User login
Negative symptoms are the major contributor to low function levels and debilitation in most patients with schizophrenia. Poorly motivated patients cannot function adequately at school or work. Relationships with family and friends decay in the face of unresponsive affect and inattention to social cues. Personal interests yield to the dampening influences of anhedonia, apathy, and inattention.
Yet because active psychosis is the most common cause of hospital admission, a primary goal of treatment—and sometimes the only objective of pharmacologic treatment—is to eliminate or reduce positive symptoms. And although controlling positive symptoms is remarkably effective in reducing hospitalizations, patients’ functional capacity improves only minimally as psychosis abates. Even with optimal antipsychotic treatment, negative symptoms tend to persist.
For psychiatrists, the three major challenges of schizophrenia’s negative symptoms are their modest therapeutic response, pervasiveness, and diminution of patients’ quality of life. To help you manage negative symptoms, we suggest the following approach to their assessment and treatment.
Importance of negative symptoms
Schizophrenia is a heterogeneous disorder characterized by positive, negative, cognitive, and mood symptoms. The relative severity of these four pathologic domains varies from case to case and within the same individual over time. Though related, these domains have distinct underlying mechanisms and are differentially related to functional capacity and quality of life. They also show different patterns of response to treatment. Whereas positive symptoms refer to new psychological experiences outside the range of normal (e.g., delusions, hallucinations, suspiciousness, disorganized thinking), negative symptoms represent loss of normal function.
Negative symptoms include blunting of affect, poverty of speech and thought, apathy, anhedonia, reduced social drive, loss of motivation, lack of social interest, and inattention to social or cognitive input. These symptoms have devastating consequences on patients’ lives, and only modest progress has been made in treating them effectively.
From negative to positive. Early investigators1,2 considered negative symptoms to represent the fundamental defect of schizophrenia. Over the years, however, the importance of negative symptoms was progressively downplayed. Positive symptoms were increasingly emphasized because:
- positive symptoms have a more dramatic and easily recognized presentation
- negative symptoms are more difficult to reliably define and document
- antipsychotics, which revolutionized schizophrenia treatment, produce their most dramatic improvement in positive symptoms.
Renewed interest. The almost universal presence and relative persistence of negative symptoms, and the fact that they represent the most debilitating and refractory aspect of schizophrenic psychopathology, make them difficult to ignore. Consequently, interest in negative symptoms resurged in the 1980s-90s, with intense efforts to better understand them and treat them more effectively.3-5
Table
SCHIZOPHRENIA’S NEGATIVE SYMPTOMS: PRIMARY AND SECONDARY COMPONENTS
| Primary Associated with positive symptoms Deficit or primary enduring symptoms (premorbid and deteriorative) |
| Secondary Associated with extrapyramidal symptoms, depression, or environmental deprivation |
| Source: Adapted from DeQuardo JR, Tandon R. J Psychiatr Res 1998;32 (3-4):229-42. |
Negative symptoms are now better (but still incompletely) understood, and their treatment has improved but is still inadequate. Because intense effort yielded only modest success, researchers and clinicians have again begun to pay less attention to negative symptoms and shifted their focus to cognition in schizophrenia. Negative symptoms remain relevant, however, because they constitute the main barrier to a better quality of life for patients with schizophrenia.
Assessment for negative symptoms
The four major clinical subgroups of negative symptoms are affective, communicative, conational, and relational.
Affective. Blunted affect—including deficits in facial expression, eye contact, gestures, and voice pattern—is perhaps the most conspicuous negative symptom. In mild form, gestures may seem artificial or mechanical, and the voice is stilted or lacks normal inflection. Patients with severe blunted affect may appear devoid of facial expression or communicative gestures. They may sit impassively with little spontaneous movement, speak in a monotone, and gaze blankly in no particular direction.
Even when conversation becomes emotional, the patient’s affect does not adjust appropriately to reflect his or her feelings. Nor does the patient display even a basic level of understanding or responsiveness that typically characterize casual human interactions. The ability to experience pleasure (anhedonia) and sense of caring (apathy) are also reduced.
Communicative. The patient’s speech may be reduced in quantity (poverty of speech) and information (poverty of content of speech). In mild forms of impoverished speech (alogia), the patient makes brief, unelaborated statements; in the more severe form, the patient can be virtually mute. Whatever speech is present tends to be vague and overly generalized. Periods of silence may occur, either before the patient answers a question (increased latency) or in the midst of a response (blocking).
Conational. The patient may show a lack of drive or goal-directed behavior (avolition). Personal grooming may be poor. Physical activity may be limited. Patients typically have great difficulty following a work schedule or hospital ward routine. They fail to initiate activities, participate grudgingly, and require frequent direction and encouragement.
Continue to: Relational
Relational. Interest in social activities and relationships is reduced (asociality). Even enjoyable and recreational activities are neglected. Interpersonal relations may be of little interest. Friendships become rare and shallow, with little sharing of intimacy. Contacts with family are neglected. Sexual interest declines. As symptoms progress, patients become increasingly isolated.
Primary and secondary symptoms
Negative symptoms are an intrinsic component of schizophrenic psychopathology, and they can also be caused by secondary factors (Table).6,7 Distinguishing between primary and secondary causes of negative symptoms can help you select appropriate treatment in specific clinical situations.
Primary symptoms. From a longitudinal perspective, the three major components of primary negative symptoms are:
- premorbid negative symptoms (present prior to psychosis onset and associated with poor premorbid functioning)
- psychotic-phase, nonenduring negative symptoms that fluctuate with positive symptoms around periods of psychotic exacerbation
- deteriorative negative symptoms that intensify following each psychotic exacerbation and reflect a decline from premorbid levels of functioning.
Though little can be done to treat the premorbid component, psychotic-phase negative symptoms improve along with positive symptoms (although more slowly).8,9 Therefore, the best strategy for managing negative symptoms is to treat positive symptoms more effectively. Although there is no specific treatment for deteriorative negative symptoms, the severity of this component appears to be related to the “toxicity of psychosis” and can be reduced by early, effective antipsychotic treatment.10,11
Secondary negative symptoms occur in association with (and presumably are caused by) factors such as depression, extrapyramidal symptoms (EPS), and environmental deprivation. Secondary negative symptoms usually respond to treatment of the underlying cause.
