User login
For MD-IQ on Family Practice News, but a regular topic for Rheumatology News
Use IOM Guidelines on Calcium, Vitamin D Loosely
SAN FRANCISCO – Updated national guidelines on calcium and vitamin D intake should be followed loosely, cautioned Dr. Deborah E. Sellmeyer, director of the Metabolic Bone Center at Johns Hopkins University, Baltimore.
Controversy surrounds the Institute of Medicine's November 2010 report, “Dietary Reference Intakes for Calcium and Vitamin D,” an update of 1997 guidelines. Dr. Sellmeyer uses the latest IOM report as a starting point and then tailors the recommendations to meet the needs of her patients. As a result, the amounts of vitamin D and calcium that her patients take usually vary from the guidelines, she said at a the meeting.
There is uncertainty about the cutoff level of serum vitamin D that's considered adequate and the potential side effects from ingesting too much calcium, she said.
The IOM recommends that adults take 600 IU vitamin D/day through age 50 and 800 IU/day for those aged 51 years and older, with a suggested upper tolerability limit of 4,000 IU/day. Those are the intake amounts that generally would be needed to reach a serum level of 20 ng/mL.
But many experts think that physiologic and fracture data suggest that a “sufficient” serum level should be in the 30–32-ng/mL range, she said. “It takes most people about 1,200 IU/day to reach that” serum level, said Dr. Sellmeyer, who advises her patients accordingly.
A 2010 study of high-dose vitamin D and fracture risk caused “a lot of consternation,” she noted. The double-blind trial randomized 2,256 older women to a once-yearly oral dose of 500,000 IU cholecalciferol or placebo, and found higher rates of falls and fractures in the vitamin D group (JAMA 2010;303:1815–22).
“It's almost a moot point because you wouldn't give 500,000 IU once a year, but it did raise the idea that there may be some administration techniques, some regimens that would not be beneficial,” Dr. Sellmeyer said.
The IOM committee that compiled the 2010 report expressed a great deal of concern about a potentially higher mortality risk with excessively high vitamin D serum levels. The concern was sparked by the committee's interpretation of an analysis of data from the Third National Health and Nutrition Examination Survey. Overall, that survey documented higher mortality rates in patients in the lowest quartile of serum vitamin D levels (Arch. Intern. Med. 2008;168:1629–37). However, the IOM committee noticed a statistically nonsignificant dip in mortality risk between the highest and second-highest quartiles of serum vitamin D before the mortality risk increased in each of the two lowest quartiles, constituting what some saw as a J-shaped curve of mortality risk.
Numerically, the lowest mortality was in patients with 24-32 ng/mL of serum vitamin D, but this was statistically not significantly different than in patients with a serum level greater than 32 ng/mL.
“I'm really not sure that there is a higher mortality,” Dr. Sellmeyer said. “I think there is enough evidence to suggest that we probably ought to be a little more in the 30–40-ng/mL range.”
The IOM recommends that adult males get 1,000 mg/day of calcium through age 70 years and 1,200 mg/day for those who are older. Adult women should get 1,000 mg/day through age 50 and 1,200 mg/day in older ages. The maximum tolerability limits were set at 2,500 mg/day for adults younger than 50 years or 2,000 mg/day for older adults.
It's important to remember that the recommended level includes both dietary and supplemental sources of calcium, she emphasized. “We see a lot of women who are taking 1,200–1,500 mg/day in supplements and also drinking two glasses of milk a day,” she said. “Those [are the patients who] can get into trouble.”
There are no data to suggest that ingesting more than 1,200 mg/day is better for skeletal health, and high doses of calcium increase the risk of developing kidney stones, studies show.
The most controversial aspect of calcium supplementation in recent years has been some preliminary evidence of a possible increased risk for vascular calcification with higher doses.
Initially, an analysis of data on 36,282 participants in the Women's Health Initiative (WHI) who were randomized to take 500 mg calcium carbonate with 200 IU vitamin D twice daily found no effect on risk of myocardial infarction (MI) or vascular calcification (Circulation 2007;115:846–54).
Then a randomized, controlled trial of 1,471 healthy women found that the group taking 1 g/day of calcium citrate showed a doubling in risk for MI and a trend toward higher risk of angina, compared with the placebo group (BMJ 2008;336:262–6). The investigators in that study reanalyzed the WHI data and found a 22% increase in risk for MI in women who at baseline had no personal calcium use (BMJ 2011;19:342:d2040).
There were significant differences in the comparison groups in the reanalysis, including differences in personal history of MI, Dr. Sellmeyer noted. “Whether this truly represents an increased risk or not is unclear,” she said.
Another study by some of the same investigators “got a ton of press” even though it was a relatively small meta-analysis, she added. The attempted meta-analysis of 190 trials of calcium supplementation yielded 15 eligible trials, but most of the data came from 5 trials. The meta-analysis reported a 31% increase in risk for MI in calcium supplement users, with possibly a higher risk in those taking more than 1,600 mg/day (BMJ 2010;341:c3691). “It's really hard to know at this point” whether the risk of vascular calcification from supplementation is significant, Dr. Sellmeyer said. “I think it does behoove us to be judicious with our calcium and not let people consume more calcium than we think is really beneficial.”
Dr. Sellmeyer said she has no relevant conflicts of interest.
{kind=link}
Most people need about 1,200 IU/day of vitamin D to reach 'sufficient' serum levels in the 30–32-ng/mL range.
Source DR. SELLMEYER
SAN FRANCISCO – Updated national guidelines on calcium and vitamin D intake should be followed loosely, cautioned Dr. Deborah E. Sellmeyer, director of the Metabolic Bone Center at Johns Hopkins University, Baltimore.
Controversy surrounds the Institute of Medicine's November 2010 report, “Dietary Reference Intakes for Calcium and Vitamin D,” an update of 1997 guidelines. Dr. Sellmeyer uses the latest IOM report as a starting point and then tailors the recommendations to meet the needs of her patients. As a result, the amounts of vitamin D and calcium that her patients take usually vary from the guidelines, she said at a the meeting.
There is uncertainty about the cutoff level of serum vitamin D that's considered adequate and the potential side effects from ingesting too much calcium, she said.
The IOM recommends that adults take 600 IU vitamin D/day through age 50 and 800 IU/day for those aged 51 years and older, with a suggested upper tolerability limit of 4,000 IU/day. Those are the intake amounts that generally would be needed to reach a serum level of 20 ng/mL.
But many experts think that physiologic and fracture data suggest that a “sufficient” serum level should be in the 30–32-ng/mL range, she said. “It takes most people about 1,200 IU/day to reach that” serum level, said Dr. Sellmeyer, who advises her patients accordingly.
A 2010 study of high-dose vitamin D and fracture risk caused “a lot of consternation,” she noted. The double-blind trial randomized 2,256 older women to a once-yearly oral dose of 500,000 IU cholecalciferol or placebo, and found higher rates of falls and fractures in the vitamin D group (JAMA 2010;303:1815–22).
“It's almost a moot point because you wouldn't give 500,000 IU once a year, but it did raise the idea that there may be some administration techniques, some regimens that would not be beneficial,” Dr. Sellmeyer said.
The IOM committee that compiled the 2010 report expressed a great deal of concern about a potentially higher mortality risk with excessively high vitamin D serum levels. The concern was sparked by the committee's interpretation of an analysis of data from the Third National Health and Nutrition Examination Survey. Overall, that survey documented higher mortality rates in patients in the lowest quartile of serum vitamin D levels (Arch. Intern. Med. 2008;168:1629–37). However, the IOM committee noticed a statistically nonsignificant dip in mortality risk between the highest and second-highest quartiles of serum vitamin D before the mortality risk increased in each of the two lowest quartiles, constituting what some saw as a J-shaped curve of mortality risk.
Numerically, the lowest mortality was in patients with 24-32 ng/mL of serum vitamin D, but this was statistically not significantly different than in patients with a serum level greater than 32 ng/mL.
“I'm really not sure that there is a higher mortality,” Dr. Sellmeyer said. “I think there is enough evidence to suggest that we probably ought to be a little more in the 30–40-ng/mL range.”
The IOM recommends that adult males get 1,000 mg/day of calcium through age 70 years and 1,200 mg/day for those who are older. Adult women should get 1,000 mg/day through age 50 and 1,200 mg/day in older ages. The maximum tolerability limits were set at 2,500 mg/day for adults younger than 50 years or 2,000 mg/day for older adults.
It's important to remember that the recommended level includes both dietary and supplemental sources of calcium, she emphasized. “We see a lot of women who are taking 1,200–1,500 mg/day in supplements and also drinking two glasses of milk a day,” she said. “Those [are the patients who] can get into trouble.”
There are no data to suggest that ingesting more than 1,200 mg/day is better for skeletal health, and high doses of calcium increase the risk of developing kidney stones, studies show.
The most controversial aspect of calcium supplementation in recent years has been some preliminary evidence of a possible increased risk for vascular calcification with higher doses.
Initially, an analysis of data on 36,282 participants in the Women's Health Initiative (WHI) who were randomized to take 500 mg calcium carbonate with 200 IU vitamin D twice daily found no effect on risk of myocardial infarction (MI) or vascular calcification (Circulation 2007;115:846–54).
Then a randomized, controlled trial of 1,471 healthy women found that the group taking 1 g/day of calcium citrate showed a doubling in risk for MI and a trend toward higher risk of angina, compared with the placebo group (BMJ 2008;336:262–6). The investigators in that study reanalyzed the WHI data and found a 22% increase in risk for MI in women who at baseline had no personal calcium use (BMJ 2011;19:342:d2040).
There were significant differences in the comparison groups in the reanalysis, including differences in personal history of MI, Dr. Sellmeyer noted. “Whether this truly represents an increased risk or not is unclear,” she said.
Another study by some of the same investigators “got a ton of press” even though it was a relatively small meta-analysis, she added. The attempted meta-analysis of 190 trials of calcium supplementation yielded 15 eligible trials, but most of the data came from 5 trials. The meta-analysis reported a 31% increase in risk for MI in calcium supplement users, with possibly a higher risk in those taking more than 1,600 mg/day (BMJ 2010;341:c3691). “It's really hard to know at this point” whether the risk of vascular calcification from supplementation is significant, Dr. Sellmeyer said. “I think it does behoove us to be judicious with our calcium and not let people consume more calcium than we think is really beneficial.”
Dr. Sellmeyer said she has no relevant conflicts of interest.
Most people need about 1,200 IU/day of vitamin D to reach 'sufficient' serum levels in the 30–32-ng/mL range.
Source DR. SELLMEYER
SAN FRANCISCO – Updated national guidelines on calcium and vitamin D intake should be followed loosely, cautioned Dr. Deborah E. Sellmeyer, director of the Metabolic Bone Center at Johns Hopkins University, Baltimore.
Controversy surrounds the Institute of Medicine's November 2010 report, “Dietary Reference Intakes for Calcium and Vitamin D,” an update of 1997 guidelines. Dr. Sellmeyer uses the latest IOM report as a starting point and then tailors the recommendations to meet the needs of her patients. As a result, the amounts of vitamin D and calcium that her patients take usually vary from the guidelines, she said at a the meeting.
There is uncertainty about the cutoff level of serum vitamin D that's considered adequate and the potential side effects from ingesting too much calcium, she said.
The IOM recommends that adults take 600 IU vitamin D/day through age 50 and 800 IU/day for those aged 51 years and older, with a suggested upper tolerability limit of 4,000 IU/day. Those are the intake amounts that generally would be needed to reach a serum level of 20 ng/mL.
But many experts think that physiologic and fracture data suggest that a “sufficient” serum level should be in the 30–32-ng/mL range, she said. “It takes most people about 1,200 IU/day to reach that” serum level, said Dr. Sellmeyer, who advises her patients accordingly.
A 2010 study of high-dose vitamin D and fracture risk caused “a lot of consternation,” she noted. The double-blind trial randomized 2,256 older women to a once-yearly oral dose of 500,000 IU cholecalciferol or placebo, and found higher rates of falls and fractures in the vitamin D group (JAMA 2010;303:1815–22).
“It's almost a moot point because you wouldn't give 500,000 IU once a year, but it did raise the idea that there may be some administration techniques, some regimens that would not be beneficial,” Dr. Sellmeyer said.
The IOM committee that compiled the 2010 report expressed a great deal of concern about a potentially higher mortality risk with excessively high vitamin D serum levels. The concern was sparked by the committee's interpretation of an analysis of data from the Third National Health and Nutrition Examination Survey. Overall, that survey documented higher mortality rates in patients in the lowest quartile of serum vitamin D levels (Arch. Intern. Med. 2008;168:1629–37). However, the IOM committee noticed a statistically nonsignificant dip in mortality risk between the highest and second-highest quartiles of serum vitamin D before the mortality risk increased in each of the two lowest quartiles, constituting what some saw as a J-shaped curve of mortality risk.
Numerically, the lowest mortality was in patients with 24-32 ng/mL of serum vitamin D, but this was statistically not significantly different than in patients with a serum level greater than 32 ng/mL.
“I'm really not sure that there is a higher mortality,” Dr. Sellmeyer said. “I think there is enough evidence to suggest that we probably ought to be a little more in the 30–40-ng/mL range.”
The IOM recommends that adult males get 1,000 mg/day of calcium through age 70 years and 1,200 mg/day for those who are older. Adult women should get 1,000 mg/day through age 50 and 1,200 mg/day in older ages. The maximum tolerability limits were set at 2,500 mg/day for adults younger than 50 years or 2,000 mg/day for older adults.
It's important to remember that the recommended level includes both dietary and supplemental sources of calcium, she emphasized. “We see a lot of women who are taking 1,200–1,500 mg/day in supplements and also drinking two glasses of milk a day,” she said. “Those [are the patients who] can get into trouble.”
There are no data to suggest that ingesting more than 1,200 mg/day is better for skeletal health, and high doses of calcium increase the risk of developing kidney stones, studies show.
The most controversial aspect of calcium supplementation in recent years has been some preliminary evidence of a possible increased risk for vascular calcification with higher doses.
Initially, an analysis of data on 36,282 participants in the Women's Health Initiative (WHI) who were randomized to take 500 mg calcium carbonate with 200 IU vitamin D twice daily found no effect on risk of myocardial infarction (MI) or vascular calcification (Circulation 2007;115:846–54).
Then a randomized, controlled trial of 1,471 healthy women found that the group taking 1 g/day of calcium citrate showed a doubling in risk for MI and a trend toward higher risk of angina, compared with the placebo group (BMJ 2008;336:262–6). The investigators in that study reanalyzed the WHI data and found a 22% increase in risk for MI in women who at baseline had no personal calcium use (BMJ 2011;19:342:d2040).
There were significant differences in the comparison groups in the reanalysis, including differences in personal history of MI, Dr. Sellmeyer noted. “Whether this truly represents an increased risk or not is unclear,” she said.
Another study by some of the same investigators “got a ton of press” even though it was a relatively small meta-analysis, she added. The attempted meta-analysis of 190 trials of calcium supplementation yielded 15 eligible trials, but most of the data came from 5 trials. The meta-analysis reported a 31% increase in risk for MI in calcium supplement users, with possibly a higher risk in those taking more than 1,600 mg/day (BMJ 2010;341:c3691). “It's really hard to know at this point” whether the risk of vascular calcification from supplementation is significant, Dr. Sellmeyer said. “I think it does behoove us to be judicious with our calcium and not let people consume more calcium than we think is really beneficial.”
Dr. Sellmeyer said she has no relevant conflicts of interest.
Most people need about 1,200 IU/day of vitamin D to reach 'sufficient' serum levels in the 30–32-ng/mL range.
Source DR. SELLMEYER
Denosumab Effect Greater in Selected Patients : Patients with femoral neck osteoporosis had fewer fractures.
SAN FRANCISCO – The pivotal clinical trial of denosumab showed a 20% decrease in nonvertebral fractures compared with placebo treatment, but a new subgroup analysis shows the protective effect is significantly higher in patients with femoral neck osteoporosis.
The preplanned subgroup analysis of data from the FREEDOM (Fracture Reduction Evaluation of Denosumab in Osteoporosis Every 6 Months) trial found that denosumab decreased nonvertebral fractures by 35% in patients with a femoral neck bone mineral density T score of −2.5 or lower and by only 3% in patients with higher femoral neck T scores, compared with patients in those subgroups who received placebo, Dr. Steven R. Cummings said.
The report of a 20% reduction in nonvertebral fractures in the overall trial for denosumab “underestimates its efficacy for those patients that we're most interested in treating with this drug – those with osteoporosis,” he said at a conference on osteoporosis sponsored by the University of California, San Francisco.
The findings have been submitted for publication. The analysis is one of several preplanned subgroup analyses being conducted, though this one is “the most interesting result for clinical care,” said Dr. Cummings, emeritus professor of medicine, epidemiology and biostatistics at the university.
