User login
More than 50% of psychiatrists have experienced the death of a patient by suicide.1 For many of us, suicide represents the most feared outcome of a patient’s mental illness and makes managing suicide risk critical to everyday practice.
Unfortunately, we have little ability to predict suicide. Research into risk factors and the use of suicide rating scales have produced no consistently definitive methods to determine who will and who will not attempt or complete suicide.2 The purpose of suicide assessment, then, is not to predict suicide but to help us understand the sources of a patient’s suicidality and develop an informed intervention.
This article describes a practical, commonly accepted approach to suicide risk assessment and intervention, based on the B-SAFE model (Basic Suicide Assessment Five-step Evaluation) proposed by Jacobs et al (Figure).3 Using this method to assess suicide risk can help you answer questions such as:
- Which factors are most important to consider when evaluating suicide risk in my patient?
- What questions should I ask my patient to find out if he or she is suicidal?
- How do I know if a patient is at risk for suicide?
- What emergent interventions are called for when managing the acutely suicidal patient?
- How should I document a suicide risk assessment?
Figure Basic Suicide Assessment Five-step Evaluation (B-SAFE)
Source: Created from information in references 2,11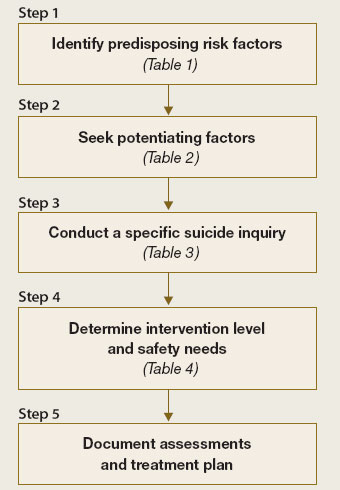
Why ask about suicide?
No single risk factor or combination of risk factors can predict or preclude suicide. Even so, attempting to evaluate an individual’s risk by asking about suicidal thinking, reviewing risk factors, or using clinical rating scales helps you determine the next appropriate action (discharge, medication, psychiatric referral, consultation, or hospitalization).
While talking to patients and evaluating their risk for suicide, you may begin to understand their suffering—described as the most common denominator in suicide2 and perhaps the most important clue to heightened suicide risk. Such an exploration allows you to identify potential:
- risk factors that can be modified
- preventative factors to promote.
Don’t be afraid to ask. Asking about suicidal thoughts is necessary—but not enough—to understand an individual’s potential for suicide. Never be afraid to ask patients about suicide, believing that doing so will “put ideas into their heads.” By the same token, a patient who denies thoughts or plans for suicide may still be at risk.
Identifying at-risk patients is much more difficult than just asking if they are considering suicide. Opening a concerned dialogue can provide a sense of relief to the patient while allowing you to explore:
- the extent and seriousness of the suicidal thoughts
- associated risk factors or conditions, such as depression.
Stepwise risk assessment
The first 3 steps of Jacobs’ B-SAFE model focus on identifying predisposing and protective factors for suicide.3 For an in-depth discussion, consult the American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors4 (available at http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf).
STEP 1: Risk factors. Use the patient interview, medical records, and collateral information to uncover potential suicide risk factors (Table 1).2
Psychopathology. Focus on depression, bipolar disorder, schizophrenia, substance abuse, and personality disorders, which are strongly associated with suicide. These disorders are considered modifiable risk factors—diagnosis and appropriate treatment can diminish suicide risk.
Suicidality has been associated with early depression or bipolar disorder, often before patients receive a diagnosis or effective treatment. Recovery and immediate post-discharge periods also are thought to be times of heightened suicide risk.
Psychosocial variables. Demographic and psychosocial variables may influence suicide risk estimation. A retrospective study of 100 patients who attempted suicide suggests that the most predictive factors for suicide are:
- living alone
- being aged 17 to 35 (although in other studies, more advanced age also has been linked to increased suicide risk3)
- complaints of severe hopelessness, anhedonia, and insomnia.5
Physical illness may potentiate suicide risk. Medical illnesses that produce great pain, disfigurement, limited function, or fear of dependence may reduce a person’s will to live and increase suicide risk.6 Epilepsy has been associated with a 4- to 5-fold increase in suicide risk7 and is the only medical diagnosis to carry a documented increase in suicide among children and adolescents.8 Often these medical disorders coexist with psychiatric disorders, complicating the task of determining independent risk.
Severity of attempts or self-mutilation. When evaluating self-injurious or suicidal behavior in the emergency setting, consider the severity of the attempt as part of overall suicide assessment. Self-injurious behavior (cutting or burning) or impulsive suicide attempts (planned for <3 hours, committed in the presence others, or where discovery is very probable) appear to carry less severity or intent to die than do carefully planned and/or hidden suicide attempts.9 However, consider at high risk for suicide any patient with self-mutilating or suicidal behavior who expresses persistent intent to die; acute stabilization on an in-patient unit may be necessary.
STEP 2: ‘Protective’ factors. Discover and discuss internal and external factors that might help prevent the individual with suicidal thoughts from converting those thoughts into action (Table 2).2 When discussing these potentially protective effects, emphasize the patient’s:
- resilience during past personal crises
- family responsibilities
- religious or spiritual beliefs.
‘No-harm contracts.’ Suicide (or “no-harm”) contracts with patients might help open communication about factors that promote or mitigate suicide risk. Such contacts do not prevent suicide or lessen medicolegal risk in the event of a patient suicide, however.10
STEP 3: Suicide plans. Ask about suicide thoughts, plans, and behaviors (Table 3).11 Probe gently to allow the individual to discuss his or her feelings and to explore the next appropriate avenue of care.
In my experience, patients who reveal passive suicidal ideation (such as, “I sometimes wish I would just die in my sleep”) and strong deterrents to acting on thoughts of suicide (such as, “My children need me,” or “It’s against my religion”) should continue outpatient treatment. Those without deterrents or who discuss active and imminent thoughts and recent actions—writing suicide notes, buying a weapon, stockpiling pills—require emergent evaluation for psychiatric admission. Ask about thoughts of self-injury or mutilation (such as cutting or burning), as well as homicidal ideation.
