User login
Encountering the Victim of Sexual Assault
Each year in the United States, between 300,000 and 700,000 adult women are estimated to experience sexual assault, with 40,000 of such victims typically seeking treatment in an emergency department (ED).1 In a survey of hospital EDs published in 2008, only 9.6% of the 117 responding hospitals provided to presenting victims of sexual assault all of the following elements of comprehensive medical care management2:
• Acute medical care
•
History and physical examination
•
Acute and long-term rape crisis counseling
•
Prophylactic and therapeutic management for HIV or other sexually transmitted infection (STI)
•
Provision of emergency contraception, with appropriate counseling.2
Specific data from a similar survey included these findings: appropriate, CDC-recommended prophylaxis against STI prescribed in only 6.7% of cases, HIV serology testing in only 13%, and information about follow-up care given to only 31% of patients. Nearly 80% of sexual assault victims treated in the responding hospital EDs received less than optimal care.3,4
In the ED, where victims of sexual assault are most likely to be evaluated, the responsibilities involved in managing the department may hamper emergency physicians’ ability to provide the detailed, time-consuming, one-on-one care such patients require; often, this care is entrusted to an NP or an RN.1 Clinicians in this setting, as well as those who practice in student health, primary care, and women’s health, must be competent in assessing and treating the injuries assaulted patients have sustained, providing STI prophylaxis and pregnancy prevention, collecting forensic evidence in order to facilitate prosecution of the perpetrator, and providing appropriate referrals to promote physical and emotional recovery through counseling and other follow-up care—in short, meeting these patients’ medical, legal, and psychosocial needs.5,6 (See “Specialized Training, a Team Response.”5-7)
DEFINITIONS: RAPE AND SEXUAL ASSAULT
The definition of rape varies from state to state, but three criteria are typically present:
•
Sexual penetration of the victim’s vagina, mouth, or rectum
•
Absence of consent from the victim
• The use or threat of force.8
Sexual assault is a less restrictive term, referring to the sexual contact of one person with another without appropriate consent. Specified manifestations vary state by state but typically include child sexual assault, incest, marital rape, and other forced sexual acts.7
“Julie,” 18, presents to the ED, accompanied by a female friend, after being sexually assaulted by a male student from the college Julie attends. Earlier that evening, Julie was drinking alcohol at a party in the suspect’s apartment. While everyone else was dancing, he invited Julie to his room. She admits that she was willing to “fool around” with him, but when he asked to have intercourse, she said “no.” The suspect insisted that she “wanted it” and proceeded to engage in unprotected intercourse with her. Julie is distressed because she was a virgin until the encounter and had not been using any form of birth control.
On presentation of a victim of sexual assault, local law enforcement and an advocate from the local rape crisis center should be promptly notified; however, the patient’s permission must be obtained before the police department is contacted. A victim may not want to report a sexual assault to the police for a number of reasons, including:
•
A belief that the police are limited in their ability to intervene effectively
•
A perception that victims of sexual assault are often considered at fault
•
Fear that the assailant may assault the victim again
•
Misplaced feelings of fear and shame.5
The NP or PA who performs the initial examination should make every effort to interview the patient while both law enforcement and the advocate are present so that the victim is not required to describe and relive the traumatic situation repeatedly. The advocate is present to support the victim throughout the ED or office visit and evidence collection process; and to provide referrals for follow-up care.
The clinician must strive to remain objective during the evaluation and evidence collection process. For example, the detection of another person’s DNA on the body of the patient is not proof, in and of itself, of that person’s guilt, but only the presence of his or her DNA.9
HISTORY AND PHYSICAL
A thorough medical history and assessment should always be completed, either before or after the forensic examination, depending on the patient’s condition.
Evidence collection is begun by obtaining consent and interviewing the patient. The patient’s account of the assault will guide the practitioner to specific areas of the body where evidence may be found (for example, the case patient said the suspect had kissed her neck, which was swabbed to corroborate her story). Whatever the patient’s age, the presence of a family member or friend is not recommended during the interview, as this could cause the victim to withhold information, and any emotional reaction may be a distraction for the patient. Additionally, having a family member or friend present during the interview process puts that individual at risk for subpoena and court appearance.7
The interview should be concise, with the patient’s account of the assault recorded in some way so that he or she can later be quoted as closely as possible. The clinician should avoid using medical or legal terms or abbreviations, or altering the patient’s own words.
Before the physical examination is begun, the patient’s clothing must be collected and each piece packaged in a separate paper bag. Women’s underpants are the garment most likely to contain “transfer from the perpetrator.”10
Julie had changed her clothes before coming to the ED but was wearing the same underpants she had on at the time of the assault. This garment was collected in a paper bag.
The physical exam is conducted in a head-to-toe manner. Each marking found on the victim must be charted on a diagram of the body or the genitalia (see Figure 1). Injuries should be described using the mnemonic TEARS: tissue integrity, ecchymoses, abrasions, redness, and swelling.11 The most common descriptors include abrasions that are tangential or patterned, fingernail markings, contusions, and lacerations.

When the clinician examines the patient’s genitalia and anal area, it is important to report a thorough description of any injuries. The most common area of injury in the female sexual assault victim is a small tear to the posterior fourchette. Visualization can be enhanced by use of toluidine blue dye—but this must be applied before use of a speculum,12 and not until after any photographs of the outer genitalia have been taken.