The original FREEDOM study enrolled 7,808 postmenopausal women aged 60-80 years with osteoporosis to receive every 6 months either a subcutaneous injection of denosumab (60 mg) or placebo along with daily calcium and vitamin D supplements. All of the subjects had bone mineral density T scores that were less than −2.5 but not less than −4.0 at the lumbar spine or total hip. At 36 months, denosumab was associated with reductions of 68% in vertebral fracture and 40% in hip fracture (N. Engl. J. Med. 2009;361:756–65).
The FREEDOM results were the basis of the Food and Drug Administration's approval of denosumab in June 2010.
Data for 2,343 patients who continued denosumab for another 2 years and 2,207 patients who switched from placebo to denosumab in an ongoing extension of the trial suggest that the incidence of nonvertebral fractures continues to decline in the first 5 years of denosumab use. The 5-year results have been submitted for publication, he said.
For nonvertebral fractures, the incidence decreased from 2.6% in the denosumab group in the first year of the FREEDOM trial to 2.1% in year 2 and 2.2% in year 3. Nonvertebral fractures were seen in 1.4% of patients in year 4 and 1.1% of patients in year 5, extension study data show. Similar rates were seen for vertebral fractures.
The extension study did not include a placebo comparison, so “we did a pretty rigorous estimate of what the rates would be if the placebo group had continued out to 5 years,” Dr. Cummings said. They estimated that nonvertebral or vertebral fracture rates would be 2.6% in the placebo group in years 4 and 5, more than twice that of patients on denosumab in the extension study.
A separate study highlighted another advantage of denosumab that it shares with zoledronic acid – greater adherence rates compared with oral therapies, he added. An open-label study of 250 women with untreated osteoporosis found an 87% adherence rate in the first year in patients randomized to get a denosumab injection every 6 months, compared with a 77% adherence rate for patients randomized to weekly oral alendronate therapy. Alendronate use was monitored by electronic bottle caps (Osteoporos. Int. 2011;22:1725–35).
The study's 2-year results, which have not yet been published, show that the difference in adherence rates between groups continues to widen, Dr. Cummings said.
Dr. Cummings has been a consultant to Amgen Pharmaceuticals, which markets denosumab; to Merck, which markets alendronate; and to Eli Lilly & Co.
SAN FRANCISCO – The pivotal clinical trial of denosumab showed a 20% decrease in nonvertebral fractures compared with placebo treatment, but a new subgroup analysis shows the protective effect is significantly higher in patients with femoral neck osteoporosis.
The preplanned subgroup analysis of data from the FREEDOM (Fracture Reduction Evaluation of Denosumab in Osteoporosis Every 6 Months) trial found that denosumab decreased nonvertebral fractures by 35% in patients with a femoral neck bone mineral density T score of −2.5 or lower and by only 3% in patients with higher femoral neck T scores, compared with patients in those subgroups who received placebo, Dr. Steven R. Cummings said.
The report of a 20% reduction in nonvertebral fractures in the overall trial for denosumab “underestimates its efficacy for those patients that we're most interested in treating with this drug – those with osteoporosis,” he said at a conference on osteoporosis sponsored by the University of California, San Francisco.
The findings have been submitted for publication. The analysis is one of several preplanned subgroup analyses being conducted, though this one is “the most interesting result for clinical care,” said Dr. Cummings, emeritus professor of medicine, epidemiology and biostatistics at the university.
The original FREEDOM study enrolled 7,808 postmenopausal women aged 60-80 years with osteoporosis to receive every 6 months either a subcutaneous injection of denosumab (60 mg) or placebo along with daily calcium and vitamin D supplements. All of the subjects had bone mineral density T scores that were less than −2.5 but not less than −4.0 at the lumbar spine or total hip. At 36 months, denosumab was associated with reductions of 68% in vertebral fracture and 40% in hip fracture (N. Engl. J. Med. 2009;361:756–65).
The FREEDOM results were the basis of the Food and Drug Administration's approval of denosumab in June 2010.
Data for 2,343 patients who continued denosumab for another 2 years and 2,207 patients who switched from placebo to denosumab in an ongoing extension of the trial suggest that the incidence of nonvertebral fractures continues to decline in the first 5 years of denosumab use. The 5-year results have been submitted for publication, he said.
For nonvertebral fractures, the incidence decreased from 2.6% in the denosumab group in the first year of the FREEDOM trial to 2.1% in year 2 and 2.2% in year 3. Nonvertebral fractures were seen in 1.4% of patients in year 4 and 1.1% of patients in year 5, extension study data show. Similar rates were seen for vertebral fractures.
The extension study did not include a placebo comparison, so “we did a pretty rigorous estimate of what the rates would be if the placebo group had continued out to 5 years,” Dr. Cummings said. They estimated that nonvertebral or vertebral fracture rates would be 2.6% in the placebo group in years 4 and 5, more than twice that of patients on denosumab in the extension study.
A separate study highlighted another advantage of denosumab that it shares with zoledronic acid – greater adherence rates compared with oral therapies, he added. An open-label study of 250 women with untreated osteoporosis found an 87% adherence rate in the first year in patients randomized to get a denosumab injection every 6 months, compared with a 77% adherence rate for patients randomized to weekly oral alendronate therapy. Alendronate use was monitored by electronic bottle caps (Osteoporos. Int. 2011;22:1725–35).
The study's 2-year results, which have not yet been published, show that the difference in adherence rates between groups continues to widen, Dr. Cummings said.
Dr. Cummings has been a consultant to Amgen Pharmaceuticals, which markets denosumab; to Merck, which markets alendronate; and to Eli Lilly & Co.
SAN FRANCISCO – The pivotal clinical trial of denosumab showed a 20% decrease in nonvertebral fractures compared with placebo treatment, but a new subgroup analysis shows the protective effect is significantly higher in patients with femoral neck osteoporosis.
The preplanned subgroup analysis of data from the FREEDOM (Fracture Reduction Evaluation of Denosumab in Osteoporosis Every 6 Months) trial found that denosumab decreased nonvertebral fractures by 35% in patients with a femoral neck bone mineral density T score of −2.5 or lower and by only 3% in patients with higher femoral neck T scores, compared with patients in those subgroups who received placebo, Dr. Steven R. Cummings said.
The report of a 20% reduction in nonvertebral fractures in the overall trial for denosumab “underestimates its efficacy for those patients that we're most interested in treating with this drug – those with osteoporosis,” he said at a conference on osteoporosis sponsored by the University of California, San Francisco.
The findings have been submitted for publication. The analysis is one of several preplanned subgroup analyses being conducted, though this one is “the most interesting result for clinical care,” said Dr. Cummings, emeritus professor of medicine, epidemiology and biostatistics at the university.
The original FREEDOM study enrolled 7,808 postmenopausal women aged 60-80 years with osteoporosis to receive every 6 months either a subcutaneous injection of denosumab (60 mg) or placebo along with daily calcium and vitamin D supplements. All of the subjects had bone mineral density T scores that were less than −2.5 but not less than −4.0 at the lumbar spine or total hip. At 36 months, denosumab was associated with reductions of 68% in vertebral fracture and 40% in hip fracture (N. Engl. J. Med. 2009;361:756–65).
The FREEDOM results were the basis of the Food and Drug Administration's approval of denosumab in June 2010.
Data for 2,343 patients who continued denosumab for another 2 years and 2,207 patients who switched from placebo to denosumab in an ongoing extension of the trial suggest that the incidence of nonvertebral fractures continues to decline in the first 5 years of denosumab use. The 5-year results have been submitted for publication, he said.
For nonvertebral fractures, the incidence decreased from 2.6% in the denosumab group in the first year of the FREEDOM trial to 2.1% in year 2 and 2.2% in year 3. Nonvertebral fractures were seen in 1.4% of patients in year 4 and 1.1% of patients in year 5, extension study data show. Similar rates were seen for vertebral fractures.
The extension study did not include a placebo comparison, so “we did a pretty rigorous estimate of what the rates would be if the placebo group had continued out to 5 years,” Dr. Cummings said. They estimated that nonvertebral or vertebral fracture rates would be 2.6% in the placebo group in years 4 and 5, more than twice that of patients on denosumab in the extension study.
A separate study highlighted another advantage of denosumab that it shares with zoledronic acid – greater adherence rates compared with oral therapies, he added. An open-label study of 250 women with untreated osteoporosis found an 87% adherence rate in the first year in patients randomized to get a denosumab injection every 6 months, compared with a 77% adherence rate for patients randomized to weekly oral alendronate therapy. Alendronate use was monitored by electronic bottle caps (Osteoporos. Int. 2011;22:1725–35).
The study's 2-year results, which have not yet been published, show that the difference in adherence rates between groups continues to widen, Dr. Cummings said.
Dr. Cummings has been a consultant to Amgen Pharmaceuticals, which markets denosumab; to Merck, which markets alendronate; and to Eli Lilly & Co.
Be Alert for Significant Bone Loss After Bariatric Surgery
SAN FRANCISCO – Bariatric surgery can be beneficial for obese people, but it also can lead to significant bone loss.
The limited data so far suggest that decreased bone mineral density after bariatric surgery is a real problem that increases the risk for fracture, Dr. Anne Schafer said at a meeting on osteoporosis sponsored by the University of California, San Francisco.
The extent of bone loss within a year after the most common bariatric surgery, Roux-en-Y gastric bypass, can be equivalent to “what you would expect in the first 5 years of menopause” in some women, said Dr. Schafer of the division of endocrinology at the University of California, San Francisco.
A 2011 study not yet published by the Mayo Clinic, Rochester, Minn., compared fracture rates in 277 patients undergoing bariatric surgery with local age- and sex-matched fracture rates. The surgeries occurred in 1985-2004, and 94% were gastric bypasses. The retrospective chart study found 138 fractures in 82 patients since the surgery, with a standardized incidence ratio of 2.1 for any fracture and 1.9 for fractures of the hip, spine, wrist, or arm after bariatric surgery, she said.
Dr. Schafer incorporated her own clinical experience with recommendations from the Endocrine Society and from Tufts University in advising clinicians to take the following steps in managing patients undergoing bariatric surgery.
Prior to surgery, check serum 25-hydroxyvitamin D (25[OH]D) levels and prescribe preoperative treatment to augment vitamin D in patients with low levels. After surgery, all patients should take two multivitamins per day to make sure their micronutrient needs are met.
After malabsorptive bariatric surgery, such as gastric bypass, patients also should take calcium supplements, although there are not enough data to pinpoint the best dose or to identify which patients might most need the calcium, Dr. Schafer said. She recommended 1,200–2,000 mg/day (preferably in citrate form) after malabsorptive surgery and possibly after restrictive bariatric surgery such as adjustable gastric banding.
Based on the preoperative vitamin D level, prescribe 800-2,000 IU/day of vitamin D3 supplementation after malabsorptive surgery and possibly after restrictive bariatric surgery. “I've had people who need more” than that dose range, she added.
For postoperative surveillance, check calcium homeostasis laboratory tests every 6 months for the first 2 years and then annually after malabsorptive surgery and possibly after any bariatric surgery. The tests include calcium, albumin, phosphate, creatinine, 25(OH)D, and parathyroid hormone.
If the parathyroid hormone level is high, but the 25(OH)D level is low, treat with vitamin D supplementation. If the parathyroid hormone level is high and the 25(OH)D level is ideal, check the patient's 24-hour urinary calcium, and if that is low, increase calcium intake.
Because some of the etiology of bariatric surgery–induced bone loss may be the preferential loss of lean mass over fat mass, or changes in fat distribution, encourage patients to consume protein and to exercise, she said.
The Endocrine Society recommends dual-energy x-ray absorptiometry (DXA) at baseline and annually in people who are undergoing malabsorptive bariatric surgery. No data show that such monitoring actually improves outcomes, “but I do think that you should consider it for any people who can fit on the DXA scan before the operation,” Dr. Schafer said. The weight limit for the scanner is approximately 275–350 pounds.
Dr. Schafer also said that she advises a DXA scan 1-2 years postoperatively. Incorporate those results into “your clinical judgment and other risk factors like age or prior history of fractures to set up an individualized plan for monitoring bone density from there.”
In general, high body mass index has been associated with high bone mineral density, and either voluntary or involuntary weight loss is associated with bone loss and increased fracture risk. Bariatric surgery leads to loss of bone mass for multiple reasons, she said, including nutritional deficiencies from malabsorption, the body's signals about decreased skeletal loading with weight loss, and changes in fat-secreted hormone.
Most of the data on bone loss after bariatric surgery is for Roux-en-Y gastric bypass, which induces early and sustained increases in bone turnover and decreases in bone mineral density. Fewer data are available on other procedures, but a handful of studies suggest that another malabsorptive procedure, biliopancreatic diversion, may produce effects similar to those of gastric bypass, and that adjustable gastric banding may have less of an impact on bone, she said.
For gastric bypass, one study of 15 patients reported an 8% decrease in total hip bone mineral density within 9 months (J. Clin. Endocrinol. Metab. 2004;89:1061–5). Femoral neck bone density decreased by 9% within 1 year of gastric bypass in a separate study of 23 patients (J. Clin. Endocrinol. Metab. 2008;93:3735–40). A third study of 42 patients reported a 7% decrease in spine bone density and a 10% decrease in total hip bone density a year after gastric bypass (Obes. Surg. 2009;19:41–6).
Vitamin D deficiency can be a problem after bariatric surgery because many patients have low vitamin D levels before surgery, some of the surgeries are designed to create malabsorption, and patients eat less food and different kinds of food after surgery. In the worst cases, patients may develop secondary hyperparathyroidism or bone loss, and there have been case reports of osteomalacia.
All the studies used DXA scans to assess bone density after bariatric surgery, but DXA assessment may be biased in the setting of marked weight loss because of changes in soft tissue surrounding the bones. The informal consensus among experts is that the bone density losses reported by studies are real, “but we need nonbiased methods of assessing bone mineral density” for future studies of bariatric surgery's effects, she said.
Dr. Schafer said that she has no disclosures.
To watch an interview with Dr. Schafer, scan the QR code or visit www.rheumatologynews.com
SAN FRANCISCO – Bariatric surgery can be beneficial for obese people, but it also can lead to significant bone loss.
The limited data so far suggest that decreased bone mineral density after bariatric surgery is a real problem that increases the risk for fracture, Dr. Anne Schafer said at a meeting on osteoporosis sponsored by the University of California, San Francisco.
The extent of bone loss within a year after the most common bariatric surgery, Roux-en-Y gastric bypass, can be equivalent to “what you would expect in the first 5 years of menopause” in some women, said Dr. Schafer of the division of endocrinology at the University of California, San Francisco.
A 2011 study not yet published by the Mayo Clinic, Rochester, Minn., compared fracture rates in 277 patients undergoing bariatric surgery with local age- and sex-matched fracture rates. The surgeries occurred in 1985-2004, and 94% were gastric bypasses. The retrospective chart study found 138 fractures in 82 patients since the surgery, with a standardized incidence ratio of 2.1 for any fracture and 1.9 for fractures of the hip, spine, wrist, or arm after bariatric surgery, she said.
Dr. Schafer incorporated her own clinical experience with recommendations from the Endocrine Society and from Tufts University in advising clinicians to take the following steps in managing patients undergoing bariatric surgery.
Prior to surgery, check serum 25-hydroxyvitamin D (25[OH]D) levels and prescribe preoperative treatment to augment vitamin D in patients with low levels. After surgery, all patients should take two multivitamins per day to make sure their micronutrient needs are met.
After malabsorptive bariatric surgery, such as gastric bypass, patients also should take calcium supplements, although there are not enough data to pinpoint the best dose or to identify which patients might most need the calcium, Dr. Schafer said. She recommended 1,200–2,000 mg/day (preferably in citrate form) after malabsorptive surgery and possibly after restrictive bariatric surgery such as adjustable gastric banding.
Based on the preoperative vitamin D level, prescribe 800-2,000 IU/day of vitamin D3 supplementation after malabsorptive surgery and possibly after restrictive bariatric surgery. “I've had people who need more” than that dose range, she added.
For postoperative surveillance, check calcium homeostasis laboratory tests every 6 months for the first 2 years and then annually after malabsorptive surgery and possibly after any bariatric surgery. The tests include calcium, albumin, phosphate, creatinine, 25(OH)D, and parathyroid hormone.
If the parathyroid hormone level is high, but the 25(OH)D level is low, treat with vitamin D supplementation. If the parathyroid hormone level is high and the 25(OH)D level is ideal, check the patient's 24-hour urinary calcium, and if that is low, increase calcium intake.
Because some of the etiology of bariatric surgery–induced bone loss may be the preferential loss of lean mass over fat mass, or changes in fat distribution, encourage patients to consume protein and to exercise, she said.
The Endocrine Society recommends dual-energy x-ray absorptiometry (DXA) at baseline and annually in people who are undergoing malabsorptive bariatric surgery. No data show that such monitoring actually improves outcomes, “but I do think that you should consider it for any people who can fit on the DXA scan before the operation,” Dr. Schafer said. The weight limit for the scanner is approximately 275–350 pounds.
