User login
If ignorance is bliss, then a substantial slice of hospital medicine group (HMG) leaders are in heaven—about finance, that is. Perhaps they didn’t become physicians to solve the sub-prime mortgage mess or take their companies public, as Dr. Adam Singer, MD, CEO of IPC: The Hospitalist Company, did in January 2008.
Dr. Singer, recently named 2008 Physician Entrepreneur of the Year by Modern Physician, always has insisted HMGs can be financially self-supporting. In 2002, he wrote in Physician Executive “when revenue (fees divided by number of patient encounters) exceeds expenses, the practice becomes economically viable.” He calculated that factoring in malpractice insurance, general expenses, 10 percent of revenue for billing and collection, two patient encounters a day per full-time equivalent employee was an HMGs’ break-even point. “Even at a ridiculously minimum encounter volume of two, a hospitalist practice is viable without any outside subsidy,” he concluded. To drive home his point, Dr. Singer suggested HMGs augment their revenues by serving nursing homes and rehab facilities, teaching, securing research grants, medical directorships, and taking on contracts to manage ER unassigned patients.
Nevertheless, a recent Society of Hospital Medicine survey shows a number of HMG leaders lack the basic financial acumen to get and keep their practices fiscally healthy. Data from SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement reveals the vast majority of HMGs fall short of economic independence. Survey results show many HMG leaders’ grasp of basic finance leaves room for improvement.
Key findings include:
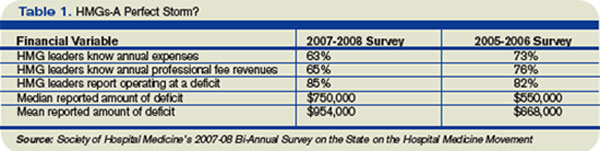
- 37% of HMG leaders didn’t know their annual expenses;
- 35% didn’t know their annual professional fee revenues; and
- Among those that didn’t know their expenses and revenues, 85% were operating at a deficit.
Additionally, a negative correlation exists between HMG financial performance and compensation. HMG production remained flat, while average hospitalist compensation increased 13% to $193,000 annually. Cushiony subsidies persist; the survey showed 91% of HMGs receive some form of financial support, an average of $954,000 per group or $97,375 for each full-time physician.
Drilling down into the survey’s financial data, analysis by Joe Miller, SHM Executive Advisor to the CEO, points to an ominous monetary “perfect storm” brewing for HMG leaders. Deficits are growing as hospitalist leaders’ knowledge about their groups’ finances are declining.
The trend data also suggest subsidies obscure declining financial support in several areas. Compared to the 2005-06 SHM survey, the latest survey shows the percentage of HMGs receiving financial support dropped in all five categories in which HMGs receive subsidies. Results from the two most recent surveys showed hospital financial support dropped from 60% to 51%; other support from 17% to 12%; income guarantees fell from 72% to 61%; services in-kind declined from 71% to 60%; and case rates slid from 12% to 11%.
Fuzzy Math?
An oft-cited rationale for hospital medicine’s generous subsidies from other stakeholders is that it “creates value,” in terms of reducing hospital length of stay, costs per case and improved outcomes. Throughout the years, such savings have received increased scrutiny. Blogger and SHM member Dr. Robert Wachter, MD, professor and associated chairman of the Department of Medicine at the University of California, San Francisco, said in May “research on these metrics is disappointing. … The move toward hospitalist shift work and the resulting fragmentation of care during hospitalization may be eroding any slim advantage the model had in cost savings.” He concluded, “the bubble will burst the morning CEOs wake up and realize that there is no longer a shortage of hospitalists.”
Burke Kealey, MD, assistant medical director, Hospital Medicine Division of HealthPartners Medical Group in St. Paul, Minn., offers powerful reasons for why hospitalists struggle with Finance 101:
- Hospitalists have little incentive to meet financial performance targets;
- HMG leaders are too busy with recruiting, scheduling and retention to focus on finance;
- Difficulties obtaining useful data from hospital administrators; and
- Too few business models that centralize data from multiple hospitals, making financial analysis of an individual group difficult.