Photographs should be taken of all injuries, then presented to the police. It is suggested that each injury be photographed from a medium distance, and up close with a ruler or other scale.7
Julie stated that she had been a virgin prior to the assault. She was placed in the lithotomy position, and a careful internal inspection was performed. Gentle retraction of the labia with a good light source allowed adequate visualization. Photographs were taken of an acute laceration of the hymen at the 5:00 position.
PHYSICAL EVIDENCE
Next, evidence is collected from the patient’s body. Fingernails are clipped and saved for possible DNA from the suspect, especially if the victim reports having tried to fight back. The fingernail trimmings from each hand should be packaged separately, with labels.7
Debris is combed from the head hair and pubic hair. This can be significant for confirming details from the victim’s story, such as being attacked and thrown into the mud. Next, the patient’s head hair is collected. When plucking the hair, the examiner must ensure that the root is intact, since the patient’s DNA is contained therein. This can be important for distinguishing the patient’s hair from that of the suspect. Hairs should be chosen from a few different areas of the patient’s head.7
Oral, genital, and anal swabs are collected. For collection of evidence from a female patient, a speculum exam is required.12 The vagina is swabbed with at least four different cotton swabs: one for the cervix, and the other three to collect visualized secretions.10 For each area, a clean, sterile swab should be moistened with distilled water and used to swab lightly, rotating downward. A dry sterile swab is then used to re-swab the area lightly and lift the DNA. Collected swabs should be allowed to dry completely before the packaging is sealed to minimize the risk for contamination by bacterial growth.
Use of a Wood’s lamp can help the examiner detect semen and saliva on the patient’s body.10 However, a recent examination of alternate light sources with appropriate wavelengths has demonstrated improved detection of trace DNA evidence.13
Once the steps in evidence collection have been completed, the patient can be permitted to urinate, shower, brush his or her teeth, and make any necessary phone calls.
Storing and Protecting the Evidence
It is imperative for the NP or PA who completes the kit to maintain the chain of custody—that is, never leaving the evidence unattended until the police collect it. This will eliminate the possibility of tampering or any other reason for the legal system to designate the evidence as inadmissible. If it is not feasible for the responsible clinician to guard the evidence, it must be placed under lock and key, with limited availability to others.10
Evidence that cannot be thoroughly dried during the examination (eg, tampon, condom, tissues) should be collected in a sterile specimen cup and sent to the crime lab immediately.7 Otherwise, if such a sample is packaged and left to sit, the risk increases for any DNA to become contaminated by bacterial growth.
To verify that the chain of custody was maintained, several items must be signed or initialed by both the provider and the law enforcement officer who receives the kit:
•
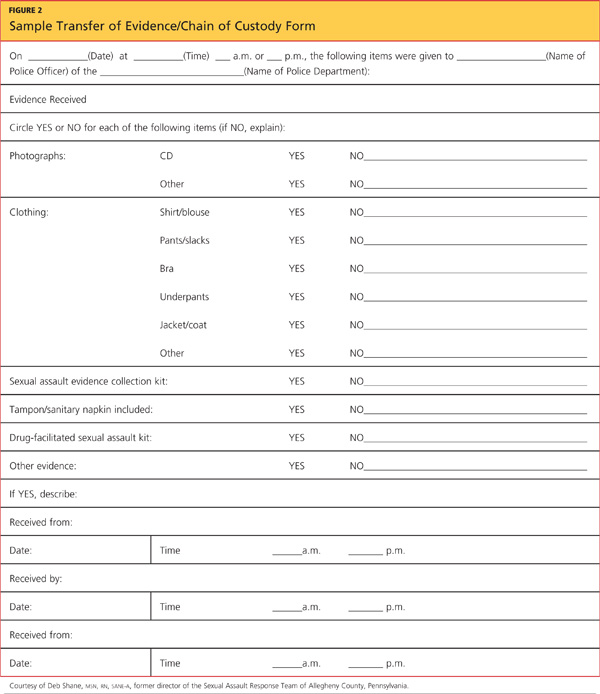
The evidence log sheet. This should be included in the original kit (see Figure 2 for a sample). It should be removed from the kit, completed, and affixed to the outside of the kit before the kit is sealed. A copy of this log should be kept attached to the patient chart.
•
The evidence kit itself. The lid bears a form to be completed by the practitioner.
•
The components of evidence other than the kit (ie, clothing bags, sterile specimen cups containing collected specimens). These bear labels, preprinted with the patient’s name, date of birth, and medical record number, which are signed by the practitioner.
TREATMENT AND
PROPHYLAXIS
The likelihood for a sexual assault victim to have contracted an STI is 26.3%.3 Current recommendations from the CDC,4 including postexposure vaccination against hepatitis B, must be followed for prevention of and treatment for STI. Prophylactic treatment for gonorrhea, chlamydia, and trichomonas should be offered to all victims of sexual assault, as cultures are not taken until patient follow-up at the primary care provider’s office or the county health department.4 Prophylactic treatment for hepatitis B or HIV may be discussed with the patient; he or she must be fully informed about the rigorous follow-up treatment regimens required, as well as the associated adverse effects.
