User login
PE in COPD, Board Certification, Neutropenic Cancer, and More
Gatifloxacin and Dysglycemia
Park-Wyllie LY, Juurlink DN, Kopp A, et al. Outpatient gatifloxacin therapy and dysglycemia in older adults. N Engl J Med. 2006 Mar;354(13):1352-1361.
Fluoroquinolones are the most commonly prescribed antibiotics in the United States. Side effects associated with some fluoroquinolones (temafloxacin, grepafloxacin, sparfloxacin, and trovafloxacin) have prompted their restriction or withdrawal. Until now, dysglycemia had been associated with gatifloxacin only in small studies or case reports.
This study sought to examine, by a nested case control design, the association between gatifloxacin and dysglycemia that required hospital care. The researchers reviewed all prescription records from the Ontario (Canada) Drug Benefit database, which houses complete prescription drug sales for all patients older than age 65 (1.4 million residents). They linked this with a national Canadian database of those same patients’ emergency room visits and hospital admissions. Cases were patients who received hospital care for hypoglycemia (or hyperglycemia) within 30 days of filling an antibiotic prescription (macrolide, cephalosporin, or fluoroquinolone). Controls were patients who had not received hospital care after an antibiotic prescription in the same time period. They were matched by age, gender, whether or not they had been diagnosed as having diabetes, diabetic drug use, and time of antibiotic prescription. Patients were excluded if they turned 65 within the year, had been hospitalized within 90 days, had subsequent hospitalizations for dysglycemia, or had more than one antibiotic in 30 days. Logistic regression was used to determine the odds ratio for the association between dysglycemia and recent antibiotic use. In multivariable analysis, they adjusted for liver disease, renal disease, alcohol use, hospitalizations, physician visits, diabetic and P-450 medications, socioeconomic status, and number of prescription drugs. They were also stratified by diabetes status.
The cases treated for hypoglycemia were four times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 4.3, CI 2.9-6.3). The association was slightly less with levofloxacin (OR 1.5, CI 1.2-2.0), and there was no association of hypoglycemia with moxifloxacin, ciprofloxacin, or cephalosporins. The cases treated for hyperglycemia were 17 times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 16.7, CI 10.4-26.8). There was no association of hyperglycemia with the other fluoroquinolones or cephalosporins. The analyses were similar when stratified by diabetes status. In total, 1.1% of all gatifloxacin treatments were associated with dysglycemia requiring hospital care within 30 days. As to what to do with gatifloxacin, as stated precisely in an accompanying editorial, “For every approved indication for gatifloxacin, there are safer, equally effective, and less costly alternatives.”
Physician Board Certification and Acute MI Quality Measures.
Chen J, Rathore SS, Wang Y, et al. Physician board certification and the care and outcomes of elderly patients with acute myocardial infarction. J Gen Intern Med. 2006 Mar;21(3):238-244.
Board certification may have implications for practicing physicians because there is evidence that both hiring organizations and patients prefer board-certified physicians over non-board certified physicians. However, it is unknown if such certification translates into better quality of patient care.
In this study researchers sought to examine the relationship between physician board certification and quality of care in patients with acute myocardial infarction (AMI). Medical records were abstracted from the Cooperative Cardiovascular Project, a cohort of Medicare beneficiaries hospitalized with AMI. Board certification was obtained from the American Medical Association (AMA) Physician Masterfile, which is reportedly 94% accurate. Quality of care measures included ASA and beta-blocker use at the time of admission and discharge. Researchers also evaluated 30-day and one-year mortality.
They evaluated these quality measures on 101,251 patients and 36,668 physicians, of which 80% were board certified. In multivariable analyses adjusting for patient, hospital, and physician characteristics, board-certified internal medicine and cardiology physicians (but not family practitioners) were more likely to prescribe ASA and beta-blockers at admission and discharge than non-board certified physicians (adjusted relative risk ranged from 1.04 to 1.20). There was no difference in 30-day and one-year mortality among any specialty after multivariable adjustment.
These results, albeit modest, suggest that physician board certification may be associated with superior quality of care in elderly patients with AMI. The authors offer that board-certified physicians may be more aware or familiar with guidelines or may be more likely to agree with clinical guidelines. Although board-certified physicians have been shown to complete more hours of CME and spend more time reading journals, they caution that board certification should not be used as a surrogate marker of quality. Because 30% of U.S. practicing physicians are not currently board certified, these results certainly warrant further study.
PE in COPD
Tillie-Leblond I, Marquette CH, Perez T, et al. Pulmonary embolism in patients with unexplained exacerbation of chronic obstructive pulmonary disease: prevalence and risk factors. Ann Intern Med. 2006 Mar 21;144(6):390-396.
This study sought to evaluate the prevalence and risk factors for pulmonary embolus (PE) in patients with unexplained exacerbations of COPD. All patients with an unexplained COPD exacerbation requiring hospitalization (not ICU) were evaluated for PE by spiral chest CT and lower limb venous ultrasound (USG). The COPD flare was “unexplained” if there were no signs or symptoms of respiratory tract infection, no pneumothorax, or a discrepancy between the clinical/radiologic features and the degree of hypoxemia. Patients were considered to have a PE if either of the two tests (CT or USG) were positive. Patients were not considered to have a PE if both tests were negative, and there was no evidence of PE at three-month follow-up.
Of 211 referred patients, 14 were not included due to inconclusive results or iodine intolerance. Of 197 enrolled patients, 25% had PE. There was no difference between the PE and non-PE groups with respect to referral location, clinical symptoms (dyspnea, pleuritic pain, hemoptysis, tachycardia, lower limb edema), need for long term oxygen therapy, admission P02 or PC02, recent trauma, recent surgery, obesity, or immobilization for more than seven days. Factors associated with PE on bivariate analysis included a decrease in PC02 >5mmHg from baseline, previous thromboembolism, and malignancy.
Researchers then calculated these patient’s Geneva score (a PE predictor score based on age, history, pulse, ABG, and chest X-ray findings. Those with a low probability Geneva score had a 9% incidence of PE, those with an intermediate score had a 47% incidence, and those with a high Geneva score had a 100% incidence.
In conclusion, in this study population of non-ICU patients with unexplained exacerbations of COPD, one in four had evidence of thromboembolic disease. Significant risk ratios between groups were found for patients with a prior history of thromboembolism, malignancy, or a decrease in their baseline PC02. These factors should be weighted heavily in determining which patients with unexplained COPD exacerbations should undergo workup to exclude a PE. The Geneva score also correlated well with PE incidence in this population.
Telithromycin in Asthma Exacerbations
Johnston SL, Blasi FB, Black PN, et al. The effect of telithromycin in acute exacerbations of asthma. New Engl J Med. 2006 Apr 13;354(15):1589-1600.
The use of antibiotics for uncomplicated asthma exacerbations is not currently considered standard of care. This randomized placebo controlled trial was designed to determine if telithromycin (a ketolide, structurally similar to macrolides, with efficacy against mycoplasma and chlamydia pneumonia) improves symptoms and peak flow rates in patients with asthma exacerbations. Researchers enrolled 278 patients age 18 to 55 with a history of asthma (less than six months) with an exacerbation (peak flow <80% and symptoms of wheeze and dyspnea). They excluded those requiring ICU care, smokers, known infection/recent antibiotic use, or regular use of oral steroids. Baseline demographics, pulmonary function, and acute medication use (steroids and beta agonists) were similar between the groups.
Intervention patients received telithromycin 800 mg a day for 10 days. The primary outcome was change in their asthma symptom score (rated on a seven-point scale) and change in their peak flows (recorded every morning for the study duration). Secondary outcomes were clinic pulmonary function tests (PFTs).
The intervention group had a mean decrease in their symptom score of 1.3 versus 1.0 in the placebo group (40% versus 27% reduction, p=.004). There was no difference between the groups in home peak flow measurements. There were statistically significant differences between the groups in clinic PFTs (FEV1, FVC, FEF 25%-75%), although the P values were not adjusted for multiple outcomes. The intervention group had a higher percentage of symptom-free days (16% versus 8%, P=.006). A total of 61% of the patients had serologic evidence of chlamydia or mycoplasma infection. Nausea (seven versus 0) and LFT elevations (two versus 0) were more frequent in the intervention group.
In conclusion, this is the first trial to report a benefit of antibiotic use in uncomplicated asthma exacerbations. This conclusion must be tempered by the underwhelming clinical improvement (1.3 versus 1.0 improvement in symptom scores), lack of peak flow improvement, recent reports of serious hepatotoxicity associated with telithromycin, and the possibility for antibiotic over-prescribing in unrefined patient populations.
Pneumonia Quality and Outcomes by Volume of Care
Lindenauer PK, Behal R, Murray CK, et al. Volume, quality of care, and outcome in pneumonia. Ann Intern Med. 2006 Feb 21;144(4):262-269.
It is widely known that, for many medical conditions and surgical procedures, outcomes are better when delivered by high-volume providers. It is not known if this holds true for patients with community-acquired pneumonia. To determine the association between physician/hospital volume and patient quality/outcomes, researchers utilized data from the Medicare National Pneumonia Quality Improvement Project. They included patients with an ICD9 diagnosis of pneumonia (850 patients were randomly selected from each state) at acute care hospitals with general or family medicine attendings. They excluded patients with no documentation of pneumonia, a normal chest X-ray, age <65, death on day one, comfort measures only, and departure against medical advice or transfer. Each physician and hospital volume were calculated from Medicare Part A claims for the same calendar year and analyzed by quartiles of volume.
Of the 9,741 physicians analyzed (13,480 patients), the median annual number of pneumonia patients was four, nine, 15, and 29 (in quartiles 1-4). Physician volume of care had little or no effect on performance rates of the timing of antibiotics, appropriate initial antibiotic, use of blood cultures, or in-hospital/30-day mortality rates. Low volume providers were significantly more likely to provide pneumococcal and influenza screening.