To address the needs, Dr. Kealey, who chairs SHM’s Practice Analysis Committee, has spearheaded SHM’s development of dashboards that utilize performance metrics, such as volume data, case mix, length of stay, resource utilization, productivity, and readmission rates, to help leaders guide a practice to economic health.
Steve Liu, MD, the CEO and founder of Ingenious Med, is a hospitalist in one of the nation’s largest HMGs, with 100,000-plus patient encounters annually at Emory Healthcare in Atlanta. A member of SHM’s Benchmarks Committee, Liu puts HMG leaders’ financial ignorance in the context of a growth industry. “Hospital medicine is young, it’s moving very fast, and it is filled with a youngish crowd who don’t feel they have enough time to focus on financial deficits and inefficiencies,” Dr. Liu says.
Still, a lack of financial knowledge can trip up the best of physician. Dr. Liu advises hospitalist leaders to focus on professional fee revenues, particularly on fees collected per full-time equivalent employee (FTE); eliminating high expenses from inefficiencies; and checking local and national compensation packages to address what he estimates as 30 percent of HMGs who fail to pay physicians appropriately. Other financial mistakes, he says, are HMG leaders throwing warm bodies at problems without enough back-office support; agreeing to see more patients than they can handle in a day; overspending on recruiters; and failure to understand each full-time employee’s return on investment.
Numerous hospitalists, according to Dr. Liu, believe they don’t have enough time to build partnerships with administrators that would lead to more sharing of financial data. “They may even be in a power struggle with administrators over access to financial data. … If you can’t measure it, you can’t manage it. That’s the essence of Finance 101,” Dr. Liu says, “and it’s very frustrating to hospitalists who don’t have the business skill sets and tools to succeed financially.” Since data is power, it’s imperative to ask the chief financial officer (CFO) for data; that way the HMG can work toward profitability.
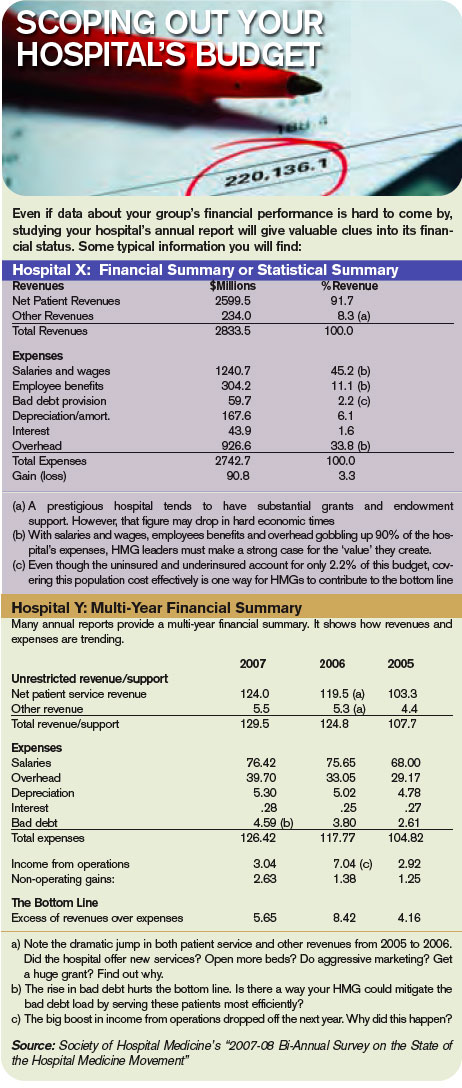
Making sense of financial data is critical, says Leslie Flores, director of SHM’s Practice Management Institute. “HMG leaders have to learn to take data, such as number of encounters, relative value units, average daily census, number of days worked per year, the total subsidy for the practice, and average subsidy per hospitalist, and make sense of it. Where do the numbers come from and what do they mean are critical questions,” she says.
Big Picture
SHM’s most recent survey reflects the average hospitalist medicine group’s business model. Production is flat; compensation is up 13%; and 91% of HMGs receive subsidies nearing $1 million each. From a dollars-and-sense vantage point, the business case for hospital medicine doesn’t work. So why do hospitals go along with a broken business model, especially at a time when a hospital’s cost curve is growing faster than its revenue curve, making it even more difficult to justify HMG subsidies?