According to the CDC,4 baseline test results for HIV, hepatitis B, and syphilis may be negative, but antibodies can develop over time; thus, reexamination with re-testing should be performed at three months, six months, and 12 months postassault.
Progestin-only emergency contraceptive tablets should be offered through 72 hours postassault to all female sexual assault victims with a negative pregnancy test result in the ED.14
Julie was treated with intramuscular ceftriaxone 250 mg for prevention of gonorrhea, azithromycin 1 g by mouth for prevention of chlamydia, and progestin for pregnancy prevention. She had undergone the hepatitis B vaccination series as a child and had a positive titer drawn before the current school year. Julie declined prophylaxis for HIV because she felt the suspect was at low risk for HIV; however, she was encouraged to undergo HIV testing at her follow-up visit at the local health department.
FOLLOW-UP
Follow-up counseling is a vital component of care for the victim of sexual assault. The police will arrange to ensure the patient’s safety at home before he or she is discharged. A victim of sexual assault should never be discharged if suicidal ideation is evident; in this case, a psychiatry consult must be arranged. For survivors of sexual assault who reside in remote or rural areas, treatment via videoconferencing-based technology has been shown to reduce measures of depression and posttraumatic stress.15
Information regarding rape crisis services should be provided before patients are discharged; the advocate present during the exam should be familiar with services offered in the area. These centers offer emotional support, helpful medical and legal information, and post-rape counseling.7
CONCLUSION
Although the ED is ordinarily the first medical entry point for a sexual assault victim, clinicians in other settings, too, must be prepared to offer medical care to these patients and collect forensic evidence appropriately. Comprehensive care of a sexual assault victim must be completed in a timely and sensitive manner, with documentation that can withstand the exacting requirements of the court system.
REFERENCES
1. Sampsel K, Szobota L, Joyce D, et al. The impact of a sexual assault/domestic violence program on ED care. J Emerg Nurs. 2009;35(4): 282-289.
2. Patel A, Panchal H, Piotrowski ZH, Patel D. Comprehensive medical care for victims of sexual assault: a survey of Illinois hospital emergency departments. Contraception. 2008;77(6):426-430.
3. Straight JD, Heaton PC. Emergency department care for victims of sexual offense. Am J Health Syst Pharm. 2007;64(17):1845-1850.
4. CDC. Sexually transmitted disease treatment guidelines, 2010: sexual assault and STDs (2010). www.cdc.gov/std/treat ment/2010/sexual-assault.htm. Accessed November 26, 2012.
5. Stermac L, Dunlap H, Bainbridge D. Sexual assault services delivered by SANEs. J Forensic Nurs. 2005;1(3):124-128.
6. Plichta SB, Clements PT, Houseman C. Why SANEs matter: models of care for sexual violence victims in the emergency department.
J Forensic Nurs. 2007;3(1):15-23.
7. National Criminal Justice Reference Services. A national protocol for sexual assault medical forensic examinations: adults/adolescents (2004). www.ncjrs.gov/pdffiles1/ovw/206554.pdf. Accessed November 26, 2012.
8. Burgess AW, Hazelwood RR. Victim care services and the Comprehensive Sexual Assault Assessment Tool (CSAAT). In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:47-68.
9. Burg A, Kahn R, Welch K. DNA testing of sexual assault evidence: the laboratory perspective. J Forensic Nurs. 2011;7(3):145-152.
10. Brown K. Forensic examination of sexual assault victims. In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:365-381.
11. Slaughter L, Brown CR, Crowley S, Peck R. Patterns of genital injury in female sexual assault victims. Am J Obstet Gynecol. 1997; 176(3):609-616.
12. Jones JS, Dunnuck C, Rossman L, et al. Significance of toluidine blue positive findings after speculum examination for sexual assault. Am J Emerg Med. 2004;22(3):201-203.
13. Eldredge K, Huggins E, Pugh LC. Alternate light sources in sexual assault examinations: an evidence-based practice project. J Forensic Nurs. 2012;8(1):39-44.
14. Ledray LE. Evidence collection and care of the sexual assault survivor: the SANE/SART response (2001). www.mincava.umn.edu/documents/commissioned/2forensicevidence/2forensicevidence.pdf. Accessed November 26, 2012.
