User login
ICD-10 Codes: More Specificity With More Characters
As I have mentioned in prior columns, the key to success with International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) coding will be additional specificity, which will come in the form of more characters to communicate with payors and statisticians regarding the services that have been provided during the office visit. The addition of characters will permit more information about the visit to be delivered in the code.
Some of these additional characters will be required to submit the code for processing. Specifically look out for codes that communicate accidents or injury. Some common circumstances for dermatologists will be lacerations, abrasions, laceration repairs, and burns. The structure of the ICD-10-CM codes is outlined below to explain circumstances in which the increased number of characters will be most important for dermatologists.
The ICD-10-CM codes will be 3 to 7 characters long.1 The first 3 characters are the general categories. For example, L70 is the 3-character category for acne and L40 is the category for psoriasis. The next 3 characters (ie, characters 4–6) correspond to the related etiology (ie, the cause, set of causes, manner of causation of a disease or condition), anatomic site, severity, and other vital clinical details.1
Take the case of a burn on the hand. With the International Classification of Diseases, Ninth Revision, a first-degree burn on the back of the hand is coded with 5 characters (944.16).2 According to the ICD-10-CM coding system, the code for an initial visit for a first-degree burn on the back of the hand would include 7 characters (T23.169A).1 There will be times when the sixth character may not be necessary; in these instances, an X must be placed in this position as a placeholder, but the absence of a sixth character does not negate the need for a seventh. Thankfully, the seventh character can only be 1 of 3 letters. As illustrated above in the code for a first-degree burn on the back of the hand, the A designates an initial encounter; a D would designate a follow-up visit for this burn, and an S would represent a sequela from the initial burn, such as a postinflammatory change, which would have its own code.1
Conclusion
To be reimbursed, appropriate ICD-10-CM codes must be used. Be sure to master the structure of these codes before the October 1, 2015, compliance deadline; plan now for a training and testing period.
1. Centers for Medicare & Medicaid Services. ICD-10-CM Tabular List of Diseases and Injuries. http://www.cms.gov/Medicare/Coding/ICD10/downloads/6_I10tab2010.pdf. Published 2010. Accessed September 18, 2014.
2. ICD-9 code lookup. Centers for Medicare & Medicaid Services Web site. http://www.cms.gov/medicare-coverage-database/staticpages/icd-9-code-lookup.aspx. Accessed September 18, 2014.
As I have mentioned in prior columns, the key to success with International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) coding will be additional specificity, which will come in the form of more characters to communicate with payors and statisticians regarding the services that have been provided during the office visit. The addition of characters will permit more information about the visit to be delivered in the code.
Some of these additional characters will be required to submit the code for processing. Specifically look out for codes that communicate accidents or injury. Some common circumstances for dermatologists will be lacerations, abrasions, laceration repairs, and burns. The structure of the ICD-10-CM codes is outlined below to explain circumstances in which the increased number of characters will be most important for dermatologists.
The ICD-10-CM codes will be 3 to 7 characters long.1 The first 3 characters are the general categories. For example, L70 is the 3-character category for acne and L40 is the category for psoriasis. The next 3 characters (ie, characters 4–6) correspond to the related etiology (ie, the cause, set of causes, manner of causation of a disease or condition), anatomic site, severity, and other vital clinical details.1
Take the case of a burn on the hand. With the International Classification of Diseases, Ninth Revision, a first-degree burn on the back of the hand is coded with 5 characters (944.16).2 According to the ICD-10-CM coding system, the code for an initial visit for a first-degree burn on the back of the hand would include 7 characters (T23.169A).1 There will be times when the sixth character may not be necessary; in these instances, an X must be placed in this position as a placeholder, but the absence of a sixth character does not negate the need for a seventh. Thankfully, the seventh character can only be 1 of 3 letters. As illustrated above in the code for a first-degree burn on the back of the hand, the A designates an initial encounter; a D would designate a follow-up visit for this burn, and an S would represent a sequela from the initial burn, such as a postinflammatory change, which would have its own code.1
Conclusion
To be reimbursed, appropriate ICD-10-CM codes must be used. Be sure to master the structure of these codes before the October 1, 2015, compliance deadline; plan now for a training and testing period.
As I have mentioned in prior columns, the key to success with International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) coding will be additional specificity, which will come in the form of more characters to communicate with payors and statisticians regarding the services that have been provided during the office visit. The addition of characters will permit more information about the visit to be delivered in the code.
Some of these additional characters will be required to submit the code for processing. Specifically look out for codes that communicate accidents or injury. Some common circumstances for dermatologists will be lacerations, abrasions, laceration repairs, and burns. The structure of the ICD-10-CM codes is outlined below to explain circumstances in which the increased number of characters will be most important for dermatologists.
The ICD-10-CM codes will be 3 to 7 characters long.1 The first 3 characters are the general categories. For example, L70 is the 3-character category for acne and L40 is the category for psoriasis. The next 3 characters (ie, characters 4–6) correspond to the related etiology (ie, the cause, set of causes, manner of causation of a disease or condition), anatomic site, severity, and other vital clinical details.1
Take the case of a burn on the hand. With the International Classification of Diseases, Ninth Revision, a first-degree burn on the back of the hand is coded with 5 characters (944.16).2 According to the ICD-10-CM coding system, the code for an initial visit for a first-degree burn on the back of the hand would include 7 characters (T23.169A).1 There will be times when the sixth character may not be necessary; in these instances, an X must be placed in this position as a placeholder, but the absence of a sixth character does not negate the need for a seventh. Thankfully, the seventh character can only be 1 of 3 letters. As illustrated above in the code for a first-degree burn on the back of the hand, the A designates an initial encounter; a D would designate a follow-up visit for this burn, and an S would represent a sequela from the initial burn, such as a postinflammatory change, which would have its own code.1
Conclusion
To be reimbursed, appropriate ICD-10-CM codes must be used. Be sure to master the structure of these codes before the October 1, 2015, compliance deadline; plan now for a training and testing period.
1. Centers for Medicare & Medicaid Services. ICD-10-CM Tabular List of Diseases and Injuries. http://www.cms.gov/Medicare/Coding/ICD10/downloads/6_I10tab2010.pdf. Published 2010. Accessed September 18, 2014.
2. ICD-9 code lookup. Centers for Medicare & Medicaid Services Web site. http://www.cms.gov/medicare-coverage-database/staticpages/icd-9-code-lookup.aspx. Accessed September 18, 2014.
1. Centers for Medicare & Medicaid Services. ICD-10-CM Tabular List of Diseases and Injuries. http://www.cms.gov/Medicare/Coding/ICD10/downloads/6_I10tab2010.pdf. Published 2010. Accessed September 18, 2014.
2. ICD-9 code lookup. Centers for Medicare & Medicaid Services Web site. http://www.cms.gov/medicare-coverage-database/staticpages/icd-9-code-lookup.aspx. Accessed September 18, 2014.
Practice Points
- The addition of characters in International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes will permit more information about the visit to be communicated to payors and statisticians.
- Codes with ICD-10-CM will be 3 to 7 characters long and indicate the disease category, followed by the related etiology, anatomic site, severity, and other vital clinical details. The last character is 1 of 3 letters to indicate if the visit is an initial encounter, subsequent encounter, or sequela.
Private Practice Will Survive But Patient Billing Will Not
For many years I have advised physicians that aggressive management of accounts receivable is the key to financial health for any private practice. In the current health care reform climate, it has become more important than ever. A crucial step toward proper management of accounts receivable in the age of the Patient Protection and Affordable Care Act is minimization, if not outright elimination, of patient billing, which is a hallowed yet obsolete tradition in private practice. Billing, in effect, is extending free credit to patients, and independent physicians can no longer afford it.
Some physicians of a traditional bent cling to the idea that accepting credit cards or even asking for payment at the time of service smacks of “storekeeping.” They feel more comfortable billing patients for outstanding balances but complain that their bills often are ignored; with each passing day following treatment in your office, the likelihood decreases that a patient will pay the bill.
Patient billing also is expensive. When you total the costs of materials, postage, and staff labor, each bill can cost anywhere from $2 to $10 or more. Every minute the office staff spends producing and mailing bills is time not spent on more productive work. Billing services are an alternative, but they also are expensive, and those bills get ignored too. Requiring immediate payment may seem distasteful to some physicians, but for physicians who wish to keep their office private and independent, it is rapidly becoming the only viable option.
Health Savings Accounts
Private practices will need to become increasingly flexible in how they accept payments as the population continues to age. This flexibility becomes increasingly important as more and more patients rely on health savings accounts (HSAs). Enrollment in these specialized, tax-deductible, tax-free accounts has increased 10-fold over the last decade.1 Private practice physicians will want to accommodate for HSAs as much as possible.
A few credit companies are already promoting cards to finance HSAs and other private-pay portions of health care expenses, such as The HELPcard (www.helpcard.com). Major credit card companies also have begun to appreciate this largely untapped segment of potential business for them. Soon you may begin receiving help from them in setting up creative payment plans for your patients. Some financial institutions have even begun creating medical credit and debit cards called health benefit cards that are designed specifically for use at physicians’ offices.2
Credit and Debit Cards
Credit and debit cards eliminate many of the problems associated with patient billing. They allow you to collect more fees at the time of service while you still have the patient’s attention and the service you provided is still appreciated.
