User login
Health care reform coverage: Spot on or missing key options?
“Health care reform: Possibilities & opportunities for primary care” (J Fam Pract. 2014;63:298-304) was terrific. You nailed the opportunities and challenges with implementing advanced primary care.
Joseph Scherger, MD
La Quinta, Calif
Your article focuses on so-called “value-based” care and Affordable Care Act (ACA) options and ignores other forms of free market health care, such as concierge and direct primary care, that are growing in popularity with physicians and patients. When patients shop for and pursue self-paid care, they are invested in the process, participate in their own care, and have better outcomes. The free market will bring many diverse options to the table, increase the quality of care, and decrease the price of care to stay competitive.
Physicians must step up for their individual patients and be health care leaders, not followers of government mandates and insurance company policies. Patients deserve nothing less than a free-market, competitive environment, and a variety of care and insurance options—not just a few, as dictated by the ACA.
Craig M. Wax, DO
Mullica Hill, NJ
Authors’ response:
We appreciate the comments of Drs. Scherger and Wax. We also agree that there is a move in some areas of the country toward direct primary care, as well as toward concierge medicine. However, it is our opinion that in their current form, these models are a symptom of today’s health care system and not a solution.
The vast majority of Americans cannot afford to pay directly for their care. And since health care is not a free market system, free market reforms are not likely to be the solution for most Americans. However, if concierge medicine or direct primary care could be part of a menu of options through existing insurance, government, or employer models, the potential negative impact (including the exacerbation of the current strained primary care system) could be ameliorated.
We agree that physicians should always advocate on behalf of their patients, but we also believe we should think of all patients and how policy changes may impact society as a whole.
Randy Wexler, MD, MPH
Jennifer Hefner, PhD, MPH
Mary Jo Welker, MD
Ann Scheck McAlearney, ScD, MS
Columbus, Ohio
“Health care reform: Possibilities & opportunities for primary care” (J Fam Pract. 2014;63:298-304) was terrific. You nailed the opportunities and challenges with implementing advanced primary care.
Joseph Scherger, MD
La Quinta, Calif
Your article focuses on so-called “value-based” care and Affordable Care Act (ACA) options and ignores other forms of free market health care, such as concierge and direct primary care, that are growing in popularity with physicians and patients. When patients shop for and pursue self-paid care, they are invested in the process, participate in their own care, and have better outcomes. The free market will bring many diverse options to the table, increase the quality of care, and decrease the price of care to stay competitive.
Physicians must step up for their individual patients and be health care leaders, not followers of government mandates and insurance company policies. Patients deserve nothing less than a free-market, competitive environment, and a variety of care and insurance options—not just a few, as dictated by the ACA.
Craig M. Wax, DO
Mullica Hill, NJ
Authors’ response:
We appreciate the comments of Drs. Scherger and Wax. We also agree that there is a move in some areas of the country toward direct primary care, as well as toward concierge medicine. However, it is our opinion that in their current form, these models are a symptom of today’s health care system and not a solution.
The vast majority of Americans cannot afford to pay directly for their care. And since health care is not a free market system, free market reforms are not likely to be the solution for most Americans. However, if concierge medicine or direct primary care could be part of a menu of options through existing insurance, government, or employer models, the potential negative impact (including the exacerbation of the current strained primary care system) could be ameliorated.
We agree that physicians should always advocate on behalf of their patients, but we also believe we should think of all patients and how policy changes may impact society as a whole.
Randy Wexler, MD, MPH
Jennifer Hefner, PhD, MPH
Mary Jo Welker, MD
Ann Scheck McAlearney, ScD, MS
Columbus, Ohio
“Health care reform: Possibilities & opportunities for primary care” (J Fam Pract. 2014;63:298-304) was terrific. You nailed the opportunities and challenges with implementing advanced primary care.
Joseph Scherger, MD
La Quinta, Calif
Your article focuses on so-called “value-based” care and Affordable Care Act (ACA) options and ignores other forms of free market health care, such as concierge and direct primary care, that are growing in popularity with physicians and patients. When patients shop for and pursue self-paid care, they are invested in the process, participate in their own care, and have better outcomes. The free market will bring many diverse options to the table, increase the quality of care, and decrease the price of care to stay competitive.
Physicians must step up for their individual patients and be health care leaders, not followers of government mandates and insurance company policies. Patients deserve nothing less than a free-market, competitive environment, and a variety of care and insurance options—not just a few, as dictated by the ACA.
Craig M. Wax, DO
Mullica Hill, NJ
Authors’ response:
We appreciate the comments of Drs. Scherger and Wax. We also agree that there is a move in some areas of the country toward direct primary care, as well as toward concierge medicine. However, it is our opinion that in their current form, these models are a symptom of today’s health care system and not a solution.
The vast majority of Americans cannot afford to pay directly for their care. And since health care is not a free market system, free market reforms are not likely to be the solution for most Americans. However, if concierge medicine or direct primary care could be part of a menu of options through existing insurance, government, or employer models, the potential negative impact (including the exacerbation of the current strained primary care system) could be ameliorated.
We agree that physicians should always advocate on behalf of their patients, but we also believe we should think of all patients and how policy changes may impact society as a whole.
Randy Wexler, MD, MPH
Jennifer Hefner, PhD, MPH
Mary Jo Welker, MD
Ann Scheck McAlearney, ScD, MS
Columbus, Ohio
Health care reform: Possibilities & opportunities for primary care
Pressure to reform our health care system is at an all-time high, driven by relentlessly rising costs and fragmentation of care. These persistent problems have led to lower quality care and limited access to care for a large proportion of the US population—issues that accountable care organizations (ACOs), as well as other value-based models, are designed to address.
While the terms used to describe the means by which health care systems attempt to do more to meet the needs of those they serve may vary, the importance of reorganizing care delivery to better integrate services is gaining traction nationwide. As we move to new models, primary care takes center stage.
ACOs (or ACO-type arrangements) anchored by primary care networks can help meet the goals of health care reform by responding to changes in reimbursement, reducing fragmented care, and focusing on improving the quality of care for defined patient populations. In addition, these delivery models can take advantage of new health information technology (IT) and the move toward patient-centered medical homes (PCMHs).
In the pages that follow, we examine opportunities for new care delivery models to slow rising costs and improve population health in family medicine. The introduction of these models has important implications for patients, physicians, and provider organizations, and our aim is to ensure that family physicians are prepared to take these vital steps toward achieving health reform goals.
Shifting from volume-based to value-based reimbursement
According to the Congressional Budget Office, ACOs are expected to save $5 billion during their first 8 years of existence.1 After one year of ACO activity, the Centers for Medicare and Medicaid Services (CMS) reported savings of $30 million.2 The expected savings will be driven by the increased provider accountability associated with ACOs.
Various means of increasing provider accountability through changes in reimbursement strategies have been proposed; several are new, while others are improvements on—or variations of—methods that have been tried before. The most common approaches—shared savings, shared savings plus penalty, capitation, episodic payment, prospective payment, pay-for-performance, and hospital-physician bundling—are detailed in TABLE 1.3-7 Broad implementation of any of these reimbursement mechanisms within a new model of care would represent a shift away from the traditional volume-based provider payment model to a value-based system—a key step in slowing the rise in health care costs.
TABLE 1
Reimbursement strategies designed to promote physician accountability3-7
Model | Description | Implications for FPs |
Shared savings | FFS plus a portion of dollars saved relative to predicted costs if quality and patient satisfaction are enhanced3 | Focus on population health incentivizes well care and preventive services |
Shared savings plus penalty | Same as shared savings, plus a penalty if expenses exceed spending targets; bonus potential is increased to account for increased risk3 | Potential for care coordination payments in addition to shared savings |
Capitation | Flat payments plus bonuses and penalties; provider organization assumes full risk for a defined patient population3 | A better understanding of population management and IT now makes capitation a viable strategy in certain settings |
Episodic payments | Reimbursement is for defined episodes of care, which may extend from time of admission to days or weeks after discharge; may also include home health, extended care, or ancillary services4 | No incentive for prevention or PCMH coordination |
Prospective payment | Reimbursement for inpatient services based on a prepaid amount that covers a defined period of time; uses DRG system that bases payment on disease classification by CMS5 | It is important for FPs to partner with specialists willing to share reimbursement commensurate with the value of care provided |
Pay-for-performance | Reimbursement is tied to achievement of metrics (eg, number of patients immunized for a specific disease, desired clinical outcomes, high patient satisfaction scores) mutually agreed upon by ACO and payer6 | Be sure any agreed-upon “targets” are achievable and patient-focused |
Hospital-physician bundling | Reimbursement is based on the cost of a procedure or diagnosis that includes both hospital and physician components. One payment is made for the collective services associated with a hospitalization7 | Similar to prospective payment from FP perspective; it is important to work with those who value the care of FPs |
ACO, accountable care organization; CMS, Centers for Medicare and Medicaid Services; DRG, diagnosis-related group; FFS, fee-for-service; FPs, family physicians; IT, information technology; PCMH, patient-centered medical home.
Although it is too soon to be certain of the effect such changes will have on the earnings of family physicians, it is reasonable to think that new payment strategies—and a larger role for primary care providers—will improve their financial standing.
Moving toward population health management
New ACO-type models also make it easier to improve health care for specific populations, using strategies designed to organize, provide, and manage care for defined groups. In addition to controlling the cost of caring for specific groups, well-designed and implemented population health management strategies can increase continuity of care by ensuring oversight of patients across the spectrum of health care settings.
Five broad categories of population health management are most prominent: lifestyle management and demand management (both for relatively healthy people), disease management (for those with chronic conditions), catastrophic care management (for patients with rare or catastrophic illness or injury), and disability management (for groups of employees).8TABLE 28 describes the population targeted and activities associated with each. It is important to remember, however, that no single strategy is mutually exclusive for a particular group.
Comprehensive Primary Care (CPC) initiative. In a collaboration made possible by the Affordable Care Act, CMS initiated the CPC initiative in 2012.9 A 4-year project designed to test and further identify the benefits of population health management and strengthen coordination of care for Medicare patients within primary care settings, the CPC initiative involves 497 sites and 2347 providers caring for approximately 315,000 Medicare beneficiaries.9 More information is available at http://innovation.cms.gov/initiatives/comprehensive-primary-care-initiative/.
TABLE 2
Population health management strategies8
Strategy | Target/goal | Key elements | Evidence of effectiveness |
Lifestyle management | To help relatively healthy individuals make good choices about health behaviors and risks | • Prevention • Risk reduction • Self-care | • Adherence to guidelines for clinical screenings • Reduced costs resulting from prevention programs |
Demand management | To help relatively healthy individuals take an active role in decisions about health and medical care; aims to reduce inappropriate demand for services | • Telephone triage • Advice and referrals • Decision and behavioral support • Education to promote self-care | • Reduced variation in care unexplained by morbidity • Improved understanding of perceived need for care • Improved access, better outcomes, lower cost |
Disease management | To identify and target chronically ill patients (eg, those with diabetes, heart failure, or asthma) with specific interventions | • Clinical oversight/management of patients with chronic disease • Education and self-care • Coordination of care/providers | • Reduced costs for treatment of chronic diseases • Decreased complications associated with chronic illness |
Catastrophic care management | To identify those with rare or catastrophic illness or injury and provide services needed to improve outcomes | • Immediate referral to appropriate providers • Coordination of care • Medical/care management | • Reduced hospitalizations and total claims costs • Reduced morbidity; improved QOL • Realistic, patient-specific goals |
Disability management | To develop and deliver employer-driven initiatives for employees to reduce lost time from work, improve productivity, and optimize health and well-being | • Disability prevention programs • Return-to-work programs • Employer-based lifestyle management programs • Coordination of care/providers for employees with chronic disease, disability, and/or serious illness or injury • Absence management programs (ie, designed to control/limit unexplained, unscheduled, or excessive absenteeism) • Workplace rehabilitation | • Lower workers’ compensation/disability benefit costs • Reduced number of injuries • Reduced lost time from work • Increased productivity |
QOL, quality of life.
Building infrastructure and leveraging IT
ACOs and ACO-type models will take a variety of forms, depending in part on geographic need and local demographics. Yet, all share a common need for a strong infrastructure to support improved transitions, integration, and coordination of care. Incorporation of a strong health IT system is critical so that data regarding the process and cost of care, as well as outcomes, can be collected and put to optimal use.10-13
Across health care settings, health IT innovations are being successfully implemented in efforts to enhance physician decision support, improve patient safety, increase guideline adherence, and improve chronic disease treatment.11,13 In primary care, for example, an IT infrastructure can create disease registries so that data on patients with specific conditions can be tracked and acted upon—eg, a diabetes registry could be used to identify and contact patients who have an hemoglobin A1c >9 and have not been seen in 9 months or more.
Similarly, an IT system with the ability to identify patients at high risk for disease decompensation, hospitalization, and/or increased morbidity and mortality linked to progression of a chronic disease is needed. Identifying medical conditions associated with higher costs would make it possible to focus care coordination and chronic care management efforts on this targeted population.
As health IT continues to evolve, additional means of interacting with patients and improving patient care will be developed. Physicians and organizations that are ready to take advantage of these advances in technology will be well positioned to address the goals of health reform. (See “Health care reform: Recommendations for family physicians” below.3-7,14,15)
How the patient-centered medical home fits into the picture
The implementation of ACOs and other new models of care has promising implications for the establishment of PCMHs. Consistent with the goals of health reform, the PCMH movement focuses on a coordinated teamwork approach, anchored within a general practice or family medicine setting.
An evaluation of the PCMH National Demonstration Project funded by the American Academy of Family Physicians found that the adoption of more components of the PCMH at the practice level was associated with improvement in patient outcomes, as measured by the Ambulatory Care Quality Alliance starter set16 (a compilation of clinical performance measures developed by a broad coalition of providers, payers, consumers, and government agencies).
A recent look at the Southeastern Pennsylvania Chronic Care Initiative17 found less promising results. “A multipayer medical home pilot, in which participating practices adopted new structural capabilities and received NCQA [National Committee for Quality Assurance] certification, was associated with limited improvements in quality and was not associated with reductions in utilization of hospital, emergency department, or ambulatory care services or total costs over 3 years,” Friedberg et al17 concluded. The authors did note, however, that NCQA recognition was what the practices involved in this initiative were rewarded for—not PCMH activity.
It is also important to keep in mind that PCMH activity has been shown to improve care and reduce costs—not NCQA recognition in and of itself. In fact, a large body of evidence clearly demonstrates the positive patient care outcomes and reductions in overall cost associated with the PCMH. These findings were compiled by the Patient-Centered Primary Care Collaborative—which issues annual reports on the progress of the PCMH—in a January 2014 update.18
In a PCMH model, the focus shifts away from the procedure(s) or treatment to the whole person. However, all components of care (eg, primary and specialty care, hospital, ancillary services, laboratory, and radiology) are vital and need to be connected to increase efficiency and reduce cost—creating what is sometimes referred to as a “medical neighborhood.”19-21
What’s in the neighborhood?
In a medical neighborhood, such as an ACO, each patient is cared for by a team of providers at multiple locations. The PCMH serves as the base, ensuring that all providers work together toward a common goal. In addition to providing primary care, the PCMH coordinates each patient’s specialty and support services and communicates the care plan to all involved.
Successful implementation of a medical neighborhood requires a close working relationship among providers, payers, and community resources. For example, payers can provide real-time information about patients who have been admitted to the hospital or discharged from the emergency department, which enables close follow-up and coordination across multiple systems.
Given the emerging opportunities for new care delivery models to advance primary care, we urge family physicians to respond positively to these changes and challenges. Here’s what we recommend:
Carefully consider payment methodologies. Changes in the way physicians are paid will vary by payer source, as well as geographic market.3-7 Regardless of the reimbursement model you’re offered, however, do not agree to it until you have the opportunity to evaluate it, along with your particular circumstances, to ensure that you have the infrastructure to support whatever changes the new model will require.