Of the 3,243 hospitals analyzed, the median annual pneumonia caseload was 57, 142, 262, and 465 (in quartiles 1-4). Hospital volume of care had little or no effect on performance rates of the appropriate initial antibiotic, use of blood cultures, pneumococcal/influenza screening, or in-hospital/30-day mortality rates (after severity of illness adjustment). Low volume centers were significantly more likely to give the first antibiotic within four hours.
In conclusion, volume of care by individual providers and hospital systems does not necessarily translate into better quality outcomes in pneumonia care. This may be partially explained by the challenges that larger medical centers face regarding delivering timely care (in overcrowded emergency rooms) and influencing behavior change (such as with standardized order sets).
By Debra Anoff, MD, assistant professor of medicine, Lucy Guerra, MD, assistant professor of medicine, Bjorn Holmstrom, MD, assistant professor of medicine, Asha Ramsakal, DO, assistant professor of medicine and chief, Richard Gross, MD, FACP, professor of medicine and chief, Division of Internal and Hospital Medicine H. Lee Moffitt Cancer Center and Research Institute, University of South Florida College of Medicine
Risk Factors for Mortality in Neutropenic Cancer Patients
Kuderer, NM, Dale DC, Crawford J, et al. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer. 2006 May 15;106(10):2258-2266.
Background: Neutropenic fever in a cancer patient is considered a medical emergency. Most episodes of febrile neutropenia result in hospital admission with prompt institution of broad spectrum antibiotics. The definition of neutropenia is usually regarded as an absolute neutrophil count (neutrophils plus bands) less than 500 cells/µL. The mortality rate of a cancer patient hospitalized with neutropenic fever ranges from 5 to 11%. There have been numerous small studies looking at risk factors associated with inpatient mortality. However, their small sample size and very select group of patients limit their generalizability to a standard hospitalist practice.
Methods: The authors used a longitudinal discharge database derived from 115 U.S. medical centers—both academic and community-based—in 39 states, looking retrospectively at all adult cancer patients hospitalized for febrile neutropenia between 1995 and 2000. The database included 55,276 hospitalizations and 41,779 patients and was analyzed for length of stay, cost per episode, mortality, and the clinical factors associated with mortality and prolonged hospitalization.
Results: The mortality rate for cancer patients with neutropenic fever averaged 9.5% per hospital. The average mortality rate was 14.3% for leukemia, 8.9% for lymphoma, and 8.0% for solid tumors. Lung cancer had the highest average mortality rate, 13.4%, followed by colorectal cancer at 8.8%, and breast cancer, which had the lowest mortality rate with 3.6%. Moreover, the highest mortality rate, 39.2%, was seen in those patients with a documented infection with invasive aspergillosis, while the rate of mortality for invasive candidiasis was 36.7%, followed by gram-negative bacteremia at 33.9%, pneumonia at 26.5%, and gram-positive bacteremia at 21.2%.
Patients without comorbidities, including common illnesses such as diabetes, congestive heart failure, and renal failure, had an average 2.6 % risk of dying. Those with one comorbidity had a 10.3% risk, and patients with more than one comorbidity had a mortality risk of 21.4%. Multivariate analysis revealed that the odds ratios for inpatient mortality were 3.94 for lung disease, 3.26 for cerebrovascular disease, 3.16 for renal disease, 2.89 for liver disease, 1.94 for pulmonary embolism, and 1.58 for heart disease.
The study also showed that patients hospitalized for longer than 10 days (comprising 35% of all patients) accounted for the majority of overall deaths (65%), overall cost (78%), and overall days spent in the hospital (74%).
Conclusions: The study provided an estimate of inpatient mortality associated with neutropenic fever in cancer patients and highlighted those subgroups as being at heightened risk for death. Important limitations include the retrospective nature of the study, the use of administrative data sets as the primary data source, and a failure to analyze for the duration of neutropenia prior to treatment. The authors’ conclusion that the identified factors may be useful in determining which patients warrant “more aggressive supportive care measures” is plausible, but does not find enough support in the study to warrant general implementation.
Long-Term Value of Electrocardiogram Before Noncardiac Surgery
Jeger RV, Probst C, Arsenic R, et al. Long-term prognostic value of the preoperative 12-lead electrocardiogram before major noncardiac surgery in coronary artery disease. Am Heart J. 2006 Feb;151(2):508-513.
Background: The 12-lead electrocardiogram is commonly utilized as part of the cardiovascular preoperative risk stratification. Certain ECG abnormalities, such as left bundle branch block, Q waves, ST-T abnormalities, arrhythmias, and left ventricular hypertrophy (LVH), have been associated with elevated risk in the perioperative period.1,2 This article prospectively evaluated whether an exhaustive analysis of preoperative ECGs in this population would have long-term predictive validity.
Methods: The study utilized a “predefined” analysis applied retrospectively on data obtained for another study.3,4
The study analyzed 172 patients, all of whom had documented coronary artery disease (CAD) as defined by previous myocardial infarction (MI), prior revascularization, significant stenoses on prior catheterization, ischemia (by dobutamine stress echocardiogram or adenosine thallium imaging), or who were high risk for CAD. High risk required at least two of the following: age over 70, hypertension, diabetes mellitus, prior stroke, exercise intolerance, or a “pathological resting ECG.” These patients were to undergo noncardiac surgery. The primary endpoint was all-cause mortality after two years, and the secondary endpoint was major adverse cardiac events (MACE) after two years. The MACE were defined as nonfatal MI, coronary revascularization, re-hospitalization due to recurrent ischemia, and/or cardiac death.
The ECGs were obtained one day prior to surgery and analyzed using the Minnesota classification. Telephone interviews were done at six, 12, and 24 months to evaluate outcome, and the Swiss Mortality Registry was used to determine cause of death. Analyzed data were adjusted for current beta-blocker use and perioperative ischemia using a sensitivity analysis-like correction that is described briefly in the report.
Results: ST depression (odds ratio [OR] 4.5) and faster heart rate (OR 1.6) were independent predictors of all-cause mortality. Faster heart rate (OR 1.7) was also an independent predictor of MACE.
Commentary: The results of this relatively small study raise awareness of resting tachycardia and ST depression as possible markers for poor perioperative and two-year postoperative outcomes. The latter is already included in risk stratification guidelines5, and the former is of uncertain validity due to possible confounding variables such as anxiety or pain, beta blocker dosing differences, and lack of intra- and postoperative beta blocker usage data which may affect postoperative cardiac morbidity and mortality long after the drugs are stopped.
For hospitalists and other physicians performing cardiac risk stratification for noncardiac surgery patients, the current study does not warrant any change in current practice as recommended in the American College of Cardiology/American Heart Association Guidelines 2002.5 As to whether resting tachycardia should be considered as a predictive ECG criterion in this context, further valid and applicable evidence is needed.
References
- De Bacquer D, De Backer G, Kornitzer M, et al. Prognostic value of ECG findings for total, cardiovascular disease, and coronary heart disease death in men and women. Heart. 1998 Dec;80(6):570-577.
- Tervahauta M, Pekkanen J, Punsar S, et al. Resting electrocardiographic abnormalities as predictors of coronary events and total mortality among elderly men. Am J Med. 1996 Jun;100(6):641-645.
- Filipovic M, Jeger R, Probst C, et al. Heart rate variability and cardiac troponin I are incremental and independent predictors of one-year all-cause mortality after major noncardiac surgery in patients at risk of coronary artery disease. J Am Coll Cardiol. 2003 Nov 19;42(10):1767-76.
- Filipovic M, Jeger RV, Girard T, et al. Predictors of long-term mortality and cardiac events in patients with known or suspected coronary artery disease who survive major noncardiac surgery. Anaesthesia. 2005 Jan;60(1):5-11.
- Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update for perioperative cardiovascular evaluation for noncardiac surgery—executive summary. Circulation. 2002 Mar 12;105(10):1257-1267.
Statins and Cardiovascular Disease
Hackam DG, Mamdani M, Li P, et al. Statins and sepsis in patients with cardiovascular disease: a population-based cohort analysis. Lancet. 2006 Feb 4;367(9508):413-418.
Background: The benefits of statins in secondary prevention of MI and ischemic CVA, as well as in reduction of all-cause mortality and their primary prevention in diabetics, are well documented in the literature.1 The concept of statins reducing subsequent sepsis in humans with atherosclerotic cardiovascular disease (CVD) is relatively new. One hypothesis holds that such an effect may be due to several common pathophysiologic mechanisms of sepsis and CVD: endothelial instability, immune dysregulation, inflammation, and thrombogenesis. Statins have been shown to provide improved outcomes from sepsis in animal studies, and observational studies in humans have raised similar hypotheses. This study attempts to analyze whether statin use in humans is associated with similar benefits regarding prevention of sepsis.
Methods: This was a population-based cohort analysis of 141,487 patients in Ontario, Canada, during the period of time from 1997-2002, who were older than age 65 and had been hospitalized for acute coronary syndrome or ischemic stroke, or had revascularization and survived three months post discharge. Using four reputable linked administrative databases, the authors found that 46,662 (33%) patients were prescribed a statin within three months of the discharge date (the index date), and 94,825 (67%) were not. About 19% of enrolled patients died within nine months and were excluded from the analysis. Of the eligible patients, propensity-based matching was used to identify 69,168 patients, of whom half were prescribed a statin and half were not. The patients were then analyzed through provincial administrative databases for the end points of hospital admission with an International Classification of Disease (ICD) code of sepsis, severe sepsis, fatal sepsis, death, or the end of the study.
