User login
At 6 Months Postcesarean, 3% Have Chronic Pain
MONTEREY, CALIF. – Chronic pain after cesarean delivery is uncommon and generally mild, new data show. Additionally, women undergoing repeat cesarean do not have worse pain than their counterparts undergoing primary cesarean.
These were among the key findings of a pair of prospective longitudinal studies that investigators reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
The studies took place among healthy women from Brazil and the United States who were having scheduled elective cesarean deliveries with no prior labor, using standardized spinal anesthesia, surgical techniques, and multimodal postoperative analgesia.
Prevalence and description of chronic pain
In the first study, investigators led by Dr. Clemens M. Ortner of the department of anesthesiology and pain medicine at the University of Washington Medical Center in Seattle, followed 360 women from São Paulo, Brazil.
They used two tools recommended by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT), which is endorsed by the Food and Drug Administration: the Brief Pain Inventory (BPI), which captures the effect of pain on physical functioning, and the Short-Form McGill Pain Questionnaire 2 (SF-MPQ-2), which evaluates the nature of pain using 22 descriptors that are grouped into four overarching types of pain.
The women were a mean 31 years. For the large majority (70%), the cesarean was their first. Mean surgical time was 40 minutes.
Results with the BPI showed that 3% of women had pain at 6 months, Dr. Ortner reported. However, in the majority of cases, the pain was rated as mild.
Data from the SF-MPQ-2 suggested that the pain was most often of the neuropathic type and seldom of the continuous, intermittent, or affective types.
The leading descriptor the women selected for the pain, cited by 38% of those affected, was numbness. "Some would actually even argue [that numbness] does not qualify as a pain symptom," commented Dr. Ortner. Descriptors such as throbbing, tender, cramping, stabbing, and piercing were rarely used.
"This is the first prospective longitudinal study to characterize chronic pain after cesarean delivery using the SF-MPQ-2, and to our knowledge, is actually the first study that uses the SF-MPQ-2 that tries to characterize chronic postoperative pain," Dr. Ortner noted.
"Our incidence of chronic pain was very low at 6 months: It was 3%. However, this population was a very healthy population that had no other risk factors, like prior sensitization or other chronic pain syndromes," he cautioned.
"We can take this information from our study as a control for future analysis where we can use the SF-MPQ-2 to investigate chronic pain in high-risk populations undergoing cesarean delivery," he added.
Dr. Kenneth E. Nelson, session moderator and an obstetrical anesthesiologist at Wake Forest Baptist Medical Center in Winston Salem, N.C., wondered if the pain descriptors of the SF-MPQ-2 had the same meaning in the Brazilian context. "Some of those words are pretty esoteric. How culturally sensitive are they? Do you see a difference in different cultures using those words to describe pain, and is that potentially an issue with comparing one of these studies to another?" he asked.
"It is true that the SF-MPQ-2 was validated in an English-speaking population. However, these descriptors have been retrieved from a very, very large population of patients, how they describe their pain," Dr. Ortner replied. Additionally, the questionnaire underwent a rigorous validation process, whereby it was translated for a Portuguese-speaking population and then translated back to English. "However, of course, cultural differences can have an impact on these results, yes."
Pain with primary vs. repeat cesarean
In the second study – the only prospective evaluation of pain among healthy women after primary vs. repeat cesareans – a team led by Dr. Ruth Landau studied 451 women from São Paulo, Brazil, and Seattle.
Subsequent cesarean deliveries are noteworthy among surgical procedures in that surgeons typically go through the same scar again, a process that some speculate may contribute to greater pain, she noted.
"The hypothesis is that central sensitization as can be elicited by scar hyperalgesia after a previous cesarean section could result in increased pain if the surgery is repeated," she explained. "And the clinical implications for that would be that analgesic regimens may need to be adapted in women undergoing a repeat cesarean delivery, and that we should tailor our postoperative analgesia based on whether it’s a primary or repeat cesarean section."
Overall, 67% of the women studied were undergoing a primary cesarean delivery, whereas 33% were undergoing a repeat cesarean delivery. They had a mean age of about 30 years.
Results on the BPI showed relatively low scores (2-5 points on a 10-point scale) for pain – at rest, while sitting, and specifically for uterine cramping – at 12 hours and at 24 hours postoperatively, with no significant differences between the primary and repeat cesarean groups, reported Dr. Landau, who is professor and director of obstetric anesthesiology and clinical genetics, anesthesiology, and pain medicine at the University of Washington Medical Center.
At 48 hours, there was a trend whereby women undergoing repeat cesarean had a higher level of pain while at rest relative to women undergoing primary cesarean, but pain while sitting, uterine cramping, wound hyperalgesia, and opioid use were essentially the same.
There also were no significant differences between the primary and repeat cesarean groups with respect to average pain in the past week, worst pain in the past week, and pain now, at either 8 weeks or at 6 months postoperatively.
"In this cohort of healthy women undergoing an elective cesarean delivery under what is considered the best modality to have good intraoperative anesthesia and postoperative analgesia, we did not find a relevant difference in pain scores or analgesic use in the first 48 hours. Therefore, I cannot recommend we should change our practice in giving everybody the same thing," said Dr. Landau.
"I would however caution that we shouldn’t yet extrapolate these results to other clinical contexts, in particular, women who have high risk for pain, prior pain, a nonelective primary cesarean delivery, or women [operated on] with different surgical techniques," she added. "And I would propose ... that we do look into scar hyperalgesia in those who have had a previous cesarean delivery, in trying to tease out women who are potentially at risk for more severe pain postoperatively."
Session moderator Dr. Dennis C. Shay in a group anesthesia practice in San Diego asked, "Did you look at activity levels? I would imagine with a repeat C-section, they have a young child, so if the child is visiting, maybe they are getting up and walking around a lot more than if it was just their first child. And maybe that would make a difference."
It would be challenging to interpret how activity data relate to pain data, Dr. Landau replied. For example, women could be less active because they have more pain or because they are more comfortable.
Dr. Ortner and Dr. Landau said they had no relevant financial conflicts of interest.
MONTEREY, CALIF. – Chronic pain after cesarean delivery is uncommon and generally mild, new data show. Additionally, women undergoing repeat cesarean do not have worse pain than their counterparts undergoing primary cesarean.
These were among the key findings of a pair of prospective longitudinal studies that investigators reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
The studies took place among healthy women from Brazil and the United States who were having scheduled elective cesarean deliveries with no prior labor, using standardized spinal anesthesia, surgical techniques, and multimodal postoperative analgesia.
Prevalence and description of chronic pain
In the first study, investigators led by Dr. Clemens M. Ortner of the department of anesthesiology and pain medicine at the University of Washington Medical Center in Seattle, followed 360 women from São Paulo, Brazil.
They used two tools recommended by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT), which is endorsed by the Food and Drug Administration: the Brief Pain Inventory (BPI), which captures the effect of pain on physical functioning, and the Short-Form McGill Pain Questionnaire 2 (SF-MPQ-2), which evaluates the nature of pain using 22 descriptors that are grouped into four overarching types of pain.
The women were a mean 31 years. For the large majority (70%), the cesarean was their first. Mean surgical time was 40 minutes.
Results with the BPI showed that 3% of women had pain at 6 months, Dr. Ortner reported. However, in the majority of cases, the pain was rated as mild.
Data from the SF-MPQ-2 suggested that the pain was most often of the neuropathic type and seldom of the continuous, intermittent, or affective types.
The leading descriptor the women selected for the pain, cited by 38% of those affected, was numbness. "Some would actually even argue [that numbness] does not qualify as a pain symptom," commented Dr. Ortner. Descriptors such as throbbing, tender, cramping, stabbing, and piercing were rarely used.
"This is the first prospective longitudinal study to characterize chronic pain after cesarean delivery using the SF-MPQ-2, and to our knowledge, is actually the first study that uses the SF-MPQ-2 that tries to characterize chronic postoperative pain," Dr. Ortner noted.
"Our incidence of chronic pain was very low at 6 months: It was 3%. However, this population was a very healthy population that had no other risk factors, like prior sensitization or other chronic pain syndromes," he cautioned.
"We can take this information from our study as a control for future analysis where we can use the SF-MPQ-2 to investigate chronic pain in high-risk populations undergoing cesarean delivery," he added.
Dr. Kenneth E. Nelson, session moderator and an obstetrical anesthesiologist at Wake Forest Baptist Medical Center in Winston Salem, N.C., wondered if the pain descriptors of the SF-MPQ-2 had the same meaning in the Brazilian context. "Some of those words are pretty esoteric. How culturally sensitive are they? Do you see a difference in different cultures using those words to describe pain, and is that potentially an issue with comparing one of these studies to another?" he asked.
"It is true that the SF-MPQ-2 was validated in an English-speaking population. However, these descriptors have been retrieved from a very, very large population of patients, how they describe their pain," Dr. Ortner replied. Additionally, the questionnaire underwent a rigorous validation process, whereby it was translated for a Portuguese-speaking population and then translated back to English. "However, of course, cultural differences can have an impact on these results, yes."
Pain with primary vs. repeat cesarean
In the second study – the only prospective evaluation of pain among healthy women after primary vs. repeat cesareans – a team led by Dr. Ruth Landau studied 451 women from São Paulo, Brazil, and Seattle.
Subsequent cesarean deliveries are noteworthy among surgical procedures in that surgeons typically go through the same scar again, a process that some speculate may contribute to greater pain, she noted.
"The hypothesis is that central sensitization as can be elicited by scar hyperalgesia after a previous cesarean section could result in increased pain if the surgery is repeated," she explained. "And the clinical implications for that would be that analgesic regimens may need to be adapted in women undergoing a repeat cesarean delivery, and that we should tailor our postoperative analgesia based on whether it’s a primary or repeat cesarean section."
Overall, 67% of the women studied were undergoing a primary cesarean delivery, whereas 33% were undergoing a repeat cesarean delivery. They had a mean age of about 30 years.
Results on the BPI showed relatively low scores (2-5 points on a 10-point scale) for pain – at rest, while sitting, and specifically for uterine cramping – at 12 hours and at 24 hours postoperatively, with no significant differences between the primary and repeat cesarean groups, reported Dr. Landau, who is professor and director of obstetric anesthesiology and clinical genetics, anesthesiology, and pain medicine at the University of Washington Medical Center.
At 48 hours, there was a trend whereby women undergoing repeat cesarean had a higher level of pain while at rest relative to women undergoing primary cesarean, but pain while sitting, uterine cramping, wound hyperalgesia, and opioid use were essentially the same.
There also were no significant differences between the primary and repeat cesarean groups with respect to average pain in the past week, worst pain in the past week, and pain now, at either 8 weeks or at 6 months postoperatively.
"In this cohort of healthy women undergoing an elective cesarean delivery under what is considered the best modality to have good intraoperative anesthesia and postoperative analgesia, we did not find a relevant difference in pain scores or analgesic use in the first 48 hours. Therefore, I cannot recommend we should change our practice in giving everybody the same thing," said Dr. Landau.
"I would however caution that we shouldn’t yet extrapolate these results to other clinical contexts, in particular, women who have high risk for pain, prior pain, a nonelective primary cesarean delivery, or women [operated on] with different surgical techniques," she added. "And I would propose ... that we do look into scar hyperalgesia in those who have had a previous cesarean delivery, in trying to tease out women who are potentially at risk for more severe pain postoperatively."
Session moderator Dr. Dennis C. Shay in a group anesthesia practice in San Diego asked, "Did you look at activity levels? I would imagine with a repeat C-section, they have a young child, so if the child is visiting, maybe they are getting up and walking around a lot more than if it was just their first child. And maybe that would make a difference."
It would be challenging to interpret how activity data relate to pain data, Dr. Landau replied. For example, women could be less active because they have more pain or because they are more comfortable.
Dr. Ortner and Dr. Landau said they had no relevant financial conflicts of interest.
MONTEREY, CALIF. – Chronic pain after cesarean delivery is uncommon and generally mild, new data show. Additionally, women undergoing repeat cesarean do not have worse pain than their counterparts undergoing primary cesarean.
These were among the key findings of a pair of prospective longitudinal studies that investigators reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
The studies took place among healthy women from Brazil and the United States who were having scheduled elective cesarean deliveries with no prior labor, using standardized spinal anesthesia, surgical techniques, and multimodal postoperative analgesia.
Prevalence and description of chronic pain
In the first study, investigators led by Dr. Clemens M. Ortner of the department of anesthesiology and pain medicine at the University of Washington Medical Center in Seattle, followed 360 women from São Paulo, Brazil.
They used two tools recommended by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT), which is endorsed by the Food and Drug Administration: the Brief Pain Inventory (BPI), which captures the effect of pain on physical functioning, and the Short-Form McGill Pain Questionnaire 2 (SF-MPQ-2), which evaluates the nature of pain using 22 descriptors that are grouped into four overarching types of pain.
The women were a mean 31 years. For the large majority (70%), the cesarean was their first. Mean surgical time was 40 minutes.
Results with the BPI showed that 3% of women had pain at 6 months, Dr. Ortner reported. However, in the majority of cases, the pain was rated as mild.
Data from the SF-MPQ-2 suggested that the pain was most often of the neuropathic type and seldom of the continuous, intermittent, or affective types.
The leading descriptor the women selected for the pain, cited by 38% of those affected, was numbness. "Some would actually even argue [that numbness] does not qualify as a pain symptom," commented Dr. Ortner. Descriptors such as throbbing, tender, cramping, stabbing, and piercing were rarely used.
"This is the first prospective longitudinal study to characterize chronic pain after cesarean delivery using the SF-MPQ-2, and to our knowledge, is actually the first study that uses the SF-MPQ-2 that tries to characterize chronic postoperative pain," Dr. Ortner noted.
"Our incidence of chronic pain was very low at 6 months: It was 3%. However, this population was a very healthy population that had no other risk factors, like prior sensitization or other chronic pain syndromes," he cautioned.
"We can take this information from our study as a control for future analysis where we can use the SF-MPQ-2 to investigate chronic pain in high-risk populations undergoing cesarean delivery," he added.
Dr. Kenneth E. Nelson, session moderator and an obstetrical anesthesiologist at Wake Forest Baptist Medical Center in Winston Salem, N.C., wondered if the pain descriptors of the SF-MPQ-2 had the same meaning in the Brazilian context. "Some of those words are pretty esoteric. How culturally sensitive are they? Do you see a difference in different cultures using those words to describe pain, and is that potentially an issue with comparing one of these studies to another?" he asked.
"It is true that the SF-MPQ-2 was validated in an English-speaking population. However, these descriptors have been retrieved from a very, very large population of patients, how they describe their pain," Dr. Ortner replied. Additionally, the questionnaire underwent a rigorous validation process, whereby it was translated for a Portuguese-speaking population and then translated back to English. "However, of course, cultural differences can have an impact on these results, yes."
Pain with primary vs. repeat cesarean
In the second study – the only prospective evaluation of pain among healthy women after primary vs. repeat cesareans – a team led by Dr. Ruth Landau studied 451 women from São Paulo, Brazil, and Seattle.
Subsequent cesarean deliveries are noteworthy among surgical procedures in that surgeons typically go through the same scar again, a process that some speculate may contribute to greater pain, she noted.
"The hypothesis is that central sensitization as can be elicited by scar hyperalgesia after a previous cesarean section could result in increased pain if the surgery is repeated," she explained. "And the clinical implications for that would be that analgesic regimens may need to be adapted in women undergoing a repeat cesarean delivery, and that we should tailor our postoperative analgesia based on whether it’s a primary or repeat cesarean section."
Overall, 67% of the women studied were undergoing a primary cesarean delivery, whereas 33% were undergoing a repeat cesarean delivery. They had a mean age of about 30 years.
Results on the BPI showed relatively low scores (2-5 points on a 10-point scale) for pain – at rest, while sitting, and specifically for uterine cramping – at 12 hours and at 24 hours postoperatively, with no significant differences between the primary and repeat cesarean groups, reported Dr. Landau, who is professor and director of obstetric anesthesiology and clinical genetics, anesthesiology, and pain medicine at the University of Washington Medical Center.
At 48 hours, there was a trend whereby women undergoing repeat cesarean had a higher level of pain while at rest relative to women undergoing primary cesarean, but pain while sitting, uterine cramping, wound hyperalgesia, and opioid use were essentially the same.
There also were no significant differences between the primary and repeat cesarean groups with respect to average pain in the past week, worst pain in the past week, and pain now, at either 8 weeks or at 6 months postoperatively.
"In this cohort of healthy women undergoing an elective cesarean delivery under what is considered the best modality to have good intraoperative anesthesia and postoperative analgesia, we did not find a relevant difference in pain scores or analgesic use in the first 48 hours. Therefore, I cannot recommend we should change our practice in giving everybody the same thing," said Dr. Landau.