The short answer is that most hospital medicine programs are invited in by hospital administrators and serve a specific purpose related to overall revenue generation and/or cost controls. Common reasons for creating hospitalist programs are improving Emergency Department throughput, relieving community-based physicians from hospital duties, boosting subspecialist revenues with medical co-management, and cost cutting through reduced length of stay and improved resource utilization. Each has different financial metrics associated with it, and HMG leaders should understand each metric thoroughly.
If, for example, relieving the pressure on community-based doctors is the HMG’s primary goal, an HMG leader’s strategy might be to attract the best hospitalists available, offering a high compensation package and recruiting bonus. That would help cover the increased patient load, but it might pressure the hospital to shoulder a steep subsidy.
Alternatively, relying on financial and performance metrics might yield better rules about when to justify a new hire. Seasoned HMG leaders would rely on a group’s average daily census of 50 to 70 patients as the tipping point for adding a FTE hospitalist. Similarly, night admissions of 10 to 14 patients should trigger the hiring of a nocturnist, with his or her premium pay.
Brian Bossard, MD, founder of Inpatient Physicians Associates in Lincoln, Neb., relies on that type of data and other “lean” management concepts. To optimize each physicians’ patient loads and productivity, he has patients assigned by physical proximity, so his hospitalists won’t waste time running around the hospital seeing patients. Saving time and manpower contributes to an HMG’s financial health.
Once HMGs satisfy the primary service goals set by their hospitals, leaders should focus on enhancing their hospitals’ revenue generation from various sources. The typical mix of hospital revenue streams are, in size order—clinical services, research, philanthropic grants, interest income on cash assets, and royalties from intellectual property. Clinical services and research account for about 95% of the average hospital revenues, with the balance split among the other three.
Hospitals try to boost revenue by adding product lines, enhancing the value of current products, increasing market share, and capitalizing on production efficiencies. Translating business concepts from widgets to wards, increasing both volume and acuity of patient encounters, should be commonplace and a revenue booster. Research revenues are another story, particularly with slowdowns in National Institutes of Health funding. Recruiting hospitalists who want to do research leaves hospitals covering their salaries and labs for long periods of time without revenue generation.
Focusing on proven revenue generators—enhancing the value of current products, increasing market share, and boosting production efficiencies—can help HMG leaders carve out a niche that truly creates value for the hospital.
It may take a lot for an HMG leader to build solid financial performance on a strong clinical foundation, however, it is doable. Dr. Liu sums up how HMG finances will improve: “As hospital medicine matures, expect its leaders to mature as well,” he says. “They will become more business savvy and learn to speak the language of business, even if they have to force themselves to learn.” TH
If ignorance is bliss, then a substantial slice of hospital medicine group (HMG) leaders are in heaven—about finance, that is. Perhaps they didn’t become physicians to solve the sub-prime mortgage mess or take their companies public, as Dr. Adam Singer, MD, CEO of IPC: The Hospitalist Company, did in January 2008.
Dr. Singer, recently named 2008 Physician Entrepreneur of the Year by Modern Physician, always has insisted HMGs can be financially self-supporting. In 2002, he wrote in Physician Executive “when revenue (fees divided by number of patient encounters) exceeds expenses, the practice becomes economically viable.” He calculated that factoring in malpractice insurance, general expenses, 10 percent of revenue for billing and collection, two patient encounters a day per full-time equivalent employee was an HMGs’ break-even point. “Even at a ridiculously minimum encounter volume of two, a hospitalist practice is viable without any outside subsidy,” he concluded. To drive home his point, Dr. Singer suggested HMGs augment their revenues by serving nursing homes and rehab facilities, teaching, securing research grants, medical directorships, and taking on contracts to manage ER unassigned patients.
Nevertheless, a recent Society of Hospital Medicine survey shows a number of HMG leaders lack the basic financial acumen to get and keep their practices fiscally healthy. Data from SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement reveals the vast majority of HMGs fall short of economic independence. Survey results show many HMG leaders’ grasp of basic finance leaves room for improvement.
