User login
- For patients with an elevated international normalized ratio (INR) with mild or no bleeding, withhold the warfarin and recheck INR in 1 to 2 days; if INR >5, add oral vitamin K supplementation (C).
- For major bleeding and elevated INR, hospital admission, vitamin K, fresh frozen plasma, and frequent monitoring are needed (B).
- Emergent situations call for hospitalization, clotting factor replacement, and vitamin K administered by slow intravenous infusion (A).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
I feel weak,” reports Mary Jo, a 67-year-old patient who scheduled today’s appointment when she began noticing black, tarry stools 2 days ago. Her chart reveals that she’s on warfarin therapy for chronic atrial fibrillation, and today’s labs show a hematocrit of 18 and an international normalized ratio (INR) of 6.
If Mary Jo were your patient, what would you do?
With some 30.6 million outpatient prescriptions dispensed in the United States in a single year,1 warfarin is among the nation’s most commonly prescribed medications. It is also a dangerous drug. Warfarin’s anticoagulant and antithrombotic effects occur through its ability to inhibit the enzymes responsible for the reduction of vitamin K—an essential cofactor in the normal production of vitamin K-dependent clotting factors II, VII, XI, and X and anticoagulant factors protein C and S. In the presence of warfarin, these clotting factors are produced in a partially carboxylated state with reduced or absent biological activity. The result is a hypocoagulability that can be life-threatening.
Given the sheer number of patients receiving warfarin therapy and the potential for hemorrhage and other adverse effects, primary care physicians need to be familiar with evidence-based recommendations for managing warfarin-induced hypocoagulation. This review will help ensure that when you see patients like Mary Jo, you’ll be prepared to take the best approach to reversing their hypocoagulable state.
Which patients face the highest risk?
The reported incidence of bleeding in patients taking warfarin varies significantly, but is generally in the range of 1% annually.2 Among those who develop warfarin-related major bleeds, however, the fatality rate may be as high as 13.4%.3
The risk of bleeding is highest in the first 30 days of warfarin therapy,3 and increases exponentially once the INR exceeds 5.4 Other risk factors include:
- age (the risk increases to about 5% per year for patients >75 years)5
- hypertension
- cerebrovascular disease
- ischemic stroke
- a history of bleeds.6-8
Multiple medications and herbal substances can interfere with warfarin therapy. Some agents work by augmenting warfarin’s effect; others, such as antiplatelet agents, directly increase the risk of bleeding through unrelated mechanisms; still others may counteract warfarin therapy by enhancing coagulation. Ask patients on warfarin therapy to tell you everything they’re taking, including all over-the-counter medications, supplements, and prescription drugs. TABLE 1 lists herbal substances with the potential to increase or decrease INR. A comprehensive list of drugs that can interact with warfarin is available at http://www.drugs.com/drug-interactions/coumadin_d00022.html.
TABLE 1
Herbal substances that may affect INR38-40
| INCREASE INR | DECREASE INR | |
|---|---|---|
| Angelica root Anise Arnica flower Asafoetida Bogbean Boldo-fenugreek Borage seed oil Bromelain Capsicum Celery Chamomile Clove Dashen Devil’s claw Dong quai Feverfew Fish oil Garlic Ginger Ginkgo | Goldenseal Horse chestnut Licorice root Lovage root Lycium barbarum (wolfberry) Meadowsweet Onion Papain Parsley Passionflower Poplar Quassia Quilinggao Red clover Rue Sweet clover Turmeric Vitamin E Willow bark | Coenzyme Q10 Ginseng Green tea St. John’s wort |
When reversal is needed, how best to achieve it?
The options for reversing warfarin-induced anticoagulation include withholding 1 or more doses of warfarin and providing vitamin K supplementation and clotting factor replacement, as needed. The decision of which combination to use is based on both the urgency ( TABLE 2 ) and completeness of reversal required (target INR range) and the risk of thrombosis when the anticoagulation is reversed.9
Vitamin K is actually a group of lipid-soluble chemicals that are necessary for the production of functional carboxylated clotting factors II, VII, IX, and X. Vitamin K1 (phytonadione), which is available in food and as a supplement, is the particular chemical that competes with warfarin. When it is used as a reversal agent, phytonadione is generally referred to simply as vitamin K.
The oral route of vitamin K is preferred, but its effect is delayed because of the time required for absorption and production of factors. Thus, a slow (15-30 min) infusion of intravenous (IV) vitamin K should be used if reversal is needed within 6 hours—or oral therapy is unavailable. Avoid subcutaneous administration; it is not reliable and may take up to 72 hours to reverse the INR.10-12 Intramuscular (IM) administration of vitamin K should also be avoided in patients taking warfarin because of concerns about hematoma formation, although a 2003 study of patients in teaching hospitals found that the IM route is used about 10% of the time.13
The optimal dose of vitamin K varies, based on patient-specific factors such as comorbidities, metabolic and genetic variation, weight, age, and liver function. Doses as low as 0.5 mg IV or 1 mg oral vitamin K have been effective in reversing an elevated INR to a therapeutic range in nonlife-threatening situations.11,14,15 The American College of Chest Physicians (ACCP), which issued new guidelines in 2008, recommends doses of <5 mg for an INR >5 but <9 if there is a high risk of bleeding; 5 to 10 mg is the recommended dose for all patients with an INR ≥9. In cases of significant bleeding, a dose of 10 mg IV is recommended.16 Excessive vitamin K supplementation may lead to warfarin resistance, making it necessary to use much higher doses of warfarin down the road to achieve therapeutic INR levels.
Fresh frozen plasma (FFP) replaces functional vitamin K-dependent clotting factors that are decreased in patients taking warfarin. The suggested dose is 15 mL/kg,17,18 but patients must be monitored with coagulation laboratory values to assess the amount needed. One unit of FFP is roughly 250 mL, which corresponds to roughly 250 units of clotting factors.
FFP works to offset coagulopathy quickly. But because the plasma is frozen, it has to be thawed and blood type-matched, which is time-consuming. FFP transfusion also may be associated with infections, although the risk is generally believed to be minimal.17 Other limitations in using FFP include the large volume of fluid that must be administered—with the attendant risk of fluid overload—and the possibility of significant infusion reactions that may require slowing the infusion rate.19
Prothrombin complex concentrate (PCC) is pooled from donor plasma and lyophilized to a powder. It is then reconstituted for clotting factor replacement, and is available through the pharmacy rather than the blood bank.20 PCC is dosed in international units of factor IX, although it includes proportional amounts of factors II, VII, and X and proteins C and S. The typical recommended dose is 30 to 50 U/kg.20,21
Although PCC contains human coagulation factors, it does not involve the same risks of fluid overload or infectious transmission as FFP. It can be given IV over 5 to 10 minutes. The risk of thrombogenicity has been reported in patients with hemophilia who receive PCC,22 but studies of PCC use in warfarin reversal have not shown this adverse effect.23,24 Data from the use of PCC for the treatment of hemophilia suggest that the risk of thromboembolic events begins with daily doses >200 U/kg. There is limited information about the safety of giving PCC to patients with mechanical valve replacement, pregnant women, and those in other high-risk situations.