Dr. Schafer also said that she advises a DXA scan 1-2 years postoperatively. Incorporate those results into “your clinical judgment and other risk factors like age or prior history of fractures to set up an individualized plan for monitoring bone density from there.”
In general, high body mass index has been associated with high bone mineral density, and either voluntary or involuntary weight loss is associated with bone loss and increased fracture risk. Bariatric surgery leads to loss of bone mass for multiple reasons, she said, including nutritional deficiencies from malabsorption, the body's signals about decreased skeletal loading with weight loss, and changes in fat-secreted hormone.
Most of the data on bone loss after bariatric surgery is for Roux-en-Y gastric bypass, which induces early and sustained increases in bone turnover and decreases in bone mineral density. Fewer data are available on other procedures, but a handful of studies suggest that another malabsorptive procedure, biliopancreatic diversion, may produce effects similar to those of gastric bypass, and that adjustable gastric banding may have less of an impact on bone, she said.
For gastric bypass, one study of 15 patients reported an 8% decrease in total hip bone mineral density within 9 months (J. Clin. Endocrinol. Metab. 2004;89:1061–5). Femoral neck bone density decreased by 9% within 1 year of gastric bypass in a separate study of 23 patients (J. Clin. Endocrinol. Metab. 2008;93:3735–40). A third study of 42 patients reported a 7% decrease in spine bone density and a 10% decrease in total hip bone density a year after gastric bypass (Obes. Surg. 2009;19:41–6).
Vitamin D deficiency can be a problem after bariatric surgery because many patients have low vitamin D levels before surgery, some of the surgeries are designed to create malabsorption, and patients eat less food and different kinds of food after surgery. In the worst cases, patients may develop secondary hyperparathyroidism or bone loss, and there have been case reports of osteomalacia.
All the studies used DXA scans to assess bone density after bariatric surgery, but DXA assessment may be biased in the setting of marked weight loss because of changes in soft tissue surrounding the bones. The informal consensus among experts is that the bone density losses reported by studies are real, “but we need nonbiased methods of assessing bone mineral density” for future studies of bariatric surgery's effects, she said.
Dr. Schafer said that she has no disclosures.
To watch an interview with Dr. Schafer, scan the QR code or visit www.rheumatologynews.com
SAN FRANCISCO – Bariatric surgery can be beneficial for obese people, but it also can lead to significant bone loss.
The limited data so far suggest that decreased bone mineral density after bariatric surgery is a real problem that increases the risk for fracture, Dr. Anne Schafer said at a meeting on osteoporosis sponsored by the University of California, San Francisco.
The extent of bone loss within a year after the most common bariatric surgery, Roux-en-Y gastric bypass, can be equivalent to “what you would expect in the first 5 years of menopause” in some women, said Dr. Schafer of the division of endocrinology at the University of California, San Francisco.
A 2011 study not yet published by the Mayo Clinic, Rochester, Minn., compared fracture rates in 277 patients undergoing bariatric surgery with local age- and sex-matched fracture rates. The surgeries occurred in 1985-2004, and 94% were gastric bypasses. The retrospective chart study found 138 fractures in 82 patients since the surgery, with a standardized incidence ratio of 2.1 for any fracture and 1.9 for fractures of the hip, spine, wrist, or arm after bariatric surgery, she said.
Dr. Schafer incorporated her own clinical experience with recommendations from the Endocrine Society and from Tufts University in advising clinicians to take the following steps in managing patients undergoing bariatric surgery.
Prior to surgery, check serum 25-hydroxyvitamin D (25[OH]D) levels and prescribe preoperative treatment to augment vitamin D in patients with low levels. After surgery, all patients should take two multivitamins per day to make sure their micronutrient needs are met.
After malabsorptive bariatric surgery, such as gastric bypass, patients also should take calcium supplements, although there are not enough data to pinpoint the best dose or to identify which patients might most need the calcium, Dr. Schafer said. She recommended 1,200–2,000 mg/day (preferably in citrate form) after malabsorptive surgery and possibly after restrictive bariatric surgery such as adjustable gastric banding.
Based on the preoperative vitamin D level, prescribe 800-2,000 IU/day of vitamin D3 supplementation after malabsorptive surgery and possibly after restrictive bariatric surgery. “I've had people who need more” than that dose range, she added.
For postoperative surveillance, check calcium homeostasis laboratory tests every 6 months for the first 2 years and then annually after malabsorptive surgery and possibly after any bariatric surgery. The tests include calcium, albumin, phosphate, creatinine, 25(OH)D, and parathyroid hormone.
If the parathyroid hormone level is high, but the 25(OH)D level is low, treat with vitamin D supplementation. If the parathyroid hormone level is high and the 25(OH)D level is ideal, check the patient's 24-hour urinary calcium, and if that is low, increase calcium intake.
Because some of the etiology of bariatric surgery–induced bone loss may be the preferential loss of lean mass over fat mass, or changes in fat distribution, encourage patients to consume protein and to exercise, she said.
The Endocrine Society recommends dual-energy x-ray absorptiometry (DXA) at baseline and annually in people who are undergoing malabsorptive bariatric surgery. No data show that such monitoring actually improves outcomes, “but I do think that you should consider it for any people who can fit on the DXA scan before the operation,” Dr. Schafer said. The weight limit for the scanner is approximately 275–350 pounds.
Dr. Schafer also said that she advises a DXA scan 1-2 years postoperatively. Incorporate those results into “your clinical judgment and other risk factors like age or prior history of fractures to set up an individualized plan for monitoring bone density from there.”
In general, high body mass index has been associated with high bone mineral density, and either voluntary or involuntary weight loss is associated with bone loss and increased fracture risk. Bariatric surgery leads to loss of bone mass for multiple reasons, she said, including nutritional deficiencies from malabsorption, the body's signals about decreased skeletal loading with weight loss, and changes in fat-secreted hormone.
Most of the data on bone loss after bariatric surgery is for Roux-en-Y gastric bypass, which induces early and sustained increases in bone turnover and decreases in bone mineral density. Fewer data are available on other procedures, but a handful of studies suggest that another malabsorptive procedure, biliopancreatic diversion, may produce effects similar to those of gastric bypass, and that adjustable gastric banding may have less of an impact on bone, she said.
For gastric bypass, one study of 15 patients reported an 8% decrease in total hip bone mineral density within 9 months (J. Clin. Endocrinol. Metab. 2004;89:1061–5). Femoral neck bone density decreased by 9% within 1 year of gastric bypass in a separate study of 23 patients (J. Clin. Endocrinol. Metab. 2008;93:3735–40). A third study of 42 patients reported a 7% decrease in spine bone density and a 10% decrease in total hip bone density a year after gastric bypass (Obes. Surg. 2009;19:41–6).
Vitamin D deficiency can be a problem after bariatric surgery because many patients have low vitamin D levels before surgery, some of the surgeries are designed to create malabsorption, and patients eat less food and different kinds of food after surgery. In the worst cases, patients may develop secondary hyperparathyroidism or bone loss, and there have been case reports of osteomalacia.
All the studies used DXA scans to assess bone density after bariatric surgery, but DXA assessment may be biased in the setting of marked weight loss because of changes in soft tissue surrounding the bones. The informal consensus among experts is that the bone density losses reported by studies are real, “but we need nonbiased methods of assessing bone mineral density” for future studies of bariatric surgery's effects, she said.
Dr. Schafer said that she has no disclosures.
To watch an interview with Dr. Schafer, scan the QR code or visit www.rheumatologynews.com
Compare Drugs for Steroid-Induced Osteoporosis : Head-to-head trials back options in treatment to allay 'skeletal cruelty'
SAN FRANCISCO – Physicians know that corticosteroids are bad for bones. So bad that rheumatologist Jonathan D. Graf calls them “a case of skeletal cruelty.”
Given the bad reputation of chronic steroid use when it comes to bone health, one might expect physicians to be aware of the medical evidence for choosing a drug to prevent or treat glucocorticoid-induced osteoporosis. Many physicians may be unaware of the evidence, however, judging by a poll Dr. Graf conducted at a meeting on osteoporosis sponsored by the University of California, San Francisco.
Nearly everyone present believed that there have been no comparative head-to-head studies of different medications to manage glucocorticoid-induced osteoporosis.
In reality, two of the approved drugs for managing glucocorticoid-induced osteoporosis – alendronate and risedronate – were shown to be effective in only placebo-controlled trials. But two others – zoledronic acid and teriparatide – showed some advantages over risedronate or alendronate, respectively, in head-to-head comparisons, said Dr. Graf of San Francisco General Hospital.
▸ Alendronate: A 48-week study randomized 477 patients who were taking at least 7.5 mg/day of prednisone (or the equivalent) to treatment with alendronate 5 mg/day or 10 mg/day or placebo. The 10-mg alendronate group showed significantly improved lumbar bone mineral density at 48 weeks compared with the placebo group. Bone density benefits were less impressive but statistically significant for the femoral neck, trochanter, and total body compared with placebo (N. Engl. J. Med. 1998;339:292–9).
The bone density improvements on 10 mg alendronate were seen in all subgroups of patients but especially in postmenopausal women who were not taking estrogen. The risk for fractures did not differ significantly between groups for the cohort as a whole, but postmenopausal women had a significantly lower risk of fracture if they were on 10 mg alendronate, compared with placebo (4% vs. 13%).
In an extension study that followed 208 of the patients on their same regimens for another 12 months, the difference in fracture risk became significant for the cohort as a whole at 2 years: 1% in the alendronate groups and 7% on placebo. All patients in the extension study received calcium and vitamin D supplementation (Arthritis Rheum. 2001;44:202-11).
▸ Risedronate: Two separate multicenter, double-blind studies randomized patients to 2.5 mg/day or 5 mg/day risedronate or placebo, and all received calcium and vitamin D supplementation.
In one study of 224 adults starting long-term glucocorticoid therapy, patients on risedronate maintained or improved bone mineral density, which decreased significantly in patients on placebo. There was a trend toward a lower rate of new vertebral fractures at 1 year on risedronate 5 mg (6%) than on placebo (17%), but the difference was not statistically significant (Arthritis Rheum. 1999;42:2309–18).
In a separate study of 290 adults who already had been using at least 7.5 mg/day of prednisone for at least 6 months, the rate of new vertebral fractures was significantly lower at 1 year in the combined risedronate groups (5%), compared with the placebo group (15%), while rates of adverse events did not differ significantly. The risedronate groups also showed significantly higher bone mineral density at the hip and spine, compared with the placebo group (J. Bone Miner. Res. 2000;15:1006–13).
▸ Zoledronic acid: A multicenter double-blind, double-dummy trial randomized 833 patients who were on steroid therapy to either a single intravenous infusion of 5 mg zoledronic acid or oral risedronate 5 mg/day. The cohort was “very representative of patients that I see” in practice, Dr. Graf said. Most were on 7.5 mg/day or more of prednisone daily, mostly for rheumatologic disorders.
Patients receiving zoledronic acid showed significantly better bone density at the lumbar spine after 1 year, compared with patients on risedronate (Lancet 2009;373:1253–63). The advantage was true both for preventing osteoporosis in “new” steroid users (less than 3 months use) and for treating chronic steroid users (more than 3 months).
“There are a whole bunch of issues with toxicity with zoledronic acid, compared with the other bisphosphonates, and there are cost issues and infusion issues,” Dr. Graf said. “Whether or not you should use it in your practice is your choice, but I think you have to be aware of the fact that this drug has been studied head to head.”
The study did not assess fracture risk. “Clinically speaking, we really don't know if this improves fracture risk, but we do know that there is a superior effect on bone mineral density,” he said.
▸ Teriparatide: A 3-year double-blinded trial randomized 428 adults who had been on the equivalent of 5 mg/day of prednisone for at least 3 months to treatment with 20 mcg/day of teriparatide or 10 mg/day of alendronate. These were high-risk patients with baseline bone mineral density T scores of less than −2.0 or less than −1.0 with a history of fragility fracture. In all, 20% in each group had a history of nonvertebral fragility fracture. The reason for taking glucocorticoids was rheumatologic disease in 75% of each group.
A quarter of patients in each group dropped out of the study. In intent-to-treat analyses, bone mineral densities were higher in the teriparatide group than in those on alendronate at 18 months or at 36 months. A highly significant difference emerged in radiographically identified vertebral fractures in the teriparatide group (1%), compared with the alendronate group (6%) at the interim 18-month analysis (N. Engl. J. Med. 2007;357: 2028–39).
By 36 months, the teriparatide group showed significantly lower rates of radiographic vertebral fractures (2%) and clinical vertebral fractures (0%), compared with the alendronate group (8% and 12%). No significant differences in nonvertebral fractures were seen at either time point.
“So, this primarily is of clinical benefit in the spine,” Dr. Graf said, “but the overall rate of clinical fractures is low in both groups.”
He suggested that clinicians consider teriparatide for patients with the most severe glucocorticoid-induced osteoporosis or patients at highest risk for fracture, such as those with previous fragility fractures.
▸ Denosumab: Although this drug is not yet approved for managing glucocorticoid-induced osteoporosis, a subgroup analysis from phase II trial data on 218 patients who were taking either glucocorticoids or bisphosphonates showed that adding denosumab significantly improved lumbar bone mineral density “on top of what you would normally see from the bisphosphonate,” Dr. Graf said (Ann. Rheum. Dis. 2010;69:872–5).
Dr. Graf said he has no conflicts of interest.
{kind=link}
Consider teriparatide for patients with the most severe cases, or those at highest risk for fracture.
Source DR. GRAF
SAN FRANCISCO – Physicians know that corticosteroids are bad for bones. So bad that rheumatologist Jonathan D. Graf calls them “a case of skeletal cruelty.”
Given the bad reputation of chronic steroid use when it comes to bone health, one might expect physicians to be aware of the medical evidence for choosing a drug to prevent or treat glucocorticoid-induced osteoporosis. Many physicians may be unaware of the evidence, however, judging by a poll Dr. Graf conducted at a meeting on osteoporosis sponsored by the University of California, San Francisco.
Nearly everyone present believed that there have been no comparative head-to-head studies of different medications to manage glucocorticoid-induced osteoporosis.
In reality, two of the approved drugs for managing glucocorticoid-induced osteoporosis – alendronate and risedronate – were shown to be effective in only placebo-controlled trials. But two others – zoledronic acid and teriparatide – showed some advantages over risedronate or alendronate, respectively, in head-to-head comparisons, said Dr. Graf of San Francisco General Hospital.
▸ Alendronate: A 48-week study randomized 477 patients who were taking at least 7.5 mg/day of prednisone (or the equivalent) to treatment with alendronate 5 mg/day or 10 mg/day or placebo. The 10-mg alendronate group showed significantly improved lumbar bone mineral density at 48 weeks compared with the placebo group. Bone density benefits were less impressive but statistically significant for the femoral neck, trochanter, and total body compared with placebo (N. Engl. J. Med. 1998;339:292–9).
The bone density improvements on 10 mg alendronate were seen in all subgroups of patients but especially in postmenopausal women who were not taking estrogen. The risk for fractures did not differ significantly between groups for the cohort as a whole, but postmenopausal women had a significantly lower risk of fracture if they were on 10 mg alendronate, compared with placebo (4% vs. 13%).
In an extension study that followed 208 of the patients on their same regimens for another 12 months, the difference in fracture risk became significant for the cohort as a whole at 2 years: 1% in the alendronate groups and 7% on placebo. All patients in the extension study received calcium and vitamin D supplementation (Arthritis Rheum. 2001;44:202-11).
▸ Risedronate: Two separate multicenter, double-blind studies randomized patients to 2.5 mg/day or 5 mg/day risedronate or placebo, and all received calcium and vitamin D supplementation.
In one study of 224 adults starting long-term glucocorticoid therapy, patients on risedronate maintained or improved bone mineral density, which decreased significantly in patients on placebo. There was a trend toward a lower rate of new vertebral fractures at 1 year on risedronate 5 mg (6%) than on placebo (17%), but the difference was not statistically significant (Arthritis Rheum. 1999;42:2309–18).
In a separate study of 290 adults who already had been using at least 7.5 mg/day of prednisone for at least 6 months, the rate of new vertebral fractures was significantly lower at 1 year in the combined risedronate groups (5%), compared with the placebo group (15%), while rates of adverse events did not differ significantly. The risedronate groups also showed significantly higher bone mineral density at the hip and spine, compared with the placebo group (J. Bone Miner. Res. 2000;15:1006–13).
▸ Zoledronic acid: A multicenter double-blind, double-dummy trial randomized 833 patients who were on steroid therapy to either a single intravenous infusion of 5 mg zoledronic acid or oral risedronate 5 mg/day. The cohort was “very representative of patients that I see” in practice, Dr. Graf said. Most were on 7.5 mg/day or more of prednisone daily, mostly for rheumatologic disorders.