Results: A total of 551 out of 34,584 patients were admitted for sepsis from the statin group, and 667 out of 34,584 were admitted from the control group during a mean follow-up of 2.2 years. The rate of sepsis in the statin group was significantly lower than in the control group (71.2 versus 88.0 per 10,000 person-years; p=0.0003). Statin use was also associated with fewer episodes of sepsis in an extended duration of 3.8 years, and with a lower risk of severe and fatal sepsis where sepsis was the admission diagnosis. This protection was evident at both high and low doses. The hazard ratio for sepsis was .81. There was a 19% relative reduction in the risk of sepsis in patients older than 65 with atherosclerosis. The absolute risk reduction for the occurrence of sepsis per 10,000 person-years was 16.8%, or .168% per person-year, with a corresponding number needed to treat (NNT) of 595 patients to prevent one episode of sepsis per year.
Comments: Though sophisticated and diverse statistical methods were used to assess the robustness of the analysis, this study is retrospective. Unidentified confounders, clinical sepsis risk stratification (the presence of obstructive uropathy or impairments leading to aspiration or skin breakdown, for example) are not accounted for in the analysis. Nonetheless, the hypothesis is of high relevance to hospitalists; it has biologic plausibility, and the results are intriguing if not definitive.
From a practical perspective, it seems prudent to ensure ongoing statin use for all patients with appropriate traditional indications. Initiating statins for the sole purpose of reducing future risk of sepsis is not yet sufficiently supported by the available evidence, and the NNT of almost 600 patients per year in the current study does little to alter that recommendation. In reply to a subsequent letter to the editor, the authors pointed out that the high NNT in part reflects the low-risk profile of the cohort and would be lower in higher risk patients; for example, patients with chronic renal failure, previous infections, or corticosteroid use would have NNTs of 166, 250, and 250, respectively.2 A randomized, controlled prospective trial would be a welcome addition to the evidence on this important topic, as would studies of the use of statins solely as an acute intervention upon suspicion of sepsis.
References
- MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002 Jul 6;360(9326):7-22.
- Hackam DG, Redelmeier DA. Statins and sepsis—authors' reply. Lancet. 2006;367:1651.
Review: Impact of Health Information Technology
Advances in information technology have transformed the world of business and education and will undoubtedly change the delivery and implementation of medical services. What arguably sets the world of health information apart from other systems is, however, the extreme sensitivity of the data involved and the impact it has on human lives.
Methods and data sources: In the article, “Systemic Review: Impact of Health Information Technology on Quality, Efficiency, and Costs of Medical Care,” the authors reviewed four data sources and extracted information on system design, effects on quality and cost benefit analysis. Four data sources were utilized including a MEDLINE analysis of articles indexed as health information technology (HIT) from 1995 to January 2004 utilizing:
- Cochrane Center Registry of Controlled Trials;
- Cochrane Database of Abstracts of Reviews of Effects;
- Periodical Abstracts Database; and
- Studies singled out by experts up to April of 2005
Of the four data sources, 24% of all studies came from the following academic centers: the Regenstrief Institute (Indianapolis), Brigham and Women’s Hospital (Boston), Department of Veterans Affairs, and the Latter Day Saints Hospital/Intermountain Health Care.
Inclusion criteria: The HIT evaluation and efficacy information derived was from these four academic institutions, each with its own EHR (electronic health record) system. Of 4,582 initial articles derived from a title review, 867 were deemed suitable given their title matter, but only 257 met inclusion criteria.
A modified framework from the Institute of Medicine’s six aims for care and a framework to analyze costs developed by the authors themselves was used for analysis.1
Reasons for rejection: Articles that did not have HIT as the subject, others that did not report outcomes data, and those that did not examine barriers for outcomes analysis were rejected.
Information examined: Extracted information on system capabilities including components of the system such as:
- User friendliness;
- Types of systems such as EHR that allowed for medical decision making support and e-prescribing; and
- Functional capabilities such as order entry and clinical documentation.
Common characteristics shared by the HIT systems evaluated by the four academic institutions: they were all multifunctional and included medical decision making support, all were internally developed by research experts and all had capabilities that had been improved upon and added incrementally over time.
The data supported five primary goals:
- Increasing delivery of healthcare according to established protocols and guidelines;
- Enhancing capacity to perform surveillance and monitoring of disease conditions and care delivery;
- Reducing medication error rates;
- Decreasing utilization of care; and
- Producing a mixed effect on time utilization.
Major findings: (see Figure 1, below).
The authors of the article summarized 22 other studies in Appendix 22 from other institutions. The benefits noted were very similar to those found in the studies from the benchmark institutions; however, one major difference was the use of pre/post time-series designs that did not have a control or comparative group. Internally and commercially, HIT systems were evaluated in most of these studies with thirteen focusing on the former and nine on the later.
Summary and discussion: This study raises several questions worthy of further research and study:
- How are systems to interface with regard to the portability of health care information?
- Which are better: internally devised systems or commercially available systems?
- Who is going to be responsible for establishing standard guidelines for the implementation of HIT systems across the diverse healthcare systems in the United States? and
- How are the data to be used and analyzed by insurers and even public health entities?
HIT has shown many benefits with regard to quality of patient care issues and efficiency. Studies from these four benchmark institutions had one important limitation, however, and that is that the development of an internally developed HIT system took many years and is unlikely to be applicable to other institutions that have fewer resources and are struggling to implement the technology in a timely manner.
As the authors of the article acknowledge, it is not clear if HIT systems, though useful as tools, alter states of disease and health. More research looking at the direct impact of HIT information on morbidity and mortality is needed. As the authors state, this raises the question of a national HIT system, thereby making adoption of HIT a bipartisan initiative.
Providers need better evidence on information systems in order to make informed decisions about acquiring and implementing technology in community settings. The authors of this article made the first attempt to collate and appraise such evidence. Additional research is needed in academic, governmental, and community settings in both acute and nonacute facilities. As the authors point out, a uniform standard should be devised at the federal, state, and local level to report research on the implementation of HIT systems similar to the CONSORT and Quorum statement.
References
- Chaudry B, Wang J, Wu S, et al. Systematic review: impact of health information technology on quality, efficiency and costs of medical care. Ann Intern Med. 2006 May 16;144(10):742-752.
- Bates DW, Leape LL Cullen DJ. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998 Oct 21;280(15):1311-1316.
Gatifloxacin and Dysglycemia
Park-Wyllie LY, Juurlink DN, Kopp A, et al. Outpatient gatifloxacin therapy and dysglycemia in older adults. N Engl J Med. 2006 Mar;354(13):1352-1361.
Fluoroquinolones are the most commonly prescribed antibiotics in the United States. Side effects associated with some fluoroquinolones (temafloxacin, grepafloxacin, sparfloxacin, and trovafloxacin) have prompted their restriction or withdrawal. Until now, dysglycemia had been associated with gatifloxacin only in small studies or case reports.
This study sought to examine, by a nested case control design, the association between gatifloxacin and dysglycemia that required hospital care. The researchers reviewed all prescription records from the Ontario (Canada) Drug Benefit database, which houses complete prescription drug sales for all patients older than age 65 (1.4 million residents). They linked this with a national Canadian database of those same patients’ emergency room visits and hospital admissions. Cases were patients who received hospital care for hypoglycemia (or hyperglycemia) within 30 days of filling an antibiotic prescription (macrolide, cephalosporin, or fluoroquinolone). Controls were patients who had not received hospital care after an antibiotic prescription in the same time period. They were matched by age, gender, whether or not they had been diagnosed as having diabetes, diabetic drug use, and time of antibiotic prescription. Patients were excluded if they turned 65 within the year, had been hospitalized within 90 days, had subsequent hospitalizations for dysglycemia, or had more than one antibiotic in 30 days. Logistic regression was used to determine the odds ratio for the association between dysglycemia and recent antibiotic use. In multivariable analysis, they adjusted for liver disease, renal disease, alcohol use, hospitalizations, physician visits, diabetic and P-450 medications, socioeconomic status, and number of prescription drugs. They were also stratified by diabetes status.
The cases treated for hypoglycemia were four times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 4.3, CI 2.9-6.3). The association was slightly less with levofloxacin (OR 1.5, CI 1.2-2.0), and there was no association of hypoglycemia with moxifloxacin, ciprofloxacin, or cephalosporins. The cases treated for hyperglycemia were 17 times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 16.7, CI 10.4-26.8). There was no association of hyperglycemia with the other fluoroquinolones or cephalosporins. The analyses were similar when stratified by diabetes status. In total, 1.1% of all gatifloxacin treatments were associated with dysglycemia requiring hospital care within 30 days. As to what to do with gatifloxacin, as stated precisely in an accompanying editorial, “For every approved indication for gatifloxacin, there are safer, equally effective, and less costly alternatives.”
Physician Board Certification and Acute MI Quality Measures.
Chen J, Rathore SS, Wang Y, et al. Physician board certification and the care and outcomes of elderly patients with acute myocardial infarction. J Gen Intern Med. 2006 Mar;21(3):238-244.
Board certification may have implications for practicing physicians because there is evidence that both hiring organizations and patients prefer board-certified physicians over non-board certified physicians. However, it is unknown if such certification translates into better quality of patient care.
In this study researchers sought to examine the relationship between physician board certification and quality of care in patients with acute myocardial infarction (AMI). Medical records were abstracted from the Cooperative Cardiovascular Project, a cohort of Medicare beneficiaries hospitalized with AMI. Board certification was obtained from the American Medical Association (AMA) Physician Masterfile, which is reportedly 94% accurate. Quality of care measures included ASA and beta-blocker use at the time of admission and discharge. Researchers also evaluated 30-day and one-year mortality.
They evaluated these quality measures on 101,251 patients and 36,668 physicians, of which 80% were board certified. In multivariable analyses adjusting for patient, hospital, and physician characteristics, board-certified internal medicine and cardiology physicians (but not family practitioners) were more likely to prescribe ASA and beta-blockers at admission and discharge than non-board certified physicians (adjusted relative risk ranged from 1.04 to 1.20). There was no difference in 30-day and one-year mortality among any specialty after multivariable adjustment.