Recombinant activated factor VII (rFVIIa) is also effective in reversing elevated INR.25,26 It replaces 1 of the clotting factors that is decreased in anticoagulated patients (factor VII), but the significance of not replacing factors II, IX, and X is unknown.27 The recommended quantity of rFVIIa ranges from a single dose of 1200 mcg to weight-based dosing (10-160 mcg/kg).25,28-30 (IV vitamin K and FFP are also given in emergent situations in which rFVIIa is administered.) Thrombogenicity is a possible complication with the use of rFVIIa, but data are scarce regarding the incidence of adverse effects.
Neither PCC nor rFVIIa has US Food and Drug Administration approval for use in reversing warfarin-induced anticoagulation. Their use for this purpose may be warranted only in situations that threaten life or limb, and must be guided by clinical judgment.
TABLE 2
How fast? Reversal agents and time of action32
| SPEED/TYPE OF REVERSAL REQUIRED | WHAT TO USE |
|---|---|
| Rapid (complete; within 10-15 minutes) | PCC or rFVIIa + vitamin K IV |
| Fast (partial) | FFP + vitamin K IV |
| Prompt (4-6 hours) | Vitamin K IV |
| Slow (within 24 hours) | Oral vitamin K |
| Ultra-slow (over a period of days) | Omit warfarin dose (no vitamin K) |
| FFP, fresh frozen plasma; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII. | |
Severity of bleeding as a treatment guide
Studies of methods used to reverse warfarin’s anticoagulation effect are difficult to compare because of a lack of a standardized approach to the classification of bleeds.18,31,32 We’ve used the following classification system, modified from that of Fihn et al,31 to avoid confusion and inform treatment decisions:
- Minor bleed: Reported, not requiring additional testing
- Major bleed: Requiring medical evaluation and inpatient treatment and/or blood transfusion
- Life-threatening bleed: Leading to cardiac arrest, surgical/angiographic intervention, or irreversible sequelae (loss of limb/sight).
Here’s how to put this classification system—and the ACCP’s 2008 guidelines for managing patients with elevated INR16 ( FIGURE )—into action:
In the case of minor bleeding and elevated INR, withhold the next 1 to 2 doses of warfarin.16 If the patient is considered high risk, give oral vitamin K in small amounts (1-2.5 mg). Keep in mind that excessive amounts of vitamin K will promote warfarin resistance.
FIGURE
Reversal of warfarin-induced anticoagulation
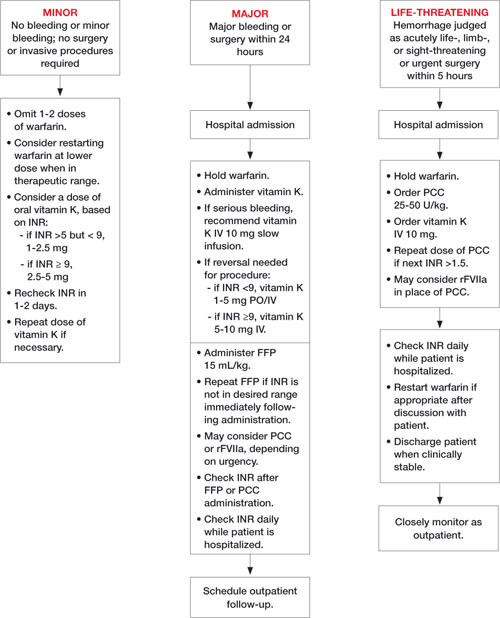
FFP, fresh frozen plasma; INR, international normalized ratio; IV, intravenous; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII.
Adapted from: Ansell J et al. Chest. 2008.16 Ask the patient to return to your office in 1 or 2 days for a recheck of INR. If it remains elevated, give another dose of vitamin K. Warfarin may need to be restarted at a lower dose depending on the clinical situation.17,32
In cases of major bleeding and elevated INR, stop the warfarin, give vitamin K (the administration route will be based on clinical presentation and the urgency of reversal), and arrange for factor replacement and hospital admission.16 Use FFP, if possible, because more is known about its safety than the safety of PCC or rFVIIa. That said, the choice of factor replacement should be based on the urgency of reversal and on clinical condition.16,33,34
INR should be rechecked immediately after factor replacement. Because coagulation factors have varied half-lives, INR should be checked daily for the next 4 days to confirm that it remains at a therapeutic level.16
In cases of life-threatening bleeding, stop the warfarin, give 10 mg vitamin K IV, and replace clotting factors.16 PCC should be considered because it will reverse the anticoagulation in the shortest amount of time, without limitations associated with fluid status, blood type-matching, or infusion reaction.35,36 While the risk of thrombosis needs to be evaluated in each high-risk circumstance, the use of either PCC or rFVIIa, depending on availability, is appropriate for a life-threatening bleed.29,37
Classifying—and treating—our patient
Based on our classification system, we determined that Mary Jo had major bleeding: She needed inpatient monitoring, with the possibility of a blood transfusion, but her condition was not life-threatening. She was hospitalized immediately. Her warfarin was withheld and she was given vitamin K IV and FFP to reverse her hypocoagulable state.
Once Mary Jo’s hypocoagulable state was reversed, which took about 4 hours, she was evaluated and found to have a small bleeding ulcer. The ulcer was cauterized, and her condition remained stable. A detailed investigation of possible reasons for the patient’s elevated INR did not reveal any causes. Three days after the cauterization, Mary Jo was started back on a lower dosing schedule of warfarin. She was discharged after a 5-day stay, with instructions to return to the clinic in 5 days for continued monitoring.
CORRESPONDENCE
Shailendra Prasad, MBBS, MPH, 1020 W. Broadway, Minneapolis, MN 55411; pras0054@umn.edu
1. Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007;167:1414-1419.
2. Beyth RJ. Hemorrhagic complications of oral anticoagulant therapy. Clin Geriatr Med. 2001;17:49-56.
3. Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann Intern Med. 2003;139:893-900.
4. Levine MN, Raskob G, Beyth RJ, et al. Hemorrhagic complications of anticoagulant treatment: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S287-S310.
5. Pengo V, Legnani C, Noventa F, et al. ISCOAT Study Group. (Italian Study on Complications of Oral Anticoagulant Therapy). Oral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and risk of bleeding. A multicenter inception cohort study. Thromb Haemost. 2001;85:418-422.
6. White RH, McKittrick T, Takakuwa J, et al. Management and prognosis of life-threatening bleeding during warfarin therapy. National Consortium of Anticoagulation Clinics. Arch Intern Med. 1996;156:1197-1201.
7. Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med. 1998;105:91-99.
8. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. EAFT (European Atrial Fibrillation Trial) Study Group. Lancet. 1993;342:1255-1262.
9. Ansell J, Hirsh J, Poller L, et al. The pharmacology and management of the vitamin K antagonists: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S204-S233.
10. Crowther MA, Douketis JD, Schnurr T, et al. Oral vitamin K lowers the international normalized ratio more rapidly than subcutaneous vitamin K in the treatment of warfarin-associated coagulopathy. A randomized, controlled trial. Ann Intern Med. 2002;137:251-254.
11. Whitling AM, Bussey HI, Lyons RM. Comparing different routes and doses of phytonadione for reversing excessive anticoagulation. Arch Intern Med. 1998;158:2136-2140.
