User login
• Encourage home BP monitoring. Home readings are often lower than those taken in the office and closer to the average BP recorded by 24-hour ambulatory monitors. C
• Tell patients that reducing sodium intake not only reduces mortality, but it has positive cardiovascular effects separate from BP reduction, such as improved endothelium-dependent vasodilation. A
• Search for secondary causes of resistant hypertension, such as renal artery stenosis, pheochromocytoma, obstructive sleep apnea, and hyperaldosteronism. A
• Consider pseudohypertension in elderly patients who exhibit postural hypotension and fail to respond to increased doses of medication. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Mr. Brown is a 60-year-old African American man who works as a mid-level executive at a local bank. About a year and a half ago, he was diagnosed with hypertension, joining a number of other family members who also have the condition. Reviewing his chart, you note that at many of his visits—but not all of them—his systolic blood pressure runs close to 150 mm Hg, with diastolic pressure <90 mm Hg. Today his blood pressure is 148/88 mm Hg, numbers that exceed the parameters of the currently accepted definition of hypertension: blood pressure ≥140 mm Hg systolic or ≥90 mm Hg diastolic, taken on 2 separate occasions with the patient sitting down.1
Mr. Brown is one of the more than 65 million American adults suffering from high blood pressure—the No. 1 diagnosis reported in outpatient medical offices.2,3 Despite such prevalence, blood pressure control in the United States is suboptimal, with only one-third of hypertensive patients under adequate control.1 In 2007, the total estimated cost of treating high blood pressure in the United States exceeded $66 billion.4
When you tell Mr. Brown that his blood pressure doesn’t meet the therapeutic goal of <140/90 mm Hg, he gives you his reasons: He was late, he rushed, the traffic was bad, and the nurse rushed him into the exam room before he even had time to catch his breath. He insists his blood pressure is “normal” at home, and blames the elevated numbers on anxiety. He also tells you he was up working most of the night before, drinking coffee to stay awake to finish an urgent project.
Mr. Brown’s current medication regimen includes daily doses of lisinopril-hydrochlorothiazide (HCTZ) 20/25 mg daily and simvastatin 20 mg. He tells you he has no chest pain, shortness of breath, cough, edema, claudication, paroxysmal nocturnal dyspnea, or orthopnea. When you ask if he takes his lisinopril-HCTZ every day, he says Yes, but you have your suspicions.
Consider pseudo-resistance
Suboptimal blood pressure control can be classified as either pseudo-resistant or resistant hypertension. According to the definition used in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7), resistance is the “failure to achieve goal BP in patients who are adhering to full doses of an appropriate 3-drug regimen that includes a diuretic.”1
Hypertension is described as “pseudo-resistant” when persistent elevations in blood pressure are the result of a failure to comply with the medication regimen, “white-coat” syndrome, poor blood pressure technique, or a combination of these.5,6 Physician failure to prescribe adequate doses of medication, so-called clinical inertia, may also be a factor.5,7 Causes and remedies for pseudo-resistance are summarized in the algorithm.
In Mr. Brown’s case, he’s told you that he’s taking his lisinopril-HCTZ every day, but when you check your records, you see that the intervals between his refill requests range between 34 and 36 days. So you ask him, again, whether he is taking his lisinopril-HCTZ daily, and this time he says he takes the medication “at least 5 or 6 days a week.”
Encourage compliance. To motivate Mr. Brown, you tell him his blood pressure does not meet the goal of <140/90 mm Hg and that pressure higher than goal is a significant risk factor for cardiovascular disease. You emphasize the importance of taking his medication every day—a mantra you’ve repeated to countless patients over the years. In fact, it’s estimated that up to 40% of patients will discontinue their medication at some point during treatment.8 Patients’ reasons vary and may include medication side effects, the cost of treatment, or a patient’s personal philosophy. Cultural differences may also play a role in noncompliance.9
You talk with Mr. Brown a bit more and confirm that his poor compliance is due to simple forgetfulness and not another underlying reason that would need to be addressed. You hand him a pill calendar to help him keep track of his medication. You review the dosage and feel confident that you’ve prescribed a regimen simple enough for Mr. Brown to stick to and adequate to bring his pressure down.
When your white coat is the problem. Though not the case with Mr. Brown, a patient’s elevated readings could be a case of white coat hypertension—a conditioned response in some patients that is probably the result of anxiety in the medical setting.10 Patients with white coat hypertension have significantly less risk of death and reduced target organ damage than patients with truly resistant hypertension.11,12
If you suspect that a patient of yours has white coat hypertension, you can test your hypothesis by encouraging him or her to buy a blood pressure monitor to use at home, keep a log of the readings, and bring the log in to the next appointment. Improved technology has made home blood pressure monitoring an important tool in the treatment of high blood pressure.13-15
According to a 2008 statement issued jointly by the American Heart Association, the American Society of Hypertension, and the Preventive Cardiovascular Nurses Association, “There is a rapidly growing literature showing that measurements taken by patients at home are often lower than readings taken in the office and closer to the average blood pressure recorded by 24-hour ambulatory monitors, which is the blood pressure that best predicts cardiovascular risk.”14
Arm monitors are the most accurate because they measure brachial artery blood pressure.14 Most wrist monitors have not been validated in studies, but obese patients who cannot find a properly sized cuff may need to use them.14 Finger devices should never be used.14
Sometimes technique is at fault. To ensure that you get proper readings when your patient is in the office, advise the nursing staff not to take a patient’s blood pressure for at least 5 minutes after bringing him or her to an exam room. Specifically, the nurse can either make blood pressure measurement the last thing she (or he) does when “rooming” the patient, or she may prefer to go back to the exam room a few minutes after the patient is there to take the reading. The nurse should take care that the cuff is the right size and that the pressure is taken with the patient’s arm at heart level. In hypertensive patients, placing the arm below the horizontal in the dependent position can raise blood pressure 23/10 mm Hg.1,16,17
Newer blood pressure monitoring devices for the office are available that obviate artificially high readings caused by errors in technique and by white coat syndrome. Researchers have found that readings taken with the BpTRU automatic device, which obtains and records 5 blood pressure readings over a 5-minute period, are lower than those taken by office personnel, and that the white coat effect is eliminated.18,19
One pseudo-resistant case solved. At Mr. Brown’s next visit, you review his pill calendar with him and note that his blood pressure is now running 138/88 mm Hg and he is within his target goal of less than 140/90 mm Hg.