"I would however caution that we shouldn’t yet extrapolate these results to other clinical contexts, in particular, women who have high risk for pain, prior pain, a nonelective primary cesarean delivery, or women [operated on] with different surgical techniques," she added. "And I would propose ... that we do look into scar hyperalgesia in those who have had a previous cesarean delivery, in trying to tease out women who are potentially at risk for more severe pain postoperatively."
Session moderator Dr. Dennis C. Shay in a group anesthesia practice in San Diego asked, "Did you look at activity levels? I would imagine with a repeat C-section, they have a young child, so if the child is visiting, maybe they are getting up and walking around a lot more than if it was just their first child. And maybe that would make a difference."
It would be challenging to interpret how activity data relate to pain data, Dr. Landau replied. For example, women could be less active because they have more pain or because they are more comfortable.
Dr. Ortner and Dr. Landau said they had no relevant financial conflicts of interest.
FROM THE ANNUAL MEETING OF THE SOCIETY FOR OBSTETRIC ANESTHESIA AND PERINATOLOGY
Major Finding: Only 3% of women in the first study had pain at 6 months, and it was usually mild.
Data Source: Results were taken from one of a pair of prospective longitudinal studies. The first study was based on a cohort of 360 healthy women undergoing elective cesarean delivery with standardized spinal anesthesia, surgical techniques, and multimodal postoperative analgesia.
Disclosures: Dr. Ortner and Dr. Landau disclosed no relevant conflicts of interest.
Drug Combination Improved Local Analgesia After Cesarean
MONTEREY, CALIF. – Two drugs work better than one when it comes to reducing pain and inflammation with local therapy after cesarean delivery, researchers reported.
In a randomized trial of 60 women who used subcutaneous drug delivery, the area under the curve for postoperative pain scores while sitting was roughly 30% less and supplemental opioid requirements were roughly 40% less when the nonsteroidal anti-inflammatory drug ketorolac was added to bupivacaine. Wound exudate levels of the inflammatory markers interleukin-6 and -10 also were lower.
"Giving a low dose peripherally of nonsteroidal ketorolac has both an anti-inflammatory and an analgesic effect," commented lead author Dr. Brendan Carvalho, an anesthesiologist at Lucile Packard Children’s Hospital in Stanford, Calif.
"This suggests that there is a local mediation effect – this is not a systemic effect – and it may give birth to the whole concept of being able to give very small doses directly in the wound," he said at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
"You could even create a multimodal analgesic protocol with small doses of drugs that will not have the high side effects based on big systemic doses, and they can work exactly in the area that we know is most important for inflammation and pain propagation."
In contrast, there were no significant improvements in study outcomes when subcutaneous hydromorphone was added to bupivacaine. "This probably could have been anticipated if you look at the balance of the literature, looking at the efficacy of opioids and nonsteroidals peripherally administered," Dr. Carvalho said.
Session attendee Dr. David R. Gambling of the Sharp Mary Birch Hospital for Women in San Diego questioned the impact of the catheter used to deliver the drugs. "Do you think that having that foreign body in place affects the release of the mediators you were measuring, and if that’s the case, do you think patient movement and irritation of the foreign body could have had an effect on the result?" he asked.
The point is a good one, Dr. Carvalho acknowledged. However, "to be able to follow someone continuously [without a catheter in place] would require invasive [needle procedures] as well as punch biopsies. ... There’s sort of a long way to go, and maybe the whole idea behind this is to encourage people to think of better ways of doing this."
Dr. Andrea Fuller of the University of Colorado Hospital in Aurora, who also attended the session, said, "I’m wondering clinically how to use this. If you don’t have an ON-Q pump [to deliver the drug], are you doing things like asking your obstetricians to put some ketorolac in infiltrate right at the site, or even putting it in a TAP [transversus abdominus plane] block – it might be close enough."
"It’s way too early to say," Dr. Carvalho replied. "I am not recommending the use [of a nonsteroidal agent peripherally] yet, until we truly understand what these drugs are doing. ... It’s a growing area, and I think a few years from now, a lot of the drug administration will be where it should be as opposed to systemically."
The trial participants were 60 healthy women with term singleton pregnancies who underwent elective cesarean delivery with spinal anesthesia. The investigators placed elastomeric ON-Q pumps subcutaneously in the incisional wound to permit collection of wound exudate and instillation of agents.
The women were randomized equally into three groups given continuous subcutaneous instillation for 48 hours after surgery of bupivacaine at 10 mg/hr only (as an active control); bupivacaine plus ketorolac at 0.6 mg/hr; or bupivacaine plus hydromorphone at 0.04 mg/hr.
The drugs were intentionally "given in very small doses, which we believe would not be systemically effective, so it’s not a systemic absorption effect," Dr. Carvalho noted.
Pain intensity was measured at 4, 24, and 48 hours post surgery, both at rest and during activity, using the verbal pain scale, on which values range from 0 to 10. Wound exudate was collected at the same time points and assayed for a wide variety of cytokines.
On average, the women were about 32 years old and had a parity of 1. Eighty percent had had a previous cesarean delivery.
Trial results showed that the area under the curve for postoperative pain scores while sitting was approximately 250 for women given bupivacaine only, versus 175 for women given bupivacaine plus ketorolac (P = .018), Dr. Carvalho reported. There were no significant differences in pain scores while at rest.
Compared with bupivacaine alone, bupivacaine plus ketorolac was associated with lower levels of interleukin-6 (P = .012) and interleukin-10 (P = .004) in wound exudate.
Postoperative supplemental opioid analgesic use was approximately 25 mg of morphine equivalents for women in the bupivacaine-ketorolac group, compared with 40 mg for their counterparts in the bupivacaine-only group (P = .020).
None of the women had significant adverse events or study-related complications, and there were no hematomas, infections, or delays in wound healing. One woman developed a subincisional fluid collection.
"The majority of patients we enrolled had had previous cesarean deliveries, which may [have introduced] bias, as patients having second C-sections may respond differently from someone who is undergoing a cesarean for the first time," Dr. Carvalho acknowledged. Additionally, there was some "empiric guessing" involved in the selection of drug doses, and the study focused only on the acute inflammatory period.
"The next plan is to compare systemic versus peripheral administration of various other drugs, and to start understanding the mechanisms behind what is happening in the periphery," he concluded. "We have a very delicate balance where if we inhibit inflammation too much, then we have delayed wound healing. If we accelerate it too much, we might get hypertrophic scarring. So it’s a delicate balance that we can intervene on and maybe improve analgesia, but we mustn’t affect the balance of wound healing."
Dr. Carvalho disclosed that he has a relationship with I-Flow, manufacturer of the pump used in the study.
MONTEREY, CALIF. – Two drugs work better than one when it comes to reducing pain and inflammation with local therapy after cesarean delivery, researchers reported.
In a randomized trial of 60 women who used subcutaneous drug delivery, the area under the curve for postoperative pain scores while sitting was roughly 30% less and supplemental opioid requirements were roughly 40% less when the nonsteroidal anti-inflammatory drug ketorolac was added to bupivacaine. Wound exudate levels of the inflammatory markers interleukin-6 and -10 also were lower.
"Giving a low dose peripherally of nonsteroidal ketorolac has both an anti-inflammatory and an analgesic effect," commented lead author Dr. Brendan Carvalho, an anesthesiologist at Lucile Packard Children’s Hospital in Stanford, Calif.
"This suggests that there is a local mediation effect – this is not a systemic effect – and it may give birth to the whole concept of being able to give very small doses directly in the wound," he said at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
"You could even create a multimodal analgesic protocol with small doses of drugs that will not have the high side effects based on big systemic doses, and they can work exactly in the area that we know is most important for inflammation and pain propagation."
In contrast, there were no significant improvements in study outcomes when subcutaneous hydromorphone was added to bupivacaine. "This probably could have been anticipated if you look at the balance of the literature, looking at the efficacy of opioids and nonsteroidals peripherally administered," Dr. Carvalho said.
Session attendee Dr. David R. Gambling of the Sharp Mary Birch Hospital for Women in San Diego questioned the impact of the catheter used to deliver the drugs. "Do you think that having that foreign body in place affects the release of the mediators you were measuring, and if that’s the case, do you think patient movement and irritation of the foreign body could have had an effect on the result?" he asked.
The point is a good one, Dr. Carvalho acknowledged. However, "to be able to follow someone continuously [without a catheter in place] would require invasive [needle procedures] as well as punch biopsies. ... There’s sort of a long way to go, and maybe the whole idea behind this is to encourage people to think of better ways of doing this."
Dr. Andrea Fuller of the University of Colorado Hospital in Aurora, who also attended the session, said, "I’m wondering clinically how to use this. If you don’t have an ON-Q pump [to deliver the drug], are you doing things like asking your obstetricians to put some ketorolac in infiltrate right at the site, or even putting it in a TAP [transversus abdominus plane] block – it might be close enough."
"It’s way too early to say," Dr. Carvalho replied. "I am not recommending the use [of a nonsteroidal agent peripherally] yet, until we truly understand what these drugs are doing. ... It’s a growing area, and I think a few years from now, a lot of the drug administration will be where it should be as opposed to systemically."
The trial participants were 60 healthy women with term singleton pregnancies who underwent elective cesarean delivery with spinal anesthesia. The investigators placed elastomeric ON-Q pumps subcutaneously in the incisional wound to permit collection of wound exudate and instillation of agents.
The women were randomized equally into three groups given continuous subcutaneous instillation for 48 hours after surgery of bupivacaine at 10 mg/hr only (as an active control); bupivacaine plus ketorolac at 0.6 mg/hr; or bupivacaine plus hydromorphone at 0.04 mg/hr.
The drugs were intentionally "given in very small doses, which we believe would not be systemically effective, so it’s not a systemic absorption effect," Dr. Carvalho noted.
Pain intensity was measured at 4, 24, and 48 hours post surgery, both at rest and during activity, using the verbal pain scale, on which values range from 0 to 10. Wound exudate was collected at the same time points and assayed for a wide variety of cytokines.
On average, the women were about 32 years old and had a parity of 1. Eighty percent had had a previous cesarean delivery.
Trial results showed that the area under the curve for postoperative pain scores while sitting was approximately 250 for women given bupivacaine only, versus 175 for women given bupivacaine plus ketorolac (P = .018), Dr. Carvalho reported. There were no significant differences in pain scores while at rest.
Compared with bupivacaine alone, bupivacaine plus ketorolac was associated with lower levels of interleukin-6 (P = .012) and interleukin-10 (P = .004) in wound exudate.
Postoperative supplemental opioid analgesic use was approximately 25 mg of morphine equivalents for women in the bupivacaine-ketorolac group, compared with 40 mg for their counterparts in the bupivacaine-only group (P = .020).
None of the women had significant adverse events or study-related complications, and there were no hematomas, infections, or delays in wound healing. One woman developed a subincisional fluid collection.
"The majority of patients we enrolled had had previous cesarean deliveries, which may [have introduced] bias, as patients having second C-sections may respond differently from someone who is undergoing a cesarean for the first time," Dr. Carvalho acknowledged. Additionally, there was some "empiric guessing" involved in the selection of drug doses, and the study focused only on the acute inflammatory period.
"The next plan is to compare systemic versus peripheral administration of various other drugs, and to start understanding the mechanisms behind what is happening in the periphery," he concluded. "We have a very delicate balance where if we inhibit inflammation too much, then we have delayed wound healing. If we accelerate it too much, we might get hypertrophic scarring. So it’s a delicate balance that we can intervene on and maybe improve analgesia, but we mustn’t affect the balance of wound healing."
Dr. Carvalho disclosed that he has a relationship with I-Flow, manufacturer of the pump used in the study.
MONTEREY, CALIF. – Two drugs work better than one when it comes to reducing pain and inflammation with local therapy after cesarean delivery, researchers reported.
In a randomized trial of 60 women who used subcutaneous drug delivery, the area under the curve for postoperative pain scores while sitting was roughly 30% less and supplemental opioid requirements were roughly 40% less when the nonsteroidal anti-inflammatory drug ketorolac was added to bupivacaine. Wound exudate levels of the inflammatory markers interleukin-6 and -10 also were lower.
"Giving a low dose peripherally of nonsteroidal ketorolac has both an anti-inflammatory and an analgesic effect," commented lead author Dr. Brendan Carvalho, an anesthesiologist at Lucile Packard Children’s Hospital in Stanford, Calif.
"This suggests that there is a local mediation effect – this is not a systemic effect – and it may give birth to the whole concept of being able to give very small doses directly in the wound," he said at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
"You could even create a multimodal analgesic protocol with small doses of drugs that will not have the high side effects based on big systemic doses, and they can work exactly in the area that we know is most important for inflammation and pain propagation."
In contrast, there were no significant improvements in study outcomes when subcutaneous hydromorphone was added to bupivacaine. "This probably could have been anticipated if you look at the balance of the literature, looking at the efficacy of opioids and nonsteroidals peripherally administered," Dr. Carvalho said.
Session attendee Dr. David R. Gambling of the Sharp Mary Birch Hospital for Women in San Diego questioned the impact of the catheter used to deliver the drugs. "Do you think that having that foreign body in place affects the release of the mediators you were measuring, and if that’s the case, do you think patient movement and irritation of the foreign body could have had an effect on the result?" he asked.
The point is a good one, Dr. Carvalho acknowledged. However, "to be able to follow someone continuously [without a catheter in place] would require invasive [needle procedures] as well as punch biopsies. ... There’s sort of a long way to go, and maybe the whole idea behind this is to encourage people to think of better ways of doing this."
Dr. Andrea Fuller of the University of Colorado Hospital in Aurora, who also attended the session, said, "I’m wondering clinically how to use this. If you don’t have an ON-Q pump [to deliver the drug], are you doing things like asking your obstetricians to put some ketorolac in infiltrate right at the site, or even putting it in a TAP [transversus abdominus plane] block – it might be close enough."
"It’s way too early to say," Dr. Carvalho replied. "I am not recommending the use [of a nonsteroidal agent peripherally] yet, until we truly understand what these drugs are doing. ... It’s a growing area, and I think a few years from now, a lot of the drug administration will be where it should be as opposed to systemically."
The trial participants were 60 healthy women with term singleton pregnancies who underwent elective cesarean delivery with spinal anesthesia. The investigators placed elastomeric ON-Q pumps subcutaneously in the incisional wound to permit collection of wound exudate and instillation of agents.
The women were randomized equally into three groups given continuous subcutaneous instillation for 48 hours after surgery of bupivacaine at 10 mg/hr only (as an active control); bupivacaine plus ketorolac at 0.6 mg/hr; or bupivacaine plus hydromorphone at 0.04 mg/hr.
The drugs were intentionally "given in very small doses, which we believe would not be systemically effective, so it’s not a systemic absorption effect," Dr. Carvalho noted.
Pain intensity was measured at 4, 24, and 48 hours post surgery, both at rest and during activity, using the verbal pain scale, on which values range from 0 to 10. Wound exudate was collected at the same time points and assayed for a wide variety of cytokines.
On average, the women were about 32 years old and had a parity of 1. Eighty percent had had a previous cesarean delivery.
Trial results showed that the area under the curve for postoperative pain scores while sitting was approximately 250 for women given bupivacaine only, versus 175 for women given bupivacaine plus ketorolac (P = .018), Dr. Carvalho reported. There were no significant differences in pain scores while at rest.
Compared with bupivacaine alone, bupivacaine plus ketorolac was associated with lower levels of interleukin-6 (P = .012) and interleukin-10 (P = .004) in wound exudate.
Postoperative supplemental opioid analgesic use was approximately 25 mg of morphine equivalents for women in the bupivacaine-ketorolac group, compared with 40 mg for their counterparts in the bupivacaine-only group (P = .020).
None of the women had significant adverse events or study-related complications, and there were no hematomas, infections, or delays in wound healing. One woman developed a subincisional fluid collection.
"The majority of patients we enrolled had had previous cesarean deliveries, which may [have introduced] bias, as patients having second C-sections may respond differently from someone who is undergoing a cesarean for the first time," Dr. Carvalho acknowledged. Additionally, there was some "empiric guessing" involved in the selection of drug doses, and the study focused only on the acute inflammatory period.
"The next plan is to compare systemic versus peripheral administration of various other drugs, and to start understanding the mechanisms behind what is happening in the periphery," he concluded. "We have a very delicate balance where if we inhibit inflammation too much, then we have delayed wound healing. If we accelerate it too much, we might get hypertrophic scarring. So it’s a delicate balance that we can intervene on and maybe improve analgesia, but we mustn’t affect the balance of wound healing."