12. Nee R, Doppenschmidt D, Donovan DJ, et al. Intravenous versus subcutaneous vitamin K1 in reversing excessive oral anticoagulation. Am J Cardiol. 1999;83:286-288.
13. Fan J, Armitstead JA, Adams AG, et al. A retrospective evaluation of vitamin K1 therapy to reverse the anticoagulant effect of warfarin. Pharmacotherapy. 2003;23:1245-1250.
14. Lubetsky A, Yonath H, Olchovsky D, et al. Comparison of oral vs intravenous phytonadione (vitamin K1) in patients with excessive anticoagulation: a prospective randomized controlled study. Arch Intern Med. 2003;163:2469-2473.
15. Hung A, Singh S, Tait RC. A prospective randomized study to determine the optimal dose of intravenous vitamin K in reversal of over-warfarinization. Br J Haematol. 2000;109:537-539.
16. Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists. Chest. 2008;133(suppl):160S-198S.
17. Dentali F, Ageno W, Crowther M. Treatment of coumarin-associated coagulopathy: a systematic review and proposed algorithms. J Thromb Haemost. 2006;4:1853-1863.
18. Makris M, Watson HG. The management of coumarin-induced over-anticoagulation Annotation [see comment]. Br J Haematol. 2001;114:271-280.
19. O’Shaughnessy DF, Atterbury C, Bolton Maggs P, et al. British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol. 2004;126:11-28.
20. Makris M. Optimisation of the prothrombin complex concentrate dose for warfarin reversal. Thromb Res. 2005;115:451-453.
21. Vigue B, Ract C, Tremey B, et al. Ultra-rapid management of oral anticoagulant therapy-related surgical intracranial hemorrhage. Intensive Care Med. 2007;33:721-725.
22. Kohler M. Thrombogenicity of prothrombin complex concentrates. Thromb Res. 1999;95(suppl 1):S13-S17.
23. Lorenz R, Kienast J, Otto U, et al. Successful emergency reversal of phenprocoumon anticoagulation with prothrombin complex concentrate: a prospective clinical study. Blood Coagul Fibrinolysis. 2007;18:565-570.
24. Pabinger I, Brenner B, Kalina U, et al. Beriplex P/N Anticoagulation Reversal Study Group. Prothrombin complex concentrate (Beriplex P/N) for emergency anticoagulation reversal: a prospective multinational clinical trial. J Thromb Haemost. 2008;6:622-631.
25. Sorensen B, Johansen P, Nielsen GL, et al. Reversal of the International Normalized Ratio with recombinant activated factor VII in central nervous system bleeding during warfarin thromboprophylaxis: clinical and biochemical aspects. Blood Coagul Fibrinolysis. 2003;14:469-477.
26. Brody DL, Aiyagari V, Shackleford AM, et al. Use of recombinant factor VIIa in patients with warfarin-associated intracranial hemorrhage. Neurocrit Care. 2005;2:263-267.
27. Tanaka KA, Szlam F, Dickneite G, et al. Effects of prothrombin complex concentrate and recombinant activated factor VII on vitamin K antagonist induced anticoagulation. Thromb Res. 2008;122:117-123.
28. Lin J, Hanigan WC, Tarantino M, et al. The use of recombinant activated factor VII to reverse warfarin-induced anticoagulation in patients with hemorrhages in the central nervous system: preliminary findings. J Neurosurg. 2003;98:737-740.
29. Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 2005;352:777-785.
30. Dager WE, King JH, Regalia RC, et al. Reversal of elevated international normalized ratio and bleeding with low-dose recombinant factor VII in patients receiving warfarin. Pharmacotherapy. 2006;26:1091-1098.
31. Fihn SD, McDonell M, Martin D, et al. Risk factors for complications of chronic anticoagulation. A multicenter study. Warfarin Optimized Outpatient Follow-up Study Group. Ann Intern Med. 1993;118:511-520.
32. Hanley JP. Warfarin reversal. J Clin Pathol. 2004;57:1132-1139.
33. Yasaka M, Sakata T, Minematsu K, et al. Correction of INR by prothrombin complex concentrate and vitamin K in patients with warfarin related hemorrhagic complication. Thromb Res. 2002;108:25-30.
34. Evans G, Luddington R, Baglin T. Beriplex P/N reverses severe warfarin-induced anticoagulation immediately and completely in patients presenting with major bleeding. Br J Haematol. 2001;115:998-1001.
35. Lubetsky A, Hoffman R, Zimlichman R, et al. Efficacy and safety of complex concentrate (Octaplex) for rapid reversal of oral anticoagulation. Thromb Res. 2004;113:371-378.
36. Cartmill M, Dolan G, Byrne JL, et al. Prothrombin complex concentrate for oral anticoagulant reversal in neurosurgical emergencies. Br J Neurosurg. 2000;14:458-461.
37. Deveras RA, Kessler CM. Reversal of warfarin-induced excessive anticoagulation with recombinant human factor VIIa concentrate. Ann Intern Med. 2002;137:884-888.
38. Holbrook AM, Pereira JA, Labiris R, et al. Systematic overview of warfarin and its drug and food interactions. Arch Intern Med. 2005;165:1095-1106.
39. Haines ST, Zeolla M, Witt DM. Venous Thromboembolism. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A Pathophysiological Approach. 6th ed. New York: McGraw-Hill Companies, Inc.; 2005:373-413.
40. Micromedex Healthcare Series. Drug-REAX System. New York: Thomson Reuters; 2008.
- For patients with an elevated international normalized ratio (INR) with mild or no bleeding, withhold the warfarin and recheck INR in 1 to 2 days; if INR >5, add oral vitamin K supplementation (C).
- For major bleeding and elevated INR, hospital admission, vitamin K, fresh frozen plasma, and frequent monitoring are needed (B).
- Emergent situations call for hospitalization, clotting factor replacement, and vitamin K administered by slow intravenous infusion (A).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
I feel weak,” reports Mary Jo, a 67-year-old patient who scheduled today’s appointment when she began noticing black, tarry stools 2 days ago. Her chart reveals that she’s on warfarin therapy for chronic atrial fibrillation, and today’s labs show a hematocrit of 18 and an international normalized ratio (INR) of 6.
If Mary Jo were your patient, what would you do?
With some 30.6 million outpatient prescriptions dispensed in the United States in a single year,1 warfarin is among the nation’s most commonly prescribed medications. It is also a dangerous drug. Warfarin’s anticoagulant and antithrombotic effects occur through its ability to inhibit the enzymes responsible for the reduction of vitamin K—an essential cofactor in the normal production of vitamin K-dependent clotting factors II, VII, XI, and X and anticoagulant factors protein C and S. In the presence of warfarin, these clotting factors are produced in a partially carboxylated state with reduced or absent biological activity. The result is a hypocoagulability that can be life-threatening.
Given the sheer number of patients receiving warfarin therapy and the potential for hemorrhage and other adverse effects, primary care physicians need to be familiar with evidence-based recommendations for managing warfarin-induced hypocoagulation. This review will help ensure that when you see patients like Mary Jo, you’ll be prepared to take the best approach to reversing their hypocoagulable state.
