us family physicians get together to discuss three cases based on handouts and a fact section” he says. The CME group meets twice a month for eight months of the year.
In short, Dr. Eddy describes himself as having energy to burn. His hospitalist colleague Dr. Kramer seconds that.
“The amount of work he does is phenomenal,” Dr. Kramer says. “He is very thorough, and it’s remarkable to see how much he still loves practicing medicine. It’s hard to believe that when he’s finished with his hospitalist job he heads off to his office practice, house calls, and nursing home work.”
And what does Dr. Eddy think of his colleagues?
“They seem quite young,” he says of Brantford’s cadre of six full-time and six part-time hospitalists. “But come to think of it most are in their 40s, and some in their 50s and 60s. Maybe they aren’t so young.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
A t 77, Robert Eddy, MD, is a busy fellow. As a hospitalist at the 278-bed Brantford General Hospital in Brantford, Ontario, Canada, he works an average of 70 hours a week.
What keeps him going?
“After a long day at work I really look forward to my gin and tonic,” he says. “I have a picture of it in my mind when I’m driving home.”
On a more serious note, Dr. Eddy attributes his career longevity to good health, good genes, never smoking, and not overdoing the booze.
“I’m very lucky,” he says. “As a doctor you can keep going as long as you don’t have major health problems. My dad died in his 90s, so longevity runs in my family.”
Dr. Eddy rises early to do paperwork at his home office, then drives 20 minutes to the hospital and performs his hospitalist duties five mornings a week, Monday through Friday. On an average day he sees 12 inpatients, completes his charts, then grabs a quick lunch before heading out to see patients in a shared office practice in Burford, about nine miles away.
Scheduling around his hospitalist work and the office practice, he also makes house calls and nursing home visits to his sickest and frailest patients. He covers for his community-based colleagues and hospitalists, and twice a month organizes CME meetings for family physicians. From March to July he adds a temporary assignment at St. Joseph’s Villa in Dundas, tending to 70 patients at that retirement community.
Janice Legere, MD, medical director of the hospitalist program of Brantford General Hospital, calls him “a country guy with a very dry sense of humor. The other hospitalists look up to him because he is the real deal as a doctor.”
Not bad for a gentleman born in the same year and month as the beginning of the Great Depression—October 1929. In his sixth decade of medicine, Dr. Eddy may be the oldest practicing hospitalist.
—Sandra Eddy, wife of Robert Eddy, MD, hospitalist at Brantford General Hospital in Ontario, Canada
No Sign of Slowing
Although he has practiced medicine for more than 52 years, retirement is not on his agenda.
“I closed my solo practice in 1999 because I didn’t want to work so hard, but I’m busier than ever now,” he says.
While Dr. Eddy and his second wife, Sandra, seriously discuss the possibility of his retirement every year, they have reupped for the hospitalist work, office practice, and house/nursing home visits at least through 2008. As they describe it, the overburdened Canadian healthcare system needs every qualified pair of physician hands it can get.
Ontario’s healthcare system can ill afford to lose someone of Dr. Eddy’s commitment, knowledge, and experience.
“I love medicine and am very lucky to have the energy and the stamina to keep going,” Dr. Eddy says. “I enjoy seeing hospitalized patients because I have as much time as I need to do a general assessment of their medical condition. I get my mind around the whole patient.”
His wife affirms Dr. Eddy’s commitment.
“We have been together for 28 years, and we have a good marriage,” she says. ‘‘But he is on call 24/7, and medicine always comes first. Then there’s us.”
But Dr. Eddy’s not just a nose-to-the-grindstone type of guy—he and Sandra do relax together. Along with his nightly after-work gin and tonic and an annual week’s trip to Las Vegas, they enjoy outings to the local casino, golf, dinners with friends, and frequent visits from three grandchildren.
“I enjoy the variety in my career as a physician and the quality of my life,” he concludes.
The New Hospitalist
Becoming a hospitalist seemed a logical step for Dr. Eddy when he opted to leave full-time office practice in 1999. Brantford General Hospital, where he had admitting privileges, covered a catchment area of 80,000 people.
When the only two other hospitals in the area were closed, Brantford General was overwhelmed. Adding to the systemic distress, 80% of community doctors had given up their hospital privileges. Hospitalists were urgently needed to pick up the slack. Dr. Eddy went for it.
In Canada, hospital throughput isn’t a priority. The system lacks enough sub-acute and rehab beds to discharge patients from hospitals in a timely fashion, leaving patients hospitalized longer compared with similar care in the United States. The average length of stay for heart failure is 6.1 days in the U.S. versus 8.5 days in Canada; for aortic aneurysm repair it’s seven days (U.S.) versus nine days (Canada), according to the Journal of Cardiology.
Those bottlenecks lead to hospitalized patients ready for a less acute level of care occupying beds needed for acute patients. For example, patients wait months for knee replacement surgery, then spend three to four weeks on the rehab ward in the hospital. A step-down facility would probably be ideal but doesn’t exist. “There are people lying in the ER overnight, people who need to be in palliative care units who are in acute care beds,” Dr. Eddy notes. “It is very tough.”
As a family physician, Dr. Eddy favored a hospitalist career because he would have the time to do a general assessment—a whole-patient, complete check-up. He doesn’t admit patients or work in the ED (“Not my forte; I’m not looking for more stress,” he says), but works on the general medical units.
According to Dr. Legere, the septuagenarian physician works approximately 75% of full-time hospitalist hours. He puts in at least 40 weeks a year and covers at least 10 weekends for the hospitalist service.
Hospitalist Larry Kramer, MD, who has worked side by side with Dr. Eddy since 2002, calls him a compassionate, sensitive physician attuned to the small kindnesses patients and family appreciate, such as remembering everyone’s name.
“He’s an excellent team member, always open to referrals and consultations,” says Dr. Kramer, who’s also impressed with Dr. Eddy’s interest in mastering a Palm Pilot when he discovered how much easier and faster it was to access clinical and pharmaceutical information. “He didn’t grow up with computers, but he sure learned how to use his Palm,” adds Dr. Kramer.
The Office Practice
When he started his hospitalist career, Dr. Eddy fully intended to relinquish the office practice to another family physician. It didn’t happen that way—there were about 200 patients he couldn’t give up.
“They are elderly, and I make house calls if it’s too much of a burden for them to come to the office,” he says. “I also see them in nursing homes or retirement homes.” He also covers the office practice for the month of August so his practice partner can have the month off.
His wife, who fields home office phone calls, attends to the issues of 200 special patients and also tries to guide those looking for a primary care doctor to someone else willing to take them.
“My wife works very hard at managing my private practice,” says Dr. Eddy. “She’s a people person but is not soft-minded at all. She helps a lot of patients find primary care physicians who will take them on as well as fielding calls from my private patients.”
The Ontario Health Insurance Plan (OHIP) pays him on a fee-for-service basis. In 2000, when bureaucrats tried to avoid reimbursing him for making house calls by stipulating that at least 50% had to be for palliative care, he made a list of all 200 patients. He made his case for palliative care—“they’ll all die within four years.” The medical establishment accepted it, and he continues making house calls—for which he says the health authorities are relaxing the regulations.
As if the hospitalist and office practice weren’t enough, Dr. Eddy runs a small group practice CME program sponsored by McMaster University and the College of Family Physicians of Canada. “Six of us family physicians get together to discuss three cases based on handouts and a fact section” he says. The CME group meets twice a month for eight months of the year.
In short, Dr. Eddy describes himself as having energy to burn. His hospitalist colleague Dr. Kramer seconds that.
“The amount of work he does is phenomenal,” Dr. Kramer says. “He is very thorough, and it’s remarkable to see how much he still loves practicing medicine. It’s hard to believe that when he’s finished with his hospitalist job he heads off to his office practice, house calls, and nursing home work.”
And what does Dr. Eddy think of his colleagues?
“They seem quite young,” he says of Brantford’s cadre of six full-time and six part-time hospitalists. “But come to think of it most are in their 40s, and some in their 50s and 60s. Maybe they aren’t so young.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
A t 77, Robert Eddy, MD, is a busy fellow. As a hospitalist at the 278-bed Brantford General Hospital in Brantford, Ontario, Canada, he works an average of 70 hours a week.
What keeps him going?
“After a long day at work I really look forward to my gin and tonic,” he says. “I have a picture of it in my mind when I’m driving home.”
On a more serious note, Dr. Eddy attributes his career longevity to good health, good genes, never smoking, and not overdoing the booze.
“I’m very lucky,” he says. “As a doctor you can keep going as long as you don’t have major health problems. My dad died in his 90s, so longevity runs in my family.”
Dr. Eddy rises early to do paperwork at his home office, then drives 20 minutes to the hospital and performs his hospitalist duties five mornings a week, Monday through Friday. On an average day he sees 12 inpatients, completes his charts, then grabs a quick lunch before heading out to see patients in a shared office practice in Burford, about nine miles away.
Scheduling around his hospitalist work and the office practice, he also makes house calls and nursing home visits to his sickest and frailest patients. He covers for his community-based colleagues and hospitalists, and twice a month organizes CME meetings for family physicians. From March to July he adds a temporary assignment at St. Joseph’s Villa in Dundas, tending to 70 patients at that retirement community.
Janice Legere, MD, medical director of the hospitalist program of Brantford General Hospital, calls him “a country guy with a very dry sense of humor. The other hospitalists look up to him because he is the real deal as a doctor.”
Not bad for a gentleman born in the same year and month as the beginning of the Great Depression—October 1929. In his sixth decade of medicine, Dr. Eddy may be the oldest practicing hospitalist.
—Sandra Eddy, wife of Robert Eddy, MD, hospitalist at Brantford General Hospital in Ontario, Canada
No Sign of Slowing
Although he has practiced medicine for more than 52 years, retirement is not on his agenda.
“I closed my solo practice in 1999 because I didn’t want to work so hard, but I’m busier than ever now,” he says.
While Dr. Eddy and his second wife, Sandra, seriously discuss the possibility of his retirement every year, they have reupped for the hospitalist work, office practice, and house/nursing home visits at least through 2008. As they describe it, the overburdened Canadian healthcare system needs every qualified pair of physician hands it can get.
Ontario’s healthcare system can ill afford to lose someone of Dr. Eddy’s commitment, knowledge, and experience.
“I love medicine and am very lucky to have the energy and the stamina to keep going,” Dr. Eddy says. “I enjoy seeing hospitalized patients because I have as much time as I need to do a general assessment of their medical condition. I get my mind around the whole patient.”
His wife affirms Dr. Eddy’s commitment.
“We have been together for 28 years, and we have a good marriage,” she says. ‘‘But he is on call 24/7, and medicine always comes first. Then there’s us.”
But Dr. Eddy’s not just a nose-to-the-grindstone type of guy—he and Sandra do relax together. Along with his nightly after-work gin and tonic and an annual week’s trip to Las Vegas, they enjoy outings to the local casino, golf, dinners with friends, and frequent visits from three grandchildren.
“I enjoy the variety in my career as a physician and the quality of my life,” he concludes.
The New Hospitalist
Becoming a hospitalist seemed a logical step for Dr. Eddy when he opted to leave full-time office practice in 1999. Brantford General Hospital, where he had admitting privileges, covered a catchment area of 80,000 people.
When the only two other hospitals in the area were closed, Brantford General was overwhelmed. Adding to the systemic distress, 80% of community doctors had given up their hospital privileges. Hospitalists were urgently needed to pick up the slack. Dr. Eddy went for it.
In Canada, hospital throughput isn’t a priority. The system lacks enough sub-acute and rehab beds to discharge patients from hospitals in a timely fashion, leaving patients hospitalized longer compared with similar care in the United States. The average length of stay for heart failure is 6.1 days in the U.S. versus 8.5 days in Canada; for aortic aneurysm repair it’s seven days (U.S.) versus nine days (Canada), according to the Journal of Cardiology.
Those bottlenecks lead to hospitalized patients ready for a less acute level of care occupying beds needed for acute patients. For example, patients wait months for knee replacement surgery, then spend three to four weeks on the rehab ward in the hospital. A step-down facility would probably be ideal but doesn’t exist. “There are people lying in the ER overnight, people who need to be in palliative care units who are in acute care beds,” Dr. Eddy notes. “It is very tough.”
As a family physician, Dr. Eddy favored a hospitalist career because he would have the time to do a general assessment—a whole-patient, complete check-up. He doesn’t admit patients or work in the ED (“Not my forte; I’m not looking for more stress,” he says), but works on the general medical units.
According to Dr. Legere, the septuagenarian physician works approximately 75% of full-time hospitalist hours. He puts in at least 40 weeks a year and covers at least 10 weekends for the hospitalist service.
Hospitalist Larry Kramer, MD, who has worked side by side with Dr. Eddy since 2002, calls him a compassionate, sensitive physician attuned to the small kindnesses patients and family appreciate, such as remembering everyone’s name.
“He’s an excellent team member, always open to referrals and consultations,” says Dr. Kramer, who’s also impressed with Dr. Eddy’s interest in mastering a Palm Pilot when he discovered how much easier and faster it was to access clinical and pharmaceutical information. “He didn’t grow up with computers, but he sure learned how to use his Palm,” adds Dr. Kramer.
The Office Practice
When he started his hospitalist career, Dr. Eddy fully intended to relinquish the office practice to another family physician. It didn’t happen that way—there were about 200 patients he couldn’t give up.
“They are elderly, and I make house calls if it’s too much of a burden for them to come to the office,” he says. “I also see them in nursing homes or retirement homes.” He also covers the office practice for the month of August so his practice partner can have the month off.
His wife, who fields home office phone calls, attends to the issues of 200 special patients and also tries to guide those looking for a primary care doctor to someone else willing to take them.
“My wife works very hard at managing my private practice,” says Dr. Eddy. “She’s a people person but is not soft-minded at all. She helps a lot of patients find primary care physicians who will take them on as well as fielding calls from my private patients.”
The Ontario Health Insurance Plan (OHIP) pays him on a fee-for-service basis. In 2000, when bureaucrats tried to avoid reimbursing him for making house calls by stipulating that at least 50% had to be for palliative care, he made a list of all 200 patients. He made his case for palliative care—“they’ll all die within four years.” The medical establishment accepted it, and he continues making house calls—for which he says the health authorities are relaxing the regulations.