If Mr. Brown’s blood pressure control had continued to be suboptimal even after you’d taken steps to address cause(s) of pseudo-resistance, you would have had to shift gears and consider his case one of resistant hypertension.1
Consider resistant hypertension
Causes of resistant hypertension include lifestyle factors, side effects of medications, and secondary causes.5,6 Tobacco use, obesity, lack of exercise, a high sodium diet, and alcohol consumption can all contribute to hypertension.1,5,6,20,21 Dietary sodium in particular has significant adverse effects. Reducing dietary sodium not only reduces mortality, but has positive cardiovascular effects separate from blood pressure reduction, such as improved endothelium-dependent vasodilation.22-24
Medications including nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, sympathomimetics, glucocorticoids, and black licorice (found in some herbal supplements) may all raise blood pressure.5 Medications and other substances associated with increased blood pressure are listed in the TABLE. A search for such products, with changes or discontinuations that are clinically appropriate, should be part of any evaluation for resistant hypertension.
CASE 2 Ms. Stevens is a 30-year-old woman who was diagnosed with high blood pressure 7 months ago. She is currently taking triamterene-HCTZ 37.5/25 mg daily, amlodipine 10 mg daily, and metoprolol succinate 100 mg daily. She is compliant with medication, sticks to a low-sodium diet, and exercises 5 days a week. She does not drink alcohol. A review of her chart tells you her baseline serum chemistries, chest x-ray, and urinalysis are all normal. Today’s blood pressure taken in the sitting position after a 5-minute rest is 160/92 mm Hg. How should you proceed?
TABLE
Medications and other agents that may cause hypertension
| • Alcohol | • Cyclosporine | • Nicotine |
| • Antidepressants | • Erythropoietin | • NSAIDs |
| • Buspirone (Buspar) | • Estrogen preparations | • St. John’s wort |
| • Cocaine | • Licorice | • Tyramine-containing foods |
| • Corticosteroids | • Metoclopramide (Reglan) | |
| NSAIDs, nonsteroidal anti-infiammatory drugs. | ||
| Source: Chobanian A, et al. Hypertension. 2003.1 | ||
Is it resistant hypertension? Look for clues
You go over Ms. Stevens’ history carefully. Her hypertension medications should be adequate, and she is compliant with the prescribed regimen. Lifestyle factors are clearly not to blame: She’s not obese, she follows a low-sodium diet, doesn’t drink or smoke, and gets plenty of exercise. You ask her about other medications or over-the-counter supplements she takes, and nothing on her list raises a red flag. This doesn’t seem to be pseudo-resistance, and though you’re aware that only about 5% of cases of hypertension can be attributed to secondary causes, you think Ms. Stevens may be one of those patients.25
Numerous causes of secondary hypertension exist, and evaluations for such causes should be considered in all patients with resistant hypertension. Renal artery stenosis and pheochromocytoma are the most well-known causes, but less well known but significant contributors are obstructive sleep apnea and hyperaldosteronism.1,6,26,27
The relationship between obstructive sleep apnea and hypertension is not clear, and most of the studies linking the 2 conditions are population based.28 Nevertheless, because studies show that continuous positive airway pressure (CPAP) does improve blood pressure control in patients with obstructive sleep apnea, it is appropriate to investigate patients with resistant hypertension for this condition.29
Aldosterone’s role in resistant hypertension appears to be greatest in those with insulin resistance. The mechanism appears to be amplified sodium retention resulting in increased volume expansion, negative effects on oxidative stress, and elevated inflammation.27 Many patients with hypertension also have insulin resistance, so testing for hyperaldosteronism should be part of your investigation.
Test, and as necessary, test some more
Taking into consideration that 2 of the more common causes of secondary hypertension are obstructive sleep apnea and renal artery stenosis, you schedule an overnight sleep study for Ms. Stevens and a magnetic resonance arteriogram of the kidneys.26,30 (For more on the diagnostic tests and treatments for secondary causes of resistant hypertension, see the ALGORITHM.)
Reconsider medications. Ms. Stevens is already receiving the maximum dose of amlodipine, so you increase her metoprolol succinate to 200 mg daily and ask her to return in 1 month after the results of her tests come in.
Change medications and keep testing. At her next visit, Ms. Stevens’ blood pressure is 150/88 mm Hg, and her pulse rate is 64. Results of her overnight sleep study and magnetic resonance arteriogram are normal. At this juncture, with her work-up for common secondary causes of hypertension negative, you consider changes in her medication regimen. Because her pulse rate of 64 rules out any increase in the metoprolol, you decide to add lisinopril-HCTZ 10/12.5 mg to her regimen and discontinue her triamterene-HCTZ. Because her blood pressure is still elevated at this visit, you schedule additional testing to look for other secondary causes.
More tests, higher doses. One month later, Ms. Stevens returns with a blood pressure of 146/88 mm Hg. Appropriate testing for primary aldosteronism, pheochromocytoma, Cushing’s disease, and coarctation are all normal. Her lisinopril-HCTZ dose is increased to 20/12.5 mg, and when she returns 1 month later her blood pressure reading is 138/88 mm Hg.
You conclude that she is a patient with hard-to-control hypertension with no underlying cause who requires a significant amount of medication. That is not an uncommon situation. Although her blood pressure is now controlled to an appropriate level, you make a chart notation to consider referral to a hypertension specialist if her blood pressure become elevated again and treatment changes are not effective.6
ALGORITHM
Hard-to-control hypertension? This treatment algorithm can help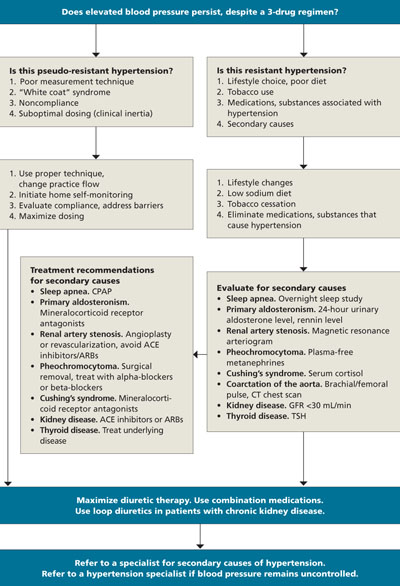
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CPAP, continuous positive airway pressure; CT, computed tomography; GFR, glomerular filtration rate; TSH, thyroid-stimulating hormone.
Adapted from: Calhoun DA, et al. Hypertension. 2008.6
Another consideration: Pseudohypertension
This uncommon condition sometimes occurs in elderly patients who suffer from a stiffened or thickened brachial artery.1 Because the blood pressure cuff cannot compress the artery, blood pressure readings overestimate true arterial pressure. The condition should be considered in patients when increased doses of medication fail to achieve the desired response, particularly in patients who exhibit postural hypotension.1
This was not a likely explanation for Ms. Stevens, however, given the clinical scenario and her young age.