Patients receiving zoledronic acid showed significantly better bone density at the lumbar spine after 1 year, compared with patients on risedronate (Lancet 2009;373:1253–63). The advantage was true both for preventing osteoporosis in “new” steroid users (less than 3 months use) and for treating chronic steroid users (more than 3 months).
“There are a whole bunch of issues with toxicity with zoledronic acid, compared with the other bisphosphonates, and there are cost issues and infusion issues,” Dr. Graf said. “Whether or not you should use it in your practice is your choice, but I think you have to be aware of the fact that this drug has been studied head to head.”
The study did not assess fracture risk. “Clinically speaking, we really don't know if this improves fracture risk, but we do know that there is a superior effect on bone mineral density,” he said.
▸ Teriparatide: A 3-year double-blinded trial randomized 428 adults who had been on the equivalent of 5 mg/day of prednisone for at least 3 months to treatment with 20 mcg/day of teriparatide or 10 mg/day of alendronate. These were high-risk patients with baseline bone mineral density T scores of less than −2.0 or less than −1.0 with a history of fragility fracture. In all, 20% in each group had a history of nonvertebral fragility fracture. The reason for taking glucocorticoids was rheumatologic disease in 75% of each group.
A quarter of patients in each group dropped out of the study. In intent-to-treat analyses, bone mineral densities were higher in the teriparatide group than in those on alendronate at 18 months or at 36 months. A highly significant difference emerged in radiographically identified vertebral fractures in the teriparatide group (1%), compared with the alendronate group (6%) at the interim 18-month analysis (N. Engl. J. Med. 2007;357: 2028–39).
By 36 months, the teriparatide group showed significantly lower rates of radiographic vertebral fractures (2%) and clinical vertebral fractures (0%), compared with the alendronate group (8% and 12%). No significant differences in nonvertebral fractures were seen at either time point.
“So, this primarily is of clinical benefit in the spine,” Dr. Graf said, “but the overall rate of clinical fractures is low in both groups.”
He suggested that clinicians consider teriparatide for patients with the most severe glucocorticoid-induced osteoporosis or patients at highest risk for fracture, such as those with previous fragility fractures.
▸ Denosumab: Although this drug is not yet approved for managing glucocorticoid-induced osteoporosis, a subgroup analysis from phase II trial data on 218 patients who were taking either glucocorticoids or bisphosphonates showed that adding denosumab significantly improved lumbar bone mineral density “on top of what you would normally see from the bisphosphonate,” Dr. Graf said (Ann. Rheum. Dis. 2010;69:872–5).
Dr. Graf said he has no conflicts of interest.
Consider teriparatide for patients with the most severe cases, or those at highest risk for fracture.
Source DR. GRAF
SAN FRANCISCO – Physicians know that corticosteroids are bad for bones. So bad that rheumatologist Jonathan D. Graf calls them “a case of skeletal cruelty.”
Given the bad reputation of chronic steroid use when it comes to bone health, one might expect physicians to be aware of the medical evidence for choosing a drug to prevent or treat glucocorticoid-induced osteoporosis. Many physicians may be unaware of the evidence, however, judging by a poll Dr. Graf conducted at a meeting on osteoporosis sponsored by the University of California, San Francisco.
Nearly everyone present believed that there have been no comparative head-to-head studies of different medications to manage glucocorticoid-induced osteoporosis.
In reality, two of the approved drugs for managing glucocorticoid-induced osteoporosis – alendronate and risedronate – were shown to be effective in only placebo-controlled trials. But two others – zoledronic acid and teriparatide – showed some advantages over risedronate or alendronate, respectively, in head-to-head comparisons, said Dr. Graf of San Francisco General Hospital.
▸ Alendronate: A 48-week study randomized 477 patients who were taking at least 7.5 mg/day of prednisone (or the equivalent) to treatment with alendronate 5 mg/day or 10 mg/day or placebo. The 10-mg alendronate group showed significantly improved lumbar bone mineral density at 48 weeks compared with the placebo group. Bone density benefits were less impressive but statistically significant for the femoral neck, trochanter, and total body compared with placebo (N. Engl. J. Med. 1998;339:292–9).
The bone density improvements on 10 mg alendronate were seen in all subgroups of patients but especially in postmenopausal women who were not taking estrogen. The risk for fractures did not differ significantly between groups for the cohort as a whole, but postmenopausal women had a significantly lower risk of fracture if they were on 10 mg alendronate, compared with placebo (4% vs. 13%).
In an extension study that followed 208 of the patients on their same regimens for another 12 months, the difference in fracture risk became significant for the cohort as a whole at 2 years: 1% in the alendronate groups and 7% on placebo. All patients in the extension study received calcium and vitamin D supplementation (Arthritis Rheum. 2001;44:202-11).
▸ Risedronate: Two separate multicenter, double-blind studies randomized patients to 2.5 mg/day or 5 mg/day risedronate or placebo, and all received calcium and vitamin D supplementation.
In one study of 224 adults starting long-term glucocorticoid therapy, patients on risedronate maintained or improved bone mineral density, which decreased significantly in patients on placebo. There was a trend toward a lower rate of new vertebral fractures at 1 year on risedronate 5 mg (6%) than on placebo (17%), but the difference was not statistically significant (Arthritis Rheum. 1999;42:2309–18).
In a separate study of 290 adults who already had been using at least 7.5 mg/day of prednisone for at least 6 months, the rate of new vertebral fractures was significantly lower at 1 year in the combined risedronate groups (5%), compared with the placebo group (15%), while rates of adverse events did not differ significantly. The risedronate groups also showed significantly higher bone mineral density at the hip and spine, compared with the placebo group (J. Bone Miner. Res. 2000;15:1006–13).
▸ Zoledronic acid: A multicenter double-blind, double-dummy trial randomized 833 patients who were on steroid therapy to either a single intravenous infusion of 5 mg zoledronic acid or oral risedronate 5 mg/day. The cohort was “very representative of patients that I see” in practice, Dr. Graf said. Most were on 7.5 mg/day or more of prednisone daily, mostly for rheumatologic disorders.
Patients receiving zoledronic acid showed significantly better bone density at the lumbar spine after 1 year, compared with patients on risedronate (Lancet 2009;373:1253–63). The advantage was true both for preventing osteoporosis in “new” steroid users (less than 3 months use) and for treating chronic steroid users (more than 3 months).
“There are a whole bunch of issues with toxicity with zoledronic acid, compared with the other bisphosphonates, and there are cost issues and infusion issues,” Dr. Graf said. “Whether or not you should use it in your practice is your choice, but I think you have to be aware of the fact that this drug has been studied head to head.”
The study did not assess fracture risk. “Clinically speaking, we really don't know if this improves fracture risk, but we do know that there is a superior effect on bone mineral density,” he said.
▸ Teriparatide: A 3-year double-blinded trial randomized 428 adults who had been on the equivalent of 5 mg/day of prednisone for at least 3 months to treatment with 20 mcg/day of teriparatide or 10 mg/day of alendronate. These were high-risk patients with baseline bone mineral density T scores of less than −2.0 or less than −1.0 with a history of fragility fracture. In all, 20% in each group had a history of nonvertebral fragility fracture. The reason for taking glucocorticoids was rheumatologic disease in 75% of each group.
A quarter of patients in each group dropped out of the study. In intent-to-treat analyses, bone mineral densities were higher in the teriparatide group than in those on alendronate at 18 months or at 36 months. A highly significant difference emerged in radiographically identified vertebral fractures in the teriparatide group (1%), compared with the alendronate group (6%) at the interim 18-month analysis (N. Engl. J. Med. 2007;357: 2028–39).
By 36 months, the teriparatide group showed significantly lower rates of radiographic vertebral fractures (2%) and clinical vertebral fractures (0%), compared with the alendronate group (8% and 12%). No significant differences in nonvertebral fractures were seen at either time point.
“So, this primarily is of clinical benefit in the spine,” Dr. Graf said, “but the overall rate of clinical fractures is low in both groups.”
He suggested that clinicians consider teriparatide for patients with the most severe glucocorticoid-induced osteoporosis or patients at highest risk for fracture, such as those with previous fragility fractures.
▸ Denosumab: Although this drug is not yet approved for managing glucocorticoid-induced osteoporosis, a subgroup analysis from phase II trial data on 218 patients who were taking either glucocorticoids or bisphosphonates showed that adding denosumab significantly improved lumbar bone mineral density “on top of what you would normally see from the bisphosphonate,” Dr. Graf said (Ann. Rheum. Dis. 2010;69:872–5).
Dr. Graf said he has no conflicts of interest.
Consider teriparatide for patients with the most severe cases, or those at highest risk for fracture.
Source DR. GRAF
MRI Poised to Boost Early Osteoarthritis Detection
Magnetic resonance imaging has an increasingly important role in the early detection and diagnosis of osteoarthritis, although for now it remains one of several diagnostic tools that also include x-rays, clinical findings, and lab results.
Physicians who treat patients with osteoarthritis (OA) need further research results to better clarify the best use of MRI in early OA detection, said Dr. Philip Conaghan, professor of musculoskeletal medicine at the University of Leeds (England).

In June, Dr. Conaghan and his colleagues on the OA Imaging Working Group for the Osteoarthritis Research Society International (OARSI) issued 11 propositions on using MRI to define OA – propositions that the group said need formal testing "regarding their diagnostic performance before they are more widely used" (Osteoarthritis Cartilage 2011;19:963-9).
The working group clearly endorsed MRI, saying that "MRI may add to the diagnosis of OA and should be incorporated into the [American College of Rheumatology] diagnostic criteria," but in the same proposition, the working group also reiterated the role of x-ray, clinical, and laboratory parameters. Other propositions caution that "no single MRI finding is diagnostic of MRI," and that "certain MRI changes in isolation ... are not diagnostic of osteoarthritis."
The working group’s propositions included two MRI-based definitions of OA, for the tibiofemoral form and for the patellofemoral type.
In a recent talk on MRI and OA, Dr. Conaghan stressed the potential that MRI holds for early OA detection.
"We need to develop an early OA culture," similar to what has emerged for rheumatoid arthritis, he said speaking in May at the annual European Congress of Rheumatology in London. "In OA, we need a culture of early intervention" that would rely on early detection, most likely using MRI.
"Clinical features may suffice at present" for early OA detection, but MRI offers the best individualized option for assessing cartilage, bone features, and possibly the meniscus, he said. Soluble biomarkers may be more feasible than MRI, but biomarkers need more development and for early detection are "not there yet."
The sheer frequency of MRI lesions in OA patients may prove limiting. OA lesions appear more often on MRI than on x-rays. In five different reported series, the prevalence of cartilage defects visible by MRI in OA patients was 85%-98%, and the prevalence of osteophytes was 70%-100%, Dr. Conaghan noted. Often the MRI changes appear with no radiographic change visible. Other MRI changes that look like promising OA markers are bone marrow lesions and bone shape.
The OARSI Working Group defined tibiofemoral OA by MRI as either both items from group A, or one group A item and at least two from group B. The group A diagnostic features are definite osteophyte formation and full-thickness cartilage loss. The group B items are a subchondral bone marrow lesion or cyst that is not associated with meniscal or ligamentous attachments; meniscal subluxation, maceration, or degenerative tear; partial-thickness cartilage loss, and bone attrition.
The working group’s definition of patellofemoral OA requires both a definitive osteophyte and partial- or full-thickness cartilage loss.
Dr. Conaghan said that he had no relevant disclosures.
Magnetic resonance imaging has an increasingly important role in the early detection and diagnosis of osteoarthritis, although for now it remains one of several diagnostic tools that also include x-rays, clinical findings, and lab results.
Physicians who treat patients with osteoarthritis (OA) need further research results to better clarify the best use of MRI in early OA detection, said Dr. Philip Conaghan, professor of musculoskeletal medicine at the University of Leeds (England).
In June, Dr. Conaghan and his colleagues on the OA Imaging Working Group for the Osteoarthritis Research Society International (OARSI) issued 11 propositions on using MRI to define OA – propositions that the group said need formal testing "regarding their diagnostic performance before they are more widely used" (Osteoarthritis Cartilage 2011;19:963-9).
The working group clearly endorsed MRI, saying that "MRI may add to the diagnosis of OA and should be incorporated into the [American College of Rheumatology] diagnostic criteria," but in the same proposition, the working group also reiterated the role of x-ray, clinical, and laboratory parameters. Other propositions caution that "no single MRI finding is diagnostic of MRI," and that "certain MRI changes in isolation ... are not diagnostic of osteoarthritis."
The working group’s propositions included two MRI-based definitions of OA, for the tibiofemoral form and for the patellofemoral type.
In a recent talk on MRI and OA, Dr. Conaghan stressed the potential that MRI holds for early OA detection.
"We need to develop an early OA culture," similar to what has emerged for rheumatoid arthritis, he said speaking in May at the annual European Congress of Rheumatology in London. "In OA, we need a culture of early intervention" that would rely on early detection, most likely using MRI.
"Clinical features may suffice at present" for early OA detection, but MRI offers the best individualized option for assessing cartilage, bone features, and possibly the meniscus, he said. Soluble biomarkers may be more feasible than MRI, but biomarkers need more development and for early detection are "not there yet."
The sheer frequency of MRI lesions in OA patients may prove limiting. OA lesions appear more often on MRI than on x-rays. In five different reported series, the prevalence of cartilage defects visible by MRI in OA patients was 85%-98%, and the prevalence of osteophytes was 70%-100%, Dr. Conaghan noted. Often the MRI changes appear with no radiographic change visible. Other MRI changes that look like promising OA markers are bone marrow lesions and bone shape.
The OARSI Working Group defined tibiofemoral OA by MRI as either both items from group A, or one group A item and at least two from group B. The group A diagnostic features are definite osteophyte formation and full-thickness cartilage loss. The group B items are a subchondral bone marrow lesion or cyst that is not associated with meniscal or ligamentous attachments; meniscal subluxation, maceration, or degenerative tear; partial-thickness cartilage loss, and bone attrition.
The working group’s definition of patellofemoral OA requires both a definitive osteophyte and partial- or full-thickness cartilage loss.
Dr. Conaghan said that he had no relevant disclosures.
Magnetic resonance imaging has an increasingly important role in the early detection and diagnosis of osteoarthritis, although for now it remains one of several diagnostic tools that also include x-rays, clinical findings, and lab results.
Physicians who treat patients with osteoarthritis (OA) need further research results to better clarify the best use of MRI in early OA detection, said Dr. Philip Conaghan, professor of musculoskeletal medicine at the University of Leeds (England).
In June, Dr. Conaghan and his colleagues on the OA Imaging Working Group for the Osteoarthritis Research Society International (OARSI) issued 11 propositions on using MRI to define OA – propositions that the group said need formal testing "regarding their diagnostic performance before they are more widely used" (Osteoarthritis Cartilage 2011;19:963-9).
The working group clearly endorsed MRI, saying that "MRI may add to the diagnosis of OA and should be incorporated into the [American College of Rheumatology] diagnostic criteria," but in the same proposition, the working group also reiterated the role of x-ray, clinical, and laboratory parameters. Other propositions caution that "no single MRI finding is diagnostic of MRI," and that "certain MRI changes in isolation ... are not diagnostic of osteoarthritis."
The working group’s propositions included two MRI-based definitions of OA, for the tibiofemoral form and for the patellofemoral type.
In a recent talk on MRI and OA, Dr. Conaghan stressed the potential that MRI holds for early OA detection.
"We need to develop an early OA culture," similar to what has emerged for rheumatoid arthritis, he said speaking in May at the annual European Congress of Rheumatology in London. "In OA, we need a culture of early intervention" that would rely on early detection, most likely using MRI.
"Clinical features may suffice at present" for early OA detection, but MRI offers the best individualized option for assessing cartilage, bone features, and possibly the meniscus, he said. Soluble biomarkers may be more feasible than MRI, but biomarkers need more development and for early detection are "not there yet."
The sheer frequency of MRI lesions in OA patients may prove limiting. OA lesions appear more often on MRI than on x-rays. In five different reported series, the prevalence of cartilage defects visible by MRI in OA patients was 85%-98%, and the prevalence of osteophytes was 70%-100%, Dr. Conaghan noted. Often the MRI changes appear with no radiographic change visible. Other MRI changes that look like promising OA markers are bone marrow lesions and bone shape.
The OARSI Working Group defined tibiofemoral OA by MRI as either both items from group A, or one group A item and at least two from group B. The group A diagnostic features are definite osteophyte formation and full-thickness cartilage loss. The group B items are a subchondral bone marrow lesion or cyst that is not associated with meniscal or ligamentous attachments; meniscal subluxation, maceration, or degenerative tear; partial-thickness cartilage loss, and bone attrition.
The working group’s definition of patellofemoral OA requires both a definitive osteophyte and partial- or full-thickness cartilage loss.
Dr. Conaghan said that he had no relevant disclosures.
Hand Osteoarthritis Affects More Women Than Men
Hand osteoarthritis becomes more prevalent with advancing age and is more common in women than men, but not in all joint areas, results from a long-term analysis demonstrated.