Charging to a credit or debit card also reduces the chances of a balance owed falling through the cracks, getting lost in the mail, or getting embezzled, and it cannot bounce so it is better than a check. Card payments also can improve your practice’s cash flow, which is always a welcome benefit. Additionally, if a patient is delinquent in paying a credit card bill, it is the credit card company’s problem, not yours.
Credit cards also offer more payment flexibility for patients. In the case of a large balance, offer your patient the option of charging all of the services to a credit card, which he/she can then pay off in affordable monthly installments. Your practice will get reimbursed in full, even as the patient is paying it off slowly, and the patient is able to pay off the debt at a pace that makes sense for his/her finances.
Payment Policies
Beyond simply accepting credit cards, the next step is one that every hotel, rental car agency, and many other businesses have used for years: Retain a card number in each patient’s file, and bill balances as they come in.
Every new patient in my office receives a letter at his/her first visit explaining our policy: We will keep a credit card number on file and use it to bill any outstanding balances after third parties pay their portion. At the bottom of the letter is a brief statement of consent for the patient to sign, along with a place to write the credit card number and expiration date. This policy also comes in handy for patients who claim to have come to the office without cash, a checkbook, credit cards, or any other method of payment. In such situations, my office manager can say, “No problem, we have your credit card information on file!”
Do patients object to this policy? Some do, mostly older patients. But when we explain that we are doing nothing different than hotels do at check-in and that this policy also will work to their advantage by decreasing the number of bills they receive and checks they must write, most come around. Make it an option at first if you wish; then, when everyone is accustomed, you can make it a mandatory policy. My office manager has the authority to make exceptions on a case-by-case basis when necessary.
Do patients worry about confidentiality or unauthorized use? Most individuals do not worry when they use a credit card at a restaurant, hotel, or the Internet. Guard your patients’ financial information as carefully as their medical information. If you have electronic health records, the patient’s credit card number can go in the medical chart. Otherwise use a separate portable filing system that can be locked up each night.
Does this policy work? In only 1 year, my total accounts receivable dropped by nearly 50%; after another year they stabilized at 30% to 35% of prior levels and have remained there ever since, which was a source of consternation for our new accountant who we hired shortly thereafter. “Something must be wrong,” he said nervously after his first look at our books. “Accounts receivable totals are never that low in a medical office with your level of volume.” His eyes widened as I explained our system. “Why doesn’t every private practice do that?” he asked. Why, indeed.
Final Thoughts
The business of health care delivery is currently being rocked at its foundations, as I have been detailing in this column. Without considerable adaptation to these fundamental changes, a private practice can do little more than survive, and even that will take luck. A crucial component of adaptation involves doing more of what we do best, treating patients. Leave the business of extending credit to the banks and credit card companies.
1. Stroud M. Making the most of that shiny new HSA. Reuters. April 19, 2012. http://www.reuters.com/article/2012/04/19/us-healthcare-savings-idU BRE83I0ZI20120419. Accessed September 16, 2014.
2. Prater C. Is there a health care debit card in your future? CreditCards.com Web site. http://www.credit cards.com/credit-card-news/payment-cards-health-care-expenses-1271.php. Published April 14, 2009. Accessed September 16, 2014.
For many years I have advised physicians that aggressive management of accounts receivable is the key to financial health for any private practice. In the current health care reform climate, it has become more important than ever. A crucial step toward proper management of accounts receivable in the age of the Patient Protection and Affordable Care Act is minimization, if not outright elimination, of patient billing, which is a hallowed yet obsolete tradition in private practice. Billing, in effect, is extending free credit to patients, and independent physicians can no longer afford it.
Some physicians of a traditional bent cling to the idea that accepting credit cards or even asking for payment at the time of service smacks of “storekeeping.” They feel more comfortable billing patients for outstanding balances but complain that their bills often are ignored; with each passing day following treatment in your office, the likelihood decreases that a patient will pay the bill.
Patient billing also is expensive. When you total the costs of materials, postage, and staff labor, each bill can cost anywhere from $2 to $10 or more. Every minute the office staff spends producing and mailing bills is time not spent on more productive work. Billing services are an alternative, but they also are expensive, and those bills get ignored too. Requiring immediate payment may seem distasteful to some physicians, but for physicians who wish to keep their office private and independent, it is rapidly becoming the only viable option.
Health Savings Accounts
Private practices will need to become increasingly flexible in how they accept payments as the population continues to age. This flexibility becomes increasingly important as more and more patients rely on health savings accounts (HSAs). Enrollment in these specialized, tax-deductible, tax-free accounts has increased 10-fold over the last decade.1 Private practice physicians will want to accommodate for HSAs as much as possible.
A few credit companies are already promoting cards to finance HSAs and other private-pay portions of health care expenses, such as The HELPcard (www.helpcard.com). Major credit card companies also have begun to appreciate this largely untapped segment of potential business for them. Soon you may begin receiving help from them in setting up creative payment plans for your patients. Some financial institutions have even begun creating medical credit and debit cards called health benefit cards that are designed specifically for use at physicians’ offices.2
Credit and Debit Cards
Credit and debit cards eliminate many of the problems associated with patient billing. They allow you to collect more fees at the time of service while you still have the patient’s attention and the service you provided is still appreciated.
Charging to a credit or debit card also reduces the chances of a balance owed falling through the cracks, getting lost in the mail, or getting embezzled, and it cannot bounce so it is better than a check. Card payments also can improve your practice’s cash flow, which is always a welcome benefit. Additionally, if a patient is delinquent in paying a credit card bill, it is the credit card company’s problem, not yours.
Credit cards also offer more payment flexibility for patients. In the case of a large balance, offer your patient the option of charging all of the services to a credit card, which he/she can then pay off in affordable monthly installments. Your practice will get reimbursed in full, even as the patient is paying it off slowly, and the patient is able to pay off the debt at a pace that makes sense for his/her finances.
Payment Policies
Beyond simply accepting credit cards, the next step is one that every hotel, rental car agency, and many other businesses have used for years: Retain a card number in each patient’s file, and bill balances as they come in.
Every new patient in my office receives a letter at his/her first visit explaining our policy: We will keep a credit card number on file and use it to bill any outstanding balances after third parties pay their portion. At the bottom of the letter is a brief statement of consent for the patient to sign, along with a place to write the credit card number and expiration date. This policy also comes in handy for patients who claim to have come to the office without cash, a checkbook, credit cards, or any other method of payment. In such situations, my office manager can say, “No problem, we have your credit card information on file!”
Do patients object to this policy? Some do, mostly older patients. But when we explain that we are doing nothing different than hotels do at check-in and that this policy also will work to their advantage by decreasing the number of bills they receive and checks they must write, most come around. Make it an option at first if you wish; then, when everyone is accustomed, you can make it a mandatory policy. My office manager has the authority to make exceptions on a case-by-case basis when necessary.
Do patients worry about confidentiality or unauthorized use? Most individuals do not worry when they use a credit card at a restaurant, hotel, or the Internet. Guard your patients’ financial information as carefully as their medical information. If you have electronic health records, the patient’s credit card number can go in the medical chart. Otherwise use a separate portable filing system that can be locked up each night.
Does this policy work? In only 1 year, my total accounts receivable dropped by nearly 50%; after another year they stabilized at 30% to 35% of prior levels and have remained there ever since, which was a source of consternation for our new accountant who we hired shortly thereafter. “Something must be wrong,” he said nervously after his first look at our books. “Accounts receivable totals are never that low in a medical office with your level of volume.” His eyes widened as I explained our system. “Why doesn’t every private practice do that?” he asked. Why, indeed.
Final Thoughts
The business of health care delivery is currently being rocked at its foundations, as I have been detailing in this column. Without considerable adaptation to these fundamental changes, a private practice can do little more than survive, and even that will take luck. A crucial component of adaptation involves doing more of what we do best, treating patients. Leave the business of extending credit to the banks and credit card companies.
For many years I have advised physicians that aggressive management of accounts receivable is the key to financial health for any private practice. In the current health care reform climate, it has become more important than ever. A crucial step toward proper management of accounts receivable in the age of the Patient Protection and Affordable Care Act is minimization, if not outright elimination, of patient billing, which is a hallowed yet obsolete tradition in private practice. Billing, in effect, is extending free credit to patients, and independent physicians can no longer afford it.
Some physicians of a traditional bent cling to the idea that accepting credit cards or even asking for payment at the time of service smacks of “storekeeping.” They feel more comfortable billing patients for outstanding balances but complain that their bills often are ignored; with each passing day following treatment in your office, the likelihood decreases that a patient will pay the bill.
Patient billing also is expensive. When you total the costs of materials, postage, and staff labor, each bill can cost anywhere from $2 to $10 or more. Every minute the office staff spends producing and mailing bills is time not spent on more productive work. Billing services are an alternative, but they also are expensive, and those bills get ignored too. Requiring immediate payment may seem distasteful to some physicians, but for physicians who wish to keep their office private and independent, it is rapidly becoming the only viable option.