Read the fine print. Look out for your own interests by carefully reading the terms you are presented with. Consider seeking advice from those who understand the particular nuances faced by family physicians under particular reimbursement strategies. Just because a payment method benefits a particular specialty does not mean it will be favorable to family physicians.
Before you join an ACO
Before joining an accountable care organization (ACO ) or a similar entity, find out whether it supports primary care principles and the patient-centered medical home (PCMH ). Some questions to ask:
• Does the ACO have the infrastructure necessary to be successful, including the requisite health information technology, administrative support, actuarial knowledge, and experience with population health management?
• Is the ACO founded on primary care principles? Find out, for example, whether primary care physicians are represented at all levels of the organization and provide appropriate input on all important issues.
If you practice in a rural area … The growth of ACO activity is expected to be slow in both rural and underserved metropolitan markets. To address this issue, the Centers for Medicare and Medicaid Services is allowing primary care physicians in such markets to participate in more than one Medicare ACO and providing financial incentives in the form of savings exemptions to smaller, rural ACOs.14,15 Another option for rural providers is the adoption of a “virtual ACO ”—a loosely organized group of providers, united in the effort to achieve high-quality care and reduced costs and willing to submit to computer analysis that will determine their relative contributions to efficiency and the distribution of savings.14
Get involved
It is important for all family physicians to engage in discussions about health care reform, and to represent both their patients and their specialty. Familiarity with what is happening is essential. One way to do that is to become an active member of your state or local American Academy of Family Physicians affiliate.
More information is available at:
• www.aafp.org
Practical information with regard to health reform, in addition to suggesting ways to get involved
• http://www.tafp.org/Media/Default/Downloads/practice%20resources/aco-guide.pdf
Information to consider before joining or forming an ACO
• http://www.ncqa.org/Programs/Recognition/PatientCenteredMedicalHomePCMH.aspx and http://www.transformed.com/
Resources for practitioners considering transformation to a PCMH
• http://innovation.cms.gov
Information, including webinars and forums, on innovative payment and service delivery models.
Nontraditional settings. Another facet of the medical neighborhood is the provision of health care services in nontraditional settings. For example, some grocery stores in our area employ nutritionists to whom we refer patients for nutritional counseling regarding their health in general or a disease process in particular.
Changes in reimbursement also will affect how care is delivered within the medical neighborhood. As we move away from fee-for-service (volume-based) to value-based payments, physicians who have made the transition from working individually with a panel of patients to providing team-based care within a PCMH will be better positioned to meet the goals of health care reform. (See “Team-based care is key inside the PCMH, too”22 below.) Nonetheless, the transition is a dynamic process. With changes in reimbursement and delivery models, physicians also will be expected to develop and implement continuous quality improvement measures so patient care can be continually evaluated and improved.
Now comes the hard part
While a PCMH requires primary care physicians to collaborate with other health professionals, it has the potential to lead to conflicts and debates about who is at the head of the health care team. This is particularly true within mental health services because, while primary care visits are frequently related to psychosocial issues, the mental health and general practice sectors have traditionally been distinct. In recent years, however, coordinated delivery models that integrate primary care and mental health services have been shown to increase access and reduce the stigma associated with mental health services—and to be cost-effective.23
In many ways, moving the primary care culture from the traditional focus on the physician as “captain of the ship” to a physician-led, team-based approach is one of the most difficult tasks for organizations attempting to transform their care delivery models.3,24 Physicians historically have been autonomous providers of medical care, relying on their own experience, expertise, and beliefs to guide decisions about patient care. Now they’re being asked to give up some of the direct control they may have had over patient care decisions and learn to work more collaboratively with other providers, as well as nonclinicians (eg, health coaches), to achieve desired outcomes.3 A successful transition depends on a reimbursement framework in which patient care goals are properly aligned with incentives for primary care physicians to work in a team-based environment.3,25-27
In addition to operating as a team with providers in other settings in the medical neighborhood, innovative primary care practices—typically those that have already achieved patient-centered medical home (PCMH ) status—have strong teams within their walls. In “In search of joy in practice: A report of 23 high-functioning primary care practices,” Sinsky et al22 highlight a number of ways in which the practices they studied are maximizing this approach.
Nonphysician care. A number of practices expanded the roles of medical assistants (MAs), nurses, and even nonclinician health coaches. In one case, MAs nearly tripled the time they spend with each patient, to enable them to do medication review, fill out forms, give immunizations, and book appointments for screening tests such as mammography. In another, registered nurses were given standing orders to treat routine problems such as ear infections and urinary tract infections; at a third, health coaches counsel patients with chronic conditions and MAs conduct depression screening, as needed.
Documentation and computerized order entry—which ties up many hours of physician time—is another area in which some practices have adopted a team approach. A number of practices use nurses or MAs as scribes, entering orders and preparing after-visit summaries, for example. Not only are the physicians more satisfied, but the MAs and nurses are happy to have more involvement in patient care, the researchers report.
Communication is crucial to a successful team approach. In some practices, this is accomplished with weekly physician-clinical staff meetings; in others, with brief group “huddles” or by an office design featuring “co-location.” In one example of the latter, MAs and physicians sit side-by-side, so they can easily talk to each other—the doctor could communicate key patient information that the MA would then follow up on, for example. Regular analysis of workflow to identify and address undue delays is an effective team function, as well.
Helping patients help themselves. Moving toward more patient-focused care will also require a concerted effort to increase patients’ engagement in their own health and medical care. In practice, very little of an individual’s time is spent in a physician’s office. Thus, optimal outcomes can be achieved only when patients are actively involved. Helping patients become proactive—ie, by arming them with the knowledge, skill, and confidence to do their part in staying healthy28—also represents a major shift in primary care culture, as patients become active participants in medical decision making rather than passive recipients of physicians’ advice.
Alternative approaches. To deliver the continuum of care that is central to new care delivery models and shift the culture of primary care toward a PCMH, physicians can implement a number of clinic-based engagement approaches—interacting with patients via e-visits such as e-mail through a secure portal, telemedicine, and group medical visits, for example. Physicians can encourage patient participation by starting patient interest groups and advisory panels29—recommended by the NCQA and the Agency for Healthcare Research and Quality and used at our institution—and conducting patient needs assessments on a regular basis. Opportunities for primary care practices to engage with the community include partnering with local health departments, churches, nonprofits, and advocacy organizations to conduct health promotion and educational activities.
CORRESPONDENCE
Randy Wexler, MD, MPH, Department of Family Medicine, College of Medicine, The Ohio State University, 2231 North High Street, Northwood and High Building, Columbus, OH 43201; randy.wexler@osumc.edu
1. Shortell SM, Casalino LP, Fisher ES. How the Center for Medicare and Medicaid Innovation should test accountable care organizations. Health Aff. 2010;29:1293-1298.
2. Medicare’s delivery system reform initiatives achieve significant savings and quality improvements - off to a strong start [press release]. Washington, DC: US Department of Health & Human Services; January 30, 2014. Available at: http://www.hhs.gov/news/press/2014pres/01/20140130a.html. Accessed March 28, 2014.
3. The family physician’s ACO blueprint for success: Preparing family medicine for the approaching accountable care era. Texas Academy of Family Physicians Web site. Available at: http://www.tafp.org/Media/Default/Downloads/practice%20resources/acoguide.pdf. Accessed March 28, 2014.
4. Mechanic RE. Opportunities and challenges for episode-based payment. N Engl J Med. 2011;365:777-779.
5. Medicare prospective payment systems (PPS): A summary. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/practice/reimbursement/medicare/pps_sum.htm. Accessed March 28, 2014.
6. Pay for performance (P4P): AHRQ resources. Agency for Healthcare Research and Quality Web site. Available at: http://www.ahrq.gov/legacy/qual/pay4per.htm. Accessed March 29, 2014.
7. Komisar H, Feder J, Ginsburg PB. “Bundling” payment for episodes of hospital care: Issues and recommendations for the new pilot program in Medicare. Available at: http://www.americanprogress.org/issues/2011/07/pdf/medicare_bundling.pdf. Accessed May 20, 2014.
8. McAlearney AS. Population health management: Strategies to improve outcomes. Chicago, IL: Health Administration Press; 2003.
9. Centers for Medicare and Medicaid Services Web site. Comprehensive primary care initiative. Available at: http://innovation.cms.gov/initiatives/comprehensive-primary-care-initiative/. Accessed March 29, 2014.
10. Robertson DC, Lerner JC. Top technology issues for ambulatory care facilities this year and beyond. J Ambul Care Manag. 2009;32:303-319.
11. Linder JA, Ma J, Bates DW, et al. Electronic health record use and the quality of ambulatory care in the united states. Arch Intern Med. 2007;167:1400-1405.
12. Vest JR. Health information exchange and healthcare utilization. J Med Syst. 2009;33:223-231.
13. Parente ST, McCullough JS. Health information technology and patient safety: evidence from panel data. Health Affairs (Millwood). 2009;28:357-360.
14. FAQ on Accountable Care Organizations. American Academy of Family Physicians Web site. Available at: http://www.aafp.org/practice-management/payment/acos/faq.html. Accessed March 29, 2014.
15. Torrieri M. CMS appeals to rural practices with another ACO participation perk. Physicians Practice blog. June 1, 2011. Available at: http://www.physicianspractice.com/blog/cms-appealsrural-practices-another-aco-participation-perk. Accessed March 29, 2014.
16. Crabtree BF, Nutting PA, Miller WL, et al. Summary of the national demonstration project and recommendations for the patient-centered medical home. Ann Fam Med. 2010;8 suppl 1:S80-S92.
17. Friedberg MW, Schneider EC, Rosenthal MB, et al. Association between participation in a multipayer medical home intervention and changes in quality, utilization, and costs of care. JAMA. 2014;311:815-825.
18. Nielsen M, Olayiwola JN, Grundy P, et al. The patient-centered medical home’s impact on cost & quality: An annual update of the evidence, 2012-2013. Available at: http://www.pcpcc.org/resource/medical-homes-impact-cost-quality. Accessed May 20, 2014.
19. Laine C. Welcome to the patient-centered medical neighborhood. Ann Intern Med. 2011;154:60.
20. Pham HH. Good neighbors: how will the patient-centered medical home relate to the rest of the health-care delivery system? J Gen Intern Med. 2010;25:630-634.
21. Taylor EF, Lake T, Nysenbaum J, et al; Mathematica Policy Research. Coordinating care in the medical neighborhood: critical components and available mechanisms: White paper. Available at: http://pcmh.ahrq.gov/sites/default/files/attachments/Coordinating%20Care%20in%20the%20Medical%20Neighborhood.pdf. Accessed May 20, 2014.
22. Sinsky CA, Willard-Grace R, Schutzbank AM, et al. In search of joy in practice: a report of 23 high-functioning primary care practices. Ann Fam Med. 2013;11:272-278.
23. Collins C, Hewson DL, Munger R, et al. Evolving models of behavioral health integration in primary care. Available at: http://www.milbank.org/uploads/documents/10430EvolvingCare/EvolvingCare.pdf. Accessed April 10, 2014.
24. The cornerstones of accountable care. Health Leaders Media Web site. Available at: http://www.healthleadersmedia.com/content/256694.pdf. Accessed March 29, 2014.
25. AAFP statement: AAFP commends CMS for improving Medicare ACO final rule, announcing the advance payment model [press release]. Leawood, Kansas: American Academy of Family Physicians; October 21, 2011. Available at: http://www.aafp.org/media-center/releases-statements/all/2011/aco-final-rule.html. Accessed March 29, 2014.
26. Fisher ES, Staiger DO, Bynum JP, et al. Creating accountable care organizations: the extended hospital medical staff. Health Affairs (Millwood). 2007;26:w44-w57.
27. Shields MC, Patel PH, Manning M, et al. A model for integrating independent physicians into accountable care organizations. Health Affairs (Millwood). 2011;30:161-172.
28. Hibbard JH. Patient engagement in accountable care organizations. Webinar. 2008. https://acoregister.rti.org/display_docs7.cfm. Accessed April 11, 2014.
29. Developing a community-based patient safety advisory council. Agency for Healthcare Research and Quality Web site. Available at: http://www.ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/resources/patient-safety-advisorycouncil/. Accessed March 31, 2014.
Pressure to reform our health care system is at an all-time high, driven by relentlessly rising costs and fragmentation of care. These persistent problems have led to lower quality care and limited access to care for a large proportion of the US population—issues that accountable care organizations (ACOs), as well as other value-based models, are designed to address.
While the terms used to describe the means by which health care systems attempt to do more to meet the needs of those they serve may vary, the importance of reorganizing care delivery to better integrate services is gaining traction nationwide. As we move to new models, primary care takes center stage.
ACOs (or ACO-type arrangements) anchored by primary care networks can help meet the goals of health care reform by responding to changes in reimbursement, reducing fragmented care, and focusing on improving the quality of care for defined patient populations. In addition, these delivery models can take advantage of new health information technology (IT) and the move toward patient-centered medical homes (PCMHs).
In the pages that follow, we examine opportunities for new care delivery models to slow rising costs and improve population health in family medicine. The introduction of these models has important implications for patients, physicians, and provider organizations, and our aim is to ensure that family physicians are prepared to take these vital steps toward achieving health reform goals.
Shifting from volume-based to value-based reimbursement
According to the Congressional Budget Office, ACOs are expected to save $5 billion during their first 8 years of existence.1 After one year of ACO activity, the Centers for Medicare and Medicaid Services (CMS) reported savings of $30 million.2 The expected savings will be driven by the increased provider accountability associated with ACOs.
Various means of increasing provider accountability through changes in reimbursement strategies have been proposed; several are new, while others are improvements on—or variations of—methods that have been tried before. The most common approaches—shared savings, shared savings plus penalty, capitation, episodic payment, prospective payment, pay-for-performance, and hospital-physician bundling—are detailed in TABLE 1.3-7 Broad implementation of any of these reimbursement mechanisms within a new model of care would represent a shift away from the traditional volume-based provider payment model to a value-based system—a key step in slowing the rise in health care costs.
TABLE 1
Reimbursement strategies designed to promote physician accountability3-7
Model | Description | Implications for FPs |
Shared savings | FFS plus a portion of dollars saved relative to predicted costs if quality and patient satisfaction are enhanced3 | Focus on population health incentivizes well care and preventive services |
Shared savings plus penalty | Same as shared savings, plus a penalty if expenses exceed spending targets; bonus potential is increased to account for increased risk3 | Potential for care coordination payments in addition to shared savings |
Capitation | Flat payments plus bonuses and penalties; provider organization assumes full risk for a defined patient population3 | A better understanding of population management and IT now makes capitation a viable strategy in certain settings |
Episodic payments | Reimbursement is for defined episodes of care, which may extend from time of admission to days or weeks after discharge; may also include home health, extended care, or ancillary services4 | No incentive for prevention or PCMH coordination |
Prospective payment | Reimbursement for inpatient services based on a prepaid amount that covers a defined period of time; uses DRG system that bases payment on disease classification by CMS5 | It is important for FPs to partner with specialists willing to share reimbursement commensurate with the value of care provided |
Pay-for-performance | Reimbursement is tied to achievement of metrics (eg, number of patients immunized for a specific disease, desired clinical outcomes, high patient satisfaction scores) mutually agreed upon by ACO and payer6 | Be sure any agreed-upon “targets” are achievable and patient-focused |
Hospital-physician bundling | Reimbursement is based on the cost of a procedure or diagnosis that includes both hospital and physician components. One payment is made for the collective services associated with a hospitalization7 | Similar to prospective payment from FP perspective; it is important to work with those who value the care of FPs |
ACO, accountable care organization; CMS, Centers for Medicare and Medicaid Services; DRG, diagnosis-related group; FFS, fee-for-service; FPs, family physicians; IT, information technology; PCMH, patient-centered medical home.