Key findings include:
- 37% of HMG leaders didn’t know their annual expenses;
- 35% didn’t know their annual professional fee revenues; and
- Among those that didn’t know their expenses and revenues, 85% were operating at a deficit.
Additionally, a negative correlation exists between HMG financial performance and compensation. HMG production remained flat, while average hospitalist compensation increased 13% to $193,000 annually. Cushiony subsidies persist; the survey showed 91% of HMGs receive some form of financial support, an average of $954,000 per group or $97,375 for each full-time physician.
Drilling down into the survey’s financial data, analysis by Joe Miller, SHM Executive Advisor to the CEO, points to an ominous monetary “perfect storm” brewing for HMG leaders. Deficits are growing as hospitalist leaders’ knowledge about their groups’ finances are declining.
The trend data also suggest subsidies obscure declining financial support in several areas. Compared to the 2005-06 SHM survey, the latest survey shows the percentage of HMGs receiving financial support dropped in all five categories in which HMGs receive subsidies. Results from the two most recent surveys showed hospital financial support dropped from 60% to 51%; other support from 17% to 12%; income guarantees fell from 72% to 61%; services in-kind declined from 71% to 60%; and case rates slid from 12% to 11%.
Fuzzy Math?
An oft-cited rationale for hospital medicine’s generous subsidies from other stakeholders is that it “creates value,” in terms of reducing hospital length of stay, costs per case and improved outcomes. Throughout the years, such savings have received increased scrutiny. Blogger and SHM member Dr. Robert Wachter, MD, professor and associated chairman of the Department of Medicine at the University of California, San Francisco, said in May “research on these metrics is disappointing. … The move toward hospitalist shift work and the resulting fragmentation of care during hospitalization may be eroding any slim advantage the model had in cost savings.” He concluded, “the bubble will burst the morning CEOs wake up and realize that there is no longer a shortage of hospitalists.”
Burke Kealey, MD, assistant medical director, Hospital Medicine Division of HealthPartners Medical Group in St. Paul, Minn., offers powerful reasons for why hospitalists struggle with Finance 101:
- Hospitalists have little incentive to meet financial performance targets;
- HMG leaders are too busy with recruiting, scheduling and retention to focus on finance;
- Difficulties obtaining useful data from hospital administrators; and
- Too few business models that centralize data from multiple hospitals, making financial analysis of an individual group difficult.
To address the needs, Dr. Kealey, who chairs SHM’s Practice Analysis Committee, has spearheaded SHM’s development of dashboards that utilize performance metrics, such as volume data, case mix, length of stay, resource utilization, productivity, and readmission rates, to help leaders guide a practice to economic health.
Steve Liu, MD, the CEO and founder of Ingenious Med, is a hospitalist in one of the nation’s largest HMGs, with 100,000-plus patient encounters annually at Emory Healthcare in Atlanta. A member of SHM’s Benchmarks Committee, Liu puts HMG leaders’ financial ignorance in the context of a growth industry. “Hospital medicine is young, it’s moving very fast, and it is filled with a youngish crowd who don’t feel they have enough time to focus on financial deficits and inefficiencies,” Dr. Liu says.
Still, a lack of financial knowledge can trip up the best of physician. Dr. Liu advises hospitalist leaders to focus on professional fee revenues, particularly on fees collected per full-time equivalent employee (FTE); eliminating high expenses from inefficiencies; and checking local and national compensation packages to address what he estimates as 30 percent of HMGs who fail to pay physicians appropriately. Other financial mistakes, he says, are HMG leaders throwing warm bodies at problems without enough back-office support; agreeing to see more patients than they can handle in a day; overspending on recruiters; and failure to understand each full-time employee’s return on investment.
Numerous hospitalists, according to Dr. Liu, believe they don’t have enough time to build partnerships with administrators that would lead to more sharing of financial data. “They may even be in a power struggle with administrators over access to financial data. … If you can’t measure it, you can’t manage it. That’s the essence of Finance 101,” Dr. Liu says, “and it’s very frustrating to hospitalists who don’t have the business skill sets and tools to succeed financially.” Since data is power, it’s imperative to ask the chief financial officer (CFO) for data; that way the HMG can work toward profitability.