Health Savings Accounts
Private practices will need to become increasingly flexible in how they accept payments as the population continues to age. This flexibility becomes increasingly important as more and more patients rely on health savings accounts (HSAs). Enrollment in these specialized, tax-deductible, tax-free accounts has increased 10-fold over the last decade.1 Private practice physicians will want to accommodate for HSAs as much as possible.
A few credit companies are already promoting cards to finance HSAs and other private-pay portions of health care expenses, such as The HELPcard (www.helpcard.com). Major credit card companies also have begun to appreciate this largely untapped segment of potential business for them. Soon you may begin receiving help from them in setting up creative payment plans for your patients. Some financial institutions have even begun creating medical credit and debit cards called health benefit cards that are designed specifically for use at physicians’ offices.2
Credit and Debit Cards
Credit and debit cards eliminate many of the problems associated with patient billing. They allow you to collect more fees at the time of service while you still have the patient’s attention and the service you provided is still appreciated.
Charging to a credit or debit card also reduces the chances of a balance owed falling through the cracks, getting lost in the mail, or getting embezzled, and it cannot bounce so it is better than a check. Card payments also can improve your practice’s cash flow, which is always a welcome benefit. Additionally, if a patient is delinquent in paying a credit card bill, it is the credit card company’s problem, not yours.
Credit cards also offer more payment flexibility for patients. In the case of a large balance, offer your patient the option of charging all of the services to a credit card, which he/she can then pay off in affordable monthly installments. Your practice will get reimbursed in full, even as the patient is paying it off slowly, and the patient is able to pay off the debt at a pace that makes sense for his/her finances.
Payment Policies
Beyond simply accepting credit cards, the next step is one that every hotel, rental car agency, and many other businesses have used for years: Retain a card number in each patient’s file, and bill balances as they come in.
Every new patient in my office receives a letter at his/her first visit explaining our policy: We will keep a credit card number on file and use it to bill any outstanding balances after third parties pay their portion. At the bottom of the letter is a brief statement of consent for the patient to sign, along with a place to write the credit card number and expiration date. This policy also comes in handy for patients who claim to have come to the office without cash, a checkbook, credit cards, or any other method of payment. In such situations, my office manager can say, “No problem, we have your credit card information on file!”
Do patients object to this policy? Some do, mostly older patients. But when we explain that we are doing nothing different than hotels do at check-in and that this policy also will work to their advantage by decreasing the number of bills they receive and checks they must write, most come around. Make it an option at first if you wish; then, when everyone is accustomed, you can make it a mandatory policy. My office manager has the authority to make exceptions on a case-by-case basis when necessary.
Do patients worry about confidentiality or unauthorized use? Most individuals do not worry when they use a credit card at a restaurant, hotel, or the Internet. Guard your patients’ financial information as carefully as their medical information. If you have electronic health records, the patient’s credit card number can go in the medical chart. Otherwise use a separate portable filing system that can be locked up each night.
Does this policy work? In only 1 year, my total accounts receivable dropped by nearly 50%; after another year they stabilized at 30% to 35% of prior levels and have remained there ever since, which was a source of consternation for our new accountant who we hired shortly thereafter. “Something must be wrong,” he said nervously after his first look at our books. “Accounts receivable totals are never that low in a medical office with your level of volume.” His eyes widened as I explained our system. “Why doesn’t every private practice do that?” he asked. Why, indeed.
Final Thoughts
The business of health care delivery is currently being rocked at its foundations, as I have been detailing in this column. Without considerable adaptation to these fundamental changes, a private practice can do little more than survive, and even that will take luck. A crucial component of adaptation involves doing more of what we do best, treating patients. Leave the business of extending credit to the banks and credit card companies.
1. Stroud M. Making the most of that shiny new HSA. Reuters. April 19, 2012. http://www.reuters.com/article/2012/04/19/us-healthcare-savings-idU BRE83I0ZI20120419. Accessed September 16, 2014.
2. Prater C. Is there a health care debit card in your future? CreditCards.com Web site. http://www.credit cards.com/credit-card-news/payment-cards-health-care-expenses-1271.php. Published April 14, 2009. Accessed September 16, 2014.
1. Stroud M. Making the most of that shiny new HSA. Reuters. April 19, 2012. http://www.reuters.com/article/2012/04/19/us-healthcare-savings-idU BRE83I0ZI20120419. Accessed September 16, 2014.
2. Prater C. Is there a health care debit card in your future? CreditCards.com Web site. http://www.credit cards.com/credit-card-news/payment-cards-health-care-expenses-1271.php. Published April 14, 2009. Accessed September 16, 2014.
Practice Points
- Aggressive management of accounts receivable is the key to the financial health of any private practice. Physicians must become increasingly flexible in how they accept payments as the population continues to age.
- Consider requiring patients to supply a credit card or debit card to bill for outstanding balances after third parties pay their portion.
- Accommodate health savings accounts and health benefit cards.

Medical Billing Protocol for Discharge Summary Preparation, Signoff

I just read your article regarding billing. My supervising physician is a surgeon. She and I are both employed by the same hospital. Can she have me dictate the discharge summary before she signs off on it? Or does she have to dictate it because it is in the global post-op period and she is paid for the surgery? If she has me perform an inpatient consult one afternoon/evening, but she doesn't lay eyes on the patient until the following morning, can she bill for the initial consult? Or does she bill for the first subsequent consult? Where is the information to back up your responses, please?
—Concerned with Coding
Dr. Hospitalist responds:
You don’t say so, but I’m assuming you work as a physician assistant (PA) or a nurse practitioner (NP). Since you and your supervising physician are employed by the same hospital, I also assume your fees are assigned to the hospital and you are both considered members of the same “surgical group.”
Just so we’re all on the same page, let’s further define “global surgical” period. Even though there are three types of global surgical packages, they are all based on the number of expected post-operative days. In general, there are the zero- and 10-day post-op periods (for minor procedures) and the 90-day post-op period (for most major procedures). Almost all services, supplies, wound management, and follow-up visits related to the procedure are included in the global surgery payment.
The discharge summary also is part of the global surgery package. When your supervising physician co-signs and validates your note, she can bill as though she did the note herself as defined in the scope of practice and credentialing process at your hospital.
If allowed by your state and sanctioned by your hospital, you can bill separately; however, the global surgery payment would be decreased as per the Medicare Claims Processing Manual (Chapter 12, Sections 40 and 40.1-Physician/Nonphysician Practitioners), which states that “when a NP, PA, or CNS furnish services to a patient during a global surgical period, contractors shall determine the level of NP [nurse practitioner], PA [physician assistant], or CNS [clinical nurse specialist] involvement in furnishing part of the surgeon’s global surgical package consistent with their current practice of processing such claims.” The manual goes on to say that those NP, PA, or CNS services furnished are paid at 80% of the lesser of the actual charge or 85% of what a physician is paid under the Medicare Physician Fee Schedule.
Now you see why it’s more lucrative for the physician to bill than the NP/PA, especially if the extender is working under the “supervision” of the physician.
As I’m sure you’re aware, effective Jan. 1, 2010, the consultation codes were no longer recognized for Medicare Part B payment. Practitioners are directed to code patient evaluation and management (E/M) visits with E/M codes that represent where the visit occurs and identify the complexity of the visit performed.
Medicare directives are pretty clear that in order to bill for a visit, the physician or clinician must have a “face-to-face” encounter with the patient on the day of service billed. There is an opportunity for the physician and NP/PA from the same group practice to bill a split/shared E/M code under either unique physician identification number (UPIN), but the physician must still have a face-to-face encounter on the day of service or the bill must be submitted using the NP/PA’s UPIN (Medicare Claims Processing Manual, Chapter 12 – Physician/Nonphysician Practitioners. Section 30.6.1-Selection of Level of Evaluation and Management Service. Implemented: 01-04-10).
Therefore, in the situation that you describe, the supervising physician must bill for a subsequent visit E/M code.
Occasionally, teaching institutions with residents have formalized agreements with insurers that allow residents to see patients one day, with the attending physician allowed to bill for that day without seeing the patient. You should check with your group’s billing specialist to see if such arrangements have been made for your group.
After taking all this into consideration, however, I perceive the bigger issue as underlying tension or mistrust between you and the supervising physician. I suggest sitting down and having a conversation about scope of practice and expectations, and then you can better determine if you are the right person for that position.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
I just read your article regarding billing. My supervising physician is a surgeon. She and I are both employed by the same hospital. Can she have me dictate the discharge summary before she signs off on it? Or does she have to dictate it because it is in the global post-op period and she is paid for the surgery? If she has me perform an inpatient consult one afternoon/evening, but she doesn't lay eyes on the patient until the following morning, can she bill for the initial consult? Or does she bill for the first subsequent consult? Where is the information to back up your responses, please?
—Concerned with Coding
Dr. Hospitalist responds:
You don’t say so, but I’m assuming you work as a physician assistant (PA) or a nurse practitioner (NP). Since you and your supervising physician are employed by the same hospital, I also assume your fees are assigned to the hospital and you are both considered members of the same “surgical group.”
Just so we’re all on the same page, let’s further define “global surgical” period. Even though there are three types of global surgical packages, they are all based on the number of expected post-operative days. In general, there are the zero- and 10-day post-op periods (for minor procedures) and the 90-day post-op period (for most major procedures). Almost all services, supplies, wound management, and follow-up visits related to the procedure are included in the global surgery payment.