Assessment
Symptom severity. Assessing the severity of a patient’s negative symptoms on an ongoing basis is a most important first step towards optimal treatment:
- Our objective is to improve patients’ function and quality of life, and negative symptoms compromise both of these more than any other factor.
- Ongoing assessment can track whether prescribed treatments are improving or worsening a patient’s symptoms.
Tools to assess the severity of negative symptoms include the Brief Psychiatric Rating Scale (BPRS) and Positive and Negative Symptom Scale (PANSS).12 The Scale for the Assessment of Negative Symptoms (SANS)13 measures them exclusively, and others such as the Schedule for the Deficit Syndrome (SDS)14 attempt to classify them into subgroups.
Discussing these instruments is beyond the scope of this article, but they differ greatly in their approach to assessing negative symptoms. Instead of using cumbersome assessment instruments, however, we recommend that you focus on two to four of a patient’s “target” symptoms or behaviors and note their severity on an ongoing basis.
Contributing factors. Determining the overall contribution of different factors to a patient’s negative symptoms allows us to target treatments. Sorting out these relative factors can be difficult, however. For example:
- In a patient on antipsychotic treatment who is experiencing psychotic symptoms (eg, persecutory delusions), depressive symptoms, and prominent negative symptoms, the clinician can only guess whether the negative symptoms are primary or secondary.
- In a patient who is socially withdrawn and delusional, withdrawal may be secondary to delusions or may represent a primary negative symptom.
- In a patient on typical antipsychotics, a flat affect may be caused by antipsychotic-induced EPS or it may be a primary negative symptom.
- A disorganized patient with schizophrenia and depression is often unable to convey his or her feelings coherently, so that negative symptoms secondary to affective disturbance may often be mistaken as primary.
Even in research settings, the distinction between primary and secondary symptoms is quite unreliable; nevertheless, it is of great clinical importance. Two strategies may be helpful:
- Consider whether symptoms are specific to the presumed etiology, such as guilt and sadness in depression or cogwheeling and tremor in EPS.
- Treat empirically, and monitor whether negative symptoms improve. If they improve with antidepressant treatment, for example, then depression was the presumable cause. If they improve with anticholinergics, they were presumably secondary to EPS.
Treatment
Negative symptoms are generally viewed as treatment-resistant, but evidence suggests that they do respond to pharmacologic and social interventions (Box). Most responsive to treatment are negative symptoms that occur in association with positive symptoms (psychotic-phase) and secondary negative symptoms caused by neuroleptic medication, depression, or lack of stimulation.
The most effective treatment for secondary symptoms is to target the underlying cause. Neuroleptic-induced akinesia may respond to anticholinergic agents, reduction in antipsychotic dose, or a change in antipsychotic. Using one of the newer-generation antipsychotics (clozapine, risperidone, olanzapine, quetiapine, or ziprasidone) may prevent EPS.
Apsychosocial approach to schizophrenia builds on relationships between the patient and others and may involve social skills training, vocational rehabilitation, and psychotherapy. Activity-oriented therapies appear to be significantly more effective than verbal therapies.
Goals of psychosocial therapy:
- set realistic expectations for the patient
- stay active in treatment in the face of a protracted illness
- create a benign and supportive environment for the patient and caregivers.
Social skills training, designed to help the patient correctly perceive and respond to social situations, is the most widely studied and applied psychosocial intervention. The training is similar to that used in educational settings but focuses on remedying social rather than academic deficits. In schizophrenia, skills training programs address living skills, communication, conflict resolution, vocational skills, etc.
In early studies of social skills training, patients and their families described enhanced social adjustment, and hospitalization rates improved. More recent studies have confirmed improved social adjustment and relapse rates but suggest that overall symptom improvement is modest.
Continue to: Comorbid depression
Comorbid depression may require adding an antidepressant, or it may respond directly to an antipsychotic. Lack of stimulation is best handled by placing the patient in a more appropriately stimulating (but not overstimulating) and supportive environment. Nonenduring primary or psychotic-phase negative symptoms respond to effective antipsychotic treatment of the positive symptoms.
Atypical antipsychotics. Conventional antipsychotics (e.g., haloperidol, chlorpromazine) clearly offer some benefit in treating negative symptoms, but they have a much greater effect on positive symptoms.15 Using higher-than-appropriate doses diminishes their effect on negative symptoms and may result in severe EPS.
Two-thirds of the approximately 35 studies comparing conventional and atypical antipsychotics in treating negative symptoms have found atypicals to be significantly more effective (regardless of which atypical was used). In general, atypical antipsychotics improve negative symptoms by about 25%, compared with 10 to 15% improvement with conventional agents.16,17
Much of the greater benefit with atypicals appears to be related to their at least equivalent ability to improve positive symptoms without causing EPS. Consequently, the key to improved patient outcomes is appropriate dosing of atypical antipsychotics that reduces positive symptoms optimally without EPS and without the need for an anticholinergic (Figure).
Whether the greater improvement with atypical agents implies an improvement in primary versus secondary negative symptoms is academic.18 From the patient’s perspective, the greater reduction in negative symptoms is meaningful, regardless of why it occurs.
Other medications. Secondary negative symptoms are most effectively treated with medications directed at the primary etiology. For EPS, change the antipsychotic, reduce the dosage, or add an anticholinergic. For depression, try an antidepressant (preferably a selective serotonin reuptake inhibitor). If a likely contributing factor can be identified, then initiate specific treatment.