15. Hassija C, Gray MJ. The effectiveness and feasibility of videoconferencing technology to provide evidence-based treatment to rural domestic violence and sexual assault populations. Telemed J E Health. 2011;17(4):30
Each year in the United States, between 300,000 and 700,000 adult women are estimated to experience sexual assault, with 40,000 of such victims typically seeking treatment in an emergency department (ED).1 In a survey of hospital EDs published in 2008, only 9.6% of the 117 responding hospitals provided to presenting victims of sexual assault all of the following elements of comprehensive medical care management2:
• Acute medical care
•
History and physical examination
•
Acute and long-term rape crisis counseling
•
Prophylactic and therapeutic management for HIV or other sexually transmitted infection (STI)
•
Provision of emergency contraception, with appropriate counseling.2
Specific data from a similar survey included these findings: appropriate, CDC-recommended prophylaxis against STI prescribed in only 6.7% of cases, HIV serology testing in only 13%, and information about follow-up care given to only 31% of patients. Nearly 80% of sexual assault victims treated in the responding hospital EDs received less than optimal care.3,4
In the ED, where victims of sexual assault are most likely to be evaluated, the responsibilities involved in managing the department may hamper emergency physicians’ ability to provide the detailed, time-consuming, one-on-one care such patients require; often, this care is entrusted to an NP or an RN.1 Clinicians in this setting, as well as those who practice in student health, primary care, and women’s health, must be competent in assessing and treating the injuries assaulted patients have sustained, providing STI prophylaxis and pregnancy prevention, collecting forensic evidence in order to facilitate prosecution of the perpetrator, and providing appropriate referrals to promote physical and emotional recovery through counseling and other follow-up care—in short, meeting these patients’ medical, legal, and psychosocial needs.5,6 (See “Specialized Training, a Team Response.”5-7)
DEFINITIONS: RAPE AND SEXUAL ASSAULT
The definition of rape varies from state to state, but three criteria are typically present:
•
Sexual penetration of the victim’s vagina, mouth, or rectum
•
Absence of consent from the victim
• The use or threat of force.8
Sexual assault is a less restrictive term, referring to the sexual contact of one person with another without appropriate consent. Specified manifestations vary state by state but typically include child sexual assault, incest, marital rape, and other forced sexual acts.7
“Julie,” 18, presents to the ED, accompanied by a female friend, after being sexually assaulted by a male student from the college Julie attends. Earlier that evening, Julie was drinking alcohol at a party in the suspect’s apartment. While everyone else was dancing, he invited Julie to his room. She admits that she was willing to “fool around” with him, but when he asked to have intercourse, she said “no.” The suspect insisted that she “wanted it” and proceeded to engage in unprotected intercourse with her. Julie is distressed because she was a virgin until the encounter and had not been using any form of birth control.
On presentation of a victim of sexual assault, local law enforcement and an advocate from the local rape crisis center should be promptly notified; however, the patient’s permission must be obtained before the police department is contacted. A victim may not want to report a sexual assault to the police for a number of reasons, including:
•
A belief that the police are limited in their ability to intervene effectively
•
A perception that victims of sexual assault are often considered at fault
•
Fear that the assailant may assault the victim again
•
Misplaced feelings of fear and shame.5
The NP or PA who performs the initial examination should make every effort to interview the patient while both law enforcement and the advocate are present so that the victim is not required to describe and relive the traumatic situation repeatedly. The advocate is present to support the victim throughout the ED or office visit and evidence collection process; and to provide referrals for follow-up care.
The clinician must strive to remain objective during the evaluation and evidence collection process. For example, the detection of another person’s DNA on the body of the patient is not proof, in and of itself, of that person’s guilt, but only the presence of his or her DNA.9
HISTORY AND PHYSICAL
A thorough medical history and assessment should always be completed, either before or after the forensic examination, depending on the patient’s condition.
Evidence collection is begun by obtaining consent and interviewing the patient. The patient’s account of the assault will guide the practitioner to specific areas of the body where evidence may be found (for example, the case patient said the suspect had kissed her neck, which was swabbed to corroborate her story). Whatever the patient’s age, the presence of a family member or friend is not recommended during the interview, as this could cause the victim to withhold information, and any emotional reaction may be a distraction for the patient. Additionally, having a family member or friend present during the interview process puts that individual at risk for subpoena and court appearance.7
The interview should be concise, with the patient’s account of the assault recorded in some way so that he or she can later be quoted as closely as possible. The clinician should avoid using medical or legal terms or abbreviations, or altering the patient’s own words.
Before the physical examination is begun, the patient’s clothing must be collected and each piece packaged in a separate paper bag. Women’s underpants are the garment most likely to contain “transfer from the perpetrator.”10
Julie had changed her clothes before coming to the ED but was wearing the same underpants she had on at the time of the assault. This garment was collected in a paper bag.
The physical exam is conducted in a head-to-toe manner. Each marking found on the victim must be charted on a diagram of the body or the genitalia (see Figure 1). Injuries should be described using the mnemonic TEARS: tissue integrity, ecchymoses, abrasions, redness, and swelling.11 The most common descriptors include abrasions that are tangential or patterned, fingernail markings, contusions, and lacerations.
When the clinician examines the patient’s genitalia and anal area, it is important to report a thorough description of any injuries. The most common area of injury in the female sexual assault victim is a small tear to the posterior fourchette. Visualization can be enhanced by use of toluidine blue dye—but this must be applied before use of a speculum,12 and not until after any photographs of the outer genitalia have been taken.
Photographs should be taken of all injuries, then presented to the police. It is suggested that each injury be photographed from a medium distance, and up close with a ruler or other scale.7
Julie stated that she had been a virgin prior to the assault. She was placed in the lithotomy position, and a careful internal inspection was performed. Gentle retraction of the labia with a good light source allowed adequate visualization. Photographs were taken of an acute laceration of the hymen at the 5:00 position.