These results, albeit modest, suggest that physician board certification may be associated with superior quality of care in elderly patients with AMI. The authors offer that board-certified physicians may be more aware or familiar with guidelines or may be more likely to agree with clinical guidelines. Although board-certified physicians have been shown to complete more hours of CME and spend more time reading journals, they caution that board certification should not be used as a surrogate marker of quality. Because 30% of U.S. practicing physicians are not currently board certified, these results certainly warrant further study.
PE in COPD
Tillie-Leblond I, Marquette CH, Perez T, et al. Pulmonary embolism in patients with unexplained exacerbation of chronic obstructive pulmonary disease: prevalence and risk factors. Ann Intern Med. 2006 Mar 21;144(6):390-396.
This study sought to evaluate the prevalence and risk factors for pulmonary embolus (PE) in patients with unexplained exacerbations of COPD. All patients with an unexplained COPD exacerbation requiring hospitalization (not ICU) were evaluated for PE by spiral chest CT and lower limb venous ultrasound (USG). The COPD flare was “unexplained” if there were no signs or symptoms of respiratory tract infection, no pneumothorax, or a discrepancy between the clinical/radiologic features and the degree of hypoxemia. Patients were considered to have a PE if either of the two tests (CT or USG) were positive. Patients were not considered to have a PE if both tests were negative, and there was no evidence of PE at three-month follow-up.
Of 211 referred patients, 14 were not included due to inconclusive results or iodine intolerance. Of 197 enrolled patients, 25% had PE. There was no difference between the PE and non-PE groups with respect to referral location, clinical symptoms (dyspnea, pleuritic pain, hemoptysis, tachycardia, lower limb edema), need for long term oxygen therapy, admission P02 or PC02, recent trauma, recent surgery, obesity, or immobilization for more than seven days. Factors associated with PE on bivariate analysis included a decrease in PC02 >5mmHg from baseline, previous thromboembolism, and malignancy.
Researchers then calculated these patient’s Geneva score (a PE predictor score based on age, history, pulse, ABG, and chest X-ray findings. Those with a low probability Geneva score had a 9% incidence of PE, those with an intermediate score had a 47% incidence, and those with a high Geneva score had a 100% incidence.
In conclusion, in this study population of non-ICU patients with unexplained exacerbations of COPD, one in four had evidence of thromboembolic disease. Significant risk ratios between groups were found for patients with a prior history of thromboembolism, malignancy, or a decrease in their baseline PC02. These factors should be weighted heavily in determining which patients with unexplained COPD exacerbations should undergo workup to exclude a PE. The Geneva score also correlated well with PE incidence in this population.
Telithromycin in Asthma Exacerbations
Johnston SL, Blasi FB, Black PN, et al. The effect of telithromycin in acute exacerbations of asthma. New Engl J Med. 2006 Apr 13;354(15):1589-1600.
The use of antibiotics for uncomplicated asthma exacerbations is not currently considered standard of care. This randomized placebo controlled trial was designed to determine if telithromycin (a ketolide, structurally similar to macrolides, with efficacy against mycoplasma and chlamydia pneumonia) improves symptoms and peak flow rates in patients with asthma exacerbations. Researchers enrolled 278 patients age 18 to 55 with a history of asthma (less than six months) with an exacerbation (peak flow <80% and symptoms of wheeze and dyspnea). They excluded those requiring ICU care, smokers, known infection/recent antibiotic use, or regular use of oral steroids. Baseline demographics, pulmonary function, and acute medication use (steroids and beta agonists) were similar between the groups.
Intervention patients received telithromycin 800 mg a day for 10 days. The primary outcome was change in their asthma symptom score (rated on a seven-point scale) and change in their peak flows (recorded every morning for the study duration). Secondary outcomes were clinic pulmonary function tests (PFTs).
The intervention group had a mean decrease in their symptom score of 1.3 versus 1.0 in the placebo group (40% versus 27% reduction, p=.004). There was no difference between the groups in home peak flow measurements. There were statistically significant differences between the groups in clinic PFTs (FEV1, FVC, FEF 25%-75%), although the P values were not adjusted for multiple outcomes. The intervention group had a higher percentage of symptom-free days (16% versus 8%, P=.006). A total of 61% of the patients had serologic evidence of chlamydia or mycoplasma infection. Nausea (seven versus 0) and LFT elevations (two versus 0) were more frequent in the intervention group.
In conclusion, this is the first trial to report a benefit of antibiotic use in uncomplicated asthma exacerbations. This conclusion must be tempered by the underwhelming clinical improvement (1.3 versus 1.0 improvement in symptom scores), lack of peak flow improvement, recent reports of serious hepatotoxicity associated with telithromycin, and the possibility for antibiotic over-prescribing in unrefined patient populations.
Pneumonia Quality and Outcomes by Volume of Care
Lindenauer PK, Behal R, Murray CK, et al. Volume, quality of care, and outcome in pneumonia. Ann Intern Med. 2006 Feb 21;144(4):262-269.
It is widely known that, for many medical conditions and surgical procedures, outcomes are better when delivered by high-volume providers. It is not known if this holds true for patients with community-acquired pneumonia. To determine the association between physician/hospital volume and patient quality/outcomes, researchers utilized data from the Medicare National Pneumonia Quality Improvement Project. They included patients with an ICD9 diagnosis of pneumonia (850 patients were randomly selected from each state) at acute care hospitals with general or family medicine attendings. They excluded patients with no documentation of pneumonia, a normal chest X-ray, age <65, death on day one, comfort measures only, and departure against medical advice or transfer. Each physician and hospital volume were calculated from Medicare Part A claims for the same calendar year and analyzed by quartiles of volume.
Of the 9,741 physicians analyzed (13,480 patients), the median annual number of pneumonia patients was four, nine, 15, and 29 (in quartiles 1-4). Physician volume of care had little or no effect on performance rates of the timing of antibiotics, appropriate initial antibiotic, use of blood cultures, or in-hospital/30-day mortality rates. Low volume providers were significantly more likely to provide pneumococcal and influenza screening.
Of the 3,243 hospitals analyzed, the median annual pneumonia caseload was 57, 142, 262, and 465 (in quartiles 1-4). Hospital volume of care had little or no effect on performance rates of the appropriate initial antibiotic, use of blood cultures, pneumococcal/influenza screening, or in-hospital/30-day mortality rates (after severity of illness adjustment). Low volume centers were significantly more likely to give the first antibiotic within four hours.
In conclusion, volume of care by individual providers and hospital systems does not necessarily translate into better quality outcomes in pneumonia care. This may be partially explained by the challenges that larger medical centers face regarding delivering timely care (in overcrowded emergency rooms) and influencing behavior change (such as with standardized order sets).
By Debra Anoff, MD, assistant professor of medicine, Lucy Guerra, MD, assistant professor of medicine, Bjorn Holmstrom, MD, assistant professor of medicine, Asha Ramsakal, DO, assistant professor of medicine and chief, Richard Gross, MD, FACP, professor of medicine and chief, Division of Internal and Hospital Medicine H. Lee Moffitt Cancer Center and Research Institute, University of South Florida College of Medicine
Risk Factors for Mortality in Neutropenic Cancer Patients
Kuderer, NM, Dale DC, Crawford J, et al. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer. 2006 May 15;106(10):2258-2266.
Background: Neutropenic fever in a cancer patient is considered a medical emergency. Most episodes of febrile neutropenia result in hospital admission with prompt institution of broad spectrum antibiotics. The definition of neutropenia is usually regarded as an absolute neutrophil count (neutrophils plus bands) less than 500 cells/µL. The mortality rate of a cancer patient hospitalized with neutropenic fever ranges from 5 to 11%. There have been numerous small studies looking at risk factors associated with inpatient mortality. However, their small sample size and very select group of patients limit their generalizability to a standard hospitalist practice.
Methods: The authors used a longitudinal discharge database derived from 115 U.S. medical centers—both academic and community-based—in 39 states, looking retrospectively at all adult cancer patients hospitalized for febrile neutropenia between 1995 and 2000. The database included 55,276 hospitalizations and 41,779 patients and was analyzed for length of stay, cost per episode, mortality, and the clinical factors associated with mortality and prolonged hospitalization.
Results: The mortality rate for cancer patients with neutropenic fever averaged 9.5% per hospital. The average mortality rate was 14.3% for leukemia, 8.9% for lymphoma, and 8.0% for solid tumors. Lung cancer had the highest average mortality rate, 13.4%, followed by colorectal cancer at 8.8%, and breast cancer, which had the lowest mortality rate with 3.6%. Moreover, the highest mortality rate, 39.2%, was seen in those patients with a documented infection with invasive aspergillosis, while the rate of mortality for invasive candidiasis was 36.7%, followed by gram-negative bacteremia at 33.9%, pneumonia at 26.5%, and gram-positive bacteremia at 21.2%.
Patients without comorbidities, including common illnesses such as diabetes, congestive heart failure, and renal failure, had an average 2.6 % risk of dying. Those with one comorbidity had a 10.3% risk, and patients with more than one comorbidity had a mortality risk of 21.4%. Multivariate analysis revealed that the odds ratios for inpatient mortality were 3.94 for lung disease, 3.26 for cerebrovascular disease, 3.16 for renal disease, 2.89 for liver disease, 1.94 for pulmonary embolism, and 1.58 for heart disease.
The study also showed that patients hospitalized for longer than 10 days (comprising 35% of all patients) accounted for the majority of overall deaths (65%), overall cost (78%), and overall days spent in the hospital (74%).