As if the hospitalist and office practice weren’t enough, Dr. Eddy runs a small group practice CME program sponsored by McMaster University and the College of Family Physicians of Canada. “Six of us family physicians get together to discuss three cases based on handouts and a fact section” he says. The CME group meets twice a month for eight months of the year.
In short, Dr. Eddy describes himself as having energy to burn. His hospitalist colleague Dr. Kramer seconds that.
“The amount of work he does is phenomenal,” Dr. Kramer says. “He is very thorough, and it’s remarkable to see how much he still loves practicing medicine. It’s hard to believe that when he’s finished with his hospitalist job he heads off to his office practice, house calls, and nursing home work.”
And what does Dr. Eddy think of his colleagues?
“They seem quite young,” he says of Brantford’s cadre of six full-time and six part-time hospitalists. “But come to think of it most are in their 40s, and some in their 50s and 60s. Maybe they aren’t so young.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
Hospitalists on Top
Many technically skilled professionals—including computer programmers, stockbrokers, or hospitalists—aspire to the executive suite.
The burgeoning field of hospital medicine offers especially enticing rewards for business-minded doctors, inducing frontline leaders to trade the white coat for wing tips and a shot at the top.
The pinnacle can be stratospheric. Adam Singer, MD, CEO of California-based IPC-The Hospitalist Company, traded his white coat for the so-called C suite. He has since filed an initial public offering that should produce $105 million for IPC’s stakeholders.
There’s also lots of room for hospitalists with more modest executive aspirations. The skills acquired by good hospitalists—thoroughness, the ability to solve complex problems, critical thinking, strong motivation, sound work ethic, and teamwork—serve physician executives well. Some physicians back into the executive suite once they realize they’re attracted to the business end of medicine. Those are the clinicians who volunteer to do the group’s scheduling or find that they enjoy negotiating contracts with new hires and payers. Others pursue a personal road map to the C suite.
Balancing Act
The biggest decision facing a hospitalist with managerial aspirations is whether to relinquish patient care.
“For most of your career you must remain active clinically, even though your time is disjointed because you’re intensely needed in both clinical and administrative areas,” says Andrew Urbach, MD, medical director of clinical excellence and service at Children’s Hospital of Pittsburgh. He manages both by constantly adapting. His time had been evenly split between clinical and administrative duties until July, when he cut back on his clinical duties. He now spends one week every quarter as a hospitalist and a half-day a week at the clinic. “It’s difficult balancing both, and reaching the highest level of excellence in two areas is demanding,” he says. “But the best hospitalist managers continue to see patients to maintain credibility with their peers.”
Stacy Goldsholl, MD, president of Knoxville, Tenn.-based Team Health, Hospital Medicine Division, was a staff hospitalist who ceded clinical work for a managerial career. After a three-year stint as a hospitalist with Covenant HealthCare’s hospital medicine program at Covenant Medical Center in Saginaw, Mich., her mentors recruited her to “jump around the country starting hospitalist programs during 2004 and 2005,” she says. “I was in the right place at the right time, and I had the confidence to move my agenda in a diplomatic way and with humor.”
Dr. Goldsholl reluctantly gave up clinical responsibilities three years ago. “It’s all about balance in my life,” she says. “It was a conscious decision to give up patient care. I miss it, but I wanted to take my career to a national level. I travel a great deal, which isn’t compatible with patient care.”
Business School
Hospitalists attracted to management often realize they need more business schooling, says Kevin Shulman, MD, MBA, professor of medicine and management at Duke University Medical Center and the Fuqua School of Business in Durham, N.C.
“The issues in medical training are clinical, not organizational,” he says. “As you move up in administration you don’t have business skills you need. When doctors feel frustrated about not being effective organizationally, that’s when they think about business school.”
Edward Ogata, MD, MBA, chief medical officer of Children’s Memorial Hospital in Chicago, and a pediatric neonatologist, realized how useful an MBA would be as he moved from clinical work to management. “I went back to school for an MBA at Northwestern University Kellogg School of Management 27 years after graduating from medical school,” he says. Pushed by the healthcare market into negotiating managed-care contracts in the 1980s, Dr. Ogata realized he knew little about accounting and finance. The always-precarious financial situations of children’s hospitals encouraged him to get the business skills to cope.
At Kellogg, in Chicago, Dr. Ogata was assigned homework and teamwork with executives from Motorola, Lucent, and GE. The first year was difficult because he was still covering call and juggling administrative tasks. He got up at 4 a.m. every day to study. Armed with business skills, Dr. Ogata feels better equipped to meet the financial and administrative needs of his inner-city hospital. “We’re not in a nice suburb with a favorable payer mix, and a hospital isn’t really a business in the conventional sense,’’ he notes. “But we are committed to doing the best.”
For Joy Drass, MD, MBA, a critical care trauma surgeon for 13 years and president of Georgetown University Hospital in Washington, D.C., methodically performing clinical tasks prepared her for top management. She assumed the presidency of the troubled hospital in 2001, one year after MedStar Health in Columbia, Md., acquired it. The hospital had recorded losses in excess of $200 million before MedStar stepped in.
“Many skills I developed as a critical care physician had an absolute application in this stressed organization,” she says. “In medicine, it’s called triage. In business, it’s prioritizing. You look at a situation and quickly set goals to get from point A to point B, encourage team work, and develop structures to support people when they are struggling through uncertainty.” Skills she learned as a graduate of the Wharton business school in Philadelphia helped her stabilize hospital operations, improve customer service and revenue collection, and develop a long-term strategic plan to improve the hospital’s chances of survival.

Varied Paths
Some hospitalists acquire business smarts from instinct and experience. When he was 13 years old, Dr. Urbach ran his family’s retail business for weeks at a time when his parents were away.
“I’ve had no formal [business] school training, but my entrepreneurial instincts and management skills were honed early in life,” he says.
Team Health’s Dr. Goldsholl intended to get a formal MBA, but was too busy. “SHM’s Leadership Academy and other programs gave me management skills, and I chose CME credits in business and management areas,” she says. “I’m also more of an experiential than a classroom learner. Mentoring and other informal settings work for me.”
Michael Ruhlen, MD, MHM, Toledo (Ohio) Children’s Hospital corporate vice president of medical informatics and vice president of medical affairs, made a successful if not easy move from clinician to manager. Acting as a hospitalist seven years before the discipline was named in 1996, he developed systematic, data-driven clinical pathways and trained other would-be pediatric hospitalists in acute care pediatrics. In 2001 he was the first recipient of the National Association of Inpatient Physician’s Award for Outstanding Service in Hospital Medicine. The award recognized his managerial skill in building a hospitalist program from scratch.
Unlike hospitalists who are moving from well-defined clinical tracks to managerial roles, Dr. Ruhlen operated in uncharted territory in his first decade as a hospitalist. From the beginning of his hospitalist career, Dr. Ruhlen’s business head identified volume-dependent competency as critical to clinical and financial success. “I saw how to create time and quality efficiencies,” he explains. “If you do one or two lumbar punctures a year, you might stick a child five or six times. Doing a higher volume of procedures led to smoother operations.”
Recognizing the complexities of hospital management, Dr. Ruhlen returned to school to sharpen his management skills. He chose the Harvard School of Public Health’s master’s in healthcare management over an MBA because, as he puts it, “I’m interested in managing a hospital, not running Campbell’s Soup.” As a hospitalist executive, he works on improving the hospital’s IT systems, developing new physician leaders, and taking the lead on change management and patient safety issues. He also has been tapped twice to serve as acting hospital president.
Medicine as Business
Hospitalists enjoy an array of career choices. Those who savor the pure joy of clinical work can continue on that path, while others can choose a career in management; some can blend both. No matter what their career paths, healthcare’s increasing complexity will keep them fully occupied.
“As medicine grows more complex, students spend their time mastering clinical issues,” Dr. Shulman notes. “Many third-year med students don’t even know the difference between Medicaid and Medicare. As they practice as hospitalists and want to move up the administrative ranks, they will acquire the general business skills that will help them be effective and reshape healthcare policy.” TH
Marlene Piturro is a medical writer based in New York.
Many technically skilled professionals—including computer programmers, stockbrokers, or hospitalists—aspire to the executive suite.
The burgeoning field of hospital medicine offers especially enticing rewards for business-minded doctors, inducing frontline leaders to trade the white coat for wing tips and a shot at the top.
The pinnacle can be stratospheric. Adam Singer, MD, CEO of California-based IPC-The Hospitalist Company, traded his white coat for the so-called C suite. He has since filed an initial public offering that should produce $105 million for IPC’s stakeholders.
There’s also lots of room for hospitalists with more modest executive aspirations. The skills acquired by good hospitalists—thoroughness, the ability to solve complex problems, critical thinking, strong motivation, sound work ethic, and teamwork—serve physician executives well. Some physicians back into the executive suite once they realize they’re attracted to the business end of medicine. Those are the clinicians who volunteer to do the group’s scheduling or find that they enjoy negotiating contracts with new hires and payers. Others pursue a personal road map to the C suite.
Balancing Act
The biggest decision facing a hospitalist with managerial aspirations is whether to relinquish patient care.
“For most of your career you must remain active clinically, even though your time is disjointed because you’re intensely needed in both clinical and administrative areas,” says Andrew Urbach, MD, medical director of clinical excellence and service at Children’s Hospital of Pittsburgh. He manages both by constantly adapting. His time had been evenly split between clinical and administrative duties until July, when he cut back on his clinical duties. He now spends one week every quarter as a hospitalist and a half-day a week at the clinic. “It’s difficult balancing both, and reaching the highest level of excellence in two areas is demanding,” he says. “But the best hospitalist managers continue to see patients to maintain credibility with their peers.”
Stacy Goldsholl, MD, president of Knoxville, Tenn.-based Team Health, Hospital Medicine Division, was a staff hospitalist who ceded clinical work for a managerial career. After a three-year stint as a hospitalist with Covenant HealthCare’s hospital medicine program at Covenant Medical Center in Saginaw, Mich., her mentors recruited her to “jump around the country starting hospitalist programs during 2004 and 2005,” she says. “I was in the right place at the right time, and I had the confidence to move my agenda in a diplomatic way and with humor.”
Dr. Goldsholl reluctantly gave up clinical responsibilities three years ago. “It’s all about balance in my life,” she says. “It was a conscious decision to give up patient care. I miss it, but I wanted to take my career to a national level. I travel a great deal, which isn’t compatible with patient care.”
Business School
Hospitalists attracted to management often realize they need more business schooling, says Kevin Shulman, MD, MBA, professor of medicine and management at Duke University Medical Center and the Fuqua School of Business in Durham, N.C.
“The issues in medical training are clinical, not organizational,” he says. “As you move up in administration you don’t have business skills you need. When doctors feel frustrated about not being effective organizationally, that’s when they think about business school.”
Edward Ogata, MD, MBA, chief medical officer of Children’s Memorial Hospital in Chicago, and a pediatric neonatologist, realized how useful an MBA would be as he moved from clinical work to management. “I went back to school for an MBA at Northwestern University Kellogg School of Management 27 years after graduating from medical school,” he says. Pushed by the healthcare market into negotiating managed-care contracts in the 1980s, Dr. Ogata realized he knew little about accounting and finance. The always-precarious financial situations of children’s hospitals encouraged him to get the business skills to cope.
At Kellogg, in Chicago, Dr. Ogata was assigned homework and teamwork with executives from Motorola, Lucent, and GE. The first year was difficult because he was still covering call and juggling administrative tasks. He got up at 4 a.m. every day to study. Armed with business skills, Dr. Ogata feels better equipped to meet the financial and administrative needs of his inner-city hospital. “We’re not in a nice suburb with a favorable payer mix, and a hospital isn’t really a business in the conventional sense,’’ he notes. “But we are committed to doing the best.”
For Joy Drass, MD, MBA, a critical care trauma surgeon for 13 years and president of Georgetown University Hospital in Washington, D.C., methodically performing clinical tasks prepared her for top management. She assumed the presidency of the troubled hospital in 2001, one year after MedStar Health in Columbia, Md., acquired it. The hospital had recorded losses in excess of $200 million before MedStar stepped in.
“Many skills I developed as a critical care physician had an absolute application in this stressed organization,” she says. “In medicine, it’s called triage. In business, it’s prioritizing. You look at a situation and quickly set goals to get from point A to point B, encourage team work, and develop structures to support people when they are struggling through uncertainty.” Skills she learned as a graduate of the Wharton business school in Philadelphia helped her stabilize hospital operations, improve customer service and revenue collection, and develop a long-term strategic plan to improve the hospital’s chances of survival.
Varied Paths
Some hospitalists acquire business smarts from instinct and experience. When he was 13 years old, Dr. Urbach ran his family’s retail business for weeks at a time when his parents were away.
“I’ve had no formal [business] school training, but my entrepreneurial instincts and management skills were honed early in life,” he says.
Team Health’s Dr. Goldsholl intended to get a formal MBA, but was too busy. “SHM’s Leadership Academy and other programs gave me management skills, and I chose CME credits in business and management areas,” she says. “I’m also more of an experiential than a classroom learner. Mentoring and other informal settings work for me.”
Michael Ruhlen, MD, MHM, Toledo (Ohio) Children’s Hospital corporate vice president of medical informatics and vice president of medical affairs, made a successful if not easy move from clinician to manager. Acting as a hospitalist seven years before the discipline was named in 1996, he developed systematic, data-driven clinical pathways and trained other would-be pediatric hospitalists in acute care pediatrics. In 2001 he was the first recipient of the National Association of Inpatient Physician’s Award for Outstanding Service in Hospital Medicine. The award recognized his managerial skill in building a hospitalist program from scratch.
Unlike hospitalists who are moving from well-defined clinical tracks to managerial roles, Dr. Ruhlen operated in uncharted territory in his first decade as a hospitalist. From the beginning of his hospitalist career, Dr. Ruhlen’s business head identified volume-dependent competency as critical to clinical and financial success. “I saw how to create time and quality efficiencies,” he explains. “If you do one or two lumbar punctures a year, you might stick a child five or six times. Doing a higher volume of procedures led to smoother operations.”