Recognizing that patients with suicidal thoughts are almost always ambivalent about suicide to some extent—conflicted by simultaneous desires to live and to die—gives you the opportunity to intervene by allying with the part of the patient that wants to live. Creating a therapeutic connection also will help you determine the level of intervention required.
STEP 4: Intervention. Understanding why a patient feels suicidal—gathered in Steps 1 to 3—can help you choose the appropriate intervention. Among the 5 steps, Step 4 relies most heavily on clinical judgment:
- Is the suicidality acute or chronic?
- How great is the risk for suicide?
- To keep the patient safe, how urgent is the required intervention?
Acute risk. Suicidality related to Axis I psychiatric disorders tends to be acute, with prominent pain, anguish, and a desire to escape. Patients may describe a driven quality to the suicidality, which commands a treatment plan that maintains patient safety until suicidal feelings remit.
Hospitalization is often needed, plus focused treatments such as medication, psychotherapy, or electroconvulsive therapy. Intensive outpatient follow-up or partial hospitalization programs might be considered for patients:
- with whom you have a strong therapeutic alliance
- who have sturdy psychosocial support
- whose precipitating factors for suicidality have resolved.
Chronic risk. Suicide risk tends to be more chronic and has an impulsive quality for patients with suicidality related to personality disorders and environmental factors. Personality disordered patients may report feelings of anger, rage, or vengeance connected with their suicidal thoughts.
Hospitalization might become necessary, although multiple hospitalizations can be counter-therapeutic. Attempting in therapy to teach the patient to cope with suicidal thoughts and feelings might be a more effective intervention.
Malingering. Use your best judgment when patients make suicide threats that could represent malingering to achieve hospitalization.
Step 5: Documentation. Document your assessment of the suicidal patient and decision making to:
- clarify the treatment plan
- communicate to other caregivers
- manage medicolegal risk.
Include a brief summary (Box) that is timely, legible, and communicates the estimated degree of risk, known data, diagnosis, and planned interventions such as medications, tests, consultations, and follow-up reassessments.
This 46-year-old, recently divorced man is experiencing his second episode of major depression associated with clear-cut panic attacks and suspected psychotic features. Although he denies current suicidal ideation, the treatment team believes he is at moderate to high risk for suicide because of known past history of serious suicide attempt with first depression, the presence of panic/anxiety, and possibly psychotic features. Additional risk is posed by loss of marital support and his inability to verbalize meaningful protective factors.
The plan is to convert from observation status on the inpatient unit to full admission, as the suicide risk precludes discharge at present. Further medication management and consideration for electroconvulsive therapy will take place, with daily reassessments. Suicide precautions ordered.
Table 1
Factors associated with potential for increased suicide risk
| Variable | Risk Factors |
|---|---|
| Demographic | Male gender, Caucasian race, rural residence, possibly age (varies among studies) |
| Imprisoned; widowed, divorced, or separated; living alone; no children or no children living in the home | |
| Psychosocial | Lack or loss of social supports, recent loss of employment, decrease in socioeconomic status or poverty, hopelessness |
| History of victimization (physical or sexual abuse), psychological turmoil, severe relationship conflict, aggressive or impulsive traits | |
| Writing suicide notes; family history of suicide, previous attempts, ‘imitation’ suicide, gun ownership | |
| Occupational risk (physicians, dentists, nurses, pharmacists, veterinarians, farmers) | |
| Psychiatric | Psychiatric diagnosis of recent onset |
| Mood disorder, particularly major depression and bipolar disorder | |
| Schizophrenia; alcohol or other substance abuse or addiction; personality disorder; panic attacks or severe psychic anxiety | |
| Insomnia; poor concentration or confusion; anhedonia | |
| Medical | Huntington’s disease, stroke, multiple sclerosis, head injury, spinal cord injury, systemic lupus erythematosus, AIDS |
| Epilepsy, pain, malignant neoplasms, peptic ulcer disease, renal disease | |
| Source: Adapted with permission from reference 3 | |
Table 2
Potentially protective factors against suicide
| Internal |
| Successful past responses to stress |
| Positive coping skills |
| Spirituality |
| Capacity for reality testing |
| Frustration tolerance/optimism |
| Overall individual resiliency |
| External |
| Children or pets in the home |
| Religious prohibition or beliefs |
| Positive therapeutic relationships |
| Sense of responsibility to family |
| Social supports and connections |
| Financial incentives or deterrents |
| Source: Adapted from reference 11 |
Table 3
Evaluating suicide risk: Questions to ask patients
| Have you felt so sad or depressed that you thought life is not worth living? |
| Have you thought about hurting yourself or taking your own life? |
| Have you thought about a way or plan to kill yourself? |
| Do you have the means to complete the plan? (such as, do you have access to weapons or pills?) |
| Have you practiced or rehearsed this plan to end your own life? |
| Do you have a location picked out? |
| What has stopped you from following through with the plan? |
| Have you ever attempted suicide? |
| Has anyone in your family ever attempted or committed suicide? |
| Source: Adapted with permission from reference 3 |
Interventions for suicidal patients
Physical protection. Take decisive action when you determine that suicide risk is elevated and imminent. Pursue urgent psychiatric hospitalization, with or without patient consent, in accordance with local probate and involuntary commitment statutes.
The logistics of protective action can be challenging; transportation is often required, and the patient is not always cooperative with admission. Table 4 lists measures and precautions that can help keep the suicidal patient safe.
Disease-specific interventions. Because suicidal ideation is often symptomatic of a primary psychiatric disorder, rapidly identifying major depression, bipolar disorder, or a psychotic illness is crucial to reducing suicidal thoughts and behaviors. Prescribe appropriate antidepressants, mood stabilizers, and antipsychotics at adequate doses and for sufficient duration.
Be vigilant for distressing symptoms that may be elevating the patient’s suicide risk, such as anxiety, panic, agitation, insomnia, or pain. Pharmacotherapies—such as anxiolytics, sedative-hypnotics, antipsychotics, or analgesics—may rapidly reduce suffering.
Impulsivity associated with substance use disorders—particularly during intoxication and withdrawal syndromes—requires aggressive attempts by the treatment team to engage the patient in detoxification and rehabilitation.