Conclusions: The study provided an estimate of inpatient mortality associated with neutropenic fever in cancer patients and highlighted those subgroups as being at heightened risk for death. Important limitations include the retrospective nature of the study, the use of administrative data sets as the primary data source, and a failure to analyze for the duration of neutropenia prior to treatment. The authors’ conclusion that the identified factors may be useful in determining which patients warrant “more aggressive supportive care measures” is plausible, but does not find enough support in the study to warrant general implementation.
Long-Term Value of Electrocardiogram Before Noncardiac Surgery
Jeger RV, Probst C, Arsenic R, et al. Long-term prognostic value of the preoperative 12-lead electrocardiogram before major noncardiac surgery in coronary artery disease. Am Heart J. 2006 Feb;151(2):508-513.
Background: The 12-lead electrocardiogram is commonly utilized as part of the cardiovascular preoperative risk stratification. Certain ECG abnormalities, such as left bundle branch block, Q waves, ST-T abnormalities, arrhythmias, and left ventricular hypertrophy (LVH), have been associated with elevated risk in the perioperative period.1,2 This article prospectively evaluated whether an exhaustive analysis of preoperative ECGs in this population would have long-term predictive validity.
Methods: The study utilized a “predefined” analysis applied retrospectively on data obtained for another study.3,4
The study analyzed 172 patients, all of whom had documented coronary artery disease (CAD) as defined by previous myocardial infarction (MI), prior revascularization, significant stenoses on prior catheterization, ischemia (by dobutamine stress echocardiogram or adenosine thallium imaging), or who were high risk for CAD. High risk required at least two of the following: age over 70, hypertension, diabetes mellitus, prior stroke, exercise intolerance, or a “pathological resting ECG.” These patients were to undergo noncardiac surgery. The primary endpoint was all-cause mortality after two years, and the secondary endpoint was major adverse cardiac events (MACE) after two years. The MACE were defined as nonfatal MI, coronary revascularization, re-hospitalization due to recurrent ischemia, and/or cardiac death.
The ECGs were obtained one day prior to surgery and analyzed using the Minnesota classification. Telephone interviews were done at six, 12, and 24 months to evaluate outcome, and the Swiss Mortality Registry was used to determine cause of death. Analyzed data were adjusted for current beta-blocker use and perioperative ischemia using a sensitivity analysis-like correction that is described briefly in the report.
Results: ST depression (odds ratio [OR] 4.5) and faster heart rate (OR 1.6) were independent predictors of all-cause mortality. Faster heart rate (OR 1.7) was also an independent predictor of MACE.
Commentary: The results of this relatively small study raise awareness of resting tachycardia and ST depression as possible markers for poor perioperative and two-year postoperative outcomes. The latter is already included in risk stratification guidelines5, and the former is of uncertain validity due to possible confounding variables such as anxiety or pain, beta blocker dosing differences, and lack of intra- and postoperative beta blocker usage data which may affect postoperative cardiac morbidity and mortality long after the drugs are stopped.
For hospitalists and other physicians performing cardiac risk stratification for noncardiac surgery patients, the current study does not warrant any change in current practice as recommended in the American College of Cardiology/American Heart Association Guidelines 2002.5 As to whether resting tachycardia should be considered as a predictive ECG criterion in this context, further valid and applicable evidence is needed.
References
- De Bacquer D, De Backer G, Kornitzer M, et al. Prognostic value of ECG findings for total, cardiovascular disease, and coronary heart disease death in men and women. Heart. 1998 Dec;80(6):570-577.
- Tervahauta M, Pekkanen J, Punsar S, et al. Resting electrocardiographic abnormalities as predictors of coronary events and total mortality among elderly men. Am J Med. 1996 Jun;100(6):641-645.
- Filipovic M, Jeger R, Probst C, et al. Heart rate variability and cardiac troponin I are incremental and independent predictors of one-year all-cause mortality after major noncardiac surgery in patients at risk of coronary artery disease. J Am Coll Cardiol. 2003 Nov 19;42(10):1767-76.
- Filipovic M, Jeger RV, Girard T, et al. Predictors of long-term mortality and cardiac events in patients with known or suspected coronary artery disease who survive major noncardiac surgery. Anaesthesia. 2005 Jan;60(1):5-11.
- Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update for perioperative cardiovascular evaluation for noncardiac surgery—executive summary. Circulation. 2002 Mar 12;105(10):1257-1267.
Statins and Cardiovascular Disease
Hackam DG, Mamdani M, Li P, et al. Statins and sepsis in patients with cardiovascular disease: a population-based cohort analysis. Lancet. 2006 Feb 4;367(9508):413-418.
Background: The benefits of statins in secondary prevention of MI and ischemic CVA, as well as in reduction of all-cause mortality and their primary prevention in diabetics, are well documented in the literature.1 The concept of statins reducing subsequent sepsis in humans with atherosclerotic cardiovascular disease (CVD) is relatively new. One hypothesis holds that such an effect may be due to several common pathophysiologic mechanisms of sepsis and CVD: endothelial instability, immune dysregulation, inflammation, and thrombogenesis. Statins have been shown to provide improved outcomes from sepsis in animal studies, and observational studies in humans have raised similar hypotheses. This study attempts to analyze whether statin use in humans is associated with similar benefits regarding prevention of sepsis.
Methods: This was a population-based cohort analysis of 141,487 patients in Ontario, Canada, during the period of time from 1997-2002, who were older than age 65 and had been hospitalized for acute coronary syndrome or ischemic stroke, or had revascularization and survived three months post discharge. Using four reputable linked administrative databases, the authors found that 46,662 (33%) patients were prescribed a statin within three months of the discharge date (the index date), and 94,825 (67%) were not. About 19% of enrolled patients died within nine months and were excluded from the analysis. Of the eligible patients, propensity-based matching was used to identify 69,168 patients, of whom half were prescribed a statin and half were not. The patients were then analyzed through provincial administrative databases for the end points of hospital admission with an International Classification of Disease (ICD) code of sepsis, severe sepsis, fatal sepsis, death, or the end of the study.
Results: A total of 551 out of 34,584 patients were admitted for sepsis from the statin group, and 667 out of 34,584 were admitted from the control group during a mean follow-up of 2.2 years. The rate of sepsis in the statin group was significantly lower than in the control group (71.2 versus 88.0 per 10,000 person-years; p=0.0003). Statin use was also associated with fewer episodes of sepsis in an extended duration of 3.8 years, and with a lower risk of severe and fatal sepsis where sepsis was the admission diagnosis. This protection was evident at both high and low doses. The hazard ratio for sepsis was .81. There was a 19% relative reduction in the risk of sepsis in patients older than 65 with atherosclerosis. The absolute risk reduction for the occurrence of sepsis per 10,000 person-years was 16.8%, or .168% per person-year, with a corresponding number needed to treat (NNT) of 595 patients to prevent one episode of sepsis per year.
Comments: Though sophisticated and diverse statistical methods were used to assess the robustness of the analysis, this study is retrospective. Unidentified confounders, clinical sepsis risk stratification (the presence of obstructive uropathy or impairments leading to aspiration or skin breakdown, for example) are not accounted for in the analysis. Nonetheless, the hypothesis is of high relevance to hospitalists; it has biologic plausibility, and the results are intriguing if not definitive.
From a practical perspective, it seems prudent to ensure ongoing statin use for all patients with appropriate traditional indications. Initiating statins for the sole purpose of reducing future risk of sepsis is not yet sufficiently supported by the available evidence, and the NNT of almost 600 patients per year in the current study does little to alter that recommendation. In reply to a subsequent letter to the editor, the authors pointed out that the high NNT in part reflects the low-risk profile of the cohort and would be lower in higher risk patients; for example, patients with chronic renal failure, previous infections, or corticosteroid use would have NNTs of 166, 250, and 250, respectively.2 A randomized, controlled prospective trial would be a welcome addition to the evidence on this important topic, as would studies of the use of statins solely as an acute intervention upon suspicion of sepsis.
References
- MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002 Jul 6;360(9326):7-22.
- Hackam DG, Redelmeier DA. Statins and sepsis—authors' reply. Lancet. 2006;367:1651.
Review: Impact of Health Information Technology
Advances in information technology have transformed the world of business and education and will undoubtedly change the delivery and implementation of medical services. What arguably sets the world of health information apart from other systems is, however, the extreme sensitivity of the data involved and the impact it has on human lives.
Methods and data sources: In the article, “Systemic Review: Impact of Health Information Technology on Quality, Efficiency, and Costs of Medical Care,” the authors reviewed four data sources and extracted information on system design, effects on quality and cost benefit analysis. Four data sources were utilized including a MEDLINE analysis of articles indexed as health information technology (HIT) from 1995 to January 2004 utilizing:
- Cochrane Center Registry of Controlled Trials;
- Cochrane Database of Abstracts of Reviews of Effects;
- Periodical Abstracts Database; and
- Studies singled out by experts up to April of 2005
Of the four data sources, 24% of all studies came from the following academic centers: the Regenstrief Institute (Indianapolis), Brigham and Women’s Hospital (Boston), Department of Veterans Affairs, and the Latter Day Saints Hospital/Intermountain Health Care.
Inclusion criteria: The HIT evaluation and efficacy information derived was from these four academic institutions, each with its own EHR (electronic health record) system. Of 4,582 initial articles derived from a title review, 867 were deemed suitable given their title matter, but only 257 met inclusion criteria.
A modified framework from the Institute of Medicine’s six aims for care and a framework to analyze costs developed by the authors themselves was used for analysis.1
Reasons for rejection: Articles that did not have HIT as the subject, others that did not report outcomes data, and those that did not examine barriers for outcomes analysis were rejected.
Information examined: Extracted information on system capabilities including components of the system such as:
- User friendliness;
- Types of systems such as EHR that allowed for medical decision making support and e-prescribing; and
- Functional capabilities such as order entry and clinical documentation.