Making sense of financial data is critical, says Leslie Flores, director of SHM’s Practice Management Institute. “HMG leaders have to learn to take data, such as number of encounters, relative value units, average daily census, number of days worked per year, the total subsidy for the practice, and average subsidy per hospitalist, and make sense of it. Where do the numbers come from and what do they mean are critical questions,” she says.
Big Picture
SHM’s most recent survey reflects the average hospitalist medicine group’s business model. Production is flat; compensation is up 13%; and 91% of HMGs receive subsidies nearing $1 million each. From a dollars-and-sense vantage point, the business case for hospital medicine doesn’t work. So why do hospitals go along with a broken business model, especially at a time when a hospital’s cost curve is growing faster than its revenue curve, making it even more difficult to justify HMG subsidies?
The short answer is that most hospital medicine programs are invited in by hospital administrators and serve a specific purpose related to overall revenue generation and/or cost controls. Common reasons for creating hospitalist programs are improving Emergency Department throughput, relieving community-based physicians from hospital duties, boosting subspecialist revenues with medical co-management, and cost cutting through reduced length of stay and improved resource utilization. Each has different financial metrics associated with it, and HMG leaders should understand each metric thoroughly.
If, for example, relieving the pressure on community-based doctors is the HMG’s primary goal, an HMG leader’s strategy might be to attract the best hospitalists available, offering a high compensation package and recruiting bonus. That would help cover the increased patient load, but it might pressure the hospital to shoulder a steep subsidy.
Alternatively, relying on financial and performance metrics might yield better rules about when to justify a new hire. Seasoned HMG leaders would rely on a group’s average daily census of 50 to 70 patients as the tipping point for adding a FTE hospitalist. Similarly, night admissions of 10 to 14 patients should trigger the hiring of a nocturnist, with his or her premium pay.
Brian Bossard, MD, founder of Inpatient Physicians Associates in Lincoln, Neb., relies on that type of data and other “lean” management concepts. To optimize each physicians’ patient loads and productivity, he has patients assigned by physical proximity, so his hospitalists won’t waste time running around the hospital seeing patients. Saving time and manpower contributes to an HMG’s financial health.
Once HMGs satisfy the primary service goals set by their hospitals, leaders should focus on enhancing their hospitals’ revenue generation from various sources. The typical mix of hospital revenue streams are, in size order—clinical services, research, philanthropic grants, interest income on cash assets, and royalties from intellectual property. Clinical services and research account for about 95% of the average hospital revenues, with the balance split among the other three.
Hospitals try to boost revenue by adding product lines, enhancing the value of current products, increasing market share, and capitalizing on production efficiencies. Translating business concepts from widgets to wards, increasing both volume and acuity of patient encounters, should be commonplace and a revenue booster. Research revenues are another story, particularly with slowdowns in National Institutes of Health funding. Recruiting hospitalists who want to do research leaves hospitals covering their salaries and labs for long periods of time without revenue generation.
Focusing on proven revenue generators—enhancing the value of current products, increasing market share, and boosting production efficiencies—can help HMG leaders carve out a niche that truly creates value for the hospital.
It may take a lot for an HMG leader to build solid financial performance on a strong clinical foundation, however, it is doable. Dr. Liu sums up how HMG finances will improve: “As hospital medicine matures, expect its leaders to mature as well,” he says. “They will become more business savvy and learn to speak the language of business, even if they have to force themselves to learn.” TH
If ignorance is bliss, then a substantial slice of hospital medicine group (HMG) leaders are in heaven—about finance, that is. Perhaps they didn’t become physicians to solve the sub-prime mortgage mess or take their companies public, as Dr. Adam Singer, MD, CEO of IPC: The Hospitalist Company, did in January 2008.
Dr. Singer, recently named 2008 Physician Entrepreneur of the Year by Modern Physician, always has insisted HMGs can be financially self-supporting. In 2002, he wrote in Physician Executive “when revenue (fees divided by number of patient encounters) exceeds expenses, the practice becomes economically viable.” He calculated that factoring in malpractice insurance, general expenses, 10 percent of revenue for billing and collection, two patient encounters a day per full-time equivalent employee was an HMGs’ break-even point. “Even at a ridiculously minimum encounter volume of two, a hospitalist practice is viable without any outside subsidy,” he concluded. To drive home his point, Dr. Singer suggested HMGs augment their revenues by serving nursing homes and rehab facilities, teaching, securing research grants, medical directorships, and taking on contracts to manage ER unassigned patients.