PHYSICAL EVIDENCE
Next, evidence is collected from the patient’s body. Fingernails are clipped and saved for possible DNA from the suspect, especially if the victim reports having tried to fight back. The fingernail trimmings from each hand should be packaged separately, with labels.7
Debris is combed from the head hair and pubic hair. This can be significant for confirming details from the victim’s story, such as being attacked and thrown into the mud. Next, the patient’s head hair is collected. When plucking the hair, the examiner must ensure that the root is intact, since the patient’s DNA is contained therein. This can be important for distinguishing the patient’s hair from that of the suspect. Hairs should be chosen from a few different areas of the patient’s head.7
Oral, genital, and anal swabs are collected. For collection of evidence from a female patient, a speculum exam is required.12 The vagina is swabbed with at least four different cotton swabs: one for the cervix, and the other three to collect visualized secretions.10 For each area, a clean, sterile swab should be moistened with distilled water and used to swab lightly, rotating downward. A dry sterile swab is then used to re-swab the area lightly and lift the DNA. Collected swabs should be allowed to dry completely before the packaging is sealed to minimize the risk for contamination by bacterial growth.
Use of a Wood’s lamp can help the examiner detect semen and saliva on the patient’s body.10 However, a recent examination of alternate light sources with appropriate wavelengths has demonstrated improved detection of trace DNA evidence.13
Once the steps in evidence collection have been completed, the patient can be permitted to urinate, shower, brush his or her teeth, and make any necessary phone calls.
Storing and Protecting the Evidence
It is imperative for the NP or PA who completes the kit to maintain the chain of custody—that is, never leaving the evidence unattended until the police collect it. This will eliminate the possibility of tampering or any other reason for the legal system to designate the evidence as inadmissible. If it is not feasible for the responsible clinician to guard the evidence, it must be placed under lock and key, with limited availability to others.10
Evidence that cannot be thoroughly dried during the examination (eg, tampon, condom, tissues) should be collected in a sterile specimen cup and sent to the crime lab immediately.7 Otherwise, if such a sample is packaged and left to sit, the risk increases for any DNA to become contaminated by bacterial growth.
To verify that the chain of custody was maintained, several items must be signed or initialed by both the provider and the law enforcement officer who receives the kit:
•
The evidence log sheet. This should be included in the original kit (see Figure 2 for a sample). It should be removed from the kit, completed, and affixed to the outside of the kit before the kit is sealed. A copy of this log should be kept attached to the patient chart.
•
The evidence kit itself. The lid bears a form to be completed by the practitioner.
•
The components of evidence other than the kit (ie, clothing bags, sterile specimen cups containing collected specimens). These bear labels, preprinted with the patient’s name, date of birth, and medical record number, which are signed by the practitioner.
TREATMENT AND
PROPHYLAXIS
The likelihood for a sexual assault victim to have contracted an STI is 26.3%.3 Current recommendations from the CDC,4 including postexposure vaccination against hepatitis B, must be followed for prevention of and treatment for STI. Prophylactic treatment for gonorrhea, chlamydia, and trichomonas should be offered to all victims of sexual assault, as cultures are not taken until patient follow-up at the primary care provider’s office or the county health department.4 Prophylactic treatment for hepatitis B or HIV may be discussed with the patient; he or she must be fully informed about the rigorous follow-up treatment regimens required, as well as the associated adverse effects.
According to the CDC,4 baseline test results for HIV, hepatitis B, and syphilis may be negative, but antibodies can develop over time; thus, reexamination with re-testing should be performed at three months, six months, and 12 months postassault.
Progestin-only emergency contraceptive tablets should be offered through 72 hours postassault to all female sexual assault victims with a negative pregnancy test result in the ED.14
Julie was treated with intramuscular ceftriaxone 250 mg for prevention of gonorrhea, azithromycin 1 g by mouth for prevention of chlamydia, and progestin for pregnancy prevention. She had undergone the hepatitis B vaccination series as a child and had a positive titer drawn before the current school year. Julie declined prophylaxis for HIV because she felt the suspect was at low risk for HIV; however, she was encouraged to undergo HIV testing at her follow-up visit at the local health department.
FOLLOW-UP
Follow-up counseling is a vital component of care for the victim of sexual assault. The police will arrange to ensure the patient’s safety at home before he or she is discharged. A victim of sexual assault should never be discharged if suicidal ideation is evident; in this case, a psychiatry consult must be arranged. For survivors of sexual assault who reside in remote or rural areas, treatment via videoconferencing-based technology has been shown to reduce measures of depression and posttraumatic stress.15
Information regarding rape crisis services should be provided before patients are discharged; the advocate present during the exam should be familiar with services offered in the area. These centers offer emotional support, helpful medical and legal information, and post-rape counseling.7
CONCLUSION
Although the ED is ordinarily the first medical entry point for a sexual assault victim, clinicians in other settings, too, must be prepared to offer medical care to these patients and collect forensic evidence appropriately. Comprehensive care of a sexual assault victim must be completed in a timely and sensitive manner, with documentation that can withstand the exacting requirements of the court system.
REFERENCES
1. Sampsel K, Szobota L, Joyce D, et al. The impact of a sexual assault/domestic violence program on ED care. J Emerg Nurs. 2009;35(4): 282-289.
2. Patel A, Panchal H, Piotrowski ZH, Patel D. Comprehensive medical care for victims of sexual assault: a survey of Illinois hospital emergency departments. Contraception. 2008;77(6):426-430.
3. Straight JD, Heaton PC. Emergency department care for victims of sexual offense. Am J Health Syst Pharm. 2007;64(17):1845-1850.