Recognizing the complexities of hospital management, Dr. Ruhlen returned to school to sharpen his management skills. He chose the Harvard School of Public Health’s master’s in healthcare management over an MBA because, as he puts it, “I’m interested in managing a hospital, not running Campbell’s Soup.” As a hospitalist executive, he works on improving the hospital’s IT systems, developing new physician leaders, and taking the lead on change management and patient safety issues. He also has been tapped twice to serve as acting hospital president.
Medicine as Business
Hospitalists enjoy an array of career choices. Those who savor the pure joy of clinical work can continue on that path, while others can choose a career in management; some can blend both. No matter what their career paths, healthcare’s increasing complexity will keep them fully occupied.
“As medicine grows more complex, students spend their time mastering clinical issues,” Dr. Shulman notes. “Many third-year med students don’t even know the difference between Medicaid and Medicare. As they practice as hospitalists and want to move up the administrative ranks, they will acquire the general business skills that will help them be effective and reshape healthcare policy.” TH
Marlene Piturro is a medical writer based in New York.
Many technically skilled professionals—including computer programmers, stockbrokers, or hospitalists—aspire to the executive suite.
The burgeoning field of hospital medicine offers especially enticing rewards for business-minded doctors, inducing frontline leaders to trade the white coat for wing tips and a shot at the top.
The pinnacle can be stratospheric. Adam Singer, MD, CEO of California-based IPC-The Hospitalist Company, traded his white coat for the so-called C suite. He has since filed an initial public offering that should produce $105 million for IPC’s stakeholders.
There’s also lots of room for hospitalists with more modest executive aspirations. The skills acquired by good hospitalists—thoroughness, the ability to solve complex problems, critical thinking, strong motivation, sound work ethic, and teamwork—serve physician executives well. Some physicians back into the executive suite once they realize they’re attracted to the business end of medicine. Those are the clinicians who volunteer to do the group’s scheduling or find that they enjoy negotiating contracts with new hires and payers. Others pursue a personal road map to the C suite.
Balancing Act
The biggest decision facing a hospitalist with managerial aspirations is whether to relinquish patient care.
“For most of your career you must remain active clinically, even though your time is disjointed because you’re intensely needed in both clinical and administrative areas,” says Andrew Urbach, MD, medical director of clinical excellence and service at Children’s Hospital of Pittsburgh. He manages both by constantly adapting. His time had been evenly split between clinical and administrative duties until July, when he cut back on his clinical duties. He now spends one week every quarter as a hospitalist and a half-day a week at the clinic. “It’s difficult balancing both, and reaching the highest level of excellence in two areas is demanding,” he says. “But the best hospitalist managers continue to see patients to maintain credibility with their peers.”
Stacy Goldsholl, MD, president of Knoxville, Tenn.-based Team Health, Hospital Medicine Division, was a staff hospitalist who ceded clinical work for a managerial career. After a three-year stint as a hospitalist with Covenant HealthCare’s hospital medicine program at Covenant Medical Center in Saginaw, Mich., her mentors recruited her to “jump around the country starting hospitalist programs during 2004 and 2005,” she says. “I was in the right place at the right time, and I had the confidence to move my agenda in a diplomatic way and with humor.”
Dr. Goldsholl reluctantly gave up clinical responsibilities three years ago. “It’s all about balance in my life,” she says. “It was a conscious decision to give up patient care. I miss it, but I wanted to take my career to a national level. I travel a great deal, which isn’t compatible with patient care.”
Business School
Hospitalists attracted to management often realize they need more business schooling, says Kevin Shulman, MD, MBA, professor of medicine and management at Duke University Medical Center and the Fuqua School of Business in Durham, N.C.
“The issues in medical training are clinical, not organizational,” he says. “As you move up in administration you don’t have business skills you need. When doctors feel frustrated about not being effective organizationally, that’s when they think about business school.”
Edward Ogata, MD, MBA, chief medical officer of Children’s Memorial Hospital in Chicago, and a pediatric neonatologist, realized how useful an MBA would be as he moved from clinical work to management. “I went back to school for an MBA at Northwestern University Kellogg School of Management 27 years after graduating from medical school,” he says. Pushed by the healthcare market into negotiating managed-care contracts in the 1980s, Dr. Ogata realized he knew little about accounting and finance. The always-precarious financial situations of children’s hospitals encouraged him to get the business skills to cope.
At Kellogg, in Chicago, Dr. Ogata was assigned homework and teamwork with executives from Motorola, Lucent, and GE. The first year was difficult because he was still covering call and juggling administrative tasks. He got up at 4 a.m. every day to study. Armed with business skills, Dr. Ogata feels better equipped to meet the financial and administrative needs of his inner-city hospital. “We’re not in a nice suburb with a favorable payer mix, and a hospital isn’t really a business in the conventional sense,’’ he notes. “But we are committed to doing the best.”
For Joy Drass, MD, MBA, a critical care trauma surgeon for 13 years and president of Georgetown University Hospital in Washington, D.C., methodically performing clinical tasks prepared her for top management. She assumed the presidency of the troubled hospital in 2001, one year after MedStar Health in Columbia, Md., acquired it. The hospital had recorded losses in excess of $200 million before MedStar stepped in.
“Many skills I developed as a critical care physician had an absolute application in this stressed organization,” she says. “In medicine, it’s called triage. In business, it’s prioritizing. You look at a situation and quickly set goals to get from point A to point B, encourage team work, and develop structures to support people when they are struggling through uncertainty.” Skills she learned as a graduate of the Wharton business school in Philadelphia helped her stabilize hospital operations, improve customer service and revenue collection, and develop a long-term strategic plan to improve the hospital’s chances of survival.
Varied Paths
Some hospitalists acquire business smarts from instinct and experience. When he was 13 years old, Dr. Urbach ran his family’s retail business for weeks at a time when his parents were away.
“I’ve had no formal [business] school training, but my entrepreneurial instincts and management skills were honed early in life,” he says.
Team Health’s Dr. Goldsholl intended to get a formal MBA, but was too busy. “SHM’s Leadership Academy and other programs gave me management skills, and I chose CME credits in business and management areas,” she says. “I’m also more of an experiential than a classroom learner. Mentoring and other informal settings work for me.”
Michael Ruhlen, MD, MHM, Toledo (Ohio) Children’s Hospital corporate vice president of medical informatics and vice president of medical affairs, made a successful if not easy move from clinician to manager. Acting as a hospitalist seven years before the discipline was named in 1996, he developed systematic, data-driven clinical pathways and trained other would-be pediatric hospitalists in acute care pediatrics. In 2001 he was the first recipient of the National Association of Inpatient Physician’s Award for Outstanding Service in Hospital Medicine. The award recognized his managerial skill in building a hospitalist program from scratch.
Unlike hospitalists who are moving from well-defined clinical tracks to managerial roles, Dr. Ruhlen operated in uncharted territory in his first decade as a hospitalist. From the beginning of his hospitalist career, Dr. Ruhlen’s business head identified volume-dependent competency as critical to clinical and financial success. “I saw how to create time and quality efficiencies,” he explains. “If you do one or two lumbar punctures a year, you might stick a child five or six times. Doing a higher volume of procedures led to smoother operations.”
Recognizing the complexities of hospital management, Dr. Ruhlen returned to school to sharpen his management skills. He chose the Harvard School of Public Health’s master’s in healthcare management over an MBA because, as he puts it, “I’m interested in managing a hospital, not running Campbell’s Soup.” As a hospitalist executive, he works on improving the hospital’s IT systems, developing new physician leaders, and taking the lead on change management and patient safety issues. He also has been tapped twice to serve as acting hospital president.
Medicine as Business
Hospitalists enjoy an array of career choices. Those who savor the pure joy of clinical work can continue on that path, while others can choose a career in management; some can blend both. No matter what their career paths, healthcare’s increasing complexity will keep them fully occupied.
“As medicine grows more complex, students spend their time mastering clinical issues,” Dr. Shulman notes. “Many third-year med students don’t even know the difference between Medicaid and Medicare. As they practice as hospitalists and want to move up the administrative ranks, they will acquire the general business skills that will help them be effective and reshape healthcare policy.” TH
Marlene Piturro is a medical writer based in New York.
Ahead of the Curve
Twenty years before the term “hospitalist” was coined, and not long after serving as a battlefield surgeon in Vietnam, Tracy Spencer III, MD, selected a path few—if any—had chosen before.
Fresh from his combat experience, he became chief resident at the University of Colorado School of Medicine in Denver in 1975. He dreaded clinic hours but enjoyed the hospital. The flash, dash, and adrenaline of battlefield medicine were still in his blood; he wanted challenges.
“I didn’t want an outpatient practice with the overhead of an office,” says Dr. Spencer, 63, “I wanted to do internal medicine in a hospital setting. I had tons of energy to deal with the unassigned patients who came in the ER, and [I liked] the idea of being a hospital-based physician.”
He began searching for the right setting for his skills and temperament. Eventually, the third-generation physician made a bold leap—he started a hospital-based internal medicine practice in Everett, Wash.
Grass-roots Campaign
In 1976, Dr. Spencer knocked on lots of doors and convinced scores of Everett’s primary care physicians that his caring for their hospitalized patients would free them to build their practices. Although many of those physicians thought it bizarre that Dr. Spencer had no outpatients, they readily turned over their inpatients to him.
“I believe he was one of the first, if not the first, hospitalist in the state of Washington, and perhaps the country,” says John Cramer, MD, MBA, an intern at the University of Colorado 1974-1975 when Dr. Spencer was chief resident. Their relationship has endured more than three decades—with a twist. Now the former intern, who joined Dr. Spencer as a hospitalist in 1979, supervises his former boss in the growing 32-physician hospitalist group at Providence Everett Medical Center.
“Tracy is a member of the team, dispensing wisdom to the younger docs,” says Dr. Cramer. “I have never seen him happier professionally than he is now.”
Early Influence
Dr. Spencer’s medical training and early experiences shed light on how he came to be an inpatient physician two decades before hospitalist medicine formally emerged.
Theodore Woodward, MD, nominated for a Nobel Prize in 1948 for his work on typhus and typhoid, was Dr. Spencer’s professor at the University of Maryland, Baltimore. He impressed Dr. Woodward with “an old-fashioned, knowledge-based, and holistic approach to patients.”
Later, Thomas Petty, MD, an eminent pulmonologist who headed a respiratory team at the University of Colorado Medical Center and became chairman of the National Lung Educational Program, introduced the young physician to a team-based approach to hospital care. During his 1968-1969 internship at the University of Colorado under Dr. Petty, Dr. Spencer found he enjoyed working on a hospital team and the discipline of the hospital hierarchy.
After graduating from medical school, Dr. Spencer was drafted in 1970 by the Marines and was sent to Dà Nang, Vietnam. As a regimental doctor, he worked alone—and didn’t like it. “There was no collegiality for field combat docs,” he recalls. “There were ship-based specialists who didn’t even talk to us. The most serious cases we triaged were [taken] to the ship, and I didn’t see them again. I was dissatisfied and felt that the doctors in the field deserved more respect.”
Maurice Ramirez, DO, an emergency physician and federal medical officer with the Department of Homeland Security, suggests the military’s command structure may have influenced Dr. Spencer more than he realizes. “Before hospitalist medicine, physicians were like British aristocrats in their fiefdoms, ordering their lessers about,” explains Dr. Ramirez. “[The] hospitalist movement has changed all that.”
Turning Point
Dr. Spencer returned from his tour of duty and began his chief resident stint at the University of Colorado in 1975.
That year, Boyd Bigelow, MD, “a maverick with a plane” by Dr. Spencer’s account, hired him to admit and manage patients at Denver’s St. Anthony’s Central Hospital, which had no house staff. “To compete with big hospitals, we’d fly referrals into Stapleton [Air Force Base],” Dr. Spencer says. Dr. Bigelow became medical director of Flight for Life, the first civilian airborne emergency medical service, which has flown more than 65,000 patients to critical care facilities. He would swoop down from the sky through Colorado’s whirling snow, delivering patients to Dr. Spencer.
In 1976 Dr. Spencer took stock of his career and recognized he wanted to be a hospital-based physician. He contacted John Hoidal, MD, from his University of Colorado days, expecting to buddy up, move both of their families to Everett, and cover inpatients at two hospitals 24/7. But Dr. Hoidal chose not to go.
“It would have been easier if the two of us had started the hospitalist practice together, but it wasn’t right for him,” says Dr. Spencer. “I saw that I could do it on my own. I had energy to burn and ambition to succeed.”
Undaunted, he soldiered on to Everett.
“It is an absolutely gorgeous place to live,” he says. “When we arrived I found Everett loaded with GPs in their busy offices, and I had the expertise they needed to manage their inpatients. I hooked them with my three A’s: availability, affability, and ability.”
Everett Hospital hired him to provide 24/7 coverage for respiratory care, the intensive care unit, medical/surgical consults, and overall inpatient management. He worked solo for more than a year and grew exhausted. He hired a second physician in 1977, then Dr. Cramer in 1979.
Also in 1977, Dr. Spencer forged what has become a 30-year professional relationship with Eric Larson, MD, MPH, executive director of the Center for Health Studies Group in Everett.
“In 1977 I was chief resident at Providence General [which merged with Everett Hospital to become Providence Everett Medical Center in 1994],” Dr. Larson says. “Tracy introduced himself as a hospitalist and said he took care of patients in the hospital for GPs. It seemed like an interesting solo practice model.”
What struck Dr. Larson at the time was the contrast between the commotion of a teaching hospital with medical students, interns, residents, and attendings “tripping all over each other” and Dr. Spencer’s approach.
“He embodied the principle of keeping things simple and was organized and methodical in his approach to patients,” Dr. Larson says. “He was superb in pulmonary medicine and the ICU.”
Challenging Times
The hospitalist practice and Everett’s medical community kept growing through the early ’80s, with specialists joining general practitioners in using Dr. Spencer’s group for consults and co-management. Then came managed care in the mid-’80s, and the hospitalists’ gains seemed threatened. “Managed care’s tight controls and preauthorizes of inpatient services were terribly frustrating,” says Dr. Larson. Dr. Spencer found himself competing for managed-care contracts rather than seeing patients.