Over 9 years of follow-up, more men than women developed metacarpal and wrist osteoarthritis (OA), yet more women than men developed erosive and symptomatic OA, according to a report by researchers led by Dr. Ida K. Haugen of the department of rheumatology at Diakonhjemmet Hospital, Oslo, that was published in the September 2011 edition of the Annals of the Rheumatic Diseases.
In what they describe as the first study of its kind, the researchers analyzed data from 2,300 adults who participated in the Framingham OA Study to determine the prevalence and course of radiographic, erosive, and symptomatic hand OA in the general population. All study participants had bilateral hand radiographs at baseline and at 9-year follow-up (Ann. Rheum. Dis. 2011;70:1581-6).
Dr. Ida Haugen and her associates defined radiographic hand OA at the joint level as a Kellgren-Lawrence scale grade 2 or greater, erosive hand OA as a Kellgren-Lawrence grade 2 or greater plus erosion, and symptomatic hand OA as a Kellgren-Lawrence grade 2 or greater plus pain/aching/stiffness. Study participants with one or more affected joint were classified as having hand OA.
The mean age of the study participants was 59 years, 57% were women, and 96% were white. The age-standardized prevalence of hand OA was modestly higher in women compared with men (44% vs. 38%, respectively), but women had a significantly higher age-standardized prevalence of erosive OA (10% vs. 3%) and symptomatic OA (16% vs. 8%).
Over the 9 years of follow-up, the crude incidence was similar between women and men (35% vs. 34%, respectively), whereas 96% of women and 91% of men who had hand OA at baseline showed progression during follow-up.
The researchers also reported that metacarpophalangeal and wrist OA occurred more frequently and from a younger age in men, compared with women, and that development of erosive disease occurred more frequently in women, compared with men (17% vs. 10%, respectively).
"Consistent with previous studies, we found no clear evidence of higher hand OA incidence in the right hand (usually dominant)," the researchers wrote. "The symmetrical joint affection indicates that ‘wear and tear’ alone is not sufficient to explain the pattern of hand OA, and neurogenic and hormonal influences have been suggested."
They acknowledged certain limitations of the study, including the fact that participants were from a limited geographic area, which makes it "uncertain whether the results can be generalized to larger geographical areas or [nonwhite] groups," they wrote. "The offspring cohort [of the Framingham OA Study] was not randomly selected from the population. However, the participants were not chosen based on joint symptoms, and previous studies have indicated that the cohort is reasonably representative of the US population. The mean time of follow-up was 9 years, and almost all participants showed progression, making discrimination between groups difficult. It is possible but unproven that reading of radiographs in known time sequence may lead to overestimation of progression."
The Framingham Osteoarthritis Study is supported by the National Institutes of Health. Dr. Haugen disclosed that she received grants from the South-Eastern Norway Regional Health Authority and a scholarship from OARSI. Another study investigator, Dr. Martin Englund, disclosed that he received funding support from Swedish Research Council and Lund (Sweden) University, Sweden.
Hand osteoarthritis becomes more prevalent with advancing age and is more common in women than men, but not in all joint areas, results from a long-term analysis demonstrated.
Over 9 years of follow-up, more men than women developed metacarpal and wrist osteoarthritis (OA), yet more women than men developed erosive and symptomatic OA, according to a report by researchers led by Dr. Ida K. Haugen of the department of rheumatology at Diakonhjemmet Hospital, Oslo, that was published in the September 2011 edition of the Annals of the Rheumatic Diseases.
In what they describe as the first study of its kind, the researchers analyzed data from 2,300 adults who participated in the Framingham OA Study to determine the prevalence and course of radiographic, erosive, and symptomatic hand OA in the general population. All study participants had bilateral hand radiographs at baseline and at 9-year follow-up (Ann. Rheum. Dis. 2011;70:1581-6).
Dr. Ida Haugen and her associates defined radiographic hand OA at the joint level as a Kellgren-Lawrence scale grade 2 or greater, erosive hand OA as a Kellgren-Lawrence grade 2 or greater plus erosion, and symptomatic hand OA as a Kellgren-Lawrence grade 2 or greater plus pain/aching/stiffness. Study participants with one or more affected joint were classified as having hand OA.
The mean age of the study participants was 59 years, 57% were women, and 96% were white. The age-standardized prevalence of hand OA was modestly higher in women compared with men (44% vs. 38%, respectively), but women had a significantly higher age-standardized prevalence of erosive OA (10% vs. 3%) and symptomatic OA (16% vs. 8%).
Over the 9 years of follow-up, the crude incidence was similar between women and men (35% vs. 34%, respectively), whereas 96% of women and 91% of men who had hand OA at baseline showed progression during follow-up.
The researchers also reported that metacarpophalangeal and wrist OA occurred more frequently and from a younger age in men, compared with women, and that development of erosive disease occurred more frequently in women, compared with men (17% vs. 10%, respectively).
"Consistent with previous studies, we found no clear evidence of higher hand OA incidence in the right hand (usually dominant)," the researchers wrote. "The symmetrical joint affection indicates that ‘wear and tear’ alone is not sufficient to explain the pattern of hand OA, and neurogenic and hormonal influences have been suggested."
They acknowledged certain limitations of the study, including the fact that participants were from a limited geographic area, which makes it "uncertain whether the results can be generalized to larger geographical areas or [nonwhite] groups," they wrote. "The offspring cohort [of the Framingham OA Study] was not randomly selected from the population. However, the participants were not chosen based on joint symptoms, and previous studies have indicated that the cohort is reasonably representative of the US population. The mean time of follow-up was 9 years, and almost all participants showed progression, making discrimination between groups difficult. It is possible but unproven that reading of radiographs in known time sequence may lead to overestimation of progression."
The Framingham Osteoarthritis Study is supported by the National Institutes of Health. Dr. Haugen disclosed that she received grants from the South-Eastern Norway Regional Health Authority and a scholarship from OARSI. Another study investigator, Dr. Martin Englund, disclosed that he received funding support from Swedish Research Council and Lund (Sweden) University, Sweden.
Hand osteoarthritis becomes more prevalent with advancing age and is more common in women than men, but not in all joint areas, results from a long-term analysis demonstrated.
Over 9 years of follow-up, more men than women developed metacarpal and wrist osteoarthritis (OA), yet more women than men developed erosive and symptomatic OA, according to a report by researchers led by Dr. Ida K. Haugen of the department of rheumatology at Diakonhjemmet Hospital, Oslo, that was published in the September 2011 edition of the Annals of the Rheumatic Diseases.
In what they describe as the first study of its kind, the researchers analyzed data from 2,300 adults who participated in the Framingham OA Study to determine the prevalence and course of radiographic, erosive, and symptomatic hand OA in the general population. All study participants had bilateral hand radiographs at baseline and at 9-year follow-up (Ann. Rheum. Dis. 2011;70:1581-6).
Dr. Ida Haugen and her associates defined radiographic hand OA at the joint level as a Kellgren-Lawrence scale grade 2 or greater, erosive hand OA as a Kellgren-Lawrence grade 2 or greater plus erosion, and symptomatic hand OA as a Kellgren-Lawrence grade 2 or greater plus pain/aching/stiffness. Study participants with one or more affected joint were classified as having hand OA.
The mean age of the study participants was 59 years, 57% were women, and 96% were white. The age-standardized prevalence of hand OA was modestly higher in women compared with men (44% vs. 38%, respectively), but women had a significantly higher age-standardized prevalence of erosive OA (10% vs. 3%) and symptomatic OA (16% vs. 8%).
Over the 9 years of follow-up, the crude incidence was similar between women and men (35% vs. 34%, respectively), whereas 96% of women and 91% of men who had hand OA at baseline showed progression during follow-up.
The researchers also reported that metacarpophalangeal and wrist OA occurred more frequently and from a younger age in men, compared with women, and that development of erosive disease occurred more frequently in women, compared with men (17% vs. 10%, respectively).
"Consistent with previous studies, we found no clear evidence of higher hand OA incidence in the right hand (usually dominant)," the researchers wrote. "The symmetrical joint affection indicates that ‘wear and tear’ alone is not sufficient to explain the pattern of hand OA, and neurogenic and hormonal influences have been suggested."
They acknowledged certain limitations of the study, including the fact that participants were from a limited geographic area, which makes it "uncertain whether the results can be generalized to larger geographical areas or [nonwhite] groups," they wrote. "The offspring cohort [of the Framingham OA Study] was not randomly selected from the population. However, the participants were not chosen based on joint symptoms, and previous studies have indicated that the cohort is reasonably representative of the US population. The mean time of follow-up was 9 years, and almost all participants showed progression, making discrimination between groups difficult. It is possible but unproven that reading of radiographs in known time sequence may lead to overestimation of progression."
The Framingham Osteoarthritis Study is supported by the National Institutes of Health. Dr. Haugen disclosed that she received grants from the South-Eastern Norway Regional Health Authority and a scholarship from OARSI. Another study investigator, Dr. Martin Englund, disclosed that he received funding support from Swedish Research Council and Lund (Sweden) University, Sweden.
FROM THE ANNALS OF THE RHEUMATIC DISEASES
Major Finding: The age-standardized prevalence of hand OA was modestly higher in women compared with men (44% vs. 38%, respectively), but women had a significantly higher age-standardized prevalence of erosive OA (10% vs. 3%) and symptomatic OA (16% vs. 8%).
Data Source: An analysis of 2,300 adults from the ongoing Framingham Osteoarthritis Study who had bilateral hand radiographs at baseline and at 9-year follow-up.
Disclosures: The Framingham OA Study is supported by the National Institutes of Health. Dr. Haugen disclosed that she received grants from the South-Eastern Norway Regional Health Authority and a scholarship from OARSI. Another study investigator, Dr. Martin Englund, disclosed that he received funding support from Swedish Research Council and Lund (Sweden) University.
Study Questions Combining Analgesics for Knee Pain
Combining ibuprofen and paracetamol at nonprescription doses conferred a modest improvement in pain relief in adults with knee pain/osteoarthritis. But this gain came at the expense of an increase in presumed gastrointestinal bleeding, results from a large randomized, controlled trial demonstrated.
The trial, published in the September 2011 edition of the Annals of Rheumatic Diseases, found that paracetamol 3 g/day may cause similar levels of blood loss as ibuprofen 1,200 mg/day, and that the combination of the two appears to be additive or even synergistic in terms of the number of individuals with a decrease in hemoglobin greater than 2 g/dL.
"These results need to be confirmed, along with their clinical relevance and identification of the site of gastrointestinal bleeding," wrote the researchers, who were led by Dr. Michael Doherty of the Arthritis UK Pain Center at Nottingham (England) City Hospital. "If confirmed, this observation should lead to the reconsideration of current recommendations for oral analgesic use in osteoarthritis and in chronic pain in general, and to the consideration of strategies to reduce this side effect."
Over a period of 13 weeks, Dr. Doherty and his associates followed 892 adults with chronic knee pain who were randomized to one of four treatment regimens, each taken three times a day: ibuprofen (400 mg), paracetamol (1,000 mg), one fixed-dose combination tablet (ibuprofen 200 mg/paracetamol 500 mg), or two fixed-dose combination tablets (ibuprofen 400 mg/paracetamol 1,000 mg).
The primary short-term efficacy end point was the difference at 10 days between groups in the WOMAC (Western Ontario McMaster Universities) osteoarthritis index pain subscale, which was normalized to a 0- to 100-mm scale.
The primary long-term efficacy end point was the patient global assessment of study medication after 13 weeks. This was determined by asking patients, "Taking into account both how your medicine worked for you and any side effects you think it caused you, how would you rate your medication as a treatment for your painful knee?" Respondents used a 5-point scale for replies (1, excellent; 2, good; 3, fair; 4, poor; 5, unacceptable).
The primary safety end point was the incidence of moderate and severe adverse events reported during the study period (Ann. Rheum. Dis. 2011;70:1534-41).
Criteria for inclusion were age of at least 40 years; knee pain for most of the past 3 months and on 4 of 7 preceding days; discontinuation of current analgesics; Steinbrocker functional capacity class I-III; and pain affecting the index knee (after a washout period if currently taking analgesics) of 30 mm or greater and 80 mm or less on a 100-mm visual analog scale over the previous 48 hours for one or more of the following: walking on a flat surface, going up/down stairs, at night, sitting, lying, or standing upright.
The mean age of patients was 61 years, and 51% were men. More than half of the study participants (63%) had radiographic osteoarthritis, and 85% fulfilled American College of Rheumatology criteria for the condition.
The Effects of Combination Tablets
After measuring the mean change in WOMAC pain scores from baseline, the researchers found that at day 10, two combination tablets provided significantly more pain relief, compared with paracetamol alone (P less than .01). At 13 weeks, a significantly greater proportion of participants taking one or two combination tablets rated their treatment as excellent/good, compared with paracetamol alone (P = .015 and .0002, respectively).
The incidence of adverse events was comparable among groups and consisted mainly of dyspepsia, diarrhea, and nausea. However, at 13 weeks a decrease in hemoglobin level by at least 1g/dL was observed among some participants in all treatment groups. More than two-thirds of patients taking two combination tablets experienced this decrease (38%), compared with 24% taking one combination tablet, 20% taking paracetamol monotherapy, and 20% taking ibuprofen monotherapy.
At 13 weeks, a significantly greater proportion of patients in the two combination tablet group experienced a decrease in hemoglobin level by 2 g/L or greater (6.9%), compared with their counterparts in the one combination tablet (1.8%), paracetamol (0.9%), and ibuprofen (0.9%) treatment groups.
Dr. Doherty and his associates acknowledged certain limitations of the study, including the fact that it lacked a placebo arm, "but withholding analgesia for a chronic painful condition raises ethical concerns," they wrote. "Other caveats included the fact that the study was not sufficiently powered to show benefit of the combination tablet over ibuprofen monotherapy, and the WOMAC scale (designed for osteoarthritis rather than knee pain) was used to determine efficacy. However, most participants fulfilled the criteria for osteoarthritis, and pain, stiffness and restricted activity are important patient-centered domains irrespective of confirmed osteoarthritis."
The study was sponsored by Reckitt Benckiser Healthcare International Ltd. Dr. Doherty disclosed that he has received honoraria for attending two advisory boards for Reckitt Benckiser. In addition, one of the study authors is currently employed by the company and two others are former employees.
This cautious and excellent long-term study reveals many new and important findings that should be the basis for reconsidering treatment of musculoskeletal conditions with OTC analgesics. It may turn out that many of our widely held beliefs are wrong and that recommendations for our patients need to be changed.
The results indicate that we should reconsider the use of a combination of analgesics and also the use of paracetamol alone, as it is not sufficiently effective yet causes many unwanted effects including dyspepsia, diarrhea, and GI blood loss. In line with this notion, studies published during the past few years have shown that paracetamol increases blood pressure when taken for short or prolonged periods and augments the risk of major cardiovascular events when administered at high frequency or dose.
Moreover, there is no mechanistic justification for the combination of paracetamol with another cyclooxygenase-2 inhibitor: The enzyme responsible for the formation of algesic prostaglandin E2 can only be blocked once. Two blockers cannot achieve more effects than one blocker! The analgesic action increases only marginally (if at all), but the unwanted drug effects increase substantially.
On the basis of this study, one wonders why combinations of analgesics of the type described and investigated here should remain on the OTC market. Obviously, there is no scientific evidence that either claim (higher efficacy and/or less toxicity) can be substantiated; rather, the contrary is true.
Kay Brune, M.D., is with the department of experimental and clinical pharmacology and toxicology at Friedrich-Alexander-University of Erlangen-Nuremberg (Germany). Burkhard Hinz, Ph.D., is with the Institute of Toxicology and Pharmacology at the University of Rostock (Germany). This was adapted from an editorial that accompanied the study (Ann. Rheum. Dis. 2011;70:1521-2).
This cautious and excellent long-term study reveals many new and important findings that should be the basis for reconsidering treatment of musculoskeletal conditions with OTC analgesics. It may turn out that many of our widely held beliefs are wrong and that recommendations for our patients need to be changed.
The results indicate that we should reconsider the use of a combination of analgesics and also the use of paracetamol alone, as it is not sufficiently effective yet causes many unwanted effects including dyspepsia, diarrhea, and GI blood loss. In line with this notion, studies published during the past few years have shown that paracetamol increases blood pressure when taken for short or prolonged periods and augments the risk of major cardiovascular events when administered at high frequency or dose.
Moreover, there is no mechanistic justification for the combination of paracetamol with another cyclooxygenase-2 inhibitor: The enzyme responsible for the formation of algesic prostaglandin E2 can only be blocked once. Two blockers cannot achieve more effects than one blocker! The analgesic action increases only marginally (if at all), but the unwanted drug effects increase substantially.
