User login
The phone rang at 6 a.m. on a cold, stormy winter morning. It was a consult: Would I come see a patient in the ICU? I was in my second year of nephrology fellowship, moonlighting out on the frozen tundra of Minnesota. It was Garrison Keillor country, and—as he says about Lake Wobegon—on that day the woman was strong, but I was one man who was not looking too good. I rolled over and brought up the labs on my bedside computer. The patient’s potassium was 7.8 mmol/L; she also had a creatinine of 6.1 mg/dL, a bicarbonate of 8 mmol/L, and a blood urea nitrogen (BUN) more than 140 mg/dL.
This was a small community hospital with no dialysis facility, and my first thought was that it was time to warm up the Medevac helicopter. I could envision the flight nurses loading the patient and saying, “Welcome aboard Medevac One. Today we will be serving normal saline, insulin, and glucose. Sit back and enjoy the flight, and thank you for choosing Medevac One.” One look outside at the flying snow canceled that plan. I went to see the patient.
One of the first symptoms of uremia is anorexia, and the patient will frequently self-avert from taking protein—sort of a survival mechanism in an attempt to control uremia. I arrived in the ICU to find a woman finishing off a plate of bacon and eggs. She told me she had had a gynecologic procedure done a little over a week before. The pain had been intolerable during the past week. She had not felt like eating or drinking and had been taking a lot of ibuprofen. It was the pain that had brought her to the emergency department, and the narcotics had worked wonders. She was finally feeling well enough to eat. Her ECG was stone-cold unchanged from one obtained pre-operatively.
I treated immediately with intravenous insulin, dextrose, and sodium polystyrene sulfonate. By exam she was volume depleted, and her urine output overnight was less than 10 mL per hour. An arterial blood gas demonstrated a significant mixed acidemia; both anion and nonanion gap acidosis were present. I used a bolus of bicarbonate solution, and the urine output in one hour was 50 mL. This was better, and she had just proven to me that she could make urine. Great news for a nephrologist in training! I ordered a constant infusion of bicarbonate.
Despite these labs, she was hypertensive, so I ordered furosemide—200 mg IV—to attempt a forced diuresis. After another hour, the urine output was 200 mL, and I was much more comfortable. Hyperkalemia is much easier to control when a patient is nonoliguric, and I continued aggressive fluid administration. Within four hours, the patient’s potassium and the acidemia were much improved. By the end of my shift, the potassium was within normal range, the creatinine and BUN had also improved significantly, and the patient was transferred to the medical floor.
This patient’s story illustrates the potential difficulties involved in diagnosing and treating potassium-related problems. With these challenges in mind, here are 10 pieces of information every hospitalist should have when dealing with this type of patient.
1) Hyperkalemia in the patient with acute renal failure is usually a problem of poor perfusion; acute decreases in glomerular filtration rate (GFR) that occur in acute renal failure could lead to a marked decrease in sodium and water at the distal tubule, which might decrease distal potassium secretion.
When acute renal failure is oliguric, distal delivery of sodium and water is low, and hyperkalemia is a frequent problem. What to do? If respiratory status allows, add aggressive volume resuscitation to your medical management. If the patient’s urine output increases, or when acute renal failure is nonoliguric, distal delivery is usually sufficient and hyperkalemia is less of an issue. Concerned about giving IV fluids to an oliguric patient? Medical management is a temporizing measure in the oliguric patient, and hyperkalemia will always be difficult to treat; a fluid challenge might be worthwhile prior to initiating hemodialysis. Urgent dialysis might be hours away, but fluids can be started within minutes.
If hemodynamics allow, I start forced diuresis with high-dose loop diuretics in an attempt to convert to nonoliguria and promote renal potassium excretion. In life-threatening hyperkalemia all is fair, and—once a patient is nonoliguric—hyperkalemia is much easier to manage.
