News
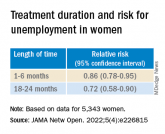
Adherence to ADHD meds may lower unemployment risk
Among women in particular, longer treatment duration was associated with a lower risk of subsequent long-term unemployment.
News
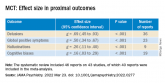
Metacognitive training an effective, durable treatment for schizophrenia
MCT led to improvement in self-esteem and functioning, and all benefits were maintained up to 1 year post intervention.
News
New guidance to optimize antipsychotic treatment
Patients receiving polypharmacy can benefit from TDM because some coprescribed medications can raise or lower antipsychotic blood levels.
News

Domestic violence amid COVID-19: Helping your patients from afar
In the United States, 2,345 calls were placed to the National Domestic Violence Hotline during March 16–April 6, 2020.
News
New ‘atlas’ maps links between mental disorders, physical illnesses
“We found that women with anxiety disorders have a 50% increased risk of developing a heart condition or stroke,” said Dr. John McGrath.