The discharge summary also is part of the global surgery package. When your supervising physician co-signs and validates your note, she can bill as though she did the note herself as defined in the scope of practice and credentialing process at your hospital.
If allowed by your state and sanctioned by your hospital, you can bill separately; however, the global surgery payment would be decreased as per the Medicare Claims Processing Manual (Chapter 12, Sections 40 and 40.1-Physician/Nonphysician Practitioners), which states that “when a NP, PA, or CNS furnish services to a patient during a global surgical period, contractors shall determine the level of NP [nurse practitioner], PA [physician assistant], or CNS [clinical nurse specialist] involvement in furnishing part of the surgeon’s global surgical package consistent with their current practice of processing such claims.” The manual goes on to say that those NP, PA, or CNS services furnished are paid at 80% of the lesser of the actual charge or 85% of what a physician is paid under the Medicare Physician Fee Schedule.
Now you see why it’s more lucrative for the physician to bill than the NP/PA, especially if the extender is working under the “supervision” of the physician.
As I’m sure you’re aware, effective Jan. 1, 2010, the consultation codes were no longer recognized for Medicare Part B payment. Practitioners are directed to code patient evaluation and management (E/M) visits with E/M codes that represent where the visit occurs and identify the complexity of the visit performed.
Medicare directives are pretty clear that in order to bill for a visit, the physician or clinician must have a “face-to-face” encounter with the patient on the day of service billed. There is an opportunity for the physician and NP/PA from the same group practice to bill a split/shared E/M code under either unique physician identification number (UPIN), but the physician must still have a face-to-face encounter on the day of service or the bill must be submitted using the NP/PA’s UPIN (Medicare Claims Processing Manual, Chapter 12 – Physician/Nonphysician Practitioners. Section 30.6.1-Selection of Level of Evaluation and Management Service. Implemented: 01-04-10).
Therefore, in the situation that you describe, the supervising physician must bill for a subsequent visit E/M code.
Occasionally, teaching institutions with residents have formalized agreements with insurers that allow residents to see patients one day, with the attending physician allowed to bill for that day without seeing the patient. You should check with your group’s billing specialist to see if such arrangements have been made for your group.
After taking all this into consideration, however, I perceive the bigger issue as underlying tension or mistrust between you and the supervising physician. I suggest sitting down and having a conversation about scope of practice and expectations, and then you can better determine if you are the right person for that position.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
I just read your article regarding billing. My supervising physician is a surgeon. She and I are both employed by the same hospital. Can she have me dictate the discharge summary before she signs off on it? Or does she have to dictate it because it is in the global post-op period and she is paid for the surgery? If she has me perform an inpatient consult one afternoon/evening, but she doesn't lay eyes on the patient until the following morning, can she bill for the initial consult? Or does she bill for the first subsequent consult? Where is the information to back up your responses, please?
—Concerned with Coding
Dr. Hospitalist responds:
You don’t say so, but I’m assuming you work as a physician assistant (PA) or a nurse practitioner (NP). Since you and your supervising physician are employed by the same hospital, I also assume your fees are assigned to the hospital and you are both considered members of the same “surgical group.”
Just so we’re all on the same page, let’s further define “global surgical” period. Even though there are three types of global surgical packages, they are all based on the number of expected post-operative days. In general, there are the zero- and 10-day post-op periods (for minor procedures) and the 90-day post-op period (for most major procedures). Almost all services, supplies, wound management, and follow-up visits related to the procedure are included in the global surgery payment.
The discharge summary also is part of the global surgery package. When your supervising physician co-signs and validates your note, she can bill as though she did the note herself as defined in the scope of practice and credentialing process at your hospital.
If allowed by your state and sanctioned by your hospital, you can bill separately; however, the global surgery payment would be decreased as per the Medicare Claims Processing Manual (Chapter 12, Sections 40 and 40.1-Physician/Nonphysician Practitioners), which states that “when a NP, PA, or CNS furnish services to a patient during a global surgical period, contractors shall determine the level of NP [nurse practitioner], PA [physician assistant], or CNS [clinical nurse specialist] involvement in furnishing part of the surgeon’s global surgical package consistent with their current practice of processing such claims.” The manual goes on to say that those NP, PA, or CNS services furnished are paid at 80% of the lesser of the actual charge or 85% of what a physician is paid under the Medicare Physician Fee Schedule.
Now you see why it’s more lucrative for the physician to bill than the NP/PA, especially if the extender is working under the “supervision” of the physician.
As I’m sure you’re aware, effective Jan. 1, 2010, the consultation codes were no longer recognized for Medicare Part B payment. Practitioners are directed to code patient evaluation and management (E/M) visits with E/M codes that represent where the visit occurs and identify the complexity of the visit performed.
Medicare directives are pretty clear that in order to bill for a visit, the physician or clinician must have a “face-to-face” encounter with the patient on the day of service billed. There is an opportunity for the physician and NP/PA from the same group practice to bill a split/shared E/M code under either unique physician identification number (UPIN), but the physician must still have a face-to-face encounter on the day of service or the bill must be submitted using the NP/PA’s UPIN (Medicare Claims Processing Manual, Chapter 12 – Physician/Nonphysician Practitioners. Section 30.6.1-Selection of Level of Evaluation and Management Service. Implemented: 01-04-10).
Therefore, in the situation that you describe, the supervising physician must bill for a subsequent visit E/M code.
Occasionally, teaching institutions with residents have formalized agreements with insurers that allow residents to see patients one day, with the attending physician allowed to bill for that day without seeing the patient. You should check with your group’s billing specialist to see if such arrangements have been made for your group.
After taking all this into consideration, however, I perceive the bigger issue as underlying tension or mistrust between you and the supervising physician. I suggest sitting down and having a conversation about scope of practice and expectations, and then you can better determine if you are the right person for that position.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
Clear Identification Needed for Hospitalists in Medicare
In recent months, numerous articles have come out targeting high-billing physicians—looking for smoking guns in recently released 2012 Medicare fee-for-service physician claims data. These data include both the amount each individual physician billed and the amount Medicare paid on average for services performed by all physicians treating Medicare beneficiaries.
Many physician groups, including the AMA, criticized the data release as having significant limitations, including clinical and billing practice realities that confound the layperson’s understanding of the data’s implications. Still, there is much physicians can learn by exploring this information, particularly those in a still-growing field like hospital medicine (HM).
There is no clear method to identify hospitalists within these data. Hospitalists are dispersed throughout their respective board certifications—internal medicine, family practice, pediatrics. The designations come directly from the Medicare specialty billing code; the code associated with the largest number of services becomes that provider’s de facto specialty. For the majority of providers, this will correspond with their board certification and their professional identity. A hospitalist’s unique practice is lost within these general identifiers.
However, the contours of that unique practice may provide some tools to identify hospitalists, albeit roughly, within the data and in the absence of a specialty billing code. Things like practice location and commonly billed Healthcare Common Procedure Coding System (HCPCS) codes can help sketch the boundaries of the field. Certainly, any classification methodology will have its share of imperfections and may exclude individuals who would otherwise identify as hospitalists. Regardless, such an exercise could identify trends in hospital medicine while providing a better understanding of the field as a whole.
HM does not have the traditional hallmark signifiers—board certification and Medicare specialty billing code—used by many specialties and subspecialties to frame their fields and to classify and compare physicians. The Medicare specialty billing code is a unique code applied to Medicare billing claims that tells Medicare exactly how the provider would like to be identified.
Because of its relative specificity and ready accessibility, the Centers for Medicare and Medicaid Services (CMS) uses the specialty billing code to create specialty comparison groups in pay-for-performance programs. Under the value-based payment modifier, hospitalists are compared against outpatient internal medicine or family medicine physicians, which makes them seem all the more expensive and less efficient.
SHM has been attuned to this particular issue since the early days of the physician value-based payment modifier. For nearly two years, SHM has repeatedly admonished CMS to compare hospitalists against other hospitalists in order for a pay-for-performance scheme to fairly and reasonably evaluate quality and efficiency. CMS acknowledged that many specialties and subspecialties may be masked within the current listing of Medicare specialty billing codes but yielded only so far as to say that aggrieved specialties can apply for their own code. SHM, for its part, applied for a specialty billing code for hospitalists in May 2014.
SHM has been actively exploring the data and looking at ways to identify hospitalists within this Medicare data. There’s an inherent value to this sort of self-reflection—it explains who we are and where we have been.
More importantly, it helps inform where we are going.
Joshua Lapps is SHM’s government relations manager.
In recent months, numerous articles have come out targeting high-billing physicians—looking for smoking guns in recently released 2012 Medicare fee-for-service physician claims data. These data include both the amount each individual physician billed and the amount Medicare paid on average for services performed by all physicians treating Medicare beneficiaries.
Many physician groups, including the AMA, criticized the data release as having significant limitations, including clinical and billing practice realities that confound the layperson’s understanding of the data’s implications. Still, there is much physicians can learn by exploring this information, particularly those in a still-growing field like hospital medicine (HM).
There is no clear method to identify hospitalists within these data. Hospitalists are dispersed throughout their respective board certifications—internal medicine, family practice, pediatrics. The designations come directly from the Medicare specialty billing code; the code associated with the largest number of services becomes that provider’s de facto specialty. For the majority of providers, this will correspond with their board certification and their professional identity. A hospitalist’s unique practice is lost within these general identifiers.