Dr. Carvalho disclosed that he has a relationship with I-Flow, manufacturer of the pump used in the study.
FROM THE ANNUAL MEETING OF THE SOCIETY FOR OBSTETRIC ANESTHESIA AND PERINATOLOGY
Some Risk Factors for Failed Epidural Conversion Are Modifiable
MONTEREY, CALIF. – Several factors, some of them modifiable, increase the odds of a failed conversion from epidural analgesia for labor to epidural anesthesia for cesarean delivery, concluded the first systematic review and meta-analysis of this issue.
The analysis found that 1 in every 20 women having an epidural in place and needing a cesarean had to undergo general anesthesia because the epidural could not be used for anesthesia, lead investigator Melissa E.B. Bauer, D.O., reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.

Women had a more than tripling of the odds of failed conversion if they needed two or more epidural analgesia boluses (so-called top-ups) during labor, had a general anesthesiologist instead of an obstetric anesthesiologist, or required a cesarean on a more urgent basis.
The findings underscored the need to investigate if a patient needs top-ups, according to Dr. Bauer. If a patient makes two or more requests for more analgesia, has breakthrough pain, and is really uncomfortable, she needs to be assessed to see if she has a nonworking epidural. If so, it needs to be replaced, she said in an interview, while noting that other factors, such as dystocia, may also be a cause.
The higher odds of failed conversion that are seen with a general anesthesiologist suggest that "people who manage labor and delivery more often are going to be a little bit more comfortable troubleshooting epidurals and trying to avoid a general anesthetic," commented Dr. Bauer, who is an obstetric anesthesiologist at the University of Michigan Health System in Ann Arbor.
The risk with an urgent cesarean may be the hardest to modify. "We can’t really do anything about that, except to have better communication of obstetricians and [obstetric] anesthesia; to say, if you tell us [a cesarean is coming], maybe we can run to the room and start bolusing that epidural so that by the time the [patient] gets to the OR, we have enough of a level so that [you] can start and avoid a general," she explained. "So the main points are, having more cooperation and also evaluating the [fetal-monitoring] strip, and saying okay, do we have 5 or 10 minutes to convert [the epidural] or not – those things might be helpful."
Dr. Brenda A. Bucklin, professor of anesthesiology at the University of Colorado at Denver, Aurora, and comoderator of a related poster discussion session, asked, "Are [obstetric] anesthesiologists less comfortable in providing general anesthesia for cesarean delivery?"
"I think that it’s the opposite," Dr. Bauer replied. "Since we provide anesthesia for pregnant patients on a daily or weekly basis, we have more familiarity with the obstetric airway, and we are also called to the main hospital to provide anesthesia on any pregnant patient there as well."
Dr. Bucklin also wanted to know, "Are [obstetric] anesthesiologists more likely to limp along with a bad epidural for cesarean delivery?"
"I would say no, but part of the difference is that we tend to troubleshoot our epidurals sooner because we can look at the fetal strips and say, oh, I think [the baby’s] coming, and we go and evaluate the patient on a regular basis," Dr. Bauer said. "Also, once a C-section is called, we’re in the room and we have some familiarity with the surgeons to see [if this is] really an emergency, is there time for me to bolus this. I think that [because of] those relationships and also our understanding of [obstetrics] in general, we have a decreased rate of general anesthesia."
There are several reasons to want to avoid a failed epidural conversion and have to resort to general anesthesia, she noted in the interview. Managing the airway in obstetric patients can be challenging, and there are risks associated with using another type of anesthesia on top of an epidural. "You always want the mother to be able to participate in the birth as well," she added.
The investigators identified 13 observational studies with a total of 8,628 women that assessed the rate of failed conversion and risk factors for this outcome.
Results showed that the percentage of patients having an epidural catheter in place who still had to undergo general anesthesia for their cesarean averaged 5%, with a range of 0%-21% across studies, reported Dr. Bauer.
Women’s odds of failed conversion increased significantly if they needed at least two clinician-administered top-ups of analgesia during labor vs. no top-ups (odds ratio, 3.2), had a general vs. obstetric anesthesiologist (OR, 4.6), or required a more urgent cesarean delivery (OR, 40.4).
A variety of other factors were not significantly associated with the odds of failed conversion: combined spinal-epidural instead of standard epidural techniques, the duration of epidural analgesia, the extent of cervical dilation at the time of epidural placement, and obesity.
However, Dr. Bauer noted, the lack of association for obesity is uncertain, given that studies varied widely in terms of when they assessed body mass index or weight relative to pregnancy. "Also, most anesthesiologists are not going to let a patient who is really obese have a nonworking epidural because we don’t want to put her to sleep" and use general anesthesia, she added.
Dr. Bauer disclosed no relevant conflicts of interest.
MONTEREY, CALIF. – Several factors, some of them modifiable, increase the odds of a failed conversion from epidural analgesia for labor to epidural anesthesia for cesarean delivery, concluded the first systematic review and meta-analysis of this issue.
The analysis found that 1 in every 20 women having an epidural in place and needing a cesarean had to undergo general anesthesia because the epidural could not be used for anesthesia, lead investigator Melissa E.B. Bauer, D.O., reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
Women had a more than tripling of the odds of failed conversion if they needed two or more epidural analgesia boluses (so-called top-ups) during labor, had a general anesthesiologist instead of an obstetric anesthesiologist, or required a cesarean on a more urgent basis.
The findings underscored the need to investigate if a patient needs top-ups, according to Dr. Bauer. If a patient makes two or more requests for more analgesia, has breakthrough pain, and is really uncomfortable, she needs to be assessed to see if she has a nonworking epidural. If so, it needs to be replaced, she said in an interview, while noting that other factors, such as dystocia, may also be a cause.
The higher odds of failed conversion that are seen with a general anesthesiologist suggest that "people who manage labor and delivery more often are going to be a little bit more comfortable troubleshooting epidurals and trying to avoid a general anesthetic," commented Dr. Bauer, who is an obstetric anesthesiologist at the University of Michigan Health System in Ann Arbor.
The risk with an urgent cesarean may be the hardest to modify. "We can’t really do anything about that, except to have better communication of obstetricians and [obstetric] anesthesia; to say, if you tell us [a cesarean is coming], maybe we can run to the room and start bolusing that epidural so that by the time the [patient] gets to the OR, we have enough of a level so that [you] can start and avoid a general," she explained. "So the main points are, having more cooperation and also evaluating the [fetal-monitoring] strip, and saying okay, do we have 5 or 10 minutes to convert [the epidural] or not – those things might be helpful."
Dr. Brenda A. Bucklin, professor of anesthesiology at the University of Colorado at Denver, Aurora, and comoderator of a related poster discussion session, asked, "Are [obstetric] anesthesiologists less comfortable in providing general anesthesia for cesarean delivery?"
"I think that it’s the opposite," Dr. Bauer replied. "Since we provide anesthesia for pregnant patients on a daily or weekly basis, we have more familiarity with the obstetric airway, and we are also called to the main hospital to provide anesthesia on any pregnant patient there as well."
Dr. Bucklin also wanted to know, "Are [obstetric] anesthesiologists more likely to limp along with a bad epidural for cesarean delivery?"
"I would say no, but part of the difference is that we tend to troubleshoot our epidurals sooner because we can look at the fetal strips and say, oh, I think [the baby’s] coming, and we go and evaluate the patient on a regular basis," Dr. Bauer said. "Also, once a C-section is called, we’re in the room and we have some familiarity with the surgeons to see [if this is] really an emergency, is there time for me to bolus this. I think that [because of] those relationships and also our understanding of [obstetrics] in general, we have a decreased rate of general anesthesia."
There are several reasons to want to avoid a failed epidural conversion and have to resort to general anesthesia, she noted in the interview. Managing the airway in obstetric patients can be challenging, and there are risks associated with using another type of anesthesia on top of an epidural. "You always want the mother to be able to participate in the birth as well," she added.
The investigators identified 13 observational studies with a total of 8,628 women that assessed the rate of failed conversion and risk factors for this outcome.
Results showed that the percentage of patients having an epidural catheter in place who still had to undergo general anesthesia for their cesarean averaged 5%, with a range of 0%-21% across studies, reported Dr. Bauer.
Women’s odds of failed conversion increased significantly if they needed at least two clinician-administered top-ups of analgesia during labor vs. no top-ups (odds ratio, 3.2), had a general vs. obstetric anesthesiologist (OR, 4.6), or required a more urgent cesarean delivery (OR, 40.4).
A variety of other factors were not significantly associated with the odds of failed conversion: combined spinal-epidural instead of standard epidural techniques, the duration of epidural analgesia, the extent of cervical dilation at the time of epidural placement, and obesity.
However, Dr. Bauer noted, the lack of association for obesity is uncertain, given that studies varied widely in terms of when they assessed body mass index or weight relative to pregnancy. "Also, most anesthesiologists are not going to let a patient who is really obese have a nonworking epidural because we don’t want to put her to sleep" and use general anesthesia, she added.
Dr. Bauer disclosed no relevant conflicts of interest.
MONTEREY, CALIF. – Several factors, some of them modifiable, increase the odds of a failed conversion from epidural analgesia for labor to epidural anesthesia for cesarean delivery, concluded the first systematic review and meta-analysis of this issue.
The analysis found that 1 in every 20 women having an epidural in place and needing a cesarean had to undergo general anesthesia because the epidural could not be used for anesthesia, lead investigator Melissa E.B. Bauer, D.O., reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
Women had a more than tripling of the odds of failed conversion if they needed two or more epidural analgesia boluses (so-called top-ups) during labor, had a general anesthesiologist instead of an obstetric anesthesiologist, or required a cesarean on a more urgent basis.
The findings underscored the need to investigate if a patient needs top-ups, according to Dr. Bauer. If a patient makes two or more requests for more analgesia, has breakthrough pain, and is really uncomfortable, she needs to be assessed to see if she has a nonworking epidural. If so, it needs to be replaced, she said in an interview, while noting that other factors, such as dystocia, may also be a cause.
The higher odds of failed conversion that are seen with a general anesthesiologist suggest that "people who manage labor and delivery more often are going to be a little bit more comfortable troubleshooting epidurals and trying to avoid a general anesthetic," commented Dr. Bauer, who is an obstetric anesthesiologist at the University of Michigan Health System in Ann Arbor.
The risk with an urgent cesarean may be the hardest to modify. "We can’t really do anything about that, except to have better communication of obstetricians and [obstetric] anesthesia; to say, if you tell us [a cesarean is coming], maybe we can run to the room and start bolusing that epidural so that by the time the [patient] gets to the OR, we have enough of a level so that [you] can start and avoid a general," she explained. "So the main points are, having more cooperation and also evaluating the [fetal-monitoring] strip, and saying okay, do we have 5 or 10 minutes to convert [the epidural] or not – those things might be helpful."
Dr. Brenda A. Bucklin, professor of anesthesiology at the University of Colorado at Denver, Aurora, and comoderator of a related poster discussion session, asked, "Are [obstetric] anesthesiologists less comfortable in providing general anesthesia for cesarean delivery?"
"I think that it’s the opposite," Dr. Bauer replied. "Since we provide anesthesia for pregnant patients on a daily or weekly basis, we have more familiarity with the obstetric airway, and we are also called to the main hospital to provide anesthesia on any pregnant patient there as well."
Dr. Bucklin also wanted to know, "Are [obstetric] anesthesiologists more likely to limp along with a bad epidural for cesarean delivery?"
"I would say no, but part of the difference is that we tend to troubleshoot our epidurals sooner because we can look at the fetal strips and say, oh, I think [the baby’s] coming, and we go and evaluate the patient on a regular basis," Dr. Bauer said. "Also, once a C-section is called, we’re in the room and we have some familiarity with the surgeons to see [if this is] really an emergency, is there time for me to bolus this. I think that [because of] those relationships and also our understanding of [obstetrics] in general, we have a decreased rate of general anesthesia."
There are several reasons to want to avoid a failed epidural conversion and have to resort to general anesthesia, she noted in the interview. Managing the airway in obstetric patients can be challenging, and there are risks associated with using another type of anesthesia on top of an epidural. "You always want the mother to be able to participate in the birth as well," she added.
The investigators identified 13 observational studies with a total of 8,628 women that assessed the rate of failed conversion and risk factors for this outcome.
Results showed that the percentage of patients having an epidural catheter in place who still had to undergo general anesthesia for their cesarean averaged 5%, with a range of 0%-21% across studies, reported Dr. Bauer.
Women’s odds of failed conversion increased significantly if they needed at least two clinician-administered top-ups of analgesia during labor vs. no top-ups (odds ratio, 3.2), had a general vs. obstetric anesthesiologist (OR, 4.6), or required a more urgent cesarean delivery (OR, 40.4).
A variety of other factors were not significantly associated with the odds of failed conversion: combined spinal-epidural instead of standard epidural techniques, the duration of epidural analgesia, the extent of cervical dilation at the time of epidural placement, and obesity.
However, Dr. Bauer noted, the lack of association for obesity is uncertain, given that studies varied widely in terms of when they assessed body mass index or weight relative to pregnancy. "Also, most anesthesiologists are not going to let a patient who is really obese have a nonworking epidural because we don’t want to put her to sleep" and use general anesthesia, she added.
Dr. Bauer disclosed no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE SOCIETY FOR OBSTETRIC ANESTHESIA AND PERINATOLOGY
Major Finding: Women’s odds of failed conversion were increased if they received two or more analgesia boluses during labor (OR, 3.2), had a general vs. obstetric anesthesiologist (OR, 4.6), or required a more urgent cesarean delivery (OR, 40.4).
Data Source: The data are from systematic review and meta-analysis of 13 studies with a total of 8,628 women that assessed conversion of epidural labor analgesia to epidural cesarean anesthesia.
Disclosures: Dr. Bauer disclosed no relevant conflicts of interest.
Obstetric Outcomes Fairly Good Despite Maternal CHD
MONTEREY, CALIF. – Parturients with congenital heart disease do have a rockier obstetric course, but generally fare quite well in the peripartum period, a retrospective cohort study found.
Researchers at the University of Colorado Hospital in Denver led by Christine M. Warrick found that roughly 1% of women delivering there over a 4-year period had congenital heart disease.
This group had higher rates of cesarean delivery and neonatal ICU admission than did parturients overall, according to results reported in a poster session at the annual meeting of the Society for Obstetric Anesthesia and Perinatology. Maternal ICU admissions were rare, however, and there were no cases of maternal mortality.
"Congenital heart disease is definitely a risk factor for maternal and fetal complications, but overall the women seemed to do pretty well. The main things to look out for would be neonatal ICU admissions and respiratory distress in the babies," Ms. Warrick commented in an interview.
In additional study findings, although the large majority of women received regional anesthesia for labor and delivery, only a minority had an epidural placed early, before 4 cm of cervical dilation.
"There is some literature that suggests that early epidural placement is beneficial for these women because it decreases the stress on the heart secondary to pain," she noted. "Some of these women come [to the hospital] in labor and they are already beyond 4 cm of dilation, so that may be a big reason why there weren’t so many early epidurals placed."
In a related poster discussion session, comoderator Dr. Katherine W. Arendt of the Mayo Clinic in Rochester, Minn., asked, "Do you believe that the geographical elevation of your hospital improved or worsened your outcomes compared to a sea-level hospital?"
"It’s difficult to say exactly how the elevation affected all of these women, since we had so many different varieties of congenital heart disease," replied Ms. Warrick, who is a fourth-year medical student at the University of Colorado in Aurora. "But it is possible that women with more severe congenital heart disease would not tolerate a lower partial pressure of oxygen in our environment, and there were some women who were advised to deliver at lower altitudes because of this. So that probably improved our outcomes in women who received adequate prenatal care. I also think that points to the importance of prenatal care in these women."
"We know that more women are surviving to childbearing age with congenital heart disease due to the recent advances in surgical repair of these defects, and it is actually one of the major causes of cardiac diseases in pregnant women in the United States," she said. Many of the normal changes of pregnancy, labor, and delivery put stress on the heart and would be expected to exacerbate matters.
The investigators studied 13,109 parturients in the hospital’s perinatal database between October 2005 and December 2009. Medical history and record review identified 75 women, or 0.6%, as having congenital heart disease.
These women had a mean age of 26 years. The majority were non-Hispanic white (60%) and nulliparous (55%). Fully 34% were overweight or obese, and 8% smoked.
According to cardiologists’ notes of symptoms during the third trimester of pregnancy, 60%, 33%, and 7% of the women had New York Heart Association functional class I, II, and III, respectively. The leading congenital anomalies were atrial septal defects (28%), valvular disorders (19%), and tetralogy of Fallot (11%).