By the time managed care loosened its grip in the 1990s and the hospitalist movement was officially launched, there were new challenges and frustrations. Dr. Spencer felt worn out administrating rather than doctoring. Dr. Larson felt something else: futility. “One of the hardest things about being a hospitalist is dealing with the futility of treating old people with multiple co-morbidities who shouldn’t even be in a hospital,” explains Dr. Larson. “Hospitals are now so protocolized. Once a patient gets in the hospital he’s almost on automatic.”
Frustrated and tired 25 years after becoming the first hospitalist, Dr. Spencer retired in April 2001. Then he realized he wasn’t finished with medicine. Six months later he joined the hospitalist cadre led by his former intern, Dr. Cramer, at the Everett Clinic, a multispecialty group with 250 physicians and 65 midlevel providers.
Putting 30 years of hospitalist experience to work, Dr. Spencer recruits young hospitalists, teaches best practices, and continues to build relationships with general practitioners and specialists. From his unique vantage point, he sees hospital medicine as a maturing discipline gone mainstream.
“There’s still so much to do,” he says. He plans to explore a variety of hospitalist growth areas, such as efficient use of diagnostic testing, higher intensity medicine with patients of markedly higher acuity, step-down cardiac telemetry, more involvement with ICUs, and managing complex patients living with multiple co-morbidities.
But Dr. Ramirez says that with all he’s already accomplished, Dr. Spencer has earned a place of note: “I hope that hospitalists recognize he was three decades and six generations of physicians ahead of his time.” TH
Marlene Piturro is a medical writer based in New York.
Twenty years before the term “hospitalist” was coined, and not long after serving as a battlefield surgeon in Vietnam, Tracy Spencer III, MD, selected a path few—if any—had chosen before.
Fresh from his combat experience, he became chief resident at the University of Colorado School of Medicine in Denver in 1975. He dreaded clinic hours but enjoyed the hospital. The flash, dash, and adrenaline of battlefield medicine were still in his blood; he wanted challenges.
“I didn’t want an outpatient practice with the overhead of an office,” says Dr. Spencer, 63, “I wanted to do internal medicine in a hospital setting. I had tons of energy to deal with the unassigned patients who came in the ER, and [I liked] the idea of being a hospital-based physician.”
He began searching for the right setting for his skills and temperament. Eventually, the third-generation physician made a bold leap—he started a hospital-based internal medicine practice in Everett, Wash.
Grass-roots Campaign
In 1976, Dr. Spencer knocked on lots of doors and convinced scores of Everett’s primary care physicians that his caring for their hospitalized patients would free them to build their practices. Although many of those physicians thought it bizarre that Dr. Spencer had no outpatients, they readily turned over their inpatients to him.
“I believe he was one of the first, if not the first, hospitalist in the state of Washington, and perhaps the country,” says John Cramer, MD, MBA, an intern at the University of Colorado 1974-1975 when Dr. Spencer was chief resident. Their relationship has endured more than three decades—with a twist. Now the former intern, who joined Dr. Spencer as a hospitalist in 1979, supervises his former boss in the growing 32-physician hospitalist group at Providence Everett Medical Center.
“Tracy is a member of the team, dispensing wisdom to the younger docs,” says Dr. Cramer. “I have never seen him happier professionally than he is now.”
Early Influence
Dr. Spencer’s medical training and early experiences shed light on how he came to be an inpatient physician two decades before hospitalist medicine formally emerged.
Theodore Woodward, MD, nominated for a Nobel Prize in 1948 for his work on typhus and typhoid, was Dr. Spencer’s professor at the University of Maryland, Baltimore. He impressed Dr. Woodward with “an old-fashioned, knowledge-based, and holistic approach to patients.”
Later, Thomas Petty, MD, an eminent pulmonologist who headed a respiratory team at the University of Colorado Medical Center and became chairman of the National Lung Educational Program, introduced the young physician to a team-based approach to hospital care. During his 1968-1969 internship at the University of Colorado under Dr. Petty, Dr. Spencer found he enjoyed working on a hospital team and the discipline of the hospital hierarchy.
After graduating from medical school, Dr. Spencer was drafted in 1970 by the Marines and was sent to Dà Nang, Vietnam. As a regimental doctor, he worked alone—and didn’t like it. “There was no collegiality for field combat docs,” he recalls. “There were ship-based specialists who didn’t even talk to us. The most serious cases we triaged were [taken] to the ship, and I didn’t see them again. I was dissatisfied and felt that the doctors in the field deserved more respect.”
Maurice Ramirez, DO, an emergency physician and federal medical officer with the Department of Homeland Security, suggests the military’s command structure may have influenced Dr. Spencer more than he realizes. “Before hospitalist medicine, physicians were like British aristocrats in their fiefdoms, ordering their lessers about,” explains Dr. Ramirez. “[The] hospitalist movement has changed all that.”
Turning Point
Dr. Spencer returned from his tour of duty and began his chief resident stint at the University of Colorado in 1975.
That year, Boyd Bigelow, MD, “a maverick with a plane” by Dr. Spencer’s account, hired him to admit and manage patients at Denver’s St. Anthony’s Central Hospital, which had no house staff. “To compete with big hospitals, we’d fly referrals into Stapleton [Air Force Base],” Dr. Spencer says. Dr. Bigelow became medical director of Flight for Life, the first civilian airborne emergency medical service, which has flown more than 65,000 patients to critical care facilities. He would swoop down from the sky through Colorado’s whirling snow, delivering patients to Dr. Spencer.
In 1976 Dr. Spencer took stock of his career and recognized he wanted to be a hospital-based physician. He contacted John Hoidal, MD, from his University of Colorado days, expecting to buddy up, move both of their families to Everett, and cover inpatients at two hospitals 24/7. But Dr. Hoidal chose not to go.
“It would have been easier if the two of us had started the hospitalist practice together, but it wasn’t right for him,” says Dr. Spencer. “I saw that I could do it on my own. I had energy to burn and ambition to succeed.”
Undaunted, he soldiered on to Everett.
“It is an absolutely gorgeous place to live,” he says. “When we arrived I found Everett loaded with GPs in their busy offices, and I had the expertise they needed to manage their inpatients. I hooked them with my three A’s: availability, affability, and ability.”
Everett Hospital hired him to provide 24/7 coverage for respiratory care, the intensive care unit, medical/surgical consults, and overall inpatient management. He worked solo for more than a year and grew exhausted. He hired a second physician in 1977, then Dr. Cramer in 1979.
Also in 1977, Dr. Spencer forged what has become a 30-year professional relationship with Eric Larson, MD, MPH, executive director of the Center for Health Studies Group in Everett.
“In 1977 I was chief resident at Providence General [which merged with Everett Hospital to become Providence Everett Medical Center in 1994],” Dr. Larson says. “Tracy introduced himself as a hospitalist and said he took care of patients in the hospital for GPs. It seemed like an interesting solo practice model.”
What struck Dr. Larson at the time was the contrast between the commotion of a teaching hospital with medical students, interns, residents, and attendings “tripping all over each other” and Dr. Spencer’s approach.
“He embodied the principle of keeping things simple and was organized and methodical in his approach to patients,” Dr. Larson says. “He was superb in pulmonary medicine and the ICU.”
Challenging Times
The hospitalist practice and Everett’s medical community kept growing through the early ’80s, with specialists joining general practitioners in using Dr. Spencer’s group for consults and co-management. Then came managed care in the mid-’80s, and the hospitalists’ gains seemed threatened. “Managed care’s tight controls and preauthorizes of inpatient services were terribly frustrating,” says Dr. Larson. Dr. Spencer found himself competing for managed-care contracts rather than seeing patients.
By the time managed care loosened its grip in the 1990s and the hospitalist movement was officially launched, there were new challenges and frustrations. Dr. Spencer felt worn out administrating rather than doctoring. Dr. Larson felt something else: futility. “One of the hardest things about being a hospitalist is dealing with the futility of treating old people with multiple co-morbidities who shouldn’t even be in a hospital,” explains Dr. Larson. “Hospitals are now so protocolized. Once a patient gets in the hospital he’s almost on automatic.”
Frustrated and tired 25 years after becoming the first hospitalist, Dr. Spencer retired in April 2001. Then he realized he wasn’t finished with medicine. Six months later he joined the hospitalist cadre led by his former intern, Dr. Cramer, at the Everett Clinic, a multispecialty group with 250 physicians and 65 midlevel providers.
Putting 30 years of hospitalist experience to work, Dr. Spencer recruits young hospitalists, teaches best practices, and continues to build relationships with general practitioners and specialists. From his unique vantage point, he sees hospital medicine as a maturing discipline gone mainstream.
“There’s still so much to do,” he says. He plans to explore a variety of hospitalist growth areas, such as efficient use of diagnostic testing, higher intensity medicine with patients of markedly higher acuity, step-down cardiac telemetry, more involvement with ICUs, and managing complex patients living with multiple co-morbidities.
But Dr. Ramirez says that with all he’s already accomplished, Dr. Spencer has earned a place of note: “I hope that hospitalists recognize he was three decades and six generations of physicians ahead of his time.” TH
Marlene Piturro is a medical writer based in New York.
Twenty years before the term “hospitalist” was coined, and not long after serving as a battlefield surgeon in Vietnam, Tracy Spencer III, MD, selected a path few—if any—had chosen before.
Fresh from his combat experience, he became chief resident at the University of Colorado School of Medicine in Denver in 1975. He dreaded clinic hours but enjoyed the hospital. The flash, dash, and adrenaline of battlefield medicine were still in his blood; he wanted challenges.
“I didn’t want an outpatient practice with the overhead of an office,” says Dr. Spencer, 63, “I wanted to do internal medicine in a hospital setting. I had tons of energy to deal with the unassigned patients who came in the ER, and [I liked] the idea of being a hospital-based physician.”
He began searching for the right setting for his skills and temperament. Eventually, the third-generation physician made a bold leap—he started a hospital-based internal medicine practice in Everett, Wash.
Grass-roots Campaign
In 1976, Dr. Spencer knocked on lots of doors and convinced scores of Everett’s primary care physicians that his caring for their hospitalized patients would free them to build their practices. Although many of those physicians thought it bizarre that Dr. Spencer had no outpatients, they readily turned over their inpatients to him.
“I believe he was one of the first, if not the first, hospitalist in the state of Washington, and perhaps the country,” says John Cramer, MD, MBA, an intern at the University of Colorado 1974-1975 when Dr. Spencer was chief resident. Their relationship has endured more than three decades—with a twist. Now the former intern, who joined Dr. Spencer as a hospitalist in 1979, supervises his former boss in the growing 32-physician hospitalist group at Providence Everett Medical Center.
“Tracy is a member of the team, dispensing wisdom to the younger docs,” says Dr. Cramer. “I have never seen him happier professionally than he is now.”
Early Influence
Dr. Spencer’s medical training and early experiences shed light on how he came to be an inpatient physician two decades before hospitalist medicine formally emerged.
Theodore Woodward, MD, nominated for a Nobel Prize in 1948 for his work on typhus and typhoid, was Dr. Spencer’s professor at the University of Maryland, Baltimore. He impressed Dr. Woodward with “an old-fashioned, knowledge-based, and holistic approach to patients.”
Later, Thomas Petty, MD, an eminent pulmonologist who headed a respiratory team at the University of Colorado Medical Center and became chairman of the National Lung Educational Program, introduced the young physician to a team-based approach to hospital care. During his 1968-1969 internship at the University of Colorado under Dr. Petty, Dr. Spencer found he enjoyed working on a hospital team and the discipline of the hospital hierarchy.
After graduating from medical school, Dr. Spencer was drafted in 1970 by the Marines and was sent to Dà Nang, Vietnam. As a regimental doctor, he worked alone—and didn’t like it. “There was no collegiality for field combat docs,” he recalls. “There were ship-based specialists who didn’t even talk to us. The most serious cases we triaged were [taken] to the ship, and I didn’t see them again. I was dissatisfied and felt that the doctors in the field deserved more respect.”
Maurice Ramirez, DO, an emergency physician and federal medical officer with the Department of Homeland Security, suggests the military’s command structure may have influenced Dr. Spencer more than he realizes. “Before hospitalist medicine, physicians were like British aristocrats in their fiefdoms, ordering their lessers about,” explains Dr. Ramirez. “[The] hospitalist movement has changed all that.”
Turning Point
Dr. Spencer returned from his tour of duty and began his chief resident stint at the University of Colorado in 1975.
That year, Boyd Bigelow, MD, “a maverick with a plane” by Dr. Spencer’s account, hired him to admit and manage patients at Denver’s St. Anthony’s Central Hospital, which had no house staff. “To compete with big hospitals, we’d fly referrals into Stapleton [Air Force Base],” Dr. Spencer says. Dr. Bigelow became medical director of Flight for Life, the first civilian airborne emergency medical service, which has flown more than 65,000 patients to critical care facilities. He would swoop down from the sky through Colorado’s whirling snow, delivering patients to Dr. Spencer.
In 1976 Dr. Spencer took stock of his career and recognized he wanted to be a hospital-based physician. He contacted John Hoidal, MD, from his University of Colorado days, expecting to buddy up, move both of their families to Everett, and cover inpatients at two hospitals 24/7. But Dr. Hoidal chose not to go.
“It would have been easier if the two of us had started the hospitalist practice together, but it wasn’t right for him,” says Dr. Spencer. “I saw that I could do it on my own. I had energy to burn and ambition to succeed.”
Undaunted, he soldiered on to Everett.
“It is an absolutely gorgeous place to live,” he says. “When we arrived I found Everett loaded with GPs in their busy offices, and I had the expertise they needed to manage their inpatients. I hooked them with my three A’s: availability, affability, and ability.”
Everett Hospital hired him to provide 24/7 coverage for respiratory care, the intensive care unit, medical/surgical consults, and overall inpatient management. He worked solo for more than a year and grew exhausted. He hired a second physician in 1977, then Dr. Cramer in 1979.
Also in 1977, Dr. Spencer forged what has become a 30-year professional relationship with Eric Larson, MD, MPH, executive director of the Center for Health Studies Group in Everett.