Common characteristics shared by the HIT systems evaluated by the four academic institutions: they were all multifunctional and included medical decision making support, all were internally developed by research experts and all had capabilities that had been improved upon and added incrementally over time.
The data supported five primary goals:
- Increasing delivery of healthcare according to established protocols and guidelines;
- Enhancing capacity to perform surveillance and monitoring of disease conditions and care delivery;
- Reducing medication error rates;
- Decreasing utilization of care; and
- Producing a mixed effect on time utilization.
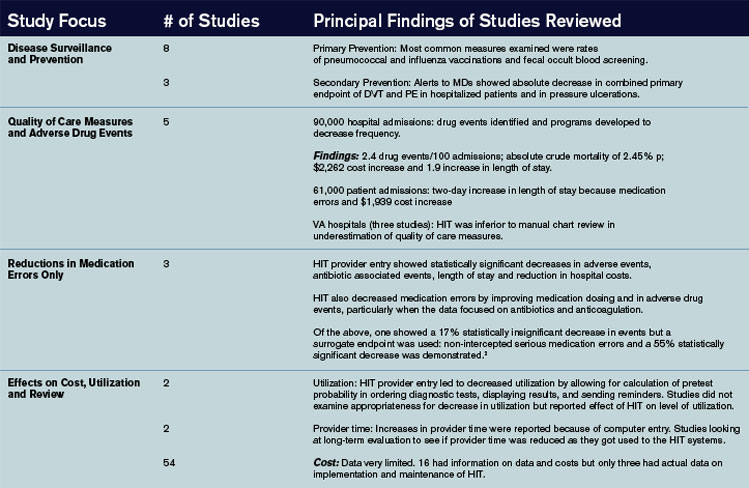
Major findings: (see Figure 1, below).
The authors of the article summarized 22 other studies in Appendix 22 from other institutions. The benefits noted were very similar to those found in the studies from the benchmark institutions; however, one major difference was the use of pre/post time-series designs that did not have a control or comparative group. Internally and commercially, HIT systems were evaluated in most of these studies with thirteen focusing on the former and nine on the later.
Summary and discussion: This study raises several questions worthy of further research and study:
- How are systems to interface with regard to the portability of health care information?
- Which are better: internally devised systems or commercially available systems?
- Who is going to be responsible for establishing standard guidelines for the implementation of HIT systems across the diverse healthcare systems in the United States? and
- How are the data to be used and analyzed by insurers and even public health entities?
HIT has shown many benefits with regard to quality of patient care issues and efficiency. Studies from these four benchmark institutions had one important limitation, however, and that is that the development of an internally developed HIT system took many years and is unlikely to be applicable to other institutions that have fewer resources and are struggling to implement the technology in a timely manner.
As the authors of the article acknowledge, it is not clear if HIT systems, though useful as tools, alter states of disease and health. More research looking at the direct impact of HIT information on morbidity and mortality is needed. As the authors state, this raises the question of a national HIT system, thereby making adoption of HIT a bipartisan initiative.
Providers need better evidence on information systems in order to make informed decisions about acquiring and implementing technology in community settings. The authors of this article made the first attempt to collate and appraise such evidence. Additional research is needed in academic, governmental, and community settings in both acute and nonacute facilities. As the authors point out, a uniform standard should be devised at the federal, state, and local level to report research on the implementation of HIT systems similar to the CONSORT and Quorum statement.
References
- Chaudry B, Wang J, Wu S, et al. Systematic review: impact of health information technology on quality, efficiency and costs of medical care. Ann Intern Med. 2006 May 16;144(10):742-752.
- Bates DW, Leape LL Cullen DJ. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998 Oct 21;280(15):1311-1316.
Gatifloxacin and Dysglycemia
Park-Wyllie LY, Juurlink DN, Kopp A, et al. Outpatient gatifloxacin therapy and dysglycemia in older adults. N Engl J Med. 2006 Mar;354(13):1352-1361.
Fluoroquinolones are the most commonly prescribed antibiotics in the United States. Side effects associated with some fluoroquinolones (temafloxacin, grepafloxacin, sparfloxacin, and trovafloxacin) have prompted their restriction or withdrawal. Until now, dysglycemia had been associated with gatifloxacin only in small studies or case reports.
This study sought to examine, by a nested case control design, the association between gatifloxacin and dysglycemia that required hospital care. The researchers reviewed all prescription records from the Ontario (Canada) Drug Benefit database, which houses complete prescription drug sales for all patients older than age 65 (1.4 million residents). They linked this with a national Canadian database of those same patients’ emergency room visits and hospital admissions. Cases were patients who received hospital care for hypoglycemia (or hyperglycemia) within 30 days of filling an antibiotic prescription (macrolide, cephalosporin, or fluoroquinolone). Controls were patients who had not received hospital care after an antibiotic prescription in the same time period. They were matched by age, gender, whether or not they had been diagnosed as having diabetes, diabetic drug use, and time of antibiotic prescription. Patients were excluded if they turned 65 within the year, had been hospitalized within 90 days, had subsequent hospitalizations for dysglycemia, or had more than one antibiotic in 30 days. Logistic regression was used to determine the odds ratio for the association between dysglycemia and recent antibiotic use. In multivariable analysis, they adjusted for liver disease, renal disease, alcohol use, hospitalizations, physician visits, diabetic and P-450 medications, socioeconomic status, and number of prescription drugs. They were also stratified by diabetes status.
The cases treated for hypoglycemia were four times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 4.3, CI 2.9-6.3). The association was slightly less with levofloxacin (OR 1.5, CI 1.2-2.0), and there was no association of hypoglycemia with moxifloxacin, ciprofloxacin, or cephalosporins. The cases treated for hyperglycemia were 17 times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 16.7, CI 10.4-26.8). There was no association of hyperglycemia with the other fluoroquinolones or cephalosporins. The analyses were similar when stratified by diabetes status. In total, 1.1% of all gatifloxacin treatments were associated with dysglycemia requiring hospital care within 30 days. As to what to do with gatifloxacin, as stated precisely in an accompanying editorial, “For every approved indication for gatifloxacin, there are safer, equally effective, and less costly alternatives.”
Physician Board Certification and Acute MI Quality Measures.
Chen J, Rathore SS, Wang Y, et al. Physician board certification and the care and outcomes of elderly patients with acute myocardial infarction. J Gen Intern Med. 2006 Mar;21(3):238-244.
Board certification may have implications for practicing physicians because there is evidence that both hiring organizations and patients prefer board-certified physicians over non-board certified physicians. However, it is unknown if such certification translates into better quality of patient care.
In this study researchers sought to examine the relationship between physician board certification and quality of care in patients with acute myocardial infarction (AMI). Medical records were abstracted from the Cooperative Cardiovascular Project, a cohort of Medicare beneficiaries hospitalized with AMI. Board certification was obtained from the American Medical Association (AMA) Physician Masterfile, which is reportedly 94% accurate. Quality of care measures included ASA and beta-blocker use at the time of admission and discharge. Researchers also evaluated 30-day and one-year mortality.
They evaluated these quality measures on 101,251 patients and 36,668 physicians, of which 80% were board certified. In multivariable analyses adjusting for patient, hospital, and physician characteristics, board-certified internal medicine and cardiology physicians (but not family practitioners) were more likely to prescribe ASA and beta-blockers at admission and discharge than non-board certified physicians (adjusted relative risk ranged from 1.04 to 1.20). There was no difference in 30-day and one-year mortality among any specialty after multivariable adjustment.
These results, albeit modest, suggest that physician board certification may be associated with superior quality of care in elderly patients with AMI. The authors offer that board-certified physicians may be more aware or familiar with guidelines or may be more likely to agree with clinical guidelines. Although board-certified physicians have been shown to complete more hours of CME and spend more time reading journals, they caution that board certification should not be used as a surrogate marker of quality. Because 30% of U.S. practicing physicians are not currently board certified, these results certainly warrant further study.
PE in COPD
Tillie-Leblond I, Marquette CH, Perez T, et al. Pulmonary embolism in patients with unexplained exacerbation of chronic obstructive pulmonary disease: prevalence and risk factors. Ann Intern Med. 2006 Mar 21;144(6):390-396.
This study sought to evaluate the prevalence and risk factors for pulmonary embolus (PE) in patients with unexplained exacerbations of COPD. All patients with an unexplained COPD exacerbation requiring hospitalization (not ICU) were evaluated for PE by spiral chest CT and lower limb venous ultrasound (USG). The COPD flare was “unexplained” if there were no signs or symptoms of respiratory tract infection, no pneumothorax, or a discrepancy between the clinical/radiologic features and the degree of hypoxemia. Patients were considered to have a PE if either of the two tests (CT or USG) were positive. Patients were not considered to have a PE if both tests were negative, and there was no evidence of PE at three-month follow-up.
Of 211 referred patients, 14 were not included due to inconclusive results or iodine intolerance. Of 197 enrolled patients, 25% had PE. There was no difference between the PE and non-PE groups with respect to referral location, clinical symptoms (dyspnea, pleuritic pain, hemoptysis, tachycardia, lower limb edema), need for long term oxygen therapy, admission P02 or PC02, recent trauma, recent surgery, obesity, or immobilization for more than seven days. Factors associated with PE on bivariate analysis included a decrease in PC02 >5mmHg from baseline, previous thromboembolism, and malignancy.
Researchers then calculated these patient’s Geneva score (a PE predictor score based on age, history, pulse, ABG, and chest X-ray findings. Those with a low probability Geneva score had a 9% incidence of PE, those with an intermediate score had a 47% incidence, and those with a high Geneva score had a 100% incidence.