Figure
ANTIPSYCHOTICS IMPROVE NEGATIVE SYMPTOMS THROUGH THEIR EFFECT ON PSYCHOSIS
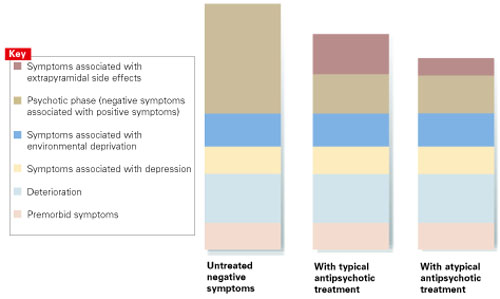
Source: Adapted from Tandon et al. J Psychiatric Res. 1993;27:341-347.
Antipsychotics improve negative symptoms through their effect on positive (psychotic) symptoms, but they do not affect secondary components—such as environmental deprivation and depression—or the primary components of deterioration and premorbid symptoms. Typical and atypical antipsychotics have similar effects on positive symptoms, but atypical antipsychotics carry a lower risk of extrapyramidal side effects.
Empiric therapy—trying one agent and then another in an effort to reduce negative symptoms—is appropriate if done systematically and sequentially. Medications that are found not to be helpful should be discontinued. Electroconvulsive therapy is not effective in treating negative symptoms.
Related resources
- Greden JF, Tandon R (eds). Negative schizophrenic symptoms: pathophysiology and clinical implications. Washington, DC: American Psychiatric Press, 1991.
- Keefe RSE, McEvoy JP (eds). Negative symptom and cognitive deficit treatment response in schizophrenia. Washington, DC: American Psychiatric Press, 2001.
Drug brand names
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
1. Kraepelin E. Dementia praecox and paraphrenia. Translated by Barclay RM, Robertson GM. Edinburgh: E&S Livingstone; 1919.
2. Bleuler E. Dementia praecox or the group of schizophrenias. Translated by Zinkin H. New York: International Universities Press; 1911.
3. Crow TJ. Molecular pathology of schizophrenia: More than one disease process. Br Med J. 1980;280:66-68.
4. Andreasen NC. Negative symptoms in schizophrenia: definition and reliability. Arch Gen Psychiatry. 1982;39:784-788.
5. Carpenter WT Jr, Heinrichs DW, Alphs LD. Treatment of negative symptoms. Schizophrenia Bull. 1985;11:440-452.
6. Carpenter WT, Jr, Heinrichs DW, Wagman AMI. Deficit and nondeficit forms of schizophrenia: the concept. Am J Psychiatry. 1988;145:578-583.
7. DeQuardo JR, Tandon R. Do atypical antipsychotic medications favorably alter the long-term course of schizophrenia? J Psychiatric Res. 1998;32:229-242.
8. Tandon R, Greden JF. Cholinergic hyperactivity and negative schizophrenic symptoms. Arch Gen Psychiatry. 1989;46:745-753.
9. Tandon R, et al. Covariance of positive and negative symptoms during neuroleptic treatment in schizophrenia: a replication. Biol Psychiatry. 1993;34(7):495-497.
10. Tandon R, Milner K, Jibson MD. Antipsychotics from theory to practice: integrating clinical and basic data. J Clin Psychiatry. 1999;60(suppl 8):21-28.
11. Jibson MD, Tandon R. Treatment of schizophrenia. Psych Clin North Am Annual of Drug Therapy. 2000;7:83-113.
12. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS). Schizophrenia Bull. 1987;13:261-276.
13. Andreasen NC. Scale for the Assessment of Negative Symptoms (SANS). Iowa City: University of Iowa; 1983.
14. Kirkpatrick B, Buchanan RW, McKenney PD, Alphs LD, Carpenter WT, Jr. The Schedule for the Deficit Syndrome: an instrument for research in schizophrenia. Psychiatry Res. 1989;30(2):119-124.
15. Meltzer HY, Sommers AA, Luchins DJ. The effect of neuroleptics and other psychotropic drugs on negative symptoms in schizophrenia. J Clin Psychopharmacol. 1986;6:329-338.
16. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic: a double-blind comparison with chlorpromazine. Arch Gen Psychiatry. 1988;45(9):789-796.
17. Tandon R, Goldman R, DeQuardo JR, et al. Positive and negative symptoms covary during clozapine treatment in schizophrenia. J Psychiatric Res. 1993;27:341-347.
18. Breier A, Buchanan RW, Kirkpatrick B, et al. Effect of clozapine on positive and negative symptoms in outpatients with schizophrenia. Am J Psychiatry. 1994;151(1):20-26.
Negative symptoms are the major contributor to low function levels and debilitation in most patients with schizophrenia. Poorly motivated patients cannot function adequately at school or work. Relationships with family and friends decay in the face of unresponsive affect and inattention to social cues. Personal interests yield to the dampening influences of anhedonia, apathy, and inattention.
Yet because active psychosis is the most common cause of hospital admission, a primary goal of treatment—and sometimes the only objective of pharmacologic treatment—is to eliminate or reduce positive symptoms. And although controlling positive symptoms is remarkably effective in reducing hospitalizations, patients’ functional capacity improves only minimally as psychosis abates. Even with optimal antipsychotic treatment, negative symptoms tend to persist.
For psychiatrists, the three major challenges of schizophrenia’s negative symptoms are their modest therapeutic response, pervasiveness, and diminution of patients’ quality of life. To help you manage negative symptoms, we suggest the following approach to their assessment and treatment.
Importance of negative symptoms
Schizophrenia is a heterogeneous disorder characterized by positive, negative, cognitive, and mood symptoms. The relative severity of these four pathologic domains varies from case to case and within the same individual over time. Though related, these domains have distinct underlying mechanisms and are differentially related to functional capacity and quality of life. They also show different patterns of response to treatment. Whereas positive symptoms refer to new psychological experiences outside the range of normal (e.g., delusions, hallucinations, suspiciousness, disorganized thinking), negative symptoms represent loss of normal function.
Negative symptoms include blunting of affect, poverty of speech and thought, apathy, anhedonia, reduced social drive, loss of motivation, lack of social interest, and inattention to social or cognitive input. These symptoms have devastating consequences on patients’ lives, and only modest progress has been made in treating them effectively.