Which patients face the highest risk?
The reported incidence of bleeding in patients taking warfarin varies significantly, but is generally in the range of 1% annually.2 Among those who develop warfarin-related major bleeds, however, the fatality rate may be as high as 13.4%.3
The risk of bleeding is highest in the first 30 days of warfarin therapy,3 and increases exponentially once the INR exceeds 5.4 Other risk factors include:
- age (the risk increases to about 5% per year for patients >75 years)5
- hypertension
- cerebrovascular disease
- ischemic stroke
- a history of bleeds.6-8
Multiple medications and herbal substances can interfere with warfarin therapy. Some agents work by augmenting warfarin’s effect; others, such as antiplatelet agents, directly increase the risk of bleeding through unrelated mechanisms; still others may counteract warfarin therapy by enhancing coagulation. Ask patients on warfarin therapy to tell you everything they’re taking, including all over-the-counter medications, supplements, and prescription drugs. TABLE 1 lists herbal substances with the potential to increase or decrease INR. A comprehensive list of drugs that can interact with warfarin is available at http://www.drugs.com/drug-interactions/coumadin_d00022.html.
TABLE 1
Herbal substances that may affect INR38-40
| INCREASE INR | DECREASE INR | |
|---|---|---|
| Angelica root Anise Arnica flower Asafoetida Bogbean Boldo-fenugreek Borage seed oil Bromelain Capsicum Celery Chamomile Clove Dashen Devil’s claw Dong quai Feverfew Fish oil Garlic Ginger Ginkgo | Goldenseal Horse chestnut Licorice root Lovage root Lycium barbarum (wolfberry) Meadowsweet Onion Papain Parsley Passionflower Poplar Quassia Quilinggao Red clover Rue Sweet clover Turmeric Vitamin E Willow bark | Coenzyme Q10 Ginseng Green tea St. John’s wort |
When reversal is needed, how best to achieve it?
The options for reversing warfarin-induced anticoagulation include withholding 1 or more doses of warfarin and providing vitamin K supplementation and clotting factor replacement, as needed. The decision of which combination to use is based on both the urgency ( TABLE 2 ) and completeness of reversal required (target INR range) and the risk of thrombosis when the anticoagulation is reversed.9
Vitamin K is actually a group of lipid-soluble chemicals that are necessary for the production of functional carboxylated clotting factors II, VII, IX, and X. Vitamin K1 (phytonadione), which is available in food and as a supplement, is the particular chemical that competes with warfarin. When it is used as a reversal agent, phytonadione is generally referred to simply as vitamin K.
The oral route of vitamin K is preferred, but its effect is delayed because of the time required for absorption and production of factors. Thus, a slow (15-30 min) infusion of intravenous (IV) vitamin K should be used if reversal is needed within 6 hours—or oral therapy is unavailable. Avoid subcutaneous administration; it is not reliable and may take up to 72 hours to reverse the INR.10-12 Intramuscular (IM) administration of vitamin K should also be avoided in patients taking warfarin because of concerns about hematoma formation, although a 2003 study of patients in teaching hospitals found that the IM route is used about 10% of the time.13
The optimal dose of vitamin K varies, based on patient-specific factors such as comorbidities, metabolic and genetic variation, weight, age, and liver function. Doses as low as 0.5 mg IV or 1 mg oral vitamin K have been effective in reversing an elevated INR to a therapeutic range in nonlife-threatening situations.11,14,15 The American College of Chest Physicians (ACCP), which issued new guidelines in 2008, recommends doses of <5 mg for an INR >5 but <9 if there is a high risk of bleeding; 5 to 10 mg is the recommended dose for all patients with an INR ≥9. In cases of significant bleeding, a dose of 10 mg IV is recommended.16 Excessive vitamin K supplementation may lead to warfarin resistance, making it necessary to use much higher doses of warfarin down the road to achieve therapeutic INR levels.
Fresh frozen plasma (FFP) replaces functional vitamin K-dependent clotting factors that are decreased in patients taking warfarin. The suggested dose is 15 mL/kg,17,18 but patients must be monitored with coagulation laboratory values to assess the amount needed. One unit of FFP is roughly 250 mL, which corresponds to roughly 250 units of clotting factors.
FFP works to offset coagulopathy quickly. But because the plasma is frozen, it has to be thawed and blood type-matched, which is time-consuming. FFP transfusion also may be associated with infections, although the risk is generally believed to be minimal.17 Other limitations in using FFP include the large volume of fluid that must be administered—with the attendant risk of fluid overload—and the possibility of significant infusion reactions that may require slowing the infusion rate.19
Prothrombin complex concentrate (PCC) is pooled from donor plasma and lyophilized to a powder. It is then reconstituted for clotting factor replacement, and is available through the pharmacy rather than the blood bank.20 PCC is dosed in international units of factor IX, although it includes proportional amounts of factors II, VII, and X and proteins C and S. The typical recommended dose is 30 to 50 U/kg.20,21
Although PCC contains human coagulation factors, it does not involve the same risks of fluid overload or infectious transmission as FFP. It can be given IV over 5 to 10 minutes. The risk of thrombogenicity has been reported in patients with hemophilia who receive PCC,22 but studies of PCC use in warfarin reversal have not shown this adverse effect.23,24 Data from the use of PCC for the treatment of hemophilia suggest that the risk of thromboembolic events begins with daily doses >200 U/kg. There is limited information about the safety of giving PCC to patients with mechanical valve replacement, pregnant women, and those in other high-risk situations.
Recombinant activated factor VII (rFVIIa) is also effective in reversing elevated INR.25,26 It replaces 1 of the clotting factors that is decreased in anticoagulated patients (factor VII), but the significance of not replacing factors II, IX, and X is unknown.27 The recommended quantity of rFVIIa ranges from a single dose of 1200 mcg to weight-based dosing (10-160 mcg/kg).25,28-30 (IV vitamin K and FFP are also given in emergent situations in which rFVIIa is administered.) Thrombogenicity is a possible complication with the use of rFVIIa, but data are scarce regarding the incidence of adverse effects.
Neither PCC nor rFVIIa has US Food and Drug Administration approval for use in reversing warfarin-induced anticoagulation. Their use for this purpose may be warranted only in situations that threaten life or limb, and must be guided by clinical judgment.
TABLE 2
How fast? Reversal agents and time of action32
| SPEED/TYPE OF REVERSAL REQUIRED | WHAT TO USE |
|---|---|
| Rapid (complete; within 10-15 minutes) | PCC or rFVIIa + vitamin K IV |
| Fast (partial) | FFP + vitamin K IV |
| Prompt (4-6 hours) | Vitamin K IV |
| Slow (within 24 hours) | Oral vitamin K |
| Ultra-slow (over a period of days) | Omit warfarin dose (no vitamin K) |
| FFP, fresh frozen plasma; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII. | |
Severity of bleeding as a treatment guide
Studies of methods used to reverse warfarin’s anticoagulation effect are difficult to compare because of a lack of a standardized approach to the classification of bleeds.18,31,32 We’ve used the following classification system, modified from that of Fihn et al,31 to avoid confusion and inform treatment decisions:
- Minor bleed: Reported, not requiring additional testing
- Major bleed: Requiring medical evaluation and inpatient treatment and/or blood transfusion
- Life-threatening bleed: Leading to cardiac arrest, surgical/angiographic intervention, or irreversible sequelae (loss of limb/sight).
