User login
A 79 year-old man sought care at our clinic for pain in his left ear and a severe sore throat that had been bothering him for the past 2 days. He also complained of pain when he swallowed, a decreased appetite, and dizziness. He denied weight loss, fever, tinnitus, subjective hearing loss, unilateral facial droop, or weakness.
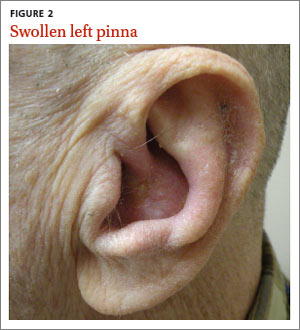
On physical exam, we noted vesicles on an erythematous base on his hard palate. They were on the left side and didn’t cross the midline (FIGURE 1). The left pinna was mildly erythematous and swollen (FIGURE 2) without obvious vesicles, although we noted vesicles in the external auditory canal on otoscopic examination. The tympanic membrane was normal, as was the patient’s right ear.

WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Ramsay Hunt syndrome
Based on our patient’s clinical presentation, we diagnosed herpes zoster oticus—also known as Ramsay Hunt syndrome. This syndrome is a rare complication of herpes zoster that occurs when latent varicella zoster virus (VZV) infection reactivates and spreads to affect the geniculate ganglion.1 An estimated 5 out of every 100,000 people develop Ramsay Hunt syndrome each year in the United States; men and women are equally affected.1 Any patient who’s had VZV infection runs the risk of developing Ramsay Hunt syndrome, but it most often develops in individuals older than age 60.1
Ramsay Hunt syndrome classically presents with unilateral facial paralysis and erythematous vesicles located ipsilaterally on the ear and/or in the mouth. Vesicles in the mouth usually develop on the tongue or hard palate. Other symptoms may include tinnitus, hearing loss, nausea, vomiting, vertigo, and nystagmus.2
Several types of infection are in the differential diagnosis
Because the symptoms of Ramsay Hunt syndrome suggest a possible infection, the differential diagnosis should include herpes simplex virus type 1 (HSV-1), Epstein-Barr virus (EBV), group A Streptococcus (GAS), and measles.
HSV-1 can cause oral symptoms similar to Ramsay Hunt syndrome. However,
HSV-1 doesn’t cause vesicles in the ear. Also worth noting: Recurrent HSV-1 infections normally involve keratinized surfaces such as the vermilion border and gums, but rarely the hard palate.3
EBV can cause multiple systemic symptoms. It can cause leukoplakia in the mouth— most often on the sides of the tongue—but does not cause vesicles.4
GAS presents as a sore throat, fever, anterior cervical lymphadenitis, and a scarlatiniform rash. Oral manifestations can include tonsillar erythema with or without exudate, soft palate petechiae, and a red swollen uvula.5 Use of validated clinical prediction tools, such as the sore throat tool found at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1228750/pdf/cmaj_158_1_75.pdf, can help distinguish GAS infection from other conditions.6-8
Measles typically occurs in children and young adults. Infection in immunized individuals is rare. It presents with fever and the “3 Cs”—cough, coryza, and conjunctivitis. Koplik’s spots are blue to white ulcerated lesions on the buccal mucosa, typically opposite the first and second molars, although they can occur anywhere in the mouth. They precede the generalized maculopapular rash of measles.9
Although it’s a clinical Dx, lab testing can provide confirmation
Diagnosis of Ramsay Hunt syndrome is typically made clinically, but can be confirmed with direct fluorescent antibody (DFA) analysis,10 polymerase chain reaction (PCR) testing,11 or viral culture of vesicular exudates. DFA for VZV has an 87% sensitivity.10 PCR has a higher sensitivity (92%),11 is widely available, and is the diagnostic test of choice according to the Centers for Disease Control and Prevention.12
For our patient, we obtained swabs of the oral vesicles and ordered a DFA analysis; however, the sample didn’t show VZV. This may have been due to inadequate sampling. (Proper sampling requires that there be an adequate collection of cells from the base of the vesicles.)