From negative to positive. Early investigators1,2 considered negative symptoms to represent the fundamental defect of schizophrenia. Over the years, however, the importance of negative symptoms was progressively downplayed. Positive symptoms were increasingly emphasized because:
- positive symptoms have a more dramatic and easily recognized presentation
- negative symptoms are more difficult to reliably define and document
- antipsychotics, which revolutionized schizophrenia treatment, produce their most dramatic improvement in positive symptoms.
Renewed interest. The almost universal presence and relative persistence of negative symptoms, and the fact that they represent the most debilitating and refractory aspect of schizophrenic psychopathology, make them difficult to ignore. Consequently, interest in negative symptoms resurged in the 1980s-90s, with intense efforts to better understand them and treat them more effectively.3-5
Table
SCHIZOPHRENIA’S NEGATIVE SYMPTOMS: PRIMARY AND SECONDARY COMPONENTS
| Primary Associated with positive symptoms Deficit or primary enduring symptoms (premorbid and deteriorative) |
| Secondary Associated with extrapyramidal symptoms, depression, or environmental deprivation |
| Source: Adapted from DeQuardo JR, Tandon R. J Psychiatr Res 1998;32 (3-4):229-42. |
Negative symptoms are now better (but still incompletely) understood, and their treatment has improved but is still inadequate. Because intense effort yielded only modest success, researchers and clinicians have again begun to pay less attention to negative symptoms and shifted their focus to cognition in schizophrenia. Negative symptoms remain relevant, however, because they constitute the main barrier to a better quality of life for patients with schizophrenia.
Assessment for negative symptoms
The four major clinical subgroups of negative symptoms are affective, communicative, conational, and relational.
Affective. Blunted affect—including deficits in facial expression, eye contact, gestures, and voice pattern—is perhaps the most conspicuous negative symptom. In mild form, gestures may seem artificial or mechanical, and the voice is stilted or lacks normal inflection. Patients with severe blunted affect may appear devoid of facial expression or communicative gestures. They may sit impassively with little spontaneous movement, speak in a monotone, and gaze blankly in no particular direction.
Even when conversation becomes emotional, the patient’s affect does not adjust appropriately to reflect his or her feelings. Nor does the patient display even a basic level of understanding or responsiveness that typically characterize casual human interactions. The ability to experience pleasure (anhedonia) and sense of caring (apathy) are also reduced.
Communicative. The patient’s speech may be reduced in quantity (poverty of speech) and information (poverty of content of speech). In mild forms of impoverished speech (alogia), the patient makes brief, unelaborated statements; in the more severe form, the patient can be virtually mute. Whatever speech is present tends to be vague and overly generalized. Periods of silence may occur, either before the patient answers a question (increased latency) or in the midst of a response (blocking).
Conational. The patient may show a lack of drive or goal-directed behavior (avolition). Personal grooming may be poor. Physical activity may be limited. Patients typically have great difficulty following a work schedule or hospital ward routine. They fail to initiate activities, participate grudgingly, and require frequent direction and encouragement.
Continue to: Relational
Relational. Interest in social activities and relationships is reduced (asociality). Even enjoyable and recreational activities are neglected. Interpersonal relations may be of little interest. Friendships become rare and shallow, with little sharing of intimacy. Contacts with family are neglected. Sexual interest declines. As symptoms progress, patients become increasingly isolated.
Primary and secondary symptoms
Negative symptoms are an intrinsic component of schizophrenic psychopathology, and they can also be caused by secondary factors (Table).6,7 Distinguishing between primary and secondary causes of negative symptoms can help you select appropriate treatment in specific clinical situations.
Primary symptoms. From a longitudinal perspective, the three major components of primary negative symptoms are:
- premorbid negative symptoms (present prior to psychosis onset and associated with poor premorbid functioning)
- psychotic-phase, nonenduring negative symptoms that fluctuate with positive symptoms around periods of psychotic exacerbation
- deteriorative negative symptoms that intensify following each psychotic exacerbation and reflect a decline from premorbid levels of functioning.
Though little can be done to treat the premorbid component, psychotic-phase negative symptoms improve along with positive symptoms (although more slowly).8,9 Therefore, the best strategy for managing negative symptoms is to treat positive symptoms more effectively. Although there is no specific treatment for deteriorative negative symptoms, the severity of this component appears to be related to the “toxicity of psychosis” and can be reduced by early, effective antipsychotic treatment.10,11
Secondary negative symptoms occur in association with (and presumably are caused by) factors such as depression, extrapyramidal symptoms (EPS), and environmental deprivation. Secondary negative symptoms usually respond to treatment of the underlying cause.
Assessment
Symptom severity. Assessing the severity of a patient’s negative symptoms on an ongoing basis is a most important first step towards optimal treatment:
- Our objective is to improve patients’ function and quality of life, and negative symptoms compromise both of these more than any other factor.
- Ongoing assessment can track whether prescribed treatments are improving or worsening a patient’s symptoms.
Tools to assess the severity of negative symptoms include the Brief Psychiatric Rating Scale (BPRS) and Positive and Negative Symptom Scale (PANSS).12 The Scale for the Assessment of Negative Symptoms (SANS)13 measures them exclusively, and others such as the Schedule for the Deficit Syndrome (SDS)14 attempt to classify them into subgroups.
Discussing these instruments is beyond the scope of this article, but they differ greatly in their approach to assessing negative symptoms. Instead of using cumbersome assessment instruments, however, we recommend that you focus on two to four of a patient’s “target” symptoms or behaviors and note their severity on an ongoing basis.
Contributing factors. Determining the overall contribution of different factors to a patient’s negative symptoms allows us to target treatments. Sorting out these relative factors can be difficult, however. For example:
- In a patient on antipsychotic treatment who is experiencing psychotic symptoms (eg, persecutory delusions), depressive symptoms, and prominent negative symptoms, the clinician can only guess whether the negative symptoms are primary or secondary.