Here’s how to put this classification system—and the ACCP’s 2008 guidelines for managing patients with elevated INR16 ( FIGURE )—into action:
In the case of minor bleeding and elevated INR, withhold the next 1 to 2 doses of warfarin.16 If the patient is considered high risk, give oral vitamin K in small amounts (1-2.5 mg). Keep in mind that excessive amounts of vitamin K will promote warfarin resistance.
FIGURE
Reversal of warfarin-induced anticoagulation
FFP, fresh frozen plasma; INR, international normalized ratio; IV, intravenous; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII.
Adapted from: Ansell J et al. Chest. 2008.16 Ask the patient to return to your office in 1 or 2 days for a recheck of INR. If it remains elevated, give another dose of vitamin K. Warfarin may need to be restarted at a lower dose depending on the clinical situation.17,32
In cases of major bleeding and elevated INR, stop the warfarin, give vitamin K (the administration route will be based on clinical presentation and the urgency of reversal), and arrange for factor replacement and hospital admission.16 Use FFP, if possible, because more is known about its safety than the safety of PCC or rFVIIa. That said, the choice of factor replacement should be based on the urgency of reversal and on clinical condition.16,33,34
INR should be rechecked immediately after factor replacement. Because coagulation factors have varied half-lives, INR should be checked daily for the next 4 days to confirm that it remains at a therapeutic level.16
In cases of life-threatening bleeding, stop the warfarin, give 10 mg vitamin K IV, and replace clotting factors.16 PCC should be considered because it will reverse the anticoagulation in the shortest amount of time, without limitations associated with fluid status, blood type-matching, or infusion reaction.35,36 While the risk of thrombosis needs to be evaluated in each high-risk circumstance, the use of either PCC or rFVIIa, depending on availability, is appropriate for a life-threatening bleed.29,37
Classifying—and treating—our patient
Based on our classification system, we determined that Mary Jo had major bleeding: She needed inpatient monitoring, with the possibility of a blood transfusion, but her condition was not life-threatening. She was hospitalized immediately. Her warfarin was withheld and she was given vitamin K IV and FFP to reverse her hypocoagulable state.
Once Mary Jo’s hypocoagulable state was reversed, which took about 4 hours, she was evaluated and found to have a small bleeding ulcer. The ulcer was cauterized, and her condition remained stable. A detailed investigation of possible reasons for the patient’s elevated INR did not reveal any causes. Three days after the cauterization, Mary Jo was started back on a lower dosing schedule of warfarin. She was discharged after a 5-day stay, with instructions to return to the clinic in 5 days for continued monitoring.
CORRESPONDENCE
Shailendra Prasad, MBBS, MPH, 1020 W. Broadway, Minneapolis, MN 55411; pras0054@umn.edu
- For patients with an elevated international normalized ratio (INR) with mild or no bleeding, withhold the warfarin and recheck INR in 1 to 2 days; if INR >5, add oral vitamin K supplementation (C).
- For major bleeding and elevated INR, hospital admission, vitamin K, fresh frozen plasma, and frequent monitoring are needed (B).
- Emergent situations call for hospitalization, clotting factor replacement, and vitamin K administered by slow intravenous infusion (A).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
I feel weak,” reports Mary Jo, a 67-year-old patient who scheduled today’s appointment when she began noticing black, tarry stools 2 days ago. Her chart reveals that she’s on warfarin therapy for chronic atrial fibrillation, and today’s labs show a hematocrit of 18 and an international normalized ratio (INR) of 6.
If Mary Jo were your patient, what would you do?
With some 30.6 million outpatient prescriptions dispensed in the United States in a single year,1 warfarin is among the nation’s most commonly prescribed medications. It is also a dangerous drug. Warfarin’s anticoagulant and antithrombotic effects occur through its ability to inhibit the enzymes responsible for the reduction of vitamin K—an essential cofactor in the normal production of vitamin K-dependent clotting factors II, VII, XI, and X and anticoagulant factors protein C and S. In the presence of warfarin, these clotting factors are produced in a partially carboxylated state with reduced or absent biological activity. The result is a hypocoagulability that can be life-threatening.
Given the sheer number of patients receiving warfarin therapy and the potential for hemorrhage and other adverse effects, primary care physicians need to be familiar with evidence-based recommendations for managing warfarin-induced hypocoagulation. This review will help ensure that when you see patients like Mary Jo, you’ll be prepared to take the best approach to reversing their hypocoagulable state.
Which patients face the highest risk?
The reported incidence of bleeding in patients taking warfarin varies significantly, but is generally in the range of 1% annually.2 Among those who develop warfarin-related major bleeds, however, the fatality rate may be as high as 13.4%.3
The risk of bleeding is highest in the first 30 days of warfarin therapy,3 and increases exponentially once the INR exceeds 5.4 Other risk factors include:
- age (the risk increases to about 5% per year for patients >75 years)5
- hypertension
- cerebrovascular disease
- ischemic stroke
- a history of bleeds.6-8
Multiple medications and herbal substances can interfere with warfarin therapy. Some agents work by augmenting warfarin’s effect; others, such as antiplatelet agents, directly increase the risk of bleeding through unrelated mechanisms; still others may counteract warfarin therapy by enhancing coagulation. Ask patients on warfarin therapy to tell you everything they’re taking, including all over-the-counter medications, supplements, and prescription drugs. TABLE 1 lists herbal substances with the potential to increase or decrease INR. A comprehensive list of drugs that can interact with warfarin is available at http://www.drugs.com/drug-interactions/coumadin_d00022.html.
TABLE 1
Herbal substances that may affect INR38-40
| INCREASE INR | DECREASE INR | |
|---|---|---|
| Angelica root Anise Arnica flower Asafoetida Bogbean Boldo-fenugreek Borage seed oil Bromelain Capsicum Celery Chamomile Clove Dashen Devil’s claw Dong quai Feverfew Fish oil Garlic Ginger Ginkgo | Goldenseal Horse chestnut Licorice root Lovage root Lycium barbarum (wolfberry) Meadowsweet Onion Papain Parsley Passionflower Poplar Quassia Quilinggao Red clover Rue Sweet clover Turmeric Vitamin E Willow bark | Coenzyme Q10 Ginseng Green tea St. John’s wort |
When reversal is needed, how best to achieve it?
The options for reversing warfarin-induced anticoagulation include withholding 1 or more doses of warfarin and providing vitamin K supplementation and clotting factor replacement, as needed. The decision of which combination to use is based on both the urgency ( TABLE 2 ) and completeness of reversal required (target INR range) and the risk of thrombosis when the anticoagulation is reversed.9
Vitamin K is actually a group of lipid-soluble chemicals that are necessary for the production of functional carboxylated clotting factors II, VII, IX, and X. Vitamin K1 (phytonadione), which is available in food and as a supplement, is the particular chemical that competes with warfarin. When it is used as a reversal agent, phytonadione is generally referred to simply as vitamin K.