In conclusion, in this study population of non-ICU patients with unexplained exacerbations of COPD, one in four had evidence of thromboembolic disease. Significant risk ratios between groups were found for patients with a prior history of thromboembolism, malignancy, or a decrease in their baseline PC02. These factors should be weighted heavily in determining which patients with unexplained COPD exacerbations should undergo workup to exclude a PE. The Geneva score also correlated well with PE incidence in this population.
Telithromycin in Asthma Exacerbations
Johnston SL, Blasi FB, Black PN, et al. The effect of telithromycin in acute exacerbations of asthma. New Engl J Med. 2006 Apr 13;354(15):1589-1600.
The use of antibiotics for uncomplicated asthma exacerbations is not currently considered standard of care. This randomized placebo controlled trial was designed to determine if telithromycin (a ketolide, structurally similar to macrolides, with efficacy against mycoplasma and chlamydia pneumonia) improves symptoms and peak flow rates in patients with asthma exacerbations. Researchers enrolled 278 patients age 18 to 55 with a history of asthma (less than six months) with an exacerbation (peak flow <80% and symptoms of wheeze and dyspnea). They excluded those requiring ICU care, smokers, known infection/recent antibiotic use, or regular use of oral steroids. Baseline demographics, pulmonary function, and acute medication use (steroids and beta agonists) were similar between the groups.
Intervention patients received telithromycin 800 mg a day for 10 days. The primary outcome was change in their asthma symptom score (rated on a seven-point scale) and change in their peak flows (recorded every morning for the study duration). Secondary outcomes were clinic pulmonary function tests (PFTs).
The intervention group had a mean decrease in their symptom score of 1.3 versus 1.0 in the placebo group (40% versus 27% reduction, p=.004). There was no difference between the groups in home peak flow measurements. There were statistically significant differences between the groups in clinic PFTs (FEV1, FVC, FEF 25%-75%), although the P values were not adjusted for multiple outcomes. The intervention group had a higher percentage of symptom-free days (16% versus 8%, P=.006). A total of 61% of the patients had serologic evidence of chlamydia or mycoplasma infection. Nausea (seven versus 0) and LFT elevations (two versus 0) were more frequent in the intervention group.
In conclusion, this is the first trial to report a benefit of antibiotic use in uncomplicated asthma exacerbations. This conclusion must be tempered by the underwhelming clinical improvement (1.3 versus 1.0 improvement in symptom scores), lack of peak flow improvement, recent reports of serious hepatotoxicity associated with telithromycin, and the possibility for antibiotic over-prescribing in unrefined patient populations.
Pneumonia Quality and Outcomes by Volume of Care
Lindenauer PK, Behal R, Murray CK, et al. Volume, quality of care, and outcome in pneumonia. Ann Intern Med. 2006 Feb 21;144(4):262-269.
It is widely known that, for many medical conditions and surgical procedures, outcomes are better when delivered by high-volume providers. It is not known if this holds true for patients with community-acquired pneumonia. To determine the association between physician/hospital volume and patient quality/outcomes, researchers utilized data from the Medicare National Pneumonia Quality Improvement Project. They included patients with an ICD9 diagnosis of pneumonia (850 patients were randomly selected from each state) at acute care hospitals with general or family medicine attendings. They excluded patients with no documentation of pneumonia, a normal chest X-ray, age <65, death on day one, comfort measures only, and departure against medical advice or transfer. Each physician and hospital volume were calculated from Medicare Part A claims for the same calendar year and analyzed by quartiles of volume.
Of the 9,741 physicians analyzed (13,480 patients), the median annual number of pneumonia patients was four, nine, 15, and 29 (in quartiles 1-4). Physician volume of care had little or no effect on performance rates of the timing of antibiotics, appropriate initial antibiotic, use of blood cultures, or in-hospital/30-day mortality rates. Low volume providers were significantly more likely to provide pneumococcal and influenza screening.
Of the 3,243 hospitals analyzed, the median annual pneumonia caseload was 57, 142, 262, and 465 (in quartiles 1-4). Hospital volume of care had little or no effect on performance rates of the appropriate initial antibiotic, use of blood cultures, pneumococcal/influenza screening, or in-hospital/30-day mortality rates (after severity of illness adjustment). Low volume centers were significantly more likely to give the first antibiotic within four hours.
In conclusion, volume of care by individual providers and hospital systems does not necessarily translate into better quality outcomes in pneumonia care. This may be partially explained by the challenges that larger medical centers face regarding delivering timely care (in overcrowded emergency rooms) and influencing behavior change (such as with standardized order sets).
By Debra Anoff, MD, assistant professor of medicine, Lucy Guerra, MD, assistant professor of medicine, Bjorn Holmstrom, MD, assistant professor of medicine, Asha Ramsakal, DO, assistant professor of medicine and chief, Richard Gross, MD, FACP, professor of medicine and chief, Division of Internal and Hospital Medicine H. Lee Moffitt Cancer Center and Research Institute, University of South Florida College of Medicine
Risk Factors for Mortality in Neutropenic Cancer Patients
Kuderer, NM, Dale DC, Crawford J, et al. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer. 2006 May 15;106(10):2258-2266.
Background: Neutropenic fever in a cancer patient is considered a medical emergency. Most episodes of febrile neutropenia result in hospital admission with prompt institution of broad spectrum antibiotics. The definition of neutropenia is usually regarded as an absolute neutrophil count (neutrophils plus bands) less than 500 cells/µL. The mortality rate of a cancer patient hospitalized with neutropenic fever ranges from 5 to 11%. There have been numerous small studies looking at risk factors associated with inpatient mortality. However, their small sample size and very select group of patients limit their generalizability to a standard hospitalist practice.
Methods: The authors used a longitudinal discharge database derived from 115 U.S. medical centers—both academic and community-based—in 39 states, looking retrospectively at all adult cancer patients hospitalized for febrile neutropenia between 1995 and 2000. The database included 55,276 hospitalizations and 41,779 patients and was analyzed for length of stay, cost per episode, mortality, and the clinical factors associated with mortality and prolonged hospitalization.
Results: The mortality rate for cancer patients with neutropenic fever averaged 9.5% per hospital. The average mortality rate was 14.3% for leukemia, 8.9% for lymphoma, and 8.0% for solid tumors. Lung cancer had the highest average mortality rate, 13.4%, followed by colorectal cancer at 8.8%, and breast cancer, which had the lowest mortality rate with 3.6%. Moreover, the highest mortality rate, 39.2%, was seen in those patients with a documented infection with invasive aspergillosis, while the rate of mortality for invasive candidiasis was 36.7%, followed by gram-negative bacteremia at 33.9%, pneumonia at 26.5%, and gram-positive bacteremia at 21.2%.
Patients without comorbidities, including common illnesses such as diabetes, congestive heart failure, and renal failure, had an average 2.6 % risk of dying. Those with one comorbidity had a 10.3% risk, and patients with more than one comorbidity had a mortality risk of 21.4%. Multivariate analysis revealed that the odds ratios for inpatient mortality were 3.94 for lung disease, 3.26 for cerebrovascular disease, 3.16 for renal disease, 2.89 for liver disease, 1.94 for pulmonary embolism, and 1.58 for heart disease.
The study also showed that patients hospitalized for longer than 10 days (comprising 35% of all patients) accounted for the majority of overall deaths (65%), overall cost (78%), and overall days spent in the hospital (74%).
Conclusions: The study provided an estimate of inpatient mortality associated with neutropenic fever in cancer patients and highlighted those subgroups as being at heightened risk for death. Important limitations include the retrospective nature of the study, the use of administrative data sets as the primary data source, and a failure to analyze for the duration of neutropenia prior to treatment. The authors’ conclusion that the identified factors may be useful in determining which patients warrant “more aggressive supportive care measures” is plausible, but does not find enough support in the study to warrant general implementation.
Long-Term Value of Electrocardiogram Before Noncardiac Surgery
Jeger RV, Probst C, Arsenic R, et al. Long-term prognostic value of the preoperative 12-lead electrocardiogram before major noncardiac surgery in coronary artery disease. Am Heart J. 2006 Feb;151(2):508-513.
Background: The 12-lead electrocardiogram is commonly utilized as part of the cardiovascular preoperative risk stratification. Certain ECG abnormalities, such as left bundle branch block, Q waves, ST-T abnormalities, arrhythmias, and left ventricular hypertrophy (LVH), have been associated with elevated risk in the perioperative period.1,2 This article prospectively evaluated whether an exhaustive analysis of preoperative ECGs in this population would have long-term predictive validity.
Methods: The study utilized a “predefined” analysis applied retrospectively on data obtained for another study.3,4
The study analyzed 172 patients, all of whom had documented coronary artery disease (CAD) as defined by previous myocardial infarction (MI), prior revascularization, significant stenoses on prior catheterization, ischemia (by dobutamine stress echocardiogram or adenosine thallium imaging), or who were high risk for CAD. High risk required at least two of the following: age over 70, hypertension, diabetes mellitus, prior stroke, exercise intolerance, or a “pathological resting ECG.” These patients were to undergo noncardiac surgery. The primary endpoint was all-cause mortality after two years, and the secondary endpoint was major adverse cardiac events (MACE) after two years. The MACE were defined as nonfatal MI, coronary revascularization, re-hospitalization due to recurrent ischemia, and/or cardiac death.
The ECGs were obtained one day prior to surgery and analyzed using the Minnesota classification. Telephone interviews were done at six, 12, and 24 months to evaluate outcome, and the Swiss Mortality Registry was used to determine cause of death. Analyzed data were adjusted for current beta-blocker use and perioperative ischemia using a sensitivity analysis-like correction that is described briefly in the report.
Results: ST depression (odds ratio [OR] 4.5) and faster heart rate (OR 1.6) were independent predictors of all-cause mortality. Faster heart rate (OR 1.7) was also an independent predictor of MACE.