Direct antisuicide therapy. Clozapine carries an FDA-approved indication for preventing suicide in patients with schizophrenia or schizoaffective disorder. The mechanism by which clozapine helps prevent suicide is not known, but its anti-suicidal effects appear to be independent of its antipsychotic effects.12
Lithium has been reported to reduce risk of suicide and suicide attempts in patients with bipolar disorder, perhaps by as much as 80%.13 Such benefit has not been observed with other mood stabilizers, suggesting that lithium confers protective effects against suicide beyond its mood-stabilizing effects. Suicide risk is known to increase after lithium is discontinued.14
Lithium’s antisuicidal effects may arise from its ability to enhance serotonin. This theory, although unproven, is consistent with observations associating central serotonergic deficiency with suicidal and aggressive behaviors.
Psychosocial measures. Address psychosocial variables that may increase suicide risk (Table 1). Recruit and involve the patient’s support system, augmented with a close follow-up plan. Case management to explore housing and job opportunities can help. Work with the patient’s family or others to remove guns from the patient’s access. Individual, marital, and family therapies can reduce conflicts and strengthen coping skills.
Table 4
Safety measures to protect the suicidal patient
| Hospitalize—voluntarily or involuntarily—on a locked psychiatric unit |
| Provide constant 1-to-1 observation by staff |
| Transport the patient, accompanied by adequate personnel |
| Use physical restraints or seclusion while maintaining continuous observation |
| Employ metal detector to remove dangerous, hidden objects |
| Remove and secure patient’s belongings (bags, coats, purses may contain pills or weapons) |
| Search visitors’ belongings before allowing access to unit |
| Ensure that inpatient unit meets all coded safety regulations |
Related resources
- National Suicide Prevention Lifeline, sponsored by the Substance Abuse & Mental Health Services Administration: 1-800-SUICIDE or 1-800-273-TALK (8255); www.suicidepreventionlifeline.org.
- American Foundation for Suicide Prevention (AFSP) 1-888-333-AFSP; www.afsp.org.
- Simon RI, Hales RE. Textbook of suicide assessment and management. Washington, DC: American Psychiatric Publishing; 2006.
Drug brand names
- Clozapine • Clozaril
- Lithium • Eskalith, Lithobid, others
Disclosure
Dr. Muzina has received grants from or served as a consultant to Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Novartis Pharmaceuticals Corp., Pfizer, and Repligen.
1. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry 1988;145(2):224-8.
2. Muzina DJ. What physicians can do to prevent suicide. Cleve Clin J Med 2004;71(3):242-50.
3. Jacobs DG, Brewer ML, Klein-Benheim M. Suicide assessment: an overview and recommended protocol. In: Jacobs DG, ed. The Harvard Medical School guide to suicide assessment and intervention.. San Francisco, CA: Jossey-Bass Publishers; 1999:3-39.
4. Jacobs DG, Baldessarini RJ, Conwell Y, et al. American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors. Available at: http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf. Accessed May 14, 2007.
5. Hall RC, Platt DE, Hall RC. Suicide risk assessment: a review of risk factors for suicide in 100 patients who made severe suicide attempts. Evaluation of suicide risk in a time of managed care. Psychosomatics 1999;40(1):18-27.
6. Mackenzie TB, Popkin MK. Suicide in the medical patient. Int J Psychiatry Med 1987;17(1):3-22.
7. Barraclough BM. The suicide rate of epilepsy. Acta Psychiatr Scand 1987;76(4):339-45
8. Brent DA, Kolko DJ, Allan MJ, Brown RV. Suicidality in affectively disordered adolescent inpatients. J Am Acad Child Adolesc Psychiatry 1990;29(4):586-93.
9. Polewka A, Mikolaszek-Boba M, Chrostek Maj J, Groszek B. The characteristics of suicide attempts based on the suicidal intent scale scores. Przegl Lek 2005;62(6):415-8.
10. Lewis LM. No-harm contracts: a review of what we know. Suicide Life Threat Behav 2007;37(1):50-7.
11. Jacobs DG. A resource guide for implementing the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) 2007 patient safety goals on suicide. Available at: http://www.sprc.org/library/jcahosafetygoals.pdf. Accessed May 14, 2007.
12. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry 2003;60(1):82-91.
13. Baldessarini RJ, Tondo L, Davis P, et al. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disord 2006;8(5 Pt 2):625-39.
14. Baldessarini RJ, Tondo L, Viguera AC. Discontinuing lithium maintenance treatment in bipolar disorders: risks and implications. Bipolar Disord 1999;1(1):17-24.
More than 50% of psychiatrists have experienced the death of a patient by suicide.1 For many of us, suicide represents the most feared outcome of a patient’s mental illness and makes managing suicide risk critical to everyday practice.
Unfortunately, we have little ability to predict suicide. Research into risk factors and the use of suicide rating scales have produced no consistently definitive methods to determine who will and who will not attempt or complete suicide.2 The purpose of suicide assessment, then, is not to predict suicide but to help us understand the sources of a patient’s suicidality and develop an informed intervention.
This article describes a practical, commonly accepted approach to suicide risk assessment and intervention, based on the B-SAFE model (Basic Suicide Assessment Five-step Evaluation) proposed by Jacobs et al (Figure).3 Using this method to assess suicide risk can help you answer questions such as:
- Which factors are most important to consider when evaluating suicide risk in my patient?
- What questions should I ask my patient to find out if he or she is suicidal?
- How do I know if a patient is at risk for suicide?
- What emergent interventions are called for when managing the acutely suicidal patient?
- How should I document a suicide risk assessment?
Figure Basic Suicide Assessment Five-step Evaluation (B-SAFE)
Source: Created from information in references 2,11
Why ask about suicide?
No single risk factor or combination of risk factors can predict or preclude suicide. Even so, attempting to evaluate an individual’s risk by asking about suicidal thinking, reviewing risk factors, or using clinical rating scales helps you determine the next appropriate action (discharge, medication, psychiatric referral, consultation, or hospitalization).
While talking to patients and evaluating their risk for suicide, you may begin to understand their suffering—described as the most common denominator in suicide2 and perhaps the most important clue to heightened suicide risk. Such an exploration allows you to identify potential:
- risk factors that can be modified
- preventative factors to promote.