Oral antivirals, steroids are mainstays of treatment
Treatment with an oral steroid such as prednisone in addition to an antiviral such as acyclovir or valacyclovir may reduce the likelihood of postherpetic neuralgia and improve facial motor function; however, these benefits have not been demonstrated in randomized controlled trials.13
Our patient was treated with oral valacyclovir 1 g 3 times a day for 7 days and oral prednisone 50 mg/d for 5 days. After one week of treatment, his symptoms resolved and the vesicles in his mouth crusted over. He did not experience postherpetic neuralgia or have a recurrence.
CORRESPONDENCE
David A. Moss, MD, 4700 North Las Vegas Boulevard, Nellis AFB, NV 89191; david.moss.3@us.af.mil
1. National Organization for Rare Disorders. Ramsay Hunt Syndrome. National Organization for Rare Disorders Web site. Available at: http://www.rarediseases.org/rare-disease-information/rare-diseases/byID/1153/viewFullReport. Accessed December 30, 2014.
2. Sweeney CJ, Gilden DH. Ramsay Hunt syndrome. J Neurol Neurosurg Psychiatry. 2001;71:149-154.
3. Habif TP. Warts, herpes simplex, and other viral infections. Clinical Dermatology. A Color Guide to Diagnosis and Therapy. 5th ed. Maryland Heights, Missouri: Mosby Elsevier; 2010: 467-471.
4. Habif TP. Premalignant and malignant nonmelanoma skin tumors. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Maryland Heights, Missouri: Mosby; 2010:829.
5. Bope ET, Kellerman RD. Pharyngitis. Conn’s Current Therapy 2012. Philadelphia, PA: Saunders; 2012:32.
6. Centor RM, Witherspoon JM, Dalton HP, et al. The diagnosis of strep throat in adults in the emergency room. Med Decis Making. 1981;1:239-246.
7. McIsaac WJ, Goel V, To T, et al. The validity of a sore throat score in family practice. CMAJ. 2000;163:811-815.
8. McIsaac WJ, White D, Tannenbaum D, et al. A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ. 1998;158:75-83.
9. Habif TP. Exanthems and drug eruptions. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Maryland Heights, Missouri: Mosby; 2010:544-547.
10. Chan EL, Brandt K, Horsman GB. Comparison of Chemicon SimulFluor direct fluorescent antibody staining with cell culture and shell vial direct immunoperoxidase staining for detection of herpes simplex virus and with cytospin direct immunofluorescence staining for detection of varicella-zoster virus. Clin Diagn Lab Immunol. 2001;8:909-912.
11. Harbecke R, Oxman MN, Arnold BA, et al; Shingles Prevention Study Group. A real-time PCR assay to identify and discriminate among wild-type and vaccine strains of varicella-zoster virus and herpes simplex virus in clinical specimens, and comparison with the clinical diagnoses. J Med Virol. 2009;81: 1310-1322.
12. Lopez A, Schmid S, Bialek S. Varicella. In: Roush SW, McIntyre L, Baldy LM, eds. Manual for the Surveillance of Vaccine-Preventable Diseases. 5th ed. Atlanta, GA: Centers for Disease Control and Prevention; 2011.
13. Murakami S, Hato N, Horiuchi J, et al. Treatment of Ramsay Hunt syndrome with acyclovir-prednisone: significance of early diagnosis and treatment. Ann Neurol. 1997;41:353-357.
A 79 year-old man sought care at our clinic for pain in his left ear and a severe sore throat that had been bothering him for the past 2 days. He also complained of pain when he swallowed, a decreased appetite, and dizziness. He denied weight loss, fever, tinnitus, subjective hearing loss, unilateral facial droop, or weakness.
On physical exam, we noted vesicles on an erythematous base on his hard palate. They were on the left side and didn’t cross the midline (FIGURE 1). The left pinna was mildly erythematous and swollen (FIGURE 2) without obvious vesicles, although we noted vesicles in the external auditory canal on otoscopic examination. The tympanic membrane was normal, as was the patient’s right ear.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Ramsay Hunt syndrome
Based on our patient’s clinical presentation, we diagnosed herpes zoster oticus—also known as Ramsay Hunt syndrome. This syndrome is a rare complication of herpes zoster that occurs when latent varicella zoster virus (VZV) infection reactivates and spreads to affect the geniculate ganglion.1 An estimated 5 out of every 100,000 people develop Ramsay Hunt syndrome each year in the United States; men and women are equally affected.1 Any patient who’s had VZV infection runs the risk of developing Ramsay Hunt syndrome, but it most often develops in individuals older than age 60.1
Ramsay Hunt syndrome classically presents with unilateral facial paralysis and erythematous vesicles located ipsilaterally on the ear and/or in the mouth. Vesicles in the mouth usually develop on the tongue or hard palate. Other symptoms may include tinnitus, hearing loss, nausea, vomiting, vertigo, and nystagmus.2
Several types of infection are in the differential diagnosis
Because the symptoms of Ramsay Hunt syndrome suggest a possible infection, the differential diagnosis should include herpes simplex virus type 1 (HSV-1), Epstein-Barr virus (EBV), group A Streptococcus (GAS), and measles.