2) A little potassium is not always bad. There is robust evidence supporting the use of angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARB) in patients with chronic kidney disease with both diabetic and non-diabetic causes. In most patients, according to the National Kidney Foundation’s Clinical Guidelines, the ACE inhibitor or ARB can be continued if the GFR decline over four months is <30% from baseline value and serum potassium is equal to 5.5 mEq/L. The proper way for the inpatient physician to initiate treatment with an ACE inhibitor or ARB is to start at a low dose, with follow-up in one week for a serum potassium measurement and titration of dose as necessary.
3) During my fellowship, I had an attending who would start a discussion with the phrase “I’m just a dumb nephrologist” and then talk for 25 minutes about the physiology of, theories about, and potential therapeutic interventions for just about any type of kidney disease. I prefer a simple approach, too: insulin and dextrose. Why? Because it works well on just about all patients and is quick to administer. Just about every hospital floor in America has a supply of insulin and dextrose on hand. Give the order and, in most cases, the patient is receiving treatment in a matter of minutes.
4) Sodium bicarbonate buffers hydrogen ions extracellularly while shifting potassium intracellularly to maintain electrical neutrality. Sodium bicarbonate should be reserved for cases with severe metabolic acidosis, because effects might be delayed or unreliable, especially in patients with chronic kidney disease.
5) Beta-2 adrenergic agonists drive potassium intracellularly via the Na,K-ATPase mechanism. Albuterol is most commonly used; however, the dosage used by clinicians is frequently insufficient. A dose of albuterol that is 10–20 mg via nebulizer is required, and response time to lowering of potassium might be up to 90 minutes.1
6) I am often asked what ECG changes need to be present before I recommend treatment of hyperkalemia with calcium chloride or calcium gluconate. In a patient without central venous access the concern is that peripheral intravenous infusions of calcium might extravasate, leading to local cellular necrosis and possible loss of limb.
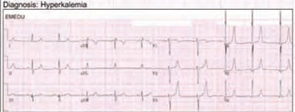
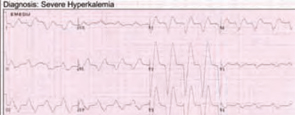
The answer I give is that I don’t know what exact ECG changes would benefit from treatment versus no treatment. In fact, patients with life-threatening hyperkalemia might have subtle changes on ECG.2 Therefore, I believe that every patient with electrocardiographic manifestations of hyperkalemia can be treated with calcium infusion. In my mind, the outcome of sudden cardiac death is far worse than the possible negative effects of calcium infusion.
7) If you suspect a renal cause for a potassium derangement, please check the urine electrolytes. This test is best done at the time of admission or when the patient is in a steady state. As a practicing nephrologist, I find that most of my consults for electrolyte abnormalities are for the patient with a chronic potassium abnormality. I am usually called on the second or third day, when the patient has received a multitude of IV fluids, treatment, medication changes, and so on. All too often, no urine studies have been obtained at the time of consultation. Would you consult your cardiologist for chest pain without first obtaining an ECG?
8) Normally, when blood is drawn and allowed to clot before centrifugation, enough potassium is released from platelets to raise the serum level by approximately 0.5 mEq/L. This is accounted for within the limits of the normal range. Excessive errors could occur, however, in the presence of marked leukocytosis or thrombocytosis. These conditions are referred to as pseudohyperkalemia. This can be confirmed by remeasuring serum potassium in a blood sample collected in a heparinized sample tube.3
9) Oral sodium phosphate is a cathartic used in bowel preparation prior to colonoscopy. This agent has been associated with changes in serum electrolyte levels that are generally within the normal range but could occasionally cause serious electrolyte disturbances. Significant hypokalemia could develop, particularly in the elderly, and is due to intestinal potassium loss.4
Other abnormalities reported include hyperphosphatemia, hypocalcemia, and hypernatremia. In addition to increased age, risk factors for these disturbances include the presence of bowel obstruction, poor gut motility, and unrecognized renal disease. Additionally, phosphate nephropathy has been well reported after administration of sodium phosphate and might cause irreversible kidney disease with histology resembling nephrocalcinosis.5
10) The most commonly used cation-exchange resin, sodium polystyrene sulfonate, is frequently used to manage hyperkalemia in patients with chronic kidney disease. Use of this resin could result in hypokalemia, hypomagnesemia, and—occasionally—metabolic alkalosis. After the oral administration of this drug, sodium is released from the resin in exchange for hydrogen in the gastric juice. As the resin passes through the rest of the gastrointestinal tract, the hydrogen is then exchanged for other cations, including potassium, which is present in greater quantities, particularly in the distal gut. Potassium binding to the resin is influenced by duration of exposure, which is primarily determined by gut transit time.