CORRESPONDENCE Randy Wexler, MD, MPH, B0902B Cramblett Hall, 456 W 10th Avenue, Columbus, OH 43210; randy.wexler@osumc.edu
1. Chobanian A, Bakris GL, Black HR, et al. Seventh Report of The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7). Hypertension. 2003;42:1206-1252.
2. Fields L, Burt V, Cutler J, et al. The burden of adult hypertension in the United States 1999-2000: A rising tide. Hypertension. 2004;44:1-7.
3. Fang J, Alderman MH, Keenan NL, et al. Hypertension control at physicians’ offices in the United States. Am J Hypertens. 2008;21:136-142.
4. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics–2007 update. Circulation. 2007;115:e69-e171.
5. Sarafidis PA, Bakris GL. Resistant hypertension: an overview of evaluation and treatment. J Am Coll Cardiol. 2008;52:1749-1757.
6. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403-1419.
7. Phillips LS, Branch WT, Book CB, et al. Clinical inertia. Ann Intern Med. 2001;135:825-834.
8. Van Wijk BL, Klungel OH, Heerdink ER, et al. Rate and determinants of 10-year persistence with antihypertensive drugs. J Hypertens. 2005;23:2101-2107.
9. Wexler R, Pleister A, Feldman D. Sociology meets genetics: sociogenetic implications for future management of hypertension and heart failure. Curr Treat Options Cardiovasc Med. 2009;11:305-315.
10. Ogedegbe G, Pickering TG, Clemow L, et al. The misdiagnosis of hypertension: the role of patient anxiety. Arch Intern Med. 2008;168:2459-2465.
11. Dawes MG, Bartlett G, Coats AJ, et al. Comparing the effects of white coat hypertension and sustained hypertension on mortality in a UK primary care setting. Ann Fam Med. 2008;6:390-396.
12. Pierdomenico SD, Lapenna D, Bucci A, et al. Cardiovascular outcome in treated hypertensive patients with responder, masked, false resistant, and true resistant hypertension. Am J Hypertens. 2005;18:1422-1428.
13. Verberk WJ, Kroon AA, Kessels AGH, et al. Home blood pressure monitoring: a systematic review. J Am Coll Cardiol. 2005;46:743-751.
14. Pickering TG, Miller NH, Ogedegbe G, et al. AHA/ASH/PCNA scientific statement. Call to action on use and reimbursement for home blood pressure monitoring. Hypertension. 2008;52:10-29.
15. O’Brien E. Ambulatory blood pressure measurement: the case for implementation in primary care. Hypertension. 2008;51:1435-1441.
16. O’Brien E, Asmar R, Beilin L, et al. On behalf of the European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension recommendations for conventional ambulatory and home blood pressure measurements. J Hypertens. 2003;21:821-848.
17. Mourad A, Carney S, Gillies A, et al. Arm position and blood pressure: a risk factor for hypertension. J Hum Hypertens. 2003;17:389-395.
18. Myers MG. Automated blood pressure measurement in routine clinical practice. Blood Press Monit. 2006;11:59-62.
19. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce white coat hypertension. J Hypertens. 2009;27:280-286.
20. He J, Paul J, Whelton P, Appel L, et al. Long-term effects of weight loss and dietary sodium reduction on incidence of hypertension. Hypertension. 2000;35:544-549.
21. PREMIER Collaborative Research Writing Group. Effects of comprehensive lifestyle modification on blood pressure control. JAMA. 2003;289:2083-2093.
22. Cook NR, Cutler JA, Obarzanek E, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP). BMJ. 2007;334:885-888.
23. Dickinson BD, Havas S. Reducing the population burden of cardiovascular disease by reducing sodium intake. Arch Intern Med. 2007;167:1460-1468.
24. Li J, White J, Guo L, et al. Salt inactivates endothelial nitric oxide synthase in endothelial cells. J Nutr. 2009;139:1-5.
25. Beevers G, Lip G, O’Brien E. ABCs of hypertension: the pathophysiology of hypertension. BMJ. 2001;322:912-916.
26. Peppard PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378-1384.
27. Sowers JR, Whaley-Connell A, Epstein M. Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med. 2009;150:776-783.
28. Young T, Peppard P, Palta M, et al. Population-based study of sleep-disordered breathing as a risk factor for hypertension. Arch Intern Med. 1997;157:1746-1752.
29. Haentjens P, Van Meerhaeghe A, Moscariello A. The impact of continuous positive airway pressure on blood pressure in patients with obstructive sleep apnea syndrome: evidence from a meta-analysis of placebo-controlled randomized trials. Arch Intern Med. 2007;167:757-764.
30. Kawashima A, Francis IR, Baumgarten DA, et al. For the Expert Panel on Urologic Imaging. Renovascular hypertension. Reston, Va: American College of Radiology; 2007. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=11590&nbr=6003. Accessed April 4, 2009.
• Encourage home BP monitoring. Home readings are often lower than those taken in the office and closer to the average BP recorded by 24-hour ambulatory monitors. C
• Tell patients that reducing sodium intake not only reduces mortality, but it has positive cardiovascular effects separate from BP reduction, such as improved endothelium-dependent vasodilation. A
• Search for secondary causes of resistant hypertension, such as renal artery stenosis, pheochromocytoma, obstructive sleep apnea, and hyperaldosteronism. A
• Consider pseudohypertension in elderly patients who exhibit postural hypotension and fail to respond to increased doses of medication. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Mr. Brown is a 60-year-old African American man who works as a mid-level executive at a local bank. About a year and a half ago, he was diagnosed with hypertension, joining a number of other family members who also have the condition. Reviewing his chart, you note that at many of his visits—but not all of them—his systolic blood pressure runs close to 150 mm Hg, with diastolic pressure <90 mm Hg. Today his blood pressure is 148/88 mm Hg, numbers that exceed the parameters of the currently accepted definition of hypertension: blood pressure ≥140 mm Hg systolic or ≥90 mm Hg diastolic, taken on 2 separate occasions with the patient sitting down.1
Mr. Brown is one of the more than 65 million American adults suffering from high blood pressure—the No. 1 diagnosis reported in outpatient medical offices.2,3 Despite such prevalence, blood pressure control in the United States is suboptimal, with only one-third of hypertensive patients under adequate control.1 In 2007, the total estimated cost of treating high blood pressure in the United States exceeded $66 billion.4
When you tell Mr. Brown that his blood pressure doesn’t meet the therapeutic goal of <140/90 mm Hg, he gives you his reasons: He was late, he rushed, the traffic was bad, and the nurse rushed him into the exam room before he even had time to catch his breath. He insists his blood pressure is “normal” at home, and blames the elevated numbers on anxiety. He also tells you he was up working most of the night before, drinking coffee to stay awake to finish an urgent project.