Don’t be afraid to ask. Asking about suicidal thoughts is necessary—but not enough—to understand an individual’s potential for suicide. Never be afraid to ask patients about suicide, believing that doing so will “put ideas into their heads.” By the same token, a patient who denies thoughts or plans for suicide may still be at risk.
Identifying at-risk patients is much more difficult than just asking if they are considering suicide. Opening a concerned dialogue can provide a sense of relief to the patient while allowing you to explore:
- the extent and seriousness of the suicidal thoughts
- associated risk factors or conditions, such as depression.
Stepwise risk assessment
The first 3 steps of Jacobs’ B-SAFE model focus on identifying predisposing and protective factors for suicide.3 For an in-depth discussion, consult the American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors4 (available at http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf).
STEP 1: Risk factors. Use the patient interview, medical records, and collateral information to uncover potential suicide risk factors (Table 1).2
Psychopathology. Focus on depression, bipolar disorder, schizophrenia, substance abuse, and personality disorders, which are strongly associated with suicide. These disorders are considered modifiable risk factors—diagnosis and appropriate treatment can diminish suicide risk.
Suicidality has been associated with early depression or bipolar disorder, often before patients receive a diagnosis or effective treatment. Recovery and immediate post-discharge periods also are thought to be times of heightened suicide risk.
Psychosocial variables. Demographic and psychosocial variables may influence suicide risk estimation. A retrospective study of 100 patients who attempted suicide suggests that the most predictive factors for suicide are:
- living alone
- being aged 17 to 35 (although in other studies, more advanced age also has been linked to increased suicide risk3)
- complaints of severe hopelessness, anhedonia, and insomnia.5
Physical illness may potentiate suicide risk. Medical illnesses that produce great pain, disfigurement, limited function, or fear of dependence may reduce a person’s will to live and increase suicide risk.6 Epilepsy has been associated with a 4- to 5-fold increase in suicide risk7 and is the only medical diagnosis to carry a documented increase in suicide among children and adolescents.8 Often these medical disorders coexist with psychiatric disorders, complicating the task of determining independent risk.
Severity of attempts or self-mutilation. When evaluating self-injurious or suicidal behavior in the emergency setting, consider the severity of the attempt as part of overall suicide assessment. Self-injurious behavior (cutting or burning) or impulsive suicide attempts (planned for <3 hours, committed in the presence others, or where discovery is very probable) appear to carry less severity or intent to die than do carefully planned and/or hidden suicide attempts.9 However, consider at high risk for suicide any patient with self-mutilating or suicidal behavior who expresses persistent intent to die; acute stabilization on an in-patient unit may be necessary.
STEP 2: ‘Protective’ factors. Discover and discuss internal and external factors that might help prevent the individual with suicidal thoughts from converting those thoughts into action (Table 2).2 When discussing these potentially protective effects, emphasize the patient’s:
- resilience during past personal crises
- family responsibilities
- religious or spiritual beliefs.
‘No-harm contracts.’ Suicide (or “no-harm”) contracts with patients might help open communication about factors that promote or mitigate suicide risk. Such contacts do not prevent suicide or lessen medicolegal risk in the event of a patient suicide, however.10
STEP 3: Suicide plans. Ask about suicide thoughts, plans, and behaviors (Table 3).11 Probe gently to allow the individual to discuss his or her feelings and to explore the next appropriate avenue of care.
In my experience, patients who reveal passive suicidal ideation (such as, “I sometimes wish I would just die in my sleep”) and strong deterrents to acting on thoughts of suicide (such as, “My children need me,” or “It’s against my religion”) should continue outpatient treatment. Those without deterrents or who discuss active and imminent thoughts and recent actions—writing suicide notes, buying a weapon, stockpiling pills—require emergent evaluation for psychiatric admission. Ask about thoughts of self-injury or mutilation (such as cutting or burning), as well as homicidal ideation.
Recognizing that patients with suicidal thoughts are almost always ambivalent about suicide to some extent—conflicted by simultaneous desires to live and to die—gives you the opportunity to intervene by allying with the part of the patient that wants to live. Creating a therapeutic connection also will help you determine the level of intervention required.
STEP 4: Intervention. Understanding why a patient feels suicidal—gathered in Steps 1 to 3—can help you choose the appropriate intervention. Among the 5 steps, Step 4 relies most heavily on clinical judgment:
- Is the suicidality acute or chronic?
- How great is the risk for suicide?
- To keep the patient safe, how urgent is the required intervention?
Acute risk. Suicidality related to Axis I psychiatric disorders tends to be acute, with prominent pain, anguish, and a desire to escape. Patients may describe a driven quality to the suicidality, which commands a treatment plan that maintains patient safety until suicidal feelings remit.
Hospitalization is often needed, plus focused treatments such as medication, psychotherapy, or electroconvulsive therapy. Intensive outpatient follow-up or partial hospitalization programs might be considered for patients:
- with whom you have a strong therapeutic alliance
- who have sturdy psychosocial support
- whose precipitating factors for suicidality have resolved.
Chronic risk. Suicide risk tends to be more chronic and has an impulsive quality for patients with suicidality related to personality disorders and environmental factors. Personality disordered patients may report feelings of anger, rage, or vengeance connected with their suicidal thoughts.
Hospitalization might become necessary, although multiple hospitalizations can be counter-therapeutic. Attempting in therapy to teach the patient to cope with suicidal thoughts and feelings might be a more effective intervention.
Malingering. Use your best judgment when patients make suicide threats that could represent malingering to achieve hospitalization.
Step 5: Documentation. Document your assessment of the suicidal patient and decision making to:
- clarify the treatment plan
- communicate to other caregivers
- manage medicolegal risk.
Include a brief summary (Box) that is timely, legible, and communicates the estimated degree of risk, known data, diagnosis, and planned interventions such as medications, tests, consultations, and follow-up reassessments.
This 46-year-old, recently divorced man is experiencing his second episode of major depression associated with clear-cut panic attacks and suspected psychotic features. Although he denies current suicidal ideation, the treatment team believes he is at moderate to high risk for suicide because of known past history of serious suicide attempt with first depression, the presence of panic/anxiety, and possibly psychotic features. Additional risk is posed by loss of marital support and his inability to verbalize meaningful protective factors.