However, the contours of that unique practice may provide some tools to identify hospitalists, albeit roughly, within the data and in the absence of a specialty billing code. Things like practice location and commonly billed Healthcare Common Procedure Coding System (HCPCS) codes can help sketch the boundaries of the field. Certainly, any classification methodology will have its share of imperfections and may exclude individuals who would otherwise identify as hospitalists. Regardless, such an exercise could identify trends in hospital medicine while providing a better understanding of the field as a whole.
HM does not have the traditional hallmark signifiers—board certification and Medicare specialty billing code—used by many specialties and subspecialties to frame their fields and to classify and compare physicians. The Medicare specialty billing code is a unique code applied to Medicare billing claims that tells Medicare exactly how the provider would like to be identified.
Because of its relative specificity and ready accessibility, the Centers for Medicare and Medicaid Services (CMS) uses the specialty billing code to create specialty comparison groups in pay-for-performance programs. Under the value-based payment modifier, hospitalists are compared against outpatient internal medicine or family medicine physicians, which makes them seem all the more expensive and less efficient.
SHM has been attuned to this particular issue since the early days of the physician value-based payment modifier. For nearly two years, SHM has repeatedly admonished CMS to compare hospitalists against other hospitalists in order for a pay-for-performance scheme to fairly and reasonably evaluate quality and efficiency. CMS acknowledged that many specialties and subspecialties may be masked within the current listing of Medicare specialty billing codes but yielded only so far as to say that aggrieved specialties can apply for their own code. SHM, for its part, applied for a specialty billing code for hospitalists in May 2014.
SHM has been actively exploring the data and looking at ways to identify hospitalists within this Medicare data. There’s an inherent value to this sort of self-reflection—it explains who we are and where we have been.
More importantly, it helps inform where we are going.
Joshua Lapps is SHM’s government relations manager.
In recent months, numerous articles have come out targeting high-billing physicians—looking for smoking guns in recently released 2012 Medicare fee-for-service physician claims data. These data include both the amount each individual physician billed and the amount Medicare paid on average for services performed by all physicians treating Medicare beneficiaries.
Many physician groups, including the AMA, criticized the data release as having significant limitations, including clinical and billing practice realities that confound the layperson’s understanding of the data’s implications. Still, there is much physicians can learn by exploring this information, particularly those in a still-growing field like hospital medicine (HM).
There is no clear method to identify hospitalists within these data. Hospitalists are dispersed throughout their respective board certifications—internal medicine, family practice, pediatrics. The designations come directly from the Medicare specialty billing code; the code associated with the largest number of services becomes that provider’s de facto specialty. For the majority of providers, this will correspond with their board certification and their professional identity. A hospitalist’s unique practice is lost within these general identifiers.
However, the contours of that unique practice may provide some tools to identify hospitalists, albeit roughly, within the data and in the absence of a specialty billing code. Things like practice location and commonly billed Healthcare Common Procedure Coding System (HCPCS) codes can help sketch the boundaries of the field. Certainly, any classification methodology will have its share of imperfections and may exclude individuals who would otherwise identify as hospitalists. Regardless, such an exercise could identify trends in hospital medicine while providing a better understanding of the field as a whole.
HM does not have the traditional hallmark signifiers—board certification and Medicare specialty billing code—used by many specialties and subspecialties to frame their fields and to classify and compare physicians. The Medicare specialty billing code is a unique code applied to Medicare billing claims that tells Medicare exactly how the provider would like to be identified.
Because of its relative specificity and ready accessibility, the Centers for Medicare and Medicaid Services (CMS) uses the specialty billing code to create specialty comparison groups in pay-for-performance programs. Under the value-based payment modifier, hospitalists are compared against outpatient internal medicine or family medicine physicians, which makes them seem all the more expensive and less efficient.
SHM has been attuned to this particular issue since the early days of the physician value-based payment modifier. For nearly two years, SHM has repeatedly admonished CMS to compare hospitalists against other hospitalists in order for a pay-for-performance scheme to fairly and reasonably evaluate quality and efficiency. CMS acknowledged that many specialties and subspecialties may be masked within the current listing of Medicare specialty billing codes but yielded only so far as to say that aggrieved specialties can apply for their own code. SHM, for its part, applied for a specialty billing code for hospitalists in May 2014.
SHM has been actively exploring the data and looking at ways to identify hospitalists within this Medicare data. There’s an inherent value to this sort of self-reflection—it explains who we are and where we have been.
More importantly, it helps inform where we are going.
Joshua Lapps is SHM’s government relations manager.
CODE-H Interactive Tool Guides Hospitalists in Coding Decisions
Have you ever worried about which billing code is appropriate? Worried that your coding decisions could be called into question, but reading up on the topic only left you more confused?
SHM’s new, first-of-its-kind online educational tool can help.
CODE-H Interactive—short for “Coding Optimally for Documenting Effectively for Hospitalists”—gives hospitalists an online guided tour through six different coding scenarios, enabling them to choose the codes they believe are appropriate. Then, SHM’s coding expert highlights the correct codes and offers rationales for each.
HM groups can enroll multiple team members using a single subscription, making educating entire teams easy. Each participant receives a certificate documenting his or her participation in the program.
CODE-H Interactive is available today at www.hospitalmedicine.org/codehi.
Have you ever worried about which billing code is appropriate? Worried that your coding decisions could be called into question, but reading up on the topic only left you more confused?
SHM’s new, first-of-its-kind online educational tool can help.
CODE-H Interactive—short for “Coding Optimally for Documenting Effectively for Hospitalists”—gives hospitalists an online guided tour through six different coding scenarios, enabling them to choose the codes they believe are appropriate. Then, SHM’s coding expert highlights the correct codes and offers rationales for each.
HM groups can enroll multiple team members using a single subscription, making educating entire teams easy. Each participant receives a certificate documenting his or her participation in the program.
CODE-H Interactive is available today at www.hospitalmedicine.org/codehi.
Have you ever worried about which billing code is appropriate? Worried that your coding decisions could be called into question, but reading up on the topic only left you more confused?
SHM’s new, first-of-its-kind online educational tool can help.
CODE-H Interactive—short for “Coding Optimally for Documenting Effectively for Hospitalists”—gives hospitalists an online guided tour through six different coding scenarios, enabling them to choose the codes they believe are appropriate. Then, SHM’s coding expert highlights the correct codes and offers rationales for each.
HM groups can enroll multiple team members using a single subscription, making educating entire teams easy. Each participant receives a certificate documenting his or her participation in the program.
CODE-H Interactive is available today at www.hospitalmedicine.org/codehi.
ICD-10 Will Allow Dermatologists to Effectively Communicate With Payors About Patient Visits
It is important that dermatologists do not overlook the changes associated with the transition to International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). Some physicians believe that providing this level of specificity is not important because at the end of the day, who is watching? You will see with several of the codes highlighted in this column that specificity may be required before a claim can be submitted to the payor for processing. In addition, some older catchall codes will go away, forcing us to provide additional specificity.1
Scabies coding is a good example of an added specificity requirement. Currently, with the International Classification of Diseases, Ninth Revision (ICD-9), we have a code for scabies but no code to address the postscabetic pruritus that patients often develop. The ICD-9 code 133.0 applies to scabies, and if we would like to code for the itch, we must enter a second code for unspecified pruritic disorder (698.9).2 With ICD-10-CM, we can be more specific and actually code for the cause of the itch. We will be able to mark the initial visit as B86 (scabies), but subsequent visits for the itch related to scabies can be coded as pruritus using the primary code L29.8 (other pruritus) and a new sequelae or late effect code of B94 (sequelae of other and unspecified infectious and parasitic diseases).3 You will still be able to submit the second visit with scabies as the primary diagnosis, but this practice should be avoided to prevent claim rejection on the backend. In addition, there will be codes to allow for evaluation of a family member or close contact for this condition. Although coding these patients as an initial visit for scabies may be easier, for epidemiologic purposes a more complete code to provide would be the ICD-10-CM code of Z11.8 (encounter for screening for other infectious and parasitic diseases), particularly if they are not found to have scabies.3 This code also would be useful when screening for head lice when a close contact is not found to have it. What do we currently code when someone comes for screening of head lice because a classmate or sibling has it? With ICD-10-CM we will have a more accurate way to communicate with the payor.
The increase in the number of codes with ICD-10-CM permits us to give a description on a situation or circumstance when a person who may not be sick comes into the office for a specific reason or when circumstances influence a person’s health status but those circumstances are not an actual illness or injury. It is frustrating that I currently am not able to code for a skin examination appropriately using ICD-9. Let me be clear, I am not saying that this new code will be reimbursable. We will have to wait and see how we are reimbursed for all of these codes, but at least we will have the option of coding for the reason the patient presents to me, which is often a skin examination, and then the secondary code could be benign nevi or seborrheic keratosis. The code Z12.83 (encounter for screening for malignant neoplasm of skin) will now be the best code for these purposes.3 In addition, codes that address postoperative nursing visits have not been available. With ICD-10-CM we will have a new code for encounter for surgical aftercare following surgery on the skin and subcutaneous tissue that does not include a standard suture removal but is a necessary visit (Z48.817). In addition, we will have a specific code to document encounters for allergy testing (Z01.82).3 With ICD-9, rash not otherwise specified or eczema would have to be the primary code (782.1) and you were forced to place a code for the patient’s allergy, regardless of whether or not the allergy was known.