The oral route of vitamin K is preferred, but its effect is delayed because of the time required for absorption and production of factors. Thus, a slow (15-30 min) infusion of intravenous (IV) vitamin K should be used if reversal is needed within 6 hours—or oral therapy is unavailable. Avoid subcutaneous administration; it is not reliable and may take up to 72 hours to reverse the INR.10-12 Intramuscular (IM) administration of vitamin K should also be avoided in patients taking warfarin because of concerns about hematoma formation, although a 2003 study of patients in teaching hospitals found that the IM route is used about 10% of the time.13
The optimal dose of vitamin K varies, based on patient-specific factors such as comorbidities, metabolic and genetic variation, weight, age, and liver function. Doses as low as 0.5 mg IV or 1 mg oral vitamin K have been effective in reversing an elevated INR to a therapeutic range in nonlife-threatening situations.11,14,15 The American College of Chest Physicians (ACCP), which issued new guidelines in 2008, recommends doses of <5 mg for an INR >5 but <9 if there is a high risk of bleeding; 5 to 10 mg is the recommended dose for all patients with an INR ≥9. In cases of significant bleeding, a dose of 10 mg IV is recommended.16 Excessive vitamin K supplementation may lead to warfarin resistance, making it necessary to use much higher doses of warfarin down the road to achieve therapeutic INR levels.
Fresh frozen plasma (FFP) replaces functional vitamin K-dependent clotting factors that are decreased in patients taking warfarin. The suggested dose is 15 mL/kg,17,18 but patients must be monitored with coagulation laboratory values to assess the amount needed. One unit of FFP is roughly 250 mL, which corresponds to roughly 250 units of clotting factors.
FFP works to offset coagulopathy quickly. But because the plasma is frozen, it has to be thawed and blood type-matched, which is time-consuming. FFP transfusion also may be associated with infections, although the risk is generally believed to be minimal.17 Other limitations in using FFP include the large volume of fluid that must be administered—with the attendant risk of fluid overload—and the possibility of significant infusion reactions that may require slowing the infusion rate.19
Prothrombin complex concentrate (PCC) is pooled from donor plasma and lyophilized to a powder. It is then reconstituted for clotting factor replacement, and is available through the pharmacy rather than the blood bank.20 PCC is dosed in international units of factor IX, although it includes proportional amounts of factors II, VII, and X and proteins C and S. The typical recommended dose is 30 to 50 U/kg.20,21
Although PCC contains human coagulation factors, it does not involve the same risks of fluid overload or infectious transmission as FFP. It can be given IV over 5 to 10 minutes. The risk of thrombogenicity has been reported in patients with hemophilia who receive PCC,22 but studies of PCC use in warfarin reversal have not shown this adverse effect.23,24 Data from the use of PCC for the treatment of hemophilia suggest that the risk of thromboembolic events begins with daily doses >200 U/kg. There is limited information about the safety of giving PCC to patients with mechanical valve replacement, pregnant women, and those in other high-risk situations.
Recombinant activated factor VII (rFVIIa) is also effective in reversing elevated INR.25,26 It replaces 1 of the clotting factors that is decreased in anticoagulated patients (factor VII), but the significance of not replacing factors II, IX, and X is unknown.27 The recommended quantity of rFVIIa ranges from a single dose of 1200 mcg to weight-based dosing (10-160 mcg/kg).25,28-30 (IV vitamin K and FFP are also given in emergent situations in which rFVIIa is administered.) Thrombogenicity is a possible complication with the use of rFVIIa, but data are scarce regarding the incidence of adverse effects.
Neither PCC nor rFVIIa has US Food and Drug Administration approval for use in reversing warfarin-induced anticoagulation. Their use for this purpose may be warranted only in situations that threaten life or limb, and must be guided by clinical judgment.
TABLE 2
How fast? Reversal agents and time of action32
| SPEED/TYPE OF REVERSAL REQUIRED | WHAT TO USE |
|---|---|
| Rapid (complete; within 10-15 minutes) | PCC or rFVIIa + vitamin K IV |
| Fast (partial) | FFP + vitamin K IV |
| Prompt (4-6 hours) | Vitamin K IV |
| Slow (within 24 hours) | Oral vitamin K |
| Ultra-slow (over a period of days) | Omit warfarin dose (no vitamin K) |
| FFP, fresh frozen plasma; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII. | |
Severity of bleeding as a treatment guide
Studies of methods used to reverse warfarin’s anticoagulation effect are difficult to compare because of a lack of a standardized approach to the classification of bleeds.18,31,32 We’ve used the following classification system, modified from that of Fihn et al,31 to avoid confusion and inform treatment decisions:
- Minor bleed: Reported, not requiring additional testing
- Major bleed: Requiring medical evaluation and inpatient treatment and/or blood transfusion
- Life-threatening bleed: Leading to cardiac arrest, surgical/angiographic intervention, or irreversible sequelae (loss of limb/sight).
Here’s how to put this classification system—and the ACCP’s 2008 guidelines for managing patients with elevated INR16 ( FIGURE )—into action:
In the case of minor bleeding and elevated INR, withhold the next 1 to 2 doses of warfarin.16 If the patient is considered high risk, give oral vitamin K in small amounts (1-2.5 mg). Keep in mind that excessive amounts of vitamin K will promote warfarin resistance.
FIGURE
Reversal of warfarin-induced anticoagulation
FFP, fresh frozen plasma; INR, international normalized ratio; IV, intravenous; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII.
Adapted from: Ansell J et al. Chest. 2008.16 Ask the patient to return to your office in 1 or 2 days for a recheck of INR. If it remains elevated, give another dose of vitamin K. Warfarin may need to be restarted at a lower dose depending on the clinical situation.17,32
In cases of major bleeding and elevated INR, stop the warfarin, give vitamin K (the administration route will be based on clinical presentation and the urgency of reversal), and arrange for factor replacement and hospital admission.16 Use FFP, if possible, because more is known about its safety than the safety of PCC or rFVIIa. That said, the choice of factor replacement should be based on the urgency of reversal and on clinical condition.16,33,34
INR should be rechecked immediately after factor replacement. Because coagulation factors have varied half-lives, INR should be checked daily for the next 4 days to confirm that it remains at a therapeutic level.16
In cases of life-threatening bleeding, stop the warfarin, give 10 mg vitamin K IV, and replace clotting factors.16 PCC should be considered because it will reverse the anticoagulation in the shortest amount of time, without limitations associated with fluid status, blood type-matching, or infusion reaction.35,36 While the risk of thrombosis needs to be evaluated in each high-risk circumstance, the use of either PCC or rFVIIa, depending on availability, is appropriate for a life-threatening bleed.29,37
Classifying—and treating—our patient
Based on our classification system, we determined that Mary Jo had major bleeding: She needed inpatient monitoring, with the possibility of a blood transfusion, but her condition was not life-threatening. She was hospitalized immediately. Her warfarin was withheld and she was given vitamin K IV and FFP to reverse her hypocoagulable state.
Once Mary Jo’s hypocoagulable state was reversed, which took about 4 hours, she was evaluated and found to have a small bleeding ulcer. The ulcer was cauterized, and her condition remained stable. A detailed investigation of possible reasons for the patient’s elevated INR did not reveal any causes. Three days after the cauterization, Mary Jo was started back on a lower dosing schedule of warfarin. She was discharged after a 5-day stay, with instructions to return to the clinic in 5 days for continued monitoring.