The plan is to convert from observation status on the inpatient unit to full admission, as the suicide risk precludes discharge at present. Further medication management and consideration for electroconvulsive therapy will take place, with daily reassessments. Suicide precautions ordered.
Table 1
Factors associated with potential for increased suicide risk
| Variable | Risk Factors |
|---|---|
| Demographic | Male gender, Caucasian race, rural residence, possibly age (varies among studies) |
| Imprisoned; widowed, divorced, or separated; living alone; no children or no children living in the home | |
| Psychosocial | Lack or loss of social supports, recent loss of employment, decrease in socioeconomic status or poverty, hopelessness |
| History of victimization (physical or sexual abuse), psychological turmoil, severe relationship conflict, aggressive or impulsive traits | |
| Writing suicide notes; family history of suicide, previous attempts, ‘imitation’ suicide, gun ownership | |
| Occupational risk (physicians, dentists, nurses, pharmacists, veterinarians, farmers) | |
| Psychiatric | Psychiatric diagnosis of recent onset |
| Mood disorder, particularly major depression and bipolar disorder | |
| Schizophrenia; alcohol or other substance abuse or addiction; personality disorder; panic attacks or severe psychic anxiety | |
| Insomnia; poor concentration or confusion; anhedonia | |
| Medical | Huntington’s disease, stroke, multiple sclerosis, head injury, spinal cord injury, systemic lupus erythematosus, AIDS |
| Epilepsy, pain, malignant neoplasms, peptic ulcer disease, renal disease | |
| Source: Adapted with permission from reference 3 | |
Table 2
Potentially protective factors against suicide
| Internal |
| Successful past responses to stress |
| Positive coping skills |
| Spirituality |
| Capacity for reality testing |
| Frustration tolerance/optimism |
| Overall individual resiliency |
| External |
| Children or pets in the home |
| Religious prohibition or beliefs |
| Positive therapeutic relationships |
| Sense of responsibility to family |
| Social supports and connections |
| Financial incentives or deterrents |
| Source: Adapted from reference 11 |
Table 3
Evaluating suicide risk: Questions to ask patients
| Have you felt so sad or depressed that you thought life is not worth living? |
| Have you thought about hurting yourself or taking your own life? |
| Have you thought about a way or plan to kill yourself? |
| Do you have the means to complete the plan? (such as, do you have access to weapons or pills?) |
| Have you practiced or rehearsed this plan to end your own life? |
| Do you have a location picked out? |
| What has stopped you from following through with the plan? |
| Have you ever attempted suicide? |
| Has anyone in your family ever attempted or committed suicide? |
| Source: Adapted with permission from reference 3 |
Interventions for suicidal patients
Physical protection. Take decisive action when you determine that suicide risk is elevated and imminent. Pursue urgent psychiatric hospitalization, with or without patient consent, in accordance with local probate and involuntary commitment statutes.
The logistics of protective action can be challenging; transportation is often required, and the patient is not always cooperative with admission. Table 4 lists measures and precautions that can help keep the suicidal patient safe.
Disease-specific interventions. Because suicidal ideation is often symptomatic of a primary psychiatric disorder, rapidly identifying major depression, bipolar disorder, or a psychotic illness is crucial to reducing suicidal thoughts and behaviors. Prescribe appropriate antidepressants, mood stabilizers, and antipsychotics at adequate doses and for sufficient duration.
Be vigilant for distressing symptoms that may be elevating the patient’s suicide risk, such as anxiety, panic, agitation, insomnia, or pain. Pharmacotherapies—such as anxiolytics, sedative-hypnotics, antipsychotics, or analgesics—may rapidly reduce suffering.
Impulsivity associated with substance use disorders—particularly during intoxication and withdrawal syndromes—requires aggressive attempts by the treatment team to engage the patient in detoxification and rehabilitation.
Direct antisuicide therapy. Clozapine carries an FDA-approved indication for preventing suicide in patients with schizophrenia or schizoaffective disorder. The mechanism by which clozapine helps prevent suicide is not known, but its anti-suicidal effects appear to be independent of its antipsychotic effects.12
Lithium has been reported to reduce risk of suicide and suicide attempts in patients with bipolar disorder, perhaps by as much as 80%.13 Such benefit has not been observed with other mood stabilizers, suggesting that lithium confers protective effects against suicide beyond its mood-stabilizing effects. Suicide risk is known to increase after lithium is discontinued.14
Lithium’s antisuicidal effects may arise from its ability to enhance serotonin. This theory, although unproven, is consistent with observations associating central serotonergic deficiency with suicidal and aggressive behaviors.
Psychosocial measures. Address psychosocial variables that may increase suicide risk (Table 1). Recruit and involve the patient’s support system, augmented with a close follow-up plan. Case management to explore housing and job opportunities can help. Work with the patient’s family or others to remove guns from the patient’s access. Individual, marital, and family therapies can reduce conflicts and strengthen coping skills.
Table 4
Safety measures to protect the suicidal patient
| Hospitalize—voluntarily or involuntarily—on a locked psychiatric unit |
| Provide constant 1-to-1 observation by staff |
| Transport the patient, accompanied by adequate personnel |
| Use physical restraints or seclusion while maintaining continuous observation |
| Employ metal detector to remove dangerous, hidden objects |
| Remove and secure patient’s belongings (bags, coats, purses may contain pills or weapons) |
| Search visitors’ belongings before allowing access to unit |
| Ensure that inpatient unit meets all coded safety regulations |
Related resources
- National Suicide Prevention Lifeline, sponsored by the Substance Abuse & Mental Health Services Administration: 1-800-SUICIDE or 1-800-273-TALK (8255); www.suicidepreventionlifeline.org.
- American Foundation for Suicide Prevention (AFSP) 1-888-333-AFSP; www.afsp.org.
- Simon RI, Hales RE. Textbook of suicide assessment and management. Washington, DC: American Psychiatric Publishing; 2006.
Drug brand names
- Clozapine • Clozaril
- Lithium • Eskalith, Lithobid, others
Disclosure
Dr. Muzina has received grants from or served as a consultant to Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Novartis Pharmaceuticals Corp., Pfizer, and Repligen.