- In a patient who is socially withdrawn and delusional, withdrawal may be secondary to delusions or may represent a primary negative symptom.
- In a patient on typical antipsychotics, a flat affect may be caused by antipsychotic-induced EPS or it may be a primary negative symptom.
- A disorganized patient with schizophrenia and depression is often unable to convey his or her feelings coherently, so that negative symptoms secondary to affective disturbance may often be mistaken as primary.
Even in research settings, the distinction between primary and secondary symptoms is quite unreliable; nevertheless, it is of great clinical importance. Two strategies may be helpful:
- Consider whether symptoms are specific to the presumed etiology, such as guilt and sadness in depression or cogwheeling and tremor in EPS.
- Treat empirically, and monitor whether negative symptoms improve. If they improve with antidepressant treatment, for example, then depression was the presumable cause. If they improve with anticholinergics, they were presumably secondary to EPS.
Treatment
Negative symptoms are generally viewed as treatment-resistant, but evidence suggests that they do respond to pharmacologic and social interventions (Box). Most responsive to treatment are negative symptoms that occur in association with positive symptoms (psychotic-phase) and secondary negative symptoms caused by neuroleptic medication, depression, or lack of stimulation.
The most effective treatment for secondary symptoms is to target the underlying cause. Neuroleptic-induced akinesia may respond to anticholinergic agents, reduction in antipsychotic dose, or a change in antipsychotic. Using one of the newer-generation antipsychotics (clozapine, risperidone, olanzapine, quetiapine, or ziprasidone) may prevent EPS.
Apsychosocial approach to schizophrenia builds on relationships between the patient and others and may involve social skills training, vocational rehabilitation, and psychotherapy. Activity-oriented therapies appear to be significantly more effective than verbal therapies.
Goals of psychosocial therapy:
- set realistic expectations for the patient
- stay active in treatment in the face of a protracted illness
- create a benign and supportive environment for the patient and caregivers.
Social skills training, designed to help the patient correctly perceive and respond to social situations, is the most widely studied and applied psychosocial intervention. The training is similar to that used in educational settings but focuses on remedying social rather than academic deficits. In schizophrenia, skills training programs address living skills, communication, conflict resolution, vocational skills, etc.
In early studies of social skills training, patients and their families described enhanced social adjustment, and hospitalization rates improved. More recent studies have confirmed improved social adjustment and relapse rates but suggest that overall symptom improvement is modest.
Continue to: Comorbid depression
Comorbid depression may require adding an antidepressant, or it may respond directly to an antipsychotic. Lack of stimulation is best handled by placing the patient in a more appropriately stimulating (but not overstimulating) and supportive environment. Nonenduring primary or psychotic-phase negative symptoms respond to effective antipsychotic treatment of the positive symptoms.
Atypical antipsychotics. Conventional antipsychotics (e.g., haloperidol, chlorpromazine) clearly offer some benefit in treating negative symptoms, but they have a much greater effect on positive symptoms.15 Using higher-than-appropriate doses diminishes their effect on negative symptoms and may result in severe EPS.
Two-thirds of the approximately 35 studies comparing conventional and atypical antipsychotics in treating negative symptoms have found atypicals to be significantly more effective (regardless of which atypical was used). In general, atypical antipsychotics improve negative symptoms by about 25%, compared with 10 to 15% improvement with conventional agents.16,17
Much of the greater benefit with atypicals appears to be related to their at least equivalent ability to improve positive symptoms without causing EPS. Consequently, the key to improved patient outcomes is appropriate dosing of atypical antipsychotics that reduces positive symptoms optimally without EPS and without the need for an anticholinergic (Figure).
Whether the greater improvement with atypical agents implies an improvement in primary versus secondary negative symptoms is academic.18 From the patient’s perspective, the greater reduction in negative symptoms is meaningful, regardless of why it occurs.
Other medications. Secondary negative symptoms are most effectively treated with medications directed at the primary etiology. For EPS, change the antipsychotic, reduce the dosage, or add an anticholinergic. For depression, try an antidepressant (preferably a selective serotonin reuptake inhibitor). If a likely contributing factor can be identified, then initiate specific treatment.
Figure
ANTIPSYCHOTICS IMPROVE NEGATIVE SYMPTOMS THROUGH THEIR EFFECT ON PSYCHOSIS
Source: Adapted from Tandon et al. J Psychiatric Res. 1993;27:341-347.
Antipsychotics improve negative symptoms through their effect on positive (psychotic) symptoms, but they do not affect secondary components—such as environmental deprivation and depression—or the primary components of deterioration and premorbid symptoms. Typical and atypical antipsychotics have similar effects on positive symptoms, but atypical antipsychotics carry a lower risk of extrapyramidal side effects.
Empiric therapy—trying one agent and then another in an effort to reduce negative symptoms—is appropriate if done systematically and sequentially. Medications that are found not to be helpful should be discontinued. Electroconvulsive therapy is not effective in treating negative symptoms.
Related resources
- Greden JF, Tandon R (eds). Negative schizophrenic symptoms: pathophysiology and clinical implications. Washington, DC: American Psychiatric Press, 1991.
- Keefe RSE, McEvoy JP (eds). Negative symptom and cognitive deficit treatment response in schizophrenia. Washington, DC: American Psychiatric Press, 2001.
Drug brand names
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Negative symptoms are the major contributor to low function levels and debilitation in most patients with schizophrenia. Poorly motivated patients cannot function adequately at school or work. Relationships with family and friends decay in the face of unresponsive affect and inattention to social cues. Personal interests yield to the dampening influences of anhedonia, apathy, and inattention.
Yet because active psychosis is the most common cause of hospital admission, a primary goal of treatment—and sometimes the only objective of pharmacologic treatment—is to eliminate or reduce positive symptoms. And although controlling positive symptoms is remarkably effective in reducing hospitalizations, patients’ functional capacity improves only minimally as psychosis abates. Even with optimal antipsychotic treatment, negative symptoms tend to persist.