Nevertheless, a recent Society of Hospital Medicine survey shows a number of HMG leaders lack the basic financial acumen to get and keep their practices fiscally healthy. Data from SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement reveals the vast majority of HMGs fall short of economic independence. Survey results show many HMG leaders’ grasp of basic finance leaves room for improvement.
Key findings include:
- 37% of HMG leaders didn’t know their annual expenses;
- 35% didn’t know their annual professional fee revenues; and
- Among those that didn’t know their expenses and revenues, 85% were operating at a deficit.
Additionally, a negative correlation exists between HMG financial performance and compensation. HMG production remained flat, while average hospitalist compensation increased 13% to $193,000 annually. Cushiony subsidies persist; the survey showed 91% of HMGs receive some form of financial support, an average of $954,000 per group or $97,375 for each full-time physician.
Drilling down into the survey’s financial data, analysis by Joe Miller, SHM Executive Advisor to the CEO, points to an ominous monetary “perfect storm” brewing for HMG leaders. Deficits are growing as hospitalist leaders’ knowledge about their groups’ finances are declining.
The trend data also suggest subsidies obscure declining financial support in several areas. Compared to the 2005-06 SHM survey, the latest survey shows the percentage of HMGs receiving financial support dropped in all five categories in which HMGs receive subsidies. Results from the two most recent surveys showed hospital financial support dropped from 60% to 51%; other support from 17% to 12%; income guarantees fell from 72% to 61%; services in-kind declined from 71% to 60%; and case rates slid from 12% to 11%.
Fuzzy Math?
An oft-cited rationale for hospital medicine’s generous subsidies from other stakeholders is that it “creates value,” in terms of reducing hospital length of stay, costs per case and improved outcomes. Throughout the years, such savings have received increased scrutiny. Blogger and SHM member Dr. Robert Wachter, MD, professor and associated chairman of the Department of Medicine at the University of California, San Francisco, said in May “research on these metrics is disappointing. … The move toward hospitalist shift work and the resulting fragmentation of care during hospitalization may be eroding any slim advantage the model had in cost savings.” He concluded, “the bubble will burst the morning CEOs wake up and realize that there is no longer a shortage of hospitalists.”
Burke Kealey, MD, assistant medical director, Hospital Medicine Division of HealthPartners Medical Group in St. Paul, Minn., offers powerful reasons for why hospitalists struggle with Finance 101:
- Hospitalists have little incentive to meet financial performance targets;
- HMG leaders are too busy with recruiting, scheduling and retention to focus on finance;
- Difficulties obtaining useful data from hospital administrators; and
- Too few business models that centralize data from multiple hospitals, making financial analysis of an individual group difficult.
To address the needs, Dr. Kealey, who chairs SHM’s Practice Analysis Committee, has spearheaded SHM’s development of dashboards that utilize performance metrics, such as volume data, case mix, length of stay, resource utilization, productivity, and readmission rates, to help leaders guide a practice to economic health.
Steve Liu, MD, the CEO and founder of Ingenious Med, is a hospitalist in one of the nation’s largest HMGs, with 100,000-plus patient encounters annually at Emory Healthcare in Atlanta. A member of SHM’s Benchmarks Committee, Liu puts HMG leaders’ financial ignorance in the context of a growth industry. “Hospital medicine is young, it’s moving very fast, and it is filled with a youngish crowd who don’t feel they have enough time to focus on financial deficits and inefficiencies,” Dr. Liu says.
Still, a lack of financial knowledge can trip up the best of physician. Dr. Liu advises hospitalist leaders to focus on professional fee revenues, particularly on fees collected per full-time equivalent employee (FTE); eliminating high expenses from inefficiencies; and checking local and national compensation packages to address what he estimates as 30 percent of HMGs who fail to pay physicians appropriately. Other financial mistakes, he says, are HMG leaders throwing warm bodies at problems without enough back-office support; agreeing to see more patients than they can handle in a day; overspending on recruiters; and failure to understand each full-time employee’s return on investment.