The primary potential complication of using sodium polystyrene sulfonate is the development of sodium overload. The absorption of sodium from the resin by the gut might lead to heart failure, hypertension, and occasionally hypernatremia. Because the resin binds other divalent cations, hypocalcemia and hypomagnesemia could also develop. Decreased plasma levels of magnesium and calcium are more likely to occur in patients taking diuretics or in those with poor nutrition.6 Use of the resin could also lead to metabolic alkalosis when administered with antacids or phosphate binders such as magnesium hydroxide or calcium carbonate. As magnesium and calcium bind to the resin, the base is then free to be absorbed into the systemic circulation. TH
Dr. Casey works in the Department of Internal Medicine, Section of Hospital Internal Medicine, Division of Nephrology and Hypertension at the Mayo Clinic, Rochester, Minn.
References
- Liou HH, Chiang SS, Wu SC, et al. Hypokalemic effects of intravenous infusion or nebulization of salbutamol in patients with chronic renal failure: comparative study. Am J Kidney Dis. 1994 Feb;23(2):266-271.
- Martinez-Vea A, Bardaji A, Garcia C, et al. Severe hyperkalemia with minimal electrocardiographic manifestations: a report of seven cases. J Electrocardiol. 1999 Jan;32(1):45-49.
- Stankovic AK, Smith S. Elevated serum potassium values: the role of preanalytic variables. Am J Clin Pathol. 2004 Jun;121 Suppl:S105–S112.
- Beloosesky Y, Grinblat J, Weiss A, et al. Electrolyte disorders following oral sodium phosphate administration for bowel cleansing in elderly patients. Arch Intern Med. 2003 Apr 14;163(7):803–808.
- Curran MP, Plosker GL. Oral sodium phosphate solution: a review of its use as a colorectal cleanser. Drugs. 2004;64(15):1697-1714.
- Chen CC, Chen CA, Chau T, et al. Hypokalaemia and hypomagnesaemia in an oedematous diabetic patient with advanced renal failure. Nephrol Dial Transplant. 2005 Oct;20(10):2271-2273.
The phone rang at 6 a.m. on a cold, stormy winter morning. It was a consult: Would I come see a patient in the ICU? I was in my second year of nephrology fellowship, moonlighting out on the frozen tundra of Minnesota. It was Garrison Keillor country, and—as he says about Lake Wobegon—on that day the woman was strong, but I was one man who was not looking too good. I rolled over and brought up the labs on my bedside computer. The patient’s potassium was 7.8 mmol/L; she also had a creatinine of 6.1 mg/dL, a bicarbonate of 8 mmol/L, and a blood urea nitrogen (BUN) more than 140 mg/dL.
This was a small community hospital with no dialysis facility, and my first thought was that it was time to warm up the Medevac helicopter. I could envision the flight nurses loading the patient and saying, “Welcome aboard Medevac One. Today we will be serving normal saline, insulin, and glucose. Sit back and enjoy the flight, and thank you for choosing Medevac One.” One look outside at the flying snow canceled that plan. I went to see the patient.