Although it is too soon to be certain of the effect such changes will have on the earnings of family physicians, it is reasonable to think that new payment strategies—and a larger role for primary care providers—will improve their financial standing.
Moving toward population health management
New ACO-type models also make it easier to improve health care for specific populations, using strategies designed to organize, provide, and manage care for defined groups. In addition to controlling the cost of caring for specific groups, well-designed and implemented population health management strategies can increase continuity of care by ensuring oversight of patients across the spectrum of health care settings.
Five broad categories of population health management are most prominent: lifestyle management and demand management (both for relatively healthy people), disease management (for those with chronic conditions), catastrophic care management (for patients with rare or catastrophic illness or injury), and disability management (for groups of employees).8TABLE 28 describes the population targeted and activities associated with each. It is important to remember, however, that no single strategy is mutually exclusive for a particular group.
Comprehensive Primary Care (CPC) initiative. In a collaboration made possible by the Affordable Care Act, CMS initiated the CPC initiative in 2012.9 A 4-year project designed to test and further identify the benefits of population health management and strengthen coordination of care for Medicare patients within primary care settings, the CPC initiative involves 497 sites and 2347 providers caring for approximately 315,000 Medicare beneficiaries.9 More information is available at http://innovation.cms.gov/initiatives/comprehensive-primary-care-initiative/.
TABLE 2
Population health management strategies8
Strategy | Target/goal | Key elements | Evidence of effectiveness |
Lifestyle management | To help relatively healthy individuals make good choices about health behaviors and risks | • Prevention • Risk reduction • Self-care | • Adherence to guidelines for clinical screenings • Reduced costs resulting from prevention programs |
Demand management | To help relatively healthy individuals take an active role in decisions about health and medical care; aims to reduce inappropriate demand for services | • Telephone triage • Advice and referrals • Decision and behavioral support • Education to promote self-care | • Reduced variation in care unexplained by morbidity • Improved understanding of perceived need for care • Improved access, better outcomes, lower cost |
Disease management | To identify and target chronically ill patients (eg, those with diabetes, heart failure, or asthma) with specific interventions | • Clinical oversight/management of patients with chronic disease • Education and self-care • Coordination of care/providers | • Reduced costs for treatment of chronic diseases • Decreased complications associated with chronic illness |
Catastrophic care management | To identify those with rare or catastrophic illness or injury and provide services needed to improve outcomes | • Immediate referral to appropriate providers • Coordination of care • Medical/care management | • Reduced hospitalizations and total claims costs • Reduced morbidity; improved QOL • Realistic, patient-specific goals |
Disability management | To develop and deliver employer-driven initiatives for employees to reduce lost time from work, improve productivity, and optimize health and well-being | • Disability prevention programs • Return-to-work programs • Employer-based lifestyle management programs • Coordination of care/providers for employees with chronic disease, disability, and/or serious illness or injury • Absence management programs (ie, designed to control/limit unexplained, unscheduled, or excessive absenteeism) • Workplace rehabilitation | • Lower workers’ compensation/disability benefit costs • Reduced number of injuries • Reduced lost time from work • Increased productivity |
QOL, quality of life.
Building infrastructure and leveraging IT
ACOs and ACO-type models will take a variety of forms, depending in part on geographic need and local demographics. Yet, all share a common need for a strong infrastructure to support improved transitions, integration, and coordination of care. Incorporation of a strong health IT system is critical so that data regarding the process and cost of care, as well as outcomes, can be collected and put to optimal use.10-13
Across health care settings, health IT innovations are being successfully implemented in efforts to enhance physician decision support, improve patient safety, increase guideline adherence, and improve chronic disease treatment.11,13 In primary care, for example, an IT infrastructure can create disease registries so that data on patients with specific conditions can be tracked and acted upon—eg, a diabetes registry could be used to identify and contact patients who have an hemoglobin A1c >9 and have not been seen in 9 months or more.
Similarly, an IT system with the ability to identify patients at high risk for disease decompensation, hospitalization, and/or increased morbidity and mortality linked to progression of a chronic disease is needed. Identifying medical conditions associated with higher costs would make it possible to focus care coordination and chronic care management efforts on this targeted population.
As health IT continues to evolve, additional means of interacting with patients and improving patient care will be developed. Physicians and organizations that are ready to take advantage of these advances in technology will be well positioned to address the goals of health reform. (See “Health care reform: Recommendations for family physicians” below.3-7,14,15)
How the patient-centered medical home fits into the picture
The implementation of ACOs and other new models of care has promising implications for the establishment of PCMHs. Consistent with the goals of health reform, the PCMH movement focuses on a coordinated teamwork approach, anchored within a general practice or family medicine setting.
An evaluation of the PCMH National Demonstration Project funded by the American Academy of Family Physicians found that the adoption of more components of the PCMH at the practice level was associated with improvement in patient outcomes, as measured by the Ambulatory Care Quality Alliance starter set16 (a compilation of clinical performance measures developed by a broad coalition of providers, payers, consumers, and government agencies).
A recent look at the Southeastern Pennsylvania Chronic Care Initiative17 found less promising results. “A multipayer medical home pilot, in which participating practices adopted new structural capabilities and received NCQA [National Committee for Quality Assurance] certification, was associated with limited improvements in quality and was not associated with reductions in utilization of hospital, emergency department, or ambulatory care services or total costs over 3 years,” Friedberg et al17 concluded. The authors did note, however, that NCQA recognition was what the practices involved in this initiative were rewarded for—not PCMH activity.
It is also important to keep in mind that PCMH activity has been shown to improve care and reduce costs—not NCQA recognition in and of itself. In fact, a large body of evidence clearly demonstrates the positive patient care outcomes and reductions in overall cost associated with the PCMH. These findings were compiled by the Patient-Centered Primary Care Collaborative—which issues annual reports on the progress of the PCMH—in a January 2014 update.18
In a PCMH model, the focus shifts away from the procedure(s) or treatment to the whole person. However, all components of care (eg, primary and specialty care, hospital, ancillary services, laboratory, and radiology) are vital and need to be connected to increase efficiency and reduce cost—creating what is sometimes referred to as a “medical neighborhood.”19-21
What’s in the neighborhood?
In a medical neighborhood, such as an ACO, each patient is cared for by a team of providers at multiple locations. The PCMH serves as the base, ensuring that all providers work together toward a common goal. In addition to providing primary care, the PCMH coordinates each patient’s specialty and support services and communicates the care plan to all involved.
Successful implementation of a medical neighborhood requires a close working relationship among providers, payers, and community resources. For example, payers can provide real-time information about patients who have been admitted to the hospital or discharged from the emergency department, which enables close follow-up and coordination across multiple systems.
Given the emerging opportunities for new care delivery models to advance primary care, we urge family physicians to respond positively to these changes and challenges. Here’s what we recommend:
Carefully consider payment methodologies. Changes in the way physicians are paid will vary by payer source, as well as geographic market.3-7 Regardless of the reimbursement model you’re offered, however, do not agree to it until you have the opportunity to evaluate it, along with your particular circumstances, to ensure that you have the infrastructure to support whatever changes the new model will require.
Read the fine print. Look out for your own interests by carefully reading the terms you are presented with. Consider seeking advice from those who understand the particular nuances faced by family physicians under particular reimbursement strategies. Just because a payment method benefits a particular specialty does not mean it will be favorable to family physicians.
Before you join an ACO
Before joining an accountable care organization (ACO ) or a similar entity, find out whether it supports primary care principles and the patient-centered medical home (PCMH ). Some questions to ask:
• Does the ACO have the infrastructure necessary to be successful, including the requisite health information technology, administrative support, actuarial knowledge, and experience with population health management?
• Is the ACO founded on primary care principles? Find out, for example, whether primary care physicians are represented at all levels of the organization and provide appropriate input on all important issues.
If you practice in a rural area … The growth of ACO activity is expected to be slow in both rural and underserved metropolitan markets. To address this issue, the Centers for Medicare and Medicaid Services is allowing primary care physicians in such markets to participate in more than one Medicare ACO and providing financial incentives in the form of savings exemptions to smaller, rural ACOs.14,15 Another option for rural providers is the adoption of a “virtual ACO ”—a loosely organized group of providers, united in the effort to achieve high-quality care and reduced costs and willing to submit to computer analysis that will determine their relative contributions to efficiency and the distribution of savings.14
Get involved
It is important for all family physicians to engage in discussions about health care reform, and to represent both their patients and their specialty. Familiarity with what is happening is essential. One way to do that is to become an active member of your state or local American Academy of Family Physicians affiliate.
More information is available at:
• www.aafp.org
Practical information with regard to health reform, in addition to suggesting ways to get involved
• http://www.tafp.org/Media/Default/Downloads/practice%20resources/aco-guide.pdf
Information to consider before joining or forming an ACO
• http://www.ncqa.org/Programs/Recognition/PatientCenteredMedicalHomePCMH.aspx and http://www.transformed.com/
Resources for practitioners considering transformation to a PCMH
• http://innovation.cms.gov
Information, including webinars and forums, on innovative payment and service delivery models.
Nontraditional settings. Another facet of the medical neighborhood is the provision of health care services in nontraditional settings. For example, some grocery stores in our area employ nutritionists to whom we refer patients for nutritional counseling regarding their health in general or a disease process in particular.
Changes in reimbursement also will affect how care is delivered within the medical neighborhood. As we move away from fee-for-service (volume-based) to value-based payments, physicians who have made the transition from working individually with a panel of patients to providing team-based care within a PCMH will be better positioned to meet the goals of health care reform. (See “Team-based care is key inside the PCMH, too”22 below.) Nonetheless, the transition is a dynamic process. With changes in reimbursement and delivery models, physicians also will be expected to develop and implement continuous quality improvement measures so patient care can be continually evaluated and improved.
Now comes the hard part
While a PCMH requires primary care physicians to collaborate with other health professionals, it has the potential to lead to conflicts and debates about who is at the head of the health care team. This is particularly true within mental health services because, while primary care visits are frequently related to psychosocial issues, the mental health and general practice sectors have traditionally been distinct. In recent years, however, coordinated delivery models that integrate primary care and mental health services have been shown to increase access and reduce the stigma associated with mental health services—and to be cost-effective.23
In many ways, moving the primary care culture from the traditional focus on the physician as “captain of the ship” to a physician-led, team-based approach is one of the most difficult tasks for organizations attempting to transform their care delivery models.3,24 Physicians historically have been autonomous providers of medical care, relying on their own experience, expertise, and beliefs to guide decisions about patient care. Now they’re being asked to give up some of the direct control they may have had over patient care decisions and learn to work more collaboratively with other providers, as well as nonclinicians (eg, health coaches), to achieve desired outcomes.3 A successful transition depends on a reimbursement framework in which patient care goals are properly aligned with incentives for primary care physicians to work in a team-based environment.3,25-27
In addition to operating as a team with providers in other settings in the medical neighborhood, innovative primary care practices—typically those that have already achieved patient-centered medical home (PCMH ) status—have strong teams within their walls. In “In search of joy in practice: A report of 23 high-functioning primary care practices,” Sinsky et al22 highlight a number of ways in which the practices they studied are maximizing this approach.
Nonphysician care. A number of practices expanded the roles of medical assistants (MAs), nurses, and even nonclinician health coaches. In one case, MAs nearly tripled the time they spend with each patient, to enable them to do medication review, fill out forms, give immunizations, and book appointments for screening tests such as mammography. In another, registered nurses were given standing orders to treat routine problems such as ear infections and urinary tract infections; at a third, health coaches counsel patients with chronic conditions and MAs conduct depression screening, as needed.
Documentation and computerized order entry—which ties up many hours of physician time—is another area in which some practices have adopted a team approach. A number of practices use nurses or MAs as scribes, entering orders and preparing after-visit summaries, for example. Not only are the physicians more satisfied, but the MAs and nurses are happy to have more involvement in patient care, the researchers report.
Communication is crucial to a successful team approach. In some practices, this is accomplished with weekly physician-clinical staff meetings; in others, with brief group “huddles” or by an office design featuring “co-location.” In one example of the latter, MAs and physicians sit side-by-side, so they can easily talk to each other—the doctor could communicate key patient information that the MA would then follow up on, for example. Regular analysis of workflow to identify and address undue delays is an effective team function, as well.
Helping patients help themselves. Moving toward more patient-focused care will also require a concerted effort to increase patients’ engagement in their own health and medical care. In practice, very little of an individual’s time is spent in a physician’s office. Thus, optimal outcomes can be achieved only when patients are actively involved. Helping patients become proactive—ie, by arming them with the knowledge, skill, and confidence to do their part in staying healthy28—also represents a major shift in primary care culture, as patients become active participants in medical decision making rather than passive recipients of physicians’ advice.
Alternative approaches. To deliver the continuum of care that is central to new care delivery models and shift the culture of primary care toward a PCMH, physicians can implement a number of clinic-based engagement approaches—interacting with patients via e-visits such as e-mail through a secure portal, telemedicine, and group medical visits, for example. Physicians can encourage patient participation by starting patient interest groups and advisory panels29—recommended by the NCQA and the Agency for Healthcare Research and Quality and used at our institution—and conducting patient needs assessments on a regular basis. Opportunities for primary care practices to engage with the community include partnering with local health departments, churches, nonprofits, and advocacy organizations to conduct health promotion and educational activities.
CORRESPONDENCE
Randy Wexler, MD, MPH, Department of Family Medicine, College of Medicine, The Ohio State University, 2231 North High Street, Northwood and High Building, Columbus, OH 43201; randy.wexler@osumc.edu
Pressure to reform our health care system is at an all-time high, driven by relentlessly rising costs and fragmentation of care. These persistent problems have led to lower quality care and limited access to care for a large proportion of the US population—issues that accountable care organizations (ACOs), as well as other value-based models, are designed to address.
While the terms used to describe the means by which health care systems attempt to do more to meet the needs of those they serve may vary, the importance of reorganizing care delivery to better integrate services is gaining traction nationwide. As we move to new models, primary care takes center stage.
ACOs (or ACO-type arrangements) anchored by primary care networks can help meet the goals of health care reform by responding to changes in reimbursement, reducing fragmented care, and focusing on improving the quality of care for defined patient populations. In addition, these delivery models can take advantage of new health information technology (IT) and the move toward patient-centered medical homes (PCMHs).
In the pages that follow, we examine opportunities for new care delivery models to slow rising costs and improve population health in family medicine. The introduction of these models has important implications for patients, physicians, and provider organizations, and our aim is to ensure that family physicians are prepared to take these vital steps toward achieving health reform goals.
Shifting from volume-based to value-based reimbursement
According to the Congressional Budget Office, ACOs are expected to save $5 billion during their first 8 years of existence.1 After one year of ACO activity, the Centers for Medicare and Medicaid Services (CMS) reported savings of $30 million.2 The expected savings will be driven by the increased provider accountability associated with ACOs.
Various means of increasing provider accountability through changes in reimbursement strategies have been proposed; several are new, while others are improvements on—or variations of—methods that have been tried before. The most common approaches—shared savings, shared savings plus penalty, capitation, episodic payment, prospective payment, pay-for-performance, and hospital-physician bundling—are detailed in TABLE 1.3-7 Broad implementation of any of these reimbursement mechanisms within a new model of care would represent a shift away from the traditional volume-based provider payment model to a value-based system—a key step in slowing the rise in health care costs.