For psychiatrists, the three major challenges of schizophrenia’s negative symptoms are their modest therapeutic response, pervasiveness, and diminution of patients’ quality of life. To help you manage negative symptoms, we suggest the following approach to their assessment and treatment.
Importance of negative symptoms
Schizophrenia is a heterogeneous disorder characterized by positive, negative, cognitive, and mood symptoms. The relative severity of these four pathologic domains varies from case to case and within the same individual over time. Though related, these domains have distinct underlying mechanisms and are differentially related to functional capacity and quality of life. They also show different patterns of response to treatment. Whereas positive symptoms refer to new psychological experiences outside the range of normal (e.g., delusions, hallucinations, suspiciousness, disorganized thinking), negative symptoms represent loss of normal function.
Negative symptoms include blunting of affect, poverty of speech and thought, apathy, anhedonia, reduced social drive, loss of motivation, lack of social interest, and inattention to social or cognitive input. These symptoms have devastating consequences on patients’ lives, and only modest progress has been made in treating them effectively.
From negative to positive. Early investigators1,2 considered negative symptoms to represent the fundamental defect of schizophrenia. Over the years, however, the importance of negative symptoms was progressively downplayed. Positive symptoms were increasingly emphasized because:
- positive symptoms have a more dramatic and easily recognized presentation
- negative symptoms are more difficult to reliably define and document
- antipsychotics, which revolutionized schizophrenia treatment, produce their most dramatic improvement in positive symptoms.
Renewed interest. The almost universal presence and relative persistence of negative symptoms, and the fact that they represent the most debilitating and refractory aspect of schizophrenic psychopathology, make them difficult to ignore. Consequently, interest in negative symptoms resurged in the 1980s-90s, with intense efforts to better understand them and treat them more effectively.3-5
Table
SCHIZOPHRENIA’S NEGATIVE SYMPTOMS: PRIMARY AND SECONDARY COMPONENTS
| Primary Associated with positive symptoms Deficit or primary enduring symptoms (premorbid and deteriorative) |
| Secondary Associated with extrapyramidal symptoms, depression, or environmental deprivation |
| Source: Adapted from DeQuardo JR, Tandon R. J Psychiatr Res 1998;32 (3-4):229-42. |
Negative symptoms are now better (but still incompletely) understood, and their treatment has improved but is still inadequate. Because intense effort yielded only modest success, researchers and clinicians have again begun to pay less attention to negative symptoms and shifted their focus to cognition in schizophrenia. Negative symptoms remain relevant, however, because they constitute the main barrier to a better quality of life for patients with schizophrenia.
Assessment for negative symptoms
The four major clinical subgroups of negative symptoms are affective, communicative, conational, and relational.
Affective. Blunted affect—including deficits in facial expression, eye contact, gestures, and voice pattern—is perhaps the most conspicuous negative symptom. In mild form, gestures may seem artificial or mechanical, and the voice is stilted or lacks normal inflection. Patients with severe blunted affect may appear devoid of facial expression or communicative gestures. They may sit impassively with little spontaneous movement, speak in a monotone, and gaze blankly in no particular direction.
Even when conversation becomes emotional, the patient’s affect does not adjust appropriately to reflect his or her feelings. Nor does the patient display even a basic level of understanding or responsiveness that typically characterize casual human interactions. The ability to experience pleasure (anhedonia) and sense of caring (apathy) are also reduced.
Communicative. The patient’s speech may be reduced in quantity (poverty of speech) and information (poverty of content of speech). In mild forms of impoverished speech (alogia), the patient makes brief, unelaborated statements; in the more severe form, the patient can be virtually mute. Whatever speech is present tends to be vague and overly generalized. Periods of silence may occur, either before the patient answers a question (increased latency) or in the midst of a response (blocking).
Conational. The patient may show a lack of drive or goal-directed behavior (avolition). Personal grooming may be poor. Physical activity may be limited. Patients typically have great difficulty following a work schedule or hospital ward routine. They fail to initiate activities, participate grudgingly, and require frequent direction and encouragement.
Continue to: Relational
Relational. Interest in social activities and relationships is reduced (asociality). Even enjoyable and recreational activities are neglected. Interpersonal relations may be of little interest. Friendships become rare and shallow, with little sharing of intimacy. Contacts with family are neglected. Sexual interest declines. As symptoms progress, patients become increasingly isolated.
Primary and secondary symptoms
Negative symptoms are an intrinsic component of schizophrenic psychopathology, and they can also be caused by secondary factors (Table).6,7 Distinguishing between primary and secondary causes of negative symptoms can help you select appropriate treatment in specific clinical situations.
Primary symptoms. From a longitudinal perspective, the three major components of primary negative symptoms are:
- premorbid negative symptoms (present prior to psychosis onset and associated with poor premorbid functioning)
- psychotic-phase, nonenduring negative symptoms that fluctuate with positive symptoms around periods of psychotic exacerbation
- deteriorative negative symptoms that intensify following each psychotic exacerbation and reflect a decline from premorbid levels of functioning.
Though little can be done to treat the premorbid component, psychotic-phase negative symptoms improve along with positive symptoms (although more slowly).8,9 Therefore, the best strategy for managing negative symptoms is to treat positive symptoms more effectively. Although there is no specific treatment for deteriorative negative symptoms, the severity of this component appears to be related to the “toxicity of psychosis” and can be reduced by early, effective antipsychotic treatment.10,11
Secondary negative symptoms occur in association with (and presumably are caused by) factors such as depression, extrapyramidal symptoms (EPS), and environmental deprivation. Secondary negative symptoms usually respond to treatment of the underlying cause.
Assessment
Symptom severity. Assessing the severity of a patient’s negative symptoms on an ongoing basis is a most important first step towards optimal treatment:
- Our objective is to improve patients’ function and quality of life, and negative symptoms compromise both of these more than any other factor.
- Ongoing assessment can track whether prescribed treatments are improving or worsening a patient’s symptoms.