Mr. Brown’s current medication regimen includes daily doses of lisinopril-hydrochlorothiazide (HCTZ) 20/25 mg daily and simvastatin 20 mg. He tells you he has no chest pain, shortness of breath, cough, edema, claudication, paroxysmal nocturnal dyspnea, or orthopnea. When you ask if he takes his lisinopril-HCTZ every day, he says Yes, but you have your suspicions.
Consider pseudo-resistance
Suboptimal blood pressure control can be classified as either pseudo-resistant or resistant hypertension. According to the definition used in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7), resistance is the “failure to achieve goal BP in patients who are adhering to full doses of an appropriate 3-drug regimen that includes a diuretic.”1
Hypertension is described as “pseudo-resistant” when persistent elevations in blood pressure are the result of a failure to comply with the medication regimen, “white-coat” syndrome, poor blood pressure technique, or a combination of these.5,6 Physician failure to prescribe adequate doses of medication, so-called clinical inertia, may also be a factor.5,7 Causes and remedies for pseudo-resistance are summarized in the algorithm.
In Mr. Brown’s case, he’s told you that he’s taking his lisinopril-HCTZ every day, but when you check your records, you see that the intervals between his refill requests range between 34 and 36 days. So you ask him, again, whether he is taking his lisinopril-HCTZ daily, and this time he says he takes the medication “at least 5 or 6 days a week.”
Encourage compliance. To motivate Mr. Brown, you tell him his blood pressure does not meet the goal of <140/90 mm Hg and that pressure higher than goal is a significant risk factor for cardiovascular disease. You emphasize the importance of taking his medication every day—a mantra you’ve repeated to countless patients over the years. In fact, it’s estimated that up to 40% of patients will discontinue their medication at some point during treatment.8 Patients’ reasons vary and may include medication side effects, the cost of treatment, or a patient’s personal philosophy. Cultural differences may also play a role in noncompliance.9
You talk with Mr. Brown a bit more and confirm that his poor compliance is due to simple forgetfulness and not another underlying reason that would need to be addressed. You hand him a pill calendar to help him keep track of his medication. You review the dosage and feel confident that you’ve prescribed a regimen simple enough for Mr. Brown to stick to and adequate to bring his pressure down.
When your white coat is the problem. Though not the case with Mr. Brown, a patient’s elevated readings could be a case of white coat hypertension—a conditioned response in some patients that is probably the result of anxiety in the medical setting.10 Patients with white coat hypertension have significantly less risk of death and reduced target organ damage than patients with truly resistant hypertension.11,12
If you suspect that a patient of yours has white coat hypertension, you can test your hypothesis by encouraging him or her to buy a blood pressure monitor to use at home, keep a log of the readings, and bring the log in to the next appointment. Improved technology has made home blood pressure monitoring an important tool in the treatment of high blood pressure.13-15
According to a 2008 statement issued jointly by the American Heart Association, the American Society of Hypertension, and the Preventive Cardiovascular Nurses Association, “There is a rapidly growing literature showing that measurements taken by patients at home are often lower than readings taken in the office and closer to the average blood pressure recorded by 24-hour ambulatory monitors, which is the blood pressure that best predicts cardiovascular risk.”14
Arm monitors are the most accurate because they measure brachial artery blood pressure.14 Most wrist monitors have not been validated in studies, but obese patients who cannot find a properly sized cuff may need to use them.14 Finger devices should never be used.14
Sometimes technique is at fault. To ensure that you get proper readings when your patient is in the office, advise the nursing staff not to take a patient’s blood pressure for at least 5 minutes after bringing him or her to an exam room. Specifically, the nurse can either make blood pressure measurement the last thing she (or he) does when “rooming” the patient, or she may prefer to go back to the exam room a few minutes after the patient is there to take the reading. The nurse should take care that the cuff is the right size and that the pressure is taken with the patient’s arm at heart level. In hypertensive patients, placing the arm below the horizontal in the dependent position can raise blood pressure 23/10 mm Hg.1,16,17
Newer blood pressure monitoring devices for the office are available that obviate artificially high readings caused by errors in technique and by white coat syndrome. Researchers have found that readings taken with the BpTRU automatic device, which obtains and records 5 blood pressure readings over a 5-minute period, are lower than those taken by office personnel, and that the white coat effect is eliminated.18,19
One pseudo-resistant case solved. At Mr. Brown’s next visit, you review his pill calendar with him and note that his blood pressure is now running 138/88 mm Hg and he is within his target goal of less than 140/90 mm Hg.
If Mr. Brown’s blood pressure control had continued to be suboptimal even after you’d taken steps to address cause(s) of pseudo-resistance, you would have had to shift gears and consider his case one of resistant hypertension.1
Consider resistant hypertension
Causes of resistant hypertension include lifestyle factors, side effects of medications, and secondary causes.5,6 Tobacco use, obesity, lack of exercise, a high sodium diet, and alcohol consumption can all contribute to hypertension.1,5,6,20,21 Dietary sodium in particular has significant adverse effects. Reducing dietary sodium not only reduces mortality, but has positive cardiovascular effects separate from blood pressure reduction, such as improved endothelium-dependent vasodilation.22-24
Medications including nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, sympathomimetics, glucocorticoids, and black licorice (found in some herbal supplements) may all raise blood pressure.5 Medications and other substances associated with increased blood pressure are listed in the TABLE. A search for such products, with changes or discontinuations that are clinically appropriate, should be part of any evaluation for resistant hypertension.
CASE 2 Ms. Stevens is a 30-year-old woman who was diagnosed with high blood pressure 7 months ago. She is currently taking triamterene-HCTZ 37.5/25 mg daily, amlodipine 10 mg daily, and metoprolol succinate 100 mg daily. She is compliant with medication, sticks to a low-sodium diet, and exercises 5 days a week. She does not drink alcohol. A review of her chart tells you her baseline serum chemistries, chest x-ray, and urinalysis are all normal. Today’s blood pressure taken in the sitting position after a 5-minute rest is 160/92 mm Hg. How should you proceed?