TABLE 1
Reimbursement strategies designed to promote physician accountability3-7
Model | Description | Implications for FPs |
Shared savings | FFS plus a portion of dollars saved relative to predicted costs if quality and patient satisfaction are enhanced3 | Focus on population health incentivizes well care and preventive services |
Shared savings plus penalty | Same as shared savings, plus a penalty if expenses exceed spending targets; bonus potential is increased to account for increased risk3 | Potential for care coordination payments in addition to shared savings |
Capitation | Flat payments plus bonuses and penalties; provider organization assumes full risk for a defined patient population3 | A better understanding of population management and IT now makes capitation a viable strategy in certain settings |
Episodic payments | Reimbursement is for defined episodes of care, which may extend from time of admission to days or weeks after discharge; may also include home health, extended care, or ancillary services4 | No incentive for prevention or PCMH coordination |
Prospective payment | Reimbursement for inpatient services based on a prepaid amount that covers a defined period of time; uses DRG system that bases payment on disease classification by CMS5 | It is important for FPs to partner with specialists willing to share reimbursement commensurate with the value of care provided |
Pay-for-performance | Reimbursement is tied to achievement of metrics (eg, number of patients immunized for a specific disease, desired clinical outcomes, high patient satisfaction scores) mutually agreed upon by ACO and payer6 | Be sure any agreed-upon “targets” are achievable and patient-focused |
Hospital-physician bundling | Reimbursement is based on the cost of a procedure or diagnosis that includes both hospital and physician components. One payment is made for the collective services associated with a hospitalization7 | Similar to prospective payment from FP perspective; it is important to work with those who value the care of FPs |
ACO, accountable care organization; CMS, Centers for Medicare and Medicaid Services; DRG, diagnosis-related group; FFS, fee-for-service; FPs, family physicians; IT, information technology; PCMH, patient-centered medical home.
Although it is too soon to be certain of the effect such changes will have on the earnings of family physicians, it is reasonable to think that new payment strategies—and a larger role for primary care providers—will improve their financial standing.
Moving toward population health management
New ACO-type models also make it easier to improve health care for specific populations, using strategies designed to organize, provide, and manage care for defined groups. In addition to controlling the cost of caring for specific groups, well-designed and implemented population health management strategies can increase continuity of care by ensuring oversight of patients across the spectrum of health care settings.
Five broad categories of population health management are most prominent: lifestyle management and demand management (both for relatively healthy people), disease management (for those with chronic conditions), catastrophic care management (for patients with rare or catastrophic illness or injury), and disability management (for groups of employees).8TABLE 28 describes the population targeted and activities associated with each. It is important to remember, however, that no single strategy is mutually exclusive for a particular group.
Comprehensive Primary Care (CPC) initiative. In a collaboration made possible by the Affordable Care Act, CMS initiated the CPC initiative in 2012.9 A 4-year project designed to test and further identify the benefits of population health management and strengthen coordination of care for Medicare patients within primary care settings, the CPC initiative involves 497 sites and 2347 providers caring for approximately 315,000 Medicare beneficiaries.9 More information is available at http://innovation.cms.gov/initiatives/comprehensive-primary-care-initiative/.
TABLE 2
Population health management strategies8
Strategy | Target/goal | Key elements | Evidence of effectiveness |
Lifestyle management | To help relatively healthy individuals make good choices about health behaviors and risks | • Prevention • Risk reduction • Self-care | • Adherence to guidelines for clinical screenings • Reduced costs resulting from prevention programs |
Demand management | To help relatively healthy individuals take an active role in decisions about health and medical care; aims to reduce inappropriate demand for services | • Telephone triage • Advice and referrals • Decision and behavioral support • Education to promote self-care | • Reduced variation in care unexplained by morbidity • Improved understanding of perceived need for care • Improved access, better outcomes, lower cost |
Disease management | To identify and target chronically ill patients (eg, those with diabetes, heart failure, or asthma) with specific interventions | • Clinical oversight/management of patients with chronic disease • Education and self-care • Coordination of care/providers | • Reduced costs for treatment of chronic diseases • Decreased complications associated with chronic illness |
Catastrophic care management | To identify those with rare or catastrophic illness or injury and provide services needed to improve outcomes | • Immediate referral to appropriate providers • Coordination of care • Medical/care management | • Reduced hospitalizations and total claims costs • Reduced morbidity; improved QOL • Realistic, patient-specific goals |
Disability management | To develop and deliver employer-driven initiatives for employees to reduce lost time from work, improve productivity, and optimize health and well-being | • Disability prevention programs • Return-to-work programs • Employer-based lifestyle management programs • Coordination of care/providers for employees with chronic disease, disability, and/or serious illness or injury • Absence management programs (ie, designed to control/limit unexplained, unscheduled, or excessive absenteeism) • Workplace rehabilitation | • Lower workers’ compensation/disability benefit costs • Reduced number of injuries • Reduced lost time from work • Increased productivity |
QOL, quality of life.
Building infrastructure and leveraging IT
ACOs and ACO-type models will take a variety of forms, depending in part on geographic need and local demographics. Yet, all share a common need for a strong infrastructure to support improved transitions, integration, and coordination of care. Incorporation of a strong health IT system is critical so that data regarding the process and cost of care, as well as outcomes, can be collected and put to optimal use.10-13
Across health care settings, health IT innovations are being successfully implemented in efforts to enhance physician decision support, improve patient safety, increase guideline adherence, and improve chronic disease treatment.11,13 In primary care, for example, an IT infrastructure can create disease registries so that data on patients with specific conditions can be tracked and acted upon—eg, a diabetes registry could be used to identify and contact patients who have an hemoglobin A1c >9 and have not been seen in 9 months or more.
Similarly, an IT system with the ability to identify patients at high risk for disease decompensation, hospitalization, and/or increased morbidity and mortality linked to progression of a chronic disease is needed. Identifying medical conditions associated with higher costs would make it possible to focus care coordination and chronic care management efforts on this targeted population.
As health IT continues to evolve, additional means of interacting with patients and improving patient care will be developed. Physicians and organizations that are ready to take advantage of these advances in technology will be well positioned to address the goals of health reform. (See “Health care reform: Recommendations for family physicians” below.3-7,14,15)
How the patient-centered medical home fits into the picture
The implementation of ACOs and other new models of care has promising implications for the establishment of PCMHs. Consistent with the goals of health reform, the PCMH movement focuses on a coordinated teamwork approach, anchored within a general practice or family medicine setting.
An evaluation of the PCMH National Demonstration Project funded by the American Academy of Family Physicians found that the adoption of more components of the PCMH at the practice level was associated with improvement in patient outcomes, as measured by the Ambulatory Care Quality Alliance starter set16 (a compilation of clinical performance measures developed by a broad coalition of providers, payers, consumers, and government agencies).
A recent look at the Southeastern Pennsylvania Chronic Care Initiative17 found less promising results. “A multipayer medical home pilot, in which participating practices adopted new structural capabilities and received NCQA [National Committee for Quality Assurance] certification, was associated with limited improvements in quality and was not associated with reductions in utilization of hospital, emergency department, or ambulatory care services or total costs over 3 years,” Friedberg et al17 concluded. The authors did note, however, that NCQA recognition was what the practices involved in this initiative were rewarded for—not PCMH activity.
It is also important to keep in mind that PCMH activity has been shown to improve care and reduce costs—not NCQA recognition in and of itself. In fact, a large body of evidence clearly demonstrates the positive patient care outcomes and reductions in overall cost associated with the PCMH. These findings were compiled by the Patient-Centered Primary Care Collaborative—which issues annual reports on the progress of the PCMH—in a January 2014 update.18
In a PCMH model, the focus shifts away from the procedure(s) or treatment to the whole person. However, all components of care (eg, primary and specialty care, hospital, ancillary services, laboratory, and radiology) are vital and need to be connected to increase efficiency and reduce cost—creating what is sometimes referred to as a “medical neighborhood.”19-21
What’s in the neighborhood?
In a medical neighborhood, such as an ACO, each patient is cared for by a team of providers at multiple locations. The PCMH serves as the base, ensuring that all providers work together toward a common goal. In addition to providing primary care, the PCMH coordinates each patient’s specialty and support services and communicates the care plan to all involved.
Successful implementation of a medical neighborhood requires a close working relationship among providers, payers, and community resources. For example, payers can provide real-time information about patients who have been admitted to the hospital or discharged from the emergency department, which enables close follow-up and coordination across multiple systems.
Given the emerging opportunities for new care delivery models to advance primary care, we urge family physicians to respond positively to these changes and challenges. Here’s what we recommend:
Carefully consider payment methodologies. Changes in the way physicians are paid will vary by payer source, as well as geographic market.3-7 Regardless of the reimbursement model you’re offered, however, do not agree to it until you have the opportunity to evaluate it, along with your particular circumstances, to ensure that you have the infrastructure to support whatever changes the new model will require.
Read the fine print. Look out for your own interests by carefully reading the terms you are presented with. Consider seeking advice from those who understand the particular nuances faced by family physicians under particular reimbursement strategies. Just because a payment method benefits a particular specialty does not mean it will be favorable to family physicians.
Before you join an ACO
Before joining an accountable care organization (ACO ) or a similar entity, find out whether it supports primary care principles and the patient-centered medical home (PCMH ). Some questions to ask:
• Does the ACO have the infrastructure necessary to be successful, including the requisite health information technology, administrative support, actuarial knowledge, and experience with population health management?
• Is the ACO founded on primary care principles? Find out, for example, whether primary care physicians are represented at all levels of the organization and provide appropriate input on all important issues.
If you practice in a rural area … The growth of ACO activity is expected to be slow in both rural and underserved metropolitan markets. To address this issue, the Centers for Medicare and Medicaid Services is allowing primary care physicians in such markets to participate in more than one Medicare ACO and providing financial incentives in the form of savings exemptions to smaller, rural ACOs.14,15 Another option for rural providers is the adoption of a “virtual ACO ”—a loosely organized group of providers, united in the effort to achieve high-quality care and reduced costs and willing to submit to computer analysis that will determine their relative contributions to efficiency and the distribution of savings.14
Get involved
It is important for all family physicians to engage in discussions about health care reform, and to represent both their patients and their specialty. Familiarity with what is happening is essential. One way to do that is to become an active member of your state or local American Academy of Family Physicians affiliate.
More information is available at:
• www.aafp.org
Practical information with regard to health reform, in addition to suggesting ways to get involved
• http://www.tafp.org/Media/Default/Downloads/practice%20resources/aco-guide.pdf
Information to consider before joining or forming an ACO
• http://www.ncqa.org/Programs/Recognition/PatientCenteredMedicalHomePCMH.aspx and http://www.transformed.com/
Resources for practitioners considering transformation to a PCMH
• http://innovation.cms.gov
Information, including webinars and forums, on innovative payment and service delivery models.
Nontraditional settings. Another facet of the medical neighborhood is the provision of health care services in nontraditional settings. For example, some grocery stores in our area employ nutritionists to whom we refer patients for nutritional counseling regarding their health in general or a disease process in particular.
Changes in reimbursement also will affect how care is delivered within the medical neighborhood. As we move away from fee-for-service (volume-based) to value-based payments, physicians who have made the transition from working individually with a panel of patients to providing team-based care within a PCMH will be better positioned to meet the goals of health care reform. (See “Team-based care is key inside the PCMH, too”22 below.) Nonetheless, the transition is a dynamic process. With changes in reimbursement and delivery models, physicians also will be expected to develop and implement continuous quality improvement measures so patient care can be continually evaluated and improved.
Now comes the hard part
While a PCMH requires primary care physicians to collaborate with other health professionals, it has the potential to lead to conflicts and debates about who is at the head of the health care team. This is particularly true within mental health services because, while primary care visits are frequently related to psychosocial issues, the mental health and general practice sectors have traditionally been distinct. In recent years, however, coordinated delivery models that integrate primary care and mental health services have been shown to increase access and reduce the stigma associated with mental health services—and to be cost-effective.23
In many ways, moving the primary care culture from the traditional focus on the physician as “captain of the ship” to a physician-led, team-based approach is one of the most difficult tasks for organizations attempting to transform their care delivery models.3,24 Physicians historically have been autonomous providers of medical care, relying on their own experience, expertise, and beliefs to guide decisions about patient care. Now they’re being asked to give up some of the direct control they may have had over patient care decisions and learn to work more collaboratively with other providers, as well as nonclinicians (eg, health coaches), to achieve desired outcomes.3 A successful transition depends on a reimbursement framework in which patient care goals are properly aligned with incentives for primary care physicians to work in a team-based environment.3,25-27
In addition to operating as a team with providers in other settings in the medical neighborhood, innovative primary care practices—typically those that have already achieved patient-centered medical home (PCMH ) status—have strong teams within their walls. In “In search of joy in practice: A report of 23 high-functioning primary care practices,” Sinsky et al22 highlight a number of ways in which the practices they studied are maximizing this approach.
Nonphysician care. A number of practices expanded the roles of medical assistants (MAs), nurses, and even nonclinician health coaches. In one case, MAs nearly tripled the time they spend with each patient, to enable them to do medication review, fill out forms, give immunizations, and book appointments for screening tests such as mammography. In another, registered nurses were given standing orders to treat routine problems such as ear infections and urinary tract infections; at a third, health coaches counsel patients with chronic conditions and MAs conduct depression screening, as needed.
Documentation and computerized order entry—which ties up many hours of physician time—is another area in which some practices have adopted a team approach. A number of practices use nurses or MAs as scribes, entering orders and preparing after-visit summaries, for example. Not only are the physicians more satisfied, but the MAs and nurses are happy to have more involvement in patient care, the researchers report.
Communication is crucial to a successful team approach. In some practices, this is accomplished with weekly physician-clinical staff meetings; in others, with brief group “huddles” or by an office design featuring “co-location.” In one example of the latter, MAs and physicians sit side-by-side, so they can easily talk to each other—the doctor could communicate key patient information that the MA would then follow up on, for example. Regular analysis of workflow to identify and address undue delays is an effective team function, as well.
Helping patients help themselves. Moving toward more patient-focused care will also require a concerted effort to increase patients’ engagement in their own health and medical care. In practice, very little of an individual’s time is spent in a physician’s office. Thus, optimal outcomes can be achieved only when patients are actively involved. Helping patients become proactive—ie, by arming them with the knowledge, skill, and confidence to do their part in staying healthy28—also represents a major shift in primary care culture, as patients become active participants in medical decision making rather than passive recipients of physicians’ advice.
Alternative approaches. To deliver the continuum of care that is central to new care delivery models and shift the culture of primary care toward a PCMH, physicians can implement a number of clinic-based engagement approaches—interacting with patients via e-visits such as e-mail through a secure portal, telemedicine, and group medical visits, for example. Physicians can encourage patient participation by starting patient interest groups and advisory panels29—recommended by the NCQA and the Agency for Healthcare Research and Quality and used at our institution—and conducting patient needs assessments on a regular basis. Opportunities for primary care practices to engage with the community include partnering with local health departments, churches, nonprofits, and advocacy organizations to conduct health promotion and educational activities.
CORRESPONDENCE
Randy Wexler, MD, MPH, Department of Family Medicine, College of Medicine, The Ohio State University, 2231 North High Street, Northwood and High Building, Columbus, OH 43201; randy.wexler@osumc.edu
1. Shortell SM, Casalino LP, Fisher ES. How the Center for Medicare and Medicaid Innovation should test accountable care organizations. Health Aff. 2010;29:1293-1298.
2. Medicare’s delivery system reform initiatives achieve significant savings and quality improvements - off to a strong start [press release]. Washington, DC: US Department of Health & Human Services; January 30, 2014. Available at: http://www.hhs.gov/news/press/2014pres/01/20140130a.html. Accessed March 28, 2014.