In terms of cardiac outcomes, 11% of the women had an arrhythmia in the peripartum period, and 5% required diuresis, Ms. Warrick reported. Although 87% received regional anesthesia for labor and delivery, only 31% received an early epidural.
Some 19% of the women had a preterm birth (one occurring before 37 weeks’ gestation), and 45% had a prolonged hospital stay (lasting more than 2 days after a vaginal delivery or more than 3 days after a cesarean delivery).
Although 3% of the women were admitted to the ICU for prophylactic monitoring, there were no maternal deaths in the peripartum period.
Compared with parturients overall, those with congenital heart disease were more likely to have a cesarean delivery (31% vs. 27%) and a neonatal ICU admission (23% vs. 15%). The majority of the neonatal ICU admissions were for prematurity or respiratory distress.
"In anyone with congenital heart disease, prenatal care is very important, and a lot of these women were followed closely by a team of physicians [specializing in high-risk pregnancies]," noted Ms. Warrick.
"All in all, pregnant women with congenital heart disease can undergo labor and delivery without many complications, but tend to have longer hospital stays and more neonatal ICU admissions," she concluded.
Ms. Warrick disclosed no relevant conflicts of interest.
MONTEREY, CALIF. – Parturients with congenital heart disease do have a rockier obstetric course, but generally fare quite well in the peripartum period, a retrospective cohort study found.
Researchers at the University of Colorado Hospital in Denver led by Christine M. Warrick found that roughly 1% of women delivering there over a 4-year period had congenital heart disease.
This group had higher rates of cesarean delivery and neonatal ICU admission than did parturients overall, according to results reported in a poster session at the annual meeting of the Society for Obstetric Anesthesia and Perinatology. Maternal ICU admissions were rare, however, and there were no cases of maternal mortality.
"Congenital heart disease is definitely a risk factor for maternal and fetal complications, but overall the women seemed to do pretty well. The main things to look out for would be neonatal ICU admissions and respiratory distress in the babies," Ms. Warrick commented in an interview.
In additional study findings, although the large majority of women received regional anesthesia for labor and delivery, only a minority had an epidural placed early, before 4 cm of cervical dilation.
"There is some literature that suggests that early epidural placement is beneficial for these women because it decreases the stress on the heart secondary to pain," she noted. "Some of these women come [to the hospital] in labor and they are already beyond 4 cm of dilation, so that may be a big reason why there weren’t so many early epidurals placed."
In a related poster discussion session, comoderator Dr. Katherine W. Arendt of the Mayo Clinic in Rochester, Minn., asked, "Do you believe that the geographical elevation of your hospital improved or worsened your outcomes compared to a sea-level hospital?"
"It’s difficult to say exactly how the elevation affected all of these women, since we had so many different varieties of congenital heart disease," replied Ms. Warrick, who is a fourth-year medical student at the University of Colorado in Aurora. "But it is possible that women with more severe congenital heart disease would not tolerate a lower partial pressure of oxygen in our environment, and there were some women who were advised to deliver at lower altitudes because of this. So that probably improved our outcomes in women who received adequate prenatal care. I also think that points to the importance of prenatal care in these women."
"We know that more women are surviving to childbearing age with congenital heart disease due to the recent advances in surgical repair of these defects, and it is actually one of the major causes of cardiac diseases in pregnant women in the United States," she said. Many of the normal changes of pregnancy, labor, and delivery put stress on the heart and would be expected to exacerbate matters.
The investigators studied 13,109 parturients in the hospital’s perinatal database between October 2005 and December 2009. Medical history and record review identified 75 women, or 0.6%, as having congenital heart disease.
These women had a mean age of 26 years. The majority were non-Hispanic white (60%) and nulliparous (55%). Fully 34% were overweight or obese, and 8% smoked.
According to cardiologists’ notes of symptoms during the third trimester of pregnancy, 60%, 33%, and 7% of the women had New York Heart Association functional class I, II, and III, respectively. The leading congenital anomalies were atrial septal defects (28%), valvular disorders (19%), and tetralogy of Fallot (11%).
In terms of cardiac outcomes, 11% of the women had an arrhythmia in the peripartum period, and 5% required diuresis, Ms. Warrick reported. Although 87% received regional anesthesia for labor and delivery, only 31% received an early epidural.
Some 19% of the women had a preterm birth (one occurring before 37 weeks’ gestation), and 45% had a prolonged hospital stay (lasting more than 2 days after a vaginal delivery or more than 3 days after a cesarean delivery).
Although 3% of the women were admitted to the ICU for prophylactic monitoring, there were no maternal deaths in the peripartum period.
Compared with parturients overall, those with congenital heart disease were more likely to have a cesarean delivery (31% vs. 27%) and a neonatal ICU admission (23% vs. 15%). The majority of the neonatal ICU admissions were for prematurity or respiratory distress.
"In anyone with congenital heart disease, prenatal care is very important, and a lot of these women were followed closely by a team of physicians [specializing in high-risk pregnancies]," noted Ms. Warrick.
"All in all, pregnant women with congenital heart disease can undergo labor and delivery without many complications, but tend to have longer hospital stays and more neonatal ICU admissions," she concluded.
Ms. Warrick disclosed no relevant conflicts of interest.
MONTEREY, CALIF. – Parturients with congenital heart disease do have a rockier obstetric course, but generally fare quite well in the peripartum period, a retrospective cohort study found.
Researchers at the University of Colorado Hospital in Denver led by Christine M. Warrick found that roughly 1% of women delivering there over a 4-year period had congenital heart disease.
This group had higher rates of cesarean delivery and neonatal ICU admission than did parturients overall, according to results reported in a poster session at the annual meeting of the Society for Obstetric Anesthesia and Perinatology. Maternal ICU admissions were rare, however, and there were no cases of maternal mortality.
"Congenital heart disease is definitely a risk factor for maternal and fetal complications, but overall the women seemed to do pretty well. The main things to look out for would be neonatal ICU admissions and respiratory distress in the babies," Ms. Warrick commented in an interview.
In additional study findings, although the large majority of women received regional anesthesia for labor and delivery, only a minority had an epidural placed early, before 4 cm of cervical dilation.
"There is some literature that suggests that early epidural placement is beneficial for these women because it decreases the stress on the heart secondary to pain," she noted. "Some of these women come [to the hospital] in labor and they are already beyond 4 cm of dilation, so that may be a big reason why there weren’t so many early epidurals placed."
In a related poster discussion session, comoderator Dr. Katherine W. Arendt of the Mayo Clinic in Rochester, Minn., asked, "Do you believe that the geographical elevation of your hospital improved or worsened your outcomes compared to a sea-level hospital?"
"It’s difficult to say exactly how the elevation affected all of these women, since we had so many different varieties of congenital heart disease," replied Ms. Warrick, who is a fourth-year medical student at the University of Colorado in Aurora. "But it is possible that women with more severe congenital heart disease would not tolerate a lower partial pressure of oxygen in our environment, and there were some women who were advised to deliver at lower altitudes because of this. So that probably improved our outcomes in women who received adequate prenatal care. I also think that points to the importance of prenatal care in these women."
"We know that more women are surviving to childbearing age with congenital heart disease due to the recent advances in surgical repair of these defects, and it is actually one of the major causes of cardiac diseases in pregnant women in the United States," she said. Many of the normal changes of pregnancy, labor, and delivery put stress on the heart and would be expected to exacerbate matters.
The investigators studied 13,109 parturients in the hospital’s perinatal database between October 2005 and December 2009. Medical history and record review identified 75 women, or 0.6%, as having congenital heart disease.
These women had a mean age of 26 years. The majority were non-Hispanic white (60%) and nulliparous (55%). Fully 34% were overweight or obese, and 8% smoked.
According to cardiologists’ notes of symptoms during the third trimester of pregnancy, 60%, 33%, and 7% of the women had New York Heart Association functional class I, II, and III, respectively. The leading congenital anomalies were atrial septal defects (28%), valvular disorders (19%), and tetralogy of Fallot (11%).
In terms of cardiac outcomes, 11% of the women had an arrhythmia in the peripartum period, and 5% required diuresis, Ms. Warrick reported. Although 87% received regional anesthesia for labor and delivery, only 31% received an early epidural.
Some 19% of the women had a preterm birth (one occurring before 37 weeks’ gestation), and 45% had a prolonged hospital stay (lasting more than 2 days after a vaginal delivery or more than 3 days after a cesarean delivery).
Although 3% of the women were admitted to the ICU for prophylactic monitoring, there were no maternal deaths in the peripartum period.
Compared with parturients overall, those with congenital heart disease were more likely to have a cesarean delivery (31% vs. 27%) and a neonatal ICU admission (23% vs. 15%). The majority of the neonatal ICU admissions were for prematurity or respiratory distress.
"In anyone with congenital heart disease, prenatal care is very important, and a lot of these women were followed closely by a team of physicians [specializing in high-risk pregnancies]," noted Ms. Warrick.
"All in all, pregnant women with congenital heart disease can undergo labor and delivery without many complications, but tend to have longer hospital stays and more neonatal ICU admissions," she concluded.
Ms. Warrick disclosed no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE SOCIETY FOR OBSTETRIC ANESTHESIA AND PERINATOLOGY
Latex-Free Works Best to Prevent Anaphylaxis During Cesareans
MONTEREY, CALIF. – A screening questionnaire with targeted replacement of latex-containing medical products dramatically reduces the risk of latex anaphylaxis among women undergoing cesarean delivery, but a latex-free policy appears to be the only surefire way to eliminate this risk entirely, according to one institution’s experience.
Investigators at the tertiary-care Hadassah Hebrew University Medical Center, Ein Kerem campus, Jerusalem, found that 2% of women undergoing cesarean delivery experienced latex anaphylaxis with the center’s usual procedures, involving use of latex products and no special screening.

The incidence was more than two-thirds lower, 0.6%, when the center implemented a screening questionnaire in elective cases to assess latex sensitivity and used latex-free gloves and urinary catheters in women who screened as potentially sensitive, Dr. Carolyn F. Weiniger reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology. However, it was even lower, 0%, when the center implemented a latex-free policy for all women undergoing cesareans.
An economic analysis favored use of the questionnaire when the probability of latex anaphylaxis during cesarean was less than 2% and use of the latex-free policy when the probability was greater than that. "The economic analysis was a sensitivity analysis, so it could be used outside of our setting for a wide range of ICU costs. You just need to decide what your ICU costs are," Dr. Weiniger commented in a poster discussion session.
"I think this [study] is very applicable to our practices. ... You can look at your practice and decide if your rate of latex anaphylaxis is greater than or equal to 2%," said session comoderator Dr. Katherine W. Arendt of the Mayo Clinic, Rochester, Minn. She asked the authors what the perceived barriers were to making delivery rooms latex free.
"The main problem is that latex-free gloves, when we started the study, were five times more expensive than regular latex gloves," Dr. Weiniger replied.
Additionally, rewinding a bit, centers must be aware that a problem even exists. "Have a high index of suspicion for latex anaphylaxis because the signs are very subtle. If you have a case of hypotension unexpectedly during surgery that doesn’t have an obvious cause, like bleeding," look into it further, she recommended in an interview.
Centers that do identify a problem should crunch their numbers. "You can use our sensitivity cost analysis, where you just plot your own cost of gloves and cost of an ICU bed, and work out whether you are above or below a cost-benefit position, whereby it would be cheaper for your institution to switch to latex-free gloves as opposed to using latex gloves," she elaborated. Those numbers can then be taken to management to make the case for a change in policy.
But the effort does not necessarily end there, according to Dr. Weiniger. "We knew that all cesarean sections should be done with latex-free gloves, but one patient was rushed to the main OR, and the message hadn’t gotten through, and she had latex anaphylaxis during emergency cesarean section when regular gloves were used. So we had to institute an educational program as well to make sure everybody knew about the policy," she said.
In the study of 1,569 parturients, the investigators analyzed the incidence of latex anaphylaxis among those undergoing elective cesarean delivery during four consecutive periods spanning 40 months.
In the baseline period (n = 460 women), the center followed usual procedures, with use of latex products and no special screening. In the second period (n = 302), it implemented a latex-free policy for cesareans. In the third period (n = 281), it discontinued the latex-free policy because of costs. And in the fourth period (n = 526), it implemented the screening questionnaire with targeted intervention as an alternative approach; the questionnaire contained items validated in previous studies with skin prick test results and/or serum latex IgE antibodies to have high sensitivity and specificity for detection of latex allergy.

Study results showed that the incidence of latex anaphylaxis (possible, probable, or definite) was 2% in the first period, 0% in the second period (P = .003 vs. first), and 0.6% in the fourth period (P = .015 vs. first), Dr. Weiniger reported.
In all, 15% of women completing a questionnaire during the period when it was used had suspected latex sensitivity on the basis of the results.
Women experiencing anaphylaxis received many verbal and written reminders to be evaluated at the center’s allergy clinic, but just 44% did so. All were found to be positive for latex allergy on skin prick testing.
The financial analysis took into account a variety of costs. "When we were looking at ICU costs, we were looking at the costs per treating a case of anaphylaxis, so that could range from very minor to major costs, including lawsuits if there was a fatality," Dr. Weiniger explained. Other costs included those of using latex-free gloves, at $1 per pair and five pair needed per cesarean case.
"The management, when they understood that a cesarean section anaphylaxis could cost them a minimum of $500 per case, and the latex gloves [would cost] $5 per case, they just did the math, with a 2% incidence of latex anaphylaxis in our hospital. They agreed [on a latex-free policy] only for cesarean sections, not for other surgeries, and not for urinary catheters," as the literature suggests that gloves are the main source of the problem.
Many institutions have not assessed anaphylaxis in their cesarean populations, according to Dr. Weiniger. "So we are planning a national study to get other institutions to identify any case of potential anaphylaxis, to do mast cell tryptase to confirm if it was anaphylaxis, and to do latex testing to see if the cause was latex, so the other institutions can identify if they also have a problem," she said.
Dr. Weiniger disclosed no financial conflicts of interests.
MONTEREY, CALIF. – A screening questionnaire with targeted replacement of latex-containing medical products dramatically reduces the risk of latex anaphylaxis among women undergoing cesarean delivery, but a latex-free policy appears to be the only surefire way to eliminate this risk entirely, according to one institution’s experience.
Investigators at the tertiary-care Hadassah Hebrew University Medical Center, Ein Kerem campus, Jerusalem, found that 2% of women undergoing cesarean delivery experienced latex anaphylaxis with the center’s usual procedures, involving use of latex products and no special screening.
The incidence was more than two-thirds lower, 0.6%, when the center implemented a screening questionnaire in elective cases to assess latex sensitivity and used latex-free gloves and urinary catheters in women who screened as potentially sensitive, Dr. Carolyn F. Weiniger reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology. However, it was even lower, 0%, when the center implemented a latex-free policy for all women undergoing cesareans.
An economic analysis favored use of the questionnaire when the probability of latex anaphylaxis during cesarean was less than 2% and use of the latex-free policy when the probability was greater than that. "The economic analysis was a sensitivity analysis, so it could be used outside of our setting for a wide range of ICU costs. You just need to decide what your ICU costs are," Dr. Weiniger commented in a poster discussion session.
"I think this [study] is very applicable to our practices. ... You can look at your practice and decide if your rate of latex anaphylaxis is greater than or equal to 2%," said session comoderator Dr. Katherine W. Arendt of the Mayo Clinic, Rochester, Minn. She asked the authors what the perceived barriers were to making delivery rooms latex free.
"The main problem is that latex-free gloves, when we started the study, were five times more expensive than regular latex gloves," Dr. Weiniger replied.
Additionally, rewinding a bit, centers must be aware that a problem even exists. "Have a high index of suspicion for latex anaphylaxis because the signs are very subtle. If you have a case of hypotension unexpectedly during surgery that doesn’t have an obvious cause, like bleeding," look into it further, she recommended in an interview.
Centers that do identify a problem should crunch their numbers. "You can use our sensitivity cost analysis, where you just plot your own cost of gloves and cost of an ICU bed, and work out whether you are above or below a cost-benefit position, whereby it would be cheaper for your institution to switch to latex-free gloves as opposed to using latex gloves," she elaborated. Those numbers can then be taken to management to make the case for a change in policy.
But the effort does not necessarily end there, according to Dr. Weiniger. "We knew that all cesarean sections should be done with latex-free gloves, but one patient was rushed to the main OR, and the message hadn’t gotten through, and she had latex anaphylaxis during emergency cesarean section when regular gloves were used. So we had to institute an educational program as well to make sure everybody knew about the policy," she said.
In the study of 1,569 parturients, the investigators analyzed the incidence of latex anaphylaxis among those undergoing elective cesarean delivery during four consecutive periods spanning 40 months.