More than 50% of psychiatrists have experienced the death of a patient by suicide.1 For many of us, suicide represents the most feared outcome of a patient’s mental illness and makes managing suicide risk critical to everyday practice.
Unfortunately, we have little ability to predict suicide. Research into risk factors and the use of suicide rating scales have produced no consistently definitive methods to determine who will and who will not attempt or complete suicide.2 The purpose of suicide assessment, then, is not to predict suicide but to help us understand the sources of a patient’s suicidality and develop an informed intervention.
This article describes a practical, commonly accepted approach to suicide risk assessment and intervention, based on the B-SAFE model (Basic Suicide Assessment Five-step Evaluation) proposed by Jacobs et al (Figure).3 Using this method to assess suicide risk can help you answer questions such as:
- Which factors are most important to consider when evaluating suicide risk in my patient?
- What questions should I ask my patient to find out if he or she is suicidal?
- How do I know if a patient is at risk for suicide?
- What emergent interventions are called for when managing the acutely suicidal patient?
- How should I document a suicide risk assessment?
Figure Basic Suicide Assessment Five-step Evaluation (B-SAFE)
Source: Created from information in references 2,11
Why ask about suicide?
No single risk factor or combination of risk factors can predict or preclude suicide. Even so, attempting to evaluate an individual’s risk by asking about suicidal thinking, reviewing risk factors, or using clinical rating scales helps you determine the next appropriate action (discharge, medication, psychiatric referral, consultation, or hospitalization).
While talking to patients and evaluating their risk for suicide, you may begin to understand their suffering—described as the most common denominator in suicide2 and perhaps the most important clue to heightened suicide risk. Such an exploration allows you to identify potential:
- risk factors that can be modified
- preventative factors to promote.
Don’t be afraid to ask. Asking about suicidal thoughts is necessary—but not enough—to understand an individual’s potential for suicide. Never be afraid to ask patients about suicide, believing that doing so will “put ideas into their heads.” By the same token, a patient who denies thoughts or plans for suicide may still be at risk.
Identifying at-risk patients is much more difficult than just asking if they are considering suicide. Opening a concerned dialogue can provide a sense of relief to the patient while allowing you to explore:
- the extent and seriousness of the suicidal thoughts
- associated risk factors or conditions, such as depression.
Stepwise risk assessment
The first 3 steps of Jacobs’ B-SAFE model focus on identifying predisposing and protective factors for suicide.3 For an in-depth discussion, consult the American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors4 (available at http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf).
STEP 1: Risk factors. Use the patient interview, medical records, and collateral information to uncover potential suicide risk factors (Table 1).2
Psychopathology. Focus on depression, bipolar disorder, schizophrenia, substance abuse, and personality disorders, which are strongly associated with suicide. These disorders are considered modifiable risk factors—diagnosis and appropriate treatment can diminish suicide risk.
Suicidality has been associated with early depression or bipolar disorder, often before patients receive a diagnosis or effective treatment. Recovery and immediate post-discharge periods also are thought to be times of heightened suicide risk.
Psychosocial variables. Demographic and psychosocial variables may influence suicide risk estimation. A retrospective study of 100 patients who attempted suicide suggests that the most predictive factors for suicide are:
- living alone
- being aged 17 to 35 (although in other studies, more advanced age also has been linked to increased suicide risk3)
- complaints of severe hopelessness, anhedonia, and insomnia.5
Physical illness may potentiate suicide risk. Medical illnesses that produce great pain, disfigurement, limited function, or fear of dependence may reduce a person’s will to live and increase suicide risk.6 Epilepsy has been associated with a 4- to 5-fold increase in suicide risk7 and is the only medical diagnosis to carry a documented increase in suicide among children and adolescents.8 Often these medical disorders coexist with psychiatric disorders, complicating the task of determining independent risk.
Severity of attempts or self-mutilation. When evaluating self-injurious or suicidal behavior in the emergency setting, consider the severity of the attempt as part of overall suicide assessment. Self-injurious behavior (cutting or burning) or impulsive suicide attempts (planned for <3 hours, committed in the presence others, or where discovery is very probable) appear to carry less severity or intent to die than do carefully planned and/or hidden suicide attempts.9 However, consider at high risk for suicide any patient with self-mutilating or suicidal behavior who expresses persistent intent to die; acute stabilization on an in-patient unit may be necessary.
STEP 2: ‘Protective’ factors. Discover and discuss internal and external factors that might help prevent the individual with suicidal thoughts from converting those thoughts into action (Table 2).2 When discussing these potentially protective effects, emphasize the patient’s:
- resilience during past personal crises
- family responsibilities
- religious or spiritual beliefs.
‘No-harm contracts.’ Suicide (or “no-harm”) contracts with patients might help open communication about factors that promote or mitigate suicide risk. Such contacts do not prevent suicide or lessen medicolegal risk in the event of a patient suicide, however.10
STEP 3: Suicide plans. Ask about suicide thoughts, plans, and behaviors (Table 3).11 Probe gently to allow the individual to discuss his or her feelings and to explore the next appropriate avenue of care.
In my experience, patients who reveal passive suicidal ideation (such as, “I sometimes wish I would just die in my sleep”) and strong deterrents to acting on thoughts of suicide (such as, “My children need me,” or “It’s against my religion”) should continue outpatient treatment. Those without deterrents or who discuss active and imminent thoughts and recent actions—writing suicide notes, buying a weapon, stockpiling pills—require emergent evaluation for psychiatric admission. Ask about thoughts of self-injury or mutilation (such as cutting or burning), as well as homicidal ideation.
Recognizing that patients with suicidal thoughts are almost always ambivalent about suicide to some extent—conflicted by simultaneous desires to live and to die—gives you the opportunity to intervene by allying with the part of the patient that wants to live. Creating a therapeutic connection also will help you determine the level of intervention required.
STEP 4: Intervention. Understanding why a patient feels suicidal—gathered in Steps 1 to 3—can help you choose the appropriate intervention. Among the 5 steps, Step 4 relies most heavily on clinical judgment:
- Is the suicidality acute or chronic?
- How great is the risk for suicide?