3. The family physician’s ACO blueprint for success: Preparing family medicine for the approaching accountable care era. Texas Academy of Family Physicians Web site. Available at: http://www.tafp.org/Media/Default/Downloads/practice%20resources/acoguide.pdf. Accessed March 28, 2014.
4. Mechanic RE. Opportunities and challenges for episode-based payment. N Engl J Med. 2011;365:777-779.
5. Medicare prospective payment systems (PPS): A summary. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/practice/reimbursement/medicare/pps_sum.htm. Accessed March 28, 2014.
6. Pay for performance (P4P): AHRQ resources. Agency for Healthcare Research and Quality Web site. Available at: http://www.ahrq.gov/legacy/qual/pay4per.htm. Accessed March 29, 2014.
7. Komisar H, Feder J, Ginsburg PB. “Bundling” payment for episodes of hospital care: Issues and recommendations for the new pilot program in Medicare. Available at: http://www.americanprogress.org/issues/2011/07/pdf/medicare_bundling.pdf. Accessed May 20, 2014.
8. McAlearney AS. Population health management: Strategies to improve outcomes. Chicago, IL: Health Administration Press; 2003.
9. Centers for Medicare and Medicaid Services Web site. Comprehensive primary care initiative. Available at: http://innovation.cms.gov/initiatives/comprehensive-primary-care-initiative/. Accessed March 29, 2014.
10. Robertson DC, Lerner JC. Top technology issues for ambulatory care facilities this year and beyond. J Ambul Care Manag. 2009;32:303-319.
11. Linder JA, Ma J, Bates DW, et al. Electronic health record use and the quality of ambulatory care in the united states. Arch Intern Med. 2007;167:1400-1405.
12. Vest JR. Health information exchange and healthcare utilization. J Med Syst. 2009;33:223-231.
13. Parente ST, McCullough JS. Health information technology and patient safety: evidence from panel data. Health Affairs (Millwood). 2009;28:357-360.
14. FAQ on Accountable Care Organizations. American Academy of Family Physicians Web site. Available at: http://www.aafp.org/practice-management/payment/acos/faq.html. Accessed March 29, 2014.
15. Torrieri M. CMS appeals to rural practices with another ACO participation perk. Physicians Practice blog. June 1, 2011. Available at: http://www.physicianspractice.com/blog/cms-appealsrural-practices-another-aco-participation-perk. Accessed March 29, 2014.
16. Crabtree BF, Nutting PA, Miller WL, et al. Summary of the national demonstration project and recommendations for the patient-centered medical home. Ann Fam Med. 2010;8 suppl 1:S80-S92.
17. Friedberg MW, Schneider EC, Rosenthal MB, et al. Association between participation in a multipayer medical home intervention and changes in quality, utilization, and costs of care. JAMA. 2014;311:815-825.
18. Nielsen M, Olayiwola JN, Grundy P, et al. The patient-centered medical home’s impact on cost & quality: An annual update of the evidence, 2012-2013. Available at: http://www.pcpcc.org/resource/medical-homes-impact-cost-quality. Accessed May 20, 2014.
19. Laine C. Welcome to the patient-centered medical neighborhood. Ann Intern Med. 2011;154:60.
20. Pham HH. Good neighbors: how will the patient-centered medical home relate to the rest of the health-care delivery system? J Gen Intern Med. 2010;25:630-634.
21. Taylor EF, Lake T, Nysenbaum J, et al; Mathematica Policy Research. Coordinating care in the medical neighborhood: critical components and available mechanisms: White paper. Available at: http://pcmh.ahrq.gov/sites/default/files/attachments/Coordinating%20Care%20in%20the%20Medical%20Neighborhood.pdf. Accessed May 20, 2014.
22. Sinsky CA, Willard-Grace R, Schutzbank AM, et al. In search of joy in practice: a report of 23 high-functioning primary care practices. Ann Fam Med. 2013;11:272-278.
23. Collins C, Hewson DL, Munger R, et al. Evolving models of behavioral health integration in primary care. Available at: http://www.milbank.org/uploads/documents/10430EvolvingCare/EvolvingCare.pdf. Accessed April 10, 2014.
24. The cornerstones of accountable care. Health Leaders Media Web site. Available at: http://www.healthleadersmedia.com/content/256694.pdf. Accessed March 29, 2014.
25. AAFP statement: AAFP commends CMS for improving Medicare ACO final rule, announcing the advance payment model [press release]. Leawood, Kansas: American Academy of Family Physicians; October 21, 2011. Available at: http://www.aafp.org/media-center/releases-statements/all/2011/aco-final-rule.html. Accessed March 29, 2014.
26. Fisher ES, Staiger DO, Bynum JP, et al. Creating accountable care organizations: the extended hospital medical staff. Health Affairs (Millwood). 2007;26:w44-w57.
27. Shields MC, Patel PH, Manning M, et al. A model for integrating independent physicians into accountable care organizations. Health Affairs (Millwood). 2011;30:161-172.
28. Hibbard JH. Patient engagement in accountable care organizations. Webinar. 2008. https://acoregister.rti.org/display_docs7.cfm. Accessed April 11, 2014.
29. Developing a community-based patient safety advisory council. Agency for Healthcare Research and Quality Web site. Available at: http://www.ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/resources/patient-safety-advisorycouncil/. Accessed March 31, 2014.
1. Shortell SM, Casalino LP, Fisher ES. How the Center for Medicare and Medicaid Innovation should test accountable care organizations. Health Aff. 2010;29:1293-1298.
2. Medicare’s delivery system reform initiatives achieve significant savings and quality improvements - off to a strong start [press release]. Washington, DC: US Department of Health & Human Services; January 30, 2014. Available at: http://www.hhs.gov/news/press/2014pres/01/20140130a.html. Accessed March 28, 2014.
3. The family physician’s ACO blueprint for success: Preparing family medicine for the approaching accountable care era. Texas Academy of Family Physicians Web site. Available at: http://www.tafp.org/Media/Default/Downloads/practice%20resources/acoguide.pdf. Accessed March 28, 2014.
4. Mechanic RE. Opportunities and challenges for episode-based payment. N Engl J Med. 2011;365:777-779.
5. Medicare prospective payment systems (PPS): A summary. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/practice/reimbursement/medicare/pps_sum.htm. Accessed March 28, 2014.
6. Pay for performance (P4P): AHRQ resources. Agency for Healthcare Research and Quality Web site. Available at: http://www.ahrq.gov/legacy/qual/pay4per.htm. Accessed March 29, 2014.
7. Komisar H, Feder J, Ginsburg PB. “Bundling” payment for episodes of hospital care: Issues and recommendations for the new pilot program in Medicare. Available at: http://www.americanprogress.org/issues/2011/07/pdf/medicare_bundling.pdf. Accessed May 20, 2014.
8. McAlearney AS. Population health management: Strategies to improve outcomes. Chicago, IL: Health Administration Press; 2003.
9. Centers for Medicare and Medicaid Services Web site. Comprehensive primary care initiative. Available at: http://innovation.cms.gov/initiatives/comprehensive-primary-care-initiative/. Accessed March 29, 2014.
10. Robertson DC, Lerner JC. Top technology issues for ambulatory care facilities this year and beyond. J Ambul Care Manag. 2009;32:303-319.
11. Linder JA, Ma J, Bates DW, et al. Electronic health record use and the quality of ambulatory care in the united states. Arch Intern Med. 2007;167:1400-1405.
12. Vest JR. Health information exchange and healthcare utilization. J Med Syst. 2009;33:223-231.
13. Parente ST, McCullough JS. Health information technology and patient safety: evidence from panel data. Health Affairs (Millwood). 2009;28:357-360.
14. FAQ on Accountable Care Organizations. American Academy of Family Physicians Web site. Available at: http://www.aafp.org/practice-management/payment/acos/faq.html. Accessed March 29, 2014.
15. Torrieri M. CMS appeals to rural practices with another ACO participation perk. Physicians Practice blog. June 1, 2011. Available at: http://www.physicianspractice.com/blog/cms-appealsrural-practices-another-aco-participation-perk. Accessed March 29, 2014.
16. Crabtree BF, Nutting PA, Miller WL, et al. Summary of the national demonstration project and recommendations for the patient-centered medical home. Ann Fam Med. 2010;8 suppl 1:S80-S92.
17. Friedberg MW, Schneider EC, Rosenthal MB, et al. Association between participation in a multipayer medical home intervention and changes in quality, utilization, and costs of care. JAMA. 2014;311:815-825.
18. Nielsen M, Olayiwola JN, Grundy P, et al. The patient-centered medical home’s impact on cost & quality: An annual update of the evidence, 2012-2013. Available at: http://www.pcpcc.org/resource/medical-homes-impact-cost-quality. Accessed May 20, 2014.
19. Laine C. Welcome to the patient-centered medical neighborhood. Ann Intern Med. 2011;154:60.
20. Pham HH. Good neighbors: how will the patient-centered medical home relate to the rest of the health-care delivery system? J Gen Intern Med. 2010;25:630-634.
21. Taylor EF, Lake T, Nysenbaum J, et al; Mathematica Policy Research. Coordinating care in the medical neighborhood: critical components and available mechanisms: White paper. Available at: http://pcmh.ahrq.gov/sites/default/files/attachments/Coordinating%20Care%20in%20the%20Medical%20Neighborhood.pdf. Accessed May 20, 2014.
22. Sinsky CA, Willard-Grace R, Schutzbank AM, et al. In search of joy in practice: a report of 23 high-functioning primary care practices. Ann Fam Med. 2013;11:272-278.
23. Collins C, Hewson DL, Munger R, et al. Evolving models of behavioral health integration in primary care. Available at: http://www.milbank.org/uploads/documents/10430EvolvingCare/EvolvingCare.pdf. Accessed April 10, 2014.
24. The cornerstones of accountable care. Health Leaders Media Web site. Available at: http://www.healthleadersmedia.com/content/256694.pdf. Accessed March 29, 2014.
25. AAFP statement: AAFP commends CMS for improving Medicare ACO final rule, announcing the advance payment model [press release]. Leawood, Kansas: American Academy of Family Physicians; October 21, 2011. Available at: http://www.aafp.org/media-center/releases-statements/all/2011/aco-final-rule.html. Accessed March 29, 2014.
26. Fisher ES, Staiger DO, Bynum JP, et al. Creating accountable care organizations: the extended hospital medical staff. Health Affairs (Millwood). 2007;26:w44-w57.
27. Shields MC, Patel PH, Manning M, et al. A model for integrating independent physicians into accountable care organizations. Health Affairs (Millwood). 2011;30:161-172.
28. Hibbard JH. Patient engagement in accountable care organizations. Webinar. 2008. https://acoregister.rti.org/display_docs7.cfm. Accessed April 11, 2014.
29. Developing a community-based patient safety advisory council. Agency for Healthcare Research and Quality Web site. Available at: http://www.ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/resources/patient-safety-advisorycouncil/. Accessed March 31, 2014.

When your patient’s blood pressure won’t come down
• Encourage home BP monitoring. Home readings are often lower than those taken in the office and closer to the average BP recorded by 24-hour ambulatory monitors. C
• Tell patients that reducing sodium intake not only reduces mortality, but it has positive cardiovascular effects separate from BP reduction, such as improved endothelium-dependent vasodilation. A
• Search for secondary causes of resistant hypertension, such as renal artery stenosis, pheochromocytoma, obstructive sleep apnea, and hyperaldosteronism. A
• Consider pseudohypertension in elderly patients who exhibit postural hypotension and fail to respond to increased doses of medication. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Mr. Brown is a 60-year-old African American man who works as a mid-level executive at a local bank. About a year and a half ago, he was diagnosed with hypertension, joining a number of other family members who also have the condition. Reviewing his chart, you note that at many of his visits—but not all of them—his systolic blood pressure runs close to 150 mm Hg, with diastolic pressure <90 mm Hg. Today his blood pressure is 148/88 mm Hg, numbers that exceed the parameters of the currently accepted definition of hypertension: blood pressure ≥140 mm Hg systolic or ≥90 mm Hg diastolic, taken on 2 separate occasions with the patient sitting down.1
Mr. Brown is one of the more than 65 million American adults suffering from high blood pressure—the No. 1 diagnosis reported in outpatient medical offices.2,3 Despite such prevalence, blood pressure control in the United States is suboptimal, with only one-third of hypertensive patients under adequate control.1 In 2007, the total estimated cost of treating high blood pressure in the United States exceeded $66 billion.4
When you tell Mr. Brown that his blood pressure doesn’t meet the therapeutic goal of <140/90 mm Hg, he gives you his reasons: He was late, he rushed, the traffic was bad, and the nurse rushed him into the exam room before he even had time to catch his breath. He insists his blood pressure is “normal” at home, and blames the elevated numbers on anxiety. He also tells you he was up working most of the night before, drinking coffee to stay awake to finish an urgent project.
Mr. Brown’s current medication regimen includes daily doses of lisinopril-hydrochlorothiazide (HCTZ) 20/25 mg daily and simvastatin 20 mg. He tells you he has no chest pain, shortness of breath, cough, edema, claudication, paroxysmal nocturnal dyspnea, or orthopnea. When you ask if he takes his lisinopril-HCTZ every day, he says Yes, but you have your suspicions.
Consider pseudo-resistance
Suboptimal blood pressure control can be classified as either pseudo-resistant or resistant hypertension. According to the definition used in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7), resistance is the “failure to achieve goal BP in patients who are adhering to full doses of an appropriate 3-drug regimen that includes a diuretic.”1
Hypertension is described as “pseudo-resistant” when persistent elevations in blood pressure are the result of a failure to comply with the medication regimen, “white-coat” syndrome, poor blood pressure technique, or a combination of these.5,6 Physician failure to prescribe adequate doses of medication, so-called clinical inertia, may also be a factor.5,7 Causes and remedies for pseudo-resistance are summarized in the algorithm.
In Mr. Brown’s case, he’s told you that he’s taking his lisinopril-HCTZ every day, but when you check your records, you see that the intervals between his refill requests range between 34 and 36 days. So you ask him, again, whether he is taking his lisinopril-HCTZ daily, and this time he says he takes the medication “at least 5 or 6 days a week.”
Encourage compliance. To motivate Mr. Brown, you tell him his blood pressure does not meet the goal of <140/90 mm Hg and that pressure higher than goal is a significant risk factor for cardiovascular disease. You emphasize the importance of taking his medication every day—a mantra you’ve repeated to countless patients over the years. In fact, it’s estimated that up to 40% of patients will discontinue their medication at some point during treatment.8 Patients’ reasons vary and may include medication side effects, the cost of treatment, or a patient’s personal philosophy. Cultural differences may also play a role in noncompliance.9
You talk with Mr. Brown a bit more and confirm that his poor compliance is due to simple forgetfulness and not another underlying reason that would need to be addressed. You hand him a pill calendar to help him keep track of his medication. You review the dosage and feel confident that you’ve prescribed a regimen simple enough for Mr. Brown to stick to and adequate to bring his pressure down.