On the basis of this study, one wonders why combinations of analgesics of the type described and investigated here should remain on the OTC market. Obviously, there is no scientific evidence that either claim (higher efficacy and/or less toxicity) can be substantiated; rather, the contrary is true.
Kay Brune, M.D., is with the department of experimental and clinical pharmacology and toxicology at Friedrich-Alexander-University of Erlangen-Nuremberg (Germany). Burkhard Hinz, Ph.D., is with the Institute of Toxicology and Pharmacology at the University of Rostock (Germany). This was adapted from an editorial that accompanied the study (Ann. Rheum. Dis. 2011;70:1521-2).
This cautious and excellent long-term study reveals many new and important findings that should be the basis for reconsidering treatment of musculoskeletal conditions with OTC analgesics. It may turn out that many of our widely held beliefs are wrong and that recommendations for our patients need to be changed.
The results indicate that we should reconsider the use of a combination of analgesics and also the use of paracetamol alone, as it is not sufficiently effective yet causes many unwanted effects including dyspepsia, diarrhea, and GI blood loss. In line with this notion, studies published during the past few years have shown that paracetamol increases blood pressure when taken for short or prolonged periods and augments the risk of major cardiovascular events when administered at high frequency or dose.
Moreover, there is no mechanistic justification for the combination of paracetamol with another cyclooxygenase-2 inhibitor: The enzyme responsible for the formation of algesic prostaglandin E2 can only be blocked once. Two blockers cannot achieve more effects than one blocker! The analgesic action increases only marginally (if at all), but the unwanted drug effects increase substantially.
On the basis of this study, one wonders why combinations of analgesics of the type described and investigated here should remain on the OTC market. Obviously, there is no scientific evidence that either claim (higher efficacy and/or less toxicity) can be substantiated; rather, the contrary is true.
Kay Brune, M.D., is with the department of experimental and clinical pharmacology and toxicology at Friedrich-Alexander-University of Erlangen-Nuremberg (Germany). Burkhard Hinz, Ph.D., is with the Institute of Toxicology and Pharmacology at the University of Rostock (Germany). This was adapted from an editorial that accompanied the study (Ann. Rheum. Dis. 2011;70:1521-2).
Combining ibuprofen and paracetamol at nonprescription doses conferred a modest improvement in pain relief in adults with knee pain/osteoarthritis. But this gain came at the expense of an increase in presumed gastrointestinal bleeding, results from a large randomized, controlled trial demonstrated.
The trial, published in the September 2011 edition of the Annals of Rheumatic Diseases, found that paracetamol 3 g/day may cause similar levels of blood loss as ibuprofen 1,200 mg/day, and that the combination of the two appears to be additive or even synergistic in terms of the number of individuals with a decrease in hemoglobin greater than 2 g/dL.
"These results need to be confirmed, along with their clinical relevance and identification of the site of gastrointestinal bleeding," wrote the researchers, who were led by Dr. Michael Doherty of the Arthritis UK Pain Center at Nottingham (England) City Hospital. "If confirmed, this observation should lead to the reconsideration of current recommendations for oral analgesic use in osteoarthritis and in chronic pain in general, and to the consideration of strategies to reduce this side effect."
Over a period of 13 weeks, Dr. Doherty and his associates followed 892 adults with chronic knee pain who were randomized to one of four treatment regimens, each taken three times a day: ibuprofen (400 mg), paracetamol (1,000 mg), one fixed-dose combination tablet (ibuprofen 200 mg/paracetamol 500 mg), or two fixed-dose combination tablets (ibuprofen 400 mg/paracetamol 1,000 mg).
The primary short-term efficacy end point was the difference at 10 days between groups in the WOMAC (Western Ontario McMaster Universities) osteoarthritis index pain subscale, which was normalized to a 0- to 100-mm scale.
The primary long-term efficacy end point was the patient global assessment of study medication after 13 weeks. This was determined by asking patients, "Taking into account both how your medicine worked for you and any side effects you think it caused you, how would you rate your medication as a treatment for your painful knee?" Respondents used a 5-point scale for replies (1, excellent; 2, good; 3, fair; 4, poor; 5, unacceptable).
The primary safety end point was the incidence of moderate and severe adverse events reported during the study period (Ann. Rheum. Dis. 2011;70:1534-41).
Criteria for inclusion were age of at least 40 years; knee pain for most of the past 3 months and on 4 of 7 preceding days; discontinuation of current analgesics; Steinbrocker functional capacity class I-III; and pain affecting the index knee (after a washout period if currently taking analgesics) of 30 mm or greater and 80 mm or less on a 100-mm visual analog scale over the previous 48 hours for one or more of the following: walking on a flat surface, going up/down stairs, at night, sitting, lying, or standing upright.
The mean age of patients was 61 years, and 51% were men. More than half of the study participants (63%) had radiographic osteoarthritis, and 85% fulfilled American College of Rheumatology criteria for the condition.
The Effects of Combination Tablets
After measuring the mean change in WOMAC pain scores from baseline, the researchers found that at day 10, two combination tablets provided significantly more pain relief, compared with paracetamol alone (P less than .01). At 13 weeks, a significantly greater proportion of participants taking one or two combination tablets rated their treatment as excellent/good, compared with paracetamol alone (P = .015 and .0002, respectively).
The incidence of adverse events was comparable among groups and consisted mainly of dyspepsia, diarrhea, and nausea. However, at 13 weeks a decrease in hemoglobin level by at least 1g/dL was observed among some participants in all treatment groups. More than two-thirds of patients taking two combination tablets experienced this decrease (38%), compared with 24% taking one combination tablet, 20% taking paracetamol monotherapy, and 20% taking ibuprofen monotherapy.
At 13 weeks, a significantly greater proportion of patients in the two combination tablet group experienced a decrease in hemoglobin level by 2 g/L or greater (6.9%), compared with their counterparts in the one combination tablet (1.8%), paracetamol (0.9%), and ibuprofen (0.9%) treatment groups.
Dr. Doherty and his associates acknowledged certain limitations of the study, including the fact that it lacked a placebo arm, "but withholding analgesia for a chronic painful condition raises ethical concerns," they wrote. "Other caveats included the fact that the study was not sufficiently powered to show benefit of the combination tablet over ibuprofen monotherapy, and the WOMAC scale (designed for osteoarthritis rather than knee pain) was used to determine efficacy. However, most participants fulfilled the criteria for osteoarthritis, and pain, stiffness and restricted activity are important patient-centered domains irrespective of confirmed osteoarthritis."
The study was sponsored by Reckitt Benckiser Healthcare International Ltd. Dr. Doherty disclosed that he has received honoraria for attending two advisory boards for Reckitt Benckiser. In addition, one of the study authors is currently employed by the company and two others are former employees.
Combining ibuprofen and paracetamol at nonprescription doses conferred a modest improvement in pain relief in adults with knee pain/osteoarthritis. But this gain came at the expense of an increase in presumed gastrointestinal bleeding, results from a large randomized, controlled trial demonstrated.
The trial, published in the September 2011 edition of the Annals of Rheumatic Diseases, found that paracetamol 3 g/day may cause similar levels of blood loss as ibuprofen 1,200 mg/day, and that the combination of the two appears to be additive or even synergistic in terms of the number of individuals with a decrease in hemoglobin greater than 2 g/dL.
"These results need to be confirmed, along with their clinical relevance and identification of the site of gastrointestinal bleeding," wrote the researchers, who were led by Dr. Michael Doherty of the Arthritis UK Pain Center at Nottingham (England) City Hospital. "If confirmed, this observation should lead to the reconsideration of current recommendations for oral analgesic use in osteoarthritis and in chronic pain in general, and to the consideration of strategies to reduce this side effect."
Over a period of 13 weeks, Dr. Doherty and his associates followed 892 adults with chronic knee pain who were randomized to one of four treatment regimens, each taken three times a day: ibuprofen (400 mg), paracetamol (1,000 mg), one fixed-dose combination tablet (ibuprofen 200 mg/paracetamol 500 mg), or two fixed-dose combination tablets (ibuprofen 400 mg/paracetamol 1,000 mg).
The primary short-term efficacy end point was the difference at 10 days between groups in the WOMAC (Western Ontario McMaster Universities) osteoarthritis index pain subscale, which was normalized to a 0- to 100-mm scale.
The primary long-term efficacy end point was the patient global assessment of study medication after 13 weeks. This was determined by asking patients, "Taking into account both how your medicine worked for you and any side effects you think it caused you, how would you rate your medication as a treatment for your painful knee?" Respondents used a 5-point scale for replies (1, excellent; 2, good; 3, fair; 4, poor; 5, unacceptable).
The primary safety end point was the incidence of moderate and severe adverse events reported during the study period (Ann. Rheum. Dis. 2011;70:1534-41).
Criteria for inclusion were age of at least 40 years; knee pain for most of the past 3 months and on 4 of 7 preceding days; discontinuation of current analgesics; Steinbrocker functional capacity class I-III; and pain affecting the index knee (after a washout period if currently taking analgesics) of 30 mm or greater and 80 mm or less on a 100-mm visual analog scale over the previous 48 hours for one or more of the following: walking on a flat surface, going up/down stairs, at night, sitting, lying, or standing upright.
The mean age of patients was 61 years, and 51% were men. More than half of the study participants (63%) had radiographic osteoarthritis, and 85% fulfilled American College of Rheumatology criteria for the condition.
The Effects of Combination Tablets
After measuring the mean change in WOMAC pain scores from baseline, the researchers found that at day 10, two combination tablets provided significantly more pain relief, compared with paracetamol alone (P less than .01). At 13 weeks, a significantly greater proportion of participants taking one or two combination tablets rated their treatment as excellent/good, compared with paracetamol alone (P = .015 and .0002, respectively).
The incidence of adverse events was comparable among groups and consisted mainly of dyspepsia, diarrhea, and nausea. However, at 13 weeks a decrease in hemoglobin level by at least 1g/dL was observed among some participants in all treatment groups. More than two-thirds of patients taking two combination tablets experienced this decrease (38%), compared with 24% taking one combination tablet, 20% taking paracetamol monotherapy, and 20% taking ibuprofen monotherapy.
At 13 weeks, a significantly greater proportion of patients in the two combination tablet group experienced a decrease in hemoglobin level by 2 g/L or greater (6.9%), compared with their counterparts in the one combination tablet (1.8%), paracetamol (0.9%), and ibuprofen (0.9%) treatment groups.
Dr. Doherty and his associates acknowledged certain limitations of the study, including the fact that it lacked a placebo arm, "but withholding analgesia for a chronic painful condition raises ethical concerns," they wrote. "Other caveats included the fact that the study was not sufficiently powered to show benefit of the combination tablet over ibuprofen monotherapy, and the WOMAC scale (designed for osteoarthritis rather than knee pain) was used to determine efficacy. However, most participants fulfilled the criteria for osteoarthritis, and pain, stiffness and restricted activity are important patient-centered domains irrespective of confirmed osteoarthritis."
The study was sponsored by Reckitt Benckiser Healthcare International Ltd. Dr. Doherty disclosed that he has received honoraria for attending two advisory boards for Reckitt Benckiser. In addition, one of the study authors is currently employed by the company and two others are former employees.
FROM THE ANNALS OF RHEUMATIC DISEASES
Major Finding: Combining ibuprofen and paracetamol at nonprescription doses conferred a modest improvement in pain relief after 10 days in adults with knee pain/osteoarthritis (P less than .01), but at the expense of an increase in presumed GI bleeding at 13 weeks.
Data Source: A study of 892 adults with chronic knee pain who were randomized to one of four treatment regimens, each taken three times a day.
Disclosures: The study was sponsored by Reckitt Benckiser Healthcare International Ltd. Dr. Doherty disclosed that he has received honoraria for attending two advisory boards for Reckitt Benckiser. In addition, one of the study authors is currently employed by the company and two others are former employees.
Rheums, Patients Shift Views on CAM
Dr. Daniel Muller used to teach a class on complementary and alternative medicine at the University of Wisconsin, Madison, but he hasn’t offered it in 2 years. The once-popular elective just wasn’t attracting students.
But today’s medical students don’t see complementary and alternative medicine (CAM) as being out of the mainstream, said Dr. Muller, an associate professor of rheumatology at the university. "They know all about this stuff."
Dr. Muller has literally written the book on CAM in rheumatology. He is the author of "Integrative Rheumatology," which explains how lifestyle interventions and mind-body approaches can fill gaps where traditional therapies fall short. Acceptance of CAM is generally more widespread among younger physicians, he said. Some of them may be elite athletes who have used energy medicine, some suffer from chronic pain and have explored CAM for that reason, and others may be the children of hippies who grew up surrounded by unconventional ideas, Dr. Muller said.

And increasingly, practicing rheumatologists have a positive opinion of CAM approaches, at least according to a survey conducted in 2007 (BMC. Complement. Altern. Med. 2010;10:5). The poll of 345 rheumatologists under age 65 years found that physicians seemed very comfortable recommending certain forms of CAM. For instance, 70% of respondents said they considered body work like massage to be very beneficial or moderately beneficial. And 65% would be very or somewhat likely to recommend it to their patients. Other CAM approaches that were rated highly by physicians include meditation practices and acupuncture.
But rheumatologists who responded to the survey did not have favorable opinions about energy medicine practices like Reiki. Only 11% said energy medicine was beneficial, and only 10% would recommend it to patients. In other areas, such as the use of glucosamine and chondroitin, the findings were mixed. Less than 40% of rheumatologists found the supplements to be beneficial, but 57% would be likely to recommend their use anyway.
Accepting Complementary and Alternative Medicine
The findings generally show a widespread acceptance of CAM, said Dr. Nisha Manek, with the rheumatology department at the Mayo Clinic in Rochester, Minn., and the lead author of the study. Dr. Manek said the figures show that doctors aren’t just approving of these approaches, but they are also willing to give them their stamp of approval with patients.
"It’s one thing to believe in the benefits of a therapy; it’s quite another to recommend it to patients," she said.
Dr. Manek speculated that in the 4 years since the survey was conducted, rheumatologists’ views have likely grown warmer toward CAM. One of the drivers is the enthusiasm among patients.
"Our patients are saying, ‘Look, I want to do better than a prescription. I really want to take charge of my health,’ " she said. "I think complementary therapies are potentially a very powerful driver in preventive medicine."
Dr. Sharon L. Kolasinski, the interim division director of rheumatology at the University of Pennsylvania, Philadelphia, agrees that patients are driving not just the popularity of CAM, but its transformation. For instance, over the last decade, interest in herbal medicines has waned in favor of a greater focus on mind-body and physical interventions. And these physical techniques are adjunctive to conventional treatment, not done as stand-alone therapy, she said.
Yoga, mindfulness meditation, acupuncture, and cognitive therapy are all practices in which patients can participate, she said, and that has helped to spur their popularity. "Patients don’t want to just take pills," said Dr. Kolasinski, who has conducted research on yoga for osteoarthritis management.
Patients are also drawn to the sensibility of some alternative medicine practitioners who take a whole patient approach, she said, as they like the focus on their daily functioning.
Talking to Rheumatology Patients
While the popularity of CAM is still going strong, especially among rheumatology patients with chronic pain, many physicians continue to struggle with how to discuss CAM with their patients. The biggest problem seems to be how to find out what patients are doing besides taking their traditional medications, whether it’s taking dietary supplements or attending a yoga class.
A recent survey conducted by the National Center for Complimentary and Alternative Medicine (NCCAM), part of the National Institutes of Health, and the AARP found that people age 50 years and older don’t talk to their doctors about using CAM. The telephone survey of more than 1,000 people found that while 53% of respondents had used CAM at some point, only about 42% had discussed it with their health care provider. The major reasons respondents gave for not talking about it with their doctors was that their physician never asks and they didn’t know they should bring it up.
NCCAM is trying to address that problem with its "Time to Talk" campaign. It encourages physicians to start a conversation about CAM and includes tips for how find time to address it during a brief office visit.
Dr. Josephine Briggs, the NCCAM director, suggests that physicians begin the conversation by asking, "What are you trying to do to be healthy?" Physicians need to recognize that even if they have doubts about a certain CAM modality, patients are generally turning to CAM as a way to be healthy or to help better manage their symptoms, she said. "I think being open to that dialogue and making it a thoughtful one is the way all of us can best help our patients."
She also encouraged physicians to talk to their patients about how they manage pain, since this is often what drives the use of CAM. Ask patients what helps them relieve their pain outside of traditional medications, she suggested, and if they have tried alternative approaches just as relaxation techniques.
Another problem for physicians in talking about CAM is that they may not be familiar with the evidence around a particular CAM treatment. NCCAM is also trying to tackle that. As part of "Time to Talk," they have put together a list of reliable sources on the latest CAM research. And NCCAM is funding a wide portfolio of research on CAM modalities that could potentially be used to treat musculoskeletal conditions, such as tai chi and yoga in the management of fibromyalgia, back pain, and osteoarthritis of the knee.