In the baseline period (n = 460 women), the center followed usual procedures, with use of latex products and no special screening. In the second period (n = 302), it implemented a latex-free policy for cesareans. In the third period (n = 281), it discontinued the latex-free policy because of costs. And in the fourth period (n = 526), it implemented the screening questionnaire with targeted intervention as an alternative approach; the questionnaire contained items validated in previous studies with skin prick test results and/or serum latex IgE antibodies to have high sensitivity and specificity for detection of latex allergy.
Study results showed that the incidence of latex anaphylaxis (possible, probable, or definite) was 2% in the first period, 0% in the second period (P = .003 vs. first), and 0.6% in the fourth period (P = .015 vs. first), Dr. Weiniger reported.
In all, 15% of women completing a questionnaire during the period when it was used had suspected latex sensitivity on the basis of the results.
Women experiencing anaphylaxis received many verbal and written reminders to be evaluated at the center’s allergy clinic, but just 44% did so. All were found to be positive for latex allergy on skin prick testing.
The financial analysis took into account a variety of costs. "When we were looking at ICU costs, we were looking at the costs per treating a case of anaphylaxis, so that could range from very minor to major costs, including lawsuits if there was a fatality," Dr. Weiniger explained. Other costs included those of using latex-free gloves, at $1 per pair and five pair needed per cesarean case.
"The management, when they understood that a cesarean section anaphylaxis could cost them a minimum of $500 per case, and the latex gloves [would cost] $5 per case, they just did the math, with a 2% incidence of latex anaphylaxis in our hospital. They agreed [on a latex-free policy] only for cesarean sections, not for other surgeries, and not for urinary catheters," as the literature suggests that gloves are the main source of the problem.
Many institutions have not assessed anaphylaxis in their cesarean populations, according to Dr. Weiniger. "So we are planning a national study to get other institutions to identify any case of potential anaphylaxis, to do mast cell tryptase to confirm if it was anaphylaxis, and to do latex testing to see if the cause was latex, so the other institutions can identify if they also have a problem," she said.
Dr. Weiniger disclosed no financial conflicts of interests.
MONTEREY, CALIF. – A screening questionnaire with targeted replacement of latex-containing medical products dramatically reduces the risk of latex anaphylaxis among women undergoing cesarean delivery, but a latex-free policy appears to be the only surefire way to eliminate this risk entirely, according to one institution’s experience.
Investigators at the tertiary-care Hadassah Hebrew University Medical Center, Ein Kerem campus, Jerusalem, found that 2% of women undergoing cesarean delivery experienced latex anaphylaxis with the center’s usual procedures, involving use of latex products and no special screening.
The incidence was more than two-thirds lower, 0.6%, when the center implemented a screening questionnaire in elective cases to assess latex sensitivity and used latex-free gloves and urinary catheters in women who screened as potentially sensitive, Dr. Carolyn F. Weiniger reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology. However, it was even lower, 0%, when the center implemented a latex-free policy for all women undergoing cesareans.
An economic analysis favored use of the questionnaire when the probability of latex anaphylaxis during cesarean was less than 2% and use of the latex-free policy when the probability was greater than that. "The economic analysis was a sensitivity analysis, so it could be used outside of our setting for a wide range of ICU costs. You just need to decide what your ICU costs are," Dr. Weiniger commented in a poster discussion session.
"I think this [study] is very applicable to our practices. ... You can look at your practice and decide if your rate of latex anaphylaxis is greater than or equal to 2%," said session comoderator Dr. Katherine W. Arendt of the Mayo Clinic, Rochester, Minn. She asked the authors what the perceived barriers were to making delivery rooms latex free.
"The main problem is that latex-free gloves, when we started the study, were five times more expensive than regular latex gloves," Dr. Weiniger replied.
Additionally, rewinding a bit, centers must be aware that a problem even exists. "Have a high index of suspicion for latex anaphylaxis because the signs are very subtle. If you have a case of hypotension unexpectedly during surgery that doesn’t have an obvious cause, like bleeding," look into it further, she recommended in an interview.
Centers that do identify a problem should crunch their numbers. "You can use our sensitivity cost analysis, where you just plot your own cost of gloves and cost of an ICU bed, and work out whether you are above or below a cost-benefit position, whereby it would be cheaper for your institution to switch to latex-free gloves as opposed to using latex gloves," she elaborated. Those numbers can then be taken to management to make the case for a change in policy.
But the effort does not necessarily end there, according to Dr. Weiniger. "We knew that all cesarean sections should be done with latex-free gloves, but one patient was rushed to the main OR, and the message hadn’t gotten through, and she had latex anaphylaxis during emergency cesarean section when regular gloves were used. So we had to institute an educational program as well to make sure everybody knew about the policy," she said.
In the study of 1,569 parturients, the investigators analyzed the incidence of latex anaphylaxis among those undergoing elective cesarean delivery during four consecutive periods spanning 40 months.
In the baseline period (n = 460 women), the center followed usual procedures, with use of latex products and no special screening. In the second period (n = 302), it implemented a latex-free policy for cesareans. In the third period (n = 281), it discontinued the latex-free policy because of costs. And in the fourth period (n = 526), it implemented the screening questionnaire with targeted intervention as an alternative approach; the questionnaire contained items validated in previous studies with skin prick test results and/or serum latex IgE antibodies to have high sensitivity and specificity for detection of latex allergy.
Study results showed that the incidence of latex anaphylaxis (possible, probable, or definite) was 2% in the first period, 0% in the second period (P = .003 vs. first), and 0.6% in the fourth period (P = .015 vs. first), Dr. Weiniger reported.
In all, 15% of women completing a questionnaire during the period when it was used had suspected latex sensitivity on the basis of the results.
Women experiencing anaphylaxis received many verbal and written reminders to be evaluated at the center’s allergy clinic, but just 44% did so. All were found to be positive for latex allergy on skin prick testing.
The financial analysis took into account a variety of costs. "When we were looking at ICU costs, we were looking at the costs per treating a case of anaphylaxis, so that could range from very minor to major costs, including lawsuits if there was a fatality," Dr. Weiniger explained. Other costs included those of using latex-free gloves, at $1 per pair and five pair needed per cesarean case.
"The management, when they understood that a cesarean section anaphylaxis could cost them a minimum of $500 per case, and the latex gloves [would cost] $5 per case, they just did the math, with a 2% incidence of latex anaphylaxis in our hospital. They agreed [on a latex-free policy] only for cesarean sections, not for other surgeries, and not for urinary catheters," as the literature suggests that gloves are the main source of the problem.
Many institutions have not assessed anaphylaxis in their cesarean populations, according to Dr. Weiniger. "So we are planning a national study to get other institutions to identify any case of potential anaphylaxis, to do mast cell tryptase to confirm if it was anaphylaxis, and to do latex testing to see if the cause was latex, so the other institutions can identify if they also have a problem," she said.
Dr. Weiniger disclosed no financial conflicts of interests.
FROM THE ANNUAL MEETING OF THE SOCIETY FOR OBSTETRIC ANESTHESIA AND PERINATALOGY
Transport Compromises Quality of CPR for Obstetric Patients in Arrest
MONTEREY, CALIF. – The quality of cardiopulmonary resuscitation deteriorates when women experiencing cardiac arrest during labor and delivery are transported to the operating room for emergent cesarean section, suggests a randomized trial using simulation.
Results of the trial, conducted by investigators at Stanford (Calif.) University involving 26 multidisciplinary obstetric teams using mannequins, were reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
Main findings showed that teams that stayed put, starting and continuing CPR in the labor room, administered most chest compressions correctly. In contrast, teams that transported their mannequins on a gurney to the operating room had a marked drop-off in CPR performance, administering only a third of compressions correctly while in motion.
The transport group almost universally experienced interruptions in CPR, whereas the stationary group seldom did. In addition, ventilatory tidal volume fell sharply in the transport group during transport, whereas it remained stable in the stationary group.
"The quality of CPR definitely decreases when you move patients," commented presenting author Dr. Brendan Carvalho, an anesthesiologist at Lucile Packard Children’s Hospital at Stanford. He noted that a similar earlier study, also using simulation, found that the average time to incision for perimortem cesarean was almost doubled by transport to the operating room, from 4:25 minutes to 7:53 minutes (Obstet. Gynecol. 2011;118:1090-4).
Taken together, the studies’ results "would suggest strongly that we would recommend you to perform perimortem cesarean delivery at the site where the arrest occurs, either in labor & delivery or in the operating room, but not to move the patient if they are not in the operating room," he maintained.
Dr. Vilma E. Ortiz, session moderator and an anesthesiologist at the Massachusetts General Hospital in Boston, said, "In general, the overall quality of resuscitation – line placement, intubation, fluids – seems to be better in the operating room. Do you think that in practice, that might offset perhaps the poorer chest compressions [during transport]?"
The earlier study also found that other important tasks were forgotten or performed more poorly under conditions of transport, Dr. Carvalho replied. "Now clearly, it would be easier to do the cesarean in an operating room setting, but these patients are often dead and they are not going to bleed. Once you get the baby out, you can then move them later on if you want to. So I think the importance is getting the delivery, and moving the patient to the operating room will pretty much guarantee you will not be able to do this within 5 minutes [of the arrest], which is the recommendation from the guidelines."
A session attendee noted, "If we are going to do these emergent C-sections in the labor room, one of the advantages to being in the operating room is all the equipment for surgery exists. Do you have some special equipment on your code carts or somewhere else that would help facilitate that cesarean delivery? Can you make recommendations about what we all should have if we are going to do these sections in the delivery room?"
"That’s a very good point," Dr. Carvalho remarked. "If you propose this at your institution, it’s important that you get the surgical pack there so in an arrest situation, when a code comes up, someone’s job is to get the pack there." He noted that his own institution had to deal with logistics to ensure that scalpels for performing cesareans were always available in the labor room. "So you have to work through this and make those logistic changes, whatever works at your institution – each institution is different. But you must think out the scenario before just proposing it as the right scenario."
Institutions should also be aware that changing the place of delivery may change behaviors, he added. For example, in the earlier study, "when the cesareans were done in the labor & delivery room, the vast majority were vertical incisions, as the [obstetricians] have been taught to do in a perimortem section. In the group that moved to the operating room, the majority did Pfannenstiel incisions, because they sort of went back to old habits from the operating room days. So there are behavior changes based on whether you move or don’t move."
In the new study, the investigators created 26 obstetric teams, each having two staff members (obstetricians, nurses, and/or anesthesiologists). The teams were randomly assigned to stationary or transport groups.
The study period had three phases. During phase I, lasting 4 minutes, teams in both groups performed stationary CPR in the labor room. During phase II, lasting 2 minutes, the stationary teams continued with CPR there, whereas the transport teams performed CPR while transporting their mannequin to the operating room. During phase III, lasting 4 minutes, teams in both groups performed stationary CPR at their respective location.
The investigators simulated cardiac arrest using mannequins that provide real-time feedback on the effectiveness of chest compressions and ventilations, according to Dr. Carvalho.
Chest compressions were defined as correctly performed if they were administered at a rate of at least 100/minute, with correct sternal hand placement, a depth of at least 1.5 inches, and a release step.
"The teams were very similar in terms of age, gender, self-reported fitness, and years of experience," Dr. Carvalho reported. Overall, 46% of team members were registered nurses, 15% were obstetricians, and 39% were anesthesiologists. Most (88%) had current certification in advanced cardiac life support.
Study results showed that within the transport group, there was a significant decrease in the percentage of chest compressions performed correctly between phase I and phase II, with a return to baseline in phase III. In contrast, the percentage was generally similar across phases in the stationary group, except for a small fall-off in phase III that he attributed to possible fatigue.
During phase II, the percentage of chest compressions performed correctly was 93% in the stationary group, compared with only 32% in the transport group.
"The reason for [more incorrect compressions] was primarily insufficient depth, but also the sternal hand being too low and no release," Dr. Carvalho commented. "Interestingly, we thought that the rate would be different [between groups], but we did not find significant differences. No one actually did a rate below 100."
Additional analyses showed that there was an interruption in CPR for 92% of teams in the transport group during phase II, compared with just 7% in the stationary group.
In the transport group, team members used a variety of positions when attempting to administer CPR while moving: most knelt next to the mannequin on the gurney, but some straddled the mannequin or ran alongside the gurney. Those running alongside "tended to have a lot of interruptions as they moved past the usual obstructions," he noted.
Mean tidal volume also dropped significantly in the transport group in phase II, whereas it remained essentially constant in the stationary group. However, Dr. Carvalho cautioned, the mannequins were only mask-ventilated and not intubated, which may have affected these results.
"There’s a lot of limitations with any simulated study," he acknowledged. "Obviously, this was a simulated arrest. The mannequin is really just a torso; we can’t administer left uterine displacement, it doesn’t have a pregnant belly, and we didn’t intubate." Also, teams were trained on the mannequin just before the study.
Dr. Carvalho disclosed no relevant conflicts of interest.
MONTEREY, CALIF. – The quality of cardiopulmonary resuscitation deteriorates when women experiencing cardiac arrest during labor and delivery are transported to the operating room for emergent cesarean section, suggests a randomized trial using simulation.
Results of the trial, conducted by investigators at Stanford (Calif.) University involving 26 multidisciplinary obstetric teams using mannequins, were reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
Main findings showed that teams that stayed put, starting and continuing CPR in the labor room, administered most chest compressions correctly. In contrast, teams that transported their mannequins on a gurney to the operating room had a marked drop-off in CPR performance, administering only a third of compressions correctly while in motion.
The transport group almost universally experienced interruptions in CPR, whereas the stationary group seldom did. In addition, ventilatory tidal volume fell sharply in the transport group during transport, whereas it remained stable in the stationary group.
"The quality of CPR definitely decreases when you move patients," commented presenting author Dr. Brendan Carvalho, an anesthesiologist at Lucile Packard Children’s Hospital at Stanford. He noted that a similar earlier study, also using simulation, found that the average time to incision for perimortem cesarean was almost doubled by transport to the operating room, from 4:25 minutes to 7:53 minutes (Obstet. Gynecol. 2011;118:1090-4).
Taken together, the studies’ results "would suggest strongly that we would recommend you to perform perimortem cesarean delivery at the site where the arrest occurs, either in labor & delivery or in the operating room, but not to move the patient if they are not in the operating room," he maintained.
Dr. Vilma E. Ortiz, session moderator and an anesthesiologist at the Massachusetts General Hospital in Boston, said, "In general, the overall quality of resuscitation – line placement, intubation, fluids – seems to be better in the operating room. Do you think that in practice, that might offset perhaps the poorer chest compressions [during transport]?"
The earlier study also found that other important tasks were forgotten or performed more poorly under conditions of transport, Dr. Carvalho replied. "Now clearly, it would be easier to do the cesarean in an operating room setting, but these patients are often dead and they are not going to bleed. Once you get the baby out, you can then move them later on if you want to. So I think the importance is getting the delivery, and moving the patient to the operating room will pretty much guarantee you will not be able to do this within 5 minutes [of the arrest], which is the recommendation from the guidelines."
A session attendee noted, "If we are going to do these emergent C-sections in the labor room, one of the advantages to being in the operating room is all the equipment for surgery exists. Do you have some special equipment on your code carts or somewhere else that would help facilitate that cesarean delivery? Can you make recommendations about what we all should have if we are going to do these sections in the delivery room?"
"That’s a very good point," Dr. Carvalho remarked. "If you propose this at your institution, it’s important that you get the surgical pack there so in an arrest situation, when a code comes up, someone’s job is to get the pack there." He noted that his own institution had to deal with logistics to ensure that scalpels for performing cesareans were always available in the labor room. "So you have to work through this and make those logistic changes, whatever works at your institution – each institution is different. But you must think out the scenario before just proposing it as the right scenario."
Institutions should also be aware that changing the place of delivery may change behaviors, he added. For example, in the earlier study, "when the cesareans were done in the labor & delivery room, the vast majority were vertical incisions, as the [obstetricians] have been taught to do in a perimortem section. In the group that moved to the operating room, the majority did Pfannenstiel incisions, because they sort of went back to old habits from the operating room days. So there are behavior changes based on whether you move or don’t move."
In the new study, the investigators created 26 obstetric teams, each having two staff members (obstetricians, nurses, and/or anesthesiologists). The teams were randomly assigned to stationary or transport groups.
The study period had three phases. During phase I, lasting 4 minutes, teams in both groups performed stationary CPR in the labor room. During phase II, lasting 2 minutes, the stationary teams continued with CPR there, whereas the transport teams performed CPR while transporting their mannequin to the operating room. During phase III, lasting 4 minutes, teams in both groups performed stationary CPR at their respective location.