CORRESPONDENCE
Shailendra Prasad, MBBS, MPH, 1020 W. Broadway, Minneapolis, MN 55411; pras0054@umn.edu
1. Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007;167:1414-1419.
2. Beyth RJ. Hemorrhagic complications of oral anticoagulant therapy. Clin Geriatr Med. 2001;17:49-56.
3. Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann Intern Med. 2003;139:893-900.
4. Levine MN, Raskob G, Beyth RJ, et al. Hemorrhagic complications of anticoagulant treatment: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S287-S310.
5. Pengo V, Legnani C, Noventa F, et al. ISCOAT Study Group. (Italian Study on Complications of Oral Anticoagulant Therapy). Oral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and risk of bleeding. A multicenter inception cohort study. Thromb Haemost. 2001;85:418-422.
6. White RH, McKittrick T, Takakuwa J, et al. Management and prognosis of life-threatening bleeding during warfarin therapy. National Consortium of Anticoagulation Clinics. Arch Intern Med. 1996;156:1197-1201.
7. Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med. 1998;105:91-99.
8. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. EAFT (European Atrial Fibrillation Trial) Study Group. Lancet. 1993;342:1255-1262.
9. Ansell J, Hirsh J, Poller L, et al. The pharmacology and management of the vitamin K antagonists: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S204-S233.
10. Crowther MA, Douketis JD, Schnurr T, et al. Oral vitamin K lowers the international normalized ratio more rapidly than subcutaneous vitamin K in the treatment of warfarin-associated coagulopathy. A randomized, controlled trial. Ann Intern Med. 2002;137:251-254.
11. Whitling AM, Bussey HI, Lyons RM. Comparing different routes and doses of phytonadione for reversing excessive anticoagulation. Arch Intern Med. 1998;158:2136-2140.
12. Nee R, Doppenschmidt D, Donovan DJ, et al. Intravenous versus subcutaneous vitamin K1 in reversing excessive oral anticoagulation. Am J Cardiol. 1999;83:286-288.
13. Fan J, Armitstead JA, Adams AG, et al. A retrospective evaluation of vitamin K1 therapy to reverse the anticoagulant effect of warfarin. Pharmacotherapy. 2003;23:1245-1250.
14. Lubetsky A, Yonath H, Olchovsky D, et al. Comparison of oral vs intravenous phytonadione (vitamin K1) in patients with excessive anticoagulation: a prospective randomized controlled study. Arch Intern Med. 2003;163:2469-2473.
15. Hung A, Singh S, Tait RC. A prospective randomized study to determine the optimal dose of intravenous vitamin K in reversal of over-warfarinization. Br J Haematol. 2000;109:537-539.
16. Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists. Chest. 2008;133(suppl):160S-198S.
17. Dentali F, Ageno W, Crowther M. Treatment of coumarin-associated coagulopathy: a systematic review and proposed algorithms. J Thromb Haemost. 2006;4:1853-1863.
18. Makris M, Watson HG. The management of coumarin-induced over-anticoagulation Annotation [see comment]. Br J Haematol. 2001;114:271-280.
19. O’Shaughnessy DF, Atterbury C, Bolton Maggs P, et al. British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol. 2004;126:11-28.
20. Makris M. Optimisation of the prothrombin complex concentrate dose for warfarin reversal. Thromb Res. 2005;115:451-453.
21. Vigue B, Ract C, Tremey B, et al. Ultra-rapid management of oral anticoagulant therapy-related surgical intracranial hemorrhage. Intensive Care Med. 2007;33:721-725.
22. Kohler M. Thrombogenicity of prothrombin complex concentrates. Thromb Res. 1999;95(suppl 1):S13-S17.
23. Lorenz R, Kienast J, Otto U, et al. Successful emergency reversal of phenprocoumon anticoagulation with prothrombin complex concentrate: a prospective clinical study. Blood Coagul Fibrinolysis. 2007;18:565-570.
24. Pabinger I, Brenner B, Kalina U, et al. Beriplex P/N Anticoagulation Reversal Study Group. Prothrombin complex concentrate (Beriplex P/N) for emergency anticoagulation reversal: a prospective multinational clinical trial. J Thromb Haemost. 2008;6:622-631.
25. Sorensen B, Johansen P, Nielsen GL, et al. Reversal of the International Normalized Ratio with recombinant activated factor VII in central nervous system bleeding during warfarin thromboprophylaxis: clinical and biochemical aspects. Blood Coagul Fibrinolysis. 2003;14:469-477.
26. Brody DL, Aiyagari V, Shackleford AM, et al. Use of recombinant factor VIIa in patients with warfarin-associated intracranial hemorrhage. Neurocrit Care. 2005;2:263-267.
27. Tanaka KA, Szlam F, Dickneite G, et al. Effects of prothrombin complex concentrate and recombinant activated factor VII on vitamin K antagonist induced anticoagulation. Thromb Res. 2008;122:117-123.
28. Lin J, Hanigan WC, Tarantino M, et al. The use of recombinant activated factor VII to reverse warfarin-induced anticoagulation in patients with hemorrhages in the central nervous system: preliminary findings. J Neurosurg. 2003;98:737-740.
29. Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 2005;352:777-785.
30. Dager WE, King JH, Regalia RC, et al. Reversal of elevated international normalized ratio and bleeding with low-dose recombinant factor VII in patients receiving warfarin. Pharmacotherapy. 2006;26:1091-1098.
31. Fihn SD, McDonell M, Martin D, et al. Risk factors for complications of chronic anticoagulation. A multicenter study. Warfarin Optimized Outpatient Follow-up Study Group. Ann Intern Med. 1993;118:511-520.
32. Hanley JP. Warfarin reversal. J Clin Pathol. 2004;57:1132-1139.
33. Yasaka M, Sakata T, Minematsu K, et al. Correction of INR by prothrombin complex concentrate and vitamin K in patients with warfarin related hemorrhagic complication. Thromb Res. 2002;108:25-30.
34. Evans G, Luddington R, Baglin T. Beriplex P/N reverses severe warfarin-induced anticoagulation immediately and completely in patients presenting with major bleeding. Br J Haematol. 2001;115:998-1001.
35. Lubetsky A, Hoffman R, Zimlichman R, et al. Efficacy and safety of complex concentrate (Octaplex) for rapid reversal of oral anticoagulation. Thromb Res. 2004;113:371-378.
36. Cartmill M, Dolan G, Byrne JL, et al. Prothrombin complex concentrate for oral anticoagulant reversal in neurosurgical emergencies. Br J Neurosurg. 2000;14:458-461.
37. Deveras RA, Kessler CM. Reversal of warfarin-induced excessive anticoagulation with recombinant human factor VIIa concentrate. Ann Intern Med. 2002;137:884-888.
38. Holbrook AM, Pereira JA, Labiris R, et al. Systematic overview of warfarin and its drug and food interactions. Arch Intern Med. 2005;165:1095-1106.
39. Haines ST, Zeolla M, Witt DM. Venous Thromboembolism. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A Pathophysiological Approach. 6th ed. New York: McGraw-Hill Companies, Inc.; 2005:373-413.