One of the first symptoms of uremia is anorexia, and the patient will frequently self-avert from taking protein—sort of a survival mechanism in an attempt to control uremia. I arrived in the ICU to find a woman finishing off a plate of bacon and eggs. She told me she had had a gynecologic procedure done a little over a week before. The pain had been intolerable during the past week. She had not felt like eating or drinking and had been taking a lot of ibuprofen. It was the pain that had brought her to the emergency department, and the narcotics had worked wonders. She was finally feeling well enough to eat. Her ECG was stone-cold unchanged from one obtained pre-operatively.
I treated immediately with intravenous insulin, dextrose, and sodium polystyrene sulfonate. By exam she was volume depleted, and her urine output overnight was less than 10 mL per hour. An arterial blood gas demonstrated a significant mixed acidemia; both anion and nonanion gap acidosis were present. I used a bolus of bicarbonate solution, and the urine output in one hour was 50 mL. This was better, and she had just proven to me that she could make urine. Great news for a nephrologist in training! I ordered a constant infusion of bicarbonate.
Despite these labs, she was hypertensive, so I ordered furosemide—200 mg IV—to attempt a forced diuresis. After another hour, the urine output was 200 mL, and I was much more comfortable. Hyperkalemia is much easier to control when a patient is nonoliguric, and I continued aggressive fluid administration. Within four hours, the patient’s potassium and the acidemia were much improved. By the end of my shift, the potassium was within normal range, the creatinine and BUN had also improved significantly, and the patient was transferred to the medical floor.
This patient’s story illustrates the potential difficulties involved in diagnosing and treating potassium-related problems. With these challenges in mind, here are 10 pieces of information every hospitalist should have when dealing with this type of patient.
1) Hyperkalemia in the patient with acute renal failure is usually a problem of poor perfusion; acute decreases in glomerular filtration rate (GFR) that occur in acute renal failure could lead to a marked decrease in sodium and water at the distal tubule, which might decrease distal potassium secretion.
When acute renal failure is oliguric, distal delivery of sodium and water is low, and hyperkalemia is a frequent problem. What to do? If respiratory status allows, add aggressive volume resuscitation to your medical management. If the patient’s urine output increases, or when acute renal failure is nonoliguric, distal delivery is usually sufficient and hyperkalemia is less of an issue. Concerned about giving IV fluids to an oliguric patient? Medical management is a temporizing measure in the oliguric patient, and hyperkalemia will always be difficult to treat; a fluid challenge might be worthwhile prior to initiating hemodialysis. Urgent dialysis might be hours away, but fluids can be started within minutes.
If hemodynamics allow, I start forced diuresis with high-dose loop diuretics in an attempt to convert to nonoliguria and promote renal potassium excretion. In life-threatening hyperkalemia all is fair, and—once a patient is nonoliguric—hyperkalemia is much easier to manage.
2) A little potassium is not always bad. There is robust evidence supporting the use of angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARB) in patients with chronic kidney disease with both diabetic and non-diabetic causes. In most patients, according to the National Kidney Foundation’s Clinical Guidelines, the ACE inhibitor or ARB can be continued if the GFR decline over four months is <30% from baseline value and serum potassium is equal to 5.5 mEq/L. The proper way for the inpatient physician to initiate treatment with an ACE inhibitor or ARB is to start at a low dose, with follow-up in one week for a serum potassium measurement and titration of dose as necessary.
3) During my fellowship, I had an attending who would start a discussion with the phrase “I’m just a dumb nephrologist” and then talk for 25 minutes about the physiology of, theories about, and potential therapeutic interventions for just about any type of kidney disease. I prefer a simple approach, too: insulin and dextrose. Why? Because it works well on just about all patients and is quick to administer. Just about every hospital floor in America has a supply of insulin and dextrose on hand. Give the order and, in most cases, the patient is receiving treatment in a matter of minutes.
4) Sodium bicarbonate buffers hydrogen ions extracellularly while shifting potassium intracellularly to maintain electrical neutrality. Sodium bicarbonate should be reserved for cases with severe metabolic acidosis, because effects might be delayed or unreliable, especially in patients with chronic kidney disease.