“In 1977 I was chief resident at Providence General [which merged with Everett Hospital to become Providence Everett Medical Center in 1994],” Dr. Larson says. “Tracy introduced himself as a hospitalist and said he took care of patients in the hospital for GPs. It seemed like an interesting solo practice model.”
What struck Dr. Larson at the time was the contrast between the commotion of a teaching hospital with medical students, interns, residents, and attendings “tripping all over each other” and Dr. Spencer’s approach.
“He embodied the principle of keeping things simple and was organized and methodical in his approach to patients,” Dr. Larson says. “He was superb in pulmonary medicine and the ICU.”
Challenging Times
The hospitalist practice and Everett’s medical community kept growing through the early ’80s, with specialists joining general practitioners in using Dr. Spencer’s group for consults and co-management. Then came managed care in the mid-’80s, and the hospitalists’ gains seemed threatened. “Managed care’s tight controls and preauthorizes of inpatient services were terribly frustrating,” says Dr. Larson. Dr. Spencer found himself competing for managed-care contracts rather than seeing patients.
By the time managed care loosened its grip in the 1990s and the hospitalist movement was officially launched, there were new challenges and frustrations. Dr. Spencer felt worn out administrating rather than doctoring. Dr. Larson felt something else: futility. “One of the hardest things about being a hospitalist is dealing with the futility of treating old people with multiple co-morbidities who shouldn’t even be in a hospital,” explains Dr. Larson. “Hospitals are now so protocolized. Once a patient gets in the hospital he’s almost on automatic.”
Frustrated and tired 25 years after becoming the first hospitalist, Dr. Spencer retired in April 2001. Then he realized he wasn’t finished with medicine. Six months later he joined the hospitalist cadre led by his former intern, Dr. Cramer, at the Everett Clinic, a multispecialty group with 250 physicians and 65 midlevel providers.
Putting 30 years of hospitalist experience to work, Dr. Spencer recruits young hospitalists, teaches best practices, and continues to build relationships with general practitioners and specialists. From his unique vantage point, he sees hospital medicine as a maturing discipline gone mainstream.
“There’s still so much to do,” he says. He plans to explore a variety of hospitalist growth areas, such as efficient use of diagnostic testing, higher intensity medicine with patients of markedly higher acuity, step-down cardiac telemetry, more involvement with ICUs, and managing complex patients living with multiple co-morbidities.
But Dr. Ramirez says that with all he’s already accomplished, Dr. Spencer has earned a place of note: “I hope that hospitalists recognize he was three decades and six generations of physicians ahead of his time.” TH
Marlene Piturro is a medical writer based in New York.
Care & Prayer
Charles Petit, MD, like many healthcare professionals, spends a good deal of time addressing the needs of the underprivileged. Since 2004, he has taken up the cause of the indigenous Miskito Indians of Puerto Lempira, Honduras. He is putting his own money into developing a modern clinic and international medicine program there.
But medicine isn’t his only mission. Dr. Petit, 56, a hospitalist at Palmetto Health Care’s Richland Memorial Hospital in Columbia, S.C., is also an Episcopal priest.
He joined Palmetto Health Senior Care as its first medical director in 1988 and reconnected with the group in 2004—not in his previous role as an office-based physician but as a hospitalist. In between those stints he pursued his ordination and medical missionary work in Africa and Latin America.
As a physician, Dr. Petit says he feels God’s presence at each patient’s bedside. Years ago he wondered how to handle that.
To deepen his connection between medicine and spirituality, he lived in a Christian intentional community in Indiana, Pa., from 1981 to 1988. Gradually, his views on medicine and spirituality crystallized.
“How does God do what he does?” Dr. Petit wondered. “Can medicine put Him to the test? I have seen that prayer works, including a patient miraculously healed of metastatic ovarian cancer. But God isn’t a vending machine. You don’t drop in a prayer and get a healing back.”
The Second Calling
Recognizing he needed something more to integrate medicine and spirituality, Dr. Petit sought a firmer grounding in religious studies.
He moved to Simpsonville, S.C., in 1995 and entered the Episcopal seminary, working as an emergency department doctor to pay the bills. Later, he earned a master’s of divinity from the University of the South in Sewanee, Tenn., in 2003.
His spiritual “internship” was a transitional deaconship from 2003 to 2005, under the Rev. Michael Flanagan, rector at Simpsonville’s Holy Cross Episcopal Church. Both had dual vocations—Flanagan was an engineer who sold electrical equipment for 10 years before ordination. Prior to meeting Dr. Petit, Flanagan was leery of the doctor’s ability to balance pastoral and medical duties.
“Would he be a doctor/priest?” Flanagan wondered. “A priest/doctor? His desire was to meld both and he did. Medicine and spirituality are both in his blood. He sees both as calls from God and connects medicine with spirituality into a holistic view of each person.” He says Dr. Petit “seems to know everything and sucks up knowledge, which he wants to share. He loves being the doctor and having the knowledge to fix the patient’s problem.”
While Dr. Petit keeps his hospitalist and priest roles mostly separate, working with elderly patients sometimes requires the skills of both disciplines. At Richland he wears a clerical collar on pastoral rounds. If a family or patient asks him to pray with them or discuss life’s ending, he does. He has conducted funerals for his own and colleagues’ patients.
“It’s a very powerful experience being both a priest and a doctor,” he says. “I grow so close to the patients and their families that it is natural for me to serve in both roles.”

Honduras Mission
As a seminarian, Dr. Petit took medical mission trips and briefly supported an African orphanage, looking for a cause to call his own. Until his first trip to Puerto Lempira, a village on the Miskito Coast of the Atlantic Ocean.
The abject poverty and medical needs of the Miskito Indians there pulled at him. Early on he enlisted the help of Ennis Whiddon, a builder and Holy Cross parishioner. Whiddon, who usually accompanies Dr. Petit to Puerto Lempira, says of his friend: “I knew him as [an emergency department] doctor first. Then I realized his extraordinary spiritual commitment. I went to Puerto Lempira on his first mission trip and I asked myself why anyone would want to be there, but I knew Chuck couldn’t bear not to be there. I also knew he wasn’t just going to give people two aspirins, come home and pray for them.”
Dr. Petit returns to Puerto Lempira three or four times a year with a team of doctors, seeing several hundred patients a day. During one two-week stint he dispensed $200,000 worth of medication he cadged from drug companies for $600 out of his pocket to rid the town’s youngsters of debilitating parasites.
Dr. Petit works with a Miskito nurse who runs their rudimentary clinic in his absence. He also uses hyperbaric medicine to treat divers whose crippling injuries result from diving deeply using pressurized oxygen tanks and rising too quickly to the surface.
“You wouldn’t believe the indescribably poor facilities we found there,” Whiddon says of the town’s clinic. “You wouldn’t have your dog treated there if you loved your dog.”
Last year Dr. Petit ratcheted up his commitment to Puerto Lempira, dreaming of building a permanent clinic there.
He decided to use his money to buy land to build a clinic, but got stonewalled by a stubborn local bureaucracy.
Then Andres Leone, a like-minded younger doctor who was part of the mission trip, stepped in with handy language and cultural skills. Leone who had attended medical school in Ecuador, is a Lutheran seminarian, and is completing a geriatric hospitalist fellowship at Palmetto Healthcare.
“We were in Puerto Lempira for two weeks and visited the mayor several times to buy land,” Dr. Leone explains. “He said the price was $600,000, which was ridiculous. In the town I overheard some conversations, which led to us meeting the 77-year-old daughter of missionaries. She sold us some of her land and even donated money to help build the clinic, which will be dedicated in her name.”
Thinking big, Dr. Petit is adding an apartment complete with air conditioning and a modern bathroom to the clinic’s blueprint, to attract residents in a to-be-formed international medicine program. As an assistant professor of family medicine at the University of South Carolina’s (USC) School of Medicine, he intends to oversee those residents.
Just back from Puerto Lempira, Dr. Petit finalized the clinic’s design, lined up local workers to figure out how to make concrete building blocks with native materials, and met with Anglican bishop the Right Rev. Lloyd E. Allen, bolstering support for the new clinic and the possibility of HIV outreach. Side by side with Honduran and Cuban doctors, Dr. Petit treated hundreds of Puerto Lempira’s villagers every day.
Back in the Hospital
Dr. Petit always wanted to be a doctor. Although his father suggested he become a hospital orderly, Dr. Petit knew being a physician was his calling, graduating from the University of West Virginia School of Medicine (Morgantown) family medicine program in 1978.
He enjoys hospital medicine as a holistic approach to caring for patients, consistent with his work early in his career.
An earlier 10-year stint as a hospitalist at HealthSouth Rehabilitation Hospital, also at USC, involved teaching residents and students rotating through the hospital, as well as a consultative service for neurosurgical patients at Richland. At Wheeling Hospital early in his career he became comfortable as a generalist, covering intensive care, assisting in surgery, and delivering many babies.
Being a hospitalist keeps that spirit alive. “It gives me the gift of time to spend with patients,” he says. “I try not to tie frail elderly patients down with IVs, Foley catheters, EKG monitors, worries that eating a leafy green vegetable will react badly with their Coumadin [warfarin], and polypharmacy.”
He discusses advanced directives, palliative care, and how the elderly in fragile condition can maintain as much freedom as possible. The hospital medicine group’s accommodating scheduling allows time for his parish duties and medical mission trips.
The group’s medical director, Victor Hirth, MD, describes Dr. Petit as a borderline workaholic who’s always looking for ways to make things better for the practice and patients. “The patients absolutely love him because he takes time to sit and talk to them,” says Dr. Hirth.
Dr. Petit also embraces new technologies. “Our [electronic medical record] makes working with my outpatient colleagues smooth and straightforward.” He relies on a personal digital device assistant for updates on clinical guidelines and optimal drug doses for elderly patients. Integrating a healer’s touch with new technology he says: “While medicine is a science, it’s still an art, a ministry, and a gift.”
What’s Next?
Back in South Carolina, Dr. Petit has picked up his hospitalist and pastoral responsibilities without missing a beat. He looks forward to building the palliative care consulting service and intends to launch a nonprofit corporation to receive donations to support the Puerto Lempira clinic’s construction.
He is planning more mission trips. He thrives on the work. Infused with boundless energy, he’s always looking for more to do.
“I love what I do,” he concludes. “If I felt much better they’d charge me an amusement tax.” TH
Marlene Piturro is a medical writer based in New York.
Charles Petit, MD, like many healthcare professionals, spends a good deal of time addressing the needs of the underprivileged. Since 2004, he has taken up the cause of the indigenous Miskito Indians of Puerto Lempira, Honduras. He is putting his own money into developing a modern clinic and international medicine program there.
But medicine isn’t his only mission. Dr. Petit, 56, a hospitalist at Palmetto Health Care’s Richland Memorial Hospital in Columbia, S.C., is also an Episcopal priest.
He joined Palmetto Health Senior Care as its first medical director in 1988 and reconnected with the group in 2004—not in his previous role as an office-based physician but as a hospitalist. In between those stints he pursued his ordination and medical missionary work in Africa and Latin America.
As a physician, Dr. Petit says he feels God’s presence at each patient’s bedside. Years ago he wondered how to handle that.
To deepen his connection between medicine and spirituality, he lived in a Christian intentional community in Indiana, Pa., from 1981 to 1988. Gradually, his views on medicine and spirituality crystallized.
“How does God do what he does?” Dr. Petit wondered. “Can medicine put Him to the test? I have seen that prayer works, including a patient miraculously healed of metastatic ovarian cancer. But God isn’t a vending machine. You don’t drop in a prayer and get a healing back.”
The Second Calling
Recognizing he needed something more to integrate medicine and spirituality, Dr. Petit sought a firmer grounding in religious studies.
He moved to Simpsonville, S.C., in 1995 and entered the Episcopal seminary, working as an emergency department doctor to pay the bills. Later, he earned a master’s of divinity from the University of the South in Sewanee, Tenn., in 2003.
His spiritual “internship” was a transitional deaconship from 2003 to 2005, under the Rev. Michael Flanagan, rector at Simpsonville’s Holy Cross Episcopal Church. Both had dual vocations—Flanagan was an engineer who sold electrical equipment for 10 years before ordination. Prior to meeting Dr. Petit, Flanagan was leery of the doctor’s ability to balance pastoral and medical duties.
“Would he be a doctor/priest?” Flanagan wondered. “A priest/doctor? His desire was to meld both and he did. Medicine and spirituality are both in his blood. He sees both as calls from God and connects medicine with spirituality into a holistic view of each person.” He says Dr. Petit “seems to know everything and sucks up knowledge, which he wants to share. He loves being the doctor and having the knowledge to fix the patient’s problem.”
While Dr. Petit keeps his hospitalist and priest roles mostly separate, working with elderly patients sometimes requires the skills of both disciplines. At Richland he wears a clerical collar on pastoral rounds. If a family or patient asks him to pray with them or discuss life’s ending, he does. He has conducted funerals for his own and colleagues’ patients.
“It’s a very powerful experience being both a priest and a doctor,” he says. “I grow so close to the patients and their families that it is natural for me to serve in both roles.”
Honduras Mission
As a seminarian, Dr. Petit took medical mission trips and briefly supported an African orphanage, looking for a cause to call his own. Until his first trip to Puerto Lempira, a village on the Miskito Coast of the Atlantic Ocean.
The abject poverty and medical needs of the Miskito Indians there pulled at him. Early on he enlisted the help of Ennis Whiddon, a builder and Holy Cross parishioner. Whiddon, who usually accompanies Dr. Petit to Puerto Lempira, says of his friend: “I knew him as [an emergency department] doctor first. Then I realized his extraordinary spiritual commitment. I went to Puerto Lempira on his first mission trip and I asked myself why anyone would want to be there, but I knew Chuck couldn’t bear not to be there. I also knew he wasn’t just going to give people two aspirins, come home and pray for them.”
Dr. Petit returns to Puerto Lempira three or four times a year with a team of doctors, seeing several hundred patients a day. During one two-week stint he dispensed $200,000 worth of medication he cadged from drug companies for $600 out of his pocket to rid the town’s youngsters of debilitating parasites.