The reimbursement of these codes has not been addressed, so ideally during the testing period there can be a head-to-head comparison. By adhering to some of the new rules, hopefully we will be able to more completely communicate about what is occurring during the patient visit.
1. Lamb A. Dermatology coding changes with ICD-10. Cutis. 2014;93:284-285.
2. ICD-9 code lookup. Centers for Medicare & Medicaid Services Web site. http://www.cms.gov/medicare-coverage-database/staticpages/icd-9-code-lookup.aspx. Accessed July 17, 2014.
3. Centers for Medicare & Medicaid Services. ICD-10-CM Tabular List of Diseases and Injuries. http://www.cms.gov/Medicare/Coding/ICD10/downloads/6_I10tab2010.pdf. Published 2010. Accessed July 17, 2014.
It is important that dermatologists do not overlook the changes associated with the transition to International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). Some physicians believe that providing this level of specificity is not important because at the end of the day, who is watching? You will see with several of the codes highlighted in this column that specificity may be required before a claim can be submitted to the payor for processing. In addition, some older catchall codes will go away, forcing us to provide additional specificity.1
Scabies coding is a good example of an added specificity requirement. Currently, with the International Classification of Diseases, Ninth Revision (ICD-9), we have a code for scabies but no code to address the postscabetic pruritus that patients often develop. The ICD-9 code 133.0 applies to scabies, and if we would like to code for the itch, we must enter a second code for unspecified pruritic disorder (698.9).2 With ICD-10-CM, we can be more specific and actually code for the cause of the itch. We will be able to mark the initial visit as B86 (scabies), but subsequent visits for the itch related to scabies can be coded as pruritus using the primary code L29.8 (other pruritus) and a new sequelae or late effect code of B94 (sequelae of other and unspecified infectious and parasitic diseases).3 You will still be able to submit the second visit with scabies as the primary diagnosis, but this practice should be avoided to prevent claim rejection on the backend. In addition, there will be codes to allow for evaluation of a family member or close contact for this condition. Although coding these patients as an initial visit for scabies may be easier, for epidemiologic purposes a more complete code to provide would be the ICD-10-CM code of Z11.8 (encounter for screening for other infectious and parasitic diseases), particularly if they are not found to have scabies.3 This code also would be useful when screening for head lice when a close contact is not found to have it. What do we currently code when someone comes for screening of head lice because a classmate or sibling has it? With ICD-10-CM we will have a more accurate way to communicate with the payor.
The increase in the number of codes with ICD-10-CM permits us to give a description on a situation or circumstance when a person who may not be sick comes into the office for a specific reason or when circumstances influence a person’s health status but those circumstances are not an actual illness or injury. It is frustrating that I currently am not able to code for a skin examination appropriately using ICD-9. Let me be clear, I am not saying that this new code will be reimbursable. We will have to wait and see how we are reimbursed for all of these codes, but at least we will have the option of coding for the reason the patient presents to me, which is often a skin examination, and then the secondary code could be benign nevi or seborrheic keratosis. The code Z12.83 (encounter for screening for malignant neoplasm of skin) will now be the best code for these purposes.3 In addition, codes that address postoperative nursing visits have not been available. With ICD-10-CM we will have a new code for encounter for surgical aftercare following surgery on the skin and subcutaneous tissue that does not include a standard suture removal but is a necessary visit (Z48.817). In addition, we will have a specific code to document encounters for allergy testing (Z01.82).3 With ICD-9, rash not otherwise specified or eczema would have to be the primary code (782.1) and you were forced to place a code for the patient’s allergy, regardless of whether or not the allergy was known.
The reimbursement of these codes has not been addressed, so ideally during the testing period there can be a head-to-head comparison. By adhering to some of the new rules, hopefully we will be able to more completely communicate about what is occurring during the patient visit.
It is important that dermatologists do not overlook the changes associated with the transition to International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). Some physicians believe that providing this level of specificity is not important because at the end of the day, who is watching? You will see with several of the codes highlighted in this column that specificity may be required before a claim can be submitted to the payor for processing. In addition, some older catchall codes will go away, forcing us to provide additional specificity.1
Scabies coding is a good example of an added specificity requirement. Currently, with the International Classification of Diseases, Ninth Revision (ICD-9), we have a code for scabies but no code to address the postscabetic pruritus that patients often develop. The ICD-9 code 133.0 applies to scabies, and if we would like to code for the itch, we must enter a second code for unspecified pruritic disorder (698.9).2 With ICD-10-CM, we can be more specific and actually code for the cause of the itch. We will be able to mark the initial visit as B86 (scabies), but subsequent visits for the itch related to scabies can be coded as pruritus using the primary code L29.8 (other pruritus) and a new sequelae or late effect code of B94 (sequelae of other and unspecified infectious and parasitic diseases).3 You will still be able to submit the second visit with scabies as the primary diagnosis, but this practice should be avoided to prevent claim rejection on the backend. In addition, there will be codes to allow for evaluation of a family member or close contact for this condition. Although coding these patients as an initial visit for scabies may be easier, for epidemiologic purposes a more complete code to provide would be the ICD-10-CM code of Z11.8 (encounter for screening for other infectious and parasitic diseases), particularly if they are not found to have scabies.3 This code also would be useful when screening for head lice when a close contact is not found to have it. What do we currently code when someone comes for screening of head lice because a classmate or sibling has it? With ICD-10-CM we will have a more accurate way to communicate with the payor.
The increase in the number of codes with ICD-10-CM permits us to give a description on a situation or circumstance when a person who may not be sick comes into the office for a specific reason or when circumstances influence a person’s health status but those circumstances are not an actual illness or injury. It is frustrating that I currently am not able to code for a skin examination appropriately using ICD-9. Let me be clear, I am not saying that this new code will be reimbursable. We will have to wait and see how we are reimbursed for all of these codes, but at least we will have the option of coding for the reason the patient presents to me, which is often a skin examination, and then the secondary code could be benign nevi or seborrheic keratosis. The code Z12.83 (encounter for screening for malignant neoplasm of skin) will now be the best code for these purposes.3 In addition, codes that address postoperative nursing visits have not been available. With ICD-10-CM we will have a new code for encounter for surgical aftercare following surgery on the skin and subcutaneous tissue that does not include a standard suture removal but is a necessary visit (Z48.817). In addition, we will have a specific code to document encounters for allergy testing (Z01.82).3 With ICD-9, rash not otherwise specified or eczema would have to be the primary code (782.1) and you were forced to place a code for the patient’s allergy, regardless of whether or not the allergy was known.
The reimbursement of these codes has not been addressed, so ideally during the testing period there can be a head-to-head comparison. By adhering to some of the new rules, hopefully we will be able to more completely communicate about what is occurring during the patient visit.
1. Lamb A. Dermatology coding changes with ICD-10. Cutis. 2014;93:284-285.
2. ICD-9 code lookup. Centers for Medicare & Medicaid Services Web site. http://www.cms.gov/medicare-coverage-database/staticpages/icd-9-code-lookup.aspx. Accessed July 17, 2014.
3. Centers for Medicare & Medicaid Services. ICD-10-CM Tabular List of Diseases and Injuries. http://www.cms.gov/Medicare/Coding/ICD10/downloads/6_I10tab2010.pdf. Published 2010. Accessed July 17, 2014.
1. Lamb A. Dermatology coding changes with ICD-10. Cutis. 2014;93:284-285.
2. ICD-9 code lookup. Centers for Medicare & Medicaid Services Web site. http://www.cms.gov/medicare-coverage-database/staticpages/icd-9-code-lookup.aspx. Accessed July 17, 2014.
3. Centers for Medicare & Medicaid Services. ICD-10-CM Tabular List of Diseases and Injuries. http://www.cms.gov/Medicare/Coding/ICD10/downloads/6_I10tab2010.pdf. Published 2010. Accessed July 17, 2014.
Practice Points
- With International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM), dermatologists will have a more accurate way to communicate with the payor. For example, physicians will be able to code for scabies as well as the cause of postscabetic pruritus.
- Physicians will have the option of coding for the reason the patient presented. For example, dermatologists may code for a skin examination to screen for a malignant neoplasm.
- The reimbursement of the new codes has not been addressed; a head-to-head comparison will be needed during the testing period.