The investigators simulated cardiac arrest using mannequins that provide real-time feedback on the effectiveness of chest compressions and ventilations, according to Dr. Carvalho.
Chest compressions were defined as correctly performed if they were administered at a rate of at least 100/minute, with correct sternal hand placement, a depth of at least 1.5 inches, and a release step.
"The teams were very similar in terms of age, gender, self-reported fitness, and years of experience," Dr. Carvalho reported. Overall, 46% of team members were registered nurses, 15% were obstetricians, and 39% were anesthesiologists. Most (88%) had current certification in advanced cardiac life support.
Study results showed that within the transport group, there was a significant decrease in the percentage of chest compressions performed correctly between phase I and phase II, with a return to baseline in phase III. In contrast, the percentage was generally similar across phases in the stationary group, except for a small fall-off in phase III that he attributed to possible fatigue.
During phase II, the percentage of chest compressions performed correctly was 93% in the stationary group, compared with only 32% in the transport group.
"The reason for [more incorrect compressions] was primarily insufficient depth, but also the sternal hand being too low and no release," Dr. Carvalho commented. "Interestingly, we thought that the rate would be different [between groups], but we did not find significant differences. No one actually did a rate below 100."
Additional analyses showed that there was an interruption in CPR for 92% of teams in the transport group during phase II, compared with just 7% in the stationary group.
In the transport group, team members used a variety of positions when attempting to administer CPR while moving: most knelt next to the mannequin on the gurney, but some straddled the mannequin or ran alongside the gurney. Those running alongside "tended to have a lot of interruptions as they moved past the usual obstructions," he noted.
Mean tidal volume also dropped significantly in the transport group in phase II, whereas it remained essentially constant in the stationary group. However, Dr. Carvalho cautioned, the mannequins were only mask-ventilated and not intubated, which may have affected these results.
"There’s a lot of limitations with any simulated study," he acknowledged. "Obviously, this was a simulated arrest. The mannequin is really just a torso; we can’t administer left uterine displacement, it doesn’t have a pregnant belly, and we didn’t intubate." Also, teams were trained on the mannequin just before the study.
Dr. Carvalho disclosed no relevant conflicts of interest.
MONTEREY, CALIF. – The quality of cardiopulmonary resuscitation deteriorates when women experiencing cardiac arrest during labor and delivery are transported to the operating room for emergent cesarean section, suggests a randomized trial using simulation.
Results of the trial, conducted by investigators at Stanford (Calif.) University involving 26 multidisciplinary obstetric teams using mannequins, were reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
Main findings showed that teams that stayed put, starting and continuing CPR in the labor room, administered most chest compressions correctly. In contrast, teams that transported their mannequins on a gurney to the operating room had a marked drop-off in CPR performance, administering only a third of compressions correctly while in motion.
The transport group almost universally experienced interruptions in CPR, whereas the stationary group seldom did. In addition, ventilatory tidal volume fell sharply in the transport group during transport, whereas it remained stable in the stationary group.
"The quality of CPR definitely decreases when you move patients," commented presenting author Dr. Brendan Carvalho, an anesthesiologist at Lucile Packard Children’s Hospital at Stanford. He noted that a similar earlier study, also using simulation, found that the average time to incision for perimortem cesarean was almost doubled by transport to the operating room, from 4:25 minutes to 7:53 minutes (Obstet. Gynecol. 2011;118:1090-4).
Taken together, the studies’ results "would suggest strongly that we would recommend you to perform perimortem cesarean delivery at the site where the arrest occurs, either in labor & delivery or in the operating room, but not to move the patient if they are not in the operating room," he maintained.
Dr. Vilma E. Ortiz, session moderator and an anesthesiologist at the Massachusetts General Hospital in Boston, said, "In general, the overall quality of resuscitation – line placement, intubation, fluids – seems to be better in the operating room. Do you think that in practice, that might offset perhaps the poorer chest compressions [during transport]?"
The earlier study also found that other important tasks were forgotten or performed more poorly under conditions of transport, Dr. Carvalho replied. "Now clearly, it would be easier to do the cesarean in an operating room setting, but these patients are often dead and they are not going to bleed. Once you get the baby out, you can then move them later on if you want to. So I think the importance is getting the delivery, and moving the patient to the operating room will pretty much guarantee you will not be able to do this within 5 minutes [of the arrest], which is the recommendation from the guidelines."
A session attendee noted, "If we are going to do these emergent C-sections in the labor room, one of the advantages to being in the operating room is all the equipment for surgery exists. Do you have some special equipment on your code carts or somewhere else that would help facilitate that cesarean delivery? Can you make recommendations about what we all should have if we are going to do these sections in the delivery room?"
"That’s a very good point," Dr. Carvalho remarked. "If you propose this at your institution, it’s important that you get the surgical pack there so in an arrest situation, when a code comes up, someone’s job is to get the pack there." He noted that his own institution had to deal with logistics to ensure that scalpels for performing cesareans were always available in the labor room. "So you have to work through this and make those logistic changes, whatever works at your institution – each institution is different. But you must think out the scenario before just proposing it as the right scenario."
Institutions should also be aware that changing the place of delivery may change behaviors, he added. For example, in the earlier study, "when the cesareans were done in the labor & delivery room, the vast majority were vertical incisions, as the [obstetricians] have been taught to do in a perimortem section. In the group that moved to the operating room, the majority did Pfannenstiel incisions, because they sort of went back to old habits from the operating room days. So there are behavior changes based on whether you move or don’t move."
In the new study, the investigators created 26 obstetric teams, each having two staff members (obstetricians, nurses, and/or anesthesiologists). The teams were randomly assigned to stationary or transport groups.
The study period had three phases. During phase I, lasting 4 minutes, teams in both groups performed stationary CPR in the labor room. During phase II, lasting 2 minutes, the stationary teams continued with CPR there, whereas the transport teams performed CPR while transporting their mannequin to the operating room. During phase III, lasting 4 minutes, teams in both groups performed stationary CPR at their respective location.
The investigators simulated cardiac arrest using mannequins that provide real-time feedback on the effectiveness of chest compressions and ventilations, according to Dr. Carvalho.
Chest compressions were defined as correctly performed if they were administered at a rate of at least 100/minute, with correct sternal hand placement, a depth of at least 1.5 inches, and a release step.
"The teams were very similar in terms of age, gender, self-reported fitness, and years of experience," Dr. Carvalho reported. Overall, 46% of team members were registered nurses, 15% were obstetricians, and 39% were anesthesiologists. Most (88%) had current certification in advanced cardiac life support.
Study results showed that within the transport group, there was a significant decrease in the percentage of chest compressions performed correctly between phase I and phase II, with a return to baseline in phase III. In contrast, the percentage was generally similar across phases in the stationary group, except for a small fall-off in phase III that he attributed to possible fatigue.
During phase II, the percentage of chest compressions performed correctly was 93% in the stationary group, compared with only 32% in the transport group.
"The reason for [more incorrect compressions] was primarily insufficient depth, but also the sternal hand being too low and no release," Dr. Carvalho commented. "Interestingly, we thought that the rate would be different [between groups], but we did not find significant differences. No one actually did a rate below 100."
Additional analyses showed that there was an interruption in CPR for 92% of teams in the transport group during phase II, compared with just 7% in the stationary group.
In the transport group, team members used a variety of positions when attempting to administer CPR while moving: most knelt next to the mannequin on the gurney, but some straddled the mannequin or ran alongside the gurney. Those running alongside "tended to have a lot of interruptions as they moved past the usual obstructions," he noted.
Mean tidal volume also dropped significantly in the transport group in phase II, whereas it remained essentially constant in the stationary group. However, Dr. Carvalho cautioned, the mannequins were only mask-ventilated and not intubated, which may have affected these results.
"There’s a lot of limitations with any simulated study," he acknowledged. "Obviously, this was a simulated arrest. The mannequin is really just a torso; we can’t administer left uterine displacement, it doesn’t have a pregnant belly, and we didn’t intubate." Also, teams were trained on the mannequin just before the study.
Dr. Carvalho disclosed no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE SOCIETY FOR OBSTETRIC ANESTHESIA AND PERINATOLOGY
Sharp Rise Seen in Rate of Delivery-Related Severe Sepsis
MONTEREY, CALIF. – The rate of severe sepsis among women hospitalized for delivery more than doubled during a recent 10-year period, according to a cohort study reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
In the analysis of more than 9.24 million admissions for delivery from the Nationwide Inpatient Sample, the rate rose from 0.64 to 1.37 per 10,000 deliveries between 1998-2000 and 2007-2008, reported lead investigator Dr. Melissa E.B. Bauer, an obstetric anesthesiologist with the University of Michigan Health System in Ann Arbor.

Several comorbidities and obstetric factors independently increased the risk of severe sepsis. For example, women with congestive heart failure had a more than fourfold higher risk, and women undergoing cesarean delivery had a more than fivefold higher risk.
"The etiology of the increase [in severe sepsis] in this population is unknown," she commented. "Possible hypotheses for the increase ... could be the increased cesarean delivery rate. At the start of the study period, the cesarean delivery rate was 21.2%; by 2008, the national rate was 32.3%."
"There’s also a higher-risk patient population. More women today have comorbidities that increase their risk of severe sepsis," she added. "And there’s an increased microbial resistance that could also be contributing."
Dr. Bauer noted that an important related issue is the difficulty of diagnosing sepsis during pregnancy. Some of the physiologic values typically used to establish the presence of the systemic inflammatory response syndrome (SIRS), often seen in sepsis, are actually considered normal for a pregnant woman.
"As the population at risk for severe sepsis continues to increase, unless we also increase our identification of patients with sepsis in this population, the rate of severe sepsis and death will continue to increase," she maintained. "A priority of future research will be to redefine SIRS in pregnant patients."
Session moderator Dr. Alan C. Santos of St. Luke’s Roosevelt Hospital Center in New York said, "I realize there were limitations to this type of study and what data you were able to extract. Could this all just be related to an increase in the background infections, HIV, and substance abuse among our population?"
Dr. Bauer acknowledged that those factors may have contributed and were not captured by administrative data. Factors often went uncoded "unless there was a reason to code a certain factor, basically, if it complicated the delivery and there would be more reimbursement for that type of situation," she said. For example, the investigators found a code for obesity in only about 1% of the sample, when roughly 20% of the population is obese.
"The only risk factor that appears to be at all modifiable is cesarean delivery, and it may add another nail in the coffin of this conversation," commented session attendee Dr. Stephen Pratt of Beth Israel Deaconess Hospital in Boston. "I was just wondering, are you able to look at either indications for cesarean delivery or even at, more broadly, elective versus intrapartum cesarean delivery? My guess is it’s going to be the intrapartum cesarean deliveries that are high risk for sepsis."
"That's an excellent point," Dr. Bauer replied. "The problem is, it’s difficult to determine exactly." However, it may be possible to get a general sense from measures such as the duration of hospitalization before cesarean. "We are certainly going to tease out more of the data," she said.
Previous research has suggested that sepsis of any severity complicates about 1 in every 8,000 deliveries in the United States. But "this has been determined by single-institution, retrospective cohort studies. To date, there has not been a United States population–based study looking at incidence, temporal trends, and risk factors for sepsis," Dr. Bauer noted.
The investigators identified hospital admissions having pregnancy- and delivery-related diagnostic codes, excluding those pertaining to ectopic or molar pregnancy, or abortion. Within this set, they then assessed outcomes of sepsis, severe sepsis (sepsis with organ failure and/or hypotension), and sepsis-related death.
Results showed that the rate of sepsis remained essentially the same during the study period, affecting about 1 in every 3,300 deliveries, according to Dr. Bauer. However, the rate of severe sepsis doubled.
Multivariate analyses showed a variety of comorbidities and demographic and obstetric factors that were independently associated with an elevated risk of severe sepsis: diabetes (odds ratio, 1.4), black race (1.8), delivery before 37 weeks (1.8), cerclage (2.7), hypertensive diseases of pregnancy (4.5), congestive heart failure (4.5), cesarean delivery (5.1), stillbirth (6.5), retained products of conception (6.9), chronic renal disease (16.2), and chronic liver disease (22.3).
Several other factors – age, insurance, obesity, and preterm premature rupture of membranes (PPROM) – did not significantly affect the risk of this outcome. However, data on PPROM may be misleading because of the heterogeneity of that group, Dr. Bauer cautioned. "It includes any patient who had rupture 24 hours prior to labor; that includes the patient who had rupture 1 day prior to labor and also the patient who has been sitting on the [hospital] floor for several months prior to labor," she explained.
"Of note, teaching-hospital status as well as delivery volume were found to [confer] a mildly increased risk for severe sepsis, but had a minimal effect size when compared to the rest of these variables," Dr. Bauer further reported.
In additional findings, the rate of sepsis-related death among women with sepsis also more than doubled during the study period, from 2.2% to 4.9%. As of 2006-2008, there were 1.31 deaths due to sepsis for every 100,000 deliveries in the United States. "This mirrors the findings in the United Kingdom for increased deaths related to sepsis," she noted (BJOG 2011;118:1-203). There were too few sepsis-related deaths to assess risk factors for this outcome.
Dr. Bauer disclosed no relevant conflicts of interest.
MONTEREY, CALIF. – The rate of severe sepsis among women hospitalized for delivery more than doubled during a recent 10-year period, according to a cohort study reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
In the analysis of more than 9.24 million admissions for delivery from the Nationwide Inpatient Sample, the rate rose from 0.64 to 1.37 per 10,000 deliveries between 1998-2000 and 2007-2008, reported lead investigator Dr. Melissa E.B. Bauer, an obstetric anesthesiologist with the University of Michigan Health System in Ann Arbor.
Several comorbidities and obstetric factors independently increased the risk of severe sepsis. For example, women with congestive heart failure had a more than fourfold higher risk, and women undergoing cesarean delivery had a more than fivefold higher risk.
"The etiology of the increase [in severe sepsis] in this population is unknown," she commented. "Possible hypotheses for the increase ... could be the increased cesarean delivery rate. At the start of the study period, the cesarean delivery rate was 21.2%; by 2008, the national rate was 32.3%."
"There’s also a higher-risk patient population. More women today have comorbidities that increase their risk of severe sepsis," she added. "And there’s an increased microbial resistance that could also be contributing."
Dr. Bauer noted that an important related issue is the difficulty of diagnosing sepsis during pregnancy. Some of the physiologic values typically used to establish the presence of the systemic inflammatory response syndrome (SIRS), often seen in sepsis, are actually considered normal for a pregnant woman.
"As the population at risk for severe sepsis continues to increase, unless we also increase our identification of patients with sepsis in this population, the rate of severe sepsis and death will continue to increase," she maintained. "A priority of future research will be to redefine SIRS in pregnant patients."
Session moderator Dr. Alan C. Santos of St. Luke’s Roosevelt Hospital Center in New York said, "I realize there were limitations to this type of study and what data you were able to extract. Could this all just be related to an increase in the background infections, HIV, and substance abuse among our population?"
Dr. Bauer acknowledged that those factors may have contributed and were not captured by administrative data. Factors often went uncoded "unless there was a reason to code a certain factor, basically, if it complicated the delivery and there would be more reimbursement for that type of situation," she said. For example, the investigators found a code for obesity in only about 1% of the sample, when roughly 20% of the population is obese.
"The only risk factor that appears to be at all modifiable is cesarean delivery, and it may add another nail in the coffin of this conversation," commented session attendee Dr. Stephen Pratt of Beth Israel Deaconess Hospital in Boston. "I was just wondering, are you able to look at either indications for cesarean delivery or even at, more broadly, elective versus intrapartum cesarean delivery? My guess is it’s going to be the intrapartum cesarean deliveries that are high risk for sepsis."
"That's an excellent point," Dr. Bauer replied. "The problem is, it’s difficult to determine exactly." However, it may be possible to get a general sense from measures such as the duration of hospitalization before cesarean. "We are certainly going to tease out more of the data," she said.
Previous research has suggested that sepsis of any severity complicates about 1 in every 8,000 deliveries in the United States. But "this has been determined by single-institution, retrospective cohort studies. To date, there has not been a United States population–based study looking at incidence, temporal trends, and risk factors for sepsis," Dr. Bauer noted.
The investigators identified hospital admissions having pregnancy- and delivery-related diagnostic codes, excluding those pertaining to ectopic or molar pregnancy, or abortion. Within this set, they then assessed outcomes of sepsis, severe sepsis (sepsis with organ failure and/or hypotension), and sepsis-related death.
Results showed that the rate of sepsis remained essentially the same during the study period, affecting about 1 in every 3,300 deliveries, according to Dr. Bauer. However, the rate of severe sepsis doubled.