"I see these as very promising adjuncts for certain patients," Dr. Briggs said. "The question partly is, ‘Is the patient motivated?’ "
NCCAM is also sponsoring studies on dietary supplements. For example, NCCAM funded a large investigation of glucosamine and chondroitin sulfate to treat pain associated with osteoarthritis of the knee in the Glucosamine /Chondroitin Arthritis Intervention Trial (GAIT). The results, which were originally published in 2006, showed that the combination did not provide significant relief from pain. In addition, a number of NCCAM-funded researchers are studying herb-drug interactions to see how over-the-counter dietary supplements could affect traditional treatments for chronic disease.
Dr. Muller, Dr. Briggs, Dr. Kolasinski, and Dr. Manek had no financial conflicts of interest to disclose.
Dr. Daniel Muller used to teach a class on complementary and alternative medicine at the University of Wisconsin, Madison, but he hasn’t offered it in 2 years. The once-popular elective just wasn’t attracting students.
But today’s medical students don’t see complementary and alternative medicine (CAM) as being out of the mainstream, said Dr. Muller, an associate professor of rheumatology at the university. "They know all about this stuff."
Dr. Muller has literally written the book on CAM in rheumatology. He is the author of "Integrative Rheumatology," which explains how lifestyle interventions and mind-body approaches can fill gaps where traditional therapies fall short. Acceptance of CAM is generally more widespread among younger physicians, he said. Some of them may be elite athletes who have used energy medicine, some suffer from chronic pain and have explored CAM for that reason, and others may be the children of hippies who grew up surrounded by unconventional ideas, Dr. Muller said.
And increasingly, practicing rheumatologists have a positive opinion of CAM approaches, at least according to a survey conducted in 2007 (BMC. Complement. Altern. Med. 2010;10:5). The poll of 345 rheumatologists under age 65 years found that physicians seemed very comfortable recommending certain forms of CAM. For instance, 70% of respondents said they considered body work like massage to be very beneficial or moderately beneficial. And 65% would be very or somewhat likely to recommend it to their patients. Other CAM approaches that were rated highly by physicians include meditation practices and acupuncture.
But rheumatologists who responded to the survey did not have favorable opinions about energy medicine practices like Reiki. Only 11% said energy medicine was beneficial, and only 10% would recommend it to patients. In other areas, such as the use of glucosamine and chondroitin, the findings were mixed. Less than 40% of rheumatologists found the supplements to be beneficial, but 57% would be likely to recommend their use anyway.
Accepting Complementary and Alternative Medicine
The findings generally show a widespread acceptance of CAM, said Dr. Nisha Manek, with the rheumatology department at the Mayo Clinic in Rochester, Minn., and the lead author of the study. Dr. Manek said the figures show that doctors aren’t just approving of these approaches, but they are also willing to give them their stamp of approval with patients.
"It’s one thing to believe in the benefits of a therapy; it’s quite another to recommend it to patients," she said.
Dr. Manek speculated that in the 4 years since the survey was conducted, rheumatologists’ views have likely grown warmer toward CAM. One of the drivers is the enthusiasm among patients.
"Our patients are saying, ‘Look, I want to do better than a prescription. I really want to take charge of my health,’ " she said. "I think complementary therapies are potentially a very powerful driver in preventive medicine."
Dr. Sharon L. Kolasinski, the interim division director of rheumatology at the University of Pennsylvania, Philadelphia, agrees that patients are driving not just the popularity of CAM, but its transformation. For instance, over the last decade, interest in herbal medicines has waned in favor of a greater focus on mind-body and physical interventions. And these physical techniques are adjunctive to conventional treatment, not done as stand-alone therapy, she said.
Yoga, mindfulness meditation, acupuncture, and cognitive therapy are all practices in which patients can participate, she said, and that has helped to spur their popularity. "Patients don’t want to just take pills," said Dr. Kolasinski, who has conducted research on yoga for osteoarthritis management.
Patients are also drawn to the sensibility of some alternative medicine practitioners who take a whole patient approach, she said, as they like the focus on their daily functioning.
Talking to Rheumatology Patients
While the popularity of CAM is still going strong, especially among rheumatology patients with chronic pain, many physicians continue to struggle with how to discuss CAM with their patients. The biggest problem seems to be how to find out what patients are doing besides taking their traditional medications, whether it’s taking dietary supplements or attending a yoga class.
A recent survey conducted by the National Center for Complimentary and Alternative Medicine (NCCAM), part of the National Institutes of Health, and the AARP found that people age 50 years and older don’t talk to their doctors about using CAM. The telephone survey of more than 1,000 people found that while 53% of respondents had used CAM at some point, only about 42% had discussed it with their health care provider. The major reasons respondents gave for not talking about it with their doctors was that their physician never asks and they didn’t know they should bring it up.
NCCAM is trying to address that problem with its "Time to Talk" campaign. It encourages physicians to start a conversation about CAM and includes tips for how find time to address it during a brief office visit.
Dr. Josephine Briggs, the NCCAM director, suggests that physicians begin the conversation by asking, "What are you trying to do to be healthy?" Physicians need to recognize that even if they have doubts about a certain CAM modality, patients are generally turning to CAM as a way to be healthy or to help better manage their symptoms, she said. "I think being open to that dialogue and making it a thoughtful one is the way all of us can best help our patients."
She also encouraged physicians to talk to their patients about how they manage pain, since this is often what drives the use of CAM. Ask patients what helps them relieve their pain outside of traditional medications, she suggested, and if they have tried alternative approaches just as relaxation techniques.
Another problem for physicians in talking about CAM is that they may not be familiar with the evidence around a particular CAM treatment. NCCAM is also trying to tackle that. As part of "Time to Talk," they have put together a list of reliable sources on the latest CAM research. And NCCAM is funding a wide portfolio of research on CAM modalities that could potentially be used to treat musculoskeletal conditions, such as tai chi and yoga in the management of fibromyalgia, back pain, and osteoarthritis of the knee.
"I see these as very promising adjuncts for certain patients," Dr. Briggs said. "The question partly is, ‘Is the patient motivated?’ "
NCCAM is also sponsoring studies on dietary supplements. For example, NCCAM funded a large investigation of glucosamine and chondroitin sulfate to treat pain associated with osteoarthritis of the knee in the Glucosamine /Chondroitin Arthritis Intervention Trial (GAIT). The results, which were originally published in 2006, showed that the combination did not provide significant relief from pain. In addition, a number of NCCAM-funded researchers are studying herb-drug interactions to see how over-the-counter dietary supplements could affect traditional treatments for chronic disease.
Dr. Muller, Dr. Briggs, Dr. Kolasinski, and Dr. Manek had no financial conflicts of interest to disclose.
Dr. Daniel Muller used to teach a class on complementary and alternative medicine at the University of Wisconsin, Madison, but he hasn’t offered it in 2 years. The once-popular elective just wasn’t attracting students.
But today’s medical students don’t see complementary and alternative medicine (CAM) as being out of the mainstream, said Dr. Muller, an associate professor of rheumatology at the university. "They know all about this stuff."
Dr. Muller has literally written the book on CAM in rheumatology. He is the author of "Integrative Rheumatology," which explains how lifestyle interventions and mind-body approaches can fill gaps where traditional therapies fall short. Acceptance of CAM is generally more widespread among younger physicians, he said. Some of them may be elite athletes who have used energy medicine, some suffer from chronic pain and have explored CAM for that reason, and others may be the children of hippies who grew up surrounded by unconventional ideas, Dr. Muller said.
And increasingly, practicing rheumatologists have a positive opinion of CAM approaches, at least according to a survey conducted in 2007 (BMC. Complement. Altern. Med. 2010;10:5). The poll of 345 rheumatologists under age 65 years found that physicians seemed very comfortable recommending certain forms of CAM. For instance, 70% of respondents said they considered body work like massage to be very beneficial or moderately beneficial. And 65% would be very or somewhat likely to recommend it to their patients. Other CAM approaches that were rated highly by physicians include meditation practices and acupuncture.
But rheumatologists who responded to the survey did not have favorable opinions about energy medicine practices like Reiki. Only 11% said energy medicine was beneficial, and only 10% would recommend it to patients. In other areas, such as the use of glucosamine and chondroitin, the findings were mixed. Less than 40% of rheumatologists found the supplements to be beneficial, but 57% would be likely to recommend their use anyway.
Accepting Complementary and Alternative Medicine
The findings generally show a widespread acceptance of CAM, said Dr. Nisha Manek, with the rheumatology department at the Mayo Clinic in Rochester, Minn., and the lead author of the study. Dr. Manek said the figures show that doctors aren’t just approving of these approaches, but they are also willing to give them their stamp of approval with patients.
"It’s one thing to believe in the benefits of a therapy; it’s quite another to recommend it to patients," she said.
Dr. Manek speculated that in the 4 years since the survey was conducted, rheumatologists’ views have likely grown warmer toward CAM. One of the drivers is the enthusiasm among patients.
"Our patients are saying, ‘Look, I want to do better than a prescription. I really want to take charge of my health,’ " she said. "I think complementary therapies are potentially a very powerful driver in preventive medicine."
Dr. Sharon L. Kolasinski, the interim division director of rheumatology at the University of Pennsylvania, Philadelphia, agrees that patients are driving not just the popularity of CAM, but its transformation. For instance, over the last decade, interest in herbal medicines has waned in favor of a greater focus on mind-body and physical interventions. And these physical techniques are adjunctive to conventional treatment, not done as stand-alone therapy, she said.
Yoga, mindfulness meditation, acupuncture, and cognitive therapy are all practices in which patients can participate, she said, and that has helped to spur their popularity. "Patients don’t want to just take pills," said Dr. Kolasinski, who has conducted research on yoga for osteoarthritis management.
Patients are also drawn to the sensibility of some alternative medicine practitioners who take a whole patient approach, she said, as they like the focus on their daily functioning.
Talking to Rheumatology Patients
While the popularity of CAM is still going strong, especially among rheumatology patients with chronic pain, many physicians continue to struggle with how to discuss CAM with their patients. The biggest problem seems to be how to find out what patients are doing besides taking their traditional medications, whether it’s taking dietary supplements or attending a yoga class.
A recent survey conducted by the National Center for Complimentary and Alternative Medicine (NCCAM), part of the National Institutes of Health, and the AARP found that people age 50 years and older don’t talk to their doctors about using CAM. The telephone survey of more than 1,000 people found that while 53% of respondents had used CAM at some point, only about 42% had discussed it with their health care provider. The major reasons respondents gave for not talking about it with their doctors was that their physician never asks and they didn’t know they should bring it up.
NCCAM is trying to address that problem with its "Time to Talk" campaign. It encourages physicians to start a conversation about CAM and includes tips for how find time to address it during a brief office visit.
Dr. Josephine Briggs, the NCCAM director, suggests that physicians begin the conversation by asking, "What are you trying to do to be healthy?" Physicians need to recognize that even if they have doubts about a certain CAM modality, patients are generally turning to CAM as a way to be healthy or to help better manage their symptoms, she said. "I think being open to that dialogue and making it a thoughtful one is the way all of us can best help our patients."
She also encouraged physicians to talk to their patients about how they manage pain, since this is often what drives the use of CAM. Ask patients what helps them relieve their pain outside of traditional medications, she suggested, and if they have tried alternative approaches just as relaxation techniques.
Another problem for physicians in talking about CAM is that they may not be familiar with the evidence around a particular CAM treatment. NCCAM is also trying to tackle that. As part of "Time to Talk," they have put together a list of reliable sources on the latest CAM research. And NCCAM is funding a wide portfolio of research on CAM modalities that could potentially be used to treat musculoskeletal conditions, such as tai chi and yoga in the management of fibromyalgia, back pain, and osteoarthritis of the knee.
"I see these as very promising adjuncts for certain patients," Dr. Briggs said. "The question partly is, ‘Is the patient motivated?’ "
NCCAM is also sponsoring studies on dietary supplements. For example, NCCAM funded a large investigation of glucosamine and chondroitin sulfate to treat pain associated with osteoarthritis of the knee in the Glucosamine /Chondroitin Arthritis Intervention Trial (GAIT). The results, which were originally published in 2006, showed that the combination did not provide significant relief from pain. In addition, a number of NCCAM-funded researchers are studying herb-drug interactions to see how over-the-counter dietary supplements could affect traditional treatments for chronic disease.
Dr. Muller, Dr. Briggs, Dr. Kolasinski, and Dr. Manek had no financial conflicts of interest to disclose.
Joint Distraction May Delay Need for Knee Replacement
Joint distraction can induce tissue structure modification in knee osteoarthritis, possibly reversing structural damage to cartilage tissue and delaying the need for knee replacement surgery. This is according to results of an open 1-year pilot study reported in the August issue of Annals of the Rheumatic Diseases.
Endoprosthesis currently is the accepted method for treating pain caused by end-stage knee OA. However, the growing number of procedures carries a high price tag, and there is a higher risk of failure in patients aged younger than 65 years.
With that in mind, Dr. Femke Intema of the University Medical Center Utrecht (the Netherlands) and colleagues wanted to determine whether joint distraction could halt and possibly reverse joint degeneration in knee OA (Ann. Rheum. Dis. 2011;70:1441-6).

The study included 11 men and 9 women who had knee OA and in whom knee replacement surgery was indicated in 2006-2008. Patients were an average of 48 years old; 18 of them had predominant OA in the medial compartment; the remaining two had OA in the lateral compartment. Patients had a score of 60 mm or higher on the Visual Analogue Scale (VAS) of pain, as well as radiographic signs of joint damage, and primarily tibiofemoral OA.
Joint distraction was applied for 2 months via an external fixation frame. At the 1-year follow-up, researchers evaluated tissue structure modification according to the following:
• Radiographic analysis. This showed that the mean joint space width (JSW) of the most affected compartment increased from 2.7 mm to 3.6 mm between baseline and 12 months, whereas the minimum JSW increased from 1 mm to 1.9 mm.
• Quantitative MRI analysis. At 1 year, this showed an increase in the mean thickness of cartilage over total area of bone (ThCtAB) from 2.4 mm to 3 mm in the most affected compartment, and a decrease in mean percentage area of denuded bone (dABp) from 22% to 5%. The thickness of cartilage over area of bone covered with cartilage (ThCcAB), a secondary structural outcome parameter, showed a borderline increase from 2.9 mm to 3.1 mm.
• Biomarker analysis on serum and urine samples. These showed an 11% decrease of CTXII (a collagen type II breakdown marker), and a 103% increase in PILANP/CTXII (a collage type II synthesis marker), between 6 and 12 months. These findings suggest a net increase in collagen synthesis, the researchers said.
The primary outcome parameter of this study was the WOMAC (Western Ontario and McMaster Universities) osteoarthritis index questionnaire, which decreased from 55 points at baseline to 23 points at 1 year. In all, 18 of the 20 patients showed a greater-than-10% improvement, and 16 showed a greater-than-25% improvement. There were significant improvements in the individual components of the WOMAC index, namely pain, stiffness, and function.
One secondary measure, the VAS pain score, decreased from 73 mm at baseline to 31 mm at 1 year. Physical examination of the joint, which assessed crepitus, pain on palpation, pain with flexion, and joint effusion, showed improvement from 46% to 75%.
"This study is the first to demonstrate intrinsic tissue structure repair in OA," the researchers said. "Historically, the regenerative capacity of cartilage has been questioned owing to the slow turnover rate of cartilage matrix, especially of collagen. However, this study shows that a significant amount of cartilage tissue is formed within 1 year after the distraction, demonstrating that under certain conditions, cartilage has regenerative capacity."
There is uncertainty as to the underlying mechanism of the structural repair that was seen in this study. One possibility is that temporary distraction prevents mechanical stress on the cartilage, eliminates further wear and tear, and allows tissue repair to begin, the researchers said.
For now, the researchers are unsure which patients may benefit from this procedure, as the study included only those patients who were younger than 50 years, had severe OA, and were likely candidates for joint replacement surgery. Referrals from peripheral hospitals may have led to selection bias, the researchers say.
Safety concerns exist as well. Two patients developed lung emboli and required hospitalization and anticoagulative treatment. Also, 17 patients developed single or multiple pin-tract infections, all of which were successfully treated with antibiotics.
Larger and longer trials in a variety of OA populations are needed to optimize treatment, to determine which patients would benefit the most and for the longest period of time, and to pay attention to reducing the number of complications, the researchers said.
The authors had no relationships to disclose. The Dutch Arthritis Foundation provided financial support for this study.
Joint distraction can induce tissue structure modification in knee osteoarthritis, possibly reversing structural damage to cartilage tissue and delaying the need for knee replacement surgery. This is according to results of an open 1-year pilot study reported in the August issue of Annals of the Rheumatic Diseases.
Endoprosthesis currently is the accepted method for treating pain caused by end-stage knee OA. However, the growing number of procedures carries a high price tag, and there is a higher risk of failure in patients aged younger than 65 years.