TABLE
Medications and other agents that may cause hypertension
| • Alcohol | • Cyclosporine | • Nicotine |
| • Antidepressants | • Erythropoietin | • NSAIDs |
| • Buspirone (Buspar) | • Estrogen preparations | • St. John’s wort |
| • Cocaine | • Licorice | • Tyramine-containing foods |
| • Corticosteroids | • Metoclopramide (Reglan) | |
| NSAIDs, nonsteroidal anti-infiammatory drugs. | ||
| Source: Chobanian A, et al. Hypertension. 2003.1 | ||
Is it resistant hypertension? Look for clues
You go over Ms. Stevens’ history carefully. Her hypertension medications should be adequate, and she is compliant with the prescribed regimen. Lifestyle factors are clearly not to blame: She’s not obese, she follows a low-sodium diet, doesn’t drink or smoke, and gets plenty of exercise. You ask her about other medications or over-the-counter supplements she takes, and nothing on her list raises a red flag. This doesn’t seem to be pseudo-resistance, and though you’re aware that only about 5% of cases of hypertension can be attributed to secondary causes, you think Ms. Stevens may be one of those patients.25
Numerous causes of secondary hypertension exist, and evaluations for such causes should be considered in all patients with resistant hypertension. Renal artery stenosis and pheochromocytoma are the most well-known causes, but less well known but significant contributors are obstructive sleep apnea and hyperaldosteronism.1,6,26,27
The relationship between obstructive sleep apnea and hypertension is not clear, and most of the studies linking the 2 conditions are population based.28 Nevertheless, because studies show that continuous positive airway pressure (CPAP) does improve blood pressure control in patients with obstructive sleep apnea, it is appropriate to investigate patients with resistant hypertension for this condition.29
Aldosterone’s role in resistant hypertension appears to be greatest in those with insulin resistance. The mechanism appears to be amplified sodium retention resulting in increased volume expansion, negative effects on oxidative stress, and elevated inflammation.27 Many patients with hypertension also have insulin resistance, so testing for hyperaldosteronism should be part of your investigation.
Test, and as necessary, test some more
Taking into consideration that 2 of the more common causes of secondary hypertension are obstructive sleep apnea and renal artery stenosis, you schedule an overnight sleep study for Ms. Stevens and a magnetic resonance arteriogram of the kidneys.26,30 (For more on the diagnostic tests and treatments for secondary causes of resistant hypertension, see the ALGORITHM.)
Reconsider medications. Ms. Stevens is already receiving the maximum dose of amlodipine, so you increase her metoprolol succinate to 200 mg daily and ask her to return in 1 month after the results of her tests come in.
Change medications and keep testing. At her next visit, Ms. Stevens’ blood pressure is 150/88 mm Hg, and her pulse rate is 64. Results of her overnight sleep study and magnetic resonance arteriogram are normal. At this juncture, with her work-up for common secondary causes of hypertension negative, you consider changes in her medication regimen. Because her pulse rate of 64 rules out any increase in the metoprolol, you decide to add lisinopril-HCTZ 10/12.5 mg to her regimen and discontinue her triamterene-HCTZ. Because her blood pressure is still elevated at this visit, you schedule additional testing to look for other secondary causes.
More tests, higher doses. One month later, Ms. Stevens returns with a blood pressure of 146/88 mm Hg. Appropriate testing for primary aldosteronism, pheochromocytoma, Cushing’s disease, and coarctation are all normal. Her lisinopril-HCTZ dose is increased to 20/12.5 mg, and when she returns 1 month later her blood pressure reading is 138/88 mm Hg.
You conclude that she is a patient with hard-to-control hypertension with no underlying cause who requires a significant amount of medication. That is not an uncommon situation. Although her blood pressure is now controlled to an appropriate level, you make a chart notation to consider referral to a hypertension specialist if her blood pressure become elevated again and treatment changes are not effective.6
ALGORITHM
Hard-to-control hypertension? This treatment algorithm can help
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CPAP, continuous positive airway pressure; CT, computed tomography; GFR, glomerular filtration rate; TSH, thyroid-stimulating hormone.
Adapted from: Calhoun DA, et al. Hypertension. 2008.6
Another consideration: Pseudohypertension
This uncommon condition sometimes occurs in elderly patients who suffer from a stiffened or thickened brachial artery.1 Because the blood pressure cuff cannot compress the artery, blood pressure readings overestimate true arterial pressure. The condition should be considered in patients when increased doses of medication fail to achieve the desired response, particularly in patients who exhibit postural hypotension.1
This was not a likely explanation for Ms. Stevens, however, given the clinical scenario and her young age.
CORRESPONDENCE Randy Wexler, MD, MPH, B0902B Cramblett Hall, 456 W 10th Avenue, Columbus, OH 43210; randy.wexler@osumc.edu
• Encourage home BP monitoring. Home readings are often lower than those taken in the office and closer to the average BP recorded by 24-hour ambulatory monitors. C
• Tell patients that reducing sodium intake not only reduces mortality, but it has positive cardiovascular effects separate from BP reduction, such as improved endothelium-dependent vasodilation. A
• Search for secondary causes of resistant hypertension, such as renal artery stenosis, pheochromocytoma, obstructive sleep apnea, and hyperaldosteronism. A
• Consider pseudohypertension in elderly patients who exhibit postural hypotension and fail to respond to increased doses of medication. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Mr. Brown is a 60-year-old African American man who works as a mid-level executive at a local bank. About a year and a half ago, he was diagnosed with hypertension, joining a number of other family members who also have the condition. Reviewing his chart, you note that at many of his visits—but not all of them—his systolic blood pressure runs close to 150 mm Hg, with diastolic pressure <90 mm Hg. Today his blood pressure is 148/88 mm Hg, numbers that exceed the parameters of the currently accepted definition of hypertension: blood pressure ≥140 mm Hg systolic or ≥90 mm Hg diastolic, taken on 2 separate occasions with the patient sitting down.1
Mr. Brown is one of the more than 65 million American adults suffering from high blood pressure—the No. 1 diagnosis reported in outpatient medical offices.2,3 Despite such prevalence, blood pressure control in the United States is suboptimal, with only one-third of hypertensive patients under adequate control.1 In 2007, the total estimated cost of treating high blood pressure in the United States exceeded $66 billion.4
When you tell Mr. Brown that his blood pressure doesn’t meet the therapeutic goal of <140/90 mm Hg, he gives you his reasons: He was late, he rushed, the traffic was bad, and the nurse rushed him into the exam room before he even had time to catch his breath. He insists his blood pressure is “normal” at home, and blames the elevated numbers on anxiety. He also tells you he was up working most of the night before, drinking coffee to stay awake to finish an urgent project.
Mr. Brown’s current medication regimen includes daily doses of lisinopril-hydrochlorothiazide (HCTZ) 20/25 mg daily and simvastatin 20 mg. He tells you he has no chest pain, shortness of breath, cough, edema, claudication, paroxysmal nocturnal dyspnea, or orthopnea. When you ask if he takes his lisinopril-HCTZ every day, he says Yes, but you have your suspicions.