When your white coat is the problem. Though not the case with Mr. Brown, a patient’s elevated readings could be a case of white coat hypertension—a conditioned response in some patients that is probably the result of anxiety in the medical setting.10 Patients with white coat hypertension have significantly less risk of death and reduced target organ damage than patients with truly resistant hypertension.11,12
If you suspect that a patient of yours has white coat hypertension, you can test your hypothesis by encouraging him or her to buy a blood pressure monitor to use at home, keep a log of the readings, and bring the log in to the next appointment. Improved technology has made home blood pressure monitoring an important tool in the treatment of high blood pressure.13-15
According to a 2008 statement issued jointly by the American Heart Association, the American Society of Hypertension, and the Preventive Cardiovascular Nurses Association, “There is a rapidly growing literature showing that measurements taken by patients at home are often lower than readings taken in the office and closer to the average blood pressure recorded by 24-hour ambulatory monitors, which is the blood pressure that best predicts cardiovascular risk.”14
Arm monitors are the most accurate because they measure brachial artery blood pressure.14 Most wrist monitors have not been validated in studies, but obese patients who cannot find a properly sized cuff may need to use them.14 Finger devices should never be used.14
Sometimes technique is at fault. To ensure that you get proper readings when your patient is in the office, advise the nursing staff not to take a patient’s blood pressure for at least 5 minutes after bringing him or her to an exam room. Specifically, the nurse can either make blood pressure measurement the last thing she (or he) does when “rooming” the patient, or she may prefer to go back to the exam room a few minutes after the patient is there to take the reading. The nurse should take care that the cuff is the right size and that the pressure is taken with the patient’s arm at heart level. In hypertensive patients, placing the arm below the horizontal in the dependent position can raise blood pressure 23/10 mm Hg.1,16,17
Newer blood pressure monitoring devices for the office are available that obviate artificially high readings caused by errors in technique and by white coat syndrome. Researchers have found that readings taken with the BpTRU automatic device, which obtains and records 5 blood pressure readings over a 5-minute period, are lower than those taken by office personnel, and that the white coat effect is eliminated.18,19
One pseudo-resistant case solved. At Mr. Brown’s next visit, you review his pill calendar with him and note that his blood pressure is now running 138/88 mm Hg and he is within his target goal of less than 140/90 mm Hg.
If Mr. Brown’s blood pressure control had continued to be suboptimal even after you’d taken steps to address cause(s) of pseudo-resistance, you would have had to shift gears and consider his case one of resistant hypertension.1
Consider resistant hypertension
Causes of resistant hypertension include lifestyle factors, side effects of medications, and secondary causes.5,6 Tobacco use, obesity, lack of exercise, a high sodium diet, and alcohol consumption can all contribute to hypertension.1,5,6,20,21 Dietary sodium in particular has significant adverse effects. Reducing dietary sodium not only reduces mortality, but has positive cardiovascular effects separate from blood pressure reduction, such as improved endothelium-dependent vasodilation.22-24
Medications including nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, sympathomimetics, glucocorticoids, and black licorice (found in some herbal supplements) may all raise blood pressure.5 Medications and other substances associated with increased blood pressure are listed in the TABLE. A search for such products, with changes or discontinuations that are clinically appropriate, should be part of any evaluation for resistant hypertension.
CASE 2 Ms. Stevens is a 30-year-old woman who was diagnosed with high blood pressure 7 months ago. She is currently taking triamterene-HCTZ 37.5/25 mg daily, amlodipine 10 mg daily, and metoprolol succinate 100 mg daily. She is compliant with medication, sticks to a low-sodium diet, and exercises 5 days a week. She does not drink alcohol. A review of her chart tells you her baseline serum chemistries, chest x-ray, and urinalysis are all normal. Today’s blood pressure taken in the sitting position after a 5-minute rest is 160/92 mm Hg. How should you proceed?
TABLE
Medications and other agents that may cause hypertension
| • Alcohol | • Cyclosporine | • Nicotine |
| • Antidepressants | • Erythropoietin | • NSAIDs |
| • Buspirone (Buspar) | • Estrogen preparations | • St. John’s wort |
| • Cocaine | • Licorice | • Tyramine-containing foods |
| • Corticosteroids | • Metoclopramide (Reglan) | |
| NSAIDs, nonsteroidal anti-infiammatory drugs. | ||
| Source: Chobanian A, et al. Hypertension. 2003.1 | ||
Is it resistant hypertension? Look for clues
You go over Ms. Stevens’ history carefully. Her hypertension medications should be adequate, and she is compliant with the prescribed regimen. Lifestyle factors are clearly not to blame: She’s not obese, she follows a low-sodium diet, doesn’t drink or smoke, and gets plenty of exercise. You ask her about other medications or over-the-counter supplements she takes, and nothing on her list raises a red flag. This doesn’t seem to be pseudo-resistance, and though you’re aware that only about 5% of cases of hypertension can be attributed to secondary causes, you think Ms. Stevens may be one of those patients.25
Numerous causes of secondary hypertension exist, and evaluations for such causes should be considered in all patients with resistant hypertension. Renal artery stenosis and pheochromocytoma are the most well-known causes, but less well known but significant contributors are obstructive sleep apnea and hyperaldosteronism.1,6,26,27
The relationship between obstructive sleep apnea and hypertension is not clear, and most of the studies linking the 2 conditions are population based.28 Nevertheless, because studies show that continuous positive airway pressure (CPAP) does improve blood pressure control in patients with obstructive sleep apnea, it is appropriate to investigate patients with resistant hypertension for this condition.29
Aldosterone’s role in resistant hypertension appears to be greatest in those with insulin resistance. The mechanism appears to be amplified sodium retention resulting in increased volume expansion, negative effects on oxidative stress, and elevated inflammation.27 Many patients with hypertension also have insulin resistance, so testing for hyperaldosteronism should be part of your investigation.
Test, and as necessary, test some more
Taking into consideration that 2 of the more common causes of secondary hypertension are obstructive sleep apnea and renal artery stenosis, you schedule an overnight sleep study for Ms. Stevens and a magnetic resonance arteriogram of the kidneys.26,30 (For more on the diagnostic tests and treatments for secondary causes of resistant hypertension, see the ALGORITHM.)
Reconsider medications. Ms. Stevens is already receiving the maximum dose of amlodipine, so you increase her metoprolol succinate to 200 mg daily and ask her to return in 1 month after the results of her tests come in.
Change medications and keep testing. At her next visit, Ms. Stevens’ blood pressure is 150/88 mm Hg, and her pulse rate is 64. Results of her overnight sleep study and magnetic resonance arteriogram are normal. At this juncture, with her work-up for common secondary causes of hypertension negative, you consider changes in her medication regimen. Because her pulse rate of 64 rules out any increase in the metoprolol, you decide to add lisinopril-HCTZ 10/12.5 mg to her regimen and discontinue her triamterene-HCTZ. Because her blood pressure is still elevated at this visit, you schedule additional testing to look for other secondary causes.
More tests, higher doses. One month later, Ms. Stevens returns with a blood pressure of 146/88 mm Hg. Appropriate testing for primary aldosteronism, pheochromocytoma, Cushing’s disease, and coarctation are all normal. Her lisinopril-HCTZ dose is increased to 20/12.5 mg, and when she returns 1 month later her blood pressure reading is 138/88 mm Hg.
You conclude that she is a patient with hard-to-control hypertension with no underlying cause who requires a significant amount of medication. That is not an uncommon situation. Although her blood pressure is now controlled to an appropriate level, you make a chart notation to consider referral to a hypertension specialist if her blood pressure become elevated again and treatment changes are not effective.6
ALGORITHM
Hard-to-control hypertension? This treatment algorithm can help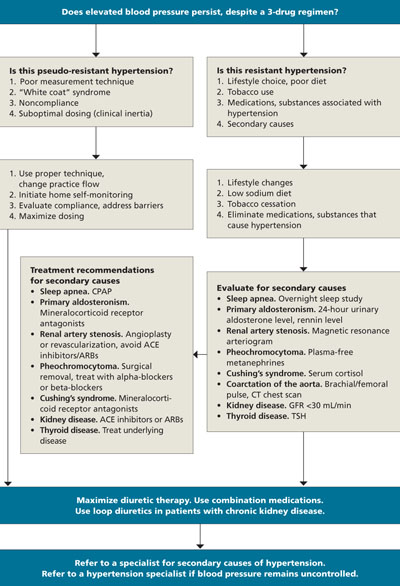
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CPAP, continuous positive airway pressure; CT, computed tomography; GFR, glomerular filtration rate; TSH, thyroid-stimulating hormone.
Adapted from: Calhoun DA, et al. Hypertension. 2008.6
Another consideration: Pseudohypertension
This uncommon condition sometimes occurs in elderly patients who suffer from a stiffened or thickened brachial artery.1 Because the blood pressure cuff cannot compress the artery, blood pressure readings overestimate true arterial pressure. The condition should be considered in patients when increased doses of medication fail to achieve the desired response, particularly in patients who exhibit postural hypotension.1
This was not a likely explanation for Ms. Stevens, however, given the clinical scenario and her young age.
CORRESPONDENCE Randy Wexler, MD, MPH, B0902B Cramblett Hall, 456 W 10th Avenue, Columbus, OH 43210; randy.wexler@osumc.edu
1. Chobanian A, Bakris GL, Black HR, et al. Seventh Report of The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7). Hypertension. 2003;42:1206-1252.
2. Fields L, Burt V, Cutler J, et al. The burden of adult hypertension in the United States 1999-2000: A rising tide. Hypertension. 2004;44:1-7.
3. Fang J, Alderman MH, Keenan NL, et al. Hypertension control at physicians’ offices in the United States. Am J Hypertens. 2008;21:136-142.
4. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics–2007 update. Circulation. 2007;115:e69-e171.
5. Sarafidis PA, Bakris GL. Resistant hypertension: an overview of evaluation and treatment. J Am Coll Cardiol. 2008;52:1749-1757.
6. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403-1419.
7. Phillips LS, Branch WT, Book CB, et al. Clinical inertia. Ann Intern Med. 2001;135:825-834.
8. Van Wijk BL, Klungel OH, Heerdink ER, et al. Rate and determinants of 10-year persistence with antihypertensive drugs. J Hypertens. 2005;23:2101-2107.
9. Wexler R, Pleister A, Feldman D. Sociology meets genetics: sociogenetic implications for future management of hypertension and heart failure. Curr Treat Options Cardiovasc Med. 2009;11:305-315.
10. Ogedegbe G, Pickering TG, Clemow L, et al. The misdiagnosis of hypertension: the role of patient anxiety. Arch Intern Med. 2008;168:2459-2465.
11. Dawes MG, Bartlett G, Coats AJ, et al. Comparing the effects of white coat hypertension and sustained hypertension on mortality in a UK primary care setting. Ann Fam Med. 2008;6:390-396.
12. Pierdomenico SD, Lapenna D, Bucci A, et al. Cardiovascular outcome in treated hypertensive patients with responder, masked, false resistant, and true resistant hypertension. Am J Hypertens. 2005;18:1422-1428.
13. Verberk WJ, Kroon AA, Kessels AGH, et al. Home blood pressure monitoring: a systematic review. J Am Coll Cardiol. 2005;46:743-751.
14. Pickering TG, Miller NH, Ogedegbe G, et al. AHA/ASH/PCNA scientific statement. Call to action on use and reimbursement for home blood pressure monitoring. Hypertension. 2008;52:10-29.
15. O’Brien E. Ambulatory blood pressure measurement: the case for implementation in primary care. Hypertension. 2008;51:1435-1441.
16. O’Brien E, Asmar R, Beilin L, et al. On behalf of the European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension recommendations for conventional ambulatory and home blood pressure measurements. J Hypertens. 2003;21:821-848.
17. Mourad A, Carney S, Gillies A, et al. Arm position and blood pressure: a risk factor for hypertension. J Hum Hypertens. 2003;17:389-395.
18. Myers MG. Automated blood pressure measurement in routine clinical practice. Blood Press Monit. 2006;11:59-62.
19. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce white coat hypertension. J Hypertens. 2009;27:280-286.
20. He J, Paul J, Whelton P, Appel L, et al. Long-term effects of weight loss and dietary sodium reduction on incidence of hypertension. Hypertension. 2000;35:544-549.
21. PREMIER Collaborative Research Writing Group. Effects of comprehensive lifestyle modification on blood pressure control. JAMA. 2003;289:2083-2093.
22. Cook NR, Cutler JA, Obarzanek E, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP). BMJ. 2007;334:885-888.
23. Dickinson BD, Havas S. Reducing the population burden of cardiovascular disease by reducing sodium intake. Arch Intern Med. 2007;167:1460-1468.
24. Li J, White J, Guo L, et al. Salt inactivates endothelial nitric oxide synthase in endothelial cells. J Nutr. 2009;139:1-5.
25. Beevers G, Lip G, O’Brien E. ABCs of hypertension: the pathophysiology of hypertension. BMJ. 2001;322:912-916.
26. Peppard PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378-1384.
27. Sowers JR, Whaley-Connell A, Epstein M. Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med. 2009;150:776-783.
28. Young T, Peppard P, Palta M, et al. Population-based study of sleep-disordered breathing as a risk factor for hypertension. Arch Intern Med. 1997;157:1746-1752.
29. Haentjens P, Van Meerhaeghe A, Moscariello A. The impact of continuous positive airway pressure on blood pressure in patients with obstructive sleep apnea syndrome: evidence from a meta-analysis of placebo-controlled randomized trials. Arch Intern Med. 2007;167:757-764.
30. Kawashima A, Francis IR, Baumgarten DA, et al. For the Expert Panel on Urologic Imaging. Renovascular hypertension. Reston, Va: American College of Radiology; 2007. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=11590&nbr=6003. Accessed April 4, 2009.
• Encourage home BP monitoring. Home readings are often lower than those taken in the office and closer to the average BP recorded by 24-hour ambulatory monitors. C
• Tell patients that reducing sodium intake not only reduces mortality, but it has positive cardiovascular effects separate from BP reduction, such as improved endothelium-dependent vasodilation. A
• Search for secondary causes of resistant hypertension, such as renal artery stenosis, pheochromocytoma, obstructive sleep apnea, and hyperaldosteronism. A
• Consider pseudohypertension in elderly patients who exhibit postural hypotension and fail to respond to increased doses of medication. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Mr. Brown is a 60-year-old African American man who works as a mid-level executive at a local bank. About a year and a half ago, he was diagnosed with hypertension, joining a number of other family members who also have the condition. Reviewing his chart, you note that at many of his visits—but not all of them—his systolic blood pressure runs close to 150 mm Hg, with diastolic pressure <90 mm Hg. Today his blood pressure is 148/88 mm Hg, numbers that exceed the parameters of the currently accepted definition of hypertension: blood pressure ≥140 mm Hg systolic or ≥90 mm Hg diastolic, taken on 2 separate occasions with the patient sitting down.1
Mr. Brown is one of the more than 65 million American adults suffering from high blood pressure—the No. 1 diagnosis reported in outpatient medical offices.2,3 Despite such prevalence, blood pressure control in the United States is suboptimal, with only one-third of hypertensive patients under adequate control.1 In 2007, the total estimated cost of treating high blood pressure in the United States exceeded $66 billion.4
When you tell Mr. Brown that his blood pressure doesn’t meet the therapeutic goal of <140/90 mm Hg, he gives you his reasons: He was late, he rushed, the traffic was bad, and the nurse rushed him into the exam room before he even had time to catch his breath. He insists his blood pressure is “normal” at home, and blames the elevated numbers on anxiety. He also tells you he was up working most of the night before, drinking coffee to stay awake to finish an urgent project.
Mr. Brown’s current medication regimen includes daily doses of lisinopril-hydrochlorothiazide (HCTZ) 20/25 mg daily and simvastatin 20 mg. He tells you he has no chest pain, shortness of breath, cough, edema, claudication, paroxysmal nocturnal dyspnea, or orthopnea. When you ask if he takes his lisinopril-HCTZ every day, he says Yes, but you have your suspicions.
Consider pseudo-resistance
Suboptimal blood pressure control can be classified as either pseudo-resistant or resistant hypertension. According to the definition used in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7), resistance is the “failure to achieve goal BP in patients who are adhering to full doses of an appropriate 3-drug regimen that includes a diuretic.”1
Hypertension is described as “pseudo-resistant” when persistent elevations in blood pressure are the result of a failure to comply with the medication regimen, “white-coat” syndrome, poor blood pressure technique, or a combination of these.5,6 Physician failure to prescribe adequate doses of medication, so-called clinical inertia, may also be a factor.5,7 Causes and remedies for pseudo-resistance are summarized in the algorithm.