5) Beta-2 adrenergic agonists drive potassium intracellularly via the Na,K-ATPase mechanism. Albuterol is most commonly used; however, the dosage used by clinicians is frequently insufficient. A dose of albuterol that is 10–20 mg via nebulizer is required, and response time to lowering of potassium might be up to 90 minutes.1
6) I am often asked what ECG changes need to be present before I recommend treatment of hyperkalemia with calcium chloride or calcium gluconate. In a patient without central venous access the concern is that peripheral intravenous infusions of calcium might extravasate, leading to local cellular necrosis and possible loss of limb.
The answer I give is that I don’t know what exact ECG changes would benefit from treatment versus no treatment. In fact, patients with life-threatening hyperkalemia might have subtle changes on ECG.2 Therefore, I believe that every patient with electrocardiographic manifestations of hyperkalemia can be treated with calcium infusion. In my mind, the outcome of sudden cardiac death is far worse than the possible negative effects of calcium infusion.
7) If you suspect a renal cause for a potassium derangement, please check the urine electrolytes. This test is best done at the time of admission or when the patient is in a steady state. As a practicing nephrologist, I find that most of my consults for electrolyte abnormalities are for the patient with a chronic potassium abnormality. I am usually called on the second or third day, when the patient has received a multitude of IV fluids, treatment, medication changes, and so on. All too often, no urine studies have been obtained at the time of consultation. Would you consult your cardiologist for chest pain without first obtaining an ECG?
8) Normally, when blood is drawn and allowed to clot before centrifugation, enough potassium is released from platelets to raise the serum level by approximately 0.5 mEq/L. This is accounted for within the limits of the normal range. Excessive errors could occur, however, in the presence of marked leukocytosis or thrombocytosis. These conditions are referred to as pseudohyperkalemia. This can be confirmed by remeasuring serum potassium in a blood sample collected in a heparinized sample tube.3
9) Oral sodium phosphate is a cathartic used in bowel preparation prior to colonoscopy. This agent has been associated with changes in serum electrolyte levels that are generally within the normal range but could occasionally cause serious electrolyte disturbances. Significant hypokalemia could develop, particularly in the elderly, and is due to intestinal potassium loss.4
Other abnormalities reported include hyperphosphatemia, hypocalcemia, and hypernatremia. In addition to increased age, risk factors for these disturbances include the presence of bowel obstruction, poor gut motility, and unrecognized renal disease. Additionally, phosphate nephropathy has been well reported after administration of sodium phosphate and might cause irreversible kidney disease with histology resembling nephrocalcinosis.5
10) The most commonly used cation-exchange resin, sodium polystyrene sulfonate, is frequently used to manage hyperkalemia in patients with chronic kidney disease. Use of this resin could result in hypokalemia, hypomagnesemia, and—occasionally—metabolic alkalosis. After the oral administration of this drug, sodium is released from the resin in exchange for hydrogen in the gastric juice. As the resin passes through the rest of the gastrointestinal tract, the hydrogen is then exchanged for other cations, including potassium, which is present in greater quantities, particularly in the distal gut. Potassium binding to the resin is influenced by duration of exposure, which is primarily determined by gut transit time.
The primary potential complication of using sodium polystyrene sulfonate is the development of sodium overload. The absorption of sodium from the resin by the gut might lead to heart failure, hypertension, and occasionally hypernatremia. Because the resin binds other divalent cations, hypocalcemia and hypomagnesemia could also develop. Decreased plasma levels of magnesium and calcium are more likely to occur in patients taking diuretics or in those with poor nutrition.6 Use of the resin could also lead to metabolic alkalosis when administered with antacids or phosphate binders such as magnesium hydroxide or calcium carbonate. As magnesium and calcium bind to the resin, the base is then free to be absorbed into the systemic circulation. TH
Dr. Casey works in the Department of Internal Medicine, Section of Hospital Internal Medicine, Division of Nephrology and Hypertension at the Mayo Clinic, Rochester, Minn.