- To keep the patient safe, how urgent is the required intervention?
Acute risk. Suicidality related to Axis I psychiatric disorders tends to be acute, with prominent pain, anguish, and a desire to escape. Patients may describe a driven quality to the suicidality, which commands a treatment plan that maintains patient safety until suicidal feelings remit.
Hospitalization is often needed, plus focused treatments such as medication, psychotherapy, or electroconvulsive therapy. Intensive outpatient follow-up or partial hospitalization programs might be considered for patients:
- with whom you have a strong therapeutic alliance
- who have sturdy psychosocial support
- whose precipitating factors for suicidality have resolved.
Chronic risk. Suicide risk tends to be more chronic and has an impulsive quality for patients with suicidality related to personality disorders and environmental factors. Personality disordered patients may report feelings of anger, rage, or vengeance connected with their suicidal thoughts.
Hospitalization might become necessary, although multiple hospitalizations can be counter-therapeutic. Attempting in therapy to teach the patient to cope with suicidal thoughts and feelings might be a more effective intervention.
Malingering. Use your best judgment when patients make suicide threats that could represent malingering to achieve hospitalization.
Step 5: Documentation. Document your assessment of the suicidal patient and decision making to:
- clarify the treatment plan
- communicate to other caregivers
- manage medicolegal risk.
Include a brief summary (Box) that is timely, legible, and communicates the estimated degree of risk, known data, diagnosis, and planned interventions such as medications, tests, consultations, and follow-up reassessments.
This 46-year-old, recently divorced man is experiencing his second episode of major depression associated with clear-cut panic attacks and suspected psychotic features. Although he denies current suicidal ideation, the treatment team believes he is at moderate to high risk for suicide because of known past history of serious suicide attempt with first depression, the presence of panic/anxiety, and possibly psychotic features. Additional risk is posed by loss of marital support and his inability to verbalize meaningful protective factors.
The plan is to convert from observation status on the inpatient unit to full admission, as the suicide risk precludes discharge at present. Further medication management and consideration for electroconvulsive therapy will take place, with daily reassessments. Suicide precautions ordered.
Table 1
Factors associated with potential for increased suicide risk
| Variable | Risk Factors |
|---|---|
| Demographic | Male gender, Caucasian race, rural residence, possibly age (varies among studies) |
| Imprisoned; widowed, divorced, or separated; living alone; no children or no children living in the home | |
| Psychosocial | Lack or loss of social supports, recent loss of employment, decrease in socioeconomic status or poverty, hopelessness |
| History of victimization (physical or sexual abuse), psychological turmoil, severe relationship conflict, aggressive or impulsive traits | |
| Writing suicide notes; family history of suicide, previous attempts, ‘imitation’ suicide, gun ownership | |
| Occupational risk (physicians, dentists, nurses, pharmacists, veterinarians, farmers) | |
| Psychiatric | Psychiatric diagnosis of recent onset |
| Mood disorder, particularly major depression and bipolar disorder | |
| Schizophrenia; alcohol or other substance abuse or addiction; personality disorder; panic attacks or severe psychic anxiety | |
| Insomnia; poor concentration or confusion; anhedonia | |
| Medical | Huntington’s disease, stroke, multiple sclerosis, head injury, spinal cord injury, systemic lupus erythematosus, AIDS |
| Epilepsy, pain, malignant neoplasms, peptic ulcer disease, renal disease | |
| Source: Adapted with permission from reference 3 | |
Table 2
Potentially protective factors against suicide
| Internal |
| Successful past responses to stress |
| Positive coping skills |
| Spirituality |
| Capacity for reality testing |
| Frustration tolerance/optimism |
| Overall individual resiliency |
| External |
| Children or pets in the home |
| Religious prohibition or beliefs |
| Positive therapeutic relationships |
| Sense of responsibility to family |
| Social supports and connections |
| Financial incentives or deterrents |
| Source: Adapted from reference 11 |
Table 3
Evaluating suicide risk: Questions to ask patients
| Have you felt so sad or depressed that you thought life is not worth living? |
| Have you thought about hurting yourself or taking your own life? |
| Have you thought about a way or plan to kill yourself? |
| Do you have the means to complete the plan? (such as, do you have access to weapons or pills?) |
| Have you practiced or rehearsed this plan to end your own life? |
| Do you have a location picked out? |
| What has stopped you from following through with the plan? |
| Have you ever attempted suicide? |
| Has anyone in your family ever attempted or committed suicide? |
| Source: Adapted with permission from reference 3 |
Interventions for suicidal patients
Physical protection. Take decisive action when you determine that suicide risk is elevated and imminent. Pursue urgent psychiatric hospitalization, with or without patient consent, in accordance with local probate and involuntary commitment statutes.
The logistics of protective action can be challenging; transportation is often required, and the patient is not always cooperative with admission. Table 4 lists measures and precautions that can help keep the suicidal patient safe.
Disease-specific interventions. Because suicidal ideation is often symptomatic of a primary psychiatric disorder, rapidly identifying major depression, bipolar disorder, or a psychotic illness is crucial to reducing suicidal thoughts and behaviors. Prescribe appropriate antidepressants, mood stabilizers, and antipsychotics at adequate doses and for sufficient duration.
Be vigilant for distressing symptoms that may be elevating the patient’s suicide risk, such as anxiety, panic, agitation, insomnia, or pain. Pharmacotherapies—such as anxiolytics, sedative-hypnotics, antipsychotics, or analgesics—may rapidly reduce suffering.
Impulsivity associated with substance use disorders—particularly during intoxication and withdrawal syndromes—requires aggressive attempts by the treatment team to engage the patient in detoxification and rehabilitation.
Direct antisuicide therapy. Clozapine carries an FDA-approved indication for preventing suicide in patients with schizophrenia or schizoaffective disorder. The mechanism by which clozapine helps prevent suicide is not known, but its anti-suicidal effects appear to be independent of its antipsychotic effects.12
Lithium has been reported to reduce risk of suicide and suicide attempts in patients with bipolar disorder, perhaps by as much as 80%.13 Such benefit has not been observed with other mood stabilizers, suggesting that lithium confers protective effects against suicide beyond its mood-stabilizing effects. Suicide risk is known to increase after lithium is discontinued.14
Lithium’s antisuicidal effects may arise from its ability to enhance serotonin. This theory, although unproven, is consistent with observations associating central serotonergic deficiency with suicidal and aggressive behaviors.