With that in mind, Dr. Femke Intema of the University Medical Center Utrecht (the Netherlands) and colleagues wanted to determine whether joint distraction could halt and possibly reverse joint degeneration in knee OA (Ann. Rheum. Dis. 2011;70:1441-6).
The study included 11 men and 9 women who had knee OA and in whom knee replacement surgery was indicated in 2006-2008. Patients were an average of 48 years old; 18 of them had predominant OA in the medial compartment; the remaining two had OA in the lateral compartment. Patients had a score of 60 mm or higher on the Visual Analogue Scale (VAS) of pain, as well as radiographic signs of joint damage, and primarily tibiofemoral OA.
Joint distraction was applied for 2 months via an external fixation frame. At the 1-year follow-up, researchers evaluated tissue structure modification according to the following:
• Radiographic analysis. This showed that the mean joint space width (JSW) of the most affected compartment increased from 2.7 mm to 3.6 mm between baseline and 12 months, whereas the minimum JSW increased from 1 mm to 1.9 mm.
• Quantitative MRI analysis. At 1 year, this showed an increase in the mean thickness of cartilage over total area of bone (ThCtAB) from 2.4 mm to 3 mm in the most affected compartment, and a decrease in mean percentage area of denuded bone (dABp) from 22% to 5%. The thickness of cartilage over area of bone covered with cartilage (ThCcAB), a secondary structural outcome parameter, showed a borderline increase from 2.9 mm to 3.1 mm.
• Biomarker analysis on serum and urine samples. These showed an 11% decrease of CTXII (a collagen type II breakdown marker), and a 103% increase in PILANP/CTXII (a collage type II synthesis marker), between 6 and 12 months. These findings suggest a net increase in collagen synthesis, the researchers said.
The primary outcome parameter of this study was the WOMAC (Western Ontario and McMaster Universities) osteoarthritis index questionnaire, which decreased from 55 points at baseline to 23 points at 1 year. In all, 18 of the 20 patients showed a greater-than-10% improvement, and 16 showed a greater-than-25% improvement. There were significant improvements in the individual components of the WOMAC index, namely pain, stiffness, and function.
One secondary measure, the VAS pain score, decreased from 73 mm at baseline to 31 mm at 1 year. Physical examination of the joint, which assessed crepitus, pain on palpation, pain with flexion, and joint effusion, showed improvement from 46% to 75%.
"This study is the first to demonstrate intrinsic tissue structure repair in OA," the researchers said. "Historically, the regenerative capacity of cartilage has been questioned owing to the slow turnover rate of cartilage matrix, especially of collagen. However, this study shows that a significant amount of cartilage tissue is formed within 1 year after the distraction, demonstrating that under certain conditions, cartilage has regenerative capacity."
There is uncertainty as to the underlying mechanism of the structural repair that was seen in this study. One possibility is that temporary distraction prevents mechanical stress on the cartilage, eliminates further wear and tear, and allows tissue repair to begin, the researchers said.
For now, the researchers are unsure which patients may benefit from this procedure, as the study included only those patients who were younger than 50 years, had severe OA, and were likely candidates for joint replacement surgery. Referrals from peripheral hospitals may have led to selection bias, the researchers say.
Safety concerns exist as well. Two patients developed lung emboli and required hospitalization and anticoagulative treatment. Also, 17 patients developed single or multiple pin-tract infections, all of which were successfully treated with antibiotics.
Larger and longer trials in a variety of OA populations are needed to optimize treatment, to determine which patients would benefit the most and for the longest period of time, and to pay attention to reducing the number of complications, the researchers said.
The authors had no relationships to disclose. The Dutch Arthritis Foundation provided financial support for this study.
Joint distraction can induce tissue structure modification in knee osteoarthritis, possibly reversing structural damage to cartilage tissue and delaying the need for knee replacement surgery. This is according to results of an open 1-year pilot study reported in the August issue of Annals of the Rheumatic Diseases.
Endoprosthesis currently is the accepted method for treating pain caused by end-stage knee OA. However, the growing number of procedures carries a high price tag, and there is a higher risk of failure in patients aged younger than 65 years.
With that in mind, Dr. Femke Intema of the University Medical Center Utrecht (the Netherlands) and colleagues wanted to determine whether joint distraction could halt and possibly reverse joint degeneration in knee OA (Ann. Rheum. Dis. 2011;70:1441-6).
The study included 11 men and 9 women who had knee OA and in whom knee replacement surgery was indicated in 2006-2008. Patients were an average of 48 years old; 18 of them had predominant OA in the medial compartment; the remaining two had OA in the lateral compartment. Patients had a score of 60 mm or higher on the Visual Analogue Scale (VAS) of pain, as well as radiographic signs of joint damage, and primarily tibiofemoral OA.
Joint distraction was applied for 2 months via an external fixation frame. At the 1-year follow-up, researchers evaluated tissue structure modification according to the following:
• Radiographic analysis. This showed that the mean joint space width (JSW) of the most affected compartment increased from 2.7 mm to 3.6 mm between baseline and 12 months, whereas the minimum JSW increased from 1 mm to 1.9 mm.
• Quantitative MRI analysis. At 1 year, this showed an increase in the mean thickness of cartilage over total area of bone (ThCtAB) from 2.4 mm to 3 mm in the most affected compartment, and a decrease in mean percentage area of denuded bone (dABp) from 22% to 5%. The thickness of cartilage over area of bone covered with cartilage (ThCcAB), a secondary structural outcome parameter, showed a borderline increase from 2.9 mm to 3.1 mm.
• Biomarker analysis on serum and urine samples. These showed an 11% decrease of CTXII (a collagen type II breakdown marker), and a 103% increase in PILANP/CTXII (a collage type II synthesis marker), between 6 and 12 months. These findings suggest a net increase in collagen synthesis, the researchers said.
The primary outcome parameter of this study was the WOMAC (Western Ontario and McMaster Universities) osteoarthritis index questionnaire, which decreased from 55 points at baseline to 23 points at 1 year. In all, 18 of the 20 patients showed a greater-than-10% improvement, and 16 showed a greater-than-25% improvement. There were significant improvements in the individual components of the WOMAC index, namely pain, stiffness, and function.
One secondary measure, the VAS pain score, decreased from 73 mm at baseline to 31 mm at 1 year. Physical examination of the joint, which assessed crepitus, pain on palpation, pain with flexion, and joint effusion, showed improvement from 46% to 75%.
"This study is the first to demonstrate intrinsic tissue structure repair in OA," the researchers said. "Historically, the regenerative capacity of cartilage has been questioned owing to the slow turnover rate of cartilage matrix, especially of collagen. However, this study shows that a significant amount of cartilage tissue is formed within 1 year after the distraction, demonstrating that under certain conditions, cartilage has regenerative capacity."
There is uncertainty as to the underlying mechanism of the structural repair that was seen in this study. One possibility is that temporary distraction prevents mechanical stress on the cartilage, eliminates further wear and tear, and allows tissue repair to begin, the researchers said.
For now, the researchers are unsure which patients may benefit from this procedure, as the study included only those patients who were younger than 50 years, had severe OA, and were likely candidates for joint replacement surgery. Referrals from peripheral hospitals may have led to selection bias, the researchers say.
Safety concerns exist as well. Two patients developed lung emboli and required hospitalization and anticoagulative treatment. Also, 17 patients developed single or multiple pin-tract infections, all of which were successfully treated with antibiotics.
Larger and longer trials in a variety of OA populations are needed to optimize treatment, to determine which patients would benefit the most and for the longest period of time, and to pay attention to reducing the number of complications, the researchers said.
The authors had no relationships to disclose. The Dutch Arthritis Foundation provided financial support for this study.
FROM ANNALS OF THE RHEUMATIC DISEASES
Major Finding: Joint distraction can induce tissue structure modification in knee osteoarthritis, as shown on radiography, MRI, and blood work, possibly delaying the need for endoprosthesis.
Data Source: An open, 1-year pilot study of 20 patients with tibiofemoral osteoarthritis who were treated surgically with joint distraction.
Disclosures: The authors had no relationships to disclose. The Dutch Arthritis Foundation provided financial support for this study.
Hereditary Hemochromatosis Linked to Increased Arthropathies and Joint Surgery
LONDON – Patients with hereditary hemochromatosis have a significantly increased prevalence of various arthropathies and an elevated need for joint-replacement surgery, compared with the general population, according to findings from a study of Swedish national registry data.
The analysis also showed that first-degree relatives of people with hereditary hemochromatosis do not have an increased rate of arthropathies or need for joint replacement, even though genetic models predict that a majority of these relatives carry one copy of an autosomal recessive mutation that causes hereditary hemochromatosis.
"This dissociation between the genotype and the phenotype" relative to the risk for arthropathy and need for joint replacement "suggests to me that the gene itself is not involved. It suggests to me that you need more than just the gene" to boost the risk for arthropathy and joint failure, noted Dr. Johan Askling.

Arthropathy is a classic phenotypic feature of patients with hereditary hemochromatosis, a genetic disease in people who carry two mutated copies of the hemochromatosis gene (HFE) associated with iron overload. But the nature of the relationship between the disease and arthropathies remains poorly understood. The new finding that increased arthropathies occur only in homozygous, affected individuals suggests that the risk is linked to iron overload itself, rather than to the causative mutated genes.
Dr. Askling and his associates identified 3,531 patients with a diagnosis of hereditary hemochromatosis from Swedish national records for the period 1999-2006. The investigators also identified another 11,794 first-degree relatives of these patients. They then identified 37,369 people as matched controls for the patients from the general Swedish population and 196,628 people as matched controls for the first-degree relatives.
The researchers then tallied the incidence of consultations or hospitalizations for rheumatoid arthritis, osteoarthritis, and other arthritides in the cases, their first-degree relatives, and the controls during the study period. They calculated a relative risk for these complications in affected people and in their relatives, compared with the controls that adjusted for differences in age, sex, and residence location. The researchers also ran similar analyses for the incidence of various joint-replacement surgeries (see table).
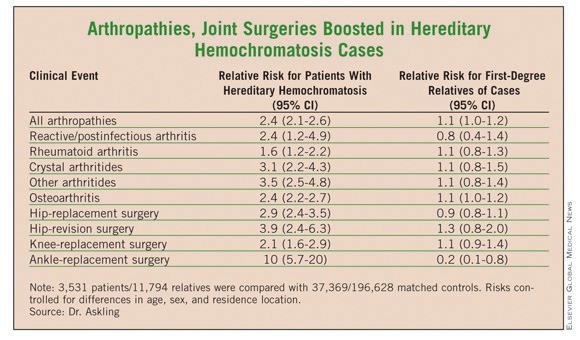
The results showed that the patients with hereditary hemochromatosis had consistent, statistically significant increased rates of arthropathies. For example, for all arthropathies the rate was 2.4-fold higher in the patients than in the controls. But this increased rate did not exist among the first-degree relatives. For all arthropathies, their rate was just 10% higher than among the matched controls, a difference that was not significant, reported Dr. Askling, an epidemiologist at the Karolinska Institute in Stockholm.
A similar pattern existed for joint-replacement surgeries. Hip surgery, for example, was 2.9-fold more frequent among the hereditary hemochromatosis patients than among their matched controls, while among the first-degree relatives the incidence of hip-replacement surgery was 10% less common than among the matched controls, a difference that was not statistically significant.
Dr. Askling said that he had no disclosures.
LONDON – Patients with hereditary hemochromatosis have a significantly increased prevalence of various arthropathies and an elevated need for joint-replacement surgery, compared with the general population, according to findings from a study of Swedish national registry data.
The analysis also showed that first-degree relatives of people with hereditary hemochromatosis do not have an increased rate of arthropathies or need for joint replacement, even though genetic models predict that a majority of these relatives carry one copy of an autosomal recessive mutation that causes hereditary hemochromatosis.
"This dissociation between the genotype and the phenotype" relative to the risk for arthropathy and need for joint replacement "suggests to me that the gene itself is not involved. It suggests to me that you need more than just the gene" to boost the risk for arthropathy and joint failure, noted Dr. Johan Askling.
Arthropathy is a classic phenotypic feature of patients with hereditary hemochromatosis, a genetic disease in people who carry two mutated copies of the hemochromatosis gene (HFE) associated with iron overload. But the nature of the relationship between the disease and arthropathies remains poorly understood. The new finding that increased arthropathies occur only in homozygous, affected individuals suggests that the risk is linked to iron overload itself, rather than to the causative mutated genes.
Dr. Askling and his associates identified 3,531 patients with a diagnosis of hereditary hemochromatosis from Swedish national records for the period 1999-2006. The investigators also identified another 11,794 first-degree relatives of these patients. They then identified 37,369 people as matched controls for the patients from the general Swedish population and 196,628 people as matched controls for the first-degree relatives.
The researchers then tallied the incidence of consultations or hospitalizations for rheumatoid arthritis, osteoarthritis, and other arthritides in the cases, their first-degree relatives, and the controls during the study period. They calculated a relative risk for these complications in affected people and in their relatives, compared with the controls that adjusted for differences in age, sex, and residence location. The researchers also ran similar analyses for the incidence of various joint-replacement surgeries (see table).
The results showed that the patients with hereditary hemochromatosis had consistent, statistically significant increased rates of arthropathies. For example, for all arthropathies the rate was 2.4-fold higher in the patients than in the controls. But this increased rate did not exist among the first-degree relatives. For all arthropathies, their rate was just 10% higher than among the matched controls, a difference that was not significant, reported Dr. Askling, an epidemiologist at the Karolinska Institute in Stockholm.
A similar pattern existed for joint-replacement surgeries. Hip surgery, for example, was 2.9-fold more frequent among the hereditary hemochromatosis patients than among their matched controls, while among the first-degree relatives the incidence of hip-replacement surgery was 10% less common than among the matched controls, a difference that was not statistically significant.
Dr. Askling said that he had no disclosures.
LONDON – Patients with hereditary hemochromatosis have a significantly increased prevalence of various arthropathies and an elevated need for joint-replacement surgery, compared with the general population, according to findings from a study of Swedish national registry data.
The analysis also showed that first-degree relatives of people with hereditary hemochromatosis do not have an increased rate of arthropathies or need for joint replacement, even though genetic models predict that a majority of these relatives carry one copy of an autosomal recessive mutation that causes hereditary hemochromatosis.
"This dissociation between the genotype and the phenotype" relative to the risk for arthropathy and need for joint replacement "suggests to me that the gene itself is not involved. It suggests to me that you need more than just the gene" to boost the risk for arthropathy and joint failure, noted Dr. Johan Askling.
Arthropathy is a classic phenotypic feature of patients with hereditary hemochromatosis, a genetic disease in people who carry two mutated copies of the hemochromatosis gene (HFE) associated with iron overload. But the nature of the relationship between the disease and arthropathies remains poorly understood. The new finding that increased arthropathies occur only in homozygous, affected individuals suggests that the risk is linked to iron overload itself, rather than to the causative mutated genes.
Dr. Askling and his associates identified 3,531 patients with a diagnosis of hereditary hemochromatosis from Swedish national records for the period 1999-2006. The investigators also identified another 11,794 first-degree relatives of these patients. They then identified 37,369 people as matched controls for the patients from the general Swedish population and 196,628 people as matched controls for the first-degree relatives.
The researchers then tallied the incidence of consultations or hospitalizations for rheumatoid arthritis, osteoarthritis, and other arthritides in the cases, their first-degree relatives, and the controls during the study period. They calculated a relative risk for these complications in affected people and in their relatives, compared with the controls that adjusted for differences in age, sex, and residence location. The researchers also ran similar analyses for the incidence of various joint-replacement surgeries (see table).
The results showed that the patients with hereditary hemochromatosis had consistent, statistically significant increased rates of arthropathies. For example, for all arthropathies the rate was 2.4-fold higher in the patients than in the controls. But this increased rate did not exist among the first-degree relatives. For all arthropathies, their rate was just 10% higher than among the matched controls, a difference that was not significant, reported Dr. Askling, an epidemiologist at the Karolinska Institute in Stockholm.
A similar pattern existed for joint-replacement surgeries. Hip surgery, for example, was 2.9-fold more frequent among the hereditary hemochromatosis patients than among their matched controls, while among the first-degree relatives the incidence of hip-replacement surgery was 10% less common than among the matched controls, a difference that was not statistically significant.
Dr. Askling said that he had no disclosures.
FROM THE ANNUAL EUROPEAN CONGRESS OF RHEUMATOLOGY
Major Finding: Patients with hereditary hemochromatosis had a 2.4-fold increased prevalence of arthropathies and a 2.9-fold increased rate of hip surgery, compared with matched controls. In contrast, first-degree relatives of hereditary hemochromatosis patients had no significantly different rates for arthropathy or need for joint-replacement surgery, compared with controls.
Data Source: Case-control study of records from Swedish national registries during 1999-2006, with 3,531 patients diagnosed with hereditary hemochromatosis and 37,369 matched controls, and 11,794 first-degree relatives of the patients and 196,628 matched controls.
Disclosures: Dr. Askling said that he had no disclosures.