Consider pseudo-resistance
Suboptimal blood pressure control can be classified as either pseudo-resistant or resistant hypertension. According to the definition used in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7), resistance is the “failure to achieve goal BP in patients who are adhering to full doses of an appropriate 3-drug regimen that includes a diuretic.”1
Hypertension is described as “pseudo-resistant” when persistent elevations in blood pressure are the result of a failure to comply with the medication regimen, “white-coat” syndrome, poor blood pressure technique, or a combination of these.5,6 Physician failure to prescribe adequate doses of medication, so-called clinical inertia, may also be a factor.5,7 Causes and remedies for pseudo-resistance are summarized in the algorithm.
In Mr. Brown’s case, he’s told you that he’s taking his lisinopril-HCTZ every day, but when you check your records, you see that the intervals between his refill requests range between 34 and 36 days. So you ask him, again, whether he is taking his lisinopril-HCTZ daily, and this time he says he takes the medication “at least 5 or 6 days a week.”
Encourage compliance. To motivate Mr. Brown, you tell him his blood pressure does not meet the goal of <140/90 mm Hg and that pressure higher than goal is a significant risk factor for cardiovascular disease. You emphasize the importance of taking his medication every day—a mantra you’ve repeated to countless patients over the years. In fact, it’s estimated that up to 40% of patients will discontinue their medication at some point during treatment.8 Patients’ reasons vary and may include medication side effects, the cost of treatment, or a patient’s personal philosophy. Cultural differences may also play a role in noncompliance.9
You talk with Mr. Brown a bit more and confirm that his poor compliance is due to simple forgetfulness and not another underlying reason that would need to be addressed. You hand him a pill calendar to help him keep track of his medication. You review the dosage and feel confident that you’ve prescribed a regimen simple enough for Mr. Brown to stick to and adequate to bring his pressure down.
When your white coat is the problem. Though not the case with Mr. Brown, a patient’s elevated readings could be a case of white coat hypertension—a conditioned response in some patients that is probably the result of anxiety in the medical setting.10 Patients with white coat hypertension have significantly less risk of death and reduced target organ damage than patients with truly resistant hypertension.11,12
If you suspect that a patient of yours has white coat hypertension, you can test your hypothesis by encouraging him or her to buy a blood pressure monitor to use at home, keep a log of the readings, and bring the log in to the next appointment. Improved technology has made home blood pressure monitoring an important tool in the treatment of high blood pressure.13-15
According to a 2008 statement issued jointly by the American Heart Association, the American Society of Hypertension, and the Preventive Cardiovascular Nurses Association, “There is a rapidly growing literature showing that measurements taken by patients at home are often lower than readings taken in the office and closer to the average blood pressure recorded by 24-hour ambulatory monitors, which is the blood pressure that best predicts cardiovascular risk.”14
Arm monitors are the most accurate because they measure brachial artery blood pressure.14 Most wrist monitors have not been validated in studies, but obese patients who cannot find a properly sized cuff may need to use them.14 Finger devices should never be used.14
Sometimes technique is at fault. To ensure that you get proper readings when your patient is in the office, advise the nursing staff not to take a patient’s blood pressure for at least 5 minutes after bringing him or her to an exam room. Specifically, the nurse can either make blood pressure measurement the last thing she (or he) does when “rooming” the patient, or she may prefer to go back to the exam room a few minutes after the patient is there to take the reading. The nurse should take care that the cuff is the right size and that the pressure is taken with the patient’s arm at heart level. In hypertensive patients, placing the arm below the horizontal in the dependent position can raise blood pressure 23/10 mm Hg.1,16,17
Newer blood pressure monitoring devices for the office are available that obviate artificially high readings caused by errors in technique and by white coat syndrome. Researchers have found that readings taken with the BpTRU automatic device, which obtains and records 5 blood pressure readings over a 5-minute period, are lower than those taken by office personnel, and that the white coat effect is eliminated.18,19
One pseudo-resistant case solved. At Mr. Brown’s next visit, you review his pill calendar with him and note that his blood pressure is now running 138/88 mm Hg and he is within his target goal of less than 140/90 mm Hg.
If Mr. Brown’s blood pressure control had continued to be suboptimal even after you’d taken steps to address cause(s) of pseudo-resistance, you would have had to shift gears and consider his case one of resistant hypertension.1
Consider resistant hypertension
Causes of resistant hypertension include lifestyle factors, side effects of medications, and secondary causes.5,6 Tobacco use, obesity, lack of exercise, a high sodium diet, and alcohol consumption can all contribute to hypertension.1,5,6,20,21 Dietary sodium in particular has significant adverse effects. Reducing dietary sodium not only reduces mortality, but has positive cardiovascular effects separate from blood pressure reduction, such as improved endothelium-dependent vasodilation.22-24
Medications including nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, sympathomimetics, glucocorticoids, and black licorice (found in some herbal supplements) may all raise blood pressure.5 Medications and other substances associated with increased blood pressure are listed in the TABLE. A search for such products, with changes or discontinuations that are clinically appropriate, should be part of any evaluation for resistant hypertension.
CASE 2 Ms. Stevens is a 30-year-old woman who was diagnosed with high blood pressure 7 months ago. She is currently taking triamterene-HCTZ 37.5/25 mg daily, amlodipine 10 mg daily, and metoprolol succinate 100 mg daily. She is compliant with medication, sticks to a low-sodium diet, and exercises 5 days a week. She does not drink alcohol. A review of her chart tells you her baseline serum chemistries, chest x-ray, and urinalysis are all normal. Today’s blood pressure taken in the sitting position after a 5-minute rest is 160/92 mm Hg. How should you proceed?