Common Coding Mistakes Hospitalists Should Avoid

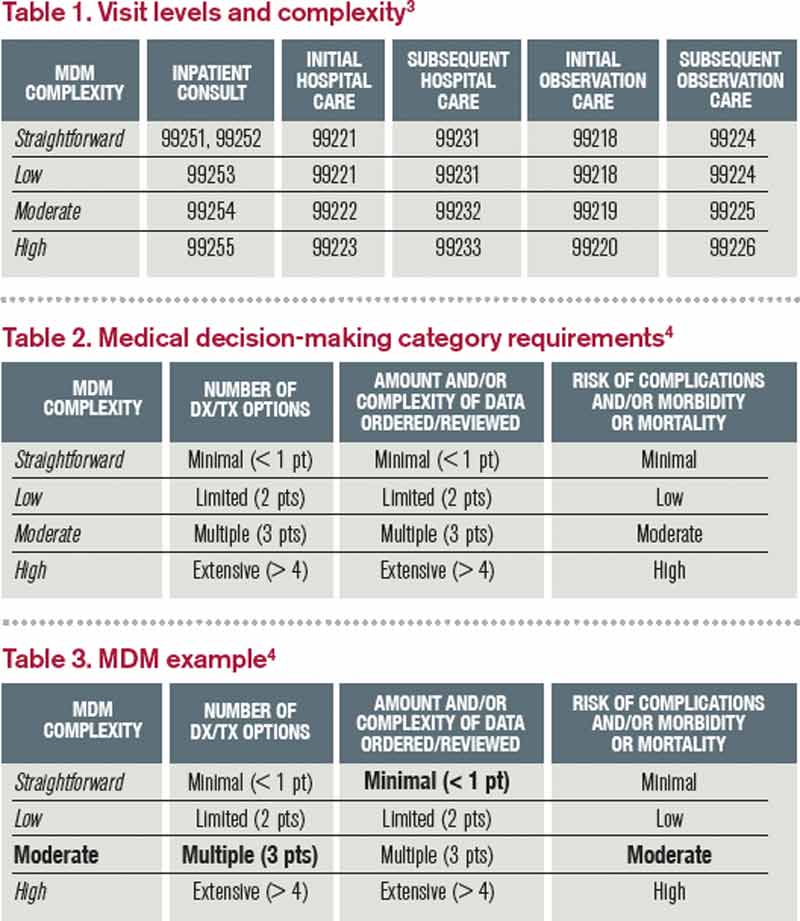
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
CODE-H Medical Coding Education Program Becomes Interactive
SHM’s coding education program, CODE-H, now has an interactive component through the SHM Learning Portal. CODE-H originally was developed as a series of live and on-demand webinars complemented by online forums; today, CODE-H Interactive brings the same expertise to an interactive platform ideal for new hospitalists learning the nuances of coding, hospital medicine groups assessing the coding skills of their caregivers, or even coders using it as a training tool for conducting audits of hospital medicine groups.
To learn more about CODE-H and CODE-H Interactive, visit www.hospitalmedicine.org/codeh.
SHM’s coding education program, CODE-H, now has an interactive component through the SHM Learning Portal. CODE-H originally was developed as a series of live and on-demand webinars complemented by online forums; today, CODE-H Interactive brings the same expertise to an interactive platform ideal for new hospitalists learning the nuances of coding, hospital medicine groups assessing the coding skills of their caregivers, or even coders using it as a training tool for conducting audits of hospital medicine groups.
To learn more about CODE-H and CODE-H Interactive, visit www.hospitalmedicine.org/codeh.
SHM’s coding education program, CODE-H, now has an interactive component through the SHM Learning Portal. CODE-H originally was developed as a series of live and on-demand webinars complemented by online forums; today, CODE-H Interactive brings the same expertise to an interactive platform ideal for new hospitalists learning the nuances of coding, hospital medicine groups assessing the coding skills of their caregivers, or even coders using it as a training tool for conducting audits of hospital medicine groups.
To learn more about CODE-H and CODE-H Interactive, visit www.hospitalmedicine.org/codeh.
Medical Decision-Making: Avoid These Common Coding & Documentation Mistakes
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Proper Inpatient Documentation, Coding Essential to Avoid a Medicare Audit

Several years ago we sent a CPT coding auditor 15 chart notes generated by each doctor in our group. Among each doctors’ 15 notes were at least one or two billed as initial hospital care, follow up, discharge, critical care, and so on. This coding expert returned a report showing that, out of all the notes reviewed, a significant portion were not billed at the correct level. Most of the incorrectly billed notes were judged to reflect “up-coding,” and a few were seen as “down-coded.”
This was distressing and hard to believe.
So I took the same set of notes and paid a second coding expert for an independent review. She didn’t know about the first audit but returned a report that showed a nearly identical portion of incorrectly coded notes.
Two independent audits showing nearly the same portion of notes coded incorrectly was alarming. But it was difficult for my partners and me to address, because the auditors didn’t agree on the correct code for many of the notes. In some cases, both flagged a note as incorrectly coded but didn’t agree on the correct code. For a number of the notes, one auditor said the visit was “up-coded,” while the other said it was “down-coded.” There was so little agreement between the two of them that we had a hard time coming up with any firm conclusions about what we should do to improve our performance.
If experts who think about coding all the time can’t agree on the right code for a given note, how can hospitalists be expected to code nearly all of our visits accurately?
RAC: Recovery Audit Contractor
Despite what I believe is poor inter-rater reliability among coding auditors, we need to work diligently to comply with coding guidelines. A 2003 Federal law mandated a program of Recovery Audit Contractors, or RAC for short, to find cases of “up-coding” or other overbilling and require the provider to repay any resulting loss.
A number of companies are in the business of conducting RAC audits (one of them, CGI, is the Canadian company blamed for the failed “Obamacare” exchange websites), and there is a reasonable chance one of these companies has reviewed some of your charges—or those of your hospitalist colleagues.
The RAC auditors review information about your charges, and if they determine that you up-coded or overbilled, they send a “demand letter” summarizing their findings, along with the amount of money they have determined you should pay back. (Theoretically, they could notify you of “under-coding,” so that you can be paid more for past work, but I haven’t yet come across an example of that.)
It is common to appeal the RAC findings, but that can be a long process, and many organizations decide to pay back all the money requested by the RAC as quickly as possible to avoid paying interest on a delayed payment if the appeal is unsuccessful. In the case of a successful appeal, the money previously refunded by the doctor would be returned.
Page 338 of the CMS Fiscal Year 2015 “Justification of Estimates for Appropriations Committees” says that “…about 50 percent of the estimated 43,000 appeals [of adverse RAC audit findings] were fully or partially overturned…” This could mean the RACs are a sort of loose cannon, accusing many providers of overbilling while knowing that some won’t bother to appeal because they don’t understand the process or because the dollar amount involved for a single provider is too small to justify the time and expense of conducting the appeal. In this way, a RAC audit is like the $15 rebate on the last electronic gadget you bought. The seller knows that many people, including me, will fail to do the work required to claim the rebate.
Accuracy Strategies
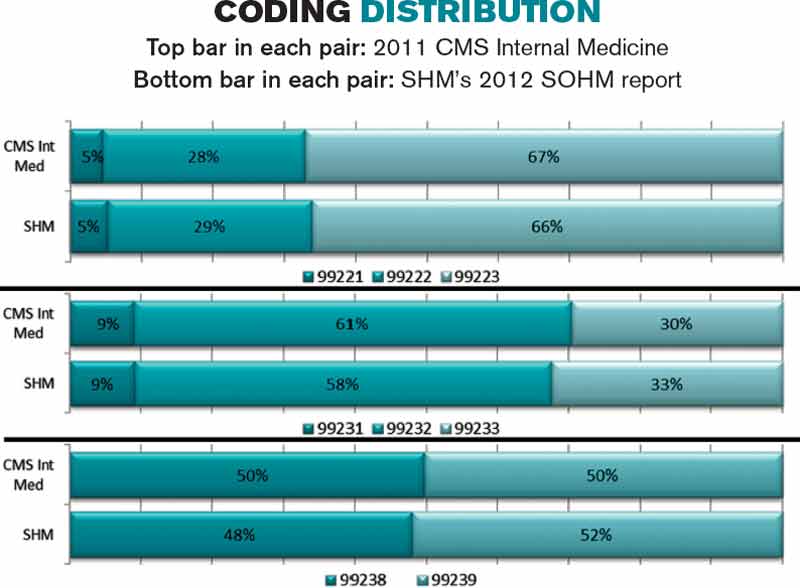
There are a number of ways to help your group ensure appropriate CPT coding and reduce the chance a RAC will ask for money back.
Education. There are many ways to help providers in your practice understand the elements of documentation and coding. Periodic training classes (e.g. during orientation and annually thereafter) are useful but may not be enough. For me, this is a little like learning a foreign language by going to a couple of classes. Instead, I think “immersion training” is more effective. That might mean a doctor spends a few minutes with a certified coder on most working days for a few weeks. For example, they could meet for 15 minutes near lunchtime and review how the doctor plans to bill visits made that morning. Lastly, consider targeted education for each doctor, based on any problems found in an audit of his/her coding.
Review coding patterns. As I wrote in my August 2007 column, there is value in ensuring that each doctor in the group can see how her coding pattern differs from the group as a whole or any individual in the group. That is, what portion of follow-up visits was billed at the lowest, middle, and highest levels? What about admissions, discharges, and so on? I provided a sample report in that same column.
It also is worth taking the time to compare each doctor’s coding pattern to both the CMS Internal Medicine data and SHM’s State of Hospital Medicine report. The accompanying figure shows the most current data sets available.
Keep in mind that the goal is not to simply ensure that your coding pattern matches these external data sets; knowing where yours differs from these sets can suggest where you might want to investigate further or seek additional education.