References
- Liou HH, Chiang SS, Wu SC, et al. Hypokalemic effects of intravenous infusion or nebulization of salbutamol in patients with chronic renal failure: comparative study. Am J Kidney Dis. 1994 Feb;23(2):266-271.
- Martinez-Vea A, Bardaji A, Garcia C, et al. Severe hyperkalemia with minimal electrocardiographic manifestations: a report of seven cases. J Electrocardiol. 1999 Jan;32(1):45-49.
- Stankovic AK, Smith S. Elevated serum potassium values: the role of preanalytic variables. Am J Clin Pathol. 2004 Jun;121 Suppl:S105–S112.
- Beloosesky Y, Grinblat J, Weiss A, et al. Electrolyte disorders following oral sodium phosphate administration for bowel cleansing in elderly patients. Arch Intern Med. 2003 Apr 14;163(7):803–808.
- Curran MP, Plosker GL. Oral sodium phosphate solution: a review of its use as a colorectal cleanser. Drugs. 2004;64(15):1697-1714.
- Chen CC, Chen CA, Chau T, et al. Hypokalaemia and hypomagnesaemia in an oedematous diabetic patient with advanced renal failure. Nephrol Dial Transplant. 2005 Oct;20(10):2271-2273.
The phone rang at 6 a.m. on a cold, stormy winter morning. It was a consult: Would I come see a patient in the ICU? I was in my second year of nephrology fellowship, moonlighting out on the frozen tundra of Minnesota. It was Garrison Keillor country, and—as he says about Lake Wobegon—on that day the woman was strong, but I was one man who was not looking too good. I rolled over and brought up the labs on my bedside computer. The patient’s potassium was 7.8 mmol/L; she also had a creatinine of 6.1 mg/dL, a bicarbonate of 8 mmol/L, and a blood urea nitrogen (BUN) more than 140 mg/dL.
This was a small community hospital with no dialysis facility, and my first thought was that it was time to warm up the Medevac helicopter. I could envision the flight nurses loading the patient and saying, “Welcome aboard Medevac One. Today we will be serving normal saline, insulin, and glucose. Sit back and enjoy the flight, and thank you for choosing Medevac One.” One look outside at the flying snow canceled that plan. I went to see the patient.
One of the first symptoms of uremia is anorexia, and the patient will frequently self-avert from taking protein—sort of a survival mechanism in an attempt to control uremia. I arrived in the ICU to find a woman finishing off a plate of bacon and eggs. She told me she had had a gynecologic procedure done a little over a week before. The pain had been intolerable during the past week. She had not felt like eating or drinking and had been taking a lot of ibuprofen. It was the pain that had brought her to the emergency department, and the narcotics had worked wonders. She was finally feeling well enough to eat. Her ECG was stone-cold unchanged from one obtained pre-operatively.
I treated immediately with intravenous insulin, dextrose, and sodium polystyrene sulfonate. By exam she was volume depleted, and her urine output overnight was less than 10 mL per hour. An arterial blood gas demonstrated a significant mixed acidemia; both anion and nonanion gap acidosis were present. I used a bolus of bicarbonate solution, and the urine output in one hour was 50 mL. This was better, and she had just proven to me that she could make urine. Great news for a nephrologist in training! I ordered a constant infusion of bicarbonate.
Despite these labs, she was hypertensive, so I ordered furosemide—200 mg IV—to attempt a forced diuresis. After another hour, the urine output was 200 mL, and I was much more comfortable. Hyperkalemia is much easier to control when a patient is nonoliguric, and I continued aggressive fluid administration. Within four hours, the patient’s potassium and the acidemia were much improved. By the end of my shift, the potassium was within normal range, the creatinine and BUN had also improved significantly, and the patient was transferred to the medical floor.