4. CDC. Sexually transmitted disease treatment guidelines, 2010: sexual assault and STDs (2010). www.cdc.gov/std/treat ment/2010/sexual-assault.htm. Accessed November 26, 2012.
5. Stermac L, Dunlap H, Bainbridge D. Sexual assault services delivered by SANEs. J Forensic Nurs. 2005;1(3):124-128.
6. Plichta SB, Clements PT, Houseman C. Why SANEs matter: models of care for sexual violence victims in the emergency department.
J Forensic Nurs. 2007;3(1):15-23.
7. National Criminal Justice Reference Services. A national protocol for sexual assault medical forensic examinations: adults/adolescents (2004). www.ncjrs.gov/pdffiles1/ovw/206554.pdf. Accessed November 26, 2012.
8. Burgess AW, Hazelwood RR. Victim care services and the Comprehensive Sexual Assault Assessment Tool (CSAAT). In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:47-68.
9. Burg A, Kahn R, Welch K. DNA testing of sexual assault evidence: the laboratory perspective. J Forensic Nurs. 2011;7(3):145-152.
10. Brown K. Forensic examination of sexual assault victims. In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:365-381.
11. Slaughter L, Brown CR, Crowley S, Peck R. Patterns of genital injury in female sexual assault victims. Am J Obstet Gynecol. 1997; 176(3):609-616.
12. Jones JS, Dunnuck C, Rossman L, et al. Significance of toluidine blue positive findings after speculum examination for sexual assault. Am J Emerg Med. 2004;22(3):201-203.
13. Eldredge K, Huggins E, Pugh LC. Alternate light sources in sexual assault examinations: an evidence-based practice project. J Forensic Nurs. 2012;8(1):39-44.
14. Ledray LE. Evidence collection and care of the sexual assault survivor: the SANE/SART response (2001). www.mincava.umn.edu/documents/commissioned/2forensicevidence/2forensicevidence.pdf. Accessed November 26, 2012.
15. Hassija C, Gray MJ. The effectiveness and feasibility of videoconferencing technology to provide evidence-based treatment to rural domestic violence and sexual assault populations. Telemed J E Health. 2011;17(4):30
Each year in the United States, between 300,000 and 700,000 adult women are estimated to experience sexual assault, with 40,000 of such victims typically seeking treatment in an emergency department (ED).1 In a survey of hospital EDs published in 2008, only 9.6% of the 117 responding hospitals provided to presenting victims of sexual assault all of the following elements of comprehensive medical care management2:
• Acute medical care
•
History and physical examination
•
Acute and long-term rape crisis counseling
•
Prophylactic and therapeutic management for HIV or other sexually transmitted infection (STI)
•
Provision of emergency contraception, with appropriate counseling.2
Specific data from a similar survey included these findings: appropriate, CDC-recommended prophylaxis against STI prescribed in only 6.7% of cases, HIV serology testing in only 13%, and information about follow-up care given to only 31% of patients. Nearly 80% of sexual assault victims treated in the responding hospital EDs received less than optimal care.3,4
In the ED, where victims of sexual assault are most likely to be evaluated, the responsibilities involved in managing the department may hamper emergency physicians’ ability to provide the detailed, time-consuming, one-on-one care such patients require; often, this care is entrusted to an NP or an RN.1 Clinicians in this setting, as well as those who practice in student health, primary care, and women’s health, must be competent in assessing and treating the injuries assaulted patients have sustained, providing STI prophylaxis and pregnancy prevention, collecting forensic evidence in order to facilitate prosecution of the perpetrator, and providing appropriate referrals to promote physical and emotional recovery through counseling and other follow-up care—in short, meeting these patients’ medical, legal, and psychosocial needs.5,6 (See “Specialized Training, a Team Response.”5-7)
DEFINITIONS: RAPE AND SEXUAL ASSAULT
The definition of rape varies from state to state, but three criteria are typically present:
•
Sexual penetration of the victim’s vagina, mouth, or rectum
•
Absence of consent from the victim
• The use or threat of force.8
Sexual assault is a less restrictive term, referring to the sexual contact of one person with another without appropriate consent. Specified manifestations vary state by state but typically include child sexual assault, incest, marital rape, and other forced sexual acts.7
“Julie,” 18, presents to the ED, accompanied by a female friend, after being sexually assaulted by a male student from the college Julie attends. Earlier that evening, Julie was drinking alcohol at a party in the suspect’s apartment. While everyone else was dancing, he invited Julie to his room. She admits that she was willing to “fool around” with him, but when he asked to have intercourse, she said “no.” The suspect insisted that she “wanted it” and proceeded to engage in unprotected intercourse with her. Julie is distressed because she was a virgin until the encounter and had not been using any form of birth control.
On presentation of a victim of sexual assault, local law enforcement and an advocate from the local rape crisis center should be promptly notified; however, the patient’s permission must be obtained before the police department is contacted. A victim may not want to report a sexual assault to the police for a number of reasons, including:
•
A belief that the police are limited in their ability to intervene effectively
•
A perception that victims of sexual assault are often considered at fault
•
Fear that the assailant may assault the victim again
•
Misplaced feelings of fear and shame.5
The NP or PA who performs the initial examination should make every effort to interview the patient while both law enforcement and the advocate are present so that the victim is not required to describe and relive the traumatic situation repeatedly. The advocate is present to support the victim throughout the ED or office visit and evidence collection process; and to provide referrals for follow-up care.