TABLE
Medications and other agents that may cause hypertension
| • Alcohol | • Cyclosporine | • Nicotine |
| • Antidepressants | • Erythropoietin | • NSAIDs |
| • Buspirone (Buspar) | • Estrogen preparations | • St. John’s wort |
| • Cocaine | • Licorice | • Tyramine-containing foods |
| • Corticosteroids | • Metoclopramide (Reglan) | |
| NSAIDs, nonsteroidal anti-infiammatory drugs. | ||
| Source: Chobanian A, et al. Hypertension. 2003.1 | ||
Is it resistant hypertension? Look for clues
You go over Ms. Stevens’ history carefully. Her hypertension medications should be adequate, and she is compliant with the prescribed regimen. Lifestyle factors are clearly not to blame: She’s not obese, she follows a low-sodium diet, doesn’t drink or smoke, and gets plenty of exercise. You ask her about other medications or over-the-counter supplements she takes, and nothing on her list raises a red flag. This doesn’t seem to be pseudo-resistance, and though you’re aware that only about 5% of cases of hypertension can be attributed to secondary causes, you think Ms. Stevens may be one of those patients.25
Numerous causes of secondary hypertension exist, and evaluations for such causes should be considered in all patients with resistant hypertension. Renal artery stenosis and pheochromocytoma are the most well-known causes, but less well known but significant contributors are obstructive sleep apnea and hyperaldosteronism.1,6,26,27
The relationship between obstructive sleep apnea and hypertension is not clear, and most of the studies linking the 2 conditions are population based.28 Nevertheless, because studies show that continuous positive airway pressure (CPAP) does improve blood pressure control in patients with obstructive sleep apnea, it is appropriate to investigate patients with resistant hypertension for this condition.29
Aldosterone’s role in resistant hypertension appears to be greatest in those with insulin resistance. The mechanism appears to be amplified sodium retention resulting in increased volume expansion, negative effects on oxidative stress, and elevated inflammation.27 Many patients with hypertension also have insulin resistance, so testing for hyperaldosteronism should be part of your investigation.
Test, and as necessary, test some more
Taking into consideration that 2 of the more common causes of secondary hypertension are obstructive sleep apnea and renal artery stenosis, you schedule an overnight sleep study for Ms. Stevens and a magnetic resonance arteriogram of the kidneys.26,30 (For more on the diagnostic tests and treatments for secondary causes of resistant hypertension, see the ALGORITHM.)
Reconsider medications. Ms. Stevens is already receiving the maximum dose of amlodipine, so you increase her metoprolol succinate to 200 mg daily and ask her to return in 1 month after the results of her tests come in.
Change medications and keep testing. At her next visit, Ms. Stevens’ blood pressure is 150/88 mm Hg, and her pulse rate is 64. Results of her overnight sleep study and magnetic resonance arteriogram are normal. At this juncture, with her work-up for common secondary causes of hypertension negative, you consider changes in her medication regimen. Because her pulse rate of 64 rules out any increase in the metoprolol, you decide to add lisinopril-HCTZ 10/12.5 mg to her regimen and discontinue her triamterene-HCTZ. Because her blood pressure is still elevated at this visit, you schedule additional testing to look for other secondary causes.
More tests, higher doses. One month later, Ms. Stevens returns with a blood pressure of 146/88 mm Hg. Appropriate testing for primary aldosteronism, pheochromocytoma, Cushing’s disease, and coarctation are all normal. Her lisinopril-HCTZ dose is increased to 20/12.5 mg, and when she returns 1 month later her blood pressure reading is 138/88 mm Hg.
You conclude that she is a patient with hard-to-control hypertension with no underlying cause who requires a significant amount of medication. That is not an uncommon situation. Although her blood pressure is now controlled to an appropriate level, you make a chart notation to consider referral to a hypertension specialist if her blood pressure become elevated again and treatment changes are not effective.6
ALGORITHM
Hard-to-control hypertension? This treatment algorithm can help
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CPAP, continuous positive airway pressure; CT, computed tomography; GFR, glomerular filtration rate; TSH, thyroid-stimulating hormone.
Adapted from: Calhoun DA, et al. Hypertension. 2008.6
Another consideration: Pseudohypertension
This uncommon condition sometimes occurs in elderly patients who suffer from a stiffened or thickened brachial artery.1 Because the blood pressure cuff cannot compress the artery, blood pressure readings overestimate true arterial pressure. The condition should be considered in patients when increased doses of medication fail to achieve the desired response, particularly in patients who exhibit postural hypotension.1
This was not a likely explanation for Ms. Stevens, however, given the clinical scenario and her young age.
CORRESPONDENCE Randy Wexler, MD, MPH, B0902B Cramblett Hall, 456 W 10th Avenue, Columbus, OH 43210; randy.wexler@osumc.edu
1. Chobanian A, Bakris GL, Black HR, et al. Seventh Report of The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7). Hypertension. 2003;42:1206-1252.
2. Fields L, Burt V, Cutler J, et al. The burden of adult hypertension in the United States 1999-2000: A rising tide. Hypertension. 2004;44:1-7.
3. Fang J, Alderman MH, Keenan NL, et al. Hypertension control at physicians’ offices in the United States. Am J Hypertens. 2008;21:136-142.
4. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics–2007 update. Circulation. 2007;115:e69-e171.
5. Sarafidis PA, Bakris GL. Resistant hypertension: an overview of evaluation and treatment. J Am Coll Cardiol. 2008;52:1749-1757.
6. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403-1419.
7. Phillips LS, Branch WT, Book CB, et al. Clinical inertia. Ann Intern Med. 2001;135:825-834.
8. Van Wijk BL, Klungel OH, Heerdink ER, et al. Rate and determinants of 10-year persistence with antihypertensive drugs. J Hypertens. 2005;23:2101-2107.
9. Wexler R, Pleister A, Feldman D. Sociology meets genetics: sociogenetic implications for future management of hypertension and heart failure. Curr Treat Options Cardiovasc Med. 2009;11:305-315.
10. Ogedegbe G, Pickering TG, Clemow L, et al. The misdiagnosis of hypertension: the role of patient anxiety. Arch Intern Med. 2008;168:2459-2465.
11. Dawes MG, Bartlett G, Coats AJ, et al. Comparing the effects of white coat hypertension and sustained hypertension on mortality in a UK primary care setting. Ann Fam Med. 2008;6:390-396.
12. Pierdomenico SD, Lapenna D, Bucci A, et al. Cardiovascular outcome in treated hypertensive patients with responder, masked, false resistant, and true resistant hypertension. Am J Hypertens. 2005;18:1422-1428.
13. Verberk WJ, Kroon AA, Kessels AGH, et al. Home blood pressure monitoring: a systematic review. J Am Coll Cardiol. 2005;46:743-751.
14. Pickering TG, Miller NH, Ogedegbe G, et al. AHA/ASH/PCNA scientific statement. Call to action on use and reimbursement for home blood pressure monitoring. Hypertension. 2008;52:10-29.
15. O’Brien E. Ambulatory blood pressure measurement: the case for implementation in primary care. Hypertension. 2008;51:1435-1441.
16. O’Brien E, Asmar R, Beilin L, et al. On behalf of the European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension recommendations for conventional ambulatory and home blood pressure measurements. J Hypertens. 2003;21:821-848.
17. Mourad A, Carney S, Gillies A, et al. Arm position and blood pressure: a risk factor for hypertension. J Hum Hypertens. 2003;17:389-395.