In Mr. Brown’s case, he’s told you that he’s taking his lisinopril-HCTZ every day, but when you check your records, you see that the intervals between his refill requests range between 34 and 36 days. So you ask him, again, whether he is taking his lisinopril-HCTZ daily, and this time he says he takes the medication “at least 5 or 6 days a week.”
Encourage compliance. To motivate Mr. Brown, you tell him his blood pressure does not meet the goal of <140/90 mm Hg and that pressure higher than goal is a significant risk factor for cardiovascular disease. You emphasize the importance of taking his medication every day—a mantra you’ve repeated to countless patients over the years. In fact, it’s estimated that up to 40% of patients will discontinue their medication at some point during treatment.8 Patients’ reasons vary and may include medication side effects, the cost of treatment, or a patient’s personal philosophy. Cultural differences may also play a role in noncompliance.9
You talk with Mr. Brown a bit more and confirm that his poor compliance is due to simple forgetfulness and not another underlying reason that would need to be addressed. You hand him a pill calendar to help him keep track of his medication. You review the dosage and feel confident that you’ve prescribed a regimen simple enough for Mr. Brown to stick to and adequate to bring his pressure down.
When your white coat is the problem. Though not the case with Mr. Brown, a patient’s elevated readings could be a case of white coat hypertension—a conditioned response in some patients that is probably the result of anxiety in the medical setting.10 Patients with white coat hypertension have significantly less risk of death and reduced target organ damage than patients with truly resistant hypertension.11,12
If you suspect that a patient of yours has white coat hypertension, you can test your hypothesis by encouraging him or her to buy a blood pressure monitor to use at home, keep a log of the readings, and bring the log in to the next appointment. Improved technology has made home blood pressure monitoring an important tool in the treatment of high blood pressure.13-15
According to a 2008 statement issued jointly by the American Heart Association, the American Society of Hypertension, and the Preventive Cardiovascular Nurses Association, “There is a rapidly growing literature showing that measurements taken by patients at home are often lower than readings taken in the office and closer to the average blood pressure recorded by 24-hour ambulatory monitors, which is the blood pressure that best predicts cardiovascular risk.”14
Arm monitors are the most accurate because they measure brachial artery blood pressure.14 Most wrist monitors have not been validated in studies, but obese patients who cannot find a properly sized cuff may need to use them.14 Finger devices should never be used.14
Sometimes technique is at fault. To ensure that you get proper readings when your patient is in the office, advise the nursing staff not to take a patient’s blood pressure for at least 5 minutes after bringing him or her to an exam room. Specifically, the nurse can either make blood pressure measurement the last thing she (or he) does when “rooming” the patient, or she may prefer to go back to the exam room a few minutes after the patient is there to take the reading. The nurse should take care that the cuff is the right size and that the pressure is taken with the patient’s arm at heart level. In hypertensive patients, placing the arm below the horizontal in the dependent position can raise blood pressure 23/10 mm Hg.1,16,17
Newer blood pressure monitoring devices for the office are available that obviate artificially high readings caused by errors in technique and by white coat syndrome. Researchers have found that readings taken with the BpTRU automatic device, which obtains and records 5 blood pressure readings over a 5-minute period, are lower than those taken by office personnel, and that the white coat effect is eliminated.18,19
One pseudo-resistant case solved. At Mr. Brown’s next visit, you review his pill calendar with him and note that his blood pressure is now running 138/88 mm Hg and he is within his target goal of less than 140/90 mm Hg.
If Mr. Brown’s blood pressure control had continued to be suboptimal even after you’d taken steps to address cause(s) of pseudo-resistance, you would have had to shift gears and consider his case one of resistant hypertension.1
Consider resistant hypertension
Causes of resistant hypertension include lifestyle factors, side effects of medications, and secondary causes.5,6 Tobacco use, obesity, lack of exercise, a high sodium diet, and alcohol consumption can all contribute to hypertension.1,5,6,20,21 Dietary sodium in particular has significant adverse effects. Reducing dietary sodium not only reduces mortality, but has positive cardiovascular effects separate from blood pressure reduction, such as improved endothelium-dependent vasodilation.22-24
Medications including nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, sympathomimetics, glucocorticoids, and black licorice (found in some herbal supplements) may all raise blood pressure.5 Medications and other substances associated with increased blood pressure are listed in the TABLE. A search for such products, with changes or discontinuations that are clinically appropriate, should be part of any evaluation for resistant hypertension.
CASE 2 Ms. Stevens is a 30-year-old woman who was diagnosed with high blood pressure 7 months ago. She is currently taking triamterene-HCTZ 37.5/25 mg daily, amlodipine 10 mg daily, and metoprolol succinate 100 mg daily. She is compliant with medication, sticks to a low-sodium diet, and exercises 5 days a week. She does not drink alcohol. A review of her chart tells you her baseline serum chemistries, chest x-ray, and urinalysis are all normal. Today’s blood pressure taken in the sitting position after a 5-minute rest is 160/92 mm Hg. How should you proceed?
TABLE
Medications and other agents that may cause hypertension
| • Alcohol | • Cyclosporine | • Nicotine |
| • Antidepressants | • Erythropoietin | • NSAIDs |
| • Buspirone (Buspar) | • Estrogen preparations | • St. John’s wort |
| • Cocaine | • Licorice | • Tyramine-containing foods |
| • Corticosteroids | • Metoclopramide (Reglan) | |
| NSAIDs, nonsteroidal anti-infiammatory drugs. | ||
| Source: Chobanian A, et al. Hypertension. 2003.1 | ||
Is it resistant hypertension? Look for clues
You go over Ms. Stevens’ history carefully. Her hypertension medications should be adequate, and she is compliant with the prescribed regimen. Lifestyle factors are clearly not to blame: She’s not obese, she follows a low-sodium diet, doesn’t drink or smoke, and gets plenty of exercise. You ask her about other medications or over-the-counter supplements she takes, and nothing on her list raises a red flag. This doesn’t seem to be pseudo-resistance, and though you’re aware that only about 5% of cases of hypertension can be attributed to secondary causes, you think Ms. Stevens may be one of those patients.25
Numerous causes of secondary hypertension exist, and evaluations for such causes should be considered in all patients with resistant hypertension. Renal artery stenosis and pheochromocytoma are the most well-known causes, but less well known but significant contributors are obstructive sleep apnea and hyperaldosteronism.1,6,26,27
The relationship between obstructive sleep apnea and hypertension is not clear, and most of the studies linking the 2 conditions are population based.28 Nevertheless, because studies show that continuous positive airway pressure (CPAP) does improve blood pressure control in patients with obstructive sleep apnea, it is appropriate to investigate patients with resistant hypertension for this condition.29
Aldosterone’s role in resistant hypertension appears to be greatest in those with insulin resistance. The mechanism appears to be amplified sodium retention resulting in increased volume expansion, negative effects on oxidative stress, and elevated inflammation.27 Many patients with hypertension also have insulin resistance, so testing for hyperaldosteronism should be part of your investigation.
Test, and as necessary, test some more
Taking into consideration that 2 of the more common causes of secondary hypertension are obstructive sleep apnea and renal artery stenosis, you schedule an overnight sleep study for Ms. Stevens and a magnetic resonance arteriogram of the kidneys.26,30 (For more on the diagnostic tests and treatments for secondary causes of resistant hypertension, see the ALGORITHM.)
Reconsider medications. Ms. Stevens is already receiving the maximum dose of amlodipine, so you increase her metoprolol succinate to 200 mg daily and ask her to return in 1 month after the results of her tests come in.
Change medications and keep testing. At her next visit, Ms. Stevens’ blood pressure is 150/88 mm Hg, and her pulse rate is 64. Results of her overnight sleep study and magnetic resonance arteriogram are normal. At this juncture, with her work-up for common secondary causes of hypertension negative, you consider changes in her medication regimen. Because her pulse rate of 64 rules out any increase in the metoprolol, you decide to add lisinopril-HCTZ 10/12.5 mg to her regimen and discontinue her triamterene-HCTZ. Because her blood pressure is still elevated at this visit, you schedule additional testing to look for other secondary causes.
More tests, higher doses. One month later, Ms. Stevens returns with a blood pressure of 146/88 mm Hg. Appropriate testing for primary aldosteronism, pheochromocytoma, Cushing’s disease, and coarctation are all normal. Her lisinopril-HCTZ dose is increased to 20/12.5 mg, and when she returns 1 month later her blood pressure reading is 138/88 mm Hg.
You conclude that she is a patient with hard-to-control hypertension with no underlying cause who requires a significant amount of medication. That is not an uncommon situation. Although her blood pressure is now controlled to an appropriate level, you make a chart notation to consider referral to a hypertension specialist if her blood pressure become elevated again and treatment changes are not effective.6
ALGORITHM
Hard-to-control hypertension? This treatment algorithm can help
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CPAP, continuous positive airway pressure; CT, computed tomography; GFR, glomerular filtration rate; TSH, thyroid-stimulating hormone.
Adapted from: Calhoun DA, et al. Hypertension. 2008.6
Another consideration: Pseudohypertension
This uncommon condition sometimes occurs in elderly patients who suffer from a stiffened or thickened brachial artery.1 Because the blood pressure cuff cannot compress the artery, blood pressure readings overestimate true arterial pressure. The condition should be considered in patients when increased doses of medication fail to achieve the desired response, particularly in patients who exhibit postural hypotension.1
This was not a likely explanation for Ms. Stevens, however, given the clinical scenario and her young age.
CORRESPONDENCE Randy Wexler, MD, MPH, B0902B Cramblett Hall, 456 W 10th Avenue, Columbus, OH 43210; randy.wexler@osumc.edu
• Encourage home BP monitoring. Home readings are often lower than those taken in the office and closer to the average BP recorded by 24-hour ambulatory monitors. C
• Tell patients that reducing sodium intake not only reduces mortality, but it has positive cardiovascular effects separate from BP reduction, such as improved endothelium-dependent vasodilation. A
• Search for secondary causes of resistant hypertension, such as renal artery stenosis, pheochromocytoma, obstructive sleep apnea, and hyperaldosteronism. A
• Consider pseudohypertension in elderly patients who exhibit postural hypotension and fail to respond to increased doses of medication. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Mr. Brown is a 60-year-old African American man who works as a mid-level executive at a local bank. About a year and a half ago, he was diagnosed with hypertension, joining a number of other family members who also have the condition. Reviewing his chart, you note that at many of his visits—but not all of them—his systolic blood pressure runs close to 150 mm Hg, with diastolic pressure <90 mm Hg. Today his blood pressure is 148/88 mm Hg, numbers that exceed the parameters of the currently accepted definition of hypertension: blood pressure ≥140 mm Hg systolic or ≥90 mm Hg diastolic, taken on 2 separate occasions with the patient sitting down.1
Mr. Brown is one of the more than 65 million American adults suffering from high blood pressure—the No. 1 diagnosis reported in outpatient medical offices.2,3 Despite such prevalence, blood pressure control in the United States is suboptimal, with only one-third of hypertensive patients under adequate control.1 In 2007, the total estimated cost of treating high blood pressure in the United States exceeded $66 billion.4
When you tell Mr. Brown that his blood pressure doesn’t meet the therapeutic goal of <140/90 mm Hg, he gives you his reasons: He was late, he rushed, the traffic was bad, and the nurse rushed him into the exam room before he even had time to catch his breath. He insists his blood pressure is “normal” at home, and blames the elevated numbers on anxiety. He also tells you he was up working most of the night before, drinking coffee to stay awake to finish an urgent project.
Mr. Brown’s current medication regimen includes daily doses of lisinopril-hydrochlorothiazide (HCTZ) 20/25 mg daily and simvastatin 20 mg. He tells you he has no chest pain, shortness of breath, cough, edema, claudication, paroxysmal nocturnal dyspnea, or orthopnea. When you ask if he takes his lisinopril-HCTZ every day, he says Yes, but you have your suspicions.
Consider pseudo-resistance
Suboptimal blood pressure control can be classified as either pseudo-resistant or resistant hypertension. According to the definition used in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7), resistance is the “failure to achieve goal BP in patients who are adhering to full doses of an appropriate 3-drug regimen that includes a diuretic.”1
Hypertension is described as “pseudo-resistant” when persistent elevations in blood pressure are the result of a failure to comply with the medication regimen, “white-coat” syndrome, poor blood pressure technique, or a combination of these.5,6 Physician failure to prescribe adequate doses of medication, so-called clinical inertia, may also be a factor.5,7 Causes and remedies for pseudo-resistance are summarized in the algorithm.
In Mr. Brown’s case, he’s told you that he’s taking his lisinopril-HCTZ every day, but when you check your records, you see that the intervals between his refill requests range between 34 and 36 days. So you ask him, again, whether he is taking his lisinopril-HCTZ daily, and this time he says he takes the medication “at least 5 or 6 days a week.”
Encourage compliance. To motivate Mr. Brown, you tell him his blood pressure does not meet the goal of <140/90 mm Hg and that pressure higher than goal is a significant risk factor for cardiovascular disease. You emphasize the importance of taking his medication every day—a mantra you’ve repeated to countless patients over the years. In fact, it’s estimated that up to 40% of patients will discontinue their medication at some point during treatment.8 Patients’ reasons vary and may include medication side effects, the cost of treatment, or a patient’s personal philosophy. Cultural differences may also play a role in noncompliance.9
You talk with Mr. Brown a bit more and confirm that his poor compliance is due to simple forgetfulness and not another underlying reason that would need to be addressed. You hand him a pill calendar to help him keep track of his medication. You review the dosage and feel confident that you’ve prescribed a regimen simple enough for Mr. Brown to stick to and adequate to bring his pressure down.
When your white coat is the problem. Though not the case with Mr. Brown, a patient’s elevated readings could be a case of white coat hypertension—a conditioned response in some patients that is probably the result of anxiety in the medical setting.10 Patients with white coat hypertension have significantly less risk of death and reduced target organ damage than patients with truly resistant hypertension.11,12
If you suspect that a patient of yours has white coat hypertension, you can test your hypothesis by encouraging him or her to buy a blood pressure monitor to use at home, keep a log of the readings, and bring the log in to the next appointment. Improved technology has made home blood pressure monitoring an important tool in the treatment of high blood pressure.13-15
According to a 2008 statement issued jointly by the American Heart Association, the American Society of Hypertension, and the Preventive Cardiovascular Nurses Association, “There is a rapidly growing literature showing that measurements taken by patients at home are often lower than readings taken in the office and closer to the average blood pressure recorded by 24-hour ambulatory monitors, which is the blood pressure that best predicts cardiovascular risk.”14
Arm monitors are the most accurate because they measure brachial artery blood pressure.14 Most wrist monitors have not been validated in studies, but obese patients who cannot find a properly sized cuff may need to use them.14 Finger devices should never be used.14
Sometimes technique is at fault. To ensure that you get proper readings when your patient is in the office, advise the nursing staff not to take a patient’s blood pressure for at least 5 minutes after bringing him or her to an exam room. Specifically, the nurse can either make blood pressure measurement the last thing she (or he) does when “rooming” the patient, or she may prefer to go back to the exam room a few minutes after the patient is there to take the reading. The nurse should take care that the cuff is the right size and that the pressure is taken with the patient’s arm at heart level. In hypertensive patients, placing the arm below the horizontal in the dependent position can raise blood pressure 23/10 mm Hg.1,16,17
Newer blood pressure monitoring devices for the office are available that obviate artificially high readings caused by errors in technique and by white coat syndrome. Researchers have found that readings taken with the BpTRU automatic device, which obtains and records 5 blood pressure readings over a 5-minute period, are lower than those taken by office personnel, and that the white coat effect is eliminated.18,19
One pseudo-resistant case solved. At Mr. Brown’s next visit, you review his pill calendar with him and note that his blood pressure is now running 138/88 mm Hg and he is within his target goal of less than 140/90 mm Hg.