Coding audits. Having a certified coder audit your performance at least annually is a good idea. It can help uncover areas in which you’d benefit from further review and training, and if, heaven forbid, questions are ever raised about whether you’re intentionally up-coding (fraud), showing that you’re audited regularly could help demonstrate your efforts to code correctly. In the latter case, it is probably more valuable if the audit is done independently of your employer.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Several years ago we sent a CPT coding auditor 15 chart notes generated by each doctor in our group. Among each doctors’ 15 notes were at least one or two billed as initial hospital care, follow up, discharge, critical care, and so on. This coding expert returned a report showing that, out of all the notes reviewed, a significant portion were not billed at the correct level. Most of the incorrectly billed notes were judged to reflect “up-coding,” and a few were seen as “down-coded.”
This was distressing and hard to believe.
So I took the same set of notes and paid a second coding expert for an independent review. She didn’t know about the first audit but returned a report that showed a nearly identical portion of incorrectly coded notes.
Two independent audits showing nearly the same portion of notes coded incorrectly was alarming. But it was difficult for my partners and me to address, because the auditors didn’t agree on the correct code for many of the notes. In some cases, both flagged a note as incorrectly coded but didn’t agree on the correct code. For a number of the notes, one auditor said the visit was “up-coded,” while the other said it was “down-coded.” There was so little agreement between the two of them that we had a hard time coming up with any firm conclusions about what we should do to improve our performance.
If experts who think about coding all the time can’t agree on the right code for a given note, how can hospitalists be expected to code nearly all of our visits accurately?
RAC: Recovery Audit Contractor
Despite what I believe is poor inter-rater reliability among coding auditors, we need to work diligently to comply with coding guidelines. A 2003 Federal law mandated a program of Recovery Audit Contractors, or RAC for short, to find cases of “up-coding” or other overbilling and require the provider to repay any resulting loss.
A number of companies are in the business of conducting RAC audits (one of them, CGI, is the Canadian company blamed for the failed “Obamacare” exchange websites), and there is a reasonable chance one of these companies has reviewed some of your charges—or those of your hospitalist colleagues.
The RAC auditors review information about your charges, and if they determine that you up-coded or overbilled, they send a “demand letter” summarizing their findings, along with the amount of money they have determined you should pay back. (Theoretically, they could notify you of “under-coding,” so that you can be paid more for past work, but I haven’t yet come across an example of that.)
It is common to appeal the RAC findings, but that can be a long process, and many organizations decide to pay back all the money requested by the RAC as quickly as possible to avoid paying interest on a delayed payment if the appeal is unsuccessful. In the case of a successful appeal, the money previously refunded by the doctor would be returned.
Page 338 of the CMS Fiscal Year 2015 “Justification of Estimates for Appropriations Committees” says that “…about 50 percent of the estimated 43,000 appeals [of adverse RAC audit findings] were fully or partially overturned…” This could mean the RACs are a sort of loose cannon, accusing many providers of overbilling while knowing that some won’t bother to appeal because they don’t understand the process or because the dollar amount involved for a single provider is too small to justify the time and expense of conducting the appeal. In this way, a RAC audit is like the $15 rebate on the last electronic gadget you bought. The seller knows that many people, including me, will fail to do the work required to claim the rebate.
Accuracy Strategies
There are a number of ways to help your group ensure appropriate CPT coding and reduce the chance a RAC will ask for money back.
Education. There are many ways to help providers in your practice understand the elements of documentation and coding. Periodic training classes (e.g. during orientation and annually thereafter) are useful but may not be enough. For me, this is a little like learning a foreign language by going to a couple of classes. Instead, I think “immersion training” is more effective. That might mean a doctor spends a few minutes with a certified coder on most working days for a few weeks. For example, they could meet for 15 minutes near lunchtime and review how the doctor plans to bill visits made that morning. Lastly, consider targeted education for each doctor, based on any problems found in an audit of his/her coding.
Review coding patterns. As I wrote in my August 2007 column, there is value in ensuring that each doctor in the group can see how her coding pattern differs from the group as a whole or any individual in the group. That is, what portion of follow-up visits was billed at the lowest, middle, and highest levels? What about admissions, discharges, and so on? I provided a sample report in that same column.
It also is worth taking the time to compare each doctor’s coding pattern to both the CMS Internal Medicine data and SHM’s State of Hospital Medicine report. The accompanying figure shows the most current data sets available.
Keep in mind that the goal is not to simply ensure that your coding pattern matches these external data sets; knowing where yours differs from these sets can suggest where you might want to investigate further or seek additional education.
Coding audits. Having a certified coder audit your performance at least annually is a good idea. It can help uncover areas in which you’d benefit from further review and training, and if, heaven forbid, questions are ever raised about whether you’re intentionally up-coding (fraud), showing that you’re audited regularly could help demonstrate your efforts to code correctly. In the latter case, it is probably more valuable if the audit is done independently of your employer.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Several years ago we sent a CPT coding auditor 15 chart notes generated by each doctor in our group. Among each doctors’ 15 notes were at least one or two billed as initial hospital care, follow up, discharge, critical care, and so on. This coding expert returned a report showing that, out of all the notes reviewed, a significant portion were not billed at the correct level. Most of the incorrectly billed notes were judged to reflect “up-coding,” and a few were seen as “down-coded.”
This was distressing and hard to believe.
So I took the same set of notes and paid a second coding expert for an independent review. She didn’t know about the first audit but returned a report that showed a nearly identical portion of incorrectly coded notes.
Two independent audits showing nearly the same portion of notes coded incorrectly was alarming. But it was difficult for my partners and me to address, because the auditors didn’t agree on the correct code for many of the notes. In some cases, both flagged a note as incorrectly coded but didn’t agree on the correct code. For a number of the notes, one auditor said the visit was “up-coded,” while the other said it was “down-coded.” There was so little agreement between the two of them that we had a hard time coming up with any firm conclusions about what we should do to improve our performance.
If experts who think about coding all the time can’t agree on the right code for a given note, how can hospitalists be expected to code nearly all of our visits accurately?
RAC: Recovery Audit Contractor
Despite what I believe is poor inter-rater reliability among coding auditors, we need to work diligently to comply with coding guidelines. A 2003 Federal law mandated a program of Recovery Audit Contractors, or RAC for short, to find cases of “up-coding” or other overbilling and require the provider to repay any resulting loss.
A number of companies are in the business of conducting RAC audits (one of them, CGI, is the Canadian company blamed for the failed “Obamacare” exchange websites), and there is a reasonable chance one of these companies has reviewed some of your charges—or those of your hospitalist colleagues.
The RAC auditors review information about your charges, and if they determine that you up-coded or overbilled, they send a “demand letter” summarizing their findings, along with the amount of money they have determined you should pay back. (Theoretically, they could notify you of “under-coding,” so that you can be paid more for past work, but I haven’t yet come across an example of that.)
It is common to appeal the RAC findings, but that can be a long process, and many organizations decide to pay back all the money requested by the RAC as quickly as possible to avoid paying interest on a delayed payment if the appeal is unsuccessful. In the case of a successful appeal, the money previously refunded by the doctor would be returned.
Page 338 of the CMS Fiscal Year 2015 “Justification of Estimates for Appropriations Committees” says that “…about 50 percent of the estimated 43,000 appeals [of adverse RAC audit findings] were fully or partially overturned…” This could mean the RACs are a sort of loose cannon, accusing many providers of overbilling while knowing that some won’t bother to appeal because they don’t understand the process or because the dollar amount involved for a single provider is too small to justify the time and expense of conducting the appeal. In this way, a RAC audit is like the $15 rebate on the last electronic gadget you bought. The seller knows that many people, including me, will fail to do the work required to claim the rebate.
Accuracy Strategies
There are a number of ways to help your group ensure appropriate CPT coding and reduce the chance a RAC will ask for money back.
Education. There are many ways to help providers in your practice understand the elements of documentation and coding. Periodic training classes (e.g. during orientation and annually thereafter) are useful but may not be enough. For me, this is a little like learning a foreign language by going to a couple of classes. Instead, I think “immersion training” is more effective. That might mean a doctor spends a few minutes with a certified coder on most working days for a few weeks. For example, they could meet for 15 minutes near lunchtime and review how the doctor plans to bill visits made that morning. Lastly, consider targeted education for each doctor, based on any problems found in an audit of his/her coding.
Review coding patterns. As I wrote in my August 2007 column, there is value in ensuring that each doctor in the group can see how her coding pattern differs from the group as a whole or any individual in the group. That is, what portion of follow-up visits was billed at the lowest, middle, and highest levels? What about admissions, discharges, and so on? I provided a sample report in that same column.
It also is worth taking the time to compare each doctor’s coding pattern to both the CMS Internal Medicine data and SHM’s State of Hospital Medicine report. The accompanying figure shows the most current data sets available.
Keep in mind that the goal is not to simply ensure that your coding pattern matches these external data sets; knowing where yours differs from these sets can suggest where you might want to investigate further or seek additional education.
Coding audits. Having a certified coder audit your performance at least annually is a good idea. It can help uncover areas in which you’d benefit from further review and training, and if, heaven forbid, questions are ever raised about whether you’re intentionally up-coding (fraud), showing that you’re audited regularly could help demonstrate your efforts to code correctly. In the latter case, it is probably more valuable if the audit is done independently of your employer.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.