HSV-1 can cause oral symptoms similar to Ramsay Hunt syndrome. However,
HSV-1 doesn’t cause vesicles in the ear. Also worth noting: Recurrent HSV-1 infections normally involve keratinized surfaces such as the vermilion border and gums, but rarely the hard palate.3
EBV can cause multiple systemic symptoms. It can cause leukoplakia in the mouth— most often on the sides of the tongue—but does not cause vesicles.4
GAS presents as a sore throat, fever, anterior cervical lymphadenitis, and a scarlatiniform rash. Oral manifestations can include tonsillar erythema with or without exudate, soft palate petechiae, and a red swollen uvula.5 Use of validated clinical prediction tools, such as the sore throat tool found at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1228750/pdf/cmaj_158_1_75.pdf, can help distinguish GAS infection from other conditions.6-8
Measles typically occurs in children and young adults. Infection in immunized individuals is rare. It presents with fever and the “3 Cs”—cough, coryza, and conjunctivitis. Koplik’s spots are blue to white ulcerated lesions on the buccal mucosa, typically opposite the first and second molars, although they can occur anywhere in the mouth. They precede the generalized maculopapular rash of measles.9
Although it’s a clinical Dx, lab testing can provide confirmation
Diagnosis of Ramsay Hunt syndrome is typically made clinically, but can be confirmed with direct fluorescent antibody (DFA) analysis,10 polymerase chain reaction (PCR) testing,11 or viral culture of vesicular exudates. DFA for VZV has an 87% sensitivity.10 PCR has a higher sensitivity (92%),11 is widely available, and is the diagnostic test of choice according to the Centers for Disease Control and Prevention.12
For our patient, we obtained swabs of the oral vesicles and ordered a DFA analysis; however, the sample didn’t show VZV. This may have been due to inadequate sampling. (Proper sampling requires that there be an adequate collection of cells from the base of the vesicles.)
Oral antivirals, steroids are mainstays of treatment
Treatment with an oral steroid such as prednisone in addition to an antiviral such as acyclovir or valacyclovir may reduce the likelihood of postherpetic neuralgia and improve facial motor function; however, these benefits have not been demonstrated in randomized controlled trials.13
Our patient was treated with oral valacyclovir 1 g 3 times a day for 7 days and oral prednisone 50 mg/d for 5 days. After one week of treatment, his symptoms resolved and the vesicles in his mouth crusted over. He did not experience postherpetic neuralgia or have a recurrence.
CORRESPONDENCE
David A. Moss, MD, 4700 North Las Vegas Boulevard, Nellis AFB, NV 89191; david.moss.3@us.af.mil
A 79 year-old man sought care at our clinic for pain in his left ear and a severe sore throat that had been bothering him for the past 2 days. He also complained of pain when he swallowed, a decreased appetite, and dizziness. He denied weight loss, fever, tinnitus, subjective hearing loss, unilateral facial droop, or weakness.
On physical exam, we noted vesicles on an erythematous base on his hard palate. They were on the left side and didn’t cross the midline (FIGURE 1). The left pinna was mildly erythematous and swollen (FIGURE 2) without obvious vesicles, although we noted vesicles in the external auditory canal on otoscopic examination. The tympanic membrane was normal, as was the patient’s right ear.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Ramsay Hunt syndrome
Based on our patient’s clinical presentation, we diagnosed herpes zoster oticus—also known as Ramsay Hunt syndrome. This syndrome is a rare complication of herpes zoster that occurs when latent varicella zoster virus (VZV) infection reactivates and spreads to affect the geniculate ganglion.1 An estimated 5 out of every 100,000 people develop Ramsay Hunt syndrome each year in the United States; men and women are equally affected.1 Any patient who’s had VZV infection runs the risk of developing Ramsay Hunt syndrome, but it most often develops in individuals older than age 60.1
Ramsay Hunt syndrome classically presents with unilateral facial paralysis and erythematous vesicles located ipsilaterally on the ear and/or in the mouth. Vesicles in the mouth usually develop on the tongue or hard palate. Other symptoms may include tinnitus, hearing loss, nausea, vomiting, vertigo, and nystagmus.2
Several types of infection are in the differential diagnosis
Because the symptoms of Ramsay Hunt syndrome suggest a possible infection, the differential diagnosis should include herpes simplex virus type 1 (HSV-1), Epstein-Barr virus (EBV), group A Streptococcus (GAS), and measles.