The clinician must strive to remain objective during the evaluation and evidence collection process. For example, the detection of another person’s DNA on the body of the patient is not proof, in and of itself, of that person’s guilt, but only the presence of his or her DNA.9
HISTORY AND PHYSICAL
A thorough medical history and assessment should always be completed, either before or after the forensic examination, depending on the patient’s condition.
Evidence collection is begun by obtaining consent and interviewing the patient. The patient’s account of the assault will guide the practitioner to specific areas of the body where evidence may be found (for example, the case patient said the suspect had kissed her neck, which was swabbed to corroborate her story). Whatever the patient’s age, the presence of a family member or friend is not recommended during the interview, as this could cause the victim to withhold information, and any emotional reaction may be a distraction for the patient. Additionally, having a family member or friend present during the interview process puts that individual at risk for subpoena and court appearance.7
The interview should be concise, with the patient’s account of the assault recorded in some way so that he or she can later be quoted as closely as possible. The clinician should avoid using medical or legal terms or abbreviations, or altering the patient’s own words.
Before the physical examination is begun, the patient’s clothing must be collected and each piece packaged in a separate paper bag. Women’s underpants are the garment most likely to contain “transfer from the perpetrator.”10
Julie had changed her clothes before coming to the ED but was wearing the same underpants she had on at the time of the assault. This garment was collected in a paper bag.
The physical exam is conducted in a head-to-toe manner. Each marking found on the victim must be charted on a diagram of the body or the genitalia (see Figure 1). Injuries should be described using the mnemonic TEARS: tissue integrity, ecchymoses, abrasions, redness, and swelling.11 The most common descriptors include abrasions that are tangential or patterned, fingernail markings, contusions, and lacerations.
When the clinician examines the patient’s genitalia and anal area, it is important to report a thorough description of any injuries. The most common area of injury in the female sexual assault victim is a small tear to the posterior fourchette. Visualization can be enhanced by use of toluidine blue dye—but this must be applied before use of a speculum,12 and not until after any photographs of the outer genitalia have been taken.
Photographs should be taken of all injuries, then presented to the police. It is suggested that each injury be photographed from a medium distance, and up close with a ruler or other scale.7
Julie stated that she had been a virgin prior to the assault. She was placed in the lithotomy position, and a careful internal inspection was performed. Gentle retraction of the labia with a good light source allowed adequate visualization. Photographs were taken of an acute laceration of the hymen at the 5:00 position.
PHYSICAL EVIDENCE
Next, evidence is collected from the patient’s body. Fingernails are clipped and saved for possible DNA from the suspect, especially if the victim reports having tried to fight back. The fingernail trimmings from each hand should be packaged separately, with labels.7
Debris is combed from the head hair and pubic hair. This can be significant for confirming details from the victim’s story, such as being attacked and thrown into the mud. Next, the patient’s head hair is collected. When plucking the hair, the examiner must ensure that the root is intact, since the patient’s DNA is contained therein. This can be important for distinguishing the patient’s hair from that of the suspect. Hairs should be chosen from a few different areas of the patient’s head.7
Oral, genital, and anal swabs are collected. For collection of evidence from a female patient, a speculum exam is required.12 The vagina is swabbed with at least four different cotton swabs: one for the cervix, and the other three to collect visualized secretions.10 For each area, a clean, sterile swab should be moistened with distilled water and used to swab lightly, rotating downward. A dry sterile swab is then used to re-swab the area lightly and lift the DNA. Collected swabs should be allowed to dry completely before the packaging is sealed to minimize the risk for contamination by bacterial growth.
Use of a Wood’s lamp can help the examiner detect semen and saliva on the patient’s body.10 However, a recent examination of alternate light sources with appropriate wavelengths has demonstrated improved detection of trace DNA evidence.13
Once the steps in evidence collection have been completed, the patient can be permitted to urinate, shower, brush his or her teeth, and make any necessary phone calls.
Storing and Protecting the Evidence
It is imperative for the NP or PA who completes the kit to maintain the chain of custody—that is, never leaving the evidence unattended until the police collect it. This will eliminate the possibility of tampering or any other reason for the legal system to designate the evidence as inadmissible. If it is not feasible for the responsible clinician to guard the evidence, it must be placed under lock and key, with limited availability to others.10
Evidence that cannot be thoroughly dried during the examination (eg, tampon, condom, tissues) should be collected in a sterile specimen cup and sent to the crime lab immediately.7 Otherwise, if such a sample is packaged and left to sit, the risk increases for any DNA to become contaminated by bacterial growth.
To verify that the chain of custody was maintained, several items must be signed or initialed by both the provider and the law enforcement officer who receives the kit:
•
The evidence log sheet. This should be included in the original kit (see Figure 2 for a sample). It should be removed from the kit, completed, and affixed to the outside of the kit before the kit is sealed. A copy of this log should be kept attached to the patient chart.
•
The evidence kit itself. The lid bears a form to be completed by the practitioner.
•
The components of evidence other than the kit (ie, clothing bags, sterile specimen cups containing collected specimens). These bear labels, preprinted with the patient’s name, date of birth, and medical record number, which are signed by the practitioner.