18. Myers MG. Automated blood pressure measurement in routine clinical practice. Blood Press Monit. 2006;11:59-62.
19. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce white coat hypertension. J Hypertens. 2009;27:280-286.
20. He J, Paul J, Whelton P, Appel L, et al. Long-term effects of weight loss and dietary sodium reduction on incidence of hypertension. Hypertension. 2000;35:544-549.
21. PREMIER Collaborative Research Writing Group. Effects of comprehensive lifestyle modification on blood pressure control. JAMA. 2003;289:2083-2093.
22. Cook NR, Cutler JA, Obarzanek E, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP). BMJ. 2007;334:885-888.
23. Dickinson BD, Havas S. Reducing the population burden of cardiovascular disease by reducing sodium intake. Arch Intern Med. 2007;167:1460-1468.
24. Li J, White J, Guo L, et al. Salt inactivates endothelial nitric oxide synthase in endothelial cells. J Nutr. 2009;139:1-5.
25. Beevers G, Lip G, O’Brien E. ABCs of hypertension: the pathophysiology of hypertension. BMJ. 2001;322:912-916.
26. Peppard PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378-1384.
27. Sowers JR, Whaley-Connell A, Epstein M. Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med. 2009;150:776-783.
28. Young T, Peppard P, Palta M, et al. Population-based study of sleep-disordered breathing as a risk factor for hypertension. Arch Intern Med. 1997;157:1746-1752.
29. Haentjens P, Van Meerhaeghe A, Moscariello A. The impact of continuous positive airway pressure on blood pressure in patients with obstructive sleep apnea syndrome: evidence from a meta-analysis of placebo-controlled randomized trials. Arch Intern Med. 2007;167:757-764.
30. Kawashima A, Francis IR, Baumgarten DA, et al. For the Expert Panel on Urologic Imaging. Renovascular hypertension. Reston, Va: American College of Radiology; 2007. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=11590&nbr=6003. Accessed April 4, 2009.
1. Chobanian A, Bakris GL, Black HR, et al. Seventh Report of The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7). Hypertension. 2003;42:1206-1252.
2. Fields L, Burt V, Cutler J, et al. The burden of adult hypertension in the United States 1999-2000: A rising tide. Hypertension. 2004;44:1-7.
3. Fang J, Alderman MH, Keenan NL, et al. Hypertension control at physicians’ offices in the United States. Am J Hypertens. 2008;21:136-142.
4. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics–2007 update. Circulation. 2007;115:e69-e171.
5. Sarafidis PA, Bakris GL. Resistant hypertension: an overview of evaluation and treatment. J Am Coll Cardiol. 2008;52:1749-1757.
6. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403-1419.
7. Phillips LS, Branch WT, Book CB, et al. Clinical inertia. Ann Intern Med. 2001;135:825-834.
8. Van Wijk BL, Klungel OH, Heerdink ER, et al. Rate and determinants of 10-year persistence with antihypertensive drugs. J Hypertens. 2005;23:2101-2107.
9. Wexler R, Pleister A, Feldman D. Sociology meets genetics: sociogenetic implications for future management of hypertension and heart failure. Curr Treat Options Cardiovasc Med. 2009;11:305-315.
10. Ogedegbe G, Pickering TG, Clemow L, et al. The misdiagnosis of hypertension: the role of patient anxiety. Arch Intern Med. 2008;168:2459-2465.
11. Dawes MG, Bartlett G, Coats AJ, et al. Comparing the effects of white coat hypertension and sustained hypertension on mortality in a UK primary care setting. Ann Fam Med. 2008;6:390-396.
12. Pierdomenico SD, Lapenna D, Bucci A, et al. Cardiovascular outcome in treated hypertensive patients with responder, masked, false resistant, and true resistant hypertension. Am J Hypertens. 2005;18:1422-1428.
13. Verberk WJ, Kroon AA, Kessels AGH, et al. Home blood pressure monitoring: a systematic review. J Am Coll Cardiol. 2005;46:743-751.
14. Pickering TG, Miller NH, Ogedegbe G, et al. AHA/ASH/PCNA scientific statement. Call to action on use and reimbursement for home blood pressure monitoring. Hypertension. 2008;52:10-29.
15. O’Brien E. Ambulatory blood pressure measurement: the case for implementation in primary care. Hypertension. 2008;51:1435-1441.
16. O’Brien E, Asmar R, Beilin L, et al. On behalf of the European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension recommendations for conventional ambulatory and home blood pressure measurements. J Hypertens. 2003;21:821-848.
17. Mourad A, Carney S, Gillies A, et al. Arm position and blood pressure: a risk factor for hypertension. J Hum Hypertens. 2003;17:389-395.
18. Myers MG. Automated blood pressure measurement in routine clinical practice. Blood Press Monit. 2006;11:59-62.
19. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce white coat hypertension. J Hypertens. 2009;27:280-286.
20. He J, Paul J, Whelton P, Appel L, et al. Long-term effects of weight loss and dietary sodium reduction on incidence of hypertension. Hypertension. 2000;35:544-549.
21. PREMIER Collaborative Research Writing Group. Effects of comprehensive lifestyle modification on blood pressure control. JAMA. 2003;289:2083-2093.
22. Cook NR, Cutler JA, Obarzanek E, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP). BMJ. 2007;334:885-888.
23. Dickinson BD, Havas S. Reducing the population burden of cardiovascular disease by reducing sodium intake. Arch Intern Med. 2007;167:1460-1468.
24. Li J, White J, Guo L, et al. Salt inactivates endothelial nitric oxide synthase in endothelial cells. J Nutr. 2009;139:1-5.
25. Beevers G, Lip G, O’Brien E. ABCs of hypertension: the pathophysiology of hypertension. BMJ. 2001;322:912-916.
26. Peppard PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378-1384.
27. Sowers JR, Whaley-Connell A, Epstein M. Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med. 2009;150:776-783.
28. Young T, Peppard P, Palta M, et al. Population-based study of sleep-disordered breathing as a risk factor for hypertension. Arch Intern Med. 1997;157:1746-1752.
29. Haentjens P, Van Meerhaeghe A, Moscariello A. The impact of continuous positive airway pressure on blood pressure in patients with obstructive sleep apnea syndrome: evidence from a meta-analysis of placebo-controlled randomized trials. Arch Intern Med. 2007;167:757-764.
30. Kawashima A, Francis IR, Baumgarten DA, et al. For the Expert Panel on Urologic Imaging. Renovascular hypertension. Reston, Va: American College of Radiology; 2007. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=11590&nbr=6003. Accessed April 4, 2009.