HSV-1 can cause oral symptoms similar to Ramsay Hunt syndrome. However,
HSV-1 doesn’t cause vesicles in the ear. Also worth noting: Recurrent HSV-1 infections normally involve keratinized surfaces such as the vermilion border and gums, but rarely the hard palate.3
EBV can cause multiple systemic symptoms. It can cause leukoplakia in the mouth— most often on the sides of the tongue—but does not cause vesicles.4
GAS presents as a sore throat, fever, anterior cervical lymphadenitis, and a scarlatiniform rash. Oral manifestations can include tonsillar erythema with or without exudate, soft palate petechiae, and a red swollen uvula.5 Use of validated clinical prediction tools, such as the sore throat tool found at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1228750/pdf/cmaj_158_1_75.pdf, can help distinguish GAS infection from other conditions.6-8
Measles typically occurs in children and young adults. Infection in immunized individuals is rare. It presents with fever and the “3 Cs”—cough, coryza, and conjunctivitis. Koplik’s spots are blue to white ulcerated lesions on the buccal mucosa, typically opposite the first and second molars, although they can occur anywhere in the mouth. They precede the generalized maculopapular rash of measles.9
Although it’s a clinical Dx, lab testing can provide confirmation
Diagnosis of Ramsay Hunt syndrome is typically made clinically, but can be confirmed with direct fluorescent antibody (DFA) analysis,10 polymerase chain reaction (PCR) testing,11 or viral culture of vesicular exudates. DFA for VZV has an 87% sensitivity.10 PCR has a higher sensitivity (92%),11 is widely available, and is the diagnostic test of choice according to the Centers for Disease Control and Prevention.12
For our patient, we obtained swabs of the oral vesicles and ordered a DFA analysis; however, the sample didn’t show VZV. This may have been due to inadequate sampling. (Proper sampling requires that there be an adequate collection of cells from the base of the vesicles.)
Oral antivirals, steroids are mainstays of treatment
Treatment with an oral steroid such as prednisone in addition to an antiviral such as acyclovir or valacyclovir may reduce the likelihood of postherpetic neuralgia and improve facial motor function; however, these benefits have not been demonstrated in randomized controlled trials.13
Our patient was treated with oral valacyclovir 1 g 3 times a day for 7 days and oral prednisone 50 mg/d for 5 days. After one week of treatment, his symptoms resolved and the vesicles in his mouth crusted over. He did not experience postherpetic neuralgia or have a recurrence.
CORRESPONDENCE
David A. Moss, MD, 4700 North Las Vegas Boulevard, Nellis AFB, NV 89191; david.moss.3@us.af.mil
1. National Organization for Rare Disorders. Ramsay Hunt Syndrome. National Organization for Rare Disorders Web site. Available at: http://www.rarediseases.org/rare-disease-information/rare-diseases/byID/1153/viewFullReport. Accessed December 30, 2014.
2. Sweeney CJ, Gilden DH. Ramsay Hunt syndrome. J Neurol Neurosurg Psychiatry. 2001;71:149-154.
3. Habif TP. Warts, herpes simplex, and other viral infections. Clinical Dermatology. A Color Guide to Diagnosis and Therapy. 5th ed. Maryland Heights, Missouri: Mosby Elsevier; 2010: 467-471.
4. Habif TP. Premalignant and malignant nonmelanoma skin tumors. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Maryland Heights, Missouri: Mosby; 2010:829.
5. Bope ET, Kellerman RD. Pharyngitis. Conn’s Current Therapy 2012. Philadelphia, PA: Saunders; 2012:32.
6. Centor RM, Witherspoon JM, Dalton HP, et al. The diagnosis of strep throat in adults in the emergency room. Med Decis Making. 1981;1:239-246.