TREATMENT AND
PROPHYLAXIS
The likelihood for a sexual assault victim to have contracted an STI is 26.3%.3 Current recommendations from the CDC,4 including postexposure vaccination against hepatitis B, must be followed for prevention of and treatment for STI. Prophylactic treatment for gonorrhea, chlamydia, and trichomonas should be offered to all victims of sexual assault, as cultures are not taken until patient follow-up at the primary care provider’s office or the county health department.4 Prophylactic treatment for hepatitis B or HIV may be discussed with the patient; he or she must be fully informed about the rigorous follow-up treatment regimens required, as well as the associated adverse effects.
According to the CDC,4 baseline test results for HIV, hepatitis B, and syphilis may be negative, but antibodies can develop over time; thus, reexamination with re-testing should be performed at three months, six months, and 12 months postassault.
Progestin-only emergency contraceptive tablets should be offered through 72 hours postassault to all female sexual assault victims with a negative pregnancy test result in the ED.14
Julie was treated with intramuscular ceftriaxone 250 mg for prevention of gonorrhea, azithromycin 1 g by mouth for prevention of chlamydia, and progestin for pregnancy prevention. She had undergone the hepatitis B vaccination series as a child and had a positive titer drawn before the current school year. Julie declined prophylaxis for HIV because she felt the suspect was at low risk for HIV; however, she was encouraged to undergo HIV testing at her follow-up visit at the local health department.
FOLLOW-UP
Follow-up counseling is a vital component of care for the victim of sexual assault. The police will arrange to ensure the patient’s safety at home before he or she is discharged. A victim of sexual assault should never be discharged if suicidal ideation is evident; in this case, a psychiatry consult must be arranged. For survivors of sexual assault who reside in remote or rural areas, treatment via videoconferencing-based technology has been shown to reduce measures of depression and posttraumatic stress.15
Information regarding rape crisis services should be provided before patients are discharged; the advocate present during the exam should be familiar with services offered in the area. These centers offer emotional support, helpful medical and legal information, and post-rape counseling.7
CONCLUSION
Although the ED is ordinarily the first medical entry point for a sexual assault victim, clinicians in other settings, too, must be prepared to offer medical care to these patients and collect forensic evidence appropriately. Comprehensive care of a sexual assault victim must be completed in a timely and sensitive manner, with documentation that can withstand the exacting requirements of the court system.
REFERENCES
1. Sampsel K, Szobota L, Joyce D, et al. The impact of a sexual assault/domestic violence program on ED care. J Emerg Nurs. 2009;35(4): 282-289.
2. Patel A, Panchal H, Piotrowski ZH, Patel D. Comprehensive medical care for victims of sexual assault: a survey of Illinois hospital emergency departments. Contraception. 2008;77(6):426-430.
3. Straight JD, Heaton PC. Emergency department care for victims of sexual offense. Am J Health Syst Pharm. 2007;64(17):1845-1850.
4. CDC. Sexually transmitted disease treatment guidelines, 2010: sexual assault and STDs (2010). www.cdc.gov/std/treat ment/2010/sexual-assault.htm. Accessed November 26, 2012.
5. Stermac L, Dunlap H, Bainbridge D. Sexual assault services delivered by SANEs. J Forensic Nurs. 2005;1(3):124-128.
6. Plichta SB, Clements PT, Houseman C. Why SANEs matter: models of care for sexual violence victims in the emergency department.
J Forensic Nurs. 2007;3(1):15-23.
7. National Criminal Justice Reference Services. A national protocol for sexual assault medical forensic examinations: adults/adolescents (2004). www.ncjrs.gov/pdffiles1/ovw/206554.pdf. Accessed November 26, 2012.
8. Burgess AW, Hazelwood RR. Victim care services and the Comprehensive Sexual Assault Assessment Tool (CSAAT). In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:47-68.
9. Burg A, Kahn R, Welch K. DNA testing of sexual assault evidence: the laboratory perspective. J Forensic Nurs. 2011;7(3):145-152.
10. Brown K. Forensic examination of sexual assault victims. In: Hazelwood RR, Burgess AW, eds. Practical Aspects of Rape Investigation: A Multidisciplinary Approach. 4th ed. Boca Raton, FL: CRC Press; 2009:365-381.
11. Slaughter L, Brown CR, Crowley S, Peck R. Patterns of genital injury in female sexual assault victims. Am J Obstet Gynecol. 1997; 176(3):609-616.
12. Jones JS, Dunnuck C, Rossman L, et al. Significance of toluidine blue positive findings after speculum examination for sexual assault. Am J Emerg Med. 2004;22(3):201-203.
13. Eldredge K, Huggins E, Pugh LC. Alternate light sources in sexual assault examinations: an evidence-based practice project. J Forensic Nurs. 2012;8(1):39-44.
14. Ledray LE. Evidence collection and care of the sexual assault survivor: the SANE/SART response (2001). www.mincava.umn.edu/documents/commissioned/2forensicevidence/2forensicevidence.pdf. Accessed November 26, 2012.
15. Hassija C, Gray MJ. The effectiveness and feasibility of videoconferencing technology to provide evidence-based treatment to rural domestic violence and sexual assault populations. Telemed J E Health. 2011;17(4):30