Dr. Petit works with a Miskito nurse who runs their rudimentary clinic in his absence. He also uses hyperbaric medicine to treat divers whose crippling injuries result from diving deeply using pressurized oxygen tanks and rising too quickly to the surface.
“You wouldn’t believe the indescribably poor facilities we found there,” Whiddon says of the town’s clinic. “You wouldn’t have your dog treated there if you loved your dog.”
Last year Dr. Petit ratcheted up his commitment to Puerto Lempira, dreaming of building a permanent clinic there.
He decided to use his money to buy land to build a clinic, but got stonewalled by a stubborn local bureaucracy.
Then Andres Leone, a like-minded younger doctor who was part of the mission trip, stepped in with handy language and cultural skills. Leone who had attended medical school in Ecuador, is a Lutheran seminarian, and is completing a geriatric hospitalist fellowship at Palmetto Healthcare.
“We were in Puerto Lempira for two weeks and visited the mayor several times to buy land,” Dr. Leone explains. “He said the price was $600,000, which was ridiculous. In the town I overheard some conversations, which led to us meeting the 77-year-old daughter of missionaries. She sold us some of her land and even donated money to help build the clinic, which will be dedicated in her name.”
Thinking big, Dr. Petit is adding an apartment complete with air conditioning and a modern bathroom to the clinic’s blueprint, to attract residents in a to-be-formed international medicine program. As an assistant professor of family medicine at the University of South Carolina’s (USC) School of Medicine, he intends to oversee those residents.
Just back from Puerto Lempira, Dr. Petit finalized the clinic’s design, lined up local workers to figure out how to make concrete building blocks with native materials, and met with Anglican bishop the Right Rev. Lloyd E. Allen, bolstering support for the new clinic and the possibility of HIV outreach. Side by side with Honduran and Cuban doctors, Dr. Petit treated hundreds of Puerto Lempira’s villagers every day.
Back in the Hospital
Dr. Petit always wanted to be a doctor. Although his father suggested he become a hospital orderly, Dr. Petit knew being a physician was his calling, graduating from the University of West Virginia School of Medicine (Morgantown) family medicine program in 1978.
He enjoys hospital medicine as a holistic approach to caring for patients, consistent with his work early in his career.
An earlier 10-year stint as a hospitalist at HealthSouth Rehabilitation Hospital, also at USC, involved teaching residents and students rotating through the hospital, as well as a consultative service for neurosurgical patients at Richland. At Wheeling Hospital early in his career he became comfortable as a generalist, covering intensive care, assisting in surgery, and delivering many babies.
Being a hospitalist keeps that spirit alive. “It gives me the gift of time to spend with patients,” he says. “I try not to tie frail elderly patients down with IVs, Foley catheters, EKG monitors, worries that eating a leafy green vegetable will react badly with their Coumadin [warfarin], and polypharmacy.”
He discusses advanced directives, palliative care, and how the elderly in fragile condition can maintain as much freedom as possible. The hospital medicine group’s accommodating scheduling allows time for his parish duties and medical mission trips.
The group’s medical director, Victor Hirth, MD, describes Dr. Petit as a borderline workaholic who’s always looking for ways to make things better for the practice and patients. “The patients absolutely love him because he takes time to sit and talk to them,” says Dr. Hirth.
Dr. Petit also embraces new technologies. “Our [electronic medical record] makes working with my outpatient colleagues smooth and straightforward.” He relies on a personal digital device assistant for updates on clinical guidelines and optimal drug doses for elderly patients. Integrating a healer’s touch with new technology he says: “While medicine is a science, it’s still an art, a ministry, and a gift.”
What’s Next?
Back in South Carolina, Dr. Petit has picked up his hospitalist and pastoral responsibilities without missing a beat. He looks forward to building the palliative care consulting service and intends to launch a nonprofit corporation to receive donations to support the Puerto Lempira clinic’s construction.
He is planning more mission trips. He thrives on the work. Infused with boundless energy, he’s always looking for more to do.
“I love what I do,” he concludes. “If I felt much better they’d charge me an amusement tax.” TH
Marlene Piturro is a medical writer based in New York.
Charles Petit, MD, like many healthcare professionals, spends a good deal of time addressing the needs of the underprivileged. Since 2004, he has taken up the cause of the indigenous Miskito Indians of Puerto Lempira, Honduras. He is putting his own money into developing a modern clinic and international medicine program there.
But medicine isn’t his only mission. Dr. Petit, 56, a hospitalist at Palmetto Health Care’s Richland Memorial Hospital in Columbia, S.C., is also an Episcopal priest.
He joined Palmetto Health Senior Care as its first medical director in 1988 and reconnected with the group in 2004—not in his previous role as an office-based physician but as a hospitalist. In between those stints he pursued his ordination and medical missionary work in Africa and Latin America.
As a physician, Dr. Petit says he feels God’s presence at each patient’s bedside. Years ago he wondered how to handle that.
To deepen his connection between medicine and spirituality, he lived in a Christian intentional community in Indiana, Pa., from 1981 to 1988. Gradually, his views on medicine and spirituality crystallized.
“How does God do what he does?” Dr. Petit wondered. “Can medicine put Him to the test? I have seen that prayer works, including a patient miraculously healed of metastatic ovarian cancer. But God isn’t a vending machine. You don’t drop in a prayer and get a healing back.”
The Second Calling
Recognizing he needed something more to integrate medicine and spirituality, Dr. Petit sought a firmer grounding in religious studies.
He moved to Simpsonville, S.C., in 1995 and entered the Episcopal seminary, working as an emergency department doctor to pay the bills. Later, he earned a master’s of divinity from the University of the South in Sewanee, Tenn., in 2003.
His spiritual “internship” was a transitional deaconship from 2003 to 2005, under the Rev. Michael Flanagan, rector at Simpsonville’s Holy Cross Episcopal Church. Both had dual vocations—Flanagan was an engineer who sold electrical equipment for 10 years before ordination. Prior to meeting Dr. Petit, Flanagan was leery of the doctor’s ability to balance pastoral and medical duties.
“Would he be a doctor/priest?” Flanagan wondered. “A priest/doctor? His desire was to meld both and he did. Medicine and spirituality are both in his blood. He sees both as calls from God and connects medicine with spirituality into a holistic view of each person.” He says Dr. Petit “seems to know everything and sucks up knowledge, which he wants to share. He loves being the doctor and having the knowledge to fix the patient’s problem.”
While Dr. Petit keeps his hospitalist and priest roles mostly separate, working with elderly patients sometimes requires the skills of both disciplines. At Richland he wears a clerical collar on pastoral rounds. If a family or patient asks him to pray with them or discuss life’s ending, he does. He has conducted funerals for his own and colleagues’ patients.
“It’s a very powerful experience being both a priest and a doctor,” he says. “I grow so close to the patients and their families that it is natural for me to serve in both roles.”
Honduras Mission
As a seminarian, Dr. Petit took medical mission trips and briefly supported an African orphanage, looking for a cause to call his own. Until his first trip to Puerto Lempira, a village on the Miskito Coast of the Atlantic Ocean.
The abject poverty and medical needs of the Miskito Indians there pulled at him. Early on he enlisted the help of Ennis Whiddon, a builder and Holy Cross parishioner. Whiddon, who usually accompanies Dr. Petit to Puerto Lempira, says of his friend: “I knew him as [an emergency department] doctor first. Then I realized his extraordinary spiritual commitment. I went to Puerto Lempira on his first mission trip and I asked myself why anyone would want to be there, but I knew Chuck couldn’t bear not to be there. I also knew he wasn’t just going to give people two aspirins, come home and pray for them.”
Dr. Petit returns to Puerto Lempira three or four times a year with a team of doctors, seeing several hundred patients a day. During one two-week stint he dispensed $200,000 worth of medication he cadged from drug companies for $600 out of his pocket to rid the town’s youngsters of debilitating parasites.
Dr. Petit works with a Miskito nurse who runs their rudimentary clinic in his absence. He also uses hyperbaric medicine to treat divers whose crippling injuries result from diving deeply using pressurized oxygen tanks and rising too quickly to the surface.
“You wouldn’t believe the indescribably poor facilities we found there,” Whiddon says of the town’s clinic. “You wouldn’t have your dog treated there if you loved your dog.”
Last year Dr. Petit ratcheted up his commitment to Puerto Lempira, dreaming of building a permanent clinic there.
He decided to use his money to buy land to build a clinic, but got stonewalled by a stubborn local bureaucracy.
Then Andres Leone, a like-minded younger doctor who was part of the mission trip, stepped in with handy language and cultural skills. Leone who had attended medical school in Ecuador, is a Lutheran seminarian, and is completing a geriatric hospitalist fellowship at Palmetto Healthcare.
“We were in Puerto Lempira for two weeks and visited the mayor several times to buy land,” Dr. Leone explains. “He said the price was $600,000, which was ridiculous. In the town I overheard some conversations, which led to us meeting the 77-year-old daughter of missionaries. She sold us some of her land and even donated money to help build the clinic, which will be dedicated in her name.”
Thinking big, Dr. Petit is adding an apartment complete with air conditioning and a modern bathroom to the clinic’s blueprint, to attract residents in a to-be-formed international medicine program. As an assistant professor of family medicine at the University of South Carolina’s (USC) School of Medicine, he intends to oversee those residents.
Just back from Puerto Lempira, Dr. Petit finalized the clinic’s design, lined up local workers to figure out how to make concrete building blocks with native materials, and met with Anglican bishop the Right Rev. Lloyd E. Allen, bolstering support for the new clinic and the possibility of HIV outreach. Side by side with Honduran and Cuban doctors, Dr. Petit treated hundreds of Puerto Lempira’s villagers every day.
Back in the Hospital
Dr. Petit always wanted to be a doctor. Although his father suggested he become a hospital orderly, Dr. Petit knew being a physician was his calling, graduating from the University of West Virginia School of Medicine (Morgantown) family medicine program in 1978.
He enjoys hospital medicine as a holistic approach to caring for patients, consistent with his work early in his career.
An earlier 10-year stint as a hospitalist at HealthSouth Rehabilitation Hospital, also at USC, involved teaching residents and students rotating through the hospital, as well as a consultative service for neurosurgical patients at Richland. At Wheeling Hospital early in his career he became comfortable as a generalist, covering intensive care, assisting in surgery, and delivering many babies.
Being a hospitalist keeps that spirit alive. “It gives me the gift of time to spend with patients,” he says. “I try not to tie frail elderly patients down with IVs, Foley catheters, EKG monitors, worries that eating a leafy green vegetable will react badly with their Coumadin [warfarin], and polypharmacy.”
He discusses advanced directives, palliative care, and how the elderly in fragile condition can maintain as much freedom as possible. The hospital medicine group’s accommodating scheduling allows time for his parish duties and medical mission trips.
The group’s medical director, Victor Hirth, MD, describes Dr. Petit as a borderline workaholic who’s always looking for ways to make things better for the practice and patients. “The patients absolutely love him because he takes time to sit and talk to them,” says Dr. Hirth.
Dr. Petit also embraces new technologies. “Our [electronic medical record] makes working with my outpatient colleagues smooth and straightforward.” He relies on a personal digital device assistant for updates on clinical guidelines and optimal drug doses for elderly patients. Integrating a healer’s touch with new technology he says: “While medicine is a science, it’s still an art, a ministry, and a gift.”
What’s Next?
Back in South Carolina, Dr. Petit has picked up his hospitalist and pastoral responsibilities without missing a beat. He looks forward to building the palliative care consulting service and intends to launch a nonprofit corporation to receive donations to support the Puerto Lempira clinic’s construction.
He is planning more mission trips. He thrives on the work. Infused with boundless energy, he’s always looking for more to do.
“I love what I do,” he concludes. “If I felt much better they’d charge me an amusement tax.” TH
Marlene Piturro is a medical writer based in New York.
Experts in the Elderly
The average young or middle-age person probably finds a hospital stay stressful, uncomfortable, and inconvenient. The experience can be strikingly more disruptive for a geriatric patient.
A frail elderly person can easily succumb to delirium, a fall, dehydration, polypharmacy, and deterioration in basic life skills, quickly turning even a routine hospitalization into a catastrophic downhill slide. But if a patient is lucky, she will be treated by a geriatric hospitalist—a physician who by training and temperament is uniquely suited to care for her.
Geriatric hospitalists bring heightened sensitivity and experience to treating and preventing the common syndromes that can overwhelm the elderly during hospitalizations. Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan, has been a geriatrician since the 1980s. He sees a great opportunity for hospitalist geriatricians to improve the metrics by which hospitalist programs are judged: reduced length of stay, bounceback, and morbidity. They do this, he says, with a unique blend of skills, mindset, and temperament.
“In one or two minutes at the bedside, a geriatric hospitalist can do a basic functional assessment of an elderly patient,” he says. “We can understand their ADL [activities of daily living] skills, mental status, and what resources we have to mobilize during the hospital stay and for a safe discharge plan. We don’t want to turn hospitalists into social workers, but geriatricians can teach them a body of knowledge to help them better understand and develop a holistic approach to elderly patients.”
How geriatricians work best, though, can be somewhat out of synch with hospital medicine’s fast pace. “Many hospitalists are younger and have been trained very recently,” Dr. Sherman says. “They quickly learn to take care of a 55-year-old with a [myocardial infarction], but they sometimes lack a global view of geriatric patients that is more a frame of mind than about the physician’s technical skills.”
Challenges Ahead
As hospital medicine groups integrate geriatricians into their ranks, they will have recruited major players invested in improving the care of hospitalized elderly patients. There’s a lot at stake in caring for them.
The Healthcare Cost and Utilization Project’s (HCUP) most recent figures of what hospitalizations of the elderly cost is staggering. Medicare patients account for 76% of public spending on hospital care. The costliest diagnoses for Medicare-paid hospitalizations are coronary arteriosclerosis ($44 billion), acute myocardial infarction ($31 billion), and heart failure ($29 billion). Further, 90% of elderly patients with osteoarthritis are hospitalized for elective hip or knee joint replacement therapy.