40. Micromedex Healthcare Series. Drug-REAX System. New York: Thomson Reuters; 2008.
1. Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007;167:1414-1419.
2. Beyth RJ. Hemorrhagic complications of oral anticoagulant therapy. Clin Geriatr Med. 2001;17:49-56.
3. Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann Intern Med. 2003;139:893-900.
4. Levine MN, Raskob G, Beyth RJ, et al. Hemorrhagic complications of anticoagulant treatment: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S287-S310.
5. Pengo V, Legnani C, Noventa F, et al. ISCOAT Study Group. (Italian Study on Complications of Oral Anticoagulant Therapy). Oral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and risk of bleeding. A multicenter inception cohort study. Thromb Haemost. 2001;85:418-422.
6. White RH, McKittrick T, Takakuwa J, et al. Management and prognosis of life-threatening bleeding during warfarin therapy. National Consortium of Anticoagulation Clinics. Arch Intern Med. 1996;156:1197-1201.
7. Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med. 1998;105:91-99.
8. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. EAFT (European Atrial Fibrillation Trial) Study Group. Lancet. 1993;342:1255-1262.
9. Ansell J, Hirsh J, Poller L, et al. The pharmacology and management of the vitamin K antagonists: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S204-S233.
10. Crowther MA, Douketis JD, Schnurr T, et al. Oral vitamin K lowers the international normalized ratio more rapidly than subcutaneous vitamin K in the treatment of warfarin-associated coagulopathy. A randomized, controlled trial. Ann Intern Med. 2002;137:251-254.
11. Whitling AM, Bussey HI, Lyons RM. Comparing different routes and doses of phytonadione for reversing excessive anticoagulation. Arch Intern Med. 1998;158:2136-2140.
12. Nee R, Doppenschmidt D, Donovan DJ, et al. Intravenous versus subcutaneous vitamin K1 in reversing excessive oral anticoagulation. Am J Cardiol. 1999;83:286-288.
13. Fan J, Armitstead JA, Adams AG, et al. A retrospective evaluation of vitamin K1 therapy to reverse the anticoagulant effect of warfarin. Pharmacotherapy. 2003;23:1245-1250.
14. Lubetsky A, Yonath H, Olchovsky D, et al. Comparison of oral vs intravenous phytonadione (vitamin K1) in patients with excessive anticoagulation: a prospective randomized controlled study. Arch Intern Med. 2003;163:2469-2473.
15. Hung A, Singh S, Tait RC. A prospective randomized study to determine the optimal dose of intravenous vitamin K in reversal of over-warfarinization. Br J Haematol. 2000;109:537-539.
16. Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists. Chest. 2008;133(suppl):160S-198S.
17. Dentali F, Ageno W, Crowther M. Treatment of coumarin-associated coagulopathy: a systematic review and proposed algorithms. J Thromb Haemost. 2006;4:1853-1863.
18. Makris M, Watson HG. The management of coumarin-induced over-anticoagulation Annotation [see comment]. Br J Haematol. 2001;114:271-280.
19. O’Shaughnessy DF, Atterbury C, Bolton Maggs P, et al. British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol. 2004;126:11-28.
20. Makris M. Optimisation of the prothrombin complex concentrate dose for warfarin reversal. Thromb Res. 2005;115:451-453.
21. Vigue B, Ract C, Tremey B, et al. Ultra-rapid management of oral anticoagulant therapy-related surgical intracranial hemorrhage. Intensive Care Med. 2007;33:721-725.
22. Kohler M. Thrombogenicity of prothrombin complex concentrates. Thromb Res. 1999;95(suppl 1):S13-S17.
23. Lorenz R, Kienast J, Otto U, et al. Successful emergency reversal of phenprocoumon anticoagulation with prothrombin complex concentrate: a prospective clinical study. Blood Coagul Fibrinolysis. 2007;18:565-570.
24. Pabinger I, Brenner B, Kalina U, et al. Beriplex P/N Anticoagulation Reversal Study Group. Prothrombin complex concentrate (Beriplex P/N) for emergency anticoagulation reversal: a prospective multinational clinical trial. J Thromb Haemost. 2008;6:622-631.
25. Sorensen B, Johansen P, Nielsen GL, et al. Reversal of the International Normalized Ratio with recombinant activated factor VII in central nervous system bleeding during warfarin thromboprophylaxis: clinical and biochemical aspects. Blood Coagul Fibrinolysis. 2003;14:469-477.
26. Brody DL, Aiyagari V, Shackleford AM, et al. Use of recombinant factor VIIa in patients with warfarin-associated intracranial hemorrhage. Neurocrit Care. 2005;2:263-267.
27. Tanaka KA, Szlam F, Dickneite G, et al. Effects of prothrombin complex concentrate and recombinant activated factor VII on vitamin K antagonist induced anticoagulation. Thromb Res. 2008;122:117-123.
28. Lin J, Hanigan WC, Tarantino M, et al. The use of recombinant activated factor VII to reverse warfarin-induced anticoagulation in patients with hemorrhages in the central nervous system: preliminary findings. J Neurosurg. 2003;98:737-740.
29. Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 2005;352:777-785.
30. Dager WE, King JH, Regalia RC, et al. Reversal of elevated international normalized ratio and bleeding with low-dose recombinant factor VII in patients receiving warfarin. Pharmacotherapy. 2006;26:1091-1098.
31. Fihn SD, McDonell M, Martin D, et al. Risk factors for complications of chronic anticoagulation. A multicenter study. Warfarin Optimized Outpatient Follow-up Study Group. Ann Intern Med. 1993;118:511-520.
32. Hanley JP. Warfarin reversal. J Clin Pathol. 2004;57:1132-1139.
33. Yasaka M, Sakata T, Minematsu K, et al. Correction of INR by prothrombin complex concentrate and vitamin K in patients with warfarin related hemorrhagic complication. Thromb Res. 2002;108:25-30.
34. Evans G, Luddington R, Baglin T. Beriplex P/N reverses severe warfarin-induced anticoagulation immediately and completely in patients presenting with major bleeding. Br J Haematol. 2001;115:998-1001.
35. Lubetsky A, Hoffman R, Zimlichman R, et al. Efficacy and safety of complex concentrate (Octaplex) for rapid reversal of oral anticoagulation. Thromb Res. 2004;113:371-378.
36. Cartmill M, Dolan G, Byrne JL, et al. Prothrombin complex concentrate for oral anticoagulant reversal in neurosurgical emergencies. Br J Neurosurg. 2000;14:458-461.
37. Deveras RA, Kessler CM. Reversal of warfarin-induced excessive anticoagulation with recombinant human factor VIIa concentrate. Ann Intern Med. 2002;137:884-888.
38. Holbrook AM, Pereira JA, Labiris R, et al. Systematic overview of warfarin and its drug and food interactions. Arch Intern Med. 2005;165:1095-1106.
39. Haines ST, Zeolla M, Witt DM. Venous Thromboembolism. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A Pathophysiological Approach. 6th ed. New York: McGraw-Hill Companies, Inc.; 2005:373-413.
40. Micromedex Healthcare Series. Drug-REAX System. New York: Thomson Reuters; 2008.