This patient’s story illustrates the potential difficulties involved in diagnosing and treating potassium-related problems. With these challenges in mind, here are 10 pieces of information every hospitalist should have when dealing with this type of patient.
1) Hyperkalemia in the patient with acute renal failure is usually a problem of poor perfusion; acute decreases in glomerular filtration rate (GFR) that occur in acute renal failure could lead to a marked decrease in sodium and water at the distal tubule, which might decrease distal potassium secretion.
When acute renal failure is oliguric, distal delivery of sodium and water is low, and hyperkalemia is a frequent problem. What to do? If respiratory status allows, add aggressive volume resuscitation to your medical management. If the patient’s urine output increases, or when acute renal failure is nonoliguric, distal delivery is usually sufficient and hyperkalemia is less of an issue. Concerned about giving IV fluids to an oliguric patient? Medical management is a temporizing measure in the oliguric patient, and hyperkalemia will always be difficult to treat; a fluid challenge might be worthwhile prior to initiating hemodialysis. Urgent dialysis might be hours away, but fluids can be started within minutes.
If hemodynamics allow, I start forced diuresis with high-dose loop diuretics in an attempt to convert to nonoliguria and promote renal potassium excretion. In life-threatening hyperkalemia all is fair, and—once a patient is nonoliguric—hyperkalemia is much easier to manage.
2) A little potassium is not always bad. There is robust evidence supporting the use of angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARB) in patients with chronic kidney disease with both diabetic and non-diabetic causes. In most patients, according to the National Kidney Foundation’s Clinical Guidelines, the ACE inhibitor or ARB can be continued if the GFR decline over four months is <30% from baseline value and serum potassium is equal to 5.5 mEq/L. The proper way for the inpatient physician to initiate treatment with an ACE inhibitor or ARB is to start at a low dose, with follow-up in one week for a serum potassium measurement and titration of dose as necessary.
3) During my fellowship, I had an attending who would start a discussion with the phrase “I’m just a dumb nephrologist” and then talk for 25 minutes about the physiology of, theories about, and potential therapeutic interventions for just about any type of kidney disease. I prefer a simple approach, too: insulin and dextrose. Why? Because it works well on just about all patients and is quick to administer. Just about every hospital floor in America has a supply of insulin and dextrose on hand. Give the order and, in most cases, the patient is receiving treatment in a matter of minutes.
4) Sodium bicarbonate buffers hydrogen ions extracellularly while shifting potassium intracellularly to maintain electrical neutrality. Sodium bicarbonate should be reserved for cases with severe metabolic acidosis, because effects might be delayed or unreliable, especially in patients with chronic kidney disease.
5) Beta-2 adrenergic agonists drive potassium intracellularly via the Na,K-ATPase mechanism. Albuterol is most commonly used; however, the dosage used by clinicians is frequently insufficient. A dose of albuterol that is 10–20 mg via nebulizer is required, and response time to lowering of potassium might be up to 90 minutes.1
6) I am often asked what ECG changes need to be present before I recommend treatment of hyperkalemia with calcium chloride or calcium gluconate. In a patient without central venous access the concern is that peripheral intravenous infusions of calcium might extravasate, leading to local cellular necrosis and possible loss of limb.
The answer I give is that I don’t know what exact ECG changes would benefit from treatment versus no treatment. In fact, patients with life-threatening hyperkalemia might have subtle changes on ECG.2 Therefore, I believe that every patient with electrocardiographic manifestations of hyperkalemia can be treated with calcium infusion. In my mind, the outcome of sudden cardiac death is far worse than the possible negative effects of calcium infusion.
7) If you suspect a renal cause for a potassium derangement, please check the urine electrolytes. This test is best done at the time of admission or when the patient is in a steady state. As a practicing nephrologist, I find that most of my consults for electrolyte abnormalities are for the patient with a chronic potassium abnormality. I am usually called on the second or third day, when the patient has received a multitude of IV fluids, treatment, medication changes, and so on. All too often, no urine studies have been obtained at the time of consultation. Would you consult your cardiologist for chest pain without first obtaining an ECG?