The expertise of board-certified hospitalist geriatricians will be hard to disseminate throughout the corps of hospitalists. Only a tiny fraction of the nation’s hospitalist programs claim special expertise in geriatrics. Researchers from the University of Colorado Health Sciences Center and the Mayo Clinic College of Medicine conducted a cross-sectional survey of the hospitalist community in 2003-2004 to determine the impact of the hospitalist movement on acute care geriatrics. They found:
- Out of 1,415 hospitalist programs, 11 reported geriatric innovations.
- Four developed core clinical activities, four used geriatric QI measures, three used comprehensive geriatric assessments, and two had specific protocols for elderly patients discharged to nursing facilities; and
- In terms of staffing, four had hospitalists with no special geriatric training, four employed fellowship-trained geriatricians, two had general hospitalists and geriatricians, and four used advanced practice nurses with and without geriatric training.1
Adding to the difficulty of building a cadre of geriatric hospitalists is the national paucity of geriatricians. According to the American Geriatrics Society (AGS), there were 9,000 board-certified geriatricians in 1998. A decade later there are 7,600—and the pipeline is narrow. Of 9,780 medical school graduates in 2004, only 321 were geriatricians. The AGS estimates that the United States needs 14,000 geriatricians now and 36,000 in 2030, when there will be an estimated 70 million adults 65 years and older.
But there’s hope. Hospital medicine programs, growing by leaps and bounds, offer a new career path for physicians interested in geriatrics. As the number of hospitalists continues to grow, there’s room for physicians to have an impact by staying tuned in to the special clinical, psychosocial, emotional, spiritual, and environmental needs of elderly patients.
The Breed
According to Leslie Libow, MD, distinguished clinical professor at the Jewish Home and Hospital of New York in Manhattan, physicians who pursue a career in geriatrics do so because they have the right psychological make-up to work with elderly people.
He should know. In 1968, Dr. Libow petitioned the American Board of Internal Medicine (ABIM) to recognize geriatrics as a sub-specialty of internal medicine. Shortly after ABIM recognition, Dr. Libow established a geriatric residency/fellowship at Mount Sinai—still a national leader in geriatric education.
Being a geriatric hospitalist allows physicians with a simpatico set of personality traits to thrive. One study of geriatricians who had been practicing for up to 25 years found that they shared these traits:
- Highly value enduring relationships;
- Enjoy making small but potent changes in their patients’ lives;
- Like to make a difference personally and for society;
- Prefer working in a multidisciplinary team;
- Prefer democratic, not autocratic, decision-making;
- Desire the intellectual challenges of geriatric medicine and like to teach; and
- Perceive that they have a distinct and different career path than other physicians.2
That essentially describes Purnima Joshi, chief of medicine, at Kaiser-Permanente Mid-Atlantic States at Washington Hospital Center in Washington, D.C. She directs a group of 12 hospitalists, is the group’s only geriatrician at the 800-bed tertiary care facility, and enjoys teaching residents about geriatric medicine. A family physician by trade, she was grandfathered into geriatrics in 1992 and recertified in 2002.
“I love working with the frail elderly and practicing Kaiser’s brand of medicine because I don’t do billing—I just treat patients,” Dr. Joshi says. Additionally, Kaiser simplifies record-keeping on inpatient and outpatient treatments and makes communicating with Kaiser’s outpatient doctors about post-discharge care smooth and efficient.
Dr. Joshi explains that being a geriatric hospitalist is different than specializing in general internal medicine because she customizes the approach for each patient—including tailoring therapies to life expectancy. “Guidelines and evidence-based medicine are fine and very important, and we use geriatric guidelines on our teaching service,” she says. “But geriatrics liberates your thinking as a doctor. You treat the whole person—a diabetic with three days to live, and a 90-year-old with delirium and decubitus ulcers.”
She calls herself a surrogate primary care physician, seeing 12 patients most days. She consults frequently with other hospitalists on their toughest geriatric issues and makes daily multidisciplinary rounds—with discharge planner, pharmacist, physical therapist, palliative care specialist, nurses, and resident in tow.
“We keep length of stay and guidelines in mind, but the patient is the center of my universe,” Dr. Joshi asserts. “I deliver holistic, patient-centered care and use gentle teaching tools for our residents. I have the luxury of taking time to see the patient and talk to them and their families. It’s wonderful.”
Dr. Joshi’s attitude toward her profession reflects a consistent national finding: Geriatricians rank No. 1 in nearly every study of physician career satisfaction, from the American Medical Association to the American Geriatrics Society.
Across the country, Alpesh Amin, MD, MBA, FACP, professor and chief of general internal medicine and executive director of the University of California at Irvine’s School of Medicine Hospitalist Service, is making the most of the two geriatricians on his 15-hospitalist team. Starting about eight years ago, Dr. Amin—also a member of SHM’s board of directors—turned to his hospitalist geriatricians for a host of services: geriatric assessments, co-management of psychiatric problems, perioperative consults, critical care, and palliative care consults.
“Geriatricians have such knowledge and insight into elderly patients to share with the other hospitalists,” says Dr. Amin. “That’s why they work well side by side with internal medicine and family medicine hospitalists. They keep us aware of issues in geriatrics and the literature on what works best with these patients.”
Knowing that geriatricians are scarce, Dr. Amin accesses their expertise by using a system that focuses team members’ attention on their knowledge. There are journal clubs, frequent consults, monthly meetings, teaching rounds, geriatric fellowships, and other opportunities that keep the geriatrician’s unique perspective front and center for other team members. “They are so in tune with issues related to delirium, polypharmacy, falls risk, etc.,” he says. “Our model incorporates that expertise, and it works very well. We truly work as a multidisciplinary team with ownership and accountability of the special needs of our geriatric patients.”
—Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan
A New Generation
The rapid growth of hospital medicine has encouraged new physicians to choose this career path.
Claudene George, MD, recently completed a two-year geriatric fellowship at Mount Sinai Hospital in New York City and is starting as a geriatric hospitalist at Montefiore Hospital in the Bronx. “Becoming a geriatrician sort of surprised me because I thought I’d go into internal medicine,” she says. “But I love the approach to caring for the whole person and communicating with their families.”
As part of her contract at Montefiore, she negotiated a half-day-per-week rotation at the hospital’s outpatient clinic—part of her commitment to being a well-rounded physician.
“The geriatric assessment up front is essential to find out what the patient’s and family’s goals of care are,” says Dr. George. “If they’re 80 years old and want to stay at home, we need to help them do that safely. That may mean linking them to the [visiting nurse service], a home aide, or adult day care.”
She points out that an inpatient stay also offers seniors the opportunity to be seen by subspecialists and do a lot in a short period of time. “As a hospitalist geriatrician you can see change almost immediately; you can have an impact,” she concludes.
As the hospitalist movement affords career opportunities to geriatricians, young physicians can obtain financial incentives to pursue a career in geriatrics. For instance, in 2006 South Carolina enacted a Geriatrician Loan Forgiveness program, helping physicians to repay up to $35,000 of medical school loans if they complete a geriatrics fellowship and practice in South Carolina for five years after completing medical training.
Victor Hirth, MD, medical director for the Division of Geriatric Services of Palmetto Health of Columbia, S.C., has recruited eight geriatric fellows, two of whom will be hospitalists. A recent recruit, Andres Leone, MD, went to medical school in Ecuador, recently completed a geriatric fellowship in South Carolina, and works as a hospitalist half time and at a free clinic for Hispanics half-time. “The flexibility to work as a hospitalist and in an outpatient clinic feels right to me,” says Dr. Leone.
While the number of geriatric hospitalists today is small, some predict their growing presence is inevitable.
“The baby boomers will deluge us, and they will demand so much more of hospitalists in the near future,” Dr. Sherman says. “They will have complicated issues and be very inquisitive geriatric patients.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
References
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006 Jan;1(1):29-35.
- Shah U, Aung M, Chan S, et al. Do geriatricians stay in geriatrics? Gerontol Geriatr Educ. 2006;27(1):57-65.
The average young or middle-age person probably finds a hospital stay stressful, uncomfortable, and inconvenient. The experience can be strikingly more disruptive for a geriatric patient.
A frail elderly person can easily succumb to delirium, a fall, dehydration, polypharmacy, and deterioration in basic life skills, quickly turning even a routine hospitalization into a catastrophic downhill slide. But if a patient is lucky, she will be treated by a geriatric hospitalist—a physician who by training and temperament is uniquely suited to care for her.
Geriatric hospitalists bring heightened sensitivity and experience to treating and preventing the common syndromes that can overwhelm the elderly during hospitalizations. Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan, has been a geriatrician since the 1980s. He sees a great opportunity for hospitalist geriatricians to improve the metrics by which hospitalist programs are judged: reduced length of stay, bounceback, and morbidity. They do this, he says, with a unique blend of skills, mindset, and temperament.
“In one or two minutes at the bedside, a geriatric hospitalist can do a basic functional assessment of an elderly patient,” he says. “We can understand their ADL [activities of daily living] skills, mental status, and what resources we have to mobilize during the hospital stay and for a safe discharge plan. We don’t want to turn hospitalists into social workers, but geriatricians can teach them a body of knowledge to help them better understand and develop a holistic approach to elderly patients.”
How geriatricians work best, though, can be somewhat out of synch with hospital medicine’s fast pace. “Many hospitalists are younger and have been trained very recently,” Dr. Sherman says. “They quickly learn to take care of a 55-year-old with a [myocardial infarction], but they sometimes lack a global view of geriatric patients that is more a frame of mind than about the physician’s technical skills.”
Challenges Ahead
As hospital medicine groups integrate geriatricians into their ranks, they will have recruited major players invested in improving the care of hospitalized elderly patients. There’s a lot at stake in caring for them.
The Healthcare Cost and Utilization Project’s (HCUP) most recent figures of what hospitalizations of the elderly cost is staggering. Medicare patients account for 76% of public spending on hospital care. The costliest diagnoses for Medicare-paid hospitalizations are coronary arteriosclerosis ($44 billion), acute myocardial infarction ($31 billion), and heart failure ($29 billion). Further, 90% of elderly patients with osteoarthritis are hospitalized for elective hip or knee joint replacement therapy.
The expertise of board-certified hospitalist geriatricians will be hard to disseminate throughout the corps of hospitalists. Only a tiny fraction of the nation’s hospitalist programs claim special expertise in geriatrics. Researchers from the University of Colorado Health Sciences Center and the Mayo Clinic College of Medicine conducted a cross-sectional survey of the hospitalist community in 2003-2004 to determine the impact of the hospitalist movement on acute care geriatrics. They found:
- Out of 1,415 hospitalist programs, 11 reported geriatric innovations.
- Four developed core clinical activities, four used geriatric QI measures, three used comprehensive geriatric assessments, and two had specific protocols for elderly patients discharged to nursing facilities; and
- In terms of staffing, four had hospitalists with no special geriatric training, four employed fellowship-trained geriatricians, two had general hospitalists and geriatricians, and four used advanced practice nurses with and without geriatric training.1
Adding to the difficulty of building a cadre of geriatric hospitalists is the national paucity of geriatricians. According to the American Geriatrics Society (AGS), there were 9,000 board-certified geriatricians in 1998. A decade later there are 7,600—and the pipeline is narrow. Of 9,780 medical school graduates in 2004, only 321 were geriatricians. The AGS estimates that the United States needs 14,000 geriatricians now and 36,000 in 2030, when there will be an estimated 70 million adults 65 years and older.
But there’s hope. Hospital medicine programs, growing by leaps and bounds, offer a new career path for physicians interested in geriatrics. As the number of hospitalists continues to grow, there’s room for physicians to have an impact by staying tuned in to the special clinical, psychosocial, emotional, spiritual, and environmental needs of elderly patients.
The Breed
According to Leslie Libow, MD, distinguished clinical professor at the Jewish Home and Hospital of New York in Manhattan, physicians who pursue a career in geriatrics do so because they have the right psychological make-up to work with elderly people.
He should know. In 1968, Dr. Libow petitioned the American Board of Internal Medicine (ABIM) to recognize geriatrics as a sub-specialty of internal medicine. Shortly after ABIM recognition, Dr. Libow established a geriatric residency/fellowship at Mount Sinai—still a national leader in geriatric education.
Being a geriatric hospitalist allows physicians with a simpatico set of personality traits to thrive. One study of geriatricians who had been practicing for up to 25 years found that they shared these traits:
- Highly value enduring relationships;
- Enjoy making small but potent changes in their patients’ lives;
- Like to make a difference personally and for society;
- Prefer working in a multidisciplinary team;
- Prefer democratic, not autocratic, decision-making;
- Desire the intellectual challenges of geriatric medicine and like to teach; and
- Perceive that they have a distinct and different career path than other physicians.2
That essentially describes Purnima Joshi, chief of medicine, at Kaiser-Permanente Mid-Atlantic States at Washington Hospital Center in Washington, D.C. She directs a group of 12 hospitalists, is the group’s only geriatrician at the 800-bed tertiary care facility, and enjoys teaching residents about geriatric medicine. A family physician by trade, she was grandfathered into geriatrics in 1992 and recertified in 2002.
“I love working with the frail elderly and practicing Kaiser’s brand of medicine because I don’t do billing—I just treat patients,” Dr. Joshi says. Additionally, Kaiser simplifies record-keeping on inpatient and outpatient treatments and makes communicating with Kaiser’s outpatient doctors about post-discharge care smooth and efficient.
Dr. Joshi explains that being a geriatric hospitalist is different than specializing in general internal medicine because she customizes the approach for each patient—including tailoring therapies to life expectancy. “Guidelines and evidence-based medicine are fine and very important, and we use geriatric guidelines on our teaching service,” she says. “But geriatrics liberates your thinking as a doctor. You treat the whole person—a diabetic with three days to live, and a 90-year-old with delirium and decubitus ulcers.”
She calls herself a surrogate primary care physician, seeing 12 patients most days. She consults frequently with other hospitalists on their toughest geriatric issues and makes daily multidisciplinary rounds—with discharge planner, pharmacist, physical therapist, palliative care specialist, nurses, and resident in tow.
