A new standard classification of rosacea and its pathophysiology has been developed by the National Rosacea Society Expert Committee.
Dr. Richard L. Gallo“There has been an explosion of research on rosacea since the first standard classification system appeared in 2002, and that has resulted in a much deeper scientific understanding of this common but once little-known disorder,” Richard Gallo, MD, chairman of dermatology at the University of California, San Diego, and chairman of the National Rosacea Society consensus committee, said in a statement issued by the society. “Growing knowledge of rosacea’s pathophysiology has established that a consistent multivariate disease process underlies its various clinical manifestations, which may also potentially be associated with other systemic disorders.”
National Rosacea Society
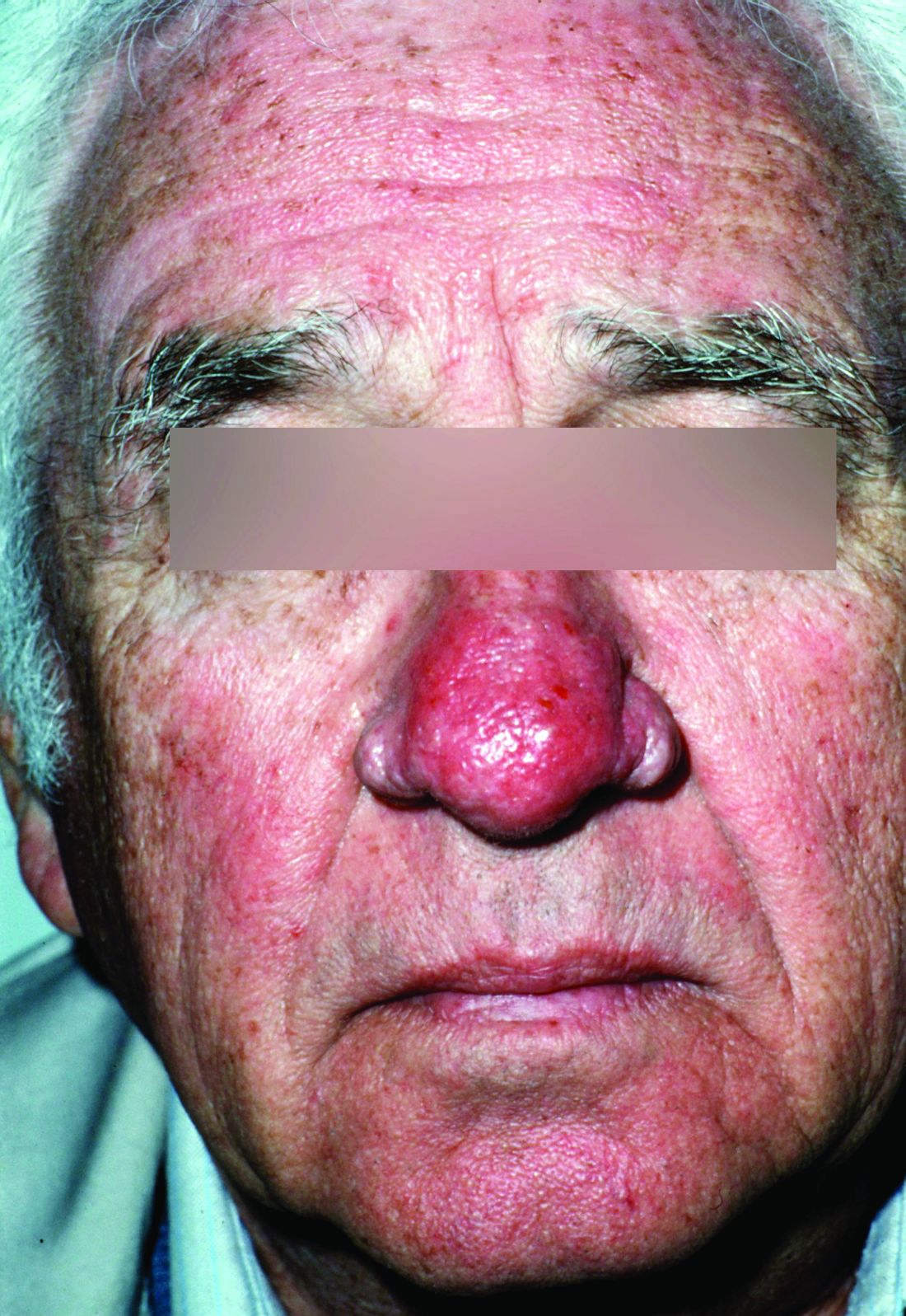
Phymatous rosacea is shown.The updated classification system requires one of two diagnostic phenotypes: phymatous changes or fixed centrofacial erythema in a characteristic pattern that may periodically intensify. If there is not a diagnostic phenotype, the presence of two or more of the following major phenotypes may be considered diagnostic: flushing, telangiectasia, ocular manifestations, or papules and pustules. Secondary phenotypes that may appear with the above-mentioned phenotypes are edema, dry appearance, or burning/stinging.
Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).
National Rosacea Society
Inflammatory rosacea, presenting with papules and pustules on the forehead, cheeks, nose and chin, is shown.In an accompanying commentary regarding rosacea comorbidities and future research by the committee, Dr. Gallo and his coauthors wrote that recent studies have found “associations between rosacea and increased risk for a variety of systemic disorders, many with potentially serious outcomes” (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.06.150). In numerous studies, there was an increased incidence of dyslipidemia, hypertension, and coronary artery disease in patients with rosacea. In one study, rosacea was significantly associated with airborne or food allergies, gastroesophageal reflux disease (GERD), and other GI diseases. Two studies have found patients with rosacea to be at increased risk of Parkinson’s. One study each found an association between rosacea and increased risk for thyroid cancer, basal cell carcinoma, and glioma.
A new standard classification of rosacea and its pathophysiology has been developed by the National Rosacea Society Expert Committee.
Dr. Richard L. Gallo“There has been an explosion of research on rosacea since the first standard classification system appeared in 2002, and that has resulted in a much deeper scientific understanding of this common but once little-known disorder,” Richard Gallo, MD, chairman of dermatology at the University of California, San Diego, and chairman of the National Rosacea Society consensus committee, said in a statement issued by the society. “Growing knowledge of rosacea’s pathophysiology has established that a consistent multivariate disease process underlies its various clinical manifestations, which may also potentially be associated with other systemic disorders.”
National Rosacea Society
Phymatous rosacea is shown.The updated classification system requires one of two diagnostic phenotypes: phymatous changes or fixed centrofacial erythema in a characteristic pattern that may periodically intensify. If there is not a diagnostic phenotype, the presence of two or more of the following major phenotypes may be considered diagnostic: flushing, telangiectasia, ocular manifestations, or papules and pustules. Secondary phenotypes that may appear with the above-mentioned phenotypes are edema, dry appearance, or burning/stinging.
Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).
National Rosacea Society
Inflammatory rosacea, presenting with papules and pustules on the forehead, cheeks, nose and chin, is shown.In an accompanying commentary regarding rosacea comorbidities and future research by the committee, Dr. Gallo and his coauthors wrote that recent studies have found “associations between rosacea and increased risk for a variety of systemic disorders, many with potentially serious outcomes” (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.06.150). In numerous studies, there was an increased incidence of dyslipidemia, hypertension, and coronary artery disease in patients with rosacea. In one study, rosacea was significantly associated with airborne or food allergies, gastroesophageal reflux disease (GERD), and other GI diseases. Two studies have found patients with rosacea to be at increased risk of Parkinson’s. One study each found an association between rosacea and increased risk for thyroid cancer, basal cell carcinoma, and glioma.
A new standard classification of rosacea and its pathophysiology has been developed by the National Rosacea Society Expert Committee.
Dr. Richard L. Gallo“There has been an explosion of research on rosacea since the first standard classification system appeared in 2002, and that has resulted in a much deeper scientific understanding of this common but once little-known disorder,” Richard Gallo, MD, chairman of dermatology at the University of California, San Diego, and chairman of the National Rosacea Society consensus committee, said in a statement issued by the society. “Growing knowledge of rosacea’s pathophysiology has established that a consistent multivariate disease process underlies its various clinical manifestations, which may also potentially be associated with other systemic disorders.”
National Rosacea Society
Phymatous rosacea is shown.The updated classification system requires one of two diagnostic phenotypes: phymatous changes or fixed centrofacial erythema in a characteristic pattern that may periodically intensify. If there is not a diagnostic phenotype, the presence of two or more of the following major phenotypes may be considered diagnostic: flushing, telangiectasia, ocular manifestations, or papules and pustules. Secondary phenotypes that may appear with the above-mentioned phenotypes are edema, dry appearance, or burning/stinging.
Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).
National Rosacea Society
Inflammatory rosacea, presenting with papules and pustules on the forehead, cheeks, nose and chin, is shown.In an accompanying commentary regarding rosacea comorbidities and future research by the committee, Dr. Gallo and his coauthors wrote that recent studies have found “associations between rosacea and increased risk for a variety of systemic disorders, many with potentially serious outcomes” (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.06.150). In numerous studies, there was an increased incidence of dyslipidemia, hypertension, and coronary artery disease in patients with rosacea. In one study, rosacea was significantly associated with airborne or food allergies, gastroesophageal reflux disease (GERD), and other GI diseases. Two studies have found patients with rosacea to be at increased risk of Parkinson’s. One study each found an association between rosacea and increased risk for thyroid cancer, basal cell carcinoma, and glioma.