Tools to assess the severity of negative symptoms include the Brief Psychiatric Rating Scale (BPRS) and Positive and Negative Symptom Scale (PANSS).12 The Scale for the Assessment of Negative Symptoms (SANS)13 measures them exclusively, and others such as the Schedule for the Deficit Syndrome (SDS)14 attempt to classify them into subgroups.
Discussing these instruments is beyond the scope of this article, but they differ greatly in their approach to assessing negative symptoms. Instead of using cumbersome assessment instruments, however, we recommend that you focus on two to four of a patient’s “target” symptoms or behaviors and note their severity on an ongoing basis.
Contributing factors. Determining the overall contribution of different factors to a patient’s negative symptoms allows us to target treatments. Sorting out these relative factors can be difficult, however. For example:
- In a patient on antipsychotic treatment who is experiencing psychotic symptoms (eg, persecutory delusions), depressive symptoms, and prominent negative symptoms, the clinician can only guess whether the negative symptoms are primary or secondary.
- In a patient who is socially withdrawn and delusional, withdrawal may be secondary to delusions or may represent a primary negative symptom.
- In a patient on typical antipsychotics, a flat affect may be caused by antipsychotic-induced EPS or it may be a primary negative symptom.
- A disorganized patient with schizophrenia and depression is often unable to convey his or her feelings coherently, so that negative symptoms secondary to affective disturbance may often be mistaken as primary.
Even in research settings, the distinction between primary and secondary symptoms is quite unreliable; nevertheless, it is of great clinical importance. Two strategies may be helpful:
- Consider whether symptoms are specific to the presumed etiology, such as guilt and sadness in depression or cogwheeling and tremor in EPS.
- Treat empirically, and monitor whether negative symptoms improve. If they improve with antidepressant treatment, for example, then depression was the presumable cause. If they improve with anticholinergics, they were presumably secondary to EPS.
Treatment
Negative symptoms are generally viewed as treatment-resistant, but evidence suggests that they do respond to pharmacologic and social interventions (Box). Most responsive to treatment are negative symptoms that occur in association with positive symptoms (psychotic-phase) and secondary negative symptoms caused by neuroleptic medication, depression, or lack of stimulation.
The most effective treatment for secondary symptoms is to target the underlying cause. Neuroleptic-induced akinesia may respond to anticholinergic agents, reduction in antipsychotic dose, or a change in antipsychotic. Using one of the newer-generation antipsychotics (clozapine, risperidone, olanzapine, quetiapine, or ziprasidone) may prevent EPS.
Apsychosocial approach to schizophrenia builds on relationships between the patient and others and may involve social skills training, vocational rehabilitation, and psychotherapy. Activity-oriented therapies appear to be significantly more effective than verbal therapies.
Goals of psychosocial therapy:
- set realistic expectations for the patient
- stay active in treatment in the face of a protracted illness
- create a benign and supportive environment for the patient and caregivers.
Social skills training, designed to help the patient correctly perceive and respond to social situations, is the most widely studied and applied psychosocial intervention. The training is similar to that used in educational settings but focuses on remedying social rather than academic deficits. In schizophrenia, skills training programs address living skills, communication, conflict resolution, vocational skills, etc.
In early studies of social skills training, patients and their families described enhanced social adjustment, and hospitalization rates improved. More recent studies have confirmed improved social adjustment and relapse rates but suggest that overall symptom improvement is modest.
Continue to: Comorbid depression
Comorbid depression may require adding an antidepressant, or it may respond directly to an antipsychotic. Lack of stimulation is best handled by placing the patient in a more appropriately stimulating (but not overstimulating) and supportive environment. Nonenduring primary or psychotic-phase negative symptoms respond to effective antipsychotic treatment of the positive symptoms.
Atypical antipsychotics. Conventional antipsychotics (e.g., haloperidol, chlorpromazine) clearly offer some benefit in treating negative symptoms, but they have a much greater effect on positive symptoms.15 Using higher-than-appropriate doses diminishes their effect on negative symptoms and may result in severe EPS.
Two-thirds of the approximately 35 studies comparing conventional and atypical antipsychotics in treating negative symptoms have found atypicals to be significantly more effective (regardless of which atypical was used). In general, atypical antipsychotics improve negative symptoms by about 25%, compared with 10 to 15% improvement with conventional agents.16,17
Much of the greater benefit with atypicals appears to be related to their at least equivalent ability to improve positive symptoms without causing EPS. Consequently, the key to improved patient outcomes is appropriate dosing of atypical antipsychotics that reduces positive symptoms optimally without EPS and without the need for an anticholinergic (Figure).
Whether the greater improvement with atypical agents implies an improvement in primary versus secondary negative symptoms is academic.18 From the patient’s perspective, the greater reduction in negative symptoms is meaningful, regardless of why it occurs.
Other medications. Secondary negative symptoms are most effectively treated with medications directed at the primary etiology. For EPS, change the antipsychotic, reduce the dosage, or add an anticholinergic. For depression, try an antidepressant (preferably a selective serotonin reuptake inhibitor). If a likely contributing factor can be identified, then initiate specific treatment.
Figure
ANTIPSYCHOTICS IMPROVE NEGATIVE SYMPTOMS THROUGH THEIR EFFECT ON PSYCHOSIS
Source: Adapted from Tandon et al. J Psychiatric Res. 1993;27:341-347.
Antipsychotics improve negative symptoms through their effect on positive (psychotic) symptoms, but they do not affect secondary components—such as environmental deprivation and depression—or the primary components of deterioration and premorbid symptoms. Typical and atypical antipsychotics have similar effects on positive symptoms, but atypical antipsychotics carry a lower risk of extrapyramidal side effects.
Empiric therapy—trying one agent and then another in an effort to reduce negative symptoms—is appropriate if done systematically and sequentially. Medications that are found not to be helpful should be discontinued. Electroconvulsive therapy is not effective in treating negative symptoms.
Related resources
- Greden JF, Tandon R (eds). Negative schizophrenic symptoms: pathophysiology and clinical implications. Washington, DC: American Psychiatric Press, 1991.