Commentary: The results of this relatively small study raise awareness of resting tachycardia and ST depression as possible markers for poor perioperative and two-year postoperative outcomes. The latter is already included in risk stratification guidelines5, and the former is of uncertain validity due to possible confounding variables such as anxiety or pain, beta blocker dosing differences, and lack of intra- and postoperative beta blocker usage data which may affect postoperative cardiac morbidity and mortality long after the drugs are stopped.
For hospitalists and other physicians performing cardiac risk stratification for noncardiac surgery patients, the current study does not warrant any change in current practice as recommended in the American College of Cardiology/American Heart Association Guidelines 2002.5 As to whether resting tachycardia should be considered as a predictive ECG criterion in this context, further valid and applicable evidence is needed.
References
- De Bacquer D, De Backer G, Kornitzer M, et al. Prognostic value of ECG findings for total, cardiovascular disease, and coronary heart disease death in men and women. Heart. 1998 Dec;80(6):570-577.
- Tervahauta M, Pekkanen J, Punsar S, et al. Resting electrocardiographic abnormalities as predictors of coronary events and total mortality among elderly men. Am J Med. 1996 Jun;100(6):641-645.
- Filipovic M, Jeger R, Probst C, et al. Heart rate variability and cardiac troponin I are incremental and independent predictors of one-year all-cause mortality after major noncardiac surgery in patients at risk of coronary artery disease. J Am Coll Cardiol. 2003 Nov 19;42(10):1767-76.
- Filipovic M, Jeger RV, Girard T, et al. Predictors of long-term mortality and cardiac events in patients with known or suspected coronary artery disease who survive major noncardiac surgery. Anaesthesia. 2005 Jan;60(1):5-11.
- Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update for perioperative cardiovascular evaluation for noncardiac surgery—executive summary. Circulation. 2002 Mar 12;105(10):1257-1267.
Statins and Cardiovascular Disease
Hackam DG, Mamdani M, Li P, et al. Statins and sepsis in patients with cardiovascular disease: a population-based cohort analysis. Lancet. 2006 Feb 4;367(9508):413-418.
Background: The benefits of statins in secondary prevention of MI and ischemic CVA, as well as in reduction of all-cause mortality and their primary prevention in diabetics, are well documented in the literature.1 The concept of statins reducing subsequent sepsis in humans with atherosclerotic cardiovascular disease (CVD) is relatively new. One hypothesis holds that such an effect may be due to several common pathophysiologic mechanisms of sepsis and CVD: endothelial instability, immune dysregulation, inflammation, and thrombogenesis. Statins have been shown to provide improved outcomes from sepsis in animal studies, and observational studies in humans have raised similar hypotheses. This study attempts to analyze whether statin use in humans is associated with similar benefits regarding prevention of sepsis.
Methods: This was a population-based cohort analysis of 141,487 patients in Ontario, Canada, during the period of time from 1997-2002, who were older than age 65 and had been hospitalized for acute coronary syndrome or ischemic stroke, or had revascularization and survived three months post discharge. Using four reputable linked administrative databases, the authors found that 46,662 (33%) patients were prescribed a statin within three months of the discharge date (the index date), and 94,825 (67%) were not. About 19% of enrolled patients died within nine months and were excluded from the analysis. Of the eligible patients, propensity-based matching was used to identify 69,168 patients, of whom half were prescribed a statin and half were not. The patients were then analyzed through provincial administrative databases for the end points of hospital admission with an International Classification of Disease (ICD) code of sepsis, severe sepsis, fatal sepsis, death, or the end of the study.
Results: A total of 551 out of 34,584 patients were admitted for sepsis from the statin group, and 667 out of 34,584 were admitted from the control group during a mean follow-up of 2.2 years. The rate of sepsis in the statin group was significantly lower than in the control group (71.2 versus 88.0 per 10,000 person-years; p=0.0003). Statin use was also associated with fewer episodes of sepsis in an extended duration of 3.8 years, and with a lower risk of severe and fatal sepsis where sepsis was the admission diagnosis. This protection was evident at both high and low doses. The hazard ratio for sepsis was .81. There was a 19% relative reduction in the risk of sepsis in patients older than 65 with atherosclerosis. The absolute risk reduction for the occurrence of sepsis per 10,000 person-years was 16.8%, or .168% per person-year, with a corresponding number needed to treat (NNT) of 595 patients to prevent one episode of sepsis per year.
Comments: Though sophisticated and diverse statistical methods were used to assess the robustness of the analysis, this study is retrospective. Unidentified confounders, clinical sepsis risk stratification (the presence of obstructive uropathy or impairments leading to aspiration or skin breakdown, for example) are not accounted for in the analysis. Nonetheless, the hypothesis is of high relevance to hospitalists; it has biologic plausibility, and the results are intriguing if not definitive.
From a practical perspective, it seems prudent to ensure ongoing statin use for all patients with appropriate traditional indications. Initiating statins for the sole purpose of reducing future risk of sepsis is not yet sufficiently supported by the available evidence, and the NNT of almost 600 patients per year in the current study does little to alter that recommendation. In reply to a subsequent letter to the editor, the authors pointed out that the high NNT in part reflects the low-risk profile of the cohort and would be lower in higher risk patients; for example, patients with chronic renal failure, previous infections, or corticosteroid use would have NNTs of 166, 250, and 250, respectively.2 A randomized, controlled prospective trial would be a welcome addition to the evidence on this important topic, as would studies of the use of statins solely as an acute intervention upon suspicion of sepsis.
References
- MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002 Jul 6;360(9326):7-22.
- Hackam DG, Redelmeier DA. Statins and sepsis—authors' reply. Lancet. 2006;367:1651.
Review: Impact of Health Information Technology
Advances in information technology have transformed the world of business and education and will undoubtedly change the delivery and implementation of medical services. What arguably sets the world of health information apart from other systems is, however, the extreme sensitivity of the data involved and the impact it has on human lives.
Methods and data sources: In the article, “Systemic Review: Impact of Health Information Technology on Quality, Efficiency, and Costs of Medical Care,” the authors reviewed four data sources and extracted information on system design, effects on quality and cost benefit analysis. Four data sources were utilized including a MEDLINE analysis of articles indexed as health information technology (HIT) from 1995 to January 2004 utilizing:
- Cochrane Center Registry of Controlled Trials;
- Cochrane Database of Abstracts of Reviews of Effects;
- Periodical Abstracts Database; and
- Studies singled out by experts up to April of 2005
Of the four data sources, 24% of all studies came from the following academic centers: the Regenstrief Institute (Indianapolis), Brigham and Women’s Hospital (Boston), Department of Veterans Affairs, and the Latter Day Saints Hospital/Intermountain Health Care.
Inclusion criteria: The HIT evaluation and efficacy information derived was from these four academic institutions, each with its own EHR (electronic health record) system. Of 4,582 initial articles derived from a title review, 867 were deemed suitable given their title matter, but only 257 met inclusion criteria.
A modified framework from the Institute of Medicine’s six aims for care and a framework to analyze costs developed by the authors themselves was used for analysis.1
Reasons for rejection: Articles that did not have HIT as the subject, others that did not report outcomes data, and those that did not examine barriers for outcomes analysis were rejected.
Information examined: Extracted information on system capabilities including components of the system such as:
- User friendliness;
- Types of systems such as EHR that allowed for medical decision making support and e-prescribing; and
- Functional capabilities such as order entry and clinical documentation.
Common characteristics shared by the HIT systems evaluated by the four academic institutions: they were all multifunctional and included medical decision making support, all were internally developed by research experts and all had capabilities that had been improved upon and added incrementally over time.
The data supported five primary goals:
- Increasing delivery of healthcare according to established protocols and guidelines;
- Enhancing capacity to perform surveillance and monitoring of disease conditions and care delivery;
- Reducing medication error rates;
- Decreasing utilization of care; and
- Producing a mixed effect on time utilization.
Major findings: (see Figure 1, below).
The authors of the article summarized 22 other studies in Appendix 22 from other institutions. The benefits noted were very similar to those found in the studies from the benchmark institutions; however, one major difference was the use of pre/post time-series designs that did not have a control or comparative group. Internally and commercially, HIT systems were evaluated in most of these studies with thirteen focusing on the former and nine on the later.
Summary and discussion: This study raises several questions worthy of further research and study:
- How are systems to interface with regard to the portability of health care information?
- Which are better: internally devised systems or commercially available systems?
- Who is going to be responsible for establishing standard guidelines for the implementation of HIT systems across the diverse healthcare systems in the United States? and
- How are the data to be used and analyzed by insurers and even public health entities?
HIT has shown many benefits with regard to quality of patient care issues and efficiency. Studies from these four benchmark institutions had one important limitation, however, and that is that the development of an internally developed HIT system took many years and is unlikely to be applicable to other institutions that have fewer resources and are struggling to implement the technology in a timely manner.
As the authors of the article acknowledge, it is not clear if HIT systems, though useful as tools, alter states of disease and health. More research looking at the direct impact of HIT information on morbidity and mortality is needed. As the authors state, this raises the question of a national HIT system, thereby making adoption of HIT a bipartisan initiative.
Providers need better evidence on information systems in order to make informed decisions about acquiring and implementing technology in community settings. The authors of this article made the first attempt to collate and appraise such evidence. Additional research is needed in academic, governmental, and community settings in both acute and nonacute facilities. As the authors point out, a uniform standard should be devised at the federal, state, and local level to report research on the implementation of HIT systems similar to the CONSORT and Quorum statement.
References
- Chaudry B, Wang J, Wu S, et al. Systematic review: impact of health information technology on quality, efficiency and costs of medical care. Ann Intern Med. 2006 May 16;144(10):742-752.
- Bates DW, Leape LL Cullen DJ. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998 Oct 21;280(15):1311-1316.