If Mr. Brown’s blood pressure control had continued to be suboptimal even after you’d taken steps to address cause(s) of pseudo-resistance, you would have had to shift gears and consider his case one of resistant hypertension.1
Consider resistant hypertension
Causes of resistant hypertension include lifestyle factors, side effects of medications, and secondary causes.5,6 Tobacco use, obesity, lack of exercise, a high sodium diet, and alcohol consumption can all contribute to hypertension.1,5,6,20,21 Dietary sodium in particular has significant adverse effects. Reducing dietary sodium not only reduces mortality, but has positive cardiovascular effects separate from blood pressure reduction, such as improved endothelium-dependent vasodilation.22-24
Medications including nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, sympathomimetics, glucocorticoids, and black licorice (found in some herbal supplements) may all raise blood pressure.5 Medications and other substances associated with increased blood pressure are listed in the TABLE. A search for such products, with changes or discontinuations that are clinically appropriate, should be part of any evaluation for resistant hypertension.
CASE 2 Ms. Stevens is a 30-year-old woman who was diagnosed with high blood pressure 7 months ago. She is currently taking triamterene-HCTZ 37.5/25 mg daily, amlodipine 10 mg daily, and metoprolol succinate 100 mg daily. She is compliant with medication, sticks to a low-sodium diet, and exercises 5 days a week. She does not drink alcohol. A review of her chart tells you her baseline serum chemistries, chest x-ray, and urinalysis are all normal. Today’s blood pressure taken in the sitting position after a 5-minute rest is 160/92 mm Hg. How should you proceed?
TABLE
Medications and other agents that may cause hypertension
| • Alcohol | • Cyclosporine | • Nicotine |
| • Antidepressants | • Erythropoietin | • NSAIDs |
| • Buspirone (Buspar) | • Estrogen preparations | • St. John’s wort |
| • Cocaine | • Licorice | • Tyramine-containing foods |
| • Corticosteroids | • Metoclopramide (Reglan) | |
| NSAIDs, nonsteroidal anti-infiammatory drugs. | ||
| Source: Chobanian A, et al. Hypertension. 2003.1 | ||
Is it resistant hypertension? Look for clues
You go over Ms. Stevens’ history carefully. Her hypertension medications should be adequate, and she is compliant with the prescribed regimen. Lifestyle factors are clearly not to blame: She’s not obese, she follows a low-sodium diet, doesn’t drink or smoke, and gets plenty of exercise. You ask her about other medications or over-the-counter supplements she takes, and nothing on her list raises a red flag. This doesn’t seem to be pseudo-resistance, and though you’re aware that only about 5% of cases of hypertension can be attributed to secondary causes, you think Ms. Stevens may be one of those patients.25
Numerous causes of secondary hypertension exist, and evaluations for such causes should be considered in all patients with resistant hypertension. Renal artery stenosis and pheochromocytoma are the most well-known causes, but less well known but significant contributors are obstructive sleep apnea and hyperaldosteronism.1,6,26,27
The relationship between obstructive sleep apnea and hypertension is not clear, and most of the studies linking the 2 conditions are population based.28 Nevertheless, because studies show that continuous positive airway pressure (CPAP) does improve blood pressure control in patients with obstructive sleep apnea, it is appropriate to investigate patients with resistant hypertension for this condition.29
Aldosterone’s role in resistant hypertension appears to be greatest in those with insulin resistance. The mechanism appears to be amplified sodium retention resulting in increased volume expansion, negative effects on oxidative stress, and elevated inflammation.27 Many patients with hypertension also have insulin resistance, so testing for hyperaldosteronism should be part of your investigation.
Test, and as necessary, test some more
Taking into consideration that 2 of the more common causes of secondary hypertension are obstructive sleep apnea and renal artery stenosis, you schedule an overnight sleep study for Ms. Stevens and a magnetic resonance arteriogram of the kidneys.26,30 (For more on the diagnostic tests and treatments for secondary causes of resistant hypertension, see the ALGORITHM.)
Reconsider medications. Ms. Stevens is already receiving the maximum dose of amlodipine, so you increase her metoprolol succinate to 200 mg daily and ask her to return in 1 month after the results of her tests come in.
Change medications and keep testing. At her next visit, Ms. Stevens’ blood pressure is 150/88 mm Hg, and her pulse rate is 64. Results of her overnight sleep study and magnetic resonance arteriogram are normal. At this juncture, with her work-up for common secondary causes of hypertension negative, you consider changes in her medication regimen. Because her pulse rate of 64 rules out any increase in the metoprolol, you decide to add lisinopril-HCTZ 10/12.5 mg to her regimen and discontinue her triamterene-HCTZ. Because her blood pressure is still elevated at this visit, you schedule additional testing to look for other secondary causes.
More tests, higher doses. One month later, Ms. Stevens returns with a blood pressure of 146/88 mm Hg. Appropriate testing for primary aldosteronism, pheochromocytoma, Cushing’s disease, and coarctation are all normal. Her lisinopril-HCTZ dose is increased to 20/12.5 mg, and when she returns 1 month later her blood pressure reading is 138/88 mm Hg.
You conclude that she is a patient with hard-to-control hypertension with no underlying cause who requires a significant amount of medication. That is not an uncommon situation. Although her blood pressure is now controlled to an appropriate level, you make a chart notation to consider referral to a hypertension specialist if her blood pressure become elevated again and treatment changes are not effective.6
ALGORITHM
Hard-to-control hypertension? This treatment algorithm can help
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CPAP, continuous positive airway pressure; CT, computed tomography; GFR, glomerular filtration rate; TSH, thyroid-stimulating hormone.
Adapted from: Calhoun DA, et al. Hypertension. 2008.6
Another consideration: Pseudohypertension
This uncommon condition sometimes occurs in elderly patients who suffer from a stiffened or thickened brachial artery.1 Because the blood pressure cuff cannot compress the artery, blood pressure readings overestimate true arterial pressure. The condition should be considered in patients when increased doses of medication fail to achieve the desired response, particularly in patients who exhibit postural hypotension.1
This was not a likely explanation for Ms. Stevens, however, given the clinical scenario and her young age.
CORRESPONDENCE Randy Wexler, MD, MPH, B0902B Cramblett Hall, 456 W 10th Avenue, Columbus, OH 43210; randy.wexler@osumc.edu
1. Chobanian A, Bakris GL, Black HR, et al. Seventh Report of The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7). Hypertension. 2003;42:1206-1252.
2. Fields L, Burt V, Cutler J, et al. The burden of adult hypertension in the United States 1999-2000: A rising tide. Hypertension. 2004;44:1-7.
3. Fang J, Alderman MH, Keenan NL, et al. Hypertension control at physicians’ offices in the United States. Am J Hypertens. 2008;21:136-142.
4. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics–2007 update. Circulation. 2007;115:e69-e171.
5. Sarafidis PA, Bakris GL. Resistant hypertension: an overview of evaluation and treatment. J Am Coll Cardiol. 2008;52:1749-1757.
6. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403-1419.
7. Phillips LS, Branch WT, Book CB, et al. Clinical inertia. Ann Intern Med. 2001;135:825-834.
8. Van Wijk BL, Klungel OH, Heerdink ER, et al. Rate and determinants of 10-year persistence with antihypertensive drugs. J Hypertens. 2005;23:2101-2107.
9. Wexler R, Pleister A, Feldman D. Sociology meets genetics: sociogenetic implications for future management of hypertension and heart failure. Curr Treat Options Cardiovasc Med. 2009;11:305-315.
10. Ogedegbe G, Pickering TG, Clemow L, et al. The misdiagnosis of hypertension: the role of patient anxiety. Arch Intern Med. 2008;168:2459-2465.
11. Dawes MG, Bartlett G, Coats AJ, et al. Comparing the effects of white coat hypertension and sustained hypertension on mortality in a UK primary care setting. Ann Fam Med. 2008;6:390-396.
12. Pierdomenico SD, Lapenna D, Bucci A, et al. Cardiovascular outcome in treated hypertensive patients with responder, masked, false resistant, and true resistant hypertension. Am J Hypertens. 2005;18:1422-1428.
13. Verberk WJ, Kroon AA, Kessels AGH, et al. Home blood pressure monitoring: a systematic review. J Am Coll Cardiol. 2005;46:743-751.
14. Pickering TG, Miller NH, Ogedegbe G, et al. AHA/ASH/PCNA scientific statement. Call to action on use and reimbursement for home blood pressure monitoring. Hypertension. 2008;52:10-29.
15. O’Brien E. Ambulatory blood pressure measurement: the case for implementation in primary care. Hypertension. 2008;51:1435-1441.
16. O’Brien E, Asmar R, Beilin L, et al. On behalf of the European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension recommendations for conventional ambulatory and home blood pressure measurements. J Hypertens. 2003;21:821-848.
17. Mourad A, Carney S, Gillies A, et al. Arm position and blood pressure: a risk factor for hypertension. J Hum Hypertens. 2003;17:389-395.
18. Myers MG. Automated blood pressure measurement in routine clinical practice. Blood Press Monit. 2006;11:59-62.
19. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce white coat hypertension. J Hypertens. 2009;27:280-286.
20. He J, Paul J, Whelton P, Appel L, et al. Long-term effects of weight loss and dietary sodium reduction on incidence of hypertension. Hypertension. 2000;35:544-549.
21. PREMIER Collaborative Research Writing Group. Effects of comprehensive lifestyle modification on blood pressure control. JAMA. 2003;289:2083-2093.
22. Cook NR, Cutler JA, Obarzanek E, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP). BMJ. 2007;334:885-888.
23. Dickinson BD, Havas S. Reducing the population burden of cardiovascular disease by reducing sodium intake. Arch Intern Med. 2007;167:1460-1468.
24. Li J, White J, Guo L, et al. Salt inactivates endothelial nitric oxide synthase in endothelial cells. J Nutr. 2009;139:1-5.
25. Beevers G, Lip G, O’Brien E. ABCs of hypertension: the pathophysiology of hypertension. BMJ. 2001;322:912-916.
26. Peppard PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378-1384.
27. Sowers JR, Whaley-Connell A, Epstein M. Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med. 2009;150:776-783.
28. Young T, Peppard P, Palta M, et al. Population-based study of sleep-disordered breathing as a risk factor for hypertension. Arch Intern Med. 1997;157:1746-1752.
29. Haentjens P, Van Meerhaeghe A, Moscariello A. The impact of continuous positive airway pressure on blood pressure in patients with obstructive sleep apnea syndrome: evidence from a meta-analysis of placebo-controlled randomized trials. Arch Intern Med. 2007;167:757-764.
30. Kawashima A, Francis IR, Baumgarten DA, et al. For the Expert Panel on Urologic Imaging. Renovascular hypertension. Reston, Va: American College of Radiology; 2007. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=11590&nbr=6003. Accessed April 4, 2009.
1. Chobanian A, Bakris GL, Black HR, et al. Seventh Report of The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7). Hypertension. 2003;42:1206-1252.
2. Fields L, Burt V, Cutler J, et al. The burden of adult hypertension in the United States 1999-2000: A rising tide. Hypertension. 2004;44:1-7.
3. Fang J, Alderman MH, Keenan NL, et al. Hypertension control at physicians’ offices in the United States. Am J Hypertens. 2008;21:136-142.
4. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics–2007 update. Circulation. 2007;115:e69-e171.
5. Sarafidis PA, Bakris GL. Resistant hypertension: an overview of evaluation and treatment. J Am Coll Cardiol. 2008;52:1749-1757.
6. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403-1419.
7. Phillips LS, Branch WT, Book CB, et al. Clinical inertia. Ann Intern Med. 2001;135:825-834.
8. Van Wijk BL, Klungel OH, Heerdink ER, et al. Rate and determinants of 10-year persistence with antihypertensive drugs. J Hypertens. 2005;23:2101-2107.
9. Wexler R, Pleister A, Feldman D. Sociology meets genetics: sociogenetic implications for future management of hypertension and heart failure. Curr Treat Options Cardiovasc Med. 2009;11:305-315.
10. Ogedegbe G, Pickering TG, Clemow L, et al. The misdiagnosis of hypertension: the role of patient anxiety. Arch Intern Med. 2008;168:2459-2465.
11. Dawes MG, Bartlett G, Coats AJ, et al. Comparing the effects of white coat hypertension and sustained hypertension on mortality in a UK primary care setting. Ann Fam Med. 2008;6:390-396.
12. Pierdomenico SD, Lapenna D, Bucci A, et al. Cardiovascular outcome in treated hypertensive patients with responder, masked, false resistant, and true resistant hypertension. Am J Hypertens. 2005;18:1422-1428.
13. Verberk WJ, Kroon AA, Kessels AGH, et al. Home blood pressure monitoring: a systematic review. J Am Coll Cardiol. 2005;46:743-751.
14. Pickering TG, Miller NH, Ogedegbe G, et al. AHA/ASH/PCNA scientific statement. Call to action on use and reimbursement for home blood pressure monitoring. Hypertension. 2008;52:10-29.
15. O’Brien E. Ambulatory blood pressure measurement: the case for implementation in primary care. Hypertension. 2008;51:1435-1441.
16. O’Brien E, Asmar R, Beilin L, et al. On behalf of the European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension recommendations for conventional ambulatory and home blood pressure measurements. J Hypertens. 2003;21:821-848.
17. Mourad A, Carney S, Gillies A, et al. Arm position and blood pressure: a risk factor for hypertension. J Hum Hypertens. 2003;17:389-395.
18. Myers MG. Automated blood pressure measurement in routine clinical practice. Blood Press Monit. 2006;11:59-62.
19. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce white coat hypertension. J Hypertens. 2009;27:280-286.
20. He J, Paul J, Whelton P, Appel L, et al. Long-term effects of weight loss and dietary sodium reduction on incidence of hypertension. Hypertension. 2000;35:544-549.
21. PREMIER Collaborative Research Writing Group. Effects of comprehensive lifestyle modification on blood pressure control. JAMA. 2003;289:2083-2093.
22. Cook NR, Cutler JA, Obarzanek E, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP). BMJ. 2007;334:885-888.
23. Dickinson BD, Havas S. Reducing the population burden of cardiovascular disease by reducing sodium intake. Arch Intern Med. 2007;167:1460-1468.
24. Li J, White J, Guo L, et al. Salt inactivates endothelial nitric oxide synthase in endothelial cells. J Nutr. 2009;139:1-5.
25. Beevers G, Lip G, O’Brien E. ABCs of hypertension: the pathophysiology of hypertension. BMJ. 2001;322:912-916.
26. Peppard PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378-1384.
27. Sowers JR, Whaley-Connell A, Epstein M. Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med. 2009;150:776-783.
28. Young T, Peppard P, Palta M, et al. Population-based study of sleep-disordered breathing as a risk factor for hypertension. Arch Intern Med. 1997;157:1746-1752.
29. Haentjens P, Van Meerhaeghe A, Moscariello A. The impact of continuous positive airway pressure on blood pressure in patients with obstructive sleep apnea syndrome: evidence from a meta-analysis of placebo-controlled randomized trials. Arch Intern Med. 2007;167:757-764.
30. Kawashima A, Francis IR, Baumgarten DA, et al. For the Expert Panel on Urologic Imaging. Renovascular hypertension. Reston, Va: American College of Radiology; 2007. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=11590&nbr=6003. Accessed April 4, 2009.