Psychosocial measures. Address psychosocial variables that may increase suicide risk (Table 1). Recruit and involve the patient’s support system, augmented with a close follow-up plan. Case management to explore housing and job opportunities can help. Work with the patient’s family or others to remove guns from the patient’s access. Individual, marital, and family therapies can reduce conflicts and strengthen coping skills.
Table 4
Safety measures to protect the suicidal patient
| Hospitalize—voluntarily or involuntarily—on a locked psychiatric unit |
| Provide constant 1-to-1 observation by staff |
| Transport the patient, accompanied by adequate personnel |
| Use physical restraints or seclusion while maintaining continuous observation |
| Employ metal detector to remove dangerous, hidden objects |
| Remove and secure patient’s belongings (bags, coats, purses may contain pills or weapons) |
| Search visitors’ belongings before allowing access to unit |
| Ensure that inpatient unit meets all coded safety regulations |
Related resources
- National Suicide Prevention Lifeline, sponsored by the Substance Abuse & Mental Health Services Administration: 1-800-SUICIDE or 1-800-273-TALK (8255); www.suicidepreventionlifeline.org.
- American Foundation for Suicide Prevention (AFSP) 1-888-333-AFSP; www.afsp.org.
- Simon RI, Hales RE. Textbook of suicide assessment and management. Washington, DC: American Psychiatric Publishing; 2006.
Drug brand names
- Clozapine • Clozaril
- Lithium • Eskalith, Lithobid, others
Disclosure
Dr. Muzina has received grants from or served as a consultant to Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Novartis Pharmaceuticals Corp., Pfizer, and Repligen.
1. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry 1988;145(2):224-8.
2. Muzina DJ. What physicians can do to prevent suicide. Cleve Clin J Med 2004;71(3):242-50.
3. Jacobs DG, Brewer ML, Klein-Benheim M. Suicide assessment: an overview and recommended protocol. In: Jacobs DG, ed. The Harvard Medical School guide to suicide assessment and intervention.. San Francisco, CA: Jossey-Bass Publishers; 1999:3-39.
4. Jacobs DG, Baldessarini RJ, Conwell Y, et al. American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors. Available at: http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf. Accessed May 14, 2007.
5. Hall RC, Platt DE, Hall RC. Suicide risk assessment: a review of risk factors for suicide in 100 patients who made severe suicide attempts. Evaluation of suicide risk in a time of managed care. Psychosomatics 1999;40(1):18-27.
6. Mackenzie TB, Popkin MK. Suicide in the medical patient. Int J Psychiatry Med 1987;17(1):3-22.
7. Barraclough BM. The suicide rate of epilepsy. Acta Psychiatr Scand 1987;76(4):339-45
8. Brent DA, Kolko DJ, Allan MJ, Brown RV. Suicidality in affectively disordered adolescent inpatients. J Am Acad Child Adolesc Psychiatry 1990;29(4):586-93.
9. Polewka A, Mikolaszek-Boba M, Chrostek Maj J, Groszek B. The characteristics of suicide attempts based on the suicidal intent scale scores. Przegl Lek 2005;62(6):415-8.
10. Lewis LM. No-harm contracts: a review of what we know. Suicide Life Threat Behav 2007;37(1):50-7.
11. Jacobs DG. A resource guide for implementing the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) 2007 patient safety goals on suicide. Available at: http://www.sprc.org/library/jcahosafetygoals.pdf. Accessed May 14, 2007.
12. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry 2003;60(1):82-91.
13. Baldessarini RJ, Tondo L, Davis P, et al. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disord 2006;8(5 Pt 2):625-39.
14. Baldessarini RJ, Tondo L, Viguera AC. Discontinuing lithium maintenance treatment in bipolar disorders: risks and implications. Bipolar Disord 1999;1(1):17-24.
1. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry 1988;145(2):224-8.
2. Muzina DJ. What physicians can do to prevent suicide. Cleve Clin J Med 2004;71(3):242-50.
3. Jacobs DG, Brewer ML, Klein-Benheim M. Suicide assessment: an overview and recommended protocol. In: Jacobs DG, ed. The Harvard Medical School guide to suicide assessment and intervention.. San Francisco, CA: Jossey-Bass Publishers; 1999:3-39.
4. Jacobs DG, Baldessarini RJ, Conwell Y, et al. American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors. Available at: http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf. Accessed May 14, 2007.
5. Hall RC, Platt DE, Hall RC. Suicide risk assessment: a review of risk factors for suicide in 100 patients who made severe suicide attempts. Evaluation of suicide risk in a time of managed care. Psychosomatics 1999;40(1):18-27.
6. Mackenzie TB, Popkin MK. Suicide in the medical patient. Int J Psychiatry Med 1987;17(1):3-22.
7. Barraclough BM. The suicide rate of epilepsy. Acta Psychiatr Scand 1987;76(4):339-45
8. Brent DA, Kolko DJ, Allan MJ, Brown RV. Suicidality in affectively disordered adolescent inpatients. J Am Acad Child Adolesc Psychiatry 1990;29(4):586-93.
9. Polewka A, Mikolaszek-Boba M, Chrostek Maj J, Groszek B. The characteristics of suicide attempts based on the suicidal intent scale scores. Przegl Lek 2005;62(6):415-8.
10. Lewis LM. No-harm contracts: a review of what we know. Suicide Life Threat Behav 2007;37(1):50-7.
11. Jacobs DG. A resource guide for implementing the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) 2007 patient safety goals on suicide. Available at: http://www.sprc.org/library/jcahosafetygoals.pdf. Accessed May 14, 2007.
12. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry 2003;60(1):82-91.
13. Baldessarini RJ, Tondo L, Davis P, et al. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disord 2006;8(5 Pt 2):625-39.
14. Baldessarini RJ, Tondo L, Viguera AC. Discontinuing lithium maintenance treatment in bipolar disorders: risks and implications. Bipolar Disord 1999;1(1):17-24.