7. McIsaac WJ, Goel V, To T, et al. The validity of a sore throat score in family practice. CMAJ. 2000;163:811-815.
8. McIsaac WJ, White D, Tannenbaum D, et al. A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ. 1998;158:75-83.
9. Habif TP. Exanthems and drug eruptions. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Maryland Heights, Missouri: Mosby; 2010:544-547.
10. Chan EL, Brandt K, Horsman GB. Comparison of Chemicon SimulFluor direct fluorescent antibody staining with cell culture and shell vial direct immunoperoxidase staining for detection of herpes simplex virus and with cytospin direct immunofluorescence staining for detection of varicella-zoster virus. Clin Diagn Lab Immunol. 2001;8:909-912.
11. Harbecke R, Oxman MN, Arnold BA, et al; Shingles Prevention Study Group. A real-time PCR assay to identify and discriminate among wild-type and vaccine strains of varicella-zoster virus and herpes simplex virus in clinical specimens, and comparison with the clinical diagnoses. J Med Virol. 2009;81: 1310-1322.
12. Lopez A, Schmid S, Bialek S. Varicella. In: Roush SW, McIntyre L, Baldy LM, eds. Manual for the Surveillance of Vaccine-Preventable Diseases. 5th ed. Atlanta, GA: Centers for Disease Control and Prevention; 2011.
13. Murakami S, Hato N, Horiuchi J, et al. Treatment of Ramsay Hunt syndrome with acyclovir-prednisone: significance of early diagnosis and treatment. Ann Neurol. 1997;41:353-357.
1. National Organization for Rare Disorders. Ramsay Hunt Syndrome. National Organization for Rare Disorders Web site. Available at: http://www.rarediseases.org/rare-disease-information/rare-diseases/byID/1153/viewFullReport. Accessed December 30, 2014.
2. Sweeney CJ, Gilden DH. Ramsay Hunt syndrome. J Neurol Neurosurg Psychiatry. 2001;71:149-154.
3. Habif TP. Warts, herpes simplex, and other viral infections. Clinical Dermatology. A Color Guide to Diagnosis and Therapy. 5th ed. Maryland Heights, Missouri: Mosby Elsevier; 2010: 467-471.
4. Habif TP. Premalignant and malignant nonmelanoma skin tumors. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Maryland Heights, Missouri: Mosby; 2010:829.
5. Bope ET, Kellerman RD. Pharyngitis. Conn’s Current Therapy 2012. Philadelphia, PA: Saunders; 2012:32.
6. Centor RM, Witherspoon JM, Dalton HP, et al. The diagnosis of strep throat in adults in the emergency room. Med Decis Making. 1981;1:239-246.
7. McIsaac WJ, Goel V, To T, et al. The validity of a sore throat score in family practice. CMAJ. 2000;163:811-815.
8. McIsaac WJ, White D, Tannenbaum D, et al. A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ. 1998;158:75-83.
9. Habif TP. Exanthems and drug eruptions. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Maryland Heights, Missouri: Mosby; 2010:544-547.
10. Chan EL, Brandt K, Horsman GB. Comparison of Chemicon SimulFluor direct fluorescent antibody staining with cell culture and shell vial direct immunoperoxidase staining for detection of herpes simplex virus and with cytospin direct immunofluorescence staining for detection of varicella-zoster virus. Clin Diagn Lab Immunol. 2001;8:909-912.
11. Harbecke R, Oxman MN, Arnold BA, et al; Shingles Prevention Study Group. A real-time PCR assay to identify and discriminate among wild-type and vaccine strains of varicella-zoster virus and herpes simplex virus in clinical specimens, and comparison with the clinical diagnoses. J Med Virol. 2009;81: 1310-1322.
12. Lopez A, Schmid S, Bialek S. Varicella. In: Roush SW, McIntyre L, Baldy LM, eds. Manual for the Surveillance of Vaccine-Preventable Diseases. 5th ed. Atlanta, GA: Centers for Disease Control and Prevention; 2011.
13. Murakami S, Hato N, Horiuchi J, et al. Treatment of Ramsay Hunt syndrome with acyclovir-prednisone: significance of early diagnosis and treatment. Ann Neurol. 1997;41:353-357.