Multivariate analyses showed a variety of comorbidities and demographic and obstetric factors that were independently associated with an elevated risk of severe sepsis: diabetes (odds ratio, 1.4), black race (1.8), delivery before 37 weeks (1.8), cerclage (2.7), hypertensive diseases of pregnancy (4.5), congestive heart failure (4.5), cesarean delivery (5.1), stillbirth (6.5), retained products of conception (6.9), chronic renal disease (16.2), and chronic liver disease (22.3).
Several other factors – age, insurance, obesity, and preterm premature rupture of membranes (PPROM) – did not significantly affect the risk of this outcome. However, data on PPROM may be misleading because of the heterogeneity of that group, Dr. Bauer cautioned. "It includes any patient who had rupture 24 hours prior to labor; that includes the patient who had rupture 1 day prior to labor and also the patient who has been sitting on the [hospital] floor for several months prior to labor," she explained.
"Of note, teaching-hospital status as well as delivery volume were found to [confer] a mildly increased risk for severe sepsis, but had a minimal effect size when compared to the rest of these variables," Dr. Bauer further reported.
In additional findings, the rate of sepsis-related death among women with sepsis also more than doubled during the study period, from 2.2% to 4.9%. As of 2006-2008, there were 1.31 deaths due to sepsis for every 100,000 deliveries in the United States. "This mirrors the findings in the United Kingdom for increased deaths related to sepsis," she noted (BJOG 2011;118:1-203). There were too few sepsis-related deaths to assess risk factors for this outcome.
Dr. Bauer disclosed no relevant conflicts of interest.
MONTEREY, CALIF. – The rate of severe sepsis among women hospitalized for delivery more than doubled during a recent 10-year period, according to a cohort study reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
In the analysis of more than 9.24 million admissions for delivery from the Nationwide Inpatient Sample, the rate rose from 0.64 to 1.37 per 10,000 deliveries between 1998-2000 and 2007-2008, reported lead investigator Dr. Melissa E.B. Bauer, an obstetric anesthesiologist with the University of Michigan Health System in Ann Arbor.
Several comorbidities and obstetric factors independently increased the risk of severe sepsis. For example, women with congestive heart failure had a more than fourfold higher risk, and women undergoing cesarean delivery had a more than fivefold higher risk.
"The etiology of the increase [in severe sepsis] in this population is unknown," she commented. "Possible hypotheses for the increase ... could be the increased cesarean delivery rate. At the start of the study period, the cesarean delivery rate was 21.2%; by 2008, the national rate was 32.3%."
"There’s also a higher-risk patient population. More women today have comorbidities that increase their risk of severe sepsis," she added. "And there’s an increased microbial resistance that could also be contributing."
Dr. Bauer noted that an important related issue is the difficulty of diagnosing sepsis during pregnancy. Some of the physiologic values typically used to establish the presence of the systemic inflammatory response syndrome (SIRS), often seen in sepsis, are actually considered normal for a pregnant woman.
"As the population at risk for severe sepsis continues to increase, unless we also increase our identification of patients with sepsis in this population, the rate of severe sepsis and death will continue to increase," she maintained. "A priority of future research will be to redefine SIRS in pregnant patients."
Session moderator Dr. Alan C. Santos of St. Luke’s Roosevelt Hospital Center in New York said, "I realize there were limitations to this type of study and what data you were able to extract. Could this all just be related to an increase in the background infections, HIV, and substance abuse among our population?"
Dr. Bauer acknowledged that those factors may have contributed and were not captured by administrative data. Factors often went uncoded "unless there was a reason to code a certain factor, basically, if it complicated the delivery and there would be more reimbursement for that type of situation," she said. For example, the investigators found a code for obesity in only about 1% of the sample, when roughly 20% of the population is obese.
"The only risk factor that appears to be at all modifiable is cesarean delivery, and it may add another nail in the coffin of this conversation," commented session attendee Dr. Stephen Pratt of Beth Israel Deaconess Hospital in Boston. "I was just wondering, are you able to look at either indications for cesarean delivery or even at, more broadly, elective versus intrapartum cesarean delivery? My guess is it’s going to be the intrapartum cesarean deliveries that are high risk for sepsis."
"That's an excellent point," Dr. Bauer replied. "The problem is, it’s difficult to determine exactly." However, it may be possible to get a general sense from measures such as the duration of hospitalization before cesarean. "We are certainly going to tease out more of the data," she said.
Previous research has suggested that sepsis of any severity complicates about 1 in every 8,000 deliveries in the United States. But "this has been determined by single-institution, retrospective cohort studies. To date, there has not been a United States population–based study looking at incidence, temporal trends, and risk factors for sepsis," Dr. Bauer noted.
The investigators identified hospital admissions having pregnancy- and delivery-related diagnostic codes, excluding those pertaining to ectopic or molar pregnancy, or abortion. Within this set, they then assessed outcomes of sepsis, severe sepsis (sepsis with organ failure and/or hypotension), and sepsis-related death.
Results showed that the rate of sepsis remained essentially the same during the study period, affecting about 1 in every 3,300 deliveries, according to Dr. Bauer. However, the rate of severe sepsis doubled.
Multivariate analyses showed a variety of comorbidities and demographic and obstetric factors that were independently associated with an elevated risk of severe sepsis: diabetes (odds ratio, 1.4), black race (1.8), delivery before 37 weeks (1.8), cerclage (2.7), hypertensive diseases of pregnancy (4.5), congestive heart failure (4.5), cesarean delivery (5.1), stillbirth (6.5), retained products of conception (6.9), chronic renal disease (16.2), and chronic liver disease (22.3).
Several other factors – age, insurance, obesity, and preterm premature rupture of membranes (PPROM) – did not significantly affect the risk of this outcome. However, data on PPROM may be misleading because of the heterogeneity of that group, Dr. Bauer cautioned. "It includes any patient who had rupture 24 hours prior to labor; that includes the patient who had rupture 1 day prior to labor and also the patient who has been sitting on the [hospital] floor for several months prior to labor," she explained.
"Of note, teaching-hospital status as well as delivery volume were found to [confer] a mildly increased risk for severe sepsis, but had a minimal effect size when compared to the rest of these variables," Dr. Bauer further reported.
In additional findings, the rate of sepsis-related death among women with sepsis also more than doubled during the study period, from 2.2% to 4.9%. As of 2006-2008, there were 1.31 deaths due to sepsis for every 100,000 deliveries in the United States. "This mirrors the findings in the United Kingdom for increased deaths related to sepsis," she noted (BJOG 2011;118:1-203). There were too few sepsis-related deaths to assess risk factors for this outcome.
Dr. Bauer disclosed no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE SOCIETY FOR OBSTETRIC ANESTHESIA AND PERINATOLOGY
Prior Postpartum Hemorrhage Raises Risk of Another
MONTEREY, CALIF. – Women have a substantially elevated risk of postpartum hemorrhage after a first occurrence, a prospective population-based cohort study has shown.
The study of more than half a million primiparas and roughly 1 million deliveries in Sweden found that women who had postpartum hemorrhage in their first pregnancy were more than three times as likely to have this complication again in their second pregnancy. Risk increased with the severity of hemorrhage in the first pregnancy and with the number of affected pregnancies.
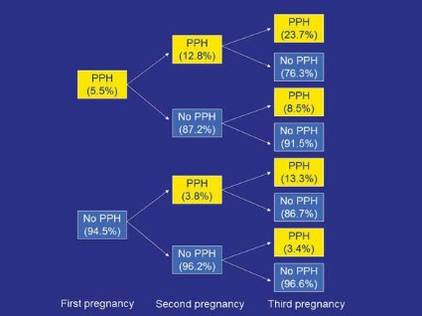
In additional findings, a history of postpartum hemorrhage due to one etiology, for example, uterine atony or retained placenta, increased the risk not only of a recurrence of hemorrhage due to the same etiology but also of occurrence of hemorrhage due to other etiologies.
"The fact that a history of postpartum hemorrhage of one subtype confers risk of other subtypes in a subsequent pregnancy suggests that there are likely shared pathological features across the different etiologies, and I think this is going to be a very interesting area to examine in the future," commented lead investigator Dr. Brian T. Bateman, an anesthesiologist at Harvard Medical School, Boston, at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
"We could speculate that it might be undiagnosed coagulopathy that explains the shared risk or perhaps characteristics of labor, placentation, or other factors. Given the strong pattern of recurrence, perhaps these are even genetic in nature," he added.
In upcoming research, the investigators will look further into possible explanations. "We are planning to collect a series of women with recurrent hemorrhage, particularly women with hemorrhage from discordant causes, and examine in real granular detail what might be mediating these effects that we are observing at the population level," Dr. Bateman explained. "We are also in the process of conducting familial aggregation studies to determine whether there is a genetic component to postpartum hemorrhage risk."
Session attendee Dr. Richard M. Smiley of Columbia University in New York questioned the reliability of coding of postpartum hemorrhage etiologies in the register used for the study. "It’s really intriguing, the cross-risk, if you will. ... With all due respect to the Swedish database, what’s the chance that that is just miscoded – that a woman bleeds maybe from the same cause, but someone needs to put a cause down on the chart or in the coding system, and they have to pick something, and they pick the wrong thing?" he asked.
"There was a study out of the same database last year looking at the role of obesity as a risk factor for postpartum hemorrhage, and they found when they looked at the risk of postpartum hemorrhage from retained placenta or from laceration, there was no effect of BMI in those categories, but a very, very strong effect on risk of atony, suggesting that there is some specificity in the way that these codes are being applied," Dr. Bateman replied.

Previous research has shown that postpartum hemorrhage is a risk factor for the same complication in subsequent pregnancies, he noted, giving some background to the study. However, "less is known about whether risk accumulates with multiple affected pregnancies and whether the severity of prior postpartum hemorrhage has additional predictive value, and if risk of recurrence varies according to postpartum hemorrhage subtype."
The investigators analyzed data from the Swedish Medical Birth Register. They included 538,332 primiparous women who delivered between 1997 and 2009, and followed this group through 2009, identifying a total of 914,933 subsequent deliveries.
Overall, 5.5% of the women had physician-diagnosed postpartum hemorrhage (an estimated blood loss of greater than 1 L) in their first pregnancy. The rate of this complication in a second pregnancy was higher when the first pregnancy was affected, and the rate was especially high in a third pregnancy when both a first and second pregnancy were affected.
Relative to their counterparts who did not have postpartum hemorrhage in their first pregnancy, women who had postpartum hemorrhage that was not severe, meaning it did not require transfusion, had increased risks of both nonsevere and severe postpartum hemorrhage in a second pregnancy (relative risk, 3.2 and 3.4, respectively).
The respective elevations of risks were even greater in women who had severe postpartum hemorrhage in their first pregnancy (RR, 4.2 and 6.9), "suggesting that severity of hemorrhage does add additional predictive value and can be potentially helpful in triaging high-risk patients," Dr. Bateman said.
Additional analyses showed that postpartum hemorrhage in the first pregnancy due to one etiology increased the risk of postpartum hemorrhage in the second pregnancy due to both that etiology and others. "These findings are really quite surprising and are novel," he commented.
For example, women who had hemorrhage due to uterine atony in their first pregnancy had a 3.9-fold higher risk of hemorrhage due to uterine atony in their second pregnancy. But they also had increased risks of postpartum hemorrhage due to retained placenta (3.1-fold), laceration (1.7-fold), and delayed postpartum hemorrhage (1.8-fold).
When the investigators repeated analyses but excluded women with stable risk factors that might be present across the reproductive years, such as fibroids, inherited coagulopathy, and cesarean delivery, the elevated risks of a recurrence of postpartum hemorrhage were essentially unchanged. "This argues that recurrence is mediated by some other factor," maintained Dr. Bateman.
Dr. Bateman disclosed that he had no conflicts of interest related to the research.
MONTEREY, CALIF. – Women have a substantially elevated risk of postpartum hemorrhage after a first occurrence, a prospective population-based cohort study has shown.
The study of more than half a million primiparas and roughly 1 million deliveries in Sweden found that women who had postpartum hemorrhage in their first pregnancy were more than three times as likely to have this complication again in their second pregnancy. Risk increased with the severity of hemorrhage in the first pregnancy and with the number of affected pregnancies.
In additional findings, a history of postpartum hemorrhage due to one etiology, for example, uterine atony or retained placenta, increased the risk not only of a recurrence of hemorrhage due to the same etiology but also of occurrence of hemorrhage due to other etiologies.
"The fact that a history of postpartum hemorrhage of one subtype confers risk of other subtypes in a subsequent pregnancy suggests that there are likely shared pathological features across the different etiologies, and I think this is going to be a very interesting area to examine in the future," commented lead investigator Dr. Brian T. Bateman, an anesthesiologist at Harvard Medical School, Boston, at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
"We could speculate that it might be undiagnosed coagulopathy that explains the shared risk or perhaps characteristics of labor, placentation, or other factors. Given the strong pattern of recurrence, perhaps these are even genetic in nature," he added.
In upcoming research, the investigators will look further into possible explanations. "We are planning to collect a series of women with recurrent hemorrhage, particularly women with hemorrhage from discordant causes, and examine in real granular detail what might be mediating these effects that we are observing at the population level," Dr. Bateman explained. "We are also in the process of conducting familial aggregation studies to determine whether there is a genetic component to postpartum hemorrhage risk."
Session attendee Dr. Richard M. Smiley of Columbia University in New York questioned the reliability of coding of postpartum hemorrhage etiologies in the register used for the study. "It’s really intriguing, the cross-risk, if you will. ... With all due respect to the Swedish database, what’s the chance that that is just miscoded – that a woman bleeds maybe from the same cause, but someone needs to put a cause down on the chart or in the coding system, and they have to pick something, and they pick the wrong thing?" he asked.
"There was a study out of the same database last year looking at the role of obesity as a risk factor for postpartum hemorrhage, and they found when they looked at the risk of postpartum hemorrhage from retained placenta or from laceration, there was no effect of BMI in those categories, but a very, very strong effect on risk of atony, suggesting that there is some specificity in the way that these codes are being applied," Dr. Bateman replied.
Previous research has shown that postpartum hemorrhage is a risk factor for the same complication in subsequent pregnancies, he noted, giving some background to the study. However, "less is known about whether risk accumulates with multiple affected pregnancies and whether the severity of prior postpartum hemorrhage has additional predictive value, and if risk of recurrence varies according to postpartum hemorrhage subtype."
The investigators analyzed data from the Swedish Medical Birth Register. They included 538,332 primiparous women who delivered between 1997 and 2009, and followed this group through 2009, identifying a total of 914,933 subsequent deliveries.
Overall, 5.5% of the women had physician-diagnosed postpartum hemorrhage (an estimated blood loss of greater than 1 L) in their first pregnancy. The rate of this complication in a second pregnancy was higher when the first pregnancy was affected, and the rate was especially high in a third pregnancy when both a first and second pregnancy were affected.
Relative to their counterparts who did not have postpartum hemorrhage in their first pregnancy, women who had postpartum hemorrhage that was not severe, meaning it did not require transfusion, had increased risks of both nonsevere and severe postpartum hemorrhage in a second pregnancy (relative risk, 3.2 and 3.4, respectively).
The respective elevations of risks were even greater in women who had severe postpartum hemorrhage in their first pregnancy (RR, 4.2 and 6.9), "suggesting that severity of hemorrhage does add additional predictive value and can be potentially helpful in triaging high-risk patients," Dr. Bateman said.
Additional analyses showed that postpartum hemorrhage in the first pregnancy due to one etiology increased the risk of postpartum hemorrhage in the second pregnancy due to both that etiology and others. "These findings are really quite surprising and are novel," he commented.
For example, women who had hemorrhage due to uterine atony in their first pregnancy had a 3.9-fold higher risk of hemorrhage due to uterine atony in their second pregnancy. But they also had increased risks of postpartum hemorrhage due to retained placenta (3.1-fold), laceration (1.7-fold), and delayed postpartum hemorrhage (1.8-fold).
When the investigators repeated analyses but excluded women with stable risk factors that might be present across the reproductive years, such as fibroids, inherited coagulopathy, and cesarean delivery, the elevated risks of a recurrence of postpartum hemorrhage were essentially unchanged. "This argues that recurrence is mediated by some other factor," maintained Dr. Bateman.
Dr. Bateman disclosed that he had no conflicts of interest related to the research.
MONTEREY, CALIF. – Women have a substantially elevated risk of postpartum hemorrhage after a first occurrence, a prospective population-based cohort study has shown.
The study of more than half a million primiparas and roughly 1 million deliveries in Sweden found that women who had postpartum hemorrhage in their first pregnancy were more than three times as likely to have this complication again in their second pregnancy. Risk increased with the severity of hemorrhage in the first pregnancy and with the number of affected pregnancies.