8) Normally, when blood is drawn and allowed to clot before centrifugation, enough potassium is released from platelets to raise the serum level by approximately 0.5 mEq/L. This is accounted for within the limits of the normal range. Excessive errors could occur, however, in the presence of marked leukocytosis or thrombocytosis. These conditions are referred to as pseudohyperkalemia. This can be confirmed by remeasuring serum potassium in a blood sample collected in a heparinized sample tube.3
9) Oral sodium phosphate is a cathartic used in bowel preparation prior to colonoscopy. This agent has been associated with changes in serum electrolyte levels that are generally within the normal range but could occasionally cause serious electrolyte disturbances. Significant hypokalemia could develop, particularly in the elderly, and is due to intestinal potassium loss.4
Other abnormalities reported include hyperphosphatemia, hypocalcemia, and hypernatremia. In addition to increased age, risk factors for these disturbances include the presence of bowel obstruction, poor gut motility, and unrecognized renal disease. Additionally, phosphate nephropathy has been well reported after administration of sodium phosphate and might cause irreversible kidney disease with histology resembling nephrocalcinosis.5
10) The most commonly used cation-exchange resin, sodium polystyrene sulfonate, is frequently used to manage hyperkalemia in patients with chronic kidney disease. Use of this resin could result in hypokalemia, hypomagnesemia, and—occasionally—metabolic alkalosis. After the oral administration of this drug, sodium is released from the resin in exchange for hydrogen in the gastric juice. As the resin passes through the rest of the gastrointestinal tract, the hydrogen is then exchanged for other cations, including potassium, which is present in greater quantities, particularly in the distal gut. Potassium binding to the resin is influenced by duration of exposure, which is primarily determined by gut transit time.
The primary potential complication of using sodium polystyrene sulfonate is the development of sodium overload. The absorption of sodium from the resin by the gut might lead to heart failure, hypertension, and occasionally hypernatremia. Because the resin binds other divalent cations, hypocalcemia and hypomagnesemia could also develop. Decreased plasma levels of magnesium and calcium are more likely to occur in patients taking diuretics or in those with poor nutrition.6 Use of the resin could also lead to metabolic alkalosis when administered with antacids or phosphate binders such as magnesium hydroxide or calcium carbonate. As magnesium and calcium bind to the resin, the base is then free to be absorbed into the systemic circulation. TH
Dr. Casey works in the Department of Internal Medicine, Section of Hospital Internal Medicine, Division of Nephrology and Hypertension at the Mayo Clinic, Rochester, Minn.
References
- Liou HH, Chiang SS, Wu SC, et al. Hypokalemic effects of intravenous infusion or nebulization of salbutamol in patients with chronic renal failure: comparative study. Am J Kidney Dis. 1994 Feb;23(2):266-271.
- Martinez-Vea A, Bardaji A, Garcia C, et al. Severe hyperkalemia with minimal electrocardiographic manifestations: a report of seven cases. J Electrocardiol. 1999 Jan;32(1):45-49.
- Stankovic AK, Smith S. Elevated serum potassium values: the role of preanalytic variables. Am J Clin Pathol. 2004 Jun;121 Suppl:S105–S112.
- Beloosesky Y, Grinblat J, Weiss A, et al. Electrolyte disorders following oral sodium phosphate administration for bowel cleansing in elderly patients. Arch Intern Med. 2003 Apr 14;163(7):803–808.
- Curran MP, Plosker GL. Oral sodium phosphate solution: a review of its use as a colorectal cleanser. Drugs. 2004;64(15):1697-1714.
- Chen CC, Chen CA, Chau T, et al. Hypokalaemia and hypomagnesaemia in an oedematous diabetic patient with advanced renal failure. Nephrol Dial Transplant. 2005 Oct;20(10):2271-2273.