- Keefe RSE, McEvoy JP (eds). Negative symptom and cognitive deficit treatment response in schizophrenia. Washington, DC: American Psychiatric Press, 2001.
Drug brand names
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
1. Kraepelin E. Dementia praecox and paraphrenia. Translated by Barclay RM, Robertson GM. Edinburgh: E&S Livingstone; 1919.
2. Bleuler E. Dementia praecox or the group of schizophrenias. Translated by Zinkin H. New York: International Universities Press; 1911.
3. Crow TJ. Molecular pathology of schizophrenia: More than one disease process. Br Med J. 1980;280:66-68.
4. Andreasen NC. Negative symptoms in schizophrenia: definition and reliability. Arch Gen Psychiatry. 1982;39:784-788.
5. Carpenter WT Jr, Heinrichs DW, Alphs LD. Treatment of negative symptoms. Schizophrenia Bull. 1985;11:440-452.
6. Carpenter WT, Jr, Heinrichs DW, Wagman AMI. Deficit and nondeficit forms of schizophrenia: the concept. Am J Psychiatry. 1988;145:578-583.
7. DeQuardo JR, Tandon R. Do atypical antipsychotic medications favorably alter the long-term course of schizophrenia? J Psychiatric Res. 1998;32:229-242.
8. Tandon R, Greden JF. Cholinergic hyperactivity and negative schizophrenic symptoms. Arch Gen Psychiatry. 1989;46:745-753.
9. Tandon R, et al. Covariance of positive and negative symptoms during neuroleptic treatment in schizophrenia: a replication. Biol Psychiatry. 1993;34(7):495-497.
10. Tandon R, Milner K, Jibson MD. Antipsychotics from theory to practice: integrating clinical and basic data. J Clin Psychiatry. 1999;60(suppl 8):21-28.
11. Jibson MD, Tandon R. Treatment of schizophrenia. Psych Clin North Am Annual of Drug Therapy. 2000;7:83-113.
12. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS). Schizophrenia Bull. 1987;13:261-276.
13. Andreasen NC. Scale for the Assessment of Negative Symptoms (SANS). Iowa City: University of Iowa; 1983.
14. Kirkpatrick B, Buchanan RW, McKenney PD, Alphs LD, Carpenter WT, Jr. The Schedule for the Deficit Syndrome: an instrument for research in schizophrenia. Psychiatry Res. 1989;30(2):119-124.
15. Meltzer HY, Sommers AA, Luchins DJ. The effect of neuroleptics and other psychotropic drugs on negative symptoms in schizophrenia. J Clin Psychopharmacol. 1986;6:329-338.
16. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic: a double-blind comparison with chlorpromazine. Arch Gen Psychiatry. 1988;45(9):789-796.
17. Tandon R, Goldman R, DeQuardo JR, et al. Positive and negative symptoms covary during clozapine treatment in schizophrenia. J Psychiatric Res. 1993;27:341-347.
18. Breier A, Buchanan RW, Kirkpatrick B, et al. Effect of clozapine on positive and negative symptoms in outpatients with schizophrenia. Am J Psychiatry. 1994;151(1):20-26.
1. Kraepelin E. Dementia praecox and paraphrenia. Translated by Barclay RM, Robertson GM. Edinburgh: E&S Livingstone; 1919.
2. Bleuler E. Dementia praecox or the group of schizophrenias. Translated by Zinkin H. New York: International Universities Press; 1911.
3. Crow TJ. Molecular pathology of schizophrenia: More than one disease process. Br Med J. 1980;280:66-68.
4. Andreasen NC. Negative symptoms in schizophrenia: definition and reliability. Arch Gen Psychiatry. 1982;39:784-788.
5. Carpenter WT Jr, Heinrichs DW, Alphs LD. Treatment of negative symptoms. Schizophrenia Bull. 1985;11:440-452.
6. Carpenter WT, Jr, Heinrichs DW, Wagman AMI. Deficit and nondeficit forms of schizophrenia: the concept. Am J Psychiatry. 1988;145:578-583.
7. DeQuardo JR, Tandon R. Do atypical antipsychotic medications favorably alter the long-term course of schizophrenia? J Psychiatric Res. 1998;32:229-242.
8. Tandon R, Greden JF. Cholinergic hyperactivity and negative schizophrenic symptoms. Arch Gen Psychiatry. 1989;46:745-753.
9. Tandon R, et al. Covariance of positive and negative symptoms during neuroleptic treatment in schizophrenia: a replication. Biol Psychiatry. 1993;34(7):495-497.
10. Tandon R, Milner K, Jibson MD. Antipsychotics from theory to practice: integrating clinical and basic data. J Clin Psychiatry. 1999;60(suppl 8):21-28.
11. Jibson MD, Tandon R. Treatment of schizophrenia. Psych Clin North Am Annual of Drug Therapy. 2000;7:83-113.
12. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS). Schizophrenia Bull. 1987;13:261-276.
13. Andreasen NC. Scale for the Assessment of Negative Symptoms (SANS). Iowa City: University of Iowa; 1983.
14. Kirkpatrick B, Buchanan RW, McKenney PD, Alphs LD, Carpenter WT, Jr. The Schedule for the Deficit Syndrome: an instrument for research in schizophrenia. Psychiatry Res. 1989;30(2):119-124.
15. Meltzer HY, Sommers AA, Luchins DJ. The effect of neuroleptics and other psychotropic drugs on negative symptoms in schizophrenia. J Clin Psychopharmacol. 1986;6:329-338.
16. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic: a double-blind comparison with chlorpromazine. Arch Gen Psychiatry. 1988;45(9):789-796.
17. Tandon R, Goldman R, DeQuardo JR, et al. Positive and negative symptoms covary during clozapine treatment in schizophrenia. J Psychiatric Res. 1993;27:341-347.
18. Breier A, Buchanan RW, Kirkpatrick B, et al. Effect of clozapine on positive and negative symptoms in outpatients with schizophrenia. Am J Psychiatry. 1994;151(1):20-26.