“We keep length of stay and guidelines in mind, but the patient is the center of my universe,” Dr. Joshi asserts. “I deliver holistic, patient-centered care and use gentle teaching tools for our residents. I have the luxury of taking time to see the patient and talk to them and their families. It’s wonderful.”
Dr. Joshi’s attitude toward her profession reflects a consistent national finding: Geriatricians rank No. 1 in nearly every study of physician career satisfaction, from the American Medical Association to the American Geriatrics Society.
Across the country, Alpesh Amin, MD, MBA, FACP, professor and chief of general internal medicine and executive director of the University of California at Irvine’s School of Medicine Hospitalist Service, is making the most of the two geriatricians on his 15-hospitalist team. Starting about eight years ago, Dr. Amin—also a member of SHM’s board of directors—turned to his hospitalist geriatricians for a host of services: geriatric assessments, co-management of psychiatric problems, perioperative consults, critical care, and palliative care consults.
“Geriatricians have such knowledge and insight into elderly patients to share with the other hospitalists,” says Dr. Amin. “That’s why they work well side by side with internal medicine and family medicine hospitalists. They keep us aware of issues in geriatrics and the literature on what works best with these patients.”
Knowing that geriatricians are scarce, Dr. Amin accesses their expertise by using a system that focuses team members’ attention on their knowledge. There are journal clubs, frequent consults, monthly meetings, teaching rounds, geriatric fellowships, and other opportunities that keep the geriatrician’s unique perspective front and center for other team members. “They are so in tune with issues related to delirium, polypharmacy, falls risk, etc.,” he says. “Our model incorporates that expertise, and it works very well. We truly work as a multidisciplinary team with ownership and accountability of the special needs of our geriatric patients.”
—Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan
A New Generation
The rapid growth of hospital medicine has encouraged new physicians to choose this career path.
Claudene George, MD, recently completed a two-year geriatric fellowship at Mount Sinai Hospital in New York City and is starting as a geriatric hospitalist at Montefiore Hospital in the Bronx. “Becoming a geriatrician sort of surprised me because I thought I’d go into internal medicine,” she says. “But I love the approach to caring for the whole person and communicating with their families.”
As part of her contract at Montefiore, she negotiated a half-day-per-week rotation at the hospital’s outpatient clinic—part of her commitment to being a well-rounded physician.
“The geriatric assessment up front is essential to find out what the patient’s and family’s goals of care are,” says Dr. George. “If they’re 80 years old and want to stay at home, we need to help them do that safely. That may mean linking them to the [visiting nurse service], a home aide, or adult day care.”
She points out that an inpatient stay also offers seniors the opportunity to be seen by subspecialists and do a lot in a short period of time. “As a hospitalist geriatrician you can see change almost immediately; you can have an impact,” she concludes.
As the hospitalist movement affords career opportunities to geriatricians, young physicians can obtain financial incentives to pursue a career in geriatrics. For instance, in 2006 South Carolina enacted a Geriatrician Loan Forgiveness program, helping physicians to repay up to $35,000 of medical school loans if they complete a geriatrics fellowship and practice in South Carolina for five years after completing medical training.
Victor Hirth, MD, medical director for the Division of Geriatric Services of Palmetto Health of Columbia, S.C., has recruited eight geriatric fellows, two of whom will be hospitalists. A recent recruit, Andres Leone, MD, went to medical school in Ecuador, recently completed a geriatric fellowship in South Carolina, and works as a hospitalist half time and at a free clinic for Hispanics half-time. “The flexibility to work as a hospitalist and in an outpatient clinic feels right to me,” says Dr. Leone.
While the number of geriatric hospitalists today is small, some predict their growing presence is inevitable.
“The baby boomers will deluge us, and they will demand so much more of hospitalists in the near future,” Dr. Sherman says. “They will have complicated issues and be very inquisitive geriatric patients.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
References
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006 Jan;1(1):29-35.
- Shah U, Aung M, Chan S, et al. Do geriatricians stay in geriatrics? Gerontol Geriatr Educ. 2006;27(1):57-65.
The average young or middle-age person probably finds a hospital stay stressful, uncomfortable, and inconvenient. The experience can be strikingly more disruptive for a geriatric patient.
A frail elderly person can easily succumb to delirium, a fall, dehydration, polypharmacy, and deterioration in basic life skills, quickly turning even a routine hospitalization into a catastrophic downhill slide. But if a patient is lucky, she will be treated by a geriatric hospitalist—a physician who by training and temperament is uniquely suited to care for her.
Geriatric hospitalists bring heightened sensitivity and experience to treating and preventing the common syndromes that can overwhelm the elderly during hospitalizations. Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan, has been a geriatrician since the 1980s. He sees a great opportunity for hospitalist geriatricians to improve the metrics by which hospitalist programs are judged: reduced length of stay, bounceback, and morbidity. They do this, he says, with a unique blend of skills, mindset, and temperament.
“In one or two minutes at the bedside, a geriatric hospitalist can do a basic functional assessment of an elderly patient,” he says. “We can understand their ADL [activities of daily living] skills, mental status, and what resources we have to mobilize during the hospital stay and for a safe discharge plan. We don’t want to turn hospitalists into social workers, but geriatricians can teach them a body of knowledge to help them better understand and develop a holistic approach to elderly patients.”
How geriatricians work best, though, can be somewhat out of synch with hospital medicine’s fast pace. “Many hospitalists are younger and have been trained very recently,” Dr. Sherman says. “They quickly learn to take care of a 55-year-old with a [myocardial infarction], but they sometimes lack a global view of geriatric patients that is more a frame of mind than about the physician’s technical skills.”
Challenges Ahead
As hospital medicine groups integrate geriatricians into their ranks, they will have recruited major players invested in improving the care of hospitalized elderly patients. There’s a lot at stake in caring for them.
The Healthcare Cost and Utilization Project’s (HCUP) most recent figures of what hospitalizations of the elderly cost is staggering. Medicare patients account for 76% of public spending on hospital care. The costliest diagnoses for Medicare-paid hospitalizations are coronary arteriosclerosis ($44 billion), acute myocardial infarction ($31 billion), and heart failure ($29 billion). Further, 90% of elderly patients with osteoarthritis are hospitalized for elective hip or knee joint replacement therapy.
The expertise of board-certified hospitalist geriatricians will be hard to disseminate throughout the corps of hospitalists. Only a tiny fraction of the nation’s hospitalist programs claim special expertise in geriatrics. Researchers from the University of Colorado Health Sciences Center and the Mayo Clinic College of Medicine conducted a cross-sectional survey of the hospitalist community in 2003-2004 to determine the impact of the hospitalist movement on acute care geriatrics. They found:
- Out of 1,415 hospitalist programs, 11 reported geriatric innovations.
- Four developed core clinical activities, four used geriatric QI measures, three used comprehensive geriatric assessments, and two had specific protocols for elderly patients discharged to nursing facilities; and
- In terms of staffing, four had hospitalists with no special geriatric training, four employed fellowship-trained geriatricians, two had general hospitalists and geriatricians, and four used advanced practice nurses with and without geriatric training.1
Adding to the difficulty of building a cadre of geriatric hospitalists is the national paucity of geriatricians. According to the American Geriatrics Society (AGS), there were 9,000 board-certified geriatricians in 1998. A decade later there are 7,600—and the pipeline is narrow. Of 9,780 medical school graduates in 2004, only 321 were geriatricians. The AGS estimates that the United States needs 14,000 geriatricians now and 36,000 in 2030, when there will be an estimated 70 million adults 65 years and older.
But there’s hope. Hospital medicine programs, growing by leaps and bounds, offer a new career path for physicians interested in geriatrics. As the number of hospitalists continues to grow, there’s room for physicians to have an impact by staying tuned in to the special clinical, psychosocial, emotional, spiritual, and environmental needs of elderly patients.
The Breed
According to Leslie Libow, MD, distinguished clinical professor at the Jewish Home and Hospital of New York in Manhattan, physicians who pursue a career in geriatrics do so because they have the right psychological make-up to work with elderly people.
He should know. In 1968, Dr. Libow petitioned the American Board of Internal Medicine (ABIM) to recognize geriatrics as a sub-specialty of internal medicine. Shortly after ABIM recognition, Dr. Libow established a geriatric residency/fellowship at Mount Sinai—still a national leader in geriatric education.
Being a geriatric hospitalist allows physicians with a simpatico set of personality traits to thrive. One study of geriatricians who had been practicing for up to 25 years found that they shared these traits:
- Highly value enduring relationships;
- Enjoy making small but potent changes in their patients’ lives;
- Like to make a difference personally and for society;
- Prefer working in a multidisciplinary team;
- Prefer democratic, not autocratic, decision-making;
- Desire the intellectual challenges of geriatric medicine and like to teach; and
- Perceive that they have a distinct and different career path than other physicians.2
That essentially describes Purnima Joshi, chief of medicine, at Kaiser-Permanente Mid-Atlantic States at Washington Hospital Center in Washington, D.C. She directs a group of 12 hospitalists, is the group’s only geriatrician at the 800-bed tertiary care facility, and enjoys teaching residents about geriatric medicine. A family physician by trade, she was grandfathered into geriatrics in 1992 and recertified in 2002.
“I love working with the frail elderly and practicing Kaiser’s brand of medicine because I don’t do billing—I just treat patients,” Dr. Joshi says. Additionally, Kaiser simplifies record-keeping on inpatient and outpatient treatments and makes communicating with Kaiser’s outpatient doctors about post-discharge care smooth and efficient.
Dr. Joshi explains that being a geriatric hospitalist is different than specializing in general internal medicine because she customizes the approach for each patient—including tailoring therapies to life expectancy. “Guidelines and evidence-based medicine are fine and very important, and we use geriatric guidelines on our teaching service,” she says. “But geriatrics liberates your thinking as a doctor. You treat the whole person—a diabetic with three days to live, and a 90-year-old with delirium and decubitus ulcers.”
She calls herself a surrogate primary care physician, seeing 12 patients most days. She consults frequently with other hospitalists on their toughest geriatric issues and makes daily multidisciplinary rounds—with discharge planner, pharmacist, physical therapist, palliative care specialist, nurses, and resident in tow.
“We keep length of stay and guidelines in mind, but the patient is the center of my universe,” Dr. Joshi asserts. “I deliver holistic, patient-centered care and use gentle teaching tools for our residents. I have the luxury of taking time to see the patient and talk to them and their families. It’s wonderful.”
Dr. Joshi’s attitude toward her profession reflects a consistent national finding: Geriatricians rank No. 1 in nearly every study of physician career satisfaction, from the American Medical Association to the American Geriatrics Society.
Across the country, Alpesh Amin, MD, MBA, FACP, professor and chief of general internal medicine and executive director of the University of California at Irvine’s School of Medicine Hospitalist Service, is making the most of the two geriatricians on his 15-hospitalist team. Starting about eight years ago, Dr. Amin—also a member of SHM’s board of directors—turned to his hospitalist geriatricians for a host of services: geriatric assessments, co-management of psychiatric problems, perioperative consults, critical care, and palliative care consults.
“Geriatricians have such knowledge and insight into elderly patients to share with the other hospitalists,” says Dr. Amin. “That’s why they work well side by side with internal medicine and family medicine hospitalists. They keep us aware of issues in geriatrics and the literature on what works best with these patients.”
Knowing that geriatricians are scarce, Dr. Amin accesses their expertise by using a system that focuses team members’ attention on their knowledge. There are journal clubs, frequent consults, monthly meetings, teaching rounds, geriatric fellowships, and other opportunities that keep the geriatrician’s unique perspective front and center for other team members. “They are so in tune with issues related to delirium, polypharmacy, falls risk, etc.,” he says. “Our model incorporates that expertise, and it works very well. We truly work as a multidisciplinary team with ownership and accountability of the special needs of our geriatric patients.”
—Fredrick Sherman, MD, FACP, medical director of Senior Health Partners and professor of geriatrics at the Mount Sinai School of Medicine in Manhattan
A New Generation
The rapid growth of hospital medicine has encouraged new physicians to choose this career path.
Claudene George, MD, recently completed a two-year geriatric fellowship at Mount Sinai Hospital in New York City and is starting as a geriatric hospitalist at Montefiore Hospital in the Bronx. “Becoming a geriatrician sort of surprised me because I thought I’d go into internal medicine,” she says. “But I love the approach to caring for the whole person and communicating with their families.”
As part of her contract at Montefiore, she negotiated a half-day-per-week rotation at the hospital’s outpatient clinic—part of her commitment to being a well-rounded physician.
“The geriatric assessment up front is essential to find out what the patient’s and family’s goals of care are,” says Dr. George. “If they’re 80 years old and want to stay at home, we need to help them do that safely. That may mean linking them to the [visiting nurse service], a home aide, or adult day care.”
She points out that an inpatient stay also offers seniors the opportunity to be seen by subspecialists and do a lot in a short period of time. “As a hospitalist geriatrician you can see change almost immediately; you can have an impact,” she concludes.
As the hospitalist movement affords career opportunities to geriatricians, young physicians can obtain financial incentives to pursue a career in geriatrics. For instance, in 2006 South Carolina enacted a Geriatrician Loan Forgiveness program, helping physicians to repay up to $35,000 of medical school loans if they complete a geriatrics fellowship and practice in South Carolina for five years after completing medical training.
Victor Hirth, MD, medical director for the Division of Geriatric Services of Palmetto Health of Columbia, S.C., has recruited eight geriatric fellows, two of whom will be hospitalists. A recent recruit, Andres Leone, MD, went to medical school in Ecuador, recently completed a geriatric fellowship in South Carolina, and works as a hospitalist half time and at a free clinic for Hispanics half-time. “The flexibility to work as a hospitalist and in an outpatient clinic feels right to me,” says Dr. Leone.
While the number of geriatric hospitalists today is small, some predict their growing presence is inevitable.
“The baby boomers will deluge us, and they will demand so much more of hospitalists in the near future,” Dr. Sherman says. “They will have complicated issues and be very inquisitive geriatric patients.” TH
Marlene Piturro is a frequent contributor to The Hospitalist.
References
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006 Jan;1(1):29-35.
- Shah U, Aung M, Chan S, et al. Do geriatricians stay in geriatrics? Gerontol Geriatr Educ. 2006;27(1):57-65.