In additional findings, a history of postpartum hemorrhage due to one etiology, for example, uterine atony or retained placenta, increased the risk not only of a recurrence of hemorrhage due to the same etiology but also of occurrence of hemorrhage due to other etiologies.
"The fact that a history of postpartum hemorrhage of one subtype confers risk of other subtypes in a subsequent pregnancy suggests that there are likely shared pathological features across the different etiologies, and I think this is going to be a very interesting area to examine in the future," commented lead investigator Dr. Brian T. Bateman, an anesthesiologist at Harvard Medical School, Boston, at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
"We could speculate that it might be undiagnosed coagulopathy that explains the shared risk or perhaps characteristics of labor, placentation, or other factors. Given the strong pattern of recurrence, perhaps these are even genetic in nature," he added.
In upcoming research, the investigators will look further into possible explanations. "We are planning to collect a series of women with recurrent hemorrhage, particularly women with hemorrhage from discordant causes, and examine in real granular detail what might be mediating these effects that we are observing at the population level," Dr. Bateman explained. "We are also in the process of conducting familial aggregation studies to determine whether there is a genetic component to postpartum hemorrhage risk."
Session attendee Dr. Richard M. Smiley of Columbia University in New York questioned the reliability of coding of postpartum hemorrhage etiologies in the register used for the study. "It’s really intriguing, the cross-risk, if you will. ... With all due respect to the Swedish database, what’s the chance that that is just miscoded – that a woman bleeds maybe from the same cause, but someone needs to put a cause down on the chart or in the coding system, and they have to pick something, and they pick the wrong thing?" he asked.
"There was a study out of the same database last year looking at the role of obesity as a risk factor for postpartum hemorrhage, and they found when they looked at the risk of postpartum hemorrhage from retained placenta or from laceration, there was no effect of BMI in those categories, but a very, very strong effect on risk of atony, suggesting that there is some specificity in the way that these codes are being applied," Dr. Bateman replied.
Previous research has shown that postpartum hemorrhage is a risk factor for the same complication in subsequent pregnancies, he noted, giving some background to the study. However, "less is known about whether risk accumulates with multiple affected pregnancies and whether the severity of prior postpartum hemorrhage has additional predictive value, and if risk of recurrence varies according to postpartum hemorrhage subtype."
The investigators analyzed data from the Swedish Medical Birth Register. They included 538,332 primiparous women who delivered between 1997 and 2009, and followed this group through 2009, identifying a total of 914,933 subsequent deliveries.
Overall, 5.5% of the women had physician-diagnosed postpartum hemorrhage (an estimated blood loss of greater than 1 L) in their first pregnancy. The rate of this complication in a second pregnancy was higher when the first pregnancy was affected, and the rate was especially high in a third pregnancy when both a first and second pregnancy were affected.
Relative to their counterparts who did not have postpartum hemorrhage in their first pregnancy, women who had postpartum hemorrhage that was not severe, meaning it did not require transfusion, had increased risks of both nonsevere and severe postpartum hemorrhage in a second pregnancy (relative risk, 3.2 and 3.4, respectively).
The respective elevations of risks were even greater in women who had severe postpartum hemorrhage in their first pregnancy (RR, 4.2 and 6.9), "suggesting that severity of hemorrhage does add additional predictive value and can be potentially helpful in triaging high-risk patients," Dr. Bateman said.
Additional analyses showed that postpartum hemorrhage in the first pregnancy due to one etiology increased the risk of postpartum hemorrhage in the second pregnancy due to both that etiology and others. "These findings are really quite surprising and are novel," he commented.
For example, women who had hemorrhage due to uterine atony in their first pregnancy had a 3.9-fold higher risk of hemorrhage due to uterine atony in their second pregnancy. But they also had increased risks of postpartum hemorrhage due to retained placenta (3.1-fold), laceration (1.7-fold), and delayed postpartum hemorrhage (1.8-fold).
When the investigators repeated analyses but excluded women with stable risk factors that might be present across the reproductive years, such as fibroids, inherited coagulopathy, and cesarean delivery, the elevated risks of a recurrence of postpartum hemorrhage were essentially unchanged. "This argues that recurrence is mediated by some other factor," maintained Dr. Bateman.
Dr. Bateman disclosed that he had no conflicts of interest related to the research.
FROM THE ANNUAL MEETING OF THE SOCIETY FOR OBSTETRIC ANESTHESIA AND PERINATOLOGY
New Model Developed for Identifying Placenta Accreta
MONTEREY, CALIF. – A new model may help take the guesswork out of identifying placenta accreta before cesarean delivery, possibly sparing some women unnecessary interventions such as general anesthesia, placement of large-bore IV lines, and elective hysterectomy.
A study team led by Dr. Carolyn F. Weiniger, an obstetrical anesthesiologist at the Hadassah Hebrew University Medical Center in Jerusalem, reviewed data for 46,623 women who were delivered at the center over a 9-year period.

They identified 92 women with antenatally suspected placenta accreta, of whom only 52 (56%) were confirmed to have had the condition at the time of surgery, she reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
At a maximal-sensitivity cut-off, a predictive model based on just three clinical factors that would be assessed in any woman evaluated for suspected placenta accreta – the presence of placenta previa (yes vs. no), the number of previous cesarean deliveries, and ultrasound suspicion of accreta (high vs. low) – identified 100% of the women who were confirmed to have the condition. The trade-off was a low specificity of 25%.
However, at the optimal cut-off, the model still identified 94% of the women who were confirmed to have placenta accreta, and specificity was better (53%).
The investigators developed a nomogram based on the model that should be easy to apply clinically, according to Dr. Weiniger. "This nomogram could be a laminated card which a physician could sit with at his desk when faced with a suspected placenta accreta patient, to decide whether she is above or below our cut point, whether we think she actually does or does not have placenta accreta," she explained.
Although the study involves one of the largest series of patients with placenta accreta, it still had a fairly small sample size, she acknowledged. "In order to validate such data, a multicenter study would be appropriate."
"Have you changed your practice ... based on your nomogram?" asked Dr. Vilma E. Ortiz, session moderator and an anesthesiologist at the Massachusetts General Hospital in Boston.
"We have just created the nomogram, just finished analyzing the statistics. We haven’t yet had an accreta patient," Dr. Weiniger replied. "But I think as we become much more experienced at managing these patients, in patients who we feel comfortable [that they] have got no risk or low suspicion [of accreta], we will do regional anesthesia."
During the study period, her center’s management in cases of suspected accreta typically included general anesthesia, the booking of an ICU bed, the insertion of two large-bore IVs, and the placement of loops on the internal iliac vessels to aid with hemostasis. It did not include planned cesarean hysterectomy.
"Surgeons were not aware of our primary study outcome [that is, the rate of surgically diagnosed accreta among all cases of antenatally suspected accreta] in order to avoid bias," she noted.
A comparison of the 52 women with and 40 women without surgically confirmed accreta showed that they were statistically indistinguishable with respect to many clinical factors. But they differed significantly on the number of previous cesarean deliveries, the presence of placenta previa, and the presence of ultrasound signs of accreta.
The predictive model based on these three factors had an area under the receiver operating characteristic curve of 0.846, according to Dr. Weiniger. "When we tried to add maternal age and antenatal bleeding, because [these factors have been found to be predictive] in previous studies, it did not improve the area under the curve."
Giving some examples using the new nomogram, she noted that a woman having two previous cesarean deliveries who has placenta previa and a high-suspicion ultrasound would have a probability score approaching 80%, which falls well above cut points based on both 100% and 94% model sensitivity. "So she would be classified as having placenta accreta and would require massive hemorrhage preparation for surgery."
In contrast, a woman having two previous cesarean deliveries who does not have placenta previa and has a low-suspicion ultrasound would have a probability score of almost 0%, which falls well below the cut points, and she would be classified as not having placenta accreta. "So we could manage her with regional anesthesia and maybe not do preparations for massive hemorrhage," Dr. Weiniger commented.
Finally, a woman having two previous cesarean deliveries who has a low-suspicion ultrasound but does have placenta previa would have a probability score of about 20%. This score falls above the cut point corresponding to 100% sensitivity, "so if that was the clinician’s practice, that patient would have massive hemorrhage preparations," she said. "But if we were using the 94% sensitivity, the optimal cut point, she would be right on that, so it would be equivocal as to whether we would classify her as having massive transfusion requirements or not. Possibly, the state of her airway would define how we would manage such a patient."
Dr. Weiniger disclosed no relevant conflicts of interest.
MONTEREY, CALIF. – A new model may help take the guesswork out of identifying placenta accreta before cesarean delivery, possibly sparing some women unnecessary interventions such as general anesthesia, placement of large-bore IV lines, and elective hysterectomy.
A study team led by Dr. Carolyn F. Weiniger, an obstetrical anesthesiologist at the Hadassah Hebrew University Medical Center in Jerusalem, reviewed data for 46,623 women who were delivered at the center over a 9-year period.
They identified 92 women with antenatally suspected placenta accreta, of whom only 52 (56%) were confirmed to have had the condition at the time of surgery, she reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
At a maximal-sensitivity cut-off, a predictive model based on just three clinical factors that would be assessed in any woman evaluated for suspected placenta accreta – the presence of placenta previa (yes vs. no), the number of previous cesarean deliveries, and ultrasound suspicion of accreta (high vs. low) – identified 100% of the women who were confirmed to have the condition. The trade-off was a low specificity of 25%.
However, at the optimal cut-off, the model still identified 94% of the women who were confirmed to have placenta accreta, and specificity was better (53%).
The investigators developed a nomogram based on the model that should be easy to apply clinically, according to Dr. Weiniger. "This nomogram could be a laminated card which a physician could sit with at his desk when faced with a suspected placenta accreta patient, to decide whether she is above or below our cut point, whether we think she actually does or does not have placenta accreta," she explained.
Although the study involves one of the largest series of patients with placenta accreta, it still had a fairly small sample size, she acknowledged. "In order to validate such data, a multicenter study would be appropriate."
"Have you changed your practice ... based on your nomogram?" asked Dr. Vilma E. Ortiz, session moderator and an anesthesiologist at the Massachusetts General Hospital in Boston.
"We have just created the nomogram, just finished analyzing the statistics. We haven’t yet had an accreta patient," Dr. Weiniger replied. "But I think as we become much more experienced at managing these patients, in patients who we feel comfortable [that they] have got no risk or low suspicion [of accreta], we will do regional anesthesia."
During the study period, her center’s management in cases of suspected accreta typically included general anesthesia, the booking of an ICU bed, the insertion of two large-bore IVs, and the placement of loops on the internal iliac vessels to aid with hemostasis. It did not include planned cesarean hysterectomy.
"Surgeons were not aware of our primary study outcome [that is, the rate of surgically diagnosed accreta among all cases of antenatally suspected accreta] in order to avoid bias," she noted.
A comparison of the 52 women with and 40 women without surgically confirmed accreta showed that they were statistically indistinguishable with respect to many clinical factors. But they differed significantly on the number of previous cesarean deliveries, the presence of placenta previa, and the presence of ultrasound signs of accreta.
The predictive model based on these three factors had an area under the receiver operating characteristic curve of 0.846, according to Dr. Weiniger. "When we tried to add maternal age and antenatal bleeding, because [these factors have been found to be predictive] in previous studies, it did not improve the area under the curve."
Giving some examples using the new nomogram, she noted that a woman having two previous cesarean deliveries who has placenta previa and a high-suspicion ultrasound would have a probability score approaching 80%, which falls well above cut points based on both 100% and 94% model sensitivity. "So she would be classified as having placenta accreta and would require massive hemorrhage preparation for surgery."
In contrast, a woman having two previous cesarean deliveries who does not have placenta previa and has a low-suspicion ultrasound would have a probability score of almost 0%, which falls well below the cut points, and she would be classified as not having placenta accreta. "So we could manage her with regional anesthesia and maybe not do preparations for massive hemorrhage," Dr. Weiniger commented.
Finally, a woman having two previous cesarean deliveries who has a low-suspicion ultrasound but does have placenta previa would have a probability score of about 20%. This score falls above the cut point corresponding to 100% sensitivity, "so if that was the clinician’s practice, that patient would have massive hemorrhage preparations," she said. "But if we were using the 94% sensitivity, the optimal cut point, she would be right on that, so it would be equivocal as to whether we would classify her as having massive transfusion requirements or not. Possibly, the state of her airway would define how we would manage such a patient."
Dr. Weiniger disclosed no relevant conflicts of interest.
MONTEREY, CALIF. – A new model may help take the guesswork out of identifying placenta accreta before cesarean delivery, possibly sparing some women unnecessary interventions such as general anesthesia, placement of large-bore IV lines, and elective hysterectomy.
A study team led by Dr. Carolyn F. Weiniger, an obstetrical anesthesiologist at the Hadassah Hebrew University Medical Center in Jerusalem, reviewed data for 46,623 women who were delivered at the center over a 9-year period.
They identified 92 women with antenatally suspected placenta accreta, of whom only 52 (56%) were confirmed to have had the condition at the time of surgery, she reported at the annual meeting of the Society for Obstetric Anesthesia and Perinatology.
At a maximal-sensitivity cut-off, a predictive model based on just three clinical factors that would be assessed in any woman evaluated for suspected placenta accreta – the presence of placenta previa (yes vs. no), the number of previous cesarean deliveries, and ultrasound suspicion of accreta (high vs. low) – identified 100% of the women who were confirmed to have the condition. The trade-off was a low specificity of 25%.
However, at the optimal cut-off, the model still identified 94% of the women who were confirmed to have placenta accreta, and specificity was better (53%).
The investigators developed a nomogram based on the model that should be easy to apply clinically, according to Dr. Weiniger. "This nomogram could be a laminated card which a physician could sit with at his desk when faced with a suspected placenta accreta patient, to decide whether she is above or below our cut point, whether we think she actually does or does not have placenta accreta," she explained.
Although the study involves one of the largest series of patients with placenta accreta, it still had a fairly small sample size, she acknowledged. "In order to validate such data, a multicenter study would be appropriate."
"Have you changed your practice ... based on your nomogram?" asked Dr. Vilma E. Ortiz, session moderator and an anesthesiologist at the Massachusetts General Hospital in Boston.
"We have just created the nomogram, just finished analyzing the statistics. We haven’t yet had an accreta patient," Dr. Weiniger replied. "But I think as we become much more experienced at managing these patients, in patients who we feel comfortable [that they] have got no risk or low suspicion [of accreta], we will do regional anesthesia."
During the study period, her center’s management in cases of suspected accreta typically included general anesthesia, the booking of an ICU bed, the insertion of two large-bore IVs, and the placement of loops on the internal iliac vessels to aid with hemostasis. It did not include planned cesarean hysterectomy.
"Surgeons were not aware of our primary study outcome [that is, the rate of surgically diagnosed accreta among all cases of antenatally suspected accreta] in order to avoid bias," she noted.
A comparison of the 52 women with and 40 women without surgically confirmed accreta showed that they were statistically indistinguishable with respect to many clinical factors. But they differed significantly on the number of previous cesarean deliveries, the presence of placenta previa, and the presence of ultrasound signs of accreta.
The predictive model based on these three factors had an area under the receiver operating characteristic curve of 0.846, according to Dr. Weiniger. "When we tried to add maternal age and antenatal bleeding, because [these factors have been found to be predictive] in previous studies, it did not improve the area under the curve."
Giving some examples using the new nomogram, she noted that a woman having two previous cesarean deliveries who has placenta previa and a high-suspicion ultrasound would have a probability score approaching 80%, which falls well above cut points based on both 100% and 94% model sensitivity. "So she would be classified as having placenta accreta and would require massive hemorrhage preparation for surgery."
In contrast, a woman having two previous cesarean deliveries who does not have placenta previa and has a low-suspicion ultrasound would have a probability score of almost 0%, which falls well below the cut points, and she would be classified as not having placenta accreta. "So we could manage her with regional anesthesia and maybe not do preparations for massive hemorrhage," Dr. Weiniger commented.
Finally, a woman having two previous cesarean deliveries who has a low-suspicion ultrasound but does have placenta previa would have a probability score of about 20%. This score falls above the cut point corresponding to 100% sensitivity, "so if that was the clinician’s practice, that patient would have massive hemorrhage preparations," she said. "But if we were using the 94% sensitivity, the optimal cut point, she would be right on that, so it would be equivocal as to whether we would classify her as having massive transfusion requirements or not. Possibly, the state of her airway would define how we would manage such a patient."
Dr. Weiniger disclosed no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE SOCIETY FOR OBSTETRIC ANESTHESIA AND PERINATOLOGY