Numerous hospitalists, according to Dr. Liu, believe they don’t have enough time to build partnerships with administrators that would lead to more sharing of financial data. “They may even be in a power struggle with administrators over access to financial data. … If you can’t measure it, you can’t manage it. That’s the essence of Finance 101,” Dr. Liu says, “and it’s very frustrating to hospitalists who don’t have the business skill sets and tools to succeed financially.” Since data is power, it’s imperative to ask the chief financial officer (CFO) for data; that way the HMG can work toward profitability.
Making sense of financial data is critical, says Leslie Flores, director of SHM’s Practice Management Institute. “HMG leaders have to learn to take data, such as number of encounters, relative value units, average daily census, number of days worked per year, the total subsidy for the practice, and average subsidy per hospitalist, and make sense of it. Where do the numbers come from and what do they mean are critical questions,” she says.
Big Picture
SHM’s most recent survey reflects the average hospitalist medicine group’s business model. Production is flat; compensation is up 13%; and 91% of HMGs receive subsidies nearing $1 million each. From a dollars-and-sense vantage point, the business case for hospital medicine doesn’t work. So why do hospitals go along with a broken business model, especially at a time when a hospital’s cost curve is growing faster than its revenue curve, making it even more difficult to justify HMG subsidies?
The short answer is that most hospital medicine programs are invited in by hospital administrators and serve a specific purpose related to overall revenue generation and/or cost controls. Common reasons for creating hospitalist programs are improving Emergency Department throughput, relieving community-based physicians from hospital duties, boosting subspecialist revenues with medical co-management, and cost cutting through reduced length of stay and improved resource utilization. Each has different financial metrics associated with it, and HMG leaders should understand each metric thoroughly.
If, for example, relieving the pressure on community-based doctors is the HMG’s primary goal, an HMG leader’s strategy might be to attract the best hospitalists available, offering a high compensation package and recruiting bonus. That would help cover the increased patient load, but it might pressure the hospital to shoulder a steep subsidy.
Alternatively, relying on financial and performance metrics might yield better rules about when to justify a new hire. Seasoned HMG leaders would rely on a group’s average daily census of 50 to 70 patients as the tipping point for adding a FTE hospitalist. Similarly, night admissions of 10 to 14 patients should trigger the hiring of a nocturnist, with his or her premium pay.
Brian Bossard, MD, founder of Inpatient Physicians Associates in Lincoln, Neb., relies on that type of data and other “lean” management concepts. To optimize each physicians’ patient loads and productivity, he has patients assigned by physical proximity, so his hospitalists won’t waste time running around the hospital seeing patients. Saving time and manpower contributes to an HMG’s financial health.
Once HMGs satisfy the primary service goals set by their hospitals, leaders should focus on enhancing their hospitals’ revenue generation from various sources. The typical mix of hospital revenue streams are, in size order—clinical services, research, philanthropic grants, interest income on cash assets, and royalties from intellectual property. Clinical services and research account for about 95% of the average hospital revenues, with the balance split among the other three.
Hospitals try to boost revenue by adding product lines, enhancing the value of current products, increasing market share, and capitalizing on production efficiencies. Translating business concepts from widgets to wards, increasing both volume and acuity of patient encounters, should be commonplace and a revenue booster. Research revenues are another story, particularly with slowdowns in National Institutes of Health funding. Recruiting hospitalists who want to do research leaves hospitals covering their salaries and labs for long periods of time without revenue generation.
Focusing on proven revenue generators—enhancing the value of current products, increasing market share, and boosting production efficiencies—can help HMG leaders carve out a niche that truly creates value for the hospital.
It may take a lot for an HMG leader to build solid financial performance on a strong clinical foundation, however, it is doable. Dr. Liu sums up how HMG finances will improve: “As hospital medicine matures, expect its leaders to mature as well,” he says. “They will become more business savvy and learn to speak the language of business, even if they have to force themselves to learn.” TH